Embed Size (px)
Citation preview

Cancer Therapy: Clinical
A Pharmacodynamic/Pharmacokinetic Study ofFiclatuzumab in Patients with Advanced Solid Tumors andLiver Metastases
Josep Tabernero1, Maria Elena Elez1, Maria Herranz1, Isabel Rico1, Ludmila Prudkin1, Jordi Andreu1,Jose Mateos2, Maria Josep Carreras1, May Han3, James Gifford3, Marc Credi3, Wei Yin3,Shefali Agarwal3, Philip Komarnitsky3, and Jose Baselga4
AbstractPurpose: This study evaluated the safety, tolerability, pharmacodynamics, pharmacokinetics, and
antitumor activity of ficlatuzumab, a humanized hepatocyte growth factor (HGF) inhibitory monoclonal
antibody, as monotherapy in patients with advanced solid tumors and liver metastases.
Patients and Methods: Patients with p-Met (phosphorylated c-Met)–positive tumors enrolled in three
dose-escalation cohorts, receivingficlatuzumab2, 10, or 20mg/kgonceper 14-day cycle. Pharmacodynamic
changes in liver tumor biopsies and serum, pharmacokinetics, safety, and clinical activity were assessed.
Results:Nodose-limiting toxicities occurred in the 19 patients enrolled (n¼ 6, 2mg/kg; n¼ 7, 10mg/kg;
n ¼ 6, 20 mg/kg). The most frequent diagnosis was colorectal cancer (n ¼ 15; 79%). The most common
treatment-emergent adverse events were asthenia, peripheral edema, hepatic pain (32% each), and cough
(26%). Laboratory abnormalities of decreased serum albumin were present in all patients. Ficlatuzumab at
20 mg/kg lowered median levels of tumor p-Met (�53%), p-ERK (�43%), p-Akt (�2%), and increased
median HGF levels (þ33%), at the last on-study time point relative to baseline. Mean serum HGF levels
increased with ficlatuzumab dose and number of treatment cycles. Ficlatuzumab exhibited linear phar-
macokinetics and long terminal half-life (7.4–10 days). Best overall response was stable disease in 28% of
patients, including 1 patient with pancreatic cancer with stable disease >1 year.
Conclusions: Ficlatuzumab exhibited good safety/tolerability and demonstrated ability tomodulate the
HGF/c-Met pathway and downstream signaling in the tumor in patients with advanced solid tumors. Safety,
pharmacodynamic, and pharmacokinetic data for ficlatuzumab confirmed the recommended phase II dose
of 20 mg/kg once per 14-day cycle. Clin Cancer Res; 20(10); 2793–804. �2014 AACR.
IntroductionActivation of the receptor tyrosine kinase c-Met via its
ligand, HGF (1, 2), mediates proliferation, motility, anddifferentiation in several different cell types (3). Dysregula-tionof theHGF/c-Met signaling axis can lead to aberrant cellproliferation and drug resistance and promote cell migra-
tion, invasive growth, and angiogenesis (3–9), and isobserved in many malignancies, including those of thepancreas, lung, stomach, breast, and kidney (3, 5, 10–16).
c-Met pathway activation has been associated with pro-gression from primary to metastatic disease, particularlywith liver metastasis (17–22). Serum HGF levels are elevat-ed inpatientswithbreast cancerwithmalignant liver lesions(18), and have been correlated with liver metastases versusmetastases at other sites (21). Dysregulation of c-Met isassociated with the presence of liver metastases in patientswith gastric (17) and colorectal cancer (22). These findingssuggest that targeting the HGF/c-Met pathway may bebeneficial for patients with advanced solid tumors and livermetastases; in addition, patients with liver metastases arelikely to have detectable p-Met (phosphorylated c-Met),making it possible to evaluate the p-Met changes in livermetastases after treatment.
Ficlatuzumab (AV-299; formerly SCH 900105) is ahumanized HGF inhibitory monoclonal antibody that neu-tralizes HGF/c-Met binding and HGF-induced c-Met phos-phorylation (23). Ficlatuzumab inhibits HGF-dependentgrowth of tumors in preclinical tumor xenograft models of
Authors' Affiliations: 1Vall d'Hebron University Hospital, Vall d'HebronInstitute of Oncology (VHIO), Universitat Aut�onoma de Barcelona; 2CRCHospital Quir�on de Barcelona, Barcelona, Spain; 3AVEO Oncology,Cambridge, Massachusetts; and 4Memorial Sloan-Kettering CancerCenter, New York, New York
Note: Supplementary data for this article are available at Clinical CancerResearch Online (http://clincancerres.aacrjournals.org/).
J. Tabernero and M.E. Elez contributed equally to this article.
Corresponding Author: Josep Tabernero,Medical OncologyDepartment,Vall d'Hebron University Hospital, Vall d'Hebron Institute of Oncology,Universitat Aut�onoma de Barcelona, P. Vall d'Hebron 119–129, 08035Barcelona, Spain. Phone: 34-93-489-4301; Fax: 34-93-274-6059; E-mail:[email protected]
doi: 10.1158/1078-0432.CCR-13-1837
�2014 American Association for Cancer Research.
ClinicalCancer
Research
www.aacrjournals.org 2793
on June 27, 2020. © 2014 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst March 14, 2014; DOI: 10.1158/1078-0432.CCR-13-1837

glioblastoma (24) and non–small cell lung cancer (NSCLC;ref. 25). In a first-in-human dose-escalation study, ficlatu-zumab 20 mg/kg once every 14-day cycle was established asthe recommended phase II dose (RP2D; ref. 26). Ficlatuzu-mab is in development for the treatment of solid tumors,including a phase Ib/II study in NSCLC (27, 28).
This study reports the safety/tolerability, pharmacody-namic effects in tumors and serum, pharmacokinetic pro-file, and preliminary antitumor activity of ficlatuzumabmonotherapy in patients who have solid tumors with livermetastases that express activated c-Met.
Patients and MethodsEnrollment criteria
All patients provided informed consent before enroll-ment. Patients were of the age�18 years with histologicallyconfirmed advanced unresectable colorectal, breast, gastric/esophageal, or pancreatic cancer with liver metastases ame-nable to biopsy. Patients had failed standard therapy,recurred/progressed following standard therapy, or had nostandard therapeutic options, and were not currently ame-nable to curative surgical intervention. Key inclusion/exclu-sion criteria were: Eastern Cooperative Oncology Groupperformance status �1; measurable p-Met by immunohis-tochemistry (IHC) of a tumor sample; and no previous useof anti–c-Met or anti-HGF therapy.
