Embed Size (px)
Citation preview

Therapeutics, Targets, and Chemical Biology
A Novel Bispecific Antibody Targeting EGFR andcMet Is Effective against EGFR Inhibitor–ResistantLung TumorsSheri L. Moores1, Mark L. Chiu1, Barbara S. Bushey1, Kristen Chevalier1, Leopoldo Luistro1,Keri Dorn1, Randall J. Brezski1, Peter Haytko1, Thomas Kelly1, Sheng-Jiun Wu1,Pauline L. Martin1, Joost Neijssen2, Paul W.H.I. Parren2,3, Janine Schuurman2,Ricardo M. Attar1, Sylvie Laquerre1, Matthew V. Lorenzi1, and G. Mark Anderson1
Abstract
Non–small cell lung cancers (NSCLC) with activating EGFRmutations become resistant to tyrosine kinase inhibitors (TKI),often through second-site mutations in EGFR (T790M) and/oractivation of the cMet pathway. We engineered a bispecificEGFR-cMet antibody (JNJ-61186372) with multiple mechan-isms of action to inhibit primary/secondary EGFR mutationsand the cMet pathway. JNJ-61186372 blocked ligand-inducedphosphorylation of EGFR and cMet and inhibited phospho-ERK and phospho-AKT more potently than the combinationof single receptor–binding antibodies. In NSCLC tumor mod-els driven by EGFR and/or cMet, JNJ-61186372 treatment
resulted in tumor regression through inhibition of signaling/receptor downmodulation and Fc-driven effector interactions.Complete and durable regression of human lung xenografttumors was observed with the combination of JNJ-61186372and a third-generation EGFR TKI. Interestingly, treatmentof cynomolgus monkeys with JNJ-61186372 resulted in nomajor toxicities, including absence of skin rash observedwith other EGFR-directed agents. These results highlight thedifferentiated potential of JNJ-61186372 to inhibit the spec-trum of mutations driving EGFR TKI resistance in NSCLC.Cancer Res; 76(13); 3942–53. �2016 AACR.
IntroductionNon–small cell lung cancer (NSCLC) is frequently driven by
activating mutations in the kinase domain of EGFR, occurringmost commonly as in-frame deletions in exon 19 and L858R exon21 mutations. Most patients initially respond to first-generationEGFR tyrosine kinase inhibitors (TKI), such as gefitinib anderlotinib, but the clinical benefits are not durable. Drug resistancelimits the response to a mean duration of <1 year (1, 2). Inaddition to the T790M secondary mutation in EGFR (�50% ofresistant cases; refs. 1, 3–6) that reduces potency of reversible TKIs(7), resistant tumors may also develop activation of the cMetpathway, throughMET gene amplification, increased cMet expres-sion, and/or increased expression of the cMet ligand, hepatocytegrowth factor (HGF; refs. 5, 6, 8, 9). Stimulation of the cMetpathway provides an alternatemechanism to bypass the TKI block
of EGFR and facilitate the survival of cancer cells. These twomechanisms can also occur simultaneously in EGFR TKI–resistantNSCLC patients (3, 6, 10, 11).
Because of the signaling cross-talk between EGFR and cMet,inhibition of both receptors in combination may limit compen-satory pathway activation and improve overall efficacy. A novelbispecific antibody platform was used to produce JNJ-61186372,an antibody that binds EGFR with one Fab arm and cMet with theother Fab arm (12, 13). We have optimized JNJ-61186372 toengage multiple mechanisms of action. First, we demonstrateddual inhibition of both EGFR and cMet signaling by blockingligand-induced activation and by inducing receptor degradation.In addition, high levels of EGFR and cMet on the surface of tumorcells allow for targeting of these cells for destruction by immuneeffector cells through Fc-dependent effector mechanisms, such asantibody-dependent cellular cytotoxicity (ADCC). JNJ-61186372is produced by an engineered Chinese hamster ovary (CHO) cellline defective for protein fucosylation. The human FcgRIIIa, criticalfor ADCC, binds antibodies with low-level core fucosylationmoretightly and consequentlymediatesmorepotent andeffectiveADCCkilling of cancer cells (14). Thus, the low-level core fucosylation inthe JNJ-61186372 molecule translates to an enhanced level ofADCCactivity comparedwith the same fully fucosylatedmolecule.
JNJ-61186372 was demonstrated to employ multiple mechan-isms to inhibit tumors with primary EGFR-activating mutations,tumors with the T790M second-site resistance mutation in EGFR,and tumorswith activation of the cMet pathway. Furthermore, thecombination of JNJ-61186372 and a third-generation EGFR TKI(AZD9291) resulted in complete and durable regression oftumors. Interestingly, treatment of cynomolgus monkeys with
1Janssen Research and Development, Spring House, Pennsylvania.2Genmab, Utrecht, the Netherlands. 3Department of Immunohema-tology and Blood Transfusion, Leiden University Medical Center, Lei-den, the Netherlands.
