Embed Size (px)
Citation preview

Vol. 42 No. 10 • October 2017 • P&T® 641
A P&T Committee’s Transition to a Complete Electronic Meeting System—A Multisite Institution Experience
Ahmed H. Al-Jedai, PharmD, MBA, BCPS, FCCP, FAST; Roaa A. Algain, PharmD, BCPS, BCACP; Said A. Alghamidi, BSCS; Abdulrazaq S. Al-Jazairi, PharmD, MBA, FCCP, BCPS (AQ-Cardiology);
Rashid Amin, PharmD, BCPS; and Ibrahim Z. Bin Hussain, MD, MBBS, ABCP, FAAP
ABSTRACTPurpose: In the last few decades, changes to formulary
management processes have taken place in institutions with closed formulary systems. However, many P&T committees continued to operate using traditional paper-based systems. Paper-based systems have many limitations, including con-fidentiality, efficiency, open voting, and paper wastage. This becomes more challenging when dealing with a multisite P&T committee that handles formulary matters across the whole health care system. In this paper, we discuss the implementa-tion of the first paperless, completely electronic, Web-based formulary management system across a large health care system in the Middle East.
Summary: We describe the transitioning of a multisite P&T committee in a large tertiary care institution from a paper-based to an all-electronic system. The challenges and limitations of running a multisite P&T committee utilizing a paper system are discussed. The design and development of a Web-based committee floor management application that can be used from notebooks, tablets, and hand-held devices is described. Implementation of a flexible, interactive, easy-to-use, and efficient electronic formulary management system is explained in detail.
Conclusion: The development of an electronic P&T com-mittee meeting system that encompasses electronic document sharing, voting, and communication could help multisite health care systems unify their formularies across multiple sites. Our experience might not be generalizable to all institutions because this depends heavily on system features, existing processes and workflow, and implementation across different sites.
Keywords: formulary management, P&T committee, pharmacy and therapeutics, formulary and therapeutics committee, electronic system, multisite health institution
Dr. Al-Jedai is Director of the Pharmaceutical Care Division, Associate Professor at Alfaisal University’s College of Medicine, and a Consultant Clinical Pharmacist in Solid Organ Transplant in the Pharmaceutical Care Division of King Faisal Specialist Hospital & Research Centre (KFSHRC) in Riyadh, Saudi Arabia. Dr. Algain is Clinical Pharmacy Specialist–Drug Information Center in KFSHRC’s Pharmaceutical Care Division. Said Alghamidi is Head, Applications Development, in Health Information Technology Affairs at KFSHRC. Dr. Al-Jazairi is Deputy Director, Pharmaceutical Care Division, and Clinical Pharmacy Consultant, Cardiology, in KFSHRC’s Pharmaceutical Care Division. Dr. Amin is Clinical Pharmacy Specialist–Critical Care in KFSHRC’s Pharmaceutical Care Division. Dr. Bin Hussain is a Consultant in Pediatric Infectious Diseases in KFSHRC’s Pediatrics Department.
INTRODUCTIONThe history of P&T committees dates back to the first half
of the 20th century.1 The importance of formulary manage-ment is well-recognized by most health care systems around the world.2,3 The World Health Organization encourages each hospital to establish a formulary committee to assume respon-sibility for medication selection, set the institutions’ policies and procedures, and develop the formulary.4,5 In 1965, the Joint Commission on Accreditation of Hospitals mandated that all hospitals establish a P&T committee.3,6 The current Joint Commission Medication Management and Use stan-dards require health care organizations to have written criteria for adding and removing medications from the formulary and to have a process to safeguard the use of nonformulary medications.3
Significant changes to formulary management systems began to take place in the 1980s.7 The early model of the “preferred drug list” (formulary) has evolved from a simple listing of medications into a more comprehensive therapeutic guide. Recent formulary systems aim to implement the rational drug use concept and provide evidence-based prescribing guid-ance. This transition was driven by the continuous increase in medications’ cost and the diversity of disease management. In 2001, the American Society of Health-System Pharmacists (ASHP) set forth guidelines for P&T committees and formulary management that serve as standards of practice for health care institutions around the world.8,9
Our institution is a multisite, multicity, large tertiary/quaternary health care organization. It is considered one of the leading referral centers in Saudi Arabia and consists of three campuses with a total capacity of 1,600 beds.10
The P&T committee was established at our institution in 1975. Similar to other institutions and until recently, the P&T committee operated using a traditional paper-based system, which had many limitations, including but not limited to the following:
• Confidentiality was not guaranteed.• Communication was not efficient.• Voting was open and manual.• A significant amount of paper was wasted by each
member prior to and during the meetings for review and preparation.