Patients should have had adequate hematologic (hemo-globin �9 g/dL; white blood cell count �3,000/mm3;absolute neutrophil count �1,500/mm3; and platelets�100,000/mm3), hepatic [serum bilirubin �1.5 � ULN(upper limit of normal) except with Gilbert Syndrome;
serum alanine and/or aspartate aminotransferase �5 �ULN], renal (serum creatinine �1.5 � ULN or calculatedcreatinine clearance >60 mL/min), and coagulation func-tion (partial thromboplastin time �1.5 � ULN; the inter-national normalized ratio�1.5�ULN). However, patientscould not have persistent, unresolved grade�2 drug-relatedtoxicity (except alopecia, erectile dysfunction, hot flashes,decreased libido, and grade 2 sensory peripheral neuropa-thy), HIV infection or HIV-related malignancy, active hep-atitis B or C, bleeding diathesis, hypersensitivity to anyficlatuzumab components, active alcohol or illicit drugabuse, or any of the following events �6 months beforeadministration of study drug: serious/symptomatic activeinfection (or infection requiring antibiotics�14days beforeadministration), myocardial infarction, severe/unstableangina, pectoris, coronary/peripheral artery bypass graft,symptomatic congestive heart failure, cerebrovascular acci-dent, transient ischemic attack, or seizure disorder. Thosewith any medical or psychiatric condition that might inter-fere with trial participation or interpretation of study resultsand those unable to comply with protocol requirementswere also excluded. In addition, patients were excluded ifthey did not have adequate recovery from prior medicalprocedures, i.e., major surgical procedure �4 weeks beforeadministration of study drug, radiotherapy�3 weeks prior,and stem cell/bone marrow transplant �6 months prior.Those with participation in any other clinical trials involv-ing therapeutic agents were also excluded. Female patientscould not be pregnant or breast-feeding, and all women ofchildbearing potential and men with partners of childbear-ing potential were required to use effective contraceptionduring the study and for 60 days after the last dose.
Study designPrimary objectives of this phase I, open-label, single-
center study were to evaluate ficlatuzumab safety/tolerabil-ity and its effect on exploratory pharmacodynamic markersin patientswith advanced solid tumors and livermetastases.Secondary objectives were to evaluate the pharmacokineticprofile and antitumor activity of ficlatuzumab.
Ficlatuzumab was administered once per 14-day cycle. Asolution of ficlatuzumab (1.0–10.0 mg/mL) in 0.9% sodi-um chloride was administered as a 30-minute intravenousinfusion through a low protein binding, 0.22 mmol/L in-line filter without premedication. The studywas designed toinclude aminimumof6patients in eachof the three cohorts(2, 10, and 20 mg/kg) for safety evaluation, which wouldalso allow for a minimum of 3 fully evaluable patients tostudy dose dependence of the pharmacodynamic changes.
Patients with intolerable grade 2 toxicity could have theirdose reduced a level or treatment discontinued (if at thelowest dose level). Patients with grade 3/4 toxicity requiringdose reduction could resume treatment at the lower doseafter the adverse event resolved to grade 0/1 or baseline.
The study protocol was approved by the appropriateethics committee and was conducted in accordance withthe principles of GoodClinical Practice and theDeclarationof Helsinki.
Translational RelevanceDysregulation of the hepatocyte growth factor (HGF)/
c-Met signaling pathway is observed in many malignan-cies and associated with progression of primary solidtumors to metastatic disease, including with presence ofliver metastases. Thus, inhibition of the HGF/c-Metpathway may be therapeutically beneficial for somepatients with cancer. Ficlatuzumab is a humanized HGFinhibitorymonoclonal antibody that neutralizesHGF/c-Met binding and HGF-induced c-Met phosphorylation.In addition to evaluation of the safety, tolerability,pharmacokinetic profile, and preliminary antitumoractivity of ficlatuzumab in patients with advanced solidtumors and liver metastases, this clinical study investi-gated the pharmacodynamic effects of ficlatuzumabtreatment in serum and tumors of patients. Mean serumHGF levels increased with ficlatuzumab dose and num-ber of treatment cycles. At 20 mg/kg, ficlatuzumab waswell tolerated and decreases in tumor p-Met, p-Erk, andp-Akt and an increase in HGF were observed, suggestingficlatuzumab canmodulate theHGF/c-Met pathway anddownstream signaling in the tumor.
Tabernero et al.
Clin Cancer Res; 20(10) May 15, 2014 Clinical Cancer Research2794
on June 27, 2020. © 2014 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst March 14, 2014; DOI: 10.1158/1078-0432.CCR-13-1837

Safety evaluationsAll patients who received �1 dose of ficlatuzumab were
considered evaluable for safety analyses. Adverse eventreporting occurred at screening, during treatment, and 1month after the final dose; other safety evaluations occurredat screening, the beginning of each treatment cycle, end oftreatment (EOT), and 1 month after treatment discontin-uation. Toxicities were graded using the National CancerInstitute CommonTerminologyCriteria for Adverse Events,version 3.0 (29).Dose-limiting toxicities (DLT) were defined as any of the
following toxicities: grade 3 toxicities (except nausea orvomiting, diarrhea, fever without neutropenia, and alanineor aspartate aminotransferase abnormalities lasting �48hours); grade 3 neutropenia with an absolute neutrophilcount�500/mm3and<1,000/mm3 lasting�5days; grade 3thrombocytopenia associated with bleeding; grade 4 hema-tologic or nonhematologic toxicities; drug-related toxicitiesof any grade that occurred during the first 2 cycles andrequired a dose reduction during the next scheduled studydrug administration; and drug-related toxicities of anygrade that resulted in interruption of treatment for >2weeks. Accrual to the next cohort occurred if�1of 6patientsexperienced a DLT during the first 2 cycles; dose escalationwas terminated if�2patients in a cohort experienced aDLT.Antidrug antibodies (ADA) against ficlatuzumab were
evaluated in serum at cycle 1 day 1 predose and at EOTusing a validated bridging electrochemiluminescence assay.Briefly, biotinylated ficlatuzumab and sulfo-tag ficlatuzu-mab (Meso Scale Discovery, MSD) were added to dilutedserum samples and incubated overnight. Samples wereadded to the wells of a streptavidin-coated plate (MSD) tocapture the biotinylated ficlatuzumab in the complex. Onlysamples containing antibody bound to both biotinylatedficlatuzumab and sulfo-tag ficlatuzumab generated theelectrochemiluminescence signal. The specificity of theADA signal was verified by ficlatuzumab spike-in. If thereading was reduced by half and/or was below the assaycutoff point after spike-in, then the sample was consideredpositive for ADA.
Pharmacodynamic evaluationsFor pharmacodynamic biomarker analyses, a minimum
of 3 patients per cohort had to meet the criteria for thepharmacodynamic evaluable population, defined aspatients with p-Met–positive tumors (i.e., H-score �30) byIHC at baseline predose and with�1 postdose p-Met result.This threshold for p-Met positivity was selected conserva-tively, to minimize inclusion of false-positive patients (par-ticularly as archival specimens were used for eligibilitydetermination for several patients), and was based on priorobservation that known low/negative tissue microarraysamples typically score below this cutoff, whereas the restscore above it; of note, literature guides were not availablefor threshold determination at the time of the study design.Sequential tumor biopsies from liver metastases were
collected at baseline predose, cycle 1 days 3 to 8, and cycle3 days 8 to 14; archived tumor tissue was also collected.
Tumor sample preparation has been described previously(30). Collected biopsies were fixed in 10% formalin for 12to 16 hours followed by a series of alcohol, xylene, andparaffin solution exchanges until final embedding in aparaffin block. Expression of HGF, c-Met, p-Met, p-ERK(phosphorylated extracellular-signal-regulated kinase), p-Akt (phosphorylated Akt), p-S6K, cleaved caspase-3, CD31,and Ki-67 in tumor samples was analyzed by IHC, usingautomated staining system [Dako Autostainer and DakoEnvision Flex Kit (K8012) detection system from DakoColorado, Inc.] and immunodetection with commerciallyavailable antibodies according to the manufacturer’sinstructions (Supplementary Table S1). The percentage ofpositive cells was reported for Ki-67 and cleaved caspase-3;CD31was quantified as a percentage of positive area withintumor tissue per high power field. H-scores (31) werecalculated for all other pharmacodynamic parameters usingthe formula: (%weak-stained cells)� 1þ (% intermediate-stained cells) � 2 þ (% strong-stained cells) � 3. Resultswere presented as percentage change from baseline, calcu-lated as: [100� (cycle "X" value� baseline value)/baselinevalue].
