Embed Size (px)
Citation preview
Partner Abuse, Volume 8, Number 1, 2017
© 2017 Springer Publishing Company 3 http://dx.doi.org/10.1891/1946-6560.8.1.3
A Review of Domestic Violence Perpetrator Programs in the United Kingdom
Elizabeth A. Bates, PhDUniversity of Cumbria, United Kingdom
Nicola Graham-Kevan, PhDUniversity of Central Lancashire, United Kingdom
Lauren T. Bolam, BSc, MScUniversity of Cumbria, United Kingdom
Abigail J. V. Thornton, PhDUniversity of Central Lancashire, United Kingdom
The aim of this study was to conduct a review of current intimate partner vio-lence (IPV) perpetrator provision within the United Kingdom. The objective of the review was to explore the characteristics of intervention programs currently within the United Kingdom. Using a questionnaire-based design, we explored characteristics of current programs including program structure, program logis-tics, facilitator characteristics, and facilitator insights around the programs. A number of organizations completed the questionnaire (N 5 21), and a review of existing literature was performed to explore the general characteristics of pro-grams being delivered within the United Kingdom. Within the sample, we found that the feminist approach was still influential, but that facilitators also reported a need to ensure programs are more inclusive in their service provision to repre-sent the diversity of perpetrators found. An unexpected finding from this study was the resistance of many organizations to engage with the research through an apparent suspicion of the agenda and motivation of the research team.
KEywoRDS: intimate partner violence; domestic violence; treatment; Duluth; United Kingdom
research
PA8-1_Final_A1_003-046.indd 3 12/22/16 2:09 PM
4 Bates et al.
The Duluth model was established in the United States in 1981 as an intervention derived from the Duluth Domestic Abuse Intervention Project (Pence & Paymar, 1993). The Duluth model curriculum was developed by activists within the battered women’s movement and five battered women (Pence & Paymar, 1993) who believed domestic vio-lence was caused by men’s patriarchal ideology. The Duluth-derived program therefore focused on reeducating partner-violent men. Reeducation (rather than treatment) was deemed appropriate because men’s violence to their intimate partners was understood as not “stemming from individual pathology, but rather from a socially reinforced sense of entitlement” (Paymar & Barnes, n.d.). Using the “power and control wheel” was cen-tral because partner violence was understood as being motivated men’s need for power and control over women. Women’s aggression was understood as self-defensive.
The authors of the model omitted to acknowledge the problems that are associated with generalizing from such a small and unrepresentative sample (Dutton & Corvo, 2006). Ellen Pence (1999) did, however, write prior to her death, “By determining that the need or desire for power was the motivating force behind battering, we created a conceptual framework that, in fact, did not fit the lived experience of many of the men and women we were working with. . . . Speaking for myself, I found that many of the men I interviewed did not seem to articulate a desire for power over their partner. Although I relentlessly took every opportunity to point out to men in the groups that they were so motivated and merely in denial, the fact that few men ever articulated such a desire went unnoticed by me and many of my coworkers. Eventually, we real-ized that we were finding what we had already predetermined to find” (pp. 29–30).
Despite Pence’s (1999) shift in position, the Duluth model and programs derived from it are prevalent throughout the Western world.
This may well be moot if programs based on Duluth or Duluth/cognitive behavioral therapy (CBT) hybrids were effective. Research has consistently found that such ap-proaches are not effective, however (Babcock, Green, & Robie, 2004; see also Babcock & La Taillade, 2000; Daly & Pelowski, 2000; Feder & Wilson, 2005). This is probably because of the model ignoring treatment need factors such as emotional dysregulation (Birkley & Eckhardt, 2015) and relationship dynamics such as bidirectional intimate partner violence (IPV; Langhinrichsen-Rohling, Misra, Selwyn, & Rohling, 2012).
By ignoring the range of influences (e.g., social, developmental, and biological) that contribute to the perpetration of IPV, interventions and treatments are unlikely to be successful. Studies that have examined the success rates of the Duluth model intervention program have unsurprisingly found it to be unsuccessful. Babcock et al. (2004) performed a meta-analysis of 22 studies that evaluated such treatment pro-gram for domestically violent men and found minimal effects, concluding that the current interventions are inadequate in reducing recidivism much beyond the effect of arrest and other criminal justice sanctions. Dutton (2006) reviewed both its lack of efficacy and the wealth of evidence contradicting its feminist foundations, concluding that its continued use is impeding effective treatment and judicial responses.
Many researchers (e.g., Ehrensaft, 2008) argue that a movement beyond gendered theories of treatment is imperative and to negotiate a move toward a developmental
PA8-1_Final_A1_003-046.indd 4 12/22/16 2:09 PM
U.K. Perpetrator Programs 5
approach, taking in all the important associated risk factors and developmental correlates. New treatment programs must be built on strong, empirically tested foundations based on the wealth of information that exists about the risk factors involved including the general violence and substance abuse literatures. Many re-searchers have suggested improvements for intervention strategies. For example, Graham-Kevan (2009) argued that in the absence of effective IPV programs, general (non-IPV) violence programs could be examined in the context of IPV perpetrators. Ideally, however, IPV programs should be designed to target criminogenic risk factors in a therapeutic rather than educational manner (Dixon, Archer, & Graham-Kevan, 2012). Other researchers argue that risk assessment should encompass both per-petrator and victim characteristics (e.g., Kropp, 2009) to more fully understand an individual’s or couple’s risk and intervention need factors. What is imperative is that assessments and interventions are informed by rigorous scientific analysis rather than social ideology, political correctness, or inertia.
EFFECTIVENESS OF PERPETRATOR PROGRAMS
The evidence for the effectiveness of current provision is mixed and often depends on the ideological beliefs of the authors. Feminist researchers tend to speak more favorably of the current perpetrator programs and claim greater effects than the evidence can support. For example, Gondolf and Jones (2001) used a multisite evalu-ation to create a natural quasi-experiment. They concluded their evaluation demon-strated that those who completed the programs in their study were 44%–64% less likely to reassault their partner than those men who did not complete the program. Completion or dropout from a lengthy program, however, is not random. For exam-ple, using a prospective design, Gruzinski and Carrillo (1988) compared completers, intake completers, and partial program completers and found that factors such as a history of abuse victimization, witnessing domestic violence in the family of ori-gin, educational attainment, and employment status all distinguished dropouts from completers. Hamberger and Hastings (1989) also compared dropouts and completers and found dropouts were younger, had lower employment levels, higher pretreatment levels of police contact for drug and alcohol-related offenses, and higher levels of bor-derline and schizoid tendencies than completers. This suggests that failing to control for preexisting characteristics of participants in IPV programs can result in unreli-ably favorable results. Therefore, issues with attrition and poor reliability of the in-struments used where not acknowledged in Gondolf ’s (2007) evaluation. Dutton and Corvo (2007), in their reply to Gondolf ’s (2007) critique of their 2006 paper, state that “. . . the burden of disproving efficacy replaces the burden of demonstrating efficacy . . . counter to the basic principles of evidence-based practice” (p. 664).
Despite the mixed evidence presented for the programs that are informed by feminist ideology, it is still the dominant curriculum used within the United States. The Duluth model remains a political model that rejects any emotional and psychological issues a male perpetrator may have because these are seen as excusing his violence; here, public
PA8-1_Final_A1_003-046.indd 5 12/22/16 2:09 PM
6 Bates et al.
policy is being dictated by politically motivated activists rather than by those who would be considered experts such as academics and psychologists (Dutton & Corvo, 2006).
PERPETRATOR PROGRAMS IN EUROPE
Most research examining perpetrator programs and their effectiveness have been based in North America (e.g., Babcock et al., 2004; Eckhardt et al., 2013). There has been little published until recently about the way perpetrator programs are delivered and evaluated within Europe. Graham-Kevan (2007) discusses the lack of cohesive policy within the European Union at the time the paper was published and comments that, like with the United States, the curriculum of perpetrator programs could be shaped by politics and not by evidence and science.
Hamilton, Koehler, and Lösel (2012) reviewed perpetrator programs that existed in practice in Europe. Their results revealed data from 19 of 23 countries—4 countries did not deliver programs. The most common model/approach was CBT (70%) followed by pro-feminist (54%) and psychodynamic (31%). Forty-one percent used a combina-tion of pro-feminist and CBT. On average, the programs had been running for 8 years with the United Kingdom having the longest one at 25 years. In contrast to the find-ings of Babcock et al. (2004), Hamilton et al. found that CBT was implemented more commonly alongside the pro-feminist models rather than instead of.
Akoensi, Koehler, Lösel, and Humphreys (2013) further systematically reviewed existing provision within Europe finding only 12 evaluations that fulfilled their cri-teria. The authors were critical of evaluation design including issues with a lack of comparison group, selection bias, attrition, and the heterogeneity of the men within the programs. They concluded that they could not draw any firm conclusions about the effectiveness of the delivery of programs within Europe.
PERPETRATOR PROGRAMS IN THE UNITED KINGDOM
The perpetrator programs present currently within the United Kingdom appear to be influenced by the same model that informs treatment programs within the United States. Eadie and Knight (2002) discuss the development of perpetrator programs within the United Kingdom crediting the Women’s Aid federation with raising aware-ness and acknowledging them as experts within the area. They discuss frustrations in the 1980s that although the victim movement was supporting women, “male per-petrators were not being confronted with their behaviour” (pp. 167–168). Graham-Kevan (2007) comments that although the efforts of this movement are deserving of praise for female victims, it does not mean they are qualified to dictate interventions with perpetrators.
The organization that accredits programs within the United Kingdom is called Respect. Respect is a government-funded charity that petitions to inform policy; their purpose of accreditation includes to provide a recognized framework and to set the standards for work with perpetrators. Dixon et al. (2012) reviewed the validity of
PA8-1_Final_A1_003-046.indd 6 12/22/16 2:09 PM
U.K. Perpetrator Programs 7
Respect’s position statement including the analysis of several assumptions that form the foundation of the model. These feminist-informed assumptions include, but are not limited to, the notion that most violence is committed by men, that women’s vio-lence is usually defensive, and that gender is the most important factor in terms of perpetration and victimization. Dixon et al.’s analysis highlights that the feminist perspective is still hugely influential in the U.K. system despite the wealth of re-search that has contradicted it. Furthermore, they call for more methodologically rig-orous evaluations and evidence that can inform practice. Debbonaire and Todd (2012) from Respect wrote a commentary stating that their work is informed by quality re-search and practice. In fact, their paper included few references to the literature, with those that were present being feminist in nature. Interestingly, this is a criticism by Archer, Dixon, and Graham-Kevan (2012) in their rejoinder.
It is clear that within the United Kingdom, as within the United States and Canada, there is still a strong feminist influence in practice. There have been many studies conducted in North America examining the effectiveness of these perpetrator programs (e.g., Babcock et al., 2004), but there have been very few studies detail-ing evaluations of perpetrator programs in the United Kingdom. Those that have, have been accompanied by similar issues as those from North America include small sample sizes, lack of long-term follow-up, a lack of a control group for comparison, and issues with selection criteria/bias (see Dutton & Corvo, 2006, for a review of these is-sues within the United States).
The first known evaluation of a U.K. perpetrator program came from Dobash, Dobash, Cavanagh, and Lewis (1999) who describe the introduction of perpetrator ser-vices and interventions originating as late as 1989. Their evaluation centered around two programs within Scotland (CHANGE and Lothian Domestic Violence Probation Project) which focused on the offender, his violent behavior and the need for him to change. The authors believed they were addressing some of the issues with previous evaluations (described earlier) by using three periods, including partner reports, a larger sample size, and including a comparison group—this was a group of men who experienced other criminal justice system (CJS) sanctions. At Time 1 interview, there were no differences between the baseline measures for these two groups; however, at Time 2, follow-up questionnaires and court records revealed an apparent reduction in violence toward partners for the program group when compared to the other CJS group. There were, however, no effect sizes reported to really understand how great a desistance was found; furthermore, there were issues with attrition.
Bowen, Gilchrist, and Beech (2005) similarly evaluated a court-mandated pro-feminist rehabilitation program based on the Duluth model. The authors explored the effectiveness of the intervention across an 11-month follow-up but concluded it had not significantly reduced reoffending among the program completers. In contrast, their results appear to support the overlap between IPV and other types of aggressive behavior that feminist researchers so often deny.
Morran (2013) used a qualitative methodology and interviewed 11 men who vol-untarily attended one of two U.K. IPV programs. Morran described an absence within
PA8-1_Final_A1_003-046.indd 7 12/22/16 2:09 PM

8 Bates et al.
the literature of studies that examined some of the dynamics and context of perpetra-tors’ lives that could positively, or negatively, impact on their desistance. Many femi-nist researchers (e.g., Dobash, Dobash, Cavanagh, & Lewis, 1998) have suggested that the only reliable source of program effectiveness is partner reports because men’s own observations could be seen as ongoing abusive tactics. However, Morran highlights that consideration of men’s own accounts of their IPV would help cre-ate tailored and personalized interventions; this is in contrast to the Duluth model. Morran’s analysis revealed the multifaceted nature of men’s desistance from violence against their partners, with many issues being similar to other offenders. The author recommends a reassessment of the current interventions to consider other aspects of men’s lived experience such as disrupted attachment which could create their desire to control (Dutton & Sonkin, 2003).
The few other U.K.-specific papers have concentrated more on either the victim’s perceptions of the perpetrator services (Madoc-Jones & Roscoe, 2010) or perceptions of the service providers (Featherstone & Fraser, 2012). Stanley, Graham-Kevan, and Borthwich (2012) acknowledged within the literature that there was little recognition of men’s role as fathers in both the U.S. and U.K. perpetrator programs. They reported very preliminary results of an evaluation of a voluntary program that offered a range of therapeutic approaches in individual sessions. Part of the program involved teaching men to recognize the effect their abuse had on the children. Those who were involved with child services demonstrated more engagement compared to those who were not. Most women further noticed a change in their partner’s behavior, and police data showed a decrease in offenses compared to the 2 years prior to the program starting.
Theoretical frameworks are crucial in helping guide practitioners and profession-als in their practice (Dixon & Graham-Kevan, 2011). Indeed, current practice in the United Kingdom is still strongly influenced by feminist work (Dixon et al., 2012) ren-dering all other research and theories into violent behavior effectively irrelevant; this can often stop practitioners considering alternative methods of intervention (Corvo & Johnson, 2003). The Duluth model seems to have experienced an “immunity” from having to answer to any external empirical evaluation; the political concerns are given more weight than the science (Corvo, Dutton, & Chen, 2008, p. 112). Further-more, critics caution that programs cannot necessarily be lifted out of one political and cultural context and placed effectively within another (Akoensi et al., 2013).
AIM OF THE CURRENT STUDY
The literature review earlier addressed the question of what current research exists evaluating perpetrator programs within the United Kingdom. The aim of this study was to conduct a review of current IPV perpetrator provision within these areas. The objective of the review was to address the following key research question: What are the characteristics of IPV perpetrator intervention programs within the United Kingdom? This will include reviewing the population they serve (e.g., male or female, age range), source referral (e.g., court mandated, voluntary/self-referred), and the
PA8-1_Final_A1_003-046.indd 8 12/22/16 2:09 PM

U.K. Perpetrator Programs 9
program characteristics (e.g., length of program, number of sessions, modality, cur-riculum informing the program).
