Embed Size (px)
Citation preview
A Single-Blind Randomized Controlled Trial on the Effectiveness of Gingko biloba in Increasing Immediate Memory Index Scores of Healthy UERMMMCI Medical
Students Using the Repeatable Battery for the Assessment of Neuropsychological Status (RBANS)
Tsang, Kelvin C. Turalba, Frances Gail M.
Udani, Cheryll G. Udaundo, Ralph Jayson C. Unabia, Antonio Miguel C. Versoza, Angelica Feliz Y.
Villamil, Alejandro Daniel G. Vitan, Daniell Lynn P.
Yazon, Keith Stephen B.
Research Adviser : Dr. Ramon Jason Javier
INTRODUCTION
• Medical students are required to study a lot and retain as much information as they could.
• Memory is an important attribute for medical students and finding a means to improve their memory would be beneficial
• Ginkgo biloba is a common herbal medicine that is thought of to have an effect on memory enhancement.
• It was reported by The Journal of the American Botanical Council (2006), that Ginkgo biloba ranked 4th in the 2005 top-selling herbal dietary supplements in the United Sates, with around $16.5M in sales.
• It is one of the most widely prescribed herbal medications in France and Germany for the treatment of a wide range of conditions, one of which is memory impairment (Birks et al 2007).
• To validate the effect of Ginkgo biloba on memory, there have been researches and studies conducted to prove its efficacy. However, there are not many published research on Ginkgo biloba done in the Philippines.

REVIEW OF RELATED LITERATURE: Ginkgo biloba
• Uses have been indicated for asthma, cough, bronchitis, and incontinence. It is also used in clinical studies as treatment of poor circulation, impotence, heart disease, eye disease, tinnitus, chronic cerebral insufficiency, short-term memory loss, brain trauma, depression, dementia and conditions related to senility (Rouse, 1998).
• According to Rouse (1998), the therapeutic effects depend on synergism of its components rather than a single biologically active compound. These include the active constituent Ginkgolides which is said to interfere with platelet activating factor, and phytochemicals such as flavinoids, bioflavonoids, proanthocyanidins, trilactonic diterpenes and bilabolide (Hanrahan and Olde, 2005). Two important groups of active constituents have been identified: flavonoids (40 types) and terpenoids (Ginkgo lides A, B, C). The flavone glycosides act by scavenging free radicals, which are responsible for lipid peroxidation and cell destruction in Alzheimer’s disease, and inhibiting platelet aggregation.
REVIEW OF RELATED LITERATURE: Ginkgo biloba and Memory
• Mix (2002) used a 6-week duration of administration of 180mg in a randomized, double-blind, fixed-dose, placebo-controlled clinical trial, which reported a significant improvement on tasks involving delayed free recall and recognition of noncontextual, auditory-verbal material, compared with placebo. • Moulton (2001) and Warot (1991) experimented independently on 30 healthy males and females, respectively, and found nonsignificant results upon performing Wechsler Adult Intelligence Scale-Revised (WAIS-R) test but found significant results using Sternberg Scanning Test on memory. • Rigney (1999) did an investigation on what dosage would have a significant effect on memory and psychomotor performance. The results showed that for acute dosages in cognitive enhancement, 120mg was more pronounced than those given 240mg or placebo.
• Kennedy et. al (2007) studied the effect of 120mg single dose Ginkgo biloba extract on cognitive performace of healthy young volunteers and found that 120 mg of Ginkgo showed a significant improvement on the quality of memory • Elsabagh et al. (2005) studied the differential effects of Ginkgo biloba after acute and chronic treatment in 52 and 40 healthy young volunteers respectively. Their results showed that the acute (single) dose of Ginkgo significantly improved performance on the sustained-attention task and pattern recognition memory but there were no effects on working memory, planning and mental flexibility. On the other hand, the subjects who received chronic treatment with Ginkgo did not show any improvement on any of the cognitive tests.
