Embed Size (px)
Citation preview
22 ostomy wound management® july 2013 www.o-wm.com
Feature
a Prospective, descriptive study of risk Factors related to Pressure ulcer development among Patients in Intensive Care unitsElçin Ülker Efteli, MSc; and Ülkü Yapucu Günes, PhD
abstractMany risk factors for the development of pressure ulcers (PUs) in the general hospital population have been identified, but consensus is lacking on specific PU risk factors for critical care patients. A prospective, descriptive study was con-ducted to determine the incidence of and risk factors for PU development among high-risk patients (Braden risk scale score <12) admitted to an intensive care unit (ICU) of a university hospital in Turkey. Demographic variables, APACHE II scores, serum albumin, hemoglobin, and glucose levels were obtained, and patients’ skin was assessed daily until dis-charge. Data were analyzed using percentage distributions, Student’s t-test, chi-square, and logistic regression analysis. Seventy (70) patients (22 women, 48 men), average age 56.2 (SD 19.2) years, mean albumin level 2.86 (median: 2.86, SD 2.73), and mean APACHE II score 17.2 (SD 6.48), completed the study. During an average length of stay of 17.2 days (SD 4.2), PU incidence was 28.6%. Of the 23 ulcers that developed, 12 (52.1%) were Stage I, eight (8, 34.8%) were Stage II, and three (3, 13.1%) were Stage III; no patient developed a Stage IV ulcer. Multivariate logistic regression analysis showed that being female (OR = 0.15, [95% CI:0.03- 0.71] P <0.05) and having a lower serum albumin level (OR=11.6, [95% CI:1.92- 70.4] P <0.01) were independent risk factors for PU development. Patient gender and serum albumin levels should be considered as risk factors for PU development in ICU patients. Larger prospective studies examining these risk factors in ICU patients are warranted.
Keywords: clinical study, logistic regression, pressure ulcer, risk factors, intensive care
Index: Ostomy Wound Management 2013;59(7):22–27
Potential Conflicts of Interest: none disclosed
Dr. Efteli is a research assistant, Department of Fundamentals of Nursing; and Dr. Günes is an Associate Professor, Ege University Faculty of Nursing, Izmir, Turkey. Please address correspondence to Dr. Ülkü Yapucu Günes, Ege University Faculty of Nursing, Bornova,İIzmir, 35040, Turkey; email: [email protected].
Pressure ulcers (PUs) are a common problem in healthcare and represent a substantial burden on patients, their rel-
atives, and caregivers.1 Descriptive studies2 involving patients who acquire PUs while in the hospital have demonstrated that these wounds not only cause pain and discomfort, but also have a great impact on quality of life. In addition, PUs are expensive and can result in a prolonged hospital stay.
Gunningberg et al’s3 prospective study reported that al-most 90% of PUs can be prevented by accurate prediction and appropriate nursing interventions. Previous prospective studies4,5 have shown a PU incidence of between 1% and 56% in intensive care units (ICUs). However, only a limited num-ber of studies have been conducted to determine the preva-lence and incidence of PUs in Turkey. The prevalence of PUs at a university hospital in Turkey was found to be 7.2%,6 and the incidence rates among postoperative surgical7 and neu-
rology ICU8 patients were 54.8% and 18.3%, respectively. More than 100 risk factors for the development of PUs in
a general hospital population have been identified in the lit-erature. According to a prospective cohort study,9 critical care patients usually have multiple risk factors for PUs. Prompt and accurate identification of risk factors associated with PU development is the first step in effective prevention.10 Various risk assessment tools such as the Braden, Norton, and Water-low scales have been developed to aid in this process; how-ever, consensus is lacking regarding the specific risk factors for PU development.11 Moreover, the current risk assessment scales do not address some of the risk factors unique to the critical care population, such as severity of disease and serum albumin and glucose level. In addition, findings on the effect of these risk factors on PU development are contradictory.
Although in the authors’ experience the severity of disease DO NOT D
UPLICATE

july 2013 ostomy wound management® 23www.o-wm.com
Pressure ulCer rIsK FaCtors In ICu PatIents
and blood glucose level upon hospital admission might be the most important factors in predicting PU development in a critical care setting, they are not included in any risk as-sessment scale. Prospective studies of serum albumin have shown conflicting results.12 For example, serum albumin has been found in a few studies to be a positive predictive fac-tor in PU,8,13 but other studies show no predictive value.11,14-17 Therefore, it is important to study these predictors further among critical care patients using multiple regression tech-niques designed to identify the most important predictors for PU development18 and to develop a new risk assessment scale for this population.
