Embed Size (px)
Citation preview

INTRODUCTION Anti-angiogenic treatment for metastatic colorectal cancer (mCRC)Almost all malignant tumors are partially dependent on angiogenesis for tumor growth. Vascular endothelial growth factors (VEGFs) are key players in angiogenesis and thus, targeting the VEGF pathway in combination with chemotherapy is a common and effective treatment strate-gy.1 The VEGF family comprises of the cytokines, VEGF-A, VEGF-B, VEGF-C, VEGF-D and placental growth factor (PIGF), and their receptors, VEGFR-1, VEGFR-2, and VEGFR-3.2
Preclinical studies have shown that the VEGF family cytokines induce angiogenic response via interaction with their receptors leading to the activation of multiple pathways.3
The combination of chemotherapy plus bevacizumab, an antibody targeting specifically VEGF-A, is commonly used as the first-line treatment for patients with metastatic colorectal cancer (mCRC).4 However, most mCRC patients treated with bevacizumab, ultimately experi-ence disease progression.5 Preclinical evidence suggests that VEGF-B and PIGF can trigger the activation of other angiogenic pathways, which can compensate for the depletion of the VEGF-A levels.6 Thus, targeting a wider range of angiogenic factors could potentially be a more effective strategy in the second-line. However, this needs to be further validated in future clinical studies. Although the mechanism of resistance to bevacizumab in the first-line is still not well known, several studies have shown that the altered expression of various plasma and tissue biomarkers can be predictive of bevacizumab-resistance.7,8 In addition, it can also be instrumental in selecting the most effective second-line anti-angiogenic option. In case of patients who progress on first-line bevacizumab therapy, a significant upregulation of various cytokines, like VEGF-A, PIGF, bFGF, HGF and MMP-9, were observed prior to progression on bevacizumab therapy.7,8 It has also been observed that the expression of VEGFR-2, growth factor receptors involved in angiogene-sis, is enhanced during treatment with bevacizumab. Based on these elevated expression levels, these cytokines may act as biomarkers of resistance to therapeutic strategies involving anti-angio-genic agents like bevacizumab. In addition, they are also known to be associated with poor clini-cal outcomes. As anti-VEGF therapy forms an essential part of first- as well as second-line mCRC treatment strategy, identifying biomarkers of resistance to anti-angiogenic agents is of utmost importance.7,9
A Rational Sequencing of Anti-Angiogenic Agents as Second-Line Treatment Choice for mCRC Patients Progressing After a Bevacizumab-Based First Line
Sara De DossoOncology Institute of Southern Switzerland (IOSI), Bellinzona, Switzerland
healthbook TIMES Oncology Hematology
hb TIMES Onco Hema healthbook.ch March 18, 2020
REVIEW
ABSTRACT
A large proportion of patients with metastatic colorectal cancer (mCRC) experience disease progression after first-line treatment with chemotherapy and bevacizumab, an anti-angiogenic agent, as a result of acquired resistance. However, blocking angiogenesis by targeted therapy towards the vascular endothelial growth factor (VEGF) pathway still forms an essential part of the second-line treatment strategy. Although three approved evidence-based choices for angiogenic agents (continuing treatment with bevaci-zumab, ramucirumab and aflibercept) are currently available in the second-line, making the most effective choice is challenging due to the lack of studies directly comparing these agents. Moreover, despite huge investigational efforts, no predictive biomarker for anti-angiogenic cancer therapies could be identified so far.
Corresponding author: Dr Sara De DossoConsultant in Medical Oncology, Oncology Institute of Southern Swit-zerland (IOSI), Via Ospedale, 6500 Bellinzona, Switzerland. Email: [email protected].
DOI:10.36000/hbT.OH.2020.03.010 ISSN: 2673-2092 (Print) and 2673-2106 (Online)
This article was published on March 18, 2020
De Dosso et al. A Rational Sequencing of Anti-Angiogenic Agents as Second-Line Treatment Choice for mCRC Patients Progressing After a Bevacizumab-Based First Line. healthbook TIMES Onco Hema 2020;(3):14-19.