REVIEW OF RELATED LITERATURE: Ginkgo biloba and Memory
• Persson et. al (2003) studied the memory enhancing effect of ginseng and Ginkgo on healthy test subjects and found no quantifiable beneficial effects on memory performance in the long term. • Solomon et al. (2002) conducted a 6-week, double-blind, placebo-controlled study on 230 healthy older adults. Their results showed that 120mg Ginkgo biloba did not provide any measurable benefits in memory and/or function to elderly adults with normal healthy cognitive function.
REVIEW OF RELATED LITERATURE: Ginkgo biloba and Memory
REVIEW OF RELATED LITERATURE: MEMORY TESTING
• In an unpublished article, Doctor et al. (2004) assessed the effects of caffeine consumption on the immediate memory index of medical students using Repeatable Battery for the Assessment of Neuropsychological Status (RBANS). The RBANS is a brief neurocognitive battery with four alternate forms, measuring immediate and delayed memory, attention, language, and visuospatial skills. It usually is used as a tool in clinical trials that assess the impact of medication in neurocognitive status.
• Selective Reminding Test (SRT), Weschler Adult Intelligence Scale III Block Design (WAIS-III BD) and Digit Symbol-Coding (WAIS-III DS) – used by Mix and Crews (2002).
• Rigney et al (1999) – used Short-term Memory Test (STM), Immediate and
Delayed Recall of Supraspan Word Lists, and Critical Flicker Fusion test (CFF). • Subhan and Hindmarch (1984), Warot et al (1991) – Choice Reaction Time (CRT),
Subjective Ratings of Drug Effect (LARS), and Sternberg Memory Scanning Test.
OBJECTIVES OF THE STUDY A. General:
• To determine whether intake of Ginkgo biloba causes a significant increase in memory as compared to placebo among UERMMMC First Year and Second Year Medical Students of school year 2009-2010 after six (6) weeks of administration of Ginkgo biloba.
A. Specific:
• To evaluate if there was an increase in Index Scores of immediate and delayed memory as tested using the Repeatable Battery for the Assessment of Neuropsychological Status.
• To test if 240 mg of Ginkgo biloba taken everyday for six (6) weeks significantly increased Index Scores of immediate and delayed memory
HYPOTHESIS A. Null Hypothesis:
• There is no significant improvement in Index scores of immediate and delayed memory between the Placebo group and Ginkgo biloba group after 6 weeks intake of 240 mg Ginkgo biloba, as tested using the RBANS.
B. Alternate Hypothesis: • Ginkgo biloba causes a significant increase in index scores of
immediate and delayed memory between the Placebo group and Ginkgo biloba group after 6 weeks intake of 240 mg Ginkgo biloba, as tested using the RBANS.
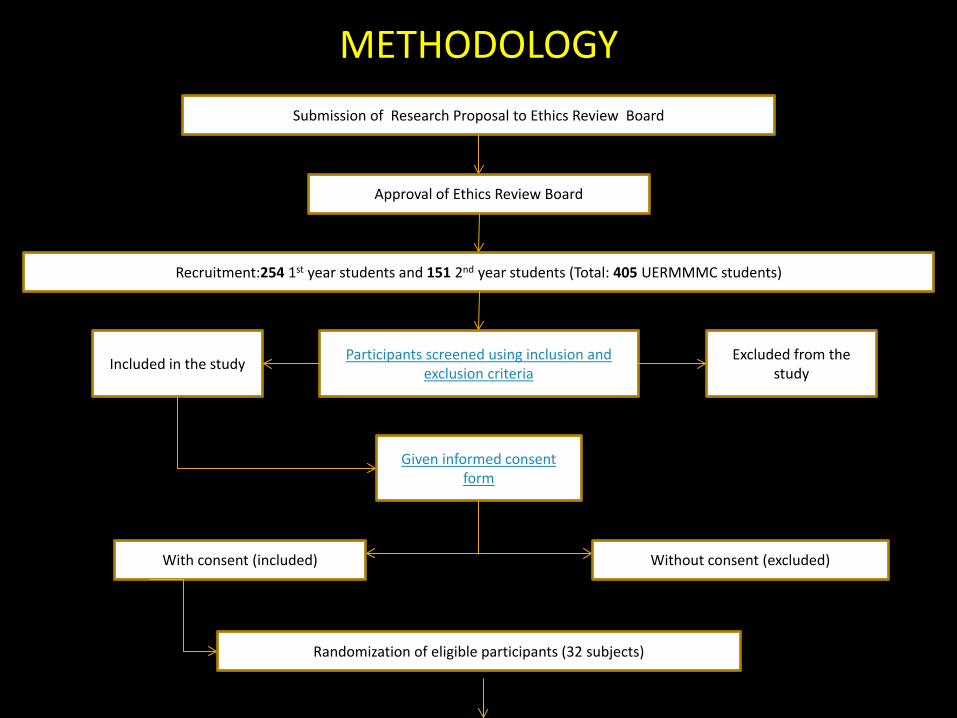
METHODOLOGY Submission of Research Proposal to Ethics Review Board
Approval of Ethics Review Board
Recruitment:254 1st year students and 151 2nd year students (Total: 405 UERMMMC students)
Participants screened using inclusion and exclusion criteria Included in the study Excluded from the
study
Given informed consent form
With consent (included) Without consent (excluded)
Randomization of eligible participants (32 subjects)

Randomization of eligible participants (32 subjects)
Placebo group (16 subjects)
Ginkgo biloba group (16 subjects)
Administered RBANS Pre-test Administered RBANS Pre-test
Given Placebo (two capsules OD) Given Ginkgo biloba (120 mg two capsules OD)
Administered RBANS Post-test Administered RBANS Post-test
Statistical Analysis of Scores* Statistical Analysis of Scores*
Analysis of Outcome Analysis of Outcome
*t-test dependent, Wilcoxon Signed Rank test, Mann-Whitney U test
RBANS scored by certified psychologist RBANS scored by certified psychologist
Methodology continuation…
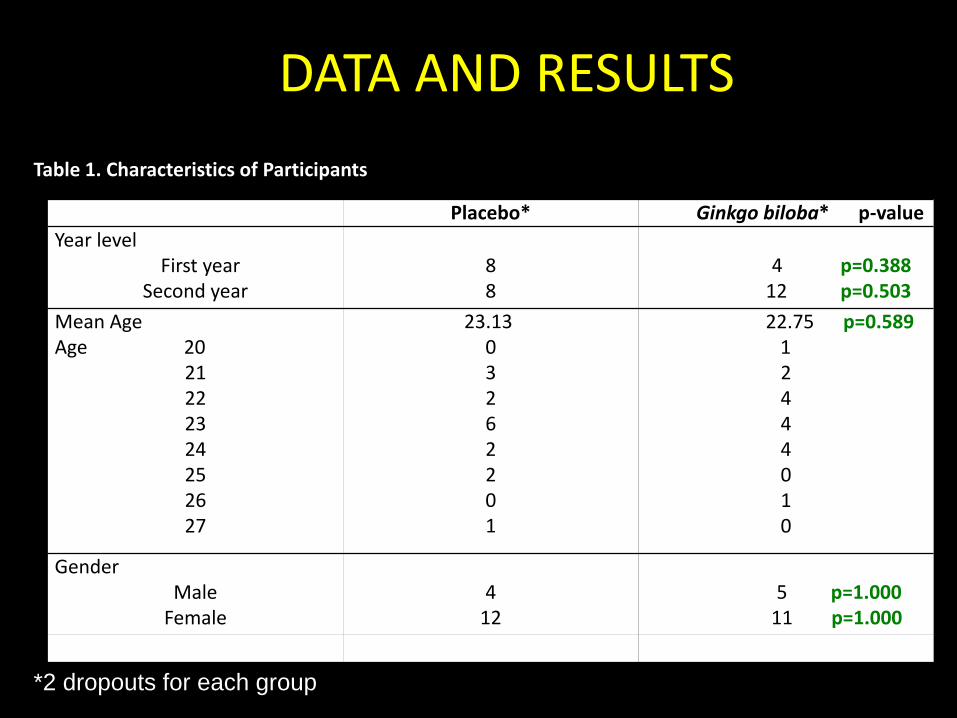
