-
8/21/2019 A Prospective Audit of Regional Anaesthesia Failure in
5080 Caesarean Sections
1/19
A prospective audit of regional anaesthesia failure in 5080
Caesarean sections*
Author(s):Kinsella, S. M.
Issue: Volume !"8#, August $008, p 8$$%8!$
Publication
Type:&'riginal articles(
Publisher: ) $008 Association of Anaesthetists of reat +ritain
-reland
Institution(s):
Consultant Anaesthetist, epartment of Anaesthesia, St Michael/s
ospital, +ristol
+S$ 81, 2K
Accepted3 $4 anuar6 $008
Stephen Michael Kinsella 17mail3 stephen.insella9u:ht.nhs.u
*ata presented in part at the ':stetric Anaesthetists/
Association annual scientific
meeting, ;ondon $005.
A:stract
Ringkasan : Anestesi untuk operasi caesar telah diaudit selama 5
tahun : 5080kasus dilakukan dengan menggunakan tulang belakang 63 %
, epidural top -up 26 % , dikombinasikan spinal - epidural 5 % dan
anestesi umum primer 5 % !ingkat kon"ersi anestesi umum anestesi
regional adalah 0,8 % untuk elekti#dan $, % untuk bagian darurat
caesar dibandingkan dengan Ro&al 'ollege o#
(okter-dokter anestesi target ) % dan 3 % !ingkat kon"ersi
regional untukanestesi umum dalam kategori ) operasi caesar adalah
20 % *eban&ak 8 %+anita memiliki anestesi umum ketika kedua
enderal utama dan kon"ersianestesi regional digabungkan !ingkat
kegagalan untuk mencapai operasibebas rasa sakit adalah 6 % dengan
spinalis , 2$ % dengan epidural top - updan )8 % dengan kombinasi
spinal - epidural *elain enis anestesi danurgensi operasi , #aktor
lain &ang berhubungan dengan kegagalan pra-operasanestesi
regional termasuk indeks massa tubuh , tidak ada operasi
caesarsebelumn&a , dan indikasi untuk caesar ga+at anin akut
atau kondisi medis
ibu emadain&a blok anestesi pra-operasi dan durasi operasi
adalah #aktorrisiko penting bagi kegagalan intra - operati# .ntuk
anestesi spinal ,penggunaan opioid spinal dikaitkan dengan
kegagalan kurang pra-operasi .ntuk anestesi epidural top -up ,
"olume &ang top - up epidural lebih rendahdikaitkan dengan
kegagalan kurang pra-operasi , dan penggunaan adrenalindikaitkan
dengan keduan&a kurang kegagalan pra-operasi dan intra -
operati#
!ingkat insiden buruk berat adalah ) : )26 dengan anestesi
umum dan ) : 50dengan anestesi regional
-
8/21/2019 A Prospective Audit of Regional Anaesthesia Failure in
5080 Caesarean Sections
2/19
istor6
unct
are not used routinel6 :ecause of concerns a:out maternal
pulmonar6 aspiration and fetal effects.
?he percentage use of general anaesthesia for Caesarean section
has :ecome a marer of the =ualit6
of the o:stetric anaesthetic service &4%!(. As the overall
use of general anaesthesia has declined,
urgenc6 of Caesarean section and failure of regional anaesthesia
have :ecome the main indications &@(. A four categor6
classification of Caesarean section urgenc6 as descri:ed in $000
ith the aim of
improving audit data collection in comparison to the :inar6
electiveBemergenc6 classification &5(.
ailure of regional anaesthesia is defined in several a6s.
':>ective outcomes include conversion to
general anaesthesia &@, , D(, conversion to an6 different
form of anaesthesia &@, 8(, or pain during
surger6 &E, 40(. -n research studies of epidural top7up
solutions here onset time is the primar6 end7
point, failure ma6 :e defined as the ina:ilit6 to achieve a
defined degree of nerve :loc suita:le for
Caesarean section &44, 4$(. ?hese studies have not
esta:lished an ideal top7up solution.
