Embed Size (px)
Citation preview
REVIEW ARTICLE
A Review of Three-Dimensional Printingin Tissue Engineering
Nick A. Sears, BS, MS, Dhruv R. Seshadri, BS, Prachi S. Dhavalikar, BS,and Elizabeth Cosgriff-Hernandez, BS, PhD
Recent advances in three-dimensional (3D) printing technologies have led to a rapid expansion of applicationsfrom the creation of anatomical training models for complex surgical procedures to the printing of tissueengineering constructs. In addition to achieving the macroscale geometry of organs and tissues, a print layerthickness as small as 20mm allows for reproduction of the microarchitectures of bone and other tissues.Techniques with even higher precision are currently being investigated to enable reproduction of smaller tissuefeatures such as hepatic lobules. Current research in tissue engineering focuses on the development of com-patible methods (printers) and materials (bioinks) that are capable of producing biomimetic scaffolds. In thisreview, an overview of current 3D printing techniques used in tissue engineering is provided with an emphasison the printing mechanism and the resultant scaffold characteristics. Current practical challenges and technicallimitations are emphasized and future trends of bioprinting are discussed.
Introduction
T issue engineers attempt to harness the body’s abilityto regenerate damaged tissue by combining cells and
bioactive factors in a biomaterial scaffold.1,2 This strategytypically involves the combination of cells and bioactivefactors with a biomaterial scaffold to form an implantableconstruct that can replace or restore physiological func-tion.2–4 Ideally, the scaffold will be resorbed as the neotissueis formed, resulting in a functional tissue replacement afterremodeling is complete.5 Biomaterial scaffolds are chosento mimic important aspects of the target tissue to restorefunction and provide an environment conducive to celldifferentiation and proliferation. There is a continued em-phasis on enhancing the function of tissue-engineered con-structs through the development of improved fabricationmethods.6–9
Traditional techniques for fabricating tissue engineeringscaffolds such as gas foaming, solvent casting, fiber bond-ing, phase separation, particulate leaching, and freeze dryingprovide macroscale scaffold features but often lack thecomplexity of native tissue.5 Many tissues, such as thelobules of the liver or nephrons of the kidney, have complexstructural units that coordinate multiple types of specializedcells and are critical for tissue function. Fabrication methodsthat can produce complex geometries have a distinct ad-vantage in their ability to fit an irregular defect site but arealso capable of mimicking tissue complexity through theprecise positioning of multiple materials and cell types.10
Scaffolds that re-create macroscale properties as well as mi-croscale features necessary for cellular function require sophis-ticated control over fabrication. Recently, three-dimensional(3D) fabrication or rapid-prototyping technologies have becomemore popular and accessible, allowing for exploration of newfabrication techniques capable of geometric accuracy at themacroscale and microscale. Precision at this level opens the doorfor innumerable approaches for tissue engineering scaffolds.
Recently, 3D printing has been used to treat a potentiallylife-threatening condition, in which the trachea is prone tocollapse, known as tracheomalacia. Researchers developed a3D-printed tracheal splint made from biodegradable poly(e-caprolactone) (PCL) for a 2-month-old child who requiredendotracheal intubation to sustain ventilation. The splintwas tested in piglets and subsequently given approval forimplantation through an emergency-use exemption. Animmediate improvement was seen after surgery, and patencywas retained after 1 year with no complications.11 In anotherexample, high-definition imaging and 3D printing technol-ogy known as laser sintering were used to create a functionaljawbone replacement for an 83-year-old woman sufferingfrom a lower jaw infection.12 Rapid manufacturing of thejaw implant allowed for creation of ‘‘articulated joints,cavities that foster muscle attachment, and grooves to guidenerve and vein regrowth’’ as well as reduced surgicalpreparation and recovery.
This control over microarchitecture allows for productionof functional tissue-engineered scaffolds that recapitulatethe natural form and function of the tissue. In addition,
Department of Biomedical Engineering, Texas A&M University, College Station, Texas.
TISSUE ENGINEERING: Part BVolume 22, Number 4, 2016ª Mary Ann Liebert, Inc.DOI: 10.1089/ten.teb.2015.0464
298
designed vasculature may enable the creation of larger,cellularized constructs by providing the requisite nutrienttransport for tissue growth.13–16 Functional tissue constructscould also be used as a diagnostic tool for cell-based assaysfor drug testing or other therapies. For example, Organovo’sexVive3D� Liver is a fully functional bioprinted humantissue that has been used to provide toxicity assessment thatis supplementing in vitro and preclinical animal testing.17
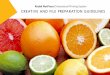
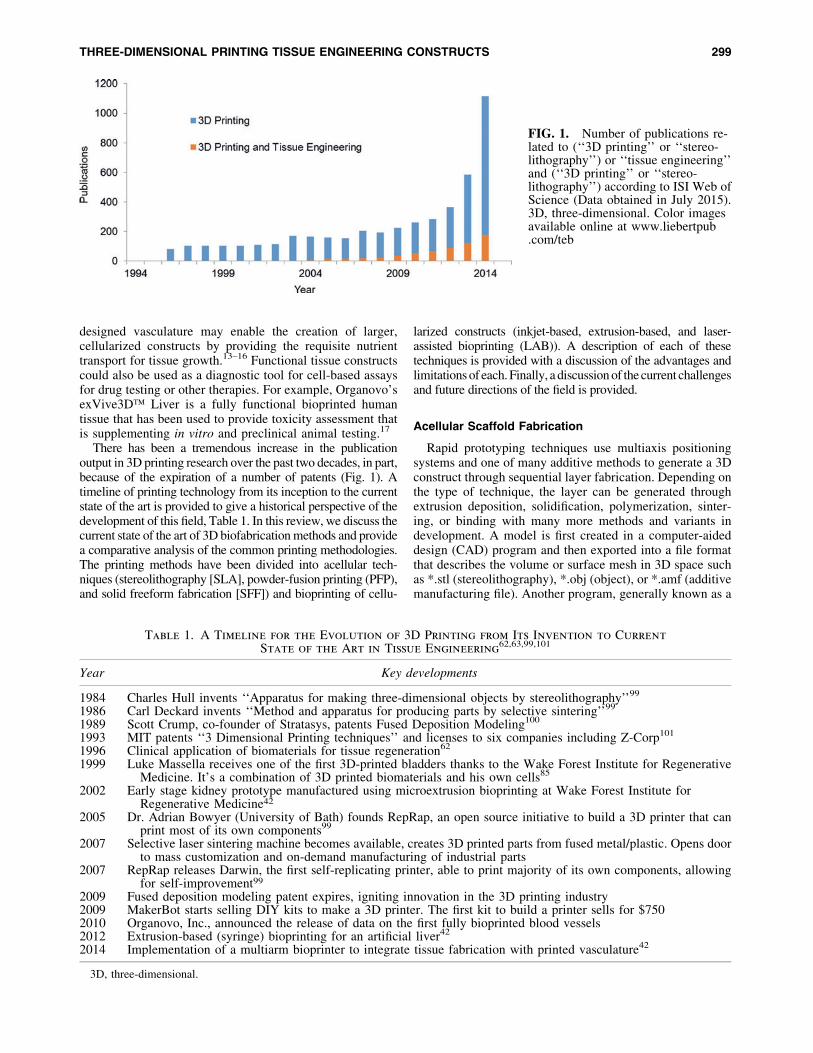
There has been a tremendous increase in the publicationoutput in 3D printing research over the past two decades, in part,because of the expiration of a number of patents (Fig. 1). Atimeline of printing technology from its inception to the currentstate of the art is provided to give a historical perspective of thedevelopment of this field, Table 1. In this review, we discuss thecurrent state of the art of 3D biofabrication methods and providea comparative analysis of the common printing methodologies.The printing methods have been divided into acellular tech-niques (stereolithography [SLA], powder-fusion printing (PFP),and solid freeform fabrication [SFF]) and bioprinting of cellu-
larized constructs (inkjet-based, extrusion-based, and laser-assisted bioprinting (LAB)). A description of each of thesetechniques is provided with a discussion of the advantages andlimitations of each. Finally, a discussion of the current challengesand future directions of the field is provided.
Acellular Scaffold Fabrication
Rapid prototyping techniques use multiaxis positioningsystems and one of many additive methods to generate a 3Dconstruct through sequential layer fabrication. Depending onthe type of technique, the layer can be generated throughextrusion deposition, solidification, polymerization, sinter-ing, or binding with many more methods and variants indevelopment. A model is first created in a computer-aideddesign (CAD) program and then exported into a file formatthat describes the volume or surface mesh in 3D space suchas *.stl (stereolithography), *.obj (object), or *.amf (additivemanufacturing file). Another program, generally known as a
FIG. 1. Number of publications re-lated to (‘‘3D printing’’ or ‘‘stereo-lithography’’) or ‘‘tissue engineering’’and (‘‘3D printing’’ or ‘‘stereo-lithography’’) according to ISI Web ofScience (Data obtained in July 2015).3D, three-dimensional. Color imagesavailable online at www.liebertpub.com/teb
Table 1. A Timeline for the Evolution of 3D Printing from Its Invention to Current
State of the Art in Tissue Engineering62,63,99,101
Year Key developments
1984 Charles Hull invents ‘‘Apparatus for making three-dimensional objects by stereolithography’’99
1986 Carl Deckard invents ‘‘Method and apparatus for producing parts by selective sintering’’99
1989 Scott Crump, co-founder of Stratasys, patents Fused Deposition Modeling100
1993 MIT patents ‘‘3 Dimensional Printing techniques’’ and licenses to six companies including Z-Corp101
1996 Clinical application of biomaterials for tissue regeneration62
1999 Luke Massella receives one of the first 3D-printed bladders thanks to the Wake Forest Institute for RegenerativeMedicine. It’s a combination of 3D printed biomaterials and his own cells85
2002 Early stage kidney prototype manufactured using microextrusion bioprinting at Wake Forest Institute forRegenerative Medicine42
2005 Dr. Adrian Bowyer (University of Bath) founds RepRap, an open source initiative to build a 3D printer that canprint most of its own components99
2007 Selective laser sintering machine becomes available, creates 3D printed parts from fused metal/plastic. Opens doorto mass customization and on-demand manufacturing of industrial parts
2007 RepRap releases Darwin, the first self-replicating printer, able to print majority of its own components, allowingfor self-improvement99
2009 Fused deposition modeling patent expires, igniting innovation in the 3D printing industry2009 MakerBot starts selling DIY kits to make a 3D printer. The first kit to build a printer sells for $7502010 Organovo, Inc., announced the release of data on the first fully bioprinted blood vessels2012 Extrusion-based (syringe) bioprinting for an artificial liver42
2014 Implementation of a multiarm bioprinter to integrate tissue fabrication with printed vasculature42
3D, three-dimensional.
THREE-DIMENSIONAL PRINTING TISSUE ENGINEERING CONSTRUCTS 299
‘‘slicer,’’ is then used to translate the 3D data into slices tobe patterned by the printer. The user can configure the al-gorithm that determines the pattern used to fill the layers andthe program calculates necessary parameters such as ex-trusion speed, cure time, or laser speed to accurately fill thepattern. Early use of these techniques was adapted for moldcasting, product development, and functional prototypes.Rapid development of these technologies has increasedversatility and precision. Current techniques have the abilityto create scaffolds that recapitulate the macroscale geometryof organs, and a print layer thickness as small as 20 mmallows for reproduction of the microarchitectures of boneand other tissues.