DATA AND RESULTS Table 1. Characteristics of Participants
*2 dropouts for each group
Placebo* Ginkgo biloba* p-value Year level First year
Second year
8 8
4 p=0.388
12 p=0.503 Mean Age Age 20
21 22 23 24 25 26 27
23.13 0 3 2 6 2 2 0 1
22.75 p=0.589 1
2 4 4 4 0 1 0
Gender Male
Female
4
12
5 p=1.000 11 p=1.000

RESULTS Table 2. Summary of Results Showing Mean Index Scores, Standard Deviation, Mean Change and p-Value for Placebo Group and Ginkgo biloba Group. TYPE OF MEMORY PLACEBO GINKGO
IMMEDIATE
Pretest (mean scores) 92.07 ± 12.68 88.93 ± 9.68
Post test (mean scores) 92.21 ± 12.58 91.14 ± 15.86
Mean change 0.14 ± 11.66 2.21 ± 17.12
p-value p = 0.964 p = 0.637
DELAYED
Pretest (mean scores) 108.36 ± 9.51 99.57 ± 7.08
Posttest (mean scores) 102.14 ± 11.99 102.29 ± 10.96
Mean change -6.21 ± 13.87 2.71 ± 12.71
p-value p = 0.118 p = 0.139
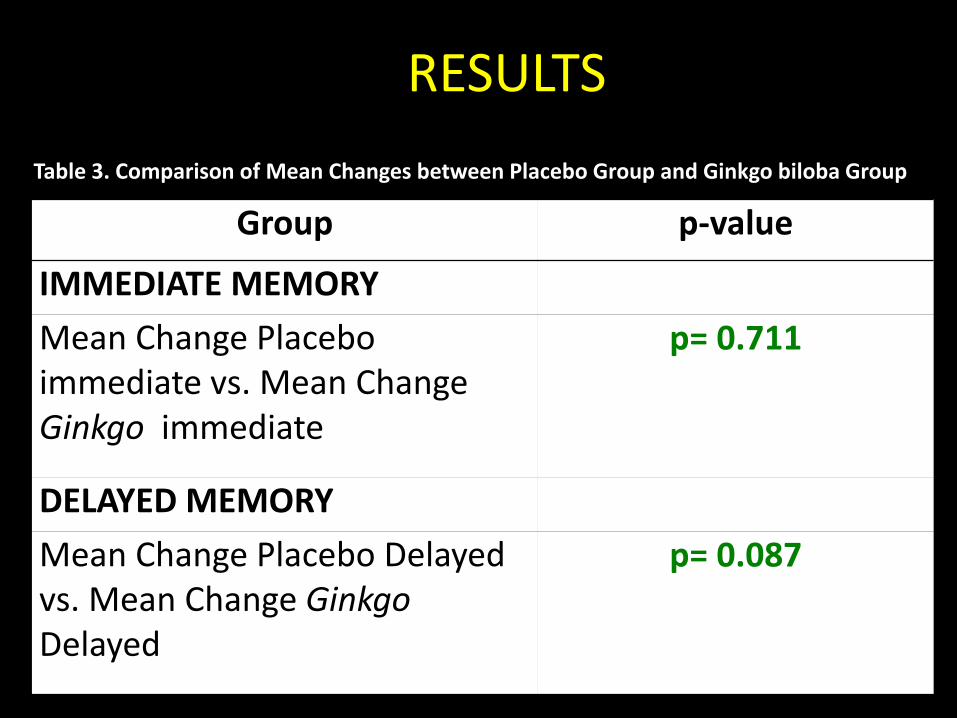
RESULTS Table 3. Comparison of Mean Changes between Placebo Group and Ginkgo biloba Group
Group p-value IMMEDIATE MEMORY Mean Change Placebo immediate vs. Mean Change Ginkgo immediate
p= 0.711
DELAYED MEMORY Mean Change Placebo Delayed vs. Mean Change Ginkgo Delayed
p= 0.087
DISCUSSION • Results showed that the mean change of index scores in both the placebo group and Ginkgo biloba group did not show an increase in the immediate and delayed memory. Also, when results from the Ginkgo group were compared with the placebo group, no statistically significant change was noted. Therefore, the researchers accepted the null hypothesis that there was no significant change in index scores between Ginkgo and placebo. • These findings coincided with the results obtained by Perrson et al. (2003) and Solomon et al. (2002). These results may be attributed to several external factors, as well as the pharmacokinetics of Ginkgo biloba, that may have had an influence on the participants’ immediate and delayed memory.