Note: Supplementary data for this article are available at Cancer ResearchOnline (http://cancerres.aacrjournals.org/).
S.L. Moores and M.L. Chiu contributed equally to this article.
Corresponding Author: Sheri L. Moores, Janssen Research & Development,1400McKean Road, Spring House, PO Box 776, PA 19477. Phone: 215-628-5740;Fax: 215-540-4763; E-mail: [email protected]
doi: 10.1158/0008-5472.CAN-15-2833
�2016 American Association for Cancer Research.
CancerResearch
Cancer Res; 76(13) July 1, 20163942
on May 11, 2020. © 2016 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Published OnlineFirst May 23, 2016; DOI: 10.1158/0008-5472.CAN-15-2833

JNJ-61186372 resulted in no toxicities, including absence of skinrash observed with other EGFR-directed agents. This profile ofpreclinical data supports the development of JNJ-61186372 inpatients with lung cancer and other malignancies associated withaberrant EGFR and cMet signaling.
Materials and MethodsPreparation of parental mAbs
The EGFR arm of JNJ-61186372 is derived from zalutumumabthat has a conformational epitope on EGFR domain III, whichoverlaps with the EGF ligand–binding site (15) but is differentfrom the epitopes of cetuximab (16) and panitumumab (17). ThecMet-binding arm of JNJ-61186372 has an epitope that blocksHGF ligand binding but is distinct from the onartuzumab epitope(18). Parental mAbs used to generate JNJ-61186372 were pre-pared from CHO cell lines that generate mAbs with low levels ofcore fucosylation. Antibody expression and purification isdescribed in detail elsewhere (19).
Controlled Fab-arm exchange to generate bispecific AbsBispecific human IgG1Abswereproduced from the twopurified
bivalent parental antibodies, each with the respective single com-plementary mutation: K409R or F405L (12). Controlled Fab-armexchange (cFAE)was performed as described previously (12), witha 5% excess of anti-EGFR-F405L. Similar conditions for prepara-tion and characterizationswere used to generate the normal fucose(EGFR-cMet) and JNJ-61186372-IgG2s Abs, and monovalentEGFR and cMet Abs. All bispecific antibodies were purified usinghydrophobic interaction chromatography. The EGFRmonovalentantibody consists of an EGFR-binding arm and a nonbinding arm(either anti-HIV-gp120 or anti-RSV-F, which did not bind the celllines used); the cMet monovalent antibody consists of a cMet-binding arm and similar aforementioned nonbinding arm.
Competitive ligand bindingEGFR-ECD-Fc (R&D Systems; 200 ng/well) was coated onHigh
Bind Plate [Meso Scale Discovery (MSD)] for 2 hours (all stepsperformed at room temperature). MSD Blocker A buffer (5%, 150mL/well)was added and incubated for 2hours. Plateswerewashed3 times with 0.1 mol/L HEPES buffer, pH 7.4, then the mixture ofthe MSD fluorescence dye–labeled Hu-EGF with different com-petitors was added. Labeled EGF (50 nmol/L) was incubated withantibodies (1 nmol/L–4 mmol/L), then added to wells (25 mLmixture). After 2 hours, plates were washed as above. MSD ReadBuffer T was diluted with distilled water (4-fold), dispensed(150 mL/well), and analyzed with a SECTOR Imager 6000.
PolyHistidine mAb050 (R&D Systems; 50 ng/well) was coatedon MSDHigh Bind Plate for 2 hours. Blocking and washing stepswere as above, followed by capturing 30 mL (10 mg/mL) of cMet-ECD-Fc (R&D Systems). After 1 hour, plates were washed asabove. After the mixture of biotinylated HGF with differentantibodies was added to plates, labeled HGF (10 nmol/L) wasincubatedwith antibodies (0.001–2mmol/L), then added towells(25 mL mixture). After 1-hour incubation, plates were washedand then MSD fluorescence dye–labeled streptavidin, 25 mL(10 nmol/L), was added to each well and incubated for 1 hour.Plates were washed, read, and analyzed as above.
Cell culture and HGF-engineered cell lineFor these studies, 7 NSCLC tumor cell lines (NCI-H292,
HCC827, NCI-H1975, NCI-H3255, HCC4006, NCI-H820, and
NCI-H1993) were selected to reflect patient diversity in themutational status of EGFR and gene copy number of MET. Thetumor cell lines were obtained (2011–2013) from the NCI(Bethesda, MD; H3255) or ATCC (all others). Cell lines wereauthenticated using short tandem repeat assay and either usedimmediately or banked, with all experiments occurring within 2months of resuscitation. The mutations in each cell line wereconfirmed using a custom somatic mutation array (SABios-ciences). Cellswere cultured in 150-cm2 tissue cultureflasks understandard culture conditions (37�C, 5% CO2, 95% humidity) andgrown in RPMI1640 medium þ GlutaMAX þ 25 mmol/L HEPES(Life Technologies), 10% heat-inactivated FBS (Life Technolo-gies), 0.1 mmol/L Non-Essential Amino Acids (Life Technolo-gies), and 1 mmol/L sodium pyruvate (Life Technologies). Sub-confluent cell monolayers were passaged after treatment with0.25%-w/v trypsin (Life Technologies).
