Embed Size (px)
Citation preview
A Restorative CarePhilosophy in Acute Care
Barbara Resnick, PhD, CRNP, FAANUniversity of Maryland,School of Nursing
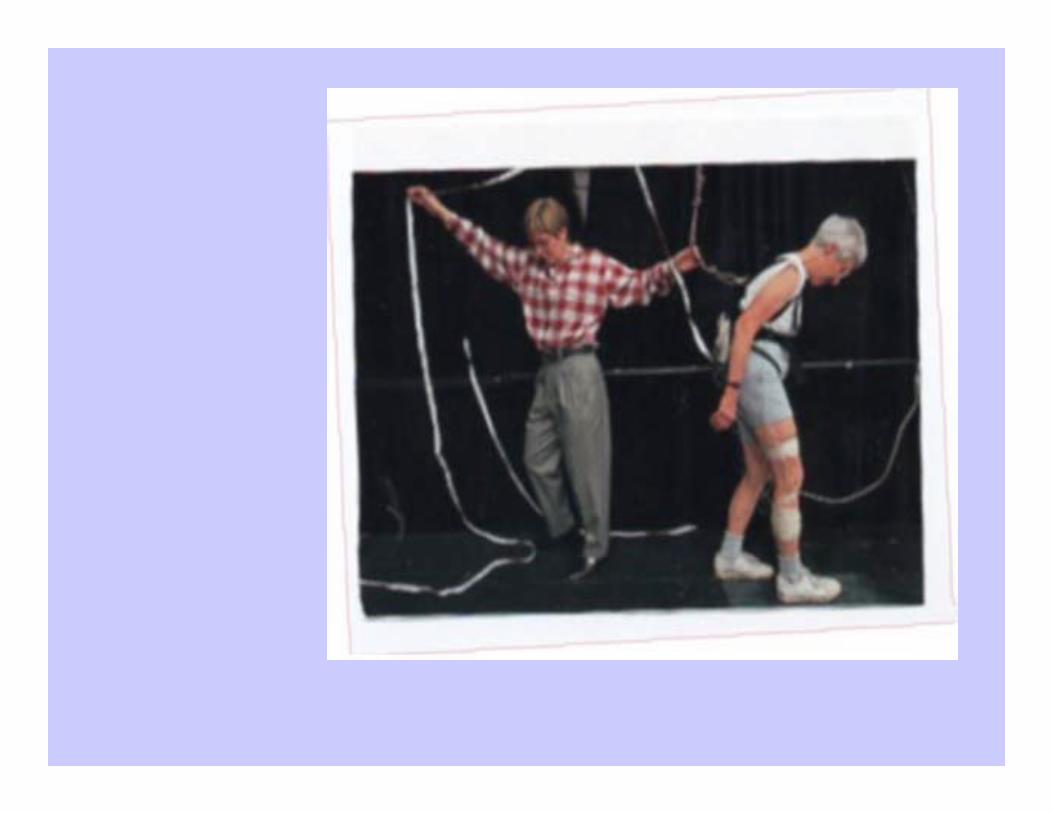
Why Should we Care????????♦Low mobility/bedrest prevalence is high in
hospitalized older adults– 23% of 3,500 patient days studied (Lazarus et
al., 2001)– 33% noted to be in bed or a chair on three
separate days (Warshaw et al., 1982)– Low mobility was noted in 16%of patients, and
intermediate mobility levels were present in 32%, and 52% had high mobility (nurse rated) (Brown et al., 2004)

Impact of Immoblity/Bedrest
♦Predict adverse outcome– 35-65% demonstrated decline in mobility from
admission to day 2 (Hirsh et al., 1990; Covinsky, 2003; Volpato, 2007; Wakefield, 2007)
– 29% showed decline in some ADL (Brown, Friedkin & Inouye, 2004)

