Embed Size (px)
DESCRIPTION
A quantitative comparative study measuring consumer satisfaction based on health record format by Moore, Vivianne E., D.M.
Citation preview

A QUANTITATIVE COMPARATIVE STUDY MEASURING CONSUMER
SATISFACTION BASED ON HEALTH RECORD FORMAT
by
Vivianne E. Moore
A Dissertation Presented in Partial Fulfillment
of the Requirements for the Degree
Doctor of Management in Organizational Leadership
UNIVERSITY OF PHOENIX
February 2013
All rights reserved
INFORMATION TO ALL USERSThe quality of this reproduction is dependent upon the quality of the copy submitted.
In the unlikely event that the author did not send a complete manuscriptand there are missing pages, these will be noted. Also, if material had to be removed,
a note will indicate the deletion.
Microform Edition © ProQuest LLC.All rights reserved. This work is protected against
unauthorized copying under Title 17, United States Code
ProQuest LLC.789 East Eisenhower Parkway
P.O. Box 1346Ann Arbor, MI 48106 - 1346
UMI 3576426
Published by ProQuest LLC (2013). Copyright in the Dissertation held by the Author.
UMI Number: 3576426

ii
© 2013 by VIVIANNE E. MOORE
ALL RIGHTS RESERVED

iv
Abstract
This research study used a quantitative comparative method to investigate the relationship
between consumer satisfaction and communication based on the format of health record. The
central problem investigated in this research study related to the format of health record used and
consumer satisfaction with care provided and effect on communication with provider. The
purpose of this current research was to ascertain if statistically significant differences existed
between the format of health records (electronic versus paper) and the level of consumer
satisfaction with care provided and communication with provider. The results of this research
study found no support for the ideas that consumer satisfaction and consumer communication
with their doctor were related to the format of the health record. Based on the results, further
investigation is suggested to specify how the implementation of electronic health records may
affect consumer satisfaction with health care provided and how this may affect communication
with health care provider.

v
Dedication
I dedicate the end result of all this work to my father; for without his love and support, I
would not have felt the need to pursue this dream. Hugo Colon Murillo Sr. will never know what
I have accomplished; but in my heart, I know that he would be proud. Dad, I love you, and this is
for you.
The motivation to complete this work came from my grandmother Rosa Digna Mera. My
grandmother was an extraordinary woman who accomplished so many things in life without the
benefit of a formal education. She inspires me to continue to grow and learn. In her loving
memory, I also dedicate the end of this journey to my Abuela Rosa.
vi
Acknowledgements
In appreciation for their support and input, I would like to acknowledge my committee
team. Thank you Janice Emanuel Bunn, Ph. D., my mentor and Committee Chair. Thank you
Hoda Bagdady-Asal, Ph. D. and Charles Von Urff, Ph. D.— my committee members. I would
also like to thank Tom Granoff, Ph.D. who patiently listened and provided insight on how to
move along this process.
My heartfelt thanks to the members and facility management from the Hunterdon County
Senior Center for allowing me the time and venue to distribute my survey. I am grateful to all the
volunteers who not only took the time to participate in the survey, but shared stories on their
various experiences with heath care professionals. A special thanks to Mary Ann Rodenberger,
Division Head; and Richard Chrysafis, Director of Senior Center Activities for supporting my
study and allowing me access to the members of the Hunterdon County Senior Center.
I extend my deepest gratitude to my family and friends for their love and support as I
traveled through this journey. There are so many people who have helped me; and to all, I say
“Thank you.” To my children, Jesse and Vivyana Moore, I thank them for giving me their love,
support, and patience as they had to share me as their mom, a working parent, and as a student.
Thank you, Jesse, for all the many hours that you gave me as my sounding board in
understanding the philosophical concepts and helping me to see the world differently. Thank
you, Yana, for being my biggest fan and bringing humor to sometimes highly stressful moments.
I love you both. Lastly to Dr. Robby Fuentes, you are the star that I followed in this journey. I
will forever be grateful.
vii
Table of Contents
Chapter 1: Introduction ................................................................................................................... 1
Background of the Problem ............................................................................................................ 2
Statement of the Problem ................................................................................................................ 5
Purpose of the Study ....................................................................................................................... 6
Significance of the Study ................................................................................................................ 8
Significance of the Study to Leadership ......................................................................................... 8
Nature of the Study ......................................................................................................................... 9
Research Questions and Hypotheses ............................................................................................ 10
Theoretical Framework ................................................................................................................. 12
Definition of Terms....................................................................................................................... 15
Assumptions .................................................................................................................................. 15
Scope, Limitations, and Delimitations .......................................................................................... 16
Chapter Summary ......................................................................................................................... 17
Chapter 2: Review of the Literature .............................................................................................. 20
Documentation .............................................................................................................................. 21
Electronic Health Record Historical Perspective .......................................................................... 22
EHRs and Communication ........................................................................................................... 27
Implementation Issues .................................................................................................................. 32
Leadership Implications ................................................................................................................ 35
Consumer Satisfaction .................................................................................................................. 36
Relationship to the Current Study ................................................................................................. 38
Originality of Current Study ......................................................................................................... 40
Synthesis ....................................................................................................................................... 45
Chapter Conclusion ....................................................................................................................... 45
Summary ....................................................................................................................................... 47
Chapter 3: Research Method ......................................................................................................... 49
Research Questions ....................................................................................................................... 49
Research Method and Design Appropriateness ............................................................................ 51
viii
Research Design............................................................................................................................ 52
Sample Population ........................................................................................................................ 53
Sampling Frame ............................................................................................................................ 55
Informed Consent.......................................................................................................................... 56
Confidentiality .............................................................................................................................. 58
Geographic Location ..................................................................................................................... 58
Data Collection ............................................................................................................................. 58
Study Pilot Testing ........................................................................................................................ 61
Validity and Reliability ................................................................................................................. 62
Data Analysis ................................................................................................................................ 63
Chapter Conclusion ....................................................................................................................... 66
Summary ....................................................................................................................................... 67
Chapter 4: Results ......................................................................................................................... 68
Demographics ............................................................................................................................... 68
Data Collection ............................................................................................................................. 68
Recruitment ................................................................................................................................... 69
Planning and Procedure ................................................................................................................ 70
Data Analysis Procedures ............................................................................................................. 71
Presentation of Findings ............................................................................................................... 72
Summary ....................................................................................................................................... 80
Conclusions ................................................................................................................................... 80
Chapter 5: Conclusions and Recommendations ........................................................................... 82
Limitations .................................................................................................................................... 82
Sample........................................................................................................................................... 83
Assumptions .................................................................................................................................. 83
Findings......................................................................................................................................... 84
Conclusions ................................................................................................................................... 86
Recommendations ......................................................................................................................... 87
Implications and Significance to Leadership ................................................................................ 89
Researcher Reflections.................................................................................................................. 90
Summary ....................................................................................................................................... 91
ix
References ..................................................................................................................................... 92
Appendix A: Informed Consent Form ........................................................................................ 102
Appendix B: PSQ-08, Electronic Health Records Survey .......................................................... 106
Appendix C: Permission to Use Existing Survey ....................................................................... 110
Appendix D: Permission to Use Premises, Hunterdon County Senior Center ........................... 112
Appendix E: Permission to Use Premises, North Hunterdon Senior Center…………...………124

x
List of Tables
Table 1 Variables .......................................................................................................................... 59
Table 2 Proposed Data Analysis Plan .......................................................................................... 65
Table 3 Psychometric Characteristics for Summated Scale Scores ............................................. 72
Table 4 Frequency Counts for Selected Variables ....................................................................... 73
Table 5 Comparison Satisfaction Ratings..................................................................................... 75
Table 6 Comparison Communication Ratings .............................................................................. 76
Table 7 Correlations for Selected Demographic Variables for Satisfaction Scales ..................... 77
Table 8 Analysis of Covariance Model Predicting Consumer Satisfaction Based on Demographic
Characteristics and Health Record Format ................................................................................ 78
Table 9 Correlations for Selected Demographic Variables for Communication Scales .............. 79
Table 10 Analysis of Covariance Model Predicting Communication Based on Demographic
Characteristics and Health Record Format ................................................................................. 80
1
Chapter 1: Introduction
Consumer input is an important consideration in the health care industry as it affects
decision-making, policy, implementation, and possibly improvements in systems and
communication. Consumers can provide information regarding “waiting time, travel time,
communication with providers, and technical care received” (Andersen, Rice, & Kominiski,
2007, p. 29). A study to determine the consumers’ views provides valuable information
regarding the effectiveness of governmental services and policies, quality of health care, and
consumer satisfaction with the care or information provided.
Consumers and patients take on the same role in the use of health care services and
access to medical information through the available communication channels. A quantitative
study using the comparative design provided data to quantify consumer satisfaction with quality
of care and communication effectiveness when either an electronic or paper copy of health
records is used in the interaction between the health care provider and consumer. The Patient
Satisfaction Questionnaire-08 (PSQ-08) Electronic Health Records (EHR) Survey was the
instrument used to collect data to measure consumers’ satisfaction and how the health record
format used affected the health care provider-consumer dynamic. The format of health records
either in electronic or paper format may affect the consumers’ satisfaction with the care or
information provided by the health care professional. The health care provider-consumer
dynamic relates to communication.
The study objective was to gather consumers’ views on how the implementation of EHRs
can affect communication through the measurement of consumer satisfaction. Communication is
important, as this relates to consumers’ satisfaction with the care provided by the health care
professional. Some studies have shown there are issues with communication when a computer is
2
put in the visiting room, whereas others have shown no change between EHR and paper copy use
affecting the health care provider-consumer dynamic (Bensing, Verheul, & van Dulmen, 2008;
Del Piccolo, Mazzi, Scardoni, Gobbi, & Zimmerman, 2008; Earnest, Ross, Wittevrongel, Moore,
& Lin, 2004; Elleuch, 2008; Fisher, Bhaynani, & Winfield, 2009; Lanseng & Andreassen, 2007).
The goal of this study through a survey instrument was to describe an association
between the format of health records (e.g., electronic versus paper) and consumer satisfaction.
The results of this study provided information for communication improvements on the use of
medical health records. The results of this study could also contribute to the literature on the
implementation of health records on a national level and to the comparative effectiveness
research (CER) to improve the delivery of care.
The background information on the implementation of EHR systems, and the role of the
consumer and health care leadership present the foundation for this quantitative comparative
study. Consumer satisfaction and communication between health care provider and the consumer
address the concerns with EHRs, how the current study will aid in understanding the consumer
views on EHR use, and how the study could contribute to improved communication channels are
the main discussion topics in this chapter. Chapter 1 concludes with the research questions and
hypotheses, the theoretical framework, and summaries of the benefit in understanding the
consumer view to promote better communication among health care professionals, governmental
agencies, and the consumer.
Background of the Problem
Tang and Lansky (2005) noted a consumer should have the opportunity to bridge the
information gap on the use of EHRs and understand how the government’s mandate to have
electronic health records by 2014 will affect communication between health care provider and
3
consumer. Health care providers, consumers, and the government will use various types of
communication channels to bridge the information gap. Some channels of communication for the
consumer are face-to-face meetings with health care professionals, government agencies, and
access through the Internet or web portals.
Andersen et al. (2007) noted that the integration of various governmental systems has
been in place for over 30 years. These systems include community integration, comprehensive
services, and continuum of care. Many problems arise when services and systems are not
managed properly that could delay or postpone many projects. The proposed government system
integration between health care systems produced problems as they relate to system adoption,
cost, compliance, and how changes in health record format can affect the consumers’ satisfaction
with health care.
Governmental agencies, service providers, insurance companies, and vendors use the
Internet as a medium to provide information. The implementation of EHR systems will raise
many concerns for consumers as this information is available with the assumption that the
information is secure. Various agencies, such as the World Health Organization; and professional
organizations, such as American Health Information Management Association and the American
Medical Informatics Association, provided suggestions and leadership regarding the protection
of and access to medical health records (Maheu, Whitten, & Allen, 2001).
The Internet can be a communication vehicle for many consumers. The implementation
of an EHR system combined with the legislative and commercial support for e-health provides
consumers the option to view their medical information online or in person through their
personal health care provider. The ease of use from the Internet provides significant changes in
how consumers become informed and provides self-care options as well as changes the patient-
4
health care provider dynamic (Maheu et al., 2001). Another change is how proactive consumers
can be in managing their personal health care. The Internet option allows health care to become
more efficient with providing access to electronic health records as well as products and
information that would not be available through any other communication medium.
The Institute of Medicine (IOM) sets goals for the improvement of health care to include
“safe, effective, patient-centered, timely, efficient, and equitable health care” (Tang & Lansky,
2005, p. 1290). Tang and Lansky noted consumers have minimal access to information and
knowledge that can be beneficial in managing their own health care. The IOM aims to ensure
consumers have access to shared knowledge and free information flow through their providers.
Various other health agencies as part of the American Recovery and Reinvestment Act (ARRA)
of 2009 also have a stake in the implementation of the EHR systems, specifically the CER
charged with providing research for improving the quality of health care (Sox, 2010).
The American Recovery and Reinvestment Act of 2009 allocated $1.1 billion for CER.
The Institute of Medicine (IOM) defined CER as the generation and synthesis of
evidence that compares the benefits and harms of alternative methods to prevent,
diagnose, treat, and monitor a clinical condition or to improve the delivery of care. The
purpose of CER is to assist consumers, clinicians, purchasers, and policymakers to make
informed decisions that will improve health care at both the individual and population
levels (Sox, 2010, p. 469).
The effects on the health care provider-consumer dynamic are not understood as the
implementation of EHRs is not complete. Health records in both electronic and paper copy are in
use at various health care facilities. This comparative study gathered data to quantify consumer
satisfaction with quality of care and communication effectiveness when either an electronic or