Techniques with even higher precision are currently beinginvestigated to enable reproduction of smaller tissue featuressuch as hepatic lobules and kidney nephrons. Despite theexpanding number of rapid prototyping techniques andvariants that have emerged, categories can be used to groupthese techniques based on the material type and method usedto combine each layer. Herein, we compare and contrastthree commonly used techniques: SLA, PFP, and SFF. A
summary of key comparisons of these three methods isprovided in Table 2.
Stereolithography
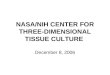
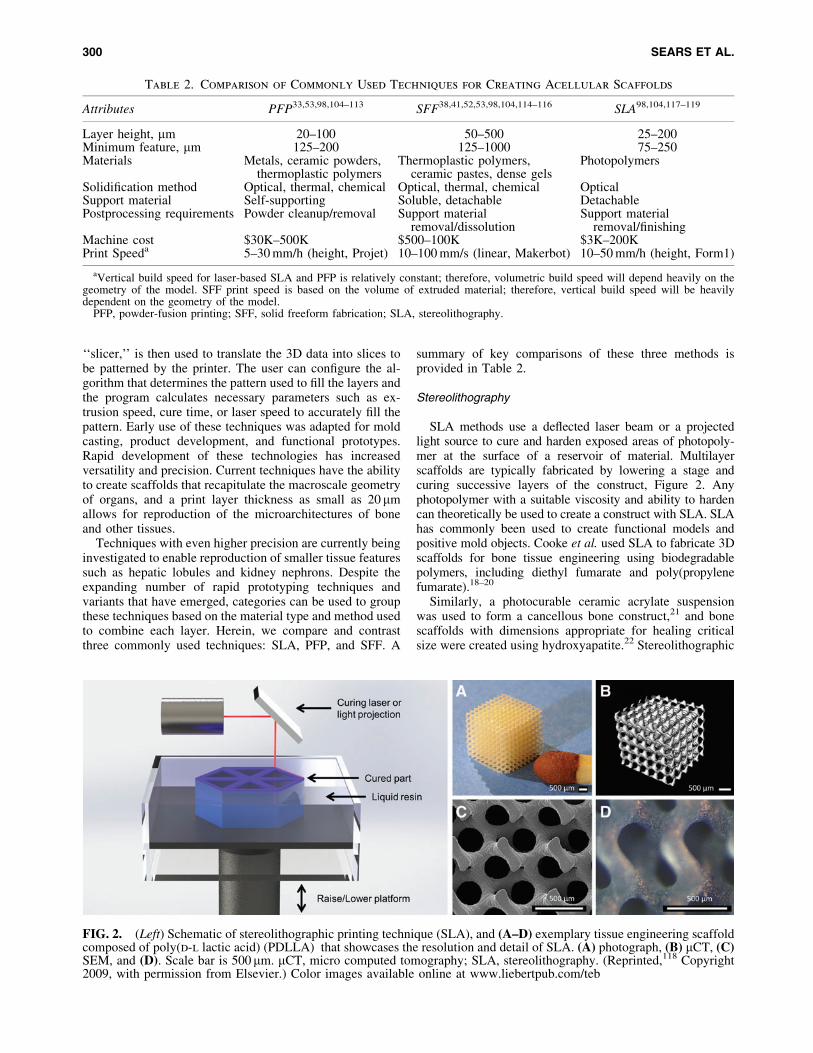
SLA methods use a deflected laser beam or a projectedlight source to cure and harden exposed areas of photopoly-mer at the surface of a reservoir of material. Multilayerscaffolds are typically fabricated by lowering a stage andcuring successive layers of the construct, Figure 2. Anyphotopolymer with a suitable viscosity and ability to hardencan theoretically be used to create a construct with SLA. SLAhas commonly been used to create functional models andpositive mold objects. Cooke et al. used SLA to fabricate 3Dscaffolds for bone tissue engineering using biodegradablepolymers, including diethyl fumarate and poly(propylenefumarate).18–20
Similarly, a photocurable ceramic acrylate suspensionwas used to form a cancellous bone construct,21 and bonescaffolds with dimensions appropriate for healing criticalsize were created using hydroxyapatite.22 Stereolithographic
Table 2. Comparison of Commonly Used Techniques for Creating Acellular Scaffolds
Attributes PFP33,53,98,104–113 SFF38,41,52,53,98,104,114–116 SLA98,104,117–119
Layer height, mm 20–100 50–500 25–200Minimum feature, mm 125–200 125–1000 75–250Materials Metals, ceramic powders,
thermoplastic polymersThermoplastic polymers,
ceramic pastes, dense gelsPhotopolymers
Solidification method Optical, thermal, chemical Optical, thermal, chemical OpticalSupport material Self-supporting Soluble, detachable DetachablePostprocessing requirements Powder cleanup/removal Support material
removal/dissolutionSupport material
removal/finishingMachine cost $30K–500K $500–100K $3K–200KPrint Speeda 5–30 mm/h (height, Projet) 10–100 mm/s (linear, Makerbot) 10–50 mm/h (height, Form1)
aVertical build speed for laser-based SLA and PFP is relatively constant; therefore, volumetric build speed will depend heavily on thegeometry of the model. SFF print speed is based on the volume of extruded material; therefore, vertical build speed will be heavilydependent on the geometry of the model.
PFP, powder-fusion printing; SFF, solid freeform fabrication; SLA, stereolithography.
FIG. 2. (Left) Schematic of stereolithographic printing technique (SLA), and (A–D) exemplary tissue engineering scaffoldcomposed of poly(d-l lactic acid) (PDLLA) that showcases the resolution and detail of SLA. (A) photograph, (B) mCT, (C)SEM, and (D). Scale bar is 500mm. mCT, micro computed tomography; SLA, stereolithography. (Reprinted,118 Copyright2009, with permission from Elsevier.) Color images available online at www.liebertpub.com/teb
300 SEARS ET AL.
techniques are limited in resolution by the diameter of thelaser beam to *250mm, although other methods such assmall-spot laser systems and digital light processing pro-jection have produced features as small as 70 mm.23 SLAtechniques can also be used to create hydrogel scaffoldsfrom natural and synthetic polymers that swell in water andare substantially less rigid than traditional SLA constructs.Hydrogels have become increasingly popular as tissue en-gineering biomaterials because of their high water contentand mechanics similar to soft tissue. Yu and Ober created 2-hydroxyethyl methacrylate scaffolds using photolithographyto create patterns from nonswollen prepolymer, which werethen hydrated and seeded with cells.24
However, one significant limitation with this technique isthat the geometric fidelity of the construct may be compro-mised by rehydration. Matsuda and Magoshi were able tomitigate the swelling effects by using formulations of vinyl-modified polysaccharides and acrylate-modified polyethyleneglycol (PEG).25 Due to the natural biocompatibility of PEGsolutions, researchers have been able to photopattern scaffoldsusing hydrogel solutions that incorporate living cells, as dis-cussed in a later section. Stereolithographic techniques havealso been used to create molds that are used to cast negativereplicas of the printed molds. Chu and colleagues reported aprinted mold of a mandible that was generated using a CADprogram and data from computed tomography imaging. Themold was filled with a hydroxyapatite/acrylate mixture andheated to cure the scaffold, while incinerating the mold. Theresult was a hydroxyapatite scaffold containing internal chan-nels of designed geometries.26 The scaffolds were then im-planted in mini pigs and shown to induce bone ingrowth over a9-week study.27
Overall, SLA is a versatile technique that is attractive forcreating tissue engineering scaffolds because of its precisionand the increasing availability of biologically relevantphotopolymers. The high resolution of this technique, layersas small as 20mm, is unmatched by other 3D printingtechniques. The high vertical resolution and small featuresize capabilities provide exceptional control over the mi-croarchitecture; however, the macromers available typicallyhave limited biocompatibility and constructs are limited toone material without sophisticated apparatuses.28,29
Powder-fusion printing
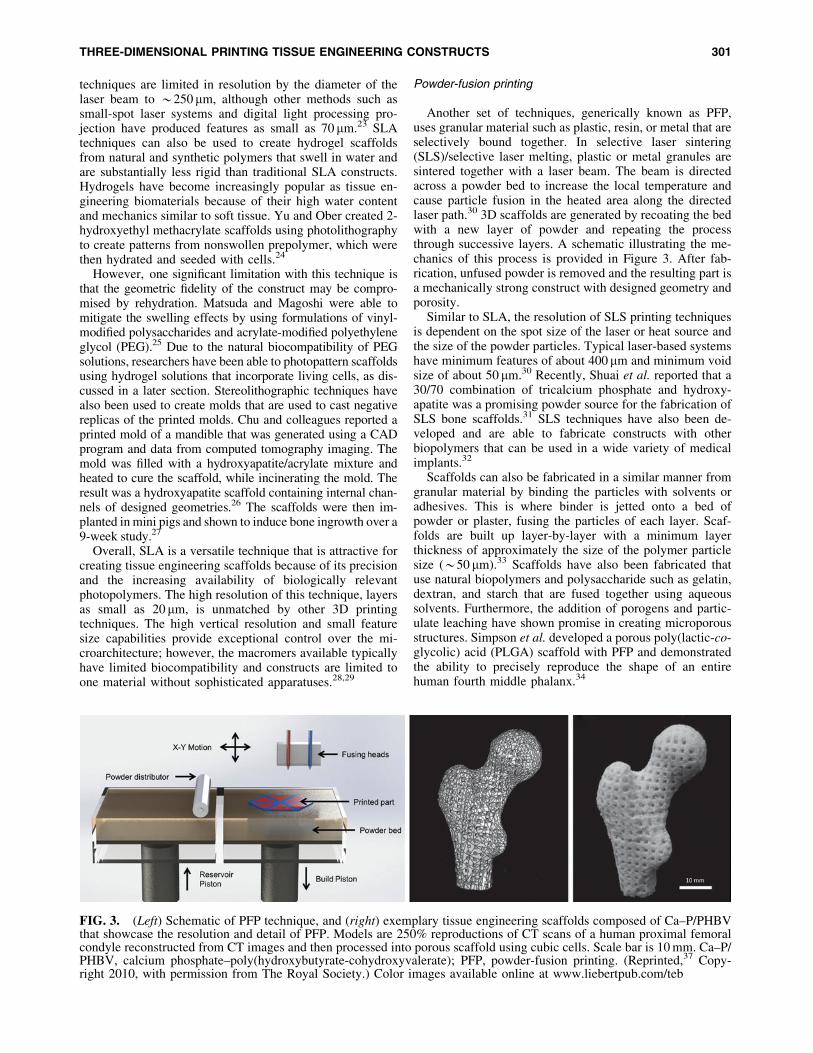
Another set of techniques, generically known as PFP,uses granular material such as plastic, resin, or metal that areselectively bound together. In selective laser sintering(SLS)/selective laser melting, plastic or metal granules aresintered together with a laser beam. The beam is directedacross a powder bed to increase the local temperature andcause particle fusion in the heated area along the directedlaser path.30 3D scaffolds are generated by recoating the bedwith a new layer of powder and repeating the processthrough successive layers. A schematic illustrating the me-chanics of this process is provided in Figure 3. After fab-rication, unfused powder is removed and the resulting part isa mechanically strong construct with designed geometry andporosity.
