Embed Size (px)
Citation preview
ELS EVI E R Clinical Eye and Vision Care 11 (1999) 199-206 www.elsevier.com/locate/clineyeviscare
Resident essay, first runner up for the John Asarkof, O.D. award
A rare ocular manifestation of non-Hodgkins’ lymphoma
Michael S. Peterson, O.D.”, Lori S. Kinvan, O.D.
VA Connecticut Healthcare System West Haven Campus, West Haven, CT, USA
Accepted 9 August 1999
Abstract
Non-Hodgkins’ lymphoma is a multisystem neoplasm that can affect the eye. Both central nervous system non-Hodgkins’ lymphoma and systemic non-Hodgkins’ lymphoma demonstrate intraocular lymphoma, although different ocular involvement patterns are observed. Ocular inflammation is common with these tumors and presents a diagnostic challenge to clinicians who discover assumed idiopathic uveitis in older patients which is refractory to steroid treatment. This paper includes a case report with an unusual retinal manifestation of intraocular lymphoma secondary to systemic non-Hodgkins’ lymphoma. 0 1999 Elsevier Science Ireland Ltd. All rights reserved.
Keywords: Non-Hodgkins’ lymphoma; Intraocular lymphoma; Uveitis; Vitritis; Choroidal infiltrate; Retinal infiltrate
1. Introduction
Lymphomas represent a group of diseases that are the result of abnormal developmental arrest and clo- nal proliferation of B or T lymphocytes. Thomas Hodgkins first described lymphomas in 1832, when he studied the enlarged lymph nodes of patients with a rapidly terminal condition. At this time, these lym- phomas were named Hodgkins’ disease, but it was then discovered that some lymphomas contained multinucleated Reed-Sternberg giant cells and others did not. Those without these specialized cells were thus named non-Hodgkins’ lymphomas (NHL). Patients with NHL have a wide variety of signs and symptoms, depending on the site of involvement. Many organs in the body may be affected, including the eye.
Intraocular lymphoma is an uncommon tumor and
* Corresponding author. Tel.: + 1-734-994-4471. E-mail address: [email protected] (M.S. Peterson)
is separated into three categories: primary intraocular lymphoma in isolation; lymphoma confined to the eye and central nervous system; and secondary intraocu- lar lymphoma from systemic NHL. Although rare, the incidence of these neoplasms is rising due to in- creased survival time as a result of advances in treat- ment. Lymphomas may involve the eye before or after affecting the rest of the body. The clinical significance of initial ocular involvement of these malignancies is the fact that greater than 90% herald the presence or development of extraocular lymphomas [ 11. Intraocu- lar lymphoma is an ocular manifestation of NHL that can masquerade as chronic uveitis, especially in patients over the age of 60.
2. Case report
An 80-year-old Caucasian male presented to the Eastern Blind Rehabilitation Center at the West Haven VA Medical Center for optometric evaluation
0953-4431/99/$ - see front matter 0 1999 Elsevier Science Ireland Ltd. All rights reserved. PII: S 0 9 5 3 - 4 4 3 1 ( 9 9 ) 0 0 0 3 5 - 1
200 M.S. Peterson, L.S. finvan /Clinical Eye and Vuion Cave 11 (1999) 199-206
and training in areas of low vision, orientation and mobility and activities of daily living. Ocular history was significant for legal blindness secondary to exuda- tive age-related macular degeneration (AMD) O.U. and ischemic branch retinal vein occlusion O.D., which occurred 8 years earlier. There was no history of eye trauma or surgery and episodes of pain and diplopia were denied. Medical history was significant for hy- pertension, chronic pulmonary obstructive disease, benign prostatic hypertrophy and sensorineural hear- ing loss. Medications included triamterene, hydro- chlorothiazide and fosinopril. An allergy to sulfa ex- isted. The patient had goals for visual rehabilitation that included reading the newspaper, photography, improved mobility skills and overall increased inde- pendence.
Best corrected visual acuities were O.D. 10/80, eccentrically viewing to 5 o'clock and O.S. 10/120 + eccentrically viewing to 9 o'clock. Visual function was optimal under dim illumination. Pupils were equally round and reactive to light in dim and bright illumina- tion with no afferent pupillary defect O.U. Extraocu- lar motilities were full and unrestricted without diplopia O.U. The bulbar conjunctiva had three dif- fuse petechial hemorrhages O.D. The corneas demon- strated endothelial pigment O.D. > O.S. The iris and anterior chamber were healthy O.U. without cells and flare. Applanation tonometry yielded pressures of 11 mmHg O.U.
