Embed Size (px)
Citation preview

Aw
XJRa
b
a
ARRAA
KCIVST
1
foht
CspS
N
0d
Atherosclerosis 218 (2011) 83– 89
Contents lists available at ScienceDirect
Atherosclerosis
jo ur nal homep age : www.elsev ier .com/ locate /a therosc leros is
pattern of disperse plaque microcalcifications identifies a subset of plaquesith high inflammatory burden in patients with acute myocardial infarction
iaoFei Lia,b,∗, Miranda C. Kramera, Chris M. van der Loosb, Karel T. Kocha, Onno J. de Boerb,osé P.S. Henriquesa, Jan Baan Jr. a, Marije M. Visa, Jan J. Pieka, Jan G.P. Tijssena,obbert J. de Wintera, Allard C. van der Walb
Department of Cardiology, Academic Medical Center, University of Amsterdam, Meibergdreef 9, 1105 AZ Amsterdam, The NetherlandsDepartment of Pathology,L2-112, Academic Medical Center, University of Amsterdam, Amsterdam, The Netherlands
r t i c l e i n f o
rticle history:eceived 17 January 2011eceived in revised form 1 April 2011ccepted 21 April 2011vailable online 5 May 2011
eywords:alcification
nflammatory biomarkerulnerable plaqueTEMIhrombectomy
a b s t r a c t
Aims: Inflammation plays a crucial role in plaque vulnerability. Calcifications can be detected by meansof in vivo imaging techniques. The study purpose is to assess a potential association between tissuelocalization of calcifications and the inflammatory biomarkers, C-reactive protein (CRP), osteopontin andlipoprotein-associated phospholipase A2 (Lp-PLA2), in plaque tissue of patients with acute myocardialinfarction (AMI).Methods and results: Thrombectomy materials obtained from patients with electrocardiographically docu-mented ST-segment elevation type of AMI (STEMI) were histologically screened for presence of thrombus,plaque tissues and calcifications. Size of calcifications was measured morphometrically, and their colocal-ization with the inflammatory biomarkers macrophages, CRP, osteopontin and Lp-PLA2 was assessed withimmunostaining. A total of 171 samples containing plaque tissues were obtained from 562 thrombectomyprocedures. Calcifications were observed in 67 (39%) plaque fragments, with diameters ranging from 4 to170 �m. Plaque tissues with calcifications contained more frequently extracellular CRP and intracellularCRP in macrophages than those without calcifications (85%, 59% vs. 64%, 32%, P = 0.012 and 0.005 respec-tively). Similar results were obtained with osteopontin immunostaining (98%, 76% vs. 56%, 40%; P < 0.001both). Furthermore, samples with calcifications were immunostained for CRP more intensely than those
without calcifications (P = 0.001). Finally, 96% of the plaque tissues stained positively for Lp-PLA2, butthere was no association with presence of microcalcifications.Conclusions: A pattern of disperse microcalcifications is positively associated with presence of the inflam-matory biomarkers macrophages, CRP and osteopontin in thrombectomy materials of STEMI patients.Based on these findings, we speculate that such microcalcifications could have the potential to serve asa surrogate marker for plaques with high inflammatory burden.. Introduction
By far most cases of acute myocardial infarction (AMI) resultrom coronary thrombus formation superimposed on disruption
f a vulnerable type of atherosclerotic plaque [1]. Many studiesave shown that the vulnerability to rupture is usually not a fea-ure of a single (culprit) plaque, but may involve several plaquesAbbreviations: ARedS, Alizarin red S stain; AMI, acute myocardial infarction;RP, C-reactive protein; EBCT, electron beam computed tomography; hsCRP, highensitivity CRP; IVUS, intravascular ultrasound; Lp-PLA2, lipoprotein-associatedhospholipase A2; OPN, osteopontin; PCI, percutaneous coronary intervention;TEMI, ST-segment elevation myocardial infarction.∗ Corresponding author at: Post Office Box 22660, 1100 DD Amsterdam, Theetherlands. Tel.: +31 20 5665715; fax: +31 20 5669523.
E-mail addresses: [email protected], [email protected] (X. Li).
021-9150 © 2011 Elsevier Ireland Ltd.
oi:10.1016/j.atherosclerosis.2011.04.032Open access under the Elsevier OA license.
© 2011 Elsevier Ireland Ltd.
in the coronary system of a patient (pan coronary vulnerability)[2]. Such insights have boosted the search for in vivo markers ofplaque vulnerability, by means of high resolution coronary imag-ing techniques or serum levels of inflammatory proteins, to identifypatients with increased cardiovascular risk.