METHOD
Design and Sampling Strategy
The aim within this study was to try and collect as many responses to the survey (described in the following text) as possible from various providers of domestic vi-olence perpetrator intervention across the United Kingdom. Ethical approval was gained through the University of Cumbria and additionally through the United Kingdom’s National Offender Management Service (NOMS) to be able to have access to front-line staff. E-mails were also sent to all the Police and Crime Commissioners within the United Kingdom to gain the information they held around organizations delivering programs. Furthermore, Internet services were conducted to contact chari-ties and organizations that were linked with these services. Letters or e-mails were sent to approximately 134 prisons, 33 probation services, and 51 additional organiza-tions. There are 218 services with responses from 21 organizations, leaving an ap-proximately 10% response rate.1
Measures
Because this review formed one part of a larger multinational research project, the questionnaire-based measure used here was similar to that used within other coun-tries. The questionnaire entitled “National Survey for Domestic Violence Intervention Programs” was developed at Tulane University in conjunction with the Association of Domestic Violence Intervention Programs. It is structured with sections that allow information to be gathered on multiple levels including program structure and con-tent (e.g., “What modalities do you use to deliver treatment to domestic violence per-petrators?” and “What does your intake/assessment procedure consist of?”), program logistics (e.g., “Approximately how many perpetrators does your program serve?” and “Please provide percentages for the demographics of client population.”), facilita-tor characteristics (e.g., “What are the educational requirements for facilitators of domestic violence perpetrator treatment at your agency?” and “Please identify the number of intervention facilitators by gender.”), facilitator insights (e.g., “Who do you think most often initiates physical violence against their intimate partners?” and “In general, male perpetrators are motivated to abuse their partners for what reason?”), and views on state/provincial standards and program improvement (e.g., “Do you think your state’s standards adequately provide effective interventions for perpetra-tors?”). Most questions were closed and required participants to respond on either a Likert scale (e.g., 1 5 strongly agree to 5 5 strongly disagree), provide percentages, or rate importance (e.g., 1 5 not at all important to 3 5 very important). Other qualita-tive questions allowed participants the opportunity to give more detailed responses
PA8-1_Final_A1_003-046.indd 9 12/22/16 2:09 PM
10 Bates et al.
around areas such as delivery (e.g., “How would you deal with a client in your group who seems to be co-operating with the program but who remains quiet and rarely talks?”), specific services (e.g., “Do you provide any LGBTQ-specific services? Please describe.”), and overall program quality (e.g., “Describe any ways this intervention program could be improved.”).
The survey further asked details around the demographics of the respondent including questions around age, gender, educational achievements, and ethnicity. Through seeking ethical approval (described earlier), we were asked to remove these questions and so do not report the responses for these questions here (please see Appendix for full questionnaire).
RESULTS
The first finding to note here was around a general unwillingness of many organi-zations to participate in the study. Many organizations failed to complete the ques-tionnaire, with others contacting the research team but then later refusing based on reasons such as differing ideological positions. One organization apologized by saying, “Now I know the source of the research I do not wish to respond.” There was a suspicion around motives, funding, agenda, and how the data would be used. Gener-ally speaking, these suspicions and doubts came from organizations that are known to be feminist-oriented. Despite the anonymous nature of the questionnaire, it was not possible to encourage many of these organizations to take part.
The data from the anonymous questionnaire was analyzed with a view to provid-ing a summary of responses within the different sections of the article. These will be discussed in the following section.
Program Structure and Content
Among respondents, all treatment programs said they used a group setting to deliver treatment and interventions to perpetrators. A further 61.9% indicated they addi-tionally used individual delivery, 9.5% also used family interventions, and 4.8% indi-cated they used couple therapy. No respondent indicated they used couples therapy in groups.
Domestic violence perpetrator programs provided a large range of services and information for their clients including a wide variety of skills and tactics. All organi-zations indicated they provided perpetrators with skills around identifying and man-aging emotions, communication skills, general self-awareness, general coping skills, and life skills (100%). Most providers also taught anger management and impulse control skills (95.2%), conflict resolution skills (95.2%), the impact of abuse on victims (90.5%), the effects of violence on children (90.5%), and about identifying power and control tactics (81%). Furthermore, a significant proportion also provided services to teach meditation and relaxation exercises (76.2%), consciousness about gender roles (76.2%), taught about socialization factors (76.2%), changing pro-violent/irrational
PA8-1_Final_A1_003-046.indd 10 12/22/16 2:09 PM
U.K. Perpetrator Programs 11
thoughts (71.4%), understanding childhood experiences (71.4%), and assertiveness training (66.7%). Far fewer agencies explored the impact of healing from past trauma (14.3%), identifying mutual conflict cycles (4.8%), or work around grief (9.5%).
All agencies provided this information at check-in time and discussion. The ma-jority used both role-play (95.2%) and also handouts and exercises (90.2%). DVDs and audio were used by several organizations (81%) with goal setting (76.2%) and progress logs/use of journals (61.9%) being used frequently too. Lectures were used relatively infrequently (23.8%), but a further 9.6% indicated the use of autobiographi-cal exercises including discussions.
Next, the survey explored what participants and facilitators considered the primary treatment/intervention approaches of their programs. Most providers included CBT (85.7%) and motivational interviewing (81%) as part of their inter-ventions. Significant proportions also included work around social learning (66.7%) and strength-based approaches (57.1%). More than half of the providers used some form of work around power and control (52.4%), although only a much smaller num-ber identified their work as feminist (19.0%). Also used frequently were solution-focused work (52.4%), self-help and peer support (47.6%), client-centered work (33.3%), and psychoeducational interventions (28.6%). Those used less frequently were narrative therapy (19%), trauma-focused (9.5%), family systems therapy (4.8%), a psychodynamic approach (4.8%), and emotion regulation (4.8%).
In terms of how providers ranked the importance of the different approaches, these were largely in line with what is indicated earlier. For example, the one ranked most important was CBT (52.4%); it was further ranked commonly at Number 2 (19%) and Number 3 (19%). Motivational interviewing was the next most common approach ranked at Number 1 (23.8%). Power and control was ranked as Number 1 to Number 5 for more than half of the providers (52.4%).
There was a wide range of program lengths. Some providers indicated the num-ber of sessions was dependent on need; one provider indicated a program could run between 12 and 52 sessions depending on the need of the client. The average num-ber of sessions across the providers was 29.15 overall, but some providers provided a breakdown of group and individual sessions. For example, some providers used 15 group sessions and 4 individual sessions. Others indicated it varied by intensity; one provider indicated it would be 65 sessions for a high-intensity program but only 32 for moderate intensity. The range across the whole sample was between 12 and 70 sessions. The average duration of session also varied from 30 to 60 minutes (4.8%), 60 to 90 minutes (19.0%), 90 to 120 minutes (23.8%), 120 to 150 minutes (33.3%), and some 150 minutes plus (19.0%).
Most providers had sessions running once a week (42.9%), with the second most common being twice a week (19.0%). Again, there was a wide range of session fre-quency here. Some providers indicated their sessions were three times a week (4.8%) and three to four times a week (14.3%), but one provider indicated their sessions ran daily. There was an average of eight people in each session. In terms of the setting of the sessions, a significant number took place in prison (33.3%), and
PA8-1_Final_A1_003-046.indd 11 12/22/16 2:09 PM

12 Bates et al.
the same proportion also took place in a community setting (33.3%), with an ad-ditional number taking place in probation settings (14.3%), private facilities (10%), and other (10%).
Most organizations had a 60-minute plus intake/assessment procedure (85.7%), with the remaining being between 31 and 59 minutes (14.3%). All providers included an oral interview as part of their assessment, and the majority also included some sort of standardized questionnaire (76.2%). These questionnaire-based measures included psychometrics, personality assessment, measures of abusive behavior, and many included risk assessment measures (e.g., Domestic Abuse, Stalking and Ha-rassment and Honor-Based Violence; Spousal Assault Risk Assessment).
Programs provided additional services to their clients. These varied in number, and some are likely a function of the setting in which the programs existed. Most common additional services were some form of career services (42.9%), counseling for those with substance abuse problems (38.1%), educational resources (38.1%), job training (38.1%), and housing (33.3%). Others were offered crisis management (31.1%), employment assistance (28.6%), financial help (28.6%), food (23.8%), and included mentoring as part of their provision (23.8%). Seen less often were parent-ing classes (14.3%), clothing (14.3%), help with transportation (9.5%), assistance in terms of police/safety (9.5%), and community advocacy (9.5%). Under the heading of “Other” (57.1%), providers had indicated they offered signposting and referral to additional services (19%). A small proportion (9.6%) indicated they did not actually provide these additional services, but these were part of the wider prison service.
In terms of contact with the victims, the providers indicated once again a wide range of contact. The majority indicated the facilitators never contacted the victim (approximately 72.0%). Others indicated they either directly or indirectly contacted the victims before, during, and after treatment. Many indicated this was through the use of a women’s safety worker and ranging from a few times to as often as the victim requested. Of the agencies who participated in the study, a number offered services to victims. A number offered peer support groups (26.6%), legal assistance (19%), tran-sitional housing (14.3%), shelter beds (14.3%), social services assistance (e.g., child care, food stamps; 14.3%), and mental health treatment (4.8%). Several agencies also indicated they offered “other” services, and these included crisis support, counseling, resettlement services, trauma recovery groups, signposting to specialist groups, and the use of women’s safety workers as a layer of support.
Program Logistics
Programs served a wide range in terms of the number of perpetrators. The data given here varied by measure, which made it difficult to average. For example, some indi-cated it was 40 per year, whereas others indicated number per course and others gave a running total of historical numbers. The range of numbers no doubt reflects the variety of organization size captured within the current dataset. Most organizations provided their training in English only. One organization indicated it also provided
PA8-1_Final_A1_003-046.indd 12 12/22/16 2:09 PM
U.K. Perpetrator Programs 13
for those of European nationalities, and a further one organization indicated some of the materials could be presented in up to 14 different languages.
Most organizations (81%) served only male perpetrators in their provision. The remaining organizations included either a small number of women (10%–15% for one provider), with three others indicating it was around 50–50. One of the latter did include victim figures, so it may have confused this figure. This was reflected in the majority indicating their sole provision was men (81%). Similarly for sexuality, 52% of the sample indicated their provision was solely provided for heterosexuals with 33.3%, indicating more than 90% of those included on their programs were heterosex-ual. One organization indicated they did not have access to that information. Simi-larly, the proportion of providers indicating they offered provision to other sexualities was small: lesbian (0%–1%), gay (0%–20%), and bisexual (0%–8%). All providers indi-cated they had not served transgender people within their sample—either highlight-ing it was 0% or a few indicating they did not have access to this information.
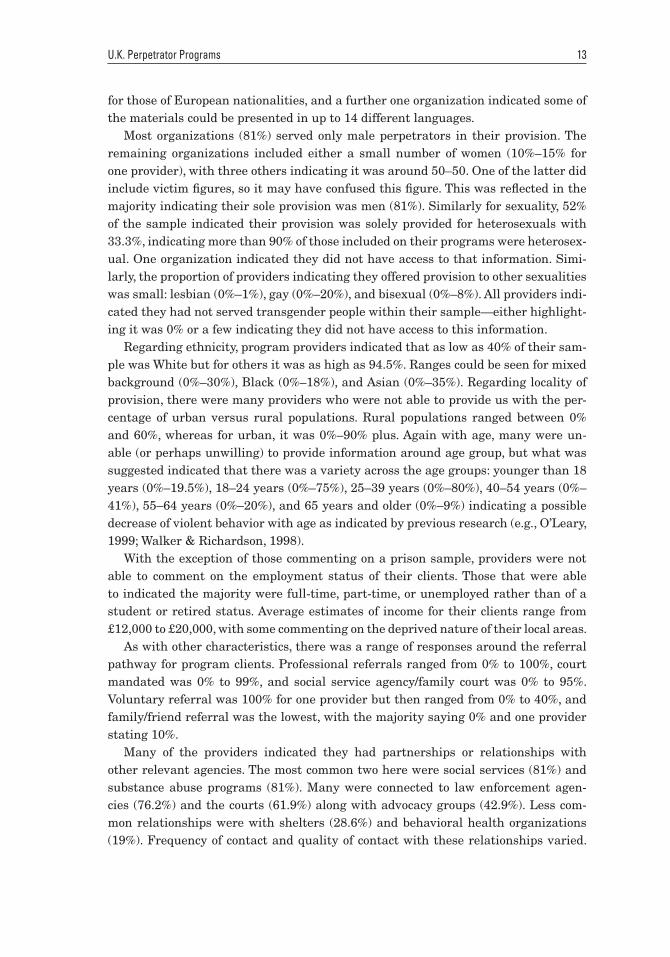
Regarding ethnicity, program providers indicated that as low as 40% of their sam-ple was White but for others it was as high as 94.5%. Ranges could be seen for mixed background (0%–30%), Black (0%–18%), and Asian (0%–35%). Regarding locality of provision, there were many providers who were not able to provide us with the per-centage of urban versus rural populations. Rural populations ranged between 0% and 60%, whereas for urban, it was 0%–90% plus. Again with age, many were un-able (or perhaps unwilling) to provide information around age group, but what was suggested indicated that there was a variety across the age groups: younger than 18 years (0%–19.5%), 18–24 years (0%–75%), 25–39 years (0%–80%), 40–54 years (0%–41%), 55–64 years (0%–20%), and 65 years and older (0%–9%) indicating a possible decrease of violent behavior with age as indicated by previous research (e.g., O’Leary, 1999; Walker & Richardson, 1998).
With the exception of those commenting on a prison sample, providers were not able to comment on the employment status of their clients. Those that were able to indicated the majority were full-time, part-time, or unemployed rather than of a student or retired status. Average estimates of income for their clients range from £12,000 to £20,000, with some commenting on the deprived nature of their local areas.
As with other characteristics, there was a range of responses around the referral pathway for program clients. Professional referrals ranged from 0% to 100%, court mandated was 0% to 99%, and social service agency/family court was 0% to 95%. Voluntary referral was 100% for one provider but then ranged from 0% to 40%, and family/friend referral was the lowest, with the majority saying 0% and one provider stating 10%.
Many of the providers indicated they had partnerships or relationships with other relevant agencies. The most common two here were social services (81%) and substance abuse programs (81%). Many were connected to law enforcement agen-cies (76.2%) and the courts (61.9%) along with advocacy groups (42.9%). Less com-mon relationships were with shelters (28.6%) and behavioral health organizations (19%). Frequency of contact and quality of contact with these relationships varied.
PA8-1_Final_A1_003-046.indd 13 12/22/16 2:09 PM

14 Bates et al.
For example, 57.9% of the sample rarely or never engaged with the courts, but of those who did, 38.1% rated the quality of the relationship as good to excellent. Social services was the most common additional agency that providers were in touch with, 42.8% of the providers being often or always in touch. Of these, 57.2% indicated the quality of the relationship was good or very good. In contrast, most providers rarely or never engaged with advocacy groups (66.7%) or behavioral health (66.7%).
Respondents estimated what percentage of the program funding came from vari-ous sources. Most of the funding seemed to come from government funding at the national and local level. The perpetrator provided funding for only two organizations, a contribution of 20% and 50%, respectively.
Facilitator Characteristics and Insights
Respondents further completed information around the facilitators’ requirements, characteristics, and perceptions of program effectiveness. For 14.3% of respondents, there were no educational requirements for facilitators to deliver programs. For 71.4% of programs, there was a requirement to have at least a high school qualifica-tion, and for a further 14.3%, a bachelor’s degree was required. No agency stated the need for postgraduate-, doctoral-, or medical-level qualifications. However, five of the agencies indicated additional requirements of training such as safeguarding qualifications, counselor accreditation, or Respect group facilitator training. When asked what the typical educational attainment was for facilitators, 47.6% responded that high school–level qualifications was typical, 71.4% indicated degrees-level quali-fications were typical, and 23.8% indicated master of science (MSc)/master of arts (MA)-level qualification could typically be found among the facilitators. As stated earlier, typically there were other qualifications present around counseling experi-ence and national vocational qualifications. Typical facilitators were stated as having anywhere between 1 and 20 years experience working in the field, with the majority falling between 1 and 10 years.
In terms of other types of training, respondents indicated anywhere between 0 (9.5% said they receive 0 hours of training) and 80 hours per year were spent on domestic violence-specific training, between 0 and 15 hours a year on non-domestic-violence-related mental health training, and between 0 and 44 hours of other types of training every year. Respondents indicated spending anywhere between 0 and 250 hours a year around case reviews and peer support.
The number of female facilitators within the current sample varied between 1 and 14, with one provider stating 100. For male providers, the figures were smaller be-tween 1 and 6, although one agency did state again there were around 100 facilitators who were male. This respondent is likely to be reporting on a larger agency.
