Embed Size (px)
Citation preview

Kidney International, Vol. 63 (2003), pp. 24–32
GENETIC DISORDERS – DEVELOPMENT
A novel mutation in the chloride channel gene, CLCNKB,as a cause of Gitelman and Bartter syndromes
ISRAEL ZELIKOVIC, RAYMONDE SZARGEL, ALI HAWASH, VALENTINA LABAY,1 IHAB HATIB,NADINE COHEN,2 and FARID NAKHOUL
Pediatric Nephrology Unit and Department of Nephrology, Rambam Medical Center, and Department of Molecular Genetics,Faculty of Medicine, Technion - Israel Institute of Technology, Haifa, Israel
linkage to the Cl� channel gene, CLCNKB, on chromosomeA novel mutation in the chloride channel gene, CLCNKB, as a1p36. Mutation analysis by direct sequencing revealed a novelcause of Gitelman and Bartter syndromes.homozygous missense mutation, arginine 438 to histidineBackground. Gitelman syndrome (GS) and Bartter syn-(R438H), in exon 13 of CLCNKB in all patients. A restrictiondrome (BS) are hereditary hypokalemic tubulopathies withfragment length polymorphism (RFLP) analysis has been de-distinct phenotypic features. GS has been considered a geneti-veloped to aid in genotyping of family members.cally homogeneous disorder caused by mutation in the gene
Conclusions. Our findings demonstrate intrafamilial hetero-encoding the NaCl cotransporter (TSC) of the distal convo-geneity, namely the presence of GS and CBS phenotypes, inluted tubule. In contrast, BS is caused by mutations in thea kindred with the CLCNKB R438H mutation. We concludegenes encoding either the Na-K-2Cl cotransporter (NKCC2),that GS can be caused by a mutation in a gene other thanthe K� channel (ROMK) or the Cl� channel (ClC-Kb) of the
thick ascending limb. The purpose of this study was to examine SLC12A3. The exact role of the CLCNKB R438H mutationthe clinical, biochemical and genetic characteristics of a very in the pathogenesis of the electrolyte and mineral abnormalitieslarge inbred Bedouin kindred in Northern Israel with heredi- in GS and CBS remains to be established.tary hypokalemic tubulopathy.
Methods. Twelve family members affected with hypoka-lemic tubulopathy, as well as 26 close relatives were clinically
Bartter syndrome is a group of closely related heredi-and biochemically evaluated. All study participants underwenttary tubulopathies. All variants of the syndrome sharegenetic linkage analysis. Mutation analysis was performed in
affected individuals. several clinical characteristics including renal salt wasting,Results. Evaluation of affected family members (age range hypokalemic metabolic alkalosis, hyperreninemic hyper-
3 to 36 years) revealed phenotypic features of both GS andaldosteronism with normal blood pressure and hyperpla-classic Bartter syndrome (CBS). Features typical of GS in-sia of the juxtaglomerular apparatus [1–3]. The syndromecluded late age of presentation (�15 years) in 7 patients (58%),
normal growth in 9 (75%), hypomagnesemia (SMg �0.7mmol/L) has been classified into three distinct phenotypes. First,in 5 (42%), hypermagnesiuria (FEMg �5%) in 6 (50%) and hy- antenatal Bartter syndrome, also known as hyperprosta-pocalciuria (urinary calcium/creatinine mmol/mmol �0.15) in glandin E syndrome, is the most severe form of the dis-5 (42%). Features typical of CBS included early age of presen-
ease. It is characterized by polyhydramnios, prematuretation (�1 year) in 3 (25%), polyuria/dehydration in 4 (33%),birth, life threatening episodes of salt and water loss ingrowth retardation in 3 (25%), hypercalciuria (urinary calcium/
creatinine mmol/mmol �0.55) in 4 (33%) and nephrolithiasis the neonatal period, hypokalemic alkalosis and failurein 1 (8%). Linkage analysis in affected patients excluded the to thrive, as well as hypercalciuria and early onset nephro-TSC gene, SLC12A3, as the mutated gene, but demonstrated calcinosis [1, 2]. Second, classic Bartter syndrome occurs
in infancy or early childhood. It is characterized by markedsalt wasting and hypokalemia leading to polyuria, poly-1 Current address: National Institute on Deafness and other Communi-
cation Disorders, National Institute of Health, 5 Research Court, Room dipsia, volume contraction, muscle weakness, and growth2A-02, Rockville, MD 20850, USA.