-
8/21/2019 A Prospective Audit of Regional Anaesthesia Failure in
5080 Caesarean Sections
3/19
pro:lems at successive stages of the esta:lishment and
management of the anaesthetic "AppendiF#.
?he definition of a satisfactor6 regional anaesthetic :loc for
Caesarean section as the loss of cold
sensation, using eth6l chloride spra6, from ?@ "the nipples# don
to S5 "the :uttocs#, as ell as
anaesthesia "no feeling# to a 4E gauge needle inserted at
several points along the line of surgical
incision at ?4$. Gain during the operation as split into mild or
severe, :ased on a cut % off for mild
pain of up to 4 mg alfentanil or 400 Hg fentan6l, and the use of
onl6 one t6pe of analgesia.
-nitiall6, data ere collected onl6 on Caesarean sections under
regional anaesthesia. Starting on 4st
une $000 "Iear $#, all Caesarean sections that had primar6
general anaesthesia ere also logged
using a separate audit num:ering se=uence. ?he indication for
the use of general anaesthesia as
included on the data form.
?he urgenc6 of Caesarean section as classified using a 57point
scale in Iear 4 and a @7point scale
from Iear $ &5(. ?he urgenc6 grade in Iear 4 cases has :een
converted to the e=uivalent @7point scale
:6 com:ining the original grades $ and ! &5(.
Spinal anaesthesia as the preferred method and the use of the
right lateral position for insertion a
encouraged. ?he standard dose as $.5 ml h6per:aric :upivacaine
0.5J ith !00 Hg diamorphine.
Spinal fentan6l as occasionall6 used, especiall6 for more urgent
cases. hen an epidural as used
for analgesia during la:our, it as usuall6 topped7up for
Caesarean section. ?he drugs used to top up
ere not standardised. ?hese ere :upivacaine and lidocaine, to
hich might :e added adrenaline 5
Hg.ml74 "4 3 $00 000#, sodium :icar:onate 8.@J, fentan6l or
diamorphine. ;aevo7:upivacaine :ecame
availa:le toards the end of the audit period. CS1 and
microspinal catheters ere reserved for
compleF cases, such as those that re=uired slo onset of the
regional :loc, omen ith anatomicaldifficulties or hen prolonged
surger6 as anticipated. eneral anaesthesia as discouraged
unless
specificall6 indicated. -f accidental dural puncture occurred
during la:our, the epidural catheter as
sometimes inserted into the spinal space in order to use it for
la:our analgesia.
Statistical anal6sis as performed to investigate factors
associated ith pre7operative or intra7
operative failure. Gre7operative failure as defined as
conversion to another anaesthetic :efore the
operation started or failure to achieve a satisfactor6 :loc "as
defined a:ove#. -ntra7operative failure
as defined as unsatisfactor6 anaesthesia that re=uired analgesia
&40(. ?his eFcluded cases here
conversion to another anaesthetic had :een performed :efore
surger6.
?he anal6sis as carried out initiall6 on all regional
anaesthesia cases. 2nivariate anal6sis of factors
that might influence pre7operative failure as performed first
using chi7s=uared tests. actors from
the audit data:ase included audit 6ear, t6pe of anaesthesia,
la:our epidural in place :ut not topped
up, indication for Caesarean, hether the oman as in la:our and
Caesarean urgenc6. ata from th
la:our ard o:stetric data:ase included height, eight at :ooing,
:od6 mass indeF "+M-#, gestation
parit6, num:er of previous Caesarean sections, neonatal eight
and decision7deliver6 interval.
http://ovidsp.tx.ovid.com/spb/ovidweb.cgi#108%23108http://ovidsp.tx.ovid.com/spb/ovidweb.cgi#89%2389http://ovidsp.tx.ovid.com/spb/ovidweb.cgi#89%2389http://ovidsp.tx.ovid.com/spb/ovidweb.cgi#94%2394http://ovidsp.tx.ovid.com/spb/ovidweb.cgi#108%23108http://ovidsp.tx.ovid.com/spb/ovidweb.cgi#89%2389http://ovidsp.tx.ovid.com/spb/ovidweb.cgi#89%2389http://ovidsp.tx.ovid.com/spb/ovidweb.cgi#94%2394
-
8/21/2019 A Prospective Audit of Regional Anaesthesia Failure in
5080 Caesarean Sections
4/19
orards and :acards stepise logistic regression anal6sis as then
used to determine hich
factors ere significant predictors of the outcome. A p value L
0.05 as used to define statistical
significance. ?he same process as repeated for intra7operative
failure, :ut including the factors
:loc ade=uate pre7operativel6/ and duration of surger6.
