Embed Size (px)
Citation preview
A Phase Ib/II Trial of Trastuzumab-DM1 (T-DM1) with Pertuzumab for Women with HER2-Positive Locally-Advanced or Metastatic Breast Cancer who were Previously Treated with Trastuzumab
K. Miller,1 L. Gianni,2 F. Andre,3 V. Dieras,4 R.L. Mahtani,5 N. Harbeck,6 J.E. Huang,7 T. Shih,7 Y. Choi,7 H.A. Burris1
1Indiana University Melvin and Bren Simon Cancer Center, Indianapolis, IN; 2Montabone Unit for New Drug Development, Istituto Nazionale dei Tumori, Milano, Italy; 3Inst Gustave Roussy, Villejuif, France; 4Institut Curie, Paris, France; 5Boca Raton Comprehensive Cancer Center, Boca Raton, FL;
6Breast Center, Dept. OB & GYN, University of Cologne, Cologne, Germany; 7Genentech, Inc., South San Francisco, CA; 8Sarah Cannon Research Institute, Nashville, TN
ASCO 2010
T-DM1
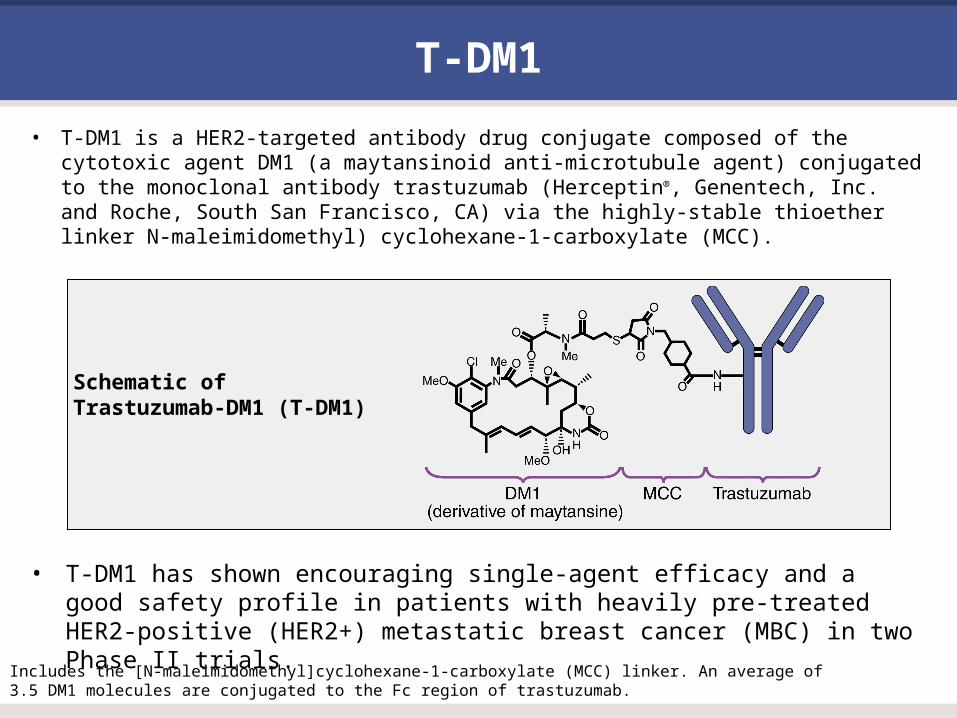
• T-DM1 is a HER2-targeted antibody drug conjugate composed of the cytotoxic agent DM1 (a maytansinoid anti-microtubule agent) conjugated to the monoclonal antibody trastuzumab (Herceptin®, Genentech, Inc. and Roche, South San Francisco, CA) via the highly-stable thioether linker N-maleimidomethyl) cyclohexane-1-carboxylate (MCC).
Includes the [N-maleimidomethyl]cyclohexane-1-carboxylate (MCC) linker. An average of 3.5 DM1 molecules are conjugated to the Fc region of trastuzumab.