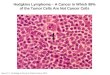
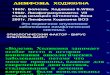
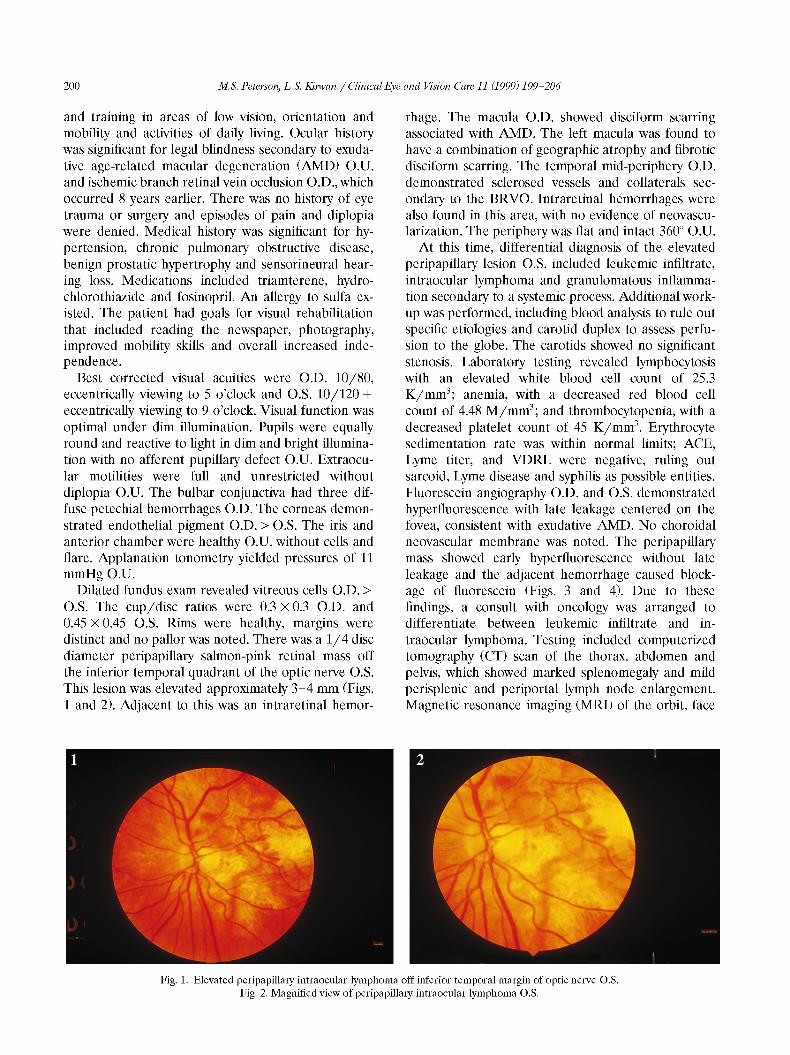
Dilated fundus exam revealed vitreous cells O.D. > O.S. The cup/disc ratios were 0.3 x 0.3 O.D. and 0.45 x 0.45 O.S. Rims were healthy, margins were distinct and no pallor was noted. There was a 1/4 disc diameter peripapillary salmon-pink retinal mass off the inferior temporal quadrant of the optic nerve O.S. This lesion was elevated approximately 3-4 mm (Figs. 1 and 2). Adjacent to this was an intraretinal hemor-
rhage. The macula O.D. showed disciform scarring associated with AMD. The left macula was found to have a combination of geographic atrophy and fibrotic disciform scarring. The temporal mid-periphery O.D. demonstrated sclerosed vessels and collaterals sec- ondary to the BRVO. Intraretinal hemorrhages were also found in this area, with no evidence of neovascu- larization. The periphery was flat and intact 360" O.U.
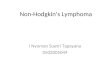
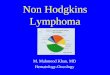
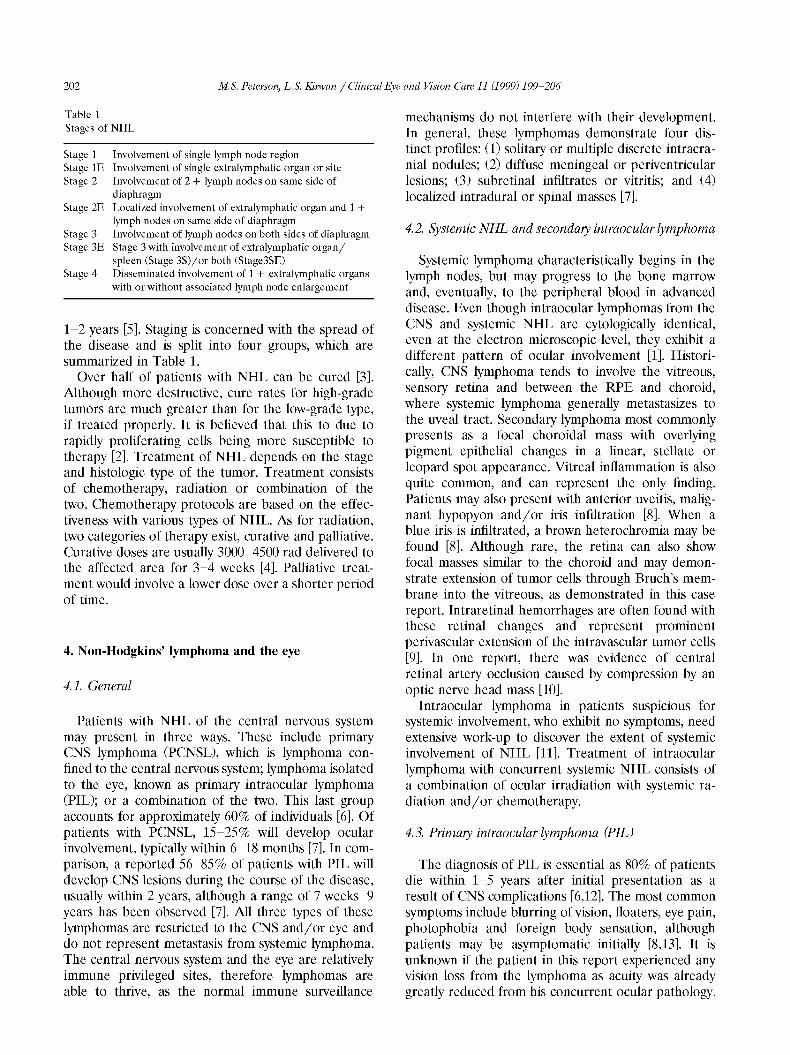
At this time, differential diagnosis of the elevated peripapillary lesion O.S. included leukemic infiltrate, intraocular lymphoma and granulomatous inflamma- tion secondary to a systemic process. Additional work- up was performed, including blood analysis to rule out specific etiologies and carotid duplex to assess perfu- sion to the globe. The carotids showed no significant stenosis. Laboratory testing revealed lymphocytosis with an elevated white blood cell count of 25.3 K/mm3; anemia, with a decreased red blood cell count of 4.48 M/mm3; and thrombocytopenia, with a decreased platelet count of 45 K/mm3. Erythrocyte sedimentation rate was within normal limits; ACE, Lyme titer, and VDRL were negative, ruling out sarcoid, Lyme disease and syphilis as