Embed Size (px)
Citation preview

ORTON Orthopaedic Hospital
Invalid Foundation Helsinki, Finland
consultation compared to specialist consultation alone for
chronic low back pain
Leena Niemistö
Academic dissertation
To be publicly discussed with the permission of the Medical Faculty of the University of Helsinki, in the auditorium of the Invalid Foundation,
Tenholantie 10, Helsinki, on May 13th, at 12 noon.
Helsinki 2005
3
therapy, stabilizing exercises, and specialist
A randomized controlled trial of combined manipulative
Author’s address: Leena Niemistö Dextra Medical Center Raumantie 1a 00350 Helsinki Finland Supervised by: Docent Karl-August Lindgren, MD, PhD ORTON Orthopaedic Hospital Invalid Foundation Helsinki, Finland Docent Heikki Hurri, MD, PhD ORTON Orthopaedic Hospital Invalid Foundation Helsinki, Finland Reviewed by: Docent Simo Taimela, MD, PhD DBC International Helsinki, Finland Docent Antti Malmivaara, MD, PhD Finnish Office for Health Care Technology Assessment Helsinki, Finland Discussed with: Docent Olavi Airaksinen, MD, PhD Kuopio University Central Hospital Kuopio, Finland ISBN 952-9657-27-7
ISSN 1455-1330 Yliopistopaino 2005 Cover: Harry Kivijärvi
4
ISBN 952-10-2466-6 (PDF)

To Kari, Kai, Karri, and Henri
5

6

CONTENTS LIST OF ORIGINAL PUBLICATIONS 9 LIST OF ABBREVIATIONS 10 ABSTRACT 11 1 INTRODUCTION 13 2 REVIEW OF THE LITERATURE 15 2.1 Multidimensional aspects of LBP 15 2.2 Biomechanical factors of LBP 17 2.2.1 Spinal stability 17 2.2.2 Clinical instability 18 2.2.3 Motor control and CLBP 19 2.3 Psychosocial factors of LBP 21 2.3.1 Psychosocial factors as determinants of treatment outcome 22 2.4 Effectiveness of conservative treatment for CLBP 23 2.4.1 Spinal manipulative therapy 23 2.4.2 Scientific evidence for manipulative therapy 25 2.4.3 Scientific evidence for exercise therapy 26 2.4.4 Scientific evidence for the cognitive-behavioral approach 28 2.4.4.1 Back school 29 2.4.4.2 Educational booklet 29 2.4.4.3 Physician consultation 30 2.5 Cost-effectiveness of the conservative treatment for LBP 31 2.5.1 Cost-effectiveness of manipulative therapy 31 2.5.2 Cost-effectiveness of exercise therapy 32 3 AIMS OF THE STUDY 34 4 STUDY OUTLINE (I, II, III, IV) 35 4.1 Study design and population 35 4.2 Assignment 36 4.3 Masking and ethical concerns 37 4.4 Participant flow and follow-up 37 4.5 Baseline characteristics (I, II, III, IV) 39 5 METHODS 40 5.1 Interventions (I, II, III, IV) 40 5.1.1 Manipulative therapy, stabilizing exercises, and specialist consultation (Combination group) 40 5.1.2 Specialist consultation (Consultation group) 41 5.2 Outcome measures (I, II, III, IV) 41
7
5.3 Statistical analysis 44

6 RESULTS 47 6.1 Outcomes 47 6.1.1 Subjective pain and disability (I, II, III, IV) 47 6.1.2 Health-related quality of life (I, III) 49 6.1.3 Use of health care services (I, III) 50 6.1.4 Cost analysis (I, III) 53 6.1.5 Satisfaction with care (IV) 56 6.1.6 Physical activity 56 6.1.7 Clinical variables 59 6.1.7.1 Reliability of the functional measurements 59 6.1.7.2 Changes in functional measurements 60 6.2 Predictive factors for unfavorable recovery (II) 60 6.2.1 Univariate analysis 60 6.2.2 Multivariate analysis 63 6.3 Psychosocial differences as determinants of treatment outcome (IV) 63 7 DISCUSSION 66 7.1 Principal findings 66 7.2 Strengths and limitations 67 7.2.1 Subjects 67 7.2.2 Methods 67 7.2.2.1 Spinal manipulative therapy 67 7.2.2.2 Stabilizing exercises 68 7.2.2.3 Cognitive-behavioral approach 69 7.2.3 Outcomes 69 7.2.3.1 Pain and disability 69 7.2.3.2 Cost-effectiveness 70 7.2.3.3 Psychosocial determinants (MPI subgroups) 71 7.2.3.4 Physical activity (MetPro®) 71 7.2.3.5 Functional changes 72 7.3 Results in relation to other studies 73 7.3.1 Effectiveness of spinal manipulative therapy and exercises (I, III) 73 7.3.2 Predictive factors for unfavorable treatment outcome (II) 74 7.3.3 Psychosocial factors as determinants of treatment outcome (IV) 74 7.4 Meaning of the study 75 7.5 Implications for practice and research 77 8 CONCLUSIONS 78 9 ACKNOWLEDGEMENTS 79 10 REFERENCES 81 ORIGINAL PUBLICATIONS
8
LIST OF ORIGINAL PUBLICATIONS
The thesis is based on the following articles, which are referred to in the text by the Roman numerals I to IV. I Niemistö L, Lahtinen-Suopanki T, Rissanen P, Sarna S, Lindgren KA,
Hurri H. A randomized trial of combined manipulation, stabilizing exer-cises, and physician consultation compared to physician consultation alone for chronic low back pain. Spine 2003;28(19):2185-91.
II Niemistö L, Sarna S, Lahtinen-Suopanki T, Lindgren KA, Hurri H. Predic-
tive factors for 1-year outcome of chronic low back pain following ma-nipulation, stabilizing exercises, and physician consultation or physician consultation alone. J Rehabil Med 2004;36(3):104-9.
III Niemistö L, Rissanen P, Sarna, S, Lahtinen-Suopanki T, Lindgren KA, Hurri H. Cost-effectiveness of combined manipulation, stabilizing exer-cises, and physician consultation compared to physician consultation alone for chronic low back pain: A prospective randomized trial with two years' follow-up. In press in Spine.
IV Riipinen M, Niemistö L, Lindgren KA, Hurri H. Psychosocial differences
as determinants of treatment outcome after combined manipulation, stabi-lizing exercises, and physician consultation or physician consultation alone. In press in J Rehabil Med.
9
Original publications are reprinted with the permission of the publishers.

LIST OF ABBREVIATIONS
AC Active copers CBA Cognitive-behavioral approach CLBP Chronic low back pain
CLT Contralateral test
DYS Dysfunctional
GP general practitioner
HRQOL Health-related quality of life
ID Interpersonally distressed
LBP Low back pain
MET Metabolic equivalent
MPI Multidimensional Pain Inventory
ODI Oswestry disability index
RCT Randomized controlled trial
RT Reaction time
SIJ Sacroiliac joint
SIMPI Finnish version of Multidimensional Pain Inventory
SLR Straight-leg raising test
TENS Transcutaneous electrical nerve stimulation
VAS Visual analogue scale
WHO The World Health Organization
10

ABSTRACT The aim of this study was to assess the effectiveness, as well as cost-effectiveness, of combined manipulative therapy, stabilizing exercises, specialist consultation, and patient education (combination treatment) compared with that from specialist con-sultation and patient education alone (consultation) for chronic low back pain (CLBP). Secondary objectives were to examine the predictive factors for one-year unfavorable outcome of CLBP and psychosocial differences as determinants for recovery from CLBP following the combination treatment or specialist consultation alone. Additionally, the aim was to assess the changes in physical activity between groups at one year and changes in functional variables between the groups at five months.
Of 204 CLBP patients, 102 were randomized to a combination group and 102 to a consultation-alone group. All patients were clinically examined, informed about back pain, and encouraged to stay active and exercise according to specific instructions based on clinical evaluation. Treatment in the combination group in-cluded four sessions both of manipulative therapy and of stabilizing exercises aimed at correcting motor control of the trunk. Subjective pain, disability, health-related quality of life, physical activity, coping strategies, satisfaction with care, days of sick leave, consumption of health services, and costs were assessed by several ques-tionnaires. For predictive analysis of treatment outcome, sociodemographic charac-teristics, work ability, and psychological variables were evaluated and functional assessments performed.
Significant improvement occurred in both groups on every self-rated out-come measurement. Within two years, the combination group showed only slightly more significant reduction on the Visual analogue scale (VAS) and clearly greater patient satisfaction than in the consultation group. Specialist consultation alone was more cost-effective in view of both health care use and work absenteeism, and led to an increase in health-related quality of life equal to that from the combination treat-ment. Patients in the consultation group also tended to increase their intensity of physical exercise, other activities, and their active time more than did those in the combination group.
Psychometric factors, longer previous sick-leave days, and a low to mod-erate level of pain intensity proved strongly to predict unfavorable treatment out-come. The Multidimensional Pain Inventory (MPI) was used to identify three patient subgroups to determine treatment outcome. These subgroups were active copers (AC), interpersonally distressed (ID), and dysfunctional (DYS) patients. They were distinguished by level of pain severity, affective distress, life control, and of activity.
11

In this study, MPI patient profile clustering determined the slightly greater effec-tiveness of the combination therapy than of the consultation alone. The effectiveness of combination therapy was due to the large changes among the dysfunctional (DYS) patients, who gained an extra advantage from combination therapy both in perceived disability (ODI) and pain intensity (VAS). The advantage for ODI disap-peared at the two-year follow-up due to the improving trend among the DYS pa-tients in the consultation group. The advantage for pain intensity remained through-out the follow-up. For the AC and ID patients, the consultation alone was as effec-tive as the combination treatment.
Both the specialist consultation group and the combination treatment group showed unexpectedly good improvement regarding pain, disability, and health-related quality of life. The combination treatment including manipulative therapy, stabilizing exercises, and specialist consultation did not clearly enhance the effect gained by the specialist consultation alone. A subgroup of dysfunctional patients appeared, however, to be more sensitive to the combination treatment, needing more repetition and fortification of the information with hands-on therapy and exercises.
12
Key words: low back pain, randomized controlled trial, spinal manipulation, cost-effectiveness, treatment outcome, predictor, psychosocial variables

1 INTRODUCTION Chronic low back pain (CLBP) and mental depression are, in Finland, the two most common complaints leading to work loss and early retirement. CLBP may with good reason be considered a medical disaster in most Western societies, causing human suffering, disability, and tremendous economic consequences with the fre-quent use of health care services and work absenteeism. Despite developments in modern medicine in general and growing knowledge of spinal diseases, the problem of nonspecific LBP remains unsolved, although the nonspecific type affects ap-proximately 85% of patients reporting any back pain. Approximately 40% of LBP patients worry that pain affects their work ability, that it will cripple them, or that it underlies some serious disease (Waddell 1998). Better understanding of multidimen-sional aspects has widened our concept of LBP.
A common clinical finding in LBP patients is decreased range of motion of the spine with increased paraspinal activity. Disturbances in neuromuscular control have also been frequently connected with CLBP and considered a possible linkage between pain and disability (Hodges and Moseley 2003). These impaired functions recover with treatment or active rehabilitation (Ebenbichler et al. 2001). Spinal ma-nipulative therapy is commonly recommended for LBP, although previous system-atic reviews and practice guidelines have produced discordant findings as to the effectiveness of this therapy (Assendelft et al. 2003a). A recent focus in the man-agement of CLBP patients has been the specific training of the deep abdominal (in-ternal oblique and transversus abdominis) and lumbar multifidus muscles. The pri-mary role of these muscles is considered to be the provision of dynamic stability and segmental control of the spine (Richardson and Jull 1995). For the treatment of CLBP with radiological diagnosis of spondylolysis or spondylolisthesis, one ran-domized controlled trial (RCT) of specific stabilizing exercises showed significant and longer-lasting reduction in pain intensity and functional disability levels than did other commonly prescribed conservative treatment programs (O'Sullivan et al. 1997).
It has also been shown that subacute LBP patients can be treated success-fully with an approach that includes a clinical examination and patient information concerning the nature of the problem to reduce fear and to motivate them to resume light activity (Indahl et al. 1995; Karjalainen et al. 2003). This program does not necessarily relieve pain noticeably, but has a clear impact on work absenteeism and the bothersomeness of the symptoms.
13

Because medical history and clinical examination constitute a cornerstone in the evaluation of common LBP patients, “the basic principles of clinical practice should be to exclude serious disease, to identify the patients likely to become dis-abled, to provide the rational basis for management aiming to restore the function, to relieve fear associated with back pain, to activate, and encourage the patients with LBP” (Waddell 1998). Dysfunction, in general, depends on the imbalance between physical stresses and individual vulnerabilities; it may be self-sustaining. Thus, even if the symptoms persist indefinitely, dysfunction does not involve any permanent change and is therefore reversible. Despite the chronic dysfunction and symptoms, there is still potential for recovery by restoration of normal function.
The aim of the present study was to compare the effectiveness and cost-effectiveness of combined spinal manipulative therapy, stabilizing exercises, and specialist consultation for CLBP with specialist consultation alone. Specialist con-sultation partly based on a protocol such as that by a Norwegian group (Indahl et al. 1995) was considered the most cost-effective alternative for economic effectiveness evaluation. The hypothesis was that this combination therapy with advice, encour-agement, and individual exercise instruction would reduce pain and disability, in-crease health-related quality of life (HRQOL), and save costs (by reducing work absenteeism and use of health care) more than would merely the specialist consulta-tion. In addition, the attempt was to focus on psychosocial differences as determi-nants of treatment outcome.
14
2 REVIEW OF THE LITERATURE
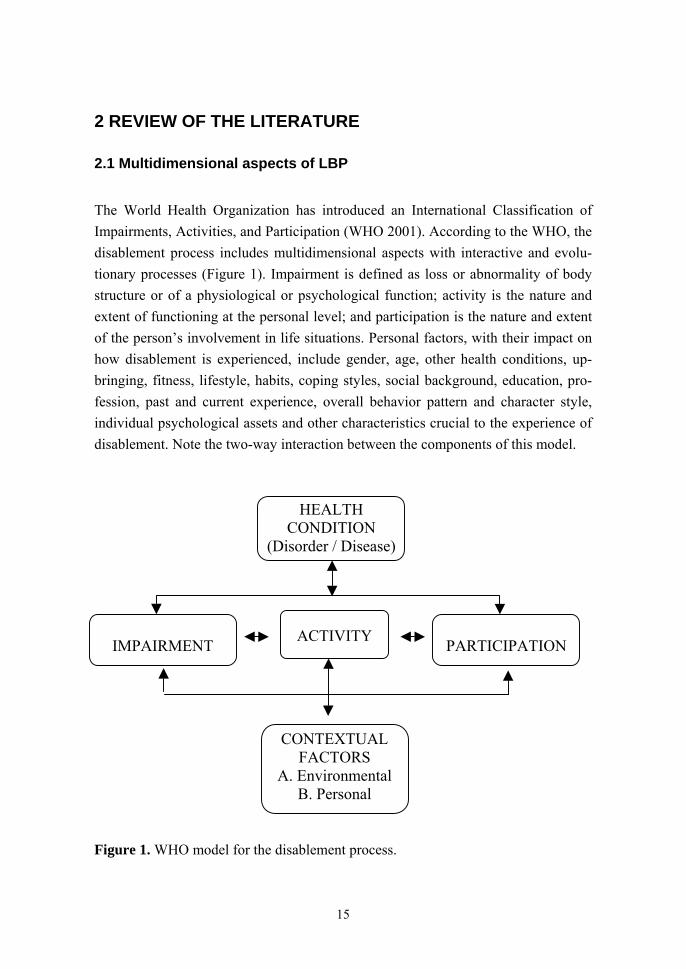
2.1 Multidimensional aspects of LBP The World Health Organization has introduced an International Classification of Impairments, Activities, and Participation (WHO 2001). According to the WHO, the disablement process includes multidimensional aspects with interactive and evolu-tionary processes (Figure 1). Impairment is defined as loss or abnormality of body structure or of a physiological or psychological function; activity is the nature and extent of functioning at the personal level; and participation is the nature and extent of the person’s involvement in life situations. Personal factors, with their impact on how disablement is experienced, include gender, age, other health conditions, up-bringing, fitness, lifestyle, habits, coping styles, social background, education, pro-fession, past and current experience, overall behavior pattern and character style, individual psychological assets and other characteristics crucial to the experience of disablement. Note the two-way interaction between the components of this model. HEALTH
CONDITION (Disorder / Disease)
IMPAIRMENT
ACTIVITY
PARTICIPATION
CONTEXTUAL FACTORS
A. Environmental B. Personal
Figure 1. WHO model for the disablement process.
15