Schematic of Trastuzumab-DM1 (T-DM1)
• T-DM1 has shown encouraging single-agent efficacy and a good safety profile in patients with heavily pre-treated HER2-positive (HER2+) metastatic breast cancer (MBC) in two Phase II trials.

Pertuzumab
• Pertuzumab (Genentech, Inc. and Roche, South San Francisco, CA), a recombinant, humanized monoclonal antibody directed against HER2, binds a domain of HER2 that does not overlap with the epitope recognized by trastuzumab, inhibits ligand-activated heterodimerization with other HER receptors, most notably HER3.
• The combination of pertuzumab and trastuzumab or T-DM1 provides a complementary mode of action that may be efficacious for treatment of HER2-overexpressing diseases.
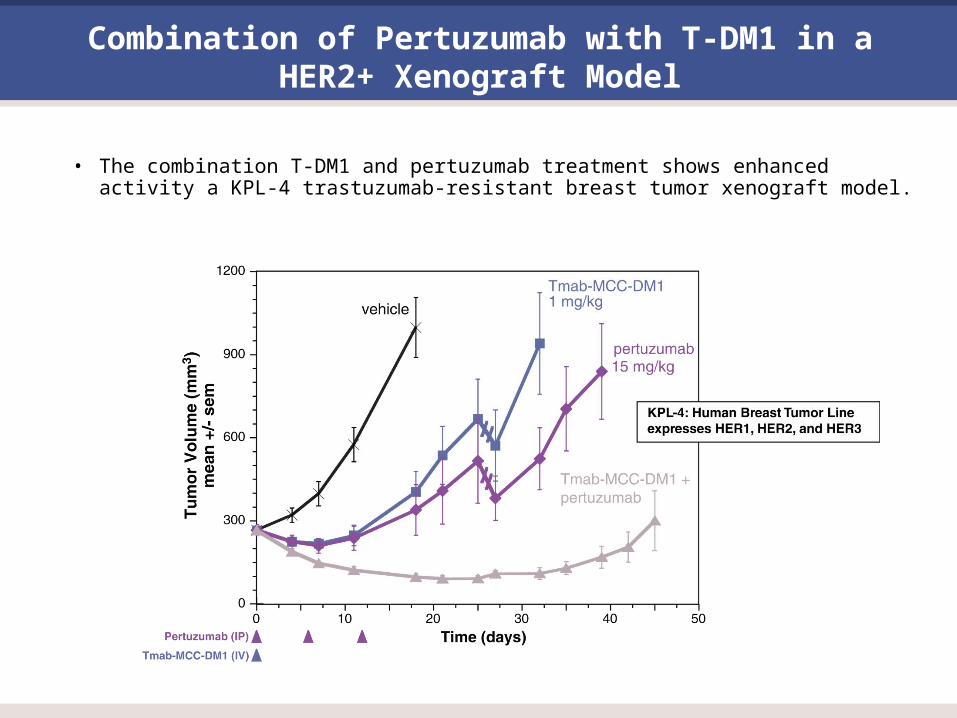
Combination of Pertuzumab with T-DM1 in a HER2+ Xenograft Model
• The combination T-DM1 and pertuzumab treatment shows enhanced activity a KPL-4 trastuzumab-resistant breast tumor xenograft model.
Study TDM4373g
• This global, single-arm, Phase Ib/II study investigates the safety and effiicacy of the combination of T-DM1 with pertuzumab in patients with HER2-positive locally advanced or MBC.
• In the 3+3 design, patients received pertuzumab (840 mg, Cycle 1; 420 mg, Cycle 2 and beyond) with T-DM1 (3.0 mg/kg in Cohort 1 and, in the absence of dose limiting toxicity [DLT], 3.6 mg/kg in Cohort 2).
• Once dose escalation was complete, additional patients were added to the expansion phase.