possible entities. Fluorescein angiography O.D. and O.S. demonstrated hyperfluorescence with late leakage centered on the fovea, consistent with exudative AMD. No choroidal neovascular membrane was noted. The peripapillary mass showed early hyperfluorescence without late leakage and the adjacent hemorrhage caused block- age of fluorescein (Figs. 3 and 4). Due to these findings, a consult with oncology was arranged to differentiate between leukemic infiltrate and in- traocular lymphoma. Testing included computerized tomography (CT) scan of the thorax, abdomen and pelvis, which showed marked splenomegaly and mild perisplenic and periportal lymph node enlargement. Magnetic resonance imaging (MRI) of the orbit, face
Fig. 1. Elevated peripapillary intraocular lymphoma off inferior temporal margin of optic nerve O.S. Fig. 2. Magnified view of peripapillary intraocular lymphoma 03.
M.S. Peterson, L.S. finvan /Clinical Eye and Vuion Cave 11 (1999) 199-206 201
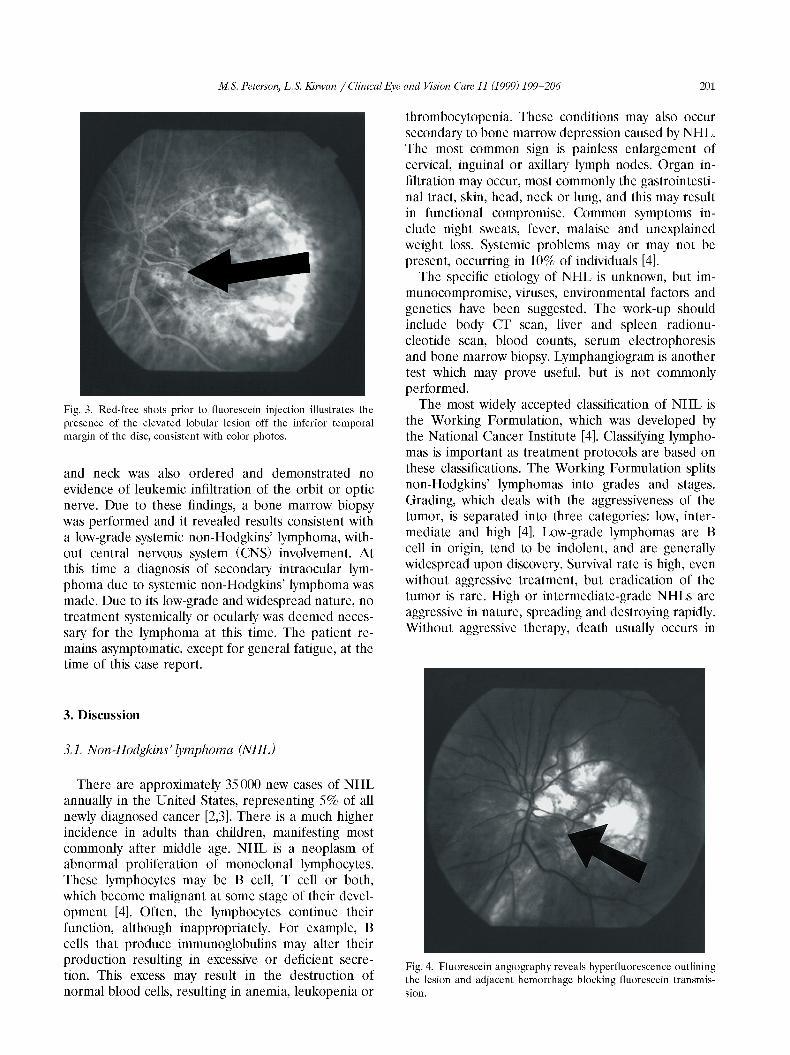
Fig. 3. Red-free shots prior to fluorescein injection illustrates the presence of the elevated lobular lesion off the inferior temporal margin of the disc, consistent with color photos.
and neck was also ordered and demonstrated no evidence of leukemic infiltration of the orbit or optic nerve. Due to these findings, a bone marrow biopsy was performed and it revealed results consistent with a low-grade systemic non-Hodgkins’ lymphoma, with- out central nervous system (CNS) involvement. At this time a diagnosis of secondary intraocular lym- phoma due to systemic non-Hodgkins’ lymphoma was made. Due to its low-grade and widespread nature, no treatment systemically or ocularly was deemed neces- sary for the lymphoma at this time. The patient re- mains asymptomatic, except for general fatigue, at the time of this case report.
