Embed Size (px)
Citation preview
29 Curr Neurobiol 2018 Volume 9 Issue 1
Curr Neurobiol 2018; 9(1): 29-32 ISSN 0975-9042
A Pathway to Alzheimer’s diseaseHerbert B. Allen, Rina M. Allawh, Kavita Goyal
Drexel University College of Medicine, Department of Dermatology, USA
AbstractWe postulate a pathway to Alzheimer’s disease that begins with microbial pathogens, spirochetes, that make biofilms which upregulate the innate immune system. This leads to the destruction of the tissue and the formation of Aβ by known biochemical and microbiological pathways. The spirochetes also form biofilms intracellularly; and, in the process, create Aβ which stimulates the hyperphosphorylation of tau protein. This ultimately leads to the formation of neurofibrillary tangles and dendritic disintegration. All the steps in this pathway have been shown to be present by direct pathological observation or by known microbiological/biochemical pathways. As one proof of concept, things that negatively impact AD, such as diabetes, smoking, and certain drug exposures have been shown to influence one or another component of the pathway.
IntroductionThe key pathological findings on routine bright field
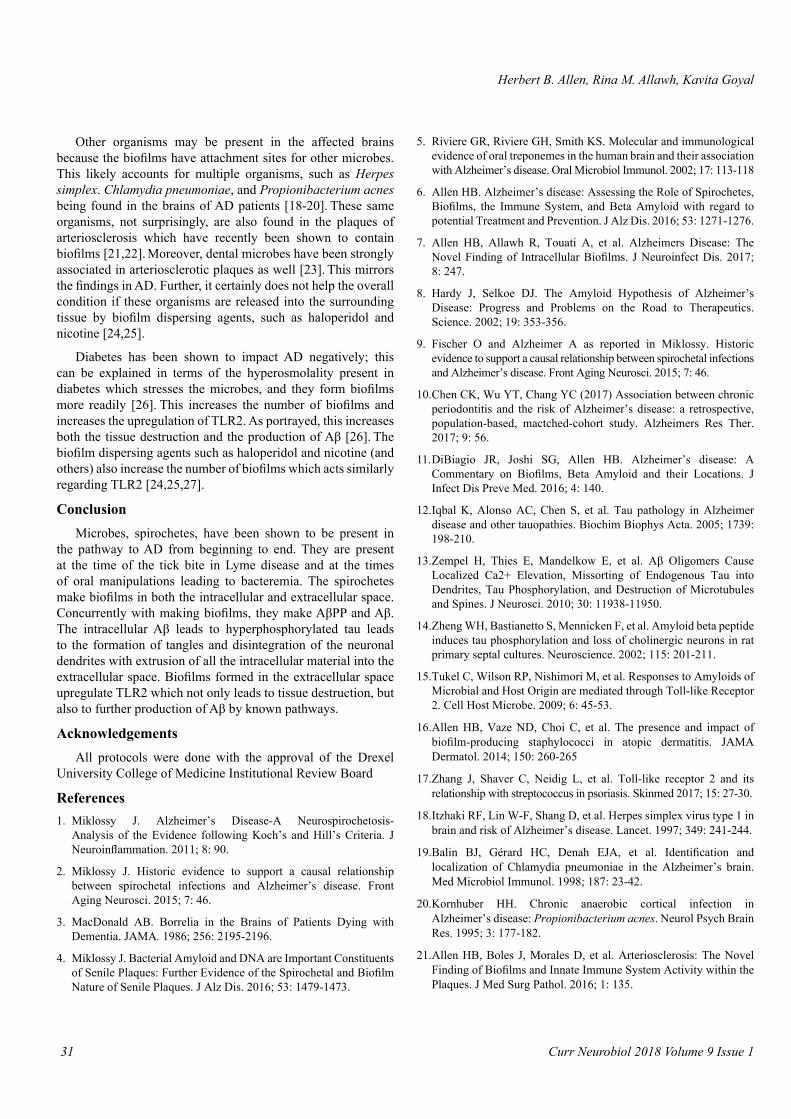
microscopy of Alzheimer’s disease (AD) brains are the presence of spirochetes, neurofibrillary tangles, senile plaques, neuronal loss, granulovacuolar degeneration, and tissue atrophy.1 With immunostaining, marked deposition of amyloid beta (Aβ) is noted [1]. On gross examination, the tissue is markedly shrunken and atrophic [1]. The pathological findings of syphilis are remarkably similar in all respects compared to AD [2] (Figure 1).