Calcification is an excellent marker for the presence ofatherosclerosis, but its role on plaque instability is still unclear.Although coronary calcifications detected by electron beam com-puted tomography (EBCT) is strongly predictive for adversecardiovascular outcome [3,4], severe calcification is not a featureof coronary luminal narrowing and plaque instability [5,6]. More-over, a systematic autopsy study on coronary arteries of sudden
Open access under the Elsevier OA license.
coronary death victims revealed that the majority of acute rupturedand thrombosed plaques is only mildly calcified [6]. In addition,a recent in vivo study by using intravascular ultrasound (IVUS)suggested that not the degree, but the pattern of calcifications

8 lerosis 218 (2011) 83– 89
(i
iptiaCap
iptmtirutbfisom
shroarsfirfiCP
2
2
pPdopwt53aIctnsrblSt
4 X. Li et al. / Atherosc
multiple, small calcium deposits) could be associated with plaquenstability [7].
In contrast to calcification, inflammation plays a crucial rolen plaque vulnerability [8]. Numerous intraplaque inflammatoryroteins are capable of degrading the fibrous cap, which may even-ually lead to plaque rupture and thrombosis. Furthermore, severalnflammatory biomarkers have been elucidated that are associ-ted with adverse cardiovascular outcome, of which particularly-reactive protein (CRP), osteopontin (OPN) and lipoprotein-ssociated phospholipase A2 (Lp-PLA2) appear to have a strongredictive value [9–14].
With the development of high resolution intravascular imag-ng techniques, several histological characteristics of vulnerablelaques (thickness of fibrous cap, size of necrotic core) can be iden-ified and quantified in vivo; but detection of the “vulnerability
arker” intraplaque inflammation is still a problem that needso be resolved in clinical practice [15]. In contrast to intraplaquenflammation, calcifications are an excellent marker of atheroscle-otic plaques and can be visualized even in micro-dimensions withse of high resolution image techniques [16]. Dystrophic calcifica-ion typifies many chronic inflammatory processes in the humanody [17], but a putative relationship between presence of calci-cations and pro-inflammatory tissue markers has not yet beentudied in vivo in the culprit lesions of AMI patients. This could bef interest, since hypothetically, distinct patterns of calcificationsay serve as a surrogate marker of plaque inflammatory activity.ST-segment elevation myocardial infarction (STEMI) is a sub-
et of AMI and characterized by severe transmural necrosis andigh short-term mortality [18,19]; as results of which emergentevascularization treatment of the occluded coronary artery is rec-mmended for patients with STEMI by means of thrombectomydjunctive to percutaneous coronary intervention (PCI) [20]. Mate-ials retrieved from thrombectomy appear suitable for histologicaltudy, since they have been shown to contain plaque fragmentsrom culprit lesions of STEMI patients (in addition to thrombus)n up to 40% of cases [21]. In the present study we investigated theelationship between distinct morphologic patterns of plaque calci-cations and the intraplaque immunolocalization of macrophages,RP, osteopontin and lipoprotein-associated phospholipase A2 (Lp-LA2) with use of the thrombectomy materials.
. Materials and methods
.1. Patient population
Between January 2005 and December 2006, a total of 562atients were treated with thrombectomy adjunctive to primaryCI. Patients were eligible if there was evidence of acute myocar-ial infarction with ST segment elevation of ≥0.2 mV in twor more contiguous leads on the admission electrocardiogra-hy and symptoms of <24 h’ duration. Thrombectomy proceduresere performed as previously described [21]. On admission, all
he patients received aspirin 300 mg and unfractionated heparin000–10,000 IU. Clopidogrel was administered in a loading dose of00 or 600 mg directly before or immediately after the procedurend was prescribed for at least 1 month. The use of glycoproteinIb/IIIa inhibitors and antithrombotic medications was at the dis-retion of operators. After access into the femoral artery, the flexiblehrombectomy catheter was advanced in the infarct-related coro-ary artery. Before balloon dilatation or stent implantation, severaluctions were performed at the site of culprit lesions. The aspi-ated materials were collected in the collection bottle, which could
e used for this study. Information with respect to cardiovascu-ar risk factors was obtained at bedside in the catheterization unit.erum hsCRP values, measured on admission, were obtained fromhe electronic hospital record.
Fig. 1. Selection of study materials. Thrombectomy materials obtained during pri-mary PCI were screened and divided into two groups based on presence or absenceof calcifications.
2.2. Selection of thrombectomy materials
All the aspirated materials were placed in 10% neutralbuffered formalin immediately after retrieval, fixed for at least24 h and embedded in paraffin. Six-micrometer-thickness sec-tions were stained with hematoxylin and eosin stains (H&Estain) for histopathological observations including identificationof calcifications. Adjacent tissue sections were stained immuno-histochemically for evaluation of the intraplaque inflammatorybiomarkers. Size of samples was measured macroscopically onglass slices. Only samples of ≥1 mm2, and of those only the sam-ples that contained histologically confirmed atherosclerotic plaquetissues, were enrolled in this study (see Fig. 1).