Sequential blood samples were collected predose and at 3hours postdose on cycle 1 day 1; cycle 1 days 3 to 4; predoseand at 2 hours postdose on cycle 2 day 1; andon cycle 3 days8 to 14. Serum HGF was measured using an ELISA (R&DSystems). c-Met levels were measured using a bridgingelectrochemiluminescence assay. Briefly, streptavidin-coat-ed plates (MSD) were coated with a biotinylated goatpolyclonal Met antibody (R&D Systems). c-Met present inserum samples was captured and subsequently detectedusing goat polyclonal c-Met antibody (R&D Systems)labeled with sulfo-tag (MSD). c-Met extracellular domain(R&D Systems) was used as a standard.
Tumormetabolic activity was followed by positron emis-sion tomography (PET) computed tomography (CT) with[18F]fluorodeoxyglucose at baseline (cycle 1 day 1 preinfu-sion and before the first liver biopsy), on day 3 or 4 (48–72hours after the first dose of study drug; only performed inpatients with evaluable PET CT scan lesions clearly distinctfrom the biopsy site), and during cycle 3 (at the time of thefirst disease assessment).
Pharmacokinetic evaluationsWhole-blood samples for serum evaluations were col-
lected predose, immediately postdose, and at 1, 3, 6, and 8hours postdose on cycle 1 day 1; cycle 1 days 3 to 4; predose,postdose, and at 2 hours postdose on cycle 2 day 1; predoseand postdose on cycle 3 day 1; cycle 3 days 8 to 14; andEOT.
Ficlatuzumab serum concentrations were measured inserum using an ELISAmethod validated according to GoodLaboratory Practice guidelines (with mean inter- andintraassay precision of 9.99% and 6.27%, respectively).Briefly, ficlatuzumab was captured from serum samples byrecombinant HGF (R&D Systems) bound on a microtiterplate, and captured ficlatuzumab was detected with perox-idase-labeled rabbit anti-human antibody (Dako) and tet-ramethylbenzidine as substrate.
Ficlatuzumab in Solid Tumor Patients with Liver Metastases
www.aacrjournals.org Clin Cancer Res; 20(10) May 15, 2014 2795
on June 27, 2020. © 2014 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst March 14, 2014; DOI: 10.1158/1078-0432.CCR-13-1837

Pharmacokinetic parameters calculated for ficlatuzumabincluded minimum and maximum plasma concentration(Cmin and Cmax), time to peak plasma concentration (tmax),area under the plasma concentration-time curve from time(AUC0!t, AUC0!¥), clearance, half-life (t1/2), apparent vol-umeof distribution (Vd), and the percentage of coefficient ofvariation (% CV), using noncompartmental analysis (Phoe-nix WinNonLin version 6.2; Pharsight Corporation).
Tumor response evaluationsThe efficacy evaluable population included those who
received �3 cycles of ficlatuzumab or were withdrawn dueto progressive disease before completing cycle 3. Diseaseand tumor response were assessed using Response Evalua-
tion Criteria in Solid Tumors, version 1.1 (32), at screening,the cycle 3 days 8 to 14 visit, and approximately every 6weeks thereafter. Efficacy parameters included overallresponse rate, duration of response, and time to progression(TTP). Time-to-event endpoints were estimated usingKaplan–Meier methodology.
ResultsPatients
From August 2009 to March 2011, 19 patients wereenrolled across three dose cohorts: n ¼ 6, the 2-mg/kgcohort; n ¼ 7, the 10-mg/kg cohort; and n ¼ 6, the 20-mg/kg cohort (baseline characteristics in Table 1). Themostcommon primary diagnosis was colorectal cancer (79%).
Table 1. Patient demographic and disease characteristics at baseline
Parameter2 mg/kg(n ¼ 6)
10 mg/kg(n ¼ 7)
20 mg/kg(n ¼ 6)
Total(n ¼ 19)
Mean age (range), y 57 (46–68) 59 (46–65) 63 (52–74) 60 (46–74)Sex, n (%)Male 5 5 5 15 (79)Female 1 2 1 4 (21)
Caucasian race, n (%) 6 (100) 7 (100) 6 (100) 19 (100)Mean BMI (range), kg/m2 26 (24–28) 24 (20–28) 26 (22–31) 25 (20–31)ECOG PS, n (%)0 1 3 4 8 (42)1 5 4 2 11 (58)
Median no. prior antitumor therapies 4 4 5 4Cancer diagnosis (%)Colorectal 5 5 5 15 (79)Pancreas 1 1 0 2 (11)
Breast 0 1 0 1 (5)Esophageal adenocarcinoma 0 0 1 1 (5)
No. of target lesions, n (%)2–3 3 5 5 13 (68)>3 3 2 1 6 (32)
Target lesion location, n (%)Liver 6 7 6 19 (100)Lung 4 3 1 8 (42)Lymph nodes 0 2 2 4 (21)Abdomen 1 0 0 1 (5)Other 1 1 0 2 (11)
No. of nontarget lesions, n (%)1 0 0 2 2 (11)2–3 6 5 4 15 (79)>3 0 2 0 2 (11)
Nontarget lesion location, n (%)Bone 0 1 0 1 (5)Liver 5 7 6 18 (95)Lung 5 6 3 14 (74)Lymph nodes 3 3 2 8 (42)Othera 1 2 0 3 (16)
Abbreviations: BMI, body mass index; ECOG, Eastern Cooperative Oncology Group; PS, performance status.aOther target lesion locations included the following: 2mg/kg,mediastinum (aorta-lungwindow lymphnode); 10mg/kg, pancreas (localrecurrence).
Tabernero et al.
Clin Cancer Res; 20(10) May 15, 2014 Clinical Cancer Research2796
on June 27, 2020. © 2014 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst March 14, 2014; DOI: 10.1158/1078-0432.CCR-13-1837

All patients had stage IV disease with measurable targetlesions at screening, including in the liver; all had �1nontarget lesion.Median (range) treatment duration was 6 (2–59) weeks.
Fifteen patients (79%) received ficlatuzumab for 2 weeks to2 months, 3 patients (16%) for >2 to 6 months, and 1patient (5%) for >6 months. All patients discontinued: 18patients (95%) for progressive disease and 1 patient (5%)for grade 4 adverse event (hyperbilirubinemia; unlikelyrelated to treatment).
Safety and tolerabilityThe safety population included all patients. No DLTs
were reported. Eighteen patients (95%) experienced �1treatment-emergent adverse event (TEAE), including 1 con-sidered possibly drug related (grade 1 pyrexia during cycle 1in the 2-mg/kg cohort). The most common TEAEs wereasthenia, peripheral edema, hepatic pain, and cough (Table2). Four patients (21%) experienced grade 3/4 unrelatedTEAEs. Grade 3 TEAEs included asthenia, hypoalbumine-mia, hypokalemia, proteinuria, and dyspnea (n ¼ 1 each).