It is widely recognized that LBP and disability can be understood and managed only according to a biopsychosocial model that suits the WHO model. Low back disabil-ity depends to some extent on degree of objective physical impairment, but all analyses show that it depends to a much greater extent on psychosocial factors. Psy-chosocial factors play a particularly important role in the development of chronic pain and disability (Waddell and Waddell 2000).
Studies on acute or subchronic patients in primary care with LBP reveal several factors linked to persistence of symptoms and progression to chronicity in LBP: high levels of psychological distress (Burton et al. 1995; Thomas et al. 1999), catastrophizing (Burton et al. 1995), dissatisfaction with employment (Coste et al. 1994; Thomas et al. 1999), longer duration of symptoms (Thomas et al. 1999; van den Hoogen et al. 1997), previous history of LBP (Burton et al. 1995; Coste et al. 1994), radiating pain (Thomas et al. 1999), higher initial disability level (Coste et al. 1994; Gatchel et al. 1995), and high compensation status (Coste et al. 1994; Gatchel et al. 1995). Young age, female gender, few sick-leave days before treatment, and low baseline severity of back pain have been identified as predictive of outcome in a functional restoration program, but also in outpatient programs with shorter follow-up and with no treatment at all (Bendix et al. 1998). The probability of a patient’s return to work and the reduction in pain intensity after an 8-week program of func-tional restoration and behavioral support was mainly based on reduction in subjec-tive feelings of disability (Hildebrandt et al. 1997). Neither medical background, diagnosis, nor physical impairment was of any predictive value. Other similar stud-ies confirm that the changes in patients’ beliefs about their pain are crucial in deter-mining the success of a multimodal treatment program (Pfingsten et al. 1997), or an active exercise program (Mannion et al. 2001), as described in Study II (Niemistö et al. 2004)
This study defines the CLBP as a multidimensional problem including pain, functional disability, and psychosocial and socioeconomic consequences. The course of back pain for most primary care patients is recurrent, characterized by variation and change, rather than having an acute self-limiting course or being chronic in the usual sense of these terms, which suggests that classifying patients with back pain as acute or chronic based on the duration of the initial episode alone may be inadequate (Von Korff and Saunders 1996). The overloading of spinal struc-tures leads to micro-injuries, inflammation, pain, and neuromuscular dysfunction (Claude et al. 2003; Solomonow et al. 2003a), which has been associated with clini-cal pain (Indahl 1999; Solomonow et al. 2003b). Even if the psychosocial compo-
16

nent is of importance in CLBP, the biomechanical factors should never be neglected but carefully evaluated.
2.2 Biomechanical factors of LBP
2.2.1 Spinal stability Several biomechanical mechanisms have been associated with CLBP: Degeneration, muscular dysfunction, and spinal instability are those most often discussed recently. The instability has traditionally been associated with the presence of abnormal mo-tion at the end-point of the range, even though instability has long been linked to degenerative disease where the segment may show a loss in total motion (Jayaraman et al. 1994; Kaigle et al. 1998). A link between motion and LBP may be found in the pattern of motion instead of the absolute magnitude of motion. Control of interseg-mental motion around the neutral zone has been identified as a major parameter of clinical spinal instability (Panjabi 1992). The load-deformation behavior of the spi-nal segment is non-linear and highly flexible in the vicinity of the neutral position, called the neutral zone. In this region of physiological intervertebral motion, the motion occurs against minimal internal resistance, with the ligamentous structures providing restraint in the elastic zone to limit the end-range of motion. In a study with porcine cervical spines exposed to high-speed trauma, the neutral zone in-creased to a greater extent than did the range of motion, and was the first indicator of onset of injury (Oxland and Panjabi 1992). In another study, after application of external fixation to cadaver cervical spine specimens, motion in the neutral zone decreased 71% compared to a 38% decrease in the total range of motion (Panjabi 1992).
Other motion pattern parameters addressed in experimental and clinical settings include instantaneous axis of rotation (Gertzbein et al. 1985), motion path-ways during complete trunk motion (Indahl et al. 1997; Kaigle et al. 1997), the asymmetry of motion (Lund et al. 2002a; Mellin et al. 1995), and the patterns of coupled motions (Lund et al. 2002a; Pearcy et al. 1985). Lund et al. (2002a), using an accurate measuring technique, measured the 3-D intervertebral motion patterns of CLBP patients during active trunk motions. They found significant differences in the symmetry during active flexion-extension and lateral bending plus coupling patterns during active lateral bending motion in the CLBP patients as compared to previous
17

data on asymptomatic subjects. Preserved motion at the suspected symptomatic lev-els before lumbar fusion surgery, although significantly reduced from normal mo-tion, was correlated with a good mid-term result from lumbar fusion surgery in cases with a positive external spinal-fixator test result (Lund et al. 2002b).
Normally, recruitment of paraspinal muscles may be coordinated opti-mally regardless of the position, which allows them to provide sufficient support for different structures in order to counteract detrimental forces and prevent injury (Indahl 1999). Sensory properties of ligaments are related to the γ spindle system, which in turn can determine muscle stiffness, coordination, movement, and position sense. Decreased γ support to a muscle may therefore be connected with poor joint stability (Richardson et al. 1999a). 2.2.2 Clinical instability Clinical instability of the spine is an intensely controversial subject (Boden and Wiesel 1990; Gardner-Morse et al. 1995; Gertzbein et al. 1985; Pope and Panjabi 1985; Stokes and Gardner-Morse 1995a; 1995b), and its diagnosis, especially in the aging, difficult. Both the clinical presentation and radiographic manifestations alone such as traction spurs (Bram et al. 1998), excessive sagittal translation and angular motion in flexion-extension (Soini et al. 1991; Stokes and Frymoyer 1987), high-intensity zone, endplate abnormalities, and bone marrow changes, especially Modic type 1 findings (Braithwaite et al. 1998; Carragee et al. 2000; Ito et al. 1998; Lam et al. 2000; Weishaupt et al. 2001) are non-specific regarding instability. Therefore, the diagnosis of clinical instability lies in understanding the biomechanics involved, in recognizing the relevant radiographic manifestations, and most importantly, in cor-relating those observations with the patient's clinical history and physical examina-tion (Vo and MacMillan 1994).
Farfan and Gracovetsky (1984) stated that clinical instability is a “symp-tomatic condition where, in the absence of new injury, a physiologic load induces abnormally large deformations at the intervertebral joint”. Evidence for the sensitiv-ity of and increase in the neutral zone relating to spinal instability has led to another definition of clinical instability: a significant decrease in the capacity of the spinal stabilizing system to maintain the intervertebral neutral zones within physiological limits, resulting in pain and disability (Panjabi 1992).
18

The instability concept in LBP has recently been challenged, and the importance of the neural control system has been emphasized instead. Based on recent studies in kinematics and stabilization (Lund 2003), it would be more precise to replace the term “instability” with mechanical LBP defined as incongruent and painful motion. The potential pathomechanism behind this instability may be a dysfunction of the neuromuscular control system. The stabilizing exercises used in the present study are based on the concept of restoring the eventual increased neutral zone to physio-logical limits. It is not a question of stiffening the spine and restriction of spinal motion, but rather maintaining the equilibrium in the posture by active movement (Hodges 2003).
All these findings suggest that the biomechanical problem with LBP is not so much an issue of strength or endurance but rather one of motor control. To achieve lasting effects, the treatment of acute or chronic low back disorder should therefore include exercises for restoring motor control.
2.2.3 Motor control and CLBP Impaired postural control is associated with chronic lumbar disorders (Luoto et al. 1996). A slow psychomotor reaction time is associated with LBP, as well (Taimela et al. 1993). Whether the poor postural control is a consequence of LBP or a major cause of the disorder is not known, but recent data indicate that experimentally in-duced pain may replicate some of the changes identified in those with LBP (Hodges and Moseley 2003).
Studies on CLBP patients have broadened our insight into the pathophysi-ology of motor control of lumbar spine stability. Normally, upper or lower limb voluntary movements evoke non-conscious muscle activation in the trunk muscles via a feed-forward mechanism (Hodges and Richardson 1996; 1998). A similar feed-forward mechanism appears in the paraspinal musculature during sudden upper limb loading (Leinonen et al. 2002a). This is regulated by the central movement control system, which maintains postural stability and prepares the trunk to bear a poten-tially increasing load by activating certain trunk muscles. In LBP patients, delayed contraction of trunk muscles, which results in reduced stiffness of the spine at the time of initiation of the movement, occurs when the equilibrium of the spine is dis-turbed by rapid movements of the upper or lower limbs (Hodges and Richardson 1996; 1998). Visual expectation reduces the response latency of paraspinal muscle
19

activity prior to the onset of the postural disturbance in the uncontrolled position in asymptomatic subjects (Leinonen et al. 2002a), but not in disc herniation-related back pain (Leinonen et al. 2001). Patients with clinically observed motor weakness had fewer shortened latencies by expectation at baseline, but after surgery they re-sponded like the controls although they showed longer latencies during the unex-pected trials (Leinonen et al. 2003). The lumbar spinal stenosis patients had a sig-nificantly poorer ability to sense a change in their lumbar position than did healthy controls and sciatica patients (Leinonen et al. 2002b).
Acute experimentally induced pain may affect feed-forward postural activ-ity of the trunk muscles, with consistent impairment of transversus abdominis activ-ity (Hodges et al. 2003). Induced LBP did not change the reaction time (RT) of the arm movement, had variable effects on RT of the superficial trunk muscles, but con-sistently led to increased RT of the deepest abdominal muscles. The effect of the attention-demanding task was the opposite: increased RT of the movement and the superficial trunk muscles but no effect on RT of the deep trunk muscles. Thus, acti-vation of the deep trunk muscles occurred earlier than did the movement. When the attention-demanding task was made stressful, the RT of the movement and superfi-cial trunk muscles was unchanged, but the RT of the deep trunk muscles increased. Thus, the temporal relationship between deep trunk muscle activation and arm movement was restored. This means that although postural activation of the deep trunk muscles is not affected when central nervous system resources are limited during an attention-demanding task, it is delayed when the individual is also under stress. However, a non-painful attention-demanding task does not replicate the effect of pain on postural control of the trunk muscles, even when the task is stressful (Moseley et al. 2004).
Active physical rehabilitation has been claimed to restore impaired neuro-muscular function (Wilder et al. 1996), but the opposite findings also exist. Impaired postural control has failed to improve after intense three-week in-patient rehabilita-tion and in the poor-outcome group even deteriorated (Luoto et al. 1998). The role played by the impaired neuromuscular control of spinal stability among CLBP pa-tients is widely accepted. Therefore, randomized controlled trials on the effects of stabilizing exercises in CLBP are clearly necessary.
20

2.3 Psychosocial factors of LBP Psychological factors may be related to the onset, development, and treatment out-come of spinal pain problems. Weiser and Cedraschi (1992) conducted a systematic literature review concerning psychosocial factors in CLBP. They found psychologi-cal distress as measured by the Minnesota Multiphasic Personality Inventory (MMPI) to relate to outcome. Cognitive factors such as coping and illness beliefs were related to recovery in chronic sufferers, with some evidence for their relation-ship to the development of the problem. Job satisfaction and stress predicted the outcome as well. Linton (2000a) examined the reviews already conducted examin-ing the relationship between psychosocial factors and neck or back pain. His search for prospective studies found 36 investigations, but no support for a “pain-prone” personality. Significant findings seemed related to personality disorders such as depression and anxiety. Stress, distress, or anxiety was reported in 11 studies, all of which found a significant relationship. Mood and depression were investigated in 16 articles, of which 14 indicated that depressed mood increases risk for pain problems. Eight of nine studies found a significant relationship between chronicity and cogni-tive functioning, including fear-avoidance beliefs and coping strategies. Finally, six of seven studies suggested that high levels of pain behavior and dysfunction served as risk factors for future back pain problems.
According to Linton’s (2000a) systematic review on prospective studies, strong evidence exists that psychosocial factors are strongly linked to the transition from acute to chronic pain disability and that they can be associated with reporting of onset of back and neck pain. Strong evidence also exists that psychosocial vari-ables generally have more impact than biomedical or biomechanical factors on back pain disability, and that attitudes, cognition, and fear-avoidance beliefs are strongly related to development of pain and disability. Depression, anxiety, distress, and re-lated emotions are strongly related to pain and disability as well (level A evidence). Poor self-perceived health is moderately related to chronic conditions (level A evi-dence), and psychosocial factors are moderate predictors for long-term pain and disability (level A/B evidence).
21

2.3.1 Psychosocial factors as determinants of treatment outcome How psychosocial patient characteristics affect rehabilitation outcome is a major concern for chronic pain rehabilitation. One attempt to classify patient subgroups for predicting rehabilitation outcome is the Multidimensional Pain Inventory (MPI), with its patient profile types (Kerns et al. 1985; Rudy et al. 1989b). Of these types, adaptive copers (AC) have lower levels of pain severity, interference with activities, affective distress, and greater perceptions of life control and activity level. Those interpersonally distressed (ID) show lower levels of social support and lower scores on solicitous and distracting responses from significant others. Dysfunctionals (DYS) show higher level of pain severity, pain markedly interfering with everyday life, high affective distress, low perceptions of life control, and low level of activity.
The few follow-up studies explore whether patients with different profiles respond differently to standard multidisciplinary treatment including psychosocial treatment components. The patients of Rudy et al. (1995) had temporomandibular disorders (TMD) and participated in conservative, standardized treatment including stress management. Turk et al. (1998) found those with fibromyalgia syndrome re-sponding in their unique manner to a standard multidisciplinary treatment program. In both studies, DYS patients showed the greatest degree of improvement, although at baseline, they had demonstrated higher levels of pain and lifestyle interference, and higher levels of depression and negativity. Their improvement in this regard was also the greatest after rehabilitation. Bergström et al. (2001) used a vocational reha-bilitation program without psychosocial components for chronic spinal pain patients, finding no effect favoring any profile group. Although all patients showed im-provement in general health status after rehabilitation, the DYS and ID patients re-mained at a lower level than did AC patients at baseline and throughout the 18-month follow-up. DYS patients also showed significantly more registered sick leaves from work and reported more need for health care both at baseline and after follow-up.
At present, no studies seem to compare various treatment elements with various patient groups. For this reason, it is unclear whether these DYS patients were favored because of the suggested need-specific treatment elements or whether they would have benefited from treatment without any psychosocial elements in-tended. Characteristic of DYS patients are their lower pain tolerance, greater pain-related anxiety, and their avoidance behavior. Without rehabilitation, such patients
22

tend to develop chronic illnesses (Asmundson et al. 1997; McCracken et al. 1999), as a result, are likely to react differently to treatment and rehabilitation. To make MPI patient clustering clinically useful and for more effective patient care, this pos-sibility requires examination in the controlled study setting.
2.4 Effectiveness of conservative treatment for CLBP According to the latest extensive systematic review on the effectiveness of various interventions for treatment of CLBP, strong evidence exists for the effectiveness of manual therapy, exercise therapy, multidisciplinary pain treatment programs, and spa therapy, especially with regard to short-term effects (van Tulder et al. 2000b). Moderate evidence exists for the effectiveness of behavioral therapy and limited evidence for back schools in an occupational setting. According to international guidelines, the major goal in the treatment of CLBP is return to work or to one’s usual activities; additional therapeutic options for symptomatic pain relief may fa-cilitate this process. The available evidence suggests that NSAIDs may be effective for this purpose, but not physical modalities such as transcutaneous electrical nerve stimulation (TENS), electromyography (EMG) biofeedback, acupuncture, and or-thoses. No evidence supports any form of long-term maintenance therapy.
Three essential topics: manipulative therapy, exercise therapy, and the cognitive-behavioral approach formed the basis for the present interventions.
2.4.1 Spinal manipulative therapy Spinal manipulation is generally defined as the application of a high-velocity, low-amplitude thrust to the spinal joint slightly beyond its passive range of motion. Mo-bilization, on the other hand, is the application of force within the passive range of the joint, without a thrust. However, the term “manipulative therapy” is often used very loosely to describe a wide range of procedures. It is often considered a com-plementary or alternative medical therapy mostly used by chiropractors, osteopaths, naprapaths, “bone setters,” or manual therapists. Medical doctors with manual skills are very few.
The muscle-energy technique is a manipulative-therapy procedure using a voluntary contraction of the patient’s muscles against a distinctly controlled counter-
23

force from a precise position and in a specific direction. This technique may be ap-plied either with mobilization or high-velocity, low-amplitude thrust manipulation, but in any case very little force is needed.
The basic idea of manipulative therapy is to influence spinal motion and so relieve pain and dysfunction. It may thus produce a change in neurophysiologic function and reduce muscle spasm (Indahl et al. 1997). Manipulative therapy should be considered for patients who need additional help with pain relief or who are fail-ing to return to normal activities. Risks of the procedure for low back pain are very low, provided patients are selected and assessed properly and it is carried out by a trained therapist or practitioner (Waddell et al. 1996).
An example of the manipulative-therapy package agreed to by the UK chi-ropractic, osteopathy, and physiotherapy professional associations is presented be-low (Harvey et al. 2003). Published with the permission of the publisher.
Low back pain type
Soft tissue Articulatory Thrust Exercises/activities Advice
Acute paraspinal cross-fiber, inhibition
small ampli-tude
short leverage or direct
encourage walking; neural mobilization
limit aggra-vating fac-tors; en-courage work/sport as soon as possible; reduce fear of future
Subchronic cross-fiber, stretching, friction
larger ampli-tude
normal leverage or direct
spinal exercises; encourage general exercise/activity; neural mobilization
early up-take of sport or work; ergo-nomic ad-vice; pro-mote posi-tive atti-tudes
Chronic stretching larger ampli-tude
normal leverage or direct
spinal exercises; encourage daily walking and exer-cise; neural mobili-zation
progressive uptake of sport; re-duce fear-avoidance; promote positive attitudes
24

2.4.2 Scientific evidence for manipulative therapy Of all relevant RCTs on manipulative therapy published up to July 1998, van Tulder et al. (2000b) identifies two high-quality and seven low-quality studies, with scores ranging from 27 to 57 points. A positive result of manual therapy is reported in stud-ies comparing manipulative therapy with back schools (Triano et al. 1995), massage, and sham manipulative therapy (Waagen et al. 1986), and bed rest, analgesics and massage (Arkuszewski 1986), usual care by the general practitioner (Koes et al. 1992), and analgesics (Evans et al. 1978). A negative outcome is reported in one high-quality trial comparing manipulative therapy with physical therapy (Koes et al. 1992). Reviewers conclude that strong evidence indicates that manipulative therapy provides more effective short-term pain relief than does a placebo treatment (level A). Moderate evidence (level B) exists that manipulative therapy is more effective for short-term pain relief than the usual general practitioner (GP) care, bed rest, an-algesics, and massage. Evidence of any long-term effects is limited and conflicting (level C).
Furlan et al. (2001) conducted a critical review of earlier systematic re-views involving CLBP, identifying nine reviews of spinal manipulative therapy comprising 27 primary trials with 3050 patients. Eight of nine performed a qualita-tive analysis of the trials using hierarchical order. The methodological quality of each individual trial was assessed, with conclusions based on only the best. Of four low-quality (scores 1-3/7) reviews, two reported uncertain and the other two positive results. Of five high-quality (scores 4-7) reviews, still four reported uncertain re-sults, and only one, positive (van Tulder et al. 1997). Overall, reviews of higher methodological quality tended to reach more uncertain or negative conclusions. This finding was accordant with another review of meta-analysis to evaluate analgesic interventions for pain including 80 reviews (Jadad and McQuay 1996). However, Assendelft et al. (1995) assessed 51 reviews of spinal manipulative therapy for spi-nal diseases and found that reviews of relatively high and high methodologic quality reached a positive conclusion.
Ferreira et al. (2002) analyzed quantitatively the findings of trials of spinal manipulative therapy for CLBP. Results suggested that spinal manipulative therapy does not produce a clinically significant reduction in pain when compared with sham treatment nor a significant improvement in disability when compared with NSAIDs. The authors concluded that to draw more definite conclusions on the efficacy of
25

spinal manipulative therapy for CLBP, improving the methodological quality of the trials is essential.
According to two recent meta-analyses, no evidence exists that spinal ma-nipulative therapy is superior to other effective conventional treatments (GP care, analgesics, physical therapy, exercises, or back school) for acute or CLBP (Assendelft et al. 2003; Cherkin et al. 2003). Neither radiation of pain, study quality, therapist skills, nor use of manipulation alone nor in combination with other thera-pies affected these results.
Spinal manipulative therapy has been the topic of most systematic reviews concerning conservative treatment of CLBP. Reviews of the same primary trials have mostly led to different conclusions. Presently, evidence is conflicting as to the efficacy of manipulative therapy for CLBP. Most primary trials are of low-quality, the time of follow-up is short, and the outcome measures are insufficient. Because spinal manipulative therapy is a widely used therapy approach all over the world, it deserves more high-quality trials. A Cochrane review on manipulative therapy for mechanical neck disorders showed short-term and long-term benefits maintained in the case of multimodal care (Gross et al. 2004). The common elements in care strat-egy were the combination of mobilization or manipulation or both with exercise. Evidence did not favor manipulative therapy alone or in combination with various other physical medicine agents. The added effect of exercise therapy has hardly ever been studied for LBP and certainly needs to be further explored.
2.4.3 Scientific evidence for exercise therapy The latest high-quality systematic review of exercise therapy for CLBP, by van Tulder et al. (2000a), included 23 RCTs, and considered nine of them high-quality trials. Nine RCTs involving 1105 patients compared exercise therapy with another active conservative treatment, and six RCTs with some type of inactive treatment. The authors found strong evidence that exercise therapy is more effective than the usual GP care, and that exercise therapy and conventional physiotherapy (consisting of hot packs, massage, traction, mobilization, short-wave diathermy, ultrasound, stretching, flexibility and coordinating exercises, and electrotherapy) are equally effective. It remained unclear whether exercise therapy was more effective than inactive treatment (hot packs and rest, semihot packs and sham traction, waiting-list controls, TENS or sham TENS, or detuned ultrasound or detuned short-wave dia-
26

thermy) and whether any specific type of exercise (flexion, extension, or strengthen-ing exercises) is more effective than another.
A review of systematic reviews of exercise therapy by Furlan et al. (2001) identified six reviews excluding the one by van Tulder et al. (2000a). These reviews included 21 trials and 1980 patients. The two low-quality reviews reported positive results. Of four high-quality reviews, two reported positive and the other two uncer-tain results. The authors concluded that in CLBP, evidence is conflicting as to the effectiveness of exercise therapy.
Despite the lack of scientific evidence for any specific exercises, the trend during the last five years has been from intensive strengthening exercises toward coordinative and what are called stabilizing exercises. Thus far, very few RCTs con-cern isometric, coordinative or stabilizing exercises for CLBP. O'Sullivan et al. (1997) compared specific training of deep abdominal muscles and co-activation of the lumbar multifidus with the usual GP care for CLBP patients with radiologically confirmed spondylolysis or spondylolisthesis. Specific training of transversus ab-dominis and internal oblique muscles (n = 22) was applied by a gradual increase to 10 contractions with 10-second holds, 10 to 15 minutes daily at home, and alone weekly visit to an experienced physiotherapist for 10 weeks. The usual GP care (n = 22) included 10-week treatment such as regular weekly general exercise (swimming, walking, gym work), supervised exercise programs, trunk curl exercises, heat, mas-sage, or ultrasound. The specific training group improved significantly more than did the usual GP-care group regarding pain intensity and functional status in an up to 30-month follow-up. The study was scored as a high-quality RCT (van Tulder et al. 2000a) and may be the best evidence so far as to the role of specific exercises in the treatment of CLBP.
At the moment, specific exercises are not widely recommended for pa-tients with either acute or chronic LBP. According to present recommendations, CLBP patients should be referred for exercise therapy to improve daily functioning and to facilitate their return to work. Exercise intensity should be increased gradu-ally at fixed times for a fixed period, independent of the presence of pain (van Tulder et al. 2000b). Still, positive results from one high-quality trial call for more RCTs on the effectiveness of stabilizing exercises as part of a manipulative-therapy program for CLBP.
27

