Embed Size (px)
Citation preview

A Novel Methodology to Evaluate Continuous Glucose Monitoring Accuracy and Clinical Representation of Glucose Exposure and Variability
1. AbstractSMBG combined with Ambulatory Glucose Profile (AGP) analysis was used to determine whether time lag and difference between glucose in blood and inter-stitial fluid (ISF) could be ameliorated. For 8 days subjects with type 1 diabetes used Guardian RT® (RT) for CGM and OneTouch Ultra® (OT) for SMBG. On the9th day subjects were monitored for 8 hours by 15-minute interval capillary blood samples analyzed simultaneously by YSI and OT while continuing RT (Figure1). Two high carbohydrate meals were given to induce hyperglycemia followed by rapid acting insulin to re-establish euglycemia. Eight subjects completed thestudy. YSI vs. OT showed overlapping paths, -0.5±1.9 min lag, and 4.8% mean relative absolute difference (RAD); YSI vs. RT produced variable lag, 21.9±4.7 min(range 17-32 min) and 19.3% RAD (exaggerated during glucose instability). Clarke Error Grid (CGM vs. YSI) showed 61% clinically accurate (A), 36% benign (B)and 3% inaccurate (D) readings. To determine the effect of time lag on daily glucose profiles, AGPs were produced for each subject. By collapsing 8 days ofCGM (averaging 2300±300) into a modal day and depicting the data as 5 algorithmically smoothed curves the effect of time lag on insulin administration (Figure2) was detected. Postprandial peaks discernible on the AGP would have occurred on average 22 minutes earlier than actually shown.The persistent and vari-able time and value differences between SMBG and ISF (as measured by RT) present a clinical conundrum: do the benefits of CGM outweigh the risks? Webelieve that the risks may be reduced if SMBG data are used to identify the error and if adjustments are incorporated in such clinical decision-making toolsas AGP analysis.
ROGER S. MAZZE 1,2 | ELLIE STROCK 1 | PHILIP STOUT 3 | JOEL RACCHINI 3 | DAVID WESLEY 1 | SARAH BORGMAN 1
1 INTERNATIONAL DIABETES CENTER, 2 UNIVERSITY OF MINNESOTA MEDICAL SCHOOL, 3 LIFESCAN, INC, MINNEAPOLIS, MN
The purposes of this investigator initiated project are to: 1) assess two different glucose measuring methodologies to evalu-ate their ability to detect patterns of significant glycemic excursions: Medtronic Guardian RT Continuous Glucose MonitoringSystem (GRT) and the DexCom Glucose Monitoring System (DEX); and, 2) obtain sufficient longitudinal data to assess the timelag, value difference and rate of change of GRT and DEX when blood glucose rapidly changes.
Continuous Glucose Monitoring: Sensor, Transmitter, Receiver and PC
Area Under the Curve (AUC) analysis determines the overall glucose exposureunder a plot measuring glucose during a time period. Using the trapezoidalmethod, the study period is divided into time intervals to correspond with eachglucose determination. The segment area is calculated by multiplying theaverage concentration (glucose value) by the segment width (15 minutes). Thetotal AUC is the sum of the hourly average concentration. The example belowcompares the AUC for YSI determinations (reference) with the AUC forGuardian RT for a single subject.
Commonly used characteristics to measure discrepancies between YSIblood glucose and ISF glucose are: (1) Rates of change-- the ascendingand descending slope in the curves measured over a 30-60 minute peri-od of relatively constant change; (2) Lag-- the difference in time when thetest curve is shifted to minimize error relative to the reference curve; (3)Mean and Median Absolute Relative Differences reflect the discrepancybetween reference and device paired measures.
Bland-Altman analysis determines whether one device can replace another. Inthe example below, using study data, the question is whether the OneTouchUltra® meter can replace the “gold standard” YSI blood glucose analyzer. Themean difference between devices for was 5 mg/dL with the 95% confidenceinterval ±30 mg/dL.
6. FindingsExample of the AGP for one subject using the DEX for 8 days.
The AGP analysis is automatically produced upon downloading receiver data.