retardation. Hypercalciuria and nephrocalcinosis may2 Current address: Johnson and Johnson Pharmaceutical Research andDevelopment, 1000 Route 202, P.O. Box 300, Raritan, NJ 08869, USA. occur [2, 3]. Finally, Gitelman syndrome is characterized
by a milder clinical presentation in older children or adultsKey words: hereditary hypokalemic tubulopathy, chloride channels,
[4]. Patients may be asymptomatic and present with tran-magnesium deficiency, phenotype, linkage (genetics), sequence analy-sis, DNA, Bedouin kindred study. sient muscle weakness, abdominal pain, symptoms of
neuromuscular irritability, or unexplained hypokalemia.Received for publication May 13, 2002Hypocalciuria and hypomagnesemia are typical [3].and in revised form July 18, 2002
Accepted for publication August 28, 2002 The genetic variants of Bartter syndrome that have beenidentified include Bartter syndrome types I, II, and III, 2003 by the International Society of Nephrology
24

Zelikovic et al: Mutation in Gitelman and Bartter syndromes 25
which are caused by mutations in the genes encoding ples for biochemical analyses were collected after appro-priate informed consent was obtained from the subjectsthe luminal Na�-K�-2Cl� cotransporter, NKCC2 [5], the
luminal K� channel, ROMK [6], and the basolateral Cl� or their guardian. Serum levels of potassium, creatinine,calcium and magnesium as well as plasma bicarbonatechannel, ClC-Kb [7], respectively, of the thick ascending
limb of the loop of Henle (TAL). In contrast, Gitelman level were analyzed using standard laboratory automatedtechniques. Urine was collected for analysis of calcium,syndrome, which has been considered a genetically ho-
mogenous disorder, is caused by mutations in the gene magnesium and creatinine levels. Calcium excretion wasexpressed as the urinary calcium/creatinine ratio and mag-encoding the thiazide-sensitive NaCl cotransporter, TSC,
of the distal convoluted tubule (DCT) [8]. nesium excretion was expressed as fractional excretionof magnesium.With respect to genotype-phenotype correlation, it
has been widely accepted that patients with the NKCC2Genetic linkage analysis[5, 9, 10] or ROMK [6, 11, 12] defect usually have the se-
vere antenatal form, those with the ClC-Kb defect have Genomic DNA was extracted from peripheral bloodlymphocytes of family members by using standard meth-the classic form [7], and the TSC defect leads to Gitelman
syndrome [8, 13]. ods [19]. Linkage analysis was performed using 4-6 dinu-cleotide repeat (CA) markers from the Genethon micro-Recent data, however, have suggested that the geno-
type-phenotype correlation is not so clear-cut and that satellite panel [20] tightly linked to each of the followingthree genetic loci: Na�-K�-2Cl� cotransporter gene (SLC-phenotypic overlap may occur. Konrad et al [14] and Jeck
et al [15] reported that mutations in the ClC-Kb gene, 12A1), thiazide-sensitive NaCl cotransporter gene (SLC-12A3) and voltage-gated Cl� channel gene (CLCNKB).CLCNKB, also can cause phenotypes that overlap with
either antenatal Bartter syndrome or Gitelman syndrome. The following markers were used: D15S132, D15S1017,D15S978, D15S126, D15S121, D15S209 (for SLC12A1),Recently, an additional variant of antenatal Bartter syn-
drome associated with sensorineural deafness and renal D16S408, D16S3140, D16S3071, D16S494 (for SLC12A3)and D1S2672, D1S507, D1S2697, D1S436 (for CLCNKB).failure has been described [16]. This variant is caused by
mutations in the BSND gene, which encodes the integral Genotyping of the markers was performed by use of anon-radioactive–labeling procedure with the enhancedmembrane protein barttin [17], a �-subunit for voltage-
gated (CLC) Cl� channels [18]. chemiluminescence (ECL) system (Amersham, Braun-schweig, Germany), on the basis of a horseradish peroxi-The purpose of the current study was to shed addi-
tional light upon this phenotypic heterogeneity by exam- dase-mediated chemiluminescent reaction [21].ining the clinical, biochemical and genetic characteristics
Mutation analysis by direct sequencingof a very large inbred Bedouin kindred in Northern Israelwith hereditary hypokalemic tubulopathy, in which a Nineteen pairs of oligonucleotide primers were gener-
ated to amplify by polymerase chain reaction (PCR) allwide spectrum of phenotypic features in affected patientshas been noted. 19 exons of the CLCNKB gene according to data ob-
tained from Simon et al [7]. PCR-amplified coding re-gions as well as exon-intron boundaries were sequenced.