The key microbiological findings from these affected brains are the cultivation of Lyme spirochetes, the polymerase chain reaction (PCR) evidence of both Lyme and dental spirochetes, the presence of biofilms both intra and extracellularly, and the innate immune system response to the presence of the extracellular biofilms [3-7]. When stressed, the cultured spirochetes formed biofilms, amyloid beta precursor protein (AβPP), and Aβ [4]. The key questions that arise from these findings is what causes them and how do they interact to cause disease? Here we compile, collate, and correlate these pathological and microbiological findings and couple them with known biochemical pathways to produce a hypothesis (based entirely on observations) regarding the development of AD.
Aβ has been considered the prime malefactor in AD for the past 25 years [8] (Figure 2) but, with all the recent findings in pathology and microbiology, a different hypothesis may be entertained. That hypothesis is the disease arises from microbial pathogens, and the specific microbes that have been identified in the tissue are spirochetes [1]. These are predominant because of the pathological and microbiological evidence of their presence along with the fact that they mirror the impact of a known spirochete, namely Treponema pallidum of syphilis (Figure 1). The spirochetes involved are oral treponema (T. denticola as representative), Borrelia burgdorferi, and (as mentioned)
T. pallidum. T. pallidum, the etiologic agent in syphilis, is included because the pathology of AD and general paresis (GP) is identical, with the tangles, plaques, and neuronal loss the same in both diseases [1,2]. Moreover, this is in keeping with the original concepts regarding the microbial origin of senile dementia addressed in the 1907 paper by Oskar Fischer which included 16 cases (and reminded him of the pathology of actinomycosis), and the paper of Alois Alzheimer in 1907 which included one case. Alzheimer in 1911 presented a more comprehensive presentation of dementia in which he included another case [9].
The role of T. pallidum in tertiary syphilis is well-defined, but the role of Borrelia burgdorferi in inducing of the pathological findings may be even better defined because the organisms have not only been identified with PCR in the affected tissue but have also been cultivated from “fresh” post mortem material [3,4]. This seems more cogent than in syphilis because the T. pallidum has never been cultured. The dental spirochetes (while not having been cultured) have been identified with PCR and with epidemiologic studies [5,10].
In syphilis, the spirochetes arrive at the brain mostly by hematologic spread after the chancre. (There may be lymphatic spread as well.) Both modes of spread are somewhat dependent
Figure 1. Spirochetes from brains in syphilitic General Paresis (left) and Alzheimer’s disease (Right) from Mikossy (reference 2).

Curr Neurobiol 2018 Volume 9 Issue 1
A Pathway to Alzheimer’s disease
30
on the location of the disease. In Lyme disease, the spread is also mostly hematogenous after the bite of an infected tick. Both syphilis and Lyme disease appear to result from a single exposure, on the one hand to a sexual encounter, and on the other, to a tick bite. Multiple exposures can occur, but these would be perhaps more likely with repeated tick bites. Exposure to dental spirochetes is more likely to occur on an ongoing basis, especially as plaque builds up on the teeth. The spread noted with dental procedures (where blood is present) would be hematogenous and has a direct pathway to the brain via the facial vein and cavernous sinus [11]. Other pathways may also be present.
Spirochetes easily cross the blood brain barrier, and, once in the brain have an affinity for neurons and position themselves both intra and extracellularly. They then multiply and divide, albeit exceedingly slowly, and when a quorum is reached, they form biofilms which have been seen inside and outside of the cells [6,7] (Figure 3). In the process of making biofilms, the microbes also make AβPP and Aβ [4]. Just as is the case with biofilms, Aβ has been seen both intra and extracellularly. Consequently, one pathway for the presence of Aβ is that created by the spirochetes. Put simply, when they make biofilms, the spirochetes also make Aβ (and AβPP) [4].
Regarding the formation of phosphorylated tau and neurofibrillary tangles, the spirochetes have been shown to make biofilms intracellularly and, at the same time, create Aβ. This gives some illumination of the pathway to the creation of hyperphosphorylated tau protein. Ordinary tau protein is necessary for structural integrity and support of the neuronal dendrites. When Aβ fibrils are in juxtaposition with ordinary tau, they promote the phosphorylation of the tau and the formation of neurofibrillary tangles [12-14]. This ultimately leads to disintegration of the dendrites and that leads to cell death (Figure 4). With this phenomenon occurring, the contents
of the cell are now exteriorized and become extracellular. Incidentally, spirochetes have been found in association with the neurofibrillary tangles on pathological examination [2].