?he same anal6sis as performed on the su:7groups of omen ith
spinal and epidural top7up
anaesthesia. -n the spinal group, factors specific to this t6pe
of anaesthesia ere also includedN theseere insertion position,
indication for position if sitting "change from lateral, o:ese,
preference of
the anaesthetist, otherBunnon#, position after insertion, local
anaesthetic volume and use of spina
opioid. -n the epidural top7up group, the specific anaesthetic
factors included ere t6pe of local
anaesthetic ":upivacaine, lidocaine, 50 3 50
:upivacaine3lidocaine, and other/ including laevo7
:upivacaine and non7standard local anaesthetic miFtures#, volume
of local anaesthetic, use of
adrenaline, use of :icar:onate and dose of epidural opioid
"including Oero dose#.
-
8/21/2019 A Prospective Audit of Regional Anaesthesia Failure in
5080 Caesarean Sections
5/19
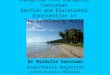
igure 4 lo diagram of spinal management. A successful spinal is
one that as used for Caesarean
section ith no intra7operative discomfort. &;A, local
anaestheticN A, general anaesthesia,
-
8/21/2019 A Prospective Audit of Regional Anaesthesia Failure in
5080 Caesarean Sections
6/19
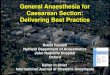
igure $ lo diagram of top7up epidural management. A successful
epidural is one that as used for
Caesarean section ith no intra7operative discomfort. &;A,
local anaestheticN A, general
anaesthesiaN
-
8/21/2019 A Prospective Audit of Regional Anaesthesia Failure in
5080 Caesarean Sections
7/19
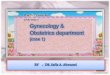
igure ! lo diagram of com:ined spinal7epidural "CS1# management.
A successful CS1 is one that
as used for Caesarean section ith no intra7operative discomfort.
&;A, local anaestheticN A,
general anaesthesiaN
-
8/21/2019 A Prospective Audit of Regional Anaesthesia Failure in
5080 Caesarean Sections
8/19
conversion as pre7operative in 8!J categor6 4 spinals and E0J
categor6 4 top7up epidurals, in
contrast to pre7operative conversion in 8J of all spinals and 8J
of all top7up epidurals.
?a:le 4 -ndications for Caesarean section and indications for
primar6 general anaesthesia. ?hese tota
are P 400J as multiple indications could :e assigned.
?a:le $ Caesarean section urgenc6, t6pe of primar6 anaesthesia
and conversion of regional anaesthesi
to general anaesthesia during 6ears $%5.
http://ovidsp.tx.ovid.com/spb/ovidweb.cgi?View+Image=00000524-200808000-00004%7CTT2&S=MJFNFPEGEADDKEOONCGLMDMLLPKMAA00&WebLinkReturn=Full+Text%3DL%7CS.sh.39.41%7C0%7C00000524-200808000-00004http://ovidsp.tx.ovid.com/spb/ovidweb.cgi?View+Image=00000524-200808000-00004%7CTT1&S=MJFNFPEGEADDKEOONCGLMDMLLPKMAA00&WebLinkReturn=Full+Text%3DL%7CS.sh.39.41%7C0%7C00000524-200808000-00004
-
8/21/2019 A Prospective Audit of Regional Anaesthesia Failure in
5080 Caesarean Sections
9/19
Most of the omen having a categor6 4 operation "8!J# and
categor6 4%! operation "D5J# ere in
la:our.
?here ere 40 cases in hich an epidural had :een esta:lished
during la:our :ut as not topped up
for Caesarean section. ?he ma>orit6 of these ere not topped
up :ecause of poor =ualit6 :loc, :ut
other reasons included epidural catheter misplaced or
disconnected, epidural onl6 recentl6 inserted,
lac of time for top up, maternal anFiet6 and previous accidental
dural puncture. 'f these 40
patients, 8 had a primar6 regional :loc for Caesarean section
and $0 had general anaesthesia3 4 fo
urgenc6 and four for maternal preference.