2.3. Morphometric analysis of tissue calcifications andvisualization of colocalization between calcifications andmacrophages
Morphometric analysis of calcifications was performed onAlizarin red S (ARedS) stained sections. Immuno-enzyme dou-ble staining with anti-HAM56 antibody (1:50, Dako, Glostrup,Denmark) and ARedS was used to study the colocalization betweencalcifications and macrophages. Images of calcifications wereacquired at ×100 magnification using a Leica DFC500 digital cam-era mounted on a Leica DM 5000 microscope. Measurement ofcalcifications was performed automatically by using computer-based image software (Image Pro Plus 5.0, Media Cybernetics). Onlythe particles ≥4 �m were measured for final evaluation, which isaround the minimum range of detection of current high resolutionimaging techniques.
2.4. Evaluation of CRP, OPN and Lp-PLA2 immunostaining
Presence of intraplaque CRP or Lp-PLA2 was evaluated withimmunodouble staining combining anti-CRP antibody (rabbitmonoclonal Y284, 1:500, Abcam, Cambridge, UK) or anti-Lp-PLA2 antibody (rabbit polyclonal HPA018157, 1:20, Sigma, St.
X. Li et al. / Atherosclerosis 218 (2011) 83– 89 85
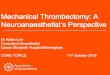
Table 1Patient clinical characteristics.
Calcification (67) Non-calcification (104) P-value
Gender (male) 68.7% 76.9% 0.29Age (years; mean, ±SD) 63.5 ± 12.1 63.1 ± 13.2 0.82Diabetes mellitus 14.1% 22.1% 0.28Hypertension 37.3% 35.6% 0.87Dyslipidemia 50.0% 54.8% 0.80Current smoker 43.1% 42.2% 1.00Previous myocardial infarction 38.8% 31.8% 0.41Statin 39.4% 33.7% 0.51
BMI (kg/m2; median,range)
25.6 26.1 0.1617.7–47.8 18.8–41.2
Serum hsCRP (mg/l;median, range)
3.8 2.6 0.240.4–71.1 0–98.1
Pre-infarct unstable angina 28.6% 18.8% 0.22
Event to balloon time (min;median, range)
184.5 185.0 0.9575.0–959.0 64.0–844.0
Location of lesionsRCA 50.8% 50.5% 0.976LCA 44.6% 45.5%LCx 4.6% 4.0%
Size of materials (mm;median, range)
3.0 3.5 0.811.0–11.0 1.0–18.0
C al varia prote
LMopoDoaapccmf
iri3p
2
entdte≤
3
3
m8
ontinuous variables are expressed as mean ± SD or median with range. Categoricrtery, LCx: left circumflex; BMI: body mass index; hsCRP: high sensitive C-reactive
ouis, USA) with anti-CD68 antibody (mouse monoclonal PG-1, 1:100, Dako). Intraplaque OPN was analyzed with the use
f immunotriple staining combining anti-OPN antibody (rabbitolyclonal 1:1000, Abcam), anti-smooth muscle actin (mouse mon-clonal 1A4, 1:2000, Dako) and anti-CD68 antibody (PG-M1, 1:500,ako). Double and triple staining methods were used as previ-usly described [22]. Diaminobenzidine (DAB, Dako), Vector Bluend Vector Red substrate kits (Vector Laboratories) were applieds chromogens. Negative controls were performed by replacing therimary antibodies with non-immune IgG of similar species, sub-lass and concentration. Steatotic liver tissue was used as positiveontrol for CRP stain, cerebral tissue for Lp-PLA2 stain and post-ortem coronary atherosclerotic plaque served as positive control
or OPN stain.In each thrombectomy sample, CRP, Lp-PLA2 and/or OPN
mmunostaining was evaluated as either present or absent, and cor-elated with presence of calcification in the samples. Furthermore,ntensity of extracellular CRP and Lp-PLA2 staining was graded into
categories: 0 (negative), 1 (mild positive staining) and 2 (strongositive staining).
.5. Statistics
Statistical analysis was performed with SPSS 11. Results arexpressed as mean ± SD or median with range. In case the data wereormally distributed, the 2 groups were compared with unpaired
test. Comparison of non-normal distributed data of two indepen-ent groups, Mann–Whitney test was used and the Kruskal–Wallisest was used for ≥3 independent groups. Categorical data werexpressed as percentage and evaluated with �2 test. A P-value of0.05 was considered statistically significant.
. Results
.1. Patient clinical characteristics
Fig. 1 shows the flow chart for selection procedure of studyaterials. Histologically confirmed materials were obtained from
2% (460/562) of all the thrombectomy procedures. Majority (63%,
ables are expressed as percentages. RCA: right coronary artery, LCA: left coronaryin.
289/460) of the materials are composed exclusively of thrombus,whereas 37% (171/460) of the materials consist of both thrombusand atherosclerotic plaque tissue. Only the thrombectomy materi-als containing plaque tissues (n = 171) were included in the currentstudy. Of these, calcifications were present in 39% (67/171) andabsent in 61% (104/171) of the samples.