1414

Table 1. Biomarkers correlated with prior bevacizumab therapy at baseline. Adapted from Tabernero et al. 2017.17
Options for second-line anti-angiogenic therapyIn the case of mCRC patients, continuing treatment with anti-angiogenic agents after first progression is an option. In the second-line setting, there are three evidence-based alternatives, based on the results of three different phase III trials, i.e. bevaci-zumab beyond progression (ML18147 trial)10, ramucirumab (RAISE trial)11, and aflibercept (VELOUR trial).12 However, making the optimal choice is challenging due to the different eligibility criteria used in the ML18147 (also known as TML trials), RAISE and VELOUR trials and the lack of head-to-head comparisons of these three anti-angiogenic agents.13,14
The phase III ML18147 trial demonstrated the superiority of bevacizumab plus chemotherapy in comparison with chemo-therapy alone in the second-line treatment of mCRC patients (median overall survival [OS]: 11.2 vs 9.8 months HR: 0.81 [95% CI: 0.69−0.94]; p=0.0062).10 It is noteworthy that in this study, the chemotherapy backbone was switched between oxalip-latin-based and irinotecan-based chemotherapy in the sec-ond-line setting based on the first-line regimen used.10 In the phase III RAISE trial, ramucirumab, another anti-angiogenic agent, which binds to VEGF-D, was investigated in combination
with chemotherapy in mCRC patients who progressed during or after treatment with bevacizumab plus chemotherapy. The results of this study showed that the ramucirumab plus FOLFI-RI (folinic acid, fluorouracil and irinotecan) led to a significant improvement in the median OS (mOS: 13.3 vs 11.7 months HR: 0.844 [95% CI: 0.73−0.97] long-rank p=0.0219).11 Sim-ilarly, the phase III VELOUR trial demonstrated that the addi-tion of aflibercept to FOLFIRI provided a statistically signifi-cant benefit in terms of OS (13.50 vs 12.06 months HR: 0.817 [95.34% CI: 0.713−0.937], p=0.0032; intention-to-treat [ITT] population and progression-free survival (PFS) (6.90 vs 4.67 months HR: 0.758 [99.99% CI: 0.578−0.995], p=0.00007; ITT population) in oxaliplatin-pretreated mCRC patients, including those treated with bevacizumab (and other prespecified subgroups as well).
Several studies have shown that the altered expression levels of various plasma and tissue biomarkers can be instrumental in selecting the most effective second-line anti-angiogenic option. For example, high VEGF-D levels after progression on bevacizumab were shown to correlate with better response to ramucirumab in the RAISE trial.14,15
hb TIMES Onco Hema healthbook.ch March 18, 2020
REVIEW
healthbook TIMES Oncology Hematology 15

In addition, certain patient characteristics can also predict response to therapy. For instance, subgroup analyses in the ML18147 and VELOUR trials suggested that short progres-sion-free survival (PFS) in first-line therapy with bevacizumab can be used to select the optimal anti-angiogenic agent in the second-line setting.16
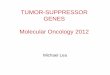
Aflibercept is an anti-angiogenic protein, comprising of key domains from the human VEGFR-1 and -2, fused with the Fc portion of the human immunoglobulin G. Unlike other anti-VEGF agents like bevacizumab (specific for VEGF-A) and ramucirumab (specific for VEGFR-2), aflibercept exhibits a wider binding range by blocking the interaction of different VEGF cytokines, including VEGF-A, VEGF-B, and PlGF with their receptors (Figure 1).13,16,17 Preclinical studies have shown that aflibercept is superior to bevacizumab irrespective of prior treatment status (i.e. with or without pretreatment with bevacizumab) by inducing a greater tumor response in mCRC animal models.4
PLASMA BIOMARKERS The current anti-angiogenic therapy is primarily based on blocking the VEGF-A pathway. However, acquired resist-ance to anti-VEGF-A therapy remains a major challenge.7,18
The results of the VELOUR study showed that aflibercept has consistent and good efficacy in mCRC patients pre-treated with oxaliplatin-based chemotherapy.12 A post hoc subgroup analysis of the VELOUR trial (n=533) showed that the expression levels of several plasma bio-markers, like VEGF-A and PIGF, implicated in angiogenesis
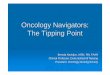