5
paper copy of health records is part of the interaction between the health care provider and
consumer. The results of this study may help foster appropriate communication improvements to
the consumer and provide data to the CER initiative to improve health care.
Statement of the Problem
Morris (2009) cited the ARRA of 2009 may accelerate the implementation of electronic
health record systems and “starting in 2011, physicians who can demonstrate meaningful use of
interoperable systems may receive extra Medicare payments over 5 years” (p. 1). The federal
government has set the goal for most Americans to have electronic health records by 2014; but
according to the National Health Statistics Reports, there were only 19.6% electronic medical
records (EMR) system implementations in 2007. Hing and Hsiao (2010) noted the expectation is
only 64.5% EMR system implementations by 2010. Hsiao et al. (2010) added as of 2008 only
41.5% of physicians report using all or partial EHR systems.
In addition to the EHR implementation government mandate, Medicare and Medicaid
legislation provides a 2% incentive for physicians to implement e-prescribing by 2009 while
instituting a 2% penalty for those who do not by 2012 (Health Information Technology for
Economic and Clinical Health (HITECH) Act of 2009). The cost to accelerate the
implementation of EHR systems may also delay the adoption of these systems so that paper copy
of health records use is still present. Adoption has been slow because of reluctance from the
medical community in computer hardware and software investments, the lack of computer
knowledge, and the lack of interoperability between systems (Berner, Detmer, & Simborg,
2005). There are also issues with data security, confidentiality, and consumer privacy.
The implementation of EHR systems will affect consumers and is a government mandate
to have electronic health records for all consumers by 2014 (Morris, 2009). The general problem
6
is that the proposed government system integration between health care systems may produce
resistance to EHR adoption by the medical community and consumers. The specific problem
explored in this study is whether there is a difference in the level of customer satisfaction with
communication and health care received from providers based on the use of electronic versus
paper health records. This quantitative comparative study collected data to measure if there is
any statistical difference with consumer satisfaction when using paper versus electronic copy of
health records. The result of this study could be used in improvements in communication
between the health care provider and consumer. These improvements could enhance the health
care provider-consumer dynamic.
This quantitative comparative study using a cross-sectional survey allowed a direct
comparison between the format of health records and how this may affect communication and
consumer satisfaction. The cross-sectional survey provided the ability to collect data at a given
point and provide feedback that may be beneficial in implementing a better program (Creswell,
2007). Volunteers from local senior citizen centers from Hunterdon County in New Jersey
provided their views on the use of EHRs through a cross-sectional survey. The recruitment of
senior citizen volunteers was from local senior citizen centers.
The study used a modified version of the Rand Corporation PSQ-18 to measure consumer
satisfaction. Volunteers did not provide any identifying information. The sample population was
a convenience sample. The volunteers provided diverse views based on gender, age, education,
and race.
Purpose of the Study
The purpose of this quantitative comparative research study was to ascertain if
statistically significant differences exist between the format of health records (electronic versus
7
paper) and the level of consumer satisfaction with care provided and communication with
provider. This study will contribute to the literature in support of the national implementation of
electronic health records. The study used a modified version of the Rand Corporation PSQ-18 to
measure consumer satisfaction. The survey instrument is the PSQ-08.
Black (1999) noted studies that compared two populations to see if there are similarities
between the populations or if they belong to a different population “based on the trait in
question” (p. 403). This quantitative comparative study measured consumer satisfaction on
communication between health care providers when using paper compared to electronic copies
of health records using a cross-sectional survey. The PSQ-08 was the instrument to collect data
in measuring consumer satisfaction relating to the EHR implementation. Volunteers from local
senior citizen centers from Hunterdon County, New Jersey, participated in the study to measure
satisfaction through a cross-sectional survey. The basis for the PSQ-08 is the PSQ-18 and is a
validated survey instrument previously used specifically to measure consumer satisfaction in
EHR studies (Marshall & Hays, 1994).
The distribution of the paper copies of the surveys was at the senior citizen centers. The
survey used a 5-point Likert scale (5 = Strongly Agree, 1 = Strongly Disagree) to measure
consumer satisfaction. The survey process followed the Institutional Review Board (IRB)
guidelines for the protection of human subjects in research studies to protect study volunteers
(Creswell, 2007).
The sample population was senior citizens using the convenience sample method. This
sample was from senior citizen centers in Hunterdon County in New Jersey. According to
Cooper and Schindler (2010), convenience samples allow researchers to choose the population
based on the convenience of engaging participants. The volunteers from the senior citizen centers
8
were convenient to recruit and provided ideas about a subject of interest. The convenience
sample was effective as it provided the opportunity to gather information regarding community
needs and presented evidence regarding the perceptions for advantages and disadvantages of
these systems.
Significance of the Study
The information gathered examined the relationship between the format of health records
and level of consumer satisfaction with communication and care received. The data collected
from this study could be beneficial for government agencies, insurance companies, and health
care professionals in promoting communication, community services, and training toward
encouraging consumer awareness and health care providers’ adoption of EHRs. Future research
using different demographic population can address how the consumer can be proactive in
managing his or her personal health care through improved communication channels.
Significance of the Study to Leadership
As leaders in health care, health care professionals have the responsibility to ensure
consumers are knowledgeable of the changes implemented for the use of EHRs, access to
personal health information, and consumer rights for privacy and security (Tang & Lansky,
2005). Tang and Lansky noted the “president and other national leaders should continue to
educate the public, perhaps using public service announcements, about the role each of us can
assume to become more informed about our own health and health care” (2005, p. 1294).
Technology has improved the way individuals shop, obtain information, manage
finances, and manage personal health. The government has also taken advantage of technology
by providing information on policy and services offered by governmental agencies. Government
agencies, such as public health agencies, health care providers, and practitioners, have taken on
9
new roles of providing leadership in terms of providing strategic direction as it affects the entire
nation and health care (Andersen et al., 2007; Maheu et al., 2001). Consumers have also changed
roles in how they use and access information.
In 1991, the IOM initiated studies on the implementation of electronic health records.
This effort helped in addressing the issues the legislation is meant to protect, such as security,
integrity, protection, and confidentiality of EHRs. The Standards for Privacy of Individually
Identifiable Health Information, released in December 2000, required its members to assume a
leadership role in compliance with state and federal laws that apply to the use of health records.
These members belong to the American Health Information Management Association (AHIMA).
As part of the leadership responsibilities, AHIMA members establish policy, train staff, develop
consents, release information, and document information used (Skurka, 2003).
This study provided consumers’ views on the consumer satisfaction with quality of care
and information provided. The data collected will contribute to the existing literature by
providing the consumer perspective on the communication channels and furnishing the health
care leadership information on improving communication to the consumer. The results of this
study could also contribute to the literature on the implementation of health records on a national
level and to the CER research to improve the delivery of care.
Nature of the Study
Communication as defined by Katz and Kahn (1978) “is the exchange of information and
the transmission of meaning” (p. 255). Communication contributes to the understanding of a
problem but should also have a mechanism to ensure that the right audience is the target based
on the problem, solution, disadvantage, or benefits. The communication process should include a
predictable relationship between the message sent and the message received. The communication
10
process should assist in understanding the rules, procedures, and policies of the system and
demonstrate gaps despite printed materials or official spokesperson (Katz & Kahn, 1978).
The consumers’ view on the EHR systems implementation used the quantitative research
method and a comparative research design with a cross-sectional survey. Comparative research
provides the understanding of social life by comparing across settings and locations (Miller &
Brewer, 2003). Comparative methods also provide the understanding of variations in “socially
worthwhile practices, policies, and institutions” (Miller & Brewer, 2003, p. 2). A quantitative
comparative study aims at determining the similarity or differences within two distinct groups
(Creswell, 2007). The quantitative comparative study was appropriate as it provided a
measurement mechanism to understand the extent consumer satisfaction with care and
communication when comparing the use of either paper or electronic health records.
Research Questions and Hypotheses
The research questions “provide critical information to the reader about the direction of
the study and raise questions that the research will answer through the data collection process”
(Creswell, 2007, p. 115). The purpose of the research questions was to measure how the
consumer perceives his or her interaction with health care providers. The research questions
addressed the relationship between format of health record, communication, and consumer
satisfaction.
The hypotheses pose the questions in a testable form (Salkind, 2008). Creswell (2007)
noted the basis for the hypothesis is on previous research results should narrow down the
research purpose, state the variables, and can be repeatable with a different audience or location.
Hypotheses contribute to quantitative research as a predictor of what the study will explore.
11
Questions
General Question: What is the difference between the format of health record used (electronic
versus paper) and the level of consumer satisfaction with care provided and communication with
provider?
RQ1: What is the relationship between the format of the health record (paper versus electronic
versus both) and the consumer satisfaction with care received?
RQ2: What is the relationship between the format of the health record used (paper versus
electronic versus both) and the level of satisfaction with communication between health care
provider and consumer?
RQ3: After controlling for consumer demographic characteristics (gender, age, education, and
race), what is the relationship between the format of the health record (paper versus electronic
versus both) and the consumer satisfaction?
RQ4: After controlling for consumer demographic characteristics (gender, age, education, and
race), what is the relationship between the format of the health record (paper versus electronic
versus both) and effect on communication?
Hypotheses
H10: There is no significant relationship between the health record format in paper, electronic or
both, and consumer satisfaction with communication and care received.
H1A: There is a significant relationship between the health record format in paper, electronic or
both, and consumer satisfaction with communication and care received.
H20: There is no significant relationship between the health record format in paper, electronic or
both, and level of communication between health provider and consumer.
12
H2A: There is a significant relationship between the health record format in paper, electronic or
both, and level of communication between health provider and consumer.
H30: There is no significant relationship between the health record format in paper, electronic or
both, based on demographic characteristic (gender, age, education, and race) and consumer
satisfaction.
H3A: There is a significant relationship between the health record format in paper, electronic or
both, based on demographic characteristic (gender, age, education, and race) and consumer
satisfaction.
H40: There is no significant relationship between the health record format in paper, electronic or
both, based on demographic characteristic (gender, age, education, and race) and the level of
communication.
H4A: There is significant relationship between the health record format in paper, electronic or
both, based on demographic characteristic (gender, age, education, and race) and the level of
communication.
Theoretical Framework
The Critical theory and Craig’s metamodel of communication provided the theoretical
framework for this quantitative comparative study. The basis for critical theory is control and
power. Craig’s metamodel of communication includes seven domains of communication. These
domains are rhetorical, semiotic, phenomenological, cybernetic, sociopsychological,
sociocultural, and critical (Miller, 2008). The basis for this study was on the government
mandate and how this mandate may affect the communication or health care provider-consumer
dynamic.
13
Critical theory views organizations as a “system of domination in which one class of
actors exploits others, and differences in interest, far from being negotiated and reconciled, are
typically resolved by the more powerful suppressing the weaker” (Scott & Davis, 2007, p. 215).
Critical theory also shapes social institutions based on organizational power and control.
Influenced by Michel Foucault, Jean-François Lyotard, and Friedrich Wilhelm Nietzsche, critical
theory stresses the cultural beliefs of society (Scott & Davis, 2007). .
The consumers’ view on the implementation of EHR system falls under the theoretical
framework of the critical theory as it applies to finding and fixing a complex problem but also
offers researchers the ability to continue to improve on problems based on the feedback
provided. Shank (2006) noted false ideology based on information received from those in power
may lead to false consciousness, which may mean that consumers do not see what is true.
Consumers may not have access or fully understand all the information that is available through
the various communication channels. The ability to gather data through consumer satisfaction
provided a statistical representation if communication is affected by the EHR implementation.
Critical theory allows the researcher to identify false consciousness so that they can
understand the implication of a situation and work toward considering alternatives. The
researcher can be the agent for change (Shank, 2006). The foundation of critical theory was
appropriate in exploring the consumer views of the EHR implementation mandated by the
government. The data collected allowed for an understanding of the implications of EHR
implementation and through feedback provided health care and national leaders the mechanism
to implement change as it relates to communication channels and consumer satisfaction.
Craig’s metamodel of communication provides an overarching way of thinking about
communication and the effects on the consumer. The metamodel of communication encompasses
14
seven domains of communication theory. These domains of communication provide the basis for
organizational communication approaches. The use of EHRs may affect communication that in
turn could affect consumer satisfaction.
The seven domains covered in Craig’s metamodel of communication include rhetorical,
semiotic, phenomenological, cybernetic, sociopsychological, sociocultural, and critical. The
rhetorical approach is discourse or the communication strategies of organizational leaders. The
semiotic approach is the intersubjective mediation by signs or corporate symbolism. The
phenomenological approach relates to the experience of others, cybernetic relates to the
processing of information, and basis for sociopsychological is expression, interaction, and
influence. The sociocultural approach relates to the reproduction of social order, and the basis of
the critical approach is on discursive reflection relating to programs designed to shift beliefs
about gender and power (Miller, 2008).
Craig’s metamodel of communication was an appropriate theoretical framework for this
study as this relates to communication between health care provider and consumer. M. H. Murad,
Gjerde, Bobula, Ostrov, and M. S. Murad (2009) noted that communication can contribute to
consumer dissatisfaction based on implied communication gaps. The rhetorical approach can
relate to the physician-consumer interaction, the phenomenological approach can relate to the
consumers experience with health care providers, and the cybernetic approach can relate to the
information processing required by both consumers and physician. The sociocultural approach
was applicable to the application of the consumer feedback into educational programs and the
improvement of communication and quality of care (Murad et al., 2009).
15
Definition of Terms
Consumer - The definition of consumer is as the recipient of medical care as it relates to
the use and access of EHRs and paper health records. The consumer and the patient have
interchangeable roles as it applies to understanding and accessing electronic health records.
e-health – E-health is health care delivery through the use of technology. E-health is also
electronic health care information used for informational, educational, and commercial purposes.
Electronic Health Records (EHR) - Electronic Health Records are the digitized version of
medical records. The EHRs contain information regarding patient health history, laboratory
work, medication, and ailments if applicable. The EHRs are part of the EHR systems that
communicate to various other medical systems, such as insurance, laboratory testing, health
monitoring, and medication. One feature with EHRs is the ability to e-prescribe that allows the
electronic prescribing of medication.
Communication Channels - Communication Channels are the mechanism for the
consumer to obtain information regarding EHRs use, access, and protection. The communication
channels can be the health care provider, the physician, the insurance company, or the Internet.
Communication channels provide information to the consumer on the access and use of EHRs
and should provide sufficient information regarding the implications to privacy and data security.
Assumptions
The assumption was that the sample population had electronic health record knowledge
and access. The assumption was made that physicians will have one form of health records either
in paper or electronic format. Another assumption was that consumers had access to information
through communication channels, such as health care providers, government agencies, and the
16
Internet. A final assumption was that consumers will be honest in their responses to questions
asked in the cross-sectional survey.
Scope, Limitations, and Delimitations
The scope of the study was to explore the consumers’ views on the implementation of
EHR systems, communication, and consumer satisfaction. The data collected through the cross-
sectional survey allowed for an association between format of health record and consumer
satisfaction. The goal of the study was to provide health care and government leadership for the
mechanism to gather consumer feedback to implement changes to improve the communication
between consumers and health care leadership.
The sample size of the population under study was a limiting factor, as the population
only included senior citizens in Hunterdon County, New Jersey. The sample population provided
diverse perspectives but may not represent the full scope of experiences related to the EHR use
and implementation. The sample population did not include non-English-speaking consumers,
which also limited the dimensions of the results.
Creswell (2007) noted a generalization of results can be accomplished using a small
population sample within a quantitative research approach. The smaller sampling size allows for
the general concept of a “cross section of people from all socioeconomic levels” (Creswell, 2007,
p. 48). This concept can be beneficial as sampling a larger group could be time and cost
intensive, but sampling a small group would allow for a generalization of the tested population.
The recommendation is to vary the demographics of the population to obtain a broader range of
responses.
Cooper and Schindler (2010) noted the lack of control to ensure precision in using
convenience samples. The informality of using convenience samples can be useful in gathering
17
consumer views, as this provides a means to gather information easily and with no cost (Cooper
& Schindler, 2010). The ease in using convenience sample may provide sufficient evidence on a
topic so that a more sophisticated approach may not be a requirement.
Another limiting factor was the observer or research bias with bringing validity and
reliability of the measurement process. Powell (2006) noted validity and reliability could be
affected by inconsistent data collection techniques, observer bias, the setting for data collection,
the instrument, the human subject behavior, and the sampling. The basis of the PSQ-08-
Electronic Health Records Survey was a publicly available and previously validated
questionnaire: the Rand Corporation PSQ-18. This questionnaire has been previously used in the
measurement of patient satisfaction as it relates to electronic health records; this made the basis
for the survey tool appropriate for this study (Bhardwaj, Raina, Bansal, & Agnihotri, 2011;
Marshall & Hays, 1994; Vrijhoef, Berbee, & Steuten, 2009).
Chapter Summary
The implementation of EHRs has been in place for over 30 years and has been supported
by many national leaders, medical organizations, privacy advocates, and legislation. The
literature presented an historical timeline of the challenges posed with the implementation of
electronic heath records and the consumer-health care provider communication dynamic.
Historical data is beneficial in understanding how the implementation process has evolved and
how the many challenges in implementation of these systems have been addressed.
The benefit of this study was that understanding the consumer view could provide
information for health care leaders to develop communication plans, community services, or
consumer training to ensure consumer awareness of the implications in using EHRs.
Improvement in communication channels would be beneficial in the adoption of EHR systems
18
and promote change in how to communicate information to the consumer. Other benefits include
understanding the consumer perspective on communication through the measurement of
satisfaction with health care or information provided.
The background information provided the challenges with implementation and adoption
of EHR systems as the basis for research on the consumer view of communication channels, the
EHR implementation, and how this may affect consumer satisfaction. The problem and purpose
statement defined the challenges with the government mandate for EHR systems by 2014 and
delineated how the rush to implement these systems may affect the consumer. The study could
provide health care and government leadership the mechanisms to explore how communication
between consumer and health care providers is affected by the use of either paper or electronic
copies of health records. The critical theory and Craig’s metamodel of communication provided
the theoretical framework to understand the societal implications based on the EHR
implementation.
Many studies (Berner et al., 2005; Heart, O’Reilly, Sammon, & Donoghue, 2009; Lee &
Meuter, 2010; Meinert & Peterson, 2009; Terry et al., 2008) conducted on the implementation of
EHRs focus on the challenges in adoption and the effects on communication between project
stakeholders such as IT professionals and the health care providers, and the communication
challenges between physicians and patients. Other studies (Bensing et al., 2008; Del Piccolo et
al., 2008; Earnest et al., 2004; Elleuch, 2008; Fisher et al., 2009; Lanseng & Andreassen, 2007)
explore the consumer views and communication channels to promote or discourage the use of
EHR systems by consumers and health care providers. A gap in literature exists as it relates to
the consumers’ view on the communication channels, consumer satisfaction, and the health care
provider-consumer dynamic. This quantitative comparative study would contribute to the
19
literature by providing the consumer perspective on communication channels and consumer
satisfaction as it relates to the implementation of EHRs.
The literature review provided empirical evidence from studies conducted in
communication, EHR implementations, and consumer satisfaction. The studies previously
conducted will provide information on current trends in communication and systems
implementation on a national and global level. Chapter 2 presents an historical perspective of the
evolution of technology and health records, consumer satisfaction, and the effects on
communication between the health care provider and the consumer. Chapter 3 presents the
methodology, the survey tool to include validity and reliability, the sample population, and
concludes with the sampling procedure. Chapter 4 presents the findings, data analysis, and will
provide the statistical measurement for consumer satisfaction and communication depending on
the format of the health record. Chapter 5 provides the summary of findings, the conclusion, and
suggestions for future studies.