Similar to SLA, the resolution of SLS printing techniquesis dependent on the spot size of the laser or heat source andthe size of the powder particles. Typical laser-based systemshave minimum features of about 400mm and minimum voidsize of about 50 mm.30 Recently, Shuai et al. reported that a30/70 combination of tricalcium phosphate and hydroxy-apatite was a promising powder source for the fabrication ofSLS bone scaffolds.31 SLS techniques have also been de-veloped and are able to fabricate constructs with otherbiopolymers that can be used in a wide variety of medicalimplants.32
Scaffolds can also be fabricated in a similar manner fromgranular material by binding the particles with solvents oradhesives. This is where binder is jetted onto a bed ofpowder or plaster, fusing the particles of each layer. Scaf-folds are built up layer-by-layer with a minimum layerthickness of approximately the size of the polymer particlesize (*50 mm).33 Scaffolds have also been fabricated thatuse natural biopolymers and polysaccharide such as gelatin,dextran, and starch that are fused together using aqueoussolvents. Furthermore, the addition of porogens and partic-ulate leaching have shown promise in creating microporousstructures. Simpson et al. developed a porous poly(lactic-co-glycolic) acid (PLGA) scaffold with PFP and demonstratedthe ability to precisely reproduce the shape of an entirehuman fourth middle phalanx.34
FIG. 3. (Left) Schematic of PFP technique, and (right) exemplary tissue engineering scaffolds composed of Ca–P/PHBVthat showcase the resolution and detail of PFP. Models are 250% reproductions of CT scans of a human proximal femoralcondyle reconstructed from CT images and then processed into porous scaffold using cubic cells. Scale bar is 10 mm. Ca–P/PHBV, calcium phosphate–poly(hydroxybutyrate-cohydroxyvalerate); PFP, powder-fusion printing. (Reprinted,37 Copy-right 2010, with permission from The Royal Society.) Color images available online at www.liebertpub.com/teb
THREE-DIMENSIONAL PRINTING TISSUE ENGINEERING CONSTRUCTS 301
The effects of particulate and pore size have also beenexplored to examine the effect on cell attachment, growth,and matrix deposition.35 Although PFP is limited to pow-dered materials, this technique is capable of fabricatingscaffolds from several materials such as titanium andmagnesium that are not readily printable with other tech-niques. PFP is well suited for bone and other rigid tissuesbecause bound or fused material typically creates constructsof superior mechanical properties. In addition, some mate-rials naturally found in bone such as tricalcium phosphateare commonly printed using PFP techniques.36 PFP alsodoes not require support material because the unfusedpowder supports each successive layer and allows forcomplex shapes, including designed, interconnected poros-ity. However, resolution and minimum pore size are limitedby the powder characteristics, and additional sintering istypically required to solidify the part that can lead tocracking and damage. Current research efforts are focusedon developing new materials for SLS and refining printparameters to improve surface finish.
Solid freeform fabrication
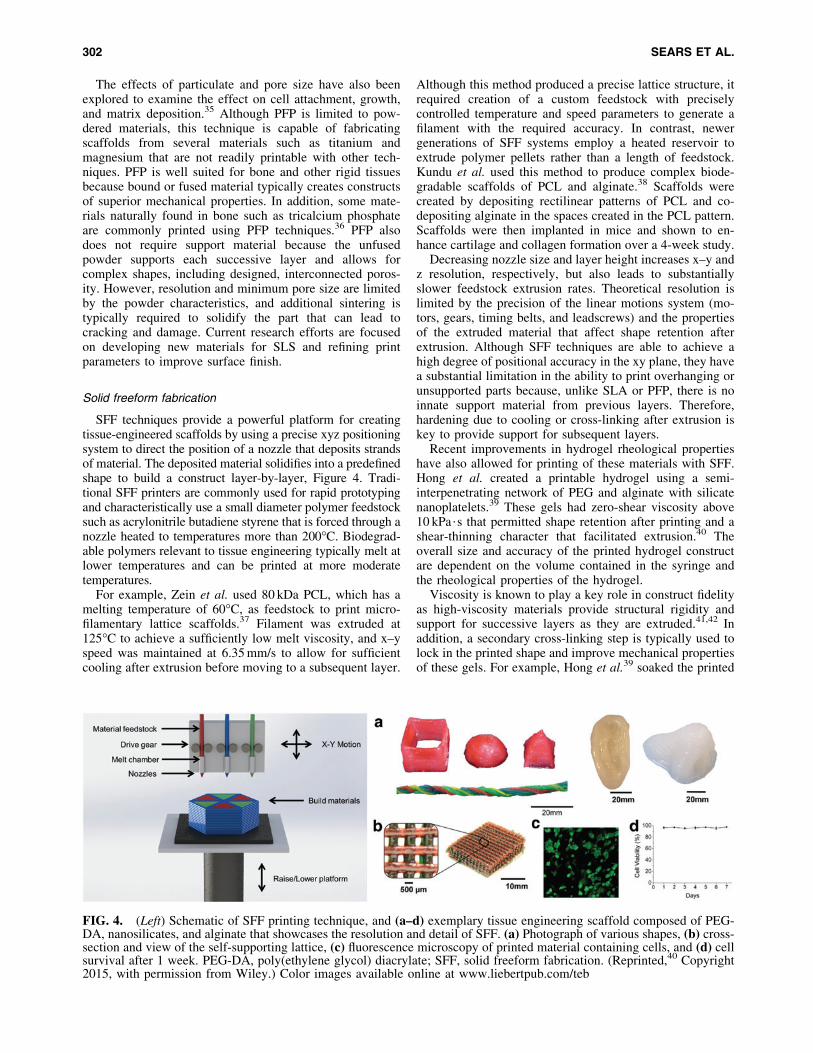
SFF techniques provide a powerful platform for creatingtissue-engineered scaffolds by using a precise xyz positioningsystem to direct the position of a nozzle that deposits strandsof material. The deposited material solidifies into a predefinedshape to build a construct layer-by-layer, Figure 4. Tradi-tional SFF printers are commonly used for rapid prototypingand characteristically use a small diameter polymer feedstocksuch as acrylonitrile butadiene styrene that is forced through anozzle heated to temperatures more than 200�C. Biodegrad-able polymers relevant to tissue engineering typically melt atlower temperatures and can be printed at more moderatetemperatures.
For example, Zein et al. used 80 kDa PCL, which has amelting temperature of 60�C, as feedstock to print micro-filamentary lattice scaffolds.37 Filament was extruded at125�C to achieve a sufficiently low melt viscosity, and x–yspeed was maintained at 6.35 mm/s to allow for sufficientcooling after extrusion before moving to a subsequent layer.
Although this method produced a precise lattice structure, itrequired creation of a custom feedstock with preciselycontrolled temperature and speed parameters to generate afilament with the required accuracy. In contrast, newergenerations of SFF systems employ a heated reservoir toextrude polymer pellets rather than a length of feedstock.Kundu et al. used this method to produce complex biode-gradable scaffolds of PCL and alginate.38 Scaffolds werecreated by depositing rectilinear patterns of PCL and co-depositing alginate in the spaces created in the PCL pattern.Scaffolds were then implanted in mice and shown to en-hance cartilage and collagen formation over a 4-week study.
Decreasing nozzle size and layer height increases x–y andz resolution, respectively, but also leads to substantiallyslower feedstock extrusion rates. Theoretical resolution islimited by the precision of the linear motions system (mo-tors, gears, timing belts, and leadscrews) and the propertiesof the extruded material that affect shape retention afterextrusion. Although SFF techniques are able to achieve ahigh degree of positional accuracy in the xy plane, they havea substantial limitation in the ability to print overhanging orunsupported parts because, unlike SLA or PFP, there is noinnate support material from previous layers. Therefore,hardening due to cooling or cross-linking after extrusion iskey to provide support for subsequent layers.
Recent improvements in hydrogel rheological propertieshave also allowed for printing of these materials with SFF.Hong et al. created a printable hydrogel using a semi-interpenetrating network of PEG and alginate with silicatenanoplatelets.39 These gels had zero-shear viscosity above10 kPa$s that permitted shape retention after printing and ashear-thinning character that facilitated extrusion.40 Theoverall size and accuracy of the printed hydrogel constructare dependent on the volume contained in the syringe andthe rheological properties of the hydrogel.
Viscosity is known to play a key role in construct fidelityas high-viscosity materials provide structural rigidity andsupport for successive layers as they are extruded.41,42 Inaddition, a secondary cross-linking step is typically used tolock in the printed shape and improve mechanical propertiesof these gels. For example, Hong et al.39 soaked the printed
FIG. 4. (Left) Schematic of SFF printing technique, and (a–d) exemplary tissue engineering scaffold composed of PEG-DA, nanosilicates, and alginate that showcases the resolution and detail of SFF. (a) Photograph of various shapes, (b) cross-section and view of the self-supporting lattice, (c) fluorescence microscopy of printed material containing cells, and (d) cellsurvival after 1 week. PEG-DA, poly(ethylene glycol) diacrylate; SFF, solid freeform fabrication. (Reprinted,40 Copyright2015, with permission from Wiley.) Color images available online at www.liebertpub.com/teb
302 SEARS ET AL.

construct in calcium chloride solution to cross-link the al-ginate portion of the gel and prevent swelling and loss ofshape. The Lewis group from the Wyss Institute have ex-panded upon these techniques to create scaffolds usingsacrificial inks to create vasculatures on the order of hun-dreds of microns in size with the potential to create scaffoldswith many materials and cell types.43,44
Extrusion-based printers typically use either pneumaticpressure or a motor actuated plunger to deposit material.45
Pneumatic systems provide simplified control over the ap-plication of force to the extruded material. The system iscalibrated for each material with adjustments made to noz-zle size, nozzle geometry (tapered tip, cylindrical needle,and length), and gas pressure.46–48 Precise control over theair pressure permits fine tuning of the material depositionwith increased pressures needed for more viscous materi-als.49,50 However, materials with different viscosities willextrude at differing rates when using the same pressure.Therefore, components of multimaterial scaffolds need to beprinted at differing speeds or using different pressures ac-cording to the viscosity of the material.
Motor-driven extrusion systems use a plunger to controlthe deposition of material, which allows for more sophisti-cated control over the deposition of material. Unlike pneu-matic systems, a motor-driven plunger permits variableextrusion speed and retraction to prevent unwanted extru-sion as a result of built up pressure. These methods havebeen capable of printing materials with a wide range of vis-cosities.16,42,51–53 Recently, Kesti et al. have shown a com-binatorial approach for printing poly(N-isopropylacrylamide)(PNIPAAm)-modified hyaluronic acid that involves dis-pensing hydrogel solution into a warm chamber at 37�C tocause gelation of the PNIPAAm, followed by ultravioletphotopolymerization for 10 s after each layer to lock in thescaffold geometry.54
Overall, SFF is one of the most versatile printing tech-niques to generate biomimetic scaffolds because of its abilityto make multimaterial constructs and print soft biomaterialssuch as hydrated gels. Adaptation of SFF techniques fortissue engineering has led to an increased range of availablematerials that have the requisite rheological properties toenable both extrusion and shape retention after extrusion.In comparison to the other techniques, SFF scaffolds aresomewhat limited in their geometry without the use of a sec-ondary support material.