These limitations created issues before, during, and after committee meetings. One of the main challenges encountered was peer pressure on committee members during the voting
Disclosures: The authors report no commercial or financial interests in regard to this article.

642 P&T® • October 2017 • Vol. 42 No. 10
process because voting was not blinded. The first step was to implement a blinded voting system using hand-held voting devices in mid-1990. However, this was not practical or sufficient when the health care system at the main campus expanded to include out-of-town sites. It was time to think about adopting an electronic system that could be used simultaneously by all members from different sites during the meeting.
In this paper we discuss the implementation of the first paper-less, completely electronic, Web-based formulary management system across a large health care system in the Middle East.
THE COMMITTEEThe Formulary and Therapeutics Committee (FTC) at our
institution is a corporate-level, decision-making committee that oversees all medication-related issues in the organization. The main objective of this committee is to provide and maintain the most rational and cost-effective armamentarium of medications for the organization. It also serves as an advisory committee to provide independent, unbiased clinical perspective in disease management and therapeutics.
All actions of the committee are referred for endorsement and approval by the Chief Executive Officer (CEO). The committee recommends the adoption of and assists in the formulation of policies, procedures, protocols, and guidelines regarding evaluation, selection, and therapeutic use of drugs in the whole organization. In addition, the FTC recommends and assists in
the formulation of programs designed to meet the continuing needs of the professional staff (physicians, nurses, pharmacists, and other health care practitioners) on matters related to medi-cation and its use. The committee is very similar in structure and function to mainstream P&T committees in the United States as outlined in the ASHP statement.8,9 However, there are minor differences, such as reporting structure. The reporting of the committee to the CEO gives it more administrative power to execute its actions in a short period of time.
In 2010, the P&T committees at each campus of our health care system were amalgamated into one corporate committee and renamed the FTC. The main campus (1,000 beds) and another campus dedicated to pediatric hematology/oncology (75 beds) are located in Riyadh, the capital of Saudi Arabia. A third campus with a 500-bed capacity is located in Jeddah city (750 miles from Riyadh).
The FTC carries the same charges as the former P&T com-mittee at each campus but was further enhanced to adapt to ever-changing pharmaceutical care and technology practices. With the amalgamation of the FTC, its members represent the whole organization with a total of 24 members including the chairman and co-chairman of the committee and one coordinator in each city in addition to the main coordinator. The members represent different specialties from the three campuses and are selected by the committee chairman to form a multidisciplinary team that includes supply chain manage-
A P&T Committee’s Transition to a Complete Electronic Meeting System
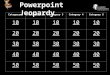
Figure 1 Formulary and Therapeutics Committee Structure
Coordinator (Riyadh)
Automated Dispensing Cabinet Override Task Force
Hepatitis C Medications Task Force
Cancer Therapeutics Subcommittee
Chairman
Antimicrobial Utilization and Evaluation Subcommittee
Chairman
Medication Safety and Utilization Subcommittee
Chairman
Coordinator
Members (18) Members (14) Members (15)
Vaccine Advisory Subcommittee
Chairman
Contrast Media and Radiopharmaceuticals
Subcommittee Chairman
Plasma-Derivative Pharmaceuticals Subcommittee
Chairman
Members (12) Members (12) Members (16)
Coordinator (Jeddah)
Coordinator Coordinator Coordinator Coordinator Coordinator
CEO (or designee)
Formulary and Therapeutics Committee (24 members)
Chairman Co-Chairman
Main Coordinator

Vol. 42 No. 10 • October 2017 • P&T® 643
A P&T Committee’s Transition to a Complete Electronic Meeting System
from all campuses and present recommen-dations to the main committee for final discussion and approval (Figure 1). The FTC has both advisory and educational charges (Table 1).