3. Discussion
3.1. Non-Hodgkins’ lymphoma (NHL)
There are approximately 35000 new cases of NHL annually in the United States, representing 5% of all newly diagnosed cancer [2,3]. There is a much higher incidence in adults than children, manifesting most commonly after middle age. NHL is a neoplasm of abnormal proliferation of monoclonal lymphocytes. These lymphocytes may be B cell, T cell or both, which become malignant at some stage of their devel- opment [4]. Often, the lymphocytes continue their function, although inappropriately. For example, B cells that produce immunoglobulins may alter their production resulting in excessive or deficient secre- tion. This excess may result in the destruction of normal blood cells, resulting in anemia, leukopenia or
thrombocytopenia. These conditions may also occur secondary to bone marrow depression caused by NHL. The most common sign is painless enlargement of cervical, inguinal or axillary lymph nodes. Organ in- filtration may occur, most commonly the gastrointesti- nal tract, skin, head, neck or lung, and this may result in functional compromise. Common symptoms in- clude night sweats, fever, malaise and unexplained weight loss. Systemic problems may or may not be present, occurring in 10% of individuals 141.
The specific etiology of NHL is unknown, but im- munocompromise, viruses, environmental factors and genetics have been suggested. The work-up should include body CT scan, liver and spleen radionu- cleotide scan, blood counts, serum electrophoresis and bone marrow biopsy. Lymphangiogram is another test which may prove useful, but is not commonly performed.
The most widely accepted classification of NHL is the Working Formulation, which was developed by the National Cancer Institute [4]. Classifying lympho- mas is important as treatment protocols are based on these classifications. The Working Formulation splits non-Hodgkins’ lymphomas into grades and stages. Grading, which deals with the aggressiveness of the tumor, is separated into three categories: low, inter- mediate and high [4]. Low-grade lymphomas are B cell in origin, tend to be indolent, and are generally widespread upon discovery. Survival rate is high, even without aggressive treatment, but eradication of the tumor is rare. High or intermediate-grade NHLs are aggressive in nature, spreading and destroying rapidly. Without aggressive therapy, death usually occurs in
Fig. 4. Fluorescein angiogaphy reveals hyperfluorescence outlining the lesion and adjacent hemorrhage blocking fluorescein transmis- sion.
202 M.S. Peterson, L.S. finvan /Clinical Eye and Vuion Cave 11 (1999) 199-206
Table 1 Stages of NHL
Stage 1 Involvement of single lymph node region Stage 1E Involvement of single extralymphatic organ or site Stage 2 Involvement of 2 + lymph nodes on same side of
diaphragm Stage 2E Localized involvement of extralymphatic organ and 1 +
lymph nodes on same side of diaphragm Stage 3 Involvement of lymph nodes on both sides of diaphragm Stage 3E Stage 3 with involvement of extralymphatic organ/
spleen (Stage %)/or both (Stage3SE) Stage 4 Disseminated involvement of 1 + extralymphatic organs
with or without associated lymph node enlargement
1-2 years [5]. Staging is concerned with the spread of the disease and is split into four groups, which are summarized in Table 1.
Over half of patients with NHL can be cured [3]. Although more destructive, cure rates for high-grade tumors are much greater than for the low-grade type, if treated properly. It is believed that this to due to rapidly proliferating cells being more susceptible to therapy 121. Treatment of NHL depends on the stage and histologic type of the tumor. Treatment consists of chemotherapy, radiation or combination of the two. Chemotherapy protocols are based on the effec- tiveness with various types of NHL. As for radiation, two categories of therapy exist, curative and palliative. Curative doses are usually 3000-4500 rad delivered to the affected area for 3-4 weeks [4]. Palliative treat- ment would involve a lower dose over a shorter period of time.
4. Non-Hodgkins’ lymphoma and the eye
4.1. General
Patients with NHL of the central nervous system may present in three ways. These include primary CNS lymphoma (PCNSL), which is lymphoma con- fined to the central nervous system; lymphoma isolated to the eye, known as primary intraocular lymphoma (PIL); or a combination of the two. This last group accounts for approximately 60% of individuals [6]. Of patients with PCNSL, 15525% will develop ocular involvement, typically within 6-18 months [7]. In com- parison, a reported 5 6 ~ 8 5 % of patients with PIL will develop CNS lesions during the course of the disease, usually within 2 years, although a range of 7 weeks-9 years has been observed [7]. All three types of these lymphomas are restricted to the CNS and/or eye and do not represent metastasis from systemic lymphoma. The central nervous system and the eye are relatively immune privileged sites, therefore lymphomas are able to thrive, as the normal immune surveillance
mechanisms do not interfere with their development. In general, these lymphomas demonstrate four dis- tinct profiles: (1) solitary or multiple discrete intracra- nial nodules; (2) diffuse meningeal or periventricular lesions; (3) subretinal infiltrates or vitritis; and (4) localized intradural or spinal masses [7].