The objective of this study was to determine the incidence of, and risk factors for, PU development in intensive care pa-tients at risk of PU development according to their Braden scale score.
methods Study design and sample. This prospective, descriptive
study was conducted in the ICU of an anesthesia and reani-mation clinic of a university hospital in Izmir, Turkey. All pa-tients admitted to this unit at the start of the study and who met the study criteria were eligible to participate. The inclu-sion criteria for the study were 1) 18 years of age or older, 2) an expected hospital stay of at least 7 days, 3) absence of a PU on admission to the unit (patients with existing PUs at admission were excluded for the incidence measure), and 4) a Braden score of <12, which indicates high risk. The data were collected between June and December 2011.
All patients received standard nursing interventions per hospital protocols for PU prevention: their position was changed every 2 hours, a pressure-relieving mattress or air bed was used, they were protected from friction and mois-ture, and bed baths were given daily.
Instruments. Data were collected using a three-part in-strument: 1) patient demographic data, including informa-tion on age, gender, body mass index, serum hemoglobin, al-bumin and glucose values, and time between admission and PU development, was recorded to determine PU incidence, defined as the number of persons who develop a new PU within a particular time period in a particular population; 2) Braden risk assessment scale score; and 3) Acute Physiology and Chronic Health Evaluation II (APACHE II) score.
Braden Risk Assessment Scale. The Braden Scale is one of the best known and widely used tools for evaluating PU risk in adults; its psychometric properties in assessing risk have been validated.19-21 The scale consists of six subscales: mobili-ty, activity, sensory perception, skin moisture, nutrition state, and friction/shear.22,23 Each subscale is rated from 1 to 3 or 4, and the summative scores range between 6 and 23. A lower score indicates a lower level of functioning and, therefore, a higher level of risk for PU development.24 A cutoff score of <12 was used to designate patients as being at high risk for PU development.8,24,25 Braden scale assessment occurred im-
mediately following admission. APACHE II. The severity of disease was evaluated using
APACHE II.26 The APACHE II model utilizes the worst val-ues of 12 physiological variables during the first 24 hours following ICU admission along with an evaluation of the patient’s chronic health and admission diagnosis to calculate the APACHE II predicted mortality.27 The APACHE II model has been widely validated and used by many ICUs to classify the severity of illness and to predict hospital mortality.28 The total score in APACHE II is 71; higher values in the APACHE systems represent a higher risk of death.
Data collection. All information relating to the patient was recorded once daily from the day of admission to the unit until the development of a PU or until being discharged from the unit. Serum hemoglobin, albumin, and glucose values of the patients were collected daily from the medical records; other data, such as Braden scale and APACHE II scores, were calculated and recorded by the research nurse. If a PU devel-oped, it was assessed and recorded as Stage I through Stage IV, as defined in the National Pressure Ulcer Advisory Panel.29 Data were de-identified for patient anonymity.
Data analyses. The daily values for all variables were recorded and then their means were determined. Statisti-cal analysis was performed using the Statistical Package for Social Sciences (SPSS) version 13.0 (SPSS Inc, Chicago, IL). The data were expressed as the mean and standard deviation (SD). Descriptive statistics were utilized in order to examine the distributions of demographic and clinic data of patients. The relationship between the risk factors and PU develop-ment was evaluated using univariate analysis. Student’s t-test was used for comparisons such as age, hemoglobin, serum albumin, and blood glucose levels between patients with and without PU; gender relationships were assessed using Fisher’s exact test. Risk was expressed as odds ratio with 95% confi-dence interval. P <0.05 was considered statistically significant. Variables indicating a P <0.20 in the univariate analysis were included in a forward stepwise logistic regression analysis to identify the risk factors associated with PU development.