HANDLING/PROCESSING FORMULARY REQUESTS
Any attending physician may request the addition of a new medication to the hos-pital formulary by submitting the request electronically. All requests from clinicians, including formulary additions, deletions, free samples, and dosage form changes, expansion of indication, or extension of privileges, are processed through another electronic system called the Business Process Manager (BPM). This system contains electronic forms designed by the FTC in collaboration with the information technology (IT) department. Once the com-plete request has been received, it is placed in an electronic queue to be discussed, and the requester is acknowledged. Next, clinical pharmacists prepare independent, evidence-based reviews. The requester is invited to the meeting to summarize the rationale behind his or her request. This is followed by a detailed presentation by the evaluator reviewing the available evidence compared to the formulary alternatives. A cost evaluation comparing formulary and nonformulary alternatives with the requested medication is presented to the FTC members. Deliberation ensues fol-lowed by an anonymous vote; the decision is made in the presence of the requester. All of the previously mentioned steps are per-formed using a fully electronic Web-based formulary management system designed in-house specifically for this purpose.
The decisions from each FTC meeting have to be endorsed and approved by the CEO for final approval. Subsequent to the approval, electronic notification is sent to all of the stakeholders, including medical departments, the pharmaceutical care division, and supply chain manage-ment, using another electronic system called Enterprise Correspondence (EC).
The electronic enterprise system allows the submission of all communications electronically to departments, request-ers, reviewers, and other committee members. This system allows the creation of internal memos with digital signatures, assignment capabilities, and electronic tracking. Both the EC and BPM systems are utilized by the committee to ensure complete automation of the requests and correspondence in a secured, monitored environment.
ment (one member), quality management (one member), nursing (one member), pharmacy (seven members), and medical departments (14 members). The committee has six subcommittees—Cancer Therapeutics, Medication Safety, Vaccine Advisory, Antimicrobial Utilization, Contrast Media and Radiopharmaceuticals, and Plasma-Derivative Pharmaceuticals, and two task forces. The subcommittees are composed of members from specific specialties and operate in the same manner as the main FTC. These subcommittees have members
Table 1 Responsibilities of a Three-Campus, Multisite Formulary and Therapeutics Committee in Riyadh and Jeddah, Saudi Arabia
1. Serve the medical staff and hospital administration in all matters pertaining to the use of drugs (including investigational drugs) in an advisory capacity.
2. Recommend the formulation of policies, protocols, procedures, and guidelines regarding evaluation, selection, and procurement of drugs and approve their use in the organization.
3. Develop, review, and evaluate formulary management policies and procedures.
4. Periodically review and proactively suggest medications for the formulary to maintain the safest, most up-to-date, dynamic formulary system. The selection of items to be included in the formulary will be based on evidence-based evaluation of their respective therapeutic merits, safety, and cost-effectiveness.
5. Establish programs and procedures that ensure cost-effective drug therapy.
6. Organize and participate in educational programs for health care professionals in the organization on matters related to drug use.
7. Participate in quality-management activities related to the distribution, administration, and use of medications.
8. Review periodic medication safety and utilization reports.
9. Review adverse drug reactions in the organization.
10. Initiate drug-use review programs and ensure follow-up of the results.
11. Advise concerned departments regarding implementation of effective drug distribution and control procedures.
12. Recommend drugs to be stocked in the organization’s patient care areas.
13. Develop and/or approve policies, procedures, and guidelines related to the selection, distribution, handling, use, and administration of drugs and diagnostic testing materials.