Whose fault is this anyway?
– Patient– Family– System– Treatments– Provider
Patient ♦ Normal Age Changes/Disuse
– Sensory changes?– Cardiovascular changes?
Decreased CO stroke volume increased HR
– Decrease total muscle fiber and lean body mass atrophy and power decline
– Decreased pulmonary expansion increased residual and decrease po2
– Decreased plasma volume and total H2O
♦ Chronic Disease– Cognitive impairment– COPD– Arterial Insufficiency– Type II Diabetes– HTN/ASCVD– CVA– Afib– Orthopedic problems– DJD– Chronic disuse
The Patient Continues♦ Acute Event
– Cardiac– Infection– Orthopedic– Elective surgery – Pulmonary
♦ ADD BEDREST– 24-48 hrs decreases
plasma volume by 7% (500ml)
– One day results in 5% decrease in muscle strength
Family
♦Want to do something to help?????????♦Believe in the rest is best approach to acute
problems♦See the best way to a safe stay is the
protective tie in
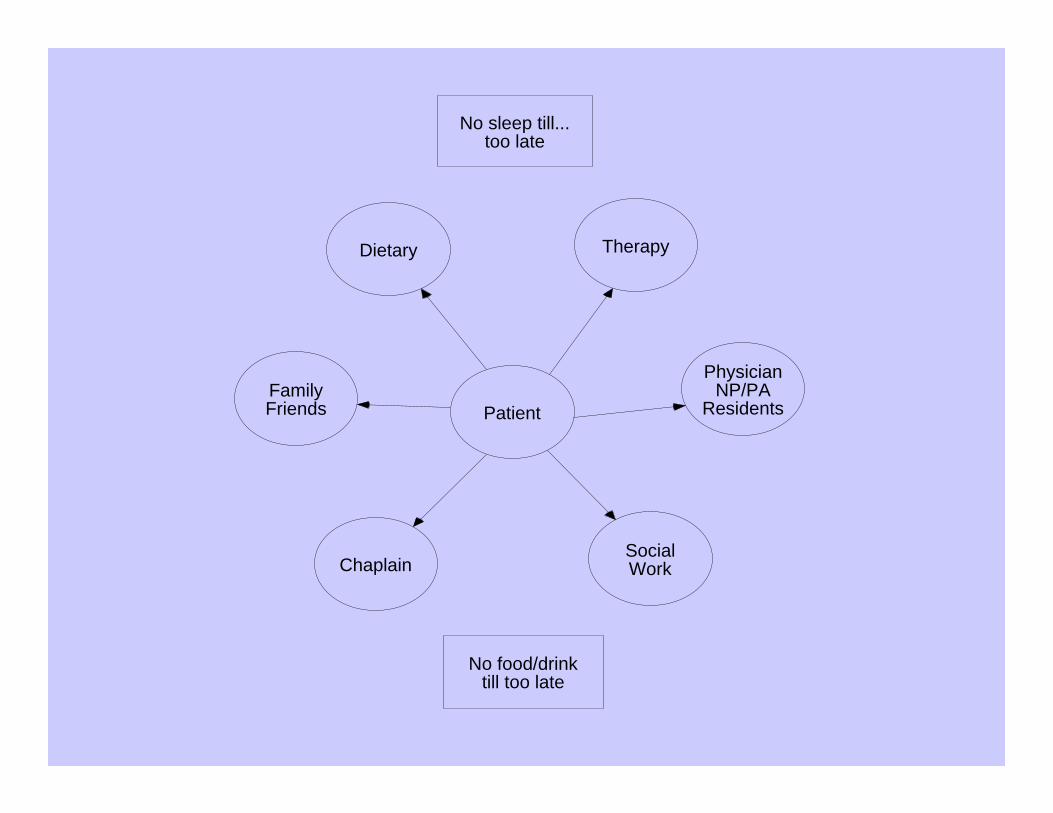
Patient
Dietary Therapy
PhysicianNP/PA
ResidentsFamilyFriends
ChaplainSocialWork
No sleep till...too late
No food/drinktill too late

Treatment
♦Xray: Wheelchair/stretcher entry only?♦Labs♦ Intravenous ♦NPO♦Procedure protocols♦Discharge opportunities: the final walk?
Provider♦The power of the pen♦The nursing unit opportunities…missed♦The fear of litigation♦The belief in rest to recovery???????????
What is Acute Care?
♦Saving Lives and Maintaining and Restoring Function….The New Mandate of Acute Care
♦OR: Using the Acute Event as a Stimulus to Change Behavior….The Missed Opportunity
PAY FOR PERFORMANCE…AN OPPORTUNITY

