Embed Size (px)
Citation preview

Journal of Investigative Surgery, 15:237± 243, 2002Copyright °c 2002 Taylor & Francis
0894-1939/02 $12.00 + .00DOI: 10.1080/08941930290086001
New Methodologies
A Rat Model for the Study of IntestinalHeterotopic Gastropathy
Maria Francelina Lopes, MD,MSc, and M. Ramos, MD
Department of Pediatric Surgery,Pediatric Hospital of Coimbra,Coimbra, Portugal
A. M. S. Cabrita, PhD,
and O. Carvalho, MSc
Center of Histophysiology,Experimental Pathology, andDevelopmental Biology, Schoolof Medicine, Universityof Coimbra, Coimbra, Portugal
J. A. B. PatrÂõcio, PhD
Laboratory of ExperimentalResearch of the UniversityHospital of Coimbra, Coimbra,Portugal
ABSTRACT This study analyzes an experimental model for the studyof reactions from gastric tissue exposed to enteric environment. Mor-phological studies were performed by histological, histochemical andimmunohistochemical methods, using formalin-� xed biopsies of full-wall-thickness gastric implants in a whole-wall jejunal defect. These graftssuffered severe lesions, characterized by chronic atrophic gastritis, fove-olar hyperplasia, glandular cystic transformation, and intestinal metapla-sia. Increase in acidic mucins was also observed. There was no proliferat-ing cell nuclear antigen (PCNA) overexpression. The results suggest thatthis model can be useful to investigate the heterotopic grastropathy andcan be applied in further research studies.
KEYWORDS ectopic gastric tissue, experimental model, full-thickness gastricpatch, heterotopic gastric tissue, histopathology, intestinal environment, seromusculargastric patch
In a hostile enteric microenvironment, gastric mucosa is continuouslyexposed to several noxa, such as enteric micro� ora and secretions.These attacks will probably induce a chain of reactions toward adap-
tive mucosal cytoprotection and, when repeated for long time, will causethe failure of mucosal defence mechanisms with permanent tissue dam-age [1].
Heterotopic gastric mucosa in intestine is frequently found in Meckel’sdiverticulum [2], occasionally in digestive duplications [3], and, rarely,as intestinal islets or polyps [4, 5]. According to Soderlund [6], a highrisk of peptic ulceration in Meckel’s diverticulum is correlated with anincreased measured area of gastric mucosa (1.2 cm2 or greater). It ispresumed that peptic ulceration arising from the presence of ectopicgastric mucosa in the mentioned malformations is due to the diges-tion of adjacent intestinal epithelium. Other reactions from gastric
Received 8 May 2001;accepted 13 February 2002.
The Portuguese Health MinistryCommittee for Investigation inHealthcare funded this research.
Address correspondence to MariaFrancelina Lopes, MD, Departmentof Surgery, Hospital Pedi Âatrico deCoimbra, 3000 Coimbra, Portugal.E-mail: [email protected]
237
J In
vest
Sur
g D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y T
he U
nive
rsity
of
Man
ches
ter
on 1
0/26
/14
For
pers
onal
use
onl
y.

New Methodologies
mucosa to enteric environment are yet insuf� cientlyunderstood, especially because experimental modelsand clinical studies are lacking [2, 7–9]. Thus, an ex-perimental model was developed by the authors tostudy tissue damage occurring after long exposure ofgastric tissue to the aforementioned environment.Histopathologic changes, pattern of mucin produc-tion, and information on cellular proliferation byproliferating cell nuclear antigen (PCNA) expressionare analyzed in the grafts.
Should this experimental model be reliable for thestudy of gastric tissue heterotopically implanted intointestine, further lines of research could be designed.
METHODS
Female Wistar rats, weighing an average of 211 §32 g, were housed according to the European UnionLaw on animal welfare. Before the surgery the ani-mals were fasted, only allowed free access to drinkingwater overnight.
Experimental Design
Rats were allocated randomly to receive a full-wall-thickness gastric patch (group I, n D 8), a mucosal-denuded gastric patch (group II, n D 13), or an inci-sion suture of jejunal wall defect (group III, n D 6).They were sacri� ced 6 months later.
Anesthesia and Surgery
Under anesthesia with intramuscular ketamine“cocktail” (ketamine 7.7–11 mg/kg C chlorpromazine3.8–5.8 mg/kg) a gastric antral � ap, pedicled onthe right gastroepiploic vessels, was tailored fromthe greater curvature of the stomach. A Heinecke–Mikulicz suture was used to close the gastric defect. Afull-thickness defect on the jejunum was then graftedwith this gastric patch.
