Embed Size (px)
Citation preview

Ac
T
Fb
rbvcypcessattt
atvse
MP
Operative Techniques in Otolaryngology (2010) 21, 39-43
1d
panoramic approach to the anterior skull base—Theombined subfrontal/subcranial and Le Fort I approach
erry Y. Shibuya, MD, FACS,a Randall Schoeman, MD, DDS,a Sooho Choi, MDb
rom the aDepartment of Head and Neck Surgery and the
Department of Neurosurgery, Southern California Permanente Medical Group, Anaheim, California.Surgical exposure for massive tumor of the anterior skull base can be difficult. We have combined twosurgical approaches, the subfrontal/subcranial approach and the Le Fort I osteotomy approach, toprovide panoramic accesses to the anterior skull base. Via this combination of exposures, we haveeasily accessed and resected tumors extending from the cribiform plate all the way down to the levelof the upper cervical spine. Additionally, we have used the nasal endoscope and microscope to assistin our resection. This approach has several advantages, which include ease of post-resection skull basereconstruction and excellent cosmetic results by avoiding anterior facial incisions. We believe thisapproach should be in the armamentarium of any surgeon resecting massive anterior skull base tumor.© 2010 Elsevier Inc. All rights reserved.
KEYWORDSSubfrontal;Subcranial;Le Fort I;Advanced head andneck tumors;Anterior skull basetumors
sadesafaoo
T
T
1
2
3
Panoramic access to the anterior skull base is frequentlyequired for massive tumors that traverse the anterior skullase and span multiple regions. Very few approaches pro-ide wide surgical exposure that spans from the anteriorribiform plate to the upper cervical spine. Over the past 8ears, we have combined the subfrontal/subcranial ap-roach with the Le Fort I approach simultaneously. Thisombination has provided a panoramic exposure of thentire anterior skull base, from cribiform to upper cervicalpine. Both are easy to perform and hide all surgical inci-ions in the scalp and sublabial regions, thereby avoidingny facial scars. We have found that, for selectively largeumors, this combination of approaches provides excellentumor access, hidden facial incisions, and easy reconstruc-ive options.
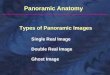
Raveh, in 1978, pioneered the subfrontal approach to thenterior skull base for the repair of high-velocity skull baserauma and congenital anomalies.1,2 This approach providesertical access from the anterior ethmoid roof down to theuperior clivus and horizontal access across both orbital roofs,xtending toward the temporal bones laterally (Figure 1). Vi-
Address reprint requests and correspondence: Terry Y. Shibuya,D, FACS, Department of Head and Neck Surgery, Southern California
ermanente Medical Group, 3460 La Palma Ave, Anaheim, CA 92806.
E-mail address: [email protected].043-1810/$ -see front matter © 2010 Elsevier Inc. All rights reserved.oi:10.1016/j.otot.2010.03.007
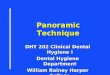
ualization of the nasal cavity and maxillary sinuses is possibles well. The subfrontal exposure allows for intra- and extra-ural tumor resection with minimal frontal lobe retraction. Tonhance visualization of the entire clivus and upper cervicalpine inferiorly, a transmaxillary or Le Fort I approach isdded3 (Figure 2). In addition, the septum is mobilized in aashion similar to a transeptal/transnasal pituitary approachfter mobilizing the lower maxilla inferiorly via a Le Fort Isteotomy. This combination of techniques allows a pan-ramic approach to the anterior skull base.
echnique
he subfrontal approach is briefly reviewed.
. The subfrontal approach begins with a coronal incisionperformed from preauricular crease to preauricular crease.
. A pericranial flap is preserved and based on the su-pratrochlear and supraorbital arteries for later use inreconstruction of the anterior skull base defect. The flapis carried down to the frontozygomatic suture line later-ally and to the rhinion and piriform aperture medially.
. The orbit is accessed and the periorbita elevated off themedial, superior, and lateral orbital walls (Figure 3A).
The anterior ethmoidal artery is ligated.
