Embed Size (px)
Citation preview
Information systems, referral criteria and patient pathways subgroup – January 2011 1
A review and discussion of psychological therapies and interventions delivered within stepped care service models Anne Joice, Laura Freeman, Laura Toplis, Geraldine Bienkowski Full section 1 report with references and appendixe s NHS Education for Scotland January 2010
Information systems, referral criteria and patient pathways subgroup – January 2011 2
Acknowledgements We are grateful for the assistance of Jacqueline Wilson, Helen Wilson, and Jennifer Davies in proof-reading and commenting on drafts of this document. We would also like to extend our thanks to Nadia Hanif and Fiona Hart for their support in subject searching and reviewing the literature.
Information systems, referral criteria and patient pathways subgroup – January 2011 3
Contents Page
Introduction 4
Aim of review 4
Scope of review 4
Method 4
Results 6
Discussion - Service Delivery systems / organisatio n 7
1.1 What are the features of stepped care service models? 7
1.2 What is the evidence for the service models in terms of clinical effectiveness, efficiency and clinical outcomes for people?
8
1.3 What clinical outcomes do people accessing low-intensity interventions obtain? 10
1.4 How are people matched to the appropriate tier? 12
1.5 What drivers (restrictions, checks and balances) are in place to encourage people to engage at each level across the tiers?
13
1.6 Do socio-economically deprived populations access and use services within each of the service models?
14
1.7 What systems are used to ensure the service is self-correcting and people matched to the incorrect tier are reallocated?
15
1.8 Are the service delivery models economical? 15
1.9 What impact do the various organisational service models have on the capacity of the system?
17
1.10 Summary of organisational service models 18
Implications for service delivery 19
References 20
Appendices 25
1. Models of stepped care 25
2. NICE Guideline for the Management of Depression 26
3. Traditional stepped care model (Arthur, 2005) 27
4. Layered care (Arthur, 2005) 28
5. Glasgow STEPs Primary Care Mental Health Team Stepped Care (White et al., 2008) 29
6. The Matrix (Scottish Government, 2008) 30
Information systems, referral criteria and patient pathways subgroup – January 2011 4
Introduction The Information Systems, Referral Criteria and Patient Pathways sub-group has been set up by the Scottish Government Mental Health Division to carry out scoping work around setting a Psychological Therapies access target. As part of this work NHS Education Scotland (NES) will be carrying out a review of current literature and services delivering psychological therapies / interventions to answer key questions posed by the sub-group. This review compliments the work currently being carried out by the Information Service Division (ISD) and the Mental Health Collaborative.
Aim of the review The aim of the review is to provide up-to-date information on psychological therapies and interventions delivered within effective stepped care service structures, clinical assessments, staff skills and competences. It is hoped that this will aid decision making and guide the development of efficient and effective stepped care psychological therapies / interventions.
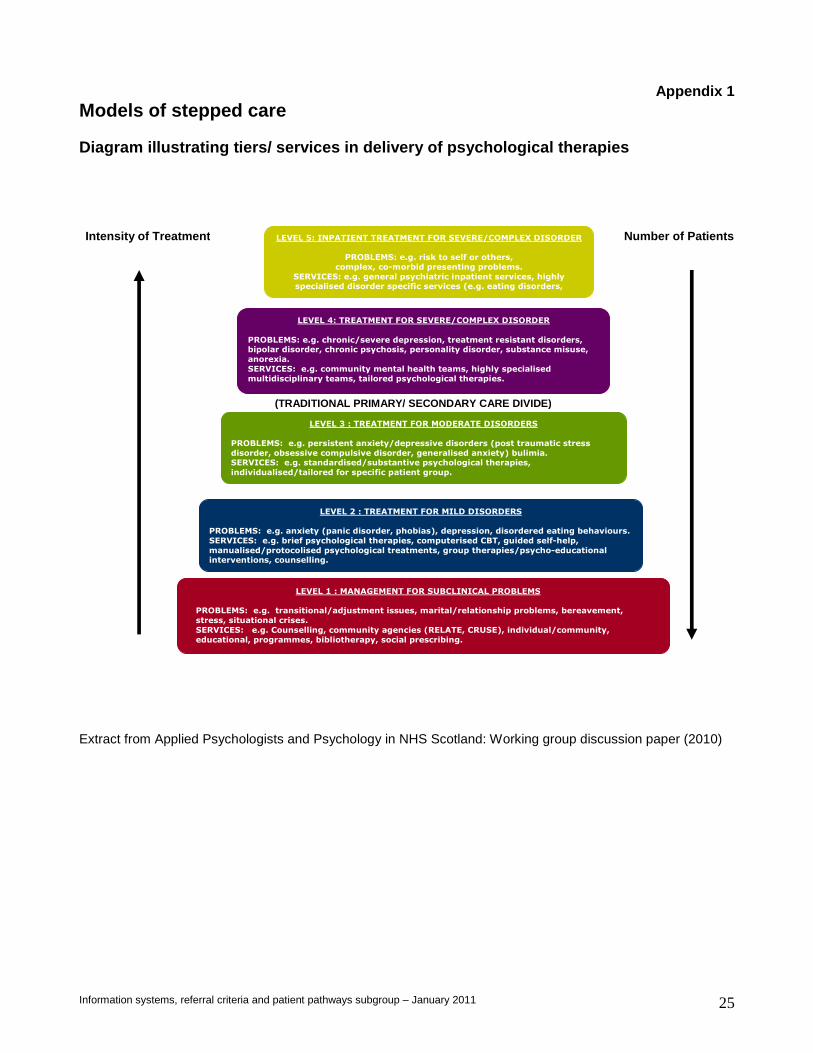
Scope of the review The review will focus on organisational structures and therapies / interventions delivered across the ‘whole’ adult mental health system; including older adults, addiction and forensic services. This will include services targeting mild (level 2), moderate (level 3), severe and complex (level 4) mental health problems and in-patient treatment for severe and complex mental health problems (level 5) (see Appendix 1).
Method A broad based exploratory search within mental health was carried out OvidSP between March – July 2010. The following databases were searched using the MeSH terms Section 1 = ‘stepped care’, ‘matched care’ and ‘mental health’.
• Journals Ovid Full text March 16 2010
• Ovid Medline 2006 – March 2010
• All EBM reviews – Cochrane, DSR, ACP Journal Club, DARE, CCTR, CMR, HTA, and NHSEED
• Embase 1996 – March 2010
• PsycINFO 2002 – March 2010 The review was carried out in three stages and aimed to answer specific questions agreed by the sub-group and the NHS Education Scotland (NES) Psychological Intervention Team.
Information systems, referral criteria and patient pathways subgroup – January 2011 5
Key questions on service delivery systems / organis ation
A range of service models are documented that provide access to psychological therapies / interventions, including; graduated access, the consultation – liaison model, the attached professional model, stepped care, stratified (matched care), case management, and collaborative care (National Collaborating Centre for Mental Health, 2009). This review will define and consider the key features of stepped care, matched care and collaborative care service models and address the following questions:
• What are the features of stepped care service models?
• What is the evidence for the service models in terms of clinical effectiveness, efficiency and clinical outcomes for people?
• What clinical outcomes do people accessing low-intensity interventions obtain?
• How are people matched to the appropriate tier?
• What drivers are in place to encourage people to engage at each level across the tiers?
• What systems are used to ensure the system is self correcting and people matched to the incorrect tier are reallocated?
• Do socio-economically deprived populations access and use services within each of the service models?
• Are the service delivery models economical?
• What impact do the various organisational service models have on the capacity of the system?