Albumin level in the patient with grade 3 hypoalbumine-mia was 26.9 g/L at screening (grade 2) and decreasedthroughout the study. Grade 4 TEAEs included hyperbilir-ubinemia associated with worsening liver metastasis result-ing in discontinuation and respiratory failure due to diseaseprogression (n¼ 1 each). Five patients (26%) had one dosedelay each for adverse event management.
Laboratory abnormalities reported as TEAEs (all grades)included hypokalemia, hypomagnesemia, hypoalbumine-mia, anemia, leukopenia, hypocalcemia, hyponatremia,proteinuria, hyperglycemia, increased gamma-glutamyltranspeptidase, and neutropenia. One patient had anabnormal change in urinalysis results (epithelial cells)considered clinically significant.
Five patients (26%) experienced serious unrelatedadverse events: hyperbilirubinemia (n ¼ 1; 2 mg/kg);fatigue and intestinal obstruction (n ¼ 1 each; 10 mg/kg),gastrointestinal hemorrhage (n ¼ 1; 20 mg/kg), and intes-tinal obstruction, hepatic pain, and respiratory failure (n¼1; 20mg/kg). The last patient died due to grade 4 respiratoryfailure considered related to disease progression.
Table 2. TEAEs of any grade occurring in �3 patients and laboratory abnormalities of grade �3 severityoccurring in �1 patient
Event, n (%)2 mg/kg(n ¼ 6)
10 mg/kg(n ¼ 7)
20 mg/kg(n ¼ 6)
Total(n ¼ 19)
TEAEa
Asthenia 2 3 1 6 (32)Hepatic pain 2 3 1 6 (32)Peripheral edema 1 3 2 6 (32)Cough 1 2 2 5 (26)Abdominal distension 1 2 1 4 (21)Abdominal pain 1 2 1 4 (21)Constipation 0 2 1 3 (16)Decreased appetite 1 2 0 3 (16)Dyspnea 0 2 1 3 (16)Anemia 0 2 1 3 (16)Increased GGTb 3 0 0 3 (16)
Grade 3 laboratory abnormalitiesHyperuricemia 2 2 1 5 (26)Increased alkaline phosphatase 1 1 2 4 (21)Hypoalbuminemiac 0 1 1 2 (11)Hyperbilirubinemiad 1 0 0 1 (5)Hyperglycemia 1 0 0 1 (5)Hypocalcemia 0 0 1 1 (5)
Grade 4 laboratory abnormalitiesHyperbilirubinemia 1 0 0 1 (5)
Abbreviation: GGT, gamma-glutamyl transferase.aGrade 3/4 TEAEs included hypoalbuminemia and proteinuria (n¼ 1 each) in the 2-mg/kg cohort; hypoalbuminemia and hypokalemia(n ¼ 1 each) in the 10-mg/kg cohort; and asthenia, dyspnea, and respiratory failure (n ¼ 1 each) in the 20-mg/cohort.bNo patient experienced a GGT laboratory abnormality of grade >2.cSerum albumin decreased to below normal for the majority of patients by the EOT visit and trended toward recovery at the follow-upvisit.dLikely related to liver metastasis biopsy procedures.
Ficlatuzumab in Solid Tumor Patients with Liver Metastases
www.aacrjournals.org Clin Cancer Res; 20(10) May 15, 2014 2797
on June 27, 2020. © 2014 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst March 14, 2014; DOI: 10.1158/1078-0432.CCR-13-1837

The most frequently occurring laboratory abnormalitieswere hepatobiliary events; average levels of lactate dehy-drogenase, alkalinephosphatase, alanine aminotransferase,and aspartate aminotransferase were high at baseline andthroughout the study. Grade 3 abnormalities includedelevated alkaline phosphatase for 4 patients (21%) andelevated total bilirubin for 1 patient (5%), which worsenedto grade 4 (Table 2). Other changes in laboratory para-meters included grade 2 increased lymphocytes, partialthromboplastin time, and potassium, and grade 3 increasedblood glucose and decreased albumin.
In a retrospective analysis, serum albumin levelsdecreased in all patients to below the lower limit of normalby study completion. Mean (SD) albumin levels decreasedfrom 36.8 (4.46) to 30.5 (6.70) g/L during treatment,reaching minimum levels at EOT. Three patients (n ¼ 1,10 mg/kg; n ¼ 2, 20 mg/kg) experienced serum albumindecreases to grade 3 at the end of cycle 2, coinciding withEOT for all 3 patients. Mean (SD) albumin level increasedduring the 30-day follow-up period for all cohorts to 31.1(4.67) g/L but remained below normal.
Antidrug antibodies were measured for 13 patients at theEOT and ficlatuzumab was not immunogenic. No patienthad clinically significant abnormal electrocardiograms.Changes in body mass index were small and not clinicallymeaningful.
Pharmacodynamic analysesThe tumor pharmacodynamic evaluable population
comprised 12 patients (n ¼ 4, 2 mg/kg; n ¼ 3, 10 mg/kg;and n¼ 5, 20 mg/kg). All patients had measurable baselinep-Met by IHC (H-score �30); median (range) H-score was115 (40–260).
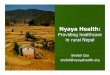
H-score changes from baseline for selected pharmaco-dynamic markers are shown in Fig. 1 (marker summary inSupplementary Table S2). More pronounced and consis-tent decrease in p-Met from baseline was apparent at theRP2D (20 mg/kg) of ficlatuzumab versus lower doses. Atcycles 1 and 3, respectively, median (range) relativechanges were: at 20 mg/kg, �21% (�42 to 17) and�53% (�81 to 9); at 10 mg/kg, 11% (11–11) and 22%(11–80); and at 2 mg/kg, 40% (0–50) and �17% (�23 to�9; Fig. 1A). Similarly, at 20 mg/kg there was a decreasein p-ERK with median (range) change of �38% (�59 to�34) and �43% (�78 to 15) and to lesser extent p-Akt,with a median (range) change of �40% (�48 to 91) and�2% (�45 to 12) at both time points (Fig. 1B, and C). At20 mg/kg, there was an increase in tumor HGF level withmedian (range) change of 17% (0–125) and 33% (�10 to138) at the same time points (Fig. 1D). Increased serumHGF levels were also observed in a time- and dose-dependent manner (Fig. 1E; Supplementary Table S3).At 10 mg/kg, there was an increase in median change p-Met and p-ERK at both time points for reasons unknown.Further, changes in p-ERK expression correlated withchanges in tumor p-Met (Spearman correlation coeffi-cient r ¼ 0.48, P ¼ 0.044; n ¼ 18; Fig. 1F), suggestingthat changes in p-ERK could result from changes in HGF/
c-Met signal transduction. No dose- or time-dependentpattern could be identified in the changes in CD31-positive microvessel density upon initiation of treatmentwith ficlatuzumab (Supplementary Table S2). No changesin serum c-Met levels were observed postdose.