In addition, because of the filamentous nature of SFF,printed scaffolds may exhibit anisotropic mechanical prop-erties. This may be detrimental because of potential delam-ination of the layers, but may be advantageous in creatingscaffolds with intended alignment such as ligament or ten-don. Although layer height and feature size are typicallylimited based on nozzle size, improvements in microdeposi-tion resolution are currently being pursued for the recreationof more complex, multimaterial scaffolds.43 A comparativeanalysis of the features and specifications of current majormethods for 3D printing scaffolds for tissue engineering isprovided in Table 2.
Bioprinting of Cellularized Constructs
Bioprinting is generally considered to be the applicationof additive manufacturing techniques to create cell-based
scaffolds. Many of these techniques can be adapted to printwith cells as long as the material, deposition method, andprocessing minimally impact cell viability and function.Biological materials used for printing need to match thenative environment of the host to support the function ofthose cells. In addition, the cells must be able to overcomethe shear stress during the printing process and survive thenonphysiological conditions of the printing regime.47,51,55–57
A wide variety of available bioprinting techniques haveshown promise in creating complex architectures by using a‘‘bioink’’ that is printed onto a substrate in a layer-by-layerprocess to create 3D constructs that mimic native tissue andorgans.41,58–60
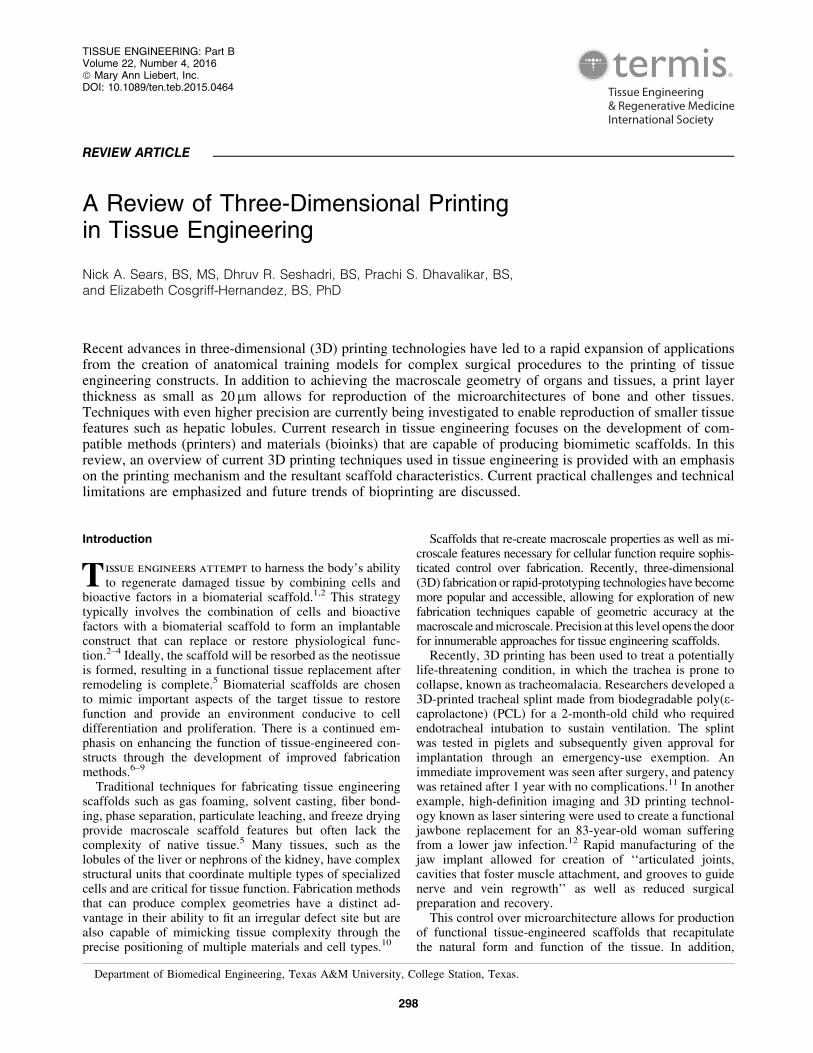
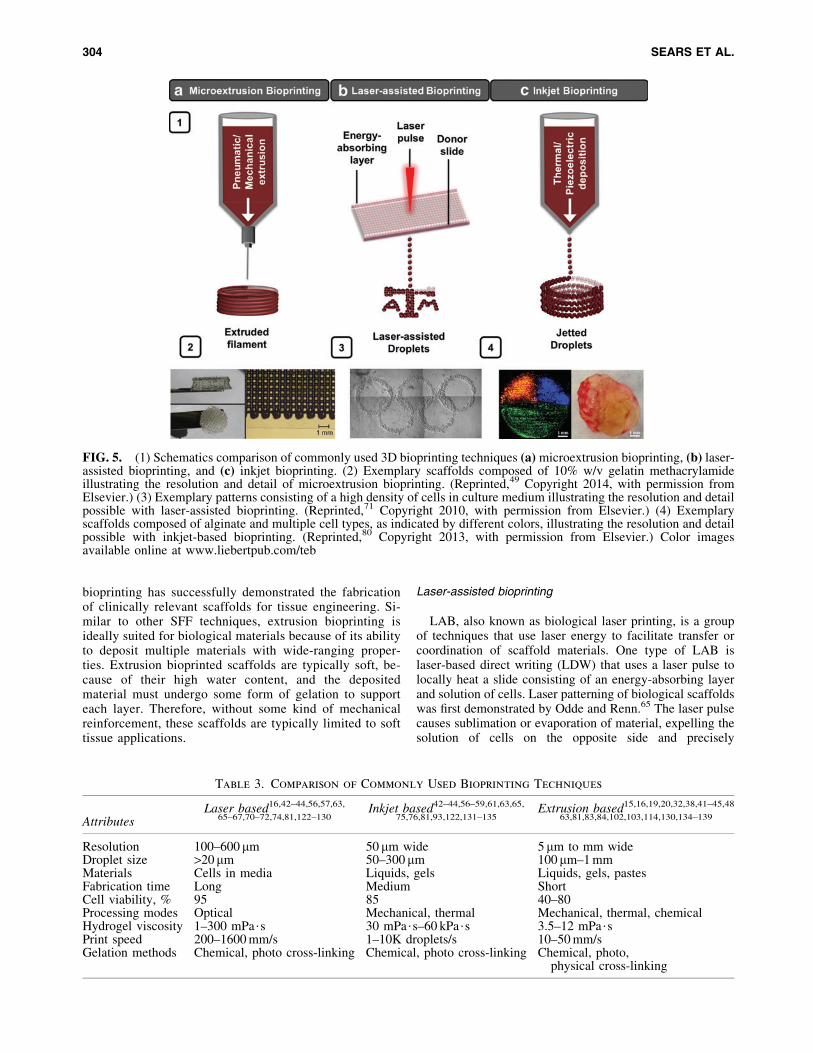
There are three broad categories of bioprinting, namely mi-croextrusion, LAB, and inkjet-based bioprinting (Fig. 5).41,61 Ininkjet-based bioprinting, bioink droplets are deposited onto asubstrate that gel to form polymeric structures. Microextrusionbioprinting, however, uses a mechanical extruder to deposit thebioink as the extruder is moved. Extrusion-based bioprintingallows for the use of high cell density with easier processing, butoccurs at a slower speed than drop-based bioprinting.58,62 LABhas a picoliter (pL) resolution through which cells and liquidmaterials can be printed. This method of printing is rapidlygrowing and shows promise to fabricate tissue-like constructsthat mimic the physiogical behavior of their host counterpart.63
Each of these bioprinting methods is discussed coupled with afocus on their respective print mechanics, applications, anddrawbacks. Key attributes of these printing techniques withcomparisons of material selection, modes of processing, and cellviability are presented in Table 3.41,42,61,62
Extrusion bioprinting
Due to the popularity of open source projects such asRepRap and Fab@home, extrusion-based printing methodshave become one of the most economical techniques forrapid prototyping. Extrusion bioprinting is a type of SFF thattypically involves pressure or screw/plunger-actuated dis-pensing of a fluid containing cells and/or biomaterials. Anideal bioink for extrusion-based bioprinting should be shearthinning to allow for minimal resistance under flow but mustalso chemically or physically cross-link relatively quicklyafter extrusion to support successive layers. Furthermore,possible detrimental effects of polymerization and shearforces on cell viability and function must be considered.
The ability of extrusion-based bioprinters to accuratelydeposit material allows for the fabrication of complex pat-terned structures, including the use of multiple cell types.42
Compared with the other methods discussed, extrusion-based bioprinting is capable of depositing materials with ahigh concentration of cells to accelerate growth and neo-tissue formation. For instance, Yan et al. were able to printgelatin and chitosan hydrogel scaffolds containing hepato-cytes by using extrusion-based bioprinting.62 Increasingprint resolution and increasing print speed are challenges inextrusion-based bioprinting. Using biocompatible materialsthat have improved mechanical properties during the print-ing process will improve cell viability. Furthermore, modi-fication of print mechanics might decrease print times andpermit coextrusion of multiple materials.
Although fabrication time is relatively long to achievehigh resolution in complex structures, extrusion-based
THREE-DIMENSIONAL PRINTING TISSUE ENGINEERING CONSTRUCTS 303
bioprinting has successfully demonstrated the fabricationof clinically relevant scaffolds for tissue engineering. Si-milar to other SFF techniques, extrusion bioprinting isideally suited for biological materials because of its abilityto deposit multiple materials with wide-ranging proper-ties. Extrusion bioprinted scaffolds are typically soft, be-cause of their high water content, and the depositedmaterial must undergo some form of gelation to supporteach layer. Therefore, without some kind of mechanicalreinforcement, these scaffolds are typically limited to softtissue applications.
