Embed Size (px)
Citation preview

Journal of Immunological Methods 311 (2006) 81–86www.elsevier.com/locate/jim
Research paper
A screening assay to detect antigen-specific antibodieswithin cerebrospinal fluid
Patricia Morris a, Nicholas W.S. Davies b, Geoffrey Keir a,⁎
a Department of Neuroimmunology, National Hospital for Neurology and Neurosurgery, Queen Square, London, WC1N 3BG, UKb Department of Clinical Neurosciences, Guy's, King's and St Thomas' School of Medicine, London, UK
Received 15 September 2005; received in revised form 16 December 2005; accepted 11 January 2006Available online 24 February 2006
Abstract
Identification of the aetiology of central nervous system infections requires the detection of either the organism or a microbe-specific immune response within the brain or cerebrospinal fluid. We describe a screening assay to detect herpes simplex virus,varicella zoster virus, cytomegalovirus, measles and Toxoplasma gondii specific antibodies in cerebrospinal fluid. Antigen-specificimmunoblotting of oligoclonal IgG and IgM was used to confirm the presence of antibody.
Of 51 consecutive cerebrospinal fluid samples received by the laboratory from patients with suspected central nervous systeminfection 18 (35%) were screen positive for one or more antigen. In only 7 of these were antigen-specific oligoclonal IgG or IgMbands confirmed.
The assay provides a simple, cheap assay to screen for microbial-specific antibody in the cerebrospinal fluid samples of patientswith suspected neurological infections.© 2006 Elsevier B.V. All rights reserved.
Keywords: Antigen-specific; Screen; Oligoclonal bands; Infection; Cerebrospinal fluid
1. Introduction
We describe an assay to screen cerebrospinal fluid(CSF) for antigen-specific antibodies, which is tailoredto assist diagnosis of neurological infections prevalentwithin the United Kingdom. Laboratory confirmation ofcentral nervous system (CNS) infections requires thedetection in tissue or CSF of either the aetiological
Abbreviations: CNS, central nervous system; CSF, cerebrospinalfluid; CMV, cytomegalovirus; HSV, herpes simplex virus; VZV,varicella zoster.⁎ Corresponding author. Tel.: +44 20 7837 3611; fax: +44 20 7837
8553.E-mail address: [email protected] (G. Keir).
0022-1759/$ - see front matter © 2006 Elsevier B.V. All rights reserved.doi:10.1016/j.jim.2006.01.015
microbe or microbe-specific antibody. Whilst moleculartechniques, such as PCR, are routinely used to detect avariety of neurotropic organisms in CSF, the diagnosticsensitivity of these techniques is dependent upon thetime of CSF sampling within the natural history of thedisease (Davies et al., 2005). Thus to diagnose CNSinfections such as herpes simplex virus encephalitis andToxoplasma gondii encephalitis, the combination ofboth PCR and antibody assays applied to CSF is recom-mended (Cinque et al., 1996; Luft and Sivadas, 2004).For other infections, such as subacute sclerosing panen-cephalitis, detection of a microbe-specific antibody inCSF is the test of choice.
Detection of microbe-specific IgM within CSFalone is sufficient to confirm the diagnosis of

82 P. Morris et al. / Journal of Immunological Methods 311 (2006) 81–86
infections such as Japanese encephalitis, where CNSinvolvement occurs at the time of primary infection(Solomon et al., 1998). However, many encephalitidesare caused by microbes, such as herpes simplex virus,which establish latency and cause CNS disease throughreactivation or re-infection. Reactivation or re-infectioncauses a poor IgM response that is not reliable fordiagnostic purposes, therefore microbe-specific IgGassays are utilised. However, in contrast to IgM assays,detection of microbe-specific IgG in CSF alone is notsufficient to confirm involvement of the centralnervous system, as high levels of IgG in CSF canresult from passive transfer from serum. Localisationof the immune response to the CNS can be confirmedby showing that intrathecal synthesis of microbe-specific IgG is present. Demonstration of intrathecalproduction of IgG requires the comparison of IgG inCSF with that in a homologous serum sample. Twotechniques are commonly used to detect antigen-specific IgG in CSF: calculation of specific-antibodyindices and antigen-specific immunoblotting of oligo-clonal IgG (Moyle et al., 1984; Reiber and Lange,1991). Both methods have similar sensitivity andspecificity for the diagnosis of herpes simplexencephalitis (Monteyne et al., 1997).
