Embed Size (px)
Citation preview
The Egyptian Heart Journal (2013) 65, 329–332
Egyptian Society of Cardiology
The Egyptian Heart Journal
www.elsevier.com/locate/ehjwww.sciencedirect.com
SHORT COMMUNICATION
A rare giant right atrial myxoma arising from crista
terminalis
* Corresponding author. Address: AMAL 5, 1555 2e etage, Rabat,
Morocco. Tel.: +212 623854130.
E-mail address: [email protected] (R. Atipo-Galloye).
Peer review under responsibility of Egyptian Society of Cardiology.
Production and hosting by Elsevier
1110-2608 ª 2013 Production and hosting by Elsevier B.V. on behalf of Egyptian Society of Cardiology.
http://dx.doi.org/10.1016/j.ehj.2013.05.001
Reddy Atipo-Galloye a,*, Rochde Sayeh a, Michel Mitsomoy a, Chami Loubna b
a Division of Cardiovascular Surgery, Avicennes Teaching Hospital, Rabat, Moroccob Division of Cardiology, Avicennes Teaching Hospital, Rabat, Morocco
Received 28 August 2012; accepted 11 May 2013Available online 4 June 2013
KEYWORDS
Myxoma;
Right atrium;
Crista terminalis
Abstract A case of giant right atrial myxoma arising from the crista terminalis in a 32-year-old
woman with a history of palpitation and dyspnea on great exersion. There was a discrepancy
between a large right atrial mass and less intensity of signs. Our patient underwent surgical treat-
ment with excision in bloc with safety margin of the atrial wall, and the right atrial wall was repaired
by autologous pericardium after tricuspid valve repair by the DEVEGA technique.ª 2013 Production and hosting by Elsevier B.V. on behalf of Egyptian Society of Cardiology.
1. Introduction
Intracardiac tumors are rare, 75% are benign and 50% of
them are myxomas with an incidence of 0, 0017% in thepopulation. Most myxomas are located in the left atrium(75–80%), arising from the interatrial septum at the border
of the fossa ovalis, but they can also originate (by descendingorder of frequency) from the right atrium, ventricles, venacave, pulmonary trunk and aorta.1 A cardiac myxoma usually
presents as a pedunculated tumor.In regard to the macroscopic aspect, the surface of myxo-
mas may have smooth or lobulated macroscopic features.
The consistency of myxomas is also variable, from firm togelatinous.
Microscopic features of myxomas are characterized by amyxoid matrix rich in mucopolysaccharides, in which polygo-nal cells with an eosinophilic cytoplasm can be detected. The
polygonal cells may appear as a star or nest shape or may bemultinucleated. Microscopic characteristics including mitoses,necrosis, or pleomorphism are usually not detected or areeventually present as mild findings.
Once a cardiac myxoma is diagnosed, surgical excisionshould be performed without delays because of the risk ofthromboembolic events.5,7 Generally, surgical treatment is
definitive and recurrence is uncommon. This report describesa rare clinical case of a large right atrial myxoma arising fromthe crista terminalis.
1.1. Case report
A 32-year-old woman had a 5 year history of palpitations,
which became more frequent and intense in the last threemonths prior to admission and which were associated withdyspnea on exersion.