Patient characteristics were summarized in Table 1. There wereno differences in major risk factors for cardiovascular diseases,in medication or serum hsCRP values between the patients withcalcifications in the thrombectomy materials and those withoutcalcifications. The interval from onset of symptom to opening ofvessels was in 96% of the patients within 12 h and no differencewas found between the study groups (P = 0.95). Pre-infarct unsta-ble angina, defined as unstable angina of <30 min in the proceeding2 weeks, was observed in 23% of all the patients and there was nodifference between the two study groups (P = 0.22).
3.2. Calcification score in plaque tissue
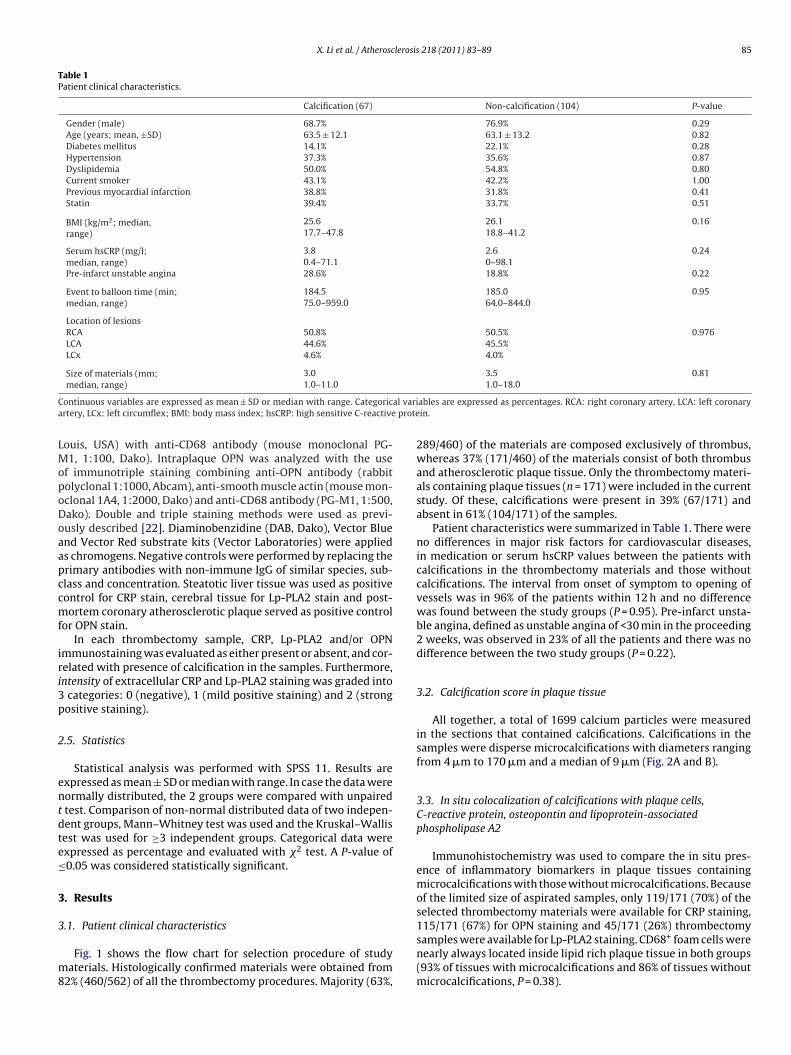
All together, a total of 1699 calcium particles were measuredin the sections that contained calcifications. Calcifications in thesamples were disperse microcalcifications with diameters rangingfrom 4 �m to 170 �m and a median of 9 �m (Fig. 2A and B).
3.3. In situ colocalization of calcifications with plaque cells,C-reactive protein, osteopontin and lipoprotein-associatedphospholipase A2
Immunohistochemistry was used to compare the in situ pres-ence of inflammatory biomarkers in plaque tissues containingmicrocalcifications with those without microcalcifications. Becauseof the limited size of aspirated samples, only 119/171 (70%) of theselected thrombectomy materials were available for CRP staining,115/171 (67%) for OPN staining and 45/171 (26%) thrombectomy
samples were available for Lp-PLA2 staining. CD68+ foam cells werenearly always located inside lipid rich plaque tissue in both groups(93% of tissues with microcalcifications and 86% of tissues withoutmicrocalcifications, P = 0.38).