2.4.4 Scientific evidence for the cognitive-behavioral approach Because psychological factors are related to pain and the development of persistent pain problems, many treatment approaches have embraced psychological therapies. The cognitive-behavioral approach (CBA) for pain has been developed as an inte-gral part of the multidimensional treatment program. It was conceptualized as a way of enhancing treatment by addressing pertinent cognitive (negative emotions and thoughts) and behavioral (altered activity and medication-taking) aspects. In addi-tion, CBA offers an educational concept whereby positive coping strategies are taught in order to enhance recovery. Pain management programs also use other techniques such as goal-setting and problem-solving. They focus on the conse-quences of pain in diverse areas of life, such as stress, family, or workplace issues. All staff members are encouraged to use these techniques, irrespective of their own profession. (Linton 2000b).
Cutler et al. (1994) employed meta-analysis to determine the effect of non-surgical pain-center treatment for chronic pain. Treatment was found approximately to double the chance of return to work compared with chronic-pain controls. Turner (1996) concluded that, according to his meta-analysis, CBA can be useful in primary care settings. Van Tulder et al. (1997) concluded in their systematic review that evi-dence is limited that behavior therapy is an effective treatment modality for CLBP, with good short-term results. CBA was also effective when the back problem was clearly linked to somatic problems. The results of several systematic reviews dem-onstrate a consistent effect in which CBA is superior to waiting-list control groups or other forms of active treatments (Compas et al. 1998; Linton 2000b; Morley et al. 1999). Several critical points in these primary studies render the final conclusions difficult. As the studies employed different assessment methods, comparison across studies as well as determination of the exact impact from a broader perspective was difficult. Finally, most studies included a small number of participants and were conducted in unique settings that may have reduced their generalizability to other patients and settings.
CBA appears a useful tool that should be employed in every patient set-ting. Three types of CBA form the basis for specialist consultation in this study.
28
2.4.4.1 Back school Back schools make the assumption that individuals are at higher risk and have more pain than they need to endure because they lack knowledge on a variety of topics as diverse as body mechanics and stress (Linton and van Tulder 2001). Programs aim, therefore, to reduce the risk for problems by enhancing the participant’s knowledge, which in turn will alter behavior in such activities as lifting. Back schools usually include a series of discussions on anatomy, biomechanics, lifting, and postural changes related to work, plus a program of exercises. They vary from a single ses-sion of less than an hour to several sessions. So far, the only high-quality RCT on back schools for CLBP (Hurri 1989) reported positive outcomes in an occupational setting for an intensive modified Swedish back school program compared with no actual treatment. According to one of the latest systematic reviews, evidence is lim-ited for an intensive back school program in an occupational setting in Scandinavia, and is conflicting in nonoccupational settings and outside Scandinavia (van Tulder et al. 2000b).
In their review of the systematic reviews, Furlan et al (2001) included 7 reviews of 17 trials, including over 2575 patients, on back schools for CLBP. Three low-quality and four high-quality reviews produced conflicting evidence for the effectiveness of back schools for CLBP. As to preventive interventions for back pain, evidence is strong and consistent that back schools are not effective in prevent-ing either neck or back pain (Linton and van Tulder 2001). 2.4.4.2 Educational booklet It is suggested that one of the main reasons patients consult physicians is to seek information and reassurance (Burton et al. 1999). In the United States, the most fre-quent reason for patient dissatisfaction with medical care was failure to receive an adequate explanation of their back pain (Cherkin et al. 1996; Deyo and Diehl 1986). These dissatisfied patients wanted more diagnostic tests, did not cooperate as well with treatment, and had poorer clinical outcomes. Hence, information and advice that health professionals give to patients may be a potent element of health care in-tervention. The Back Book was developed to provide evidence-based information and advice consistent with current clinical guidelines (Burton et al. 1999). In an RCT of patients seeking treatment in primary care for acute or recurrent LBP, it has been shown to improve back beliefs significantly, both fear-avoidance beliefs con-
29

cerning physical activity and beliefs as to the consequences of back trouble (Burton et al. 1999). Furthermore, patients with a higher initial fear-avoidance belief score were, in response to the Back Book, more likely to show clinically important im-provements both in their beliefs and of their disability. A vast population-based me-dia campaign in Australia providing positive messages about back pain using the Back Book changed the attitudes of both the general population and GPs (Buchbinder et al. 2001). The management of back pain described by GPs also changed in line with the main messages of the campaign.
Cherkin et al. (1998) showed that only providing an educational booklet led to only slightly poorer outcomes at less cost than for the McKenzie method of physical therapy or chiropractic manipulative therapy for patients with LBP. The educational booklet served as a control treatment, in which case its efficacy cannot be assessed. In the trial of Hazard et al. (2000), a pamphlet stressing psychosocial recovery issues did not prevent or reduce post-injury pain, health care use, or work absence. In another study by Cherkin et al. (1996), a 15-minute session with a clinic nurse, including the educational booklet and a follow-up telephone call, resulted in greater patient satisfaction than with the usual care and resulted in higher perceived knowledge. Nurse or booklet intervention alone, however, had no effect on percep-tions of symptoms, worry, or sense of control. Receiving full information changed how patients thought about their problem (cognitive changes) but failed to affect their feelings about the problem (affective changes).
2.4.4.3 Physician consultation A Cochrane Review on the effects of advice to stay active showed small beneficial effects for patients with acute simple LBP but little or no effect for patients with sciatica (Hilde et al. 2004). As there are potential harmful effects of prolonged bed rest, it is reasonable to advise patients with acute LBP and sciatica to stay active.
When information was combined with physician examination, a light mo-bilization program, and recommendations to stay active, two Norwegian studies could show significant effects in reducing sick leaves for patients with subacute LBP (Hagen et al. 2000; Indahl et al. 1995). Mini-intervention with fear-reducing infor-mation, careful examination, and a physiotherapist’s advice on ergonomic use of the back reduced the days of sick leave and the LBP-related costs of patients with subacute LBP (Karjalainen et al. 2003).
30

All of these studies suggest that carefully selected and presented informa-tion and advice about back pain can have a positive effect both on a patient’s beliefs and on clinical outcomes. It should be the most important tool among GPs in pri-mary care. The basic mechanisms remain obscure, however. Increasing knowledge about back pain is not enough; knowledge and improving patient empowerment are probably the essential factors which should be further evaluated.
2.5 Cost-effectiveness of the conservative treatment for LBP Because the incidence and costs of back pain are great, and the socioeconomic im-plications of disability are growing rapidly, it is important to examine how much of the burden and costs can be avoided by effective therapies. Economic evaluation studies, of which cost-effectiveness analyses are a specific example, compare both the costs and the outcomes of alternative health care interventions. This information can be used to support decision-making as to the allocation of scarce resources and to obtain the maximum gain in health. Although studies in the LBP field incorporate some cost issues in their analyses, sound economic evaluation in this area has re-ceived little attention (Goossens and Evers 2000).
2.5.1 Cost-effectiveness of manipulative therapy Most of the cost-effectiveness studies on spinal manipulative therapy and physical therapy have compared chiropractic treatment with some other type of therapy. Meade et al. (1990) compared chiropractic therapy with conventional hospital outpa-tient management, finding an obvious clinical improvement in pain intensity and disability attributable to chiropractic treatment, which may have resulted in a reduc-tion in days of absenteeism. Nyiendo and Lamm (1991) made a comparison between claimants with disabling work-related LBP injuries in Oregon, USA: those receiving chiropractic therapy and those receiving medical treatments. The difference in terms of lost working days or compensation amounts was not significant. Skargren et al. (1998) compared chiropractic treatment and physical therapy for patients with either acute or chronic back and neck pain, concluding that chiropractic treatment and physical therapy were equally cost-effective after therapy and after six months. Hemmilä (2002) compared the costs and quality of life of physiotherapy, bone set-
31
ting (traditional soft tissue, spinal, and joint manipulations, void of the chiropractic-type adjustments), and light exercise therapy for subacute or chronic back pain and found physiotherapy the cheapest and bone setting the most expensive alternative. Physiotherapy and bone setting improved quality of life equally. Of these studies, only Skargren et al. and Hemmilä included analyses of both direct and indirect costs at one year. In a study comparing physical therapy, chiropractic manipulative ther-apy, and provision of an educational booklet for LBP patients, Cherkin et al. (1998) assessed the effects and direct costs at the two-year follow-up. They showed that the McKenzie method of physical therapy and chiropractic manipulative therapy had similar effects and costs, but only marginally better effects than shown in those re-ceiving only an educational booklet. Burton et al. (2000) compared osteopathic ma-nipulative therapy with chemonucleolysis for symptomatic lumbar disc herniation and assessed effects and direct costs at one year. Mean values for pain and disability improved equally at one year, but manipulative therapy produced greater improve-ment in back pain and disability in the first few weeks. Cost analysis suggested an overall financial advantage from manipulative therapy. Hemmilä (2002) alone in-cluded an instrument to assess generic functional status, the use of which would make the results more generalizeable and comparable to those of other studies (Deyo et al. 1994).
In conclusion, rather limited evidence indicates that chiropractic treatment may be either cost-effective compared with conventional treatment or be as effective as physical therapy. On the other hand, preliminary evidence from the meta-analysis by Cherkin et al. (2003) suggests that spinal manipulative therapy may not reduce the costs of care after an initial course of therapy. An obvious gap exists in knowl-edge concerning the cost-effectiveness of manipulative-therapy methods.
2.5.2 Cost-effectiveness of exercise therapy Three cost-effectiveness studies compared active exercise therapy with several types of passive treatment. Malmivaara et al. (1995) compared three types of treatment for acute LBP: bed rest, exercises, and ordinary activity. They found that continuing ordinary activities led to less need for home help and less absenteeism than did the other two alternatives. Timm (1994), reporting on the cost-effectiveness of passive treatment (physical agents, joint manipulation) and active treatment (low-tech and high-tech) for CLBP, showed only active exercise to produce significant improve-
32

ment in objective functional measurements; low-tech exercise provided the longest internal of pain relief and was the most cost-effective. Mitchell and Carmen (1990) compared an intensive active exercise program for acute back injury with a passive program. The active group was superior in terms of earlier return to work.
To conclude, for patients with acute and CLBP, active exercise has re-duced absenteeism and increased mobility more than have several passive treat-ments. There exists, therefore, moderate evidence that active treatment may result in cost-effectiveness, and the cost-effectiveness of the differing therapies has mostly been expressed in reduced absenteeism (Goossens and Evers 2000). Interventions for patients with CLBP have rarely been subjected to economic evaluation. There is a definite need to improve the application and clarity of economic evaluation in the area of LBP. No decisions as to the most cost-effective therapies for LBP are, there-fore, possible at this moment.
33

3 AIMS OF THE STUDY The object of the present study was to assess
1. one-year effectiveness and cost-effectiveness for CLBP of combined ma-nipulative therapy, stabilizing exercises, and specialist consultation, includ-ing information and education, when compared with effectiveness of spe-cialist consultation, information, and education alone (Study I).
2. predictive factors for receiving no benefit from either combined manipulat-
ive therapy, stabilizing exercises, and specialist consultation or from special-ist consultation alone (Study II).
3. two-year effectiveness and cost-effectiveness of these two treatment arms
with special reference to the assessment of health-related quality of life (Study III).
4. psychosocial differences in determining treatment outcome for CLBP fol-
lowing combined manipulative therapy, stabilizing exercises, and specialist consultation or for specialist consultation alone (Study IV).
5. And in addition, to assess changes in overall physical activity between the
two treatment arms during the one-year follow-up and the changes in func-tional measurements between these two treatment arms at the five-month follow-up.
34

4 STUDY OUTLINE (I, II, III, IV)
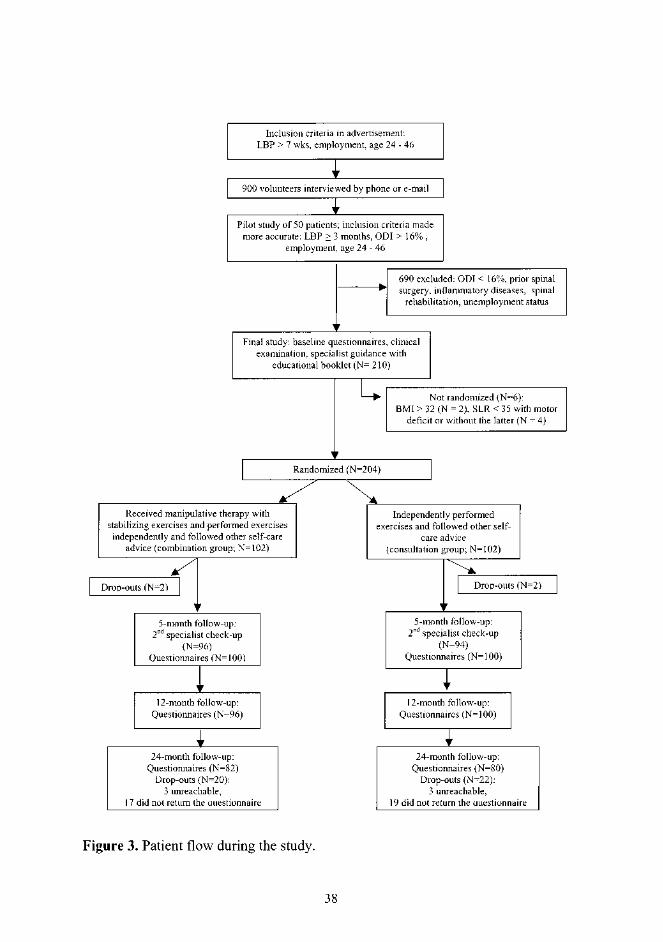
4.1 Study design and population The present study was conducted in the Rehabilitation Centre of ORTON, the Inva-lid Foundation, Helsinki, Finland. It was a prospective randomized controlled trial with two years’ follow-up. The study was initiated in March 1999 and completed in September 2001. CLBP patients were recruited voluntarily by a widely circulated newspaper (the Helsingin Sanomat) advertisement in February 1999 (Figure 2). The patients had one week to register for the study by phone, fax, mail, or e-mail. The research nurse then contacted the patients by telephone or e-mail to ensure that each candidate met the inclusion criteria. A pilot study of 50 patients was carried out to confirm the appropriate inclusion criteria. In the final study, all patients filled in a questionnaire inquiring about sociodemographics, duration and the mode of LBP, other diseases, use of medication and other earlier therapies for LBP.
Inclusion criteria: being 24- to 46-year-old employed (including students and temporary housewives) patients with LBP (with or without sciatica) of at least 3 months’ duration. The self-rated disability index (Oswestry Low Back Pain Disabil-ity Questionnaire, ODI) (Fairbank 1995) score had to reach at least 16%. Exclusion criteria: Patients with malignancies, ankylosing spondylitis, severe osteo-porosis, severe osteoarthritis, paralysis, progressive neurologic disease, hemophilia, spinal infection, previous spinal surgery, vertebral fracture during the previous 6 months, severe psychiatric disease, or severe sciatica with a straight-leg raising test (SLR) less than 35º or with at least one recent motor deficit. Other exclusion criteria included pregnancy, severe overweight (body mass index, BMI > 32), or simultane-ous spinal rehabilitation or other spinal study.
We invited eligible patients to attend the baseline trial for further evalua-tion. The clinical examination was performed prior to randomization to confirm the admission criteria. Patients were provided written and oral information on the study as required by the Declaration of Helsinki (World Medical Association 2000) before being asked to sign a document signifying informed consent.
35

Figure 2. Advertisement for patient recruitment, Helsingin Sanomat, Feb 1999.
4.2 Assignment After patients had agreed to participate in the study, and all anamnestic inclusion criteria were confirmed, they were asked to complete baseline questionnaires and then underwent specialist consultation which included a medical examination to check the clinical inclusion criteria, plus information and guidance. Once this was done, the research nurse randomized the patients to either a combination (manipulat-ive therapy with stabilizing exercises plus specialist consultation) or a specialist consultation group. The fixed allocation randomization procedure was performed to guarantee an equal number of patients in both groups. The assignments were pre-
36

sented in sealed, sequentially numbered envelopes. No stratification was based on prognostic factors. The research nurse was not responsible for determining patient eligibility.
4.3 Masking and ethical concerns Patients could not be blinded in this study (World Medical Association 2000), but a blinded clinical assessment by a specialist was performed prior to randomization and again at the 5-month follow-up. In addition, all the main outcomes were reported on by the patients themselves. The Hospital Medical Ethics Review Board approved the study. During follow-up, the patients were free to use other health care services for their LBP, the use of which they were asked to record.
4.4 Participant flow and follow-up A patient sample of 210 was selected on the basis of history from among 900 volun-teers. The clear majority of the 900 volunteers were disqualified by virtue of a low (< 16%) Oswestry score. The ODI limit of 16% was based on the pilot study of 50 patients, and was considered essential to find the patients who would benefit from the trial. Other reasons for exclusion were prior spinal surgery, inflammatory dis-eases (e.g. ulcerative colitis, Mb Bechterew, rheumatoid arthritis), simultaneous spinal rehabilitation, and unemployment status. After the specialist’s examination, 6 patients were excluded for obesity or SLR less than 35°. 204 patients were included in the trial: 102 assigned to the combination and 102 to the consultation group. All patients visited the specialist at least once prior to randomization and received a back booklet, information on the etiology of their back pain, and instructions on how to cope with low back trouble. The mean number of manipulative-therapy sessions was 4. The trial profile is summarized in Figure 3.
37