4.2. Systemic NHL and seconda y intraocular lymphoma
Systemic lymphoma characteristically begins in the lymph nodes, but may progress to the bone marrow and, eventually, to the peripheral blood in advanced disease. Even though intraocular lymphomas from the CNS and systemic NHL are cytologically identical, even at the electron microscopic level, they exhibit a different pattern of ocular involvement [l]. Histori- cally, CNS lymphoma tends to involve the vitreous, sensory retina and between the RPE and choroid, where systemic lymphoma generally metastasizes to the uveal tract. Secondary lymphoma most commonly presents as a focal choroidal mass with overlying pigment epithelial changes in a linear, stellate or leopard spot appearance. Vitreal inflammation is also quite common, and can represent the only finding. Patients may also present with anterior uveitis, malig- nant hypopyon and/or iris infiltration 181. When a blue iris is infiltrated, a brown heterochromia may be found [8]. Although rare, the retina can also show focal masses similar to the choroid and may demon- strate extension of tumor cells through Bruch’s mem- brane into the vitreous, as demonstrated in this case report. Intraretinal hemorrhages are often found with these retinal changes and represent prominent perivascular extension of the intravascular tumor cells [9]. In one report, there was evidence of central retinal artery occlusion caused by compression by an optic nerve head mass [lo].
Intraocular lymphoma in patients suspicious for systemic involvement, who exhibit no symptoms, need extensive work-up to discover the extent of systemic involvement of NHL [ll]. Treatment of intraocular lymphoma with concurrent systemic NHL consists of a combination of ocular irradiation with systemic ra- diation and/or chemotherapy.
4.3. Primay intraocular lymphoma (PIL)
The diagnosis of PIL is essential as 80% of patients die within 1-5 years after initial presentation as a result of CNS complications [6,12]. The most common symptoms include blurring of vision, floaters, eye pain, photophobia and foreign body sensation, although patients may be asymptomatic initially [8,13]. It is unknown if the patient in this report experienced any vision loss from the lymphoma as acuity was already greatly reduced from his concurrent ocular pathology.

M.S. Peterson, L.S. finvan /Clinical Eye and Vuion Cave 11 (1999) 199-206 203
Diplopia due to cranial nerve palsies has also been reported. During the early stages, mild symptoms are the rule, with increased severity with duration of disease [13]. One-third of symptoms begin unilater- ally, with 83% eventually becoming bilateral, although asymmetric [14].
The vitreous, retina and optic nerve are the most commonly affected structures in PIL. External signs of inflammation are rare, although hyperemia and salmon-pink infiltrative masses of the conjunctiva have been reported. Orbital invasion has also been found, as a metastasis from the globe [15]. Anterior uveitis is also fairly common as a result of carryover inflamma- tion from the posterior segment. Hypopyon, hyphema and neovascular glaucoma have also been described in cases of PIL [8]. Increased intraocular pressure may be noted secondary to neovascular glaucoma, steroid therapy or posterior synechiae as a result of chronic uveitis. The anterior chamber reaction is usually mild with fine cells, suggesting a non- granulomatous process, although mutton fat keratic precipitates can be seen, which would suggest a gran- ulomatous condition. Vitritis is an extremely common finding in PIL and, in contrast to anterior inflamma- tion, tends to present with larger clumps and sheets of cells. Multifocal large, yellow creamy subretinal masses, approximately 50-100 p m in diameter, with overlying solid ameboid pigment epithelial detach- ments is another standard sign associated with PIL [l]. In fact, these subretinal masses, along with vitritis, may be considered pathognomonic for PIL [2]. It is thought that tumor cells from these subretinal masses break through the internal limiting membrane to seed the vitreous, causing the associated vitritis [16]. One problem with this theory is the fact that cases have been described of vitreous cells without any retinal involvement, as well as retinal findings without vitreal involvement 1161. Interestingly, patients with vitritis are more apt to develop CNS problems, than those without vitreal involvement, although a reason for this has not been established [16]. There are many other reported retinal findings with PIL. Branch retinal vein occlusion, leading to central retinal vein occlusion secondary to subendothelial cell infiltration of large retinal vessels by lymphoma cells has been described [6]. Small white punctate dots at the RPE level similar to white-dot syndrome, acute retinal necrosis-like changes, retinochoroiditis simulating toxoplasmosis, periphlebitis, a frosted-branch angiitis-like appear- ance and intraretinal hemorrhages have all been de- scribed in PIL. Papilledema may be seen and is believed to be the result of either hypotony from chronic uveitis, increased intracranial pressure from associated cerebral neoplasm or direct lymphomatous infiltration of the optic nerve [17]. All in all, PIL can be a great masquerader and very difficult to diagnose.
4.4. NHL of the central nervous system (NHL-CNS)
NHL-CNS arises from the brain, spinal cord and leptomeninges. Half of patients with NHL-CNS will present with multifocal disease (including the eye) initially [MI. The origin of tumor cells in the CNS and the eye remains a mystery, as both areas are free of lymphatics. Viral infection or inflammation in the brain may attract non-neoplastic, reactive lymphoid cells to the area, where they are transformed into neoplastic cells, or neoplastic cells from nodal or extranodal sites may reach the eye and brain hematogenously [MI. A few potential mechanisms ex- ist that may explain how lymphomas are found in the CNS and eye simultaneously. It might be that the lymphoma originates in several non-contiguous loca- tions, either concurrently or sequentially from fixed perivascular reticuloendothelial cells and arise in the eye secondary to chronic inflammation. The fact that perivascular cuffs of chronic inflammatory cells have been found in both PIL and PCNSL may lend some evidence to this theory [MI. Another possibility may be transoptic nerve spread of the tumor which would allow access to lymphatics by extension to either ipsilateral leptomeninges or the ipsilateral central retinal artery [MI. This direct involvement has been suggested as cases exist which show lymphomatous infiltration of leptomeninges [ 181. PCNSL generally lateralizes to one side of the neuroaxis, although tumor involvement is not always exclusive to one side [l]. NHL-CNS tends to affect the eye ipsilateral to tumor involvement initially and to the greatest de- gree.
