Embed Size (px)
Citation preview
THE JOURNAL OF ALTERNATIVE AND COMPLEMENTARY MEDICINEVolume 10, Number 3, 2004, pp. 438–448© Mary Ann Liebert, Inc.
A Randomized Trial of the Effects of Remote IntercessoryPrayer: Interactions with Personal Beliefs on Problem-Specific
Outcomes and Functional Status
RAYMOND F. PALMER, Ph.D., DAVID KATERNDAHL, M.D., and JAYNE MORGAN-KIDD, M.S.
ABSTRACT
Objectives: Investigate the relevance of interpersonal belief factors as modifiers of the effectiveness of in-tercessory prayer.
Design: Randomized clinical trial.Setting/location: Community-dwelling adults recruited from seven local church groups.Subjects: Eighty-six (86) male and female participants 18–88 years of age were randomly assigned to either
treatment (n � 45) or control groups (n � 41).Interventions: Several volunteers committed to daily prayer for participants in the intervention group. In-
tercessory prayer commenced for 1 month and were directed toward a life concern or problem disclosed by theparticipant at baseline. Participants were unaware of being prayed for.
Outcomes measures: Degree to which their problem had been resolved and the current level of concern theyhad about a specific life problem they described at baseline. Four component scores from the Medical Out-comes Study SF-20 were also used.
Results: No direct intervention effect on the primary outcomes was found. A marginally significant reduc-tion in the amount of pain was observed in the intervention group compared to controls. The amount of con-cern for baseline problems at follow-up was significantly lower in the intervention group when stratified bysubject’s baseline degree of belief that their problem could be resolved. Prayer intervention appeared to effec-tively reduce the subject’s level of concern only if the subject initially believed that the problem could be re-solved. Those in the intervention group who did not believe in a possible resolution to their problem did notdiffer from controls. Better physical functioning was observed in the intervention group among those with ahigher belief in prayer and surprisingly, better mental health scores were observed in the control group withlower belief in prayer scores.
Conclusions: The results of the current study underscore the role of interpersonal belief in prayer efficacyand are consistent with the literature showing the relevance of belief in health and well-being in general. Therelevance of interpersonal belief factors of the participants is recommended in future investigations.
Department of Family and Community Medicine, University of Texas Health Science Center at San Antonio, San Antonio, TX.
438

“It is asserted by some, that men possess the faculty of obtaining results over which they have little or no directpersonal control, by means of devout and earnest prayer, while others doubt the truth of that assertion. The questionregards a matter of fact, that has to be determined by observation and not by authority: and it is one that appears tobe a very suitable topic for statistical inquiry . . . Are prayers answered or are they not? . . . Do sick persons whoare prayed for, recover on the average, more rapidly than others?”
—Francis Galton, 1883
RCT OF REMOTE INTERCESSORY PRAYER 439
INTRODUCTION
Contemporary trends in spirituality regarding health andwell-being have developed parallel to a cultural shift in
increased scientific investigation and secular involvement inthe use of alternative and complementary therapies (Astin,1998; Eisenberg et al., 1998, 2001). The National Instituteof Health, National Center for Complementary and Alter-native Medicine has funded many clinical trials related tothe investigation of the efficacy of a variety of alternativeinterventions. However, the role of spiritual practices astreatment modalities remains controversial among health re-searchers and physicians. Indeed, there is a lack of testabletheoretical models that incorporate spirituality into an allo-pathic framework of health (Oldnall, 1995) and until re-cently, replicable scientific studies have been sparse (Levinet al., Puchalski 1997). For example, in a systematic reviewof the literature, Abbot (2000) identified 59 randomized clin-ical trials where various “healing” modalities (which in-cluded prayer, spiritual, paranormal, and distant healing)were used as treatments for a variety of health outcomes.However, because of the wide heterogeneity in the group ofidentified trials, categorizing the studies is problematic andprohibits statements about the size of treatment effects. Fur-thermore, many of these trials had various methodologicalshortcomings including small sample sizes and inadequatemethodological reporting.
Notwithstanding, an expert panel from the National In-stitute for Healthcare Research has recently evaluated thescientific evidence for an association between spirituality/re-ligious practices and health. They concluded that spiri-tual/religious involvement has demonstrated to be consis-tently related to positive health outcomes across a variety ofhealth domains (Larson, 1997).
The efficacy of intercessory prayer
Within the domain of spirituality there have been a num-ber of investigations specifically focused on the efficacy ofintercessory prayer (e.g., a specific request or earnest sup-plication for a desired outcome directed toward a higherpower [Dossey, 1993]). While this literature remains in-conclusive, the general consensus across several publishedreports is that the current evidence is compelling enough towarrant further investigation. For example, a recent reportin the Cochrane Database of Systematic Reviews (Robertset al., 2000) on the efficacy of intercessory prayer concludes
that there is not enough evidence to uphold or refute the ef-fect of intercessory prayer on health care outcomes.
While the first investigations by medical practitioners areconsidered to be poorly formulated and underpowered (Col-lipp, 1969; Joyce and Welldon, 1965), subsequent studieshave used rigorous prospective randomized double-blindedtrials. Investigations of the potential therapeutic effects ofintercessory prayer have been conducted on a variety ofhealth outcomes including: cardiac (Byrd, 1988; Harris etal., 2000; Aviles et al., 2001); diabetes (Wirth and Mitchekk,1994); alcoholism (Walker et al., 1997); mental health(O’Laoire, 1997); arthritis (Matthews, et al., 2000); infec-tion (Leibovici 2001); and fertility (Cha, et al., 2001).
Summary and research questions
This study was initiated because the replicable empiricalevidence on the beneficial effectiveness of intercessoryprayer is relatively sparse, yet compelling. In particular, lit-tle attention has been given to personal belief factors as po-tential effect modifiers of intercessory prayer. Researchersin this area have recently recognized the potential relevanceof investigating subgroups based on personal beliefs or psy-chologic profiles of those being prayed for (Cha et al., 2001;Mackenzie et al., 2000; O’Laoire 1997; Walker et al., 1997).
To justify this position, it has been well documented thatinterpersonal factors such as hope, belief, faith, and attitudescan influence health outcomes (Benson and Stark, 1996;Frarran et al., 1995; Hilakivi-Clarke et al., 1994; Karren etal., 2002; Peterson and Bossio, 1994; Rabinowitz et al.,1992). The role of belief is also consistent with recent dis-cussions concerning the significance of these factors in thespiritual healing literature (Benson, 1996; Wirth, 1995).
In this study, we investigate the role of personal belief(“belief in the power of prayer,” and “belief that a personalproblem can be resolved”) as potential effect modifiers in theassociation between intercessory prayer and a specific per-sonal outcome. Furthermore, while studies of intercessoryprayer have largely been limited to hospitalized inpatients oroutpatient clinic treatment, there have been no randomizedtrials among those not seeking care. This study also addressesthe limited information on intercessory prayer among non-patient subjects, and investigates the role of belief as a po-tential moderating factor in the efficacy of intercessoryprayer in alleviating the personal concerns in this sample.
The following research questions are addressed in thisstudy: (1) does intercessory prayer measurably influence the

personal concerns of those being prayed for and (2) is prayerefficacy dependent on “belief in prayer” or the “belief thata problem can be resolved”?