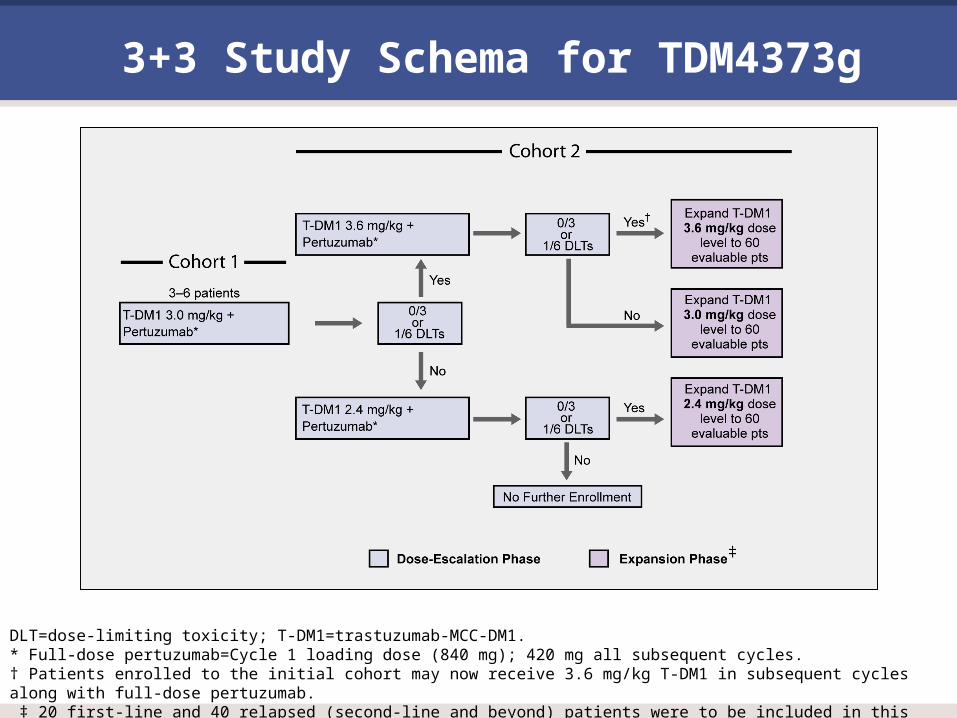
3+3 Study Schema for TDM4373g
DLT=dose-limiting toxicity; T-DM1=trastuzumab-MCC-DM1.* Full-dose pertuzumab=Cycle 1 loading dose (840 mg); 420 mg all subsequent cycles.† Patients enrolled to the initial cohort may now receive 3.6 mg/kg T-DM1 in subsequent cycles along with full-dose pertuzumab. ‡ 20 first-line and 40 relapsed (second-line and beyond) patients were to be included in this phase.
TDM4373g Objectives
Primary objectives:
• To characterize the safety and tolerability of the combination of T-DM1 and pertuzumab administered every 3 weeks (q3w) to patients with HER2-positive locally advanced or MBC
• To evaluate the pharmacokinetics of T-DM1 when T-DM1 and pertuzumab are administered on this schedule
• To make a preliminary assessment of the efficacy of T-DM1 and pertuzumab administered on this schedule, as measured by objective response rate (ORR) based on investigator assessment.
Secondary objectives:
• To estimate PFS of patients who receive T-DM1 and pertuzumab administered on this schedule
• To assess the duration of response to T-DM1 and pertuzumab administered on this schedule
• To assess the development of anti-therapeutic antibodies to T-DM1
Key Inclusion Criteria
• Histologically-documented locally advanced or metastatic HER2-positive BC (HER2-positivity documented as FISH+ or CISH+ or IHC 3+ by local laboratory assessment)
• Measurable disease
• Prior HER2-directed therapy (for patients second-line or beyond)
• No prior T-DM1 or pertuzumab therapy
• Cardiac ejection fraction >55% by either echocardiogram (ECHO) or multiple gated acquisition (MUGA scan).
Key Exclusion Criteria
• History of exposure to cumulative doses of anthracyclines >500 mg/m2 doxorubicin.
• History of cardiac dysfunction.
Study Assessments
• Patients were monitored for safety and tolerability of treatment weekly during the first 3 cycles, every cycle thereafter, at the treatment termination visit, and during the follow up period (30 days after ending study treatment).