Ethical considerations. Study approval was obtained
Key Points• Aprospectivestudywasconductedamong70pa-
tients admitted to an intensive care unit to determine the incidence of pressure ulcers (PUs) and to
evaluate PU risk factors.• Twenty-three(23)ulcersdeveloped(mostlyStageI
and Stage II) during an average stay of 17 days.• Beingfemaleandhavingalowserumalbuminlevel
were independent risk factors for PU development in this patient population.
ostomy wound management 2013;59(7):22–27
DO NOT D
UPLICATE

24 ostomy wound management® july 2013 www.o-wm.com
Feature
from the appropriate ethics committee. Informed written consent was obtained from all participants or their families.
resultsSample. A total of 98 patients was enrolled after meeting
the initial study inclusion criteria. Of those, 28 were hospital-ized for <7 days, leaving a total sample of 70 patients.
Forty-eight (48, 68.6%) patients were male; patient age ranged from 21 to 87 years, mean age 56.2 (SD 19.2) years. The mean length of stay in the ICU was 17.2 (SD 4.2) days, and the mean APACHE II score was 17.2 (SD 6.48). Diagno-ses for ICU admissions included respiratory failure (37.2%), postoperative complications (32.8%), trauma (15.7%), and organ failure (14.3 %) (see Table 1). The average Braden scale score was 10.4 (SD 0.9).
A total of 23 PUs developed in 20 of the 70 patients; three (3, 15%) of the patients had more than one PU. The inci-dence of PU in this population of ICU patients was 28.6%. Of the 23 ulcers, 12 (52.1%) were Stage I, eight (8, 34.8%) were Stage II, and three (3, 13.1%) were Stage III; no patient
developed a Stage IV ulcer. Ten (10, 50%) of the ulcers were observed between 1 and 5 days after admission to the unit, five (5, 25%) between 6 and 10 days, and three (3, 15%) be-tween 11 and 15 days after admission. The most common ar-eas for the PUs were the coccyx (39.8%) and sacrum (32.7%).
Data analysis. Univariate analysis. Ten (10, 45.5%) women and 10
(20.9%) men developed PUs (P <0.05). Patients who devel-oped a PU were significantly older (66.8 ± 15.1 years) than nonpressure ulcer patients (52.1 ± 20.1 years) (P <0.05). The mean hemoglobin levels were slightly lower in patients who developed a PU (9.44 ± 0.99 versus 9.99 ± 1.40), but this dif-ference was not statistically significant. Similarly, blood glu-cose levels were higher in patients with PUs (209.9 ± 51.2 ver-
sus 184.9 ± 48.5), but this difference was not statistically significant. In contrast, mean serum albumin levels were significantly lower (2.49 ± 0.40 versus 3.01 ± 0.56) and the mean APACHE II score was significantly higher for patients who developed a PU (19.9 ± 5.48 versus 15.1 ± 4.12) than for those who did not develop a PU (P <0.05) (see Table 2).
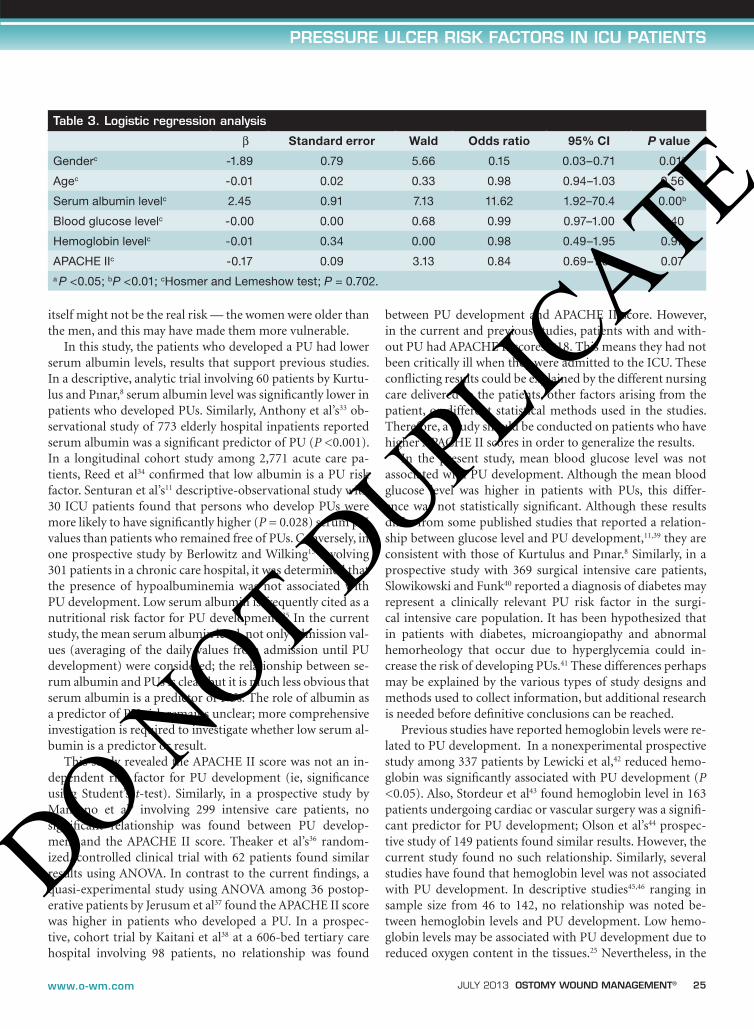