MATERIALS AND METHODS
Recruitment, survey administration, and group assignment
Seven local Presbyterian churches were contacted viaU.S. mail and a follow-up telephone call to the pastor. Thesechurches were chosen because they were part of a larger re-search network of churches agreeing to participate in effortsto study the effects of religion, spirituality, and health ingeneral. This group of churches was asked to participate ina study on health and religious behavior where a 20-minutequestionnaire would be completed at the church with a short5-minute follow-up questionnaire to be completed 1 monthlater. Six of the seven churches agreed to participate and adate was set for a researcher to attend a weekday group func-tion (e.g., general council meeting, Bible study, choir prac-tice, etc.) and administer a questionnaire on general healthand religious practices. Groups ranged in size from 10–25participants. In addition, in an attempt to diversify the sam-ple in this study, two groups consisting of nonchurch mem-bers who utilized the church facilities for meetings (e.g., lo-cal support and special interest groups) were recruited.Participants were told the researchers were interested instudying the association between health and religious be-haviors and were not told about the prayer component dur-ing the pre-questionnaire briefing.
A University Internal Review Board approved the studyprotocol. After giving written informed consent to partici-pate, subjects completed a 23-item Likert-type responsequestionnaire. The questionnaire was composed of the shortform of the Medical Outcomes Study SF-20, and religiousand spirituality scales from the Brief Multidimensional Mea-sure of Religiousness/Spirituality: 1999 (Fetzer Institute,1999). At the end of the questionnaire, subjects were askedan open-ended question about a difficult life situation theyare currently experiencing. The subjects’ reported difficultsituations could be broadly categorized as concerns for self,concerns for family, and either emotional or physical con-cerns. Subjects were asked to rate the degree of concern(from 1 � none to 5 � overwhelming) this problem cur-rently held in their lives. Participants were also asked to ratethe degree to which they believed the situation could be re-solved (1 � yes, very possible; 2 � yes; 3 � slight possi-bility; 4 � no possibility).
Respondents were asked for a contact telephone numberor e-mail address so that they could be reached in 1 monthfor a brief follow-up survey concerning their health. Of 120respondents, 72 (60%) provided e-mail addresses for con-tacting them for purposes of follow-up. The rest were con-
tacted by telephone. Those contacted by e-mail were di-rected to a project Web site where a follow-up survey couldbe completed and submitted electronically. There was nostatistically different response rate between Internet or tele-phone follow-up methods. In addition to the health mea-sures, the follow-up survey asked subjects to rate the degreeto which the problem they had indicated in the initial sur-vey had been resolved (1 � yes, completely; 2 � somewhat;3 � very little; 4 � not at all). Subjects received a brief re-minder of what problem they had identified at baseline.
Of 120 surveyed participants, 34 were not randomized toa group either because there was no life problem revealed(n � 10), the stated problem was not rated as being of suf-ficient concern (n � 22), or no follow-up contact informa-tion was given (n � 2). Using a computerized random num-ber generator, 86 participants were then randomized to eitherthe treatment or control. Each subject received a randomnumber between 0 and 1. Approximately half were evennumbers (n � 45) and approximately half were odd num-bers (n � 41). A coin toss then determined which group,odds (tails) or even (heads), would receive the prayer inter-vention. An administrative assistant who was blinded to theexperimental procedures flipped the coin. Even numbers re-ceived the intervention.
At 1-month follow-up, the response rate for the inter-vention group was 82.2% (n � 37) and the response rate forthe control group was 78% (n � 32). Sixty-four percent(64%) of the sample were church members with the re-maining 36% being nonchurch members.
The pray-ers
Those who prayed for subjects in the intervention groupconsisted of eight volunteers from one local church’s prayerchain and four retired women living in a Christian retire-ment home. To preserve anonymity, subjects who were tobe prayed for were not members of the churches from whichthe prayer group was based. Each prayer group volunteerwas asked to pray for at least one or two individuals at leastonce per day for a month. Some prayed for three or four in-dividuals. They received only the participant’s first nameand a written summary of his or her concern; no other in-formation was given. The volunteers who prayed were askedto keep a prayer log of how often and how long they prayed,and if they used a scripted or unscripted prayer. The aver-age length of each prayer session was 3 minutes. The aver-age frequency of prayer sessions was two times per day.
Measures
Prayer outcome measures. At follow-up, each participantwas asked the degree to which his or her problem had beenresolved (1 � completely to 4 � not at all). Participantswere also asked to rate the current level of concern they hadabout the problem they described at baseline. Response op-tions here ranged from 1 � no concern to 5 � overwhelm-ing concern.
PALMER ET AL.440

Secondary outcome measures. Three relevant componentscores from the Medical Outcomes Study SF-20 (Stewart,et al., 1988) were used: physical functioning, pain, and men-tal health. The SF-20 consists of 20 questions organized into6 scales. Cronbach � ranges from 0.81 to 0.88. Discrimi-nate validity of the SF-20 was made by comparing scoresbetween patient and nonpatient populations. The scoring ofthe SF-20 ranges from 1 to 100, with larger scores indicat-ing higher ratings of physical function, pain, and mentalhealth. The degree to which the situation interfered with nor-mal work or social life was also assessed (1 � radicallychange or prevent normal or social activities to 5 � does notinterfere with normal work or social activities). This itemhas been widely used in prior studies of panic disorders (Bal-lenger et al., 1988).
Intrapersonal belief. Belief in the power of prayer domainwas measured from four items developed by the current pro-ject’s research team. These items were scored on a Likert scalefrom 1 � strongly agree to 4 � strongly disagree. The ques-tions include, “I believe praying can help me cope with life’sdifficulties,” “I believe praying can help my health problems,”“I believe praying for others can be helpful,” and “I believeI can benefit when others pray for me.” The internal consis-tency of the items was 0.92 (e.g., items are highly associatedand are consistent with each other, for example high scoreson one is associated with high scores on the other—a desir-able psychometric property in scale construction). Items weresummed to form a composite variable for analysis.
A second belief item asked participants to rate the degreeto which they believed it was possible that the situation theyidentified in the survey could be resolved (1 � yes, verypossible to 4 � no possibility).
Analysis
The continuous outcome measures (three variables fromSF20) demonstrated an acceptable normal distribution andwere therefore modeled using Ordinary Least Regression(OLS) of the form below:
Y � � � �1x1 � �2x2 � �
where �1 is the coefficient for the treatment variable x1 (coded1 � treatment intervention and 0 � control group) and x2 isthe baseline covariate of the follow-up outcome (y). This an-alytic method allows the effects of an outcome variable (e.g.,physical or emotional functioning) to be estimated as a func-tion of group membership (e.g., treatment or control) andother predictor variables. To assess the moderation effects ofthe belief variables, the interaction term (belief � treatment)was entered into separate models for the two belief variables.Therefore, three different models were run. Model 1 assessedthe direct effect of treatment on the follow-up outcome; Model2 included an interaction term (treatment * belief that prob-lem can be resolved); Model 3 included a different interac-
tion term (treatment * belief in the power of prayer). In termsof forming an interaction variable, because of the potentialnonlinear associations with the outcomes and possible insta-bility in parameter estimates because of few subjects in ex-treme categories, the belief variables were dichotomizedbased on a median split in their distribution (0 � low beliefand 1 � higher belief). This dichotomized variable was usedin the interaction term with the treatment variable. Regres-sion coefficients were obtained through maximum likeli-hood estimation procedures using AMOS statistical software(Arbuckle and Wothke, 1994).