86 X. Li et al. / Atherosclerosis 218 (2011) 83– 89
F ing ws ata of
i to the
lisOmTOcasc
satpa
4
ttootaps
TO
CC
ig. 2. Morphometric analysis of calcifications. (A) Immuno-enzyme double staintained in red as shown with arrows and macrophages stained in blue. (B) Pooled dnterpretation of the references to color in this figure legend, the reader is referred
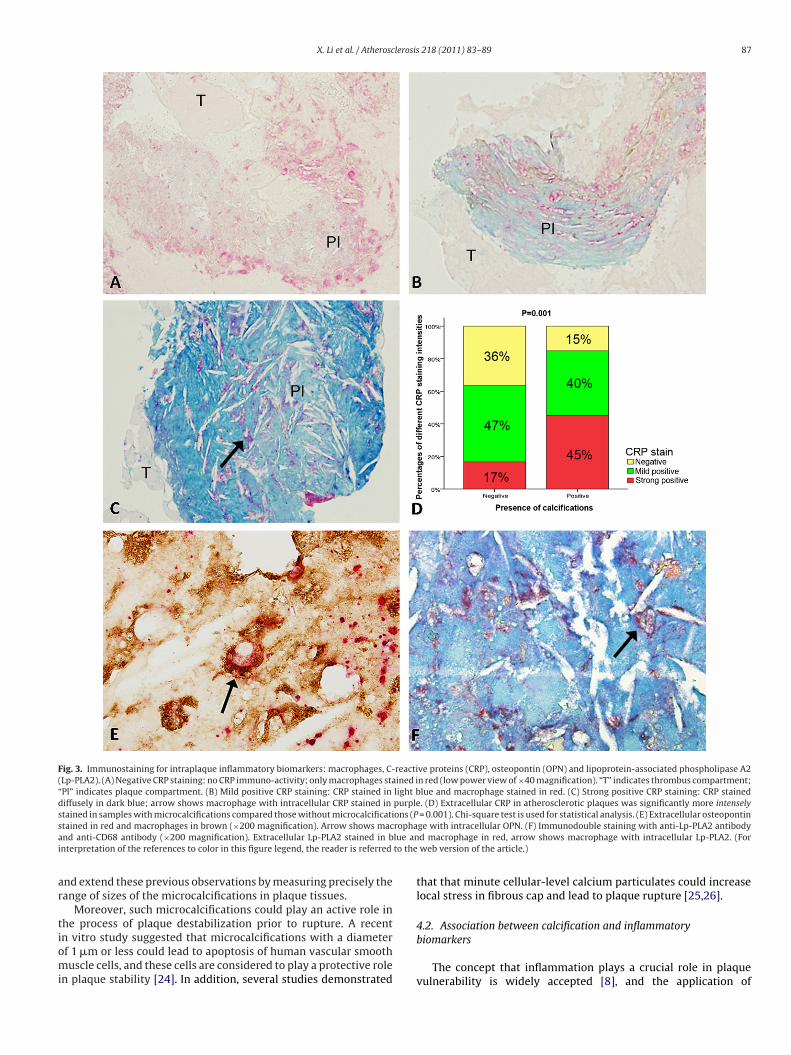
If present, extracellular CRP staining was found throughoutipid plaque tissue (Fig. 3A–C), whereas extracellular OPN stain-ng appeared bound to microcalcifications (Fig. 3E). Immunotripletaining with anti-CD68, anti-smooth muscle actin and anti-PN antibodies showed that cytoplasmic OPN was present inacrophages only, and not in smooth muscle cells. As shown in
able 2, both intra- and extracellular immunostaining of CRP andPN was found more frequently in plaque tissues with micro-alcifications than those without microcalcifications (P < 0.05 forll). Furthermore, intensity of CRP immunostaining was greater inamples with microcalcifications than those without microcalcifi-ations (P = 0.001, Fig. 3D).
Immunostainable Lp-PLA2 was present in 96% of plaque tis-ues containing thrombectomy samples, strictly localized in thereas with extracellular lipid and macrophages (vulnerable plaqueissue) (Fig. 3F). However, there were no differences observed inresence (Table 2) or staining intensity of Lp-PLA2 between calcifiednd non-calcified plaque tissues (P = 0.15).
. Discussion
Thrombectomy adjunctive to primary PCI, which is currentlyhe treatment of choice for patients with STEMI in our institu-ion, provides a unique opportunity to retrieve large numbersf tissue samples from culprit atherosclerotic lesions related tonset myocardial infarction. In the present study we demonstrated
hat thrombectomy materials can be used as ex vivo materi-ls for histopathological investigation of potential biomarkers forlaque vulnerability in STEMI patients. The primary results of thistudy show that disperse calcium deposits with dimensions ofable 2verview of results.
Calcification group
Calcification diameters (�m; median, range) 9, 4–170Macrophages 93% (49/53)
Extracellular CRP 85% (45/53)
Intracellular CRP in macrophages 59% (31/53)
Extracellular OPN 98% (49/50)
Intracellular OPN in macrophages 76% (38/50)
Smooth muscle cells 32% (16/50)
Extracellular Lp-PLA2 96% (22/23)
Intracellular Lp-PLA2 in macrophages 61% (14/23)
ontinuous variables are expressed as median with range. Categorical variables are expr-reactive protein; OPN indicates osteopontin; Lp-PLA2 indicates lipoprotein-associated
ith anti-HAM56 antibody and Alizarin Red S (×200 magnification). Calcificationsdiameters of all the measured calcifications; range: 4–170 �m; median: 9 �m. (For
web version of the article.)
microcalcifications (median = 9 �m, range 4–170 �m), can be foundin 39% of the thrombectomy samples containing plaque tissues, andare strongly associated with immunostaining of the biomarkers forcardiovascular risk CRP and OPN in plaque tissues, but not Lp-PLA2.