The H1975-HGF cell line was created by transducing H1975cells with HGF lentivirus (generated using Human HGF Plasmidand Packaging Kit; GeneCopoeia) to express the human HGFgene. H1975 cells were plated at one million cells in a 100 mmdish in RPMI media. After infection, cells were selected using2 mg/mL puromycin (Invitrogen); 20 pg/mL HGF (MSD assay)was secreted (5,000 cells/well) over 72-hour incubation.
Receptor phosphorylation assaysReceptor phosphorylation assays were performed as described,
with cells plated at 6500 to 10,000 cells per well (19). The signalswere not corrected for total levels of receptor. Data were plotted asrelative enhanced chemiluminescence (ECL; RCL) signal versusthe logarithm of antibody concentration. IC50 values were calcu-lated inGraphPadPrism5 (GraphPadSoftware, Inc.) using a four-parameter logistic (4PL) model.
ERK and AKT phosphorylation assaysCells were grown in RPMI growthmedium supplemented with
7.5 ng/mL HGF, then lysed after 30-minute (pERK assay) or 1-hour (pAkt assay) treatment with the antibodies. Phospho-ERK(Thr202/Tyr204; Thr185/Tyr187) levels and phospho-AKT(S473) levels were measured using MSD assays. The signals werenot corrected for total levels of ERK or Akt. RCL signal wasrecorded and data plotted as with receptor phosphorylationassays, with statistical analysis using GraphPad Prism 6. Extrasum-of-squares F test was used to compare treatments.
Preparation/analysis of tumor lysatesMice bearing establishedH1975-HGF tumorswere treatedwith
a single dose of JNJ-61186372 (1, 5, or 20 mg/kg) or vehiclecontrol (PBS). 72 hours postdose, tumors were harvested, flashfrozen in liquid nitrogen, and lysed in ice-cold RIPA buffer(Thermo Scientific) containing 2� HALT/EDTA protease andphosphatase inhibitor cocktail (Thermo Fisher Scientific), 50mmol/L NaF, 2 mmol/L sodium orthovanadate (activated), and1 mmol/L PMSF using a FastPrep-24 homogenizer (MP Biome-dicals). Lysates were cleared by centrifugation, and protein con-centrations were determined by BCA Protein Assay (Pierce).Protein samples (50 mg) were resolved by SDS-PAGE and trans-ferred to nitrocellulose membranes. Membranes were blocked inOdyssey blockingbuffer (LI-COR) for 1hour at roomtemperatureand incubated with the appropriate primary antibodies overnightat 4�C: anti-EGFR (EGF-R2; Santa Cruz Biotechnology), anti-Met
EGFR/cMet–Bispecific Ab in EGFR TKI–Resistant Lung Tumors
www.aacrjournals.org Cancer Res; 76(13) July 1, 2016 3943
on May 11, 2020. © 2016 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Published OnlineFirst May 23, 2016; DOI: 10.1158/0008-5472.CAN-15-2833

(L41G3; Cell Signaling Technology), anti-actin (Santa Cruz Bio-technology), and anti-GAPDH (Cell Signaling Technology).Bands were detected with anti-mouse IRDye680 (LI-COR) oranti-rabbit IRDye800 (LI-COR) and imaged using an OdysseyInfrared Imaging System (LI-COR). Average total protein quan-titated fromWestern blots, relative to loading control (GAPDHoractin), was graphed and statistical analysis performed usingGraphPad Prism 6. Total cMet data were analyzed using a two-sided, unpaired, equal variance t test, and total EGFR data wereanalyzed using a two-sided, unpaired t test withWelch Correctionfor unequal variance. Tumor lysates were examined using MSDassays for phospho-proteins (p-EGFR, p-cMet, p-ERK, or p-AKT),as described above. Ordinary one-way ANOVA and two-sided,unpairedDunnettmultiple comparisons tests on log-transformedMSD signal values were used to compare treatment groups usingGraphPad Prism 6. Multiplicity-adjusted P values were reported.
ADCC assaysHuman peripheral blood mononuclear cells (PBMC) were
isolated from normal donor leukopaks (Biological SpecialtyCorporation) for use as effector cells and were cryopreserved. ThePBMCs from donors with FcgRIIIa 158V/F (20) were used inADCC assays (21, 22).