Note: Area under the curve (AUC) is reported as mg 24 hr/dL and normalized (Norm) to an hourly value (mg-hr/dL)
Total Number of Sensor ReadingsAverage Sensor Readings Per DayMean (mg/dL)Median (mg/dL)IQR (mg/dL)10th Percentile (mg/dL)90th Percentile% Values <70% Values >180Rate of Change In Median Curve (mg/dL/hr)Minimum Value In Median Curve (mg/dL/hr)Time At Minimum Value In Median Curve (hr:min)Maximum Value In Median Curve (hr:min)Time At Maximum Value In Median Curve (hr:min)
MEAN STD MEAN STD475.67 36.51 438.83 69.75158.56 12.17 146.28 23.25177.01 39.64 194.37 53.51176.29 43.49 200.36 57.68
46.99 9.96 68.76 33.62143.60 39.67 150.67 60.68210.78 43.13 245.79 61.60
3.10 3.97 5.59 7.3444.78 26.92 46.50 27.7822.11 8.01 30.98 14.15
114.09 47.79 118.60 67.6610:20:00 6:25:54 14:20:00 9:23:23
264.91 43.24 319.28 65.7812:20:00 9:06:31 10:00:00 8:07:04
Six subjects simultaneously used the GRT and DEX devices for 48 hours.The data summarized below are based on AGP analysis which uses all raw data for calculations.
GRT DEX
7. ConclusionsWhile the study sample was not meant to derive statistical significance we conclude that:
• In terms of accuracy (time lag, value difference, rate of change and glucose exposure) the devices vary between each other and the YSI reference
• In terms of reliability, both devices lost measurements due to calibration, sensor failure anduser error
• In terms of possible clinical errors (Clarke Analysis), while both devices had over 90% valueswithin “clinically accurate” or “benign” zones, GRT had 7% of values in the “failure to treat” zone
When AGP analysis was applied, we found that despite device limitations the use of the GuardianRT and the DexCom STS for overall assessment of glycemic control is promising. During periodsof simultaneous use, the clinical differences between devices were ameliorated through applica-tion of AGP analysis. However, we do not believe that these devices, in their current state of tech-nology should be used for real-time clinical decision-making due to their variability in clinicalaccuracy and reliability.
2. IntroductionMuch of our ability to characterize blood glucose control, whether for diagnosis or treatment, is due to advances in ambulatory blood glucose measure-ment. With the advent of direct blood glucose measurements with the aid of reflectance meters (SMBG) as the means for detecting and managing glycemiccontrol, it became more feasible to characterize blood glucose levels and associate these data with both therapy and outcome. This has been furthered byadvanced computer-based technologies that provide a means of aggregating and reporting accurate and reliable self-monitored blood glucose data. Thesedata, along with independent assays for glycosylated hemoglobin, provide more precise evidence of the relationship between tight glycemic control anddiabetes-related complications. Due to our expanded understanding of the nature of glycemic control and its association with complications, we now havea potential means of improving clinical decision-making. The recent introduction of electro-chemical based glucose meters, as well as continuous bloodglucose monitoring potentially improve the ability to more precisely diagnose and treat diabetes. However, this is contingent upon the development of ameans to accurately characterize glycemic excursions and to link this characterization to clinical decision-making.
3. Technology
5. Methods of Analysis
Ambulatory Glucose Profile (AGP)AGP Production
All glucose data are collapsed into a single display and plotted according to time. Thepurpose is to determine whether there is an underlying pattern to the glucose alter-ations. The accompanying modal day displayshows some outlier high glucose values. Sincethese occur infrequently, they do not constitutepart of an overall pattern of elevated postprandi-al glucose excursions. Patterns are detected inthe modal day by subjecting the data to a seriesof smoothing algorithms. The data are firstaligned according to time of day. Next a frequency distribution divides the data into 5percentiles. The data for each percentile are then reconnected by a best fit curve. Thefive time series curves are algorithmically smoothed to represent the 10th, 25th, 50th,75th and 90th percentile glucose values and graphed by time without regard to date. Thecurves help identify underlying patterns as well as measure glucose EXPOSURE, STA-BILITY and VARIABILITY.