4.5 Baseline characteristics (I, II, III, IV) At baseline, the combination group and the consultation group were comparable in age and gender, in duration and localization of LBP, pain intensity, self-rated dis-ability, and HRQOL (Tables 1 and 2). Psychometric variables were also similar. They included depression, affective distress, life control, social support, and general activity. Level of education and vocational training in both groups were comparable to that of the Finnish working-age population. The study population differed from the metropolitan working-age population of Helsinki in that the proportion of white-collar workers was larger (45% vs. 28%) and blue-collar workers smaller (7% vs. 25%) (2000b). The percentage of employees were higher in the combination group (99%) than in the consultation group (91%) (P = 0.01). Previous use of health care services (medical services, physiotherapy, chiropractic, massage) in both groups was similar. Tobacco use was equally common in both groups (32% vs. 36%). No differ-ences existed between groups for any of the clinical tests. Biomechanical dysfunc-tion in the lumbopelvic segments appeared in 75% in the combination and 73% in the consultation groups.
Table 1. Baseline characteristics of subjects* (n = 204). From Study I (Niemistö et al.2003).Characteristic Combination group (n = 102)
Consultation group (n = 102)
Difference P value
Age (SD) 37.3 (5.6) 36.7 (5.6) 0.24
Sex - no. (%) 0.78 Male 46 (45) 48 (47) Female 56 (55) 54 (53)
Duration of pain, years (range) 6 (1-31) 6 (1-29) 0.29 Frequency of daily pain (%) 58 62 0.14 Localization of low back pain (%)
0.79
local low back pain 24 20 radiating above knee 40 43
radiating below knee 36 37 Proportion of patients using analgesics for back pain (%)
30 35 0.58
Sick leaves during previous year - days (SD)
14 (28) 20 (35) 0.07
Employed 99 91 0.01
* No statistically significant differences between groups, except for percentage of employees (P = 0.01). For all scales and questionnaires, score increases with severity of pain or symptom. All values are means, except pain duratio, shown as median values.
39
5 METHODS
5.1 Interventions (I, II, III, IV)
5.1.1 Manipulative therapy, stabilizing exercises, and specialist consultation (Combination group) Patients in the combination group attended 60-minute evaluation, treatment, and exercise sessions four times in the course of 4 weeks. An experienced manual thera-pist conducted the individual treatment sessions, including manipulative therapy with a muscle-energy technique, and stabilizing exercises aiming to correct the mo-tor control of the trunk. Manipulative therapy with a muscle-energy technique was used to correct any biomechanical dysfunction in the lumbar or pelvic segments (Chun 1991). The muscle-energy technique is a manipulative therapy procedure using voluntary contraction of the patient's muscles against a distinctly controlled counterforce from a precise position and in a specific direction. In cases of neurody-namic symptoms and findings (SLR in a supine, SLUMP in a sitting, or PKB in a prone position), neurodynamic mobilization techniques were used (Butler 1991). The stabilizing exercises were taught by asking the patients to draw in the stomach while receiving verbal, visual, and tactile feedback and during measurement of pres-sure change with a biofeedback meter. In a prone position with a pressure cushion under the lower abdomen, a pressure decrease of 4 mmHg was considered to be the lower limit for actual independent activation of the transversus abdominis muscle. The patients were instructed to perform the stabilizing exercises gradually in a more functional manner (Richardson et al. 1999b). Finally, the patients were taught to do these isometric exercises during their daily activities as often as possible. All exer-cise was by definition to be pain-free.
Of all patients in the combination group, 74% had a motor control disor-der, according to clinical assessment. 40% of the patients were considered to have discogenic pain, 44% pelvic dysfunction, 36% lumbar or thoracolumbar hypomobil-ity, and 13% other pathologies, like scoliosis, spondylolisthesis, mental exhaustion, or myofascial pain. Manipulative-therapy techniques were used for 71% of the pa-tients, on average 1.4 times per manipulated patient. Neurodynamic mobilization techniques were used for 58% of the patients. The stabilizing exercises were taught to all patients in the combination group. The chosen techniques were based on the above-mentioned findings.
40

5.1.2 Specialist consultation (Consultation group) Both the combination group and the consultation group members received a 25-page educational booklet on basic anatomy and physiology of the spine, principles of ergonomics for LBP patients, and instructions on how to exercise and to cope with the acute phase of LBP (Gerlander et al. 1995). The specialist was blinded to alloca-tion. The clinical findings were explained with the aid of a human skeleton, and the x-ray findings and possible causes of pain were clarified. The patients were told that LBP generally has a benign, self-limiting natural course, and that they could hasten the process by simple regular exercises and by avoiding inactivity. The patients re-ceived individual instructions regarding posture and three to four exercises aimed to increase spinal mobility and muscle stretch or trunk muscle stability or both, based on the clinical evaluation. Depending on the baseline activity level, exercises were usually recommended to be performed daily, gradually increasing the intensity of training. They were also advised to avoid longstanding static work by performing several countermovements. When lifting heavy objects, they were told to avoid bending over or twisting and instead to use their legs. The main principle was to encourage the patients to treat themselves instead of undergoing passive treatment. For further patient motivation and activation, each received an exercise diary and was asked to return it at the next visit to the specialist. At the 5-month follow-up, clinical tests were repeated and explained and the earlier information was reinforced. Both appointments in the two treatment arms lasted an average of one hour.
5.2 Outcome measures (I, II, III, IV) The main outcomes were pain intensity (VAS from 0 to 100), back-specific disabil-ity (Oswestry Disability Index: ODI from 0 to 100) (Fairbank 1995; Fairbank and Pynsent 2000), health-related quality of life (HRQOL) (15D) (Sintonen 1994), days on sick leave, costs of health care, productivity costs, frequency of LBP, degree of mental depression (Finnish Depression Questionnaire: DEPS) (I) (Salokangas et al. 1994), and satisfaction with care (III). Subscales of 15D of the two study groups were compared to those of average 24- to 54-year-old healthy Finns (IV) (Arinen et al. 1998). Affective distress, life control, and social support were measured by a Finnish version of the Multidimensional Pain Inventory (MPI) (SIMPI) (II, IV) (Jamison et al. 1994). Of MPI profile types, adaptive copers (AC) have reported
41

lower levels of pain severity, of interference with activities, and of affective distress, and greater perceptions of life control and activity level. Those interpersonally dis-tressed (ID) are characterized by lower levels of social support and lower scores on solicitous and distracting responses from significant others. Dysfunctionals (DYS) were distinguished by higher level of pain severity, marked interference with every-day life due to pain, high affective distress, low perceptions of life control, and low level of activity.
Additionally, physical activity at work, in commuting, during leisure time, and for miscellaneous time such as gardening or domestic chores was assessed by the MetPro® questionnaire. All activities were converted into metabolic equivalents (METs) by specific software (MetPro® 2.01,1 SciReha, Jyväskylä, Finland). A met is a relative unit representing the approximate rate of energy consumption of a seated individual at rest (3.5 ml kg-1 min-1) (Howley 2001). Physical activity at work was assessed on a 7-point scale, accompanied by illustrations and descriptions of various types of work. The scale varied from 1.5 (light work) to 10 Mets (extremely high level of work). Activity in commuting was categorized as by motor vehicle, bicycle or walking. The questionnaire had an additional question on intensity of exercise, with intensity assessed by the patient as metabolic equivalents on the basis of reported breathing rate and sweating. Assessment of intensity was based on about 900 activities included in the MetPro database (Mälkiä 1996; Mälkiä et al. 1988; 1994), in which MET values are comparable with categories in all high-quality stud-ies published in this field (American College of Sports Medicine 1975; 1980; 1995; 2000; Ainsworth et al. 2000; Durnin and Passmore 1967; Spitzer and Hettinger 1969). The physical activity questionnaire was developed from earlier inquiries (Mälkiä 1996; Mälkiä et al. 1988; 1994). The reliability of the questionnaire was tested by repeated testing during one week by 15 female librarians. Test-retest Intra-class Correlation Coefficients were between 0.62 and 0.94. An earlier one-year re-call questionnaire after 3.5 month re-examination has also proven acceptable (Mälkiä 1996).
The results of calculations based on the quality, frequency, duration, and intensity of activity were expressed as mean and maximal intensity of activity group (work, leisure, commuting, all activities) and the sum as MET minutes (force).
The questionnaires were presented at the initial examination prior to ran-domization and at follow-up examinations 5, 12, and 24 (III, IV) months after ran-domization.
42

Both direct and indirect costs were assessed from a societal and from a patient per-spective. Use of health services, direct drug and traveling costs to the patients, and productivity costs due to absence from work were measured by a questionnaire for the study population prior to randomization and at the 12- and 24-month follow-up. Service fees from the patients were not included in cost analysis. In monetary valua-tion of health services, we applied Finnish standard cost information at the year-2000 price-level (Heikkinen et al. 2001). Standard costs are average costs for vari-ous specified procedures or diagnostic tests by representative Finnish health-care providers. Productivity costs were valued at the average year-2000 wage level in Finland. Because of the theoretical and methodological controversy surrounding such valuation, we tested the effect of the valuing algorithm on total costs by using a 50% lower estimate of the average wage level. Costs were converted into US $ ($1 = 1.01 euro 9/2002). No costs or effects were discounted. Whereas no differences ex-isted in the temporal generation of costs, the discount rate was not significant be-tween the groups. Functional assessments included the following tests: 1. Mobility of the spine in forward flexion (Moll and Wright 1971) and in lateral
flexion (Moll et al. 1972) was measured with a metal tape. Sacroiliac joint mo-tion was assessed by the forward flexion (the Piedallu sign (DonTigny 1985) occuring when the posterior superior iliac spine (PSIS) reverses its height as the patient bends forward, reflecting asymmetric motion of the sacroiliac joints), backward and lateral flexion, and by the contralateral test (with patient standing and lifting the opposite knee, sacroiliac motion is assessed with one thumb on the sacrum and the other on the PSIS; in sacroiliac joint dysfunction, asymmet-ric motion is indicated by less motion on the affected side).
2. Neurodynamic symptoms (neural tissue irritation) and findings were assessed
with the straight-leg raising test in a supine and by SLUMP (Butler 1991) test in a sitting position. Tension of the rectus femoris was measured with a goniometer (Hamberg et al. 1993). Tendon reflexes and sensory and motor function of the lower limbs were evaluated.
43
3. The centralization phenomenon was assessed by repetitive end-range lumbar flexion and extension movements in the standing and prone position (Werneke et al. 1999).
4. Pain provocation tests were performed by palpation of the spinous processes of
the lumbar vertebrae. Intradiscal pain was assessed by a bony vibration stimula-tion test (Yrjämä et al. 1997). Sacroiliac provocation tests included palpation of the inferior and medial point of PSIS (Fortin sign) (Fortin and Falco 1997), sac-ral thrust (Laslett and Williams 1994), and a bony vibration stimulation test of the sacroiliac joint.
5. Postural control and co-ordination were assessed by measurement of the time
the patient could stand on one leg with eyes open and closed (Suni et al. 1998). 6. Co-activation of the transversus abdominis and lumbar multifidus was assessed
by palpation and by measurement of pressure changes by the Stabilizer® (Richardson et al. 1999a).
5.3 Statistical analysis Statistical analyses were carried out with appropriate programs for SYSTAT 10 for
attain a power of at least 0.80 for pain release on VAS at a significance level of 0.05 (nQuery 1997).
In Studies I and III, patients were included in the analysis as part of the group allocation by randomization. For missing values in questionnaires was substi-tuted the previous after-treatment value (last value carried forward technique). In cost analysis, missing values were interpreted as being zero, if there simultaneously were markings elsewhere. Continuous outcomes were analyzed according to the intention-to-treat principle, with repeated-measures ANOVA (group x time of as-sessment). In case of skewed distribution of the data, logarithmic or square root transformation was used. Comparison of proportions between groups was performed by the Pearson Chi-square test. The Mann-Whitney test served to compare work absenteeism at baseline between groups. Heterogeneity of the changes within groups
44
Windows software (2000). Power calculations were carried out prior to the study to

was tested by the McNemar Chi-square test. Cost-effectiveness estimates were con-structed for two main outcomes: pain and functional status. Statistical tests for cost-effectiveness ratios were accomplished by the bootstrapping technique, forming 5000 simulated replica data. Bootstrapping was used to assess uncertainty around point estimates of incremental costs, effectiveness, and cost-effectiveness derived from the study sample. Data were analyzed with SYSTAT 10 for Windows soft-ware. Bootstrapping and tests of the ICERs were performed with R 1.9.0 software (The R Foundation for Statistical Computing Version 2.0.1.www.r-project.org.). Significance was accepted at the 5% level. The two-tailed test was applied for all P values.
In Study II, K-means cluster analysis was conducted based on change both in pain intensity (VAS 0-100) and in self-rated disability (Oswestry Questionnaire) at one year. K-means cluster analysis is a multivariate method also referred to as unsupervised pattern recognition. Profiles for subjects to be studied are compared, and subjects closely similar are classified as being in the same cluster or group (Afifi and Clark 1998). This maximum likelihood technique iteratively seeks the optimal grouping, so that inter-group deviation is maximized compared to intra-group devia-tion. The first cluster included patients whose pain and disability clearly decreased, and the second those whose trouble persisted. Association between poor recovery from LBP and disability and the following factors: sociodemographic, pain charac-teristic, disability, work-related, and psychometric, and also physical examination tests were first evaluated by univariate analysis. Significance was considered to be at the 5% level. However, the meaningful level of association in univariate analysis (assessed as odds ratios) was determined as P < 0.10. Each factor with P < 0.10 was included in the multivariate analysis in a stepwise logistic regression procedure. It is a conventional technique to use P < 0.10 as an initial cutoff point for multivariate analysis to include all factors that may have correlations with other factors. Corre-spondingly, the cut-off level for excluding variables once they have been entered into the regression model was considered as 10% as well.
Discriminant analysis using a jackknife technique tested the accuracy of the resultant model. Jackknifing is a method of validating or assessing the fit or ap-propriateness of a model, using the same sample which was used to derive the model, as opposed to using an independent sample (Afifi and Clark 1998). The prin-ciple behind this method is to omit each sample member in turn from the data, thereby generating n separate samples, each of size n - 1.
45

Study IV also used K-means cluster analysis for clustering patients (Rudy et al. 1989a). The level of ODI and VAS during follow-up was analyzed by a two-way ANOVA for repeated measurements. Analysis of covariance (ANCOVA) served for the interaction effects of treatment, MPI grouping, and time of measure-ment upon the main outcome variables. The Huynh-Feldt correction was used for any possible violations of sphericity in repeated measures in the ANCOVA analysis. Dropouts at follow-up were imputed with the last value carried forward, the most recent previously available follow-up value substituting for each missing value in the follow-up.
Based on pretreatment results, K-means cluster analysis was carried out for the 9 SIMPI subscales. A Euclidean distance measure was used in cluster analysis, supposing an independence between the SIMPI scales. The three-cluster solution turned out to be stable and convenient, as presented in earlier studies (Rudy et al. 1989a; Turk and Rudy 1990). Since the means for the 9 subscales between the com-bination and the consultation group did not differ, profile clusters were computed for all subjects. Subscale means were analyzed for the resulting 3 clusters, called as AC, ID, and DYS, in the combination group and consultation group, together with age, duration of pain and gender.
Differences in physical activity across the two treatment arms were ana-lyzed by repeated measures ANOVA. For assessing intra-tester reliability and re-peatability of the functional measurement, the intra-class correlation (ICC) served for continuous variables and the Cohen kappa coefficient for dichotomic variables. Continuous functional outcomes were analyzed with a one-way ANOVA. A likeli-hood ratio test was used to examine the difference in the change between time points and in a categoric variable between the study groups.
46

6 RESULTS
6.1 Outcomes
6.1.1 Subjective pain and disability (I, II, III, IV)
Significant improvement occurred in both groups on every self-rated outcome meas-urement. At the one-year follow-up, the mean change on VAS score was 49 (SD 16) and on the Oswestry Disability Index (ODI) 19 (SD 11) among the good responders (N = 112). The mean changes for poor responders (N = 84) were -1 (SD 19) on VAS and 8 (SD 11) on ODI.
Within the 2-year follow-up, a significant difference appeared between the groups in pain intensity (P = 0.01, ANOVA) but not in self-rated disability (P = 0.20, ANOVA) (Table 2). The percentage of daily LBP fell from 58% to 23% (P < 0.001, McNemar Symmetry Chi-square) in the combination and from 62% to 24% (P < 0.001) in the consultation group. The proportion of patients using analge-sics for their back pain decreased from 32% to 15% and from 36% to 15% in these same two groups.
The bootstrapping results showed a significantly higher incremental effec-tiveness on the VAS in favor of the combination group (Table 5).
47


6.1.2 Health-related quality of life (I, III) HRQOL increased equally in both groups (P < 0.001, ANOVA) (Table 2) without any differences in any of the 15D dimensions between groups. At baseline, the health-related quality of life of the two study groups was significantly worse than the average for 24- to 54-year-old Finns (Arinen et al. 1998). The subscales of the 15D questionnaire mostly affecting low back pain patients were Moving, Usual daily activities, Pain, Affective Distress, and Sex life. Despite improvement in these dimensions, scores failed to equal those of the normal healthy population, except for Affective Distress (Table 3). Table 3. Dimensions of HRQOL (15D) among subjects in the combination and con-sultation groups* Outcome measure
Time point (months)
Combination group
Consultation group
Healthy controls†
P value; Time-group interaction‡
Moving 0 0.89 (0.15) (N=96)
0.86 (0.14) (N=86)
0.98 (0.08) (N=2359)
0.68
5 0.93 (0.12) (N=99)
0.90 (0.14) (N=101)
12 0.95 (0.11) (N=95)
0.92 (0.13) (N=99)
24 0.89 (0.20) (N=80)
0.89 (0.18) (N=77)
Usual daily activities
0 0.77 (0.19) (N=97)
0.77 (0.19) (N=86)
0.96 (0.13) (N=2359)
0.67
5 0.86 (0.17) (N=99)
0.84 (0.17) (N=101)
12 0.90 (0.14) (N=94)
0.85 (0.17) (N=99)
24 0.95 (0.11) (N=81)
0.94 (0.12) (N=78)
Pain 0 0.58 (0.19) (N=96)
0.60 (0.19) (N=86)
0.85 (0.19) (N=2359)
0.11
5 0.70 (0.18) (N=99)
0.62 (0.19) (N=101)
12 0.73 (0.15) (N=94)
0.67 (0.19) (N=98)
24 0.91 (0.16) (N=81)
0.90 (0.16) (N=77)
49