4
5
Ftroso
L
T
Fbe
F
40 Operative Techniques in Otolaryngology, Vol 21, No 1, March 2010
. Osteotomies are marked out, and the size of frontal boneflap removed is dependent on the size of tumor beingaccess/resected. Osteotomies are usually performed asfollows: superior osteotomy—placed across the frontalbone in a horizontal plane; lateral osteotomies—cutfrom the superior osteotomy ends inferiorly down andthru the superior orbital rims bilaterally; orbital osteoto-mies—placed from the superior orbital rim cut 1 cmposterior into the superior orbital roof, then cut 90°medially to the medial orbital wall, then cut inferiorlydown the medial orbital wall to the level of the nasolac-rimal duct, then cut anteriorly and out the medial orbitalwall; anterior osteotomy—placed along the nasomaxillarygroove horizontally just anterior to the lacrimal duct andconnected with the opposite side (Figure 3B). A final ver-tical osteotomy is performed anterior to the crista gallidetaching the frontonasal segment. The orbit and dura areprotected at all times with ribbon retractors (Figure 4A).
. There are variations in the size of bone flap removed (Fig-ure 4). A Raveh type I approach removes the frontonasalsegment while preserving the posterior wall of the frontalsinus. The posterior wall is removed in a second step and isindicated when tumor abuts this region. A Raveh type IIapproach removes the frontonasal segment, which includesthe posterior wall of the frontal sinus. This is performedwhen tumor involves the posterior wall or broader intracra-nial exposure is needed to access the tumor. Visualizationand removal of tumor extending to the sphenoid sinus andclivus is easily achieved.
or sinonasal tumors extending through the olfactory groove,he olfactory cleft may be easily keyholed and dropped infe-iorly into the sinus cavity for an en bloc resection. If tumornly involves one side of the olfactory groove, the involvedide may be easily visualized and resected while preserving the
igure 1 The subfrontal or subcranial approach to the skullase. The arrow indicates the improved view with the subfrontalxtension.
pposite side. p
e Fort I approach
he Le Fort I approach is briefly reviewed.
1. A sublabial incision is performed in the gingival-buccalsulcus, leaving a 5- to 7-mm cuff of mucosa for closureof the wound postoperatively.
2. The cheek is elevated off bilateral anterior maxillary sinuswalls to the level of the nasal aperture and superiorly bothmedial and lateral to the inferior orbital nerve exiting itsforamen on the anterior maxillary wall (Figure 5).
3. Next, the mucosa of the inferior nasal floor is elevatedbilaterally, and the mucosa is elevated off the lower nasalseptum bilaterally. This can be done via the sublabialincision or performed via a hemitransfixation incision inthe right nostril (similar to performing a septoplasty).When doing this, we elevate the mucosa off the septumcompletely on one side and on the remaining side onlyelevated to 3-5 mm above the maxillary crest/cartilaginousseptal junction. This will preserve the septal mucosal at-tachment on one side, ensuring a cartilage/mucosa vascu-lar blood supply to one side.
4. Next, osteotomies are performed along the anterior,medial, and lateral maxillary sinus walls using an os-cillating saw (Figure 6).
5. After performing the osteotomies, 1.5-mm titaniummidface plates are bent, drilled, and fixed into position.This will allow for correct anatomic positioning of themaxilla prior to fracturing. The plates are then saved incups marked with the correct anatomical position forreconstruction post tumor resection (Figure 7).
6. Next, a curved osteotome is placed in the pterygomax-illary fissure, and an osteotomy is performed on the leftand right sides.
7. After this, two small self-retaining retractors are placedbetween the anterior maxillary osteotomies on the left
igure 2 The transmaxillary with the Le Fort I osteotomy ap-
roach to the skull base. Lines indicate the extent of exposure.
1
R
B
1
viewed
Fb
41Shibuya et al Combined Subfrontal/Subcranial and Le Fort I Approach
and right sides (Figure 8). Each is then simultaneouslyopened, similar to “opening a clam shell.”
8. At the base of the clam shell or posterior wall of themaxilla, the pterygoid plates are then resected carefullyusing Takahashi forceps, and the pterygoid muscles arereleased from their insertion on the plates. As thisoccurs, the maxilla will descend, and the self-retainingretractor can be maximally opened.