Patients with gross CNS lymphoma have a much higher mortality rate than those patients who demon- strate small foci of NHL on MRI. Approximately 10% of patients with lymphoma have a history of minor neurologic deficit (i.e. memory loss, minor CVAs), whereas 30% of patients have neither neurologic, physical or even laboratory findings suggestive of NHL-CNS [19]. On autopsy, there is approximately a 7 ~ 8 % rate of metastasis outside the CNS to the rest of the body [7].
Prognosis for NHL-CNS is not promising. Without treatment, median survival is 1.5 months once debili- tating neurologic symptoms begin [ 121. Although prompt treatment substantially prolongs survival, NHL-CNS is very aggressive and most patients still die within 5 years [12].
4.5. Histopathology
Lymphomas consist of malignant lymphocytes which are in various stages of development and demonstrate a characteristic diffuse growth pattern and cytologic appearance. Lymphomas contain large pleomorphic

204 M.S. Peterson, L.S. finvan /Clinical Eye and Vuion Cave 11 (1999) 199-206
cells with scanty cytoplasmic disproportion [20]. Nu- clei are oval, bean-shaped or cloverleaf in appearance with indentations of the nuclear membrane and finger-like projections of tumor cells [20]. The nuclear chromatin is arranged in irregular clumps and multi- ple, prominent nucleoli exist [21].
Immunohistochemical staining of retinal lymphoid cells show B cell and K light-chain markers with occasional staining of T cell and macrophage markers [22]. In contrast, cells found in the choroid demon- strate mainly T cell markers [22]. Infiltrates found in the retina, choroid and CNS are in a predominantly perivascular pattern. The most characteristic finding is tumor cells within the subretinal and subpigment epithelial spaces, delineated from the choroid by an intact Bruch's membrane [21]. Partial or complete necrosis may occur, if these cells outstrip their choroidal blood supply [21]. Once the tumor cells disrupt the RPE, they may grow subretinally or invade the retina causing varying amounts of necrosis 1211. An intense lymphocytic infiltrate is found in the choroid underlying these changes [22].
4.6. Diagnosis of intraocular lymphoma
An extreme challenge may exist for diagnosis of intraocular lymphoma in the absence of CNS or sys- temic findings. Definitive diagnosis of PIL may be achieved by vitreous fine needle aspiration biopsy and this procedure is generally considered when vision becomes worse than 20/200 [23]. The vitreous is then examined using lymphocyte marker analysis 1231. Un- fortunately, the vitreous biopsy is not always helpful, due to different reasons. If the vitreous specimen is insufficient, there may not be enough lymphoma cells to diagnose the condition. Treatment with steroids may clear the vitreous of cells and this commonly happens when these individuals are treated for vitritis and, thus, steroids should be withheld until after vitrectomy [24]. Another problem can be lack of tu- mor monoclonity, as normal inflammatory cells are usually mixed with tumor cells resulting in heterogen- ity of the specimen [25]. Finally, the fact that few of the characteristic histologic findings are actually de- monstrated in vitreous specimens makes diagnosis much more difficult [24]. Due to these reasons, a second vitreal tap may be necessary [23]. Whitcup et al. [26] reported increased interleukin-10 in the vitre- ous of ocular lymphoma patients. Interleukin-10 is a growth and differentiation factor for B lymphocytes and induces the release of immunoglobulins [27]. Al- though malignant tumor cells are needed for defini- tive diagnosis, if interleukin-10 is discovered, suspi- cion should be raised, even without evidence of tumor cells. For cases of suspected CNS involvement, a lumbar puncture to check the cerebrospinal fluid for
tumor cells is used as well as thin section MRI of the brain and posterior fossa, as this imaging is more specific for CNS lymphoma 1281. If only CT is avail- able, then contrast is necessary to visualize the lesion. Another important procedure for the diagnosis, as well as an objective method for following progress, is ultrasound.
4. Z Treatment and management
Despite treatment, a vast majority of patients with PIL, 92% in one study, will develop CNS lymphoma [7]. Relapse of lymphomas is very common, regardless of therapy. Unfortunately, current treatment does not prevent local relapse or subsequent disease in distant CNS locations. These recurrences may be due to untreated reservoirs of tumor or regrowth of inade- quately treated disease. Patients with ocular NHL usually have a limited life expectancy, with one study showing an average of 31 months after diagnosis [16].
No consensus exists currently regarding the proper treatment for any of the three types of intraocular lymphoma [29]. Due to increased longevity of individ- uals with intraocular lymphoma, it is important to attempt to discover a cure and many studies have been undertaken to this end. High-dose external radi- ation therapy to the eyes, sometimes with simultane- ous whole brain irradiation and/or systemic or in- trathecal chemotherapy is the usual therapy for most patients [30]. Unfortunately, there is a large risk of ocular morbidity associated with ocular irradiation, as well as the possibility of limiting the effectiveness of whole brain irradiation, due to overlapping treatment fields [30]. These factors must be taken into account when considering to treat intraocular lymphomas. Ra- diation also limits the use of chemotherapy for CNS lymphoma [31]. Unfortunately, therapy directed at CNS lymphoma does little to alter the course of intraocular lymphoma. Patients with both ocular and CNS lymphoma typically receive treatment aimed at ridding the CNS of disease only, neglecting the ocular malignancy. Because of this, one solution might be to direct chemotherapy at the eye itself, but the blood-aqueous barrier prevents chemotaxic agents from reaching the eye in sufficient doses to be useful. Due to this fact, a number of studies have attempted injection of chemotaxic agents directly into the vitre- ous, without proven success [29,31].