Whilst these assays are useful in confirmingantigen-specific antibody within CSF they are labourintensive, require replication with multiple differentantigens, and are time consuming. Thus a simple andsensitive assay with a quick turnaround time would behelpful to screen for the presence of antigen-specificantibodies in CSF.
2. Methods
Development and use of the assay utilised sampleincubation manifolds obtained from Hoefer (Amer-sham Biosciences, UK). These are precision-machinedPerspex modules comprising a solid base and amatching lid with milled slots to contain liquidsamples. Cross-contamination between adjacent slotsis prevented by a pair of silicon rubber gaskets, one ofwhich is similarly slotted.
Freeze dried pooled herpes simplex virus (HSV)types 1 and 2, varicella zoster (VZV), cytomegalovirus(CMV), measles and T. gondii complement fixationgrade antigens (all Virion, Switzerland) were usedthroughout development of the assay. Each wasreconstituted in 1mL of deionised water and allowedto stand for 30min, after which they were centrifugedto remove particulates. These solutions formed thestock antigen solutions. For each antigen solution the
total protein concentration was determined by amodified Lowry (Bio-Rad DC Protein Assay) afterreconstitution.
The microbial and control antigens were initiallystudied by Western immunoblot. CSF samplesobtained from patients with diagnosed CNS viralinfections, that were known to possess antigen-specificoligoclonal IgG to the causal microbe, were used todemonstrate specificity of binding to the microbial butnot control antigen.
A common method was used to prepare and developthe nitrocellulose membrane. A 10 by 10cm sheet ofnitrocellulose (Transblot Membrane, Bio-Rad Labora-tories CA, USA) was cut to fit the Hoefer incubationchamber. Using the slotted silicon rubber gasket, thecentre of each slot was marked on the membrane top andbottom. This allowed identification of the positions ofeach antigen on the membrane. The membrane was thenwetted in 0.9% saline, placed on the bottom gasket andthe incubation chamber was re-assembled. A watertightseal to the manifold chamber was confirmed by allowingit to stand for 10min after adding 2mL of 0.9% saline toeach slot. Subsequently the wells were emptied and 2mLeach of a dilution of antigen was then added to the slots.The chamber was then incubated overnight at 4°C on arocker. The following day the antigen solutions weredecanted and all the wells were thoroughly washed with20 changes of tap water. The incubation chamber wasthen disassembled and the membrane removed. After abrief wash with 0.9% saline, the membrane was blockedfor 2h in 2% dried skimmed milk in saline, and thenrinsed in 3changes of 0.9% saline only. Subsequently,the incubation chamber was re-assembled but with themembrane rotated through 90°. Dilutions of CSFs couldnow be added and incubation overnight at 4°C on arocker repeated.
Following incubation the CSF solution was decantedand the membrane washed 20 times with tap water,followed by two changes in 0.9% saline and finally for5min in 2.5mL of 0.2% dried skimmed milk. Afterremoval of the milk solution 2.5mL of 1 /1000 dilutionof horse-radish peroxidase conjugated rabbit anti-humanpan immunoglobulins (Dako Cytomation, Denmark)was added and incubated for 2h at room temperature.The antibody solution was then discarded and the stripswashed in 20 changes of tap water, followed by 3rinsesin 0.9% saline then 3rinses in deionised water. The stripswere then developed using 25mL 4-chloro-1-naphtholcolour reagent (10mg dissolved in 10mL ethanol thenadded to 50mL acetate buffer pH 5.1, with 50μL hy-drogen peroxide added immediately before use) for15min at room temperature. The colour development

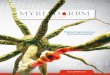
1 in 25 50 100 200 400 800 1600 3200
dilution of CSF
Dilution of antigen (in this case
measles)
1 in… .
800
400
200
100
50
Fig. 1. A typical development matrix used to optimise the amount ofantigen, and the optimum dilution of CSF to use in the screening assay.Varying amounts (expressed as dilutions) of stock antigen solution (Y-axis) and CSF (X-axis) were sequentially applied to a membrane (seetext for details). In the example shown here, using measles antigen, itcan be seen that using antigen at a dilution of 1 /50 allows CSF to betested down to a dilution of 1 in 1600. The decision on which dilutionsto choose is based upon getting a reasonable strength signal, yetconserving the amount of CSF used for screening. In this example wechose to work with an antigen preparation at a dilution of 1 /100 fromstock, and CSF at a dilution of 1 in 100. As discussed in the text wefound a dilution of CSF of 1 /100 worked well for all antigens, and thiswas chosen as the dilution for use throughout. As the working volumefor the screen is 25mL, so usingCSF at a dilution of 1 /100 is equivalentto applying 25μL of neat CSF. Each screen allows us to test for up to 9different antigens.