Multivariate logistic regression analysis. Variables in-dicating a statistically significant relationship with PU development at P <0.20 in the univariate analysis were considered potential risk factors for inclusion in the multivariate logistic regression analysis. Also, because anemia is considered an important risk factor in the de-velopment of PU,8 hemoglobin levels were included in multivariate analysis. In the multivariate logistic regres-sion, gender (OR = 0.15,[95% CI: 0.03–0.71]; P <0.05) and low serum albumin levels (OR = 11.6, [95% CI: 1.92–70.4]; P <0.01) were significant risk factors for PU development (see Table 3).
discussionThe incidence of PUs in this study was 28.6%. No compre-
hensive research study of PU incidence in Turkey was found. The PU incidence reported in two previous studies in ICUs was 16.7% to 18.3%.8,11 Therefore, the incidence of 28.6% observed in this study was higher than that reported in previ-ous studies. This may be explained by the fact that the cur-rent study was performed in an anesthesia and reanimation clinic, and patient prognosis in this unit may be much worse than in other settings. Also APACHE scores of the patients indicated that patient acuity in this unit was high.
In the current study, women developed PUs to a greater extent than men. Results relating to gender in previous PU studies are conflicting. In a retrospective, cohort study in-volving 2,120 home care patients, Kelly30 reported men de-veloped more ulcers. However, in Tannen et al’s31 descriptive study of 11,566 patients in acute care hospitals, the majority of patients with PUs were women, similar to Lindgren et al’s32 prospective study of 286 patients. Therefore, data on gender needs to be interpreted with care. In the current study, gender
table 1. Patient characteristics
Gender n (%)
Female 22 (31.4%)
Male 48 (68.6%)
Age (Mean, SD) 56.2 years (± 19.2)
Length of stay 17.2 days (± 4.2)
Diagnosis n (%)
Respiratory failure 26 (37.2%)
Postoperative complications 23 (32.8%)
Trauma n (%) 11 (15.7%)
Organ failure n (%) 10 (14.3%)
table 2. Characteristics of patients who did and who did not develop a pressure ulcer (n = 70)
Mean (SD) or n (%)
Pressure ulcer
(n=20)
No pressure ulcer
(n=50)
P value
Gendera
Female 10 (45.5%) 12 (55.5%) 0.034c
Male 10 (20.9%) 38 (79.1%)
Ageb 66.8 ±15.4 52.1 ±20.1 0.02c
Hemoglobin levelb 9.44 ±0.99 9.99 ±1.40 0.115
Serum albumin levelb 2.49 ±0.40 3.01 ±0.56 0.000d
Blood glucose levelb 209.9 ±51.2 184.9 ±48.5 0.06
APACHE II scoreb 19.9 ±5.48 15.1 ± 4.12 0.000d
aFisher exact test; bStudent’s t-testcP <0.05; dP <0.001
DO NOT D
UPLICATE
july 2013 ostomy wound management® 25www.o-wm.com
Pressure ulCer rIsK FaCtors In ICu PatIents
itself might not be the real risk — the women were older than the men, and this may have made them more vulnerable.