Affective Distress
0 0.83 (0.18) (N=96)
0.85 (0.16) (N=86)
0.90 (0.15) (N=2359)
0.99
5 0.89 (0.16) (N=99)
0.88 (0.15) (N=101)
12 0.87 (0.18) (N=95)
0.87 (0.18) (N=99)
24 0.76 (0.17) (N=81)
0.75 (0.18) (N=77)
Sex life 0 0.82 (0.18) (N=96)
0.84 (0.17) (N=86)
0.95 (0.13) (N=2359)
0.42
5 0.90 (0.16) (N=99)
0.87 (0.17) (N=101)
12 0.88 (0.15) (N=95)
0.89 (0.17) (N=98)
24 0.87 (0.17) (N=81)
0.88 (0.19) (N=77)
* All values are means (SD). For 15D questionnaire, the score decreases with severity of pain or symp-tom. N= number of participants derived from original data before substitution. † Data on a normal population of 24- to 54-year-old Finns (Arinen et al. 1998). Mean values for 15D dimensions of healthy controls standardized for gender and age with patients in the study population. ‡ P values were tested with repeated measures ANOVA. Due to the skewed distribution of the data, the square-root transformation was used. For missing values was substituted previous available value (last value forward). None of the differences between the two study groups in 15D dimensions was signifi-cant at the 5% risk level. Differences between study groups and healthy controls were statistically significant throughout follow-up.
6.1.3 Use of health care services (I, III) Annual visits to physicians and use of physiotherapy or other manipulative therapies decreased in both groups during the 2-year follow-up; this decrease was more pro-nounced in the consultation group during the second year, but differences were not significant. Use of other health services, such as hospital services, was minor in both groups, and changes in these were also very small and nonsignificant (Table 4).
50
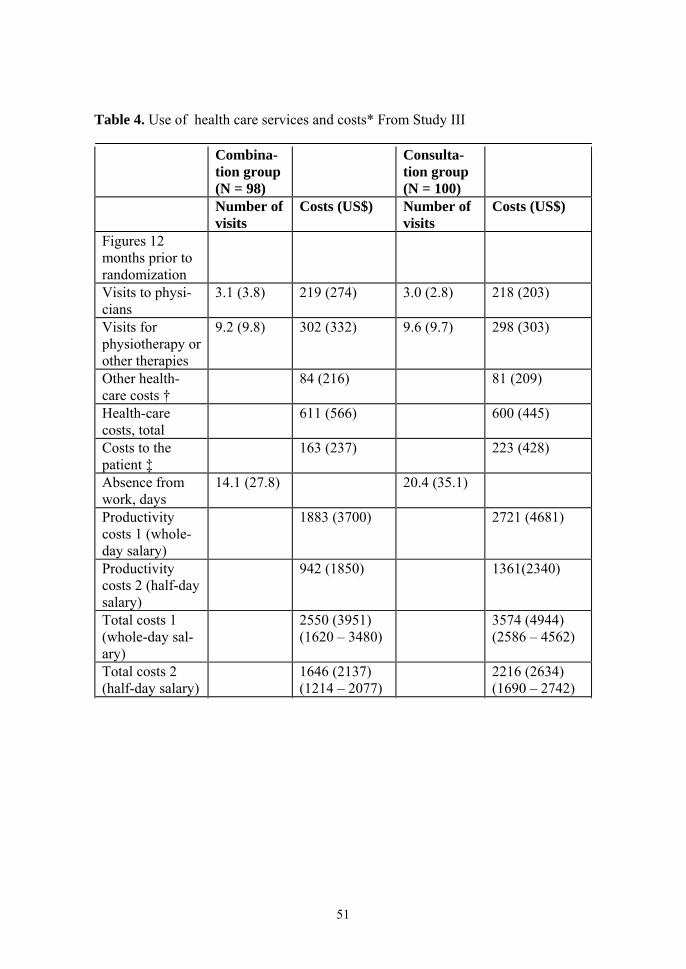
Table 4. Use of health care services and costs* From Study III
Combina-tion group (N = 98)
Consulta-tion group (N = 100)
Number of visits
Costs (US$) Number of visits
Costs (US$)
Figures 12 months prior to randomization
Visits to physi-cians
3.1 (3.8) 219 (274) 3.0 (2.8) 218 (203)
Visits for physiotherapy or other therapies
9.2 (9.8) 302 (332) 9.6 (9.7) 298 (303)
Other health-care costs †
84 (216) 81 (209)
Health-care costs, total
611 (566) 600 (445)
Costs to the patient ‡
163 (237) 223 (428)
Absence from work, days
14.1 (27.8) 20.4 (35.1)
Productivity costs 1 (whole-day salary)
1883 (3700) 2721 (4681)
Productivity costs 2 (half-day salary)
942 (1850) 1361(2340)
Total costs 1 (whole-day sal-ary)
2550 (3951) (1620 – 3480)
3574 (4944) (2586 – 4562)
Total costs 2 (half-day salary)
1646 (2137) (1214 – 2077)
2216 (2634) (1690 – 2742)
51

Annual mean figures during the 24 months after randomiza-tion
N = 81
N = 78
Visits to physi-cians
1.8 (2.6) 130 (188) 1.7 (2.1) 122 (151)
Visits for physiotherapy or other therapies
7.2 (8.1) 234 (265) 5.2 (5.3) 162 (169)
Other health-care costs †
79 (237) 77 (255)
Health-care costs, total
448 (493) 362 (449)
Costs to the patient ‡
109 (168) 99 (121)
Absence from work, days
12.3 (20.5) 14.8 (38.0)
Productivity costs 1 (whole-day salary)
1632 (2728) 1970 (5068)
Productivity costs 2 (half-day salary)
816 (1364) 985 (2534)
Total costs 1 (whole-day sal-ary)
2262 (3156) (1561 – 2963)
2280 (5294) (1081 – 3479)
Total costs 2 (half-day salary)
1427 (1807) (1025 – 1829)
1370 (2842) (1026 – 2014)
*All values are means (SD). 95% confidence intervals are reported for total costs. Costs of the 4 ma-nipulation sessions (including traveling costs to the patients) included in cost analysis. No differences between groups in cost variables were significant at the 5% risk level. † Other health care costs include visits to outpatient clinics, inpatient care in hospitals, and x-ray ex-aminations. ‡ Costs to the patient include use of drugs and traveling costs due to back pain.
52

6.1.4 Cost analysis (I, III) In the consultation group, the annual number of sick leave days decreased on aver-age 5 days during the 2-year follow-up, while in the combination group the decrease was 2 days. Variance in productivity costs was large, and consequently the differ-ence between groups was not significant. Mean annual total costs decreased $288 in the combination group and $1294 in the consultation group during the 2-year fol-low-up compared to baseline costs (Table 4). According to bootstrapping, the com-bination group showed higher incremental costs than did the consultation group (Table 5). A one-point improvement in the combination group compared to the con-sultation group on the VAS scale cost $512 (95% CI 77-949) (Table 5). The cost-effectiveness plane and acceptability curve showed that combination therapy yielded acceptable cost-effectiveness in about 75% of the bootstrapping data if the decision-makers’ willingness to pay (WTP) for a one-point improvement on VAS was at maximum $2100. Similarly, according to ODI, if WTP was $4200, 65% of boot-strapping data yielded acceptable cost-effectiveness (Figures 4a-b and 5a-b).
Table 5. Incremental cost-effectiveness plane for pain intensity (VAS) and disability (ODI).* From Study III.
Original N = 138
Incremental effec-tiveness (SD) 95% CI
Incremental costs (SD) 95% CI
Incremental C/E (SD) 95% CI
ODI
1.24 (2.13)
1.18 – 1.30
$1662 (907)
1637 - 1687
$-78 (20818)
-655 - 499
VAS
4.97 (5.24)
4.83 – 5.12
$1662 (907)
1637 - 1687
$512 (15714)
77 - 949
*Means, standard deviations (SD), and 95% confidence intervals (CI) for incremental effect tiveness, incremental costs, and incremental cost-effectiveness (ICER) analyzed for pain intensity and disability. ICER = ∆ Costs/∆ Effects. Improvement in ODI and VAS was marked as positive.
53



6.1.5 Satisfaction with care (IV) At the 2-year follow-up, patients in the combination group were more satisfied with care received during this study than were patients in the consultation group (P = 0.001, Pearson Chi-square) (Table 6). Neither group reported adverse effects. Table 6. Patient satisfaction with treatment/guidance.
Combination group (N = 79)
Consultation group (N = 75)
P value*
All (N = 154)
Yes 71 (90%) 52 (69%) 0.001
No 8 (10%) 23 (31%)
Male (N = 72)
Yes 30 (88%) 27 (71%) 0.073
No 4 (12%) 11 (29%)
Female (N=82)
Yes 41 (91%) 25 (68%) 0.007
No 4 (9%) 12 (32%)
* Pearson Chi-square
6.1.6 Physical activity Overall energy consumption did not change in either treatment arm during the one-year follow-up. For the consultation group, the calculated mean intensity (P = 0.024, repeated measures ANOVA) and maximal intensity of the physical exercise P = 0.057) tended to increase more than in the combination group (Figure 6a-b). Furthermore, the maximal intensity of the active time (P = 0.093; Figure 7) plus the calculated mean intensity (P = 0.052; Figure 8), calculated time-derived mean inten-
56




6.1.7.2 Changes in functional measurements Significant improvements were evident in every functional measurement in both groups at the 5-month follow-up (P < 0.001). The percentage of abnormal right-sided CLT dropped from 43 to 26% in the combination group and from 41 to 25% in the consultation group. Left-sided abnormal CLT values dropped from 41 to 19% in the combination group and from 40 to 31% in the consultation group. Difference in change for left-sided CLT was significant, favoring the combination group (P = 0.03, likelihood ratio test). For the same left side, the SLUMP test improved more often in the combination group than in the consultation group (P = 0.005, likelihood ratio test). Differences in the functional measurements are assumed to be due to the manipulative therapy.
6.2 Predictive factors for unfavorable recovery (II)
6.2.1 Univariate analysis Of sociodemographic factors, unmarried status and high level of education predicted poor recovery from pain and disability. The strongest single predictive factor was low to moderate level of back pain intensity (score 0-49 in VAS), which was associ-ated with a five-fold increase in odds of persistence of symptoms (Table 7).
Over 25 days of sick leave due to LBP during the year before the study was associated with an up to threefold increase in odds of a poor outcome in the whole study population and with a sevenfold increase in odds for the consultation group (Table 7).
Poor life control and weak social support at baseline were associated with a twofold increase in odds of a poor outcome in the whole study group. In the com-bination group, severe affective distress was associated with an almost threefold increase in odds of a poor outcome. In the consultation group, poor life control, weak social support, and a risk score on the MSPQ were associated with a twofold increase in odds of a poor outcome (Table7).
The noncentralization phenomenon was associated with an over twofold increase in odds of a poor outcome in the combination group. Normal neurophysi-ologic findings in the SLUMP test were associated with a 1.89 increase in odds for the whole study population (Table 7).
60

Table 7. Association between poor recovery from low back pain (LBP) and disabil-ity and: sociodemographic, pain characteristic, disability, work-related, and psy-chometric factors, and physical examination tests (univariate analysis). From Study II.
Odds ratios (95% CI) Characteristic Both groups
(N = 196) Combination group (N = 96)
Consultation group (N = 100)
Treatment group: Combination 1 Consultation 1.54 (0.9-2.7)
P-value > 0.10 Married 1 1 1 Single or divorced
2.28 (1.2-4.4) 2.19 (0.9-5.3) 2.77 (1.0-7.6)
P-value 0.01 0.08 0.04 University educa-tion:
No 1 1 1 Yes 2.65 (1.3-5.3) 2.65 (1.0-6.7) 3.00 (1.0-8.6) P-value 0.005 0.04 0.03 Visual analogue scale (0-100):
50-100 1 1 1 0-49 5.22 (2.8-9.8) 5.62 (2.3-14.0) 4.73 (2.0-11.4) P-value < 0.001 < 0.001 < 0.001 Sick-leave days during previous year:
0-24 1 1 1 >25 3.45 (1.3-9.0) 1.27 (0.3-5.2) 7.33 (1.7-32.2) P-value 0.005 > 0.10 0.001 Work ability index: Good or moderate 1 1 1 Poor 1.70 (1.0-3.0) 1.07 (0.5-2.4) 2.55 (1.1-5.8) P-value 0.07 > 0.10 0.02 Self-rated prognosis of work ability after 2 years:
Good or moderate 1 1 1
61

Poor 1.75 (0.9-3.4) 1.15 (0.4-3.3) 2.18 (0.9-5.4) P-value 0.10 > 0.10 0.09 Life control: Good or moderate 1 1 1 Poor 1.96 (0.9-4.2) 1.77 (0.6-5.2) 2.17 (0.7-6.4) P-value 0.08 > 0.10 > 0.10 Affective distress: Mild or moderate 1 1 1 Severe 1.28 (0.7-2.3) 2.65 (1.1-6.2) 0.65 (0.3-1.5) P-value > 0.10 0.02 > 0.10 Social support: Good or moderate 1 1 1 Weak 1.85 (1.0-3.3) 1.81 (0.8-4.1) 2.07 (0.9-4.6) P-value 0.03 > 0.10 0.07 MSPQ:* < 8 1 1 1 > 9 1.57 (0.8-3.1) 0.89 (0.3-2.5) 2.53 (1.0-6.7) P-value > 0.10 > 0.10 0.06 Finger-floor dis-tance in forward flexion:
> 20cm 1 1 1 < 20cm 1.75 (0.9-3.3) 1.20 (0.5-2.9) 2.52 (1.0-6.1) P-value 0.08 >0.10 0.04 Centralization phenomenon in extension: †
Yes 1 1 1 No 1.60 (0.8-3.1) 2.60 (0.9-7.2) 1.05 (0.4-2.6) P-value > 0.10 0.05 > 0.10 Slump test:‡ Abnormal 1 1 1 Normal 1.89 (1.1-3.3) 2.02 (0.9-4.6) 1.78 (0.8-3.9) P-value 0.03 0.09 > 0.10
*MSPQ = Modified Somatic Perception Questionnaire, a 13-item questionnaire to measure height-ened somatic awareness among chronic back pain patients. †Centralization phenomenon in extension = pain relief in lower extremities during back extension (Werneke et al. 1999). ‡Slump test evaluates nerve root or neural tissue irritation in a sitting position (Butler 1991).
62

6.2.2 Multivariate analysis The final model of the whole study population, which predicted poor recovery, comprised six factors: university education (OR 2.80; 95% CI 1.1-6.9), mild to moderate level of LBP intensity (score 0-49 in VAS) (OR 6.33; 2.8-14.3), absence of over 25 days from work during the previous year (OR 4.19; 1.5-11.3), poor self-evaluated prognosis for work ability after 2 years (OR 2.11; 0.9-5.0), poor life con-trol (OR 2.77; 1.0-7.4), and normal SLUMP test findings in the physical examina-tion (OR 1.96; 0.9-4.1). The potential confounding factors (age, gender) did not change the final model significantly (> 5%). With the jackknife classification ma-trix, the outcome of 74% of the patients was correctly classified.
In the combination group, the final model comprised three factors: mild to moderate level of pain intensity (OR 5.99; 2.0-18.3), severe affective distress (OR 3.81; 1.3-10.8), and noncentralization phenomenon in the physical examination (OR 2.71; 0.8-9.6). With the jackknife classification matrix, the outcome of 69% of the patients was correctly classified.
In the consultation group, the final model included five factors: university education (OR 7.93;1.6-39.7), mild to moderate level of pain intensity (OR 5.38; 1.5-19.3), over 25 days of sick leave during the previous year (OR 19.64; 3.8-102.5), a risk score of MSPQ (OR 3.18; 0.9-11.6), and poor life control (OR 9.40; 1.9-47.0). With the jackknife classification matrix, the outcome of 76% of the patients was correctly classified.
6.3 Psychosocial differences as determinants of treatment out-come (IV) At baseline, active copers (AC) reported the highest levels of life control, general activity, social support, and a low level of affective distress. The interpersonally distressed (ID) were low on social support and receiving solicitous and distracting responses. Dysfunctional patients (DYS) were high on pain severity and interference in life, and on affective distress, and low on level of life control. These three profile groups corresponded well to those reported by Rudy et al. (1989), and patients were evenly distributed among these three clusters.
63

No difference appeared in age or duration of pain between profile groups, either within or between the combination and consultation groups. In all profile groups, about half the patients were women. Within the combination group, a significant interaction emerged between patient profile group and Oswestry Disability Index (ODI). The DYS patients at baseline showed the significantly highest ODI level (P < 0.001), which decreased to the level shown by the AC or ID patients during follow-up. Within the consultation group, DYS patients showed the highest level on ODI both at baseline (P < 0.001) and during the 12-month follow-up. Reduction in ODI among the DYS patients was larger in the combination group than in the consultation group (Table 8). On the VAS index, the combination group showed no difference between the profile groups at baseline or during follow-up. Compared to the consultation group, the DYS patients showed a lower level on VAS during follow-up, and within the con-sultation group, the highest VAS level among the DYS patients (P < 0.01) persisted (Table 9).
At baseline, affective distress was also highest among the DYS patients. Despite the marked decrease among DYS patients at the 12-month follow-up (P < 0.001 for both groups), they showed the highest level during follow-up in both the combination (P < 0.01) and the consultation group (P < 0.05).
Among the DYS patients, the level of life control had clearly improved in both groups at the 12-month follow-up (P < 0.01 for the combination group and P < 0.001 for the consultation group). At the 24-month follow-up, no differences con-cerning life control were apparent any longer between the profile groups either in the combination or the consultation group.
Baseline differences in social support prevailed throughout the follow-up in both groups (P < 0.001). At the 2-year follow-up, DYS patients in the combina-tion group showed, however, a significant decrease in support, below their baseline ratings (P < 0.05). In addition, DYS patients in the combination group were also at a lower level of social support than were DYS patients in the consultation group (P < 0.01).
64

Table 8. Oswestry Disability Index (ODI) for three patient profiles (AC, ID, DYS) in combination and consultation groups.*
ODI†
AC‡
Combination group ID§
DYS¶
AC
Consultation group ID§
DYS
Baseline 26.3 (7.5)
27.1 (7.6) 34.5 (12.3)
27.5 (9.7)
25.5 (6.5) 35.0 (9.8)
5 months 15.2 (13.7)
12.9 (10.9) 17.5 (12.7)
15.0 (8.0)
15.5 (9.1) 25.5 (11.5)
12 months
12.1 (8.1)
14.4 (13.1) 15.4 (11.9)
13.7 (12.3)
12.8 (8.0) 22.4 (12.7)
24 months
10.7 (8.5)
12.2 (11.5) 13.5 (15.1)
13.1 (10.7)
11.8 (8.4) 17.2 (9.8)
*All values are means (SD). ODI scored from 0 to 100. † Oswestry questionnaire scored from 0 to 100. ‡ AC = active copers § ID = interpersonally distressed ¶ DYS = dysfunctional patients
Table 9. Visual analogue scale (VAS) for three patient profiles (AC, ID, DYS) in combination and consultation groups.* VAS†
AC‡
Combination group ID§
DYS¶
AC
Consultation group ID
DYS
Baseline 58.7 (22.2)
55.4 (20.6) 62.3 (23.3)
53.2 (21.2)
45.9 (19.2) 62.7 (18.9)
5 months 27.5 (26.2)
24.6 (22.8) 23.8 (19.2)
33.0 (22.7)
30.7 (23.4) 43.7 (24.0)
12 months
23.3 (18.1)
27.5 (25.0) 27.0 (21.5)
29.3 (27.2)
27.2 (18.9) 41.7 (25.5)
24 months
34.5 (22.4)
30.9 (25.3) 25.3 (25.7)
37.8 (26.4)
22.5 (20.4) 37.0 (24.8)
*All values are means (SD). VAS scored from 0 to 100. † Visual analogue pain scored from 0 to 100. ‡ AC = active copers § ID = interpersonally distressed ¶ DYS = dysfunctional patients
65