Information systems, referral criteria and patient pathways subgroup – January 2011 6
Results from the literature review
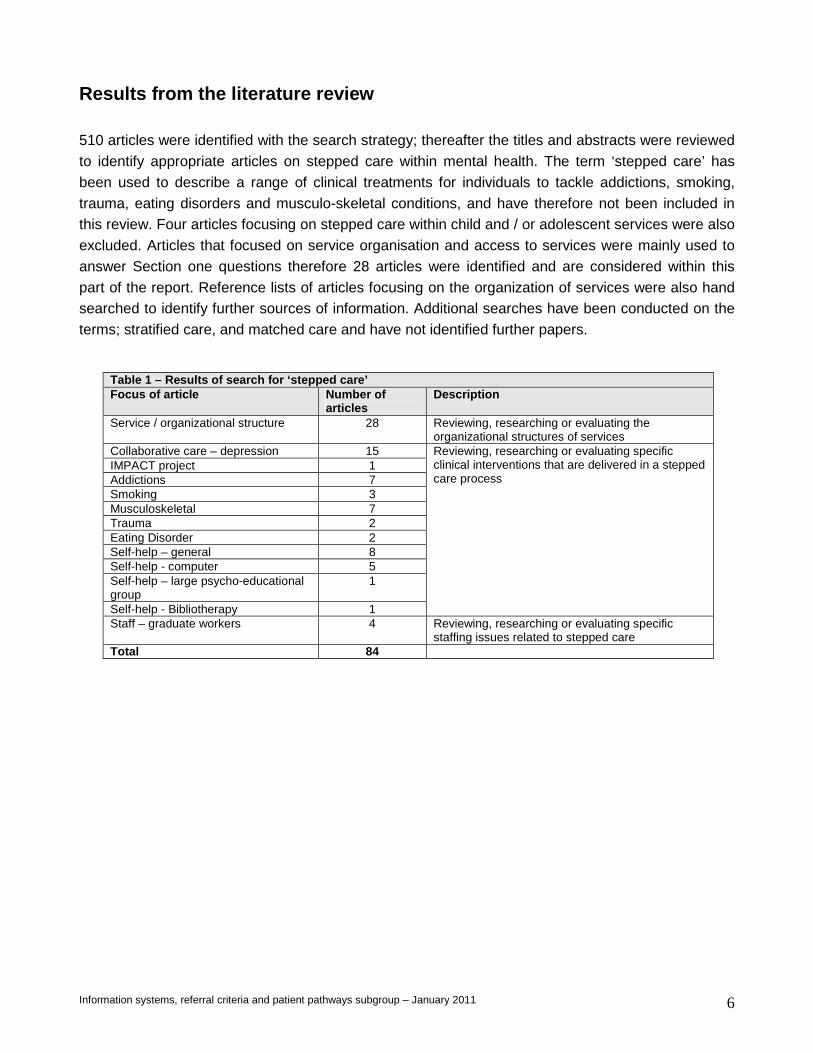
510 articles were identified with the search strategy; thereafter the titles and abstracts were reviewed to identify appropriate articles on stepped care within mental health. The term ‘stepped care’ has been used to describe a range of clinical treatments for individuals to tackle addictions, smoking, trauma, eating disorders and musculo-skeletal conditions, and have therefore not been included in this review. Four articles focusing on stepped care within child and / or adolescent services were also excluded. Articles that focused on service organisation and access to services were mainly used to answer Section one questions therefore 28 articles were identified and are considered within this part of the report. Reference lists of articles focusing on the organization of services were also hand searched to identify further sources of information. Additional searches have been conducted on the terms; stratified care, and matched care and have not identified further papers.
Table 1 – Results of search for ‘stepped care’ Focus of article Number of
articles Description
Service / organizational structure 28 Reviewing, researching or evaluating the organizational structures of services
Collaborative care – depression 15 IMPACT project 1 Addictions 7 Smoking 3 Musculoskeletal 7 Trauma 2 Eating Disorder 2 Self-help – general 8 Self-help - computer 5 Self-help – large psycho-educational group
1
Self-help - Bibliotherapy 1
Reviewing, researching or evaluating specific clinical interventions that are delivered in a stepped care process
Staff – graduate workers 4 Reviewing, researching or evaluating specific staffing issues related to stepped care
Total 84
Information systems, referral criteria and patient pathways subgroup – January 2011 7
Discussion - Service delivery systems / organisatio ns 1.1 What are the features of stepped care service m odels? Stepped care is recommended in international clinical guidelines and ‘attempts to maximise the effectiveness and efficiency of decisions about allocation of resources in therapy’ (Hagga, 2000). A variety of different organisational service delivery models are described within the literature and are called ‘stepped care’ (see Table 1). There are five fundamental features of stepped care. Firstly, stepped care enhances the capacity of mental health services and increases access to evidence based psychological interventions. Access to services should include availability, utilization, effectiveness, equity (Gulliford et al., 2001), efficiency and patient-centredness (Richards, 2010). Central to this is the notion that people should not have to ‘wait’ for a psychological service (White, 2010). Secondly, the least restrictive treatment available, that will provide significant health gain, should be offered first (Hagga, 2000: Bower & Gilbody, 2005). ‘Least restrictive’ refers to the impact on the patient’s cost and personal inconvenience as well as the amount of specialist therapist time required and treatment intensity. Davison (2000, p.584) states that ‘clinicians should intrude as little as possible into the lives of their patients while at the same time providing the maximum clinical benefit’. This minimises the likelihood of services deconstructing ‘normal’ social coping responses within the community. Thirdly, the system should be ‘self-correcting’, provide feedback and allow for the intensity of the interventions to be adjusted. An individual’s progress within the system should be monitored to ensure the treatment is achieving significant health gain. Typically if a positive outcome is not obtained with the first intervention or therapy, the person is ‘stepped up’ to a more extensive and costly treatment. Equally, stepping down is relevant. Therefore, self-correction can be applied at two stages; people may be assessed and allocated to different treatments; or subsequent reviews of patient progress may step people up to another more intense treatment (Richards, 2010). This monitoring is essential to ensure that the treatment being implemented is worth continuing, is cost effective, and that the effort required is relative to the impact it is having on the problem for which the person has sought assistance. Fourthly, Bower & Gilbody (2005) recommend that stepped care requires a range of treatments of differing intensity to be available. There should be consensus as to what treatments are effective and available (Davison, 2000). Bower & Gilbody (2005) describe ‘four qualitatively different steps’ being; pure self-help (no therapist input beyond treatment), guided self-help and group treatment (therapist input around 1 – 2 hours per patient), brief individual therapy (therapist input around 6 hours per patient), and longer-term individual therapy (therapist input around 16 hours per patient). Further to this White et al. (2008) recommend that a tier within a stepped care model should engage and work
Information systems, referral criteria and patient pathways subgroup – January 2011 8
with populations and communities. A lack of available ‘steps’ may reduce the likelihood of engagement at each level within a stepped care model. Lastly, stepped care puts in place systematic mechanisms such as guidelines, rank ordering or hierarchies of interventions, and subjective and objective measures of patient outcome, to feed into clinical decision making (Richards, 2010; Arthur, 2005) or to agree referral criteria across services to maximise efficiency. Interventions should be ‘rank ordered’ in terms of cost and intrusiveness (Davison, 2000). Several critiques are made of the organization of services within ‘stepped care’. Arthur (2005) presents a summary of these concerns;
“…when should a therapist switch from one step to the next, what are the criteria, does failure at a lower level of treatment discourage the patients from subsequent treatment, and does repeatedly changing treatment lead to patients ‘demoralised by treatment failure’ and ‘getting worse from ineffective treatments” (Arthur, 2005; p. 105).
Arthur offers ‘layered care’ as a ‘modified’ stepped care model (see Appendices 3 and 4). This model makes available multiple layers of treatment for each patient. The principle of offering the least intrusive and costly interventions first is maintained but there is still access to the higher layers. More recently Lovell et al. (2008) raise questions about the possibility that the stepped care model recommended in the National Institute for Health and Clinical Excellence (NICE) guidelines for depression may be making ‘unrealistic assumptions about the proportion of patients’ who can benefit from low intensity interventions. They recommend the adoption of a ‘stratified model, with greater attention to identifying patients who are likely to respond to these treatments, and those who require alternatives’.
1.2 What is the evidence for the service models in terms of clinical effectiveness, efficiency and clinical outcomes for people? Clinical effectiveness of psychological therapies is widely reported (National Collaborating Centre for Mental Health, 2009; NICE, 2004; Department of Health, 2001; Roth & Fonaghy, 1996). In addition to this, poor access to psychological therapy services has been reported (Richards, Lovell, McEvoy, 2003; Lovell & Richards, 2000). Service features which support the effective delivery of psychological therapies include adherence to clinical guidelines, emphasis on training, availability of supervision, and focus on outcomes. Effective implementation requires intervention at all levels (Grimshaw et al., 2004; Stein & Lambert, 1995; Cape & Barkham, 2002; Hannan et al., 2005). The Increasing Access to Psychological Services (IAPT) programme in England was developed in 2006 to test the effectiveness of providing significant increases in evidence-based psychological
Information systems, referral criteria and patient pathways subgroup – January 2011 9
therapy services to people with the common mental health problems of depression and anxiety disorders. Typically stepped-care service models have been adopted incorporating high volume, low-intensity psychological interventions (guided CBT / self-help) and high intensity CBT. Favourable outcomes for stepped care are reported in increasing the access to psychological therapies and reducing symptoms for the people accessing the services (Clark et al., 2009, Van’t Veer-Tazelaar et al., 2009). Van’t Veer-Tazelaar et al. (2009) found that a stepped-care programme designed to reduce the incidence of major depression and anxiety disorder, offered to elderly people with sub-threshold depressive or anxiety symptoms, was more effective than usual care provided. The intervention reduced the odds of developing a depressive illness or anxiety disorder by 57.9% (OR, 0.42%; 95% CI 0.18% to 0.96%). Participants were randomly assigned to either stepped care (1 = watchful waiting, 2 = CBT bibliotherapy with telephone support / visits, 3 = CBT based problem-solving, 4 = medication) or treatment as usual. Assessors were blind to randomisation although it would have been easy to identify participants through their responses to interview questions. Collaborative care treatment programmes have resulted in improvements in depression symptoms (Dietrich, Oxman, Burns, Winchell & Chin 2003; Hedrick et al., 2003; Hunkeler et al., 2006; Katon et al., 1995; Katon et al., 2006; Lin et al., 2003; Unutzer, 2002), functioning (Callahan et al., 2005; Lin et al., 2003), pain (Lin et al., 2003), work performance and productivity (Rost, Smith & Dickinson, 2004, Schoenbaum et al., 2001), marital adjustment (Whisman, 2001) and physical health (Lin, 2003). Stepped care is an integral feature of collaborative care and has therefore been included in this review. Typically it targets a population of people with severe and relapsing depression. One of the main goals for outcome is to improve compliance with prescribed medication. The psychosocial elements of the project are mainly case management from a care manager and psycho-education. However, it does increase adherence and provides opportunities to deliver enhanced care through the delivery of psychological therapies (Christiansen et al., 2008). Several critiques are made of the outcomes obtained within ‘stepped care’. Davison (2000) raises questions in his descriptive review regarding how ‘improvement’ is researched and identified. Relying on a reduction of symptoms overlooks occupational functioning and changes within life roles and social networks that may occur despite high levels of symptoms. Further to this he warns that ‘unrealistic claims of effectiveness and efficiency can compromise the access that most people have to effective mental health services’ (Davison, 2000) as high expectations cannot be met. Sobell & Sobell (2000) recommend that the treatments offered within a stepped care structure should have empirical support but Davison (2000) challenges this and suggests that some non-validated interventions can have a positive effect for people and that the organisational structure of a service should be flexible enough to allow for this. An absence of evidence of efficacy cannot be equated with an absence of evidence of effectiveness (Roth & Fonaghy, 2005), however therapies that are made available should as far as possible been subjected to rigorous scientific review. Therefore a balance should be struck between providing evidence-based interventions, remaining open-minded regarding therapies that have not been sufficiently tested, and ensuring that therapies that have been tested and found not to be beneficial or are harmful, are not offered by the service.

