Embed Size (px)
Citation preview
REVIEW
A Review of Subthreshold Micropulse Laserfor Treatment of Macular Disorders
Paula Scholz . Lebriz Altay . Sascha Fauser
Received: March 30, 2017 / Published online: May 24, 2017� The Author(s) 2017. This article is an open access publication
ABSTRACT
Micropulse laser treatment is an alternative tothe conventional continuous-wave laser for thetreatment of retinal or macular diseases. Incontrast to the conventional laser, the thera-peutic effect of the subthreshold micropulselaser is not accompanied by thermal retinaldamage. This fact is of particular importancewhen a treatment near the fovea is required.Micropulse treatment is applied in indicationssuch as central serous chorioretinopathy (CSC),diabetic macular edema (DME), or macularedema due to retinal vein occlusion (RVO). Thisreview outlines and discusses the published lit-erature of subthreshold micropulse laser treat-ment for CSC, DME, and macular edema afterRVO.
Keywords: Central serous chorioretinopathy;Diabetic macular edema; Micropulse laser;
Ophthalmology; Retinal vein occlusion;Subthreshold laser
INTRODUCTION
Traditional laser photocoagulation has beenused to treat different retinal diseases for manyyears [1–5]. Here, the endpoint is a visiblewhitening of the retina due to thermal damageof the retinal pigment epithelium (RPE) and theinner retina. However, apart from the favoredtherapeutic effect, the treatment can lead toundesirable side effects like visual field defects,epiretinal fibrosis, and choroidal neovascular-ization (CNV) in the area of the laser scar [6–10].The mechanisms which are responsible for thetherapeutic effect are still poorly understood.
Scarring seems not to be necessary to achievea therapeutic effect. It might be the stimulationof the RPE alone and not the destroying of thephotoreceptors that is needed to reach a thera-peutic effect of laser photocoagulation [11]. Thelaser energy stimulates the RPE, which leads torepair of the inner blood retinal barrier [12]. Amodification of the gene expression initiated bythe wound healing response after laser photo-coagulation could be responsible for the bene-ficial effect of laser photocoagulation.Sublethally injured RPE cells induce an up- anddownregulation of various factors [pigmentepithelium-derived factor (PEDF), vascularendothelial growth factor (VEGF) inhibitors,
Enhanced content To view enhanced content for thisarticle go to http://www.medengine.com/Redeem/4848F0600C509A9C.
P. Scholz (&) � L. Altay � S. FauserDepartment of Ophthalmology, University Hospitalof Cologne, Cologne, Germanye-mail: [email protected]
S. FauserF. Hoffmann-La Roche, Basel, Switzerland
Adv Ther (2017) 34:1528–1555
DOI 10.1007/s12325-017-0559-y
VEGF inducers, permeability factors, etc.] whichrestores the pathologic imbalance. RPE cellsdestroyed by thermal heat are not capable ofinducing this biologic activity [13, 14]. Inagakiet al. [15] showed that sublethal photothermalstimulation with a micropulse laser inducesheat shock protein expression in RPE cellswithout cellular damage in a model of humanRPE.
In subthreshold micropulse laser (SML), dif-fusion of heat to surrounding tissues is mini-mized and thereby scarring is prevented.
The neural retina can be spared by applyingthe minimum laser irradiance (watts per squaremeter) needed to raise the temperature of theRPE, but without exceeding the protein denat-uration threshold. This leads to the requiredactivation of the RPE cells, but the thermal wavewill only reach the neural retina at temperaturesbeneath the protein denaturation threshold.Since the RPE and the neural retina are closetogether, the laser pulse has to be in themicrosecond range and not in the millisecondrange like the traditionally used supra thresholdlaser. For safety reasons it is not possible todeliver the required energy in one short enoughlaser pulse. A single laser pulse would require somuch energy that there would be a high risk ofbubble formation and micro-explosions,accompanied by retinal hemorrhages [16].Those side effects can be avoided by using arepetitive series of very short pulses with lowenergy instead of a continuous-wave laser pulse[17–19].
The micropulse operating mode and termi-nology were described by Dorin [20]. In thetraditional continuous-wave mode, a singlelaser pulse of 0.1–0.5 s delivers the preset laserenergy. In the micropulse mode, a train ofrepetitive short laser pulses delivers the laserenergy within an ‘‘envelope’’ whose width istypically 0.1–0.5s. The normal length of eachpulse is 100–300 ls. The ‘‘envelope’’ includes‘‘ON’’ time, which is the duration of eachmicropulse, and ‘‘OFF’’ time, which is the timebetween the micropulses. The ‘‘OFF’’ time isimportant since here the originated heat cancool down. The sum of the ‘‘ON’’ and ‘‘OFF’’times is the period T and its reciprocal 1/T is thefrequency (pulses per second) f in hertz (Hz).
The duty cycle in percent is the ratio between‘‘ON’’ time and the period T.
DIFFERENT LASERS AVAILABLEWITH MICROPULSE MODE
810-nm Diode Laser
The commercially available diode lasers emit ata wavelength of 810 nm, which is in thenear-infrared range of the spectrum. A feature ofthe 810-nm wavelength is its deep penetrationinto the choroid, but it is not clear if thischaracteristic is relevant in micropulse treat-ment. For all indications requiring a treatmentnear the foveal avascular zone, the 810-nm laserhas the advantage that the laser energy willrelatively spare the inner neurosensory retinaand affect mainly the deeper layers [21–24]. Thedeep penetration is a possible benefit especiallyfor central serous chorioretinopathy (CSC) sincethe choroid may play a role in the pathogenesisof CSC. A potential disadvantage of the 810-nmlaser is a possible sensation of pain duringtreatment with a diode laser [24, 25], althoughthis is a rare problem in the micropulse mode.
577-nm Yellow Laser
Another laser type which is available formicropulse treatment is the 577-nm yellowlaser. The yellow laser has the advantage thatxanthophyll, the pigment which is located inthe inner and outer plexiform layers of themacula, absorbs the yellow light only mini-mally so treatment near the fovea is relativelysafe [26].
APPLICATIONSFOR SUBTHRESHOLD MICROPULSELASERS
In this article we will review the applications formicropulse laser in macular diseases, namelyCSC, diabetic macular edema (DME), and reti-nal vein occlusion (RVO). We will give anoverview of the available literature and outline
Adv Ther (2017) 34:1528–1555 1529

the current evidence for micropulse laser treat-ment in each field.
The literature search was performed in Eng-lish language in the PubMed database. We usedpairings of the terms ‘‘micropulse’’, ‘‘laser’’,‘‘subthreshold’’, and ‘‘central serous chori-oretinopathy’’, ‘‘chorioretinopathy’’, ‘‘centralserous retinopathy’’, or ‘‘diabetic macularedema’’, ‘‘macular edema’’ and ‘‘retinal veinocclusion’’, ‘‘branch retinal vein occlusion’’,‘‘central retinal vein occlusion’’. Additionally,the references of the resultant articles werechecked for publications missing in the primarysearch. Until February 2017 we found 18 articles[27–44] concerning micropulse laser in CSC; noarticles were excluded and all articles are listedin Table 1. As a result of the high number ofpublications related to DME and micropulsetreatment, we only listed the 11 prospectivestudies [45–55] in Table 2. We found four stud-ies [56–59] investigating micropulse laser forRVO, which are all listed in Table 3.
As a result of different study designs, uneveninclusion and exclusion criteria, different lasertypes, treatment parameters, and various out-come measures, a direct comparison of thestudies is limited. We looked for similaritiesreferring to the outcome measures for makingcomprehensive conclusions regarding thetreatment outcome. In Tables 1, 2, and 3, allstudies are listed, but individual studies wereexcluded from the calculations as a result ofmissing information or prior treatment. Thestudies had a high variety regarding the fol-low-up visits. If available, after calculation ofthe decrease in central retinal thickness (CRT)in optical coherence tomography (OCT) in allindividual studies, a weighted average value wascalculated on the basis of the number ofpatients in each study. The best corrected visualacuity (BCVA) was not consistently presented inthe different studies. To compare the BCVA, weconverted all visual acuity data to Early Treat-ment Diabetic Retinopathy Study (ETDRS) let-ters equivalent using the formula ETDRSletters = 85 ? 50 9 log (Snellen fraction) [60]. Ifa large enough number of studies providedinformation about a control group, we addi-tionally analyzed the control group regardingCRT, BCVA, and treatment outcome.
This article was based on previously con-ducted studies and did not involve any newstudies of human or animal subjects performedby any of the authors.
CENTRAL SEROUSCHORIORETINOPATHY (CSC)
In CSC a serous detachment of the neurosensoryretina leads to decreased vision [61]. The acuteform of CSC is often self-limiting so that treat-ment is not always necessary. But some patientsdevelop the chronic form of CSC with impendingpermanent structural damage and vision loss[62–64]. For patients with extrafoveal leakage, acontinuous-wave laser photocoagulation is atreatment option. Studies showed an accelera-tion of subretinal fluid (SRF) resolution but nochange in final visual acuity or recurrence rateafter conventional laser. Furthermore, adverseevents like CNV, scotomas, enlargement of thelaser spot, and reduction of contrast sensitivitycan occur [3, 62, 65–67]. Another treatmentoption is photodynamic therapy (PDT) which isused also in juxtafoveal or subfoveal leakage. Buteven with reduced treatment settings, compli-cations like RPE atrophy, choroidal hypoperfu-sion, transient reduction of macular function,and CNV can occur [68–71].
Bandello et al. [72] presented the first pilotstudy investigating SML treatment for CSC in2003. They reported a high treatment successwith complete resorption of SRF in five out of fiveeyes within 1 month and no recurrence of SRFduring follow-up of 2–6 month after non-visiblesubthreshold micropulse diode laser (810 nm)treatment. No evidence of RPE or retinal changeswas discernible at fluorescein angiography (FA)or fundus biomicroscopy after laser treatment.
Table 1 shows all identified studies investi-gating micropulse laser treatment for CSC. InTable 4, the treatment outcome after SML, PDT,and observation for CSC is presented.
Treatment Response
Most studies defined a treatment response as areduction in CRT measured in spectral domain
1530 Adv Ther (2017) 34:1528–1555
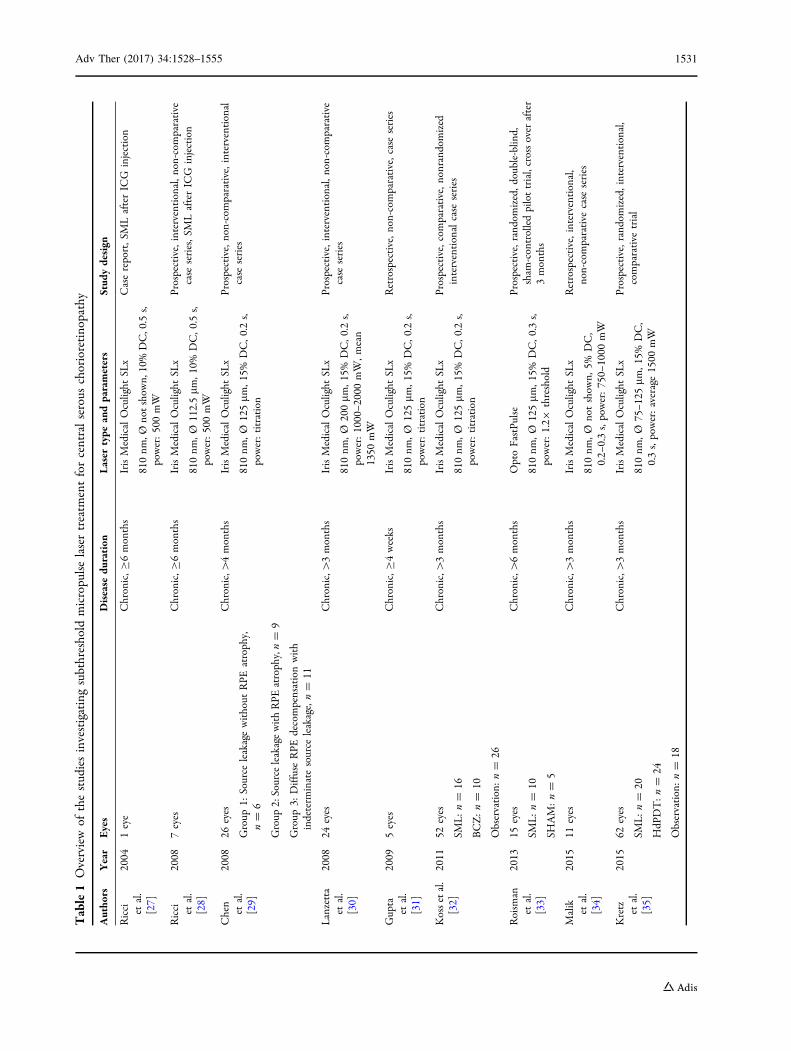
Table1
Overviewof
thestudiesinvestigatingsubthreshold
micropulse
lasertreatm
entforcentralserous
chorioretinopathy
Autho
rsYear
Eyes
Disease
duration
Laser
type
andparameters
Stud
ydesign
Ricci etal.
[27]
2004
1eye
Chronic,C
6months
IrisMedicalOculight
SLx
810nm
,Ønotshow
n,10%DC,0.5s,
power:500mW
Casereport,S
MLafterIC
Ginjection
Ricci etal.
[28]
2008
7eyes
Chronic,C
6months
IrisMedicalOculight
SLx
810nm
,Ø112.5lm
,10%
DC,0
.5s,
power:500mW
Prospective,interventional,n
on-com
parative
case
series,S
MLafterIC
Ginjection
Chen
etal.
[29]
2008
26eyes
Group
1:Source
leakagewithout
RPE
atrophy,
n=
6
Group
2:Source
leakagewithRPE
atrophy,n=
9
Group
3:DiffuseRPE
decompensationwith
indeterm
inatesource
leakage,n=
11
Chronic,[
4months
IrisMedicalOculight
SLx
810nm
,Ø125lm,1
5%DC,0
.2s,
power:titration
Prospective,non-comparative,interventional
case
series
Lanzetta
etal.
[30]
2008
24eyes
Chronic,[
3months
IrisMedicalOculight
SLx
810nm
,Ø200lm,1
5%DC,0
.2s,
power:1000–2
000mW,m
ean
1350
mW
Prospective,interventional,n
on-com
parative
case
series
Gupta
etal.
[31]
2009
5eyes
Chronic,C
4weeks
IrisMedicalOculight
SLx
810nm
,Ø125lm,1
5%DC,0
.2s,
power:titration
Retrospective,n
on-com
parative,caseseries
Kossetal.
[32]
2011
52eyes
SML:n=
16
BCZ:n=
10
Observation:n=
26
Chronic,[
3months
IrisMedicalOculight
SLx
810nm
,Ø125lm,1
5%DC,0
.2s,
power:titration
Prospective,comparative,n
onrand
omized
interventionalcase
series
Roism
anet
al.
[33]
2013
15eyes
SML:n=
10
SHAM:n=
5
Chronic,[
6months
OptoFastPu
lse
810nm
,Ø125lm,1
5%DC,0
.3s,
power:1.29
threshold
Prospective,rand
omized,d
ouble-blind,
sham
-controlledpilottrial,crossover
after
3months
Malik etal.
[34]
2015
11eyes
Chronic,[
3months
IrisMedicalOculight
SLx
810nm
,Ønotshow
n,5%
DC,
0.2–
0.3s,power:750–
1000
mW
Retrospective,interventional,
non-comparative
case
series
Kretz etal.