and correlated with resistance to bevacizumab, was altered after progression on bevacizumab therapy (Table 1).17 In par-ticular, increased expressions of VEGF-A, PIGF, serum amyloid P-component and C-reactive protein have been associated with acquired resistance to bevacizumab,7,8,19 while elevated levels of other biomarkers, like VEGF, T- cadherin and vitamin D binding protein, have been associ-ated with poor prognosis.8,20,21 From these, VEGF-A and PIGF, which have been shown to be involved in the mode of action of aflibercept, demonstrated the most significant change in expression levels (~ 5-fold and 2-fold increase in concentrations, respectively) (Figure 2A).17,22 These results further support the use of aflibercept in the second-line setting for mCRC patients who progressed on bevacizumab. The analysis of the effect of aflibercept treatment on the biomarker patient subgroup of the VELOUR trial revealed that patients with elevated VEGF-A and PIGF baseline levels were associat-ed with improved OS regardless of prior bevacizumab treat-ment (mOSVEGF-A: 11.9 vs 9.8 months, mOSPIGF: 11.5 vs 10.2 months) (Figure 2B).17,22 Thus, these findings suggest that VEGF-A and PIGF may be implicated in the mechanism of acquired resistance to bevacizumab and that aflibercept represents a viable option for patients who develop resistance to bevacizumab therapy.17
TISSUE BIOMARKERS In a follow-up retrospective study of the VELOUR trial23, tumor samples (482 out of 1,226 patients met all the sample collection criteria) were used to conduct biomarker analysis, in order to identify patient subgroups, which have a differen-tial response to therapy. Patient subgroups were determined based on certain genetic factors including the mutational sta-tus of RAS, KRAS and BRAF genes, and the location of the primary tumor (left-side of the colon vs right-side of the colon). Next-generation sequencing (NGS) assay of exon 2 for KRAS, exon 2, 3 and 4 for RAS and V600E for BRAF genes was used to analyze the mutational status, while the tumor location was extracted from the patient’s pathological report.12,23
Genetic tissue biomarkersBased on the NGS data, the patients were divided into the following subgroups (Figure 3A):
• KRAS exon 2 mutation (MUT)• KRAS wild-type (WT) • RAS mutation (MUT)• RAS wild-type (in the KRAS exon 2 gene or other KRAS- or NRAS genes) (WT)• BRAF V600E mutation (MUT)• wild-type (WT)
In this follow-up study, the tissue biomarker subgroups were representative of the intention-to-treat (ITT) population from the VELOUR trial (n=1,226) (HR: 0.82 [95% CI:
hb TIMES Onco Hema healthbook.ch March 18, 2020
A
B
healthbook TIMES Oncology Hematology
VEGFR-2
Regorafenib
Bevacizumab VEGF-A Aflibercept
VEGF-BPIGF-2
PIGF-1
VEGFR-1
Endothelial cell
Receptortyrosinekinase
Figure 1. Mechanism of action of aflibercept and bevacizumab. Adapted from Scartozzi et al. 20164 and Tang et al. 2013.35
1616

healthbook TIMES Oncology Hematology
0.71−0.93]), with respect to the therapeutic effect of afliber-cept (HR OS: 0.80 [95% CI: 0.65−0.99]; p=0.043), bevaci-zumab pretreatment status and overall patient characteristics.23
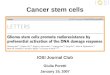
Based on OS data, there was a trend towards improved efficacy of aflibercept in the RAS wild type patient sub-group (KRAS: Ratio of HRwild-type/mutation [RoHR]: 1.21 [95% CI: 0.79–1.86]; p=0.38; RAS: RoHRwild-type/mutation: 1.39 [95% CI: 0.90–2.13; p=0.13]).23 Similar results were observed also for bevacizumab and ramucirumab. A trend showing reduced efficacy in the KRAS and RAS mutated patient subgroups was observed in case of these anti-angio-genic agents as well, which indicates that all three approved anti-angiogenic agents have comparable efficacy in these patient subgroups (Figure 3B).24–26 In case of the mutant patient subgroup (also RAS wild type), aflibercept treat-ment appears to induce a more pronounced survival benefit (RoHRwild-type/mutation: 0.49 [0.22–1.09]; p=0.08).23 In this analysis, the statistical interaction tests were negative for differential response to aflibercept therapy between the wild type and mutant patient subgroups with respect to OS and PFS. Collectively, none of the mutational subgroups demonstrated a statistically significant differential response to aflibercept treatment in the second-line (Figure 3C).