DISCUSSION • All of the participants in both the placebo group and Ginkgo biloba group were tested using the RBANS for the first time. Encountering the RBANS for the first time may have caused some degree of anxiety or stress in them. This stress may have affected their performance in answering the RBANS. • Memory impairment can result from stress (Deffenbacher et al., 2004; Morgan et al., 2004). Stressful events are those that not only elicit arousal (leading to the release of norepinephrine in the basolateral amygdala), but also activate the hypothalamus pituitary adrenal axis, leading to the release of glucocorticoid stress hormones. Norepinephrine release has been shown to enhance memory (McGaugh, 2004), but over an extended period of time, glucocorticoids can damage brain structures, including the hippocampus, necessary for encoding coherent episodic memories with contextual details (Belanoff, et al. 2001; McEwen and Sapolsky, 1995).
• Studies indicate that both long and short term stress have significant effects on learning and memory (Vedhara, 2000). Chronic stress was shown to result in impairment of various mental functions including memory. On the other hand, acutely experienced stress is associated with concurrent improvement of short term memory. These factors were not considered in the study and may have influenced the final outcome of the study especially since the participants took the post test when school started which may have added to their stress. • The participants may have been subjected to different levels of stress during the pretest and post test, thus affecting their performance. Participants who had other things to do and were pressed for time may have finished the pretest or post test hurriedly which subsequently may have also affected their index scores.
DISCUSSION
DISCUSSION • uniformity of the participants’ emotional state or mood during the pretest as compared to the post test was not constant and this could have influenced the manner in which they answered or accomplished the subtests of the RBANS. Subsequently, this may have affected their final index scores.
• Levine and Edelstein (2009) reported that emotion sometimes impairs memory. The intensity of emotional arousal may account for the varying effects of emotion on memory. Emotion can improve memory when there is low to moderate levels of arousal. However, as the intensity of arousal increases, the range of stimuli to which an organism can attend may decrease resulting in poor memory for peripheral information. The negative effect of emotion on memory for peripheral details can be attributed, at least in part, to neglect. If attention is directed toward emotional stimuli, information that is not emotional does not receive as much attention and is less likely to be encoded (Compton, 2003; O¨ hman, Flykt, and Esteves, 2001).
DISCUSSION • Activities of the participants during the pretest and 6-week intake period may also be a factor. Since this study was started during the summer vacation, there was not much intellectual stimulation and stressors as compared to the regular academic year of medical students. • Moreover, not all participants had the same level of intellectual stimulation over the summer. Medical students may possibly be in more stress than other people, affecting their performance negatively; however, they may also be engaged in a greater amount of intellectual stimulation which may work to improve their memory (Nelson, 2005). • Despite having the same academic work load, each would have reacted differently to stress and each may have been affected in their performance to a different degree (Melin, 1999). • These factors were no longer taken into account during the selection process, and each could have contributed to the confounding of the data and affected the outcome of the study.
DISCUSSION • five administrators were assigned a number of participants. This may have introduced bias from the way the tests were administered. There may have been differences in the timing between words, speaking volume, and accentuation. Human error and the exactness of administration in each participant may have altered the results. • difference in venue or location where the pretest and post test were administered. Participants may have been easily distracted by the environment and noisy surroundings which in turn may have affected their performance in the RBANS. High levels of unavoidable background noise are a major stressor. A number of studies have shown that proximity to noisy airports and busy roads have a measurable negative impact on childrens' ability to concentrate, read and learn (Stansfield, 2005). •
DISCUSSION •Pharmocokinetics of Ginkgo biloba may also have played a role in the results obtained.