[35]
2015
62eyes
SML:n=
20
HdP
DT:n=
24
Observation:n=
18
Chronic,[
3months
IrisMedicalOculight
SLx
810nm
,Ø75–1
25lm,1
5%DC,
0.3s,power:average1500
mW
Prospective,rand
omized,interventional,
comparative
trial
Adv Ther (2017) 34:1528–1555 1531
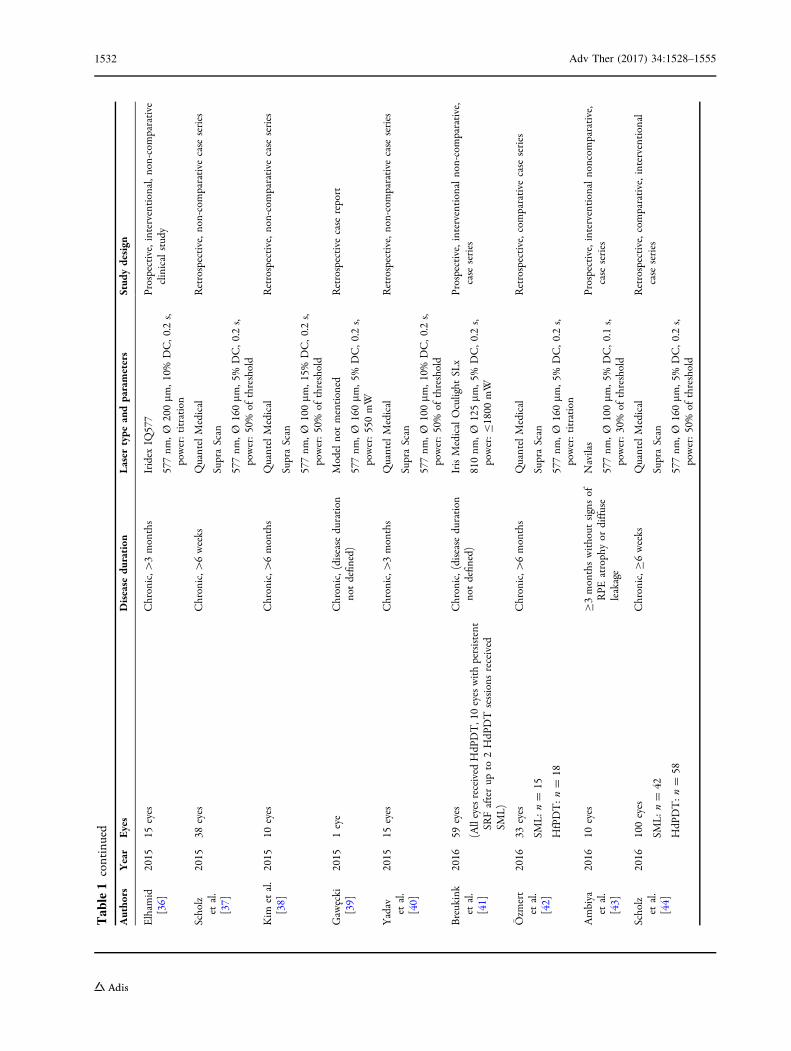
Table1
continued
Autho
rsYear
Eyes
Disease
duration
Laser
type
andparameters
Stud
ydesign
Elham
id[36]
2015
15eyes
Chronic,[
3months
Iridex
IQ577
577nm
,Ø200lm,1
0%DC,0
.2s,
power:titration
Prospective,interventional,n
on-com
parative
clinicalstudy
Scholz
etal.
[37]
2015
38eyes
Chronic,[
6weeks
QuantelMedical
SupraScan
577nm
,Ø160lm,5
%DC,0
.2s,
power:50%
ofthreshold
Retrospective,n
on-com
parative
case
series
Kim
etal.
[38]
2015
10eyes
Chronic,[
6months
QuantelMedical
SupraScan
577nm
,Ø100lm,1
5%DC,0
.2s,
power:50%
ofthreshold
Retrospective,n
on-com
parative
case
series
Gaw
ecki
[39]
2015
1eye
Chronic,(diseaseduration
notdefin
ed)
Modelnotmentioned
577nm
,Ø160lm,5
%DC,0
.2s,
power:550mW
Retrospective
case
report
Yadav etal.
[40]
2015
15eyes
Chronic,[
3months
QuantelMedical
SupraScan
577nm
,Ø100lm,1
0%DC,0
.2s,
power:50%
ofthreshold
Retrospective,n
on-com
parative
case
series
Breukink
etal.
[41]
2016
59eyes
(Alleyesreceived
HdP
DT,10eyeswithpersistent
SRFafterup
to2HdP
DT
sessions
received
SML)
Chronic,(diseaseduration
notdefin
ed)
IrisMedicalOculight
SLx
810nm
,Ø125lm,5
%DC,0
.2s,
power:B1800
mW
Prospective,interventionalnon-comparative,
case
series
Ozm
ert
etal.
[42]
2016
33eyes
SML:n=
15
HfPDT:n=
18
Chronic,[
6months
QuantelMedical
SupraScan
577nm
,Ø160lm,5
%DC,0
.2s,
power:titration
Retrospective,com
parative
case
series
Ambiya
etal.
[43]
2016
10eyes
C3monthswithout
signsof
RPE
atrophyor
diffuse
leakage
Navilas
577nm
,Ø100lm,5
%DC,0
.1s,
power:30%
ofthreshold
Prospective,interventionalnoncom
parative,
case
series
Scholz
etal.
[44]
2016
100eyes
SML:n=
42
HdP
DT:n=
58
Chronic,C
6weeks
QuantelMedical
SupraScan
577nm
,Ø160lm,5
%DC,0
.2s,
power:50%
ofthreshold
Retrospective,com
parative,interventional
case
series
1532 Adv Ther (2017) 34:1528–1555
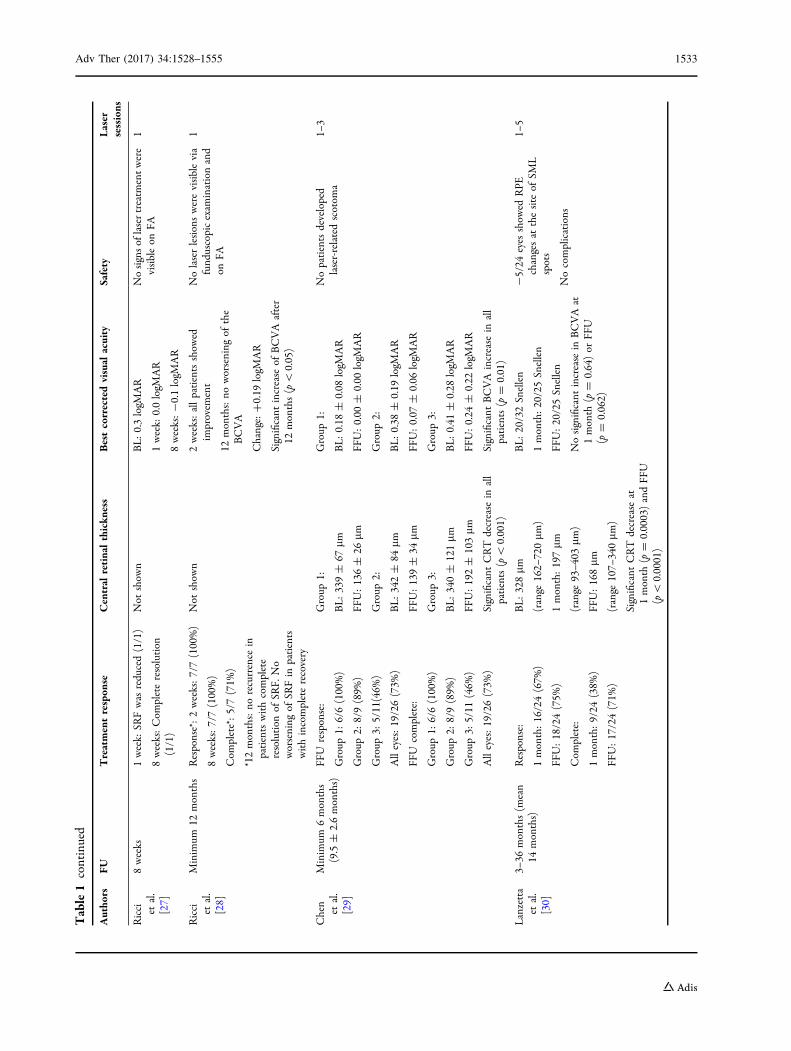
Table1
continued
Autho
rsFU
Treatmentrespon
seCentral
retinalthickn
ess
Bestcorrectedvisual
acuity
Safety
Laser
sessions
Ricci etal.
[27]
8weeks
1week:
SRFwas
reduced(1/1)
Not
show
nBL:0.3logM
AR
1week:
0.0logM
AR
8weeks:-0.1logM
AR
Nosignsof
lasertreatm
entwere
visibleon
FA1
8weeks:Com
pleteresolution
(1/1)
Ricci etal.
[28]
Minim
um12
months
Response*:2weeks:7/7(100%)
8weeks:7/7(100%)
Com
plete*:5/7(71%
)
*12months:no
recurrence
inpatientswithcomplete
resolution
ofSR
F.No
worsening
ofSR
Fin
patients
withincompleterecovery
Not
show
n2weeks:allpatientsshow
edim
provem
ent
12months:no
worsening
ofthe
BCVA
Change:?0.19
logM
AR
Significant
increase
ofBCVA
after
12months(p\
0.05)
Nolaserlesionswerevisiblevia
fund
uscopicexam
inationand
onFA
1
Chen
etal.
[29]
Minim
um6months
(9.5±
2.6months)
FFU
response:
Group
1:6/6(100%)
Group
2:8/9(89%
)
Group
3:5/11(46%
)
Alleyes:19/26(73%
)
Group
1:
BL:339±
67lm
FFU:136±
26lm
Group
2:
BL:342±
84lm
FFU:139±
34lm
Group
3:
BL:340±
121lm
FFU:192±
103lm
Significant
CRT
decrease
inall
patients(p\
0.001)
Group
1:
BL:0.18
±0.08
logM
AR
FFU:0.00
±0.00
logM
AR
Group
2:
BL:0.38
±0.19
logM
AR
FFU:0.07
±0.06
logM
AR
Group
3:
BL:0.41
±0.28
logM
AR
FFU:0.24
±0.22
logM
AR
Significant
BCVA
increase
inall
patients(p
=0.01)
Nopatientsdeveloped
laser-relatedscotom
a1–
3
FFU
complete:
Group
1:6/6(100%)
Group
2:8/9(89%
)
Group
3:5/11
(46%
)
Alleyes:19/26(73%
)
Lanzetta
etal.
[30]
3–36
months(m
ean
14months)
Response:
1month:16/24(67%
)
FFU:18/24(75%
)
BL:328lm
(range
162–
720lm)
1month:197lm
(range
93–4
03lm
)
FFU:168lm
(range
107–
340lm)
Significant
CRT
decrease
at1month
(p=
0.0003)andFF
U(p\
0.0001)
BL:20/32Snellen
1month:20/25Snellen
FFU:20/25Snellen
Nosignificant
increase
inBCVAat
1month
(p=
0.64)or
FFU
(p=
0.062)
-5/24
eyes
show
edRPE
changesat
thesite
ofSM
Lspots
Nocomplications
1–5
Com
plete:
1month:9/24
(38%
)
FFU:17/24(71%
)
Adv Ther (2017) 34:1528–1555 1533
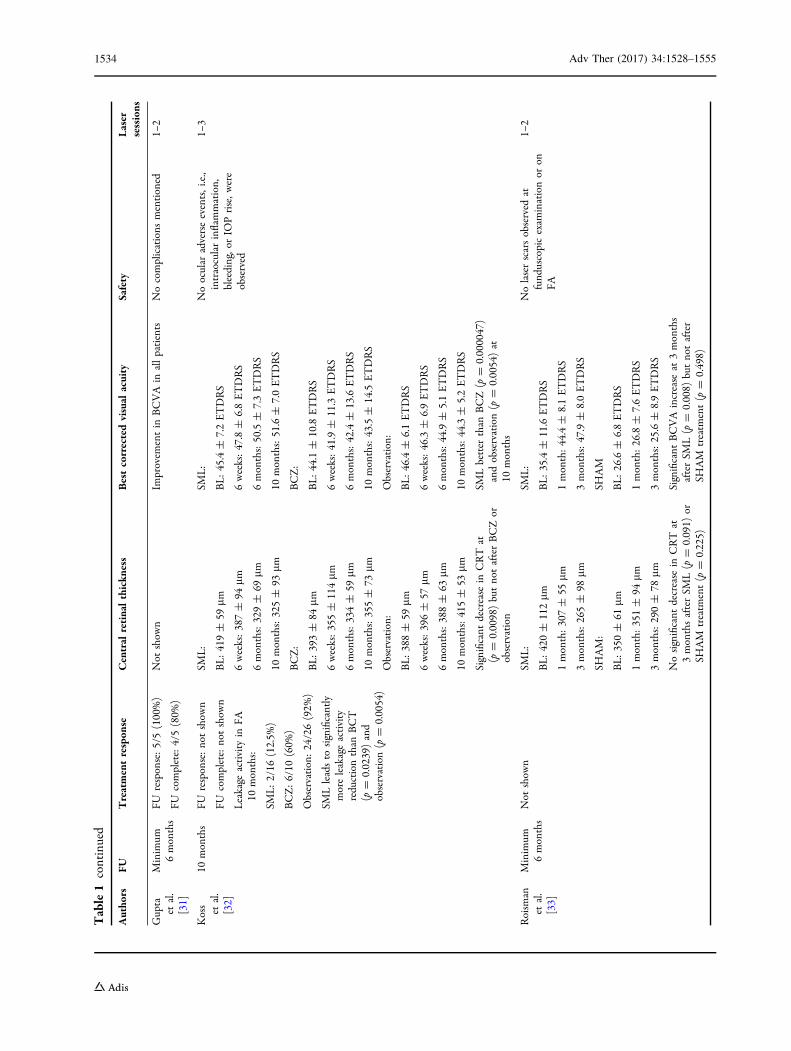
Table1
continued
Autho
rsFU
Treatmentrespon
seCentral
retinalthickn
ess
Bestcorrectedvisual
acuity
Safety
Laser
sessions
Gupta
etal.
[31]
Minim
um6months
FUresponse:5/5(100%)
Not
show
nIm
provem
entin
BCVA
inallpatients
Nocomplications
mentioned
1–2
FUcomplete:4/5(80%
)
Koss etal.
[32]
10months
FUresponse:notshow
n
FUcomplete:notshow
n
Leakage
activity
inFA
10months:
SML:2/16
(12.5%
)
BCZ:6/10
(60%
)
Observation:24/26(92%
)
SMLleadsto
significantly
moreleakageactivity
reductionthan
BCT
(p=
0.0239)and
observation(p
=0.0054)
SML:
BL:419±
59lm
6weeks:387±
94lm
6months:329±
69lm
10months:325±
93lm
BCZ:
BL:393±
84lm
6weeks:355±
114lm
6months:334±
59lm
10months:355±
73lm
Observation:
BL:388±
59lm
6weeks:396±
57lm
6months:388±
63lm
10months:415±
53lm
Significant
decrease
inCRT
at(p
=0.0098)butnotafterBCZor
observation
SML:
BL:45.4±
7.2ETDRS
6weeks:47.8±
6.8ETDRS
6months:50.5±
7.3ETDRS
10months:51.6±
7.0ETDRS
BCZ:
BL:44.1±
10.8
ETDRS
6weeks:41.9±
11.3
ETDRS
6months:42.4±
13.6
ETDRS
10months:43.5±
14.5
ETDRS
Observation:
BL:46.4±
6.1ETDRS
6weeks:46.3±
6.9ETDRS
6months:44.9±
5.1ETDRS
10months:44.3±
5.2ETDRS
SMLbetter
than
BCZ(p
=0.000047)
andobservation(p
=0.0054)at
10months
Noocular
adverseevents,i.e.,
intraocularinflammation,
bleeding,o
rIO
Prise,w
ere
observed
1–3
Roism
anet
al.
[33]
Minim
um6months
Not
show
nSM
L:
BL:420±
112lm
1month:307±
55lm
3months:265±
98lm
SHAM:
BL:350±
61lm
1month:351±
94lm
3months:290±
78lm
Nosignificant
decrease
inCRTat
3monthsafterSM
L(p
=0.091)
orSH
AM
treatm
ent(p
=0.225)
SML:
BL:35.4±
11.6
ETDRS
1month:44.4±
8.1ETDRS
3months:47.9±
8.0ETDRS
SHAM
BL:26.6±
6.8ETDRS
1month:26.8±
7.6ETDRS
3months:25.6±
8.9ETDRS
Significant
BCVA
increase
at3months
afterSM
L(p
=0.008)
butnotafter
SHAM
treatm
ent(p
=0.498)
Nolaserscarsobserved
atfund
uscopicexam
inationor
onFA
1–2
1534 Adv Ther (2017) 34:1528–1555
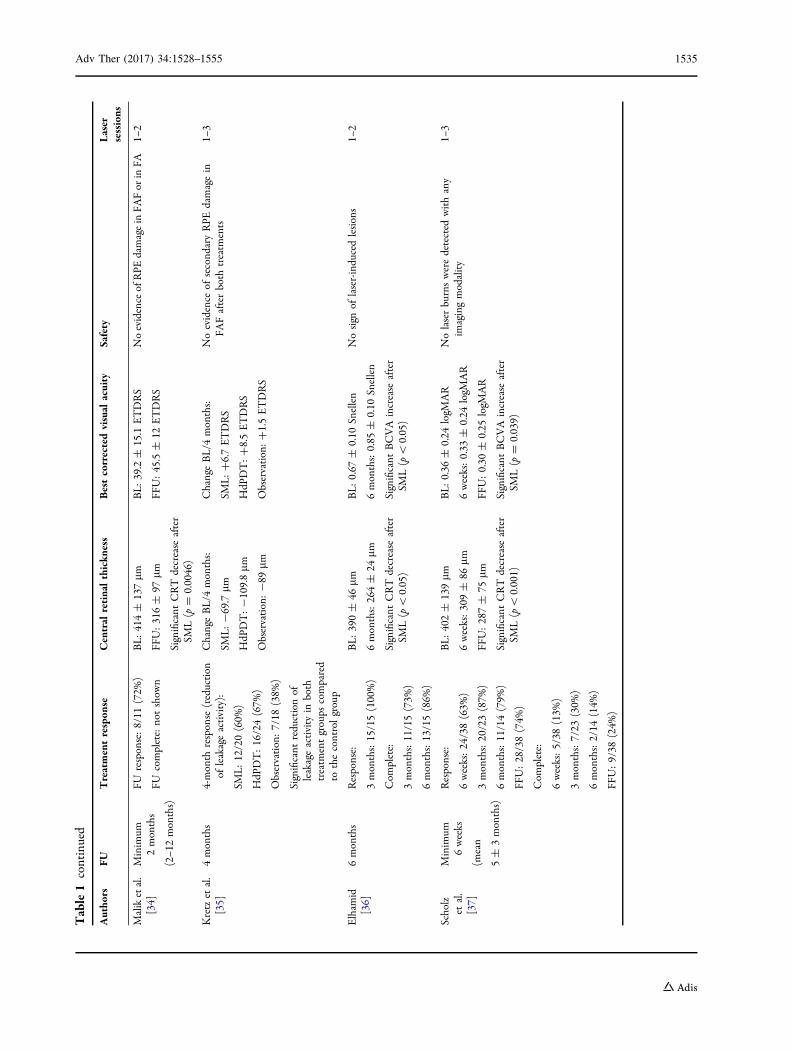
Table1
continued
Autho
rsFU
Treatmentrespon
seCentral
retinalthickn
ess
Bestcorrectedvisual
acuity
Safety
Laser
sessions
Maliketal.