In the extracellular space, biofilms attract the innate immune system molecule Toll-like receptor 2 (TLR2) [7].
The biofilms (even though they may have been made by gram negative microbes [spirochetes]) have receptor sites for TLR2 in similar fashion to TLR4 activated by other gram-negative organisms [15]. (TLR2 is upregulated by the gram-positive staphylococci on the skin in atopic dermatitis and by the gram positive streptococci in the tonsils of psoriasis) [16,17]. The ordinary way TLR2 inactivates microbes is via the MyD88 pathway which eventuates in NFκB and TNFα. Both are agents of destruction, but the TNFα seems to be the more active. In addition to the destruction, the NFκB together with beta amyloid converting enzyme (BACE) catalyzes the conversion of AβPP to Aβ together with β and γ secretase (Figure 5). Thus, Aβ may either be made by the spirochetes intracellularly (as has been mentioned previously) or by the action of the innate immune system extracellularly in response to the spirochete-derived biofilms. The upregulation of the innate immune system occurs in the extracellular space.
Figure 2. Aβ in Alzheimer’s disease hippocampus; a massive amount of Aβ is present.
Figure 3. Hippocampus from AD patient stained with PAS showing intracellular and extracellular biofilms (senile plaques). (10X)
Figure 4. Tau protein when phosphorylated causes disruption of the neuronal dendrite. (from ADEAR/Wikimedia Commons).
31 Curr Neurobiol 2018 Volume 9 Issue 1
Herbert B. Allen, Rina M. Allawh, Kavita Goyal
5. Riviere GR, Riviere GH, Smith KS. Molecular and immunological evidence of oral treponemes in the human brain and their association with Alzheimer’s disease. Oral Microbiol Immunol. 2002; 17: 113-118
6. Allen HB. Alzheimer’s disease: Assessing the Role of Spirochetes, Biofilms, the Immune System, and Beta Amyloid with regard to potential Treatment and Prevention. J Alz Dis. 2016; 53: 1271-1276.
7. Allen HB, Allawh R, Touati A, et al. Alzheimers Disease: The Novel Finding of Intracellular Biofilms. J Neuroinfect Dis. 2017; 8: 247.
8. Hardy J, Selkoe DJ. The Amyloid Hypothesis of Alzheimer’s Disease: Progress and Problems on the Road to Therapeutics. Science. 2002; 19: 353-356.
9. Fischer O and Alzheimer A as reported in Miklossy. Historic evidence to support a causal relationship between spirochetal infections and Alzheimer’s disease. Front Aging Neurosci. 2015; 7: 46.
10. Chen CK, Wu YT, Chang YC (2017) Association between chronic periodontitis and the risk of Alzheimer’s disease: a retrospective, population-based, mactched-cohort study. Alzheimers Res Ther. 2017; 9: 56.
11. DiBiagio JR, Joshi SG, Allen HB. Alzheimer’s disease: A Commentary on Biofilms, Beta Amyloid and their Locations. J Infect Dis Preve Med. 2016; 4: 140.
12. Iqbal K, Alonso AC, Chen S, et al. Tau pathology in Alzheimer disease and other tauopathies. Biochim Biophys Acta. 2005; 1739: 198-210.
13. Zempel H, Thies E, Mandelkow E, et al. Aβ Oligomers Cause Localized Ca2+ Elevation, Missorting of Endogenous Tau into Dendrites, Tau Phosphorylation, and Destruction of Microtubules and Spines. J Neurosci. 2010; 30: 11938-11950.
14. Zheng WH, Bastianetto S, Mennicken F, et al. Amyloid beta peptide induces tau phosphorylation and loss of cholinergic neurons in rat primary septal cultures. Neuroscience. 2002; 115: 201-211.
15. Tukel C, Wilson RP, Nishimori M, et al. Responses to Amyloids of Microbial and Host Origin are mediated through Toll-like Receptor 2. Cell Host Microbe. 2009; 6: 45-53.
16. Allen HB, Vaze ND, Choi C, et al. The presence and impact of biofilm-producing staphylococci in atopic dermatitis. JAMA Dermatol. 2014; 150: 260-265
17. Zhang J, Shaver C, Neidig L, et al. Toll-like receptor 2 and its relationship with streptococcus in psoriasis. Skinmed 2017; 15: 27-30.
18. Itzhaki RF, Lin W-F, Shang D, et al. Herpes simplex virus type 1 in brain and risk of Alzheimer’s disease. Lancet. 1997; 349: 241-244.