• Radiographic assessment of disease status was conducted at screening and then every two cycles thereafter throughout the duration of the study based on modified RECIST criteria.
• Echocardiograms (ECHO) or multi-gated acquisition (MUGA) scans were performed at screening, at the end of Cycle 1, and then every three cycles thereafter.
• Any patient with a significant decline in ejection fraction or with symptomatic congestive heart failure was withdrawn from study treatment.
Statistical Analysis
• This report assesses safety and efficacy among relapsed patients (n=44), who were evaluable as of December 14, 2009.
• ORR with 95% confidence intervals (CI) were estimated from complete or partial responses on two consecutive occasions >4 weeks apart, through at least 4 cycles or disease progression/death, using the Blyth-Still-Casella method.
• Patients without a valid post-baseline tumor assessment were counted as non-responders.
Results
• To date, 67 patients have enrolled in the study—45 relapsed patients (second-line or beyond therapy) and 22 patients with newly diagnosed HER2-positive MBC (first-line therapy).
• One patient did not have safety data available and was excluded from analysis, leaving 44 relapsed patients.
Dose-Escalation Phase
• 9 patients were enrolled in this phase.
• No dose-limiting toxicity (DLT) was observed among the 3 patients in Cohort 1 (3.0 mg/kg T-DM1 + full-dose pertuzumab).
• Among the first 3 patients in Cohort 2 (3.6 mg/kg T-DM1 + full-dose pertuzumab), there was 1 DLT of Grade 4 thrombocytopenia; the patient’s T-DM1 dose was reduced to 2.4 mg/kg.
• Cohort 2 expanded to 6 patients; there were no further DLTs.
• The expansion phase dose for T-DM1 was determined to be 3.6 mg/kg.
Expansion Phase
• 58 patients were added in this phase.
On-Study Treatment
• All patients were treated with at least 1 cycle of T-DM1 and pertuzumab with a median of 4 cycles of both study drugs (range 1–9).
• 12/44 (27.3%) patients had discontinued from study as of the data cutoff.
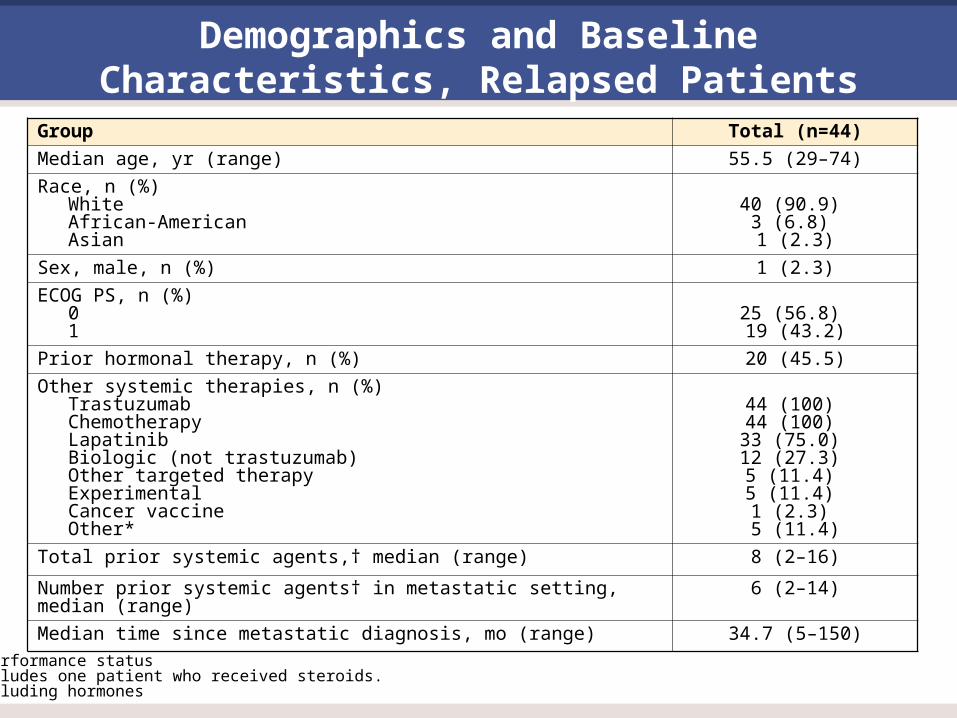
Demographics and Baseline Characteristics, Relapsed Patients
Group Total (n=44)
Median age, yr (range) 55.5 (29–74)
Race, n (%) White African-American Asian