14. Establish subcommittees and task forces that address specific therapeutic areas.
Table 2 Features Determined Essential for the Internal Development of an Electronic Formulary Management Meeting System
• Must be secure and allow access only to authorized staff during the meeting.
• Must be able to handle the main committee’s and all other subcommittees’ work, including detailed documents and motions.
• Must be very flexible in managing committee and subcommittee members’ details, including adding or deleting members, guests, and their privileges (voting/nonvoting).
• Must be able to schedule committee meetings and send notifications.
• Must be able to handle anonymous voting while generating a unique security key for each meeting and allowing only attending members to vote.
• Should have archiving and report-generating capabilities.
• Must allow chairman or main coordinator to control what meeting members view and when to vote.
• Web application that can be accessed using any operating system or platform.

644 P&T® • October 2017 • Vol. 42 No. 10
A P&T Committee’s Transition to a Complete Electronic Meeting System
DEVELOPMENT OF THE ELECTRONIC FORMULARY MANAGEMENT SYSTEM
Before implementation of the electronic formulary manage-ment system, all committee meeting matters, including floor management of the meeting itself and voting, were handled manually via a paper-based system. An electronic system was deemed necessary to address the shortcomings of a manual one. The system we were looking for needed to be flexible, interactive, easy to use, and efficient. After an extensive search, we concluded that no commercially available product provided the minimum required functionality. Therefore, we decided to internally develop a committee management application tailored to our organization’s needs. We approached our IT department, which assigned an experienced programmer. After several meetings with the programmer, we developed a list of required features (Table 2).
During the development phase, we designed the application with three different interfaces. The first interface was designed for the committee secretarial assistants, who are responsible for adding the committee members and guests, scheduling meet-ings, managing and uploading meeting documents, and entering motions prior to the meeting. The second interface, for standing meeting members, allowed them to view the content of the meeting, including all communications, medication requests, and drug cost evaluations; and to participate in voting using the blinded poll functionality. The last interface was developed for
the hosts of the meeting (the chairman and the main coordinator/secretary), who are respon-sible for managing the floor during the meeting. The chairman/coordinator can perform multiple functions, including but not limited to starting and ending the meeting electronically, publish-ing content and documents to other meeting members, editing and publishing polls (motions), and announcing the results of the voting. The system’s development took six months until the go-live date in 2009. This included the testing, validation, and implementation steps taken by the development group, which included the FTC chairman, coordinator, and IT programmer. To date, the system has had three upgrades with improved functionality, graphical user interface, and bug fixes.
IMPLEMENTATION OF THE ELECTRONIC FTC SYSTEM
There were two initial challenges: making sure that only attending members could view and vote on the motions, and permitting the host to publish content to other members. To overcome the first challenge, we added a security key that is randomly generated when the host starts the meeting. The security key must be entered by each member in order to have full access to the meeting package and motions in the system. The chairman only provides this security key verbally to the attendees during the meeting.
As for the second challenge, we were limited by the Web technologies at that time, as clients could post requests to the server, but servers could not post a request to the client. HTML5 was still under development when this system was implemented, and we could not utilize WebSockets because no browsers supported them then. Therefore, we developed a host–request–queue layer where the host request is stored and all client machines check the request queue every five seconds. When the host publishes a poll, all devices will show the poll within five seconds.
After our institution adopted the use of tablets (e.g., iPads) and after the release of HTML5, we developed an app-like Web interface for tablet users where they can easily employ touch gestures to use the system. We are also in the process of utilizing WebSockets to provide faster client response and add more functionality, such as chatting and electronically requesting permission to speak.