For the main outcome variables, an ordinal regressionmodel for discrete outcomes was used (McCullagh, 1980)and implemented using SPSS software (SPSS, Inc., Chicago,IL). The parameter estimates of these models are reportedin Table 1 along with the OLS estimates.
To correct for multiple comparisons in our analysis andadjust for potential Type 1 error (e.g., incorrectly declaringa difference between groups) we used a separate Bonfer-roni-type correction method (Schaffer, 1995) for the primaryand secondary study variables. Therefore, a significancelevel of p � 0.025 is considered statistically significant forthe former and p � 0.0125 for the latter.
Power. With 40 subjects per group, power analysis basedon Cohen’s (1988) formulas for regression demonstrates thatpower is 0.87 to detect an effect size of 0.26 (indicating thatif in fact prayer significantly effects the outcome variablesthere would be a high probability of detecting approximatelya one-quarter standard deviation difference between treat-ment and control groups).
RESULTS
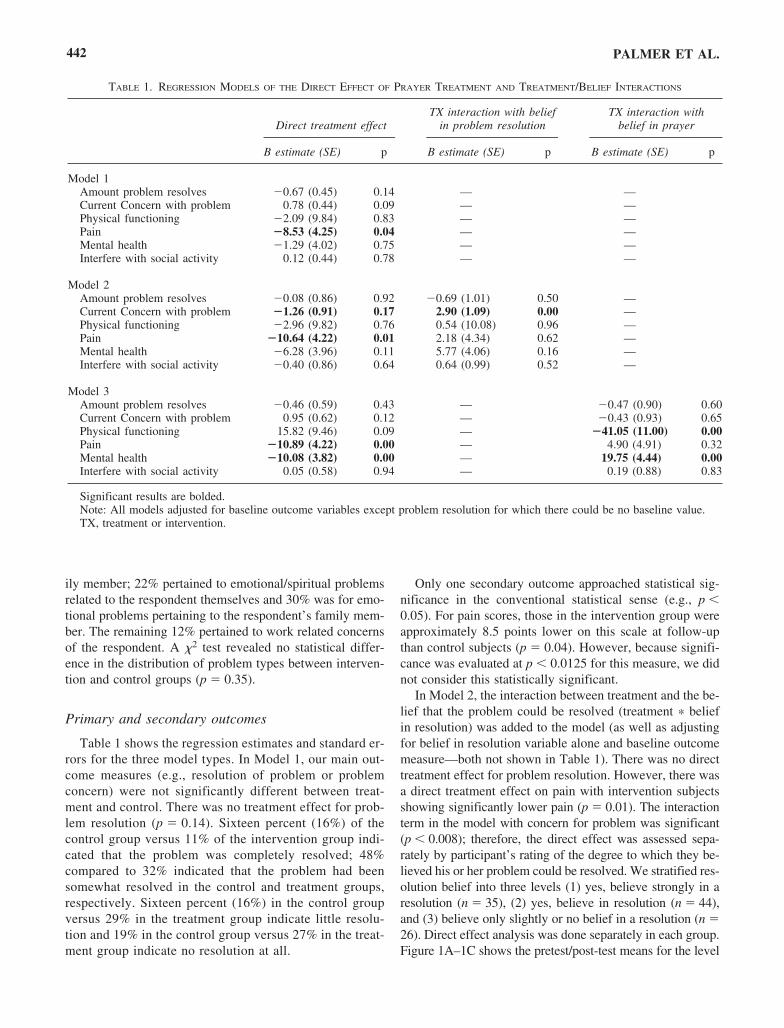
Table 2 shows the characteristics of the sample by inter-vention condition. Most subjects were white, married, andwell-educated. Between group comparisons on baselinecharacteristics were assessed using both �2 and t tests whereappropriate. There were no significant demographic differ-ences between conditions. Table 3 shows the descriptive sta-tistics of the study baseline variables by intervention condi-tion. There were no significant baseline differences betweenconditions for all variables except interference with socialactivity where controls had higher baseline scores. Subjectrating for problem resolution obviously did not have a base-line value and is therefore not shown in Table 3. Responsedescription is presented below.
Type of problems/concerns reported
Participants reported specific problems that could pre-dominantly be placed into four broad categories; physical oremotional problems relating to either one’s self or another.Approximately 27% were health problems pertaining to theparticipant themselves, 9% were health concerns for a fam-
RCT OF REMOTE INTERCESSORY PRAYER 441
ily member; 22% pertained to emotional/spiritual problemsrelated to the respondent themselves and 30% was for emo-tional problems pertaining to the respondent’s family mem-ber. The remaining 12% pertained to work related concernsof the respondent. A �2 test revealed no statistical differ-ence in the distribution of problem types between interven-tion and control groups (p � 0.35).
Primary and secondary outcomes
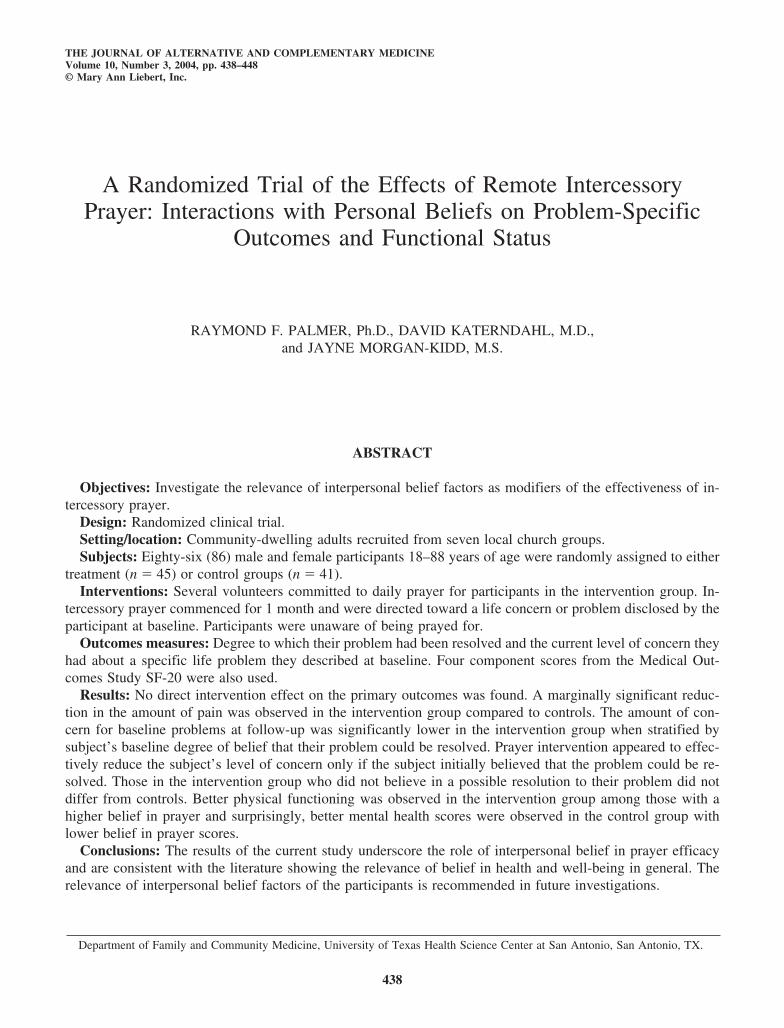
Table 1 shows the regression estimates and standard er-rors for the three model types. In Model 1, our main out-come measures (e.g., resolution of problem or problemconcern) were not significantly different between treat-ment and control. There was no treatment effect for prob-lem resolution (p � 0.14). Sixteen percent (16%) of thecontrol group versus 11% of the intervention group indi-cated that the problem was completely resolved; 48%compared to 32% indicated that the problem had beensomewhat resolved in the control and treatment groups,respectively. Sixteen percent (16%) in the control groupversus 29% in the treatment group indicate little resolu-tion and 19% in the control group versus 27% in the treat-ment group indicate no resolution at all.