40 (90.9)
3 (6.8) 1 (2.3)
Sex, male, n (%) 1 (2.3)
ECOG PS, n (%) 0 1
25 (56.8) 19 (43.2)
Prior hormonal therapy, n (%) 20 (45.5)
Other systemic therapies, n (%)Trastuzumab Chemotherapy Lapatinib Biologic (not trastuzumab) Other targeted therapy Experimental Cancer vaccine Other*
44 (100) 44 (100) 33 (75.0) 12 (27.3) 5 (11.4) 5 (11.4) 1 (2.3) 5 (11.4)
Total prior systemic agents,† median (range) 8 (2–16)
Number prior systemic agents† in metastatic setting, median (range) 6 (2–14)
Median time since metastatic diagnosis, mo (range) 34.7 (5–150)
PS=performance status* Includes one patient who received steroids.† Excluding hormones

Objective Responses among Relapsed Patients
• ORR results are from 28 patients who had been on study for at least 12 weeks (4 cycles), or progressed or died as of the data cutoff.
• The median number of T-DM1 doses received was 5 (range: 2–9).
• ORR was 35.7% (10/28 patients; 95% CI, 19.3–55.9).
– All responses were confirmed partial responses.
– Among the 13 patients with stable disease, there were 2 unconfirmed responses.

Objective Responses among Relapsed Patients (cont’d)
Cohort 1 (n=3) Cohort 2 (n=25) Total (n=28)
Complete response
0 0 0
Partial response 2 (66.7) 8 (32.0) 10 (35.7)
Stable disease 1 (33.3) 12 (48.0) 13 (46.4)
Progressive disease
0 4 (16.0) 4 (14.3)
Missing 0 1 (4.0) 1 (3.6)
Safety
• The Phase I portion of the study confirmed that it was safe to combine full doses of T-DM1 and pertuzumab.
• One Grade 5 AE (pneumonia) was reported in a patient who died concomitantly due to disease progression, prior to first tumor assessment; it was considered unrelated to study treatment.
• There were two Grade 4 events, both thrombocytopenia, in two patients (including the DLT), resulting in T-DM1 dose reduction (to 2.4 mg/kg) in one patient.
• 6 patients had dose reductions due to AEs
– Grade 4 thrombocytopenia, Grade 1–2 thrombocytopenia, Grade 2 neutropenia, Grade 3 nausea and vomiting, Grade 3 elevation in aspartate aminotransferase level, and Grade 3 elevation in aspartate and alanine aminotransferase levels with subsequent Grade 4 thrombocytopenia after dose reduction.
• One patient discontinued both drugs due to Grade 3 left ventricular dysfunction.