Information systems, referral criteria and patient pathways subgroup – January 2011 10
1.3 What clinical outcomes do people accessing low- intensity interventions obtain? The outcomes for low-intensity interventions are reported in effect sizes; 0.2 to 0.3 might be considered a ‘small’ effect, around 0.5 a ‘medium’ effect and 0.8 to infinity, a ‘large’ effect (Cohen, 1992). The standardised effect size for self-help compared with waiting list conditions indicated a moderate to large effect on the majority of anxiety disorders. Den Boer, Wiersma & Van den Bosch, (2004) originally reported a mean effect size for self-help versus control conditions as 0.84 (95% CI 0.65 to 1.02 and 0.76 (95% CI 0.09 to 1.42) at follow-up, and self-help versus treatment as -0.03 (95% CI -0.20 to 0.14) and -0.07 (95% CI 0.33 to 0.19) respectively. Hirai & Clum (2006) report average effect sizes comparing self-help to control groups for target symptoms as 0.62 at post treatment and 0.51 at follow-up. When compared to therapist-directed interventions, the average effect size was -0.42 at post treatment and -0.36 at follow-up (Hirai & Clum, 2006). Spek et al. (2007) report a large effect size of 0.96 (95% CI 0.69 – 1.22) for internet-based CBT interventions for anxiety compared to control groups. Reger & Gahm (2009) also compared internet-based CBT to wait-list controls and reported effect sizes for post traumatic stress disorder as 0.75 (95% CI 0.49 to 1.01), panic disorder as 1.2 (95% CI 0.87 to 1.58), and phobia as 0.66 (95% CI 0.30 to 1.02). No differences in effect sizes were found among clinical and community samples; for studies in which a diagnostic interview was used to determine the presence of an anxiety disorder compared with studies in which only self-report measures were used; between studies that provided professional support versus unguided self-help; or for studies in which written materials were used compared with studies in which audio / video or internet / computerised materials were used (Hirai & Clum, 2006; Spek et al., 2007; Reger & Gahm, 2009). Self-help treatments were less effective than face-to-face treatments, however when regular support was given during self-help treatment, the results do not differ significantly from face-to-face therapies (Hirai & Clum, 2006). The small number of follow-up data sets suggests that the treatment gains from self-help were sustained after 12 months and 3 years (Den Boer, Wiersma & Van den Bosch, 2004). Cuijpers et al. (2010) also recently reported that guided self-help and face-to-face treatments can have comparable effects. However the methodological quality of some studies included in the review was poor and the division between interventions included a range of variables that could have affected the results; e.g. guided self-help supported with 12 sessions, groups being defined as face-to-face. Cuijpers (1997) reported an effect size of 0.82 (95% CI 0.50 to 1.15) for CBT based self-help. Bower, Richards & Lovell’s (2001) systematic review reports a mean effect size of 0.41 (95% CI 0.09 to 0.72) for self-help treatments. They indicated short-term clinical benefits of similar effect size to non-directive counseling. There is evidence that minimal interventions (bibliotherapy, problem solving and group psycho-education, learner centred education, supporting care givers, internet delivered interventions) can be more effective than ‘usual care’ or ‘no treatment’ conditions (Cuipers, 1997; Dowick et al., 2000; Lovell & Richards, 2000; Bower et al., 2001, Kaltenthaler et al., 2002, Thulesius,
Information systems, referral criteria and patient pathways subgroup – January 2011 11
Petersson, Petersson & Hakansson, 2002; Toseland, McCallion Smith, Banks, 2004). More recently Lovell et al. (2008) reported small effect sizes on outcome measures, ranging from 0.01 to 0.28, with p values ranging from 0.57 to 0.98. Significant differences were not found between written or computerized self-help CBT (Warrilow & Beech, 2009; Gellatly et al, 2007; Cuijpers et al., 2007). Lewis et al. (2003) found greater effect sizes when different self-help materials were combined. The IAPT Doncaster site demonstrated that people accessing low-intensity interventions appear to get a reduction in their symptoms and are more likely to return to work (Clark et al. 2009). Hunkeler et al (2000) found that nurse telehealth care improved the clinical outcomes of antidepressant drug treatment and patient satisfaction and that it fits well into busy primary care settings. Studies suggest that guided CBT based self-help is more effective than CBT based self-help without minimal support from a coach (Lewis et al., 2003; Kaltenthaler et al., 2004; Morgan & Jorm, 2008; Warrilow & Beech, 2009). Indeed Gellatly et al., (2007) found that the standardized mean difference / effect size increased from 0.43 (95% CI 0.30 to 0.57) to 0.80 (95% CI 0.58 to 1.01) when therapist support was added to the treatment. Warrilow & Beech (2009) found a significantly higher effect size for interventions that utilised a CBT approach compared to an education / information approach. They also assert that when a person is assisted through a self-help programme, attrition rates are lower. Cuijpers et al’s (2007) meta-analysis also found that people with a depressive illness found pleasant activity scheduling with a professional, against a control of delayed treatment, produced an overall difference in depression in favour of activity scheduling (effect size = 0.87, 95% CI 0.60 to 1.15). In a qualitative study, Rogers et al. (2004) found that a person’s pre-conceived expectations of a self-help clinic could make them feel self-conscious and vulnerable when they were expected to regain a sense of personal control over the management of their depression. Overall attrition rates for CBT based self–help are high; ranging from 18% for a depression information website (Christensen et al., 2004) to 66% for guided self-help CBT bibliotherapy in primary care (Richards et al., 2003). Gellatly et al. (2007) and Proudfoot et al. (2004) report lower attrition and great effect sizes when participants are recruited through the media, suggesting that people with higher levels of motivation have better outcomes. This raises concerns about relying on CBT based self-help for people with low volition, such as people who have depression (Kaltenthaler et al., 2004). It would appear that attrition, suitability of the materials, level of therapist input and the profile of the patient all impact on outcomes from low-intensity interventions.
Information systems, referral criteria and patient pathways subgroup – January 2011 12
1.4 How are people matched to the appropriate tier? While driving the delivery of the lowest intensity psychological intervention, most models of stepped care allow for individuals needs to be ‘matched’ to an appropriate level to meet their needs (Bower & Gilbody, 2005). This could mean that individuals with mild to moderate mental health problems are matched to low-intensity interventions and people with more complex mental health problems are matched to more intense interventions immediately. Similarly, mental health problems that could involve adverse consequences as a result of starting a person at too low a step can be matched directly to a more intensive level. Critical to this process are the assessment of need and the monitoring of client outcomes to ensure that an effective match is made (Bower & Gilbody, 2005). Therefore, decision making is critical to access tiers, obtain outcomes within a tier, and to move between tiers. A range of factors are considered relevant in making the match, including the nature of the presenting problem and its duration, co-morbidity issues, and response to previous treatments (see Section 2 for a fuller discussion). Clinicians debate how decisions are made within stepped care and report concerns about overly relying on clinical judgment or clinical outcome measures. Davison (2000) recommends that the clinician’s personal preference should not be the only driver in place to make a match to the appropriate tier. Richards (2010) describes an ‘allocation – stepping continuum’ where a balance is made between two decision making points; assessment and allocation to an intervention, and progress review and stepping up to an intervention. Some service models give people the opportunity to ‘match themselves’, and offer people choice within a range of ‘steps’ rather than between them (White et al., 2008); for example access to advice clinics, groups, bibliotherapy or computerised CBT. Bower, Gilbody and Barkham (2006) discuss a range of issues concerning the use of routine outcome measures in stepped care. Typically, normative methods are used to define outcomes as relative to the performance of others as opposed to the particular characteristics of the patient. These criteria may relate to the treatment (reduction in symptoms in a particular population having received a particular treatment), the patient population (moving from a clinical to a non-clinical population), or the specific disorder (for example with depression, treat until full remission to reduce risk of relapse). This use of normative criteria can sit uncomfortably with clinicians who prefer traditional evidence based medicine, where decisions about treatment are based on knowledge from controlled trials of the effectiveness of treatment. Within stepped care, the clinician making the match needs to balance individual needs with population needs.