83P. Morris et al. / Journal of Immunological Methods 311 (2006) 81–86
step required accurate timing. After colour developmentthe membrane was washed thoroughly in severalchanges of tap water, and then dried with warm air.
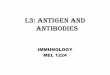
HSV (1+2)
Measles
VZV
CMV
T. carinii
control
1 2 3 4 5 6 Positive: CMV HSV HSV M
Weak positive: HSV HSV HSV
Fig. 2. Example set of screens for 11individual CSF samples; against 5micvaricella zoster virus; CMV: cytomegalovirus; T. carinii: Toxoplasma carinii)do not routinely screen serum; only CSF). Each horizontal track correspondsweak positive (lighter grey square). CSF samples 1, 9 and 10 show reactionsshow reactions to only one antigen. The weak positive result against VZVonscanned image, but is more clearly visible by eye on the original strip. Samplspecific oligoclonal IgG (for examples, see Fig. 3).
Titration studies were performed to ascertain theoptimum antigen concentration for coating the nitro-cellulose membrane as well as CSF dilution for use inthe assay. Dilutions of CSF were made with salinecontaining 0.2% milk and covered the range 1 /25down to 1 /1280. Once the optimal antigen dilutionshad been determined it was then tested against a rangeof CSF samples diluted at a constant value of 1 in100. This led to the selection of 1 /100 dilution for allantigens as acceptable. One lane acted as an assaycontrol and consisted of a lane coated with a 1 /4000dilution of normal human serum. The screening assayrequired the detection of this internal control beforebeing read. Positive results were identified by eye.
The assay was assessed using consecutive CSFsfrom patients with suspected CNS infections receivedby the laboratory. The laboratory performs all CSFanalysis on samples obtained within the hospital. Alltest samples showing a positive result for any antigenwere further investigated by antigen-specific immuno-blotting to demonstrate microbe-specific oligoclonalbands as described by Moyle et al. (1984). Afterisoelectric focusing the CSFs were blotted withmembranes previously coated with either the microbialantigen of interest or control antigen. Antigen-specificIgG or IgM bands were visualised by a colour reactionafter incubation with either goat anti-human IgG orIgM, followed by HRP-conjugated polyclonal rabbitanti-goat antibody. Detection of antigen-specific oli-goclonal IgG or IgM bands was recorded when one ormore bands were identified that were not present onthe control membrane.
7 8 9 10 11 VZV VZV
VZV VZV HSV HSV T. carinii
robial species (HSV: Herpes simplex virus; M: measles virus; VZV:. Each vertical strip (1–11) corresponds to individual CSF samples (weto a specific antigen. Results are divided into positive (dark square) andagainst more than one antigen, whilst samples 2, 3, 5, 6, 7, 8, and 11lane 8 does not show up in the figure due to limitations in sensitivity ofes that show a positive result on this screen are then tested for species-

84 P. Morris et al. / Journal of Immunological Methods 311 (2006) 81–86
3. Results
The titrations of dilutions of both coating antigen andCSF were assessed using checkerboards as illustrated inFig. 1. From checkerboards for each antigen optimumdilutions of antigen were chosen to detect known anti-body-positive CSFs diluted 1 /100. Examples of screen-positive CSFs that were also positive to the same antigenby antigen-specific immunoblotting are illustrated inFig. 2.
To check the false negative rate, 38 unselected CSFsamples were tested. The screen revealed a total of9 positive spots. All 38CSF were also tested foroligoclonal antigen-specific bands by immunoblotting
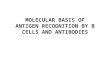
S CSF S CSF S CSF S CSF
Patient: 1 2 3 4
Antigen: Measles VZV
Fig. 3. Representative examples of screen and follow-up antigen-specific owhilst antigen-specific oligoclonal IgG immunoblots (underneath) are CSF anegative measles-specific oligoclonal IgG; Patient 2: positive for measlesshowing an identical pattern of measles-specific bands in both CSF and serumVZV-specific oligoclonal bands in CSF and serum. The serum of patient 3 shalso present in CSF). Patients 5 and 6: both negative for VZV screening, andpositive for HSV on screening, and showing mirrored HSV-specific IgG ban
(Moyle et al., 1984) against all antigens. Oligoclonalantigen-specific immunoblotting showed weak banding(either a mirror pattern or one with more bands in CSFcompared to serum) in only 6 instances. In the otherthree screen-positive spots no antigen-specific bandswere seen. The screening test therefore gave no falsenegative results, but had a false positive rate of 3 /38(∼10%), which is well tolerable when using oligoclo-nal antigen-specific immunoblotting as the final arbiter(Fig. 3).