In this study, the patients who developed a PU had lower serum albumin levels, results that support previous studies. In a descriptive, analytic trial involving 60 patients by Kurtu-lus and Pınar,8 serum albumin level was significantly lower in patients who developed PUs. Similarly, Anthony et al’s33 ob-servational study of 773 elderly hospital inpatients reported serum albumin was a significant predictor of PU (P <0.001). In a longitudinal cohort study among 2,771 acute care pa-tients, Reed et al34 confirmed that low albumin is a PU risk factor. Senturan et al’s11 descriptive-observational study with 30 ICU patients found that persons who develop PUs were more likely to have significantly higher (P = 0.028) serum pH values than patients who remained free of PUs. Conversely, in one prospective study by Berlowitz and Wilking15 involving 301 patients in a chronic care hospital, it was determined that the presence of hypoalbuminemia was not associated with PU development. Low serum albumin is frequently cited as a nutritional risk factor for PU development.35 In the current study, the mean serum albumin level, not only admission val-ues (averaging of the daily values from admission until PU development) were considered; the relationship between se-rum albumin and PUs is clear, but it is much less obvious that serum albumin is a predictor of PUs. The role of albumin as a predictor of PU risk remains unclear; more comprehensive investigation is required to investigate whether low serum al-bumin is a predictor or result.
This study revealed the APACHE II score was not an in-dependent risk factor for PU development (ie, significance using Student’s t-test). Similarly, in a prospective study by Manzano et al9 involving 299 intensive care patients, no significant relationship was found between PU develop-ment and the APACHE II score. Theaker et al’s36 random-ized, controlled clinical trial with 62 patients found similar results using ANOVA. In contrast to the current findings, a quasi-experimental study using ANOVA among 36 postop-erative patients by Jerusum et al37 found the APACHE II score was higher in patients who developed a PU. In a prospec-tive, cohort trial by Kaitani et al38 at a 606-bed tertiary care hospital involving 98 patients, no relationship was found
between PU development and APACHE II score. However, in the current and previous studies, patients with and with-out PU had APACHE II scores <18. This means they had not been critically ill when they were admitted to the ICU. These conflicting results could be explained by the different nursing care delivered to the patients, other factors arising from the patient, or different statistical methods used in the studies. Therefore, a study should be conducted on patients who have higher APACHE II scores in order to generalize the results.
In the present study, mean blood glucose level was not associated with PU development. Although the mean blood glucose level was higher in patients with PUs, this differ-ence was not statistically significant. Although these results differ from some published studies that reported a relation-ship between glucose level and PU development,11,39 they are consistent with those of Kurtulus and Pınar.8 Similarly, in a prospective study with 369 surgical intensive care patients, Slowikowski and Funk40 reported a diagnosis of diabetes may represent a clinically relevant PU risk factor in the surgi-cal intensive care population. It has been hypothesized that in patients with diabetes, microangiopathy and abnormal hemorheology that occur due to hyperglycemia could in-crease the risk of developing PUs.41 These differences perhaps may be explained by the various types of study designs and methods used to collect information, but additional research is needed before definitive conclusions can be reached.
Previous studies have reported hemoglobin levels were re-lated to PU development. In a nonexperimental prospective study among 337 patients by Lewicki et al,42 reduced hemo-globin was significantly associated with PU development (P <0.05). Also, Stordeur et al43 found hemoglobin level in 163 patients undergoing cardiac or vascular surgery was a signifi-cant predictor for PU development; Olson et al’s44 prospec-tive study of 149 patients found similar results. However, the current study found no such relationship. Similarly, several studies have found that hemoglobin level was not associated with PU development. In descriptive studies45,46 ranging in sample size from 46 to 142, no relationship was noted be-tween hemoglobin levels and PU development. Low hemo-globin levels may be associated with PU development due to reduced oxygen content in the tissues.25 Nevertheless, in the
table 3. logistic regression analysis
β Standard error Wald Odds ratio 95% CI P value
Genderc -1.89 0.79 5.66 0.15 0.03–0.71 0.01a
Agec -0.01 0.02 0.33 0.98 0.94–1.03 0.56
Serum albumin levelc 2.45 0.91 7.13 11.62 1.92–70.4 0.00b
Blood glucose levelc -0.00 0.00 0.68 0.99 0.97–1.00 0.40
Hemoglobin levelc -0.01 0.34 0.00 0.98 0.49–1.95 0.97
APACHE IIc -0.17 0.09 3.13 0.84 0.69–1.01 0.07a P <0.05; bP <0.01; cHosmer and Lemeshow test; P = 0.702.