Information systems, referral criteria and patient pathways subgroup – January 2011 13
1.5 What drivers (restrictions, checks, and balance s) are in place to encourage people to engage at each level across the tiers? Services have reported a combination of restricted and open access to respond to high volumes of referrals. Initially, the STEPS primary care mental health team offered open access to ‘rapid access services’ at the same time as restricting access to individual therapy (White et al., 2008). A brochure detailed a diverse range of options that people can select (guided self-help, large psycho-education groups, interactive groups, advice clinics) and access through a phone call negates the need to individually assess the large numbers of people accessing the service. To access individual therapy people were referred, by either the GP or health professional, and assessed with a view to their suitability for psychological therapy. Within this model the person accessing the service is empowered to make their own choice regarding the most appropriate service. White et al. (2008) point out that this model requires ‘interconnectiveness’; stepped care can only work well when its component parts are working well (e.g. an advice clinic would not work well in isolation). More recently, the STEPS primary care mental health team have reported high attrition rates for individual therapy; 32% failed to opt-in, 26% who opted-in failed to attend their first appointment, and 34% of individuals who were taken on for individual treatment failed to complete this (Grant, McMeekin, Jamieson et al. in press). They argue for a ‘root and branch change’ in how individual therapy is offered at the primary care / low intensity level. Following on from this, White, Ross, Richards et al. (submitted) present a service evaluation of ‘call back’, designed to increase access to low-intensity services. The STEPS service has been redesigned to replace GP / health care practitioner referral systems with self-referral. A person wishing to access the service ‘phones up’ and receives a ‘call back’ from a qualified therapist who discusses the most appropriate low-intensity intervention available for their problem. Between September 2008 and November 2009, 600 ‘call-backs’ were made (which represents 16% of all service user contacts), 20% booked appointments at the main therapist contact service – the advice clinic, 35% booked to attend the Stress Control class, and 17 % of callers were offered individual therapy. On average, those offered a service (therapy, class, interactive group, workshop) within STEPS started the intervention 8.9 days following the ‘call-back’. This model balances open access, choice and empowerment against restriction of high intensity therapies. The previous experience of the clinician appears to act as a powerful driver. Within the IAPT demonstration sites, low-intensity workers offering low-intensity interventions were less likely to ‘step’ people up to higher intensity interventions. High intensity therapists tended to offer high intensity treatments and were less likely to match to low-intensity options (Clark, et al., 2009). There is a sense that clinicians will tend to match based on their previous experience – if they have experience of delivering high intensity therapies they will be more likely to match to high intensity therapies. Equally it would appear that low-intensity staff with a limited experience of mental health are less likely to ‘step people up’ to another service.
Information systems, referral criteria and patient pathways subgroup – January 2011 14
It would appear that ideally a service using a stepped care model should have drivers that strongly encourage clinicians to match to the least intensive intervention. Some stepped care services achieve this by monitoring the number of sessions that clinicians have available to deliver high –intensity interventions. Offering ‘rapid access’ to a range of low-intensity interventions offers clients a range of options. However there also needs to be a mechanism where people can access more intensive treatment options when needed and that this is monitored by the service.
1.6 Do socio-economically deprived populations acce ss and use services within each of the service models? Singleton et al. (2001) found that people with depression were more likely to; be unemployed, belong to social class 4 and below, have lower predicted intellectual function, no formal educational qualifications, live in Local Authority or Housing Association accommodation, have moved 3 or more times in the last 2 years and to live in an urban environment. Despite this close relationship between economic factors and mental health problems, there is little reported on economically deprived communities across all the studies and papers on stepped care. Grant et al. (in press) specifically explored attrition rates in people accessing either individual Cognitive Behavioural Therapy (CBT) or Person Centred Counselling (PCT) and the impact of deprivation. Using the Scottish Index of Multiple Deprivation (SIMD), where 1 represents the most affluent and 10 the most deprived households (Scottish Government, 2009), they found that 40 % of referrals received for individual therapy were from the most deprived communities. Of this group, 60% opted in to either CBT or PCT, and then 23% failed to attend their first appointment. This is in contrast with less than 5% of referral being received from the most affluent communities, of which 70% opt-in, and then 63% fail to attend their first appointment. They concluded that individuals from deprived areas (those with a higher SIMD score) were more likely to fail to opt-in to the services but there was no evidence that they were more likely to fail to attend their first appointment or drop-out during therapy than those from affluent areas. Following on from this, White, Ross, Richards et al. (submitted) present a service evaluation of ‘call back’, designed to increase access to low-intensity services and found that of the calls received requesting a ‘call back from a qualified therapist, 35% were from the most deprived communities and less than 5% were from the most affluent communities. The Newham IAPT site reports a population that consisted of 49% from Black and Minority Ethnic (BME) communities, with 13% not speaking English. One in five of the people seen in Newham referred themselves to the service. When compared to GP referrals, self-referral patients were at least as ill, tended to have had their problems for longer, and more closely matched the ethnic mix of the local population. Therefore it would appear that the access arrangements to services (referral by GP, or opt-in systems) could be off-putting for both socio-economically deprived and BME populations.
Information systems, referral criteria and patient pathways subgroup – January 2011 15
1.7 What systems are used to ensure the service is self correcting and people matched to the incorrect tier are reallocated? As previously stated, getting a match to the appropriate step in the service model appears to be mainly done with a combination of standardised assessments and clinical judgment. Decisions may be based on data collected within treatment (Breslin et al., 1997). Therefore, the clinical assessments and information collected that are used to ‘make the match’ are also used to ‘self correct’. Some services models rely on people identifying that their needs have not been met and re-accessing services. General Practitioners (GP) appear to be fulfilling a ‘self correcting’ role in that they refer people to receive a more intensive intervention when outcomes from a lower intensity intervention are not achieved. For a system to be self-correcting, the service needs to have agreed the ‘outcome’ (Bower, Gilbody and Barkham, 2006) that a person should achieve (reduction in symptoms, moving into a non-clinical population, or full remission). Bower & Gilbody (2005) recommend a decision is made based on judgments about ‘significant health gain’ or ‘improvement’ but could be dependent on type of disorder, its natural history, and the effectiveness of clinical interventions. Jacobson & Truax’s (1991) ‘clinically significant and reliable change’ or individualised ‘expected outcomes’ could be used to assist in decision making. The importance of a ‘self-correcting system’ has also been reinforced by the IAPT external review and lessons can be learnt from the demonstration sites (Rick et al., 2010). Within the Dutch PIKO project (Prevention Intervention for Frail Elderly) individuals were assessed at the end of every ‘stepped’ intervention (Van’t Veer-Tazelaar et al., 2009). If a favourable outcome was not obtained, a decision was made to step-up individuals to the next intervention. In making an appropriate match for people with addiction to the appropriate treatment, Sobell & Sobell (2000) have named a process ‘aptitude treatment interaction (ATI)’ and take the following factors into account; motivation to abstain and psychiatric co-morbidity. They propose that problems in finding ATI’s may be due to relying too heavily on diagnostic assessments, such as the Diagnostic and Statistical Manual of Mental Disorders (DSM).
1.8 Are the service delivery models economical? Otto, Pollack & Maki (2000) found that the per-patient costs are considerable lower for empirically supported psychosocial treatment, and the short-term and longer-term outcomes are at least as good as what people derive from various psychotropics. However, despite this, there are a limited number of health economic studies reported in the literature (Gilbody, Bower & Whitty, 2006). The collaborative model reports that ‘primary care physician’ treatment as usual’ is more economical for mild to moderate depression than collaborative care (Von Korff et al., 1998). However, to put this in perspective, collaborative care attracts increased costs associated with delivering the intervention,
Information systems, referral criteria and patient pathways subgroup – January 2011 16
increased costs in terms of increased primary care visits, increased use of antidepressant medication, and access to secondary care (Gilbody, Bower & Whitty, 2006). Katon et al. (2002) examined cost and consequence over a 28-month period and found that excess costs associated with enhanced care in the short-term had disappeared over time. They also report that there are costs offset in terms of minimising the impact on wider health services. These conclusions are based on research carried out in the American health care system and need to be replicated in the UK. Possibly collaborative care is more economically appropriate with severe and enduring health problems. The IAPT demonstration sites observed an increase in employment of 5% (combining Doncaster 4% and Newham 10%) of the treated population which is supportive of the assumptions made in the cost-benefits analysis included in the Department of Health’s Comprehensive Spending Review proposal (Clark, Layard & Smithies, 2008). This achievement has demonstrated that costs can be off-set in providing psychological therapies to people, improving functioning and enabling them to return to work. More recently, Glover, Webb and Evison (2010) reported that, across the 32 first year IAPT sites, the overall proportion in work and not claiming benefit rose by 2% (95% CI of difference in proportions = +1.0% to +3.0%) Negative outcomes from interventions could have an economical impact on services. Wilson, Vitousek & Loeb (2000) caution that failure to respond to an initial low-intensity level of care could discourage people from seeking subsequent treatment or undermine their response to such treatment. Further to this, it is possible that a negative impact on a person’s self-esteem could reduce their motivation to continue trying to change (Davison, 2000). However, this has not been specifically evaluated in the studies identified within this review. Bower & Gilbody (2005) raise economic issues regarding offering low intensity interventions within stepped care. They present as an example; a bibliotherapy intervention being found to be superior to ‘no treatment’ incurring costs, as resources would need to be allocated to provide the bibliotherapy where none were allocated before. It would be more economical if low intensity interventions delivered positive outcomes to some populations, reducing the need for high intensity interventions. They raise methodological issues in researching equivalence between low intensity interventions and traditional psychological therapies where larger sample sizes are required to adequately examine differences in effectiveness. It is still open to question whether offering preventative interventions does reduce the longer–term demand on the service, although Van’t Veer-Tazelaar et al., (2009) offer promising results in favour of this. Adopting a population rather than individual perspective may identify greater population health benefit.