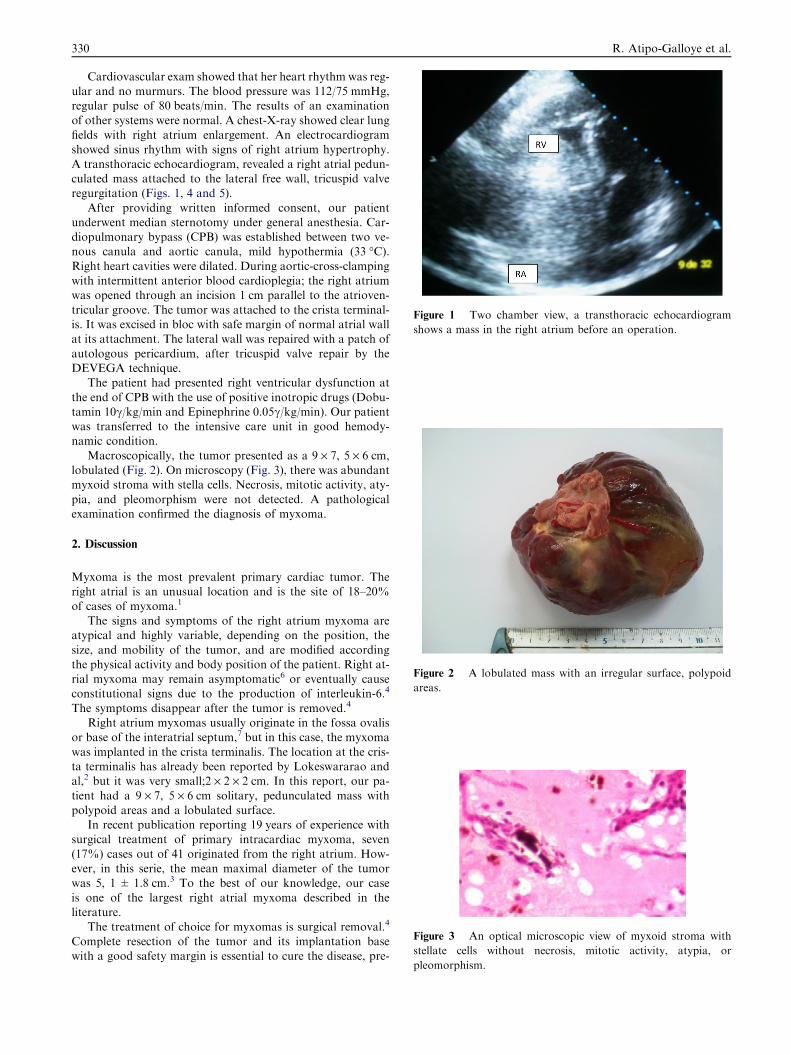
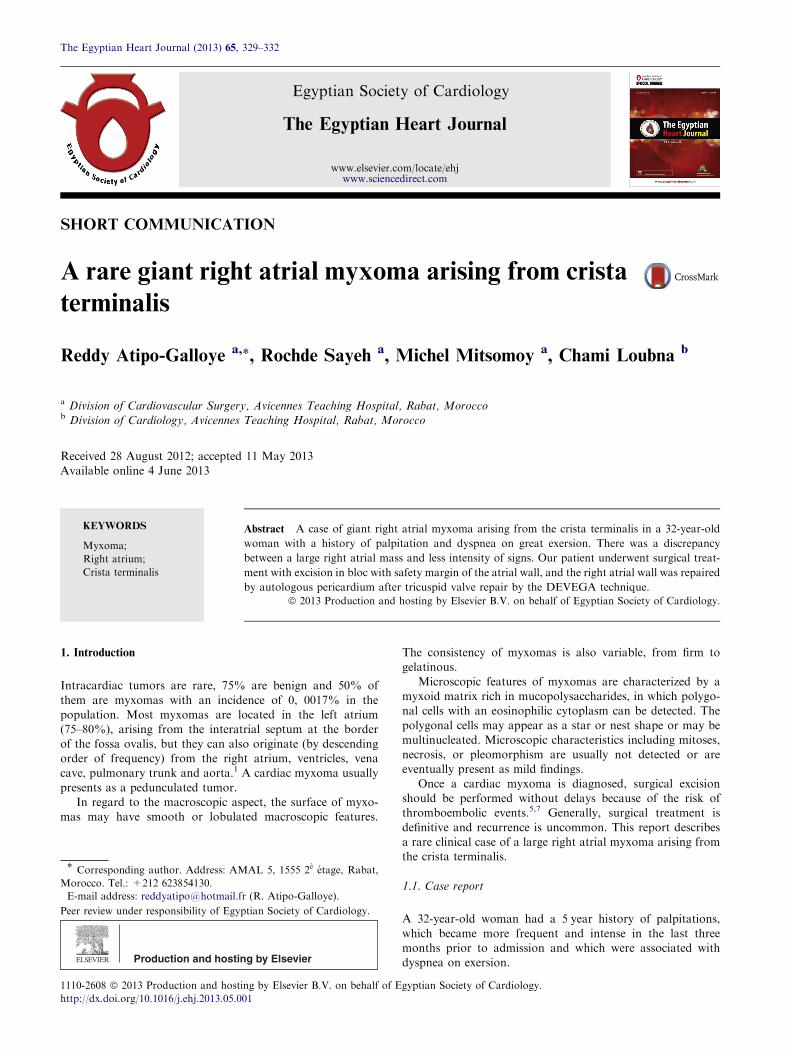
Figure 1 Two chamber view, a transthoracic echocardiogram
shows a mass in the right atrium before an operation.
Figure 2 A lobulated mass with an irregular surface, polypoid
areas.