METHODSPCR conditions for genomic amplification were as fol-
Patients lows: Denaturation at 94�C for two minutes; 35 subse-quent amplifications cycles performed at 94�C for 30 sec-A large inbred Bedouin family residing in two close
villages in the lower Galilee was investigated. Twelve onds, 55�C for 30 seconds and 72�C for seven minutes.Amplified DNA fragments were analyzed by electropho-members of the family were identified as having hypoka-
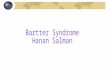
lemic tubulopathy. The pedigree of the kindred is shown resis on 2% agarose gels and purified using the QIAquickgel extraction kit. Then, purified PCR products werein Figure 1. The family has lived in the same area for
more than two centuries. The pattern of inheritance of sequenced using capillary electrophoresis on an ABIPRISM 310 automated sequencer (Perkin Elmer, War-the disease in the family is compatible with an autosomal
recessive trait. Twelve family members affected with hy- rington, UK) using the Big Dye terminator cycle se-quencing kit (Perkin Elmer). Mutation analysis was per-pokalemic tubulopathy and 26 close relatives were in-
cluded in this study. At the time of enrollment, therapy formed in ten of the twelve affected family members.of patients included various combinations of potassium
Restriction fragment length polymorphism analysissupplements, amiloride and spironolactone. No patientreceived magnesium supplementation. Restriction fragment length polymorphism (RFLP)
analysis of exon 13 of CLCNKB was performed. PCR-Phenotype analysis amplified DNA fragments containing the locus mutated
in this family were digested with the restriction enzymeClinical data were obtained from the patients, theirparents and their care providers. Blood and urine sam- Kas I and electrophoresed on a 2% agarose gel.

Fig. 1. Extended pedigree of a Bedouin family with hypokalemic tubulopathy. Filled squares (males) and circles (females) indicate affectedindividuals. Deceased individuals are indicated by a diagonal line. The autosomal recessive mode of inheritance is evident.

Zelikovic et al: Mutation in Gitelman and Bartter syndromes 27
Table 1. Clinical features in affected patients
Age Age at presentationHistory of Presence of
Patient/pedigree no. years Growth polyuria/dehydration nephrolithiasis
MZ/7 21 17 Normal No NoRZ/9 28 20 Normal No NoYZ/27 21 20 Normal No NoNZ/6 36 24 Retarded No NoMZ/10 32 20 Retarded No NoYZ/1 31 25 Normal Yes YesMZ/2 23 10 Normal Yes NoMZ/12 10 4 Normal Yes NoIZ/3 3 0.5 Retarded Yes NoMZ/5 7 0.3 Normal No NoNZ/13 3 0.1 Normal No NoBZ/14 31 29 Normal No No
Table 2. Laboratory findings in affected patients
Serum K� Plasma HCO�3 Serum Mg�� FEMg Urinary Ca/Cr
mEq/L mEq/L mmol/L % mmol/mmolPatient/pedigree no. (nl 3.5–5.3) (nl 22–26) (nl 0.7–1.2) (nl �5%) (nl 0.15–0.55)
MZ/7 3.1 27 0.65 2.6 0.08RZ/9 2.5 30 0.95 8.9 0.64YZ/27 2.3 32 0.85 4.9 0.34NZ/6 2.8 30 0.6 5.3 0.05MZ/10 3.0 28 0.8 2.5 0.17YZ/1 2.9 35 0.6 8.8 0.14MZ/2 2.7 33 0.6 4.3 0.11MZ/12 3.1 27 0.9 6.7 0.62IZ/3 3.0 28 0.8 9.0 1.70MZ/5 2.8 32 0.75 3.5 0.11NZ/13 2.9 27 0.8 7.5 0.84BZ/14 3.4 35 0.65 4.1 0.22
FEMg is fractional excretion of magnesium.