•In a study by Drago et al. (2002), results showed that a dosage of 40 mg BID q12h is accompanied by a significantly longer half-life (t ½ ) and mean residence time (MRT) than a single 80 mg dose OD. The maximum concentration time (Tmax) is 2.3 hrs after administration in both treatments. In this study, 2 capsules of 120mg Ginkgo biloba extract were administered once daily.
• If the dosing schedule was changed to 120mg capsule twice a day, it may have caused a prolonged half-life of the herbal drug which can allow the drug to work longer inside the body.
•As a consequence of the once a day dose schedule, the active component flavone glycosides which act by scavenging free radicals (Rouse, 1998) may have had a shorter time in the circulation, thus producing less positive effects on memory.
CONCLUSION •Results of this study showed that the mean change of index scores for immediate and delayed memory from both placebo group and Ginkgo biloba group were all not significant.
• This may be attributed to the presence of stress, emotional state, and inadequate intellectual stimulation. Pharmacokinetic properties, specifically the half-life and mean residence time (MRT), of Ginkgo biloba may also have influenced the results.
• 240 mg of Ginkgo biloba appears to be an inadequate dose and 6 weeks is an insufficient period of intake to produce significant increase in index scores of immediate and delayed memory in both placebo and Ginkgo biloba groups.
SCOPE and LIMITATIONS
1. limited to the assessment of the effect of Ginkgo biloba on the immediate and delayed memory of 32 healthy UERMMMC freshmen and sophomore medical students of school year 2009-2010.
2. employed a single-blind, randomized controlled trial with only two groups, Placebo group and Ginkgo biloba group.
3. Only one testing tool, RBANS, was utilized to evaluate the selected participant’s memory before and after treatment with Ginkgo and placebo capsules.
4. RBANS pre-test was done during April 2009 (summer vacation) and post-test was done in June 2009 (first week of classes).
5. In the RBANS, only the participants’ scores for the following subtests
were analyzed in this study: List Learning and Story Memory for immediate memory, and List Recall, List Recognition, Story Recall and Figure Recall (based on Figure Copy) for delayed memory.
6. The effects of Ginkgo biloba on other types of memory or
psychological parameters (i.e. cognitive function, IQ, emotions, etc.) were not measured in this study.
7. This study also did not elucidate the influence of Ginkgo on academic
performance, as well as its other therapeutic effects (i.e. for stroke, bronchitis, asthma, memory problems or memory loss).
8. Any adverse reaction that occurred during treatment with Ginkgo
biloba were noted in this experiment, but the relationship between the drug and the side effects were not examined.
SCOPE and LIMITATIONS
9. The researchers did not establish any memory enhancement or changes caused by Ginkgo biloba at different dosages. 10. Moreover, the optimal dosage of Ginkgo biloba that will improve immediate or delayed memory was not investigated. 11. Participants’ compliance was monitored and ensured through a monitoring card that was provided for each participant to record their intake. They were also reminded via text messaging everyday to take their capsules. 12. Effects of the test drug on memory after administration of the post test were not verified.
SCOPE and LIMITATIONS
1. increase the sample size to have more conclusive results. A more diverse target population may also be used, consisting of other of age groups and/or educational levels.
2. Other types of memory, aside from immediate and delayed memory, could also be tested.
3. Administering the drug at different dosages may also be employed to determine the effective dose of Ginkgo biloba that will improve memory.
4. It is also advised to use ready-made or manufactured placebos similar to the Ginkgo capsules to guarantee quality and uniformity. A capsule-making machine or hand capsule filler may also be an alternative.
RECOMMENDATIONS

RECOMMENDATIONS 5. In conducting the RBANS, it is recommended to have only
one test administrator to limit observer bias. Having a certified psychologist perform all the tests is the best option.
