Embed Size (px)
Citation preview

Electronic Clinical Challenges and Images in GI
cMemwc
nnl
A Rare Cause of CholangiopathyElizabeth C. Goode,1 Benedict W. Simpson,2 and Simon M. Rushbrook1
1Departments of Gastroenterology and 2Radiology, Norfolk and Norwich University Hospital, Norwich, UK
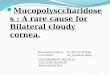
Question: A previouslyhealthy 20-year-old Cau-casian man presentedwith a 6-month historyof weight loss, anorexia,lethargy, and pruritus.Examination revealed co-njunctival pallor and hep-atomegaly. A full bloodcount demonstrated iron-deficiency anemia (hemo-globin, 7.8 g/dL; meancorpuscular volume, 63fL; ferritin, 19 �g/L) andeosinophilia (3.32 � 109/L). Liver function testsshowed cholestatic jaun-dice (bilirubin, 54 �mol/L; alkaline phosphatase,416 U/L; alanine amino-transferase, 170 �/L).Noninvasive liver screen,autoantibodies, immuno-globulin (Ig)G4, parasiticcytology, and stool cul-tures were negative.
Liver ultrasonographydemonstrated mild ir-regular intrahepatic ductdilatation. Computedtomography suggested
holangiopathy with beading of the biliary tree, splenic varices, gastric mural thickening (Figure A), and multiple small bowel polyps.agnetic resonance cholangiopancreatography confirmed intra- and extrahepatic cholangiopathy (Figure B). Gastroscopy with push
nteroscopy revealed erythematous gastric body mucosa with thickened rugal folds, but normal duodenum and proximal jejunum. Gastricucosal biopsies were nondiagnostic, and in view of the probable diagnosis, an endoscopic ultrasonographic fine-needle aspiration biopsyas considered unlikely to provide diagnostic information and therefore not performed. Cytopathology of endoscopic retrograde
holangiopancreatography biliary brushings was negative. Colonoscopy excluded inflammatory bowel disease.Bone marrow biopsy to exclude clonal hypereosinophilic syndrome or eosinophilic leukemia confirmed iron-deficiency anemia and increased
umbers of eosinophils, but revealed no evidence of clonality or lymphoma. Owing to clinical suspicion of the underlying disorder andondiagnostic surface biopsies, the patient finally underwent a laparoscopic full-thickness gastric biopsy (Figure C). Opportunistic laparoscopic
iver biopsy was also performed owing to previous nondiagnostic endoscopic retrograde cholangiopancreatography (Figure D).What is the most likely unifying diagnosis?See the GASTROENTEROLOGY web site (www.gastrojournal.org) for more information on submitting your favorite image to
Clinical Challenges and Images in GI.
Conflicts of interest: The authors disclose no conflicts.© 2013 by the AGA Institute0016-5085/$36.00
http://dx.doi.org/10.1053/j.gastro.2013.03.029GASTROENTEROLOGY 2013;144:e14 – e15

dfiPs
e(ccb
R
2
u
Electronic Clinical Challenges and Images in GI, continued
Answer to the Clinical Challenges and Images in GI Question: Image 5: ConcurrentEosinophilic Cholangiopathy and Subserosal Eosinophilic GastritisThe laparoscopic gastric biopsy (Figure C) shows a prominent eosinophilic infiltrate in the submucosa and muscular layers withperivascular lymphoid and eosinophilic infiltrate. The liver biopsy (Figure D) demonstrates preserved architecture with slight ductalproliferation, and occasional eosinophils within the portal tracts. Connective tissue stains show expansion of portal tracts withincipient bridging fibrosis. The overall appearances are consistent with a diagnosis of concurrent eosinophilic cholangiopathy andsubserosal eosinophilic gastritis. The patient was commenced on 40 mg of prednisolone daily, with subsequent resolution ofsymptoms and normalization of liver biochemistry. Repeat magnetic resonance cholangiopancreatography after a sufficient timeinterval will be used to assess radiographic resolution.
Eosinophilic cholangiopathy is a rare, benign, inflammatory condition of the biliary tree. Most commonly described in youngmen, eosinophilic infiltration of the bile ducts results in stricturing, fibrosis, and obstruction of the biliary tree.1 The following
iagnostic criteria were proposed by Matsumoto et al2: (1) stenosis or wall thickening of the biliary system, (2) histopathologicndings of eosinophilic infiltration, and (3) reversibility of biliary abnormalities without treatment or after steroid treatment.eripheral blood eosinophilia, present in the majority of patients, may provide a diagnostic clue; however, its presence is neitherensitive nor specific, and its absence does not preclude the diagnosis.
Eosinophilic cholangitis forms part of a wider spectrum of eosinophilic gastrointestinal disorders, histologically characterized byosinophilic infiltration of different tissue layers and organs of the gastrointestinal tract without any apparent cause for eosinophiliaeg, parasitic infection, neoplasia, medication reaction, vasculitis, IgG4 systemic syndrome). Concurrent eosinophilic gastritis andholangiopathy is extremely rare, with only 3 previous reported cases in the literature. Infiltration confined to the serosa meant theondition could only be diagnosed by full-thickness gastric biopsy. It is important that secondary causes and bone marrow clonalitye excluded.
eferences1. Nashed C, Sakpal S, Susharina V, et al. Eosinophilic cholangitis and cholangiopathy: a sheep in wolves clothing. HPB Surg
010;906496.2. Matsumoto N, Yokohama K, Nakai K, et al. A case of eosinophilic cholangitis: imaging findings of contrast-enhanced
ltrasonography, cholangioscopy, and intraductal ultrasonography. World J Gastroenterol 2007;13:1995–1997.
e15