All patients who had PET CT scans performed had[18F]fluorodioxyglucose avid tumors at baseline, consistentwith metabolically active neoplastic disease. Fourteenpatients had both a baseline and cycle 3 PET CT scans andwere evaluable for pharmacodynamic analyses; the remain-ing 5 patients did not have a cycle 3 PET CT scan. Amongthese 14 evaluable patients, 4 patients had stable disease,and 10 patients had increased [18F]fluorodioxyglucoseuptake consistent with progression at cycle 3. Of note, 1patient had a decrease in [18F]fluorodeoxyglucose updateafter 3 days of ficlatuzumab, which correlated withdecreased p-Met, p-MAPK (phosphorylated mitogen-acti-vated protein kinase), Ki-67, CD31, and tumorHGF expres-sion as assessed by IHC staining; however, this patient haddisease progression by the first tumor evaluation and waswithdrawn from the study before the cycle 4 dose.
One patient with colorectal carcinoma had dramaticdecreases in nearly all pharmacodynamic markers (Fig.2A–D) and an increase in HGF (Fig. 2E). This patientreceived three treatment cycles and was withdrawn fromthe study due to a new lesion observed by CT (negative byPET).
Pharmacokinetic analysesPharmacokinetic parameters are listed by the dose cohort
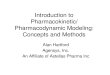
in Table 3. Ficlatuzumab exposure (assessed by Cmax andAUC) increased in an approximately dose-proportionalmanner (Fig. 3). No significant changes in the mean clear-ance and t1/2 across doses were observed (P ¼ 0.092 and0.167, respectively, by ANOVA), suggesting linear pharma-cokinetics for the 2 to 20 mg/kg dose range. Ficlatuzumabexhibited low clearance (0.178–0.261 mL/h/kg) leading toa long terminal t1/2 (7.4–10 days), with significant accu-mulation of ficlatuzumab fromcycle 1 to cycle 3.Mean (SD)Vd ranged from61 (18) to75 (15)mL/kg, suggesting limiteddistribution of ficlatuzumab to the extravascular compart-ment (33).
Antitumor activityEighteen patients were evaluable for efficacy (n ¼ 5, 2
mg/kg; n ¼ 7, 10 mg/kg; n ¼ 6, 20 mg/kg); no patient hadan objective response. Five patients (28%) achieved stabledisease; median duration was 2.6 months [95% confi-dence interval (CI), 1.5–13.7]. Four of these patients hadcolorectal adenocarcinoma with stable disease durationfrom 1.5 to 2.7 months, and 1 patient had pancreaticacinar cell carcinoma with stable disease lasting 13.7months (this particular tumor type usually has a moreindolent course than pancreatic ductal adenocarcinoma).Median TTP was 1.4 months (95% CI, 1.3–1.5). Nosignificant relationship was found between TTP and max-imum percentage change from baseline for any measuredpharmacodynamic marker.
Tabernero et al.
Clin Cancer Res; 20(10) May 15, 2014 Clinical Cancer Research2798
on June 27, 2020. © 2014 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst March 14, 2014; DOI: 10.1158/1078-0432.CCR-13-1837

DiscussionIn a previous ficlatuzumab phase I study in patients with
advanced solid tumors, the recommended treatment dosewas 20 mg/kg once every 2 weeks (14-day cycle; ref. 34). Inthis study, the same ficlatuzumab regimen was well toler-ated without DLTs; ficlatuzumab modulated HGF/c-Met
pathway pharmacodynamic markers in the tumor andserum, and had a good pharmacokinetic profile that wasconsistent with a previous study (34).
The overall safety profile of ficlatuzumab observed inthis study, characterized by peripheral edema, hypoalbu-minemia, cough, and gastrointestinal adverse events,
–100
–80
–60
–40
–20
0
20
40
60
80
p-M
et C
hang
e fr
om b
asel
ine
(%)
2 10 20
Dose, mg/kg
Biopsy timepoint Cycle 1 Day 3–8 Cycle 3 Day 8–14
A
–100
–50
0
50
100
150
200
p-ER
K C
hang
e fr
om b
asel
ine
(%)
2 10 20
Dose, mg/kg
Biopsy timepoint Cycle 1 Day 3–8 Cycle 3 Day 8–14
B
–60
–20
–40
0
40
20
60
80
100
p-A
kt C
hang
e fr
om b
asel
ine
(%)
2 10 20
Dose, mg/kg
Biopsy timepoint Cycle 1 Day 3–8 Cycle 3 Day 8–14
C
–100
100
0
200
400
300
500
600
700
HG
F ch
ange
fro
m b
asel
ine
(%)
2 10 20
Dose, mg/kg
Biopsy timepoint Cycle 1 Day 3–8 Cycle 3 Day 8–14
D
0 10 20 30 40
0
2
4
6
8
10
12
14
16
18
20
Time since ficlatuzumab treatment (d)
Fold
cha
nge
in H
GF
from
bas
elin
e
20 mg/kg10 mg/kg2 mg/kgFiclatuzumab dose
E
–90 –80 –70 –60 –50 –40 –30 –20 –10 0 10 20 30 40 50 60 70 80
–100
0
100
200
p-ER
K H
-sco
re C
hang
e fr
omba
selin
e (%
)
p-Met H-score Change from baseline (%)
p-Met versus p-ERK
2 mg/kg 10 mg/kg 20 mg/kgFiclatuzumab dose
n = 18r = 0.456P = 0.057
F
Figure 1. Pharmacodynamic analyses. Median percentage changes from baseline for p-Met (A), p-ERK (B), p-Akt (C), and HGF (D) H-scores in the tumorsamples for each cohort are depicted in box plots. Medians (horizontal lines) are shown with their first and third quartile values (boxes) and ranges(vertical lines). E, change in serum HGF levels from baseline over time for each cohort. F, percentage changes from baseline for p-ERK H-scores versuspercentage change from baseline for p-Met H-score are plotted for each cohort. Data points were offset slightly for improved visibility of the error bars.
Ficlatuzumab in Solid Tumor Patients with Liver Metastases
www.aacrjournals.org Clin Cancer Res; 20(10) May 15, 2014 2799
on June 27, 2020. © 2014 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst March 14, 2014; DOI: 10.1158/1078-0432.CCR-13-1837

matches that observed for other antibodies targeting theHGF/c-Met pathway (i.e., rilotumumab, onartuzumab,and TAK701; refs. 35–37). Edema was also among themost common adverse events observed for the ALK/c-Metinhibitor crizotinib (38). Slow recovery of albumin levelsafter EOT is consistent with the long half-life of ficlatuzu-mab. In this study, gastrointestinal adverse events (e.g.,abdominal pain, abdominal distention, and constipation),were among the most common TEAEs, consistent with thedisease state.
The pharmacokinetics of ficlatuzumab was characterizedby low clearance and a long half-life (7.4–10 days), con-
sistent with the previous phase I study (34) and the profileof other humanized immunoglobulin G1 antibodies (38).Ficlatuzumab exhibited linear pharmacokinetics across alldose levels tested.
A maximum tolerated dose was not reached with ficla-tuzumab, making the determination of the RP2D challeng-ing; this is similar to reports of other HGF/c-Met inhibitoryantibodies, including onartuzumab (37), rilotumumab(35), and TAK701 (36). The objective of this study was todetermine whether ficlatuzumab treatment could result inpharmacodynamic target modulation in the tumor to max-imize antitumor activity at the doses tested.