Only one secondary outcome approached statistical sig-nificance in the conventional statistical sense (e.g., p �0.05). For pain scores, those in the intervention group wereapproximately 8.5 points lower on this scale at follow-upthan control subjects (p � 0.04). However, because signifi-cance was evaluated at p � 0.0125 for this measure, we didnot consider this statistically significant.
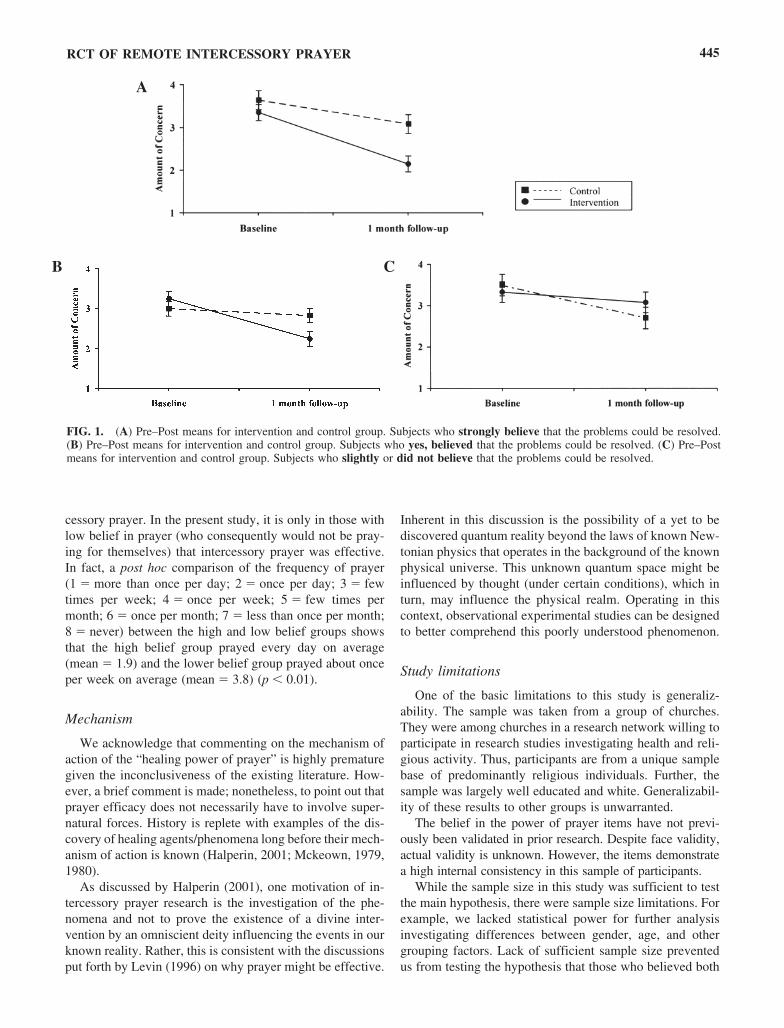
In Model 2, the interaction between treatment and the be-lief that the problem could be resolved (treatment * beliefin resolution) was added to the model (as well as adjustingfor belief in resolution variable alone and baseline outcomemeasure—both not shown in Table 1). There was no directtreatment effect for problem resolution. However, there wasa direct treatment effect on pain with intervention subjectsshowing significantly lower pain (p � 0.01). The interactionterm in the model with concern for problem was significant(p � 0.008); therefore, the direct effect was assessed sepa-rately by participant’s rating of the degree to which they be-lieved his or her problem could be resolved. We stratified res-olution belief into three levels (1) yes, believe strongly in aresolution (n � 35), (2) yes, believe in resolution (n � 44),and (3) believe only slightly or no belief in a resolution (n �26). Direct effect analysis was done separately in each group.Figure 1A–1C shows the pretest/post-test means for the level
PALMER ET AL.442
TABLE 1. REGRESSION MODELS OF THE DIRECT EFFECT OF PRAYER TREATMENT AND TREATMENT/BELIEF INTERACTIONS
TX interaction with belief TX interaction with Direct treatment effect in problem resolution belief in prayer
B estimate (SE) p B estimate (SE) p B estimate (SE) p
Model 1Amount problem resolves �0.67 (0.45) 0.14 — —Current Concern with problem 0.78 (0.44) 0.09 — —Physical functioning �2.09 (9.84) 0.83 — —Pain �8.53 (4.25) 0.04 — —Mental health �1.29 (4.02) 0.75 — —Interfere with social activity 0.12 (0.44) 0.78 — —
Model 2Amount problem resolves �0.08 (0.86) 0.92 �0.69 (1.01)�0 0.50 —Current Concern with problem �1.26 (0.91) 0.17 2.90 (1.09)0 0.00 —Physical functioning �2.96 (9.82) 0.76 0.54 (10.08) 0.96 —Pain �10.64 (4.22) 0.01 2.18 (4.34)0 0.62 —Mental health �6.28 (3.96) 0.11 5.77 (4.06)0 0.16 —Interfere with social activity �0.40 (0.86) 0.64 0.64 (0.99)0 0.52 —
Model 3Amount problem resolves �0.46 (0.59) 0.43 — �0.47 (0.90) 0.60Current Concern with problem 0.95 (0.62) 0.12 — �0.43 (0.93) 0.65Physical functioning 15.82 (9.46) 0.09 — �41.05 (11.00) 0.00Pain �10.89 (4.22) 0.00 — 4.90 (4.91) 0.32Mental health �10.08 (3.82) 0.00 — 19.75 (4.44) 0.00Interfere with social activity 0.05 (0.58) 0.94 — 0.19 (0.88) 0.83
Significant results are bolded.Note: All models adjusted for baseline outcome variables except problem resolution for which there could be no baseline value.TX, treatment or intervention.
of concern for problem outcome variable between treatmentand control groups stratified by the three levels of resolutionbelief. Post-test means were significantly different in the treat-ment group compared to the control group in those who be-lieved in a resolution to their problem. Those in the treatmentgroup who did not endorse a belief in a resolution were notstatistically different than controls.