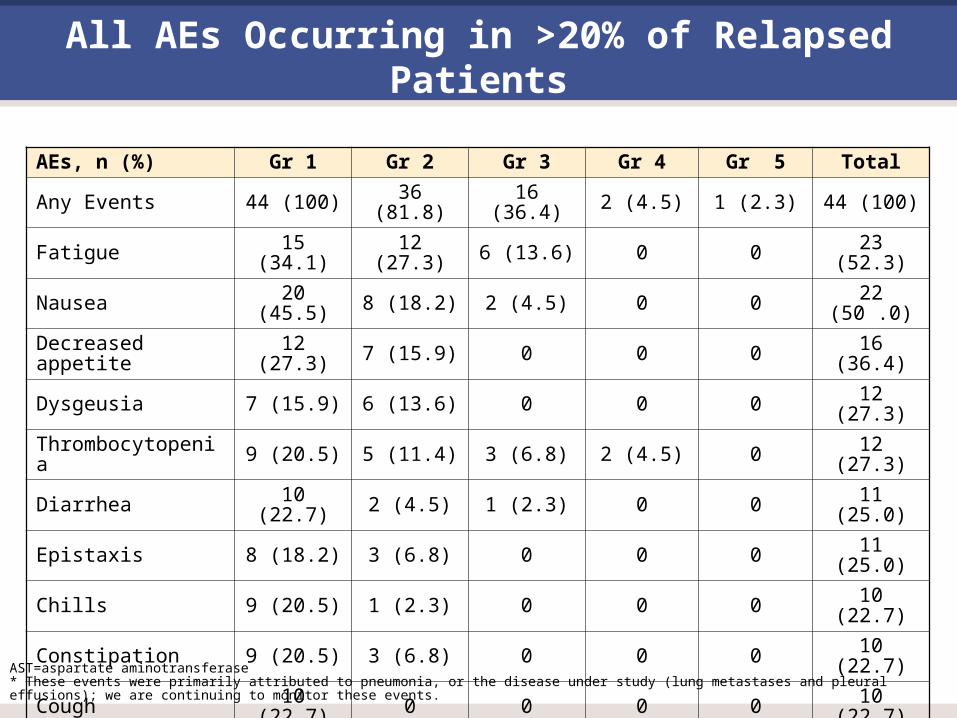
All AEs Occurring in >20% of Relapsed Patients
AEs, n (%) Gr 1 Gr 2 Gr 3 Gr 4 Gr 5 Total
Any Events 44 (100) 36 (81.8) 16 (36.4) 2 (4.5) 1 (2.3) 44 (100)
Fatigue 15 (34.1) 12 (27.3) 6 (13.6) 0 0 23 (52.3)
Nausea 20 (45.5) 8 (18.2) 2 (4.5) 0 0 22 (50 .0)
Decreased appetite 12 (27.3) 7 (15.9) 0 0 0 16 (36.4)
Dysgeusia 7 (15.9) 6 (13.6) 0 0 0 12 (27.3)
Thrombocytopenia 9 (20.5) 5 (11.4) 3 (6.8) 2 (4.5) 0 12 (27.3)
Diarrhea 10 (22.7) 2 (4.5) 1 (2.3) 0 0 11 (25.0)
Epistaxis 8 (18.2) 3 (6.8) 0 0 0 11 (25.0)
Chills 9 (20.5) 1 (2.3) 0 0 0 10 (22.7)
Constipation 9 (20.5) 3 (6.8) 0 0 0 10 (22.7)
Cough 10 (22.7) 0 0 0 0 10 (22.7)
Pyrexia 9 (20.5) 2 (4.5) 0 0 0 10 (22.7)
Vomiting 9 (20.5) 1 (2.3) 2 (4.5) 0 0 10 (22.7)
AST increase 6 (13.6) 6 (13.6) 3 (6.8) 0 0 9 (20.5)
Dyspnea* 6 (13.6) 4 (9.1) 1 (2.3) 0 0 9 (20.5)
AST=aspartate aminotransferase* These events were primarily attributed to pneumonia, or the disease under study (lung metastases and pleural effusions); we are continuing to monitor these events.
Serious AEs
• 10 serious AEs occured in 7 patients:
– Pneumonia (in 2 patients, Grades 3 and 5)
– Diarrhea/fatigue/nausea/vomiting (in 1 patient, Grade 3),
– and in 1 patient each, cellulitis, dyspnea, hematuria, and URI (Grade 3).
Conclusions
• In combination with full-dose pertuzumab (840 mg loading/420 mg thereafter), the T-DM1 dose was determined to be 3.6 mg/kg.
• T-DM1 + full dose pertuzumab has an encouraging safety and tolerability profile.
– Thrombocytopenia and hepatic transaminase elevations generally were transient, reversible, and did not occur at a higher rate than that observed with T-DM1 alone.
• Preliminary efficacy of this combination is promising.





