Laser-assisted bioprinting
LAB, also known as biological laser printing, is a groupof techniques that use laser energy to facilitate transfer orcoordination of scaffold materials. One type of LAB islaser-based direct writing (LDW) that uses a laser pulse tolocally heat a slide consisting of an energy-absorbing layerand solution of cells. Laser patterning of biological scaffoldswas first demonstrated by Odde and Renn.65 The laser pulsecauses sublimation or evaporation of material, expelling thesolution of cells on the opposite side and precisely
FIG. 5. (1) Schematics comparison of commonly used 3D bioprinting techniques (a) microextrusion bioprinting, (b) laser-assisted bioprinting, and (c) inkjet bioprinting. (2) Exemplary scaffolds composed of 10% w/v gelatin methacrylamideillustrating the resolution and detail of microextrusion bioprinting. (Reprinted,49 Copyright 2014, with permission fromElsevier.) (3) Exemplary patterns consisting of a high density of cells in culture medium illustrating the resolution and detailpossible with laser-assisted bioprinting. (Reprinted,71 Copyright 2010, with permission from Elsevier.) (4) Exemplaryscaffolds composed of alginate and multiple cell types, as indicated by different colors, illustrating the resolution and detailpossible with inkjet-based bioprinting. (Reprinted,80 Copyright 2013, with permission from Elsevier.) Color imagesavailable online at www.liebertpub.com/teb
Table 3. Comparison of Commonly Used Bioprinting Techniques
AttributesLaser based16,42–44,56,57,63,
65–67,70–72,74,81,122–130Inkjet based42–44,56–59,61,63,65,
75,76,81,93,122,131–135Extrusion based15,16,19,20,32,38,41–45,48
63,81,83,84,102,103,114,130,134–139
Resolution 100–600 mm 50 mm wide 5mm to mm wideDroplet size >20mm 50–300 mm 100mm–1 mmMaterials Cells in media Liquids, gels Liquids, gels, pastesFabrication time Long Medium ShortCell viability, % 95 85 40–80Processing modes Optical Mechanical, thermal Mechanical, thermal, chemicalHydrogel viscosity 1–300 mPa$s 30 mPa$s–60 kPa$s 3.5–12 mPa$sPrint speed 200–1600 mm/s 1–10K droplets/s 10–50 mm/sGelation methods Chemical, photo cross-linking Chemical, photo cross-linking Chemical, photo,
physical cross-linking
304 SEARS ET AL.

depositing them on the substrate. LDW methods can befurther subdivided into laser-induced forward transfer andmatrix-assisted pulsed laser evaporation direct writing,which have been used to deposit fibroblasts, keratinocytes,and human mesenchymal stem cells (hMSCs),66 variouscancer cell lines,67 and a range of biopolymers.68
LDW is nozzle free, thereby permitting the use of high-viscosity bioink unlike that of drop-based bioprinting orextrusion-based bioprinting.42,63,69,70 In addition, lasers al-low for high precision, thus making this method ideal forbioprinting the smallest details of native tissues and or-gans.42,63,69 LDW printing has been successfully demon-strated with various cells and biomaterials.69,70 Gaebel et al.used LAB printing to pattern human umbilical vein endo-thelial cells and hMSCs onto a polyester urethane cardiacpatch that showed improved cardiac function up to 8 weeksafter myocardial infarction.71
Although this technique allows for direct printing of cells,there remain several limitations that should be considered. Theheat and damaging forces resulting from the laser pulse canhave a detrimental effect on cell survival and long-term be-havior.42,69,70 Additional challenges to LAB printing includeincreased build time, difficulty building scaffold height, andneed for new biomaterials that can be cross-linked after depo-sition.48,72 Gudapati et al. reported that cell encapsulation incross-linked hydrogels was critical for cell survival in laser-based bioprinting techniques.48,72,73 LAB methods offer themost precise positioning of cells and cellular material, but arethe most limited in their ability to build constructs vertically.Laser-based methods are most applicable in conjunction withother techniques or methods to create 3D scaffolds.
Inkjet bioprinting
Inkjet bioprinting is a powerful method of precisely de-positing cells and biomaterials that leverages sophisticatedadvances in 2D inkjet printing to create 3D scaffolds. In in-kjet bioprinting, a fixed volume of fluid is jetted into a precisepattern specified by the software.42,74 Inkjet bioprinting hasbecome a popular method in fabricating cell-laden constructsthat can mimic the complexity of native tissue or organs. Onekey advantage of this technique is the speed at which it canconstruct scaffolds while maintaining a complex 3D archi-tecture.48,72 This speed also poses challenges as it severelylimits the number of polymeric materials that can be used tobioprint as it requires the gelation time to be greater than orequal to the drop deposition time.43
Inkjet bioprinters can be adjusted and specifically tailoredto allow for printing materials at increasing resolutions andspeeds.41,42,62 Inkjet bioprinting uses thermal or piezoelec-tric energy to deposit droplets of solution into a predefinedpattern.42,62 Inkjet bioprinters typically consist of one ormany ink chambers with multiple nozzles corresponding topiezoelectric or heating components75 To eject a droplet ofink, a short pulse of current is applied to actuate the com-ponent. In thermal bioprinters, the sudden increase in localtemperature causes vapor bubbles to form and collapse,ejecting ink droplets onto the substrate.62,75
In piezoelectric inkjet printing, piezocrystals actuate thechamber itself causing an increase in pressure, resulting indroplet ejection.75 Deposition from the nozzle onto the printbed results when an electric charge induces vibration in the
crystals.62,75 Heat and mechanical stresses generated duringthermal inkjet bioprinting have been shown to adverselyaffect cell viability.74 The largest detrimental effect occursin the nozzle orifice where the temperature is greatest.75
There is a need to mitigate and alleviate this issue. Lorberet al. were able to successfully print retinal ganglion andglia cells harvested from the adult central nervous systemwithout causing an adverse effect on cell viability.75 Fromthis study, researchers were able to show that piezoelectricprinting did not compromise the phenotype or activity ofthese cells.75 In an effort to increase throughput and ac-cessibility to this technology, Boland et al. reported theprinting of thermosensitive gels by using a modified car-tridge from a commercially available inkjet printer to createmultilayer scaffolds.57 In addition, researchers have suc-cessfully demonstrated a multihead inkjet-based approachfor bioprinting multiple cell lines into heterogeneous scaf-folds for tissue engineering.76–78
A key disadvantage of inkjet printing is that the biologicalagents need to be in a liquid state to permit deposition. Thedeposited droplets must then solidify into the required ge-ometry. To address this requirement, commonly used ma-terials are cross-linked using physical, chemical, pH, orultraviolet methods.79 However, chemical cross-linking ofmany natural materials, such as those derived from extra-cellular matrix, modifies both the chemical and materialproperties, and the use of some cross-linking mechanisms isknown to pose a detriment to cells, thus decreasing cellviability and functionality.80
Although inkjet bioprinting allows for encapsulation oflive cells, relatively low concentrations are required to formcohesive droplets and prevent clogging of the nozzle.81,82
Despite the addressed disadvantages, inkjet-based bio-printers continue to have great potential because of their lowcost, high resolution, and high compatibility with manybiomaterials. Because commercially available 2D printersharness this technology, researchers can easily adapt com-ponents for research applications. The versatility of inkjet-based technology has refined the capabilities of theseprinters to accurately deposit fine droplets with precisevolume to create high-resolution scaffolds with cells intact.Droplet size can be modulated from 1 to 300 pL with de-position rates from 1 to 10,000 droplets per second.42
Future work will continue to grow this technology to printmore biologically relevant materials and to further retainfunctionality and bioactivity of cells and biomaterials. Mul-timaterial printing using inkjet technology is a developingadaptation that needs to be further developed to print multiplecell types in complex constructs. Inkjet bioprinting is capableof creating scaffolds with accuracy within 100mm, whichmakes it very useful for creating complex tissue-engineeredscaffolds. Although it is limited in its ability to produce tallstructures because of the typical mechanical properties of thegel inks, the ability to print multiple materials and cell typesmakes it a useful method to create complex tissue with greataccuracy. A comparative analysis of these bioprinting tech-niques is provided in Table 3.
Summary, Key Challenges, and Future Directions
The rapid growth in the 3D printing field has opened upnew avenues and directions of research. Adaptation of
THREE-DIMENSIONAL PRINTING TISSUE ENGINEERING CONSTRUCTS 305

current 3D printing techniques for biological applicationshas enabled the fabrication of tissue grafts and artificialorgans. Although the field is still at a relatively early stage,pioneering research in tissue engineering of organs with 3Dprinting has shown great promise. Tissue engineeringstrategies have been used to replace portions of intestine,83
improve repair after myocardial infarction,84 and evencompletely replace a bladder,85,86 and augmentation ofscaffold fabrication with 3D printing technologies stands tomake enormous improvements in the sophistication of thesestrategies. In addition to tissue engineering, 3D printing hasalso been used in the field of drug delivery,87 analysis ofchemical and biological agents,88 and organ-on-a-chip de-vices.89 As highlighted in this review, the 3D printing processis continuing to evolve with different process mechanics thatare being optimized to achieve specific outcomes in regen-erative medicine.
Despite the strong potential of 3D printing to improveregenerative strategies, there remain many challenges thatrelate to both the printing process and the materials avail-able for printing. Processing challenges include the need forimproved resolution, increased speed,42,46,90 and printingprocesses that are compatible with cells.48,90,91 Current ef-forts to improve printing resolution of lithographic tech-niques include the development of methods such as electronbeam lithography and multiphoton absorption polymeriza-tion.92–95 These methods are capable of creating extremelyprecise scaffolds with feature sizes of the order of tens ofnanometers.
As we depart from the modification of current technologyand begin designing 3D printers to fabricate custom bio-materials and tissues, an expanding library of biomaterialscompatible with the printing process is needed. Materialsused for 3D bioprinting must adhere to three key criteria:scaffold materials must (i) be biocompatible, (ii) supportcell growth and differentiation, and (iii) sufficiently retainits shape to preserve scaffold integrity until solidificationlocks in the scaffold geometry.16,36,56,59,62,96 As a result,currently published work uses a limited range of materialssuch as collagen, gelatin, hyaluronic acid, alginate, modifiedcopolymers, and photopolymerizable macromers. In addi-tion, the design of complex scaffolds that mimic tissue isdriven by our understanding of the composition and cellulardistribution of those tissues. Therefore, additional funda-mental research is needed to be able to accurately image andmap complex tissues to reproduce scaffolds with the req-uisite structure and biological cues.
One of the key areas of future research in 3D printing liesin direct in situ bioprinting, namely, printing cells andbiomaterials directly onto or in a patient. Such progress willaccelerate and galvanize the convergence of two promisingfields. Earlier research has demonstrated the feasibility ofbioprinting directly into wounds or burn defects.97 In addi-tion, other researchers have bioprinted bone into calvarialdefects in mice.98 Advancements in speed and resolution ofprinting technology will enable in situ printing to enhanceregeneration of tissues and reduce recovery time. Such ad-vancements could very well be translated to the battlefield toexpedite and improve recovery for soldiers.
Finally, development of scalable and automated bio-printers is required to commercialize bioprinted constructs.Start-up companies such as Organovo have paved the way
for the commercialization of 3D printing of tissue grafts andorgans. Specifically, Organovo has focused on bioprintingliver cells to create artificial livers that can successfullymodel and mimic native livers. Other up and coming 3Dprinting companies include Carbon3D, Biobot, OxSyBio,Cyfuse, 3Dynamic, TeVido BioDevices, and RegenHu.Overall, continued multidisciplinary research combiningmaterials processing, computer modeling, medical imaging,chemistry, and biology is needed to fully achieve the po-tential of 3D printing in tissue engineering and regenerativemedicine.
Disclosure Statement
No competing financial interests exist.
References
1. Langer, R., and Vacanti, J.P. Tissue engineering: thechallenges ahead. Sci Am 280, 86, 1999.
2. Blitterswijk, C.A.V., Moroni, L., Rouwkema, J., Siddap-pa, R., and Sohier, J. Tissue Engineering—An Introduc-tion. Tissue Engineering. Burlington: Academic Press,2008, p. xii.