Activation of the c-Met pathway, indicated by p-Metlevels, tends to increase with disease progression (17–22), and tends to be higher in liver metastases than in theprimary tumor site. In this study, ficlatuzumab inhibition ofp-Met and subsequent downstream signaling was investi-gated in patients with advanced tumors with liver metas-tases accessible to repeat biopsies. Patients with positive p-Met in archival tumor biopsies were also enrolled. Predosebaseline liver tumorbiopsies for all patients hadmeasurablep-Met. Ficlatuzumab treatment led to consistentlydecreased levels of p-Met only at 20 mg/kg, confirming thatit can modulate HGF/c-Met pathway function in the tumorat the RP2D of 20 mg/kg. These findings support a mech-anism proposed by previous in vitro and in vivo studies (23–25), in which ficlatuzumab inhibits c-Met signaling.
The observed decrease in p-Akt and p-ERK only at 20mg/kg suggests that ficlatuzumab may decrease cellular prolif-eration and survival signals at RP2D. Changes in p-ERK thatcorrelated with changes in p-Met suggested that changesobserved in p-ERKmay indeed result from changes in p-Metfollowing ficlatuzumab treatment.
Treatment with 20 mg/kg ficlatuzumab also resulted inmild increases inHGF levels in livermetastases (17%–33%)andmore pronounced increases in serum (4.0-fold by cycle1, days 3–4). Although no measurable increase in tumorHGF expression levels was observed for the 2- or 10-mg/kgcohorts, the increase was observed in serum by 2.66- and3.51-fold, respectively, by the same time postdose.Increased serum HGF after ficlatuzumab administration,indicating target engagement, is consistent with previousobservations (26). The increase in HGF in tumor and morepronounced and consistent increase in serum is likely due tothe stabilization of HGF upon complex formation withficlatuzumab and/or compensatory increase in HGF pro-duction (39).
Similarly, decreased HGF/c-Met pathway–related signal-ing, as indicated by reductions in p-Met and p-ERK, wasmore pronounced in the 20-mg/kg cohort, despite a highficlatuzumab serum trough concentration (mean Cmin:7.15, 40.7, and 128 mg/mL at 2, 10, and 20 mg/kg, respec-tively) in all cohorts well exceeding the IC50 of approxi-mately 1 mg/mL in most cellular assays (23). This discrep-ancy between tumor and serum pharmacodynamic markermodulations is likely due to limited antibody penetrationinto the tumor milieu, emphasizing the importance ofestablishing an effective dosing regimen using paired
Figure 2. Pharmacodynamic changes in liver tumor biopsies. Liverbiopsies from a single patient predose (left-hand side of A–E) and 3 daysafter ficlatuzumab 20mg/kg (right-hand side of A–E) to detect levels of p-Met (A), p-MAPK (B), Ki-67 (C), CD31 (D), and tumor HGF(E).
Tabernero et al.
Clin Cancer Res; 20(10) May 15, 2014 Clinical Cancer Research2800
on June 27, 2020. © 2014 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst March 14, 2014; DOI: 10.1158/1078-0432.CCR-13-1837

Tab
le3.
Ficlatuz
umab
pha
rmac
okinetic
param
etersbytrea
tmen
tgrou
pin
cycle1
Param
eter
Cmax(mg/m
L)t m
ax(h)a
AUC0!
t(m
g�h
/mL)
AUC0-¥
(mg�h
/mL)
CL(m
L/h/kg
)t 1
/2(h)
Vd(m
L/kg
)Cmin(mg/m
L)
2mg/kg
n6
66
4a4
44
5Mea
n,SD
39.05(13.94
)1.5(0.58–
3.5)
4.36
5(2.678
)8.38
2(1.594
)0.24
52(0.048
38)
177.5(32.72
)61
.25(4.168
)7.15
(4.587
)%
CV
35.7
57.4
61.3
1919
.718
.46.8
64.2
10mg/kg
n7
77
66
66
6Mea
n,SD
173.3(39.85
)1.5(0.58–
3.58
)24
.66(9.613
)40
.52(11.24
)0.26
10(0.063
66)
206.5(46.12
)75
.43(15.06
)40
.67(13.79
)%
CV
2363
.439
.027
.724
.422
.320
.033
.920
mg/kg
n6
66
44
44
4Mea
n,SD
443(100
.7)
1.04
(0.5–1.5)
54.27(32.08
)11
7.0(27.76
)0.17
80(0.039
84)
239(43.34
)61
.15(17.83
)12
8.2(27.98
)%
CV
22.7
51.3
59.1
23.7
22.4
18.1
29.2
21.8
NOTE
:Onlypatientswith
pha
rmac
okinetic
profilesev
alua
ble
forco
mplete
nonc
ompartm
entala
nalysiswereinclud
ed.
Abbreviations
:AUC0!t,area
under
theco
ncen
tration-tim
ecu
rvefrom
timeze
roto
theen
dof
thedo
sing
interval;A
UC0!
¥,a
reaun
der
theco
ncen
tration-tim
ecu
rveex
trap
olated
toinfinite
time;
CL,
clea
ranc
e;SD,s
table
dise
ase.
at m
axis
repo
rted
asmed
ian(ra
nge).
Ficlatuzumab in Solid Tumor Patients with Liver Metastases
www.aacrjournals.org Clin Cancer Res; 20(10) May 15, 2014 2801
on June 27, 2020. © 2014 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst March 14, 2014; DOI: 10.1158/1078-0432.CCR-13-1837

predose and postdose tumor biopsies rather than solelyrelying on exposure in the serum.
Given the small number of patients at each dose and timepoint, the results need to be interpreted with caution.However, collectively, at 20 mg/kg ficlatuzumab, there isdecrease in median tumor p-Met, p-Erk, and p-Akt, and anincrease in HGF at both time points; this pattern is consis-tentwith themechanismof action of an anti-HGF antibody.These changes likely indicate that ficlatuzumab 20 mg/kginduced pharmacodynamic modulation of the HGF/c-Metpathway and downstream signaling.
Overall, ficlatuzumabmonotherapy was well tolerated inpatients with solid tumors and liver metastases. The studyconfirmed the validity of 20mg/kg as the appropriate RP2Dfor ficlatuzumab based on pharmacodynamic target mod-ulation in the tumor. These results support the clinicalevaluation of ficlatuzumab for treating patients withadvanced solid tumors. A randomized phase Ib/II trialexploring ficlatuzumab in combination with gefitinib(27, 28) is ongoing.
Disclosure of Potential Conflicts of InterestM. Han is an employee of and has ownership interest (including
patents) in AVEO. P. Komarnitsky has ownership interest (includingpatents) in AVEO. No potential conflicts of interest were disclosed bythe other authors.