Table 3. Summary of phenotypic features in affected patientsRESULTSNumber ofClinical and biochemical characteristics
Feature patients %Tables 1 and 2 summarize the clinical features and
Features typical of Gitelman syndromelaboratory findings in the 12 affected family members. Late age of presentation (� 15 years) 7 58Age at enrollment in the study ranged from 3 years to Normal growth 9 75
Hypomagnesemia (SMg � 0.7 mmol/L) 5 4236 years (median 21 years). Age at initial presentationHypermagnesiuria (FEMg � 5%) 6 50ranged from one month to 29 years (median 17 years).Hypocalciuria [urinary Ca/Cr
There were seven males and five females. All patients (mmol/mmol) � 0.15] 5 42Features typical of classic Bartter syndromehad normal blood pressure and normal glomerular fil-
Early age of presentation (�1 year) 3 25tration rate. No patient had diarrhea during the studyPolyuria/dehydration 4 33period. The clinical and biochemical evaluation revealed Growth retardation 3 25
phenotypic features of both Gitelman syndrome (GS) Hypercalciuria [urinary Ca/Cr(mmol/mmol) � 0.55] 4 33and classic Bartter syndrome (CBS; Table 3). Features
Nephrolithiasis 1 8typical of GS included late age at presentation (�15Abbreviations are: SMg, serum magnesium; FEMg, fractional excretion of mag-years) in seven patients, normal growth in nine, hypo-
nesium; Ca/Cr, calcium, creatinine.magnesemia (SMg �0.7mmol/L) in five, hypermagnesiuria(FEMg �5%) in six and hypocalciuria (calcium/creatininemmol/mmol �0.15) in five. Features typical of CBS in-
calciuria (Table 2), typical findings in GS, four had con-cluded early age of presentation (�1 year) in three, his-comitant hypomagnesemia and hypocalciuria. However,tory of polyuria and episodes of dehydration in four,generally, the group of affected patients could not begrowth retardation in three, hypercalciuria (urinary cal-subdivided into the “GS group” and the “CBS group,”cium/creatinine mmol/mmol �0.55) in four and nephroli-because the distinctive clinical/biochemical features ofthiasis in one patient.
Of the six patients with hypomagnesemia and/or hypo- either GS or CBS did not segregate in the same patient.

Zelikovic et al: Mutation in Gitelman and Bartter syndromes28
The same patient could have features of both GS andCBS. Nevertheless, five of the affected patients (pedigreenumbers 1, 3, 6, 9 and 10) have been generally character-ized by a more severe form of the disease includinghypokalemia more resistant to therapy, frequent musclesymptoms, frequent hospitalizations, growth retardation,as well as polyuria and recurrent episodes of dehydra-tion. There were no known cases with features of ante-natal Bartter syndrome (such as polyhydraoannios, pre-mature birth, manifestations in the neonatal period) andno reported cases of unexpected mortality in this family.
Linkage analysis
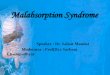
Linkage analysis using the appropriate microsatellitemarkers (Methods section) flanking the loci of the genesencoding the Na�-K�-2Cl� cotransporter (SLC12A1)and the thiazide-sensitive NaCl cotransporter (SLC12A3)did not reveal regions of homozygosity at these loci (datanot shown). Figure 2 shows the results of haplotype anal-ysis using microsatellite markers linked to the CLCNKBlocus on chromosome 1p36. For all affected individualsin the six subfamilies of this large kindred, regions ofhomozygosity by descent were observed for this genomicregion, which was then further analyzed.
Mutation analysis
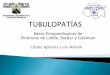
The linkage analysis data prompted a search for muta-tions in the CLCNKB gene. Mutation analysis revealeda novel homozygous missense mutation, guanine to ade-nine in exon 13 of CLCNKB (Fig. 3). The mutation sub-stitutes arginine with histidine (R438H) at amino acid438 of the channel protein. All ten affected individualstested were found to carry the same mutation, homozy-gous by decent from their related heterozygous parents.
RFLP analysis
Restriction fragment length polymorphism analysis ofPCR-amplified fragments in exon 13 of CLCNKB con-taining the mutated locus in this family was performed.The R438H mutation in the variant allele in this family re-sults in the loss of Kas I restriction enzyme site. As shownin Figure 4, the presence of the R438H mutation couldbe detected by RFLP analysis.
Fig. 2. Linkage analysis in six subfamilies of the large kindred withhypokalemic tubulopathy. Filled squares (males) and circles (females)indicate affected individuals. Each individual within the kindred is num-bered below the symbol. Haplotype analysis using microsatellite mark-ers (shown on the left side) linked to the CLCNKB locus on chromosome1p36 demonstrated cosegregation of the phenotype with the CLCNKBlocus. Regions of homozygosity are framed.