The control group received a similar seromuscu-lar gastric � ap. Excision of the gastric mucosa wasaccomplished by injection, into the submucosa, of1 or 2 mL saline.
A second control group suffered suture of an in-cision in the jejunal wall.
Follow-Up
Body weight was registered before surgery, and onpostoperative days 7, 14, and 180. Rats were observeddaily for assessment of health status.
Processing of Specimens
In all animals a full necropsy was performed.Macroscopic aspect of the patched jejunum was reg-istered and biopsy specimens were obtained. Biop-sies were � xed in buffered formalin solution andstained with hematoxylin and eosin and Van Gieson,for histological examination. Specimens were eval-uated for the presence of in� ammation, atrophicmucosa, epithelial hyperplasia, intestinal metapla-sia, glandular cysts, � brosis, dysplasia, and ulcer. Asemiquantitative scoring system was used for each ofthe observed lesions: (¡) no lesions, (C) mild, (CC)moderate, and (CCC) severe grades.
Also two histochemical staining techniques, Al-cian blue-PAS (AB-PAS) and high-iron–diamine–Alcian blue (HID-AB), which differentiate neutralfrom sulfated and nonsulfated acid mucosubstances,were performed for studying qualitative changes inmucin patterns, according to the methods used byothers [10].
Cell proliferation was studied by immunohisto-chemistry using the streptavidin–biotin–peroxidasecomplex technique, as previously described [11].Brie� y, samples were dewaxed, hydrated, and rinsedin phosphate-buffered saline (PBS). Endogenousperoxidase was inhibited with 3% hydrogen perox-ide for 15 min at room temperature. Normal rabbitserum was applied for 30 min to reduce non-speci� c antibody binding. Sections were then in-cubated with the primary antibody (PCNA clonePC10; 1:100, DAKO-M0 879), for 120 min, at roomtemperature. A biotinylated rabbit anti-mouse im-munoglobulin (1:300, DAKO-E0 354) was added for45 min, at 30±C. After rinsing with PBS, peroxidase-labeled streptavidin (1:400) was added for 1 h atroom temperature. The sections were again rinsedwith PBS and a solution of diaminobenzidine tetra-hydrocloride (DAB, 0.02%) in 0.01% hydrogen per-oxide and 0.05 mol/L Tris-HCl solution (pH 7.60)was used as the peroxidase substrate. Nuclei were
238 M. F. LOPES ET AL.
J In
vest
Sur
g D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y T
he U
nive
rsity
of
Man
ches
ter
on 1
0/26
/14
For
pers
onal
use
onl
y.

New Methodologies
counterstained with Mayer’s hematoxylin. Positiveand negative controls were used.
PCNA-positive nuclei (dark brown) identi� ed im-munoreactivity. PCNA was classi� ed as follows: (¡)no reactive cells, (C) scattered positive cells, (CC)nests of positive cells, and (CCC) diffuse positivecells.
Histology was read by two of the authors; one ofthem did it in a blinded fashion.
Statistical Analysis
Numerical results are expressed as mean § stan-dard deviation. Data were analyzed by one-way anal-ysis of variance for quantitative variables and codedchi-square analysis of contingency tables for nom-inal variables. A value of p < .05 was accepted asstatistically signi� cant.
RESULTS
Follow-Up
Surgery was well tolerated. The overall survivalrate was 77.8%, without signi� cant statistical differ-ence among the groups; 2 rats died from sepsis due toanastomotic leak, 2 rats from intestinal obstruction,1 from hypovolemic shock, and 1 from aspiration of
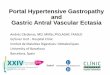
FIGURE 1 Full-thickness gastric patch showing epithelial atrophy (H&E, £40).
gastric contents. In all, 6 of 8 rats in group I, 10 in13 rats in group II, and 5 in 6 rats in group III sur-vived until the end de� ned for this experiment andwere available for study. Postoperative weight recov-ery was fast. Six months after surgery the percentageof increase in body weight was higher in animals ofgroup II and III than in those of group I, with statis-tical signi� cance.
Macroscopic Findings
The patched jejunum, presenting as tumorlike,showed more intense adhesions in group I than inthe controls. The inner surface of the graft appearedirregular, with scattered polyps and ulcers. Ulcerswere also seen in the adjacent jejunum.