Information systems, referral criteria and patient pathways subgroup – January 2011 17
1.9 What impact do the various organisational servi ce models have on the capacity of the system? There are key issues which impact on the efficiency of a stepped care service. Essentially stepped care is a balance between meeting the needs of the population in a community and meeting the needs of individuals, and the trade-offs that are required between the two;
‘…stepped care seeks to derive the greatest population benefit from available treatment resources, rather than meeting the needs and preferences of the individual patient’ (Bower, Gilbody & Barkham, 2006; p. 25).
Within stepped care, the methods of assessment that are used to make a match to and between the various steps will impact on the capacity of the system. Trade-offs are made between using the most reliable and valid assessment of need and using assessments that are quick to administer. A time consuming assessment that is used to ‘match’ people to the appropriate level could impact on the efficiency of the service. There are also inherent trade-offs between ‘false positive’ (inappropriate stepping up when it is not required) and ‘false negatives’ (failure to step-down when appropriate) (Bower, Gilbody & Barkham, 2006; Bower & Gilbody, 2005). This means that some people will spend too long at lower levels of service that are not meeting their needs, while others will be stepped up inappropriately making the system unwieldy and inefficient. Access restrictions to a service may impact on longer term outcomes. Clark et al. (2009) reports a duration effect that was noticed in the Doncaster IAPT demonstration site. A significant duration effect for depression and anxiety recovery rates (x2 = 13.1, p = 0.02) with the highest rates being observed when the problem duration was under 3 months (60%) or between 3 and 6 months (63%) and the lowest when problem duration was over 4 years (47%). Therefore, the longer the duration of a problem the less likely the person is to achieve a positive outcome. Services that set time restrictions regarding access to services may miss an optimum period of engaging a person, facilitating active responses and achieving positive outcomes for their interventions. However this should be set in context against the natural recovery of people with depression. Posternak and Miller (2001) in a meta-analysis of wait-list control groups, found average recovery from depression was around 20%, and percentage change on the Beck Depression Inventory was around 20%. The ‘emphasis’ of a service also appears to impact on capacity. Low intensity interventions are important in facilitating high throughput (Clark et al., 2009). Newham’s ‘emphasis’ on high – intensity interventions meant it failed to achieve the scale required to cope with high volumes of referrals and increase access to psychological therapies. Doncaster’s ‘emphasis’ on low-intensity interventions achieved a high throughput but appears to have resulted in a very low number of people being passed onto high intensity therapies (Clark et al. 2009), possibly even when needed. The Newham site used self-referral and found that it enabled disadvantaged ethnic groups to access and engage
Information systems, referral criteria and patient pathways subgroup – January 2011 18
with the service. It also appears from the service evaluations of the IAPT demonstration sites, that there is less likelihood to be referred onto another service if the first point of access is to a high intensity service. White et al. (2008) emphasise that stepped care can only function well when there is ‘interconnectiveness’ – providing a range of low-intensity options – and suggest that offering one low-intensity intervention in isolation will not work well within a service. 1.10 Summary of oganisational structures In summary, stepped care service models should increase access to effective, easily used services for all people with mental health problems. The following should be taken into account when providing services.
• There should be agreed consensus on the range of evidence-based treatments available and this should be reviewed as new evidence comes to light. This consensus needs to take into account individualised versus population based approaches.
• Service should be accessible with a minimum wait – possibly with direct access / self referral systems, as these appear to open access to services for ethnic populations. It appears that increasing access and offering choice to people is possible when making a selection from a range of low-intensity interventions.
• A range of options of varying levels of intensity should be offered with the stepped care model.
• The least intrusive therapy that provides significant health gain should be offered first. This should be considered in terms of resource, therapist time, and inconvenience for the person seeking help and should not work against ‘normal’ coping responses within families and the community.
• Systematic mechanisms should be agreed and monitored across services to ensure the smooth running of the services; for example agreed referral criteria.
• An individual’s needs are matched to an appropriate ‘step’ to meet their needs. Matching people’s needs to the appropriate tier / step is critical and should involve a balance between clinical judgment, standardised measures, and mechanisms that encourage clinicians to consider population versus individual needs and the impact of their own clinical experience
• The system should be self-correcting with continual monitoring of outcomes. This involves having agreement on what constitutes an ‘outcome’, people accessing the service should be monitored at the last session / every session, ‘false positives and negatives’ are monitored and corrected within the system.
• Low intensity interventions appear to deliver positive outcomes to highly motivated populations and can be used to deliver services that can cope with a large volume of referrals. Outcomes are improved when a coach guides the use of the materials, and when several low-intensity interventions are used at the same time (e.g. bibliotherapy plus large psycho-education group).
Information systems, referral criteria and patient pathways subgroup – January 2011 19
• Staff working at low-intensity levels are in a key position to ask questions that encourage compliance with medication.
• The assessments used within the service have to get a balance between matching needs accurately and ‘clogging up the system’.
• Collaborative care models appear to be most cost - effective when targeted at the population of people with relapsing depression.
Implications for service delivery There are implications for service delivery. Stepped care service models should increase access to effective, easily used services for all people with mental health problems. A range of evidence based therapies should be available in a variety of formats to meet people’s needs. Choice and self-referral systems should be incorporated as far as possible. It is likely that services will have to be able to respond to high volumes of referrals. The least intrusive therapy that provides significant health gain should be offered first.
Information systems, referral criteria and patient pathways subgroup – January 2011 20
References Arthur, A. R. (2005). Layered care: A proposal to develop better primary care mental health services. Primary Care Mental Health, 3, 103 - 109. Bower, P. and Gilbody, S. (2005). Stepped care in psychological therapies: Access, effectiveness and efficiency. British Journal of Psychiatry. 186, 11 - 17. Bower, P., Gilbody, S. and Barkham, M. (2006). Making decisions about patient progress: the application of routine outcome measurement in stepped care psychological therapy services. Primary Care Mental Health, 4, 21 - 28. Bower, P., Richards, D., Lovell, K. (2001). The clinical and cost-effectiveness of self-help treatments for anxiety and depression disorders in primary care: a systematic review. British Journal of General Practice. 51, 471, 838 - 845. Breslin F, Sobell M, Sobell L, et al. (1997). Towards a stepped care approach to treating problem drinkers: The predictive utility of within-treatment variables and therapist prognostic ratings. Addiction, 92, 1479 - 1489. Callaghan CM, Kroenke K, Counsell SR, Hendrie HC, Perkins AJ, Katon W et al. (2005). Treatment of depression improves physical functioning in older adults. Journal of the American Geriatrics Society, 53, 367 - 373. Cape, J. and Barkham, M. (2002). Practice Improvement Methods: Conceptual base, evidence-based research and practice-based recommendations. Journal of Clinical Psychology, 41 (3), 285 – 307. Christensen, H., Griffiths, K. & Jorm, A. (2004). Delivering interventions for depression by using the internet: Randomised controlled trial. British Medical Journal, 325, 265 – 268. Clark, D. M., Layard, R. and Smithies, R. (2008). Improving acess to psychological therapy: initial evaluation of the two demonstration sites. LSE Centre for Economic Performance Working Paper No 1648. Available at http://www.iapt.nhs.uk/2008/10/20/publication Accessed on 21 April 2010. Clark, D. M., Layard, D., Smithies, R., Richards, D., Suckling, R., and Wright, B. (2009). Improving access to psychological therapy: Initial evaluation of two UK demonstration sites, Behaviour Research and Therapy, 47, (11), 910 - 920. Cohen, J. (1992). A power primer. Psychological Bulletin 112, 155 –159. Cuijpers, P. (1997). Bibliotherapy in unipolar depression: A meta-analysis. Journal of Behavioural Therapy & Experimental Psychiatry 28, 2, 139 - 147. Cuijpers, P., Donker, T., van Straten, A., Li, J., Anderson, G. (2010). Is guided self-help as effective as face-to-face psychotherapy for depression and anxiety disorders? A systematic review and meta-analysis of comparative outcome studies. Psychological Medicine, April 21, 1 – 15. Cuijpers, P., Schuurmans, J. (2007). Self-help interventions for anxiety disorders: an overview. Current Psychiatry Reports, 9, 284 - 290.