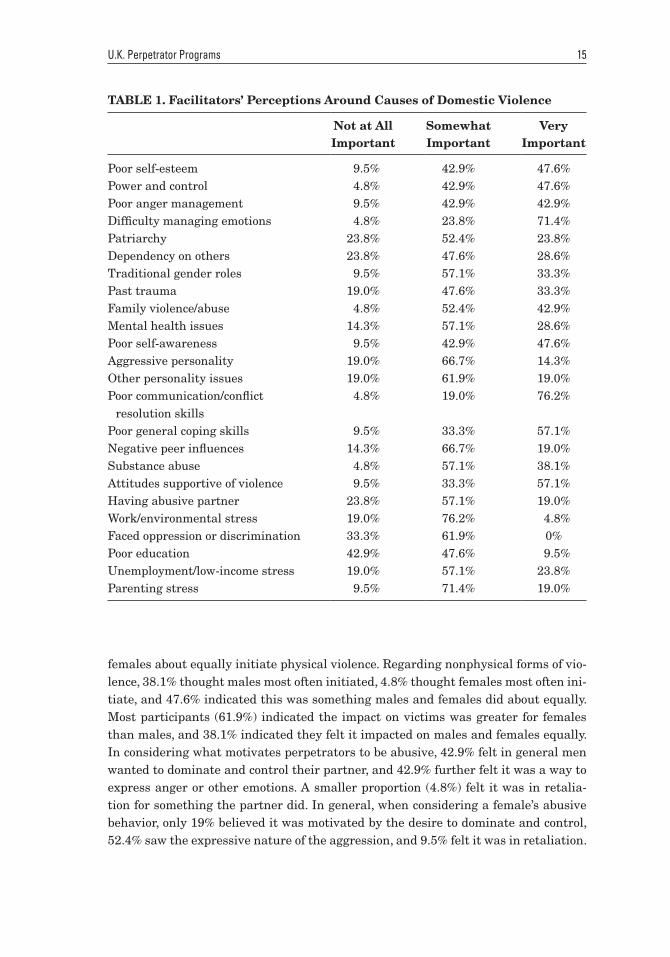
Facilitators were asked what they perceived the most important factors that cause domestic violence perpetration. The findings are illustrated in Table 1.
When asked who most often initiates physical violence within the relationships, 66.7% indicated the male most often initiates, whereas 28.6% indicated males and
PA8-1_Final_A1_003-046.indd 14 12/22/16 2:09 PM
U.K. Perpetrator Programs 15
females about equally initiate physical violence. Regarding nonphysical forms of vio-lence, 38.1% thought males most often initiated, 4.8% thought females most often ini-tiate, and 47.6% indicated this was something males and females did about equally. Most participants (61.9%) indicated the impact on victims was greater for females than males, and 38.1% indicated they felt it impacted on males and females equally. In considering what motivates perpetrators to be abusive, 42.9% felt in general men wanted to dominate and control their partner, and 42.9% further felt it was a way to express anger or other emotions. A smaller proportion (4.8%) felt it was in retalia-tion for something the partner did. In general, when considering a female’s abusive behavior, only 19% believed it was motivated by the desire to dominate and control, 52.4% saw the expressive nature of the aggression, and 9.5% felt it was in retaliation.
TABLE 1. Facilitators’ Perceptions Around Causes of Domestic Violence
Not at All Important
Somewhat Important
Very Important
Poor self-esteem 9.5% 42.9% 47.6%Power and control 4.8% 42.9% 47.6%Poor anger management 9.5% 42.9% 42.9%Difficulty managing emotions 4.8% 23.8% 71.4%Patriarchy 23.8% 52.4% 23.8%Dependency on others 23.8% 47.6% 28.6%Traditional gender roles 9.5% 57.1% 33.3%Past trauma 19.0% 47.6% 33.3%Family violence/abuse 4.8% 52.4% 42.9%Mental health issues 14.3% 57.1% 28.6%Poor self-awareness 9.5% 42.9% 47.6%Aggressive personality 19.0% 66.7% 14.3%Other personality issues 19.0% 61.9% 19.0%Poor communication/conflict
resolution skills 4.8% 19.0% 76.2%
Poor general coping skills 9.5% 33.3% 57.1%Negative peer influences 14.3% 66.7% 19.0%Substance abuse 4.8% 57.1% 38.1%Attitudes supportive of violence 9.5% 33.3% 57.1%Having abusive partner 23.8% 57.1% 19.0%Work/environmental stress 19.0% 76.2% 4.8%Faced oppression or discrimination 33.3% 61.9% 0%Poor education 42.9% 47.6% 9.5%Unemployment/low-income stress 19.0% 57.1% 23.8%Parenting stress 9.5% 71.4% 19.0%
PA8-1_Final_A1_003-046.indd 15 12/22/16 2:09 PM

16 Bates et al.
Data Collection
Most providers did collect data on their programs (95.2%); however, one provider did not. This data was largely descriptive (61.9%), with less than half the providers (28.6%) collecting outcome data around recidivism rates. Most of the sample (42.9%) collected this data monthly, quarterly (14.3%), or yearly (4.8%). This data was col-lected mostly by the agency (61.9%) and not as frequently by external evaluators or researchers (23.8%). Satisfaction with the data collection ranged from completely (9.5%), very (28.6%), moderately (42.9%), slightly (14.3%), to not at all (4.8%).
More than 90% of those completing the questionnaire indicated a 60%–97% com-pletion rate when asked to estimate the number of clients who completed the pro-gram after having taken the initial assessment. A further 9.6% estimated much lower at 28%–30% of those who started completed. In terms of recidivism, more than half of the sample (57.1%) did not know whether their program completers went on to reof-fend or be arrested for IPV-related incidents within 1 year of finishing the program. The remaining providers estimated between 0% and 20% go on to reoffend.
Most of the programs were used according to a written curriculum (85.7%). Where this was not the case, a small number (4.8%) used it according to the philosophy and expectations of the agency. Less than half the sample (23.8%) indicated the treat-ment interventions were the same for all clients with the remaining number (76.2%), indicating they adapted their interventions to fit the needs of the clients. A further proportion (38.1%) indicated they had developed their interventions specifically for various client needs and contexts. Those that had indicated this were asked to specify what populations these were for; these included different needs within the group, the use of a framework as a result of sessions with a psychiatrist, adapted for language, adapted for learning styles, adapted for those with learning difficulties, mental health problems and substance misuse, different populations, different levels of violence, for female perpetrators, and for cultural diversity.
When asked to describe any training or strategies that facilitators receive or use to make treatment interventions culturally sensitive to the given population, there were a range of responses. Some indicated that there was equality and diversity training available (on induction and annually updated), others indicated that supervision was used to explore cultural issues, liaising with relative agencies, and adapting materi-als (e.g., ethnically diverse power and control wheel), whereas others were not aware or did not receive any. One participant cited, “We do not allow culture to be used as a reason for abuse; however, we acknowledge it has an influence in the same way drugs, alcohol, childhood, etc. does.” Challenges that facilitators experience in making in-terventions relevant to populations with respect to ethnicity, gender, class, sexuality, disability, religion, age, or citizenship status were also varied. Several participants raised concerns around religious beliefs supporting abuse toward women and girls, whereas others pointed to a lack of insight into specific minority groups made it more challenging to meet their needs. Language is sometimes seen as a barrier to ac-cess, and disability requiring specific adaptations was seen as challenging because of
PA8-1_Final_A1_003-046.indd 16 12/22/16 2:09 PM
U.K. Perpetrator Programs 17
resources to support this is not always available (one participant gave an example of the hearing loop). Some indicated there were no challenges, whereas one participant suggested, “These are far too many and complex to list here!”
When asked whether they provided any lesbian, gay, bisexual, transgender, and queer (LGBTQ)-specific services, the majority said no. Only 14.3% did provide any specific interventions. Some of those who specified no added it was because they pro-vided a service exclusively for male violence against women. When asked what spe-cific services participants would like to see implemented, some felt a program written to reflect dynamics within same-sex relationships was needed, whereas others felt more was needed around awareness raising. One participant reported they wished to see LGBTQ services integrated with the main groups, something that had been requested by service users. Another commented on the development of a program cov-ering all interpersonal abuse which would cover this type of abuse as part of it. One participant suggested there was not necessarily a need for a separate service. Partici-pants felt more understanding around factors affecting the individual was required to understand the differing needs of LGBTQ populations. Other participants com-mented services would look quite different because abuse in same-sex relationships may have a different dynamic (e.g., context of “outing,” homophobia, gender). One participant commented that “they want to be treated the same throughout the pro-gram in our experience,” whereas another suggested they would need to be treated in a separate group.
Views on Program Improvement and State/Provincial Standards
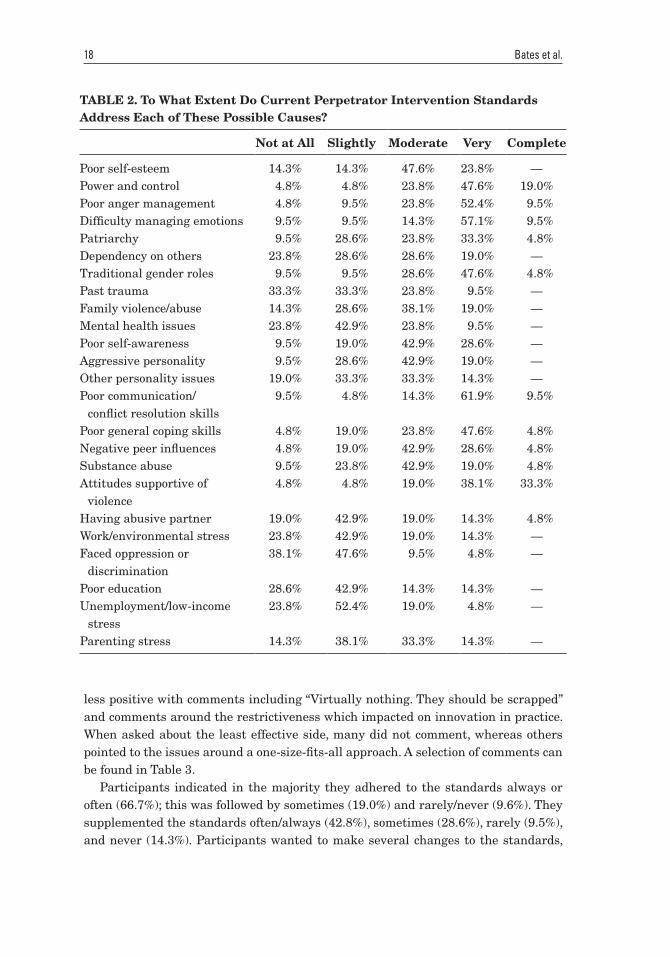
Overall, all participants were moderately, very, or extremely satisfied with the effec-tiveness of their program. When asked about the standards for perpetrator programs in the United Kingdom, some had a very strong understanding (38.1%), a moder-ate understanding (47.6%), some were not sure about whether there were any stan-dards (9.5%), and one participant stated the United Kingdom did not have any (4.8%). Within this, 38.1% indicated they agreed or strongly agreed that the United Kingdom standards adequately provided effective intervention for perpetrators, 23.8% were unsure, and 28.5% disagreed or strongly disagreed. When asked the same question specifically for female perpetrators, 57.1% disagreed or strongly disagreed, with only 9.5% agreeing. Similarly, for same-sex perpetrators, 61.9% disagreed, with only 9.5% agreeing. However, for specifically male perpetrators, 57.2% did agree that the U.K. standards adequately provided effective intervention. Table 2 details how effective participants felt the country’s standards were at addressing each possible cause of IPV.
When asked what they thought was most effective about the U.K. standards, many did not know. Others alluded to the Respect standards stating they are visible, the standards are easy to get hold of, and are clear. Some participants felt positive toward the revision and integrating of new research and practice. Some participants were
PA8-1_Final_A1_003-046.indd 17 12/22/16 2:09 PM
18 Bates et al.
TABLE 2. To What Extent Do Current Perpetrator Intervention Standards Address Each of These Possible Causes?
Not at All Slightly Moderate Very Complete
Poor self-esteem 14.3% 14.3% 47.6% 23.8% —Power and control 4.8% 4.8% 23.8% 47.6% 19.0%Poor anger management 4.8% 9.5% 23.8% 52.4% 9.5%Difficulty managing emotions 9.5% 9.5% 14.3% 57.1% 9.5%Patriarchy 9.5% 28.6% 23.8% 33.3% 4.8%Dependency on others 23.8% 28.6% 28.6% 19.0% —Traditional gender roles 9.5% 9.5% 28.6% 47.6% 4.8%Past trauma 33.3% 33.3% 23.8% 9.5% —Family violence/abuse 14.3% 28.6% 38.1% 19.0% —Mental health issues 23.8% 42.9% 23.8% 9.5% —Poor self-awareness 9.5% 19.0% 42.9% 28.6% —Aggressive personality 9.5% 28.6% 42.9% 19.0% —Other personality issues 19.0% 33.3% 33.3% 14.3% —Poor communication/
conflict resolution skills 9.5% 4.8% 14.3% 61.9% 9.5%
Poor general coping skills 4.8% 19.0% 23.8% 47.6% 4.8%Negative peer influences 4.8% 19.0% 42.9% 28.6% 4.8%Substance abuse 9.5% 23.8% 42.9% 19.0% 4.8%Attitudes supportive of
violence 4.8% 4.8% 19.0% 38.1% 33.3%
Having abusive partner 19.0% 42.9% 19.0% 14.3% 4.8%Work/environmental stress 23.8% 42.9% 19.0% 14.3% —Faced oppression or
discrimination38.1% 47.6% 9.5% 4.8% —
Poor education 28.6% 42.9% 14.3% 14.3% —Unemployment/low-income
stress23.8% 52.4% 19.0% 4.8% —
Parenting stress 14.3% 38.1% 33.3% 14.3% —
less positive with comments including “Virtually nothing. They should be scrapped” and comments around the restrictiveness which impacted on innovation in practice. When asked about the least effective side, many did not comment, whereas others pointed to the issues around a one-size-fits-all approach. A selection of comments can be found in Table 3.
Participants indicated in the majority they adhered to the standards always or often (66.7%); this was followed by sometimes (19.0%) and rarely/never (9.6%). They supplemented the standards often/always (42.8%), sometimes (28.6%), rarely (9.5%), and never (14.3%). Participants wanted to make several changes to the standards,
PA8-1_Final_A1_003-046.indd 18 12/22/16 2:09 PM

U.K. Perpetrator Programs 19
TABLE 3. Qualitative Comments Around the Most and Least Useful Aspects of the U.K. Standards
Most Effective Least Effective
Having a visible organization that pro-motes standards
I have many doubts about standards. They are restrictive and tend to reduce innovation.
Standards are clear and relatively easy to get hold on.
Insufficient resources
The quality and assurance measures that we work to ensure effective outcomes
Not compulsory
We provide various treatment pathways and appear to be constantly reviewing and integrating new research and practice.
Some issues with consistency of program rewrites
Virtually nothing! They should be scrapped.
The current Respect standard is overly complicated and difficult to achieve and includes some items that are of low rel-evance to the standards.
We find the standards set by Respect very effective.
The current standards include some items that are not evidence-based . . . and others that are not legally possible to guarantee . . . These mean they are less likely to be adopted by all programs and commissioners.
The feminist paradigm; male perpetrators and female victims only; overlong pro-grams which produce endless dropouts and total nonfocus on the individual
The limitations on who can attend the pro-gram; the lack of consideration of trauma on the individual’s thoughts and behavior
Too focused on a particular approach to delivery and ethos; etiology of domestic abuse
though. A common recommendation was around expanding provision to cover fe-male perpetrators and those in same-sex relationships. There were also comments including a single set of standards (for statutory and nonstatutory provision) which is evidence-based and raises awareness and knowledge of IPV in other agencies (e.g., courts, social care). Other comments centered on the practicalities of the standards,
PA8-1_Final_A1_003-046.indd 19 12/22/16 2:09 PM
20 Bates et al.
funding, facilitating, and key performance targets. Some more critical comments called for the abandonment of the current standards: “Respect should be scrapped and a fresh start made—as advocated by the Centre for Social Justice, Dr. Louise Brown and others”; and around more transparent publication of effectiveness.