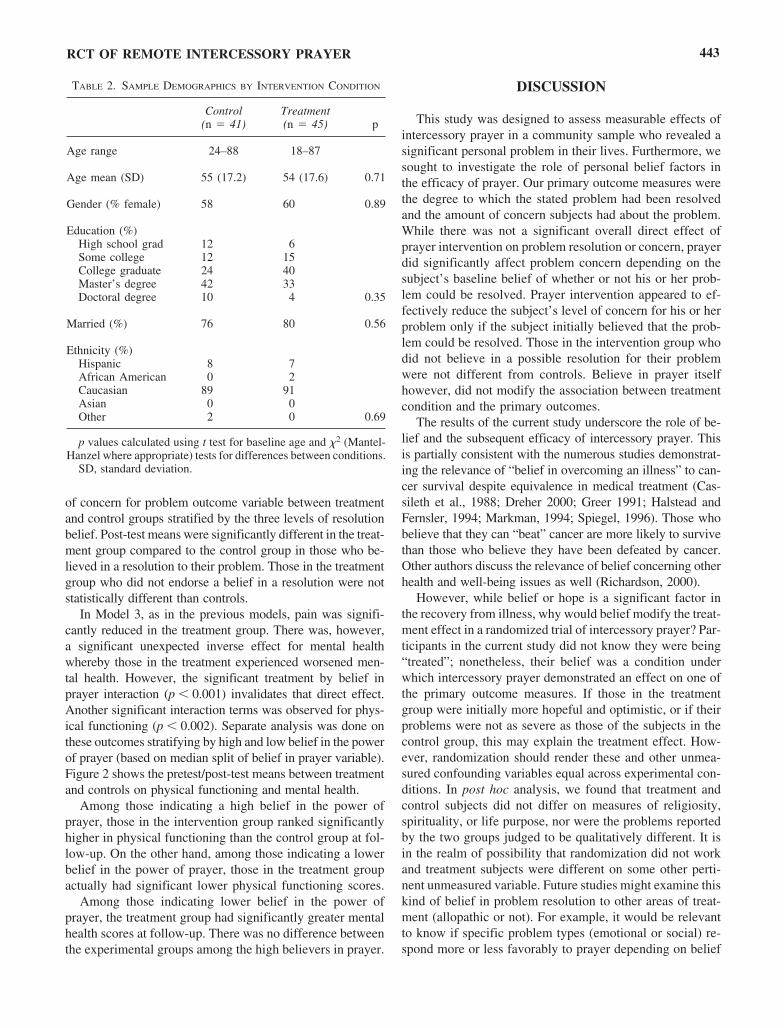
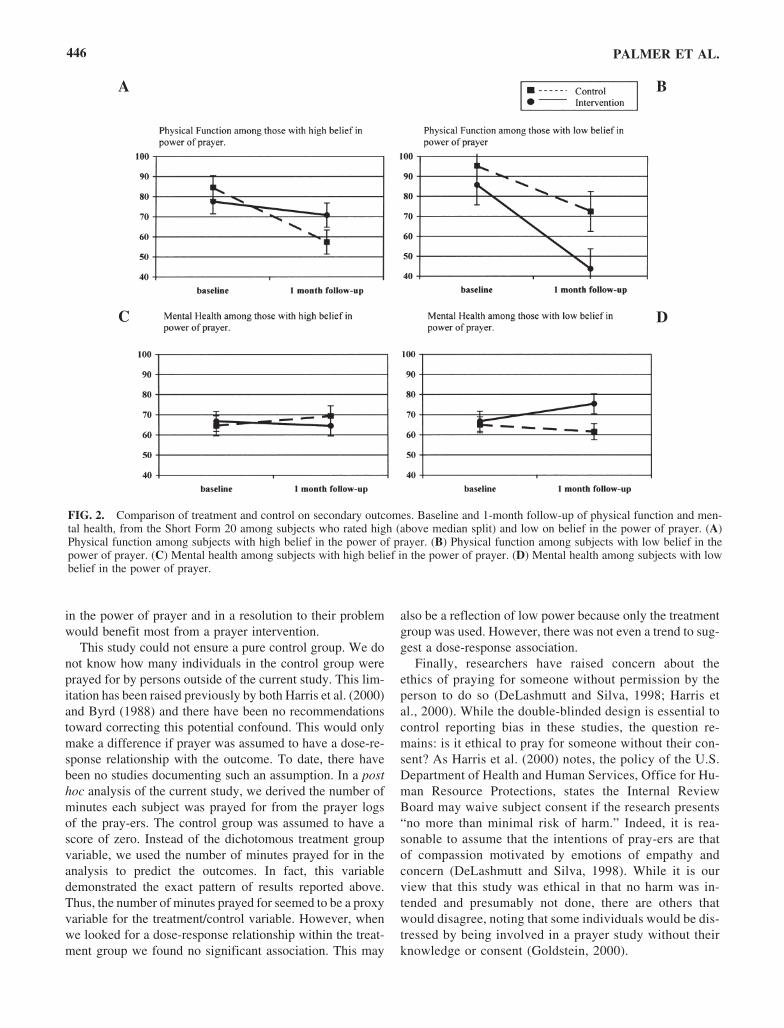
In Model 3, as in the previous models, pain was signifi-cantly reduced in the treatment group. There was, however,a significant unexpected inverse effect for mental healthwhereby those in the treatment experienced worsened men-tal health. However, the significant treatment by belief inprayer interaction (p � 0.001) invalidates that direct effect.Another significant interaction terms was observed for phys-ical functioning (p � 0.002). Separate analysis was done onthese outcomes stratifying by high and low belief in the powerof prayer (based on median split of belief in prayer variable).Figure 2 shows the pretest/post-test means between treatmentand controls on physical functioning and mental health.
Among those indicating a high belief in the power ofprayer, those in the intervention group ranked significantlyhigher in physical functioning than the control group at fol-low-up. On the other hand, among those indicating a lowerbelief in the power of prayer, those in the treatment groupactually had significant lower physical functioning scores.
Among those indicating lower belief in the power ofprayer, the treatment group had significantly greater mentalhealth scores at follow-up. There was no difference betweenthe experimental groups among the high believers in prayer.
DISCUSSION
This study was designed to assess measurable effects ofintercessory prayer in a community sample who revealed asignificant personal problem in their lives. Furthermore, wesought to investigate the role of personal belief factors inthe efficacy of prayer. Our primary outcome measures werethe degree to which the stated problem had been resolvedand the amount of concern subjects had about the problem.While there was not a significant overall direct effect ofprayer intervention on problem resolution or concern, prayerdid significantly affect problem concern depending on thesubject’s baseline belief of whether or not his or her prob-lem could be resolved. Prayer intervention appeared to ef-fectively reduce the subject’s level of concern for his or herproblem only if the subject initially believed that the prob-lem could be resolved. Those in the intervention group whodid not believe in a possible resolution for their problemwere not different from controls. Believe in prayer itselfhowever, did not modify the association between treatmentcondition and the primary outcomes.
The results of the current study underscore the role of be-lief and the subsequent efficacy of intercessory prayer. Thisis partially consistent with the numerous studies demonstrat-ing the relevance of “belief in overcoming an illness” to can-cer survival despite equivalence in medical treatment (Cas-sileth et al., 1988; Dreher 2000; Greer 1991; Halstead andFernsler, 1994; Markman, 1994; Spiegel, 1996). Those whobelieve that they can “beat” cancer are more likely to survivethan those who believe they have been defeated by cancer.Other authors discuss the relevance of belief concerning otherhealth and well-being issues as well (Richardson, 2000).