Figure 3 An optical microscopic view of myxoid stroma with
stellate cells without necrosis, mitotic activity, atypia, or
330 R. Atipo-Galloye et al.
Cardiovascular exam showed that her heart rhythm was reg-ular and no murmurs. The blood pressure was 112/75 mmHg,regular pulse of 80 beats/min. The results of an examination
of other systems were normal. A chest-X-ray showed clear lungfields with right atrium enlargement. An electrocardiogramshowed sinus rhythm with signs of right atrium hypertrophy.
A transthoracic echocardiogram, revealed a right atrial pedun-culated mass attached to the lateral free wall, tricuspid valveregurgitation (Figs. 1, 4 and 5).
After providing written informed consent, our patientunderwent median sternotomy under general anesthesia. Car-diopulmonary bypass (CPB) was established between two ve-nous canula and aortic canula, mild hypothermia (33 �C).Right heart cavities were dilated. During aortic-cross-clampingwith intermittent anterior blood cardioplegia; the right atriumwas opened through an incision 1 cm parallel to the atrioven-
tricular groove. The tumor was attached to the crista terminal-is. It was excised in bloc with safe margin of normal atrial wallat its attachment. The lateral wall was repaired with a patch of
autologous pericardium, after tricuspid valve repair by theDEVEGA technique.
The patient had presented right ventricular dysfunction at
the end of CPB with the use of positive inotropic drugs (Dobu-tamin 10c/kg/min and Epinephrine 0.05c/kg/min). Our patientwas transferred to the intensive care unit in good hemody-namic condition.
Macroscopically, the tumor presented as a 9 · 7, 5 · 6 cm,lobulated (Fig. 2). On microscopy (Fig. 3), there was abundantmyxoid stroma with stella cells. Necrosis, mitotic activity, aty-
pia, and pleomorphism were not detected. A pathologicalexamination confirmed the diagnosis of myxoma.
2. Discussion
Myxoma is the most prevalent primary cardiac tumor. Theright atrial is an unusual location and is the site of 18–20%
of cases of myxoma.1
The signs and symptoms of the right atrium myxoma areatypical and highly variable, depending on the position, the
size, and mobility of the tumor, and are modified accordingthe physical activity and body position of the patient. Right at-rial myxoma may remain asymptomatic6 or eventually causeconstitutional signs due to the production of interleukin-6.4
The symptoms disappear after the tumor is removed.4
Right atrium myxomas usually originate in the fossa ovalisor base of the interatrial septum,7 but in this case, the myxoma
was implanted in the crista terminalis. The location at the cris-ta terminalis has already been reported by Lokeswararao andal,2 but it was very small;2 · 2 · 2 cm. In this report, our pa-
tient had a 9 · 7, 5 · 6 cm solitary, pedunculated mass withpolypoid areas and a lobulated surface.
In recent publication reporting 19 years of experience withsurgical treatment of primary intracardiac myxoma, seven
(17%) cases out of 41 originated from the right atrium. How-ever, in this serie, the mean maximal diameter of the tumorwas 5, 1 ± 1.8 cm.3 To the best of our knowledge, our case
is one of the largest right atrial myxoma described in theliterature.
The treatment of choice for myxomas is surgical removal.4
Complete resection of the tumor and its implantation basewith a good safety margin is essential to cure the disease, pre-
pleomorphism.