RESULTS FROM REVIEW OF AVAILABLE LITERATURE
With a low response rate to our questionnaire, we felt it is important to consider other available literature on programs and chose to focus specifically on the two main accreditation routes found within the United Kingdom. Within the United Kingdom, there are a series of accredited programs that have been designed to reduce reoffend-ing. These can be accredited through a governmental panel and through Respect, a feminist charity. We will discuss each in turn:
The Correctional Services Advice and Accreditation Panel
Accreditation within the CJS describes the process of validating and approving interven-tions in a similar way to within the fields of education and professional training (Min-istry of Justice, 2014). The Correctional Services Advice and Accreditation Panel was established in 1999 and initially accredited interventions delivered with the prison sys-tem but also now provides advice for NOMS and the Ministry of Justice. Accreditation criteria include having a clear model of change, targeting a range of dynamic risk fac-tors, effective methods, and being skill oriented, and programs are accredited for 5 years after which they are reviewed to ensure they still meet the criteria. Within the area of domestic violence, there are four programs accredited through this process: Building Better Relationships (BBR), Community Domestic Violence Program (CDVP), Healthy Relationships Program (HRP), and the Integrated Domestic Abuse Program (IDAP).
Healthy Relationships Program. HRP is a CBT program that is targeted at male heterosexual IPV offenders that are of medium or high risk to harm. It is a 24- to 68-session program (dependent on risk) that aims to decrease problem thinking re-lated to abusive behavior, emotional mismanagement, other problems around self-regulation (e.g., around impulsivity), deficits in social and communication skills, and antisocial peer associations that may endorse the abuse of women.
Community Domestic Violence Program. This is a community-delivered program that aims to reduce risk of IPV toward women in relationships by facilitating men to change their attitudes and behavior to increase safety and reduce risk of all family-related violence. CDVP is a CBT program that consists of 25 group work sessions across 9–13 weeks.
Integrated Domestic Abuse Program. A community-based IPV program designed for men who have been violent in their intimate relationships with the aim to ending
PA8-1_Final_A1_003-046.indd 20 12/22/16 2:09 PM

U.K. Perpetrator Programs 21
all violence against their female partners. Participants learn here about abusive be-havior and new skills to help them develop nonabusive relationships. IDAP is a CBT program that consists of 27 group work sessions across approximately 27 weeks.
HRP, CDVP, and IDAP have similar theoretical frameworks with the primary aim of reducing violence against women and children. Bullock, Sarre, Tarling, and Wilkinson (2010) describe that CDVP and HRP identify issues around self-control and work with CBT models to address these. IDAP has a more feminist focus and focuses on the role of “culturally reinforced attitudes of power/control over women” (p. 1).
Building Better Relationships Program. BBR represents what was the next stage in NOMS development of IPV perpetrator programs (Ministry of Justice, n.d.). In 2009, NOMS reviewed IPV programs being offered as part of a wider review of interventions they delivered. They concluded with a commitment to “provide a flex-ible, responsive, contemporary, and evidence-based program for perpetrators have resulted in our developing BBR” (Ministry of Justice, n.d., p. 3). BBR is suitable for heterosexual men who use violence against their female partner and those who have been assessed as medium to high risk. It consists of 24 weekly group sessions across four modules: foundation module, My Thinking, My Emotions, and My Relationships. It aims to reduce risk and promote safety through helping men to achieve a better understanding of their IPV, enhance motivation to engage, encourage men to identify and build on their strengths and skills, develop practical and sustainable strategies for change, and promote the quality of life of everyone affected by their aggression.
There are few reviews available of these programs. Bloomfield and Dixon (2015) performed an outcome evaluation on IDAP and CDVP covering 6,695 offenders be-tween 2002 and 2007. They found small but significant reductions in IPV reoffend-ing including at a 2-year follow-up. They conclude that although their findings were promising, many of the men did go into reoffending, and that more up-to-date evidence around IPV and generally violent offending needs to be adopted into such programs.
Bullock et al. (2010) explored the implementation of IPV programs within the pro-bation and prison service using IDAP, CDVP, and HRP. Their finding revealed there was some uneven practice in terms of program delivery, with some adhering strictly to the principle and others deviating. Furthermore, data collection around these programs also varied, with prisons tending to keep better records than probation services where there were very few programs in the community that collected prepro-gram, postprogram, and follow-up data (n 5 40 out of 2,986).
Respect Accreditation
Within the United Kingdom, there is a further level of accreditation that some seek to achieve, that of the feminist organization, Respect. Respect (2012) indicates the ac-creditation standard applies “to all organisations providing domestic violence preven-tion programs (DVPPs) working with men who use intimate partner violence (IPV), and also providing integrated safety services (ISS) for partners and ex-partners of
PA8-1_Final_A1_003-046.indd 21 12/22/16 2:09 PM
22 Bates et al.
these perpetrators” (p. 1). They describe the development of accreditation so people can be assured of a “high quality safety-focused service from organisations accredited by Respect.” Working with both perpetrators and victims is Respect’s minimum unit that is required for consideration for accreditation. Their accreditation is currently only applicable to violent men and their female partners/ex-partners. Respect states that working with perpetrators can only be done so safely if there is an ISS that also contacts partners and ex-partners to provide them with a support service.
The aims of a Respect-accredited service (from Respect, 2012) include to increase the safety of victims; assess and manage risk; be part of a community response to IPV; and provide services that recognize a diverse community which includes being acces-sible, promote respectful relationships, work accountably, support social change, and offer a complete response. There are two stages of accreditation including Safe Mini-mum Practice, which involves being assessed and meeting the majority of the crite-ria, and full accreditation, where an organization meets all 94 of the requirements in the standard. The accreditation materials then go on to detail these criteria under a series of headings around management of the organization, service structures and process, diversity, risk management, children, and partnership working.
The model by which organizations should align their work is feminist in nature and focuses on a man’s use of violence as an instrumental mechanism to exert violence and control over his female partner. Programs should reflect this by ensuring the perpetra-tor is held completely accountable and responsible for his violence which is a behavior he has chosen to engage in. The principles here clearly state that “a willingness to choose to use violent and abusive behaviour towards a partner is influenced by learnt expectations and a gender-based sense of entitlement” (Respect, 2012, p. 28) and the “denial and minimisation of abusive behaviour or any justifications for using abusive behaviour including the use of drugs or alcohol” (Respect, 2012, p. 29). By aligning a treatment program with these principles ignores the wealth of research that indi-cates the high correlations between perpetration and victimization of IPV (e.g., Bates, Graham-Kevan, & Archer, 2014), bidirectionality in IPV (e.g., Charles, Whitaker, Le, Swahn, & DiClemente, 2011), as well as the increased risk this poses (e.g., Marcus, 2012). Men are held accountable for their IPV, and there is a denial of even being able to explore the context of aggression being used, for example, if it is under the influ-ence of drugs/alcohol, if it is as a pattern of mutual aggression, or if it is as a function of something other than these feminist assumptions. In discussing risk management, the assumption is that violence is always unidirectional. At no point within the whole standard is it suggested that women should be asked about their own behavior despite this being something which would have a significant influence on risk.
Respect lobbies the government and is influential in terms of policy development (Dixon et al., 2012), and yet its narrow focus on gender as the most important factor in IPV ignores research that demonstrates the overlap of IPV and other types of ag-gression (e.g., Bates et al., 2014) as well as a wealth of research detailing other risk factors associated with IPV for men and women (e.g., Felson & Lane, 2010; Moffitt, Caspi, Rutter, & Silva, 2001; Thornton, Graham-Kevan, & Archer, 2010, 2012).
PA8-1_Final_A1_003-046.indd 22 12/22/16 2:09 PM

U.K. Perpetrator Programs 23
Dixon et al. (2012) wrote a critique of the Respect position statement and the eight assumptions derived from this; interestingly, this statement (or any mission/position statement) cannot be found online, and Respect has failed to provide us with one de-spite multiple attempts at contact.
There are few evaluations present of these programs, but one significant here for Respect-accredited programs was Project Mirabal, conducted by researchers at Dur-ham University. Kelly and Westmarland (2015) sought to develop a new method-ological approach to evaluating DVPPs to offer what they term a “third generation” (p. 4) perpetrator program methodology. They describe first-generation methodology as concentrating on behavioral responses, with success defined as a reduction in vio-lence measured by convictions or self-reports. Second generation used a more experi-mental design using interventions and a control condition or a multisite evaluation (e.g., Gondolf, 2002). Kelly and Westmarland addressed this by including case studies of DVPPs, longitudinal survey data with women, longitudinal interviews with men and women, plus data on DVPP impact on children and program integrity. They fur-ther used a matched control group of women receiving support as victims but where there was no DVPP support for their male partner. Comparing their treatment group with the control group, the authors state that they “largely found there to be no significant differences in reductions in violence and abuse” (Kelly & Westmarland, 2015, p. 8). The authors also failed to conduct any statistical analysis of pre- and postintervention changes. The authors conclude across the data that the Respect-accredited programs under examination (N 5 12) were successful in improvements of respectful communication, improvement in women’s expanded space for action, quantitative reductions in physical and sexual violence, improved shared parenting, limited improvements in awareness of self and others, and largely a reduction in children’s fear. These “improvements,” however, were drawn from comparing all start-ers with those that completed. For example, when comparing reductions in physi-cal and sexual violence, the preprogram sample size was 99, but the postprogram sample size was only 52; such a comparison is useless in ascertaining whether female victims experienced reductions in physical and sexual violence because the prepro-gram group contained almost twice as many participants as the postprogram group. It is highly likely that those who dropped out were significantly different from those who remained. Indeed, this may be the reason why pre- and postprogram statistical analysis was not conducted: because programs such as SPSS would automatically only include participant data where both time points were represented. The authors made no attempt to explain this in the report in personal communications with one of the authors (Graham-Kevan, 2015). Instead, selected interview quotes were used to support their comparisons of men’s experiences and women’s experiences of change.
There were also significant issues including a lack of clarity around follow-up times and sample sizes, failure to ask about women’s own aggressive behavior, lack of effect sizes being reported, and a lack of exploration around attrition of partici-pants. Therefore, no conclusions can currently be made regarding the efficacy of these Respect-accredited programs.
PA8-1_Final_A1_003-046.indd 23 12/22/16 2:09 PM

24 Bates et al.
DISCUSSION AND CONCLUSIONS
The aim of this study was to review and explore the existing provision of IPV per-petrator programs within the United Kingdom. This study generated a wealth of in-formation around what the current perpetrator provision is within the participating organizations.
In terms of program approach and delivery, all programs within the current sample delivered programs in a group setting; this was still the most often used ap-proach, although some did also use individual sessions and one program include a couples therapy session. CBT was the primary focus of the program, with more than half also having a focus on power and control. Only 19% of the sample identified their program as being primarily feminist. Some believe that group work is what enables men to change by engaging in a process where they see themselves as oth-ers through being challenged (Kelly & Westmarland, 2015). The use of CBT-related techniques within these programs shows a move beyond purely education-based programs, and interventions using this approach have been found to be effective (Dixon et al., 2012).
Most programs identified they only worked with male perpetrators and those who identified as heterosexual. A small number identified work with female, but it is thought these figures may be conflated by also including victim services within this (as indicated by at least one program). This was not a surprising finding because it is well known that there is a paucity of perpetrator services currently available for female perpetrators and those from LGBTQ populations. There has been a wealth of literature that details women’s propensity for aggression and control (e.g., Ar-cher, 2000; Bates & Graham-Kevan, 2016; Bates et al., 2014) as well as literature highlighting the prevalence of aggression in same-sex relationships (e.g., Bologna, Waterman, & Dawson, 1987; Lie, Schilit, Bush, Montagne, & Reyes, 1991; Renzetti, 1992). Yet, there is a lack of service provision for these victims and perpetrators. Cur-rent feminist- and Duluth-inspired models will especially not be appropriate within these populations, and many participants in this study stated these would need to be dealt with separately as populations. Only 14.3% of programs had LGBTQ-specific provision. All comments around this in this study related to sexuality, with no pro-gram even commenting on provision for transgender groups. There was a variety in opinion in how to address this, with some suggesting they integrate provision for everyone into the same group, whereas others suggested they would need a separate service.
Facilitators indicated the most important causes of IPV to be difficulty in manag-ing emotions, poor communication/conflict resolution skills, and attitudes that were supportive of violence. Interestingly, patriarchy was one of the least frequently cited reasons for IPV along with poor education and oppression/discrimination. From the wide range of possible causes given to participants to consider, most participants had indicated that most of them were somewhat important in influencing IPV and abusive behavior. It is possible that this demonstrates a change in thinking about
PA8-1_Final_A1_003-046.indd 24 12/22/16 2:09 PM

U.K. Perpetrator Programs 25
the causes of IPV across the sector, but it is also possible that because of a lack of engagement with several feminist organizations that we have not captured the full range of insights.
Participants largely agreed that IPV was either initiated by men (this was the most endorsed opinion) or was perpetrated equally by men and women. Men’s moti-vations to perpetrate IPV were seen as being mostly driven by the desire to dominate and control, but some participants did indicate that they can also be motivated by expressing anger and emotions, with fewer still suggesting it could be motivated by retaliation. Women’s IPV in contrast was seen largely as expressive and less so in terms of the desire to dominate and control. These perceptions broadly fit with some of the more feminist perspectives on IPV in that men’s aggression is seen as a tac-tic used to dominate and control his female partner (e.g., Dobash & Dobash, 1979); however, facilitators did acknowledge the possibility of bidirectional violence which demonstrates an awareness of the context in which IPV is taking place.
Nearly all programs collected data, but the majority of this was descriptive with very few (28.6%) collecting any outcome data around recidivism. This finding indi-cates most programs cannot be engaging in methodologically rigorous evaluation to ensure their program outcomes are successful. Indeed, this fits with previous research (e.g., Bullock et al., 2010) that has indicated the variation in data collec-tion, with prisons conducting more rigorous assessments than some community- and probation-based services.
Most adhered to the curriculum of the program, but 76.2% indicated they adapted the programs to fit the needs of the perpetrator; this included in terms of learning disabilities, language skills, and learning styles rather than as tailored to the type of aggression found or the consideration of mutuality in aggression. This is a posi-tive finding because it indicates that the “one-size-fits-all” approach of the traditional feminist model is becoming less popular, with programs and facilitators recognizing the need to explore the context of aggression and the function it serves for the per-petrator rather than making assumptions. In their evaluation of program integrity, Bullock et al. (2010) found that there was wide variation in the degree to which pro-viders deviated from the manual in response to the group dynamics.
Most were satisfied with the effectiveness of their program. There was, how-ever, some disagreement around the U.K. standards. Some participants endorsed them commenting on the importance of Respect accreditation; however, others in-dicated the standards should be much more inclusive of various perpetrator char-acteristics (e.g., around gender and sexuality). There was also a call to have more published studies around the effectiveness of the programs. This fits with a lot of research currently within the field that is calling for more evidence-based practice around the use of DVPPs (e.g., Dixon et al., 2012; Dutton & Corvo, 2007; Graham-Kevan, 2007).
The findings across the current sample and the review of current accreditation processes indicates the Duluth model and feminist approach to DVPP is still strongly influential within the United Kingdom.
PA8-1_Final_A1_003-046.indd 25 12/22/16 2:09 PM

26 Bates et al.
Limitations and Challenges
An obvious limitation for this review is the response rate of providers and organiza-tions. With only 21 organizations choosing to take, it is likely there is a significant bias present within the results here. We hoped that the nature of the study would encourage all organizations to anonymously take part and report on their DVPPs, and we are disappointed that some felt ideological differences were a reason not to engage in evidence-based practice.
Furthermore, although we used a mix of quantitative- and qualitative-based ques-tions to gather a mix of data, it is possible we did not capture the full scope of ques-tions that should be asked here. The questionnaire originated from the United States; we adapted it to suit the United Kingdom in the use of terminology and context, but it is possible we missed some aspects specific to the United Kingdom.