20
Chapter 2: Review of the Literature
Introduction
The literature review presents what researchers have studied, their findings, and the
contribution to the knowledge base in relation to health care information, use of medical records,
and communication channels to the consumer. In the review of existing literature, the subject to
explore was the implementation of electronic health records, the use of electronic and paper-
based health records as well as the health care provider-consumer dynamic and how these
concepts contribute to consumer satisfaction. These were the parameters for this quantitative
comparative study. Some studies referenced support the scope of this study as the health care
system is competitive and patients as consumers are the target audience, whereas other studies
support the challenges in EHRs adoption.
The body of literature referenced supported this study in understanding the consumer’s
view in the implementation of EHRs. The studies referenced also supported communication
channels by providing an historical perspective of the EHR systems implementation challenges,
communication challenges, and trends for future use of health care systems. The various studies
referenced provided a global perspective of the EHR implementation relative to the challenges in
implementation, communication, and the health care provider-consumer dynamic. Research
conducted in countries, such as the United States, Canada, Japan, the United Kingdom, and
various others, provided insight into what researchers discovered as part of these challenges.
Ventres et al. (2006) noted that the introduction of EHR systems “influences multiple
cognitive and social dimensions of the clinical encounter” (p. 124). There were many studies
conducted supporting EHRs implementation (Earnest et al., 2004; DesRoches et al., 2008; Lee &
Meuter, 2010) and others that explored the challenges with implementation (Berner et al., 2005;
21
Heart et al., 2009; Meinert & Peterson, 2009; Terry et al., 2008). These challenges included
system adoption, project management, communication requirements, and the role of the health
care provider in ensuring the patient receives quality care and relevant information.
The key players in EHRs implementation consist of government officials, policy makers,
professional institutes, insurance companies, health care professionals, and patient
representatives as well as the media. All of these players have an important role in
communicating with the consumer. The media plays an important role in bringing all
stakeholders together with sufficient information in a balanced and informative manner
(Cockcroft, 2009). The media landscape can be public communication channels, such as the
Internet; or secured channels, such as web portals or private networks.
Chapter 2 reviews the existing literature as it applies to the historical perspective of e-
health and the digitization of medical records, the current use of health records, and the role of
health care leadership and government. The chapter identifies gaps in literature as these apply to
the consumer communication channels, health care provider-consumer dynamic, and consumer
satisfaction. The chapter concludes with a synthesis of context, the sample population, and the
environment relating to this study.
Documentation
The literature review references studies and articles posted on the University of Phoenix
online database that include e-books, specialized databases such as ProQuest and Emerald, as
well as an Internet search for current news report related to the implementation of electronic
health records. The following key words served as the search parameters: medical records,
electronic medical records, critical theory, communication, physician-consumer dynamic, e-
health, and health care information systems. The basis for the keyword search was the
22
parameters of the quantitative comparative study to gather the consumer views on the
implementation of EHRs, communication channels, and consumer satisfaction.
The literature review incorporates resources from peer-reviewed journal articles, media
reports, e-books, and reports. The documentation research timeline is between July 2010 and
February 2011. The media reports provide an historical perspective on the evolution of e-health
and the requirements set by the government for the implementation of EHRs. The historical
perspective includes early stage material, such as the evolution of health care information
through technology, e-health, legislation, and implementation requirements as well as the use of
paper-based and electronic health records.
Electronic Health Record Historical Perspective
The history of electronic health records relates to the advances in technology and
telecommunications. Telemedicine, telehealth, and e-health relate to the use of technology to
access health care services, clinical information, and education for health care providers and
consumers using telecommunications. These channels of communication were in place prior to
the implementation of the Internet (Maheu et al., 2001).
The early use of telecommunication to support health services involved group therapy,
nursing interactions, education and training, televisits to community health workers, image
transmissions, and homecare. These early examples of health services did not require interaction
with a physician. As technology evolved, the use of the Internet promoted health care delivery
termed as e-health. E-health incorporates all forms of electronic health care information to
include informational, educational, and commercial products to interested consumers and health
care professionals. Maheu et al. noted the Internet has made health care “more efficient, allowing
23
patients and professionals to do the previously impossible through the efficiencies of the
Internet” (2001, p. 11).
The Internet offers consumers and health care professionals a communication vehicle as
well as an efficient and immediate access to medical data. Studies show Internet-based
communication provides the physician a medium for easy access to patient information as well
as easy access for the consumer to gather health-related information (Lee & Meuter, 2010;
Ouschan, Sweeney, & Johnson, 2006). Internet use can also affect consumer satisfaction.
Government funding promoted the use of the Internet to provide medical information to
interested parties. Congress established various agencies throughout the 1990s to develop
telemedicine programs with the goal to improve health care access through technology. The
Internet provided greater access to health care information at a low cost. The Internet also
improved communications among patients and health care professionals using online
communities, e-mail discussion groups, and bulletin boards as well as secured websites that
covered disease management, personal health records, self-monitoring, and communication
(Maheu et al., 2001). Stockdale (2008) added online communities and Internet access to
empower patients and promote the efficiency of health care.
The government has created legislation to protect the consumer’s personal medical
information. Various state and federal laws protect patient-specific information, but these laws
vary from state to state. Health care records have a long history of existence and require
protection by these laws and regulations because these documents are legal documents that may
be a requirement in judicial matters, payment processing, research, as well as patient care.
In paper form, medical records were easier to manage as the requirements for
authentication was a signature and the requirements for destruction were either through
24
shredding or burning. As the medical records became digitized, the requirements for security
became greater because the data involves multiple types of data such as paper, electronic
documents, and electronic images (Wager, Lee, & Glaser, 2009). Because of the changes in
requirements, a change in legislation as well as new provisions were added for the new
dimension of electronic data; and protection also became a requirement.
Legislation is in place to protect medical data and has evolved as the demand for
information became greater and the use of technology became the norm. The Privacy Act of
1974 evolved from the Freedom of Information Act of 1966 (FOIA). FOIA allowed public
access to information obtained by federal agencies (Wager et al., 2009). FOIA gave limited
protection to personal medical information; hence, the legislation required updates. The Privacy
Act of 1974 followed; that legislation led to the creation of other legislation to keep up with the
implications of health care information storage, access, and protection.
The implementation of the Privacy Act of 1974 outlined the roles and responsibilities of
governmental agencies in the collection, use, and distribution of personal health information
(Maheu et al., 2001). The government continues to play an important role in setting controls to
safeguard consumer medical data. The requirements for data protection are a shared
responsibility requiring leadership on a national and international level to ensure protection
across international as well as internal borders. The shared responsibility is for health care
professionals, governmental agencies, and privacy and consumer advocates, and includes
leadership in all of these areas.
The Medical Records Confidentiality Act of 1995, the Health Insurance Portability and
Accountability Act (HIPAA) of 1996, American Recovery and Reinvestment Act (ARRA) of
2009, and the HITECH of 2009 were also created to protect consumer’s privacy and
25
confidentiality of medical health records. The provisions set by this legislation apply to both
paper-based medical records and EHRs. As technology expands and provides greater issues with
security, legislation updates are required to keep up with changes in innovation and technology.
The purpose of medical health records is to document the patient history; provide
accessibility between organizations, such as health care providers, insurance companies,
pharmacies, and laboratories; and permits both health care and consumers to manage the patient
health care. Wager et al. (2009) noted the purposes for medical records either in electronic or
paper format are for patient care, communication, legal documentation, billing and
reimbursement, as well as research and quality management. The goal is to centralize this data so
that health care providers can have a comprehensive view of the patient history as well as
provide access to interested third parties on a need to know basis. Third parties include
laboratories, pharmacies, insurance companies, government agencies or employers, and
associated information systems.
The evolution of technology and telecommunications prompts the migration of medical
health records to a digital form. The implementation of electronic health records provides
benefits that include data transmission, sharing, and accessibility through telecommunication
channels, such as the Internet or virtual private networks for secured transactions. The benefit in
using EHRs is the delivery of patient data to authorized personnel regardless of location. This
benefit allows for timely and efficient health care because the information is easier to track and
allows for a historical perspective, especially with laboratory testing and prescriptions as well as
diagnosis and intervention (Maheu et al., 2001).
EHRs also provide administrative benefits and reduce cost. Data digitization minimizes
issues with handwriting ineligibility, misplaced patient charts, storage, and redundancy or
26
inaccuracies between records in various health provider locations. The administrative benefits in
records management could also cut medication errors or adverse interactions between
medications (Lee & Meuter, 2010; Maheu et al., 2001). Wager et al. (2009) noted electronic
health records are a communication tool for individuals involved in the patient health care.
Health care leadership has evolved as the needs for health care information have become
greater. Government programs, such as Medicaid and Medicare, put a burden on administrative
requirements for funding for the elderly, poor, and individuals with long-term disabilities.
Health insurance, patient billing, patient health data, and treatment require specialized systems to
minimize the administrative and resource costs.
The administrative requirements for these applications and programs required specialized
systems to manage the data so the implementation of health care information systems progressed.
The definition of health care information systems is the arrangement of information, the
processes, the people, and the information technology to support the health care administrative
functions (Wager et al., 2009). The implementation of health care information systems expanded
the role of health care executives in not only managing health care facilities or programs but also
the information created throughout the organization. As part of the added responsibilities,
communication requirements also expanded.
Information Access. As part of legislation and ethical requirements, consumers should
be aware of informed consent requirements. Informed consent relates to the patient providing
consent for admissions, treatment, surgery, and the release of information (Wager et al., 2009).
The release of information is not complete without a patient giving consent through a signed
document. Medical professionals consider informed consent critical to patient care and a patient
should be aware of his or her rights to be informed (Ervin & Berry, 2006). The use of various
27
communication channels may affect how information is accessed and protected. Health care
leadership should take on a proactive role in protecting and limiting access to patient
information.
EHRs and Communication
As technology has evolved, so have the roles of the consumer, the health care
professional, and the various governmental agencies that have an interest in improving health
care on a national level. The consumer has the right to expect that a health care provider will
make recommendations on preventive services that are individually appropriate as well as
intervention when required (Andersen et al., 2007). The Internet has provided an alternative in
how a consumer acquires information as it pertains to managing his or her personal health care.
Communication is not only limited to consumer and health care professionals. Yoon-
Flannery et al. (2008) noted communications as a benefit within various levels of management.
These levels include executive leadership and practice leadership, practitioner-to-practitioner as
well as executive and practitioner to vendor communication. The implementation of EHRs
required adaptation to specific needs for the practitioner and institution that minimized the
duplication of efforts. The practice leadership and executive leadership also required clear
communication channels with providers regarding implementation.
The governmental agencies have also taken on different roles in providing consumers
with health care information. Andersen et al. (2007) noted the role of public health agencies has
expanded in providing leadership in terms of planning strategic objectives for health care on the
national level. As part of this process, public health programs or governmental agencies have
taken on the role of defining questions posed by the consumer regarding the quality of care
provided by health care professionals.
28
Yoon-Flannery et al. (2008) found perceived benefits in the EHR implementation, such
as improved patient care, improved communication among practitioners, enhanced efficiency, as
well as improvements in regulatory compliance. Various studies (Alkayid, Hasan, & Meloche,
2009; DesRoches et al., 2008; Zandieh et al., 2008) gathered the perspectives on the benefits and
perspectives on the EHR implementation among various areas of the health care systems from
health care leaders. A top benefit noted was communication improvement.
Karsh, Beasley, and Hagenauer (2004) conducted a study to measure the perception of
the quality of EMRs versus hard copies of medical records. The study examined the relationship
between using EMRs and the quality of work life as well as the quality of care provided by
physicians who use electronic medical records (Karsh et al., 2004). The study confirmed a
positive impact and benefits to the physicians in using EMRs.
Limited studies are available in correlating paper-based and electronic health records
with consumer satisfaction and communication. The discussion on whether communication is
positively or negatively affected with using one or the other form of medical records is
controversial. One study found the use of computers to access medical records takes away from
the consumer-patient dynamic by distracting participants either in use or issues with functionality
(Botin, 2007). Studies to measure consumer satisfaction also vary in results (Bensing et al., 2008;
Del Piccolo et al., 2008; Elleuch, 2008).
Botin (2007) found the introduction of an electronic health record system contributed to
changes in communication patterns between hospital personnel and patients. The study compared
the use of paper health records, EHR systems, and the health care provider interaction with the
patient. The interaction between physician and patient was more empathetic when using paper
29
copy where the interaction with EHRs seemed focused on the technology and not on the well-
being of the patient (Botin).
Other studies found patients are more apt to express their concerns when a health care
provider was not dominant, showed concern and empathy as well as maintained eye contact
(Bensing et al., 2008; Elleuch, 2008). Del Piccolo et al., (2008) explored the patient-physician
dynamic and found patients prefer the physician to be caring, sensitive to their health concerns,
understand the patient as a person, and mutually agree on health care management. Eye contact,
physician sensitivity, and the consumer role in proactive health care can affect the health care
provider-consumer dynamic.
Robb and Greenhalgh (2006) found lack of trust discouraged patients from complying
with health care provider’s recommended treatments; patients failed to maintain appointments
and were inconsistent with their health care plans. Fisher et al., (2009) discovered consumers
who had access to their medical records prepared consumers for a consultation, could
compensate for poor or complex communication, and reduced the fragmentation of care.
Consumer access to health records also promoted self-care, confidence, and trust in the health
care provider as well as improved shared health management (Fisher et al., 2009).
Consumer Communication Channels. Health care information systems can provide the
consumer with access to EHRs through secured channels as well as access to health care
information through an open network. Based on the ease of use and availability of information,
consumers are driving the need for health care information. Consumers are using the tools
available through the Internet to become more informed and bridging the informational gap
between health care providers and consumers.
30
The Internet offers consumers immediate access to global databases, libraries, conference
proceedings, records, support communities, and numerous resources from the comfort of their
home and with minimal, if any, cost. Maheu et al. (2001) noted e-health offers consumers the
option for an alternative channel for obtaining health care, especially when there may be a stigma
associated with a particular health concern. The abundance of information can provide the
consumer with sufficient knowledge to understand an ailment or concern as well free up health
care resources.
Consumers can use the Internet as a resource for referrals, convenience, cost, coping
strategies, and support as well as information. These resources would not require interaction with
a health care professional. The lack of interaction could empower the consumer to manage his or
her personal health care. The consumer self-care can also promote healthier habits, reduce
unnecessary visits to the physician or emergency room, reduce cost, and promote better decision-
making as it relates to personal health concerns (Camgöz-Akdag & Zineldin, 2010; Maheu et al.,
2001; Ouschan et al., 2006).
Zickmund et al. (2007) noted the use of web-based patient portals as an effort to improve
communications between physicians and patients. The technology-based communication tools
such as web portals provide access to electronic health records, laboratory test results, and
communication through secure channels to the health care provider (Zickmund et al., 2007).
Web-based tools, such as portals and the Internet, provide consumers with instant information,
asynchronous communication, and access to various resources to understand health concerns.
Examples of web portals are iHealthRecord, PatientSite, Microsoft HealthVault, Google Health,
and My Personal Health Record. This type of communication does not require physical
31
interaction with the physician as all this can be accomplished through telecommunication
channels.
Other studies have misinterpreted the use of web portals for effective communication.
Alkayid et al., (2009) noted families preferred a face-to-face option to discuss the medical
conditions of their loved ones as this relieved stress for the family. Stockdale (2008) added the
need for communication through “self-expression, spiritual support, and advocacy” as a
significant role in the delivery of health care, although the use of online communities provided
an outlet for emotional support (p. 39). Lanseng and Andreassen (2007) further added that
technology also can be beneficial in managing health concerns if the consumers trust their own
skills in locating information, as the service is tangible and easier to evaluate.
Earnest et al. (2004) confirmed that online medical records system was beneficial to some
patients and extremely beneficial to all the physicians. The benefits to the patients included easy
access, management of chronic disease, and easier to understand medical jargon on the patient
record (Earnest et al.; Ouschan et al., 2006; Stockdale, 2008). The benefits to the physician were
a change in perspective regarding patient access to medical records, as previously the physicians
had expressed concern but changed perspective after the implementation of the new system
(DesRoches et al., 2008; Earnest et al.,2004).
E-health provides consumers information through telecommunication channels such as
the Internet. Issues with e-health include the quality of the information available, the magnitude
of information, as well as the comprehension level of the interested parties of medical
information (Maheu et al., 2001). The information may be readily available, but may not always
be accurate, easy to understand, and can be subject to misinterpretation. The Internet does not
offer a filtering or accuracy check to ensure information validity or reliability. Although there are
32
guidelines, ethical considerations, and advocacy groups, it is difficult to control the information
posted on the Internet.
Implementation Issues
Berner et al. (2005) noted that the preparation for digitizing health records has been in
discussion for over 35 years. Adoption has been slow because of reluctance from the medical
community in computer hardware and software investments, the lack of computer knowledge,
and the lack of interoperability between systems (Berner et al., 2005; Heart et al., 2009; Meinert
& Peterson, 2009; Terry et al., 2008;). Other issues to resistance relate to privacy concerns and
challenges in communication and implementation. Health care providers have not adopted
electronic health records and still use paper-based copies because of these issues.
Integration poses many challenges, including resistance to adoption, lack of
communication networks, lack of flexibility in funding and regulatory relief, lack of
understanding of what exists within the communities, and lack of designation of decision-makers
(Heart et al., 2009; Katz & Kahn, 1978). Other issues with implementation arise due to system
complexity, the expectation of technology bridging communication, and the social or human
interaction between systems. Implementation issues can relate to adoption issues as they share
the same characteristics. Other studies also provided usage details regarding patient access to his
or her medical records and found factors, such as education, computer literacy, severity of
disease, and patient to physician ratio contribute to online use (Stockdale, 2008; Terry et al.,
2008).
The government mandate to have EHR systems in place by 2014 will also contribute to
implementation issues. Issues with cost, aggressive timelines, lack of resources to support
changes in information technology infrastructure as well as the lack of knowledge to support
33
these new systems will be challenging. Societal pressures to implement consumer tools for
asynchronous communication can affect physician-consumer communication negatively if not
managed correctly.
Meaningful Use. As part of the HITECH requirements, the software applications for
EHR systems should provide features to promote better clinical decision making, avoid
preventable errors, promote information sharing among health care providers, decrease the cost
of medical imaging, and decrease duplication of services (Blumenthal & Tavenner, 2010). The
meaningful use of EHRs will also provide the consumer with access to the electronic versions of
personal health records.
To measure the adoption rate of EHRs, DesRoches et al. (2008) noted the functions of
the EHRs system as “recording patients' clinical and demographic data, viewing and managing
results of laboratory tests and imaging, managing order entry (including electronic prescriptions),
and supporting clinical decisions” (para. 6). These functions are part of a fully functional EHR
system. The study results concluded positive effects in the quality of decision making,
communication between health care provided and consumer, timely access to medical records,
and avoidance of medical errors. Although these results support the benefits to EHRs adoption,
only a small percentage of health care providers have adopted a fully functional EHR system
(DesRoches et al., 2008).
Paper-based and Electronic Health Records. An issue with the static format of paper-
based medical records is that it does not allow for effective decision-making, as these files limit
the interaction between patient and health care provider. When comparing paper-copy health
records and electronic format of medical records, it should be noted that EHRs promote active
decision making because of the dynamic tools available. EHRs provide tools, such as access to
34
the relevant research data, reminders, alerts, and other knowledge resources (Ayers, Menachemi,
Ramamonjiarivelo, Mathews, & Brooks, 2009; Lee & Meuter, 2010; Wager et al., 2009;). These
are dynamic features that are available through technology.
The dynamic capability of EHRs for effective decision-making and options for electronic
resources prompted the migration of health records to electronic format. This migration posed
issues with security and confidentiality. Issues with data warehousing, centralization, and data
mining of consumer medical data raise concerns in responsible communication to the consumer.
The issues with security and confidentiality are also being addressed on an international level
with various organizations coming together to provide leadership and suggestions with regard to
the protection of consumer medical records (Maheu et al., 2001; Wager et al., 2009).
The implementations of EHRs pose similar challenges in data protection when compared
to paper-based medical records. The challenges include physical security, limiting access,
storage, and data protection. The implementation of EHRs can minimize some issues such as
data security and confidentiality, but requires due diligence from system administrators, data
owners, and health care professionals as well as government agencies, insurance companies, and
industry vendors. The due diligence in maintaining a secure posture, data protection, access
limitation, and regulatory compliance is an ongoing process and requires sufficient resources to
be successful.
Control Mechanisms. The Internet has added challenges in trying to maintain privacy
and confidentiality where anyone can have access if sufficient control mechanisms are not in
place (Edge & Groves, 2006; Maheu et al., 2001). These control mechanisms are data security
and integrity. These controls should incorporate the human aspect as well as the technology
35
aspect. Health care leadership, government agencies, third-party vendors, and the consumer play
an important role in maintaining data security and integrity.
Ervin and Berry (2006) explored concerns with the use of the Internet for a computer-
based health information network and discovered many concerns, but the issue of competitive
practices was critical. Competitive practices, such as providers offering “better services or lower
prices” to compete with other health care options, could confuse or mislead consumers (Ervin &
Berry, 2006, p. 8). Health care leadership, government agencies, third-party vendors, and the
consumer play an important role in understanding the presentation of information; but the
Internet does not have filtering capabilities, so it is difficult to govern the information posted.
Trust in Technology. Health care information systems raise other issues with
implementation. Implementation issues for EHRs systems can be the expense, workflow
requirements, and best-practice identification. Ervin and Berry (2006) noted through a study that
consumers have concerns with confidentiality and security, information accuracy, and informed
consent as these relate to the implementation of EHR systems. Whetstone and Goldsmith (2009)
found positive results in their study using college students as such results relate to confidence in
privacy and security of personal health records. Bodkin and Miaoulis (2007) confirmed the
college students’ attitudes related to security, trust in the website hosting their personal
information, and understanding how the website will use this information.
Leadership Implications
Seeley (2009) noted health care executive leadership plays an important role in system
adoption of health care information systems. Executives should understand organizational
readiness, end-user expectations that align with corporate vision of the information and systems
in place that can promote better health care as well as provide corporate communication to the
36
user community to ensure adoption (Seeley, 2009). Health care leadership can promote system
adoption by providing sufficient information regarding the benefits in information retrieval and
treatment protocol enhancements based on technological advances. There should also be a
mechanism in place to measure user satisfaction, system benefits, and impact on health care
improvements.
Consumer Satisfaction
Various studies measure consumer satisfaction based on the interaction with the health
care provided, information received, technology used, or available communication channels; but
none directly measures how the use of health records either in electronic or paper format affects
satisfaction based on communication (Bensing et al., 2008; Fisher et al., 2009; Stockdale, 2008).
Technology can affect how the consumer interacts with the health care provider either by
providing benefits by presenting information or disadvantages in supplying inaccurate
information. The measurement of consumer satisfaction can provide the various stakeholders in
the implementation of electronic health records with sufficient information to address how these
benefits and disadvantages affect consumers.
Alkayid et al. (2009) noted Internet usage affects process quality, but not outcome quality
or customer satisfaction. The study results supported the consumer decision to reuse information
on the Internet. The decision influenced consumer satisfaction (Alkayid et al., 2009). Whetstone
and Goldsmith (2009) added that patient satisfaction, perceived quality, and behavioral
intentions are also affected through the use of e-health.
Zickmund et al. (2007) noted interest in web-based patient portals was dependent on the
level of satisfaction between physician and consumer. The Internet and web portals provide easy
access but also limit the interaction between physician and consumer as it does not allow for
37
two-way communication unless a face-to-face requirement is set through an office visit. Rivers
and Glover (2008) found satisfied patients are more likely to comply with health care
professional recommendations and to cooperate or maintain the health care provider-patient
relationship.
Dissatisfied consumers with provider communication and responsiveness or the inability
to obtain medical information as well as physical access to a physician’s office are more likely to
use alternate communication channels, such as the Internet and patient web portals (Fisher et al.,
2009; Zickmund et al., 2007). Alkayid et al. (2009) added that families prefer to communicate
directly with the health care professional versus using an online option for patient updates. There
are some circumstances where a face-to-face meeting is a requirement but the consumer has the
option to research for information prior to a consultation or attain additional perspective through
the available communication channels should there be issues with trust or dissatisfaction.
Gender may relate to consumer satisfaction as some studies have shown inconsistent
conclusions in which there are no differences between males and females or there are significant
differences (H. Soleimanpour et al., 2011; Murad et al., 2009; Teunissen, & Voest, 2010;
Wessels et al., 2010). Wessels et al. (2010) found women regard most health care aspects as
important as this relates to ”means and extent of communication, manner and extent of support,
counseling and rehabilitation, consultation length, and physician assignment” (p. 649). H.
Soleimanpour et al. (2011) noted no meaningful relationship with satisfaction level between
males and females. Murad et al. (2010) found women were more likely to file complaints and
“their dissatisfaction implies communication gaps” (p. 355).
38
Relationship to the Current Study
The challenges in implementation play an important role in EHRs adoption. The
government’s role in providing applicable legislation to protect the consumers’ personal medical
information is crucial, especially as this applies to the concepts of the critical theory and the
government mandate to have EHRs in place by a specific timeline. Communication is also a key
component as the implications of protecting consumer data are the responsibility of the
government, the health care providers, insurance companies, and all stakeholders interested in
the implementation of EHRs. Craig’s metamodel of communication provided the framework for
directing communication to the consumer.
These factors as part of this comparative study provided the basis for understanding how
these changes will affect the consumer. No set standards for EHRs implementation are available,
and consumer satisfaction is difficult to measure. This quantitative comparative study using the
PSQ-08 questionnaire provided a statistical representation of how the implementation may affect
the health care provider-consumer dynamic and consumer satisfaction.
Integration incorporates a variety of information systems, services, and organizations.
Integration requires changes in information sharing, determines the necessary resources, and
delineates the clients or users (Andersen et al., 2007). The goal of health care integration is to
“improve access to comprehensive services and continuity of care; reduce service duplication,
inefficiency, and costs; and establish greater accountability” (Andersen et al., 2007, p. 364).
The various channels that consumers use for communication have been the basis for
research. One example is the media analysis study that found differences in the approach to
implementation related to centralized and decentralized EHR approaches. Depending on the
approach, the focus would be both on the standards and on interoperability versus project
39
management, budgets, and financial considerations (Cockcroft, 2009). The focus of media
analysis was the media’s role in gauging public opinion or providing information regarding
implementation success.
Concerns with protection of medical data prompted government officials to establish
guidelines, laws, and policies in the use, accessibility, and protection of consumer medical data.
In addition to legislation to protect a consumer’s rights to privacy, there are ethical
considerations. Privacy in relation to health care is the consumer’s right to limit access to
personal medical information, and confidentiality relates to the expectation that this information
is only to be used for its intended purpose (Wager et al., 2009). Edge and Groves (2006) noted
the patient has the right to confidentiality based on the relationship between physician and
patient. Confidentiality is important in the relationship between consumers and health care
professionals as a matter of trust and responsible communication.
The consumer concerns with privacy and confidentiality have led to the creation of
legislation to ensure the security and protection of medical data. Legislation such as ARRA,
HITECH, and HIPAA help protect consumer’s rights as they pertain to electronic health records.
The ARRA and the HITECH Acts change existing laws to include new provisions for patients’
rights, privacy, and security protection of medical health information (“American Recovery
Act”, n.d.; “HITECH”, 2009). HIPAA offers consumers options for protecting personal medical
data such as understanding the policies for privacy, participation issues, and protection of
sensitive health information (“Health Information Privacy”, n.d.).
The definition of communication channels is the mechanism for the consumer to obtain
information regarding EHRs use, access, and protection. The communication channels can be the
medical provider, health care professionals, governmental agencies, the insurance company, or
40
media channels, such as the Internet. Communication channels provide information to the
consumer on the access and use of EHRs and should provide sufficient information regarding the
implications to privacy and data security.
The EHRs could provide desirable outcomes, such as improved time management,
additional data provided for analysis, and improved education about services. This information
could be available prior to a visit with a health care provider where the consumer has done
research on an ailment or concern and has information to ask the right questions or provide the
applicable information. The Internet capability for consumer research on health care topics could
save time for both health care provider and consumer as well as allow for effective
communication among participants during medical visits.
Originality of Current Study
The purpose of this quantitative comparison research study was to ascertain if statistically
significant differences exist between paper versus electronic copies of health records,
communication, and consumer satisfaction. Previous studies in similar areas reference the
challenges in implementation, the effects on communication, how this may change the health
care provider-consumer dynamic, and how consumer satisfaction is affected. The context,
sample population, and environment provided an alternative view into how the EHRs may affect
consumer satisfaction. The results of this study can contribute to future trends as the EHRs
adoption becomes prevalent.
Previous Studies. Communication is an important factor for the consumer to understand
the implications of medical care either through wellness checks or when health issues or
concerns are present. A good relationship between consumer and physician allow for trust,
advice solicitation, feedback, treatment protocols, and the consumer understanding his or her
41
medical issues (Alkayid et al., 2009; Bensing et al., 2008; Rivers & Glover, 2008).
Communication is achieved through various channels to include the consumer-physician
interaction, legislation, public health organizations, printed material, and technology that include
web portals and the Internet.
Maheu et al. (2001) noted the concern with data protection, confidentiality, and how
integrity affects consumers. Consumer concerns such as security breaches, hackers, and abuse of
information from outside sources like drug companies were the basis for other research studies.
These issues are also of concern with paper-based medical records, but do not receive the same
attention as EHRs (Maheu et al., 2001).
Some studies (Bodkin & Miaoulis, 2007; Zandieh et al., 2008) address concerns
regarding patient privacy, regulatory compliance, security vulnerabilities, and limiting access to
patient data. Yoon-Flannery et al. (2008) noted important considerations in the implementation
of EHRs, such as best practices, clear communication, careful planning, appropriate technical
support, adequate protection of patient data, and an efficient business plan. Both the
technological and people challenges, such as implementation and communication, are the basis
for other research studies.
Several studies note patient satisfaction with the use of EHRs and communication, but
did not show significant differences when compared to paper copy (Alkayid et al., 2009; Stewart,
Kroth, Schuyler, & Bailey, 2010; Stockdale, 2008; Whetstone & Goldsmith, 2009). These
studies included the design of efficient EHR systems, best practices, communication, and data
collection for quality of care, cost, efficiency, and patient views (Stewart et al., 2010). This study
does not measure changes in communication patterns or changes in behavior that limit the factors
42
that contribute to consumer satisfaction as it relates to a health care provide-consumer
interaction.
Wager et al. (2009) noted consumers have concerns with privacy as well as how personal
medical information is being accessed and used. Concerns with third parties, such as health care
providers, insurance companies, government agencies, drug companies, and employers, may be
accessing medical data for inappropriate reasons are other consumer concerns. The discoveries
of these studies confirm how lack of information regarding data protection can promote mistrust
among consumers and health care professionals. This lack of trust is despite the laws,
regulations, and ethical requirements for health care data protection.
Zandieh et al. (2008) found privacy to be a concern for most patients and practitioners.
Ventres et al. (2006) through a study found a large gap in the patient understanding of the use of
EHRs in which patients lacked understanding of the use of EHRs in health care. Morpace
Omnibus conducted a study to measure consumer support of the nationwide system of medical
records. The study found most participants had little knowledge of the system, although 48%
supported the creation of the nationwide system (“Electronic Medical Records”, 2008).
Issues with communication can also have legal implications. Ervin and Berry (2006)
explored the physician’s views on health care information systems. Physicians noted that many
malpractice claims correlate to miscommunication between physician and patient (Ervin &
Berry, 2006). The issues with lack of consolidated historical information, data management, and
information inaccuracies surfaced during the study. Data management is a requirement for the
health care provider-consumer interaction to avoid mistakes with treatment protocols, data
gathering, medication error avoidance, and effective communication.
43
Cockcroft (2009) conducted a media analysis for evaluating the national health
information development. The analysis provides insight into the issues with communication and
the electronic health records implementation. Cockcroft noted the implementation of the EHRs
system is difficult to evaluate as there is no standard, and the systems are complex by nature.
Studies show that face-to-face interaction was still a requirement even when EHR systems were
in place (Cockcroft, 2009).
Context. The studies referenced provided supporting information for understanding the
issues with EHR implementation, consumer satisfaction, and communication channels. The
literature did not provide an example where the consumer views measured the use of medical
records and the communication channels available to the consumer or the effects to the health
care provider-consumer dynamic. This quantitative comparative study measuring the consumer’s
view on the implementation of EHR systems contributes to the existing literature by providing
the consumer views on the research parameters and how this may influence consumer
satisfaction.
Sample Population. Implications to the digitizing of medical records include concerns
with privacy, security, lack of control, data management, transcribing error rates, and
information dissemination. As consumers, several questions arise, such as How will the system
be managed and secured? How will the necessary information for access, protection, and usage
be acquired? What is the implication to privacy? These concerns will affect most consumers but
in particular the senior citizen population because they have limited avenues for information.
The senior citizen community has the greater need for health care due to their age and
health requirements (Bodkin & Miaoulis, 2007). The lack of understanding the implications of
privacy and controlling their health care information can contribute to misunderstanding or
44
misuse of medical records by the medical industry, vendors who support the industry, or
malicious individuals’ intent on identity theft. This community may also have limited access to
communication channels, and therefore may not be aware of the benefits or disadvantages of
using the Internet to gather information regarding health concerns.
Environment. The federal government has set the goal for most Americans to have
electronic health records by 2014. According to the National Health Statistics Reports, there
were only 19.6% EMR system implementations in 2007 (Hing & Hsiao, 2010). Hing and Hsiao
noted the expectation is only 64.5% EMR system implementations by 2010. A study conducted
in 2008 showed 41.5% of physicians report using all or partial EHR systems (Hsiao et al., 2010).
These statistics show the slow adoption of EHR systems and the current use of paper-
based medical records by health care professionals. The current environment with a mix of
paper-based and electronic health records should assist in measuring the consumer views on the
use of medical records and the effect on communication through consumer satisfaction. The
assumption is that consumers have access to either paper-based or electronic health records as
well as the communication channels to understand their use and protection.
Future Trends. As the adoption of EHRs becomes the norm, future considerations for
consumers should include appropriate legislation for security and access. Other considerations
should include consumer education on the use of health records to include methods of reporting
tests and results, and data interpretation on meaning of data provided (Wiljer et al., 2008). The
determination should also be made on how much information is available and limitations on who
can access this data. Consumer and health care provider education is critical in understanding the
implications and benefits of EHRs implementation and accessibility by the consumer. This
45
education would be supplemental to the health care provider interaction rather than a
replacement (Wiljer et al., 2008).
Synthesis
The literature review provided in this chapter aligns with the purpose and goal of the
quantitative comparative study. The purpose of this study was to measure how the consumers
perceive their interaction with health care providers based on the format of medical records
(electronic or paper) and how it affects communication and consumer satisfaction. The goal of
the study was to provide health care and government leadership the mechanism to gather
consumer feedback, to implement changes, and to improve the communication between
consumers and health care leadership by providing consumer education.
The overview information, issues, and gaps supported the study by identifying previous
research within the parameters to be measured in the quantitative comparative study. Issues with
implementation, lack of understanding legislation, health care and government leadership
communication, and the media’s role as a consumer communication vehicle aligned with what
the study was looking to measure. The sample population provided diverse views based on
gender, age, education, and race representative of the larger population who will benefit from the
discoveries of this study. The environment of medical record used in either digital or paper-based
format is appropriate in understanding how the implementation challenges and adoption affect
the consumer as it relates to communication and consumer satisfaction.
Chapter Conclusion
The health records digitization will cut health care cost, provide a source of information
for physicians and consumers, and save time in administrative functions with the ultimate goal of
improving health care. The government’s directive to have medical records digitized by 2014
46
will present many challenges. Some of these challenges will be in creating integrated systems for
access, security and management, policies, application of new technologies, and global
implementation. Digitizing medical records will have many benefits.
The benefits include a “patient-centered and patient-secure” system, promote information
sharing between systems, provide a source interface for consumers and physicians, cut costs,
possibly improve health care, and reduce paper (Noyes, 2009). How the changes will affect the
health care system and communication process is unclear; so it may be necessary for the
consumer to play a proactive role in attaining this information. As consumers, it is important to
understand the implications of digitizing medical records because the changes will have a direct
effect on information retrieval, review, and access. The benefits can also outweigh the
disadvantages. The Internet has given consumers a medium to understand these implications, but
this information is only useful if it is reliable and accurate.
Wager et al. (2009) noted the full effect of Internet resources may not be fully
understood. The Internet allows consumers universal connectivity and an affordable means to
connect to health care information and resources for personal health management. The Internet
was noted as a technology enabler that promotes the flow in information and breaks down
organizational boundaries (Wager et al., 2009).
Communication seems to be the dominant concept in the use of medical records. Some
studies reference the benefit in using EHRs for consumer-physician communication,
empowerment to consumer to self-manage health care as well as the anticipated improvements in
health care (Alkayid et al., 2009; Ouschan et al., 2006; Robb & Greenhalgh, 2006). Other studies
note the challenges in implementation and the lack of accurate communication channels in order
47
for the consumer to fully accept and understand the benefits of EHRs (Lanseng & Andreassen,
2007; Lee & Meuter, 2010; Stockdale, 2008).
Technology can bridge the information gap for many consumers, but it cannot replace the
face-to-face interaction with health care providers. Technology offers societal applications that
facilitate information gathering and provides knowledge to a consumer as it applies to medical
concerns or legislation; but it does not replace the health care provider-consumer dynamic that
can be achieved only through face-to-face interaction. This traditional form of medical
interaction provides personal interaction and individualized advice to the consumer (Alkayid et
al., 2009; Zickmund et al., 2007). The challenges in communication posed by the implementation
of medical health records align with the purpose and goal of this quantitative comparative study.
Summary
The growth of technology has evolved to the point where consumers may not require a
face-to-face meeting to obtain appropriate health care information. Advances in technology, such
as health care information systems, web portals, and the Internet, can provide an abundance of
information for the consumer and increase the consumer knowledge as well as self-management
of health care concerns. Self-management can improve health outcomes, cut costs in health care
resources, as well as empower the consumer to take an active role in managing his or her own
health.
The implementation of electronic health records should improve health care quality. The
challenges in implementation, lack of communication strategies, and the consumer lack of
knowledge in legislation in place to protect medical data may not fulfill this objective. Although
many studies have shown the benefits of using EHRs, there are many other studies that do not
support the assertion that in the current state of adoption, EHRs improve quality of care
48
(Zickmund et al., 2007). Issues with communication and technology, issues with lack of effective
communication channels, and insufficient information trickling down to the consumer may affect
the measurement of the quality of care.
Chapter 3 provides the research method for the study. The discussion includes the
justification for doing a quantitative study using the comparative design and elaborates on the
study goals. The sample population, the survey tool, and data collection process are also
presented. The discussion also includes the volunteer recruitment process that follows the IRB
guidelines for the protection of human subjects in research studies (Creswell, 2007).
49
Chapter 3: Research Method
Introduction
The purpose of this quantitative comparison research study was to ascertain if statistically
significant differences exist between paper versus electronic copies of health records,
communication, and consumer satisfaction. The instrument, PSQ-08 Electronic Health Records
Survey, was the tool to collect data regarding the consumers’ perceptions of the implications of
EHR and how this affects the health care provider-consumer dynamic. The data collected from
this study could be beneficial for government agencies, insurance companies, and health care
professionals in promoting communication, community services, and training toward
encouraging consumer awareness and health care providers’ adoption of EHRs.
Chapters 1 and 2 provide the overview of the research study and the literature review as it
applied to EHRs and communication channels. Chapter 3 provides the details of the research
design and appropriateness, the population, data gathering techniques, the survey instrument, and
the data analysis. The discussion includes the validity and reliability of the research tool. The
conclusion of Chapter 3 summarizes these concepts and introduces Chapter 4.
Research Questions
The study instrument provides answers to the research questions and hypothesis. The
research questions are:
General Question: What is the difference between the format of health record used (electronic
versus paper) and the level of consumer satisfaction with care provided and communication with
provider?
RQ1: What is the relationship between the format of the health record (paper versus electronic
versus both) and the consumer satisfaction with care received?
50
RQ2: What is the relationship between the format of the health record used (paper versus
electronic versus both) and the level of satisfaction with communication between health care
provider and consumer?
RQ3: After controlling for consumer demographic characteristics (gender, age, education, and
race), what is the relationship between the format of the health record (paper versus electronic
versus both) and the consumer satisfaction?
RQ4: After controlling for consumer demographic characteristics (gender, age, education, and
race), what is the relationship between the format of the health record (paper versus electronic
versus both) and effect on communication?
The hypotheses are:
H10: There is no significant relationship between the health record format in paper, electronic or
both, and consumer satisfaction with communication and care received.
H1A: There is a significant relationship between the health record format in paper, electronic or
both, and consumer satisfaction with communication and care received.
H20: There is no significant relationship between the health record format in paper, electronic or
both, and level of communication between health provider and consumer.
H2A: There is a significant relationship between the health record format in paper, electronic or
both, and level of communication between health provider and consumer.
H30: There is no significant relationship between the health record format in paper, electronic or
both, based on demographic characteristic (gender, age, education, and race) and consumer
satisfaction.
51
H3A: There is a significant relationship between the health record format in paper, electronic or
both, based on demographic characteristic (gender, age, education, and race) and consumer
satisfaction.
H40: There is no significant relationship between the health record format in paper, electronic or
both, based on demographic characteristic (gender, age, education, and race) and the level of
communication.
H4A: There is significant relationship between the health record format in paper, electronic or
both, based on demographic characteristic (gender, age, education, and race) and the level of
communication.
Research Method and Design Appropriateness
Either the qualitative or quantitative method would be appropriate for this study. The
basis for quantitative research strategy is hypothetical deduction and statistical data analysis. The
quantitative research approach uses various measurement tools to observe behavior, measure
attitudes, or interview an individual (Creswell, 2007). The quantitative method requires a
sampling that would provide sufficient data to be generalizable to the larger population
(Creswell, 2007).
The basis for qualitative research is a central phenomenon that a researcher seeks to
understand and explore with a specific audience and in a predetermined location (Creswell,
2007). Qualitative research uses insight, inference, evidence, and verification. Carlson (2008)
added that qualitative research is interpretive and includes introspection. Qualitative research
provides data from the human experience and allows for data collection through interviews,
observations, documented sources, and visual data.
52
The basis for the quantitative method selection was on the statistical data that could be
attained. The quantitative comparative study was appropriate as it provided a measurement
mechanism to understand consumer satisfaction when comparing the use of either paper or
electronic health records and how this may affect communication. The PSQ-08 Electronic Health
Records Survey provides the statistical data on the consumer view based on the research
questions and related hypotheses.
Research Design
A quantitative study using the comparative design provides data to compare attitudes,
opinions, or beliefs as it relates to the implementation of EHRs when compared to using paper-
based medical health records. Comparative research permits the understanding of social life by
comparing across settings and locations (Miller & Brewer, 2003). Comparative methods also
allow for the understanding of variations in “socially worthwhile practices, policies, and
institutions” (Miller & Brewer, 2003, para. 2). A quantitative comparative study aims at
determining the similarity or differences within two distinct groups (Creswell, 2007). Black
(1999) adds comparative studies compare two populations to see if there are similarities between
the populations or if they belong to a different population “based on the trait in question” (p.
403).
The quantitative comparative study was appropriate as it provided a measurement
mechanism to understand consumer satisfaction when comparing the use of either paper or
electronic health records and how this may affect communication. A cross-sectional survey is a
tool to collect statistical data. Cross-sectional surveys allow for collection of data during a
particular time frame, measure consumer attitudes, and measure community needs relating to the
electronic health record implementation. The survey includes questions regarding health care
53
provider-patient interaction and demographic information from participants, such as gender,
race, age, and educational level.
The basis for the survey questions is the Rand Corporation PSQ-18. The questions
measure general satisfaction, interpersonal manner, and communication based on the PSQ-18
questionnaire. The survey was available in paper copies and was distributed at the senior centers.
Sample Population
Testing everyone in the population can be impossible so that only a sample that is a
subset of the population is used in research. As noted by Salkind (2008), a population is a group
of potential participants where generalizability can provide sufficient information for the entire
population of the phenomenon of interest. As it would be time and cost prohibitive to engage the
entire population that may have access to medical records in either electronic or paper format,
the senior citizen residents of Hunterdon County, New Jersey, were the sample population.
The national implementation of health record digitization will affect the U.S. population,
so the assumption is made for the general population. As it is impossible to survey the general
population, the senior citizens in Hunterdon County, New Jersey, were the specific population.
A sample of this population surveyed was the senior citizen centers in Hunterdon County, New
Jersey.
According to the U.S. Census Bureau, the population in Hunterdon County for 2009 was
130,034 (Hunterdon County Facts & Figures, 2010). This population size could provide the
specific population for the generalization of results to the general population. Based on the
literature, it is expected that approximately 40% of physicians are using electronic health record
systems (Hing & Hsiao, 2010; Hsiao et al., 2010) in the United States. Based on this percentage,
it is expected there will be reasonable representation of participants who have access to
54
electronic health records within Hunterdon County, New Jersey. The sample of the population of
senior citizens in Hunterdon County, New Jersey, could provide sufficient data for a
generalization for the larger population.
Approximately 80 volunteers from the senior centers in Hunterdon County, New Jersey,
provided their views on the use of EHRs through a cross-sectional survey. The volunteers
provided diverse views based on gender, age, educational background, and race. The population
was a sample of the target population as a list provided from senior center administrators
(Creswell, 2007).
The calculation of the approximate sample size for the sample population for this study
referenced a formula recommended by Tabachnick and Fidell (2006). The recommendation for
the sample size is calculated using the following formula:
Sample Size = 104 + m
where m equals the number of independent variables.
Given that formula, the anticipated sample size for this study was between 110–115 senior
citizens. There were five independent variables that included health record format, gender, age,
education, and race and were the basis for the calculation noted by Tabachnick and Fidell for
regression testing.
The sample population were senior citizens using a convenience sample method.
According to Cooper and Schindler (2010), convenience samples provide no restrictions as
researchers can choose the population based on the convenience of engaging participants. The
volunteers from senior citizen centers were convenient to recruit and provided ideas about the
subject of interest (Cooper & Schindler, 2010).
55
Creswell (2007) noted a generalization of results can be accomplished using a small
population sample within a quantitative research approach. The smaller sampling size would be
analyzed to apply the general concept to a “cross section of people from all socioeconomic
levels” (Creswell, 2007, p. 48). This concept can be beneficial as sampling a larger group could
be time and cost intensive, but sampling a small group would allow for a generalization of the
tested population.
The participants for the study were senior citizens who are members of senior centers in
Hunterdon County, New Jersey. The demographics section for the survey contained a question
regarding the age confirmation. All participants were required to sign an informed consent form
that was part of the study package. All participant data were kept confidential.
Sampling Frame
The senior citizen volunteers were retired male or female participants who belong to
senior centers in Hunterdon County. The assumption was that the senior citizen volunteers were
a diverse group ranging from 60 and above years old and had access to health records based on
health concerns or needs. The sampling frame included male and female senior citizens but not
limited to any specific nationality, education level, income level, or profession.
The sample size of the population under study was a limiting factor as the population
only included senior citizens in Hunterdon County, New Jersey. The sample population provided
diverse perspectives, but may not represent the full scope of experiences related to the EHR use
and implementation. The sample population does not include non-English-speaking consumers,
and is limited to senior citizens who were part of a senior citizen center in Hunterdon County
that also limited the dimensions of the results.
56
Based on the literature, it was expected that approximately 40% of physicians were using
electronic health record systems (Hing & Hsiao, 2010; Hsiao et al., 2010). Based on this
percentage, it was expected that there would be reasonable representation of participants who
had access to electronic health records; however, data gathering continued until 40 to 50% of
respondents fit the criteria for sufficient data analysis.
Informed Consent
The survey process followed the IRB guidelines for the protection of human subjects in
research studies to protect study volunteers. The participant requirement to be a volunteer for the
study was to provide consent to participate. The consent form ensured cooperation and that
participants understood the purpose of the study (Creswell, 2007). See Appendix A for a copy of
the Informed Consent form.
Prior to the beginning of the study, each participant was informed of the purpose of the
research, the benefits in participating, such as contributing to the knowledge base of EHRs and
possible improvements to consumer communication. All volunteers were ensured that all
personal information would be kept confidential. The removal of any identifying information
ensured the confidentiality of all participants.
The participants could withdraw at any time during the study. The withdrawal process
during the study required the participants to verbally express their wish to withdraw from the
study. Any information gathered would be shredded to ensure confidentiality.
The researcher contact information was provided to the participants should there be any
questions regarding the survey or study questions. After the data collection was complete, if the
volunteer decided to withdraw from the study, the researcher could be contacted via email or