[34]
Minim
um2months
(2–1
2months)
FUresponse:8/11
(72%
)
FUcomplete:notshow
n
BL:414±
137lm
FFU:316±
97lm
Significant
CRTdecrease
after
SML(p
=0.0046)
BL:39.2±
15.1
ETDRS
FFU:45.5±
12ETDRS
Noevidence
ofRPE
damagein
FAFor
inFA
1–2
Kretz
etal.
[35]
4months
4-month
response
(reduction
ofleakageactivity):
SML:12/20(60%
)
HdP
DT:16/24(67%
)
Observation:7/18
(38%
)
Significant
reductionof
leakageactivity
inboth
treatm
entgroups
compared
tothecontrolgroup
ChangeBL/4
months:
SML:-69.7lm
HdP
DT:-109.8lm
Observation:-89
lm
ChangeBL/4
months:
SML:?6.7ETDRS
HdP
DT:?8.5ETDRS
Observation:?1.5ETDRS
Noevidence
ofsecond
aryRPE
damagein
FAFafterboth
treatm
ents
1–3
Elham
id[36]
6months
Response:
3months:15/15(100%)
BL:390±
46lm
6months:264±
24lm
Significant
CRTdecrease
after
SML(p\
0.05)
BL:0.67
±0.10
Snellen
6months:0.85
±0.10
Snellen
Significant
BCVA
increase
after
SML( p\
0.05)
Nosign
oflaser-inducedlesions
1–2
Com
plete:
3months:11/15(73%
)
6months:13/15(86%
)
Scholz
etal.
[37]
Minim
um6weeks
(mean
5±
3months)
Response:
6weeks:24/38(63%
)
3months:20/23(87%
)
6months:11/14(79%
)
FFU:28/38(74%
)
BL:402±
139lm
6weeks:309±
86lm
FFU:287±
75lm
Significant
CRTdecrease
after
SML(p\
0.001)
BL:0.36
±0.24
logM
AR
6weeks:0.33
±0.24
logM
AR
FFU:0.30
±0.25
logM
AR
Significant
BCVA
increase
after
SML(p
=0.039)
Nolaserburnsweredetected
withany
imagingmodality
1–3
Com
plete:
6weeks:5/38
(13%
)
3months:7/23
(30%
)
6months:2/14
(14%
)
FFU:9/38
(24%
)
Adv Ther (2017) 34:1528–1555 1535
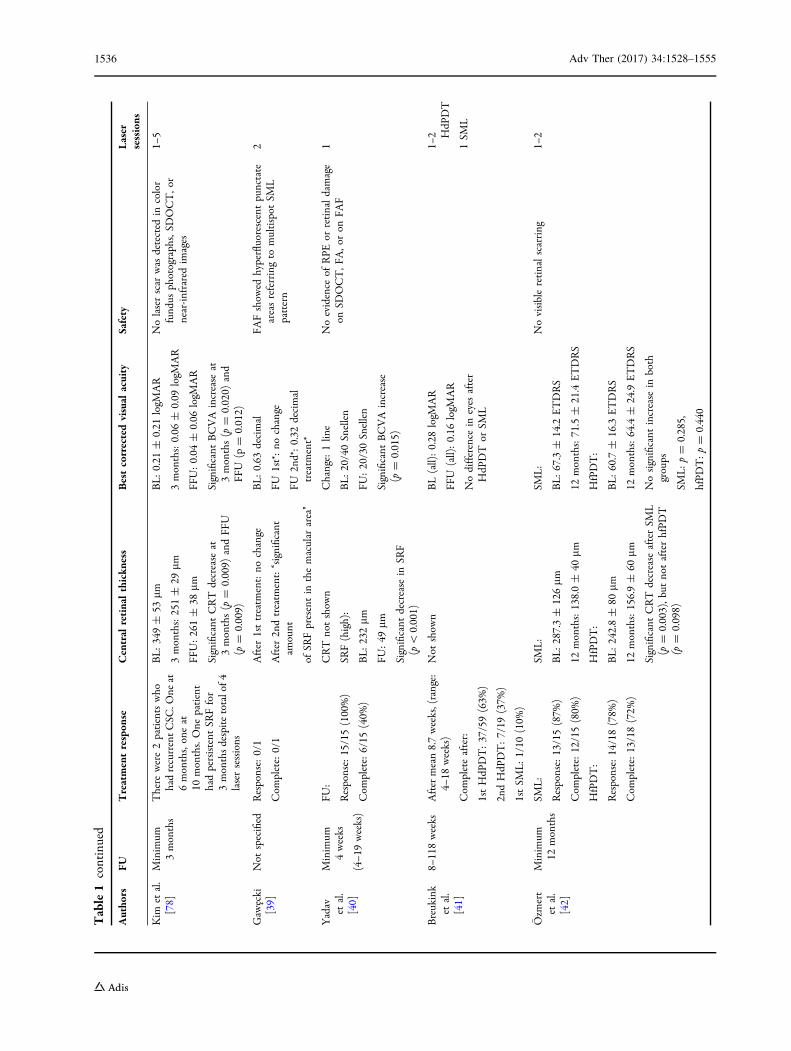
Table1
continued
Autho
rsFU
Treatmentrespon
seCentral
retinalthickn
ess
Bestcorrectedvisual
acuity
Safety
Laser
sessions
Kim
etal.
[78]
Minim
um3months
There
were2patientswho
hadrecurrentCSC
.One
at6months,oneat
10months.One
patient
hadpersistent
SRFfor
3monthsdespitetotalof4
lasersessions
BL:349±
53lm
3months:251±
29lm
FFU:261±
38lm
Significant
CRT
decrease
at3months(p
=0.009)
andFF
U(p
=0.009)
BL:0.21
±0.21
logM
AR
3months:0.06
±0.09
logM
AR
FFU:0.04
±0.06
logM
AR
Significant
BCVA
increase
at3months(p
=0.020)
and
FFU
(p=
0.012)
Nolaserscar
was
detected
incolor
fund
usphotographs,SD
OCT,o
rnear-in
frared
images
1–5
Gaw
ecki
[39]
Not
specified
Response:0/1
After
1sttreatm
ent:no
change
After
2ndtreatm
ent:‘‘significant
amount
ofSR
Fpresentin
themacular
area’’
BL:0.63
decimal
FU1st*:no
change
FU2nd*:0.32
decimal
treatm
ent*
FAFshow
edhyperfluorescentpunctate
areasreferringto
multispot
SML
pattern
2
Com
plete:0/1
Yadav etal.
[40]
Minim
um4weeks
(4–1
9weeks)
FU:
Response:15/15(100%)
Com
plete:6/15
(40%
)
CRT
notshow
n
SRF(high):
BL:232lm
FU:49
lm
Significant
decrease
inSR
F(p\
0.001)
Change:1lin
e
BL:20/40Snellen
FU:20/30Snellen
Significant
BCVA
increase
(p=
0.015)
Noevidence
ofRPE
orretinaldamage
onSD
OCT,F
A,o
ron
FAF
1
Breukink
etal.
[41]
8–118weeks
Aftermean8.7weeks,(range:
4–18
weeks)
Com
pleteafter:
1stHdP
DT:37/59(63%
)
2ndHdP
DT:7/19
(37%
)
1stSM
L:1/10
(10%
)
Not
show
nBL(all):0.28
logM
AR
FFU
(all):0.16
logM
AR
Nodifference
ineyes
after
HdP
DT
orSM
L
1–2 HdP
DT
1SM
L
Ozm
ert
etal.
[42]
Minim
um12
months
SML:
Response:13/15(87%
)
Com
plete:12/15(80%
)
HfPDT:
Response:14/18(78%
)
Com
plete:13/18(72%
)
SML:
BL:287.3±
126lm
12months:138.0±
40lm
HfPDT:
BL:242.8±
80lm
12months:156.9±
60lm
Significant
CRT
decrease
afterSM
L(p
=0.003),b
utnotafterhfPD
T(p
=0.098)
SML:
BL:67.3±
14.2
ETDRS
12months:71.5±
21.4
ETDRS
HfPDT:
BL:60.7±
16.3
ETDRS
12months:64.4±
24.9
ETDRS
Nosignificant
increase
inboth
groups
SML:p=
0.285,
hfPD
T:p=
0.440
Novisibleretinalscarring
1–2
1536 Adv Ther (2017) 34:1528–1555
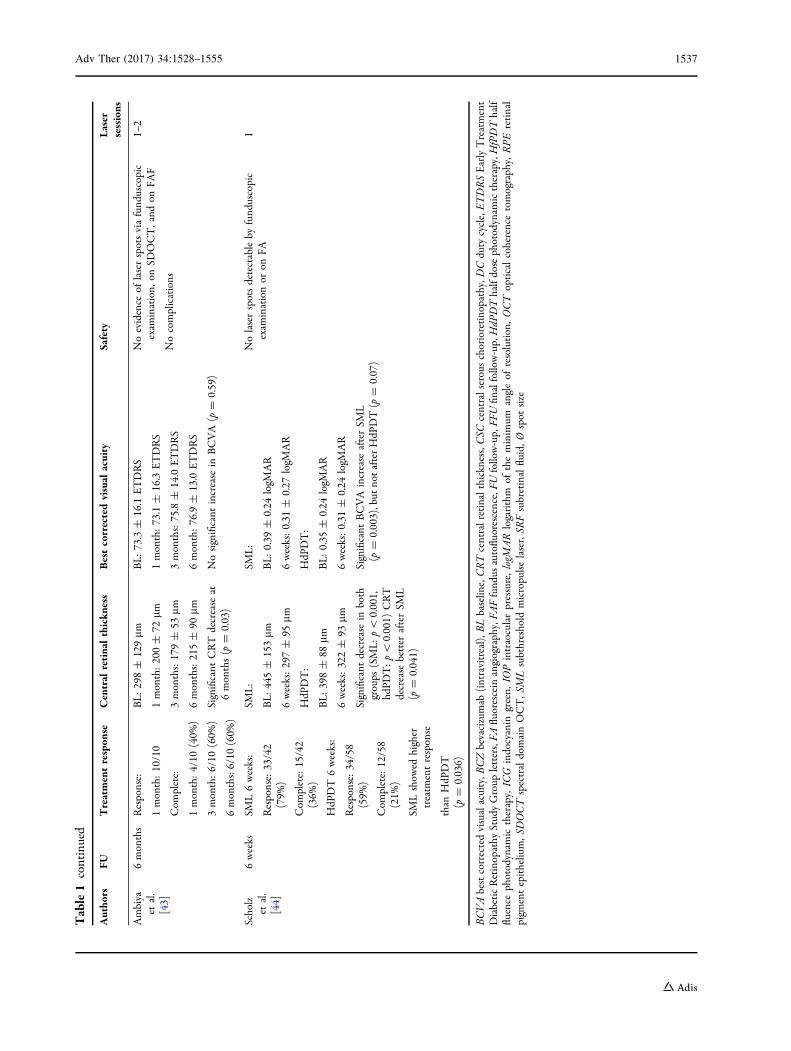
Table1
continued
Autho
rsFU
Treatmentrespon
seCentral
retinalthickn
ess
Bestcorrectedvisual
acuity
Safety
Laser
sessions
Ambiya
etal.
[43]
6months
Response:
1month:10/10
Com
plete:
1month:4/10
(40%
)
3month:6/10
(60%
)
6months:6/10
(60%
)
BL:298±
129lm
1month:200±
72lm
3months:179±
53lm
6months:215±
90lm
Significant
CRTdecrease
at6months(p
=0.03)
BL:73.3±
16.1
ETDRS
1month:73.1±
16.3
ETDRS
3months:75.8±
14.0
ETDRS
6month:76.9±
13.0
ETDRS
Nosignificant
increase
inBCVA
(p=
0.59)
Noevidence
oflaserspotsviafund
uscopic
exam
ination,
onSD
OCT,and
onFA
F
Nocomplications
1–2
Scholz
etal.