4.8. Uveitis in the elderly
Intraocular lymphoma will often present as uveitis. Characteristics associated with this type of uveitis include bilateral involvement and mild or no symp- toms initially [32]. Uveitis secondary to lymphoma may have a good initial response to steroids, but then

M.S. Peterson, L.S. finvan /Clinical Eye and Vuion Cave 11 (1999) 199-206 205
Table 2 Common tests in uveitis and their indications
Tests Indications
Angiotensin converting enzyme Antinuclear antibody (Ab) Antifungal antibody Antineutrophil cytoplasmic Ab Antitoxoplasma Ab Antiviral Ab Cultures Erythrocyte sedimentation rate Complete blood count HIV ELISA HLA typing
Liver function tests Lumbar puncture
for cell count
for CSF, VDRL for culture/Gram stain for cytology
Lyme serology Rheumatoid factor Thyroid function tests VDRL/FTA-ABS
Sarcoidosis Lupus, rheumatic disease Fungal infecton Wegener’s granulomatosis Toxoplasmosis Viral infection Possible infection Systemic disease Systemic disease HIV HLA associated with systemic disease Sarcoidosis, hepatitis
APMPEE, KH, infection, malignancy Syphilis Infection CNS lymphoma Lyme disease Rheumatoid arthritis, JRA Thyroid dysfunction Syphilis
increasing doses are required, and eventually the uveitis becomes refractory to both topical and sys- temic steroids [32]. Other individuals may not respond to steroids at all, and this is also a clue to etiology.
Acute uveitis presenting in patients over the age of 60 was classically thought to be a relatively uncom- mon finding, but with increasing longevity, it is be- coming less rare [28]. This uveitis is most commonly anterior, but may also be posterior or intermediate. Although most cases are idiopathic, an underlying disease masquerading as uveitis needs to be ruled out [28]. When an individual is diagnosed with uveitis, work-up involves a battery of laboratory, imaging and ancillary testing. A listing of possible laboratory tests
Table 3 Possible entities causing uveitis in the elderly
Acute retinal necrosis Amyloid disease Anticardiolipin Ab syndrome Ankylosing spondylitis Birdshot chorioretinopathy Cytomegalovirus retinitis Endophthalmitis
Herpes Zoster Herpes Simplex HLA B27 associated Intraocular lymphoma Lens induced Multifocal choroiditis Post traumatic
(candida, fungal, P. acnes)
Rheumatoid arthritis Rosacea Sarcoidosis Sympathetic ophthalmia Syphilis Systemic lupus erythematosus Toxoplasmosis Tuberculosis Ulcerative colitis Uveal effusion Vitreous wick syndrome Vogt-Koyanagi Harada disease Wegener’s granulomatosis Whipple’s disease
and their clinical significance is shown in Table 2. Certain diseases are found to cause uveitis more often in the elderly than in a general population (Table 3). For example, Herpes Zoster and Wegener’s granulomatosis are found at a much higher incidence in patients over 60, whereas syndromes such as Re- iter’s, Behcet’s and Posner-Schlossman, fairly com- mon culprits in a younger population, rarely manifest in the elderly [28].
Elderly patients with first time presentation of uveitis must be watched carefully, as sequelae may be severe. In addition, an etiology such as lymphoma must be considered. This case report represents a good example of a patient presenting with bilateral vitritis, secondary to a lymphoma. Intraocular pres- sure has a tendency to rise in uveitic patients over 60, resulting in increased rate of glaucoma and ocular hypertension which must be followed closely. The macula must also be monitored for changes, particu- larly cystoid macular edema, to which older eyes are more susceptible.
5. Conclusion
Intraocular lymphoma is usually found in patients over 60 and may be the result of central nervous system or systemic non-Hodgkins’ lymphoma or can be found in isolation of other findings. Clinical find- ings may be varied, as many ocular structures might be affected. Intraocular lymphoma can present as uveitis and needs to be ruled out in elderly patients with assumed idiopathic uveitis. This case report de- monstrates an unusual presentation of secondary in- traocular lymphoma from systemic NHL. Generally, this malignancy infiltrates the choroid and a localized whitish mass is observed. Rarely, the retina may ex- hibit infiltrates similar to those found in the choroid. Both types of infiltrates may migrate anteriorly and be found in the vitreous causing a vitritis. Diagnosis of intraocular lymphoma is important, as survival rates are not favorable without therapy. Even with treat- ment most patients die from CNS complications within 5 years after diagnosis. Nevertheless, the patient in this report was not treated because his NHL was considered low-grade.
References
[l] Qualman S, Mendelsohn G, Mann R, Green W. Intraocular lymphomas, natural history based on eight cases and review of the literature. Cancer 1983;52:878-886.
[2] Merchant A, Foster C. Primary intraocular lymphoma. Int Ophthalomol Clin 1997;37(4):101-115.
[3] Armitage J. Treatment of non-Hodgkins lymphoma. New Engl J Med 1993;328(14):1023-1030.