Depicted above is a comparison of two devices worn at the same time by one subject while undergoing YSI blood glucose measurements at 15 minute intervals. At the sametime of each measurement the glucose values produced by the two CGM devices were recorded. On the left panel, GRT device (green) is compared with the YSI (red), whileon the right panel DEX (blue) is compared with the same YSI (red) curve. The yellow areas represent the periods of time when the CGM device glucose value was lower thanthe reference and the green and blue areas depict the periods when the CGM device values were higher than the reference.
-hr
Aggregate data for glucose exposure, rate ofchange, absolute differences, lag time and meandifferences for GRT (N=16) and DEX (N=8)
PART A: Accuracy and Clinical Error Analysis During Laboratory Study
Bland-Altman Plot
PART B: Laboratory Comparison Using GRT and DEX Simultaneously
Bland-Altman analysisdetermined that the meandifference between deviceswas 26 mg/dL with the 95%confidence interval 197mg/dL.
0
50
100
150
200
250
300
350
400
450
12:0
0 A
M
2:00
AM
4:00
AM
6:00
AM
8:00
AM
10:0
0 A
M
12:0
0 P
M
2:00
PM
4:00
PM
6:00
PM
8:00
PM
10:0
0 P
M
12:0
0 A
M
PART C: CGM Employing AGP Analysis
Example from the same subject (above) using the GRT and DEX simultaneously for 48 hours
GRT DEX
N ABOVE WITHIN BELOW MEAN SD MAX MIN AUC Waking Sleeping376 140 70 66.5 30.6 2.9 211.3 105.6 401.0 39.0 5593.5 4247.5 1346
10th 25th 50th 75th 90th IQ Range AUC Norm AUC Fast202.0 212.0 232.7 253.6 264.7 41.6 3193.5 3793.5
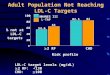
TARGETS
Acknowledgements: IDC Research staff and colleagues. Supported by an investigator-initiated grant from Lifescan, Inc.
4. Design, Procedures and SubjectsDesign Procedures and Subjects
• Eight days of continuous glucose monitoring with GRT or DEX• Self-monitored capillary glucose using OneTouch Ultra™ (LifeScan) for
all calibrations and SMBG• All CGM sensors inserted by study nurse• No change in diabetes therapy• 8 hour laboratory study with fixed meals and insulin adjustments
Subject Age Gender DM type duration (y) BMI Diabetes Meds1 62 M 1 43 29.6 Novolog (insulin pump)
2 57 F 1 49 31.7 Humalog and Lantus and NPH
3 46 F 1 7 25.3 Novolog and Lantus and metformin
4 48 F 1 36 28.9 Humalog (insulin pump)
5 31 F 1 5 22.9 Novolog and Lantus
6 41 M 1 2 22.2 Novolog and Lantus
7 53 F 1 42 29.6 Novolog (insulin pump)
8 54 F 1 21 20.8 Humalog and Lantus
9 64 M 2 11 28.1 Humalog (insulin pump); metformin
10 42 M 1 39 31.8 Novolog (insulin pump)
11 62 F 2 16 51.5 Humalog, Lantus, Metformin
12 39 F 1 21 21.6 Novolog and Lantus
13 25 F 1 12 24.4 Humalog and Lantus
14 63 F 2 15 42.6 Novolog, Lantus, Metformin, Actos
15 54 F 2 11 27.4 Novolog and Lantus
16 61 F 2 10 32.4 Humalog, Lantus, Metformin
mg/dL
mg/dL
mg/dL




















![Clinical aspects of common mineral disorders. hypocalcemia Normal [Ca2+] total = 8.5-10.5 mg/dl (2.12-2.62 mmol/L) Normal [Ca2+] ion = 4.65-5.25 mg/dL](https://img.pdfslide.us/doc/110x75/56649d1f5503460f949f3ab2/clinical-aspects-of-common-mineral-disorders-hypocalcemia-normal-ca2-total.jpg)