[44]
6weeks
SML6weeks:
Response:33/42
(79%
)
Com
plete:15/42
(36%
)
HdP
DT
6weeks:
Response:34/58
(59%
)
Com
plete:12/58
(21%
)
SMLshow
edhigher
treatm
entresponse
than
HdP
DT
(p=
0.036)
SML:
BL:445±
153lm
6weeks:297±
95lm
HdP
DT:
BL:398±
88lm
6weeks:322±
93lm
Significant
decrease
inboth
groups
(SML:p\
0.001,
hdPD
T:p \
0.001)
CRT
decrease
better
afterSM
L(p
=0.041)
SML:
BL:0.39
±0.24
logM
AR
6weeks:0.31
±0.27
logM
AR
HdP
DT:
BL:0.35
±0.24
logM
AR
6weeks:0.31
±0.24
logM
AR
Significant
BCVA
increase
afterSM
L(p
=0.003),but
notafterHdP
DT(p
=0.07)
Nolaserspotsdetectableby
fund
uscopic
exam
inationor
onFA
1
BCVAbestcorrectedvisualacuity,B
CZbevacizumab
(intravitreal),B
Lbaselin
e,CRTcentralretinalthickness,CSC
centralserouschorioretinopathy,DCduty
cycle,ETDRSEarlyTreatment
DiabeticRetinopathy
StudyGroup
letters,FA
fluorescein
angiography,FA
Ffund
usautofluorescence,FU
follow-up,FF
Ufin
alfollow-up,HdP
DThalfdosephotodynam
ictherapy,HfPDThalf
fluence
photodynam
ictherapy,ICG
indocyanin
green,
IOPintraocularpressure,logM
ARlogarithm
oftheminim
umangleof
resolution,OCT
opticalcoherencetomography,RPE
retinal
pigm
entepithelium,S
DOCTspectraldomainOCT,S
MLsubthreshold
micropulse
laser,SR
Fsubretinalfluid,Ø
spot
size
Adv Ther (2017) 34:1528–1555 1537
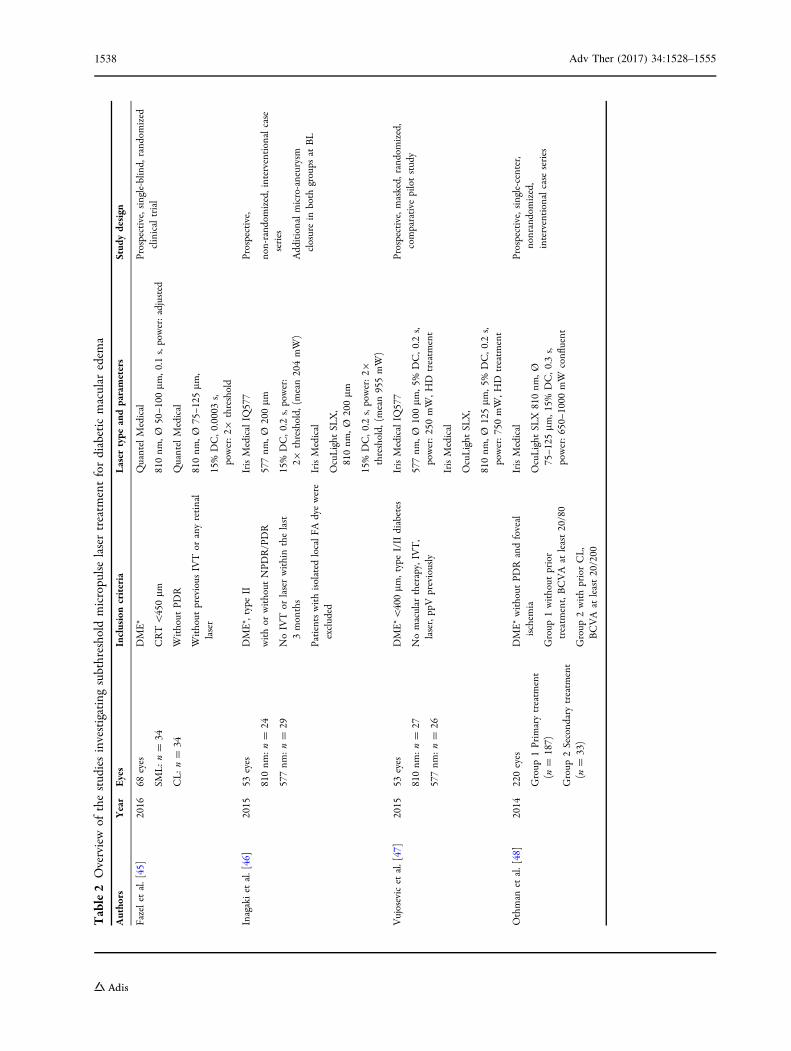
Table2
Overviewof
thestudiesinvestigatingsubthreshold
micropulse
lasertreatm
entfordiabeticmacular
edem
a
Autho
rsYear
Eyes
Inclusioncriteria
Laser
type
andparameters
Stud
ydesign
Fazelet
al.[45]
2016
68eyes
SML:n=
34
CL:n=
34
DME*
CRT\450lm
Without
PDR
Without
previous
IVTor
anyretinal
laser
QuantelMedical
810nm
,Ø50–1
00lm,0
.1s,power:adjusted
QuantelMedical
810nm
,Ø75–1
25lm,
15%
DC,0
.0003s,
power:29
threshold
Prospective,single-blin
d,rand
omized
clinicaltrial
Inagakiet
al.[46]
2015
53eyes
810nm
:n=
24
577nm
:n=
29
DME*,type
II
withor
without
NPD
R/PDR
NoIVTor
laserwithinthelast
3months
Patientswithisolated
localF
Adyewere
excluded
IrisMedicalIQ
577
577nm
,Ø200lm
15%
DC,0
.2s,power:
29threshold,
(mean204mW)
IrisMedical
OcuLight
SLX,
810nm
,Ø200lm
15%
DC,0
.2s,power:29
threshold,
(mean955mW)
Prospective,
non-rand
omized,interventionalcase
series
Additionalmicro-aneurysm
closurein
both
groups
atBL
Vujosevicet
al.[47]
2015
53eyes
810nm
:n=
27
577nm
:n=
26
DME*\
400lm
,typeI/IIdiabetes
Nomacular
therapy,IVT,
laser,ppVpreviously
IrisMedicalIQ
577
577nm
,Ø100lm
,5%
DC,0
.2s,
power:250mW,H
Dtreatm
ent
IrisMedical
OcuLight
SLX,
810nm
,Ø125lm
,5%
DC,0
.2s,
power:750mW,H
Dtreatm
ent
Prospective,masked,
rand
omized,
comparative
pilotstudy
Othman
etal.[48]
2014
220eyes
Group
1Prim
arytreatm
ent
(n=
187)
Group
2Second
arytreatm
ent
(n=
33)
DME*without
PDRandfoveal
ischem
ia
Group
1without
prior
treatm
ent,BCVA
atleast20/80
Group
2withpriorCL,
BCVA
atleast20/200
IrisMedical
OcuLight
SLX
810nm
,Ø75–1
25lm
,15%
DC,0
.3s,
power:650–
1000
mW
confl
uent
Prospective,single-center,
nonrandomized,
interventionalcase
series
1538 Adv Ther (2017) 34:1528–1555
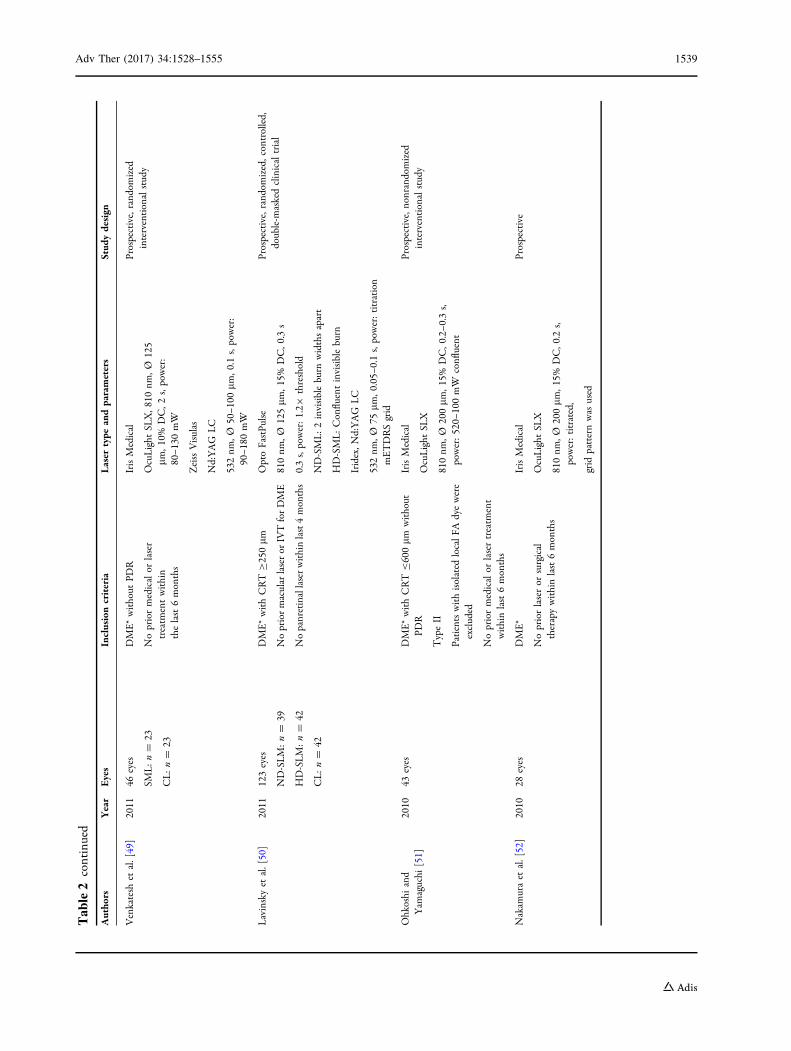
Table2
continued
Autho
rsYear
Eyes
Inclusioncriteria
Laser
type
andparameters
Stud
ydesign
Venkatesh
etal.[49]
2011
46eyes
SML:n=
23
CL:n=
23
DME*without
PDR
Nopriormedicalor
laser
treatm
entwithin
thelast6months
IrisMedical
OcuLight
SLX,8
10nm
,Ø125
lm,1
0%DC,2
s,power:
80–1
30mW
ZeissVisulas
Nd:YAG
LC
532nm
,Ø50–1
00lm,0
.1s,power:
90–1
80mW
Prospective,rand
omized
interventionalstudy
Lavinskyet
al.[50]
2011
123eyes
ND-SLM
:n=
39
HD-SLM
:n=
42
CL:n=
42
DME*withCRTC250lm
Nopriormacularlaseror
IVTforDME
Nopanretinallaserwithinlast4months
OptoFastPu
lse
810nm
,Ø125lm
,15%
DC,0
.3s
0.3s,power:1.29
threshold
ND-SML:2invisibleburn
widthsapart
HD-SML:Confluentinvisibleburn
Iridex,N
d:YAG
LC
532nm
,Ø75
lm,0
.05–
0.1s,power:titration
mETDRSgrid
Prospective,rand
omized,controlled,
double-m
askedclinicaltrial
Ohkoshi
and
Yam
aguchi
[51]
2010
43eyes
DME*withCRTB600lm
without
PDR
TypeII
Patientswithisolated
localF
Adyewere
excluded
Nopriormedicalor
lasertreatm
ent
withinlast6months
IrisMedical
OcuLight
SLX
810nm
,Ø200lm
,15%
DC,0
.2–0
.3s,
power:520–
100mW
confl
uent
Prospective,nonrandomized
interventionalstudy
Nakam
uraet
al.[52]
2010
28eyes
DME*
Nopriorlaseror
surgical
therapywithinlast6months
IrisMedical
OcuLight
SLX
810nm
,Ø200lm
,15%
DC,0
.2s,
power:titrated,
grid
patternwas
used
Prospective
Adv Ther (2017) 34:1528–1555 1539
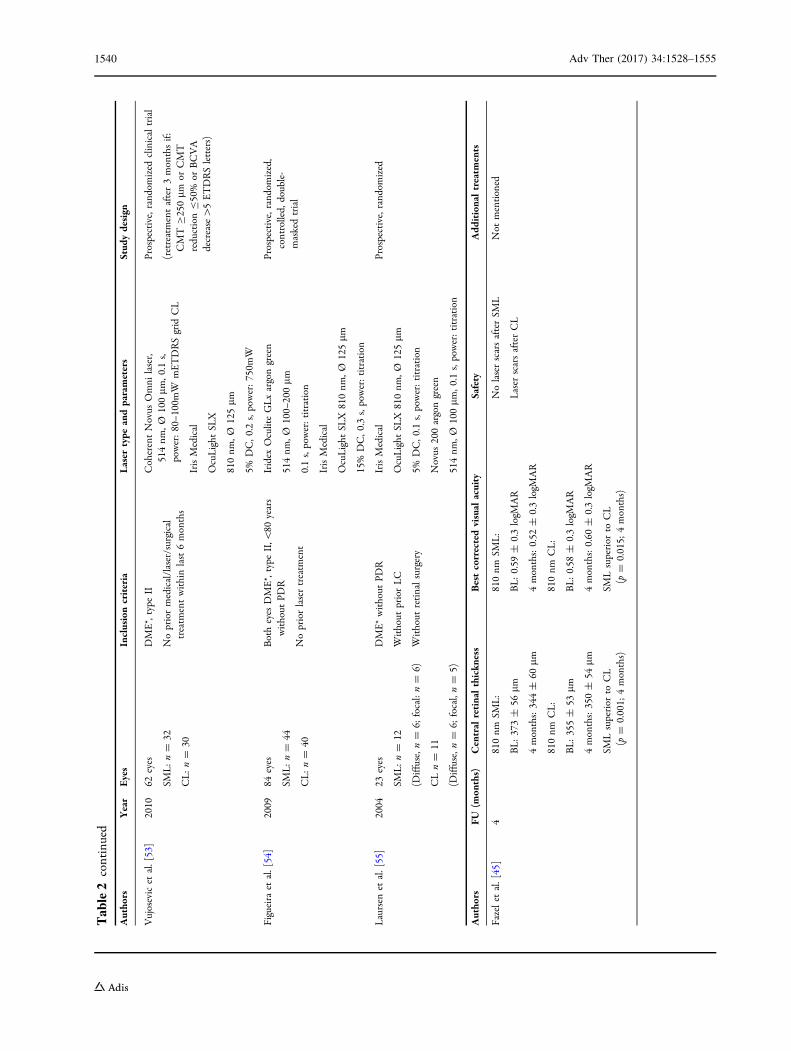
Table2
continued
Autho
rsYear
Eyes
Inclusioncriteria
Laser
type
andparameters
Stud
ydesign
Vujosevicet
al.[53]
2010
62eyes
SML:n=
32
CL:n=
30
DME*,type
II
Nopriormedical/laser/surgical
treatm
entwithinlast6months
CoherentNovus
Omni
laser,
514nm
,Ø100lm,0
.1s,
power:80–1
00mW
mETDRSgrid
CL
IrisMedical
OcuLight
SLX
810nm
,Ø125lm
5%DC,0
.2s,power:750m
W
Prospective,rand
omized
clinicaltrial
(retreatmentafter3monthsif:
CMTC250lm
orCMT
reductionB50%
orBCVA
decrease[5ETDRSletters)
Figueira
etal.[54]
2009
84eyes
SML:n=
44
CL:n=
40
Botheyes
DME*,type
II,\
80years
without
PDR
Nopriorlasertreatm
ent
Iridex
OculiteGLxargongreen
514nm
,Ø100–
200lm
0.1s,power:titration
IrisMedical
OcuLight
SLX
810nm
,Ø125lm
15%
DC,0
.3s,power:titration
Prospective,rand
omized,
controlled,
double-
maskedtrial
Laursen
etal.[55]
2004
23eyes
SML:n=
12
(Diffuse,n=
6;focal:n=
6)
CLn=
11
(Diffuse,n=
6;focal,n=
5)
DME*without
PDR
Without
priorLC
Without
retinalsurgery
IrisMedical
OcuLight
SLX
810nm
,Ø125lm
5%DC,0
.1s,power:titration
Novus
200argongreen
514nm
,Ø100lm
,0.1s,power:titration
Prospective,rand
omized
Autho
rsFU
(mon
ths)
Central
retinalthickn
ess
Bestcorrectedvisual
acuity
Safety
Add
itionaltreatm
ents
Fazelet
al.[45]
4810nm
SML:
BL:373±
56lm
4months:344±
60lm
810nm
CL:
BL:355±
53lm
4months:350±
54lm
SMLsuperior
toCL
(p=
0.001;
4months)
810nm
SML:
BL:0.59
±0.3logM
AR
4months:0.52
±0.3logM
AR
810nm
CL:
BL:0.58
±0.3logM
AR
4months:0.60
±0.3logM
AR
SMLsuperior
toCL
(p=
0.015;
4months)
NolaserscarsafterSM
L
Laser
scarsafterCL
Not
mentioned
1540 Adv Ther (2017) 34:1528–1555
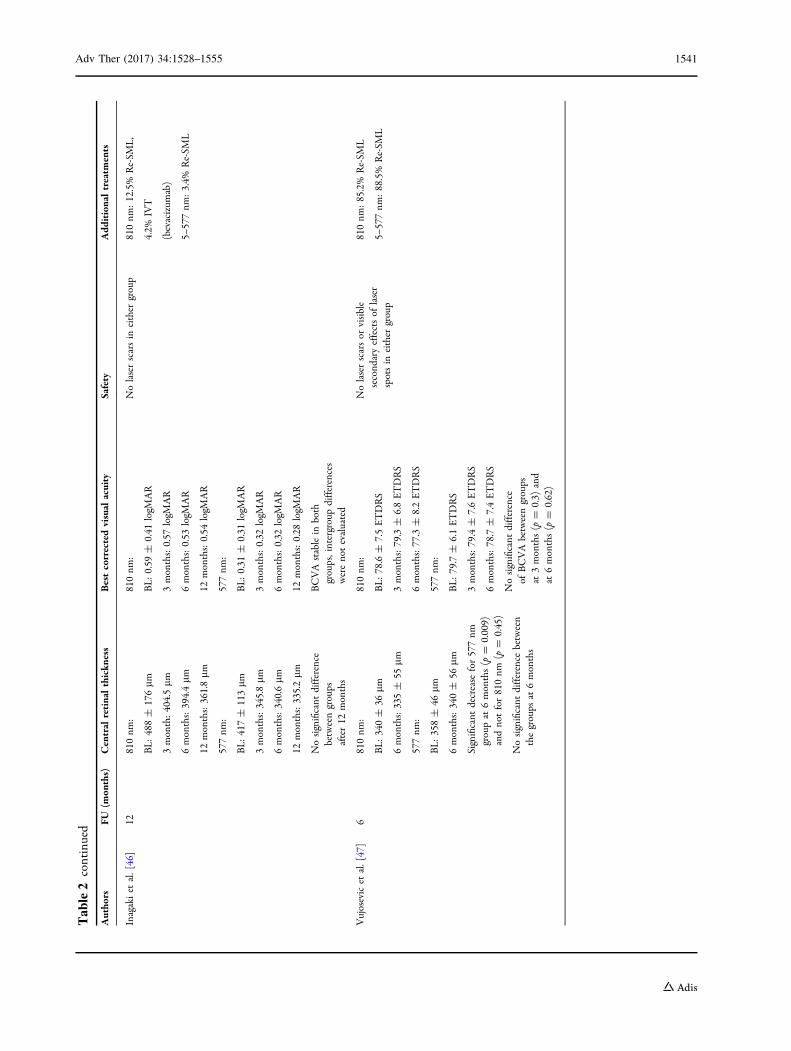
Table2
continued
Autho
rsFU
(mon
ths)
Central
retinalthickn
ess
Bestcorrectedvisual
acuity
Safety
Add
itionaltreatm
ents
Inagakiet
al.[46]
12810nm
:
BL:488±
176lm
3month:404.5lm
6months:394.4lm
12months:361.8lm
577nm
:
BL:417±
113lm
3months:345.8lm
6months:340.6lm
12months:335.2lm
Nosignificant
difference
betweengroups
after12
months
810nm
:
BL:0.59
±0.41
logM
AR
3months:0.57
logM
AR