Zelikovic et al: Mutation in Gitelman and Bartter syndromes 29
Fig. 4. Restriction fragment length polymorphism (RFLP) analysis ofpolymerase chain reaction-amplified fragment in exon 13 of CLCNKBcontaining the locus mutated in this family. The numbers correspondto the number of the individual within the kindred (see Figs. 1 and 2).The cleavage site of the restriction enzyme Kas I in the wild-type 773 bpfragment is eliminated by the R438H mutation. Healthy individuals(wild-type) have two fast migrating bands, affected patients, homozy-gotes for the mutation (Mutant), have a single, slower migrating bandand heterozygotes for the mutation have a three band pattern: two,fast migrating bands and one, slow migrating band.
Gitelman syndrome and classic Bartter syndrome canbe distinguished by their characteristic phenotypic fea-tures, which include late age, benign course and presenceof hypomagnesemia and hypocalciuria in the former andearly onset, polyuria, volume contraction, failure to thriveand hypercalciuria in the latter [1–3]. Mutations in thethiazide-sensitive NaCl cotransporter gene, SLC12A3,on chromosome 16 have been found in nearly all GSpatients studied [8, 13, 22]. On the other hand, in mostpatients with CBS, the molecular defect has been identi-fied as a mutation in the voltage-gated Cl� channel gene,CLCNKB, on chromosome 3 [7, 15].
The clinical and biochemical evaluation of affectedmembers of the family reported here has revealed phe-notypic features of both GS and CBS. An additional in-teresting characteristic of this family was the fact that,generally, the features of either GS or CBS did not segre-
Fig. 3. Mutation analysis by direct sequencing in family members af-gate in the same patient. Phenotypic features of both GSfected with hypokalemic tubulopathy. The sequence in the mutation
area for healthy individuals (A), heterozygotes (B) and affected ho- and CBS could be found in the same patient. In contrast tomozygotes (C ) is listed below the histograms. The analysis reveals a the observed phenotypic heterogeneity within the family,novel homozygous missense mutation, guanine to adenine, in exon 13 of
all affected family members were found to have the sameCLCNKB. The mutation substitutes arginine with histidine (R438H)at amino acid 438 of the channel protein. genetic defect, a missense R438H mutation in exon 13
of the voltage-gated Cl� channel gene, CLCNKB.Recent studies have provided evidence for phenotypic
overlap between the various forms of Bartter syndromeDISCUSSIONincluding CBS and GS. Bettinelli et al, who studied 34This study describes the clinical, biochemical and ge-children with primary hypokalemic tubulopathy from 15netic characteristics of the largest consanguineous kin-centers in Central Europe, reported failure to thrive indred affected with hereditary hypokalemic tubulopathy20% of the patients with GS phenotype and found hypo-reported to date. This study not only provides evidencemagnesemia in one third of the children with BS pheno-that the genotype-phenotype correlation in Bartter/Git-type [23]. Thurman reported the concomitant occurrenceelman syndrome is blurred, but also provides a uniqueof Gitelman and Bartter syndromes in the same familyopportunity to demonstrate the phenotypic variability of[24]. The author described two siblings presenting withthis syndrome in members of the same family bearing the
same genetic defect. normotensive hypokalemic alkalosis. One child had hy-

Zelikovic et al: Mutation in Gitelman and Bartter syndromes30
pomagnesemia and hypocalciuria whereas the other had curs primarily via the luminal, thiazide-sensitive NaClcotransporter (TSC) [3, 25, 26]. Chloride exit to bloodnormal serum magnesium and urinary calcium excretion.
These two reports, however, did not include a genetic is mediated via basolateral Cl� channels. The main path-way of Cl� exit from cell to blood in the distal tubule ap-analysis of affected patients. Simon et al, in their first
report on CLCNKB mutation in 17 kindreds with Bartter pears to be ClC-Kb channels, which are known to beexpressed at the basolateral membrane of the TAL andsyndrome type III, noted the marked variation in severity
of clinical features of affected patients ranging from pro- the DCT [27–29]. Hence, a defect in the activity ofClC-Kb is expected to cause a reduction in NaCl reab-found hypokalemia and severe volume depletion to mild
disease presenting at the second decade of life [7]. Kon- sorption in these tubule segments. Nevertheless, alterna-tive routes for Cl� transport such as KCl cotransporter,rad and coworkers, who screened children with Bartter’s
syndrome from 30 families for CLCNKB mutations, CFTR or the voltage-gated Cl� channel CLC5 [30–32],may participate in basolateral Cl� exit. Of great interestshowed that mutations in this gene most commonly cause
the classic Bartter syndrome [15]. Nevertheless, in a mi- is the recent identification of barttin, a Cl� channel�-subunit that colocalizes with the channel in basolateralnority of patients, various mutations in CLCNKB were
found to cause phenotypes that overlapped with either membranes of the renal tubule and inner ear epithelium[17, 18]. Barttin appears to mediate basolateral recyclingantenatal Bartter syndrome or Gitelman syndrome. Re-
cently, Jeck et al reported three patients whose clinical of Cl� [18].The summary of these interrelated transport processescourse was characterized by gradual transition from CBS
to GS phenotype, and who were found to carry three leads to the hypothesis that variation in expression and/orfunction of any one of the channels or transporters par-different mutations in the CLCNKB gene [15].