7 DISCUSSION
7.1 Principal findings For CLBP patients, spinal manipulative therapy with stabilizing exercises and spe-cialist information, advice, and encouragement was only slightly more beneficial in reducing pain and leading to patient satisfaction than was merely the specialist in-formation, advice, and encouragement alone. However, the health-related quality of life in both groups improved equally. The actual long-term clinical differences were statistically significant but from the clinical point of view still minor. The total an-nual cost-savings in the consultation group were greater. Visits to physicians, physiotherapy, or other manual therapies continued to decrease in both groups from the first follow-up year, as did sick-leave days. Mere consultation appeared to be more cost-effective than the combination therapy, which was the opposite of this study’s original hypotheses (I and III).
Psychometric factors, longer previous sick-leave days, and a low to mod-erate level of pain intensity proved to strongly predict poor treatment outcome. These psychometric factors included poor life control, poor self-evaluated prognosis of work ability in the future, and severe affective distress. University education and unmarried state were the only sociodemographic factors that predicted significantly the persistence of symptoms. Among clinical signs, only normal neurodynamic find-ings and normal range of forward flexion predicted poor recovery in the whole study group, and the noncentralization phenomenon in the combination group (II).
In perceived disability after the combined manipulative therapy, specific exercises, and information, dysfunctional (DYS) patients showed the greatest im-provement. Their high baseline ratings were improved to the same level as that of active copers (AC) or interpersonally distressed (ID) patients in the follow-up. Dur-ing the whole follow-up, their ratings for both perceived disability and pain intensity were on a lower level than among the DYS patients in the consultation group. For the AC or ID patients, the specialist’s information and encouraging instructions ap-peared to be as effective as the combined manipulative-exercise-information pro-gram (IV).
66

7.2 Strengths and limitations
7.2.1 Subjects The participants represented quite well the employed CLBP population regarding the persistence of their LBP. Baseline mean duration of LBP was 8 years (median duration 6 years). Most studies have focused on patients with acute or subacute pain, during which period the natural recovery rate is considerable.
Our patient sample was adequate for statistical power. Randomization was successful, since there were no significant differences in baseline characteristics. The dropout rate at one year was very low (3.9%) and even at two years moderate (20%), suggesting that compliance in both groups was good.
Subjects did not enter the study by the conventional medical system. They were recruited voluntarily by a widely circulated newspaper advertisement. Regard-ing subjective pain and disability, the study sample was, however, comparable to the CLBP population undergoing inpatient rehabilitation in Finland. The manner of recruitment may have gathered a patient group more motivated than the usual CLBP population and with different health behavior including work absenteeism. They were also about 6 years younger (37) than the average CLBP population, and the gender distribution was even in both groups. We set the upper age limit at 46 years, because we wanted to gather a homogenous group in a phase few years earlier with as few confusing factors (e.g., menopause) as possible. Although the clustering into three subgroups was successful, the DYS patients reported lower ODI indexes and were younger than in the study of fibromyalgia patients (Turk et al. 1998).
7.2.2 Methods 7.2.2.1 Spinal manipulative therapy The present study used manipulative therapy with a muscle-energy technique to correct any biomechanical dysfunction mainly in the pelvic segments (Chun 1991). The rationale for choosing this muscle-energy technique was that it is a safe and gentle method which suits even very acute and painful conditions. Assistance from the patient is valuable because movement is made to or through a barrier, providing the patient can be educated in gentle cooperation rather than excessive effort. The
67

technique is biomechanically justified and easily learned by medical doctors and physiotherapists. It may thus be disseminated beyond chiropractors, osteopaths, naprapaths, or manual therapists. Nor does it require any special equipment.
Sacroiliac joint dysfunction is considered the most common lesion of the lumbar-sacral region because the articular surfaces are large, the movement small, and all strains in the lower part of the body react in the SIJ (Wernham and Waldman 1981). The technique of the present study was principally directed at correcting any eventual sacral torsion which also affects the SIJ. Torsion was a common disorder in this study. Correction of sacral torsion usually relieved simultaneous radicular symptoms down to knee level. This is often empirically shown and well understood by the course of L5 and S1 nerve roots near the SIJ. The technique chosen was therefore well justified and succeeded. Nevertheless, much controversy surrounds the mechanisms and the role of the SIJ in lumbopelvic pain. According to existing evidence, SIJ pain is very resistant to identification by history and physical examina-tion (Dreyfuss et al. 1996).
7.2.2.2 Stabilizing exercises Stabilizing exercises were, in the present study, defined as relearning the motor skill of deep muscle co-contraction. The focus was on the activation of the transversus abdominis, the segmental levels of the lumbar multifidus, the diaphragm, and on the pelvic floor muscles independent of the global muscles of the outer sleeve of sup-port. The inner layer was trained to provide segmental stabilization, while the outer musculo-fascial unit was trained to provide a more general lumbopelvic stability function. After the perception and precision of the motor skill was improved and practiced repeatedly, the progression was to functional upright tasks. The final at-tempt was to change the automatic pattern of abdominal muscle activity in response to predictable arm or leg movements as well as unpredictable perturbations such as unexpected arm loading and support-surface translations (Hodges 2003).
The total number of physiotherapy sessions was quite low compared to those in similar studies on stabilizing exercises (O'Sullivan et al. 1997). The more intense training in stabilizing exercises may have resulted in larger differences be-tween group outcomes.
68

7.2.2.3 Cognitive-behavioral approach
Patients in the present study were approached in a multidimensional way without a multidisciplinary team. Both the specialist and the manual therapist employed cogni-tive-behavioral techniques including comprehensive information about patients’ individual low back trouble, education in sound ways in which to handle LBP in-cluding dosage of activity and medication, and finally improvement in patient em-powerment by reducing fear and negative thoughts and by increasing coping strate-gies. The effectiveness of this approach may even be stronger when the psychologi-cal component is more masked. Many patients have prejudices against the “psy-chologization” of their LBP and may be more open to information from either the physician or the physiotherapist. The crucial point is that the physician and the physiotherapist may constitute a “multidisciplinary team” if they are capable of treating the patients in a multidimensional manner. Dysfunctional patients benefited from this combined approach even more than from more comprehensive multidisci-plinary treatments, as shown in earlier studies (Rudy et al. 1995; Turk et al. 1998).
7.2.3 Outcomes 7.2.3.1 Pain and disability In the combination group, one cannot, of course, specify the effect of manipulative therapy, of stabilizing exercises, or of the information provided each separately. The combination group had more contacts than did the consultation group, which in it-self can be beneficial, adding to patient satisfaction. A positive association can occur between number of contacts with providers and improvement in back-related symp-toms (Coxhead et al. 1981). Thus, the slightly pronounced short-term improvement in pain and disability in the combination group may in part be due to non-specific effects such as general encouragement and supportive guidance rather than to spe-cific treatment effects.
The additional value of the educational back booklet remains unclear. Evi-dence is, however, increasing in support of the use of educational material as ad-juncts to clinical management (Burton et al. 1999). Furthermore, the effect of an
69

educational booklet seems to be enhanced by personal contact with a medical pro-fessional (Cherkin et al. 1996).
The question arises whether the outcome measure regarding pain percep-tion in the combination group as compared to the consultation group at 2 years fol-low-up still remained clinically significant. In addition to conventional statistical analysis, the concept of minimal clinically important differences (MCID) in out-come scores may be useful. This is defined as the smallest difference score which patients perceive as beneficial (Fischgrund et al. 1997; Liang 2000). Regarding VAS, the MCID value (0-10) has been assessed as 2, and regarding ODI the values in different studies as from 5.2 to 16.3 (Farrar et al. 2001; Liang 2000; Suarez-Almazor et al. 2000; Taylor et al. 1999). Based on this, the statistical difference in the present study at the 2-year follow-up (2.4 on the VAS scale of 0-100) was not clinically significant.
7.2.3.2 Cost-effectiveness The economic evaluation was carefully conducted, including analysis of both direct and indirect costs. Incremental cost-effectiveness analysis was made for pain inten-sity and disability by bootstrapping techniques. Our intervention was compared to the best available alternative for unspecific LBP patients at the moment. Karjalainen et al. (2003) showed in a sample of subacute patients that “mini-intervention” based on individual information was superior to patients’ usual health care. The personal advice and information in the present study was very similar to the regimen of Kar-jalainen et al.
The major limitation of our economic evaluation was that data were col-lected by a retrospective questionnaire. Recall bias is a well-known problem in eco-nomic evaluations. Patients barely remember health care utilization beyond 2 months. The retrospective questionnaire is, however, a common method in cost-effectiveness studies. Burdorf et al. (1996) found questionnaires on sickness absence due to back pain reliable in their 6-month survey. Aalto et al. (1999) showed ques-tionnaires on in-patient days to be reliable for the previous year. In the present study, the baseline data may be an underestimate of health care use and sickness absence. Data from the 24-month study period are more reliable, as the participants were asked to record all health care use and sick leave due to LBP.
70

7.2.3.3 Psychosocial determinants (MPI subgroups) MPI subgrouping provided valuable information on the determinants of slight dif-ferences between groups. A Finnish translation of the MPI (SIMPI) proved effective in producing the three cluster profiles. For the first time, this was used in a random-ized setting. The comparatively low level of disability observed among our patients may limit the generalizability of our findings.
Improvement shown by the DYS patients may be related to the suggested association between pain and affective distress, and the resulting non-acceptance of pain and the avoidance behavior (Asmundson et al. 1997). It is possible that the DYS patients received help in facing their fear of pain and disability in a safe and reinforcing environment during combination treatment, this helping them to accept their situation in a positive and realistic manner. As a result, they showed greater reduction in pain and disability than did patients in the consultation group. It is also possible that the companions of DYS patients were, after the therapy period, less concerned about those DYS individuals, resulting in their reported decrease in social support. 7.2.3.4 Physical activity (MetPro®) The MetPro® questionnaire was used to assess the intensity of physical activity at work, at leisure, and during commuting both at baseline and at the one-year follow-up. In general, level of physical activity was lower among patients in the consulta-tion group but increased at one year significantly more than in the combination group. In fact, the consultation group raised their maximal intensity of activity to a quite stressful exercise level equal to strenuous physical jobs, exceeding the thresh-old to enhance aerobic capacity dependent on exercise time. This may have clinical importance in the coping with symptoms. At least they could not be enduring pain during such exercise. The explanation for differences between groups could be that both the AC and ID patients in the consultation group took advice on self-care man-agement and changed their exercise habits.
Hardly any reliable indirect physical-activity measurements are available for general use. One advantage of the MetPro® questionnaire is that it takes into consideration all aspects of physical activity: quality, frequency, duration, and inten-sity. Additionally, the repeatability of the MetPro® questionnaire has proven ade-quate. Questionnaire results also correlate with hand-grip strength and with energy
71

consumption in the usual activities. It has been used in Finnish studies examining associations between physical activity and performance capacity in healthy and chronically ill populations (Mälkiä et al. 1994) and connections between physical activity and back pain (Kuukkanen and Mälkiä 1996; 2000). In a study of over 7000 subjects, Mälkiä and Impivaara (1998) assessed the intensity of physical activity of asthmatic adults in Finland and associations between intensity of physical activity and respiratory function in asthmatic and nonasthmatic individuals. Measured with the MetPro® questionnaire, results showed clear and significant associations in asthmatic men between spirometric values and intensities of physical activity at work and during leisure time.
One limitation in use of questionnaires is that respondents do not necessar-ily remember accurately their recent physical activities or may exaggerate duration or intensity of exercise. Therefore, respondents’ age and level of education must be taken into consideration (Montoye et al. 1996). Since the mean age of the patients in this study was 37, it is more probable that the results are real than if the respondents were children or were elderly. The largest source of error in MET measurements is the variation in basic energy consumption between individuals. The error may be as high as 10% (McArdle et al. 1996). Estimating intensity of energy consumption for walking, running, and cycling, the error is 5 to 10 % of laboratory values (1986). Taking these limitations into account, these results show that CLBP patients can increase the intensity of their physical activity without worsening their pain and disability. Results also show that with a specialist’s instructions for exercise, CLBP patients may maintain or even improve their functioning and so improve their work ability.
7.2.3.5 Functional changes At 5 months, significant improvements in all clinical variables were evident in both groups, but two tests favored the combination group: the contralateral test (CLT) and left-sided SLUMP. Correction of SIJ dysfunction was usually followed by im-provement in these two test-results. An interesting question arises as to why the biomechanical dysfunctions improved also among the patients in the consultation group. The specialist’s instructions for correction of the biomechanical dysfunctions appeared to have an influence on recovery. Right-sided pelvic dysfunction appeared to be more easily corrected by self-performed techniques.
72
Co-activation of the transversus abdominis and lumbar multifidus was verified by palpation and measurement of the pressure changes by use of the Stabi-lizer®. Surprisingly, patients in the consultation group tended to improve their abil-ity to activate the deep stabilizing muscles more than did patients in the combination group (P = 0.096, ANOVA). Because this kind of measurement also acts simultane-ously as a learning procedure, the consultation group was not completely naive in this sense. Since the reliability of this measurement is not confirmed, no conclusions as to the effects of the stabilizing exercises can be drawn.
7.3 Results in relation to other studies
7.3.1 Effectiveness of spinal manipulative therapy and exercises (I, III) Previous studies of LBP with at least a one-year follow-up have compared chiro-practic, osteopathic or other manipulative therapy with physiotherapy (Cherkin et al. 1998; Koes et al. 1992; Skargren et al. 1998), placebo (Koes et al. 1992), treatment by a general practitioner (Koes et al. 1992), hospital outpatient management (Meade et al. 1995), an educational booklet (Cherkin et al. 1998), or chemonucleolysis (Burton et al. 2000). No significant differences appeared in effects or costs between chiropractic manipulative therapy and physiotherapy (Cherkin et al. 1998; Skargren et al. 1998), or differences were minor in favor of manipulative therapy (Koes et al. 1992). These two treatments were only marginally better but more costly than the minimal intervention of an educational booklet (Cherkin et al. 1998) and were better than placebo or treatment given by a GP (Koes et al. 1992).
Patients seem to be more satisfied with chiropractic treatment than with hospital outpatient management (Meade et al. 1995) or medical care (Hertzman-Miller et al. 2002), as in this study as well. Self-care advice and explanation of treatment predicted satisfaction and reduced the expected difference between chiro-practic patients’ and medical patients’ satisfaction (Hertzman-Miller et al. 2002).
Thus far, very few RCTs of specific stabilizing exercises exist for CLBP treatment. One RCT involving radiological diagnosis of spondylolysis or spondylo-listhesis showed a significant and lasting reduction in pain intensity and functional
73

disability levels compared with reduction in other commonly prescribed conserva-tive treatment programs (O'Sullivan et al. 1997). In the present study, that spinal pathology was more various may have hampered the therapeutic effect of stabilizing exercises.
7.3.2 Predictive factors for unfavorable treatment outcome (II)
The centralization phenomenon allows patients to be classified either as centralizers or as noncentralizers. This trait has been considered a prognostic factor for devel-opment of CLBP (Werneke and Hart 2001), and a predictor of outcome from its conservative treatment (Long 1995). For centralizers, the directional exercises (McKenzie techniques) with repetitive back or forward flexions have been the treatment of choice. In the present study, patients with radiating pain, a positive SLUMP test, restriction in forward flexion, and with the centralization phenomenon benefited from our treatment approach. Noncentralizers, on the other hand, seem not to improve either with the combination treatment in the present study or with the McKenzie exercises (Werneke and Hart 2001; Werneke et al. 1999). Surprisingly, the overall baseline level of physical activity during daily life failed to predict out-come, unlike in the findings of Thomas et al (1999).
In the whole study group and in the consultation group, work-related fac-tors including longer history of absence from work, poor present work ability, and poor self-predicted future work ability turned out to be strong determinants for poor treatment outcome. Other studies’ association was thus confirmed (Coste et al. 1994; Gatchel et al. 1995; Thomas et al. 1999). Such work-related factors were, however, no longer barriers to success of recovery with the manipulative and exercise therapy added. This observation calls for more detailed study.
7.3.3 Psychosocial factors as determinants of treatment outcome (IV) The interpretation of earlier follow-up studies using the psychosocial patient classi-fication may thus not be warranted. Present findings correspond to earlier ones (Rudy et al. 1995; Turk et al. 1998), but the present method included no intentional
74

multidisciplinary treatment elements. Although multidisciplinary elements, in the traditional sense, were absent from the present study, the DYS patients showed the greatest improvement. Here, the decrease in perceived disability among DYS pa-tients to a level comparable to that of AC or ID patients was even more dramatic than earlier. The patient groups did, however, differ. In the Turk et al.(1998) study, their fibromyalgia patients reported ODI indexes, at least among their DYS patients, higher than those shown here. Our subjects’ level of pain corresponds to that in Bergström et al. (2001) for their long-term spinal pain patients. They found no dif-ference in improvement in any patient group, although their rehabilitation method was similar to ours. They, however, included no control group. In the present study, no improvement favored any patient group on the VAS index within the combina-tion group, but between the combination and the consultation group a remarkable difference appeared among DYS patients. As Bergström et al. (2001) used no con-trol group, one cannot say whether their DYS patients showed less improvement without treatment.
Previous studies report a decrease in affective distress among their DYS patients (Rudy et al. 1995; Turk et al. 1998), corresponding to a finding also in this study for both groups. Thus, due to the lack of any control group in previous studies, whether changes in affective distress would also have occurred with less compre-hensive treatment remains obscure.
7.4 Meaning of the study This has been the first study combining manipulative therapy and stabilizing exer-cises with a specialist’s informational package for LBP patients. Comparing the present study to other mere manipulative-therapy studies, here both inter-group changes in pain and disability (Meade et al. 1995; Skargren et al. 1998) and intra-group changes in pain were more pronounced (Meade et al. 1995). The patients were slightly more satisfied with each of the treatment arms, as well (Meade et al. 1995).
Evaluation of which components in the intervention were most effective is difficult. Based on functional assessment, manipulative therapy with correction of biomechanical dysfunction appeared to have some positive effect. Some improve-ment could also be achieved by teaching self-care techniques for correction of dys-function at least in the sacroiliac segments. Information, motivation, and encour-agement (CBA) were probably equally or even more effective than was improve-
75

ment of biomechanical dysfunction. The effects of stabilizing exercises remained unclear for these CLBP patients.
Despite the lack of a true placebo control group in this study, it is highly probable that the specialist’s information package changed the natural course of CLBP. The positive changes in the consultation group were slower to appear but long-lasting. In addition, cost savings were achieved both for the patient and for society. The effects on HRQOL were equal in both groups, but patients in the con-sultation group changed their behavior more consistently by reducing their use of health care services and sick leave and by intensifying their exercise and other ac-tivities.
Increasing evidence exists that proper patient information, explanation of the background of their symptoms and findings, and the meaning of the exercises added to encouragement and attempts to reduce pain-related fear can reduce work absenteeism (Hagen et al. 2000; Indahl et al. 1998) and increase patient satisfaction (Hertzman-Miller et al. 2002). It is important that patients consider the care-provider as a reliable and knowledgeable expert. The information provided in the consultation group, furthermore, may have directed patients more consistently and uniformly toward independent self-care and self-efficacy. Although patients in the combination group received the same information as in the consultation group, the latter may have acted more in accordance with the self-care advice.
The SIMPI classification showed predictive validity. Subgroup affiliation prior to treatment was predictive of amount of disability and pain and of subsequent changes, depending on treatment during follow-up. Dysfunctional-profile patients seem to respond to treatment more sensitively even without stress management or a multidisciplinary treatment program. Follow-up studies with patient profile groups should emphasize the importance of comparison groups.
Recalling the WHO model for the disablement process (Figure 1), the con-sultation approach produced a positive effect on all levels of disablement: impair-ment, activity, and participation. Combination therapy, in contrast, influenced pri-marily reduction in the impairment. Of personal factors, psychosocial characteristics with coping strategies were crucial to the experience and to the lessening of dis-ablement.
76