However, while belief or hope is a significant factor inthe recovery from illness, why would belief modify the treat-ment effect in a randomized trial of intercessory prayer? Par-ticipants in the current study did not know they were being“treated”; nonetheless, their belief was a condition underwhich intercessory prayer demonstrated an effect on one ofthe primary outcome measures. If those in the treatmentgroup were initially more hopeful and optimistic, or if theirproblems were not as severe as those of the subjects in thecontrol group, this may explain the treatment effect. How-ever, randomization should render these and other unmea-sured confounding variables equal across experimental con-ditions. In post hoc analysis, we found that treatment andcontrol subjects did not differ on measures of religiosity,spirituality, or life purpose, nor were the problems reportedby the two groups judged to be qualitatively different. It isin the realm of possibility that randomization did not workand treatment subjects were different on some other perti-nent unmeasured variable. Future studies might examine thiskind of belief in problem resolution to other areas of treat-ment (allopathic or not). For example, it would be relevantto know if specific problem types (emotional or social) re-spond more or less favorably to prayer depending on belief
RCT OF REMOTE INTERCESSORY PRAYER 443
TABLE 2. SAMPLE DEMOGRAPHICS BY INTERVENTION CONDITION
Control Treatment(n � 41) (n � 45) p
Age range 24–88 18–87
Age mean (SD) 55 (17.2) 54 (17.6) 0.71
Gender (% female) 58 60 0.89
Education (%)High school grad 12 6Some college 12 15College graduate 24 40Master’s degree 42 33Doctoral degree 10 4 0.35
Married (%) 76 80 0.56
Ethnicity (%)Hispanic 8 7African American 0 2Caucasian 89 91Asian 0 0Other 2 0 0.69
p values calculated using t test for baseline age and �2 (Mantel-Hanzel where appropriate) tests for differences between conditions.
SD, standard deviation.
in the resolution of the problem. Does it matter if the prayeris said specifically for the problem or is a non-specific prayeras effective? How does this interact with belief?
Secondary outcomes
Only one secondary outcome measure was directly af-fected by prayer despite belief in problem resolution or be-lief in prayer. In the models that included the belief inter-action terms (Models 2 and 3) pain scores were significantlylower in the treatment group compared to the control group.Among those with higher belief in the power of prayer, therewere significant improvements in physical functioning in theintervention group relative to the control group. Curiously,those in the intervention group with a lower belief in prayerhad a significantly worse physical function outcome. Fur-thermore, among those with a lower belief in the power ofprayer, those in the treatment group demonstrated bettermental health compared to controls. This differential treat-ment effect based on the level of belief in the power of prayer
was counter to what we would have expected. This demon-strates the complexity of the intercessory prayer phenome-non. Operating under a limited theoretical framework, onecan only speculate on aspects of the results.
Why would the potential benefits of prayer be conditionalon the belief in the power of prayer itself? We observed thata lower belief in prayer yielded positive outcomes in themental health domain and significantly worse outcomes inthe physical domain, although a higher belief yielded posi-tive results for physical function.
The paradoxical interaction of mental health with low be-lief in the power of prayer may reflect the positive correla-tion between the frequency of self-prayer and mental healthfound in other studies (Meisenhelder and Chandler, 2000).If those with an existing high belief in prayer are alreadypraying for themselves, then intercessory prayer may haveno additional benefit. This is consistent with Matthews etal. (2000), who report that while in-person prayer was aneffective adjunct to standard medical care among arthritispatients, there was no additional benefit from remote inter-
PALMER ET AL.444
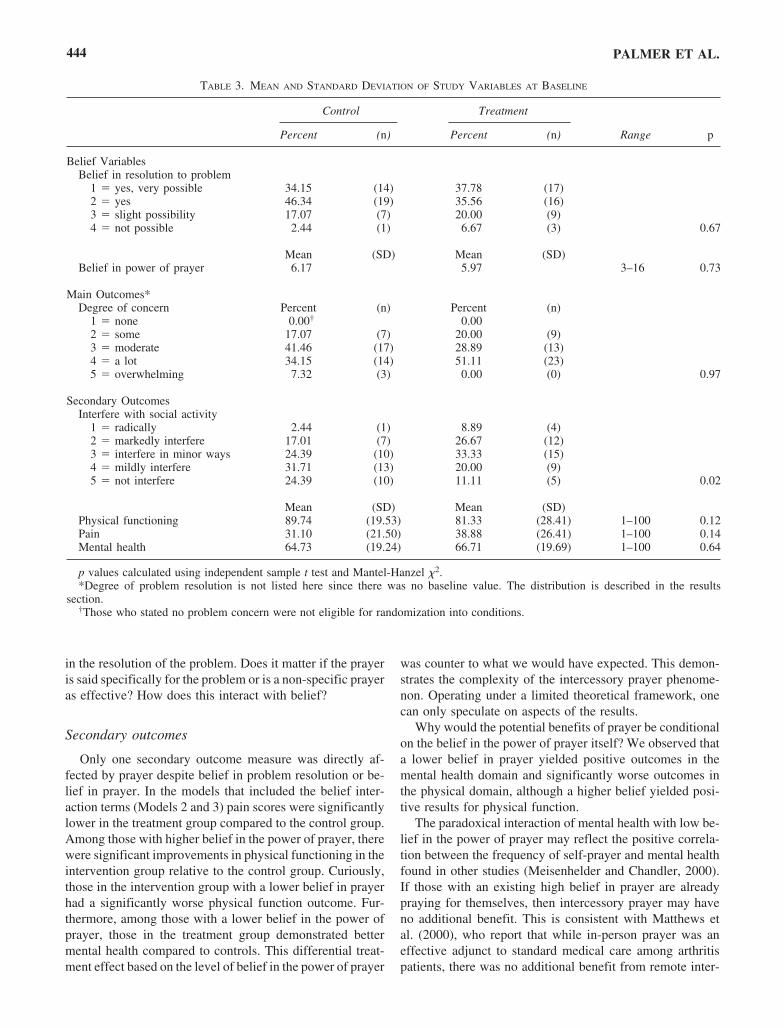
TABLE 3. MEAN AND STANDARD DEVIATION OF STUDY VARIABLES AT BASELINE
Control Treatment
Percent (n) Percent (n) Range p
Belief VariablesBelief in resolution to problem
1 � yes, very possible 34.15 (14) 37.78 (17)2 � yes 46.34 (19) 35.56 (16)3 � slight possibility 17.07 (7) 20.00 (9)4 � not possible 2.44 (1) 6.67 (3) 0.67
Mean (SD) Mean (SD)Belief in power of prayer 6.17 5.97 3–160 0.73
Main Outcomes*Degree of concern Percent (n) Percent (n)
1 � none 0.00† 0.002 � some 17.07 (7) 20.00 (9)3 � moderate 41.46 (17) 28.89 (13)4 � a lot 34.15 (14) 51.11 (23)5 � overwhelming 7.32 (3) 0.00 (0) 0.97
Secondary OutcomesInterfere with social activity
1 � radically 2.44 (1) 8.89 (4)2 � markedly interfere 17.01 (7) 26.67 (12)3 � interfere in minor ways 24.39 (10) 33.33 (15)4 � mildly interfere 31.71 (13) 20.00 (9)5 � not interfere 24.39 (10) 11.11 (5) 0.02
Mean (SD) Mean (SD)Physical functioning 89.74 (19.53) 81.33 (28.41) 1–100 0.12Pain 31.10 (21.50) 38.88 (26.41) 1–100 0.14Mental health 64.73 (19.24) 66.71 (19.69) 1–100 0.64
p values calculated using independent sample t test and Mantel-Hanzel �2.*Degree of problem resolution is not listed here since there was no baseline value. The distribution is described in the results
section.†Those who stated no problem concern were not eligible for randomization into conditions.
cessory prayer. In the present study, it is only in those withlow belief in prayer (who consequently would not be pray-ing for themselves) that intercessory prayer was effective.In fact, a post hoc comparison of the frequency of prayer(1 � more than once per day; 2 � once per day; 3 � fewtimes per week; 4 � once per week; 5 � few times permonth; 6 � once per month; 7 � less than once per month;8 � never) between the high and low belief groups showsthat the high belief group prayed every day on average(mean � 1.9) and the lower belief group prayed about onceper week on average (mean � 3.8) (p � 0.01).