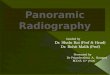
9. The septum can now be pushed to one side, and a Hardypituitary retractor can be placed trans-septally to exposethe anterior wall of the sphenoid sinus. Because the cavityis very large, the speculum lies at the level of the uppercervical spine region. To enhance exposure, we usuallyplace two Hardy retractors on top of each other to provideenhanced retraction and exposure (Figure 9).
Figure 3 The subfrontal approach. (A) Subcranial access
igure 4 Raveh type 1 and 2 approaches. (A) The frontal bone fl
one flap and view obtained.0. At this point, surgical exposure will be visible from thecribiform region all the way to the level of the uppercervical spine. The endoscope or microscope or both canbe used to assist with tumor resection using this technique.
econstruction
rief review of reconstruction option:
. Once the tumor has been resected, there are severaloptions for reconstructing the anterior skull base. A largepericranial flap that was previously harvested with thesubfrontal approach may be rotated into the defect. This
from above. (B) Osteotomies performed. FS, frontal sinus.
ated with the type 1 and 2 approaches. (B) Removal of the frontal
ap cre
2
3
4
5
6
C
Tplpflrcdlucttvcpt
Fa
Fp
Fm
F
42 Operative Techniques in Otolaryngology, Vol 21, No 1, March 2010
can be used to seal the cribiform region and sphenoidsinus and line the clivus and cervical spine.
. If the flap is too short or inadequate in length to reach,we routinely harvest tensor fascia lata from the thigh,cutting it into strips of adequate length and width tocover the defect. We routinely place three layers oftensor over the defect in a layered fashion and use fibringlue to secure into position.
. Next, the nasal mucosa is then repositioned to cover theflap or tensor.
. After this, the bone flaps are fixed back into position. Forthe maxilla, the prebend plates and screws are fixed intoposition. For the subfrontal area, the bone flap is strippedof any mucosa, and a diamond bur is used to bur anyresidual mucosa off the bone. The frontal sinus is crani-alized, and the bone is secured into proper position withmicroplates or titanium mesh.
. The nose is then packed with either strip gauze coatedwith bacitracin ointment or nasal tampons coated withointment.
. The patient is then kept intubated overnight, but willfrequently have a tracheotomy placed to reduce the
igure 5 The facial degloving approach with exposure of thenterior maxillary sinus wall.
igure 6 Osteotomies of the anterior, lateral and medial maxilla,
rior to fracturing. (Color version of figure is available online.) (chance of airway obstruction and prevention of a tensionpneumocephalous. If there is a concern regarding a po-tential cerebral spinal fluid (CSF) leak, we do not rou-tinely place suction drain in the scalp. This is to reducethe potential for the drain to create a suction fistula.
omplications
o prevent a CSF leak, meticulous dural reconstruction iserformed. Small dural defects are sutured shut, whereasarger defects may be repaired using an anteriorly basedericranial flap or a laterally based temporalis–pericranialap. Either flap is rotated into the defect and used to sepa-ate the dura from the sinonasal cavity. Other options in-lude using tensor fascia lata, temporalis fascia, lyophilizedura, or bovine pericardium to separate the regions. Forarge defects, a free or pedicled myocutaneous flap may besed as well. To prevent herniation of the medial orbitalontents, temporalis fascia or tensor fascia lata may be usedo line the medial wall. Gel foam (Pfizer, New York, NY) ishen placed on top of the fascia, and xeroform gauze (Co-idien, Mansfield, MA) is used to line the cavity. Bacitra-in-impregnated packing is placed to hold the grafts inosition for 1 week and then removed. A triple layer ofensor fascia lata has been used successfully and is very
igure 7 Plating the anterior maxilla, prior to mobilizing theaxilla. (Color version of figure is available online.)
igure 8 Opening the maxilla with self-retaining retractors.