DO NOT D
UPLICATE

26 ostomy wound management® july 2013 www.o-wm.com
Feature
current study, the mean hemoglobin levels in both patients who did and did not develop a PU was <10 g/dL. Research including patients with a wide variety of hemoglobin levels should be conducted.
limitationsThe most important limitation of this study was sample
size. The mean APACHE score was not an independent risk factor for PU development, but this might be the result of the low average score [17.2 (SD 6.48)] of the study population. Therefore, further research should be conducted on patients with a wide variety of APACHE II scores. In this study, all patients received preventive measures that may have been intensified as a result of the study potentially affecting the results. This study highlights the need for further research with larger and more diverse patient populations. In addi-tion, although the sample included patients determined to be at high risk for PUs according to the Braden scale, PUs devel-oped in only 20 patients. Therefore this instrument may not be ideal for measuring risk in intensive care patients.
ConclusionIn this patient population of acutely ill patients, blood glu-
cose level, hemoglobin level, and severity of disease were not found to be independent risk factors for PU development. However, lower serum albumin levels and being female sig-nificantly increased the risk of developing a PU. Based on this study, the odds of having a PU were almost twice as high in women as men, and PUs developed in 35% of patients with se-rum albumin levels below 3.3g/dL. Therefore, particular atten-tion should be paid to female patients and persons who have lower serum albumin levels; new risk prediction scales includ-ing these predictor factors should be developed and tested. n
references1. Hulsenboom MA, Bours GJJW, Halfens RJG. Knowledge of pressure ulcer
prevention: a cross-sectional and comparative study among nurses. BMC Nurs. 2007;6:2:doi:101186/1472-6955-6-2.
2. Schoonhoven L, Grobbee DE, Donders ART, Algra A, Grypdonck MH, Bousema MT, et al. Prediction of pressure ulcer development in hos-pitalized patients: a tool for risk assessment. Qual Saf Health Care. 2006;15(1):65–70.
3. Gunningberg L, Lindholm C, Carlsson M, Sjödén PO. Implementation of risk assessment and classification of pressure ulcers as quality indicators for patients with hip fractures. J Clin Nurs. 1999;8(4):396–406.
4. Keller BP, Wille J, van Ramshorst B, van der Werken C. Pressure ulcers in intensive care patients: a review of risks and prevention. Intensive Care Med. 2002;28(10):1379–1388.
5. Schoonhoven L, Haalboom JR, Bousema MT, Algra A, Grobbee DE, Grypdonck MH Buskens E. Prospective cohort study of routine use of risk assessment scales for prediction of pressure ulcers. BMJ. 2002;325(7368):797–800.
6. Hug E, Ünalan H, Karamehmetoglu SS, Tüzün S, Gürgöze M, Tüzün F. Bir egitim hastanesinde bası yaraları prevalansı ve bası yarası gelisiminde etkili risk faktörleri (Pressure ulcer prevalance in a teaching hospital and risk factors associated with pressure ulcer development) Türkiye Fiziksel Tıp ve Rehabilitasyon Dergisi, (Turkish Journal of Physical Medicine and Rehabilitation). 2001;47(6):3–11.
7. Karadag M, Gümüskaya N. The incidence of pressure ulcers in surgical patient: a sample hospital in Turkey. J Clin Nurs. 2006;15(4):413–421.
8. Kurtulus Z, Pınar R. Braden skalası ile belirlenen yüksek riskli hasta grubunda albümin düzeyleri ile bası yaraları arasındaki iliski (Relation be-tween albumin levels and pressure sore in high-risk patients defined with
Braden’s risk assessment tool). Cumhuriyet.Üniversitesi Hemsirelik Yük-sek Okulu Dergisi (Journal of Cumhuriyet University School of Nursing). 2003;7(2):1–10.
9. Manzano F, Navarro MJ, Roldan D, Moral MA, Levya I, Guerrero C, et al. Pressure ulcer incidence and risk factors in ventilated intensive care pa-tients. J Crit Care. 2010;25(3):469–476.
10. Karadag A. Basınç ülserleri: degerlendirme, önleme ve tedavi (Pressure ulcers: assessment, prevention, and treatment). Cumhuriyet Üniversitesi Hemsirelik Yüksekokulu Dergisi (Journal of Cumhuriyet University School of Nursing). 2003;7(2):41–46.