Table 1 shows the results of the prospective screen ofCSFs from patients with presumed CNS viral infections.Of 51CSF samples screened 18 were positive for 1 ormore antigen. Seven CSF were shown to have antigen-
S CSF S CSF S CSF S CSF
5 6 7 8
VZV HSV
ligoclonal IgG immunoblots. Screening immunoblots (top) CSF only,nd paired serum. Patient 1: negative for measles on screening and alsoon screening and showing positive measles-specific oligoclonal IgG,; Patients 3 and 4: both positive against VZVon screening, and showingows a pattern typical of a monoclonal IgG antibody to VZV (which isalso negative for VZV-specific oligoclonal IgG; Patients 7 and 8: weakds in both CSF and serum.

Table 1Results of CSF microbe-specific antibody assay compared withimmunoblotting results
HSV VZV CMV Measles Toxoplasmagondii
Screen positive a 16 3 3 2 2Immunoblotting b:
IgG positive 5 1 0 1 1IgM positive 2c 0 0 0 0Negative 9 2 3 1 1
a Of 51CSF samples screened in total 18CSFs were positive for oneor more antigen.b Two CSF samples were oligoclonal IgG band positive for two
antigens (one against HSV and VZV, the other for HSV and measles).c One positive and one negative for IgG HSV-specific oligoclonal
bands.
85P. Morris et al. / Journal of Immunological Methods 311 (2006) 81–86
specific IgG or IgM bands. Only 2CSF had IgM anti-gen-specific bands, of which one had accompanyingIgG bands to the same antigen.
4. Discussion
Microbes have varying neurotropic properties thatresult in syndromes of CNS infection ranging fromencephalitis to poliomyelitis and meningitis. In the UKthe aetiology of presumed CNS viral infections has notbe well studied (Davison et al., 2003) but world-wideHSV is thought to be the commonest cause of acutesporadic necrotising encephalitis (Whitley and Roiz-man, 2001). Amongst the immunosuppressed, particu-larly in HIV/AIDS, CMV and the protozoan T. gondiiare frequent causes of opportunistic CNS infection.More recently VZV has been highlighted as causing agreater proportion of CNS viral infections than pre-viously suspected (Koskiniemi et al., 2001). Thus ourscreening assay seeks antibody specific to aetiologiescommon to our target population.
A screening assay should have high sensitivity re-sulting in a low false negative rate and a false positiverate higher than that of the “gold standard” to which it iscompared. The sensitivity of the assay described in thispaper was established by titration with known microbe-specific antibody positive and negative CSFs. Antigen-specific immunoblotting of oligoclonal IgG and IgMwas used as the standard to which the screening assaywas compared. The screen does not incorporate control(cells without virus) and so is prone to false positiveresults. This is acceptable as all samples positive by thescreen were then tested for antigen-specific oligoclonalbands, which include a paired control lane. Hence thescreen has more positive results than the antigen-specific immunoblots.
The assay was further studied by its use on a cohortof CSFs samples from patients with suspected viralCNS infections. The sensitivity of the screening assaywas shown to be higher than the standard as themajority of screen positive samples were shown to beantigen-specific oligoclonal IgG and IgM negative. Fewof the CSFs were positive for antigen-specific oligo-clonal IgM as the CNS infections caused by herpes-viruses and T. gondii are most frequently throughreactivation, or, in the case of measles, as a remotecomplication of primary infection. The study could becriticised as the screen was capable of detectingmicrobe-specific IgA antibodies, which were not soughtby antigen-mediated immunoblot. However, the screen-ing assay was designed to identify viral and protozoalspecific antibody. CNS infections in which theintrathecal humoral response is characterised bymicrobe-specific IgA predominating over IgG or IgMare typically bacterial (Reiber and Peter, 2001). Suchaetiologies include Mycobacterium tuberculosis, Neis-seria meningitidis, and Streptococcus pneumoniae —microbes not sought by the screen.