?o cases ith an epidural catheter placed spinall6 after
accidental dural puncture had unrelia:le
analgesia during la:our and there as no attempt to top up the
intrathecal catheter/. Grimar6 spina
anaesthesia as planned, :ut in one case the spinal could not :e
located and general anaesthesia a
given.
?a:le ! shos the num:er of omen having intraoperative pain
and conversion of regional anaesthesi
to general anaesthesia related to the ade=uac6 of :loc :efore
surger6.
http://ovidsp.tx.ovid.com/spb/ovidweb.cgi#TT3%23TT3http://ovidsp.tx.ovid.com/spb/ovidweb.cgi?View+Image=00000524-200808000-00004%7CTT3&S=MJFNFPEGEADDKEOONCGLMDMLLPKMAA00&WebLinkReturn=Full+Text%3DL%7CS.sh.39.41%7C0%7C00000524-200808000-00004http://ovidsp.tx.ovid.com/spb/ovidweb.cgi#TT3%23TT3
-
8/21/2019 A Prospective Audit of Regional Anaesthesia Failure in
5080 Caesarean Sections
10/19
?a:le ! -ncidence of pain and intra7operative conversion to
general anaesthesia depending on
ade=uac6 of :loc :efore surger6 in @5@0 cases using regional
anaesthesia.
Critical incidents
A :oF asing for reporting of critical incidents as added to the
data collection form from regional
anaesthesia case no 4!00 "general anaesthesia case num:er @@#.
?hese are presented in decreasing
order of seriousness3
Grimar6 general anaesthesia
* Categor6 4N initial attempt at intu:ation failed, mas
ventilated :efore further successful attempt.
Grimar6 general anaesthesia ith la:our epidural esta:lished :ut
not topped up
* "regional anaesthesia pro:lem# categor6 !N intravenous
epidural catherN epidural ineffective and
top7ups go to m6 head/.
Conversion of regional anaesthesia to general anaesthesia
* Categor6 !N epidural top7up for failure to progress in la:our
in a pre7eclamptic omanN pain onentering the peritoneum, general
anaesthesia conversion folloed :6 :ronchospasm and pulmonar6
oedema re=uiring -?2.
* Categor6 $N acute fetal distress after eclampsia, CS1 attempt
produced inade=uate :loc, pre7
operative general anaesthesia as folloed :6 persisting
h6poFaemia and h6potension, transferred to
-?2.
* Categor6 $N maternal distress a:out sensation of spinal :loc,
pre7operative general anaesthesia
conversion and failed intu:ation at first attempt.
* Categor6 @N failure to site spinalN general anaesthesia
conversion, endo:ronchial intu:ation ith
desaturation, :rad6cardia and h6potension.
* "regional anaesthesia pro:lem# categor6 @N inade=uate spinal
re=uired general anaesthesia
conversion :efore deliver6, as6stole during peritoneal
stretching.
-
8/21/2019 A Prospective Audit of Regional Anaesthesia Failure in
5080 Caesarean Sections
11/19
:upivacaine $0 ml and fentan6l 400 HgN decreased consciousness
ensued and general anaesthesia as
induced.
* Categor6 $N fetal distress, standard spinal insertion, patient
developed severe pain after deliver6 :u
refused general anaesthesia, agreed to epidural hich as
performed in the lateral position, once
esta:lished surger6 proceeded painlessl6 "counted as general
anaesthesia conversion in totals#.
* Categor6 @N pulmonar6 oedema after deliver6 in a oman ith
severe aortic stenosis having lo dos
CS1.* Categor6 @N spinal, as6stole folloing sin incisionN
several 6ears :efore she had an almost identical
episode during her first Caesarean section.
* Categor6 $N spinal misplacement of epidural doseN a ! ml test
dose of 0.5J :upivacaine and 4 3 $00
000 adrenaline ith D.5 Hg fentan6l produced a C5 :loc ith arm
eaness.