PRIMARY TUMOR LOCATION AS A BIOMARKERAbout 70% of colorectal cancer patients have a left-sided pri-mary colon tumor. The clinical impact of tumor location (i.e., right vs left side) was first shown in the phase III E2290 trial. This study demonstrated that patients with right- ver-sus left-sided primary tumors had poorer outcomes (mOS:
10.9 vs 15.8 months, p<0.001).27,28 Developmentally, the left and the right sides of the colon originate from different groups of cells, which renders tumors arising on the two sides to be considerably diverse, both molecularly as well as clini-cally.29 Several other studies have also confirmed that the location of the tumor has a significant impact on the progno-sis of the disease and may also be predictive of response to therapy.29–33 Consistent with this, the addition of cetuximab to chemotherapy in the first-line treatment of mCRC patients prolonged OS and PFS in patients with left-sided primary tumors compared with those having right-sided tumors, first-line treatment with bevacizumab plus chemo-therapy provided better outcomes in mCRC patients with right-sided tumors.29,31 Similar results were also observed with ramucirumab in the RAISE study, where ramucirumab led to better OS benefits in left-sided primary tumors.34 In the case of patients from the VELOUR trial, tumor sided-ness was analyzed based on their pathological reports (in 502 patients). Aflibercept efficacy was similar for patients with both left and right-side origin of tumors (HR OS left: 0.86 [0.64–0.15], right HR: 0.85 [0.53−1.35], interaction p-val-ue= 0.96; HR PFS left: 0.74 [0.46–1.00], right HR: 0.70 [0.42–1.15], interaction p-value = 0.69) (Figure 3C).23 A retrospective analysis of 198 mCRC patients from M.D. Anderson Cancer Center showed that right-sided tumors are also associated with other negative prognostic factors like age, consensus molecular subtypes (CMS) 1 and 3, microsat-ellite instability (MSI), and mutation status.32 However, more prospective studies are required to confirm that the location of the tumor can be used as a predictive biomarker for the selection of therapy in second-line setting.
hb TIMES Onco Hema healthbook.ch March 18, 2020
VEG
F-A
(pg/
mL)
PIG
F (p
g/m
L)
Priorbev
n=169
No priorbev
n=384
Priorbev
n=169
No priorbev
n=384
1500
1200
900
600
300
0
50
40
30
20
10
0
VELOUR ITT1 (N=1226)
VELOUR biomarker population(n=553)
VEGF-A >medianNo prior bev (n=135)
Prior bev (n=131)
PIGF>medianNo prior bev (n=81)
Prior bev (n=80)
mOS (95% CI)
13.5 (12.5-15.0) 12.1 (11.1-13.1)
12.7 (11.6-15.3) 11.3 (10.0-12.4)
13.0 (10.4-21.8) 9.4 (7.9-11.3)11.9 (10.0-15.9) 9.8 (7.4-12.3)
14.4 (10.7-25.6) 8.65 (5.2-11.9)11.5 (8.5-14.9) 10.2 (6.8-12.5)
Aflibercept Placebo
0 0.5 1 1.5HR (95% CI)
Figure 2. A) VEGF-A and PIGF levels at base-line according to prior treatment with bevacizumab. B) Median overall survival in patients with VEGF-A or PlGF above median (aflibercept versus placebo). Bev, bevacizumab. Adapted from Van Cutsem et al. 2017.22
REVIEW
A
B
healthbook TIMES Oncology Hematology 17

hb TIMES Onco Hema healthbook.ch March 18, 2020
Figure 3. A) Genetic factors and the corresponding subgroups.26 B) Aflibercept has similar efficacy in KRAS Exon 2 WT or MUT mCRC patients in compari-son with other anti-angiogenic gents.24–26 C) Retrospective analy-sis showing that aflibercept has similar efficacy across relevant patient subgroups.23
CONCLUSIONS
Colorectal cancer is one of the most prevalent cancers world-wide and a large proportion of patients with metastatic dis-ease undergo disease progression. Thus, it is important to plan effective later-line treatment strategies, which aim to prolong survival, manage symptoms and improve quality of life.4 Also, it is essential to identify which patients can poten-tially benefit from a specific treatment. In this regard, the identification of predictive plasma or tissue biomarkers rep-resents a clinically relevant approach. Analysis of plasma bio-
markers of patients who progressed after first-line bevaci-zumab treatment showed that resistance to this agent is associated with increased plasma levels of VEGF-A and PIGF, which are also targets of aflibercept, indicating that aflibercept could be a good treatment option for the sec-ond-line setting irrespective of prior Avenues to Precision Oncology treatment status. The retrospective analysis of the VELOUR trial illustrates that aflibercept is a good candidate for overcoming bevacizumab resistance in mCRC patients. However, future studies including larger patient populations are needed to confirm this effect.