THE ELECTRONIC FORMULARY MANAGEMENT SYSTEM AND MEETING WORKFLOW
The committee assistant schedules a meeting and uploads all attendees’ lists, documents, and motions prior to the meeting. All meetings are conducted via videoconference among all campuses. Each member has an iPad to use during the meeting to view the contents and vote on motions. The link to the electronic formulary management system is available through the organization webpage. The electronic meeting workflow is summarized in Table 3.
Table 3 Meeting Workflow in the Electronic Formulary Management System
• Committee members access the system and log in using their active hospital directory ID and password.
• Main coordinator starts the meeting and verbally provides attendees with the one-time unique security key that is generated automatically.
• Attending members must enter the security key in order to access the active meeting and be able to vote.
• Attendees have different access and privileges depending on their role. For example, guests and requesters can view documents that pertain to their requests, but cannot see other documents or vote.
• Once logged in, attendees can view the meeting documents (e.g., agenda, previous meeting minutes, requests, and evaluations). They can easily navigate the system to see invited guests and their positions and privileges (Figure 2).
• The coordinator can control the electronic system view seen by others, and hence can publish motions and lock the view for voting when necessary.
• After evaluation and discussion, the chairman will call for voting. Polls (motions) will be published, and members can view the motions and voting (Figure 3).
• The chairman and the coordinator can track members’ votes to ensure complete voting for each motion anonymously. However, no one, including the chairman and the coordinator, can see what other members voted on.
• The voting result for each motion will be displayed to all members once voting is completed in the presence of the requester. The results will be displayed as a color-coded pie chart (Figure 4).
• When the meeting is adjourned, the coordinator will end the meeting electronically (Figure 5) and log out all attendees from the system.
• Meeting attendance, motions, and documents are archived permanently in the system and can be accessed for future reporting. All data are backed up off site in the hospital data warehouse.

Vol. 42 No. 10 • October 2017 • P&T® 645
A P&T Committee’s Transition to a Complete Electronic Meeting System
DISCUSSIONThe FTC was first introduced in our country at our institution
in 1975.10,11 Our formulary management committee structure and functions are similar to those reported by the U.S. national survey on hospital formulary management processes conducted by Anagnostis and colleagues in 2011.14 The survey was based on the ASHP guidelines for P&T committees and formulary systems.8,9 Moreover, the extent of formulary system manage-ment techniques used in U.S. hospitals is similar to the activities undertaken by our committee. In our institution, the FTC and its subcommittees conduct an average of 20 meetings per year compared with an average of seven to nine meetings in major U.S. hospitals (more than 400 beds).15,16
Today’s hospital FTCs are faced with advances in informa-tion technologies and the development of multisite health care systems and integrated institutions. Committees have to adapt to the dynamic changes in the medical field and integrate the technology in their processes.
Formulary management has been reported as one of the challenges in multisite health care institutions.17,18 Designing an effective model to standardize the formulary, practices, and policies requires collaboration from each site of the institution. Moreover, the model must ensure effective representation
of practitioners from all sites, timeliness of formulary deci-sions, and effective communication across all practice sites. BeQuette et al. and Reddan et al. described Clarian Health of Indiana’s experience with formulary management system transformation after the integration of a multisite institution.18,19
In 2009, Clarian became a large health care system composed of 11 sites. Clarian (now Indiana University Health) was challenged with coordinating the drug-expenditure budget and maintaining a system-wide consistent formulary management system. As a result, it established a multisite formulary committee, but did not dissolve the individual P&T committee of each hospital. This new multisite formulary committee developed a global formulary for the institution, but its responsibility was limited to formulary decisions, establishment of criteria-based restric-
Figure 2 Meeting Documents View
Figure 3 Members' View During Voting Process
Figure 4 Voting Results View
Figure 5 Meeting Actions Summary View

646 P&T® • October 2017 • Vol. 42 No. 10
A P&T Committee’s Transition to a Complete Electronic Meeting System
tions for use of certain drugs, and related information. However, this model allowed customization of formulary restriction in each hospital, and each P&T committee continued to function independently. In our setting, the health-system administration sought to unify the practice, management, and formulary among all three campuses, so a model such as Clarian’s would not be applicable. To accomplish this goal, we internally developed and established an electronic formulary management system.