6months:0.53
logM
AR
12months:0.54
logM
AR
577nm
:
BL:0.31
±0.31
logM
AR
3months:0.32
logM
AR
6months:0.32
logM
AR
12months:0.28
logM
AR
BCVAstablein
both
groups,intergroupdifferences
werenotevaluated
Nolaserscarsin
either
group
810nm
:12.5%
Re-SM
L,
4.2%
IVT
(bevacizum
ab)
5–577nm
:3.4%
Re-SM
L
Vujosevicet
al.[47]
6810nm
:
BL:340±
36lm
6months:335±
55lm
577nm
:
BL:358±
46lm
6months:340±
56lm
Significant
decrease
for577nm
groupat
6months(p
=0.009)
andnotfor810nm
(p=
0.45)
Nosignificant
difference
between
thegroups
at6months
810nm
:
BL:78.6±
7.5ETDRS
3months:79.3±
6.8ETDRS
6months:77.3±
8.2ETDRS
577nm
:
BL:79.7±
6.1ETDRS
3months:79.4±
7.6ETDRS
6months:78.7±
7.4ETDRS
Nosignificant
difference
ofBCVAbetweengroups
at3months(p
=0.3)
and
at6months(p
=0.62)
Nolaserscarsor
visible
second
aryeffectsof
laser
spotsin
either
group
810nm
:85.2%
Re-SM
L
5–577nm
:88.5%
Re-SM
L
Adv Ther (2017) 34:1528–1555 1541
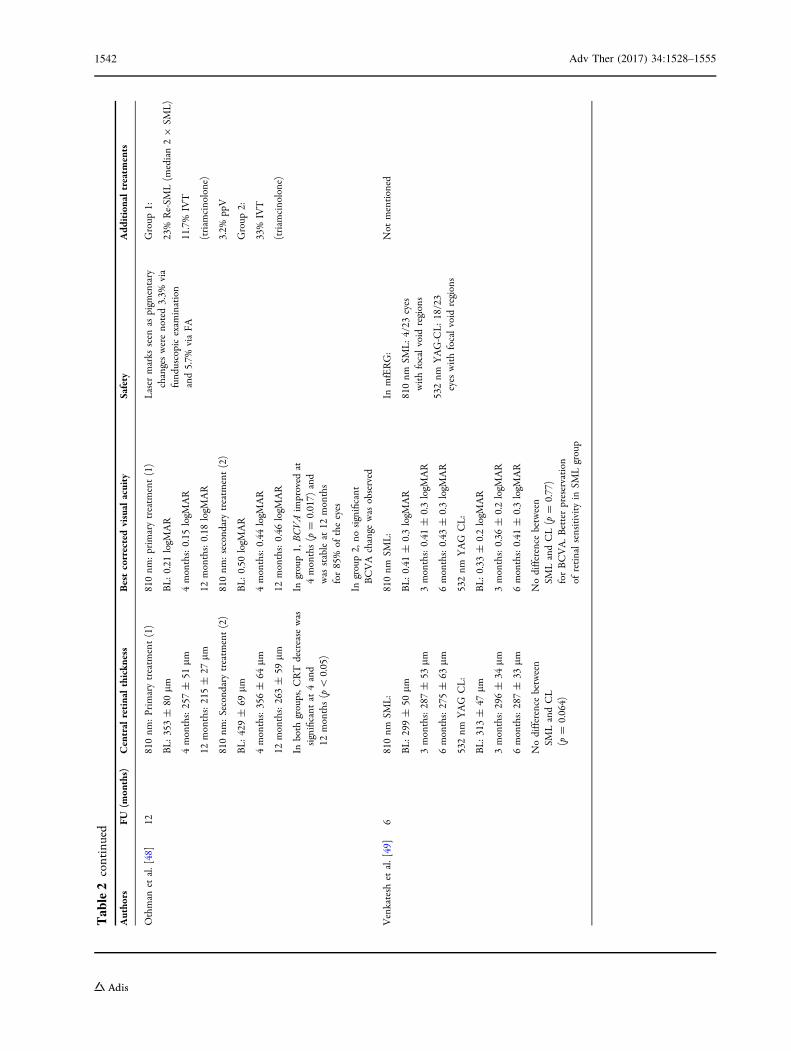
Table2
continued
Autho
rsFU
(mon
ths)
Central
retinalthickn
ess
Bestcorrectedvisual
acuity
Safety
Add
itionaltreatm
ents
Othman
etal.[48]
12810nm
:Prim
arytreatm
ent(1)
BL:353±
80lm
4months:257±
51lm
12months:215±
27lm
810nm
:Second
arytreatm
ent(2)
BL:429±
69lm
4months:356±
64lm
12months:263±
59lm
Inboth
groups,C
RT
decrease
was
significant
at4and
12months(p\
0.05)
810nm
:prim
arytreatm
ent(1)
BL:0.21
logM
AR
4months:0.15
logM
AR
12months:0.18
logM
AR
810nm
:second
arytreatm
ent(2)
BL:0.50
logM
AR
4months:0.44
logM
AR
12months:0.46
logM
AR
Ingroup1,
BCVAim
proved
at4months(p
=0.017)
and
was
stableat
12months
for85%
oftheeyes
Ingroup2,
nosignificant
BCVAchange
was
observed
Laser
marks
seen
aspigm
entary
changeswerenoted3.3%
via
fund
uscopicexam
ination
and5.7%
viaFA
Group
1:
23%
Re-SM
L(m
edian29
SML)
11.7%
IVT
(triam
cinolone)
3.2%
ppV
Group
2:
33%
IVT
(triam
cinolone)
Venkatesh
etal.[49]
6810nm
SML:
BL:299±
50lm
3months:287±
53lm
6months:275±
63lm
532nm
YAG
CL:
BL:313±
47lm
3months:296±
34lm
6months:287±
33lm
Nodifference
between
SMLandCL
(p=
0.064)
810nm
SML:
BL:0.41
±0.3logM
AR
3months:0.41
±0.3logM
AR
6months:0.43
±0.3logM
AR
532nm
YAG
CL:
BL:0.33
±0.2logM
AR
3months:0.36
±0.2logM
AR
6months:0.41
±0.3logM
AR
Nodifference
between
SMLandCL(p
=0.77)
forBCVA.B
etterpreservation
ofretinalsensitivityin
SMLgroup
InmfERG:
810nm
SML:4/23
eyes
withfocalvoid
regions
532nm
YAG-CL:18/23
eyes
withfocalvoid
regions
Not
mentioned
1542 Adv Ther (2017) 34:1528–1555
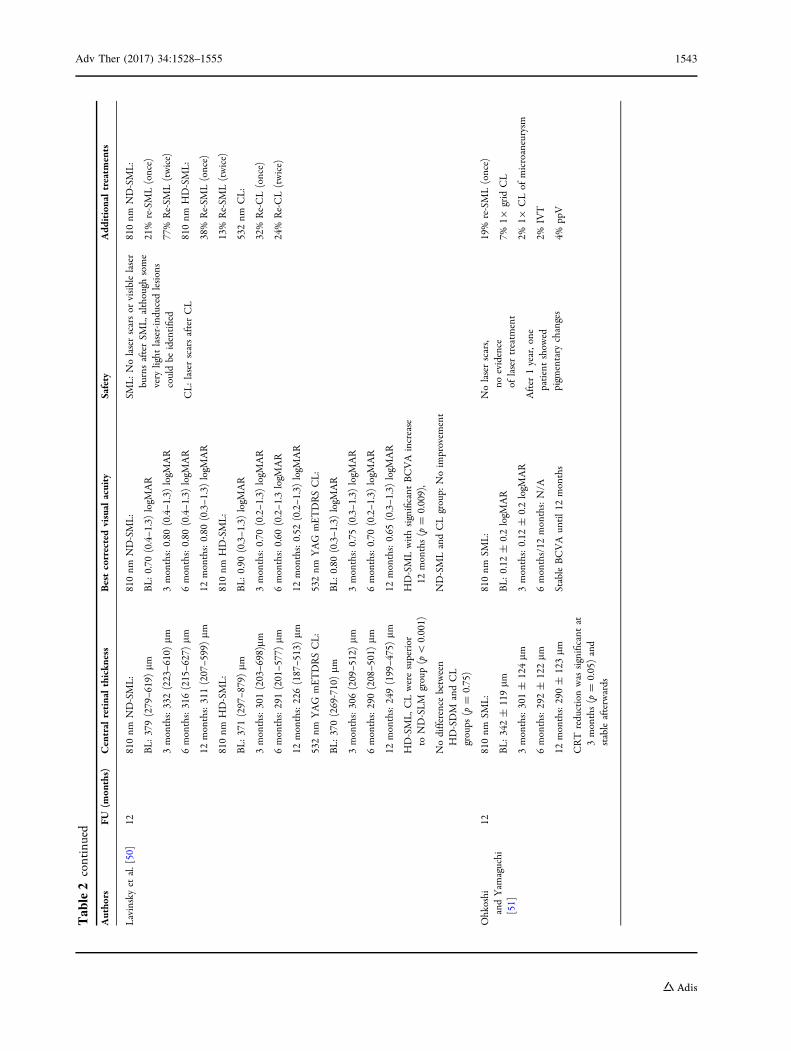
Table2
continued
Autho
rsFU
(mon
ths)
Central
retinalthickn
ess
Bestcorrectedvisual
acuity
Safety
Add
itionaltreatm
ents
Lavinskyet
al.[50]
12810nm
ND-SML:
BL:379(279–6
19)lm
3months:332(223–6
10)lm
6months:316(215–6
27)lm
12months:311(207–5
99)lm
810nm
HD-SML:
BL:371(297–8
79)lm
3months:301(203–6
98)lm
6months:291(201–5
77)lm
12months:226(187–5
13)lm
532nm
YAG
mETDRSCL:
BL:370(269-710)lm
3months:306(209–5
12)lm
6months:290(208–5
01)lm
12months:249(199–4
75)lm
HD-SML,C
Lweresuperior
toND-SLM
group(p\
0.001)
Nodifference
between
HD-SDM
andCL
groups
(p=
0.75)
810nm
ND-SML:
BL:0.70
(0.4–1
.3)logM
AR
3months:0.80
(0.4–1
.3)logM
AR
6months:0.80
(0.4–1
.3)logM
AR
12months:0.80
(0.3–1
.3)logM
AR
810nm
HD-SML:
BL:0.90
(0.3–1
.3)logM
AR
3months:0.70
(0.2–1
.3)logM
AR
6months:0.60
(0.2–1
.3logM
AR
12months:0.52
(0.2–1
.3)logM
AR
532nm
YAG
mETDRSCL:
BL:0.80
(0.3–1
.3)logM
AR
3months:0.75
(0.3–1
.3)logM
AR
6months:0.70
(0.2–1
.3)logM
AR
12months:0.65
(0.3–1
.3)logM
AR
HD-SMLwithsignificant
BCVAincrease
12months(p
=0.009),
ND-SMLandCLgroup:
Noim
provem
ent
SML:Nolaserscarsor
visiblelaser
burnsafterSM
L,alth
ough
some
very
light
laser-inducedlesions
couldbe
identified
CL:laserscarsafterCL
810nm
ND-SML:
21%
re-SML(once)
77%
Re-SM
L(twice)
810nm
HD-SML:
38%
Re-SM
L(once)
13%
Re-SM
L(twice)
532nm
CL:
32%
Re-CL(once)
24%
Re-CL(twice)
Ohkoshi
andYam
aguchi
[51]
12810nm
SML:
BL:342±
119lm
3months:301±
124lm
6months:292±
122lm
12months:290±
123lm
CRTreductionwas
significant
at3months(p
=0.05)and
stableafterwards
810nm
SML:
BL:0.12
±0.2logM
AR
3months:0.12
±0.2logM
AR
6months/12
months:N/A
StableBCVA
until12
months
Nolaserscars,
noevidence
oflasertreatm
ent
After
1year,o
nepatientshow
edpigm
entary
changes
19%
re-SML(once)
7%19
grid
CL
2%19
CLof
microaneurysm
2%IVT
4%ppV
Adv Ther (2017) 34:1528–1555 1543
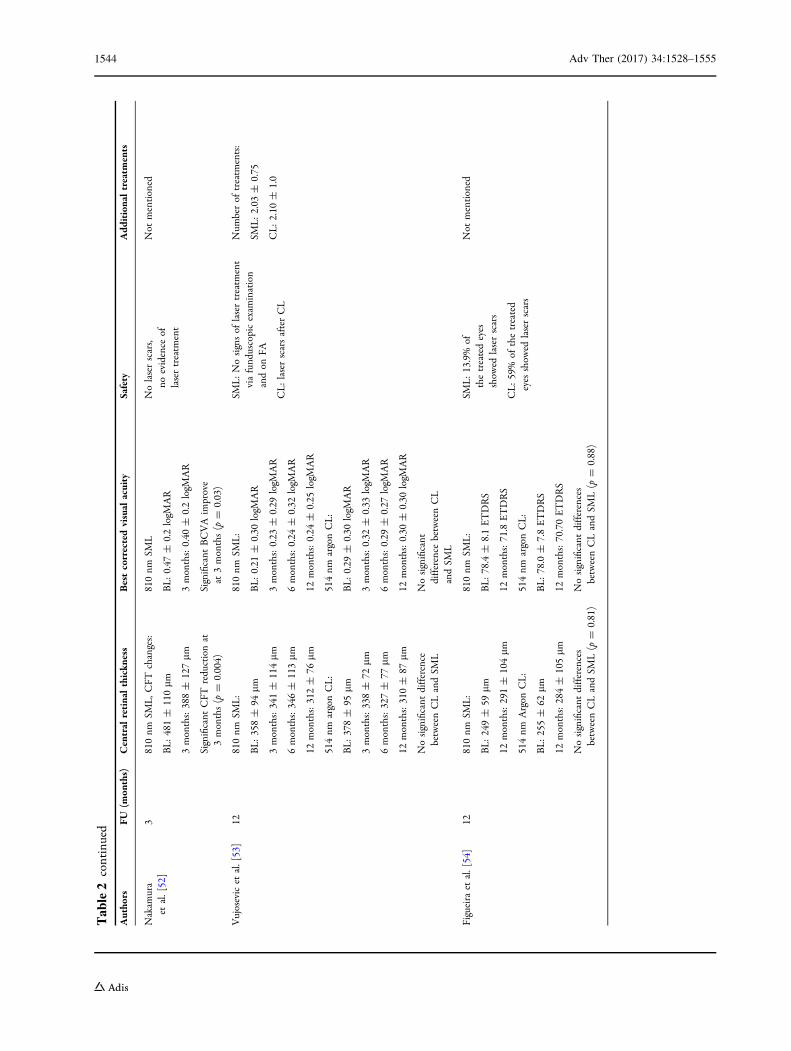
Table2
continued
Autho
rsFU
(mon
ths)
Central
retinalthickn
ess
Bestcorrectedvisual
acuity
Safety
Add
itionaltreatm
ents
Nakam
ura
etal.[52]
3810nm
SML,C
FTchanges:
BL:481±
110lm
3months:388±
127lm
Significant
CFT
reductionat
3months(p
=0.004)
810nm
SML
BL:0.47
±0.2logM
AR
3months:0.40
±0.2logM
AR
Significant
BCVAim
prove
at3months(p
=0.03)
Nolaserscars,
noevidence
oflasertreatm
ent
Not
mentioned
Vujosevicet
al.[53]
12810nm
SML:
BL:358±
94lm
3months:341±
114lm
6months:346±
113lm
12months:312±
76lm
514nm
argonCL:
BL:378±
95lm
3months:338±
72lm
6months:327±
77lm
12months:310±
87lm
Nosignificant
difference
betweenCLandSM
L
810nm
SML:
BL:0.21
±0.30
logM
AR
3months:0.23
±0.29
logM
AR
6months:0.24
±0.32
logM
AR
12months:0.24
±0.25
logM
AR
514nm
argonCL:
BL:0.29
±0.30
logM
AR
3months:0.32
±0.33
logM
AR
6months:0.29
±0.27
logM
AR
12months:0.30
±0.30
logM
AR
Nosignificant
difference
betweenCL
andSM
L
SML:Nosignsof
lasertreatm
ent
viafund
uscopicexam
ination
andon
FA
CL:laserscarsafterCL
Num
berof
treatm
ents:
SML:2.03
±0.75
CL:
2.10
±1.0
Figueira
etal.[54]
12810nm
SML:
BL:249±
59lm
12months:291±
104lm
514nm
Argon
CL:
BL:255±
62lm
12months:284±
105lm
Nosignificant
differences
betweenCLandSM
L(p
=0.81)
810nm
SML:
BL:78.4±
8.1ETDRS
12months:71.8
ETDRS
514nm
argonCL:
BL:78.0±
7.8ETDRS
12months:70.70ETDRS
Nosignificant
differences
betweenCLandSM
L(p
=0.88)
SML:13.9%
ofthetreatedeyes
show
edlaserscars
CL:59%
ofthetreated
eyes
show
edlaserscars
Not
mentioned
1544 Adv Ther (2017) 34:1528–1555
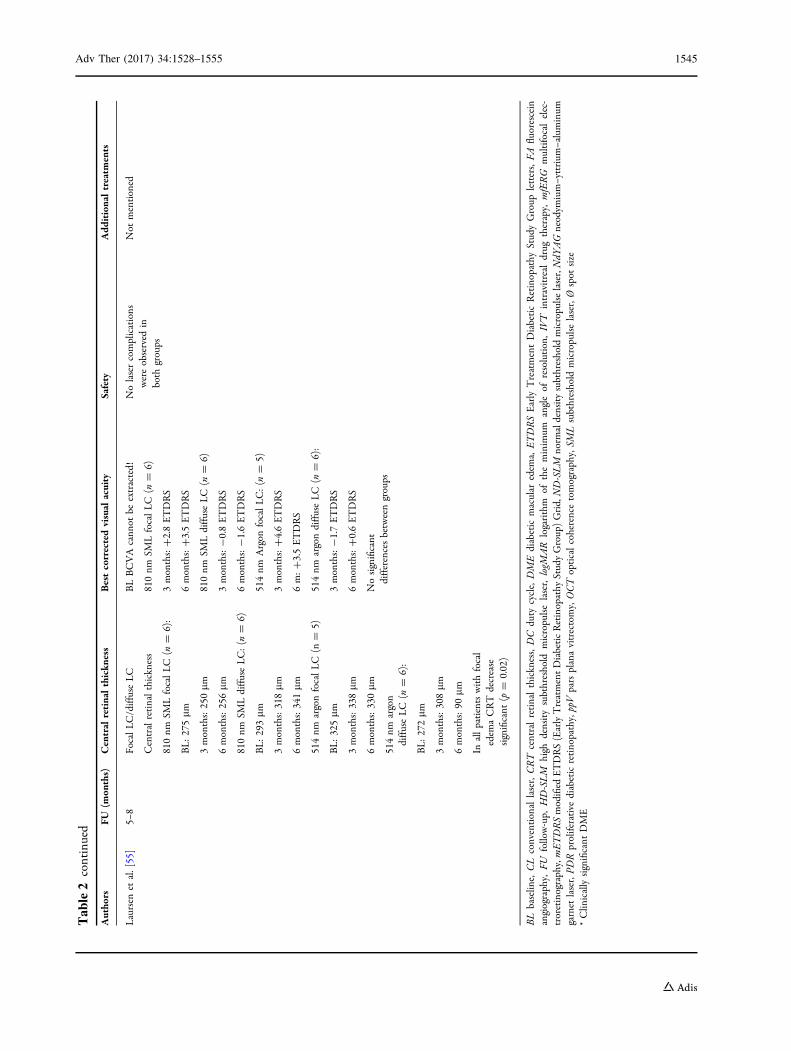
Table2
continued
Autho
rsFU
(mon
ths)
Central
retinalthickn
ess
Bestcorrectedvisual
acuity
Safety
Add
itionaltreatm
ents
Laursenet
al.[55]
5–8
FocalLC/diffuseLC
Centralretinalthickness
810nm
SMLfocalLC
(n=
6):
BL:275lm
3months:250lm
6months:256lm
810nm
SMLdiffuseLC:(n
=6)
BL:293lm
3months:318lm
6months:341lm
514nm
argonfocalLC
(n=
5)
BL:325lm
3months:338lm
6months:330lm
514nm
argon
diffuseLC
(n=
6):
BL:272lm
3months:308lm
6months:90
lm
Inallpatientswithfocal
edem
aCRTdecrease
significant
(p=
0.02)
BLBCVAcann
otbe
extracted!