Implications
The high frequency of IPV can be seen as reflective of the high levels of interde-pendence found within romantic relationships (Finkel, 2007). This interdependence renders conflict as inevitable, and given that typical conflict will begin with verbally aggressive behavior, it is not surprising that elevated levels of nonviolent conflict pre-dict higher levels of violent behavior in relationships. Finkel (2007) further contests that this interdependence is also responsible for increasing the motivation to influ-ence the partner’s behavior because it is that behavior that predicts the individual’s own outcomes (Felson, 2002). Felson (e.g., Felson, 2002, 2010) was one of the first proponents of studying IPV in the context of other types of aggression. He argued that rather than studying IPV solely from a patriarchal perspective, it should be examined in terms of the characteristics of the perpetrator (at a micro level) instead of society (at a macro level).
Finkel, DeWall, Slotter, Oaten, and Foshee (2009) suggested it is not rare for someone to experience violent impulses during serious relationship conflict. Their results demon-strated that some people experienced the impulses without acting on them. Finkel et al. feel that it is “essential . . . to understand the psychological mechanisms by which individu-als override these impulses in favour of nonviolent conflict behavior” (p. 495). So, contrary to the belief of some (e.g., Dobash & Dobash, 1979), violent impulses toward partners are not something solely experienced by patriarchal men. Implications from Finkel’s (Finkel, 2007; Finkel et al., 2009) work and this study are that interventions should be focusing on individuals and their characteristics rather than seeing IPV as a macro, societal problem that requires social change. Rather than educating men about power and control using a “one-size-fits-all” approach, practice should be tailored to different circumstances. Finkel et al. suggested an approach based on self-regulatory training and demonstrated the ef-fectiveness of a similar self-regulation bolstering in one of their studies.
The feminist approach is still so hugely influential in practice despite the wealth of literature not only criticizing it but also providing various alternative models and
PA8-1_Final_A1_003-046.indd 26 12/22/16 2:09 PM

U.K. Perpetrator Programs 27
methods to try. The lack of research-informed practice here is quite unique and does not seem to be as great a factor in less politicized fields (e.g., other types of aggression).
Conclusions
The Duluth model is cited as still being very influential in U.K.-based work with IPV perpetrators. Phillips, Kelly, and Westmarland (2013) detail in their study that DVPPs have developed in the United Kingdom through “ongoing reflections on a rich diversity of practice, underpinned by a gendered analysis of domestic violence” (p. 3). Feminist models of DVPPs work on assumptions about perpetrators, but without functional assessments of behavior for men and women, it is not possible to fully understand and therefore effectively intervene (Dixon et al., 2012). Until there is a better link between research and practice and research and policy, then this field will continue to be influenced by an ideological and inappropriate model. Rather, we should move beyond gendered analysis and feminist models and explore existing pro-grams used for generally violent offenders and seek to adapt these to working with those who are domestically violent (Graham-Kevan, 2007).
NOTE
1. Seven prisons responded to advise they did not run programs for domestically vio-lent offenders. One advised their program was the same as the national standard (see discussion in text).
REFERENCES
Akoensi, T. D., Koehler, J. A., Lösel, F., & Humphreys, D. K. (2013). Domestic violence perpetrator programs in Europe, Part II: A systematic review of the state of evidence. International Journal of Offender Therapy and Comparative Criminology, 57(10), 1206–1225.
Archer, J. (2000). Sex differences in aggression between heterosexual partners: A meta-analytic review. Psychological Bulletin, 126, 651–680. http://dx.doi .org/10.1037MJ033–2909.I26.5.651
Archer, J., Dixon, L., & Graham-Kevan, N. (2012). Perpetrator programmes for partner violence: A rejoinder to Respect. Legal and Criminological Psychology, 17, 225–232. http://dx.doi.org/10.1111/j.2044-8333.2012.02061.x
Babcock, J. C., Green, C. E., & Robie, C. (2004). Does batterers’ treatment work? A meta-analytic review of domestic violence treatment. Clinical Psychology Review, 23, 1023–1053. http://dx.doi.org/10.1016/j.cpr.2002.07.001
Babcock, J. C., & La Taillade, J. (2000). Evaluating interventions for men who batter. In J. Vincent & E. Jouriles (Eds.), Domestic violence: Guidelines for research-informed practice (pp. 37–77). Philadelphia, PA: Jessica Kingsley.
Bates, E. A., & Graham-Kevan, N. (2016). Is the presence of control related to help-seeking behavior? A test of Johnson’s assumptions regarding sex-differences and the
PA8-1_Final_A1_003-046.indd 27 12/22/16 2:09 PM
28 Bates et al.
role of control in intimate partner violence. Partner Abuse, 7(1), 3–25. http://dx.doi .org/10.1891/1946-6560.7.1.3
Bates, E. A., Graham-Kevan, N., & Archer, J. (2014). Testing predictions from the male control theory of men’s partner violence. Aggressive Behavior, 40(1), 42–55. http://dx.doi.org/10.1002/ab.21499
Birkley, E. L., & Eckhardt, C. I. (2015). Anger, hostility, internalizing negative emotions, and intimate partner violence perpetration: A meta-analytic review. Clinical Psy-chology Review, 37, 40–56. http://dx.doi.org/10.1016/j.cpr.2015.01.002
Bloomfield, S., & Dixon, L. (2015). An outcome evaluation of the Integrated Domestic Abuse Programme (IDAP) and Community Domestic Violence Programme (CDVP). London, United Kingdom: National Offender Management Service.
Bologna, M. J., Waterman, C. K., & Dawson, L. J. (1987, July). Violence in gay male and lesbian relationships: Implications for practitioners and policy makers. Paper presented at the Third National Conference of Family Violence Researchers, Durham, NH.
Bowen, E., Gilchrist, E. A., & Beech, A. R. (2005). An examination of the impact of com-munity-based rehabilitation on the offending behaviour of male domestic violence of-fenders and the characteristics associated with recidivism. Legal and Criminological Psychology, 10, 189–209. http://dx.doi.org/10.1348/135532505X36778
Bullock, K., Sarre, S., Tarling, R., & Wilkinson, M. (2010). The delivery of domestic abuse programmes: An implementation study of the delivery of domestic abuse pro-grammes in probation areas and Her Majesty’s Prison Service. Retrieved from https://www.justice.gov.uk/downloads/publications/research-and-analysis/moj-research/ delivery-domestic-abuse-programmes.pdf
Charles, D., Whitaker, D. J., Le, B., Swahn, M., & DiClemente, R. J. (2011). Differences between perpetrators of bidirectional and unidirectional physical intimate partner violence. Partner Abuse, 2(3), 344–364. http://dx.doi.org/10.1891/1946-6560.2.3.344
Corvo, K., Dutton, D. G., & Chen, W. Y. (2008). Towards evidence-based practice with domestic violence perpetrators. Journal of Aggression, Maltreatment, and Trauma, 16(2), 111–130. http://dx.doi.org/10.1080/10926770801921246
Corvo, K., & Johnson, P. T. (2003). Vilification of the “batterer”: How blame shapes domestic violence policy and interventions. Aggression and Violent Behavior, 8, 259–281. http://dx.doi.org/10.1016/S1359-1789(01)00060-X
Daly, J., & Pelowski, S. (2000). Predictors of dropout among men who batter: A review of studies with implications for research and practice. Violence and Victims, 15, 137–160.
Debbonaire, T., & Todd, J. (2012). Respect response to Dixon et al. (2012) ‘Perpetra-tor program for partner violence: Are they based on ideology or evidence?’ Legal and Criminological Psychology, 17, 216–224. http://dx.doi.org/10.1111/j.2044-8333.2012.02051.x
Dixon, L., Archer, J., & Graham-Kevan, N. (2012). Perpetrator programs for partner vio-lence: Are they based on ideology or evidence? Legal and Criminological Psychology, 17, 196–215. http://dx.doi.org/0.1111/j.2044-8333.2011.02029.x
Dixon, L., & Graham-Kevan, N. (2011). Understanding the nature and etiology of inti-mate partner violence and implications for practice and policy. Clinical Psychology Review, 31, 1145–1155. http://dx.doi.org/10.1016/j.cpr.2011.07.001
PA8-1_Final_A1_003-046.indd 28 12/22/16 2:09 PM
U.K. Perpetrator Programs 29
Dobash, R. P., & Dobash, R. E. (1979). Violence against wives: A case against the patriarchy. New York, NY: The Free Press.
Dobash, R. P., Dobash, R. E., Cavanagh, K., & Lewis, R. (1998). Separate and in-tersecting realities: A comparison of men’s and women’s accounts of violence against women, Violence Against Women, 4(4), 382–414. http://dx.doi.org/10.1177/ 1077801298004004002
Dobash, R. P., Dobash, R. E., Cavanagh, K., & Lewis, R. (1999). A research evaluation of British programmes for violent men. Journal of Social Policy, 28, 205–233. http://dx.doi.org/10.1017/S0047279499005589
Dutton, D. G. (2006). The gender debate and the feminist paradigm. In Dutton, D. G. (Ed.), Rethinking domestic violence (pp. 109–129). Vancouver, Canada: UBC Press.
Dutton, D. G., & Corvo, K. (2006). Transforming a flawed policy: A call to revive psychol-ogy and science in domestic violence research and practice. Aggression and Violent Behavior, 11, 457–483.
Dutton, D. G., & Corvo, K. (2007). The Duluth model: A data-impervious paradigm and a failed strategy. Aggression and Violent Behavior, 12, 658–667. http://dx.doi .org/10.1016/j.avb.2007.03.002
Dutton, D. G., & Sonkin, D. J. (2003). Introduction: Perspectives on the treatment of intimate partner violence. In D. Dutton & D. J. Sonkin (Eds.), Intimate violence: Con-temporary treatment innovations (pp. 1–7). New York, NY: Howarth Maltreatment & Trauma Press.
Eadie, T., & Knight, C. (2002). Domestic violence programs: Reflections on the shift from independent to statutory provision. The Howard Journal of Criminal Justice, 41(2), 167–181. http://dx.doi.org/10.1111/1468-2311.00233
Eckhardt, C. I., Murphy, C. M., Whitaker, D. J., Sprunger, J., Dykstra, R., & Woodard, K. (2013). The effectiveness of intervention programs for perpetrators and victims of in-timate partner violence. Partner Abuse, 4(2), 196–231. http://dx.doi.org/10.1891/1946-6560.4.2.196
Ehrensaft, M. K. (2008). Intimate partner violence: Persistence of myths and implica-tions for intervention. Children and Youth Services Review, 30, 276–286.
Featherstone, B., & Fraser, C. (2012). Working with fathers around domestic violence: Contemporary debates. Child Abuse Review, 21, 255–263. http://dx.doi.org/10.1002/car.2221
Feder, L., & Wilson, D. B. (2005). A meta-analytic review of court-mandated batterer intervention programs: Can courts affect abusers’ behavior? Journal of Experimental Criminology, 1, 239–262. http://dx.doi.org/10.1007/s11292-005-1179-0
Felson, R. B. (2002). Violence & gender reexamined. Washington, DC: American Psycho-logical Association.
Felson, R. B. (2010). Academic apartheid: Segregation in the study of partner violence. Partner Abuse, 1, 61–81. http://dx.doi.org/10.1891/1946-6560.1.1.61
Felson, R. B., & Lane, K. J. (2010). Does violence involving women and intimate partners have a special etiology? Criminology, 48, 321–338. http://dx.doi.org/10.1111/j.1745-9125.2010.00186.x
Finkel, E. J. (2007). Impelling and inhibiting forces in the perpetration of inti-mate partner violence. Review of General Psychology, 11, 193–207. http://dx.doi .org/10.1037/1089-2680.11.2.193
PA8-1_Final_A1_003-046.indd 29 12/22/16 2:09 PM
30 Bates et al.
Finkel, E. J., DeWall, C. N., Slotter, E. B., Oaten, M., & Foshee, V. A. (2009). Self-regulatory failure and intimate partner violence perpetration. Journal of Personality and Social Psychology, 97, 483–499. http://dx.doi.org/10.1037/a0015433
Gondolf, E. W. (2002). Batterer intervention systems: Issues, outcomes and recommenda-tions. Thousand Oaks, CA: Sage.
Gondolf, E. W. (2007). Theoretical and research support for the Duluth Model: A reply to Dutton and Corvo. Aggression and Violent Behavior, 12(6), 644–657.
Gondolf, E. W., & Jones, A. S. (2001). The program effect of batterer programs in three cities. Violence and Victims, 16(6), 693–704.
Graham-Kevan, N. (2007). Domestic violence: Research and implications for batterer programmes in Europe. European Journal on Criminal Policy and Research, 13(3–4), 213–225. http://dx.doi.org/10.1007/s10610-007-9045-4
Graham-Kevan, N. (2009). The psychology of women’ partner violence: Characteristics and cautions. Journal of Aggression, Maltreatment & Trauma, 18, 587–603. http://dx.doi.org/10.1080/10926770903103131
Gruzinski, J. R., & Carrillo, T. P. (1988). Who completes batterers’ treatment groups? An empirical investigation. Journal of Family Violence, 3,141–150.
Hamberger, L. K., & Hastings, J. E. (1989). Counseling male spouse abusers: Character-istics of treatment completers and dropouts. Violence and Victims, 4, 275–286.
Hamilton, L., Koehler, J. A., & Lösel, F. A. (2012). Domestic violence perpetrator pro-grams in Europe, Part I: A survey of current practice. International Journal of Offender Therapy and Comparative Criminology, 57(10), 1189–1205. http://dx.doi .org/10.1177/0306624X12469506
Kelly, L., & Westmarland, N. (2015). Domestic violence perpetrator programmes: Steps towards change. Project Mirabal final report. London, United Kingdom: London Metropolitan University.
Kropp, P. R. (2009). Intimate partner violence risk assessment. In J. L. Ireland, C. A. Ireland, & P. Birch (Eds.), Violent and sexual offenders: Assessment, treatment and management. Portland, OR: Willan.
Langhinrichsen-Rohling, J., Misra, T., Selwyn, C., & Rohling, M. (2012). A systematic review of rates of bidirectional versus unidirectional intimate partner violence. Part-ner Abuse, 3, 199–230.
Lie, G., Schilit, R., Bush, J., Montagne, M., & Reyes, L. (1991). Lesbians in currently ag-gressive relationships: How frequently do they report aggressive past relationships? Violence and Victims, 6, 121–135.
Madoc-Jones, I., & Roscoe, K. (2010). Women’s safety service within the Integrated Domestic Abuse Programme: Perceptions of service users. Child and Family Social Work, 15, 155–164. http://dx.doi.org/10.1111/j.1365-2206.2009.00647.x
Marcus, R. F. (2012). Patterns of intimate partner violence in young adult couples: Non-violent, unilaterally violent, and mutually violent couples. Violence and Victims, 27(3), 299–314. http://dx.doi.org/10.1891/0886-6708.27.3.299
Ministry of Justice. (n.d.). Building Better Relationships (BBR): Information for sentencers. Retrieved from http://www.devon.gov.uk/building-better-relationships-information-for-sentencers.pdf
Ministry of Justice. (2014). Freedom of information request. Retrieved from: https://www .gov.uk/government/uploads/system/uploads/attachment_data/file/326267/meaning-accreditation-body.doc
PA8-1_Final_A1_003-046.indd 30 12/22/16 2:09 PM
U.K. Perpetrator Programs 31
Moffitt, T. E., Caspi, A., Rutter, M., & Silva, P. A. (2001). Sex differences in antisocial behaviour. Cambridge, United Kingdom: Cambridge University Press.