* Categor6 !N epidural top7up for failure to progress, transient
drosiness and unresponsiveness durin
surger6 responded to naloFone.
* Categor6 !N :lood aspirated from epidural catheter after 5 ml
of top7up had :een givenN spinal
inserted for operation.
-n addition to these cases, there ere siF high :locs ith
respirator6 pro:lems, three high :locs
ith arm eaness, siF high :locs, three :rad6cardias, 40
h6potensions, three supraventricular
taFch6cardias, five non7anaesthetic drug or lateF reactions and
three miscellaneous.
uring this period, there ere 45E primar6 general anaesthetics
and E! regional anaesthetics
converted to general anaesthesia. ?here ere five critical
incidents "to serious# associated ith
general anaesthesia, all :ut one in cases of general anaesthetic
conversion. ?he rate of incidents as
$J. ?here ere 54 incidents "seven serious# related to the
regional anaesthesia in !50 regional
anaesthetics, a rate of 4.@J.
uring the period that critical incidents ere recorded, 8 cases
had a spinal anaesthetic in the
presence of an epidural that had not :een topped up for
Caesarean section. Mean volume of
h6per:aric :upivacaine 0.5J as $.@ ml &range 4.5%$.5 ml(.
'ne high sensor6 :loc "?4# as noted. -n
D4 cases ith an epidural that as apparentl6 in the correct space
:ut failed to produce an ade=uate
:loc for Caesarean after :eing topped7up, a spinal anaesthetic
as given. Mean volume of h6per:ar
:upivacaine as 4. ml &range 4.0%$.5 ml(. Seven high sensor6
:locs ere noted, ranging from C! to
C8 here documented. ive of these ere accompanied :6 d6spnoea and
one :6 hand eaness. -nthree of the D4 cases, the spinal
in>ection as apparentl6 made into the correct space :ut did
not
produce an6 change in :loc, possi:l6 :ecause it as made into the
epidural space containing local
anaesthetic rather than the su:arachnoid space.
Statistical anal6sis
2sing univariate anal6sis, there as no effect on failure rate of
audit 6ear and epidural drugs
including local anaesthetic, opioid or :icar:onate. ?here as a
significant effect of epidural
-
8/21/2019 A Prospective Audit of Regional Anaesthesia Failure in
5080 Caesarean Sections
12/19
adrenaline on the ris of :oth pre7operative and intra7operative
failure, and spinal insertion position
on the ris of pre7operative failure. urther statistical results
are availa:le from the author. ?he
results of the logistic regression anal6ses are shon in ?a:les
@%.
?a:le @ ;ogistic regression anal6sis of factors associated ith
regional anaesthesia failure. Gre7
operative failure includes conversion to another anaesthetic or
failure to achieve a satisfactor6 :loc
intra7operative failure includes unsatisfactor6 anaesthesia that
re=uired treatment.
?a:le 5 ;ogistic regression anal6sis of factors associated ith
spinal failure. Gre7operative failure
includes conversion to another anaesthetic or failure to achieve
a satisfactor6 :locN intra7operative
failure includes unsatisfactor6 anaesthesia that re=uired
treatment.
http://ovidsp.tx.ovid.com/spb/ovidweb.cgi#TT4%23TT4http://ovidsp.tx.ovid.com/spb/ovidweb.cgi?View+Image=00000524-200808000-00004%7CTT5&S=MJFNFPEGEADDKEOONCGLMDMLLPKMAA00&WebLinkReturn=Full+Text%3DL%7CS.sh.39.41%7C0%7C00000524-200808000-00004http://ovidsp.tx.ovid.com/spb/ovidweb.cgi?View+Image=00000524-200808000-00004%7CTT4&S=MJFNFPEGEADDKEOONCGLMDMLLPKMAA00&WebLinkReturn=Full+Text%3DL%7CS.sh.39.41%7C0%7C00000524-200808000-00004http://ovidsp.tx.ovid.com/spb/ovidweb.cgi#TT4%23TT4
-
8/21/2019 A Prospective Audit of Regional Anaesthesia Failure in
5080 Caesarean Sections
13/19
?a:le ;ogistic regression anal6sis of factors associated ith
epidural failure. Gre7operative failure
includes conversion to another anaesthetic or failure to achieve
a satisfactor6 :locN intra7operative
failure includes unsatisfactor6 anaesthesia that re=uired
treatment.