19. Balin BJ, Gérard HC, Denah EJA, et al. Identification and localization of Chlamydia pneumoniae in the Alzheimer’s brain. Med Microbiol Immunol. 1998; 187: 23-42.
20. Kornhuber HH. Chronic anaerobic cortical infection in Alzheimer’s disease: Propionibacterium acnes. Neurol Psych Brain Res. 1995; 3: 177-182.
21. Allen HB, Boles J, Morales D, et al. Arteriosclerosis: The Novel Finding of Biofilms and Innate Immune System Activity within the Plaques. J Med Surg Pathol. 2016; 1: 135.
Other organisms may be present in the affected brains because the biofilms have attachment sites for other microbes. This likely accounts for multiple organisms, such as Herpes simplex. Chlamydia pneumoniae, and Propionibacterium acnes being found in the brains of AD patients [18-20]. These same organisms, not surprisingly, are also found in the plaques of arteriosclerosis which have recently been shown to contain biofilms [21,22]. Moreover, dental microbes have been strongly associated in arteriosclerotic plaques as well [23]. This mirrors the findings in AD. Further, it certainly does not help the overall condition if these organisms are released into the surrounding tissue by biofilm dispersing agents, such as haloperidol and nicotine [24,25].
Diabetes has been shown to impact AD negatively; this can be explained in terms of the hyperosmolality present in diabetes which stresses the microbes, and they form biofilms more readily [26]. This increases the number of biofilms and increases the upregulation of TLR2. As portrayed, this increases both the tissue destruction and the production of Aβ [26]. The biofilm dispersing agents such as haloperidol and nicotine (and others) also increase the number of biofilms which acts similarly regarding TLR2 [24,25,27].
ConclusionMicrobes, spirochetes, have been shown to be present in
the pathway to AD from beginning to end. They are present at the time of the tick bite in Lyme disease and at the times of oral manipulations leading to bacteremia. The spirochetes make biofilms in both the intracellular and extracellular space. Concurrently with making biofilms, they make AβPP and Aβ. The intracellular Aβ leads to hyperphosphorylated tau leads to the formation of tangles and disintegration of the neuronal dendrites with extrusion of all the intracellular material into the extracellular space. Biofilms formed in the extracellular space upregulate TLR2 which not only leads to tissue destruction, but also to further production of Aβ by known pathways.
AcknowledgementsAll protocols were done with the approval of the Drexel
University College of Medicine Institutional Review Board
References1. Miklossy J. Alzheimer’s Disease-A Neurospirochetosis-
Analysis of the Evidence following Koch’s and Hill’s Criteria. J Neuroinflammation. 2011; 8: 90.
2. Miklossy J. Historic evidence to support a causal relationship between spirochetal infections and Alzheimer’s disease. Front Aging Neurosci. 2015; 7: 46.
3. MacDonald AB. Borrelia in the Brains of Patients Dying with Dementia. JAMA. 1986; 256: 2195-2196.
4. Miklossy J. Bacterial Amyloid and DNA are Important Constituents of Senile Plaques: Further Evidence of the Spirochetal and Biofilm Nature of Senile Plaques. J Alz Dis. 2016; 53: 1479-1473.

Curr Neurobiol 2018 Volume 9 Issue 1
A Pathway to Alzheimer’s disease
32
Correspondence to:Herbert B Allen219 N. Broad St., 4th floor Philadelphia, PA 19107USAE-mail: [email protected]
22. Morré SA, Stooker W, Lagrand WK, et al. Microorganisms in the aetiology of atherosclerosis. J Clin Pathol. 2000; 53: 647-654.
23. Jirina Bartova, Pavla Sommerova, Yelena Lyuya-Mi, et al. (2014) Periodontitis as a Risk Factor of Atherosclerosis. J Immunol Res. 2014; 9.
24. Huybrechts KF, Gerhard T, Crystal S, et al. Differential risk of death in older residents in nursing homes prescribed specific antipsychotic drugs: population-based cohort study. BMJ. 2012; 344e977.
25. Allen HB, Joshi SG. Nicotine and Alzheimer’s disease: how the fog of smoke increases the fog of dementia. J Neuroinfect Dis. 2016; 7: 4.
26. Allen HB, Husienzad L Joshi SG. The Impact of Diabetes on Alzheimer’s disease. JAlz Dis. 2016; http://www.j-alz.com/content/impact-diabetes-alzheimers-disease
27. Allen HB, Hossain C, Abidi N, et al. Penicillin: The Old/New Wonder Drug. Adv Tech Biol Med. 2017; 5: 197.