Morran, D. (2013). Desisting from domestic abuse: Influences, patterns and processes in the lives of formerly abusive men. The Howard Journal of Criminal Justice, 52(3), 306–320. http://dx.doi.org/10.1111/hojo.12016
O’Leary, K. D. (1999). Developmental and affective issues in assessing and treating partner aggression. Clinical Psychology, 6, 400–414. http://dx.doi.org/10.1093/clipsy.6.4.400
Paymar, M., & Barnes, G. (n.d.). Countering confusion about the Duluth model. Re-trieved from http://www.theduluthmodel.org/pdf/CounteringConfusion.pdf
Pence, E. (1999). Some thoughts on philosophy. In M. Shepherd & E. Pence (Eds.), Coor-dinating community responses to domestic violence: Lessons from Duluth and beyond (pp. 25–40). Thousand Oaks, CA: Sage.
Pence, E., & Paymar, M. (1993). Education groups for men who batter: The Duluth model. New York, NY: Springer Publishing.
Phillips, R., Kelly, L., & Westmarland, N. (2013). Domestic violence perpetrator pro-grammes: An historical overview. London, United Kingdom: London Metropolitan University.
Renzetti, C. M. (1992). Violent betrayal: Partner abuse in lesbian relationships. London, United Kingdom: Sage.
Respect. (2012). The Respect accreditation standard (2nd ed.). London, United Kingdom: Retrieved from http://www.respect.uk.net/data/files/Accreditation/respect__full_standard_july_12_v2_web.pdf
Stanley, N., Graham-Kevan, N., & Borthwich, R. (2012). Fathers and domestic violence: Building motivation for change through perpetrator programmes. Child Abuse Re-view, 21, 264–274. http://dx.doi.org/10.1002/car.2222
Thornton, A. J. V., Graham-Kevan, N.. & Archer, J. (2010). Adaptive and maladaptive personality traits as predictors of violent and nonviolent offending behavior in men and women. Aggressive Behavior, 36, 177–186. http://dx.doi.org/10.1002/ab.20340
Thornton, A. J. V., Graham-Kevan, N., & Archer, J. (2012). Prevalence of women’s violent and nonviolent offending behavior: A comparison of self-reports, victims’ reports, and third-party reports. Journal of Interpersonal Violence, 27, 1399–1427. http://dx.doi .org/10.1177/0886260511425789
Walker, S., & Richardson, D. R. (1998). Aggression strategies among older adults: De-livered but not seen. Aggression and Violent Behavior, 3, 287–294. http://dx.doi .org/10.1016/S1359-1789(96)00029-8
Correspondence regarding this article should be directed to Dr. Elizabeth A. Bates, University of Cumbria, Fusehill Street Campus, Carlisle, CA12HH, United Kingdom. E-mail: [email protected]
PA8-1_Final_A1_003-046.indd 31 12/22/16 2:09 PM
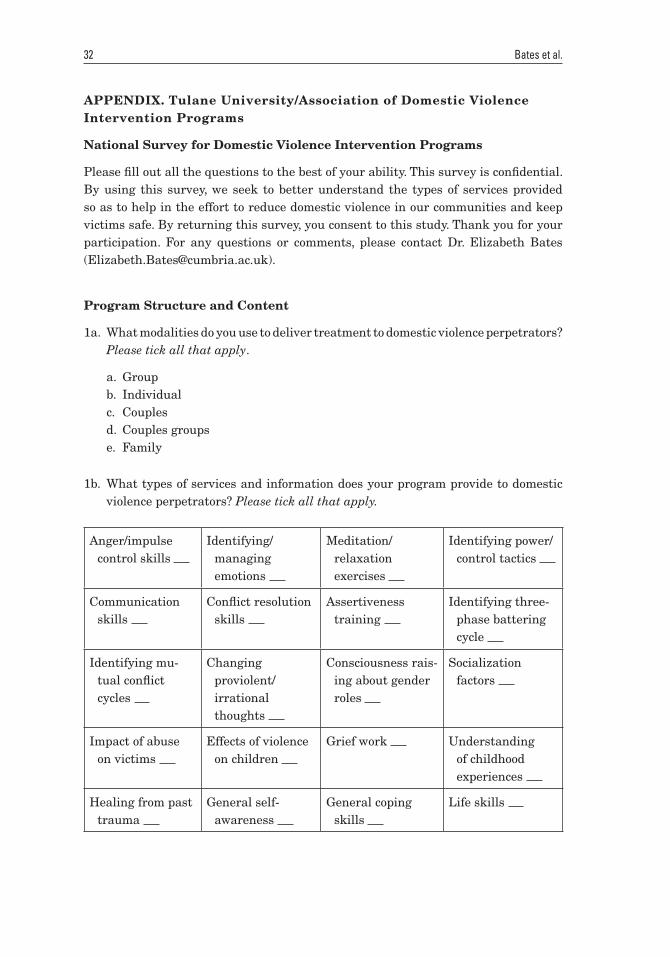
32 Bates et al.
APPENDIX. Tulane University/Association of Domestic Violence Intervention Programs
National Survey for Domestic Violence Intervention Programs
Please fill out all the questions to the best of your ability. This survey is confidential. By using this survey, we seek to better understand the types of services provided so as to help in the effort to reduce domestic violence in our communities and keep victims safe. By returning this survey, you consent to this study. Thank you for your participation. For any questions or comments, please contact Dr. Elizabeth Bates ([email protected]).
Program Structure and Content
1a. What modalities do you use to deliver treatment to domestic violence perpetrators? Please tick all that apply.
a. Groupb. Individualc. Couplesd. Couples groupse. Family
1b. What types of services and information does your program provide to domestic violence perpetrators? Please tick all that apply.
Anger/impulse control skills
Identifying/managing emotions
Meditation/relaxation exercises
Identifying power/control tactics
Communication skills
Conflict resolution skills
Assertiveness training
Identifying three-phase battering cycle
Identifying mu-tual conflict cycles
Changing proviolent/irrational thoughts
Consciousness rais-ing about gender roles
Socialization factors
Impact of abuse on victims
Effects of violence on children
Grief work Understanding of childhood experiences
Healing from past trauma
General self-awareness
General coping skills
Life skills
PA8-1_Final_A1_003-046.indd 32 12/22/16 2:09 PM
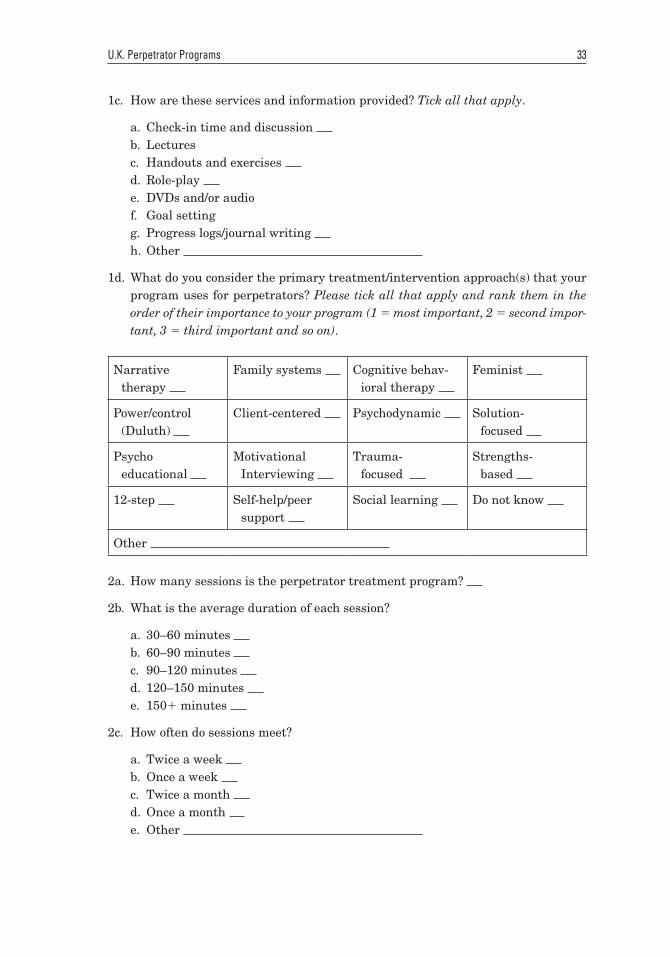
U.K. Perpetrator Programs 33
1c. How are these services and information provided? Tick all that apply.
a. Check-in time and discussion b. Lecturesc. Handouts and exercises d. Role-play e. DVDs and/or audiof. Goal settingg. Progress logs/journal writing h. Other
1d. What do you consider the primary treatment/intervention approach(s) that your program uses for perpetrators? Please tick all that apply and rank them in the order of their importance to your program (1 5 most important, 2 5 second impor-tant, 3 5 third important and so on).
Narrative therapy
Family systems Cognitive behav-ioral therapy
Feminist
Power/control (Duluth)
Client-centered Psychodynamic Solution-focused
Psycho educational
Motivational Interviewing
Trauma- focused
Strengths-based
12-step Self-help/peer support
Social learning Do not know
Other
2a. How many sessions is the perpetrator treatment program?
2b. What is the average duration of each session?
a. 30–60 minutes b. 60–90 minutes c. 90–120 minutes d. 120–150 minutes e. 1501 minutes
2c. How often do sessions meet?
a. Twice a week b. Once a week c. Twice a month d. Once a month e. Other
PA8-1_Final_A1_003-046.indd 33 12/22/16 2:09 PM
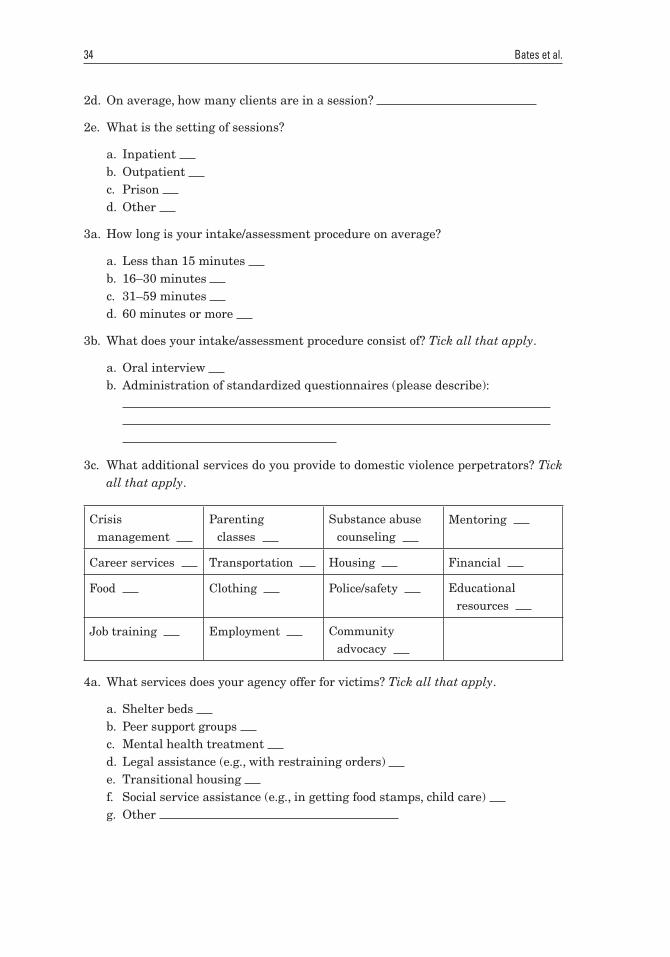
34 Bates et al.
2d. On average, how many clients are in a session?
2e. What is the setting of sessions?
a. Inpatient b. Outpatient c. Prison d. Other
3a. How long is your intake/assessment procedure on average?
a. Less than 15 minutes b. 16–30 minutes c. 31–59 minutes d. 60 minutes or more
3b. What does your intake/assessment procedure consist of? Tick all that apply.
a. Oral interview b. Administration of standardized questionnaires (please describe):
3c. What additional services do you provide to domestic violence perpetrators? Tick all that apply.
Crisis management
Parenting classes
Substance abuse counseling
Mentoring
Career services Transportation Housing Financial
Food Clothing Police/safety Educational resources
Job training Employment Community advocacy
4a. What services does your agency offer for victims? Tick all that apply.
a. Shelter beds b. Peer support groups c. Mental health treatment d. Legal assistance (e.g., with restraining orders) e. Transitional housing f. Social service assistance (e.g., in getting food stamps, child care) g. Other
PA8-1_Final_A1_003-046.indd 34 12/22/16 2:09 PM
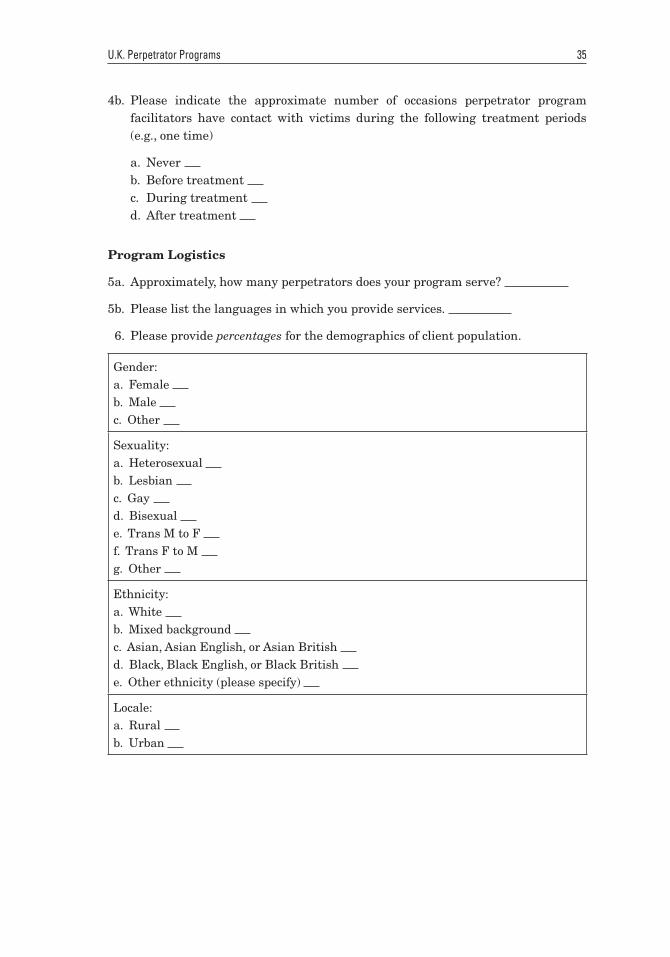
U.K. Perpetrator Programs 35
4b. Please indicate the approximate number of occasions perpetrator program facilitators have contact with victims during the following treatment periods (e.g., one time)
a. Never b. Before treatment c. During treatment d. After treatment
Program Logistics
5a. Approximately, how many perpetrators does your program serve?
5b. Please list the languages in which you provide services.
