Embed Size (px)
Citation preview

A Phase I/II Trial of Sitravatinib Combined with Nivolumabin Patients with Advanced Clear Cell Renal Cell Cancer that
Progressed on Prior Anti-Angiogenic Therapy
Pavlos Msaouel, Peter F. Thall, Ying Yuan, Xuemei Wang, Eric Jonasch, Jianjun Gao, Matthew T. Campbell, Amishi Yogesh Shah, Paul Gettys Corn, Alda Tam, Kamran Ahrar, Priya Rao, Kanishka Sircar, Hirak Der-Torossian, Nizar M. Tannir
Pavlos Msaouel, MD, PhD

Disclosures
Pavlos Msaouel, MD, PhD
• Advisory Boards / Honoraria:o Mirati Therapeutics, Bristol-Myers Squibb
• Non-branded educational programs: o Exelixis, Pfizer
• Clinical Trials with Grant Support:o Bristol-Myers Squibb, Mirati Therapeutics, Takeda Pharmaceutical Company

Sitravatinib (MGCD-516): A Spectrum-Selective Kinase Inhibitor• Sitravatinib is an orally available small molecule that inhibits a
spectrum of related receptor tyrosine kinases (RTKs) including:o TAM family (TYRO3, AXL, MERTK) o Split family (VEGFR2/PDGFR and c-KIT)o c-MET
• Inhibition of these target classes may enhance anti-tumor activity through:
o Improvement of tumor perfusion by reducing intratumoral pressureo Depletion of immunosuppressive cell subsets from the tumor
microenvironmento Increased T cell priming
TK
CMGC
CAMK
AGC
CK1
TKL
STE
TRK FAMILYRETDDR1/2METTAM FAMILYVEGFR / PDGFRSPLIT RTKS: KIT
Pavlos Msaouel, MD, PhD

Phase 1B Trial of Single-Agent Sitravatinib (Update from ESMO 2018)
Pavlos Msaouel, MD, PhD
2L+ mccRCC 516-001 Expansion Cohort (VEGF-refractory)
Study cycles of 21 days, with disease assessment scans every 2 cyclesData cut-off: 24-Jul-2019; update since initial presentation at ASCO 2018 Congress. Response data per investigator assessment.
BEST RESPONSE(Evaluable Patients, N=32)
DURATION OF TREATMENT(Evaluable Patients, N=32)
30/32 (94%) Clinical Benefit (SD+PR+CR)8/32 (25%) Confirmed Objective Response

Sitravatinib in the Tumor Microenvironment (TME)
Pavlos Msaouel, MD, PhD

Hypothesis, Objectives, Eligibility Criteria & Statistics
Pavlos Msaouel, MD, PhD
• Hypothesis: sitravatinib can be administered in combination with nivolumab at an effective dose and augment nivolumab responses in patients with metastatic clear cell RCC who progressed on anti-angiogenic therapy.
OBJECTIVES/ENDPOINTS• PRIMARY
• Dose-finding based on safety (no DLT within 12 weeks) and efficacy (no PD within 6 weeks)
• SECONDARY• Efficacy endpoints including ORR (by two consecutive
measurements), PFS, OS• Quality of life & psychosocial measures: FACT, SF-12, CES-D
(depression), history of depression, FMCS• EXPLORATORY
• Circulating PD-L1, immune cell populations and cytokines
• Tumor cell PD-L1 expression, tumor infiltrating immune cell populations & gene expression signatures
• Tumor gene alterations in circulation & in tumor tissue
KEY ELIGIBILITY CRITERIA• Similar eligibility criteria to those used for
CheckMate 025• Histologically-confirmed clear cell RCC • Disease progression after 1-2 prior anti-angiogenic
therapies (prior cytokine therapy allowed)
• Measurable disease, as per RECIST Version 1.1
• KPS ≥70
STATISTICS• Dose-finding is performed using the sequentially
adaptive phase I-II late-onset EffTox (Lo-EffTox) trade-off-based design of Jin et al. J Am Stat Assoc2014;109:525-36.

Study Design
Pavlos Msaouel, MD, PhD
Tumors Included:Metastatic RCC with a
Clear cell component and PD after VEGF tx
Four sitravatinib dose levels: 60, 80, 120 and 150 mg/day
1st cohort: 80 mg PO daily
2 weeks to achieve steady state
Day 15:Begin nivolumab 240 mg q2 wks (after week 12: can switch to nivolumab
480 mg q4 wks)
Peripheral blood and optional tissue sample for correlative studies
Week 6 (day 42):Evaluate response to treatment
Peripheral blood and optional tissue sample for correlative studies
Continue treatment & evaluate every 6 wks x1 year, then every 12 wks
until PD or toxicity
Peripheral blood and optional tissue sample for correlative studies
Day 1:Begin sitravatinibp.o. daily at pre-specified dose per
EffTox