Information systems, referral criteria and patient pathways subgroup – January 2011 21
Cuijpers, P., van Straten, A. & Warmerdam, L. (2007) Behavioural activation treatment of depression: A meta-analysis. Clinical Psychology Review, 27, 318 - 326. Davison G. C. (2000). Stepped care: Doing more with less? Journal of Consulting and Clinical Psychology, 68, (4), 580 - 585. Den Boer, P.C., Wiersma, D., Van den Bosch, B.J. (2004). Why is self-help neglected in the treatment of emotional disorders? A meta-analysis. Psychological Medicine, 34, 959 - 971. Department of Health. (2001). Treatment choice in psychological therapies and counselling: Evidence based clinical practice guideline. London: Department of Health. Dietrich, A.J., Oxman, T.E., Burns, M.R., Winchell, C.W., & Chin, T. (2003). Application of a depression management office system in community practice: A demonstration. Journal of the American Board of Family Practice, 16, 107 – 114. Dowrick, C., Dunn, G., Ayuso-Mateos, J.L., Dalgard, O.S., Page, H., Lehtinen, V., Casey, P., Wilkinson, C., Vazquez-Barquero, J.L. & Wilkinson, G. (2000). Problem solving treatment and group psycho-education for depression: Multi-centre randomized controlled trial. British Medical Journal; 321: 1450 - 1456. Gellatly, J., Bower, P., Hennessey, S., Richards, D., Gilbody, S. & Lovell, K. (2007). What makes self-help interventions effective in the management of depressive symptoms? Meta-analysis and meta-regression. Psychological medicine, 37, 1217 – 1228.
Gilbody S, Bower P, Whitty P. (2006). Costs and consequences of enhanced primary care for depression: A systematic review of randomised control trials. British Journal of Psychiatry, 189, 297 – 308. Glover, G., Webb, W., Evison, F. (2010). Improving access to psychological therapies: A review of the progress made by sites in the first roll – out year. North East Public Health Observatory. Grant, K., McMeekin, E., Jamieson, R., Fairful, A., Miller, C. & White, J. (in press). Attrition rates in a low-intensity service: A comparison of CBT and PCT and the impact of deprivation. Submitted to Behaviour and Cognitive Psychotherapy, 22 Dec 2009. Grimshaw et al., (2004). Effectiveness and Efficiency of Guidance Dissemination and Implementation Strategies. Health Technology Assessment. Gulliford, M., Hughes, D and Fieroa-Munoz, J et al. (2001). Access to health care: report of a scoping exercise for the National Co-ordinating Centre for NHS Service delivery and Organisation, RandD NCCSDO. London: Kings College. Hagga D.A. (2000). Introduction to the Special Section on Stepped Care Models in Psychotherapy, Journal of Consulting and Clinical Psychology, 68 (4), 547 – 548. Hannan, C., Lambert, M.J., Harnon, C., Nielson, S.L., Smart, D.W., Shinokawa, K. & Sutton, S.W. (2005). A lab test and algorithms for identifying clients at risk of treatment failure. Journal of Clinical Psychology, 61 (2), 155 – 163.
Information systems, referral criteria and patient pathways subgroup – January 2011 22
Hedrick, S. C., Chaney, E. F., Felker, B., Liu, C.F., Hasenberg, N., Heagarty, P. et al. (2003). Effectiveness of collaborative care depression treatment in Veterans affairs primary care. Journal of General Internal Medicine, 18, 9 - 16. Hirai, M. & Clum, G.A. (2006). A meta-analytic study of self-help interventions for anxiety problems. Behaviour Therapy, 37, 99 - 111. Hunkeler, E. M., Katon, W., Tang, L., Williams, J. W. , Kroenke, K., Lin, E. H., et al. (2006). Long term outcomes from the IMPACT randomised control trial for depressed elderly patients in primary care. British Medical Journal, 332, 259 - 263. Jacobsen N, & Truax P. (1991). Clinical significance: a statistical approach to defining meaningful change in psychotherapy research. Journal of Consulting and Clinical Psychology, 59, 12 – 19. Kaltenthaler, E., Parry, G., Beverly, C et al. (2008). Computerised cognitive-behaviour therapy for depression: Systematic review. British Journal of Psychiatry, 193, 181 – 184. Katon W, Von Korff M, Lin E, Walker E, Simon GE, Bush T, et al. (1995). Collaborative management to achieve treatment guidelines. Impact on depression in primary care. Journal of the American Medical Association, 273, 1026 – 1031. Lewis, G., Anderson, L., Araya, R., et al. (2003). Self-help interventions for mental health problems. Department of Health: Policy Research Programme, London. Lin, E.H., Katon, W., Von Korff, M., Tang, L., Williams, J.W., Kroenke K, et al. (2003). IMPACT investigators. Effects of improving depression care on pain and functional outcomes among older adults with arthritis: A randomized controlled trial. Journal of the American Medical Association, 290, 2428 – 2429. Lovell, K., Bower, P., Richards, D., Barkham, M., Sibbald, B., Roberts, C., et al. (2008). Developing guided self-help for depression using the Medical Research Council complex interventions framework: A description of the modelling phase and results of an explanatory randomised control trial [on-line]. BMC Psychiatry, 8 (91). Available at: http://www.biomedcentral.com/1471-244X-8-91. Accessed 19th March 2010. Lovell K & Richards D. (2000). Multiple access points and level of entry (MAPLE): Ensuring choice, accessibility and equity for CBT services. Behavioural and Cognitive Psychotherapy, 28, 379 - 391. National Collaborating Centre for Mental Health. (2009). Depression in Adults (update). Depression: the treatment and management of depression in adults. National Clinical Practice Guideline 90. Available at: http://guidance.nice.org.uk/CG90/Guidance/pdf/English. Accessed on 12 April 2010. National Institute for Health and Clinical Excellence. (2004). Depression: Management of depression in primary and secondary care. London, NICE. Otto, M. W., Pollack, M. H. & Maki, K. M. (2000). Empirically supported treatments for panic disorder: costs, benefits, and stepped care. Journal of Consulting Clinical Psychology, 68, 556 - 563. Posternak, M. A. & Miller, I. (2001). Untreated short-term course of major depression: A meta-analysis of outcomes from studies using wait-list control groups. Journal of Affective Disorders, 66, 139 - 146.
Information systems, referral criteria and patient pathways subgroup – January 2011 23
Proudfoot, J., Ryden, C., Everitt, B., et al. (2004). Clinical efficacy of computerised cognitive behavioural therapy for anxiety and depression in general practice. Psychological Medicine, 33, 217 - 227. Reger, M.A. & Gahm, G.A. (2009). A meta-analysis of the effects of internet- and computer- based cognitive behavioural treatments for anxiety. Journal of Clinical Psychology, 65, 53 - 75. Richards, A., Barkham, M., Cahill, J., Richards, D., Williamsn, C. & Heywood, P. (2003). PHASE: A randomised, controlled trial of supervised self-help cognitive behavioural therapy in primary care. British Journal of General Practice, 53, 764 - 770. Richards D, Lovell K, McEvoy P. (2003). Access and effectiveness in psychological therapies: Self-help as a routine health technology. Health & Social Care in the Community, 11, (2), 175 - 182. Richards, D. (2010). Access and organisation: putting low intensity interventions to work in clinical services. In Oxford Guide to Low Intensity CBT Interventions. Edited by James Bennett-Levy, David A. Richards, Paul Ferrand, Helen Christiansen, Kathleen M. Griffiths, David J. Kavanagh, Britt Klein, Mark A. Lau, Judy Proudfoot, Lee Ritterband, Jim White and Chris Williams. Oxford University Press, New York. Rick, J., Hutten, R., Chambers, E., Connell, J., Hardy, G. and Parry, G. (2010). Implementing IAPT: Lessons from the demonstration sites. University of Sheffield, SDO IAPT Evaluation Team. Rogers, A., Oliver, D., Bower, P., et al. (2004). Peoples’ understanding of a primary care-based mental health self-help clinic. Patient Education and Counselling, 53, 41 – 46. Rost, K., Smith, J.L., & Dickenson, M. (2004). The effect of improving primary care depression management on employee absenteeism and productivity: A randomized control trial. Medical Care, 42, 1202 – 1210. Roth A & Fonaghy P. (1996). What works for whom? A critical review of psychotherapy research. Guildford: London. Schoenbaum, M., Unutzer, J., Sherborune, C., Duan, N., Rubenstein, L.V., Miranda, J., et al. (2001). Cost-effectiveness of practice-initiated quality improvement for depression. Journal of the American Medical Association, 286, 1325 - 1330. Scottish Government (2009). Scottish Index of Multiple Deprivation 2009 General Report. Scottish Government National Statistics Publication. Available at: http://www.scotland.gov.uk/Publications/2009/10/28104046/21. Accessed on 8th June 2010. Singleton, N., Bumpstead, R., O’Brian, M., Lee, A., & Meltzer, H (2001). Psychiatric Morbidity among Adults living in Private Households, 2000: Summary Report. London: Office for National Statistics. Sobell MB & Sobell LC. (2000). Stepped care as a heuristic approach to the treatment of alcohol problems. Journal of Consulting and Clinical Psychology, 68, 573 - 579. Spek, V., Cuijpers, P., Nyklicek, I., Riper, H., Keyzer, J., Pop, V. (2007). Internet-based cognitive behavioural therapy for symptoms of depression and anxiety: A meta-analysis. Psychological Medicine, 37, 329 - 328.