4.1. Microcalcifications in culprit lesions of STEMI patients
Although calcification is a well-known feature of coronaryatherosclerotic plaques, its potential role in onset of plaque insta-bility remains controversial. An autopsy study by Sangiorgi et al.showed that coronary calcification was proportional to overallplaque burden, but was not associated with the severity of anatomicstenosis [5]. However, with the introduction of EBCT, coronary cal-cification can be analyzed quantitatively in vivo, and several clinicalstudies have shown that the EBCT-derived coronary calcium scorecan be considered as a strong predictor of adverse cardiovascularprognosis, even in asymptomatic patients [3,4]. Also size of calci-fications seems to be important. Virmani et al. [6,23] revealed thatcalcifications in 65% of acute ruptured plaques of sudden coronarydeath victims were radiographically so-called “speckled calcifica-tions”. Similar results were obtained by Ehara et al. [7] who, withuse of IVUS, compared calcifications in culprit lesions of acute coro-nary syndromes with those of chronic stable angina. They observedmultiple, small calcium deposits (so-called “spotty calcifications”)in the tissues of patients with acute coronary syndromes, in con-
trast to patients with stable angina who had only few but largecalcifications. Our findings of disperse microcalcifications in 39%of the thrombectomy specimens containing plaque tissues whichare all obtained from culprit plaques underlying STEMI, confirmNon-calcification group P-value
86% (57/66) 0.3864% (42/66) 0.01232% (21/66) 0.00556% (36/65) <0.00140% (26/65) <0.001
43% (29/65) 0.1896% (21/22) 146% (10/22) 0.38
essed as percentages. Chi-square test is used for statistical analysis. CRP indicatesphospholipase A2.
X. Li et al. / Atherosclerosis 218 (2011) 83– 89 87
Fig. 3. Immunostaining for intraplaque inflammatory biomarkers: macrophages, C-reactive proteins (CRP), osteopontin (OPN) and lipoprotein-associated phospholipase A2(Lp-PLA2). (A) Negative CRP staining: no CRP immuno-activity; only macrophages stained in red (low power view of ×40 magnification). “T” indicates thrombus compartment;“Pl” indicates plaque compartment. (B) Mild positive CRP staining: CRP stained in light blue and macrophage stained in red. (C) Strong positive CRP staining: CRP staineddiffusely in dark blue; arrow shows macrophage with intracellular CRP stained in purple. (D) Extracellular CRP in atherosclerotic plaques was significantly more intenselystained in samples with microcalcifications compared those without microcalcifications (P = 0.001). Chi-square test is used for statistical analysis. (E) Extracellular osteopontins rophaa lue ani to the
ar
tiomi
tained in red and macrophages in brown (×200 magnification). Arrow shows macnd anti-CD68 antibody (×200 magnification). Extracellular Lp-PLA2 stained in bnterpretation of the references to color in this figure legend, the reader is referred
nd extend these previous observations by measuring precisely theange of sizes of the microcalcifications in plaque tissues.
Moreover, such microcalcifications could play an active role inhe process of plaque destabilization prior to rupture. A recent
n vitro study suggested that microcalcifications with a diameterf 1 �m or less could lead to apoptosis of human vascular smoothuscle cells, and these cells are considered to play a protective rolen plaque stability [24]. In addition, several studies demonstrated
ge with intracellular OPN. (F) Immunodouble staining with anti-Lp-PLA2 antibodyd macrophage in red, arrow shows macrophage with intracellular Lp-PLA2. (For
web version of the article.)
that that minute cellular-level calcium particulates could increaselocal stress in fibrous cap and lead to plaque rupture [25,26].
4.2. Association between calcification and inflammatory
biomarkersThe concept that inflammation plays a crucial role in plaquevulnerability is widely accepted [8], and the application of

8 lerosis
icpacsHCdhmnwtsttCiwtmssev
aOiotmSirim
niafnmtcaLmp
5
pcsbmvrabpa
[
[
[
[
[
[
[
[
[
[
[
[
8 X. Li et al. / Atherosc
nflammatory biomarkers as tools in cardiovascular risk stratifi-ation has become a hotspot. Among all the biomarkers, the acutehase protein CRP is studied most extensively and considered to be
robust predictor of poor cardiovascular outcome [9–11]. Severallinical studies have investigated the putative relationship betweenerum CRP levels and coronary calcification. In the Framinghameart Study a positive association was reported between level ofRP in the blood and subclinical coronary calcification detectedoor EBCT [27]. In contrast, the SIRCA study showed that serumsCRP was not at all associated with coronary calcifications inen, and only weakly in women [28]. The present study also did
ot reveal any difference in serum hsCRP levels between patientsith- and without plaque microcalcifications in their thrombec-
omy materials. But, when we applied CRP-immunostaining on theame specimens of all the patients, it was shown that the plaqueissues with microcalcifications contain more frequently immunos-ainable CRP, including CD68+ macrophages with intracytoplasmicRP. Moreover, the extracellular CRP was immunostained more
ntensely in the plaque tissues with microcalcifications than thoseithout microcalcifications. These findings showed that CRP inside
he plaques associated with microcalcifications appears to be a farore common feature as can be appreciated from measurement of
erum hsCRP levels. Still such low levels of intraplaque CRP synthe-is can be of relevance, since CRP exerts several pro-inflammatoryffects inside the plaque [29], which may further increase plaqueulnerability.