11. Senturan L, Karabacak Ü, Özdilek S, Alpar SE, Bayrak S, Yüceer S, Yıldız N. The relationship among pressure ulcers, oxygenation, and perfusion in mechanically ventilated patients in an intensive care unit. J Wound Ostomy Continence Nurs. 2009;36(5):503–508.
12. Thomas DR. Pressure ulcers. In: Cassel CK. Geriatric Medicine, 3rd ed. New York, NY: Springer;1997:767–785.
13. Allman RM, Laprade CA, Noel LB, Walker JM, Moorer CA, Dear MR, Smith CR. Pressure sores among hospitalized patients. Ann Intern Med. 1986;105(3):337–342.
14. Guralnik JM, Harris TB, White LR, Cornoni-Huntley JC. Occurence and predictors of pressure sores in the National Health Service and nutrition examination survey follow-up. J Am Geriatr Soc. 1988;36(9):807–812.
15. Berlowitz D, Wilking SV. Risk factors for pressure sores. A com-parison of cross-sectional and cohort-derived data. J Am Geriatr Soc.1989;37(11):1043–1050.
16. Allman RM, Goods PS, Patrick MM, Burst N, Bartolucci AA. Pressure ul-cer risk factors among hospitalized patients with activity limitation. JAMA. 1995;273(11):865–870.
17. Sagnak KN, Çınar S. Bası yaralarının önlenmesinde havalı yatak ve koyun postu uygulamalarının etkinligi (Effective of sheep skin and air bed practise to prevention of pressure sores). Yogun Bakım Hemsireligi Dergisi (Turkish Journal of Critical Care Nurses). 2005;9(1-2):1–7.
18. Cullum N, Clark M. Intrinsic factors associated with pressure sores in el-derly people. J Advanced Nurs.1992;17(4):427–431.
19. Bergstrom N, Braden B, Kemp M, Champagen M, Ruby E. Predicting pressure ulcer risk, a multisite study of the predictive validity of the Braden scale. Nurs Res. 1998;47(5):261–269.
20. VandenBosch T, Montooye C, Satwicz M, Durkee LK, Boylan LB. Predic-tive validity of the Braden scale and nurse perception in identifying pres-sure ulcer risk. Appl Nurs Res. 1996;9(2):80–86.
21. Barnes D, Payton RG. Clinical application of the Braden scale in the acute-care setting. Dermatol Nurs. 1993;5:386–388.
22. Kwong E, Pang S, Wong T, Ho J, Shao-ling X, Li-jun T. Predicting pressure ulcer risk with the modified Braden, Braden and Norton scales in acute care hospitals in Mainland China. Appl Nurs Res. 2005;18(2):122–128.
23. Braden B, Bergstrom B. A conceptual schema for the study of the aetiol-ogy of pressure sores. Rehabil Nurs. 1987;12(1):8–12.
24. Bergstrom N, Braden B, Laguzza A, Holman V. The Braden Scale for pre-dicting pressure sore risk. Nurs Res. 1987;36(4):205–210.
25. Colwell JC. Skin integrity and wound care. In: Potter PA, Perry AG, eds. Fun-damentals of Nursing. St Louis, MO: The Mosby Company;2005:950–990.
26. Knaus WA, Draper EA, Wagner DP, Zimmerman JE. APACHE II: a severity of disease classification system. Crit Care Med. 1985;13(10):818–829.
27. Ho KM, Dobb GJ, Knuiman M, Finn J, Lee KY, Webb SAR. A comparison of admission and worst 24-hour Acute Physiology and Chronic Health Evalu-ation II scores in predicting hospital mortality: a retrospective cohort study. Crit Care. 2006;10(1):R4.
28. Oh TE, Hutchinson R, Short S, Buckley T, Lin E, Leung D. Verification of the acute physiology and chronic health evaluation scoring system in a Hong Kong intensive care unit. Crit Care Med. 1993;21(5):698–705.
29. Black J, Baharestani MM, Cuddigan J, Dorner B, Edsberg L, Langemo D, et al. National Pressure Ulcer Advisory Panel’s updated pressure ulcer staging system. Adv Skin Wound Care. 2007;20(5):269–274.