810nm
SMLfocalLC
(n=
6)
3months:?2.8ETDRS
6months:?3.5ETDRS
810nm
SMLdiffuseLC
(n=
6)
3months:-0.8ETDRS
6months:-1.6ETDRS
514nm
Argon
focalLC:(n
=5)
3months:?4.6ETDRS
6m:?3.5ETDRS
514nm
argondiffuseLC
(n=
6):
3months:-1.7ETDRS
6months:?0.6ETDRS
Nosignificant
differencesbetweengroups
Nolasercomplications
wereobserved
inboth
groups
Not
mentioned
BL
baselin
e,CLconventional
laser,CRT
centralretinalthickness,DC
duty
cycle,DMEdiabetic
macular
edem
a,ETDRSEarly
TreatmentDiabeticRetinopathy
StudyGroup
letters,FA
fluorescein
angiography,
FUfollow-up,
HD-SLM
high
densitysubthreshold
micropulse
laser,
logM
AR
logarithm
oftheminim
umangleof
resolution,IVT
intravitreal
drug
therapy,
mfERG
multifocalelec-
troretinography,mETDRSmodified
ETDRS(EarlyTreatmentDiabeticRetinopathy
StudyGroup)Grid,ND-SLM
norm
aldensitysubthresholdmicropulse
laser,NdY
AGneodym
ium–yttrium
–aluminum
garnet
laser,PD
Rproliferative
diabeticretinopathy,ppVparsplanavitrectomy,OCTopticalcoherencetomography,SM
Lsubthreshold
micropulse
laser,Ø
spot
size
*Clin
icallysignificant
DME
Adv Ther (2017) 34:1528–1555 1545
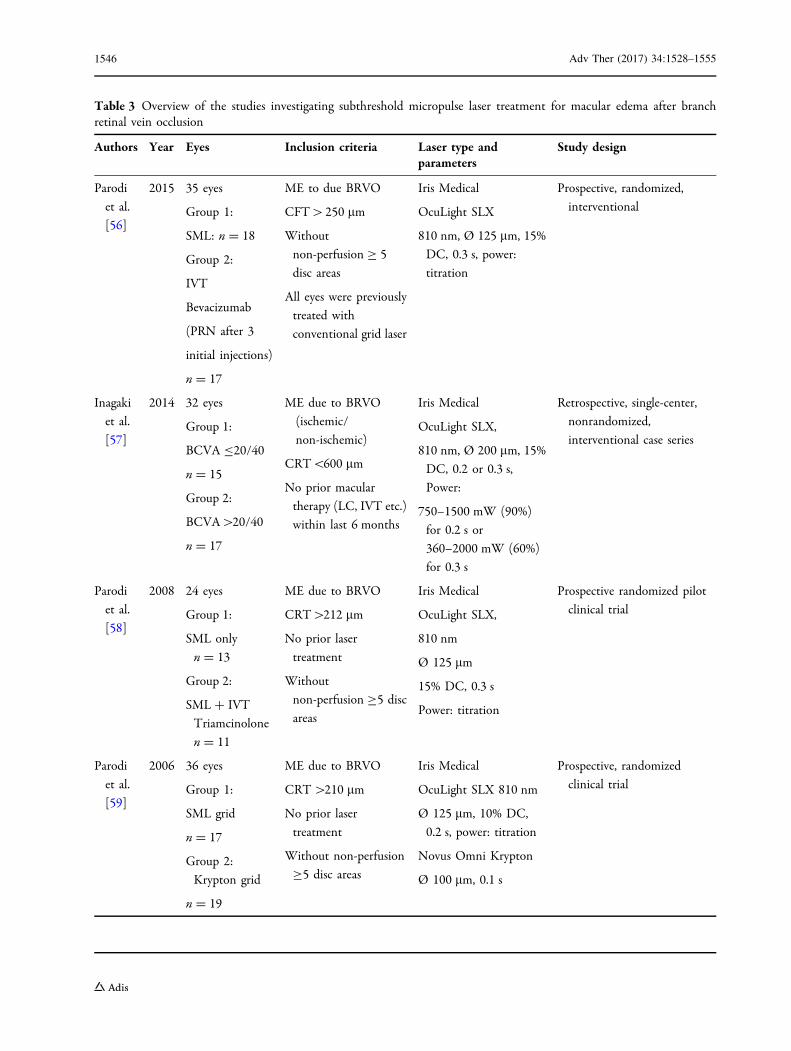
Table 3 Overview of the studies investigating subthreshold micropulse laser treatment for macular edema after branchretinal vein occlusion
Authors Year Eyes Inclusion criteria Laser type andparameters
Study design
Parodi
et al.
[56]
2015 35 eyes
Group 1:
SML: n = 18
Group 2:
IVT
Bevacizumab
(PRN after 3
initial injections)
n = 17
ME to due BRVO
CFT[250 lm
Without
non-perfusion C 5
disc areas
All eyes were previously
treated with
conventional grid laser
Iris Medical
OcuLight SLX
810 nm, Ø 125 lm, 15%
DC, 0.3 s, power:
titration
Prospective, randomized,
interventional
Inagaki
et al.
[57]
2014 32 eyes
Group 1:
BCVA B20/40
n = 15
Group 2:
BCVA[20/40
n = 17
ME due to BRVO
(ischemic/
non-ischemic)
CRT\600 lm
No prior macular
therapy (LC, IVT etc.)
within last 6 months
Iris Medical
OcuLight SLX,
810 nm, Ø 200 lm, 15%
DC, 0.2 or 0.3 s,
Power:
750–1500 mW (90%)
for 0.2 s or
360–2000 mW (60%)
for 0.3 s
Retrospective, single-center,
nonrandomized,
interventional case series
Parodi
et al.
[58]
2008 24 eyes
Group 1:
SML only
n = 13
Group 2:
SML ? IVT
Triamcinolone
n = 11
ME due to BRVO
CRT[212 lm
No prior laser
treatment
Without
non-perfusion C5 disc
areas
Iris Medical
OcuLight SLX,
810 nm
Ø 125 lm
15% DC, 0.3 s
Power: titration
Prospective randomized pilot
clinical trial
Parodi
et al.
[59]
2006 36 eyes
Group 1:
SML grid
n = 17
Group 2:
Krypton grid
n = 19
ME due to BRVO
CRT[210 lm
No prior laser
treatment
Without non-perfusion
C5 disc areas
Iris Medical
OcuLight SLX 810 nm
Ø 125 lm, 10% DC,
0.2 s, power: titration
Novus Omni Krypton
Ø 100 lm, 0.1 s
Prospective, randomized
clinical trial
1546 Adv Ther (2017) 34:1528–1555
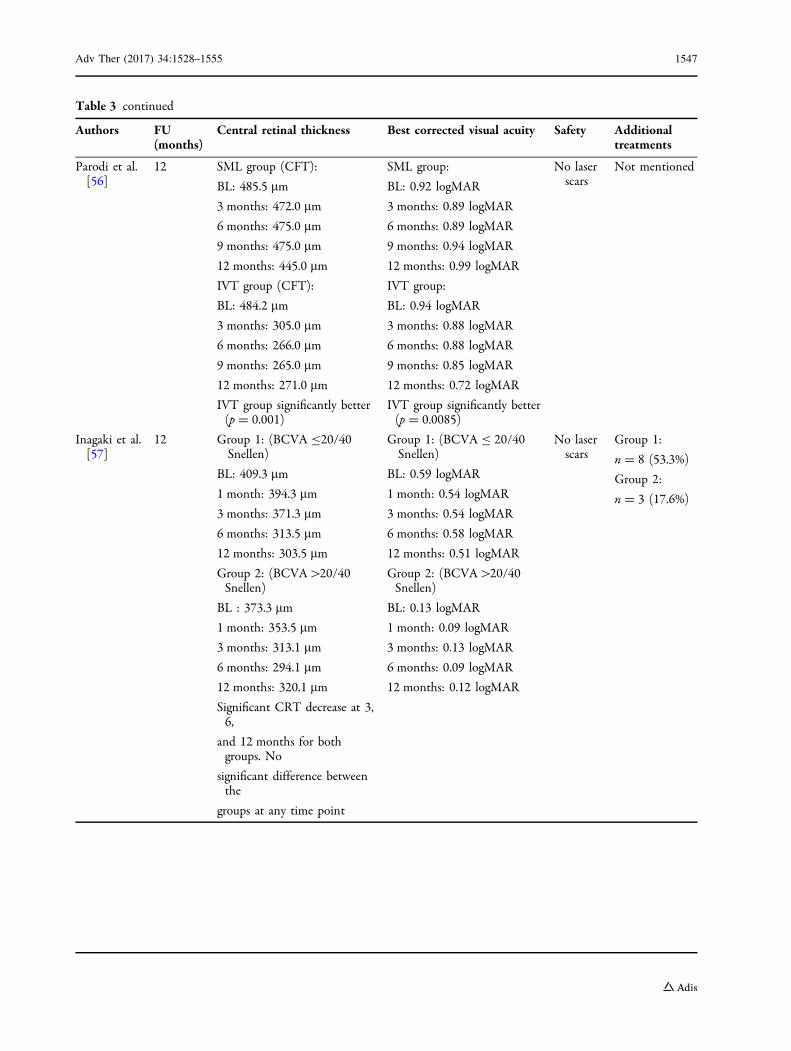
Table 3 continued
Authors FU(months)
Central retinal thickness Best corrected visual acuity Safety Additionaltreatments
Parodi et al.[56]
12 SML group (CFT):
BL: 485.5 lm
3 months: 472.0 lm
6 months: 475.0 lm
9 months: 475.0 lm
12 months: 445.0 lm
IVT group (CFT):
BL: 484.2 lm
3 months: 305.0 lm
6 months: 266.0 lm
9 months: 265.0 lm
12 months: 271.0 lm
IVT group significantly better(p = 0.001)
SML group:
BL: 0.92 logMAR
3 months: 0.89 logMAR
6 months: 0.89 logMAR
9 months: 0.94 logMAR
12 months: 0.99 logMAR
IVT group:
BL: 0.94 logMAR
3 months: 0.88 logMAR
6 months: 0.88 logMAR
9 months: 0.85 logMAR
12 months: 0.72 logMAR
IVT group significantly better(p = 0.0085)
No laserscars
Not mentioned
Inagaki et al.[57]
12 Group 1: (BCVA B20/40Snellen)
BL: 409.3 lm
1 month: 394.3 lm
3 months: 371.3 lm
6 months: 313.5 lm
12 months: 303.5 lm
Group 2: (BCVA[20/40Snellen)
BL : 373.3 lm
1 month: 353.5 lm
3 months: 313.1 lm
6 months: 294.1 lm
12 months: 320.1 lm
Significant CRT decrease at 3,6,
and 12 months for bothgroups. No
significant difference betweenthe
groups at any time point
Group 1: (BCVA B 20/40Snellen)
BL: 0.59 logMAR
1 month: 0.54 logMAR
3 months: 0.54 logMAR
6 months: 0.58 logMAR
12 months: 0.51 logMAR
Group 2: (BCVA[20/40Snellen)
BL: 0.13 logMAR
1 month: 0.09 logMAR
3 months: 0.13 logMAR
6 months: 0.09 logMAR
12 months: 0.12 logMAR
No laserscars
Group 1:
n = 8 (53.3%)
Group 2:
n = 3 (17.6%)
Adv Ther (2017) 34:1528–1555 1547
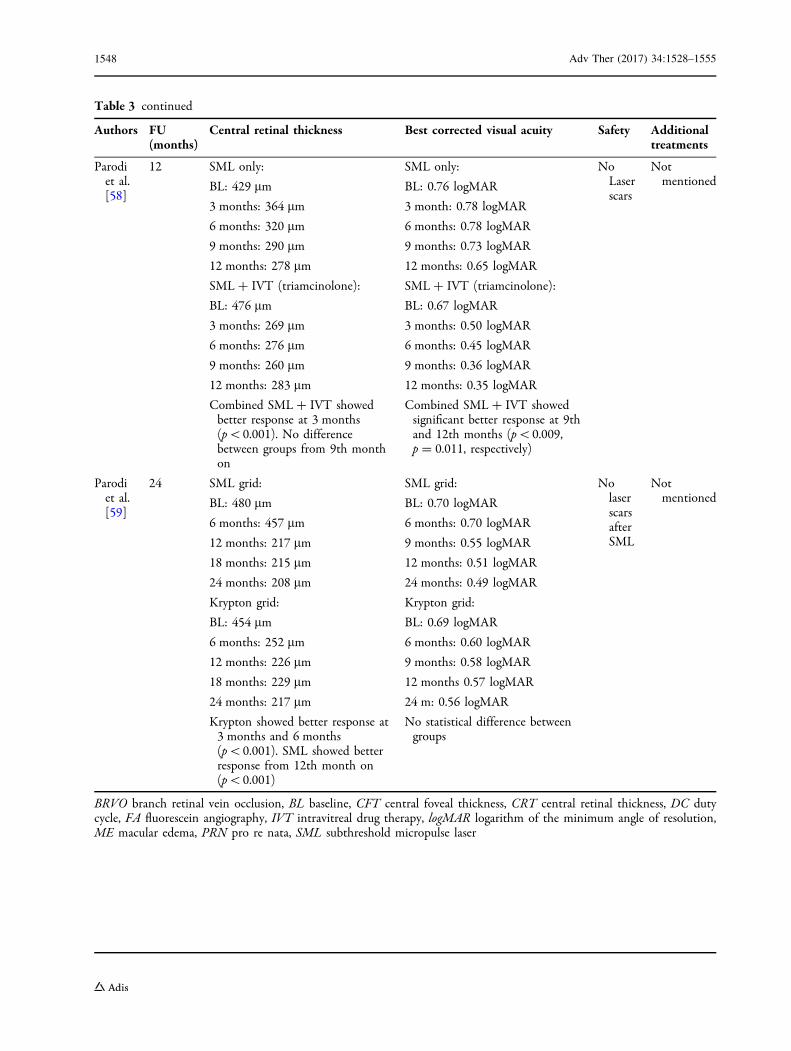
Table 3 continued
Authors FU(months)
Central retinal thickness Best corrected visual acuity Safety Additionaltreatments
Parodiet al.[58]
12 SML only:
BL: 429 lm
3 months: 364 lm
6 months: 320 lm
9 months: 290 lm
12 months: 278 lm
SML ? IVT (triamcinolone):
BL: 476 lm
3 months: 269 lm
6 months: 276 lm
9 months: 260 lm
12 months: 283 lm
Combined SML ? IVT showedbetter response at 3 months(p\0.001). No differencebetween groups from 9th monthon
SML only:
BL: 0.76 logMAR
3 month: 0.78 logMAR
6 months: 0.78 logMAR
9 months: 0.73 logMAR
12 months: 0.65 logMAR
SML ? IVT (triamcinolone):
BL: 0.67 logMAR
3 months: 0.50 logMAR
6 months: 0.45 logMAR
9 months: 0.36 logMAR
12 months: 0.35 logMAR
Combined SML ? IVT showedsignificant better response at 9thand 12th months (p\0.009,p = 0.011, respectively)
NoLaserscars
Notmentioned
Parodiet al.[59]
24 SML grid:
BL: 480 lm
6 months: 457 lm
12 months: 217 lm
18 months: 215 lm
24 months: 208 lm
Krypton grid:
BL: 454 lm
6 months: 252 lm
12 months: 226 lm
18 months: 229 lm
24 months: 217 lm
Krypton showed better response at3 months and 6 months(p\0.001). SML showed betterresponse from 12th month on(p\0.001)
SML grid:
BL: 0.70 logMAR
6 months: 0.70 logMAR
9 months: 0.55 logMAR
12 months: 0.51 logMAR
24 months: 0.49 logMAR
Krypton grid:
BL: 0.69 logMAR
6 months: 0.60 logMAR
9 months: 0.58 logMAR
12 months 0.57 logMAR
24 m: 0.56 logMAR
No statistical difference betweengroups
NolaserscarsafterSML
Notmentioned
BRVO branch retinal vein occlusion, BL baseline, CFT central foveal thickness, CRT central retinal thickness, DC dutycycle, FA fluorescein angiography, IVT intravitreal drug therapy, logMAR logarithm of the minimum angle of resolution,ME macular edema, PRN pro re nata, SML subthreshold micropulse laser
1548 Adv Ther (2017) 34:1528–1555
OCT (SDOCT). A complete resolution of SRF inSDOCT was defined as a complete treatmentresponse. Two studies measured the leakageactivity in FA as a parameter for treatmentresponse [32, 35]. For simplicity reasons we donot distinguish between the different defini-tions for treatment response in our calculations.Few studies did not mention the amount ofpatients with treatment response. If we wereable to work out the treatment response fromthe data shown in the paper, we quote theresponse; otherwise the studies were excludedfrom the calculations [33, 38]. One case reportwas excluded from the calculation because ofprior bevacizumab treatment [39], and twostudies were excluded since they includedpatients with prior PDT [37, 41]. Few studiesmentioned only the response or the completeresponse, and those studies were included in thecalculations.