Authors' ContributionsConception and design: J. Tabernero, J. Andreu, M. Han, P. Komarnitsky,J. BaselgaDevelopment of methodology: J. Tabernero, M.E. Elez, J. Andreu, M. Han,W. Yin, P. Komarnitsky, J. BaselgaAcquisitionofdata (provided animals, acquired andmanagedpatients,provided facilities, etc.): J. Tabernero, M.E. Elez, M. Herranz, L. Prudkin, J.Andreu, J. Mateos, M.J. Carreras, J. Gifford, W. Yin, S. Agarwal, P. Komar-nitsky, J. BaselgaAnalysis and interpretation of data (e.g., statistical analysis, biosta-tistics, computational analysis): J. Tabernero, M.E. Elez, J. Andreu, M.Han, J. Gifford, W. Yin, S. Agarwal, P. Komarnitsky, J. BaselgaWriting, review, and/or revision of the manuscript: J. Tabernero, M.E.Elez, L. Prudkin, J. Andreu, J.Mateos,M.J. Carreras,M.Han,M.Credi,W. Yin,S. Agarwal, P. Komarnitsky, J. BaselgaAdministrative, technical, or material support (i.e., reporting or orga-nizing data, constructing databases): M. Herranz, I. Rico, J. Gifford, M.Credi, S. AgarwalStudy supervision: J. Tabernero, J. Baselga
2 mg/kg 10 mg/kg
Mean Individual
20 mg/kg1,000
100
10
Ficl
atuz
umab
con
cent
ratio
n (μ
g/m
L)
Nominal time since first ficlatuzumab dose (d)
0 7 14 21 28 35 0 7 14 21 28 350 7 14 21 28 35
Ficlatuzumab doseA
r 2 = 0.87
2 5 10 15 20
0
100
200
300
400
500
600
Ficl
atuz
umab
Cm
ax (
μg/m
L)
Ficlatuzumab dose (mg/kg)
B
Ficlatuzumab dose (mg/kg)
150
100
50
0
2 5 10 15 20
r 2 = 0.853
Ficl
atuz
umab
AU
C0
-∞ (
mg•
h/m
L)
C
Figure 3. Ficlatuzumabpharmacokinetics. A,concentration time profiles. Serumconcentrations of ficlatuzumab areplotted as a function of treatmentvisit for each patient. Dashed linesindicate expected dosing times forcycle 1 day 1, cycle 2 day 1, andcycle 3 day 1 (0, 14, and 28 dosessince the first ficlatuzumab dose,respectively). Four patients whowithdrew before their cycle 2 dosewere included up to their lastrecorded sample point.Ficlatuzumab Cmax (B) andAUC0!¥ (C) as a function of cycle 1dose. AUC0!¥, area under theconcentration-time curveextrapolated to infinite time.
Clin Cancer Res; 20(10) May 15, 2014 Clinical Cancer Research2802
Tabernero et al.
on June 27, 2020. © 2014 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst March 14, 2014; DOI: 10.1158/1078-0432.CCR-13-1837

AcknowledgmentsThe authors thank all of the participating patients and their families as
well as the global network of investigators, research nurses, study coordi-nators, and operations staff. Medical writing support was provided byKimberly Brooks, of SciFluent.
Trial registration:This trial was registered at ClinicalTrials.gov (NCT00969410).
Grant SupportThis study was supported by AVEO Pharmaceuticals, Inc.The costs of publication of this article were defrayed in part by the
payment of page charges. This article must therefore be hereby markedadvertisement in accordance with 18 U.S.C. Section 1734 solely to indicatethis fact.
Received July 9, 2013; revised February 12, 2014; accepted February 22,2014; published OnlineFirst March 14, 2014.
References1. Bottaro DP, Rubin JS, Faletto DL, Chan AM, Kmiecik TE, Vande
Woude GF, et al. Identification of the hepatocyte growth factorreceptor as the c-met proto-oncogene product. Science 1991;251:802–4.
2. WeidnerKM,SachsM,BirchmeierW. TheMet receptor tyrosine kinasetransduces motility, proliferation, and morphogenic signals of scatterfactor/hepatocyte growth factor in epithelial cells. J Cell Biol 1993;121:145–54.
3. Birchmeier C, Birchmeier W, Gherardi E, Vande Woude GF. Met,metastasis, motility, and more. Nat Rev Mol Cell Biol 2003;4:915–25.
4. Hanahan D, Weinberg RA. Hallmarks of cancer: the next generation.Cell 2011;144:646–74.
5. Trusolino L, Comoglio PM. Scatter-factor and semaphorin recep-tors: cell signalling for invasive growth. Nat Rev Cancer 2002;2:289–300.
6. Engelman JA, Janne PA. Mechanisms of acquired resistance toepidermal growth factor receptor tyrosine kinase inhibitors in non–small cell lung cancer. Clin Cancer Res 2008;14:2895–9.
7. Gentile A, Trusolino L, Comoglio PM. The Met tyrosine kinasereceptor in development and cancer. Cancer Metastasis Rev 2008;27:85–94.
8. Engelman JA, Zejnullahu K, Mitsudomi T, Song Y, Hyland C, Park JO,et al. MET amplification leads to gefitinib resistance in lung cancer byactivating ERBB3 signaling. Science 2007;316:1039–43.
9. Wilson TR, Fridlyand J, Yan Y, Penuel E, Burton L, Chan E, et al.Widespread potential for growth-factor-driven resistance to antican-cer kinase inhibitors. Nature 2012;487:505–9.
10. Drebber U, Baldus SE, Nolden B, GrassG, Bollschweiler E, Dienes HP,et al. The overexpression of c-met as a prognostic indicator for gastriccarcinomacompared top53andp21nuclear accumulation.OncolRep2008;19:1477–83.
11. Ponzo MG, Lesurf R, Petkiewicz S, O'Malley FP, Pinnaduwage D,Andrulis IL, et al. Met induces mammary tumors with diverse histol-ogies and is associated with poor outcome and human basal breastcancer. Proc Natl Acad Sci U S A 2009;106:12903–8.
12. Pour L, Svachova H, Adam Z, Mikulkova Z, Buresova L, Kovarova L,et al. Pretreatment hepatocyte growth factor and thrombospondin-1levels predict response to high-dose chemotherapy for multiple mye-loma. Neoplasma 2010;57:29–34.
13. Betsunoh H, Mukai S, Akiyama Y, Fukushima T, Minamiguchi N, HasuiY, et al. Clinical relevance of hepsin and hepatocyte growth factoractivator inhibitor type 2 expression in renal cell carcinoma. Cancer Sci2007;98:491–8.
14. Hepatocyte growth factor/scatter factor (HGF/SF), MET and cancerreferences. 2011. http://www.vai.org/met/.
15. Salgia R. Role of c-Met in cancer: emphasis on lung cancer. SeminOncol 2009;36:S52-S58.
16. Christensen JG, Burrows J, Salgia R. c-Met as a target for humancancer and characterization of inhibitors for therapeutic intervention.Cancer Lett 2005;225:1–26.
17. Amemiya H, Kono K, Itakura J, Tang RF, Takahashi A, An FQ, et al. c-Met expression in gastric cancer with liver metastasis. Oncology2002;63:286–96.
18. Coskun U, Bukan N, Sancak B, Gunel N, Ozenirler S, Unal A, et al.Serum hepatocyte growth factor and interleukin-6 levels can distin-guish patients with primary or metastatic liver tumors from those withbenign liver lesions. Neoplasma 2004;51:209–13.
19. Eichbaum MH, de Rossi TM, Kaul S, Bruckner T, Schneeweiss A,Sohn C. Serum levels of hepatocyte growth factor/scatter factor inpatients with liver metastases from breast cancer. Tumour Biol2007;28:36–44.
20. Hansel DE, Rahman A, House M, Ashfaq R, Berg K, Yeo CJ, et al.Met protooncogene and insulin-like growth factor binding protein 3overexpression correlates with metastatic ability in well-differenti-ated pancreatic endocrine neoplasms. Clin Cancer Res 2004;10:6152–8.