Histological Assessment
Chronic atrophic gastritis, characterized bymucosal in� ammation with progressive glandularatrophy (Figure 1) and sometimes complete epithe-lial destruction, was observed in 6=6 (100%) full-wall-thickness gastric grafts. Additionally, foveolarhyperplasia was seen in 4=6 (66.6%), cystic glandu-lar dilatation with disturbance of normal architec-ture of the glandular epithelium (Figure 2) in 5=6(83.3%), intestinal metaplasia in 5=6 (83.3%), and
EXPERIMENTAL STUDY OF HETEROTOPIC GASTROPATHY 239
J In
vest
Sur
g D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y T
he U
nive
rsity
of
Man
ches
ter
on 1
0/26
/14
For
pers
onal
use
onl
y.

New Methodologies
FIGURE 2 Full-thickness gastric patch showing glandular cystic dilatation (H&E, £40).
� brosis of the muscular coat in 6=6 (100%) of thegrafts. These lesions showed a patchy distributionwith several degrees of severity, ranging from mildto severe, and some of them coexisted in the samespecimen (Table 1).
In� ammatory in� ltration and erosions, character-ized by partial loss of villi and glands, were consis-tent � ndings in the adjacent jejunum, especially in itscon� uence with the graft. In two of these specimens(33.3%) an ulcer was also identi� ed. The ulcers hadbenign appearance and were con� ned to the submu-cosa without attainment of the muscular coat.
The severe lesions observed in the patched je-junum by a full-thickness gastric � ap were opposedto a “near-normal” microscopical appearance in thecontrol groups. The seromuscular patches became
TABLE 1 Grades of severity of histological lesions in full-wall-thickness gastric grafts (n D 6)
Cases In� . in� l. Atrophic m. Absent m. Fov. hyp. Int. met. Cysts Fibrosis
1 C C ¡ CC C CC C2 CCC C CCC ¡ CCC ¡ CC3 CC CC ¡ C CC CCC C4 CCC CC C C C CCC CCC5 CC CC ¡ ¡ ¡ C CC6 CCC CC CCC C C CC CC
Note. Inf. in�l., in�ammatory in�ltrate; atrophic m., atrophic gastric mucosa; absent m., absent gastric mucosa; fov. hyp., foveolar hyperplasia;int. met., intestinal metaplasia; (¡) no lesions; (C) mild; (CC) moderate and (CCC) severe grades.
lined by neomucosa, similar to the adjacent jejunum(Figure 3), and there were no remarkable lesions inthe gastric coat–neomucosa complex, except for fo-cally mild submucosal � brosis. The neighboring in-testine also showed a normal appearance.
Concerning mucosubstances, group I showed vari-able aspects. Cysts were � lled with mucus. The neu-tral mucin of the gastric mucosa disappeared (1=6),was maintained (3=6), or diminished (2=6). Somegrafts showed it associated or replaced predominantlyby sialomucin (4=6) or by sulfomucin (2=6) (Figure 4,A and B).
A few scattered immunoreactive cells were ob-served in the mesenchyme of the grafts, in group I.Additionally, also sparse foci of PCNA cell nests sur-rounded glandular cysts (3=6). These aspects were
240 M. F. LOPES ET AL.
J In
vest
Sur
g D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y T
he U
nive
rsity
of
Man
ches
ter
on 1
0/26
/14
For
pers
onal
use
onl
y.

New Methodologies
FIGURE 3 Seromuscular gastric patch was covered by intestinal epithelium on postoperative day 180 (H&E, £100).
FIGURE 4 Full-thickness gastric patch implanted into the jejunum showing sulfomucin increase (A) when compared with thecontrol (B) (diamines, £200).
EXPERIMENTAL STUDY OF HETEROTOPIC GASTROPATHY 241
J In
vest
Sur
g D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y T
he U
nive
rsity
of
Man
ches
ter
on 1
0/26
/14
For
pers
onal
use
onl
y.

New Methodologies
similar to the ones observed in the controls, withgroup II showing the immunoreactivity nests pre-dominantly in the graft–jejunal union and group IIIin the suture line.
DISCUSSION
Very few clinical and experimental studies havefocused on the morphological aspects observed inheterotopic gastropathy [2, 12–13].
In the present work a model for the study of het-erotopic gastric tissue into intestinal environmentwas developed. Our model proved to be easily feasi-ble and successful, with low mortality.