6. Please provide percentages for the demographics of client population.
Gender:a. Female b. Male c. Other
Sexuality:a. Heterosexual b. Lesbian c. Gay d. Bisexual e. Trans M to F f. Trans F to M g. Other
Ethnicity:a. White b. Mixed background c. Asian, Asian English, or Asian British d. Black, Black English, or Black British e. Other ethnicity (please specify)
Locale:a. Rural b. Urban
PA8-1_Final_A1_003-046.indd 35 12/22/16 2:09 PM
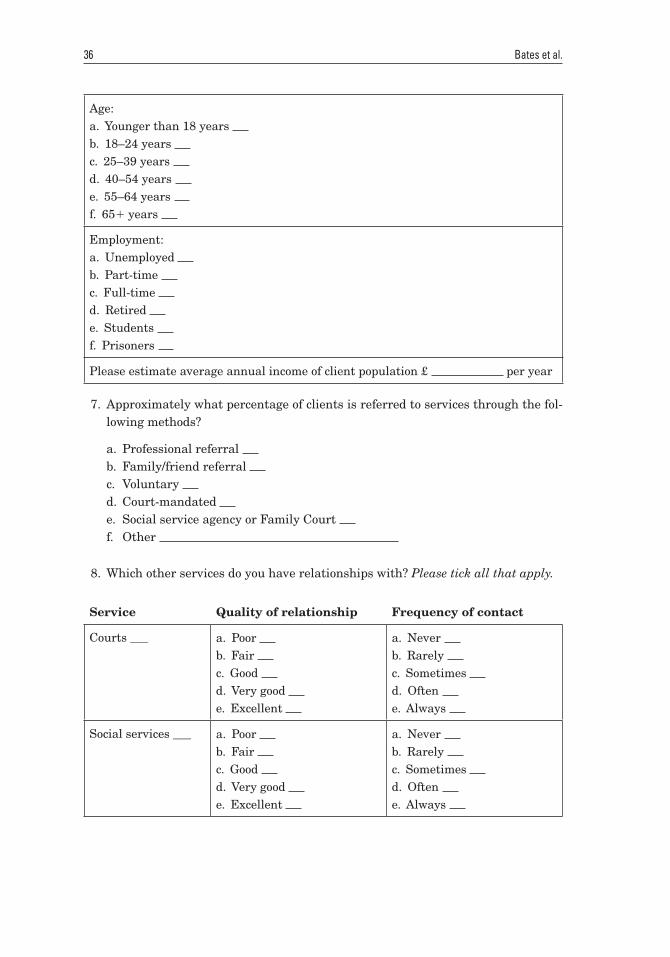
36 Bates et al.
Age:a. Younger than 18 years b. 18–24 years c. 25–39 years d. 40–54 years e. 55–64 years f. 651 years
Employment:a. Unemployed b. Part-time c. Full-time d. Retired e. Students f. Prisoners
Please estimate average annual income of client population £ per year
7. Approximately what percentage of clients is referred to services through the fol-lowing methods?
a. Professional referral b. Family/friend referral c. Voluntary d. Court-mandated e. Social service agency or Family Court f. Other
8. Which other services do you have relationships with? Please tick all that apply.
Service Quality of relationship Frequency of contact
Courts ___ a. Poor b. Fair c. Good d. Very good e. Excellent
a. Never b. Rarely c. Sometimes d. Often e. Always
Social services ___ a. Poor b. Fair c. Good d. Very good e. Excellent
a. Never b. Rarely c. Sometimes d. Often e. Always
PA8-1_Final_A1_003-046.indd 36 12/22/16 2:09 PM
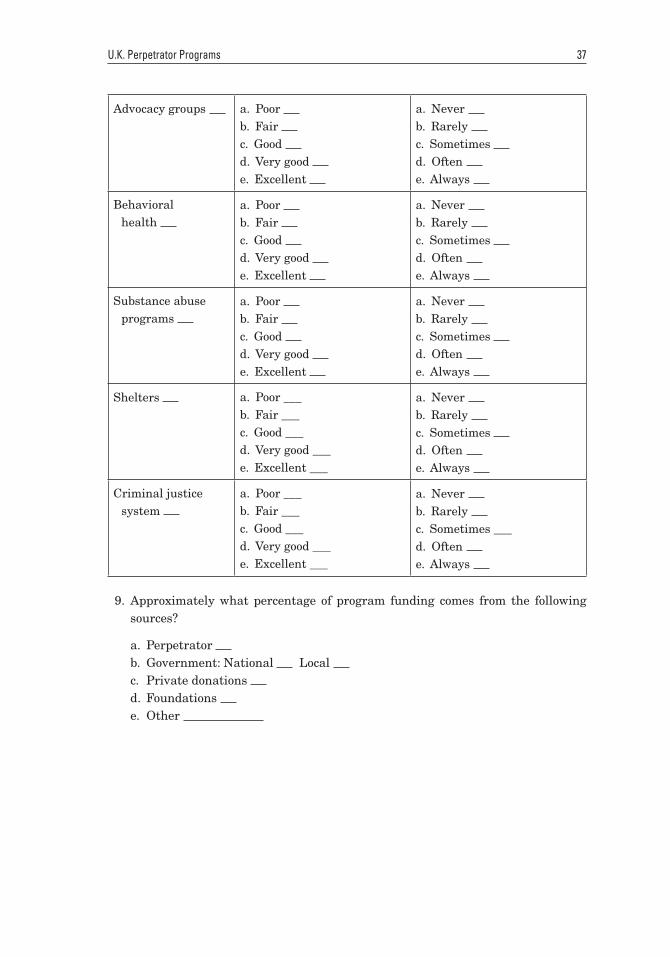
U.K. Perpetrator Programs 37
Advocacy groups a. Poor b. Fair c. Good d. Very good e. Excellent
a. Never b. Rarely c. Sometimes d. Often e. Always
Behavioral health
a. Poor b. Fair c. Good d. Very good e. Excellent
a. Never b. Rarely c. Sometimes d. Often e. Always
Substance abuse programs
a. Poor b. Fair c. Good d. Very good e. Excellent
a. Never b. Rarely c. Sometimes d. Often e. Always
Shelters a. Poor ___b. Fair ___c. Good ___d. Very good ___e. Excellent ___
a. Never b. Rarely c. Sometimes d. Often e. Always
Criminal justice system
a. Poor ___b. Fair ___c. Good ___d. Very good ___e. Excellent ___
a. Never b. Rarely c. Sometimes ___d. Often e. Always
9. Approximately what percentage of program funding comes from the following sources?
a. Perpetrator b. Government: National Local c. Private donations d. Foundations e. Other
PA8-1_Final_A1_003-046.indd 37 12/22/16 2:09 PM
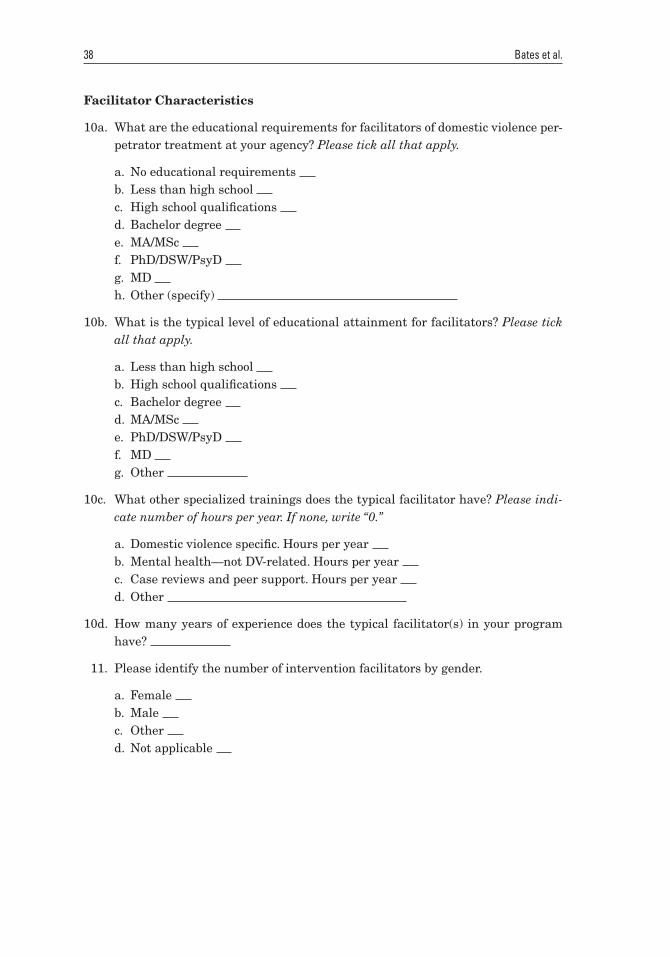
38 Bates et al.
Facilitator Characteristics
10a. What are the educational requirements for facilitators of domestic violence per-petrator treatment at your agency? Please tick all that apply.
a. No educational requirements b. Less than high school c. High school qualifications d. Bachelor degree e. MA/MSc f. PhD/DSW/PsyD g. MD h. Other (specify)
10b. What is the typical level of educational attainment for facilitators? Please tick all that apply.
a. Less than high school b. High school qualifications c. Bachelor degree d. MA/MSc e. PhD/DSW/PsyD f. MD g. Other
10c. What other specialized trainings does the typical facilitator have? Please indi-cate number of hours per year. If none, write “0.”
a. Domestic violence specific. Hours per year b. Mental health—not DV-related. Hours per year c. Case reviews and peer support. Hours per year d. Other
10d. How many years of experience does the typical facilitator(s) in your program have?
11. Please identify the number of intervention facilitators by gender.
a. Female b. Male c. Other d. Not applicable
PA8-1_Final_A1_003-046.indd 38 12/22/16 2:09 PM
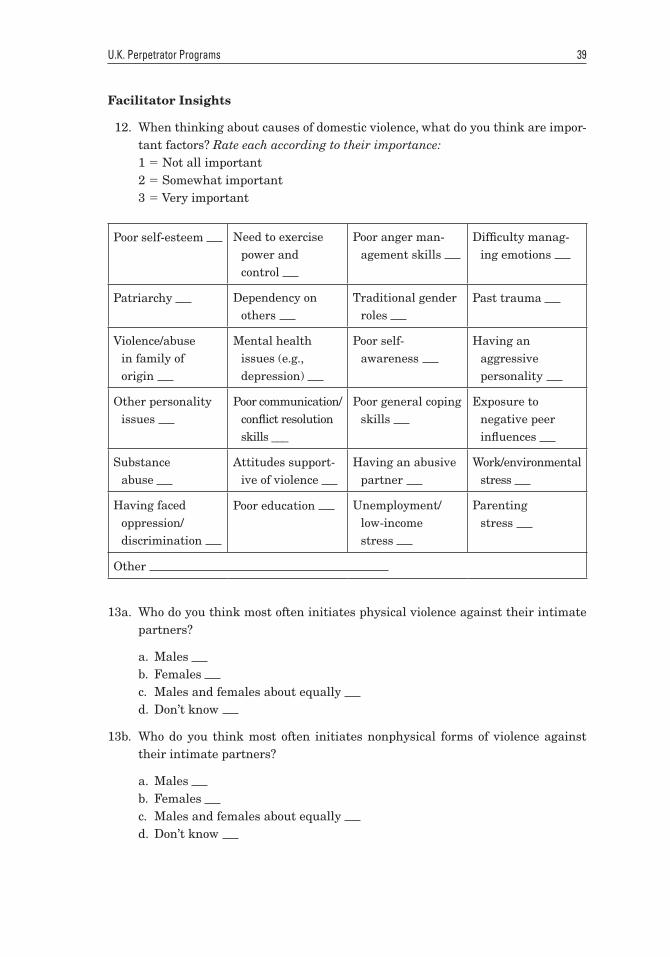
U.K. Perpetrator Programs 39
Facilitator Insights
12. When thinking about causes of domestic violence, what do you think are impor-tant factors? Rate each according to their importance:1 5 Not all important2 5 Somewhat important3 5 Very important
Poor self-esteem Need to exercise power and control
Poor anger man-agement skills
Difficulty manag-ing emotions
Patriarchy Dependency on others
Traditional gender roles
Past trauma
Violence/abuse in family of origin
Mental health issues (e.g., depression)
Poor self-awareness
Having an aggressive personality
Other personality issues
Poor communication/conflict resolution skills ___
Poor general coping skills
Exposure to negative peer influences
Substance abuse
Attitudes support-ive of violence
Having an abusive partner
Work/environmental stress
Having faced oppression/discrimination
Poor education Unemployment/low-income stress
Parenting stress
Other
13a. Who do you think most often initiates physical violence against their intimate partners?
a. Males b. Females c. Males and females about equally d. Don’t know
13b. Who do you think most often initiates nonphysical forms of violence against their intimate partners?
a. Males b. Females c. Males and females about equally d. Don’t know
PA8-1_Final_A1_003-046.indd 39 12/22/16 2:09 PM
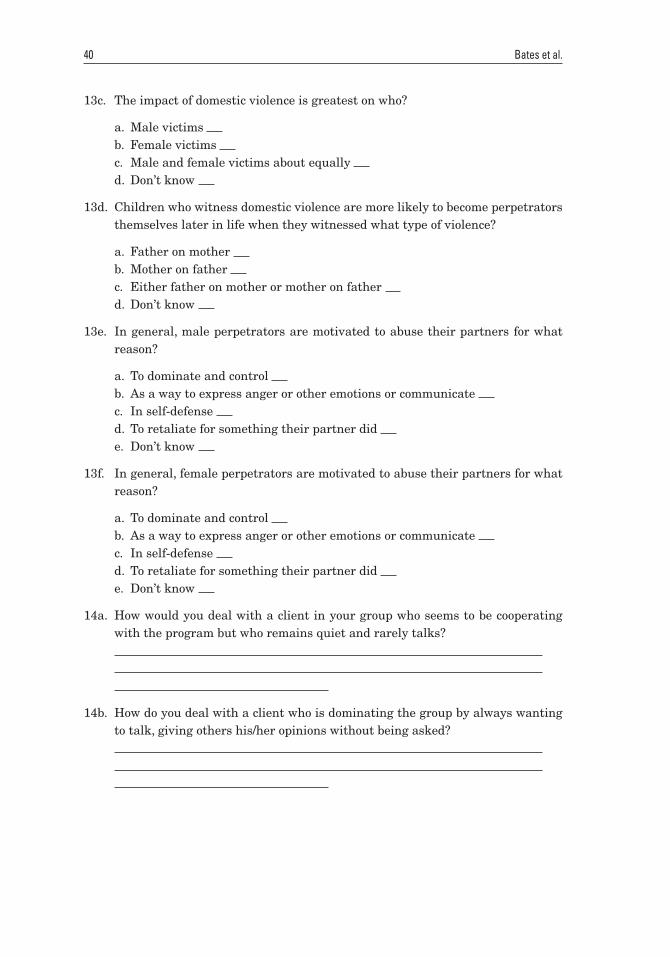
40 Bates et al.
13c. The impact of domestic violence is greatest on who?
a. Male victims b. Female victims c. Male and female victims about equally d. Don’t know
13d. Children who witness domestic violence are more likely to become perpetrators themselves later in life when they witnessed what type of violence?
a. Father on mother b. Mother on father c. Either father on mother or mother on father d. Don’t know
13e. In general, male perpetrators are motivated to abuse their partners for what reason?
a. To dominate and control b. As a way to express anger or other emotions or communicate c. In self-defense d. To retaliate for something their partner did e. Don’t know
13f. In general, female perpetrators are motivated to abuse their partners for what reason?
a. To dominate and control b. As a way to express anger or other emotions or communicate c. In self-defense d. To retaliate for something their partner did e. Don’t know
14a. How would you deal with a client in your group who seems to be cooperating with the program but who remains quiet and rarely talks?
14b. How do you deal with a client who is dominating the group by always wanting to talk, giving others his/her opinions without being asked?
PA8-1_Final_A1_003-046.indd 40 12/22/16 2:09 PM
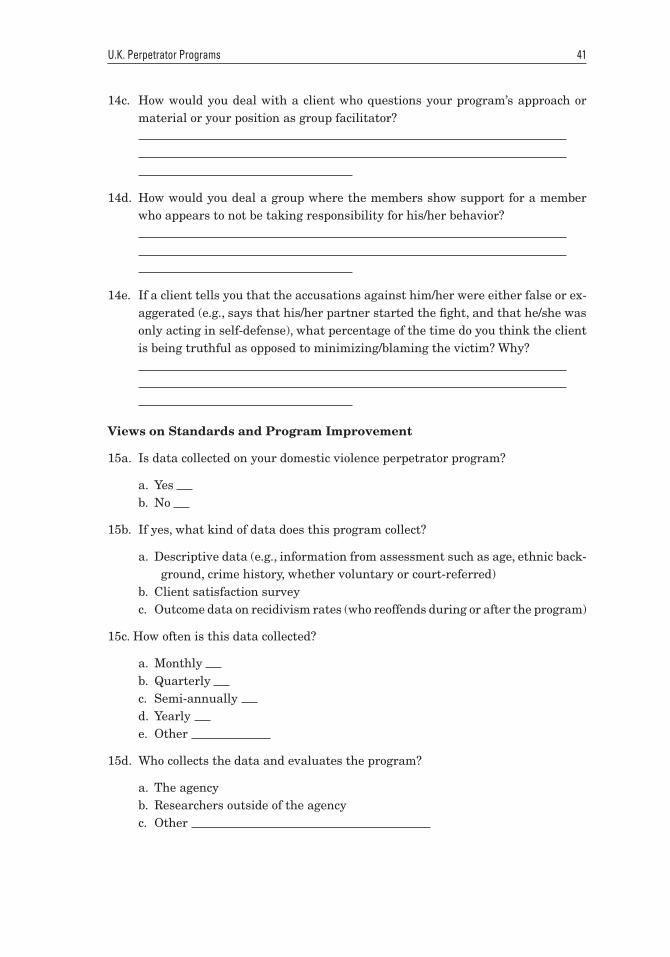
U.K. Perpetrator Programs 41
14c. How would you deal with a client who questions your program’s approach or material or your position as group facilitator?