57
telephone. The survey related to this participant would not be used and would be shredded to
ensure confidentiality.
The Informed Consent form was provided as part of the survey package. The survey
package included the introduction to the survey, the Informed Consent form, and the survey
instrument. Participants acknowledged the Informed Consent form by providing a signature on
the form to acknowledge consent. The signed consent forms are stored in a secured metal
container with access limited to the researcher. The data collected will be destroyed after six
years from the date of the study.
The study volunteers had the right to decide to participate in the research study. The
senior centers provided classroom-type activities where the researcher was given permission to
present the research details to seniors enrolled in high-participation classes. A list of classes was
provided to the researcher at the start of the study. Participants were informed of the researcher’s
presence by the senior citizen center’s personnel.
The senior citizen volunteers were asked to sit through a brief presentation of the study
topic, the objective of the study, the survey requirements, and the process for withdrawing from
the study. The survey was administered after the presentation and the surveys collected during
this time by the researcher. The participants were treated with respect and were guaranteed
confidentiality. The withdrawal process was explained, and the opportunity for any volunteer to
withdraw was honored at any time during the survey administration.
Confidentiality involves the individual’s rights to have control over the use and access of
personal information. Confidentiality also provides the expectation of privacy and protection of
personal information (Marczyk, DeMatteo, & Festinger, 2005). All study volunteers who wish to
withdraw from the survey were treated with respect, their wishes honored, and the survey
58
instrument shredded. The volunteers were required to state their preference to withdraw, the
survey instrument was shredded upon notification, and the participant was excused from the
senior citizen class. The survey was not to be part of the data analysis had a participant
withdrawn from the research study.
Confidentiality
All study participants were guaranteed confidentiality, as noted in the Informed Consent
form. The consent form had a signature line, but the information was not part of the final study
results. The hosting of signature forms is in a secure location and protected under lock and key at
the researcher’s home office. Access to the data collected is limited to the researcher.
All study participants were given the opportunity to withdraw from the study at any time.
The Informed Consent form noted that a participant may decline to participate or withdraw from
participation at any time without consequence. The request was honored by the researcher, and
all data collected from the individual asking to withdraw was immediately destroyed.
Geographic Location
The geographic location of the sample was Hunterdon County, New Jersey. Senior
citizens from local senior centers were a sample of the general population. According to the U.S.
Census Bureau, the population in Hunterdon County for 2009 was 130,034 (Hunterdon County
Facts & Figures, 2010). This population size could provide sufficient volunteers for the
generalization of result to the general population.
Data Collection
The dependent variables were consumer satisfaction and communication. The
independent variables were the demographic characteristics (gender, age, education, and race)
and the format of medical records (paper or electronic). Maheu et al. (2001) noted quantitative
59
research requires the research variable be measured numerically and uses closed-ended surveys
to collect data. The data collection process should allow for reliability, validity, responsiveness,
interpretability, and flexibility (Maheu et al., 2001).
The PSQ-18 survey is a validated survey that has been used in previous studies to
measure consumer satisfaction. The modified version of the PSQ-18 was the PSQ-08 for the
purpose of this study. Modification was limited to the removal of questions not applicable to the
objective of this study; no changes in terminology were applicable, and the exact questions were
used from the original PSQ-18 survey.
The survey has been used as a reliable instrument to gather survey responses, interpret
results, and allow for flexibility in distribution. Based on 2,197 respondents, the reliability was r
= 0.75 for general satisfaction as noted in the Rand Report as part of the Internal Consistency
Reliabilities and Correlations between PSQ-III and PSQ-18 subscales (Marshall & Hays, 1994).
Table 1
Variables
Name of Variable
Type of Variable
Construct Operationalization (Survey Items)
Measure of Reliability*
Level of Measurement
Satisfaction Dependent Consumer Satisfaction
Items 7, 8, 9, & 11
Cronbach Interval
Communication Dependent Communication Items 6 & 10 Cronbach Interval
Format Independent Record format Item 5 Factual Nominal
Gender Control Gender Item 1 Factual Nominal
Age Control Age Item 2 Factual Ratio
Education Control Education Item 3 Factual Ordinal
Race Control Race Item 4 Factual Nominal
Note. A measure of reliability will not be computed for the factual material because of the high likelihood that the respondent would answer the same way both times (test-retest reliability). As an example, it is highly likely that if a respondent reports that he is a “man,” then he would be highly likely to provide the same information at a second administration of the survey.
60
The survey used a 5-point Likert scale (5 = Strongly Agree, 1 = Strongly Disagree)
to measure consumer satisfaction based on the format of health record. The analysis used
descriptive statistics. Creswell (2007) noted descriptive statistics assist in summarizing the trends
in the data, provides the understanding of the variation of the scores, and provides insight into
where a score falls in comparison to other scores.
Study Instrument
The study instrument was a cross-sectional survey based on a publicly available and
previously validated questionnaire: the Rand Corporation PSQ-18. The selection of the
questionnaire was on the applicability to the quantitative comparative study and the ease of
administration. The questionnaire was the tool to measure how the consumer perceived his/her
interaction with health care providers, but only the specific sections related to consumer
satisfaction were applicable. See Appendix B for a copy of the survey instrument. Other
instruments available such as the Patient Assessment of Care for Chronic Conditions (PACIC)
were not considered due to the lack of focus on consumer satisfaction. The PSQ-18 specifically
measures consumer satisfaction in the context of interaction with the health care provider.
The PSQ-18 is a shortened version of a 50-item Patient Satisfaction Questionnaire III
developed by Ware, Snyder, and Wright in 1976 (Marshall & Hays, 1994). The PSQ-18 is set up
to measure seven dimensions of medical care satisfaction that include general satisfaction,
technical quality, interpersonal manner, communication, financial aspects, time spent with
doctor, and accessibility and convenience using 18 questions. Only three dimensions of the
questionnaire related to the parameters of the study hence were the basis for the survey
questions. Questions regarding technical quality, financial aspects, and accessibility and
61
convenience of the medical visit were not relevant to the parameters of this study. The PSQ-08
referred to these areas of interest.
The PSQ-18 as a subset of the PSQ has been used in various studies for planning,
administration, and evaluation of health services delivery program (Marshall & Hays, 1994). The
questionnaire is a survey tool to measure patient satisfaction and has gone through several
revisions. The PSQ-08 was appropriate in this study as it provided the questions to measure
consumer attitudes toward the use of EHRs. The questions that related to general satisfaction,
interpersonal manner, communication, and time spent with doctor aligned with the goals of the
quantitative comparative study.
Questions selected from the PSQ-18 were in both the positive and negative form to
account for acquiescent responses. The questions related to the medical services recently
received but were not limited to any specific timeframe. The questions were based on the
consumer’s interaction with their primary health care provider. The survey used a 5-point Likert
scale (5 = Strongly Agree, 1 = Strongly Disagree). The survey also contained questions on
demographics and type of health record used (e.g., paper, electronic, or both).
Study Pilot Testing
McMillan and Schumacher (2010) noted after the questions for a survey have been
written, the survey should be tested to check for bias. Bias can be through the procedures, the
interviewers, or the questions. The PSQ-18 has been used numerous times to measure consumer
satisfaction and has been validated and proven reliable (Bhardwaj et al., 2011; Marshall & Hays,
1994; Vrijhoef et al., 2009). A pilot test was not necessary for the purposes of this study as the
questions selected were directly taken from the PSQ-18 questionnaire, hence previously tested.
62
Validity and Reliability
Chaloupke (2007) stated statistical “precision of measurement of any kind of
phenomenon has two aspects: reliability and validity” (p. 1295). Powell (2006) defined reliability
as the degree in which an instrument can consistently and accurately repeat results in each use
where validity is the degree in which the instrument does what it is supposed to do. Maheu et al.
(2001) added the determination of internal validity is the data collection process. Issues with
internal validity relate to research bias and problems with sample population.
To maximize the internal validity of the study, different study designs and strict control
processes need to be in place throughout the research process. External validity relates to the
generalization of study results across population, location, and time. Random sampling,
heterogeneous sampling, population selection that would be generalizable, and long-term
research can be effective to avoid issues with external validity (Maheu et al., 2001).
M. D. Gall, J. P. Gall, and Borg (2006) noted 12 threats to the external validity of a
research study. These include: (a) the extent to which one can generalize from the experimental
sample to a defined population; (b) the extent to which personological variables interact with
treatment variables; (c) explicit description of the experimental treatment; (d) multiple-treatment
interference; (e) Hawthorne effect; (f) novelty and disruption effects; (g) experimenter effect; (h)
pretest sensitization; (i) posttest sensitization; (j) interaction of history and treatment effects; (k)
measurement of the dependent variable; and (l) interaction of time of measurement and treatment
effects. Only three threats are of concern in this study due to this being a single group descriptive
study with all those measurements taken at a point in time:
1. Specifically, the extent to which one can generalize from the sample to a defined population
63
will only be known after the data are gathered. It was hoped that at least 110 senior citizen
volunteers would participate and therefore provide 100% sampling; but due to the respondent’s
right to decline participation, this did not occur.
2. The Hawthorne effect may occur because if respondents know that they are participating in a
research study; this may in some way slant their beliefs and opinions.
3. There is a possibility that the measurement of the dependent variables (consumer satisfaction
and communication) will be slanted in some way due to the possibility of socially desirable
responses. In addition, it is unknown to what extent (if at all) that respondents will answer the
instruments in a truthful manner.
Quantitative studies require validity and reliability in the data-gathering procedures
(Creswell, 2007). As noted by Chaloupek (2007), statistical precision is required for reliability in
the “repeated, different measurement of the same subject produce different result” (p. 1295).
Reliability in measurement is “not necessarily valid, while valid measurements must be reliable”
when conducting a quantitative study (Chaloupek, 2007, p. 1295). The PSQ-18 is a validated
instrument as it has been previously used to measure consumer satisfaction (Marshall & Hays,
1994; Vrijhoef et al., 2009; Bhardwaj et al. 2011).
Data Analysis
The survey was a modified version of the PSQ-18; the PSQ-08 used eight questions from
the original survey. The PSQ-08 provided scores for the dimensions selected for this study. The
dimensions and corresponding questions are General Satisfaction, Interpersonal Manner,
Communication, and Time Spent with Doctor. The positive-worded questions reflect satisfaction
in which the negative-worded questions reflect dissatisfaction with medical care. The data
64
analysis will ignore questions with missing data, so that scale score is an average of the questions
answered (Marshall & Hays, 1994).
The data was analyzed using standard summary statistics to include means, standard
deviations, lowest scores, highest scores, and Cronbach’s Alpha for reliability. As shown in
Table 2, Research Questions 1 and 2 were analyzed using one way analysis of variance
(ANOVA) test and accompanying eta coefficient. For Research Questions 3 and 4, standard
multiple models were created. The data were also analyzed using one way ANOVA and eta
coefficients. The dependent variables were satisfaction (survey items 7, 8, 9, and 11 through 13)
and communication (survey items 6 and 10). The independent variables were the demographic
characteristics (gender, age, education, and race) and the format of medical records (paper or
electronic). The hypotheses were confirmed through multiple regression prediction equations.
Research questions 1 and 2 plus the related null hypothesis were addressed using one way
ANOVA and eta coefficient. The research questions 3 and 4 plus related null hypothesis were
addressed using standard multiple regression. The primary independent variables were the record
format (electronic versus paper) and communication with the four demographic characteristics
used as control variables. This type of model was selected to determine the maximum possible
variance to be explained.
One-Factor ANOVA is used when comparing the means of three or more independent
groups. A single-factor ANOVA assessed any differences in degree in the use of EHRs based on
participant demographic characteristics, such as age, race, education level, or gender. Eta is a
coefficient of nonlinear association. The eta coefficient assessed the correlation between the type
of health record and amount of satisfaction.