6. It is also recommended to include other subtests of the RBANS such as figure copy and line orientation for visuospatial/constructional memory, picture naming and semantic fluency for language, and digit span and coding for attention. Another testing tool to assess memory, such as Sternberg Scanning test, may also be used.
7. Steps in limiting external factors that affect the study results (i.e. stress, emotional state, intellectual stimulation, compliance) should be incorporated or considered in the experimental design to improve the validity of data.
RECOMMENDATIONS 8. Pre- and post-testing must be done in a secluded and
quiet room with only the participant and examiner present.
9. The entire experiment must be done during the school year to provide regular intellectual stimulation and to better assess the effect of the test drug on the students’ memory.
10. It is also recommended that the researchers administer the capsules to the participants during schooldays for better compliance.
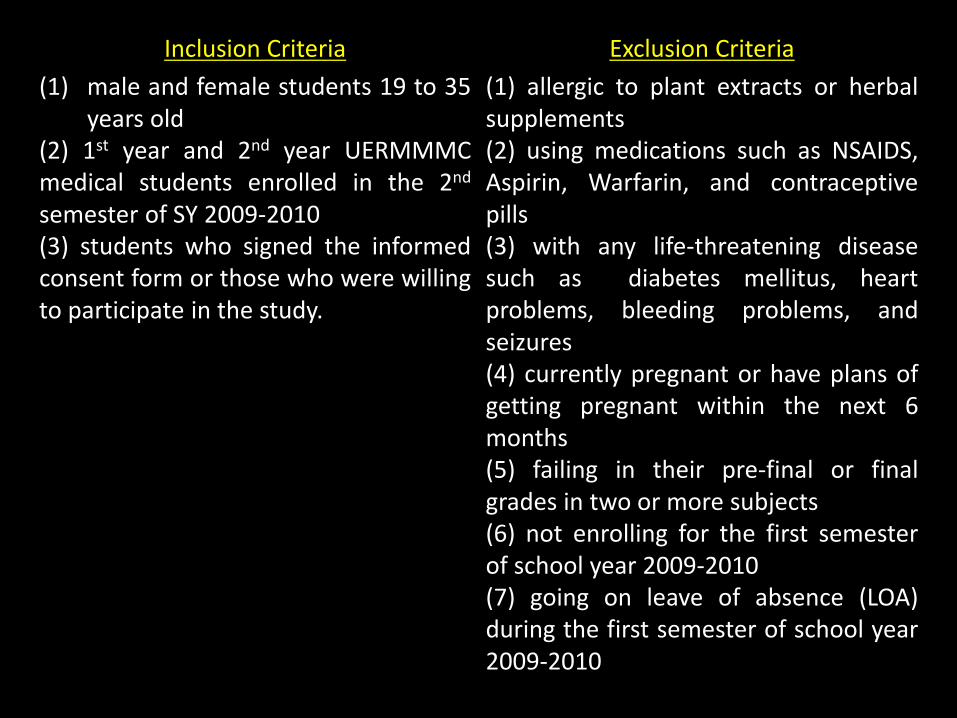
Inclusion Criteria Exclusion Criteria (1) male and female students 19 to 35
years old (2) 1st year and 2nd year UERMMMC medical students enrolled in the 2nd semester of SY 2009-2010 (3) students who signed the informed consent form or those who were willing to participate in the study.
(1) allergic to plant extracts or herbal supplements (2) using medications such as NSAIDS, Aspirin, Warfarin, and contraceptive pills (3) with any life-threatening disease such as diabetes mellitus, heart problems, bleeding problems, and seizures (4) currently pregnant or have plans of getting pregnant within the next 6 months (5) failing in their pre-final or final grades in two or more subjects (6) not enrolling for the first semester of school year 2009-2010 (7) going on leave of absence (LOA) during the first semester of school year 2009-2010

Ginkgo biloba capsules

PLACEBO capsules
RBANS Record Form A
RBANS Record Form B
Immediate Memory List learning Story memory Delayed Memory List recall List recognition Story recall Figure recall (based on figure copy)