We included 191 patients from 12 studies forthe calculations of the treatment response and176 patients from 11 studies for the completeresponse. A total of 156 (79.6%) of the 191patients showed a treatment response at the last
mentioned follow-up: 112 (63.6%) of the 176patients had a complete resolution of SRF. Onlytwo studies showed data concerning theimprovement rate in an untreated controlgroup: a complete resolution of SRF was seen in2 (8%) out of 26 eyes at the last follow-up and areduction in SRF in 7 (39%) out of 18 eyes.
Four studies had a control group consistingof patients receiving PDT treatment (half dosePDT in three studies and half fluence PDT inone). The treatment response could be calcu-lated from 100 patients in three studies and thecomplete treatment response from 135 patientsin three studies. A total of 64 (64%) of the 100patients responded to PDT and 62 (46%) of 135patients showed complete response.
Safety
The majority of studies described no visibleretinal changes after the micropulse laser treat-ment. In six patients from two studies [30, 39]pigmentary changes at the level of the RPE wereseen after SML but without any visual implica-tions for the patients. Complications like scar
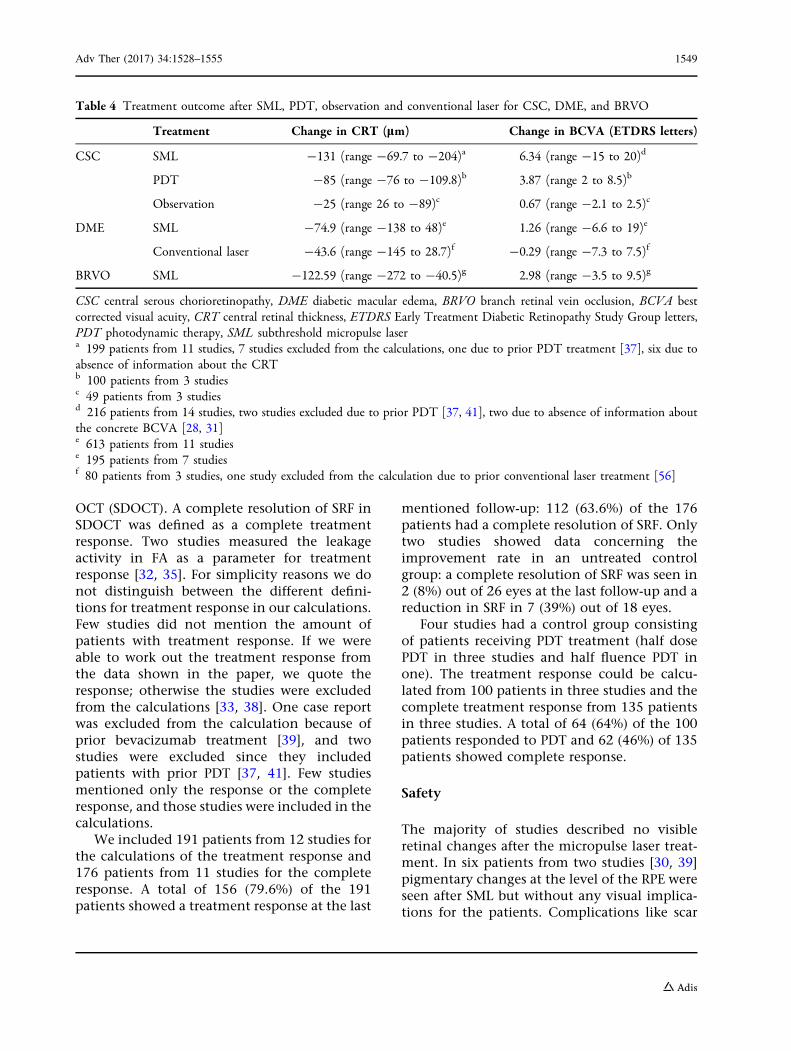
Table 4 Treatment outcome after SML, PDT, observation and conventional laser for CSC, DME, and BRVO
Treatment Change in CRT (lm) Change in BCVA (ETDRS letters)
CSC SML -131 (range -69.7 to -204)a 6.34 (range -15 to 20)d
PDT -85 (range -76 to -109.8)b 3.87 (range 2 to 8.5)b
Observation -25 (range 26 to -89)c 0.67 (range -2.1 to 2.5)c
DME SML -74.9 (range -138 to 48)e 1.26 (range -6.6 to 19)e
Conventional laser -43.6 (range -145 to 28.7)f -0.29 (range -7.3 to 7.5)f
BRVO SML -122.59 (range -272 to -40.5)g 2.98 (range -3.5 to 9.5)g
CSC central serous chorioretinopathy, DME diabetic macular edema, BRVO branch retinal vein occlusion, BCVA bestcorrected visual acuity, CRT central retinal thickness, ETDRS Early Treatment Diabetic Retinopathy Study Group letters,PDT photodynamic therapy, SML subthreshold micropulse lasera 199 patients from 11 studies, 7 studies excluded from the calculations, one due to prior PDT treatment [37], six due toabsence of information about the CRTb 100 patients from 3 studiesc 49 patients from 3 studiesd 216 patients from 14 studies, two studies excluded due to prior PDT [37, 41], two due to absence of information aboutthe concrete BCVA [28, 31]e 613 patients from 11 studiese 195 patients from 7 studiesf 80 patients from 3 studies, one study excluded from the calculation due to prior conventional laser treatment [56]
Adv Ther (2017) 34:1528–1555 1549

formation, visible laser burns, or CNV did notoccur.
DIABETIC MACULAR EDEMA (DME)
DME is a frequent complication of diabeticretinopathy (DR) and the most common causeof visual impairment in patients with DR [5].Since the ETDRS trial [1, 73] showed that laserphotocoagulation reduced the risk of moderatevisual loss by 50% in eyes with clinically sig-nificant macular edema, laser photocoagulationbecame the standard therapy for DME for manyyears. Depending on the kind of edema, thetreatment pattern can be selected: a focal pho-tocoagulation for localized areas of leakage anda grid pattern for a diffuse macular edema.Continuous-wave photocoagulation comeswith potential side effects like epiretinal fibro-sis, CNV, and enlargement of laser scars[7, 8, 74]. Table 3 shows only the prospectivestudies investigating micropulse laser treatmentfor diabetic macular edema. A total of 613patients from 11 studies were included in thecalculations. The inclusion and exclusion crite-ria varied between studies; some did not allowprior treatment at all, most of them onlyexcluded patients with treatment in the prior3–6 months. All listed studies were included inthe calculations for change in CRT and BCVA.Seven studies had a control group consisting of195 patients treated with conventional laser.The same calculations were performed for thosestudies.
Table 4 displays the treatment outcome afterSML and conventional laser for DME.
Safety
In the majority of studies no laser scars occurredafter SML. Four studies reported scar formationor pigmentary changes in a small amount ofeyes after SML treatment [48, 50, 51, 54]. Reti-nal changes were only observed in eyes treatedwith duty cycles of 15%; lower duty cycles didnot lead to scar formation in the listed studies.
Venkatesh [49] et al. reported focal voidregions in multifocal electroretinogram in 4 outof 23 eyes after SML treatment with 10% duty
cycle compared to 18 out of 23 eyes after con-ventional laser.
MACULAR EDEMA DUE TO RETINALVEIN OCCLUSION (RVO)
Macular edema is a common complication ofbranch RVO (BRVO) [75]. Grid laser photoco-agulation reduces the visual acuity loss afterBRVO with macular edema [75]. Parodi et al.[59] reported a similar outcome in visual acuityimprovement and resolution of macular edemaafter SML treatment compared to conventionallaser, but without retinal changes after SML.Table 3 summarizes studies investigating SMLtreatment for macular edema after BRVO. Intotal 80 patients from three studies could beincluded in the calculations, and one study wasexcluded because of prior conventional lasertreatment [56]. As a result of the small numberof studies and the variety in control groups(bevacizumab, SML ? triamcinolone, conven-tional laser), the control groups were not sepa-rately analyzed. Only one study [48] had acontrol group where patients were treated withanti-VEGF agents, the current standard therapyfor macular edema due to BRVO.
Table 4 presents the treatment outcome afterSML for macular edema after BRVO.
Safety
No study described complications like scar for-mation, visible laser burns, or CNV.
PROBLEMS AND CHALLENGESOF SML TREATMENT
Although the majority of the studies showedsome efficacy of the SML treatment for CSC,DME, or BRVO, the treatment parameter dif-fered significantly between the individualstudies. No study compared the outcome ofSML with different treatment parameters likehigher or lower duty cycle. Concerning thetreatment power, most authors titrated thepower individually for each patient, but the
1550 Adv Ther (2017) 34:1528–1555
path was not consistent. The titration is proba-bly the most challenging part of the SMLtreatment. Since the laser surgeon did not seean effect of the treatment, there is a high risk ofundertreatment and treatment failure accord-ingly. A solution to this problem could be to usefixed laser parameters with the same power forall patients. But so far there is not enoughpublished data to choose the best treatmentpower and to evaluate the safety and the treat-ment success of subthreshold micropulse treat-ment with fixed parameters. For the future,controlled trials comparing treatment outcomeand safety of individual titrated SML treatmentand SML treatment with fixed parameterswould be desirable. Those studies shouldinclude safety follow-up with multimodalimaging including autofluorescence, OCT, andfundus photographies as well functional fol-low-up with microperimetry or multifocalelectroretinogram.
CONCLUSION
For CSC, the presented studies showed a higherefficacy of the micropulse laser treatment forboth morphology and visual function in com-parison to no treatment or PDT. The decrease inCRT was highest after SML (-131 lm), followedby PDT (-85 lm) and the no-treatment group(-25 lm). Moreover, 64% of patients showedno SRF after SML compared to 46% after PDTand 8% after observation.
No study reported any complications afterup to five SML treatment sessions, so even anearly treatment could be considered for poten-tially better results. Chen et al. [29] showed thatthe SML treatment outcome was best in patientswith source leakage without RPE atrophy. Theinvestigated literature did not allow an evalua-tion of the best treatment parameter or the bestlaser wavelength.
Regarding the treatment of DME, the inves-tigated studies showed efficacy also in mor-phology and function. The decrease in CRT andincrease in BCVA after SML (-74.9 lm and?1.26 ETDRS letters) was better than after con-ventional laser (-43.6 lm and -0.29 ETDRSletters), but no study had a control group in
which patients were treated with anti-VEGFagents. After the RISE and RIDE studies [76] andthe approval of ranibizumab for the treatmentof DME, anti-VEGF agents became the standardtreatment for DME. Without any trial, com-paring SML treatment with anti-VEGF agents,we do not know when SML treatment could bean alternative first-line treatment for DME.Nevertheless, SML might be an option inpatients not responding sufficiently to, or whoare not able to follow an anti-VEGF therapy(e.g., high costs, compliance problems due tofrequent visits for the injections and ophthal-mological controls). Chen et al. [77] had cometo a similar result in their meta-analysis of ran-domized controlled trials comparing sub-threshold micropulse diode laserphotocoagulation and conventional laser. Theyreported a significantly better visual acuity anda similar decrease in CRT after SML compared toconventional laser. They underline the advan-tage of the SML treatment in terms of theaffordability compared to the cost-intensiveanti-VEGF therapy.
On the subject of macular edema after BRVO,SML treatment shows some efficacy as well. Butin comparison to the current standard treatment,intravitreal anti-VEGF, SML was inferior tointravitreal bevacizumab [56]. However, similarto DME, SML treatment could be an option foradjunct treatment for selected patients.
In summary, in all three indications micro-pulse laser is an efficacious and safe treatmentoption. Owing to its higher efficacy and theexcellent safety profile compared to PDT, itcould become the first-line therapy in CSC,potentially even in acute cases.
ACKNOWLEDGEMENTS
No funding or sponsorship was received for thisstudy or publication of this article. All namedauthors meet the International Committee ofMedical Journal Editors (ICMJE) criteria forauthorship for this manuscript, take responsi-bility for the integrity of the work as a whole,and have given final approval for the version tobe published.
Adv Ther (2017) 34:1528–1555 1551
Disclosures. Paula Scholz received a speakerhonorarium from Quantel Medical. Sascha Fau-ser received a speaker honorarium from QuantelMedical. Lebriz Altay has nothing to disclose.
Compliance With Ethics Guidelines. Thisarticle is based on previously conducted studiesand does not involve any new studies of humanor animal subjects performed by any of theauthors.
Data Availability. The datasets generatedand analyzed during the current study areavailable from the corresponding author onreasonable request.
Open Access. This article is distributedunder the terms of the Creative CommonsAttribution-NonCommercial 4.0 InternationalLicense (http://creativecommons.org/licenses/by-nc/4.0/), which permits any noncommer-cial use, distribution, and reproduction in anymedium, provided you give appropriate creditto the original author(s) and the source, providea link to the Creative Commons license, andindicate if changes were made.
REFERENCES
1. Early Treatment Diabetic Retinopathy StudyResearch Group. Photocoagulation for diabeticmacular edema. Early treatment diabetic retinopa-thy study report number 1. Arch Ophthalmol.1985;103:1796–806.
2. Robertson DM, Ilstrup D. Direct, indirect, and shamlaser photocoagulation in the management of cen-tral serous chorioretinopathy. Am J Ophthalmol.1983;95(4):457–66.
3. Ficker L, Vafidis G, While A, Leaver P. Long-termfollow-up of a prospective trial of argon laser pho-tocoagulation in the treatment of central serousretinopathy. Br J Ophthalmol. 1988;72(11):829–34.