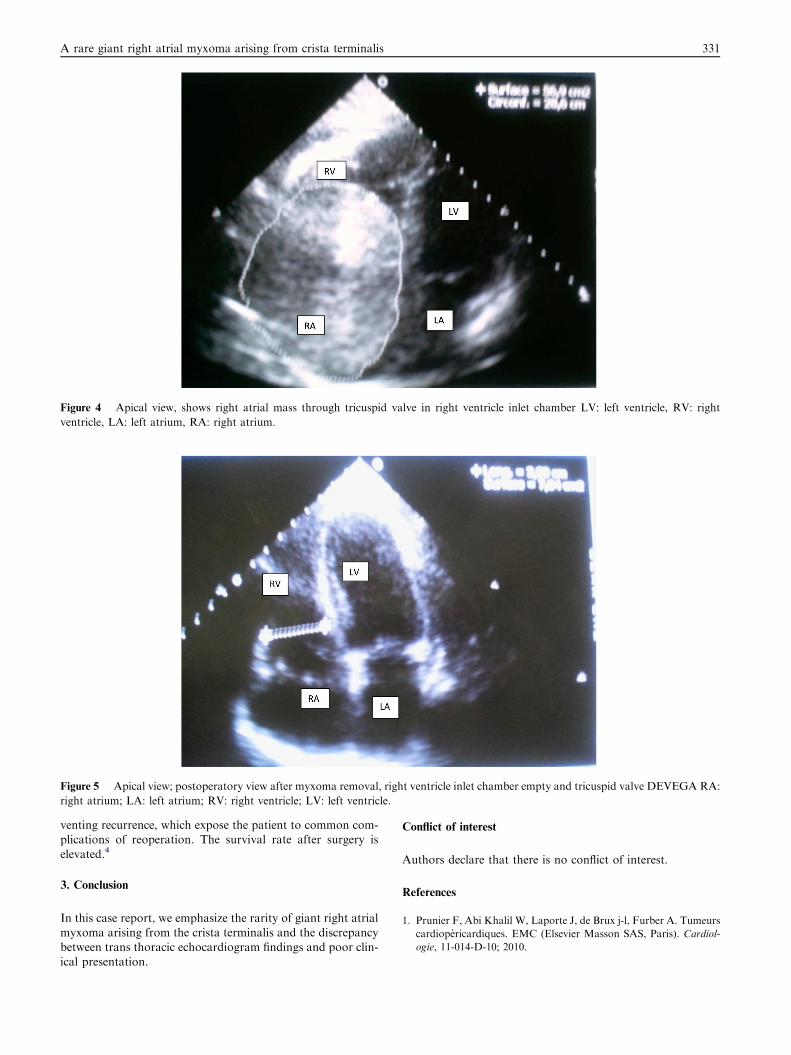
Figure 4 Apical view, shows right atrial mass through tricuspid valve in right ventricle inlet chamber LV: left ventricle, RV: right
ventricle, LA: left atrium, RA: right atrium.
Figure 5 Apical view; postoperatory view after myxoma removal, right ventricle inlet chamber empty and tricuspid valve DEVEGA RA:
right atrium; LA: left atrium; RV: right ventricle; LV: left ventricle.
A rare giant right atrial myxoma arising from crista terminalis 331
venting recurrence, which expose the patient to common com-plications of reoperation. The survival rate after surgery is
elevated.4
3. Conclusion
In this case report, we emphasize the rarity of giant right atrialmyxoma arising from the crista terminalis and the discrepancybetween trans thoracic echocardiogram findings and poor clin-
ical presentation.
Conflict of interest
Authors declare that there is no conflict of interest.
References
1. Prunier F, Abi Khalil W, Laporte J, de Brux j-l, Furber A. Tumeurs
cardiopericardiques. EMC (Elsevier Masson SAS, Paris). Cardiol-
ogie, 11-014-D-10; 2010.

332 R. Atipo-Galloye et al.
2. Lokeswararao Sajja, Gopi Chaud Mannam, Pennmatcha Krishr-
nam Raju, Srompalli Sriramulu, Angajala Rajasekham. Right atrial
myxoma arising from crista terminalis in septuagenarian. Asian
Cardiovasc Thorac Ann 2001;9:322–4.
3. Samandis G, Perreas K, Kalagoris P, Dimitriou S, Palanika M,
Amanatadis G, et al. Surgical treatment of primary intracardiac
myxoma: 19 years of experience. Interact Cardiovasc Thorac Surg
2011;13:597–600.
4. Guhathakurta S, Riordan JP. Surgical treatment of right atrial
myxoma. Tex Heart Inst J 2000;27:61–3.
5. Manfroi W, Vieira SR, Saadi EK, Alboim C. Multiple recurrences
of cardiac myxomas with acute tumoral pulmonary embolism. Arq
Bras Cardiol 2001;77:161–3.
6. Yuce M, Dagdelen S, Ergelen M, Eren N, Caglan N. A huge
obstructive myxoma located in the right atrial heart without
causing symptom. Interact J Cardiol 2007;144:405–6.
7. Stolf NA, Benicio A, Moreira LF, Rossi E. Right atrium myxoma
originating from inferior vena cava: an unusual location with
therapeutic and diagnostic implications. Rev Bras Cir Cardiovasc
2000;15:255–8.




![Mobile left atrial mass-clot or left atrial myxoma....mass includes thrombus, myxoma, lipoma and non-myxomatous neoplasm [7,8]. Among them, cardiac myxoma is the most common benign](https://img.pdfslide.us/doc/110x75/60fedab34ecd6d6c000feba7/mobile-left-atrial-mass-clot-or-left-atrial-mass-includes-thrombus-myxoma.jpg)