Information systems, referral criteria and patient pathways subgroup – January 2011 24
Stein, D.M. and Lambert, M.J. (1995). Graduate training in psychotherapy: Are therapy outcomes enhanced. Journal of Consulting and Clinical Psychology. 63, (2), 182 - 196 Thulesius, H. Petersson, C., Petersson, K., Hakansson, A. (2002). Learner-centred education in end-of-life care improved well being in home care staff: A prospective controlled study. Palliative Medicine, 16, 347 – 354. Toseland, R.W., McCallion, P., Smith, T., Banks, S. (2004). Supporting caregivers of frail older adults in an HMO setting. American Journal of Orthopsychiatry, 74, 349 – 364. Unutzer J, Katon W, Callahan CM, Williams JW, Hunkeler E, Harpole L, et al (2002) Collaborative care management of late-life depression in the primary care setting. Journal of the American Medical Association, 288, 2836 - 2845. Van’t Veer- Tazelaar N, van Marwijk H, van Oppen P, Nijpels G, van Hout H, Cuijpers P, Stalman W, Beekman A. (2006). Prevention of anxiety and depression in the age group of 75 years and over: a randomised controlled trial testing the feasibility and effectiveness of a generic stepped care programme among elderly community residents at high risk of developing anxiety and depression versus usual care. BMC Public Health 6: 186. Available at: http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1550238/pdf/1471-2458-6-186.pdf Accessed on 10th September 2010. Von Korff, M., Katon, W., Bush, T., Lin, E. H., Simon, G. E., Saunders, K., Ludman, E., Walker, E., Unutzer, J. (1998). Treatment costs, cost offset, and cost effectiveness of collaborative management of depression. Psychosomatic Medicine, 60, 143 – 149. Warrilow, A. & Beech, B. (2009). Self-help CBT for depression: Opportunities for primary care mental health nurses? Journal of Psychiatric and Mental Health Nursing, 16, 792 – 803. Whisman, M. A. (2001). Marital adjustment and outcomes following treatment for depression. Journal of Consulting & Clinical Psychology, 69, 125 – 129. White, J. (2008). Stepping up primary care. Psychologist, 21,(10), 844 - 847. White, J. (2010). The STEPS model: a high volume, multi-level, multi-purpose approach to address common mental health problems. In Oxford Guide to Low Intensity CBT Interventions. Edited by James Bennett-Levy, David A. Richards, Paul Ferrand, Helen Christiansen, Kathleen M. Griffiths, David J. Kavanagh, Britt Klein, Mark A. Lau, Judy Proudfoot, Lee Ritterband, Jim White and Chris Williams. Oxford University Press: New York. White, J., Joice, A., Petrie, P., Johnston, S., Gilroy, D., Hutton, P., Hynes, N. (2008). STEPS: Going beyond the tip of the iceberg. A multi-level, multi-purpose approach to common mental health problems. Journal of Public Mental Health, 7(1), 42 – 50. White, J., Ross, M., Richards, C., Johnston, S., Manson, V. (in press). ‘Call-back’: Increasing access to and improving choice in a multi-level, multi-purpose low-intensity service. Behavioural and Cognitive Psychotherapy. Wilson T.G., Loeb, K.L., Vitousek K.M. (2000). Stepped care treatment for eating disorders. Journal of Consulting and Clinical Psychology, 68, (4), 564 - 572.
Information systems, referral criteria and patient pathways subgroup – January 2011 25
(TRADITIONAL PRIMARY/ SECONDARY CARE DIVIDE)
LEVEL 1 : MANAGEMENT FOR SUBCLINICAL PROBLEMS
PROBLEMS: e.g. transitional/adjustment issues, marital/relationship problems, bereavement,
stress, situational crises.
SERVICES: e.g. Counselling, community agencies (RELATE, CRUSE), individual/community,
educational, programmes, bibliotherapy, social prescribing.
LEVEL 2 : TREATMENT FOR MILD DISORDERS
PROBLEMS: e.g. anxiety (panic disorder, phobias), depression, disordered eating behaviours.
SERVICES: e.g. brief psychological therapies, computerised CBT, guided self-help,
manualised/protocolised psychological treatments, group therapies/psycho-educational interventions, counselling.
LEVEL 3 : TREATMENT FOR MODERATE DISORDERS
PROBLEMS: e.g. persistent anxiety/depressive disorders (post traumatic stress
disorder, obsessive compulsive disorder, generalised anxiety) bulimia. SERVICES: e.g. standardised/substantive psychological therapies,
individualised/tailored for specific patient group.
LEVEL 4: TREATMENT FOR SEVERE/COMPLEX DISORDER
PROBLEMS: e.g. chronic/severe depression, treatment resistant disorders, bipolar disorder, chronic psychosis, personality disorder, substance misuse,
anorexia.
SERVICES: e.g. community mental health teams, highly specialised
multidisciplinary teams, tailored psychological therapies.
LEVEL 5: INPATIENT TREATMENT FOR SEVERE/COMPLEX DISORDER
PROBLEMS: e.g. risk to self or others,
complex, co-morbid presenting problems.
SERVICES: e.g. general psychiatric inpatient services, highly specialised disorder specific services (e.g. eating disorders,
forensic).
Number of Patients
Intensity of Treatment
Appendix 1 Models of stepped care Diagram illustrating tiers/ services in delivery of psychological therapies Extract from Applied Psychologists and Psychology in NHS Scotland: Working group discussion paper (2010)
Information systems, referral criteria and patient pathways subgroup – January 2011 26
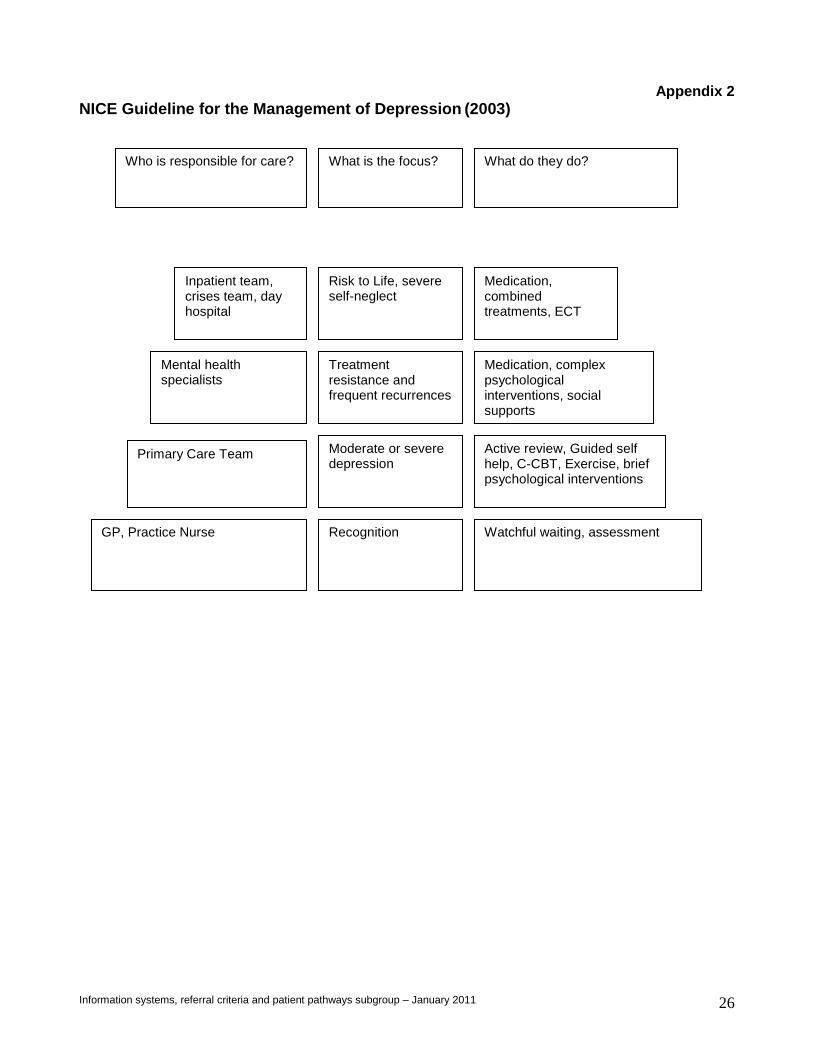
Appendix 2 NICE Guideline for the Management of Depression (2003)
Who is responsible for care? What is the focus?
Risk to Life, severe self-neglect
Medication, combined treatments, ECT
Inpatient team, crises team, day hospital
Treatment resistance and frequent recurrences
What do they do?