iscussion
?his audit o:served the anaesthetic practice in a large teaching
hospital. ?he overall use of
anaesthetic techni=ues in the 576ear period "general anaesthesia
5J, spinal !J, epidural top7up $J
CS1 5J#, is not dissimilar to national data from $00@ "general
anaesthesia 44J, spinal 55J, epidural
$0J, CS1 40J# &4@(, although the general anaesthesia rates
are not strictl6 compara:le as the nationa
data ma6 include cases of failed regional :loc.
Qational standards for rate of regional anaesthesia and
conversion of regional anaesthesia to general
anaesthesia ere pu:lished after the start of this audit. 'ur
data are largel6 compliant ith standard
first set :6 the
-
8/21/2019 A Prospective Audit of Regional Anaesthesia Failure in
5080 Caesarean Sections
14/19
provide regional anaesthesia for @J of omen having categor6 4
Caesarean section, 5J have their
operation ith a regional and are spared the riss of general
anaesthesia.
-
8/21/2019 A Prospective Audit of Regional Anaesthesia Failure in
5080 Caesarean Sections
15/19
An inade=uate pre7operative :loc as associated ith an increased
ris of intra7operative failure. -n
man6 cases here surger6 as started in the presence of an
inade=uate :loc, the reasons for this
ere unclear. oever, $0J of these cases ere started :ecause of
urgenc6 or ith a rising :loc.
+loc eFtent as assessed using cold sensation. ?he use of cold is
more specific :ut less sensitive tha
touch &4(. ?his is :orne out :6 the finding that !$J of
general anaesthetic conversions occurred
during the operation, mostl6 in the presence of an ade=uate
pre7operative :loc. Although the use of
touch to assess anaesthetic :loc for Caesarean section has :een
strongl6 recommended &4(, there ia lac of data shoing that it
can reduce the rate of intra7operative pain or general
anaesthetic
conversion, or indeed overall general anaesthetic conversion
&4D(.
?he ma>orit6 of spinals ere inserted in the right lateral
position. ?he sitting position as associated
ith a higher intra7operative failure rate using univariate
anal6sis "5.4J versus right lateral $.EJ#.
Su:dividing omen ho ere sitting for spinal insertion into groups
:ased on the indication for sittin
as an attempt to separate clinicall6 straightforard cases from
those ith o:esit6 or predicted
anatomical difficult6, hich might have :een confounding factors.
-ntra7operative failure occurred in
@.!J of cases here the spinal as inserted sitting :ecause of the
anaesthetist/s preference. 'ther
audit data has also suggested an increased chance of
intra7operative pain if the spinal is inserted
sitting &40(. oever, using logistic regression anal6sis,
insertion position as not found to :e a
significant factor affecting intra7operative failure.
-t has :een suggested that the use of spinal diamorphine does
not affect the =ualit6 of :loc assessed
ith touch sensation &48(, :ut reduces pain during surger6
&4E(. ?his audit found an increase in the
chance of pre7operative failure to achieve a successful :loc to
cold if a spinal opioid as not used,
:ut no difference in intra7operative failure. -ntra7operative
pain as found in !.5J of spinals ith anopioid and 44.4J ithout, :ut
as L 4J of spinals did not have a spinal opioid, the poer to detect
a
real difference is lacing.
An association :eteen nulliparit6 and increased pre7operative
failure for spinals is uneFplained. 'n
the other hand, preterm deliver6 has :een identified as a factor
in failure to esta:lish spinal :loc
&$0(.