We believe this is the first report that describes the imple-mentation of a fully electronic multisite formulary management system. To our knowledge, no published survey or study has described the voting procedure.
During the FTC meetings at our institution, the chairman solicits the views of all members, including the nonvoting members, and gives sufficient time for deliberation before voting takes place. The chairman will not allow any further comments during or after the voting process to avoid any potential influence on the results. Adopting electronic voting by our committee unified the voting procedure and minimized possible bias and interpersonal influences on members’ votes. This model of online and blinded voting is not expected to compromise the integrity of the voting results because all members have equal opportunity to express concerns and request clarifications during the discussion and before the voting takes place. This process is in line with the U.S. Food and Drug Administration’s guidance for voting by its advisory committees’ members.20
Our paperless electronic system received full acceptance by all members, who underwent training before its implementation. As the main committee implemented the system successfully, all subcommittees eventually adopted the same system. The organization’s administration supports and acknowledges this achievement, which has been an important factor in our FTC’s success. We believe that integrating the technology in our FTC’s operation has resulted in many positive outcomes, such as reducing meeting duration and frequency; streamlin-ing meeting communication among campuses; ensuring equal opportunity for each member to view documents, comment, and vote during the meeting; and minimizing conflict about the motions and voting. Before the new system was implemented, for example, the meeting usually lasted more than two hours and, in many instances, ended with agenda items carried over to the next meeting. However, after the implementation of the new system, the meeting time was reduced to 90 minutes.
Our committee annually receives about 120 requests of dif-ferent types (addition, deletion, etc.). This requires frequent meetings, averaging 12 to 14 throughout the year and an average of four to six for each subcommittee. The electronic system has reduced the workload for the secretaries because all documents are uploaded and archived electronically, which also allows the generation of customized reports.
Finally, effective communication of P&T decisions should assure proper implementation of action and compliance. The improvements in the reporting systems and meeting techniques were suggested to enhance the committees’ performance.21
In a recent survey in Canada, P&T committees’ actions were communicated to hospital staff via printed materials (80%), targeted emails to selected staff (61%), intranet (43%), in-service programs (39%), hospital bulletin boards (13%), or other methods (15%).22 In the U.S., most P&T committees
depend on newsletters for communicating their decisions.23
Our FTC communicates all actions via electronic memos through a homegrown Web application to the requester and department chairpersons in all branches. Multiple customized updates that summarize all meeting actions are prepared by the coordinator and sent to different departments, including supply chain management, pharmacy, nursing, or prescribers, in addition to publishing them in the pharmacy newsletter, which is done electronically.
CONCLUSIONThe development of an electronic formulary and therapeu-
tics committee meeting system that encompasses electronic document sharing, voting, and communication could help multisite health care systems unify their formularies across their sites. Our experience might not be generalizable to all institutions because this depends heavily on the system fea-tures, existing processes and workflow, and implementation across different sites.
REFERENCES1. Bernecker EL. Formulary Bellevue Hospital. JAMA
1949;140(2):258. doi: 10.1001/jama.1949.02900370126032.2. Duran-Garcia E, Santos-Ramos B, Puigventos-Latorre F, Ortega A.
Literature review on the structure and operation of pharmacy and therapeutics committees. Int J Clin Pharm 2011;33(3):475–483.
3. Balu S, O’Connor P, Vogenberg FR. Contemporary issues affecting P&T committees. Part 1: the evolution. P T 2004;29;(11):709–711.
4. Schiff GD, Galanter WL, Duhig J, et al. A prescription for improv-ing drug formulary decision making. PLoS Med 2012;9(5):1–7.