65
Regression and correlation analysis allows for the estimate of one variable based on
another. Steinberg (2008) noted “a correlation coefficient tells us about the relationship between
variables, but it does not tell us which variable, if either, caused the relationship” (p. 419). Black
(1999) stated correlations are” based on a single sample and provide an indication of the strength
of the relationship between these variables” (p. 618). Due to the constraints of the sample and the
relationship, there are limitations to what can be inferred (Black, 1999). The limitations are
based on not being able to infer if each variable is influenced by the other. Questions 3 and 4
plus the null hypotheses were analyzed using standard multiple regression.
Table 2
Proposed Data Analysis Plan
______________________________________________________________________________
Research Question Survey Item Numbers
Statistical Test (s)
Test Related Null Hypothesis
RQ1: What is the relationship between the format of the health record (paper versus electronic versus both) and the consumer satisfaction with care received?
Record Format (item 5), Satisfaction, (items 7, 8, 9, & 11-13)
One way ANOVA, eta coefficient
F, η2 H10: There is no
significant relationship between the health record format in paper, electronic or both and consumer satisfaction with communication and care received. .
RQ2: What is the relationship between the format of the health record used (paper versus electronic versus both) and the level of satisfaction with communication between health care provider and consumer?
Record Format (item 5), Communication (items 6 & 10)
One way ANOVA, eta coefficient
F, η2 H20: There is no
significant relationship between the health record format in paper, electronic or both and level of communication between health provider and consumer.

66
RQ3: After controlling for consumer demographic characteristics (gender, age, education, and race) what is the relationship between the format of the health record (paper versus electronic versus both) and the consumer satisfaction?
Gender, Age, Education, Race (items 1 – 4) Record Format (item 5) Satisfaction (items 7, 8, 9, & 11)
Standard Multiple Regression
F, R2 H30: There is no
significant relationship between the health record format in paper, electronic or both based on demographic characteristic (gender, age, education, and race) and consumer satisfaction.
RQ4: After controlling for consumer demographic characteristics (gender, age, education, and race), what is the relationship between the format of the health record (paper versus electronic versus both) and effect on communication?
Gender, Age, Education, Race (items 1 – 4) Record Format (item 5) Satisfaction (items 6 & 10)
Standard Multiple Regression
F, R2 H40: There is no
significant relationship between the health record format in paper, electronic or both based on demographic characteristic (gender, age, education, and race) and the level of communication.
Note. For all test p < .05 is the chosen level of Statistical Significance.
The reporting of the data were through tables for a visual representation. The
analysis of the data obtained from the survey instrument was done using the Statistical Package
for the Social Sciences (SPSS) tool.
Chapter Conclusion
Quantitative comparative research measures attitudes toward a particular topic, allows a
direct comparison between paper copy and electronic health records and how the format may
affect communication and consumer satisfaction. Chapter 3 described the research method and
67
design for the quantitative comparative study on the consumer’s view on the implementation of
EHR systems. The discussion included the appropriateness of the research approach. To
accomplish the goals of the study, the sample population was senior citizens in Hunterdon
County, New Jersey, attained through a convenience sampling. The survey instrument used the
PSQ-08 questions that allowed the measurement of consumer’s view on health care provider-
consumer interaction, the use of medical records and technology, as well as the ease of use of
EHRs. The PSQ-18 questionnaire has been utilized previously in studies for the use of medical
records, patient satisfaction, and communication (Bhardwaj et al., 2011; Marshall & Hays, 1994;
Vrijhoef et al., 2009). The PSQ-08 survey was modified to use specific questions to meet the
objectives of this study.
Summary
The next chapter will present the findings and data analysis of the consumer views on
how consumers perceive their interaction with health care providers and how the format of health
records may affect the health care provider-consumer dynamic. Chapter 4 will present the details
of the quantitative comparative study, the data collection process, and data analysis procedures.
68
Chapter 4: Results
Chapter 4 contains the analysis of the data gathered through this research study. The
purpose of this quantitative comparative research study was to ascertain, if statistically
significant, differences existed between the format of health records (electronic versus paper)
and the level of consumer satisfaction with care provided and communication with provider. The
study used data focused on satisfaction and communication utilizing the PSQ-08, Electronic
Health Records Survey.
The first three chapters provided the overview of the research study, the literature review,
and the research method as they applied to the purpose of this quantitative comparative research
study. Chapter 4 provides the demographics of the participants, data analysis procedure, and
presentation of findings. The conclusion of Chapter 4 will summarize these concepts and
introduce Chapter 5.
Demographics
The introduction and informed consent forms were distributed to (n=110) study
participants. Data was collected using a cross-sectional survey. Of the 110, (n=80) returned the
signed informed consent and a group of (n=77) responded to the PSQ-08. The final sample size
of respondents (n=77) was the core group for the data analysis.
Data Collection
This section describes the data collection procedure for this quantitative comparative
research study. Data collection and analysis began after the Academic and Internal Review
Boards of the University of Phoenix approved the current research study. The PSQ-08 survey
instrument was used to gather research data. The PSQ-08 specifically measures consumer
satisfaction in the context of interaction with the health care provider.
69
The PSQ-08 based on the PSQ-18 used is a well-established, approved, and tested survey
instrument. A pilot study was not conducted, as the PSQ-18 has been used numerous times to
measure consumer satisfaction. The PSQ-08 used 8 of the original 18 questions used in the PSQ-
18. Topics discussed were data collection methods, recruitment, and planning and procedure.
Additionally, data analysis was discussed.
The quantitative method was a comparative research design. This current research study
did not statistically identify a relationship between health record format and the consumer
satisfaction with care received. The results of the one way ANOVA test for satisfaction showed
no significant difference between the groups (F (3, 73) = 0.73, p = .49, reference Table 5). The
covariance model predicting consumer satisfaction based on demographic characteristics was not
significant (F (5, 71) = 0.72, p = .61, reference Table 8). This current research study also did not
statistically identify a relationship between health record format and the effect on communication
between health care provide and consumer. The results of the one way ANOVA test for
communication showed no significant difference between the groups (F (3, 73) = 1.79, p = .18,
reference Table 6).The covariance model predicting consumer communication based on
demographic characteristics was not significant (F (5, 71) = 2.08, p = .08, reference Table 10).
The chosen level of significance for all tests was p < .05.
Recruitment
In compliance with the regulations of the IRB, all participants were made aware of the
purpose of the research study, risks, and benefits in participating in this research study.
Participants were informed of the possible benefit of contributing to the knowledge base of
leadership and the implementation of electronic health records. The random selection of
volunteers from high participation classes at the Hunterdon County Senior Center was the

70
approach used to obtain the sample population. The Director of Senior Center Activities
provided a calendar and highlighted high participation classes where there would be a greater
potential for volunteers. A date and time were arranged for access to the various classes, and
team leaders were informed of the procedure for recruiting volunteers. The Informed Consent
forms and survey instrument were distributed on a predetermined date, time, and class schedule.
Planning and Procedure
The Informed Consent forms advised participants of the purpose of the research study
and addressed the risks and benefits in participating in this study. The Informed Consent forms
and the survey instrument were initially distributed to the Hunterdon County Senior Center
Division Head and the Director of Senior Center Activities for their review. A planning meeting
was scheduled two weeks prior to distribution to the members of the Hunterdon County Senior
Center.
The planning meeting addressed the procedure for survey distribution to include a brief
introduction at the beginning of each class by the team leader, recruitment of volunteers, and
requirement for survey distribution to be conducted after the classes were concluded. A calendar
of classes was provided with a list of classes that would provide the greatest possible number of
volunteers. The date was set for survey distribution, and a point of contact was established.
The survey collection time spanned two weeks. Participants were advised that personal
identifying information would be kept confidential. Participants were also advised of their right
to withdraw from the study at any point either before, during, or after survey distribution. The
process to withdraw from the study was included in the Informed Consent form.
Participants who wished to withdraw before, during, or after data collection was
completed could initiate the withdrawal process by contacting the researcher in person, by

71
cellphone, or by email. Upon notification, the collection of information from the participant to
identify data collected would be destroyed from the assessment results.
The participant received a package that included two copies of the Informed Consent
form (Appendix A) and the survey instrument (Appendix B). Participants were instructed to sign
one copy of the Informed Consent form and return to the researcher, and the other copy was for
their records. The package was numbered sequentially so that if needed, the survey can be
tracked to the Informed Consent form. Only signed Consent Forms and associated surveys were
considered for final data analysis.
The signed Consent Forms are locked in a filing cabinet in the researcher’s home. The
data collected will be destroyed after six years from the date of the completion and study to be
accepted. Participants’ confidential information that is limited to a signature was not disclosed
for any data-reporting purposes. The participants’ copy of the Informed Consent form provided
the researcher’s contact information to include cellphone number and email address.
Data Analysis Procedures
The research questions described in Chapter 3 guided this quantitative comparative
research study that determined the relationship between health record format, consumer
satisfaction, and the impact on communication. The data collection transpired as described in the
Nature of the Study section in Chapter 1 and the method section in Chapter 3. The analysis of the
data obtained from the survey instrument was done using the SPSS tool.
The data were analyzed using standard psychometric characteristics for the dependent
variables, and frequency counts for the independent variables. Research Questions 1 and 2 were
analyzed using one way ANOVA test and accompanying eta coefficients. For Research
Questions 3 and 4, analysis of covariance models was created.
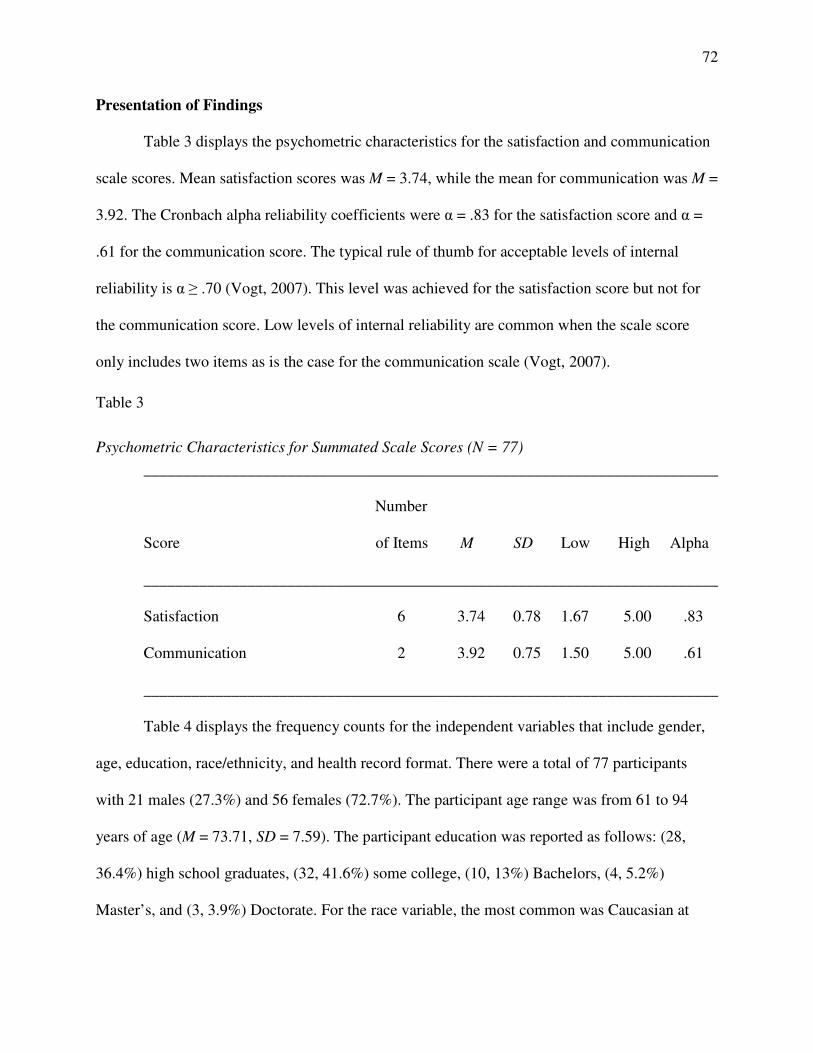
72
Presentation of Findings
Table 3 displays the psychometric characteristics for the satisfaction and communication
scale scores. Mean satisfaction scores was M = 3.74, while the mean for communication was M =
3.92. The Cronbach alpha reliability coefficients were α = .83 for the satisfaction score and α =
.61 for the communication score. The typical rule of thumb for acceptable levels of internal
reliability is α ≥ .70 (Vogt, 2007). This level was achieved for the satisfaction score but not for
the communication score. Low levels of internal reliability are common when the scale score
only includes two items as is the case for the communication scale (Vogt, 2007).
Table 3
Psychometric Characteristics for Summated Scale Scores (N = 77)
________________________________________________________________________
Number
Score of Items M SD Low High Alpha
________________________________________________________________________
Satisfaction 6 3.74 0.78 1.67 5.00 .83
Communication 2 3.92 0.75 1.50 5.00 .61
________________________________________________________________________
Table 4 displays the frequency counts for the independent variables that include gender,
age, education, race/ethnicity, and health record format. There were a total of 77 participants
with 21 males (27.3%) and 56 females (72.7%). The participant age range was from 61 to 94
years of age (M = 73.71, SD = 7.59). The participant education was reported as follows: (28,
36.4%) high school graduates, (32, 41.6%) some college, (10, 13%) Bachelors, (4, 5.2%)
Master’s, and (3, 3.9%) Doctorate. For the race variable, the most common was Caucasian at