3. Bhatia, S.N., and Chen, C.S. Tissue engineering at themicro-scale. Biomed Microdevices 2, 131, 1999.
4. Sakiyama-Elbert, S., and Hubbell, J. Functional bioma-terials: design of novel biomaterials. Annu Rev Mater Res31, 183, 2001.
5. Oberpenning, F., Meng, J., Yoo, J.J., and Atala, A. Denovo reconstitution of a functional mammalian urinarybladder by tissue engineering. Nat Biotechnol 17, 149,1999.
6. Freed, L.E., and Vunjak-Novakovic, G. Chapter 13—Tissue engineering bioreactors. In: Vacanti, R.P., Lanza,R., Langer, J., eds. Principles of Tissue Engineering, 2ndedn. San Diego: Academic Press, 2000, p. 143.
7. Konig, F., Hollweck, T., Pfeifer, S., Reichart, B., Win-termantel, E., Hagl, C., and Akra, B. A pulsatile bioreactorfor conditioning of tissue-engineered cardiovascular con-structs under endoscopic visualization. J Funct Biomater3, 480, 2005.
8. Mol, A., Driessen, N.J.B., Rutten, M.C.M., Hoerstrup,S.P., Bouten, C.V.C., and Baaijens, F.P.T. Tissue engi-neering of human heart valve leaflets: a novel bioreactorfor a strain-based conditioning approach. Ann BiomedEng 33, 1778, 2005.
9. Birla, R.K., Borschel, G.H., and Dennis, R.G. In vivoconditioning of tissue-engineered heart muscle improvescontractile performance. Artif Organs 29, 866, 2005.
10. Temple, J.P., Hutton, D.L., Hung, B.P., Huri, P.Y., Cook,C.A., Kondragunta, R., Jia, X., and Grayson, W.L. En-gineering anatomically shaped vascularized bone graftswith hASCs and 3D-printed PCL scaffolds. J BiomedMater Res Res A 102, 4317, 2014.
11. Zopf, D.A., Hollister, S.J., Nelson, M.E., Ohye, R.G., andGreen, G.E. Bioresorbable airway splint created with athree-dimensional printer. N Engl J Med 368, 2043, 2013.
12. Nickels, L. World’s first patient-specific jaw implant. MetPowder Rep 67, 12, 2012.
13. Jeffries, E.M., Nakamura, S., Lee, K.-W., Clampffer, J.,Ijima, H., and Wang, Y. Micropatterning electrospunscaffolds to create intrinsic vascular networks. MacromolBiosci 14, 1514, 2014.
306 SEARS ET AL.
14. Xu, W., Wang, X., Yan, Y., and Zhang, R. Rapid proto-typing of polyurethane for the creation of vascular sys-tems. J Bioact Compat Polym 23, 103, 2008.
15. Wang, M.O., Vorwald, C.E., Dreher, M.L., Mott, E.J.,Cheng, M.-H., Cinar, A., Mehdizadeh, H., Somo, S.,Dean, D., Brey, E.M., and Fisher, J.P. Evaluating 3D-printed biomaterials as scaffolds for vascularized bonetissue engineering. Adv Mater 27, 138, 2015.
16. Nguyen, L.H., Annabi, N., Nikkhah, M., Bae, H., Binan,L., Park, S., Kang, Y., Yang, Y., and Khademhosseini, A.Vascularized bone tissue engineering: approaches for po-tential improvement. Tissue Eng Part B Rev 18, 363, 2012.
17. Visk, D. Will advances in preclinical in vitro modelslower the costs of drug development? Appl In VitroToxicol 1, 79, 2015.
18. Cooke, M.N., Fisher, J.P., Dean, D., Rimnac, C., andMikos, A.G. Use of stereolithography to manufacturecritical-sized 3D biodegradable scaffolds for bone in-growth. J Biomed Mater Res B Appl Biomater 64B, 65,2003.
19. Moglia, R.S., Holm, J.L., Sears, N.A., Wilson, C.J., Har-rison, D.M., and Cosgriff-Hernandez, E. Injectable poly-HIPEs as high-porosity bone grafts. Biomacromolecules12, 3621, 2011.
20. Christenson, E.M., Soofi, W., Holm, J.L., Cameron, N.R.,and Mikos, A.G. Biodegradable fumarate-based poly-HIPEs as tissue engineering scaffolds. Biomacromole-cules 8, 3806, 2007.
21. Langton, C.M., Whitehead, M.A., Langton, D.K., andLangley, G. Development of a cancellous bone structuralmodel by stereolithography for ultrasound characterisationof the calcaneus. Med Eng Phys 19, 599, 1997.
22. Leukers, B., Gulkan, H., Irsen, S., Milz, S., Tille, C.,Schieker, M., and Seitz, H. Hydroxyapatite scaffolds forbone tissue engineering made by 3D printing. J Mater SciMater Med 16, 1121, 2005.
23. Yang, S., Leong, K.F., Du, Z., and Chua, C.-K. The designof scaffolds for use in tissue engineering. Part I. Tradi-tional factors. Tissue Eng 7, 679, 2001.
24. Yu, T., and Ober, C.K. Methods for the topographicalpatterning and patterned surface modification of hydrogelsbased on hydroxyethyl methacrylate. Biomacromolecules4, 1126, 2003.
25. Matsuda, T., and Magoshi, T. Preparation of vinylatedpolysaccharides and photofabrication of tubular scaffoldsas potential use in tissue engineering. Biomacromolecules3, 942, 2002.
26. Chu, T.M.G., Hollister, S.J., Halloran, J.W., Feinberg,S.E., and Orton, D.G. Manufacturing and characterizationof 3-D hydroxyapatite bone tissue engineering scaffolds.Ann N Y Acad Sci 961, 114, 2002.
27. Chu, T.M.G., Orton, D.G., Hollister, S.J., Feinberg, S.E.,and Halloran, J.W. Mechanical and in vivo performanceof hydroxyapatite implants with controlled architectures.Biomaterials 23, 1283, 2002.
28. Bartolo, P. Stereolithographic processes. In: Bartolo, P.J.,ed. Stereolithography. Berlin: Springer, 2011, p. 1.
29. Zhou, C., Chen, Y., Yang, Z., and Khoshnevis, B. Di-gital material fabrication using mask-image-projection-based stereolithography. Rapid Prototyping J 19, 153,2013.
30. Yang, S., Leong, K.-F., Du, Z., and Chua, C.-K. The de-sign of scaffolds for use in tissue engineering. Part II.Rapid prototyping techniques. Tissue Eng 8, 1, 2002.
31. Shuai, C., Li, P., Liu, J., and Peng, S. Optimization ofTCP/HAP ratio for better properties of calcium phosphatescaffold via selective laser sintering. Mater Charact 77,23, 2013.
32. Leong, K.F., Cheah, C.M., and Chua, C.K. Solid freeformfabrication of three-dimensional scaffolds for engineeringreplacement tissues and organs. Biomaterials 24, 2363, 2003.
33. Park, W., and Griffith, L. Integration of surface modifi-cation and 3D fabrication techniques to prepare patternedpoly(L-lactide) substrates allowing regionally selectivecell adhesion. J Biomater Sci Polm Ed 9, 89, 1998.
34. Simpson, R.L., Wiria, F.E., Amis, A.A., Chua, C.K.,Leong, K.F., Hansen, U.N., Chandrasekaran, M., and Lee,M.W. Development of a 95/5 poly(L-lactide-co-glyco-lide)/hydroxylapatite and beta-tricalcium phosphate scaf-fold as bone replacement material via selective lasersintering. J Biomed Mater Res B Appl Biomater 84, 17,2008.
35. Zeltinger, J., Sherwood, J.K., Graham, D.A., Mueller, R.,and Griffith, L.G. Effect of pore size and void fraction oncellular adhesion, proliferation, and matrix deposition.Tissue Eng 7, 557, 2001.
36. Bose, S., Vahabzadeh, S., and Bandyopadhyay, A. Bonetissue engineering using 3D printing. Mater Today 16,496, 2013.
37. Zein, I., Hutmacher, D.W., Tan, K.C., and Teoh, S.H.Fused deposition modeling of novel scaffold architecturesfor tissue engineering applications. Biomaterials 23, 1169,2002.
38. Kundu, J., Shim, J.H., Jang, J., Kim, S.W., and Cho, D.W.An additive manufacturing-based PCL-alginate-chondrocytebioprinted scaffold for cartilage tissue engineering. J TissueEng Regen Med 9, 1286, 2015.
39. Hong, S., Sycks, D., Chan, H.F., Lin, S., Lopez, G.P.,Guilak, F., Leong, K.W., and Zhao, X. 3D printing ofhighly stretchable and tough hydrogels into complex,cellularized structures. Adv Mater 27, 4035, 2015.
40. Compton, B., and Lewis, J.A. 3D-printing of lightweightcellular composites. Adv Mater 26, 5930, 2014.
41. Ozbolat, I., and Yu, Y. Bioprinting towards organ fabri-cation: challenged and future trends. IEEE Trans BiomedEng 60, 691, 2013.
42. Murphy, S.V., and Atala, A. 3D bioprinting of tissues andorgans. Nat Biotechnol 32, 773, 2014.
43. Kolesky, D., Truby, R., Gladman, S., Busbee, T., Homan,K., and Lewis, J.A. 3D bioprinting of vascularized, het-erogeneous cell-laden tissue constructs. Adv Mater 26,3124, 2014.
44. Wu, W., DeConinck, A., and Lewis, J.A. Omnidirectionalprinting of 3D microvascular networks. Adv Mater 23,H178, 2011.
45. Jakab, K., Norotte, C., Marga, F., Murphy, K., Vunjak-Novakovic, G., and Forgacs, G. Tissue engineering byself-assembly and bio-printing of living cells. Biofabri-cation 2, 022001, 2010.
46. Khalil, S., Nam, J., and Sun, W. Multi-nozzle depositionfor construction of 3D biopolymer tissue scaffolds. RapidPrototyping 11, 9, 2005.
47. Fedorovich, N.E., De Wijn, J.R., Verbout, A.J., Alblas, J.,and Dhert, W.J.A. Three-dimensional fiber deposition ofcell-laden, viable, patterned constructs for bone tissueprinting. Tissue Eng Part A 14, 127, 2008.
48. Billiet, T., Gevaert, E., De Schryver, T., Cornelissen, M.,and Dubruel, P. The 3D printing of gelatin methacryla-
THREE-DIMENSIONAL PRINTING TISSUE ENGINEERING CONSTRUCTS 307
mide cell-laden tissue-engineered constructs with highcell viability. Biomaterials 35, 49, 2014.
49. Smith, C.M., Christian, J.J., Warren, W.L., and Williams,S.K. Characterizing environmental factors that impact theviability of tissue-engineered constructs fabricated by adirect-write bioassembly tool. Tissue Eng 13, 373, 2007.
50. Smith, C.M., Stone, A.L., Parkhill, R.L., Stewart, R.L.,Simpkins, M.W., Kachurin, A.M., Warren, W.L., andWilliams, S.K. Three-dimensional bioassembly tool forgenerating viable tissue-engineered constructs. Tissue Eng10, 1566, 2004.