Osteopontin (OPN) is another important biomarker and stronglyssociated with poor cardiovascular prognosis [12]. In addition,PN plays an important role in migration of macrophages and
nhibits ectopic calcification in human body [30,31]. Similar tour results on CRP immunostaining, we found a positive associa-ion between extracellular immunostainable OPN, OPN containing
acrophages and the presence of microcalcifications in plaques.uch observations endorse the outcome of recent in vitro stud-es on macrophages co-cultured with calcium particles, whichevealed that microcalcifications induce a proinflammatory effectn macrophages, as became evident by their secretion of proinflam-
atory cytokines [32].Lp-PLA2, as a calcium-independent phospholipase A2, is another
ovel inflammatory biomarker. Serum levels and in situ expressionn carotid atherosclerosis of Lp-PLA2 are positively associated withdverse cardiovascular outcomes, independently of traditional riskactors [13,14]. We found positive Lp-PLA2 immunostaining inearly all the plaque fragments containing extracellular lipid andacrophages (the vulnerable plaque components), which illus-
rates the importance of the protein as a biomarker. However, inontrast to our findings on CRP and OPN, we found no positivessociation between presence of microcalcifications and plaquep-PLA2 immunopositivity, so apparently a pattern of disperseicrocalcifications cannot serve as a surrogate marker for in situ
resence of this protein.
. Conclusion
In this study we have shown that when microcalcifications areresent in plaque fragments of STEMI patients, they frequentlyolocalize with the inflammatory biomarkers CRP and OPN; asuch, a subgroup of plaques with high inflammatory burden cane identified. As a future perspective, we may speculate that theseicrocalcifications in plaques, which can be detected by means of
arious in vivo imaging techniques, could serve as a potential sur-ogate marker for intraplaque inflammatory activity. However, the
pplication of the microcalcifications as a marker for plaque insta-ility needs to be confirmed, since the sensitivity, specificity andredictive value of this marker is still undefined without compar-tive data on non-culprit lesions.[
218 (2011) 83– 89
Conflict of interest
There is no financial conflict of interest.
Acknowledgement
The study is supported by Netherlands Heart Foundation.
References
[1] Davies MJ, Thomas AC. Plaque fissuring—the cause of acute myocardialinfarction, sudden ischaemic death, and crescendo angina. Br Heart J1985;53:363–73.
[2] Goldstein JA, Demetriou D, Grines CL, et al. Multiple complex coronary plaquesin patients with acute myocardial infarction. N Engl J Med 2000;343:915–22.
[3] Arad Y, Spadaro LA, Goodman K, et al. Predictive value of electron beamcomputed tomography of the coronary arteries. 19-month follow-up of 1173asymptomatic subjects. Circulation 1996;93:1951–3.
[4] Arad Y, Spadaro LA, Goodman K, et al. Prediction of coronary events with elec-tron beam computed tomography. J Am Coll Cardiol 2000;36:1253–60.
[5] Sangiorgi G, Rumberger JA, Severson A, et al. Arterial calcification and not lumenstenosis is highly correlated with atherosclerotic plaque burden in humans:A histologic study of 723 coronary artery segments using nondecalcifyingmethodology. J Am Coll Cardiol 1998;31:126–33.
[6] Burke AP, Weber DK, Kolodgie FD, et al. Pathophysiology of calcium depositionin coronary arteries. Herz 2001;26:239–44.
[7] Ehara S, Kobayashi Y, Yoshiyama M, et al. Spotty calcification typifies the culpritplaque in patients with acute myocardial infarction: an intravascular ultra-sound study. Circulation 2004;110:3424–9.
[8] van der Wal AC, Becker AE, van der Loos CM, et al. Site of intimal ruptureor erosion of thrombosed coronary atherosclerotic plaques is characterizedby an inflammatory process irrespective of the dominant plaque morphology.Circulation 1994;89:36–44.
[9] Sabatine MS, Morrow DA, Jablonski KA, et al. Prognostic significance of the cen-ters for disease control/american heart association high-sensitivity c-reactiveprotein cut points for cardiovascular and other outcomes in patients with stablecoronary artery disease. Circulation 2007;115:1528–36.
10] Ridker PM, Cushman M, Stampfer MJ, et al. Inflammation, aspirin, and therisk of cardiovascular disease in apparently healthy men. N Engl J Med1997;336:973–9.
11] Liuzzo G, Biasucci LM, Gallimore JR, et al. The prognostic value of c-reactiveprotein and serum amyloid a protein in severe unstable angina. N Engl J Med1994;331:417–24.