The findings of these studies demonstrating the pheno- ticipating in Cl� transport in the TAL and the DCT maymodify to variable degrees the derangement in ClC-Kbtypic variability associated with CLCNKB mutations could
be potentially attributed to the nature of the genetic de- function, thereby influencing the disease phenotype. Sucha modifying effect could occur at the cellular/regulatoryfect. For example, differences in the type and/or location
of the mutation within the gene could result in differ- level, whereby one or more transport mechanisms are re-cruited to compensate for impaired ClC-Kb function or,ences in the magnitude of the loss of function of the Cl�
channel, thereby resulting in differences in clinical pic- alternatively, may be determined at the level of modifiergenes. Our linkage analysis studies have provided no evi-tures. Alternatively, age-related alterations in the activ-
ity of the defective Cl� channel could lead to a gradual dence that the phenotypic variability in our family wasrelated to a defect in the Na�-K�-2Cl� cotransporter gene,transition from one phenotype to the other, as demon-
strated by Jeck et al in their longitudinal observation of SLC12A1 or the thiazide-sensitive NaCl cotransportergene, SLC12A3. Obviously, further genetic analysis ofthree patients [15]. These considerations, however, do not
apply to the family reported here, in which the phenotypic the family, in an effort to identify such a modifier gene,would be of great importance. Such a study also shoulddifferences have been observed in a cross-sectional study
in patients bearing the same missense homozygous muta- include a careful analysis of genetic polymorphism invarious loci relevant to renal tubular ion transport.tion presumably originating in a common ancestor.
How could a specific genetic defect in CLCNKB result Hypomagnesemia and/or hypocalciuria, both typicalfindings in Gitelman syndrome [3, 33], occurred in sixin such a wide range of clinical phenotypes within the
same family? Examination of the nature of Cl� transport (50%) of the affected family members. Of these, four hadconcomitant hypomagnesemia and hypocalciuria. Thein the distal parts of the renal tubule potentially could
provide an explanation for this phenomenon. Trans- hypomagnesemia was mild as previously noted in pa-tients with CLCNKB mutations who had this laboratoryepithelial Cl� transport in the TAL is a complex process
that involves the coordinated interplay between the lu- abnormality. The exact mechanisms underlying the hy-pocalciuria and hypomagnesemia in Gitelman syndromeminal, bumetanide-sensitive Na�-K�-2Cl� cotransporter
(NKCC2), the luminal, adenosine 5�-triphosphate (ATP)- are unclear. It has been hypothesized that the loss offunction mutation in TSC causes hypocalciuria by theregulated, inwardly-rectifying K� channel (ROMK), the
basolateral Cl� channel (ClC-Kb), as well as other co- same mechanism as thiazide diuretics. According to thishypothesis, impaired Na� reabsorption across the lumi-transporters and channels [3, 25, 26]. Chloride is re-
absorbed across the luminal membrane of the TAL cell nal membrane of the distal convoluted tubular cell, cou-pled with continued exit of intracellular Cl� throughby the activity of NKCC2. This cotransporter is driven
by the low intracellular Na� and Cl� concentrations gen- basolateral Cl� channels, causes the cell to hyperpolar-ize. This, in turn, stimulates entry of calcium into theerated by the basolateral Na�-K�-ATPase and ClC-Kb,
respectively. In addition, ROMK enables the functioning cell via luminal voltage-activated Ca�� channels [34]. Inaddition, the lowering of intracellular Na� concentrationof NKCC2 by recycling K� back to the renal tubular
lumen. Cl� transport in the distal convoluted tubule oc- facilitates Ca�� exit via basolateral Na�/Ca�� exchanger.