30. Kelly C. A new look at the Braden scale for pressure ulcer risk older adults in home health care. J BSN Honors Res. 2010;1(1):2–21.
31. Tannen A, Dassen T, Bours G, Halfens R. A comparison of pressure ulcer prevalence: concerted data collection in the Netherlands and Germany. Int J Nurs Stud. 2004;41(6):607–612.
32. Lindgren M, Unosson M, Fredrikson M, Ek AC. Immobility — a major risk factor for development of pressure ulcers among adult hospitalized pa-tients: a prospective study. Scandinavian J Caring Sci. 2004;18(1):57–64.
33. Anthony D, Reynolds T, Russell L. An investigation into the use of serum albumin in pressure sore prediction. J Adv Nurs. 2000;32(2):359–365.
34. Reed RL, Hepburn K, Adelson R, Center B, McKnight P. Low serum al-bumin levels, confusion, and fecal incontinence: are these risk factors for pressure ulcers in mobility-impaired hospitalized adults? Gerontology. 2003;49(4):255–259.
35. Johnston E. Optimising nutrition to prevent pressure ulcer development.
DO NOT D
UPLICATE

july 2013 ostomy wound management® 27www.o-wm.com
Pressure ulCer rIsK FaCtors In ICu PatIents
Wounds UK. 2007;3(1):53–59.36. Theaker C, Kuper M, Soni N. Pressure ulcer prevention in intensive care:
a randomised control trial of two pressure relieving devices. Anaesthesia. 2005;60(4):395–399.
37. Jerusum J, Joseph K, Davis JM, Suki R. Balloons, beds and breakdown. Crit Care Nurs Clin North Am. 1996;8(4):423–440.
38. Kaitani T, Tokunaga K, Matsui N, Sanada H. Risk factors related to de-velopment of pressure ulcers in the critical care setting. J Clin Nurs. 2010;19(3-4):414–421.
39. Frankel H, Sperry J. Risk factors for pressure ulcer development in a best practice surgical intensive care unit. Am Surg. 2007;73(12):1215–1217.
40. Slowikowski GC, Funk M. Factors associated with pressure ulcers in pa-tients in a surgical intensive care unit. J Wound Ostomy Continence Nurs. 2010; 37(6):619–626.
41. Huang L, Nakagami G, Minematsu T, Kinoshita A, Sugama J, Nakatani T, et al. Ulceration and delayed healing following pressure loading in hyperglycemic rats with an immature dermal collagen fiber. WOUNDS. 2010;22(9):237–244.
42. Lewicki LJ, Mion L, Splane KG, Samstag D, Secic M. Patient risk factors for pressure ulcer during cardiac surgery. AORN J. 1997;65(5):933–942.
43. Stordeur S, Laurent S, D’Hoore W. The importance of repeated risk as-sessment for pressure sores in cardiovascular surgery. J Cardiovasc Surg (Torino). 1998;39(3):343–349.
44. Olson B, Langemo D, Burd C, Hanson D, Hunter S, Cathcart Silberberg T. Pressure ulcer incidence in an acute care setting. J Wound Ostomy Conti-nence Nurs. 1996;23(1):15–22.
45. Terekeci H, Küçükardalı Y, Top C, Önem Y, Çelik S, Öktenli Ç. Risk assess-ment study of the pressure ulcers in intensive care units patients. Eur J Intern Med. 2009;20(4):394–397.
46. Tel H, Özden D, Günes Çetin P. Yataga bagımlı hastalarda basınç yarası gelisme riski ve hemsirelerin bu hastalara uyguladıkları önleyici bakım (De-termination of risk for pressure ulcer development in bedridden patients and preventive measures that nurses use for these patients). Hemsirelikte Arastırma Gelistirme Dergisi (Turkish Journal of Research and Develop-ment in Nursing). 2006;1(2):35–45.
www.woundsresearch.com/tablet_appsRegister at
Unlimited Access. Anywhere, Anytime.
Access the most widely read, peer-reviewed journal focusing on wound care and wound
research on your iPad or Android tablet.
Now Available
Available Free on iPad & Android
Download Today!
wounds_IpadAd_HalfHoriz.indd 1 3/8/13 9:33 AM
DO NOT D
UPLICATE