Patient Disposition
Pavlos Msaouel, MD, PhD
Enrolled Population (as of 1/1/2020) 40
Safety Population (received ≥1 dose) 40 (100%)
Early treatment discontinuation (prior to 1st tumor assessment) due to treatment-related AE (hypertensive crisis) 1
Too early for 1st tumor assessment (<8 wks on study) 1
Evaluable Population for Efficacy (≥1 on-study tumor assessment) 38 (95%)

Baseline Patient Characteristics (N = 40 patients)
Pavlos Msaouel, MD, PhD
Age, years Median (IQR)Range
68.0 (55.5 - 71.0)45.0 - 85.0
Gender, n (%) MaleFemale
35 (87.5)5 (12.5)
Race, n (%) CaucasianBlack
38 (95)2 (5)
IMDC risk group, n (%) FavorableIntermediatePoor
5 (12.5)34 (85)1 (2.5)
Karnofsky PS, n (%) 100908070
25 (62.5)12 (30)2 (5)
1 (2.5)Previous nephrectomy,n (%)
YesNo
35 (87.5)5 (12.5)
Previous radiotherapy,n (%)
YesNo
8 (20)32 (80)
Target lesions per RECIST, n (%)
1≥2
7 (17.5)33 (82.5)
Most common active sites of metastasis, n (%)
LungLymph nodeLiverBone
21 (52.5)27 (67.5)11 (27.5)13 (32.5)
Number of previous systemic cancer therapies
12
35 (87.5)5 (12.5)
Previous anti-angiogenic therapy, n (%)
SunitinibPazopanibAxitinib
14 (35)23 (57.5)
6 (15)
Duration of 1st line systemic therapy, months
Median (IQR)Range
10.8 (4.9 – 22.3)0.5 – 93.2
Initial sitravatinib daily dose, n (%)
150 mg 120 mg
80 mg
3 (7.5)22 (55)
15 (37.5)

-100%
-30%-33%
-35%-40%-43%-45% -55% -63%
-69%-73%-75% -88% -100%
-100%
0% 0%-5% -9%-9% -17%
-17%-17%-17%-17%-18%-19% -26%
-27%-28%-29%-29%
-35% -47% -65%
83%28%27%
* * * † †
-100%-90%-80%-70%-60%-50%-40%-30%-20%-10%
0%10%20%30%40%50%60%70%80%90%
100%
120120 80120 80120120120 80120120150 80120 80 80 80 80 80 80 80120120120120120120120120120120120 80 80120150150 80
Max
imum
% C
hang
e fr
om B
asel
ine
Unconfirmed CR Confirmed PRSD PDRECIST Cutoff for PR, 30% Unconfirmed CR/PR followed by PDResidual disease in NTL On study as of 01-Jan-20
Cohort
Cut-off date 01Jan20201 METEOR (Choueiri TK, NEJM, 2015); 2 CHECKMATE-025 (Motzer RJ, NEJM, 2015)
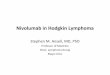
Efficacy
Pavlos Msaouel, MD, PhD
ORR in this setting:Everolimus1, 2 3-5%Cabozantinib1 17-21%Nivolumab2 25%
BEST RESPONSE(Evaluable Patients, N=38)
35/38 (92%) Clinical Benefit (SD+PR+CR)15/38 (39%) Confirmed Objective Response

Efficacy
Pavlos Msaouel, MD, PhD
Median F/U 17.7 mo(95% CI 11.0 to 24.5)
Median OS not reached30/38 patients (79%) are alive
PDPD
PDPD
PDPDPD
PDPDPDWithdrawal of consent
PDWithdrawal of consent
PDPD
PDPD
AE (pancreatitis)PD
AE (acute kidney injury)AE (myalgia)
PD
4 8 12 16 20 24 28 32 36 40 44 48 52 56 60 64 68 72 76 80 84 88 92 96 100
12080
120120
8080
12080
120120120
80120
8080
12080
12080
120120
80120150
8080
120120
80120120
80150120150120120120
Weeks
Unconfirmed CR Confirmed PR
SD PD
On Study PD Off study
Sitravatinib +Nivolumab 10.3 mo(95% CI 6.8 to 13.8)
PFS in this setting:Everolimus1, 2 3.8-4.4 moCabozantinib1 7.4 moNivolumab 2 4.6 mo
Cut-off date 01Jan20201 METEOR (Choueiri TK, NEJM, 2015); 2 CHECKMATE-025 (Motzer RJ , NEJM, 2015)