Zelikovic et al: Mutation in Gitelman and Bartter syndromes 31
characterized by hypokalemia and hypomagnesaemia. Trans AssocThe mechanisms whereby a CLCNKB mutation decreasesAm Physicians 79:221–235, 1966
Ca�� excretion in the urine, as observed in our patients, 5. Simon DB, Karet FE, Hamdan JM, et al: Bartter’s syndrome:Hypokalemic alkalosis with hypercalciuria, is caused by muta-are unclear. It is possible that impaired Cl� exit at thetions in the Na-K-2C1 cotransporter NKCC2. Nat Genet 13:183–basolateral membrane of the DCT and subsequent intra-188, 1996
cellular accumulation of Cl� directly or indirectly influ- 6. Simon DB, Karet FE, Rodriguez-Soriano J, et al: Genetic hetero-geneity of Bartter’s syndrome revealed by mutations in the K�ence DCT cell function, thereby increasing Ca�� reab-channel, ROMK. Nat Genet 14:152–156, 1996sorption in this tubule segment. The reasons for renal
7. Simon DB, Bindra RS, Mansfield TA, et al: Mutations in theMg�� wasting and hypomagnesemia in Gitelman syn- chloride channel gene, CLCNKB, cause Bartter’s syndrome type
III. Nat Genet 17:171–178, 1997drome, in general, and the role of the ClC-Kb defect8. Simon DB, Nelson-Williams C, Bia MJ, et al: Gitelman’s variantin the pathogenesis of hypomagnesemia, in particular,
of Bartter’s syndrome, inherited hypokalemic alkalosis, is causedremain to be elucidated. Whatever these mechanisms by mutations in the thiazide-sensitive Na-C1 cotransporter. Nat
Genet 12:24–30, 1996might be, it appears that in some patients with a Cl�
9. Vargas-Poussou R, Feldman D, Vollmer M, et al: Novel mo-channel defect, as observed in our family, specific mecha-lecular variants of the Na-K-2C1 cotransporter gene are responsi-
nisms are activated that compensate for the derangement ble for antenatal Bartter syndrome. Am J Hum Genet 62:1332–1340, 1998in mineral transport and prevent the development of
10. Kurtz CL, Karolyi L, Seyberth HW, et al: A common NKCC2hypomagnesemia and hypocalciuria. Moreover, somemutation in Costa Rican Bartter’s syndrome patients: Evidence
patients even develop hypercalciuria. The exact nature for a founder effect. J Am Soc Nephrol 8:1706–1711, 199711. International Collaborative Study Group for Bartter-likeof these mechanisms and the level of their operation is
Syndromes: Mutations in the gene encoding the inwardly rectifyinga subject for further investigation.renal potassium channel, ROMK, cause the antenatal variant of
In summary, our findings demonstrate intrafamilial het- Bartter syndrome: Evidence for genetic heterogeneity. Hum MolGenet 6:17–26, 1997erogeneity, namely the presence of Gitelman syndrome
12. Vollmer M, Koehrer M, Topaloglu R, et al: Two novel mutationsand classic Bartter syndrome phenotypes in a kindredof the gene for K 1.1 (ROMK) in neonatal Bartter syndrome.
with the CLCNKB R438H mutation. We conclude that Pediatr Nephrol 12:69–71, 199813. Lemmink HH, Knoers NVAM, Karolyi L, et al: Novel mutationsGS phenotype can be caused by a mutation in a gene other
in the thiazide-sensitive NaC1 cotransporter gene in patients withthan the TSC gene, SLC12A3. The mechanisms wherebyGitelman syndrome. Kidney Int 54:720–730, 1998
the same genetic defect results in such a variability of 14. Konrad M, Vollmer M, Lemmink HH, et al: Mutations in thechloride channel gene CLCNKB as a cause of classic Bartter syn-clinical features remain to be established. The exact roledrome. J Am Soc Nephrol 11:1449–1459, 2000of the CLCNKB R438H mutation in the pathogenesis 15. Jeck N, Konrad M, Peters M, et al: Mutations in the chloride
of the electrolyte and mineral abnormalities in Gitelman channel gene, CLCNKB, leading to a mixed Bartter-Gitelmanphenotype. Pediatr Res 48:754–758, 2000syndrome and Bartter syndrome is a subject for future
16. Brennan TMH, Landau D, Shalev S, et al: Linkage of infantileresearch that may include site-directed mutagenesis and Bartter syndrome with sensorineural deafness to chromosome 1p.functional studies in heterologous expression systems, Am J Hum Genet 62:355–361, 1998
17. Birkenhager R, Otto E, Schurmann MJ, et al: Mutation of BSNDas well as the use of transgenic animal models.causes Bartter syndrome with sensorineural deafness and kidneyfailure. Nat Genet 29:310–314, 2001
18. Estevez R, Boettger TH, Stein V, et al: Barttin is a C1� channel�-subunit crucial for renal C1� reabsorption and inner ear K�
ACKNOWLEDGMENTSsecretion. Nature 414:558–561, 2001
19. Sambrook J, Fritsch E, Maniatis T: Molecular Cloning: A Labora-Parts of this work were presented at the ASN/ISN World Congresstory Manual (vol 1–3). Cold Spring Harbor, Cold Spring Harborof Nephrology in San Francisco, California, USA, October 2001, andLaboratory Press, 1989were published in abstract form (J Am Soc Nephrol 12:561A, 2001).