Mechanism
We acknowledge that commenting on the mechanism ofaction of the “healing power of prayer” is highly prematuregiven the inconclusiveness of the existing literature. How-ever, a brief comment is made; nonetheless, to point out thatprayer efficacy does not necessarily have to involve super-natural forces. History is replete with examples of the dis-covery of healing agents/phenomena long before their mech-anism of action is known (Halperin, 2001; Mckeown, 1979,1980).
As discussed by Halperin (2001), one motivation of in-tercessory prayer research is the investigation of the phe-nomena and not to prove the existence of a divine inter-vention by an omniscient deity influencing the events in ourknown reality. Rather, this is consistent with the discussionsput forth by Levin (1996) on why prayer might be effective.
Inherent in this discussion is the possibility of a yet to bediscovered quantum reality beyond the laws of known New-tonian physics that operates in the background of the knownphysical universe. This unknown quantum space might beinfluenced by thought (under certain conditions), which inturn, may influence the physical realm. Operating in thiscontext, observational experimental studies can be designedto better comprehend this poorly understood phenomenon.
Study limitations
One of the basic limitations to this study is generaliz-ability. The sample was taken from a group of churches.They were among churches in a research network willing toparticipate in research studies investigating health and reli-gious activity. Thus, participants are from a unique samplebase of predominantly religious individuals. Further, thesample was largely well educated and white. Generalizabil-ity of these results to other groups is unwarranted.
The belief in the power of prayer items have not previ-ously been validated in prior research. Despite face validity,actual validity is unknown. However, the items demonstratea high internal consistency in this sample of participants.
While the sample size in this study was sufficient to testthe main hypothesis, there were sample size limitations. Forexample, we lacked statistical power for further analysis investigating differences between gender, age, and othergrouping factors. Lack of sufficient sample size preventedus from testing the hypothesis that those who believed both
RCT OF REMOTE INTERCESSORY PRAYER 445
FIG. 1. (A) Pre–Post means for intervention and control group. Subjects who strongly believe that the problems could be resolved.(B) Pre–Post means for intervention and control group. Subjects who yes, believed that the problems could be resolved. (C) Pre–Postmeans for intervention and control group. Subjects who slightly or did not believe that the problems could be resolved.
A
B C
in the power of prayer and in a resolution to their problemwould benefit most from a prayer intervention.
This study could not ensure a pure control group. We donot know how many individuals in the control group wereprayed for by persons outside of the current study. This lim-itation has been raised previously by both Harris et al. (2000)and Byrd (1988) and there have been no recommendationstoward correcting this potential confound. This would onlymake a difference if prayer was assumed to have a dose-re-sponse relationship with the outcome. To date, there havebeen no studies documenting such an assumption. In a posthoc analysis of the current study, we derived the number ofminutes each subject was prayed for from the prayer logsof the pray-ers. The control group was assumed to have ascore of zero. Instead of the dichotomous treatment groupvariable, we used the number of minutes prayed for in theanalysis to predict the outcomes. In fact, this variabledemonstrated the exact pattern of results reported above.Thus, the number of minutes prayed for seemed to be a proxyvariable for the treatment/control variable. However, whenwe looked for a dose-response relationship within the treat-ment group we found no significant association. This may
also be a reflection of low power because only the treatmentgroup was used. However, there was not even a trend to sug-gest a dose-response association.
Finally, researchers have raised concern about theethics of praying for someone without permission by theperson to do so (DeLashmutt and Silva, 1998; Harris etal., 2000). While the double-blinded design is essential tocontrol reporting bias in these studies, the question re-mains: is it ethical to pray for someone without their con-sent? As Harris et al. (2000) notes, the policy of the U.S.Department of Health and Human Services, Office for Hu-man Resource Protections, states the Internal ReviewBoard may waive subject consent if the research presents“no more than minimal risk of harm.” Indeed, it is rea-sonable to assume that the intentions of pray-ers are thatof compassion motivated by emotions of empathy andconcern (DeLashmutt and Silva, 1998). While it is ourview that this study was ethical in that no harm was in-tended and presumably not done, there are others thatwould disagree, noting that some individuals would be dis-tressed by being involved in a prayer study without theirknowledge or consent (Goldstein, 2000).
PALMER ET AL.446
FIG. 2. Comparison of treatment and control on secondary outcomes. Baseline and 1-month follow-up of physical function and men-tal health, from the Short Form 20 among subjects who rated high (above median split) and low on belief in the power of prayer. (A)Physical function among subjects with high belief in the power of prayer. (B) Physical function among subjects with low belief in thepower of prayer. (C) Mental health among subjects with high belief in the power of prayer. (D) Mental health among subjects with lowbelief in the power of prayer.
A B
DC

CONCLUSIONS
This study joins a relatively small, but growing line ofresearch that attempts to assess the value of intercessoryprayer. Given the variety of contexts and outcomes amongthese studies, it is not possible to generalize the results ofany of these studies beyond the population from which thesample was drawn, nor is it currently possible to estimatean overall treatment effect size. We therefore concur withRoberts et al. (2000) and others that this line of investiga-tion is complex, yet warrants further investigation.
Other research suggests that the interpersonal factors ofhealers themselves may be an important aspect of this work(Wirth et al., 1996), while other studies (Cha et al., 2001;O’Laoire, 1997; Walker et al., 1997), including the resultsof the present investigation, suggest that the participants in-dividual interpersonal belief factors are a critical componentin prayer efficacy. The potential influence of multiple fac-tors operating within an unknown theoretical frameworkrenders a significant challenge toward future investigationsof the efficacy of intercessory prayer.
ACKNOWLEDGMENTS
The authors would like to thank E. Mikaila Adams, M.A.,for her technical and editorial assistance in the preparationof this manuscript.
REFERENCES
Abbot NC. Healing as a therapy for human disease: A systematicreview. J Altern Complement Med 2000;6:159–169.
Arbuckle A, Wothke W. AMOS (Analysis of Moment Structures).Chicago: Small Waters, 1994.
Astin JA. Why patients use alternative medicine: Results of a na-tional study. JAMA 1998;279:1548–1553.
Aviles JM, Whelan SE, Hernke DA, Williams BA, Kenny KE, O’Fallon WM, Kopecky SL. Intercessory prayer and cardiovas-cular disease progression in a coronary care unit population: A ran-domized controlled trial. Mayo Clin Proc 2001;76:1192–1198.