Several randomised studies comparing epidural top7up solutions
have failed to find a clincall6
important difference :eteen different local anaesthetics or ith
the addition of fentan6l &44, 4$,
$4(. ?hese studies assessed time of onset of surgical :loc :ut
ere too small to detect differences in
failure rate. ?he use of different solutions in this audit as
spread such as to allo reasona:le
num:ers in each group for anal6sis ":upivacaine 58J, lidocaine
$!J, lidocaine7:upivacaine miF 4JN
adrenaline @JN :icar:onate $JN opioid 8!J#. Apart from
adrenaline, these factors did not feature in
the univariate or logistic regression anal6ses. Adrenaline,
hoever, approFimatel6 halved the ris :ot
of pre7operative and intra7operative failure. e have considered
an epidural top7up volume of $0%$@
ml to :e standard/ as anaesthetists usuall6 dra up $0 ml of
local anaesthetic and other ad>uncts
http://ovidsp.tx.ovid.com/spb/ovidweb.cgi#100%23100http://ovidsp.tx.ovid.com/spb/ovidweb.cgi#100%23100http://ovidsp.tx.ovid.com/spb/ovidweb.cgi#101%23101http://ovidsp.tx.ovid.com/spb/ovidweb.cgi#94%2394http://ovidsp.tx.ovid.com/spb/ovidweb.cgi#102%23102http://ovidsp.tx.ovid.com/spb/ovidweb.cgi#103%23103http://ovidsp.tx.ovid.com/spb/ovidweb.cgi#104%23104http://ovidsp.tx.ovid.com/spb/ovidweb.cgi#95%2395http://ovidsp.tx.ovid.com/spb/ovidweb.cgi#95%2395http://ovidsp.tx.ovid.com/spb/ovidweb.cgi#100%23100http://ovidsp.tx.ovid.com/spb/ovidweb.cgi#100%23100http://ovidsp.tx.ovid.com/spb/ovidweb.cgi#101%23101http://ovidsp.tx.ovid.com/spb/ovidweb.cgi#94%2394http://ovidsp.tx.ovid.com/spb/ovidweb.cgi#102%23102http://ovidsp.tx.ovid.com/spb/ovidweb.cgi#103%23103http://ovidsp.tx.ovid.com/spb/ovidweb.cgi#104%23104http://ovidsp.tx.ovid.com/spb/ovidweb.cgi#95%2395http://ovidsp.tx.ovid.com/spb/ovidweb.cgi#95%2395
-
8/21/2019 A Prospective Audit of Regional Anaesthesia Failure in
5080 Caesarean Sections
16/19
ma6 then :e included. Smaller volumes than $0 ml are associated
ith less ris of pre7operative
failure possi:l6 indicating ade=uac6 of the eFisting analgesic
:loc, hereas volumes of $5 ml or
a:ove are associated ith diminishing returns in terms of
success.
?he most common indication for primar6 general anaesthesia as
Caesarean section urgenc6
associated ith fetal distress, hether considering all cases,
categor6 4 cases, or cases here
epidural analgesia as used during la:our :ut not topped up.
Conversion of inade=uate regionalanaesthesia to general anaesthesia
accounted for !5J of all omen ho had a general anaesthetic.
?his percentage is higher as the the primar6 general anaesthetic
rate falls &@(. -t is pro:a:l6
appropriate that 88J of general anaesthetic conversions in
categor6 4 cases ere pre7operative.
ains et al. estimated that in the late 4E80s, the ris of death
from o:stetric general anaesthesia
as 4D times that of regional anaesthesia &$$(. Shi:li
and
-
8/21/2019 A Prospective Audit of Regional Anaesthesia Failure in
5080 Caesarean Sections
17/19
5 ;ucas Q, Ientis SM, Kinsella SM, et al. 2rgenc6 of caesarean
section3 a ne classification. ournal
of the
-
8/21/2019 A Prospective Audit of Regional Anaesthesia Failure in
5080 Caesarean Sections
18/19
4
-
8/21/2019 A Prospective Audit of Regional Anaesthesia Failure in
5080 Caesarean Sections
19/19
igure. Qo Caption availa:le.
http://ovidsp.tx.ovid.com/spb/ovidweb.cgi?View+Image=00000524-200808000-00004%7CFFAU1&S=MJFNFPEGEADDKEOONCGLMDMLLPKMAA00&WebLinkReturn=Full+Text%3DL%7CS.sh.39.41%7C0%7C00000524-200808000-00004