14d. How would you deal a group where the members show support for a member who appears to not be taking responsibility for his/her behavior?
14e. If a client tells you that the accusations against him/her were either false or ex-aggerated (e.g., says that his/her partner started the fight, and that he/she was only acting in self-defense), what percentage of the time do you think the client is being truthful as opposed to minimizing/blaming the victim? Why?
Views on Standards and Program Improvement
15a. Is data collected on your domestic violence perpetrator program?
a. Yes b. No
15b. If yes, what kind of data does this program collect?
a. Descriptive data (e.g., information from assessment such as age, ethnic back-ground, crime history, whether voluntary or court-referred)
b. Client satisfaction surveyc. Outcome data on recidivism rates (who reoffends during or after the program)
15c. How often is this data collected?
a. Monthly b. Quarterly c. Semi-annually d. Yearly e. Other
15d. Who collects the data and evaluates the program?
a. The agencyb. Researchers outside of the agencyc. Other
PA8-1_Final_A1_003-046.indd 41 12/22/16 2:09 PM
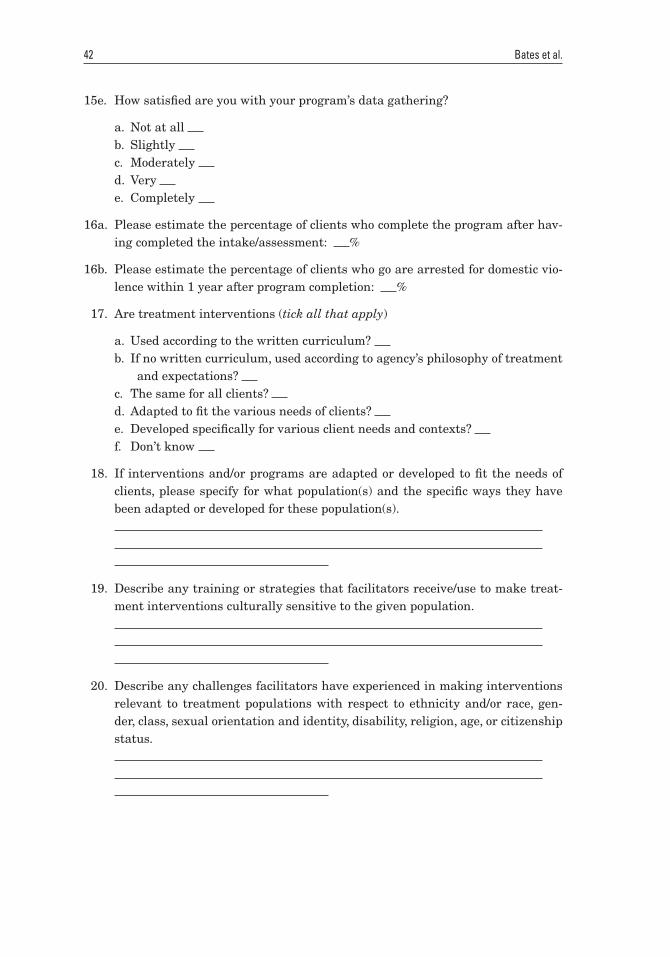
42 Bates et al.
15e. How satisfied are you with your program’s data gathering?
a. Not at all b. Slightly c. Moderately d. Very e. Completely
16a. Please estimate the percentage of clients who complete the program after hav-ing completed the intake/assessment: %
16b. Please estimate the percentage of clients who go are arrested for domestic vio-lence within 1 year after program completion: %
17. Are treatment interventions (tick all that apply)
a. Used according to the written curriculum? b. If no written curriculum, used according to agency’s philosophy of treatment
and expectations? c. The same for all clients? d. Adapted to fit the various needs of clients? e. Developed specifically for various client needs and contexts? f. Don’t know
18. If interventions and/or programs are adapted or developed to fit the needs of clients, please specify for what population(s) and the specific ways they have been adapted or developed for these population(s).
19. Describe any training or strategies that facilitators receive/use to make treat-ment interventions culturally sensitive to the given population.
20. Describe any challenges facilitators have experienced in making interventions relevant to treatment populations with respect to ethnicity and/or race, gen-der, class, sexual orientation and identity, disability, religion, age, or citizenship status.
PA8-1_Final_A1_003-046.indd 42 12/22/16 2:09 PM
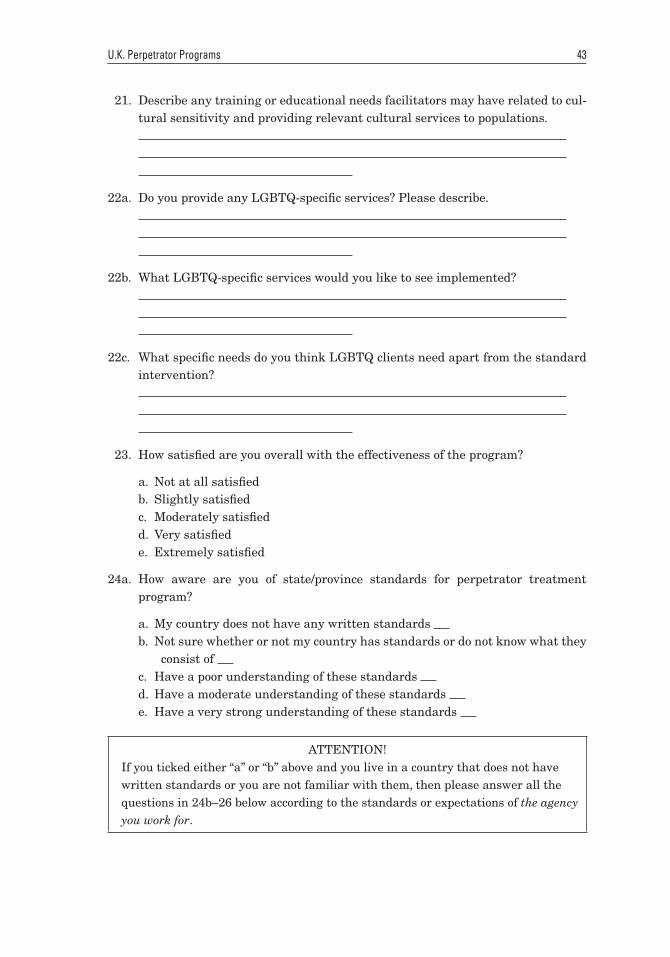
U.K. Perpetrator Programs 43
21. Describe any training or educational needs facilitators may have related to cul-tural sensitivity and providing relevant cultural services to populations.
22a. Do you provide any LGBTQ-specific services? Please describe.
22b. What LGBTQ-specific services would you like to see implemented?
22c. What specific needs do you think LGBTQ clients need apart from the standard intervention?
23. How satisfied are you overall with the effectiveness of the program?
a. Not at all satisfiedb. Slightly satisfiedc. Moderately satisfiedd. Very satisfiede. Extremely satisfied
24a. How aware are you of state/province standards for perpetrator treatment program?
a. My country does not have any written standards b. Not sure whether or not my country has standards or do not know what they
consist of c. Have a poor understanding of these standards d. Have a moderate understanding of these standards e. Have a very strong understanding of these standards
ATTENTION!If you ticked either “a” or “b” above and you live in a country that does not have written standards or you are not familiar with them, then please answer all the questions in 24b–26 below according to the standards or expectations of the agency you work for.
PA8-1_Final_A1_003-046.indd 43 12/22/16 2:09 PM
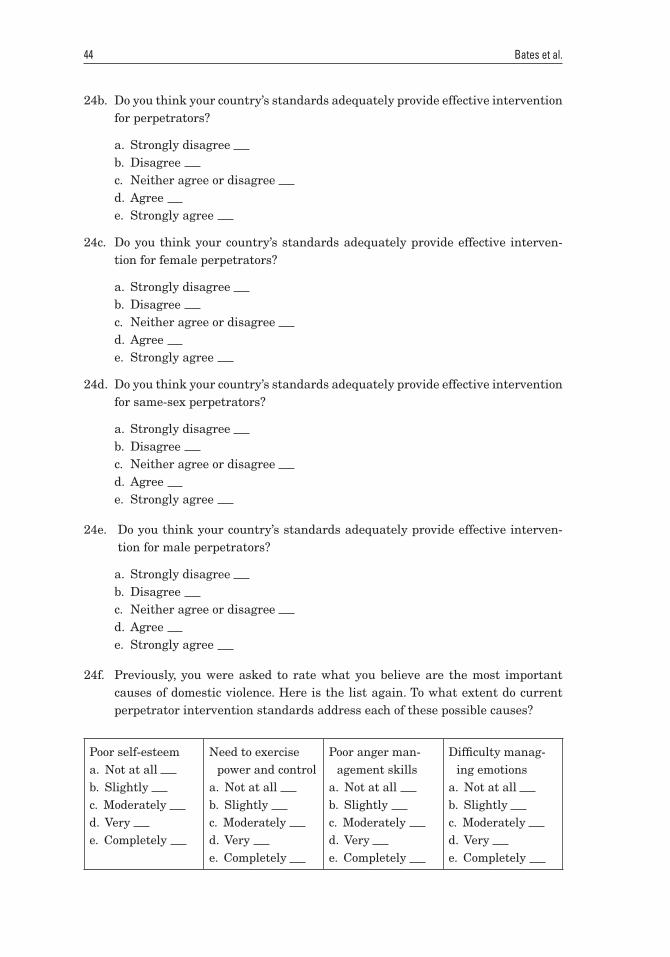
44 Bates et al.
24b. Do you think your country’s standards adequately provide effective intervention for perpetrators?
a. Strongly disagree b. Disagree c. Neither agree or disagree d. Agree e. Strongly agree
24c. Do you think your country’s standards adequately provide effective interven-tion for female perpetrators?
a. Strongly disagree b. Disagree c. Neither agree or disagree d. Agree e. Strongly agree
24d. Do you think your country’s standards adequately provide effective intervention for same-sex perpetrators?
a. Strongly disagree b. Disagree c. Neither agree or disagree d. Agree e. Strongly agree
24e. Do you think your country’s standards adequately provide effective interven-tion for male perpetrators?
a. Strongly disagree b. Disagree c. Neither agree or disagree d. Agree e. Strongly agree
24f. Previously, you were asked to rate what you believe are the most important causes of domestic violence. Here is the list again. To what extent do current perpetrator intervention standards address each of these possible causes?
Poor self-esteema. Not at all b. Slightly c. Moderately d. Very e. Completely
Need to exercise power and control
a. Not at all b. Slightly c. Moderately d. Very e. Completely
Poor anger man-agement skills
a. Not at all b. Slightly c. Moderately d. Very e. Completely
Difficulty manag-ing emotions
a. Not at all b. Slightly c. Moderately d. Very e. Completely
PA8-1_Final_A1_003-046.indd 44 12/22/16 2:09 PM
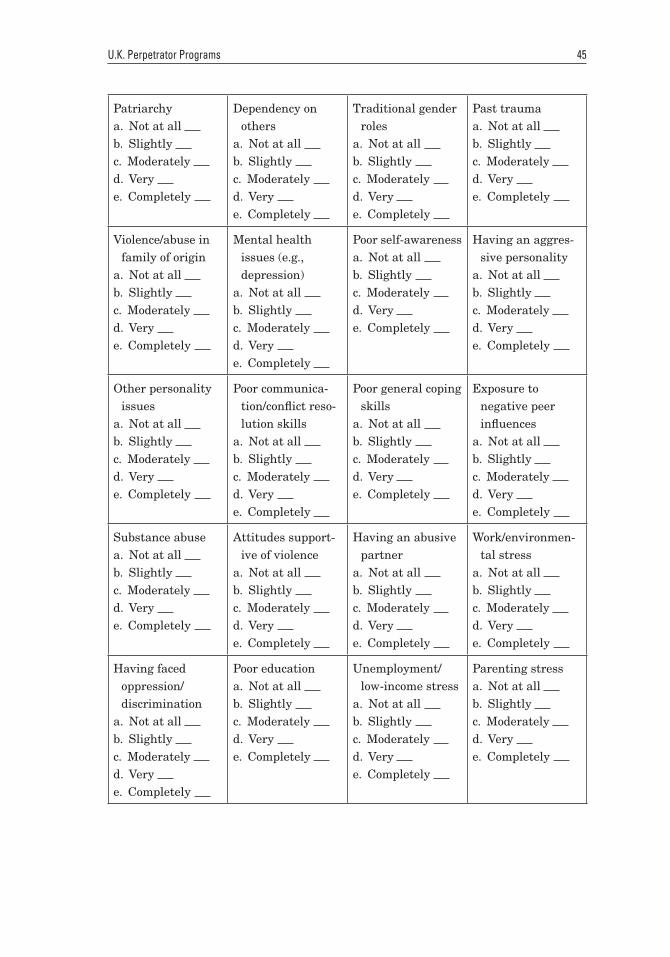
U.K. Perpetrator Programs 45
Patriarchya. Not at all b. Slightly c. Moderately d. Very e. Completely
Dependency on others
a. Not at all b. Slightly c. Moderately d. Very e. Completely
Traditional gender roles
a. Not at all b. Slightly c. Moderately d. Very e. Completely
Past traumaa. Not at all b. Slightly c. Moderately d. Very e. Completely
Violence/abuse in family of origin
a. Not at all b. Slightly c. Moderately d. Very e. Completely
Mental health issues (e.g., depression)
a. Not at all b. Slightly c. Moderately d. Very e. Completely
Poor self-awarenessa. Not at all b. Slightly c. Moderately d. Very e. Completely
Having an aggres-sive personality
a. Not at all b. Slightly c. Moderately d. Very e. Completely
Other personality issues
a. Not at all b. Slightly c. Moderately d. Very e. Completely
Poor communica-tion/conflict reso-lution skills
a. Not at all b. Slightly c. Moderately d. Very e. Completely
Poor general coping skills
a. Not at all b. Slightly c. Moderately d. Very e. Completely
Exposure to negative peer influences
a. Not at all b. Slightly c. Moderately d. Very e. Completely
Substance abusea. Not at all b. Slightly c. Moderately d. Very e. Completely
Attitudes support-ive of violence
a. Not at all b. Slightly c. Moderately d. Very e. Completely
Having an abusive partner
a. Not at all b. Slightly c. Moderately d. Very e. Completely
Work/environmen-tal stress
a. Not at all b. Slightly c. Moderately d. Very e. Completely
Having faced oppression/discrimination
a. Not at all b. Slightly c. Moderately d. Very e. Completely
Poor educationa. Not at all b. Slightly c. Moderately d. Very e. Completely
Unemployment/low-income stress
a. Not at all b. Slightly c. Moderately d. Very e. Completely
Parenting stressa. Not at all b. Slightly c. Moderately d. Very e. Completely
PA8-1_Final_A1_003-046.indd 45 12/22/16 2:09 PM
46 Bates et al.
24g. What do you think is most effective about your country’s current standards? (If you do not know, write “do not know.”)
24h. What do you think is least effective about your country’s current standards?
24i. What changes do you think should be made to your country’s standards?
25a. How often do you faithfully follow your country’s standards?
a. Never b. Rarely c. Sometimes d. Often e. Always
25b. How often do you supplement your country’s standards?
a. Never b. Rarely c. Sometimes d. Often e. Always
25c. Please describe how you supplement your country’s standards.
26. Describe any ways this intervention program could be improved.
PA8-1_Final_A1_003-046.indd 46 12/22/16 2:09 PM