Ballenger J, Burrows GD, DuPont RL Jr., Lesser IM, Noyes R Jr.,Pecknold JC, Rifkin A, Swinson RP. Alprazolam in panic dis-order and agoraphobia. Arch Gen Psychiatry 1998;45:413–422.
Benson H, Stark M. Timeless Healing: The Power and Biology ofBelief. New York: Scribner, 1996.
Byrd RC. Positive therapeutic effects of intercessory prayer in acoronary care unit population. South Med J 1988;81:826–829.
Cassileth BR, Walsh WP, Lusk EJ. Psychosocial correlates of can-cer survival: A subsequent report 3 to 8 years after cancer di-agnosis. J Clin Oncol 1988;6:1753–1759.
Cha KY, Wirth DP, Lobo RA. Does prayer influence the successof in vitro fertilization-embryo transfer? Report of a masked,randomized trial. J Reprod Med 2001;46:781–787.
Cohen J. Statistical Power Analysis for the Behavioral Sciences.Mahwan, NJ: Erlbaum, 1988.
Collipp P. The efficacy of prayer: A triple blind study. Med Times1969;97:201–204.
DeLashmutt M, Silva MC. The ethics of long-distance interces-sory prayer. Nurs Connections 1989;11:37–40.
Dossey L. Healing Words. San Francisco: Harper Collins, 1993.Dreher H. Beyond fighting spirit: What mind-states influence can-
cer survival? Adv Mind Body Med 2000;16:120–127.Eisenberg DM, Davis RB, Ettner SL, Appel S, Wilkey S, Van
Rompay M, Kessler RC. Trends in alternative medicine use inthe United States, 1990–1997: Results of a follow-up nationalsurvey. JAMA 1998;280:1569–1575.
Eisenberg DM, Kessler RC, Van Rompay MI, Kaptchuk TJ,Wilkey SA, Appel S, Davis RB. Perceptions about comple-mentary therapies relative to conventional therapies amongadults who use both: Results from a national survey. Ann InternMed 2001;135:344–351.
Fetzer Institute. Multidimensional Measurement of Religiousness/Spirituality for use in Health Research. National Institute on AgingWorking Group. Kalamazoo, MI: Fetzer Institute, 1999.
Frarran CK, Herth KA, Popovich JM. Research on Hope and Hope-lessness. In: Hope and Hopelessness: Critical Clinical Con-structs. Thousand Oaks, CA: Sage, 1995.
Goldstein J. Waiving informed consent for research on spiritualmatters? Arch Intern Med 2000;160:1870–1878.
Greer S. Psychological response to cancer and survival. PsycholMed 1991;21:43–49.
Halperin EC. Should academic medical centers conduct clinical tri-als of the efficacy of intercessory prayer? Acad Med 2001;76:791–797.
Halstead MT, Fernsler JI. Coping strategies of long-term cancersurvivors. Cancer Nurs 1994;17:94–100.
Harris WAS, Gowda M, Kolb JW. Strychacz CP, Vacek JL, JonesPG, Forker A, O’Keefe JH, McCallister BD. A randomized, con-trolled trial of the effects of remote, intercessory prayer on out-comes in patients admitted to the coronary care unit. Arch In-tern Med 2000;159:2273–2278.
Hilakivi-Clarke L, Rowland J, Clarke R, Lippman ME. Psychoso-cial factors in the development and progression of breast can-cer. Breast Cancer Res Treat 1994;29:141–160.
Joyce C, Welldon B. The objective efficacy of prayer. J Chron Dis1965;18:367–377.
Karren KJ, Hafen BQ, Smith NL, Frandsen KJ. Mind Body andHealth: The Effects of Attitudes, Emotions, and Relationships.Boston: Allyn and Bacon, 2002.
Larson D. Scientific Research on Spirituality and Health: A Con-sensus Report. Rockville, MD: National Institute for Health CareResearch, 1997.
Leibovici L. Effects of remote, retroactive intercessory prayer onoutcomes in patients with bloodstream infection: A randomizedcontrolled trial. Br Med J 2001;323:1450–1451.
Levin JS, Larson DB, Puchalski CM. Religion and spirituality inmedicine: Research and education. JAMA 1997;278:792–793.
Levin JS. How prayer heals: A theoretical model. Altern TherHealth Med 1996;2:66–73.
Mackenzie ER, Rajagopal DE, Meibohm M, Lavizzo-Mourey R.Spiritual support and psychological well-being: Older adults’perceptions of the religion and health connection. Altern TherHealth Med 2000;6:37–45.
Markman M. Cancer survival and the mind. J Cancer Res Clin On-col 1994;120:443–444.
RCT OF REMOTE INTERCESSORY PRAYER 447

Matthews DA, Marlowe SM, MacNutt FS. Effects of intercessoryprayer on patients with rheumatoid arthritis. South Med J2000;93:1177–1786.
McCullagh P. Regression models for ordinal data. J R Stat Soc[Ser B] 1980;42:109–142.
McKeown T. Mans Health the past and future. West J Med1980;132:49–57.
McKeown T. The Role of Medicine: Dream Mirage or Nemesis?Princeton, NJ: Princeton University Press, 1979.
Meisenhelder J, Chandler E. Prayer and health outcomes in churchmembers. Altern Ther Health Med 2000;6:56–60.
O’Laoire S. An experimental study of the effects of distant, inter-cessory prayer on self-esteem anxiety, and depression. AlternTher Health Med 1973;3:38–53.
Oldnall AS. On the absence of spirituality in nursing theories andmodels. J Adv Nurs 1995;21:417–418.
Peterson C, Bossio LM. Chapter 3. Health and Optimism. NewYork: The Free Press, 1991:214.
Rabinowitz S, Melamed S, Kasan R, Ribak J. Personal determi-nants of health promoting behavior. Public Health Rev 1992;20:5–14.
Richardson RL. Where there is hope, there is life: toward a biol-ogy of hope. J Pastoral Care 2000;54:75–83.
Roberts L, Ahmed I, Hall S. Intercessory prayer for the alleviationof ill health. Cochrane Database System Rev 2000:CD0003688.
Shaffer JP. Multiple hypothesis testing. Annu Rev Psychol1995:561–584.
Spiegel D. Cancer and depression. Br J Psychiatry Suppl 1996:109–116.
Stewart A, Hays R, Wan J. Medical Outcomes Study short formgeneral health survey. Med Care 1988;26:724–735.
Walker SR, Tonigan JS, Miller WR, Corner S, Kahlich L. In-tercessory prayer in the treatment of alcohol abuse and de-pendence: A pilot investigation. Altern Ther Health Med1997;3:79–86.
Wirth D, Mitchekk B. Complementary healing therapy for patientswith Type 1 Diabetes Mellitus. J Sci Explor 1994;8:350–361.
Wirth DP, Richardson JT, Eidelman WAS. Wound healing andcomplementary therapies: A review. J Altern Complement Med1996;2:493–502.
Wirth DP. The significance of belief and expectancy within thespiritual healing encounter. Soc Sci Med 1995;41:249–260.
Address reprint requests to:Raymond F. Palmer, Ph.D.
Department of Family and Community MedicineUniversity of Texas Health Science Center
at San Antonio7703 Floyd Curl Drive, MC 7795
San Antonio, TX 78229-3900
E-mail: [email protected]
PALMER ET AL.448