[4] Rahr V, Tucker R. Non-Hodgkins lymphoma understanding the disease. Cancer Nurs 1990;13(1):56-61.
206 M.S. Peterson, L.S. finvan /Clinical Eye and Vuion Cave 11 (1999) 199-206
[5] Portlock C. Non-Hodgkins lymphomas. Advances in diagno- sis, staging and management. Cancer 1990;65:718-722.
[6] Gass JD, Trattler HL. Retinal artery obstruction and athero- mas associated with non-Hodgkins large cell lymphoma (re- ticulum cell sarcoma). Arch Ophthalmol 1991;109:1134-1139.
[7] Whitcup S, Desmet M, Rubin B et al. Intraocular lymphoma, clinical and histopathologic diagnosis. Ophthalmology 1993;
[8] Zaman AG, Graham EM, Sanders MD. Anterior visual sys- tem involvement in non-Hodgkins lymphoma. Br J Ophthal- mol 1993;77:184-186. Ridley M, McDonald R, Sternberg P, Blumkranz M et al. Retinal manifestations of ocular lymphoma (reticulum cells sarcoma). Ophthalmology 1992;99:1153-1161. Guyer D, Green R, Schachat A. Bilateral ischemic optic neuropathy and retinal vascular occlusions associated with lymphoma and sepsis. Ophthalmology 1990;97:882-888.
[ l l ] Fredrick D, Char D, Ljung BM, Brinton D. Solitary intraocu- lar lymphoma as an initial presentation of widespread dis- ease. Arch Ophthalmol 1989;107:395-397.
[12] Verbraeken H, Hanssens M, Priem H et al. Ocular non- Hodgkins lymphoma: a clinical study of nine cases. Br J Ophthalmol 1997;81:31-36.
[13] Freeman N, Schachat A, Knox D, Michels D, Green WR. Clinical features, laboratory investigations, and survival in ocular reticulum cell sarcoma. Ophthalmology 1987;94:
[14] Buettner H, Bolling J. Intravitreal large-cell lymphoma. Mayo Clin Proc 1993;68:1011-1015.
[15] Noda S, Hayasaka S, Setogawa T. Intraocular lymphoma invades the optic nerve and orbit. Ann Ophthalmol
[16] Matsuo T, Yamaoka A, Shiraga F, Matsuo N. Two types of initial ocular manifestations in intraocular central nervous system lymphoma. Retina 1998;18:301-307.
[17] Bullock J, Yanes B, Kelly M, McDonald L. Non-Hodgkins lymphoma involving the optic nerve. Ann Ophthalmol
[18] Peterson K, Gordon K, Heinemann MH, DeAngelis LM. The clinical spectrum of ocular lymphoma. Cancer 1993;72:
Rankin G, Jakobiec F, Hidayat A. Intraocular lymphoprolif-
100: 1399 -1 406.
[9]
[lo]
1631-1639.
1993;25:30-33.
1979;1477-1480.
843 - 849. [19]
[201
1211
[221
1231
1251
1291
1301
erations simulating uveitis In: Albert and Jakobiec. chap
Lopez J, Chan CC, Burnier M, Rubin B, Nussenblatt R. Immunohistochemistry findings in primary intraocular lym- phoma. Am J Ophthalmol 1991;112(4):472-474. Matsuo K, Nakatuka K, Matsuura T, Yokoyama S. Primary intraocular lymphoma mimicking late postoperative endoph- thalmitis. Ophthalmologica 1995;209:331-335. Brown S, Jampol L, Cantrill H. Intraocular lymphoma pre- senting as retinal vasculitis. Surv Ophthalmol 1994;39:
Shields J, Shields C, Ehya H. Fine-needle aspiration biopsy of suspected intraocular tumors. Ophthalmology 1993;lOO:
Char D, Ljung BM, Miller T, Phillips T. Primary intraocular lymphoma. Diagnosis and management. Ophthalmology
Wilson D, Braziel R, Rosenbaum J. Intraocular lymphoma. Immunopathologic analysis of vitreous biopsy specimens. Arch Ophthalmol 1992;110:1455-1458. Whitcup S, Stark-Vancs V, Wittes R et al. Association of interleukin-10 in the vitreous and cerebrospinal fluid and primary central nervous system lymphoma. Arch Ophthalmol
Chan C, Whitcup S, Soloman D, Nussenblatt R. Interleukin-10 in the vitreous of patients with primary intraocular lym- phoma. Am J Ophthalmol 1998;120(5):671. Chatzistefanou K, Markomichelakis N. Characteristics of uveitis presenting for the first time in the elderly. Ophthalo- molgy 1998;105:347-352. Vose J, Armitage J. New approaches to therapy in patients with lymphoma. Hosp Formul 1991;26:564-570. Margolis L, Fraser R, Lichter A, Char D. The role of radia- tion therapy in the management of ocular reticulum cell sarcoma. Cancer 1980;45:688-692. Fishburne B, Wilson D, Rosenbaum J, Neuwelt E. Intravit- real methotrexate as an adjunctive treatment of intraocular lymphoma. Arch Ophthalmol 1997;115:1152-1156. Corriveau C, Easterbrook M, Payne D. Lymphoma simulating uveitis (masquerade syndrome). Can J Ophthalmol
1994;36:524-546.
133-140.
167771684,
1998;95:625-630.
1997;115:1157-1160.
1986;21(4):144-149.