The observed severe microscopic damage in groupI (full-wall-thickness gastric grafts) re� ects the effectsof an intense hostile environment on the exposedgastric mucosa. Numerous irritants are surelyinvolved. Raised pH and digestive enzymes of en-teric secretions, gastrotoxic mucosal bacteria presentin intestinal � ora, and the surgery itself are probablythe most important causes for the majority of thelesions. Additionally, in� ammation, erosion, and ul-cer surrounding the heterotopic gastric mucosa wereexpected, anticipating the deleterious effects of acidand pepsin on intestinal mucosa. Based on our re-sults in group II, removing the epithelial gastric lin-ing will protect the adjacent intestine against pepticinjury.
Our model seems to reproduce some of the le-sions reported by the Cserni histological studies ofMeckel’s diverticula containing heterotopic gastricmucosa [2, 12]. Similarly to these investigations, hy-perplasia and chronic atrophic gastritis, of the re-� ux type of gastritis or gastropathy, were amongthe most predominant lesions seen in our grafts. In-testinal metaplasia, often present in our model, wasalso a relevant � nding in the experimental model ofgastric exposure to enteric environment developedby Li and coworkers [13]. Cystic transformation ofthe heterotopic gastric epithelium, a lesion not re-ported by other authors, was additionally, with thealready reported histological lesions, a prominentfeature in our cases. It is likely that its pathogene-sis has some relationship with focal hemorrhage and
infarction, probably due to the surgical procedure.These changes would provoke damage in muscu-lar layers, which would facilitate the epithelial mi-gration towards the subserosa. This phenomenonhas been mentioned also in jejunitis cystica pro-funda [14], an entity characterized by downgrowthof small-intestinal epithelium with continuous mu-cus production.
The study of mucin allows a distinction betweentwo different types of intestinal metaplasia [15]. Oneof them is of a more mature type (small-intestinaltype or complete intestinal metaplasia) and showsneutral mucin of gastric mucosa replaced by sialo-mucin. The other is the incomplete type or “colonic”metaplasia, in which neutral mucin is replaced bysulfomucin. This latter is linked to a more advanceddisturbance.
The secretion of sulfomucins by the full-wall-thickness gastric graft may represent an important cy-toprotective mechanism. First, it is known that bilesalts disrupt the normal gastric mucosal barrier toion diffusion by decreasing the viscosity of mucusand that sufomucins may be more resistant to thiseffect. Second, an adapted cell, by its production ofsulfomucins, is able to survive and proliferate in thepresence of a carcinogenic microenvironment (e.g.,presence of bile, raised pH), while normal cells wouldbe destroyed or their division would be inhibited. Fi-nally, neoplastic clones, which are protected by thesecretion of sulfomucin, may be better able to resistpeptic digestion, because sulfate groups may assistalso in the inactivation of pepsin [15].
Dysplasia, intestinal metaplasia especially of the“colonic” type, and chronic atrophic gastritis are re-garded as precancerous. However, not all premalig-nant lesions will necessarily transform into cancers.Supporting this theory are, � rst, the extremely rareevents of malignant tumors developed in congeni-tal heterotopic gastric mucosa [16], and second, theabsence of immunoreactivity overexpression in ourantiproliferating cell nuclear antigen study.
Proliferating cell nuclear antigen is a marker ofcell proliferation that has evidenced deregulated ex-pression in gastric cancer [17]. A monoclonal anti-body to PCNA, a murine immunoglobulin G(IgG)obtained from Dako Corporation, enables detection
242 M. F. LOPES ET AL.
J In
vest
Sur
g D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y T
he U
nive
rsity
of
Man
ches
ter
on 1
0/26
/14
For
pers
onal
use
onl
y.

New Methodologies
of nuclear antigen in paraf� n embedded tissues.However, some problems can be found using thistype of specimen. A partial loss of antigenicity ofPCNA can occur, especially if tissue � xation sur-passes 48 h [18]. Although knowing the relatedproblems from PCNA application to formalin-� xedembedded paraf� n tissue [18, 19], we consider ourresults, showing an absence of signi� cant PCNAoverexpression, to be a true representation of theprocess: � rst, because we took all the recommendedprecautions to avoid loss of antigenicity of PCNA,and second, because there was a positive correlationbetween PCNA immunoreactivity results and thepresence in the graft of histological factors pointingtoward the absence of malignant transformation.