7.5 Implications for practice and research Unexpectedly favorable improvement regarding pain, disability, and health-related quality of life occurred after the specialist consultation alone with its encourage-ment, persuasive information, and expert advice. The combination treatment includ-ing manipulative therapy, stabilizing exercises, and specialist consultation did not clearly enhance the effect gained by the specialist consultation.
Based on subgroup analysis, some assumptions could be made concerning clinical practice. Generally, patients showed improvement in both treatment arms. Findings for two subgroups, however, predicted minimal improvement after short outpatient approaches. The first group included highly-educated patients with mini-mal or moderate symptoms according to VAS score and an absence of radiating pain based on neurodynamic evaluation (SLUMP test). The second group included those with a large psychosocial burden, work absenteeism, and a poor subjective expecta-tion of future work ability. For the first group, a short, informative outpatient consul-tation resulting in slight improvement may be sufficient. The second group of pa-tients, on the other hand, may need more comprehensive treatment including infor-mation, manipulative therapy, exercises, and a psychosocial approach as well. Im-plications for clinical practice are that we should - besides clinical testing - pay more attention to psychometric evaluation by careful interviewing and use of standardized questionnaires in determining the appropriate intervention.
For the clinical usefulness of MPI clustering, these results should be con-firmed with different patient groups. These findings should also be contrasted with those after various kinds of psychosocial treatment elements.
77
8 CONCLUSIONS Recalling the aims of these studies, the following results and conclusions can be summarized: 1. Both treatments, the specialist consultation alone (with encouragement, persua-sive information, and expert advice) and the combination treatment including in addition also manipulative therapy and stabilizing exercises, resulted in unexpect-edly good improvement regarding pain, disability, and health-related quality of life. The combination treatment did not enhance the effect gained after the specialist consultation to any clinically significant degree. 2. Severe affective distress predicted poor response to the combination treatment. A total of over 25 days of sick leave during the previous year, poor life control, and generalized somatic symptoms were the risk factors for gaining no benefit from the specialist consultation alone. 3. Specialist consultation alone was more cost-effective in view of both health care use and work absenteeism, and led to an increase in health-related quality of life equal to that from the combination treatment. 4. Psychosocial factors did modify the treatment effect. After the combination treatment, dysfunctional patients showed the greatest improvement in perceived disability. In the consultation group, patients showing active coping behavior as well as interpersonally distressed patients showed lower ratings for both perceived dis-ability and pain intensity than did dysfunctional patients. For the AC or ID patients, the information and encouraging instructions appeared to be as effective as the com-bination treatment. 5. Possible mechanisms behind the favorable clinical outcomes differed between groups. The consultation group tended to increase more their active time and in-crease the intensity of their physical exercise and of other activities than did the combination group. Although the functional variables in both groups improved sig-nificantly, there appeared some favorable biomechanical changes in the combination group which possibly contributed to and explained some slightly advantageous clinical outcomes after the combination treatment.
78

9 ACKNOWLEDGEMENTS This study was carried out at the Rehabilitation Unit of ORTON Orthopaedic Hospi-tal, the Invalid Foundation, Helsinki, Finland, during 1999-2005.
I devote my warmest gratitude to the supervisors of my work, Docents Karl-August Lindgren and Heikki Hurri, of the ORTON Orthopaedic Hospital, for providing me excellent research facilities, for inspiring discussions, for their enthu-siastic and endless support, and for practical guidance during the whole study pe-riod. Docent Lindgren originally refined the study idea which I presented to him and discussed the clinical methology of the study. Docent Hurri enlightened me on the methodology of scientific research and introduced to me the fascinating field of low back pain research.
My warmest appreciation goes to the official reviewers of the study, Do-cents Simo Taimela and Antti Malmivaara, for their well acquaintance with the study, constructive criticism, and exceptionally valuable advice which considerably improved the thesis.
I am deeply grateful to my co-authors: Tiina Lahtinen-Suopanki, PT, for providing vast clinical experience and intuition in manual medicine for the benefit of this study and for her inestimable friendship; Professor Seppo Sarna for sharing his time and expertise in statistics; Professor Pekka Rissanen for introducing to me the methodology of health-economic evaluation and for helping me with cost-effectiveness analyses; and Markku Riipinen, Ph.D., for sharing his expertise in psychology and for widening the perspective of this study.
My warm thanks are due to my dear friend, sculptor Harry Kivijärvi for the cover drawing despite difficult circumstances, to Carol Norris, Ph.D., for revi-sion of the thesis language including the manuscripts and for valuable advice during English oral and writing courses, and to Ulla-Maija Nurminen for helping me with the lay-out of this thesis.
I am grateful to all the patients who participated and gave their commit-ment to this study. I am also indebted to Anneli Stranden for secretarial work, to Anitta Isosalo-Ekholm for helping me searching for the references, and other staff at ORTON for cooperation and a most enthusiastic attitude.
I acknowledge my colleagues at ORTON, especially doctors Pekka Ranta-nen, Teija Lund, Jukka-Pekka Kouri, Maarit Gockel, and Simo Järvinen for inspir-ing conversations and constructive criticism. I express my warmest thanks to all my friends for support and for being such good listeners.
79

I am deeply grateful to my parents Irmeli Sandlund and Kalervo Lammen-ranta, their spouses Börje Sandlund and Ani Kivinen, my brother Markus Lammen-ranta and his wife Arja, and my late parents-in-law Henna and Pertti Niemistö for their support of and great interest in my work.
Most of all, I express my deepest feeling of gratitude and love to my hus-band Kari and to our sons Kai, Karri, and Henri for their love, patience, and support during these years. This thesis is dedicated to them.
The Social Insurance Institute of Finland and Finska Läkarsällskapet sup-ported this study, for which I am very grateful.
Helsinki, March 2005
Leena Niemistö
80

10 REFERENCES Aalto, A.-M., Klaukka, T., Rissanen, P., Hakola, R. and Kerppilä, S., [Asthma in the Finnish
population of working age], Studies in social security and health, Vol. 43, Social In-surance Institute, Finland, Helsinki, 1999.
Afifi, A.A. and Clark, V., Computer-aided multivariate analysis. Texts in statistical science., Chapman & Hall, London, 1998, 263, 395-8, 400-403 pp.
Ainsworth, B.E., Haskell, W.L., Whitt, M.C., Irwin, M.L., Swartz, A.M., Strath, S.J., O'Brien, W.L., Bassett, D.R., Jr., Schmitz, K.H., Emplaincourt, P.O., Jacobs, D.R., Jr. and Leon, A.S., Compendium of physical activities: an update of activity codes and MET intensities, Med Sci Sports Exerc, 32 (2000) S498-504.
American College of Sports Medicine. Guidelines for graded exercise testing and prescrip- tion, Lea&Febiger, Philadelphia, 1975. American College of Sports Medicine. Guidelines for graded exercise testing and prescrip-
tion, Lea&Febiger, Philadelphia, 1980. American College of Sports Medicine. Guidelines for exercise testing and prescription, PE:
Lea & Febiger, Philadelphia, 1986. American College of Sports Medicine. ACSM's guidelines for exercise testing and prescrip-
tion, Williams & Wilkins, Baltimore, 1995. American College of Sports Medicine. ACSM's guidelines for exercise testing and prescrip-
tion, Lippincott, Williams & Wilkins, Philadelphia, 2000. Arinen, S., Häkkinen, U., Klaukka, T., Klavus, J., Lehtonen, R. and Aro, S., Health and the
use of health services in Finland. Main findings of the Finnish Health Care Survey 1995/96, and changes from 1987., Official Statistics of Finland, Health Care., Vol. 5, 1998.
Arkuszewski, Z., The efficacy of manual treatment in low back pain: a clinical trial, Manual Med, 2 (1986) 68-71.
Asmundson, G.J., Norton, G.R. and Allerdings, M.D., Fear and avoidance in dysfunctional chronic back pain patients, Pain, 69 (1997) 231-6.
Assendelft, W.J., Koes, B.W., Knipschild, P.G. and Bouter, L.M., The relationship between methodological quality and conclusions in reviews of spinal manipulation, Jama, 274 (1995) 1942-8.
Assendelft, W.J., Morton, S.C., Yu, E.I., Suttorp, M.J. and Shekelle, P., Spinal manipulative therapy for low back pain. A meta-analysis of effectiveness relative to other thera-pies, Ann Intern Med, 138 (2003) 871-881.
Bendix, A.F., Bendix, T. and Haestrup, C., Can it be predicted which patients with chronic low back pain should be offered tertiary rehabilitation in a functional restoration program? A search for demographic, socioeconomic, and physical predictors, Spine, 23 (1998) 1775-83; discussion 1783-4.
Bergstrom, G., Jensen, I.B., Bodin, L., Linton, S.J. and Nygren, A.L., The impact of psycho-logically different patient groups on outcome after a vocational rehabilitation pro-gram for long-term spinal pain patients, Pain, 93 (2001) 229-37.
Boden, S.D. and Wiesel, S.W., Lumbosacral segmental motion in normal individuals. Have we been measuring instability properly?, Spine, 15 (1990) 571-6.
Braithwaite, I., White, J., Saifuddin, A., Renton, P. and Taylor, B.A., Vertebral end-plate (Modic) changes on lumbar spine MRI: correlation with pain reproduction at lum-bar discography, Eur Spine J, 7 (1998) 363-8.
81

Bram, J., Zanetti, M., Min, K. and Hodler, J., MR abnormalities of the intervertebral disks and adjacent bone marrow as predictors of segmental instability of the lumbar spine, Acta Radiol, 39 (1998) 18-23.
Buchbinder, R., Jolley, D. and Wyatt, M., 2001 Volvo Award Winner in Clinical Studies: Effects of a media campaign on back pain beliefs and its potential influence on management of low back pain in general practice, Spine, 26 (2001) 2535-42.
Burdorf, A., Post, W. and Bruggeling, T., Reliability of a questionnaire on sickness absence with specific attention to absence due to back pain and respiratory complaints, Oc-cup Environ Med, 53 (1996) 58-62.
Burton, A.K., Tillotson, K.M. and Cleary, J., Single-blind randomised controlled trial of chemonucleolysis and manipulation in the treatment of symptomatic lumbar disc herniation, Eur Spine J, 9 (2000) 202-7.
Burton, A.K., Tillotson, K.M., Main, C.J. and Hollis, S., Psychosocial predictors of outcome in acute and subchronic low back trouble, Spine, 20 (1995) 722-8.
Burton, A.K., Waddell, G., Tillotson, K.M. and Summerton, N., Information and advice to patients with back pain can have a positive effect. A randomized controlled trial of a novel educational booklet in primary care, Spine, 24 (1999) 2484-91.
Butler, D., Mobilisation of the Nervous System, Churchill Livingstone, 1991. Carragee, E.J., Paragioudakis, S.J. and Khurana, S., 2000 Volvo Award winner in clinical
studies: Lumbar high-intensity zone and discography in subjects without low back problems, Spine, 25 (2000) 2987-92.
Central Statistics of Finland, 2000b. Cherkin, D.C., Deyo, R.A., Battie, M., Street, J. and Barlow, W., A comparison of physical
therapy, chiropractic manipulation, and provision of an educational booklet for the treatment of patients with low back pain, N Engl J Med, 339 (1998) 1021-9.
Cherkin, D.C., Deyo, R.A., Street, J.H., Hunt, M. and Barlow, W., Pitfalls of patient educa-tion. Limited success of a program for back pain in primary care, Spine, 21 (1996) 345-55.
Cherkin, D.C., Sherman, K.J., Deyo, R.A. and Shekelle, P.G., A review of the evidence for the effectiveness, safety, and cost of acupuncture, massage therapy, and spinal ma-nipulation for back pain, Ann Intern Med, 138 (2003) 898-906.
Chun, L., Muscle Energy Techniques. Treating Sacral Dysfunctions. In: D. EL and S. S (Eds.), An Osteopathic Approach to Diagnosis and Treatment., Vol. 14, Lippincott Williams and Wilkins, Philadelphia, 1991, pp. 221-4.
Claude, L.N., Solomonow, M., Zhou, B.H., Baratta, R.V. and Zhu, M.P., Neuromuscular dysfunction elicited by cyclic lumbar flexion, Muscle Nerve, 27 (2003) 348-58.
Compas, B.E., Haaga, D.A., Keefe, F.J., Leitenberg, H. and Williams, D.A., Sampling of empirically supported psychological treatments from health psychology: smoking, chronic pain, cancer, and bulimia nervosa, J Consult Clin Psychol, 66 (1998) 89-112.
Coste, J., Delecoeuillerie, G., Cohen de Lara, A., Le Parc, J.M. and Paolaggi, J.B., Clinical course and prognostic factors in acute low back pain: an inception cohort study in primary care practice, Bmj, 308 (1994) 577-80.
Coxhead, C.E., Inskip, H., Meade, T.W., North, W.R. and Troup, J.D., Multicentre trial of physiotherapy in the management of sciatic symptoms, Lancet, 1 (1981) 1065-8.
Cutler, R.B., Fishbain, D.A., Rosomoff, H.L., Abdel-Moty, E., Khalil, T.M. and Rosomoff, R.S., Does nonsurgical pain center treatment of chronic pain return patients to work? A review and meta-analysis of the literature, Spine, 19 (1994) 643-52.
Deyo, R.A., Andersson, G., Bombardier, C., Cherkin, D.C., Keller, R.B., Lee, C.K., Liang, M.H., Lipscomb, B., Shekelle, P., Spratt, K.F. and et al., Outcome measures for studying patients with low back pain, Spine, 19 (1994) 2032S-2036S.
82

Deyo, R.A. and Diehl, A.K., Patient satisfaction with medical care for low-back pain, Spine, 11 (1986) 28-30.
DonTigny, R.L., Function and pathomechanics of the sacroiliac joint. A review, Phys Ther, 65 (1985) 35-44.
Dreyfuss, P., Michaelsen, M., Pauza, K., McLarty, J. and Bogduk, N., The value of medical history and physical examination in diagnosing sacroiliac joint pain, Spine, 21 (1996) 2594-602.
Durnin, J. and Passmore, R., Energy, work and leisure, Heinemann Educational Books, Lon-don, 1967.
Ebenbichler, G., Oddsson, L.I., Kollmitzer, J. and Erim, Z., Sensory-motor control of the lower back: implications for rehabilitation, Med Sci Sports Exerc, 33 (2001) 1889-98.
Evans, D.P., Burke, M.S., Lloyd, K.N., Roberts, E.E. and Roberts, G.M., Lumbar spinal manipulation on trial. Part I--clinical assessment, Rheumatol Rehabil, 17 (1978) 46-53.
Fairbank, J., Use of Oswestry Disability Index (ODI), Spine, 20 (1995) 1535-7. Fairbank, J.C. and Pynsent, P.B., The oswestry disability index, Spine, 25 (2000) 2940-53. Farfan, H.F. and Gracovetsky, S., The nature of instability, Spine, 9 (1984) 714-9. Farrar, J.T., Young, J.P.J., LaMoreaux, L., Werth, J.L. and Poole, R.M., Clinical importance
of changes in chronic pain intensity measured on an 11-point numerical pain rating scale, Pain, 94 (2001) 149-58.
Ferreira, M.L., Ferreira, P.H., Latimer, J., Herbert, R. and Maher, C.G., Does spinal manipu-lative therapy help people with chronic low back pain?, Aust J Physiother, 48 (2002) 277-84.
Fischgrund, J.S., Mackay, M., Herkowitz, H.N., Brower, R.S., Montgomery, D.M. and Kurz, L.T., 1997 Volvo award winner in clinical studies. Degenerative lumbar spondylo-listhesis with spinal stenosis: a prospective, randomized study comparing decom-pressive laminectomy and arthrodesis with and without spinal instrumentation., Spine, 22 (1997) 2807-12.
Fortin, J.D. and Falco, F.J., The Fortin finger test: an indicator of sacroiliac pain, Am J Or-thop, 26 (1997) 477-80.
Furlan, A.D., Clarke, J., Esmail, R., Sinclair, S., Irvin, E. and Bombardier, C., A critical review of reviews on the treatment of chronic low back pain, Spine, 26 (2001) E155-62.
Gardner-Morse, M., Stokes, I.A. and Laible, J.P., Role of muscles in lumbar spine stability in maximum extension efforts, J Orthop Res, 13 (1995) 802-8.
Gatchel, R.J., Polatin, P.B. and Mayer, T.G., The dominant role of psychosocial risk factors in the development of chronic low back pain disability, Spine, 20 (1995) 2702-9.
Gerlander, E., Hurri, H., Kaunola, R. and al., e., [The Back Triumph], Rehabilitation Center of Orton, Invalid Foundation, Helsinki, 1995.
Gertzbein, S.D., Seligman, J., Holtby, R., Chan, K.H., Kapasouri, A., Tile, M. and Cruick-shank, B., Centrode patterns and segmental instability in degenerative disc disease, Spine, 10 (1985) 257-61.
Goossens, M.E. and Evers, S., Cost-effectiveness of treatment for neck and low back pain. In: A. Nachemson and E. Jonsson (Eds.), Neck and back pain. The scientific evi-dence of causes, diagnosis, and treatment, Lippincott Williams & Wilkins, Phila-
Gross, A.R., Hoving, J.L., Haines, T.A., Goldsmith, C.H., Kay, T., Aker, P. and Bronfort, G., Manipulation and mobilisation for mechanical neck disorders, Cochrane Database Syst Rev, 2 (2004).
83
delphia, 2000, pp. 399-420.