5. Holloway K, Green T. Drug and Therapeutics Committees: A Practi-cal Guide. Geneva, Switzerland: World Health Organization; 2003.
6. Perrone J, Nelson LS. Pharmacy and therapeutics committees: leadership opportunities in medication safety for medical toxicolo-gists. J Med Toxicol 2011;7(2):99–102.
7. Green PE. The general practice formulary—its role in rational therapeutics. J R Coll Gen Pract 1985;35(281):570–572.
8. Principles of a sound drug formulary system. In: Hawkins B, ed. Best Practices for Hospital and Health System Pharmacy: Positions and Guidance Documents of ASHP. Bethesda, Maryland: American Society of Health–System Pharmacists; 2011.
9. Tyler LS, Cole SW, May JR, et al. ASHP guidelines on the pharmacy and therapeutics committee and the formulary system. Am J Health Syst Pharm 2008;65(13):1272–1283.
10. Al-Qadheeb NS, Alissa DA, Al-Jedai A, et al. The first inter national residency program accredited by the American Society of Health–System Pharmacists. Am J Pharm Educ 2012;76(10):190.
11. Alsultan MS, Khurshid F, Salamah HJ, et al. Hospital pharmacy practice in Saudi Arabia: prescribing and transcribing in the Riyadh region. Saudi Pharm J 2012;20(3):203–210.
12. Madani KA, Al-Husseini TH. Pharmacy and therapeutics committees in Saudi Arabia [letter]. Am J Hosp Pharm 1990;47(6):1269–1270.
13. Aljadhey H, Alhusan A, Alburikan K, et al. Medication safety prac-tices in hospitals: a national survey in Saudi Arabia. Saudi Pharm J 2013;21(2):159–164. Erratum in: Saudi Pharm J 2016;24(2):232.
14. Anagnostis E, Wordell C, Guharoy R, et al. A national survey on hospital formulary management processes. J Pharm Pract 2011;24(4):409–416.
15. Pedersen C, Schneider P, Scheckelhoff D. ASHP national survey of pharmacy practice in hospital settings: Prescribing and transcrib-ing—2004. Am J Health Syst Pharm 2005;62(4):378–390.
16. Pedersen C, Schneider P, Scheckelhoff D. ASHP national survey of pharmacy practice in hospital settings: Prescribing and tran-scribing—2013. Am J Health Syst Pharm 2014;71(11):924–942.
17. Sears EL. Development and maintenance of an online formulary for a large health system. Am J Health Syst Pharm 2008;65(6):510–512.
continued on page 651

Vol. 42 No. 10 • October 2017 • P&T® 651
18. Reddan JG, Sheehan AH, Eskew J, Elmes G. Integration of a medication manage-ment infrastructure in a large, multihos-pital system. Am J Health Syst Pharm 2004;61(23):2557–2561.
19. BeQuette L, Jordan J, Sheehan A, Jorgenson J. Medication formulary man-agement in a large, multihospital system. Am J Pharm Benefits 2010;2(5):319–323.
20. Food and Drug Administration. Guidance for FDA Advisory Committee Members and FDA staff: Voting Procedures for Advisory Committee Meetings. August 2008. Available at: www.fda.gov/down-loads/regulatoryinformation/guidances/ucm125641.pdf. Accessed August 16, 2017.
21. Vang C, Tomson G, Kounnavong S, et al. Improving the performance of drug and therapeutics committees in hospitals—a quasi-experimental study in Laos. Eur J Clin Pharmacol 2006;62(1):57–63.
22. Mittmann N, Knowles S. A survey of phar-macy and therapeutic committees across Canada: scope and responsibilities. Can J Clin Pharmacol 2009;16(1):e171–e177.
23. Mannebach MA, Ascione FJ, Gaither CA, et al. Activities, functions, and structure of pharmacy and therapeutics committees in large teaching hospitals. Am J Health Syst Pharm 1999;56(7):622–628. n
continued from page 646
P&T Meeting System