• Treatment-related Grade 4 events: ↑lipase in 3/40 (8%) pts, ↑amylase in 2/40 (5%) ptsAKI, sepsis, hypertension in 1/40 pts each (3%)
• Treatment-related Grade 5 event: nivolumab-related myasthenia gravis in 1/40 pts (3%) 1/40 pts (52.5%).
Most Frequent (>15%) Treatment-Related Adverse Events (Sitravatinib and/or Nivolumab)
Pavlos Msaouel, MD, PhD
Adverse Event Safety Population (N=40)
All Grades n (%)
Grade ≥3 n (%)
Any adverse event 40 (100%) 30/40 (75%)Diarrhea 29 (73%) 4 (10%)Fatigue 27 (68%) 4 (10%)↑ Alanine aminotransferase 23 (58%) 2 (5%)Lipase elevated 20 (50%) 12 (30%)Proteinuria 18 (45%) 5 (13%)Anorexia 17 (43%) 1 (3%)↑ Aspartate aminotransferase 17 (43%) 0Abdominal pain 14 (35%) 0Amylase elevated 14 (35%) 5 (13%)Nausea 14 (35%) 0Hoarseness 13 (32%) 0
Adverse Event Safety Population (N=40)
All Grades n (%)
Grade ≥3 n (%)
Weight loss 13 (32%) 0Constipation 12 (30%) 0↑ creatinine 12 (30%) 1 (3%)Acneiform rash 12 (30%) 0Hyperkalemia 11 (28%) 0Hypertension 11 (28%) 3 (8%)Hypothyroidism 11 (28%) 0Hand-Foot Syndrome 10 (25%) 0Maculopapular rash 9 (23%) 0Dyspnea 8 (20%) 0Other endocrine disorders 8 (20%) 1 (3%)Anemia 7 (18%) 1 (3%)

• Treatment-related Grade 4 events: ↑lipase in 3/40 (8%) pts, ↑amylase in 2/40 (5%) ptsAKI, sepsis, hypertension in 1/40 pts each (3%)
• Treatment-related Grade 5 event: nivolumab-related myasthenia gravis in 1/40 pts (3%) 1/40 pts (52.5%).
Most Frequent (>15%) Treatment-Related Adverse Events (Sitravatinib and/or Nivolumab)
Pavlos Msaouel, MD, PhD
Adverse Event Safety Population (N=40)
All Grades n (%)
Grade ≥3 n (%)
Any adverse event 40 (100%) 30/40 (75%)Diarrhea 29 (73%) 4 (10%)Fatigue 27 (68%) 4 (10%)↑ Alanine aminotransferase 23 (58%) 2 (5%)Lipase elevated 20 (50%) 12 (30%)Proteinuria 18 (45%) 5 (13%)Anorexia 17 (43%) 1 (3%)↑ Aspartate aminotransferase 17 (43%) 0Abdominal pain 14 (35%) 0Amylase elevated 14 (35%) 5 (13%)Nausea 14 (35%) 0Hoarseness 13 (32%) 0
Adverse Event Safety Population (N=40)
All Grades n (%)
Grade ≥3 n (%)
Weight loss 13 (32%) 0Constipation 12 (30%) 0↑ creatinine 12 (30%) 1 (3%)Acneiform rash 12 (30%) 0Hyperkalemia 11 (28%) 0Hypertension 11 (28%) 3 (8%)Hypothyroidism 11 (28%) 0Hand-Foot Syndrome 10 (25%) 0Maculopapular rash 9 (23%) 0Dyspnea 8 (20%) 0Other endocrine disorders 8 (20%) 1 (3%)Anemia 7 (18%) 1 (3%)
Treatment discontinuation rate due to AEs: 4/40 patients (10%)

Toxicities
Pavlos Msaouel, MD, PhD
• Toxicities requiring dose-reduction of sitravatinib have been noted in 21/40 pts (52.5%).
• 15/21 (71.4%) of these DLTs occurred within 12 weeks and were thus captured by the late-onset EffTox design.
• All three patients on the 150 mg dose of sitravatinib experienced DLT within 12 weeks.

Conclusions
Pavlos Msaouel, MD, PhD
• In this single-arm phase I/II study of sitravatinib + nivolumab using similar enrollment criteria as Checkmate 025, we observed higher ORR and longer PFS than historically reported with single-agent nivolumab or single-agent cabozantinib.
• The combination has an acceptable toxicity profile with manageable AEs.
• Sitravatinib 120 mg was the most frequently selected dose by the EffTox algorithm and can be used as the RP2D.
• Analyses of patient-reported outcomes and tissue & blood correlative studies are ongoing.
• Sitravatinib 120 mg + nivolumab is now being explored in other tumor types.

Acknowledgements
Pavlos Msaouel, MD, PhD
• Thank you to all the patients and their families.
• Thank you to our research nurses and data coordinators: Shehanie Brana, Joshua Abraham, Lauren King, Joanne Sturt-Rochon, Donna Juarez, and Cherie Perez.
• This investigator-initiated study is supported by Mirati Therapeutics, Inc., and by a grant from Gateway for Cancer Research.