The Solution
♦Restorative Care????
Restorative Care
♦ the prevention of physical or psychosocial disability, and
♦ the maintenance and restoration of physical and psychological health so that the individual can live at his or her highest functional level.
Restorative Care
♦ Ideally is:– a comprehensive team effort – geared toward restoring the individual to
his or her highest function – maintaining or maximizing remaining
function– limiting future functional losses– ongoing
Restorative CareChange in Philosophy of Providing Care --
FROM A FOCUS ON PROVIDING CARE FOR PATIENTS/RESIDENTS TO…..HELPING PATIENTS/RESIDENTS TO OPTIMIZE THEIR UNDERLYING FUNCTION.
FROM A FOCUS ON PROVIDING CARE FOR PATIENTS/RESIDENTS TO…..HELPING PATIENTS/RESIDENTS TO OPTIMIZE THEIR UNDERLYING FUNCTION.
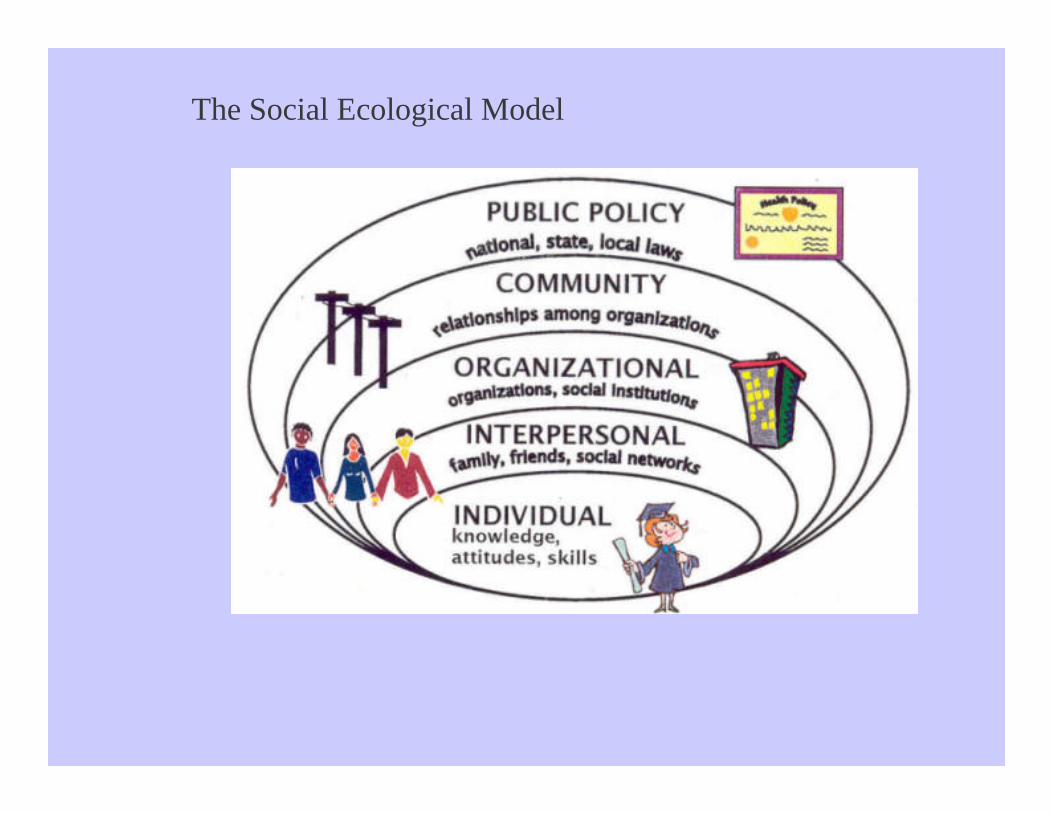
The Social Ecological Model

The Four Step ApproachStep I: Environmental and Relevant Policy AssessmentsStep II: Education/Mentoring Step III: Establishing Restorative Care GoalsStep IV: Documentation/Evaluation and Ongoing Work
Step I: Environment and Policy
♦Are there Policies/Job descriptions that are barriers???
♦Evaluate Person Environment Fit– Does the environment optimize what the
individual is able to do? – Can formally evaluate using the Housing
Enabler-INDOOR only– http://www.enabler.nu/
Step II: Education/Mentoring
♦Teaching a Philosophy…..YES YOU CAN!– What does function mean to the patient, to the
staff, to the family?– ALL must be involved with philosophy change
and discuss concerns/care related policies/priorities/what is reinforced.
– What are the benefits of activity for older adults?– What do the staff -nurses esp- really believe?
Do you believe you discharge folks home to do this?
A Four Week Series of Classes: Handouts?♦Class I: Establish the philosophy– what is
res care and why should we do it?– Define– Describe– Demonstrate outcomes





