Hagen, E.M., Eriksen, H.R. and Ursin, H., Does early intervention with a light mobilization program reduce long-term sick leave for low back pain?, Spine, 25 (2000) 1973-6.
Hamberg, J., Bjorklund, M., Nordgren, B. and Sahlstedt, B., Stretchability of the rectus femoris muscle: investigation of validity and intratester reliability of two methods including X-ray analysis of pelvic tilt, Arch Phys Med Rehabil, 74 (1993) 263-70.
Harvey, E., Burton, A.K., Moffett, J.K. and Breen, A., Spinal manipulation for low-back pain: a treatment package agreed to by the UK chiropractic, osteopathy and physio-therapy professional associations, Man Ther, 8 (2003) 46-51.
Hazard, R.G., Reid, S., Haugh, L.D. and McFarlane, G., A controlled trial of an educational pamphlet to prevent disability after occupational low back injury, Spine, 25 (2000) 1419-23.
Heikkinen, K., Hujanen, T. and Rusanen, H., [Unit expenses of the heathcare system in Finland in the year of 2000], Stakes. Aiheita, Vol. 22, Stakes, Helsinki, 2001.
Hemmilä, H.M., Quality of life and cost of care of back pain patients in Finnish general practice, Spine, 27 (2002) 647-53.
Hertzman-Miller, R.P., Morgenstern, H., Hurwitz, E.L., Yu, F., Adams, A.H., Harber, P. and Kominski, G.F., Comparing the satisfaction of low back pain patients randomized to receive medical or chiropractic care: results from the UCLA low-back pain study, Am J Public Health, 92 (2002) 1628-33.
Hilde, G., Hagen, K., Jamtvedt, G. and Winnem, M., Advice to stay active as a single treat-ment for low-back pain and sciatica, Cochrane Database Syst Rev, 2 (2004).
Hildebrandt, J., Pfingsten, M., Saur, P. and Jansen, J., Prediction of success from a multidis-ciplinary treatment program for chronic low back pain, Spine, 22 (1997) 990-1001.
Hodges, P., Neuromechanical control of the spine, Department of Neuroscience, Karolinska Institutet, Stockholm, 2003, pp. 1-47.
Hodges, P. and Moseley, L., Pain and motor control of the lumbopelvic region: effect and possible mechanisms, J Electromyogr Kinesiol, 13 (2003) 361-70.
Hodges, P.W., Moseley, G.L., Gabrielsson, A. and Gandevia, S.C., Experimental muscle pain changes feedforward postural responses of the trunk muscles, Exp Brain Res, 151 (2003) 262-71.
Hodges, P.W. and Richardson, C.A., Inefficient muscular stabilization of the lumbar spine associated with low back pain. A motor control evaluation of transversus ab-dominis, Spine, 21 (1996) 2640-50.
Hodges, P.W. and Richardson, C.A., Delayed postural contraction of transversus abdominis in low back pain associated with movement of the lower limb, J Spinal Disord, 11 (1998) 46-56.
Howley, E.T., Type of activity: resistance, aerobic and leisure versus occupational physical activity, Med Sci Sports Exerc, 33 (2001) S364-9; discussion S419-20.
Hurri, H., The Swedish back school in chronic low back pain. Part I. Benefits, Scand J Reha-bil Med, 21 (1989) 33-40.
Indahl, A., Low back pain - a functional disturbance. Physiology and treatment, Centre for Orthopaedics, National Hospital, University of Oslo, Oslo, 1999, pp. 17-20.
Indahl, A., Haldorsen, E.H., Holm, S., Reikeras, O. and Ursin, H., Five-year follow-up study of a controlled clinical trial using light mobilization and an informative approach to low back pain, Spine, 23 (1998) 2625-30.
Indahl, A., Kaigle, A.M., Reikeras, O. and Holm, S.H., Interaction between the porcine lum-bar intervertebral disc, zygapophysial joints, and paraspinal muscles, Spine, 22 (1997) 2834-40.
Indahl, A., Velund, L. and Reikeraas, O., Good prognosis for low back pain when left un-tampered. A randomized clinical trial, Spine, 20 (1995) 473-7.
84

Ito, M., Incorvaia, K.M., Yu, S.F., Fredrickson, B.E., Yuan, H.A. and Rosenbaum, A.E., Predictive signs of discogenic lumbar pain on magnetic resonance imaging with discography correlation, Spine, 23 (1998) 1252-8; discussion 1259-60.
Jadad, A.R. and McQuay, H.J., Meta-analyses to evaluate analgesic interventions: a system-atic qualitative review of their methodology, J Clin Epidemiol, 49 (1996) 235-43.
Jamison, R.N., Rudy, T.E., Penzien, D.B. and Mosley, T.H., Jr., Cognitive-behavioral classi-fications of chronic pain: replication and extension of empirically derived patient profiles, Pain, 57 (1994) 277-92.
Jayaraman, G., Nazre, A.A., McCann, V. and Redford, J.B., A computerized technique for analyzing lateral bending behavior of subjects with normal and impaired lumbar spine. A pilot study, Spine, 19 (1994) 824-32.
Kaigle, A.M., Holm, S.H. and Hansson, T.H., 1997 Volvo Award winner in biomechanical studies. Kinematic behavior of the porcine lumbar spine: a chronic lesion model, Spine, 22 (1997) 2796-806.
Kaigle, A.M., Wessberg, P. and Hansson, T.H., Muscular and kinematic behavior of the lumbar spine during flexion-extension, J Spinal Disord, 11 (1998) 163-74.
Karjalainen, K., Malmivaara, A., Pohjolainen, T., Hurri, H., Mutanen, P., Rissanen, P., Pahkajärvi, H., Levon, H., Karpoff, H. and Roine, R., Mini-intervention for subacute low back pain: a randomized controlled trial, Spine, 28 (2003) 533-40; discussion 540-1.
Kerns, R.D., Turk, D.C. and Rudy, T.E., The West Haven-Yale Multidimensional Pain In-ventory (WHYMPI), Pain, 23 (1985) 345-56.
Koes, B.W., Bouter, L.M., van Mameren, H., Essers, A.H., Verstegen, G.M., Hofhuizen, D.M., Houben, J.P. and Knipschild, P.G., Randomised clinical trial of manipulative therapy and physiotherapy for persistent back and neck complaints: results of one year follow up, Bmj, 304 (1992) 601-5.
Kuukkanen, T. and Mälkiä, E., Muscular performance after a 3 month progressive physical exercise program and 9 month follow-up in subjects with low back pain. A con-trolled study, Scand J Med Sci Sports, 6 (1996) 112-21.
Kuukkanen, T. and Mälkiä, E., Effects of a three-month therapeutic exercise programme on flexibility in subjects with low back pain, Physiother Res Int, 5 (2000) 46-61.
Lam, K.S., Carlin, D. and Mulholland, R.C., Lumbar disc high-intensity zone: the value and significance of provocative discography in the determination of the discogenic pain source, Eur Spine J, 9 (2000) 36-41.
Laslett, M. and Williams, M., The reliability of selected pain provocation tests for sacroiliac joint pathology, Spine, 19 (1994) 1243-9.
Leinonen, V., Kankaanpää, M., Hänninen, O., Airaksinen, O. and Taimela, S., Paraspinal muscle responses during sudden upper limb loading, Eur J Appl Physiol, 88 (2002a) 42-9.
Leinonen, V., Kankaanpää, M., Luukkonen, M., Hänninen, O., Airaksinen, O. and Taimela, S., Disc herniation-related back pain impairs feed-forward control of paraspinal muscles, Spine, 26 (2001) E367-72.
Leinonen, V., Kankaanpää, M., Luukkonen, M., Kansanen, M., Hänninen, O., Airaksinen, O. and Taimela, S., Lumbar paraspinal muscle function, perception of lumbar position, and postural control in disc herniation-related back pain, Spine, 28 (2003) 842-8.
Leinonen, V., Määtta, S., Taimela, S., Herno, A., Kankaanpää, M., Partanen, J., Kansanen, M., Hänninen, O. and Airaksinen, O., Impaired lumbar movement perception in as-sociation with postural stability and motor- and somatosensory-evoked potentials in lumbar spinal stenosis, Spine, 27 (2002b) 975-83.
Liang, M., Longitudinal construct validity: establishment of clinical meaning in patient evaluative instruments, Med Care, 38 (2000) II84-90.
85

Linton, S., Psychological risk factors for neck and back pain. In: A. Nachemson and E. Jons-son (Eds.), Neck and back pain: The scientific evidence of causes, diagnosis, and treatment. Lippincott Williams & Wil-kins, Philadelphia, 2000a, 57-78 pp.
Linton, S., Utility of cognitive-behavioral psychological treatments. In: A. Nachemson and E. Jonsson (Eds.), Neck and back pain: The scientific evidence of causes, diagnosis, and treatment, Lippincott Williams & Wilkins, Philadelphia, 2000b, pp. 361-81.
Linton, S.J. and van Tulder, M.W., Preventive interventions for back and neck pain prob-lems: what is the evidence?, Spine, 26 (2001) 778-87.
Long, A.L., The centralization phenomenon. Its usefulness as a predictor or outcome in con-servative treatment of chronic law back pain (a pilot study), Spine, 20 (1995) 2513-20; discussion 2521.
Lund, T., Biomechanical aspects of chronic low back pain: Kinematics and stabilization, Orton Orthopaedic Hospital, Invalid Foundation, University of Helsinki, Helsinki, 2003, pp. 7-71.
Lund, T., Nydegger, T., Schlenzka, D. and Oxland, T.R., Three-dimensional motion patterns during active bending in patients with chronic low back pain, Spine, 27 (2002a) 1865-74.
Lund, T., Oxland, T.R., Nydegger, T., Schlenzka, D., Laine, T. and Heini, P., Is there a con-nection between the clinical response after an external fixation test or a subsequent lumbar fusion and the pre-test intervertebral kinematics?, Spine, 27 (2002b) 2726-33.
Luoto, S., Aalto, H., Taimela, S., Hurri, H., Pyykkö, I. and Alaranta, H., One-footed and externally disturbed two-footed postural control in patients with chronic low back pain and healthy control subjects. A controlled study with follow-up, Spine, 23 (1998) 2081-9; discussion 2089-90.
Luoto, S., Taimela, S., Hurri, H., Aalto, H., Pyykkö, I. and Alaranta, H., Psychomotor speed and postural control in chronic low back pain patients A controlled follow-up study, Spine, 21 (1996) 2621-7.
Malmivaara, A., Hakkinen, U., Aro, T., Heinrichs, M.L., Koskenniemi, L., Kuosma, E., Lappi, S., Paloheimo, R., Servo, C., Vaaranen, V. and et al., The treatment of acute low back pain--bed rest, exercises, or ordinary activity?, N Engl J Med, 332 (1995) 351-5.
Mannion, A.F., Junge, A., Taimela, S., Muntener, M., Lorenzo, K. and Dvorak, J., Active therapy for chronic low back pain: part 3. Factors influencing self-rated disability and its change following therapy, Spine, 26 (2001) 920-9.
McArdle, W., Katch, F. and Katch, V., Exercise physiology, energy, nutrition and human performance, Williams & Wilkins, USA, 1996, 151-63 pp.
McCracken, L.M., Spertus, I.L., Janeck, A.S., Sinclair, D. and Wetzel, F.T., Behavioral di-mensions of adjustment in persons with chronic pain: pain-related anxiety and ac-ceptance, Pain, 80 (1999) 283-9.
Meade, T.W., Dyer, S., Browne, W. and Frank, A.O., Randomised comparison of chiroprac-tic and hospital outpatient management for low back pain: results from extended follow up, Bmj, 311 (1995) 349-51.
Meade, T.W., Dyer, S., Browne, W., Townsend, J. and Frank, A.O., Low back pain of me-chanical origin: randomised comparison of chiropractic and hospital outpatient treatment, Bmj, 300 (1990) 1431-7.
Mellin, G., Härkäpää, K. and Hurri, H., Asymmetry of lumbar lateral flexion and treatment outcome in chronic low-back pain patients, J Spinal Disord, 8 (1995) 15-9.
Mitchell, R.I. and Carmen, G.M., Results of a multicenter trial using an intensive active exercise program for the treatment of acute soft tissue and back injuries, Spine, 15 (1990) 514-21.
86

Moll, J.M., Liyanage, S.P. and Wright, V., An objective clinical method to measure lateral spinal flexion, Rheumatol Phys Med, 11 (1972) 225-39.
Moll, J.M. and Wright, V., Normal range of spinal mobility. An objective clinical study, Ann Rheum Dis, 30 (1971) 381-6.
Montoye, H., Kemper, H.C., Saris, W. and Washburn, R., Measuring physical activity and energy expenditure, USA, 1996.
Morley, S., Eccleston, C. and Williams, A., Systematic review and meta-analysis of random-ized controlled trials of cognitive behaviour therapy and behaviour therapy for chronic pain in adults, excluding headache, Pain, 80 (1999) 1-13.
Moseley, G.L., Nicholas, M.K. and Hodges, P.W., Pain differs from non-painful attention-demanding or stressful tasks in its effect on postural control patterns of trunk mus-cles, Exp Brain Res, 156 (2004) 64-71.
Mälkiä, E., MET based questionnaire for the study of physical activity, PainoPorras Oy, Jyväskylä, 1996, 98-103 pp.
Mälkiä, E. and Impivaara, O., Intensity of physical activity and respiratory function in sub-jects with and without bronchial asthma, Scand J Med Sci Sports, 8 (1998) 27-32.
Mälkiä, E., Impivaara, O., Heliövaara, M. and Maatela, J., The physical activity of healthy and chronically ill adults in Finland at work, at leisure and during commuting, Scand J Med Sci Sports, 4 (1994) 82-7.
Mälkiä, E., Impivaara, O., Maatela, J., Aromaa, A., Heliövaara, M. and Knekt, P., Physical activity of Finnish adults, Publications of Finnish Insurance Institution, Vol. ML:80, 1988, pp. 93-107.
Niemistö, L., Lahtinen-Suopanki, T., Rissanen, P., Lindgren, K.A., Sarna, S. and Hurri, H., A randomized trial of combined manipulation, stabilizing exercises, and physician consultation compared to physician consultation alone for chronic low back pain., Spine, 28 (2003) 2185-91.
Niemistö, L., Sarna, S., Lahtinen-Suopanki, T., Lindgren, K.A. and Hurri, H., Predictive factors for 1-year outcome of chronic low back pain following manipulation, stabi-lizing exercises, and physician consultation or physician consultation alone, J Reha-bil Med, 36 (2004) 104-9.
nQuery Advisor version 3.0. Statistical Solutions, Ireland, 1997. Nyiendo, J. and Lamm, L., Disabling low back Oregon workers' compensation claims. Part I:
Methodology and clinical categorization of chiropractic and medical cases, J Ma-nipulative Physiol Ther, 14 (1991) 177-84.
O'Sullivan, P.B., Phyty, G.D., Twomey, L.T. and Allison, G.T., Evaluation of specific stabi-lizing exercise in the treatment of chronic low back pain with radiologic diagnosis of spondylolysis or spondylolisthesis, Spine, 22 (1997) 2959-67.
Oxland, T.R. and Panjabi, M.M., The onset and progression of spinal injury: a demonstration of neutral zone sensitivity, J Biomech, 25 (1992) 1165-72.
Panjabi, M.M., The stabilizing system of the spine. Part I. Function, dysfunction, adaptation, and enhancement, J Spinal Disord, 5 (1992) 383-9; discussion 397.
Pearcy, M., Portek, I. and Shepherd, J., The effect of low-back pain on lumbar spinal move-ments measured by three-dimensional X-ray analysis, Spine, 10 (1985) 150-3.
Pfingsten, M., Hildebrandt, J., Leibing, E., Franz, C. and Saur, P., Effectiveness of a multi-modal treatment program for chronic low-back pain, Pain, 73 (1997) 77-85.
Pope, M.H. and Panjabi, M., Biomechanical definitions of spinal instability, Spine, 10 (1985) 255-6.
Richardson, C., Gwendolen, J., Hodges, P. and Hides, J., Therapeutic exercise for spinal segmental stabilization in low back pain. Scientific basis and clinical approach., Churchill Livingstone, London, 1999a.
87

Thomas, E., Silman, A.J., Croft, P.R., Papageorgiou, A.C., Jayson, M.I. and Macfarlane, G.J., Predicting who develops chronic low back pain in primary care: a prospective study, Bmj, 318 (1999) 1662-7.
Timm, K.E., A randomized-control study of active and passive treatments for chronic low back pain following L5 laminectomy, J Orthop Sports Phys Ther, 20 (1994) 276-86.
Triano, J.J., McGregor, M., Hondras, M.A. and Brennan, P.C., Manipulative therapy versus education programs in chronic low back pain, Spine, 20 (1995) 948-55.
Turk, D.C., Okifuji, A., Sinclair, J.D. and Starz, T.W., Differential responses by psychoso-cial subgroups of fibromyalgia syndrome patients to an interdisciplinary treatment, Arthritis Care Res, 11 (1998) 397-404.
Turk, D.C. and Rudy, T.E., The robustness of an empirically derived taxonomy of chronic pain patients, Pain, 43 (1990) 27-35.
Turner, J.A., Educational and behavioral interventions for back pain in primary care, Spine, 21 (1996) 2851-7; discussion 2858-9.
van den Hoogen, H.J., Koes, B.W., Deville, W., van Eijk, J.T. and Bouter, L.M., The prog-nosis of low back pain in general practice, Spine, 22 (1997) 1515-21.
van Tulder, M.W., Goossens, M.E., Waddell, G. and Nachemson, A., Conservative Treat-ment of Chronic Low Back Pain. In: A. Nachemson and E. Jonsson (Eds.), Neck and Back Pain: The Scientific Evidence of Causes, Diagnosis, and Treatment., Vol. 12, Lippincott Williams & Wilkins, Philadelphia, 2000b, pp. 271-304.
van Tulder, M.W., Koes, B.W. and Bouter, L.M., Conservative treatment of acute and chronic nonspecific low back pain. A systematic review of randomized controlled trials of the most common interventions, Spine, 22 (1997) 2128-56.
van Tulder, M.W, Malmivaara, A., Esmail, R. and Koes, B., Exercise therapy for low back pain: a systematic review within the framework of the cochrane collaboration back review group, Spine, 25 (2000a) 2784-96.
Vo, P. and MacMillan, M., The aging spine: clinical instability, South Med J, 87 (1994) S26-35.
Von Korff, M. and Saunders, K., The course of back pain in primary care, Spine, 21 (1996) 2833-7; discussion 2838-9.
Waagen, G.N., Haldeman, S., Cook, G. and al, e., Short term trial of chiropractic adjustments for the relief of chronic low-back pain, Manual Med, 2 (1986) 63-67.
Waddell, G., Diagnostic triage. In The Back Pain Revolution, Vol. 1st, Churchill Living-stone, London, 1998, 9-25 pp.
Waddell, G., Feder, G., McIntosh, A., Lewis, M. and Hutchinson, A., Clinical guidelines for the management of acute low back pain: clinical guidelines and evidence review, Royal College of General Practitioners, London, 1996.
Waddell, G. and Waddell, H., A review of social influences on neck and back pain and dis-ability, Lippincott Williams & Wilkins, Philadelphia, 2000, 13-55 pp.
Weiser, S. and Cedraschi, C., Psychosocial issues in the prevention of chronic low back pain-
-a literature review, Baillieres Clin Rheumatol, 6 (1992) 657-84. Weishaupt, D., Zanetti, M., Hodler, J., Min, K., Fuchs, B., Pfirrmann, C.W. and Boos, N.,
Painful Lumbar Disk Derangement: Relevance of Endplate Abnormalities at MR Imaging, Radiology, 218 (2001) 420-7.
Werneke, M. and Hart, D.L., Centralization phenomenon as a prognostic factor for chronic low back pain and disability, Spine, 26 (2001) 758-64; discussion 765.
Werneke, M., Hart, D.L. and Cook, D., A descriptive study of the centralization phenome-non. A prospective analysis, Spine, 24 (1999) 676-83.
Wernham, J. and Waldman, M., An illustrated manual of osteopathic technique, 1981.
89

WHO, ICIDH-2: International classification of functioning, disability, and health. Geneva, 2001
Wilder, D.G., Aleksiev, A.R., Magnusson, M.L., Pope, M.H., Spratt, K.F. and Goel, V.K., Muscular response to sudden load. A tool to evaluate fatigue and rehabilitation, Spine, 21 (1996) 2628-39.
World Medical Association Declaration of Helsinki: ethical principles for medical research involving human subjects., Jama, 284 (2000) 3043-5.
Yrjämä, M., Tervonen, O., Kurunlahti, M. and Vanharanta, H., Bony vibration stimulation test combined with magnetic resonance imaging. Can discography be replaced?, Spine, 22 (1997) 808-13.
90





