73
94.8%, 3.9% Hispanic, and 1.3% Asia Pacific Islander. The health record format in paper was
11.7%, the electronic format was 49.4%, and doctors using both were 39%.
Table 4
Frequency Counts for Selected Variables (N = 77)
________________________________________________________________________
Variable Category n %
________________________________________________________________________
Gender
Male 21 27.3
Female 56 72.7
Age a
61 - 64 7 9.1
65 - 69 21 27.3
70 - 74 18 23.4
75 - 79 12 15.6
80 - 94 19 24.7
Education
High school 28 36.4
Some college 32 41.6
Bachelors 10 13.0
Masters 4 5.2
Doctorate 3 3.9
Race/Ethnicity
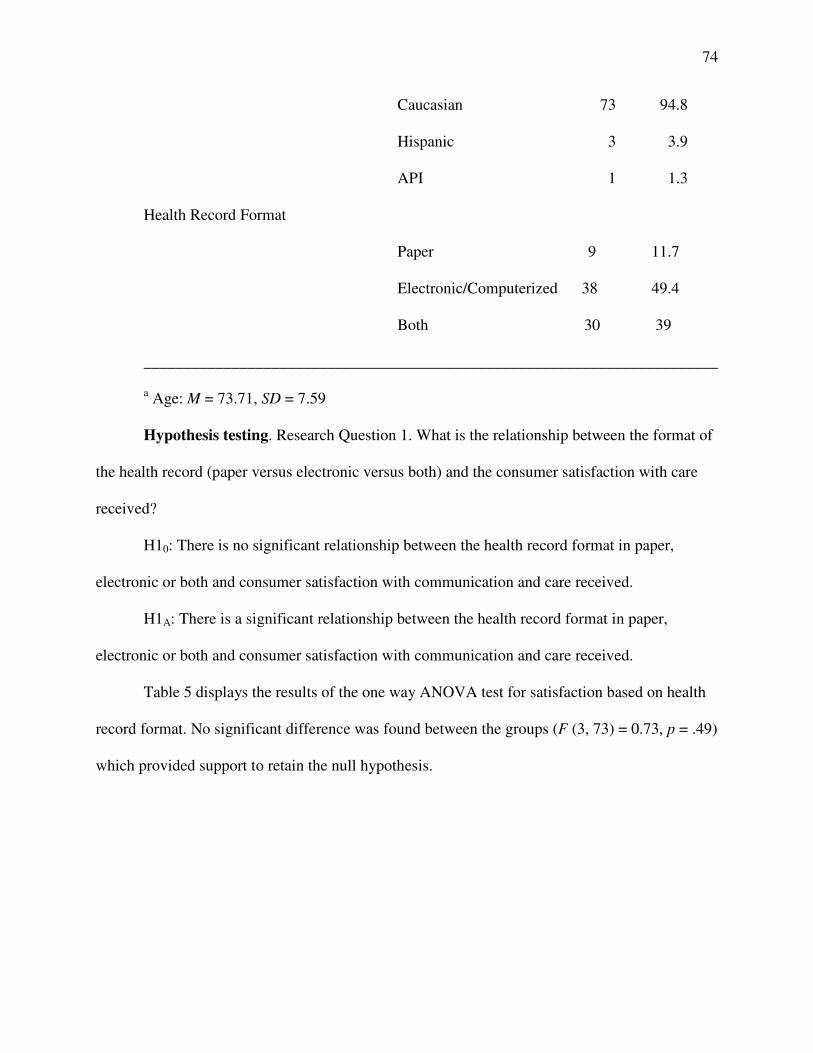
74
Caucasian 73 94.8
Hispanic 3 3.9
API 1 1.3
Health Record Format
Paper 9 11.7
Electronic/Computerized 38 49.4
Both 30 39
________________________________________________________________________
a Age: M = 73.71, SD = 7.59
Hypothesis testing. Research Question 1. What is the relationship between the format of
the health record (paper versus electronic versus both) and the consumer satisfaction with care
received?
H10: There is no significant relationship between the health record format in paper,
electronic or both and consumer satisfaction with communication and care received.
H1A: There is a significant relationship between the health record format in paper,
electronic or both and consumer satisfaction with communication and care received.
Table 5 displays the results of the one way ANOVA test for satisfaction based on health
record format. No significant difference was found between the groups (F (3, 73) = 0.73, p = .49)
which provided support to retain the null hypothesis.

75
Table 5
Comparison Satisfaction Ratings (N = 77)
________________________________________________________________________
Rating Format n M SD Eta F p
________________________________________________________________________
Satisfaction .02 0.73 .49
Paper 9 3.46 1.25
Electronic/ Computerized 38 3.75 0.77 Both 30 3.82 0.62
________________________________________________________________________
Note. Ratings based on a five-point metric: 1 = Strongly Disagree to 5 = Strongly Agree.
Research Question 2: What is the relationship between the format of the health record
used (paper versus electronic versus both) and the level of satisfaction with communication
between health care provider and consumer?
H20: There is no significant relationship between the health record format in paper,
electronic or both and level of communication between health provider and consumer.
H2A: There is a significant relationship between the health record format in paper,
electronic or both and level of communication between health provider and consumer.
Table 6 displays the results of the one way ANOVA test for communication based on
health record format. No significant difference was found between the groups (F (3, 73) = 1.79, p
= .18) which provided support to retain the null hypothesis.
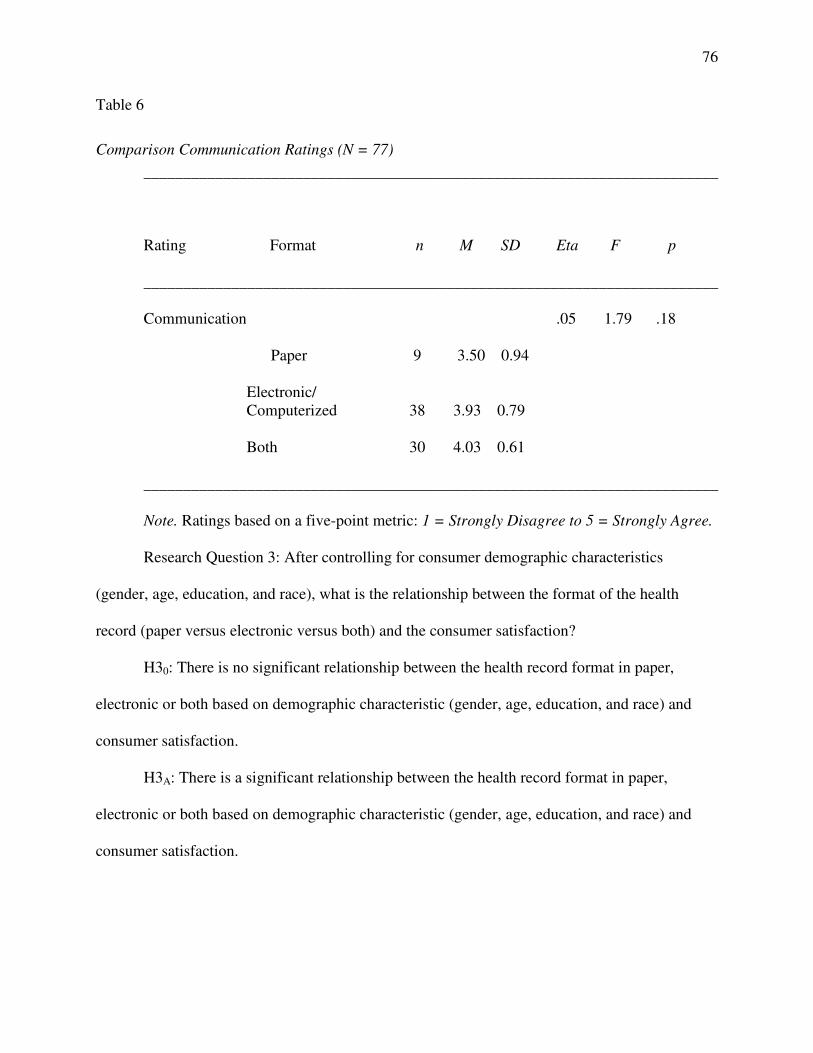
76
Table 6
Comparison Communication Ratings (N = 77)
________________________________________________________________________
Rating Format n M SD Eta F p
________________________________________________________________________
Communication .05 1.79 .18
Paper 9 3.50 0.94
Electronic/ Computerized 38 3.93 0.79
Both 30 4.03 0.61
________________________________________________________________________
Note. Ratings based on a five-point metric: 1 = Strongly Disagree to 5 = Strongly Agree.
Research Question 3: After controlling for consumer demographic characteristics
(gender, age, education, and race), what is the relationship between the format of the health
record (paper versus electronic versus both) and the consumer satisfaction?
H30: There is no significant relationship between the health record format in paper,
electronic or both based on demographic characteristic (gender, age, education, and race) and
consumer satisfaction.
H3A: There is a significant relationship between the health record format in paper,
electronic or both based on demographic characteristic (gender, age, education, and race) and
consumer satisfaction.
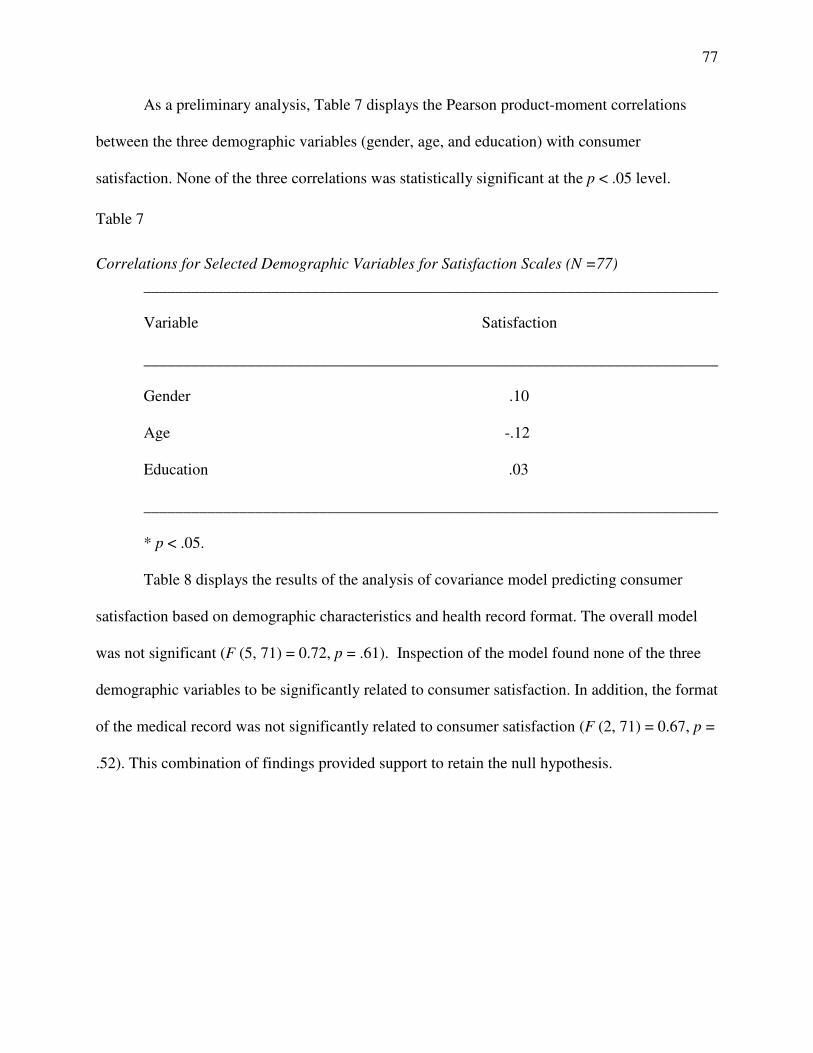
77
As a preliminary analysis, Table 7 displays the Pearson product-moment correlations
between the three demographic variables (gender, age, and education) with consumer
satisfaction. None of the three correlations was statistically significant at the p < .05 level.
Table 7
Correlations for Selected Demographic Variables for Satisfaction Scales (N =77)
________________________________________________________________________
Variable Satisfaction
________________________________________________________________________
Gender .10
Age -.12
Education .03
________________________________________________________________________
* p < .05.
Table 8 displays the results of the analysis of covariance model predicting consumer
satisfaction based on demographic characteristics and health record format. The overall model
was not significant (F (5, 71) = 0.72, p = .61). Inspection of the model found none of the three
demographic variables to be significantly related to consumer satisfaction. In addition, the format
of the medical record was not significantly related to consumer satisfaction (F (2, 71) = 0.67, p =
.52). This combination of findings provided support to retain the null hypothesis.
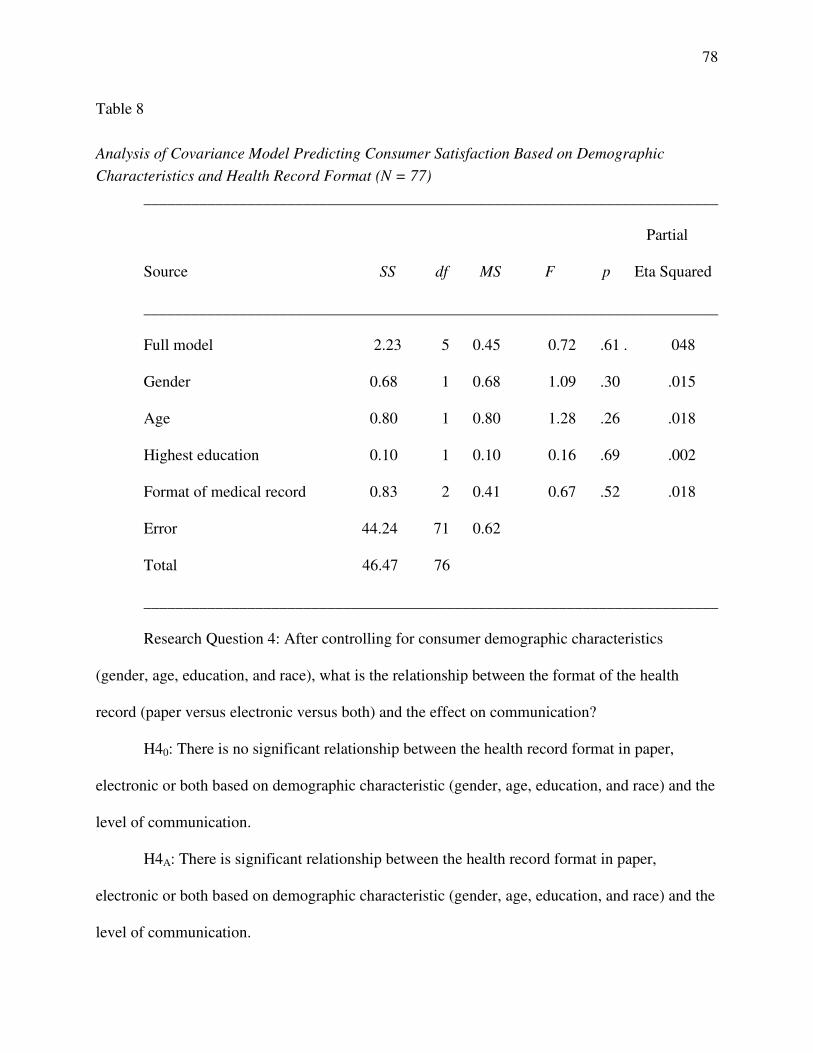
78
Table 8
Analysis of Covariance Model Predicting Consumer Satisfaction Based on Demographic
Characteristics and Health Record Format (N = 77)
________________________________________________________________________
Partial
Source SS df MS F p Eta Squared
________________________________________________________________________
Full model 2.23 5 0.45 0.72 .61 . 048
Gender 0.68 1 0.68 1.09 .30 .015
Age 0.80 1 0.80 1.28 .26 .018
Highest education 0.10 1 0.10 0.16 .69 .002
Format of medical record 0.83 2 0.41 0.67 .52 .018
Error 44.24 71 0.62
Total 46.47 76
________________________________________________________________________
Research Question 4: After controlling for consumer demographic characteristics
(gender, age, education, and race), what is the relationship between the format of the health
record (paper versus electronic versus both) and the effect on communication?
H40: There is no significant relationship between the health record format in paper,
electronic or both based on demographic characteristic (gender, age, education, and race) and the
level of communication.
H4A: There is significant relationship between the health record format in paper,
electronic or both based on demographic characteristic (gender, age, education, and race) and the
level of communication.
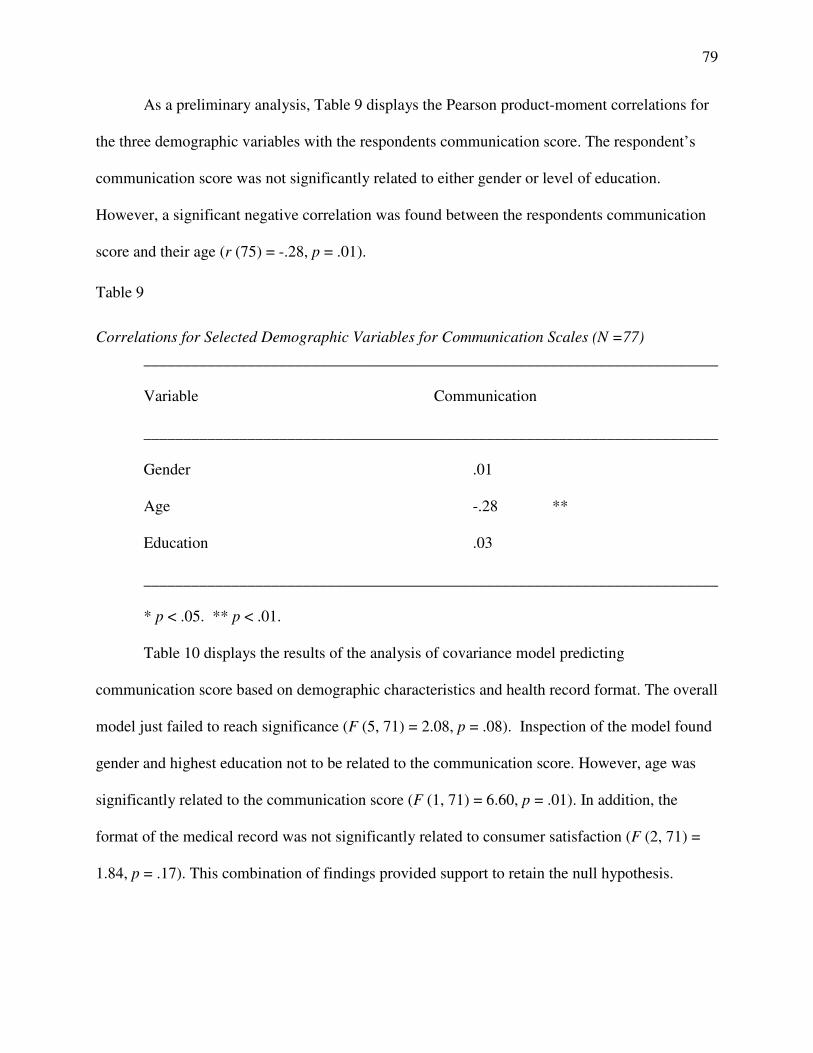
79
As a preliminary analysis, Table 9 displays the Pearson product-moment correlations for
the three demographic variables with the respondents communication score. The respondent’s
communication score was not significantly related to either gender or level of education.
However, a significant negative correlation was found between the respondents communication
score and their age (r (75) = -.28, p = .01).
Table 9
Correlations for Selected Demographic Variables for Communication Scales (N =77)
________________________________________________________________________
Variable Communication
________________________________________________________________________
Gender .01
Age -.28 **
Education .03
________________________________________________________________________
* p < .05. ** p < .01.
Table 10 displays the results of the analysis of covariance model predicting
communication score based on demographic characteristics and health record format. The overall
model just failed to reach significance (F (5, 71) = 2.08, p = .08). Inspection of the model found
gender and highest education not to be related to the communication score. However, age was
significantly related to the communication score (F (1, 71) = 6.60, p = .01). In addition, the
format of the medical record was not significantly related to consumer satisfaction (F (2, 71) =
1.84, p = .17). This combination of findings provided support to retain the null hypothesis.
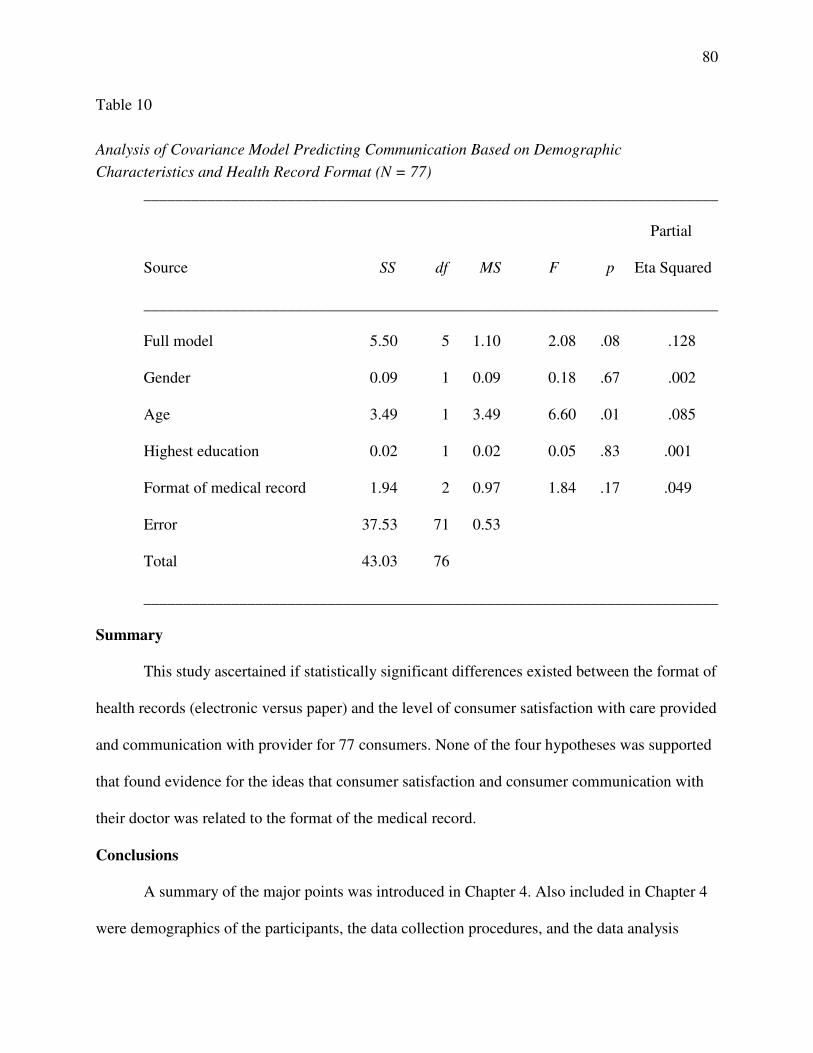
80
Table 10
Analysis of Covariance Model Predicting Communication Based on Demographic
Characteristics and Health Record Format (N = 77)
________________________________________________________________________
Partial
Source SS df MS F p Eta Squared
________________________________________________________________________
Full model 5.50 5 1.10 2.08 .08 .128
Gender 0.09 1 0.09 0.18 .67 .002
Age 3.49 1 3.49 6.60 .01 .085
Highest education 0.02 1 0.02 0.05 .83 .001
Format of medical record 1.94 2 0.97 1.84 .17 .049
Error 37.53 71 0.53
Total 43.03 76
________________________________________________________________________
Summary
This study ascertained if statistically significant differences existed between the format of
health records (electronic versus paper) and the level of consumer satisfaction with care provided
and communication with provider for 77 consumers. None of the four hypotheses was supported
that found evidence for the ideas that consumer satisfaction and consumer communication with
their doctor was related to the format of the medical record.
Conclusions
A summary of the major points was introduced in Chapter 4. Also included in Chapter 4
were demographics of the participants, the data collection procedures, and the data analysis
81
results. These results were presented in tables and included a summary of results. Study
limitations, assumptions, findings, and interpretation are presented in Chapter 5. Included in
Chapter 5 are recommendations for leadership actions, suggestions for future studies, summary
of results, and a conclusion.
82
Chapter 5: Conclusions and Recommendations
The central problem investigated in this research study is the format of health record used
and consumer satisfaction with care provided as well as the effect on communication with
provider. The purpose of this current research was to ascertain if statistically significant
differences existed between the format of health records (electronic versus paper) and the level
of consumer satisfaction with care provided and communication with provider.
The quantitative comparative method served as the framework for gathering, analyzing,
synthesizing, and evaluating the participant’s response. The relationship between the health
record format, consumer satisfaction, and communication in the studied population did not
confirm the relationship between health record format and consumer satisfaction or
communication improvement.
Chapter 5 contains the findings, implications, and recommendations for leadership
implementation and actions based on the research findings. Recommendations and suggestions
for further research based on the results of the research study are presented. The researcher’s
reflections are discussed, and a summary is presented.
Limitations
Limitations previously identified in this research study applied as the study progressed.
The sample population was based on senior citizens enrolled in the Hunterdon County Senior
Center and did not include other regions, age groups, non-English-speaking individuals, or other
organizational forms. This limitation may not give a full perspective of participants or provide a
generalizability of the entire population (Gall et al., 2006; Salkind, 2008).
The expected sample size was between 110 - 115 based on the calculation suggested by
Tabachnick and Fidell (2006), but only 77 responses contributed toward the final data analysis
83
and findings. The data gathered may not represent the full scope of experiences related to the
EHR use and implementation. The concern of the extent one can generalize from the sample was
not known until the data was gathered (M. D. Gall et al., 2006).
Other limitations included that of the human subject behavior or the Hawthorne effect.
Some participants may have slanted their beliefs and opinions due to the possibility of socially
desirable responses (M. D. Gall et al., 2006; Tabatchnick & Fidell, 2006). Some of these
limitations may be addressed by expanding the sample population and changing the research
design.
Sample
The sample in the current research study is a convenience sample limited by time and
finances. If these limitations were removed, then the options could be expanded for further
research considerations. The sample population could be expanded to include a broader range of
age groups and include regions outside of Hunterdon County, New Jersey. Another consideration
for a sample population may be employed individuals or college students, as the sample
population for this current research study was limited to individuals over 60 years of age. The
members of the Hunterdon County Senior Centers were all retired individuals, which may not
provide a diverse perspective on the implementation of electronic health records.
Assumptions
Assumptions identified for this research study included that the sample population has
knowledge of the implementation of health records, physicians will have one form of health
records, consumers have access to information, and consumers will be honest in their responses
to the survey questions. Cooper and Schindler (2010) noted that research designs are subject to
factors beyond the control of the researcher. The assumptions could have led to the introduction
84
of errors into the study to skew the study results. These errors could cause concerns regarding the
reliability or applicability of the current research study within and outside of the sample
population used in this study.
Findings
Researchers suggested a top benefit in the EHR implementation was communication
improvement (Alkayid, Hasan, & Meloche, 2009; DesRoches et al., 2008; Yoon-Flannery et al.,
2008, Zandieh et al., 2008;). Research studies based on the format of health records related to
consumer satisfaction vary in results (Bensing et al., 2008; Botin, 2007; Del Piccolo et al., 2008;
Elleuch, 2008). This current research study did not statistically confirm the relationship between
health record format and improvement on communication or consumer satisfaction. This was
confirmed by retaining all the null hypotheses.
There are limited studies available that correlate format of health records with consumer
satisfaction and communication. Botin (2007) found the introduction of an electronic health
record system contributed to changes in communication patterns between hospital personnel and
patients. The fourth null hypothesis states that there is no significant relationship between the
health record format in paper, electronic, or both based on demographic characteristic (gender,
age, education, and race) and the level of communication. Based on the Pearson product-moment
correlations, a significant negative correlation was found between the respondent’s
communication score and his/her age. The respondent’s communication score was not
significantly related to either gender or level of education. Further, the analysis of covariance
model predicting communications score found age was significantly related to the
communication score. Inspection of the model found gender and highest education not to be
related to the communication score. The null hypothesis was retained based on the combination