20. Dib C, Faure S, Fizames C, et al: A comprehensive genetic mapWe thank Dr. Karl Skorecki for helpful suggestions, and Mrs. Judiof the human genome based on 5,264 microsatellites. Nature 380:Fichman and Ms. Hagar Shafrir for their expert secretarial assistance.152–154, 1996
21. Gyapay G, Ginot F, Nguyen S, et al: Genotyping procedures inReprint requests to Israel Zelikovic, M.D., Pediatric Nephrology Unit,linkage mapping. Methods 9:91–97, 1996Rambam Medical Center, P.O. Box 9602, Haifa 31096, Israel.
22. Monkawa T, Kurihara I, Kobayashi K, et al: Novel mutationsE-mail: [email protected] thiazide-sensitive Na-C1 cotransporter gene of patients withGitelman’s syndrome. J Am Soc Nephrol 11:65–70, 2000
23. Bettinelli A, Bianchetti MG, Girardin E, et al: Use of calciumexcretion values to distinguish two forms of primary renal tubularREFERENCEShypokalemic alkalosis: Bartter and Gitelman syndromes. J Pediatr
1. Guay-Woodford LM: Bartter syndrome: Unraveling the patho- 120:38–43, 1992physiologic enigma. Am J Med 105:151–161, 1998 24. Turman MA: Concomitant occurrence of Gitelman and Bartter
2. Rodriguez-Soriano J: Bartter and related syndromes: The puzzle syndromes in the same family? Pediatr Nephrol 12:23–25, 1998is almost solved. Pediatr Nephrol 12:315–327, 1998 25. Simon DB, Lifton RP: Mutations in Na(K)C1 transporters in
3. Zelikovic I: Molecular pathophysiology of tubular transport disor- Gitelman’s and Bartter’s syndrome. Curr Opin Cell Biol 10:450–ders. Pediatr Nephrol 16:919–935, 2001 454, 1998
26. Scheinman SJ, Guay-Woodford LM, Thakker RV, et al: Genetic4. Gitelman HJ, Graham JB, Welt LG: A new familial disorder

Zelikovic et al: Mutation in Gitelman and Bartter syndromes32
disorders of renal electrolyte transport. N Engl J Med 340:1177– tion of KCC3 and KCC4, new members of the cation-chloridecotransporter gene family. J Biol Chem 274:16355–16362, 19991187, 1999
27. Vandewalle A, Cluzeaud F, Bens M, et al: Localization and 31. Luyckx VA, Goda FO, Mount DB, et al: Intrarenal and subcellularlocalization of rat CLC5. Am J Physiol 275:F761–F769, 1998induction by dehydration of CIC-K chloride channels in the rat
kidney. Am J Physiol 272:F678–F688, 1997 32. Devuyst O, Burrow CR, Schwiebert EM, et al: Developmentalregulation of CFTR expression during human nephrogenesis. Am28. Uchida SH: In vivo role of CLC chloride channels in the kidney.
Am J Physiol 279:F802–F808, 2000 J Physiol 271:F723–F735, 199633. Cole DEC, Quamme GA: Inherited disorders of renal magnesium29. Kobayashi K, Uchida SH, Mizutani SH, et al: Intrarenal and
cellular localization of CLC-K2 protein in the mouse kidney. J Am handling. J Am Soc Nephrol 11:1937–1947, 200034. Friedman PA: Codependence of renal calcium and sodium trans-Soc Nephrol 12:1327–1334, 2001
30. Mount DB, Mercado A, Song L, et al: Cloning and characteriza- port. Annu Rev Physiol 60:179–197, 1998