51. Pati, F., Jang, J., Ha, D.-H., Won Kim, S., Rhie, J.-W.,Shim, J.-H., Kim, D.-H., and Cho, D.-W. Printing three-dimensional tissue analogues with decellularized extra-cellular matrix bioink. Nat Commun 5, 3935, 2014.
52. Mota, C., Puppi, D., Chiellini, F., and Chiellini, E. Ad-ditive manufacturing techniques for the production oftissue engineering constructs. J Tissue Eng Regen Med 9,174, 2015.
53. Campos, D.F.D., Drescher, W., Rath, B., Tingart, M., andFischer, H. Supporting biomaterials for articular cartilagerepair. Cartilage 3, 205, 2012.
54. Kesti, M., Muller, M., Becher, J., Schnabelrauch, M.,D’Este, M., Eglin, D., and Zenobi-Wong, M. A versatilebioink for three-dimensional printing of cellular scaffoldsbased on thermally and photo-triggered tandem gelation.Acta Biomater 11, 162, 2015.
55. Miller, J.S. The billion cell construct: will three-dimensional printing get us there? PLoS Biol 12,e1001882, 2014.
56. Guillotin, B., and Guillemot, F. Cell patterning technol-ogies for organotypic tissue fabrication. Trends Bio-technol 29, 183, 2011.
57. Irvine, S.A., Agrawal, A., Lee, B.H., Chua, H.Y., Low,K.Y., Lau, B.C., Machluf, M., and Venkatraman, S.Printing cell-laden gelatin constructs by free-form fabri-cation and enzymatic protein crosslinking. Biomed Mi-crodevices 17, 16, 2015.
58. Boland, T., Xu, T., Damon, B., and Cui, X. Application ofinket printing to tissue engineering. Biotechnology 1, 910,2006.
59. Wust, S., Muller, R., and Hofmann, S. Controlled posi-tioning of cells in biomaterials—approaches towards 3Dtissue printing. J Funct Biomater 2, 119, 2011.
60. Fedorovich, N.E., Alblas, J., de Wijn, J.R., Hennink,W.E., Verbout, A.J., and Dhert, W.J.A. Hydrogels as ex-tracellular matrices for skeletal tissue engineering: state-of-the-art and novel application in organ printing. TissueEng 13, 1905, 2007.
61. O’Brien, C.M., Holmes, B., Faucett, S., and Zhang, L.G.Three-dimensional printing of nanomaterial scaffolds forcomplex tissue regeneration. Tissue Eng Part B Rev 21,103, 2015.
62. Dababneh, A.B., and Ozbolat, I.T. Bioprinting technolo-gy: a current state-of-the-art review. J Manuf Sci Eng 136,061016, 2014.
63. Devillard, R., Pages, E., Correa, M.M., Keriquel, V.,Remy, M., Kalisky, J., Ali, M., Guillotin, B., and Guil-lemot, F. Cell patterning by laser-assisted bioprinting.Methods Cell Biol 119, 159, 2014.
64. Yan, Y., Wang, X., Pan, Y., Liu, H., Cheng, J., Xiong, Z.,Lin, F., Wu, R., Zhang, R., and Lu, Q. Fabrication ofViable Tissue-Engineered Constructs With 3D Cell-As-sembly Technique, Biomaterials, 26(29), 5864, 2015.
65. Odde, D.J., and Renn, M.J. Laser-guided direct writing forapplications in biotechnology. Nanotechnology 17, 385,1999.
66. Wang, W., Li, G., and Huang, Y. Modeling of bubbleexpansion-induced cell mechanical profile in laser-assisted cell direct writing. J Manuf Sci Eng 131, 051013,2009.
67. Hopp, B., Smausz, T., Szabo, G., Kolozsvari, L., Ka-fetzopoulos, D., Fotakis, C., and Nogradi, A. Femtosecondlaser printing of living cells using absorbing film-assistedlaser-induced forward transfer. Opt Eng 51, 014302, 2012.
68. Riggs, B.C., Dias, A.D., Schiele, N.R., Cristescu, R.,Huang, Y., Corr, D.T., and Chrisey, D.B. Matrix-assistedpulsed laser methods for biofabrication. MRS Bull 36,1043, 2011.
69. Guillemot, F., Souquet, A., Catros, S., Guillotin, B., Lo-pez, J., Faucon, M., Pippenger, B., Bareille, R., Remy, M.,Bellance, S., Chabassier, P., Fricain, J.C., and Amedee, J.High-throughput laser printing of cells and biomaterialsfor tissue engineering. Acta Biomater 6, 2494, 2010.
70. Guillotin, B., Souquet, A., Catros, S., Duocastella, M.,Pippenger, B., Bellance, S., Bareille, R., Remy, M., Bor-denave, L., Amedee, J., and Guillemot, F. Laser assistedbioprinting of engineered tissue with high cell density andmicroscale organization. Biomaterials 31, 7250, 2010.
71. Gaebel, R., Ma, N., Liu, J., Guan, J., Koch, L., Klopsch,C., Gruene, M., Toelk, A., Wang, W., Mark, P., Wang, F.,Chichkov, B., Li, W., and Steinhoff, G. Patterning humanstem cells and endothelial cells with laser printing forcardiac regeneration. Biomaterials 32, 9218, 2011.
72. Schuurman, W., Levett, P., Pot, M., van Weeren, P.,Dhert, W., Hutmacher, D., Melchels, F., Klein, T., andMalda, J. Gelatin-methacrylamide hydrogels as potentialbiomaterials for fabrication of tissue-engineered cartilageconstructs. Macromol Biosci 13, 561, 2013.
73. Gudapati, H., Yan, J., Huang, Y., and Chrisey, D.B. Al-ginate gelation-induced cell death during laser-assistedcell printing. Biofabrication 6, 1, 2014.
74. Xu, T., Jin, J., Gregory, C., Hickman, J.J., and Boland, T.Inkjet printing of viable mammalian cells. Biomaterials26, 93, 2005.
75. Lorber, B., Hsiao, W.K., Hutchings, I.M., and Martin, K.R.Adult rat retinal ganglion cells and glia can be printed bypiezoelectric inkjet printing. Biofabrication 6, 9, 2014.
76. Phillippi, J.A., Miller, E., Weiss, L., Huard, J., Waggoner,A., and Campbell, P. Microenvironments engineered byinkjet bioprinting spatially direct adult stem cells towardmuscle- and bone-like subpopulations. Stem Cells 26,127, 2008.
77. Ker, D.F.E., Chu, B., Phillippi, J.A., Gharaibeh, B.,Huard, J., Weiss, L.E., and Campbell, P.G. Engineeringspatial control of multiple differentiation fates within astem cell population. Biomaterials 32, 3413, 2011.
78. Cooper, G.M., Miller, E.D., Decesare, G.E., Usas, A.,Lensie, E.L., Bykowski, M.R., Huard, J., Weiss, L.E.,Losee, J.E., and Campbell, P.G. Inkjet-based biopattern-ing of bone morphogenetic protein-2 to spatially controlcalvarial bone formation. Tissue Eng Part A 16, 1749, 2010.
79. Murphy, S.V., Skardal, A., and Atala, A. Evaluation ofhydrogels for bio-printing applications. J Biomed MaterRes A 101A, 272, 2013.
80. Hennink, W.E., and van Nostrum, C.F. Novel crosslinkingmethods to design hydrogels. Adv Drug Deliv Rev 54, 13,2002.
308 SEARS ET AL.
81. Skardal, A. Hyaluronan and gelatin biomaterials for bio-printing engineered tissues [Doctor of Philosophy Bioen-gineering]. The University of Utah, 2010.
82. Skardal, A., Zhang, J., McCoard, L., Xu, X., Oottama-sathien, S., and Prestwich, G.D. Photocrosslinkablehyaluronan-gelatin hydrogels for two-step bioprinting.Tissue Eng 16, 2675, 2010.
83. Choi, R.S., and Vacanti, J.P. Preliminary studies of tissue-engineered intestine using isolated epithelial organoidunits on tubular synthetic biodegradable scaffolds.Transplant Proc 29, 848, 1997.
84. Christman, K.L., Vardanian, A.J., Fang, Q., Sievers, R.E.,Fok, H.H., and Lee, R.J. Injectable fibrin scaffold im-proves cell transplant survival, reduces infarct expansion,and induces neovasculature formation in ischemic myo-cardium. J Am Coll Cardiol 44, 654, 2004.
85. Atala, A. Tissue engineering of human bladder. Br MedBull 97, 81, 2011.
86. Atala, A., Bauer, S.B., Soker, S., Yoo, J.J., and Retik,A.B. Tissue-engineered autologous bladders for patientsneeding cystoplasty. Lancet 367, 1241, 2006.
87. Low, K.H., Leong, K.F., Chua, C.K., Du, Z.H., andCheah, C.M. Characterization of SLS parts for drug de-livery devicesnull. Rapid Prototyping J 7, 262, 2001.
88. Figallo, E., Cannizzaro, C., Gerecht, S., Burdick, J.A.,Langer, R., Elvassore, N., and Vunjak-Novakovic, G.Micro-bioreactor array for controlling cellular microen-vironments. Lab Chip 7, 710, 2007.
89. Vunjak-Novakovic, G., Bhatia, S., Chen, C., and Hirschi,K. HeLiVa platform: integrated heart-liver-vascular sys-tems for drug testing in human health and disease. StemCell Res Ther 4, S8, 2013.
90. Nair, K., Gandhi, M., Khalil, S., Yan, K.C., Marcolongo, M.,Barbee, K., and Sun, W. Characterization of cell viabilityduring bioprinting processes. Biotechnol J 4, 1168, 2009.
91. Xu, T., Gregory, C.A., Molnar, P., Cui, X., Jalota, S.,Bhaduri, S.B., and Boland, T. Viability and electrophys-iology of neural cell structures generated by the inkjetprinting method. Biomaterials 27, 3580, 2006.
92. Cunningham, L.P., Veilleux, M.P., and Campagnola, P.J.Freeform multiphoton excited microfabrication for bio-logical applications using a rapid prototyping CAD-basedapproach. Opt Express 14, 8613, 2006.
93. Kabouraki, E., Giakoumaki, A.N., Danilevicius, P., Gray,D., Vamvakaki, M., and Farsari, M. Redox multiphotonpolymerization for 3D nanofabrication. Nano Lett 13,3831, 2013.
94. Maria, F., Maria, V., and Boris, N.C. Multiphoton poly-merization of hybrid materials. J Opt 12, 124001, 2010.
95. Li, L., and Fourkas, J.T. Multiphoton polymerization.Mater Today 10, 30, 2007.
96. Aliakbari, M. Additive manufacturing: state-of-the-art,capabilities, and sample applications with cost analysis[Masters Production Engineering and Management]. De-partment of Industrial Production, KTH, 2012.
97. Skardal, A., Mack, D., Kapetanovic, E., Atala, A., Jack-son, J.D., Yoo, J., and Soker, S. Bioprinted amniotic fluid-derived stem cells accelerate healing of large skin wounds.Stem Cells Transl Med 1, 792, 2012.
98. Keriquel, V., Guillemot, F., Arnault, I., Guillotin, B.,Miraux, S., Amedee, J., Fricain, J.C., and Catros, S.In vivo bioprinting for computer- and robotic-assistedmedical intervention: preliminary study in mice. Biofab-rication 2, 014101, 2010.