85
of the findings; it is worth noting how age may have an impact on communication when
compared to gender and education of the sample population.
A suggestion for future study is to change the demographic parameters to include college
students, working adults, immigrant workers, as well as non-English-speaking individuals. The
results of the data collected for research questions 3 and 4 based on demographics indicate that
based on age, the communication score is affected. The comparison could be made on how age
could be the indicator for positive or negative effects on communication.
A further suggestion is to compare the communication scores of a diverse demographic
group and compare the age parameter against the gender parameter. Studies have shown a
significant difference in consumer satisfaction where women tend to be more dissatisfied with
care provided when compared to men, while others show no difference (H, Soleimanpour, et al,
2011; Murad et al., 2009; Wessels et al, 2010). Comparison between age groups and gender may
provide more specific data for effect on communication and consumer satisfaction based on
health record format.
Additionally, the research location was a limiting factor, as the population was
predominantly Caucasian and many had some college or degreed education. Although this study
did not show a correlation between education level and consumer satisfaction or effect on
communication, the change in geographic locations may provide additional data for a
comparison based on education and race.
A summary for suggested future study includes:
• Change the demographic parameters to include college students, working adults,
immigrant workers, as well as non-English-speaking individuals.
86
• Compare the communication scores of a diverse demographic group and compare
the age parameter against the gender parameter.
• Add additional regional locations to vary the race and education demographic
parameters.
Conclusions
The current research study results present a focus on the relationship between consumer
satisfaction, communication, and the format of health records. The general question asked was
what is the difference between the format of health record used and the level of consumer
satisfaction with care provided and communication with provider. The research questions also
accounted for consumer demographic characteristics, such as gender, age, education, and race.
None of the four hypotheses supported the ideas that consumer satisfaction and communication
with the doctor was related to the format of medical record.
The study instrument, PSQ-08, focused on satisfaction and communication. As a subset
of the PSQ-18, the survey instrument has been previously used to measure consumer satisfaction
(Marshall & Hays, 1994). Questions related to general satisfaction, interpersonal manner,
communication, and time spent with the doctor provided data collection for communication and
satisfaction as the dependent variables. Based on the data analysis, no relationship was found
between consumer satisfaction and communication depending on the format of health record.
Based on previous research, the challenge to specify consumer satisfaction relying on
health care provided can be based on many variables. The current research study did not provide
a specific question on interaction with the doctor, the technology used, or the understanding of
the benefits. The results of the study are beneficial in understanding how demographic
characteristic may influence study results, such as age showing a negative correlation to the

87
communication score. Further research is suggested to understand the implication of age on
communication based on varying age groups, not just the senior citizen community.
Recommendations
The findings from this research study suggest further research may be needed. The
benefit in using this age group as the sample population in review of the literature did not
specifically measure the senior citizen population and the effect on communication with the
implementation of electronic health records. The senior citizen perspective is important, as this
age group has the greater need for health care due to his or her age and health requirements
(Bodkin & Miaoulis, 2007).
Recommendations for leadership action and future research for understanding consumer
satisfaction and communication include building programs for future practitioners to promote
communication and the understanding of the benefits in using electronic health records. Benefits
such as improved patient care, communication, legal documentation, billing and reimbursement,
as well as research and quality management (Wager et al., 2009). The understanding of benefits
may promote consumer satisfaction (Ventres et al., 2006).
Based on the literature, there are benefits with the implementation of health records, such
as improved patient care, improved communication among practitioners, and enhanced
efficiency (Yoon-Flannery et al., 2008). Other research studies note the effect on communication
based on the implementation of electronic health records, but the results vary (Bensing et al.,
2008; Botin, 2007; Del Piccolo et al., 2008; Elleuch, 2008; Robb & Greenhalgh, 2006).
However, there are limited research studies that correlate consumer satisfaction and effect on
communication based on format of health records. Therefore, future studies should address the
88
factors that contribute to consumer satisfaction with care provided and effect on communication
with health care provider.
Another recommendation is to expand the sample population. The sample population
should include various age groups, employed, unemployed, and immigrant populations to gain
the full perspective on consumer satisfaction and effect on communication. Various
organizational forms, such as sport teams, business organization, care givers, and college
students, should be considered.
A summary of recommendations include:
• Build programs for future practitioners to promote communication and the
understanding of the benefits in using electronic health records. Training, either as
part of the academic curriculum or as part of the residency requirements, could
address how to work with technology and improve communication. Additional
training could address how to build trust by maintaining a caring presence when
technology may be intrusive in the interaction between patient and health care
provider.
• Conduct future studies to address the factors that contribute to consumer
satisfaction with care provided and effect on communication with health care
provider. There may be external factors that were not considered for consumer
satisfaction as part of this study, such as access to web-based information, trust in
technology, managing personal health care records, and benefits in implementing
health care systems as part of the EHR implementation.
• Use a diverse population to include various age groups, employed, unemployed,
and immigrant populations. This can be accomplished by expanding the sample
89
population, the sample demographics, and the regions outside of Hunterdon
County, New Jersey.
Implications and Significance to Leadership
The results of this research study contribute to the literature as previous research studies
are limited to support the relationship between consumer satisfaction and communication based
on the format of health records. There may be many variables that contribute to consumer
satisfaction that were not measured as part of this study. Variables such as interaction with the
doctor, trust in technology, issues with EHR implementations, or lack of understanding with the
benefits of using electronic health records. Future research is suggested to specify what could
affect communication with the health care provider or how consumer satisfaction can be
improved.
The goal of the study was to provide health care and government leadership the
mechanism to gather consumer feedback to implement changes to improve the communication
between consumers and health care leadership. Yoon-Flannery et al. (2008) noted
communications as a benefit in the implementation of EHR, and Andersen et al. (2007) added
the role of public health agencies has expanded in providing leadership in terms of planning
strategic objectives for health care on the national level. The results of this research study
suggest further investigation is required but may be useful in providing training or leadership
consideration for the general population and the implementation of electronic health records.
Summary of suggestions for future research related to leadership implications:
• Research is suggested to specify what could affect communication with the health
care provider or how consumer satisfaction can be improved. Additional research
parameters could include interaction with the doctor, trust in technology, issues
90
with EHR implementations, or lack of understanding with the benefits of using
electronic health records.
• Investigation is suggested in identifying what is required to improve consumer
satisfaction and minimize effects on communication. This may include
communication program development to manage the use of technology as part of
health care services, communication plans on the benefits of the EHR
implementation, or adopt IT best practices, such as project management to
minimize the impact of technology requirements. These requirements could
include training for the health care professionals in using EHR systems as well as
assist in funding the transition between paper systems and electronic health record
systems.
Researcher Reflections
Time and finances were a limiting factor to this research study. A benefit, such as having
more time to visit various facilities other than senior citizen centers, could have provided varying
results. Other locations outside of Hunterdon County, New Jersey, would have also provided
varying perspectives from the sample population.
The research design was also a limiting factor. The quantitative research method was
appropriate for this research study, but the results were limited to a survey form. The benefit in
participant interaction and feedback would have provided varying results. Participants were
willing to share their perspectives with issues, such as insurance coverage changes, physician
relationships, and limitations to health care services. The input was outside of the scope of this
research study but provided input for further future research outside of the implementation of
electronic health records.
91
With changes in health care services, the implications of health care on the general
population can lead to many areas for study. The use of technology as a benefit to consumers is
helpful in integrating paper format records with electronic records systems and could impact
society with the expectations of improved health care. The expectation in the initial phase of this
research was that communication and consumer satisfaction may be affected. The results proved
interesting as a relationship was not established between format of health records and the
satisfaction or communication scores based on the data analysis.
Summary
In summary, there are many challenges with the implementation of electronic health
records. These challenges include system adoption, project management, communication
requirements, and the role of the health care provider in ensuring the patient receives quality care
and relevant information. Many research studies support the implementation of EHRs, and others
explore the challenges with implementation to include effects on communication and consumer
satisfaction (Berner et al., 2005; DesRoches et al., 2008; Earnest et al., 2004; Heart et al., 2009;
Lee & Meuter, 2010; Meinert & Peterson, 2009; Terry et al., 2008). This current research study
added another dimension to this research and debate on the benefits of the EHRs
implementation. The purpose of this research study was to statistically ascertain difference in
consumer satisfaction and effect on communication based on health record format. This was
accomplished through comparison of the data using the quantitative comparative method that
was supported by the results of this study.
92
References
Alkayid, K, Hasan, H., & Meloche, J. A. (2009). Simulating information exchanges to
investigate the utility of public health websites. Transforming Government: People
Process and Policy, 3(3), 271-288. doi:10.1108/09654280810899993
Andersen, R. M., Rice, T. H., & Kominski, G. F. (2007). Changing the U.S. Health Care System
(3rd ed.). San Francisco, CA: Jossey-Bass.
Ayers, D. J., Menachemi, N., Ramamonjiarivelo, Z., Matthews, M., & Brooks, R. G. (2009).
Adoption of electronic records: The role of network effects. Journal of Product & Brand
Management, 18(2), 127-135. doi: 10.1108/10610420910949022
Bensing, J. M., Verheul, W., & van Dulmen, A. M. (2008). Patient anxiety in the medical
encounter. A study of verbal and nonverbal communication in general practice. Health
Education, 108(5), 373-383. doi:10.1108/09654280810899993
Berner, E. S., Detmer, D. E., & Simborg, D. (2005). Will the wave finally break? A brief view of
the adoption of electronic medical records in the United States. Journal of the American
Medical Informatics Association, 12(1), 3–7. Retrieved from ProQuest Health and
Medical Complete online.
Bhardwaj, A. K., Raina, S. K., Bansal, P., & Agnihotri, R. K. (2011). Scoring the medical
outcomes among HIV/AIDS patients attending antiretroviral therapy center at Zonal
Hospital, Hamirpur, using Patient Satisfaction Questionnaire (PSQ-18). Indian Journal of
Sexually Transmitted Diseases, 32(1), 19-22. Retrieved from the EBSCOhost database.
Black, T. R. (1999). Doing quantitative research in the social sciences: An integrated approach
to research design, measurement and statistics. London, England: Sage.
93
Blumethal, D., & Tavenner, M. (2010). The “meaningful use” regulation for electronic health
records. The New England Journal of Medicine, 363(6), 501-504. Retrieved from the
MEDLINE database.
Bodkin, C., & Miaoulis, G. (2007). eHealth information quality and ethics issues: An
exploratory study of consumer perceptions. International Journal of Pharmaceutical and
Healthcare Marketing, 1(1), 27-42. doi:10.1108/17506120710740261
Botin, L. (2007). A phenomenological perspective on clinical communication and interaction:
The case of electronic health records. Journal of Information, Communication & Ethics
in Society, 5(1), 21–32. Retrieved from the Emerald Database.
Camgöz-Akdag, H., & Zineldin, M. (2010). Quality of health care and patient satisfaction: An
exploratory investigation of the 5Qs model at Turkey. Clinical Governance: An
International Journal, 15(2), 92-101. doi:10.1108/14777271011035031
Carlson, L. (2008). Qualitative vs. quantitative research traditions: A needless and useless debate
that hampers advertising and marketing knowledge development. International Journal
of Advertising, 27(4), 660-663. Retrieved from the EBSCOhost database.
Chaloupek, G. (2007). Reliability and Validity. Encyclopedia of Law and Society: American and
Global Perspectives, 3, 1295-1296. Retrieved from Gale Virtual Reference Library.
Cockcroft, S. (2009). A media analysis approach to evaluating health information infrastructure
development. Journal of Systems and Information Technology,11(3),208-229.Retrieved
from the Emerald database.
Colburn, A. (2008). Correlation and causality. The prepared practitioner, 10. Retrieved from
EBSCOhost database.
94
Committee on Ways and Means (2009). Title IV – Health Information Technology for Economic
and Clinical Health Act. Retrieved from http://waysandmeans.house.gov/
Cooper, D. R., & Schindler, P. S. (2010). Business research methods (11th ed.). Boston, MA:
Irwin.
Creswell, J. W. (2007). Educational research: Planning, conducting, and evaluating quantitative
and qualitative research (3nd ed.). Upper Saddle River, NJ: Pearson.
Del Piccolo, L., Mazzi, M. A., Scardoni, S., Gobbi, M., & Zimmerman, C. (2008). A theory-
based proposal to evaluate patient-centred communication in medical consultations: The
Verona Patient-centred Communication Evaluation scale (VR-COPE). Health Education,
108(5), 355-372. doi:10.1108/09654280810899984
DesRoches, C. M., Campbell, E. G., Rao, S. R., Donelan, K., Ferris, T. G., Jha, A., Kaushal, R.,
Levy, D. E., Rosenbaum, S., Shields, A. E., & Blumenthal, D. (2008). Electronic health
records in ambulatory care—A national survey of physicians. The New England Journal
of Medicine, 359(1), 50-60. Retrieved from the MEDLINE database.
Earnest, M. A., Ross, S. E., Wittevrongel, L., Moore, L. A., & Lin, C. T. (2004, Sep/Oct). Use of
a patient-accessible electronic medical record in a practice for congestive heart failure:
Patient and physician experiences. Journal of the American Medical Informatics
Association, 11(5), 410–417. Retrieved from ProQuest database.
Edge, R. S., & Groves, J. R. (2006). Ethics of health care: A guide for clinical practice (3rd ed.).
Clifton Park, NY: Thomson Delmar Learning.
Electronic medical records viewed favorably, but many have privacy concerns (2008).
International Journal of Micrographics & Optical Technology, 26(4), 5. Retrieved from
EBSCOhost database.
95
Elleuch, A. (2008). Patient satisfaction in Japan. International Journal of Health Care Quality
Assurance, 21(7), 692-705. doi:10.1108/09526860810910168
Ervin, N. E., & Berry, M. M. (2006). Community readiness for a computer-based health
information network. Journal of the New York State Nurses Association, 37(1), 5-11.
Retrieved from the EBSCOhost database.
Fisher, B., Bhaynani, V., & Winfield, M. (2009). How patients use access to their full health
records: A qualitative study of patients in general practice. Journal of the Royal Society
of Medicine, 102(12), 539-544. Retrieved from the MEDLINE database.
Gall, M. D., Gall, J. P., & Borg, W. R. (2006). Educational research: An introduction (8th ed..
Boston, MA: Pearson Education, Inc.
Goldberg, M. E. (2003). Correlation, causation, and smoking initiation among youths. Journal of
Advertising Research, 431-440. doi:10.1017/S0021849903030472
Heart, T, O’Reilly, P., Sammon, D., O’Donoghue, J. (2009). Bottom-up or top-down?: A
comparative analysis of electronic health record diffusion in Ireland and Israel. Journal of
Systems and Information Technology, 11(3), 244-268. doi:10.1108/13287260910983623
Hing, E. & Hsiao, C. (2010). Electronic medical record use by office-based physicians and their
practices: United States, 2007. National Health Statistics Reports, 23, 1-12. Retrieved
from http://www.cdc.gov/nchs/data/hestat/emr_ehr/emr_ehr.htm
Hsiao, C., Beatty, P. C., Hing, E. S., Woodwell, D. A., Rechsteiner, E. A., & Sick, J. E. (2009).
Electronic medical record/electronic health record use by office-based physicians: United
States, 2008 and preliminary 2009. NCHS Health E-Stats, 1-4. Retrieved from
http://www.cdc.gov/nchs/data/hestat/emr_ehr/emr_ehr.htm