21. Maemura M, Iino Y, Yokoe T, Horiguchi J, Takei H, Koibuchi Y, et al.Serum concentration of hepatocyte growth factor in patients withmetastatic breast cancer. Cancer Lett 1998;126:215–20.
22. Zeng ZS, Weiser MR, Kuntz E, Chen CT, Khan SA, Forslund A, et al.c-Met gene amplification is associatedwith advanced stage colorectalcancer and liver metastases. Cancer Lett 2008;265:258–69.
23. Han M, Breault L, Wright K, Moore C, Knuehl C, Lin J, et al. In vivogenetic screens designed to complement loss of HER2 or kRasfunctions identify c-Met/HGF pathway as potent driver of growth/survival in solid tumor models. AACR Meeting Abstracts 2007:4887.
24. Meetze KA, Connolly K, Boudrow A, Venkataraman S, Medicherla S,Gyuris J, et al. Preclinical efficacy and pharmacodynamics of SCH900105 (AV-299) an anti-HGF antibody in an intracranial glioblastomamodel. Mol Cancer Ther 2009;8:C181.
25. Meetze KA, Boudrow A, Connolly K, Huang R, Rideout W, Gyuris J,et al. Anti-tumor activity of SCH 900105 (AV299), an anti-HGF anti-body, in non–small cell lung cancer models. Mol Cancer Ther 2009;8:C173.
26. Patnaik A, Weiss GJ, Papadopoulos R, Tibes R, Tolcher AW, PayumoFC, et al. Phase I study of SCH 900105, an anti-hepatocyte growthfactor monoclonal antibody, as a single agent and in combination witherlotinib in patients with advanced solid tumors. J Clin Oncol2010;28:2525.
27. Mok T, Tan E, Park K, Jac J, Han M, Payumo FC, et al. Randomizedphase II study of ficlatuzumab (formerly AV-299), an anti-hepatocytegrowth factor (HGF) monoclonal antibody (MAb) in combination withgefitinib (G) in Asian patients (pts) with NSCLC. J Clin Oncol 2011;29:TPS213.
28. Tan E, Park K, LimWT, Ahn M, Ng QS, Ahn JS, et al. Phase Ib study officlatuzumab (formerly AV-299), an anti-hepatocyte growth factormonoclonal antibody in combination with gefitinib in Asian patientswith NSCLC. J Clin Oncol 2011;29:7571.
29. National Cancer Institute (2006) Common Terminology Criteria forAdverse Events v3.0 (CTCAE). http://www.eortc.be/services/doc/ctc/ctcaev3.pdf.
30. Tabernero J, Rojo F, Calvo E, Burris H, Judson I, Hazell K, et al. Dose-and schedule-dependent inhibition of the mammalian target of rapa-mycin pathway with everolimus: a phase I tumor pharmacodynamicstudy in patients with advanced solid tumors. J Clin Oncol 2008;26:1603–10.
31. Detre S, Saclani JG, Dowsett M. A "quickscore" method for immuno-histochemical semiquantitation: validation for oestrogen receptor inbreast carcinomas. J Clin Pathol 1995;48:876–8.
32. Eisenhauer EA, Therasse P, Bogaerts J, Schwartz LH, Sargent D, FordR, et al. New response evaluation criteria in solid tumours: revisedRECIST guideline (version 1.1). Eur J Cancer 2009;45:228–47.
33. Davies B,Morris T. Physiological parameters in laboratory animals andhumans. Pharm Res 1993;10:1093–5.
www.aacrjournals.org Clin Cancer Res; 20(10) May 15, 2014 2803
Ficlatuzumab in Solid Tumor Patients with Liver Metastases
on June 27, 2020. © 2014 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst March 14, 2014; DOI: 10.1158/1078-0432.CCR-13-1837

34. Ramanathan RK, Payumo FC, Papadopoulos KP, Weiss GJ, Cham-bersG, Iyengar T, et al. A phase 1, first in human, study of SCH900105,an antihepatocyte growth factor (HGF) monoclonal antibody, in sub-jects with advanced solid tumors. Mol Cancer Ther 2009;8:A100.
35. Gordon MS, Sweeney CS, Mendelson DS, Eckhardt SG, Anderson A,Beaupre DM, et al. Safety, pharmacokinetics, and pharmacodynamicsof AMG 102, a fully human hepatocyte growth factor-neutralizingmonoclonal antibody, in a first-in-human study of patients withadvanced solid tumors. Clin Cancer Res 2010;16:699–710.
36. Jones SF, Cohen RB, Bendell JC, Denlinger CS, Harvey RD, Para-suraman S, et al. Safety, tolerability, and pharmacokinetics of TAK-701, a humanized anti-hepatocyte growth factor (HGF) monoclonalantibody, in patients with advanced nonhematologic malignancies:first-in-human phase I dose-escalation study. J Clin Oncol 2010;28:3081.
37. Salgia R, Peterson A, Eppler S, YuW, Polite B, Geary D, et al. A phase I,open-label, dose-escalation study of the safety and pharmacology ofMetMAb, a monovalent antagonist antibody to the receptor Met,administered IV in patients with locally advanced or metastatic solidtumors [abstract]. In: Proceedings of the 20th European Organisationfor Research and Treatment of Cancer-National Cancer Institute-American Association for Cancer Research Symposium; 2008 Oct21–24; Geneva, Switzerland: AACR; 2008. Abstract nr 411.
38. Keizer RJ, Huitema AD, Schellens JH, Beijnen JH. Clinical pharmaco-kinetics of therapeutic monoclonal antibodies. Clin Pharmacokinet2010;49:493–507.
39. Penuel E, Li C, Parab V, Burton L, Cowan KJ, Merchant M, Yauch RL,et al. HGF as a circulating biomarker of onartuzumab treatment inpatients with advanced solid tumors. Mol Cancer Ther 2013;12:1122–3.
Clin Cancer Res; 20(10) May 15, 2014 Clinical Cancer Research2804
Tabernero et al.
on June 27, 2020. © 2014 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst March 14, 2014; DOI: 10.1158/1078-0432.CCR-13-1837

2014;20:2793-2804. Published OnlineFirst March 14, 2014.Clin Cancer Res Josep Tabernero, Maria Elena Elez, Maria Herranz, et al. Patients with Advanced Solid Tumors and Liver MetastasesA Pharmacodynamic/Pharmacokinetic Study of Ficlatuzumab in
Updated version
10.1158/1078-0432.CCR-13-1837doi:
Access the most recent version of this article at:
Material
Supplementary
http://clincancerres.aacrjournals.org/content/suppl/2014/03/14/1078-0432.CCR-13-1837.DC1
Access the most recent supplemental material at:
Cited articles
http://clincancerres.aacrjournals.org/content/20/10/2793.full#ref-list-1
This article cites 35 articles, 10 of which you can access for free at:
Citing articles
http://clincancerres.aacrjournals.org/content/20/10/2793.full#related-urls
This article has been cited by 1 HighWire-hosted articles. Access the articles at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications Department at
Permissions
Rightslink site. Click on "Request Permissions" which will take you to the Copyright Clearance Center's (CCC)
.http://clincancerres.aacrjournals.org/content/20/10/2793To request permission to re-use all or part of this article, use this link
on June 27, 2020. © 2014 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst March 14, 2014; DOI: 10.1158/1078-0432.CCR-13-1837