99. Pham, D.T., and Dimov, S.S. Rapid Manufacturing: TheTechnologies and Applications of Rapid Prototyping andRapid Tooling. London: Springer, 2001.
100. Stratasys, I. Fused deposition modelling for fast, safeplastic models. 12th Annual Conference on ComputerGraphics, Chicago, 1991, p. 326.
101. Sachs, E.M., Haggerty, J.S., Cima, M.J., and Williams,P.A. Three-dimensional printing techniques. Google Pa-tents 5,204,055, 1993.
102. Marcus, H., Beaman, J.J., Barlow, J.W., Bourell, D.L., andCrawford, R.H. Solid freeform fabrication proceedings.Presented at the Solid Freeform Fabrication Proceedings,Austin, TX, 1992.
103. Bose, S., Darsell, J., Kintner, M., Hosick, H., and Ban-dyopadhyay, A. Pore size and pore volume effects onalumina and TCP ceramic scaffolds. Mater Sci Eng C 23,479, 2003.
104. Lam, C.X.F., Mo, X.M., Teoh, S.H., and Hutmacher,D.W. Scaffold development using 3D printing with astarch-based polymer. Mater Sci Eng C 20, 49, 2002.
105. Suwanprateeb, J. Improvement in mechanical propertiesof three-dimensional printing parts made from naturalpolymers reinforced by acrylate resin for biomedical ap-plications: a double infiltration approach. Polym Int 55,57, 2006.
106. Giordano, R.A., Wu, B.M., Borland, S.W., Cima, L.G.,Sachs, E.M., and Cima, M.J. Mechanical properties ofdense polylactic acid structures fabricated by three di-mensional printing. J Biomater Sci Polym Ed 8, 63,1997.
107. Gbureck, U., Holzel, T., Doillon, C.J., Muller, F.A., andBarralet, J.E. Direct printing of bioceramic implants withspatially localized angiogenic factors. Adv Mater 19, 795,2007.
108. Khalyfa, A., Vogt, S., Weisser, J., Grimm, G., Re-chtenbach, A., Meyer, W., and Schnabelrauch, M. De-velopment of a new calcium phosphate powder-bindersystem for the 3D printing of patient specific implants.J Mater Sci Mater Med 18, 909, 2007.
109. Gbureck, U., Vorndran, E., Muller, F.A., and Barralet, J.E.Low temperature direct 3D printed bioceramics and bio-composites as drug release matrices. J Control Release122, 173, 2007.
110. Will, J., Melcher, R., Treul, C., Travitzky, N., Kneser, U.,Polykandriotis, E., Horch, R., and Greil, P. Porous ce-ramic bone scaffolds for vascularized bone tissue regen-eration. J Mater Sci Mater Med 19, 2781, 2008.
111. Shanjani, Y., De Croos, J.N.A., Pilliar, R.M., Kandel,R.A., and Toyserkani, E. Solid freeform fabrication andcharacterization of porous calcium polyphosphate struc-tures for tissue engineering purposes. J Biomed Mater ResB Appl Biomater 93B, 510, 2010.
112. Lewis, J.A. Direct ink writing of 3D functional materials.Adv Funct Mater 16, 2193, 2006.
113. Tarafder, S., Balla, V.K., Davies, N.M., Bandyopadhyay,A., and Bose, S. Microwave-sintered 3D printed tri-calcium phosphate scaffolds for bone tissue engineering.J Tissue Eng Regen Med 7, 631, 2013.
114. Landers, R., Hubner, U., Schmelzeisen, R., and Mulhaupt,R. Rapid prototyping of scaffolds derived from thermo-reversible hydrogels and tailored for applications in tissueengineering. Biomaterials 23, 4437, 2002.
115. Landers, R., and Mulhaupt, R. Desktop manufacturing ofcomplex objects, prototypes and biomedical scaffolds by
THREE-DIMENSIONAL PRINTING TISSUE ENGINEERING CONSTRUCTS 309
means of computer-assisted design combined with computer-guided 3D plotting of polymers and reactive oligomers.Macromol Mater Eng 282, 17, 2000.
116. Gibson, I., Rosen, D.W., and Stucker, B. Additive Man-ufacturing Technologies. Springer: New York, NY, USA,2010.
117. Melchels, F.P.W., Feijen, J., and Grijpma, D.W. Apoly(d,l-lactide) resin for the preparation of tissue engi-neering scaffolds by stereolithography. Biomaterials 30,3801, 2009.
118. Wang, X., Tuomi, J., Makitie, A., Paloheimo, K.-S.,Partanen, J., and Yliperttula, M. The integrations of bio-materials and rapid prototyping techniques for intelligentmanufacturing of complex organs. Adv Biomater SciBiomed Appl 17, 437, 2013.
119. Koch, L., Deiwick, A., Schlie, S., Michael, S., Gruene,M., Coger, V., Zychlinski, D., Schambach, A., Reimers,K., Vogt, P.M., and Chichkov, B. Skin tissue generationby laser cell printing. Biotechnol Bioeng 109, 1855,2012.
120. Koch, L., Kuhn, S., Sorg, H., Gruene, M., Schlie, S.,Gaebel, R., Polchow, B., Reimers, K., Stoelting, S., Ma,N., Vogt, P.M., Steinhoff, G., and Chichkov, B. Laserprinting of skin cells and human stem cells. Tissue EngPart C Methods 16, 847, 2010.
121. Michael, S., Sorg, H., Peck, C.-T., Koch, L., Deiwick, A.,Chichkov, B., Vogt, P.M., and Reimers, K. Tissue en-gineered skin substitutes created by laser-assisted bio-printing form skin-like structures in the dorsal skin foldchamber in mice. PLoS One 8, e57741, 2013.
122. Schiele, N., Koppes, R.A., Corr, D.T., Ellison, K.S.,Thompson, D.M., Ligon, L.A., Lippert, T.K.M., andChrisey, D.B. Laser direct writing of combinatorial li-braries of idealized cellular constructs: biomedical appli-cations. Appl Surf Sci 255, 5444, 2009.
123. Bae, H., Chu, H., Edalat, F., Cha, J.M., Sant, S., Kashyap,A., Ahari, A.F., Kwon, C.H., Nichol, J.W., Manoucheri,S., Zamanian, B., Wang, Y., and Khademhosseini, A.Development of functional biomaterials with micro- andnanoscale technologies for tissue engineering and drugdelivery applications. J Tissue Eng Regen Med 8, 1, 2014.
124. Bertassoni, L.E., Cardoso, J.C., Manoharan, V., Cristino,A.L., Bhise, N.S., Araujo, W.A., Zorlutuna, P., Vrana,N.E., Ghaemmaghami, A.M., Dokmeci, M.R., and Kha-demhosseini, A. Direct-write bioprinting of cell-ladenmethacrylated gelatin hydrogels. Biofabrication 6, 024105,2014.
125. Nichol, J.W., Koshy, S.T., Bae, H., Hwang, C.M., Ya-manlar, S., and Khademhosseini, A. Cell-laden micro-engineered gelatin methacrylate hydrogels. Biomaterials31, 5536, 2010.
126. Trachtenberg, J.E., Mountziaris, P.M., Miller, J.S., Wet-tergreen, M., Kasper, F.K., and Mikos, A.G. Open-sourcethree-dimensional printing of biodegradable polymerscaffolds for tissue engineering. J Biomed Mater Res A102, 4326, 2014.
127. Boland, T., Mironov, V., Gutowska, A., Roth, E., andMarkwald, R. Cell and organ printing 2: fusion of cellaggregates in three-dimensional gels. Anat Rec A DiscovMol Cell Evol Biol 272A, 497, 2003.
128. Chang, C.C., Boland, E.D., Williams, S.K., and Hoying,J.B. Direct-write bioprinting three-dimensional biohybrid
systems for future regenerative therapies. J Biomed MaterRes B Appl Biomater 98B, 160, 2011.
129. Mironov, V., Boland, T., Trusk, T., Forgacs, G., andMarkwal, R.R. Organ printing: computer-aided jet-based3D tissue engineering. Trends Biotechnol 21, 157, 2003.
130. Fedorovich, N., Dewijn, J., Verbout, A., Alblas, J., andDhert, W.J.A. Three-dimensional fiber deposition of cell-laden, viable, patterned constructs for bone tissue printing.Tissue Eng Part A 14, 127, 2008.
131. Visconti, R.P., Ebihara, Y., LaRue, A.C., Fleming, P.A.,McQuinn, T.C., Masuya, M., Minamiguchi, H., Markwald,R.R., Ogawa, M., and Drake, C.J. An in vivo analysis ofhematopoietic stem cell potential: hematopoietic origin ofcardiac valve interstitial cells. Circ Res 98, 690, 2006.
132. Kim, S.S., Utsunomiya, H., Koski, J.A., Wu, B.M., Cima,M.J., Sohn, J., Mukai, K., Griffith, L.G., and Vacanti, J.P.Survival and function of hepatocytes on a novel three-dimensional synthetic biodegradable polymer scaffoldwith an intrinsic network of channels. Ann Surg 228, 8,1998.
133. Muth, J., Vogt, D., Truby, R., Menguc, Y., Kolesky, D.,Wood, R., and Lewis, J.A. Embedded 3D printing of strainsensors within highly stretchable elastomers. Adv Mater26, 6307, 2014.
134. Osterbur, L.W. 3D printing of hyaluronic acid scaffoldsfor tissue engineering applications [Masters of Science].Materials Science and Engineering, University of Illinoisat Urbana-Champaign, 2013.
135. Schuurman, W., Khristov, V., Pot, M.W., van Weeren,P.R., Dhert, W.J., and Malda, J. Bioprinting of hybridtissue constructs with tailorable mechanical properties.Biofabrication 3, 021001, 2011.
136. Chen, A.A., Tsang, V.L., Albrecht, D.R., and Bhatia, S.N.Chapter 2: 3-D fabrication technology for tissue engineering.In: Ferrari, M., Desai T., Bhatia, S. (Eds.) New York, NY10013, USA. BioMEMS and Biomedical Nanotechnology.Springer, 2007, p. 23.
137. Chen, C.S., Mrksich, M., Huang, S., Whitesides, G.M.,and Ingber, D.E. Geometric control of cell life and death.Science 276, 1425, 1997.
138. Chen, H., and Ozbolat, I.T. A multi-material bioprintingplatform towards stratified articular cartilage tissue fabri-cation. Presented at the Industrial and Systems En-gineering Research Conference, Puerto Rico, 2013.
139. Wang, X., Yan, Y., Pan, Y., Xiong, Z., Liu, H., Cheng, J.,Liu, F., Lin, F., Wu, R., Zhang, R., and Lu, Q. Generationof three-dimensional hepatocyte/gelatin structures withrapid prototyping system. Tissue Eng 12, 83, 2006.
Address correspondence to:Elizabeth Cosgriff-Hernandez, BS, PhDDepartment of Biomedical Engineering
Texas A&M University3120 TAMU
5045 Engineering Technologies BuildingCollege Station, TX 77843-3120
E-mail: [email protected]
Received: October 13, 2015Accepted: January 26, 2016
Online Publication Date: April 8, 2016
310 SEARS ET AL.