4. The Branch Vein Occlusion Study Group. Argonlaser photocoagulation for macular edema inbranch vein occlusion. Am J Ophthalmol.1984;98(3):271–82.
5. The Diabetic Retinopathy Study Research Group.Preliminary report on effects of photocoagulationtherapy. Am J Ophthalmol. 1976;81(4):383–96.
6. Ulbig MR, Arden GB, Hamilton AP. Color contrastsensitivity and pattern electroretinographic find-ings after diode and argon laser photocoagulationin diabetic retinopathy. Am J Ophthalmol.1994;117(5):583–8.
7. Lewen RM. Subretinal neovascularization compli-cating laser photocoagulation of diabetic macu-lopathy. Ophthal Surg Lasers Imaging Retina.1988;19(10):734–7.
8. Smith CW, Guyer DR, D’Amico DJ. Subretinalfibrosis after laser photocoagulation for diabeticmacular edema. Am J Ophthalmol.1992;113(6):652–6.
9. Seiberth V, Alexandridis E, Feng W. Function of thediabetic retina after panretinal argon laser coagu-lation. Graefes Arch Clin Exp Ophthalmol.1987;225(6):385–90.
10. Pearson A, Tanner V, Keightley S, Casswell A. Whateffect does laser photocoagulation have on drivingvisual fields in diabetics? Eye (Lond).1998;12(1):64–8.
11. Roider J. Laser treatment of retinal diseases bysubthreshold laser effects. Semin Ophthalmol.2009;14(19–26).
12. Bresnick GH. Diabetic maculopathy: a criticalreview highlighting diffuse macular edema. Oph-thalmology. 1983;90(11):1301–17.
13. Wilson AS, Hobbs BG, Shen W-Y, et al. Argon laserphotocoagulation-induced modification of geneexpression in the retina. Invest Ophthalmol Vis Sci.2003;44(4):1426–34.
14. Dorin G. Evolution of retinal laser therapy: mini-mum intensity photocoagulation (MIP). Can thelaser heal the retina without harming it? SeminOphthalmol. 2004;19(1–2):62–8.
15. Inagaki K, Shuo T, Katakura K, Ebihara N, Mur-akami A, Ohkoshi K. Sublethal photothermalstimulation with a micropulse laser induces heatshock protein expression in ARPE-19 cells. J Oph-thalmol. 2015;2015:729792.
16. Lanzetta P, Dorin G, Pirracchio A, Bandello F.Theoretical bases of non-ophthalmoscopically visi-ble endpoint photocoagulation. Semin Ophthal-mol. 2001;16(1):8–11.
17. Anderson RR, Parrish JA. Selective photothermoly-sis: precise microsurgery by selective absorption ofpulsed radiation. Science. 1983;220(4596):524–7.
18. Roider J, Hillenkamp F, Flotte T, Birngruber R.Microphotocoagulation: selective effects of
1552 Adv Ther (2017) 34:1528–1555
repetitive short laser pulses. Proc Natl Acad Sci.1993;90(18):8643–7.
19. Roider J, Michaud NA, Flotte TJ, Birngruber R.Response of the retinal pigment epithelium toselective photocoagulation. Arch Ophthalmol.1992;110(12):1786–92.
20. Dorin G, editor. Subthreshold and micropulsediode laser photocoagulation. Seminars in Oph-thalmology. 2003;18(3):147–53.
21. McHugh J, Marshall J, Ffytche T, Hamilton A, RavenA. Macular photocagulation of human retina with adiode laser: a comparative histopathological study.Lasers Light Ophthalmol. 1990;3(1):11–28.
22. Vogel A, Birngruber R. Temperature profiles inhuman retina and choroid during laser coagulationwith different wavelengths ranging from 514 to810 nm. Lasers Light Ophthalmol. 1992;5(1):9–16.
23. Peyman GA, Raichand M, Zeimer RC. Ocular effectsof various laser wavelengths. Surv Ophthalmol.1984;28(5):391–404.
24. Friberg TR, Karatza EC. The treatment of maculardisease using a micropulsed and continuous wave810-nm diode laser. Ophthalmology.1997;104(12):2030–8.
25. Friberg TR, Venkatesh MdS. Alteration of pulseconfiguration affects the pain response duringdiode laser photocoagulation. Lasers Surg Med.1995;16(4):380–3.
26. Mainster MA. Wavelength selection in macularphotocoagulation: tissue optics, thermal effects,and laser systems. Ophthalmology.1986;93(7):952–8.
27. Ricci F, Missiroli F, Cerulli L. Indocyanine greendye-enhanced micropulsed diode laser: a novelapproach to subthreshold RPE treatment in a caseof central serous chorioretinopathy. Eur J Oph-thalmol. 2004;14(1):74–82.
28. Ricci F, Missiroli F, Regine F, Grossi M, Dorin G.Indocyanine green enhanced subthreshold diode-laser micropulse photocoagulation treatment ofchronic central serous chorioretinopathy. GraefesArch Clin Exp Ophthalmol. 2009;247(5):597–607.
29. Chen S-N, Hwang J-F, Tseng L-F, Lin C-J.Subthreshold diode micropulse photocoagulationfor the treatment of chronic central serous chori-oretinopathy with juxtafoveal leakage. Ophthal-mology. 2008;115(12):2229–34.
30. Lanzetta P, Furlan F, Morgante L, Veritti D, Ban-dello F. Nonvisible subthreshold micropulse diodelaser (810 nm) treatment of central serous
chorioretinopathy. A pilot study. Eur J Ophthalmol.2007;18(6):934–40.
31. Gupta B, Elagouz M, McHugh D, Chong V, Siva-prasad S. Micropulse diode laser photocoagulationfor central serous chorio-retinopathy. Clin ExpOphthalmol. 2009;37(8):801–5.
32. Koss M, Beger I, Koch F. Subthreshold diode lasermicropulse photocoagulation versus intravitreal injec-tions of bevacizumab in the treatment of central serouschorioretinopathy. Eye (Lond). 2011;26(2):307–14.
33. Roisman L, Magalhaes FP, Lavinsky D, et al.Micropulse diode laser treatment for chronic cen-tral serous chorioretinopathy: a randomized pilottrial. Ophthalmic Surg Lasers Imaging Retina.2013;44(5):465–70.
34. Malik KJ, Sampat KM, Mansouri A, Steiner JN,Glaser BM. Low-intensity/high-density subthresh-old micropulse diode laser for chronic central ser-ous chorioretinopathy. Retina. 2015;35(3):532–6.
35. Kretz FT, Beger I, Koch F, Nowomiejska K, AuffarthGU, Koss MJ. Randomized clinical trial to comparemicropulse photocoagulation versus half-dose ver-teporfin photodynamic therapy in the treatment ofcentral serous chorioretinopathy. Ophthalmic SurgLasers Imaging Retina. 2015;46(8):837–43.
36. Elhamid AHA. Subthreshold micropulse yellowlaser treatment for nonresolving central serouschorioretinopathy. Clin Ophthalmol. 2015;9:2277.
37. Scholz P, Ersoy L, Boon CJ, Fauser S. Subthresholdmicropulse laser (577 nm) treatment in chroniccentral serous chorioretinopathy. Ophthalmolog-ica. 2015;234(4):189–94.
38. Kim JY, Park HS, Kim SY. Short-term efficacy ofsubthreshold micropulse yellow laser (577-nm)photocoagulation for chronic central serous chori-oretinopathy. Graefes Arch Clin Exp Ophthalmol.2015;253(12):2129–35.
39. Gawecki M. Increase in central retinal edema aftersubthreshold diode micropulse laser treatment ofchronic central serous chorioretinopathy. Case RepOphthalmol Med. 2015;2015:813414.
40. Yadav N, Jayadev C, Mohan A, et al. Subthresholdmicropulse yellow laser (577 nm) in chronic centralserous chorioretinopathy: safety profile and treat-ment outcome. Eye (Lond). 2015;29(2):258–64.
41. Breukink MB, Mohr JK, Ossewaarde-van Norel A,et al. Half-dose photodynamic therapy followed bydiode micropulse laser therapy as treatment forchronic central serous chorioretinopathy: evalua-tion of a prospective treatment protocol. ActaOphthalmol. 2016;94(2):187–97.
Adv Ther (2017) 34:1528–1555 1553
42. Ozmert E, Demirel S, Yanık O, Batıoglu F. Low-flu-ence photodynamic therapy versus subthresholdmicropulse yellow wavelength laser in the treat-ment of chronic central serous chorioretinopathy.J Ophthalmol. 2016;2016:3513794.
43. Ambiya V, Goud A, Mathai A, Rani PK, Chhablani J.Microsecond yellow laser for subfoveal leaks incentral serous chorioretinopathy. Clin Ophthalmol(Auckland, NZ). 2016;10:1513.
44. Scholz P, Altay L, Fauser S. Comparison of sub-threshold micropulse laser (577 nm) treatment andhalf-dose photodynamic therapy in patients withchronic central serous chorioretinopathy. Eye(Lond). 2016;30(10):1371–7.
45. Fazel F, Bagheri M, Golabchi K, Ardakani HJ.Comparison of subthreshold diode laser micropulsetherapy versus conventional photocoagulationlaser therapy as primary treatment of diabeticmacular edema. J Curr Ophthalmol.2016;28(4):206–11.
46. Inagaki K, Ohkoshi K, Ohde S, Deshpande GA,Ebihara N, Murakami A. Comparative efficacy ofpure yellow (577-nm) and 810-nm subthresholdmicropulse laser photocoagulation combined withyellow (561–577-nm) direct photocoagulation fordiabetic macular edema. Jpn J Ophthalmol.2015;59(1):21–8.
47. Vujosevic S, Martini F, Longhin E, Convento E,Cavarzeran F, Midena E. Subthreshold micropulseyellow laser versus subthreshold micropulse infra-red laser in center-involving diabetic macularedema: morphologic and functional safety. Retina.2015;35(8):1594–603.
48. Othman IS, Eissa SA, Kotb MS, Sadek SH.Subthreshold diode-laser micropulse photocoagu-lation as a primary and secondary line of treatmentin management of diabetic macular edema. ClinOphthalmol. 2014;8:653.
49. Venkatesh P, Ramanjulu R, Azad R, Vohra R, Garg S.Subthreshold micropulse diode laser and doublefrequency neodymium:YAG laser in treatment ofdiabetic macular edema: a prospective, randomizedstudy using multifocal electroretinography. Pho-tomed Laser Surg. 2011;29(11):727–33.
50. Lavinsky D, Cardillo JA, Melo LA, Dare A, Farah ME,Belfort R. Randomized clinical trial evaluatingmETDRS versus normal or high-density micropulsephotocoagulation for diabetic macular edema.Invest Ophthalmol Vis Sci. 2011;52(7):4314–23.
51. Ohkoshi K, Yamaguchi T. Subthreshold micropulsediode laser photocoagulation for diabetic macularedema in Japanese patients. Am J Ophthalmol.2010;149(1):133–9.
52. Nakamura Y, Mitamura Y, Ogata K, Arai M, Takat-suna Y, Yamamoto S. Functional and morphologi-cal changes of macula after subthresholdmicropulse diode laser photocoagulation for dia-betic macular oedema. Eye (Lond).2010;24(5):784–8.
53. Vujosevic S, Bottega E, Casciano M, Pilotto E,Convento E, Midena E. Microperimetry and fun-dus autofluorescence in diabetic macular edema:subthreshold micropulse diode laser versus mod-ified early treatment diabetic retinopathy studylaser photocoagulation. Retina. 2010;30(6):908–16.
54. Figueira J, Khan J, Nunes S, et al. Prospective ran-domised controlled trial comparing sub-thresholdmicropulse diode laser photocoagulation and con-ventional green laser for clinically significant dia-betic macular oedema. Br J Ophthalmol.2009;93(10):1341–4.
55. Laursen M, Moeller F, Sander B, Sjoelie A.Subthreshold micropulse diode laser treatment indiabetic macular oedema. Br J Ophthalmol.2004;88(9):1173–9.
56. Parodi MB, Iacono P, Bandello F. Subthreshold gridlaser versus intravitreal bevacizumab as second-linetherapy for macular edema in branch retinal veinocclusion recurring after conventional grid lasertreatment. Graefes Arch Clin Exp Ophthalmol.2015;253(10):1647–51.
57. Inagaki K, Ohkoshi K, Ohde S, Deshpande GA,Ebihara N, Murakami A. Subthreshold micropulsephotocoagulation for persistent macular edemasecondary to branch retinal vein occlusion includ-ing best-corrected visual acuity greater than 20/40.J Ophthalmol. 2014;2014:251257.
58. Parodi MB, Iacono P, Ravalico G. Intravitreal tri-amcinolone acetonide combined with subthresholdgrid laser treatment for macular oedema in branchretinal vein occlusion: a pilot study. Br J Ophthal-mol. 2008;92(8):1046–50.
59. Parodi MB, Spasse S, Iacono P, Di Stefano G, Can-ziani T, Ravalico G. Subthreshold grid laser treat-ment of macular edema secondary to branch retinalvein occlusion with micropulse infrared (810nanometer) diode laser. Ophthalmology.2006;113(12):2237–42.
60. Gregori NZ, Feuer W, Rosenfeld PJ. Novel methodfor analyzing snellen visual acuity measurements.Retina. 2010;30(7):1046–50.
61. Gass J. Pathogenesis of disciform detachment of theneuroepithelium. II. Idiopathic central serouschoroidopathy. Am J Ophthalmol.1967;63:587–615.
1554 Adv Ther (2017) 34:1528–1555
62. Gilbert CM, Owens SL, Smith PD, Fine SL.Long-term follow-up of central serous chori-oretinopathy. Br J Ophthalmol. 1984;68(11):815–20.
63. Fok AC, Chan PP, Lam DS, Lai TY. Risk factors forrecurrence of serous macular detachment inuntreated patients with central serous chori-oretinopathy. Ophthalmic Res. 2011;46(3):160–3.
64. Wang MS, Sander B, Larsen M. Retinal atrophy inidiopathic central serous chorioretinopathy. Am JOphthalmol. 2002;133(6):787–93.
65. Schatz H, Yannuzzi LA, Gitter KA. Subretinal neo-vascularization following argon laser photocoagu-lation treatment for central serouschorioretinopathy: complication or misdiagnosis?Retina. 2012;32:OP-893–906.
66. Schatz H, Madeira D, McDonald HR, Johnson RN.Progressive enlargement of laser scars following gridlaser photocoagulation for diffuse diabetic macularedema. Arch Ophthalmol. 1991;109(11):1549–51.
67. Khosla P, Rana S, Tewari H, Azad R, Talwar D.Evaluation of visual function following argon laserphotocoagulation in central serous retinopathy.Ophthalmic Surg Lasers. 1997;28(8):693–7.
68. Piccolino FC, Eandi CM, Ventre L, de la LongraisRCR, Grignolo FM. Photodynamic therapy forchronic central serous chorioretinopathy. Retina.2003;23(6):752–63.
69. Chan W, Lam D, Lai T, Tam B, Liu D, Chan C.Choroidal vascular remodelling in central serouschorioretinopathy after indocyanine green guidedphotodynamic therapy with verteporfin: a noveltreatment at the primary disease level. Br J Oph-thalmol. 2003;87(12):1453–8.
70. Colucciello M. Choroidal neovascularization com-plicating photodynamic therapy for central serousretinopathy. Retina. 2006;26(2):239–42.
71. Lai TY, Chan W-M, Lam DS. Transient reduction inretinal function revealed by multifocal elec-troretinogram after photodynamic therapy. Am JOphthalmol. 2004;137(5):826–33.
72. Bandello F, Lanzetta P, Furlan F, Polito A. Non vis-ible subthreshold micropulse diode laser treatmentof idiopathic central serous chorioretinopathy. Apilot study. Investig Ophtalmol Vis Sci.2003;44(5):4858.
73. Early Treatment Diabetic Retinopathy StudyResearch Group. Early photocoagulation for dia-betic retinopathy: ETDRS report number 9. Oph-thalmology. 1991;98(5):766–85.
74. Morgan CM, Schatz H. Atrophic creep of the retinalpigment epithelium after focal macular photoco-agulation. Ophthalmology. 1989;96(1):96–103.
75. Greer D, Constable I, Cooper R. Macular oedemaand retinal branch vein occlusion. Aust J Opthal-mol. 1980;8(3):207–9.
76. Nguyen QD, Brown DM, Marcus DM, et al. Rani-bizumab for diabetic macular edema: results from 2phase III randomized trials: RISE and RIDE. Oph-thalmology. 2012;119(4):789–801.
77. Chen G, Tzekov R, Li W, Jiang F, Mao S, Tong Y.Subthreshold micropulse diode laser versus con-ventional laser photocoagulation for diabetic mac-ular edema: a meta-analysis of randomizedcontrolled trials. Retina. 2016;36(11):2059–65.
Adv Ther (2017) 34:1528–1555 1555