Color version of figure is available online.)
etIieobma
D
Pfacnothmraw
ta
ertuatpimghappar
itnatcecrrctlm
saebtc
R
1
2
3
Fsia
43Shibuya et al Combined Subfrontal/Subcranial and Le Fort I Approach
ffective at preventing leaks or infections. Free bone graftso reconstruct the medial orbital wall are rarely performed.f used, they must be completely surrounded by vascular-zed tissue or there will be a high risk of failure. This isspecially true in a previously irradiated tissue bed. The usef alloplastic materials or titanium mesh in irradiated tissueeds or soon-to-be-radiated beds is not routinely recom-ended due to infectious complications and extrusion of
lloplastic material over time.
iscussion
anoramic exposure of the anterior skull base from cribi-orm to upper cervical spine is occasionally required fordvanced skull base tumors. Over the past decade, we haveombined two individual approaches, the subfrontal/subcra-ial approach with the Le Fort I approach, to provide pan-ramic exposure. With this combination we have been ableo surgically resect a variety of very extensive tumors. Weave also added the assistance of the nasal endoscope andicroscope to further enhance our visualization, dissection,
esection, and reconstruction. The broader exposure hasllowed the surgeon to use a two-handed surgical approach
igure 9 Placement of two Hardy retractors trans-septally,tacked on top of each other with the maxilla pushed inferiorly formproved exposure of the skull base. (Color version of figure isvailable online.)
hile operating along the anterior skull base. Additionally,
he sublabial incision and coronal incision have preventednterior facial scars and enhanced cosmetic outcome.
Reconstruction of defects along this region can be quitextensive, especially if the clivus is resected and the onlyemaining barrier between the nasopharynx/sinus region ishe dura covering the brainstem. In such instances, we havesed a large pericranial flap rotated into the defect frombove or used a triple layering of tensor fascia lata coveringhe dura. Overlying this, we rotate nasal/septal mucosarovided it is available and has not been resected. After thiss completed, gel foam impregnated with bacitracin oint-ent is placed on top of the grafts/flap; finally, xeroform
auze with strip gauze is packed against the gel foam toold everything in place. This is kept in position for 7 daysnd then removed in the office or under sedation if theatient is not cooperative or there is concern a dehiscence isresent. Radiation for malignant tumor may be necessary,nd it is very important that the wound has healed prior toadiation. We routinely wait 6 weeks prior to initiating this.
Patient postoperative care is very important to preventnfections. Patients will frequently develop very large crustshat need to be removed. Patients are instructed to flush theirasal passage/douche with saline four to six times a day forbout a week after the packing is removed. They will needo be seen on a regular basis for nasal debridement while theavity is maturing. At times the crusting can be very adher-nt to the lateral nasal walls and posterior nasopharynx/lival wall. It is not recommended to be overly vigorous inemoving the posterior wall crusts, especially if the poste-ior bony wall has been completely removed. With time therust will mature and soften and can be gently removed inhe office. Flushing with saline is an important adjunct tooosing the scabs/crust, helping to facilitate the cavity’saturation.In conclusion, we have found the combination of the
ubfrontal/subcranial approach with the Le Fort I osteotomypproach to be a very effective exposure to massive tumorsxtending along the anterior cranial base. The access haseen panoramic in nature, allowing for excellent visualiza-ion for resection and reconstruction, while providing ex-ellent cosmesis.
eferences
. Raveh J, Laedrach K, Speiser M, et al: The subcranial approach forfronto-orbital and anteroposterior skull-base tumors. Arch OtolaryngolHead Neck Surg 119:385-393, 1993
. Shibuya TY, Armstrong WB, Shohet J: Skull base surgery, in Ensley JF,Gutkind SJ, Jacobs JR, Lippman SM (eds): Head and Neck Cancers.San Diego, CA, Academic Press, 2003, pp 339-357
. Brown H: The Le Fort I maxillary osteotomy. J Maxillofac Surg 14:
112-119, 1986













![MASTER REPORT REVIEW OF GENERAL PANORAMIC OPTICAL … · and security, panoramic endoscope, machine vision, panoramic projection system, and so on [1, 2]. Panoramic lens systems can](https://img.pdfslide.us/doc/110x75/5e184f54abc03831285efb0b/master-report-review-of-general-panoramic-optical-and-security-panoramic-endoscope.jpg)