12] Minoretti P, Falcone C, Calcagnino M, et al. Prognostic significance of plasmaosteopontin levels in patients with chronic stable angina. Eur Heart J2006;27:802–7.
13] Packard CJ, O’Reilly DS, Caslake MJ, et al. Lipoprotein-associated phospholipasea2 as an independent predictor of coronary heart disease. West of scotlandcoronary prevention study group. N Engl J Med 2000;343:1148–55.
14] Herrmann J, Mannheim D, Wohlert C, et al. Expression of lipoprotein-associatedphospholipase a(2) in carotid artery plaques predicts long-term cardiac out-come. Eur Heart J 2009;30:2930–8.
15] MacNeill BD, Lowe HC, Takano M, et al. Intravascular modalities for detec-tion of vulnerable plaque: current status. Arterioscler Thromb Vasc Biol2003;23:1333–42.
16] Kawasaki M, Bouma BE, Bressner J, et al. Diagnostic accuracy of optical coher-ence tomography and integrated backscatter intravascular ultrasound imagesfor tissue characterization of human coronary plaques. J Am Coll Cardiol2006;48:81–8.
17] Cotran RS, Kumar V, Collins T. Cellular pathology II: adaptations, intracellularaccumulations, and cell aging. Robbins pathologic basis of disease. Philadel-phia: W.B. Saunders Company; 1999. p. 43–5.
18] Nicod P, Gilpin E, Dittrich H, et al. Short- and long-term clinical outcome afterq wave and non-q wave myocardial infarction in a large patient population.Circulation 1989;79:528–36.
19] Chan MY, Sun JL, Newby LK, et al. Long-term mortality of patients undergo-ing cardiac catheterization for ST-elevation and non-ST-elevation myocardialinfarction. Circulation 2009;119:3110–7.
20] Kushner FG, Hand M, Smith Jr SC, et al. 2009 focused updates: ACC/AHA guide-lines for the management of patients with st-elevation myocardial infarction(updating the 2004 guideline and 2007 focused update) and acc/aha/scai guide-lines on percutaneous coronary intervention (updating the 2005 guideline and2007 focused update): a report of the american college of cardiology founda-tion/american heart association task force on practice guidelines. Circulation2009;120:2271–306.
21] Rittersma SZ, van der Wal AC, Koch KT, et al. Plaque instability frequentlyoccurs days or weeks before occlusive coronary thrombosis: a pathological
thrombectomy study in primary percutaneous coronary intervention. Circu-lation 2005;111:1160–5.22] van der Loos CM. Multiple immunoenzyme staining: methods and visual-izations for the observation with spectral imaging. J Histochem Cytochem2008;56:313–28.

lerosis
[
[
[
[
[
[
[
[
[
X. Li et al. / Atherosc
23] Virmani R, Burke AP, Farb A, et al. Pathology of the vulnerable plaque. J Am CollCardiol 2006;47:C13–18.
24] Ewence AE, Bootman M, Roderick HL, et al. Calcium phosphate crystalsinduce cell death in human vascular smooth muscle cells: a potentialmechanism in atherosclerotic plaque destabilization. Circ Res 2008;103:e28–34.
25] Vengrenyuk Y, Carlier S, Xanthos S, et al. A hypothesis for vulnerableplaque rupture due to stress-induced debonding around cellular micro-calcifications in thin fibrous caps. Proc Natl Acad Sci USA 2006;103:14678–83.
26] Bluestein D, Alemu Y, Avrahami I, et al. Influence of microcalcifications
on vulnerable plaque mechanics using fsi modeling. J Biomech 2008;41:1111–8.27] Wang TJ, Larson MG, Levy D, et al. C-reactive protein is associated with sub-clinical epicardial coronary calcification in men and women: the framinghamheart study. Circulation 2002;106:1189–91.
[
218 (2011) 83– 89 89
28] Reilly MP, Wolfe ML, Localio AR, et al. C-reactive protein and coronary arterycalcification: the study of inherited risk of coronary atherosclerosis (sirca).Arterioscler Thromb Vasc Biol 2003;23:1851–6.
29] Kobayashi S, Inoue N, Ohashi Y, et al. Interaction of oxidative stress and inflam-matory response in coronary plaque instability: important role of c-reactiveprotein. Arterioscler Thromb Vasc Biol 2003;23:1398–404.
30] Giachelli CM, Lombardi D, Johnson RJ, et al. Evidence for a role of osteopontin inmacrophage infiltration in response to pathological stimuli in vivo. Am J Pathol1998;152:353–8.
31] Scatena M, Liaw L, Giachelli CM. Osteopontin: a multifunctional molecule reg-ulating chronic inflammation and vascular disease. Arterioscler Thromb Vasc
Biol 2007;27:2302–9.32] Nadra I, Mason JC, Philippidis P, et al. Proinflammatory activation ofmacrophages by basic calcium phosphate crystals via protein kinase c and mapkinase pathways: a vicious cycle of inflammation and arterial calcification? CircRes 2005;96:1248–56.