96
Hunterdon County Facts & Figures (2010). Retrieved from
http://www.co.hunterdon.nj.us/facts.htm
Karsh, B., Beasley, J. W., & Hagenauer, M. E. (2004, September-October). Are electronic
medical records associated with improved perceptions of the quality of medical records,
working conditions, or quality of working life? Behaviour & Information Technology, 23
(5), 327–335. Retrieved from the EBSCOhost database.
Katz, D., & Kahn, R. L. (1978). The social psychology of organizations. Hoboken, NJ: John
Wiley & Sons.
Lanseng, E. J.,, & Andreassen, T. W. (2007). Electronic healthcare: A study of people’s
readiness and attitude toward performing self-diagnosis. International Journal of Service
Industry Management, 18(4), 394-417. doi:10.1108/09564230710778155
Lee, O. F., & Meuter, M. L. (2010). The adoption of technology orientation in healthcare
delivery: Case study of a large-scale hospital and healthcare system’s electronic health
record. International Journal of Pharmaceutical and Healthcare Marketing, 4(4), 355-
374. doi:10.1108/17506121011095209
Maheu, M., Whitten, P., & Allen, A. (2001). E-Health, telehealth, and telemedicine: A guide to
startup and success. San Francisco, CA: Jossey-Bass.
Marczyk, G., DeMatteo, D., & Festinger, D. (2005). Essentials of Research Design and
Methodology. Hoboken, NJ: John Wiley & Sons.
Marshall, G. N., & Hays, R. D. (1994). The patient satisfaction questionnaire short form (PSQ-
18), 1-39. Rand, Santa Monica, CA.
McMillan, J. H., & Schumacher, S. (2010). Research in Education. Evidence-based Inquiry (7th
ed.). Upper Saddle River, NJ: Pearson.
97
Meinert, D. B., & Peterson, D. (2009). Perceived importance of EMR functions and physician
characteristics. Journal of Systems and Information Technology, 11(1), 7-70.
doi:10.1108/13287260910932412
Miller, K. (2008). Organizational communication: Approaches and processes (5th ed.). Mason,
OH: Cengage.
Miller, R. L., & Brewer, J. D. (2003). Comparative analysis is the A-Z of social research.
Retrieved from http://www.credoreference.com/entry/sageuksr/comparative_analysis
Morris, D. (2009). Obama will try to gut Medicare. Human Events, 65(25), 1 & 5. Retrieved
from EBSCOhost database.
Murad, M. H., Gjerde, C. L., Bobula, J., Ostrov, M., & Murad, M. S. (2009). Gender and patient
complaints: Are they related? Quality in Primary Care, 17(5), 351-357. Retrieved from
EBSCOhost database.
Noyes, A. (2009, January 15). Mikulski warns against hasty work on health IT overhaul.
National Journal–-CongressDaily. Retrieved from
http://www.nationaljournal.com/congressdaily/
Ouschan, R., Sweeney, J., & Johnson, L. (2006). Customer empowerment and relationship
outcomes in healthcare consultations. European Journal of Marketing, 40(9/10), 1068-
1086. doi: 10.1108/03090560610681014
Powell, R. (2006). Evaluation research: An overview. Library Trends, 55(1), 102-120. Retrieved
from the EBSCOhost database.
Recovery.gov, Track the Money (n.d.). American Recovery and Reinvestment Act of 2009.
Retrieved from http://www.recovery.gov/About/Pages/The_Act.aspx
98
Rivers, P. A., & Glover, S. H. (2008). Health care competition, strategic mission, and patient
satisfaction: Research model and propositions. Journal of Health Organization and
Management, 22(6), 627-641. doi:10.1108/14777260810916597
Robb, N., & Greenhalgh, T. (2006). “You have to cover up the words of the doctor”: The
mediation of trust in interpreted consultations in primary care. Journal of Health
Organization and Management, 20(5), 434-455. doi:10.1108/14777260610701803
Salkind, N. (2008). Exploring research (7th ed.). Upper Saddle River, NJ: Prentice Hall.
Scott, W. R., & Davis, G. F. (2007). Organizations and organizing: Rational, natural, and open
systems perspectives. Upper Saddle River, NJ: Prentice Hall.
Seeley, B. E. (2009). Introducing a computer-based electronic record: Perceptions of clinicians.
Urologic Nursing, 29(5), 329-352. Retrieved from the EBSCOhost database.
Shank, G. D. (2006). Qualitative research: A personal skills approach (2nd ed.). Upper Saddle
River, NJ: Pearson.
Skurka, M. (2003). Health information management. San Francisco, CA: Jossey-Bass.
Soleimanpour, H., Gholipouri, C., Salarilak, S., Raoufi, P. Vahidi, G., Rouhi, A., Ghafouri, R., &
Soleimanpour, M. (2011). Emergency department patient satisfaction survey in Imam
Reza Hospital, Tabriz, Iran. International Journal of Emergency Medicine, 4(1), 1-7.
doi:10.1186/1865-1380-4-2
Sox, H. (2010). Comparative effectiveness research: A progress report. Annals of Internal
Medicine, 153(7), 469-472. Retrieved from the EBSCOhost database.
Steinberg, W. J. (2008). Statistics alive! Los Angeles, CA: Sage.
99
Stewart, R. F., Kroth, P. J., Schuyler, M., & Bailey, R. (2010). Do electronic health records
affect the patient-psychiatrist relationship? A before and after study of psychiatric
outpatients. BMC Psychiatry, 10(3), 1-10. Retrieved from EBSCOhost database.
Stockdale, R. (2008). Peer-to-peer online communities for people with chronic disease: A
conceptual framework. Journal of Systems and Information Technology, 10(1), 39-55.
doi:10.1108/13287260810876885
Tabachnick, B. G., & Fidell, L. S. (2006). Using Multivariate Statistics (5th ed.). Boston, MA:
Allyn and Bacon.
Tang, P. & Lansky, D. (2005). The missing link: bridging the patient-provider health information
gap. Health Affairs, 24(5), 1290-1295. doi:10.1377/hlthaff.24.5.1290
Terry, A., Thorpe, C. F., Giles, G., Brown, J. B., Harris, S. B., Reid, G. J., Thind, A., & Stewart,
M. (2008). Implementing electronic health records: Key factors in primary care.
Canadian Family Physician, 54(5), 730-736. Retrieved from the MEDLINE database.
U.S. Department of Health & Human Services (n.d.). Health Information Privacy. Retrieved
from http://www.hhs.gov/ocr/privacy/hipaa/understanding/consumers/index.html
U.S. Department of Justice (2003). The Privacy Act of 1974 5 U.S.C. 552a. Retrieved from
http://www.justice.gov/opcl/privstat.htm
Ventres, W., Kooienga, S., Vuckovic, N., Marlin, R., Nygren, P., & Stewart, V. (2006).
Physicians, patients, and the electronic health record: An ethnographic analysis. Annals of
Family Medicine, 4(2), 124-131. doi:10.1370/afm.425
Vogt, W. P. (2007). Quantitative Research Methods for Professionals. Boston, MA: Pearson
Education, Inc.
100
Vrijhoef, H. J .M., Berbee, R., & Steuten, L. M. G., (2009). Quality of integrated chronic care
measured by patient survey: Identification, selection and application of most appropriate
instruments. Health Expectations, (4): 417-429. Retrieved from EBSCOhost database.
Wager, K. A., Lee, F. W., & Glaser, J. P. (2009). Health care information systems: A practical
approach for health care management (2nd ed.). San Francisco, CA: Jossey-Bass.
Wessels, H., de Graeff, A., Wynia, K., de Heus, M., Kruitwagen, C. L., Woltjer, G. T.,
Teunissen, S. C., & Voest E. E. (2010). Gender-related needs and preferences in cancer
care indicate the need for an individualized approach to cancer patients. The Oncologist
[Oncologist], 15(6), 648–655. Retrieved from EBSCOhost database.
Whetstone, M., & Goldsmith, R. (2009). Factors influencing intention to use personal health
records. International Journal of Pharmaceutical and Healthcare Marketing, 3(1), 8-25.
doi:10.1108/17506120910948485
Wiljer, D., Urowitz, S., DeLenardo, C., Eysenbach, G., Harth, T., Pai, H., & Leonard, K. J.
(2008). Patient accessible electronic health records: Exploring recommendations for
successful implementation strategies. Journal of Medical Internet Research, 10(4), e34.
Retrieved from MEDLINE database.
Yoon-Flannery, K., Zandieh, S., Kuperman, G., Langsam, D., Hyman, D., & Kaushal, R. (2008).
A qualitative analysis of an electronic health record (EHR) implementation in an
academic ambulatory setting. Informatics in Primary Care, 277-284. Retrieved from the
EBSCOhost database.
Zandieh, S. O., Yoon-Flannery, K., Kuperman, G. J., Langsam, D. J., Hyman, D., & Kaushal, R.
(2008). Challenges to EHR implementation in electronic-versus paper-based office

101
practices. JGIM: Journal of General Internal Medicine, 23(6), 755-761.
doi:10.1007/s11606-008-0573-5
Zickmund, S. L., Hess, R., Bryce, C. L., McTingue, K., Olshansky, E., Fitzgerald, K., & Fischer,
G. S. (2007). Journal of Internal Medicine, 23(1), 20-26. doi:10.1007/s11606-007-0273-
6

102
Appendix A: Informed Consent Form
103
UNIVERSITY OF PHOENIX
Informed Consent: Participants 18 Years of Age and Older
Dear Survey Participant,
My name is Vivianne Moore and I am a student at the University of Phoenix working on a
Doctor of Management in Organizational Leadership degree. I am conducting a research study
entitled “A Quantitative Comparative Study Measuring Consumer Satisfaction Based on Health
Record Format.” The purpose of the research study is to ascertain if statistically significant
differences exist between paper versus electronic copies of health records as it relates to
communication and consumer satisfaction.
Your participation will involve filling out a short survey. The survey consists of 13
questions and should take approximately 15 minutes of your time. Your participation in this
study is voluntary. If you choose not to participate or to withdraw from the study at any time,
you can do so without penalty or loss of benefit to yourself. The results of the research study
may be published, but your identity will remain confidential and your name will not be disclosed
to any outside party.
In this research, there are no foreseeable risks to you.
Although there may be no direct benefit to you, a possible benefit of your participation is in
providing information regarding the use of health records and how this may affect consumer
satisfaction. The goal of this study through a survey instrument is to correlate the format of
health records (electronic or paper) and how this activity relates to consumer satisfaction and
effect on communication. The results of this study can provide information for communication
104
improvements on the use of medical health records. The results of this study will also contribute
to the literature on the implementation of health records on a national level and to the
comparative effectiveness research (CER) to improve the delivery of health care.
If you have any questions concerning the research study, please call me at 908 553 5302,
and contact me at my email address, [email protected]
As a participant in this study, you should understand the following:
1. You may decline to participate or withdraw from participation at any time without
consequences.
2. Your identity will be kept confidential.
3. Vivianne Moore, the researcher, has thoroughly explained the parameters of the research
study, and all of your questions and concerns have been addressed.
4. If the interviews are recorded, you must grant permission for the researcher, Vivianne
Moore, to digitally record the interview. You understand that the information from the
recorded interviews may be transcribed. The researcher will structure a coding process to
assure that anonymity of your name is protected.
5. Data will be stored in a secure and locked area. The data will be held for a period of six
years, and then destroyed.
6. The research results will be used for publication.
“By signing this form, you acknowledge that you understand the nature of the study, the
potential risks to you as a participant, and the means by which your identity will be kept
confidential. Your signature on this form also indicates that you are 18 years old or older and that
you give your permission to voluntarily serve as a participant in the study described.”

105
Signature of the interviewee _____________________________ Date _____________
Signature of the researcher ______________________________ Date _____________
106
Appendix B: PSQ-08, Electronic Health Records Survey
107
PSQ-08, Electronic Health Records Survey
Dear participants,
You have selected to participate in this study. The purpose of the research study is to
ascertain if statistically significant differences exist between paper versus electronic copies of
health records as it relates to communication and consumer satisfaction.
Your participation is appreciated. The data collected from this study could be
beneficial for government agencies, insurance companies, and health care professionals in
promoting communication, community services, and training toward encouraging consumer
awareness and health care providers’ adoption of electronic health records.
The first five questions of the survey ask demographic questions, and the next eight
questions measure your satisfaction level with the health care received. Please consider your last
visit to your primary physician as your reference point for the questions regarding the interaction
between you and your physician.
Questions:
1. What is your gender?
Male □ Female □
2. How old are you?
______ Years
3. What is your highest level of education completed?
High school □ Some college □ Bachelors □ Masters □ Doctorate □
108
Other □ _____________(please specify)
4. What is your race?
White, non-Hispanic □ African-American □ Hispanic □
Asian-Pacific Islander □ Native American Indian □
Other □ __________ (please specify)
Paper
Computer
5. What format of medical records does your primary health care provider use?
Paper □ Electronic/Computerized □ Both □
The following statements are some things people say about medical care. Please read each one
carefully, keeping in mind the medical care you received in your last visit to the doctor. (If you
have not received care recently, think about what you would expect if you needed care today.)
We are interested in your feelings, good and bad, about the medical care you have received.
How strongly do you AGREE or DISAGREE with each of the following statements?
(Circle One Number on Each Line)
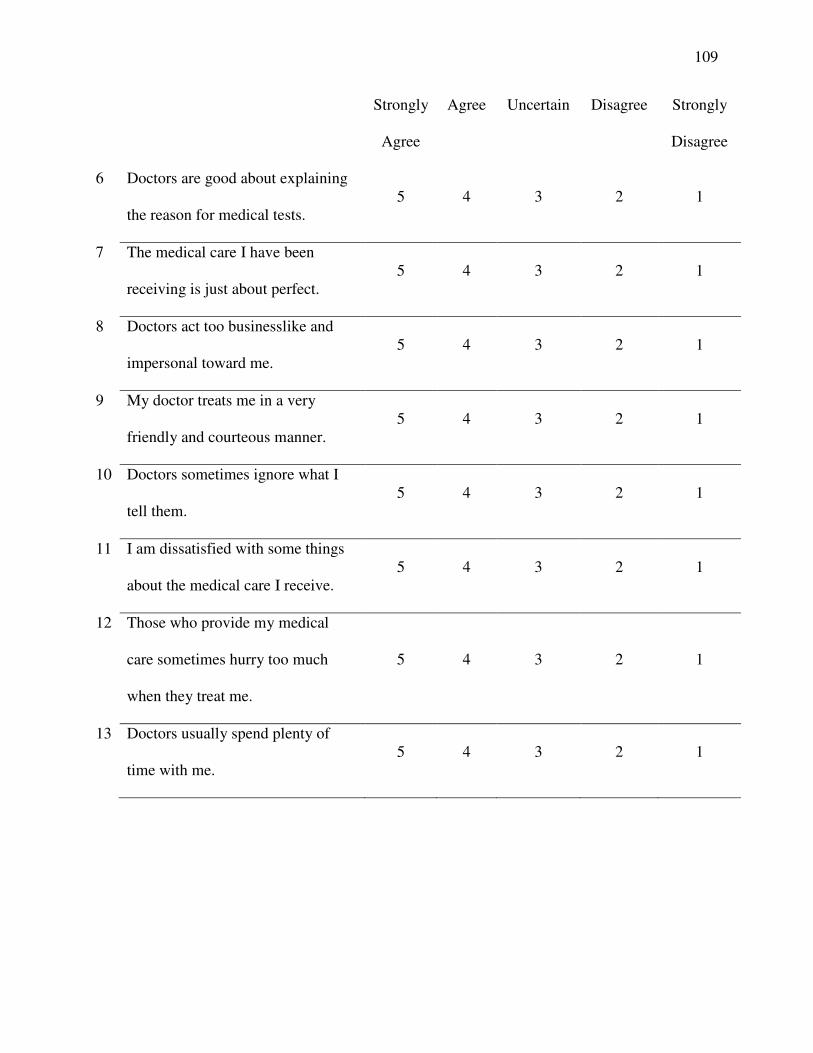
109
Strongly
Agree
Agree Uncertain Disagree Strongly
Disagree
6 Doctors are good about explaining
the reason for medical tests. 5 4 3 2 1
7 The medical care I have been
receiving is just about perfect. 5 4 3 2 1
8 Doctors act too businesslike and
impersonal toward me. 5 4 3 2 1
9 My doctor treats me in a very
friendly and courteous manner. 5 4 3 2 1
10 Doctors sometimes ignore what I
tell them. 5 4 3 2 1
11 I am dissatisfied with some things
about the medical care I receive. 5 4 3 2 1
12 Those who provide my medical
care sometimes hurry too much
when they treat me.
5 4 3 2 1
13 Doctors usually spend plenty of
time with me. 5 4 3 2 1

110
Appendix C: Permission to Use Existing Survey
111

112
Appendix D: Permission to Use Premises, Hunterdon County Senior Center
113

114

115
Appendix E: Permission to Use Premises, North Hunterdon Senior Center

116
117

![Ancient history [by D.M. Masson]....Title Ancient history [by D.M. Masson]. Author David Mather Masson](https://img.pdfslide.us/doc/110x75/60ec6d4334ac5766a325c5a1/ancient-history-by-dm-masson-title-ancient-history-by-dm-masson-author.jpg)