The assay is simple, inexpensive and has a turn-around time of 24h. An internal control ensures thataddition of the appropriate anti-sera and colour de-veloper has been undertaken. Furthermore, by cutting acoated membrane into strips 5mm wide perpendicular tothe direction of coating, individual CSFs may be tested.This reduces assay turnaround time, as samples nolonger need to be batched into groups of 10. We havefound that the coated membrane strips after being air-dried and stored at −20°C in a sealed plastic bag arestable for at least 6months.
The assay could be adapted to screen for otherantibody, specific to microbes endemic in the area ofuse, such as flaviviruses in North America or Asia.From the cohort of CSFs from patients with suspectedCNS infection 65% were screen negative. Thus theassay can limit resource expenditure by reducingthe number of target antigens for which antigen-specific immunoblotting of oligoclonal IgG and IgMis performed.
Whilst a positive result cannot be used withcertainty to predict the presence of the screened forantigen-specific oligoclonal IgG or IgM, the assaycan provide a quick negative result. A timely negativeresult, combined with clinical information regardingthe time of CSF sampling, could aid the physician inguiding the diagnostic process when a CNS infec-tion is suspected. A positive result will informchoice of antigen for definitive CSF specific-antibodystudies.

86 P. Morris et al. / Journal of Immunological Methods 311 (2006) 81–86
References
Cinque, P., Cleator, G.M., Weber, T., Monteyne, P., Sindic, C.J., vanLoon, A.M., 1996. The role of laboratory investigation in thediagnosis and management of patients with suspected herpessimplex encephalitis: a consensus report. The EU ConcertedAction on Virus Meningitis and Encephalitis. J. Neurol. Neuro-surg. Psychiatry 61, 339.
Davies, N.W., Brown, L.J., Gonde, J., Irish, D., Robinson, R.O., Swan,A.V., Banatvala, J., Howard, R.S., Sharief, M.K., Muir, P., 2005.Factors influencing PCR detection of viruses in cerebrospinal fluidof patients with suspected CNS infections. J. Neurol. Neurosurg.Psychiatry 76, 82.
Davison, K.L., Crowcroft, N.S., Ramsay, M.E., Brown, D.W.,Andrews, N.J., 2003. Viral encephalitis in England, 1989–1998:what did we miss? Emerg. Infect. Dis. 9, 234.
Koskiniemi, M., Rantalaiho, T., Piiparinen, H., von Bonsdorff, C.H.,Farkkila, M., Jarvinen, A., Kinnunen, E., Koskiniemi, S.,Mannonen, L., Muttilainen, M., Linnavuori, K., Porras, J.,Puolakkainen, M., Raiha, K., Salonen, E.M., Ukkonen, P., Vaheri,A., Valtonen, V., 2001. Infections of the central nervous system ofsuspected viral origin: a collaborative study from Finland.J. Neurovirology 7, 400.
Luft, B.J., Sivadas, R., 2004. Toxoplasmosis. In: Scheld, W.M.,Whitley, R.J.,Marra, C.M. (Eds.), Infections of the Central NervousSystem. Lippincott Williams & Wilkins, Philadelphia, p. 755.
Monteyne, P., Albert, F., Weissbrich, B., Zardini, E., Ciardi, M.,Cleator, G.M., Sindic, C.J., 1997. The detection of intrathecalsynthesis of anti-herpes simplex IgG antibodies: comparisonbetween an antigen-mediated immunoblotting technique andantibody index calculations. European Union Concerted Actionon Virus Meningitis and Encephalitis. J. Med. Virol. 53, 324.
Moyle, S., Keir, G., Thompson, E.J., 1984. Viral immunoblotting: asensitive method for detecting viral-specific oligoclonal bands inunconcentrated cerebrospinal fluid. Biosci. Rep. 4, 505.
Reiber, H., Lange, P., 1991. Quantification of virus-specific antibodiesin cerebrospinal fluid and serum: sensitive and specific detection ofantibody synthesis in brain. Clin. Chem. 37, 1153.
Reiber, H., Peter, J.B., 2001. Cerebrospinal fluid analysis: disease-related data patterns and evaluation programs. J. Neurol. Sci. 184,101.
Solomon, T., Thao, L.T., Dung, N.M., Kneen, R., Hung, N.T., Nisalak,A., Vaughn, D.W., Farrar, J., Hien, T.T., White, N.J., Cardosa, M.J.,1998. Rapid diagnosis of Japanese encephalitis by using animmunoglobulin M dot enzyme immunoassay. J. Clin. Microbiol.36, 2030.
Whitley, R.J., Roizman, B., 2001. Herpes simplex virus infections.Lancet 357, 1513.