A
B
C
healthbook TIMES Oncology Hematology
1818

healthbook TIMES Oncology Hematology
hb TIMES Onco Hema healthbook.ch March 18, 2020
1. Sun W. Angiogenesis in metastatic colorectal cancer and the benefits of targeted therapy. J Hematol Oncol. 2012; 5(1): 63. 2. Holmes DI et al. The vascular endothelial growth fac-tor (VEGF) family: angiogenic factors in health and dis-ease. Genome Biol. 2005; 6(2): 209. 3. Angelucci A et al. “Vessels in the Storm”: Searching for Prognostic and Predictive Angiogenic Factors in Colorectal Cancer. Int J Mol Sci. 2018; 19(1). 4. Scartozzi M et al. Aflibercept, a New Way to Target Angiogenesis in the Second Line Treatment of Metastatic Colorectal Cancer (mCRC). Targ Oncol. 2016; 11(4): 489–500. 5. Strickler JH et al. Bevacizumab-Based Therapies in the First-Line Treatment of Metastatic Colorectal Cancer. The Oncologist. 2012; 17(4): 513–24. 6. Brave SR et al. Placental growth factor neutralising antibodies give limited anti-angiogenic effects in an in vitro organotypic angiogenesis model. Angiogenesis. 2010; 13(4): 337–47. 7. Kopetz S et al. Phase II Trial of Infusional Fluorouracil, Irinotecan, and Bevacizumab for Metastatic Colorectal Cancer: Efficacy and Circulating Angiogenic Biomarkers Associated With Therapeutic Resistance. JCO. 2010; 28(3): 453–9. 8. Hayashi H et al. Biomarkers of reactive resistance and early disease progression during chemotherapy plus beva-cizumab treatment for colorectal carcinoma. Oncotarget. 2014; 5(9). 9. Somanath PR et al. Cooperation between integrin ανβ3 and VEGFR2 in angiogenesis. Angiogenesis. 2009; 12(2): 177–85. 10. Bennouna J et al. Continuation of bevacizumab after first progression in metastatic colorectal cancer (ML18147): a randomised phase 3 trial. The Lancet Oncology. 2013; 14(1): 29–37. 11. Tabernero J et al. Ramucirumab versus placebo in combination with second-line FOLFIRI in patients with metastatic colorectal carcinoma that progressed during or after first-line therapy with bevacizumab, oxaliplatin, and a fluoropyrimidine (RAISE): a randomised, dou-ble-blind, multicentre, phase 3 study. The Lancet Oncol-ogy. 2015; 16(5): 499–508. 12. Van Cutsem E et al. Addition of Aflibercept to Fluo-rouracil, Leucovorin, and Irinotecan Improves Survival in a Phase III Randomized Trial in Patients With Metastatic Colorectal Cancer Previously Treated With an Oxalipla-tin-Based Regimen. JCO. 2012; 30(28): 3499–506. 13. Lee JJ et al. Options for Second-Line Treatment in Metastatic Colorectal Cancer. Clinical Advances in
Hematology & Oncology. 2016; 14(1). 14. Modest DP et al. Treatment sequencing in metastatic colorectal cancer. Eur. J. Cancer. 2019; 109: 70–83. 15. Tabernero J et al. Analysis of angiogenesis biomarkers for ramucirumab efficacy in patients with metastatic colorectal cancer from RAISE, a global, randomized, double-blind, phase III study. Ann. Oncol. 2018; 29(3): 602–9. 16. Boku N et al. Selection of Second-line Anti-angio-genic Agents After Failure of Bevacizumab-containing First-line Chemotherapy in Metastatic Colorectal Can-cer. Clin Colorectal Cancer. 2018; 17(4): 251–4. 17. Tabernero J et al. Placental growth factor and the angiogenic environment based on analysis of baseline plasma biomarkers from the VELOUR trial. JCO. 2017; 35(4_suppl): 592–592. 18. Willett CG et al. Efficacy, safety, and biomarkers of neoadjuvant bevacizumab, radiation therapy, and fluoro-uracil in rectal cancer: a multidisciplinary phase II study. J. Clin. Oncol. 2009; 27(18): 3020–6. 19. Bottazzi B et al. The pentraxins PTX3 and SAP in innate immunity, regulation of inflammation and tissue remodelling. J. Hepatol. 2016; 64(6): 1416–27. 20. Martin P et al. Predicting response to vascular endothelial growth factor inhibitor and chemotherapy in metastatic colorectal cancer. BMC Cancer. 2014; 14: 887. 21. Lu KV et al. VEGF inhibits tumor cell invasion and mesenchymal transition through a MET/VEGFR2 com-plex. Cancer Cell. 2012; 22(1): 21–35. 22. Van Cutsem E et al. Impact of prior bevacizumab treatment on VEGFA and PlGF levels and patient out-comes: A retrospective analysis of baseline plasma sam-ples from the VELOUR trial. Annals of Oncology. 