All these facts suggest that this experimentalmodel is reliable for the study of histopathologyfrom heterotopic gastric tissue into intestinal envi-ronment. Future applications could be further antic-ipated, namely, its use for adjacent intestinal tissuedamage characterization, study of the mechanismsof adaptive mucosal cytoprotection, and study ofcytoprotective drugs or damaging agents.
REFERENCES
1. Konturek PC. Physiological, immunohistochemical andmolecular aspects of gastric adaptation to stress, aspirinand to H. pylori-derived gastrotoxins. J Physiol Pharmacol.1997;48:3–42.
2. Cserni G. Gastric pathology in Meckel’s diverticulum. Re-view of cases resected between 1965 and 1995. Am J ClinPathol. 1996;106:782–785.
3. Karnak I, Ocal T, Senocak ME, Tanyel FC,Buyukpamukcu N. Alimentary tract duplications inchildren: Report of 26 years’ experience. Turk J Pediatr.2000;42:118–125.
4. Nowak M, Deppisch L. Giant heterotopic gastric polypin the jejunum. Arch Pathol Lab Med. 1998;122:90–93.
5. Turck D, Bonnevalle M, Gottrand F, Farriaux JP. Intra-operative endoscopic diagnosis of heterotopic gastric
mucosa in the ileum causing recurrent acute intussuscep-tion. J Pediatr Gastroenterol Nutr. 1990;11:275–278.
6. Soderlund S. Meckel’s diverticulum, a clinical and histo-logic study. Acta Chir Scand. 1959;248:13–233.
7. de-Cothi GA, Newbold KM, Oconnor HJ. Campylobacter-like organisms and heterotopic gastric mucosa in Meckel’sdiverticula. J Clin Pathol. 1989;42:132–134.
8. Fich A, Talley NJ, Shorter RG, Phillips SF. Does Helicobacterpylori colonize the gastric mucosa of Meckel’s diverticu-lum? Mayo Clin Proc. 1990;65:187–191.
9. Stermer E, Hardoff D, Zuckerman E, Miselevich I. Heli-cobacter pylori-associated peptic ulcer in heterotopic gas-tric mucosa within ileal duplication. J Clin Gastroenterol.1994;18:133–135.
10. Sheahan DG, Jervis HR. Comparative histochem-istry of gastrointestinal mucosubstances. Am J Anat.1976;146:103–131.
11. Hsu SM, Raine L, Fangar H. Use of avidine-biotin peroxi-dase complex (ABC) in immmunoperoxidase techniques:A comparison between ABC and unlabeled antibody (PAP)procedure. J Histochem Cytochem. 1981;29:577–580.
12. Cserni G. Proliferative epithelial changes in ectopic gas-tric mucosa of Meckel’s diverticula. Pathol Onc Res.1998;4:130–134.
13. Li C, Liu W, Fang D. Histological and electron-microscopicobservations on the mucosa of pediculated gastric wallgraft transplanted to the intestines in Wistar rats. ChinMed J (Engl). 1996;109:77–82.
14. Spjut HJ, Helgason AH, Trabanino JG 2d Jejunitis cysticaprofunda in a hamartomatous polyp. Report of a case.Am J Surg Pathol. 1987;11:328–332.
15. Jass JR, Strudley I, Faludy J. Histochemistry of epithelialmetaplasia and dysplasia in human stomach and colorec-tum. In: Polak JM, Bloom SR, Wright NA, Butler AG, eds.Basic science in Gastroenterology. Diseases of the Gut.London, UK: Glaxo Group Research Limited. Royal Post-graduate Medical School; 1986:109–130.
16. Caruso ML, Marzullo F. Jejunal adenocarcinoma in con-genital heterotopic gastric mucosa. J Clin Gastroenterol.1988;10:92–94.
17. Jain S, Filipe MI, Hall PA, Waseem M, Lane DP, Levison DA.Prognostic value of proliferating cell nuclear antigen ingastric carcinoma. J Clin Pathol. 199;44:655–659.
18. Matsuno Y, Mukai K. Proliferating cell nuclear antigen(PCNA). Byori-To-Rinsyo. 1991;9:879–883.
19. McCormick D, Yu C, Hobbs C, Hall PA. The relevanceof antibody concentrations to the immunohistologicalquanti�cation of cell proliferation-associated antigens.Histopathology. 1993;22:543–547.
EXPERIMENTAL STUDY OF HETEROTOPIC GASTROPATHY 243
J In
vest
Sur
g D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y T
he U
nive
rsity
of
Man
ches
ter
on 1
0/26
/14
For
pers
onal
use
onl
y.