Mental health specialists
Medication, complex psychological interventions, social supports
Primary Care Team
Recognition GP, Practice Nurse Watchful waiting, assessment
Active review, Guided self help, C-CBT, Exercise, brief psychological interventions
Moderate or severe depression
Information systems, referral criteria and patient pathways subgroup – January 2011 27
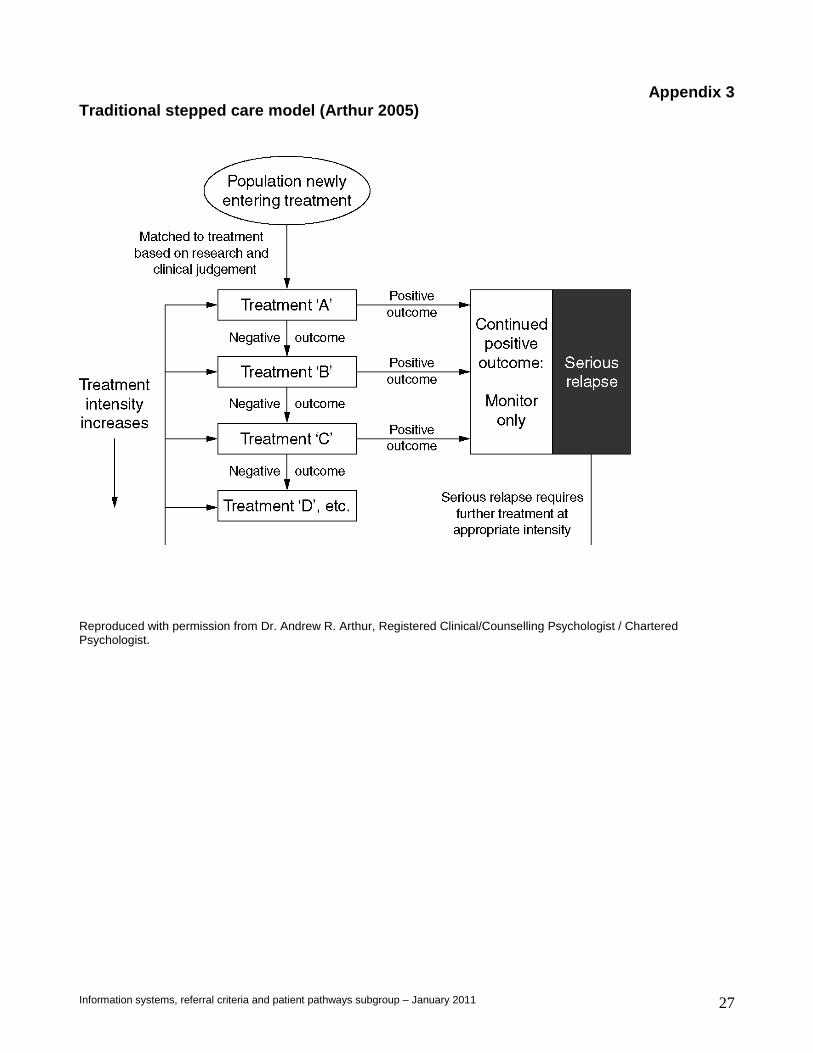
Appendix 3 Traditional stepped care model (Arthur 2005)
Reproduced with permission from Dr. Andrew R. Arthur, Registered Clinical/Counselling Psychologist / Chartered Psychologist.
Information systems, referral criteria and patient pathways subgroup – January 2011 28
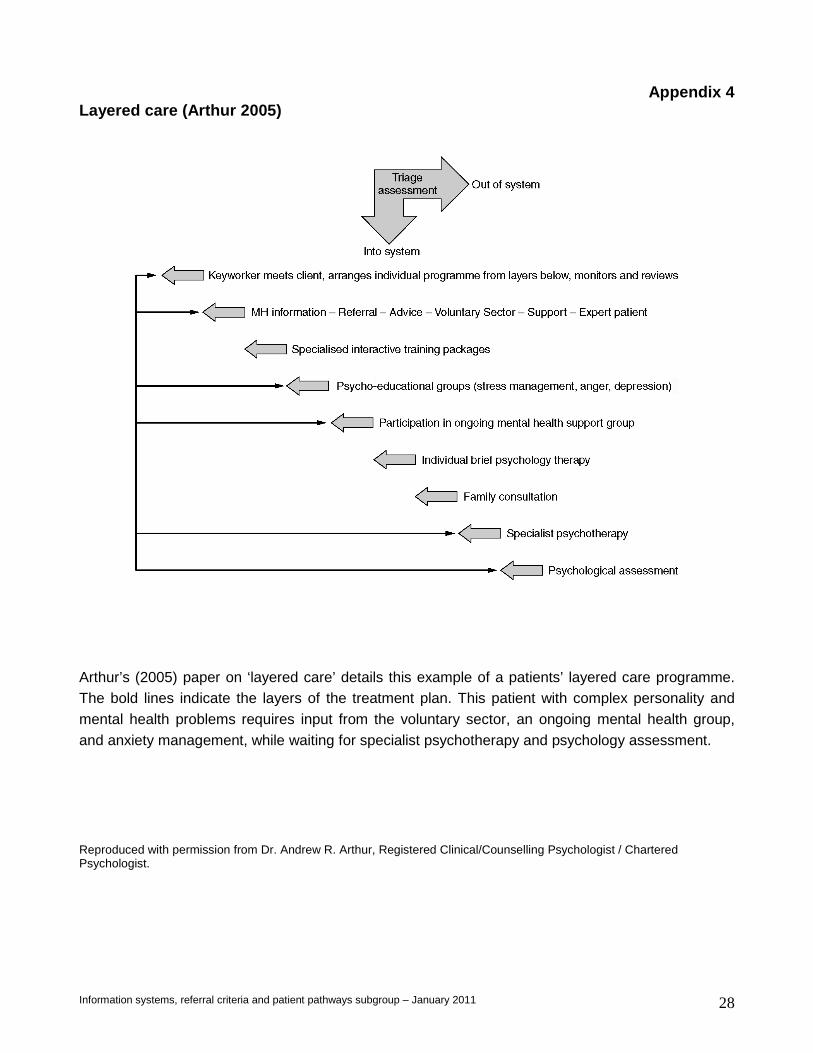
Appendix 4 Layered care (Arthur 2005)
Arthur’s (2005) paper on ‘layered care’ details this example of a patients’ layered care programme. The bold lines indicate the layers of the treatment plan. This patient with complex personality and mental health problems requires input from the voluntary sector, an ongoing mental health group, and anxiety management, while waiting for specialist psychotherapy and psychology assessment.
Reproduced with permission from Dr. Andrew R. Arthur, Registered Clinical/Counselling Psychologist / Chartered Psychologist.
Information systems, referral criteria and patient pathways subgroup – January 2011 29
Appendix 5
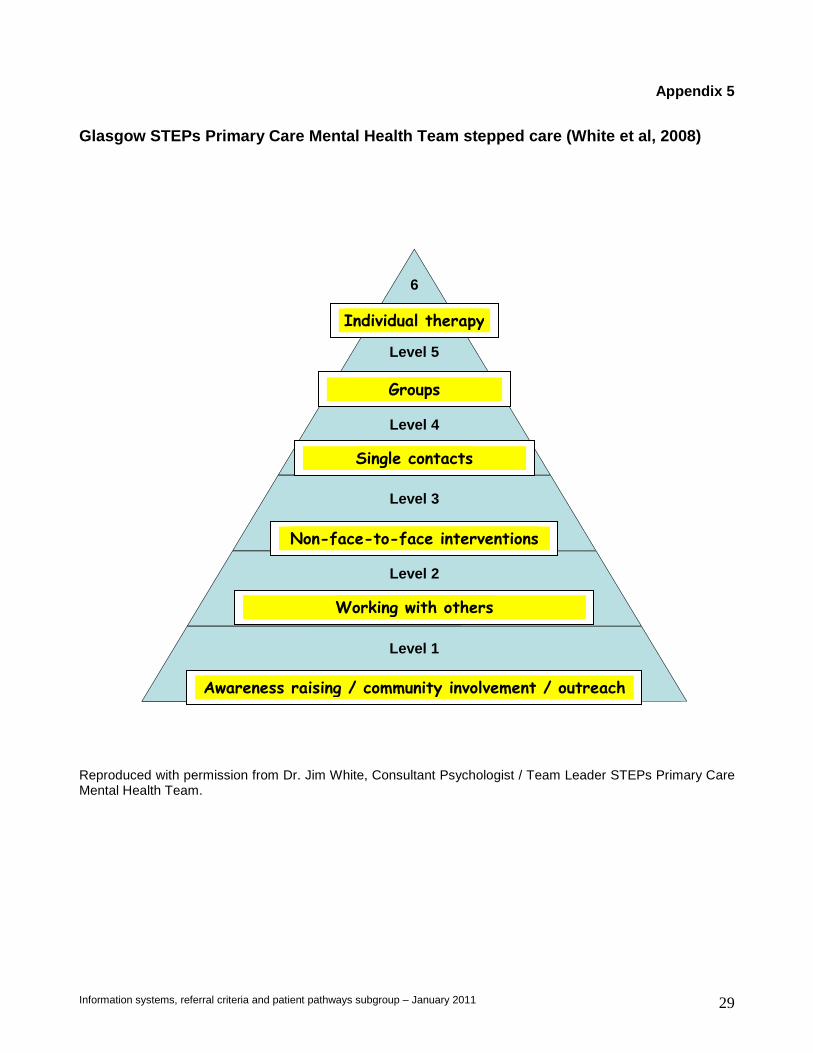
Glasgow STEPs Primary Care Mental Health Team stepp ed care (White et al, 2008)
Reproduced with permission from Dr. Jim White, Consultant Psychologist / Team Leader STEPs Primary Care Mental Health Team.
6
Level 5
Level 4
Level 3
Level 2
Level 1
Awareness raising / community involvement / outreach
Working with others
Non-face-to-face interventions
Groups
Single contacts
Individual therapy
Information systems, referral criteria and patient pathways subgroup – January 2011 30
Appendix 6 Mental Health in Scotland: A Guide to delivering ev idence based Psychological Therapies in Scotland – The Matrix)

Information systems, referral criteria and patient pathways subgroup – January 2011 31





