2017; 28(suppl_3). 23. Wirapati P et al. Velour trial biomarkers update: Impact of RAS, BRAF, and sidedness on aflibercept activity. JCO. 2017; 35(15_suppl): Abstract 3538. 24. Kubicka S et al. Bevacizumab plus chemotherapy continued beyond first progression in patients with metastatic colorectal cancer previously treated with bev-acizumab plus chemotherapy: ML18147 study KRAS subgroup findings. Ann. Oncol. 2013; 24(9): 2342–9. 25. Obermannová R et al. Subgroup analysis in RAISE: a randomized, double-blind phase III study of irinote-can, folinic acid, and 5-fluorouracil (FOLFIRI) plus ramucirumab or placebo in patients with metastatic colorectal carcinoma progression. Ann. Oncol. 2016; 27(11): 2082–90. 26. Ince WL et al. Association of k-ras, b-raf, and p53
status with the treatment effect of bevacizumab. J. Natl. Cancer Inst. 2005; 97(13): 981–9. 27. Ciombor KK et al. Primary Tumor Sidedness as Prog-nostic and Predictive Biomarker in Metastatic Colorectal Cancer: Further Validation of a Potentially Prac-tice-Changing Variable. JAMA Oncol. 2017; 3(2): 165. 28. O’Dwyer PJ et al. Fluorouracil modulation in colorectal cancer: lack of improvement with N -phospho-noacetyl- l -aspartic acid or oral leucovorin or interferon, but enhanced therapeutic index with weekly 24-hour infusion schedule--an Eastern Cooperative Oncology Group/Cancer and Leukemia Group B Study. J. Clin. Oncol. 2001; 19(9): 2413–21. 29. Tejpar S et al. Prognostic and Predictive Relevance of Primary Tumor Location in Patients With RAS Wild-Type Metastatic Colorectal Cancer: Retrospective Analy-ses of the CRYSTAL and FIRE-3 Trials. JAMA Oncol. 2017; 3(2): 194–201. 30. Loupakis F et al. Primary tumor location as a prog-nostic factor in metastatic colorectal cancer. J. Natl. Can-cer Inst. 2015; 107(3). 31. Venook AP et al. Impact of primary (1o) tumor loca-tion on overall survival (OS) and progression-free surviv-al (PFS) in patients (pts) with metastatic colorectal can-cer (mCRC): Analysis of CALGB/SWOG 80405 (Alliance). JCO. 2016; 34(15_suppl): 3504–3504. 32. Lee MS et al. Association of primary (1°) site and molecular features with progression-free survival (PFS) and overall survival (OS) of metastatic colorectal cancer (mCRC) after anti-epidermal growth factor receptor (αEGFR) therapy. JCO. 2016; 34(15_suppl): 3506–3506. 33. Arnold D et al. Prognostic and predictive value of primary tumour side in patients with RAS wild-type met-astatic colorectal cancer treated with chemotherapy and EGFR directed antibodies in six randomized trials. Ann. Oncol. 2017; 28(8): 1713–29. 34. Yoshino T et al. Biomarker analysis beyond angiogen-esis: RAS/RAF mutation status, tumour sidedness, and second-line ramucirumab efficacy in patients with meta-static colorectal carcinoma from RAISE—a global phase III study. Ann Oncol. 2019; 30(1): 124–31. 35. Tang PA et al. Aflibercept in the treatment of patients with metastatic colorectal cancer: latest findings and interpretations. Therap Adv Gastroenterol. SAGE Publi-cations Ltd STM; 2013; 6(6): 459–73.
TAKE-HOME MESSAGES
• Patients with metastatic colorectal cancer undergoing first-line bevacizumab therapy eventually develop dis-ease progression. Other anti-VEGF therapies, such as aflibercept and ramucirumab, may be given to patients as an alternative to bevacizumab.
• The identification of potential biomarkers to drive the selection of the most appropriate antiangiogenic drugs is a compelling need. In light of this, new studies are required to prospectively validate the role of predictive angiogenic biomarkers for a rational treatment allocation.
• High VEGF-A and PlGF serum levels may underlie development of resistance to bevacizumab. Aflibercept targets VEGF-A and PlGF with greater affinity than other anti-angiogenic therapies, and it may provide benefit to patients who have high VEGF-A or PlGF serum level and may be an effective second-line treat-ment for those with bevacizumab-induced resistance. Further studies are needed to clarify the importance of these biomarkers in guiding management of patients with colorectal cancer.
REVIEW
healthbook TIMES Oncology Hematology 19