In vivo tumor xenograft modelsAll of the procedures relating to animal care, handling, and
treatmentwere performed according to the guidelines approved byInstitutional Animal Care and Use Committee or under the Ani-mals in Scientific Procedures Act 1986 (Precos). For the H1975and H1975-HGF models, 5 � 106 cells were injected subcutane-ously into the flanks (0.2 mL/mouse) of female nude mice (CD-1
NU/NU, 4–6 weeks old; Charles River Laboratories). Studieswith HCC827 and HCC827-ER1 were performed at Precos.Nude mice (MF1 NU/NU, 5–8 weeks old; Harlan, Teklad) wereinjected subcutaneously with 1 � 107 cells (0.2 mL/mouse). TheLU1235andLU1868patient-derivedxenograft (PDX)modelswereperformed byCrown Biosciences. PDX tumor fragments, harvestedfromdonormice, were inoculated into female nudemice (BALB/c,8–10 weeks old; Beijing HFK Bio-Technology Co). Animals weretreated with compounds when tumors reached a mean tumor sizeof 120 to 170 mm3. Percentage tumor growth inhibition (%TGI)was defined as the difference between the control-treated groupmean tumor volume (MTV) and the test compound–treated groupMTV, expressed as a percentage of the MTV of the control-treatedgroup. The statistical analysis of oneH1975-HGF study (Fig. 4)wasperformed comparing treatment groups with control by two-wayANOVA and Bonferroni multiple comparisons tests (GraphPadPrism). The statistical analysis ofHCC827, HCC827-ER1, LU1235,LU1868, H1975, and H1975-HGF (Fig. 7) studies was performedon the log-transformed tumor volume data and a Tukey–Kramer Pvalue adjustment for multiplicity (SAS).
ResultsBispecific antibody binding to EGFR and cMet prevents ligandbinding
Parental monospecific bivalent antibodies (F405L for anti-EGFR; K409R for anti-cMet) were expressed separately in celllines incorporating low levels (<9%) of fucose to enhance ADCC.The bispecific EGFR-cMet Ab, prepared using cFAE with >95%yield (Fig. 1A; refs. 12, 13), was designated JNJ-61186372.After purification with hydrophobic interaction chromatography,
cMetA
B
EGFR JNJ-61186372
cFAE Stable hinge
Matched CH3 domains
K409RF405L
F405LK409R
EGF Binding HGF Binding120
100
80
60
40
20
0
120
100
80
60
40
20
00 1 2 3 40 1 2 3 4
log [Competitor (nmol/L)] log [Competitor (nmol/L)]
JNJ-61186372 EGFR mAb Control mAbNF910IC50 (nmol/L)
JNJ-61186372 cMet mAb Control mAbNF1530IC50 (nmol/L)
Rel
ativ
e bi
ndin
g (%
)
Rel
ativ
e bi
ndin
g (%
)
JNJ-61186372EGFR mAbControl mAb
JNJ-61186372cMet mAbControl mAb
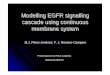
Figure 1.
Structure of JNJ-61186372 andinhibition of ligand binding. A,schematic showing the cFAE methodused to generate the bispecificantibody that binds cMet and EGFR.B, JNJ-61186372 and parental EGFRantibody inhibited EGF binding toEGFR-Fc protein (left); JNJ-61186372and parental cMet antibody inhibitedHGF binding to cMet-Fc protein(right). NF, no fit returned byGraphPad Prism.
Moores et al.
Cancer Res; 76(13) July 1, 2016 Cancer Research3944
on May 11, 2020. © 2016 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Published OnlineFirst May 23, 2016; DOI: 10.1158/0008-5472.CAN-15-2833

JNJ-61186372 was confirmed to be >99% bispecific Ab with<0.2% parental mAbs.
JNJ-61186372 binding to the extracellular domains (ECD) ofEGFR and cMet was confirmed using surface plasmon resonancemethods (19). JNJ-61186372 has an affinity (KD) of 1.4 nmol/Lfor EGFR-ECD and aKD¼ 40 pmol/L for cMet-ECD.Using similarmethods, JNJ-61186372 was shown to bind both EGFR-ECD andcMet-ECD simultaneously (19).
JNJ-61186372 blocked the ligand binding of each receptor ina dose-dependent manner (Fig. 1B). JNJ-61186372 inhibitedruthenium-labeled EGF binding to EGFR-ECD with an IC50 ¼10 nmol/L and inhibited biotinylated-labeled HGF binding tocMet-ECDwith an IC50¼ 30 nmol/L. These results demonstratedthat JNJ-61186372 bound to both EGFR and cMet with highaffinity and furthermore inhibited ligand binding to each receptorwith similar potency compared with the parental monospecificbivalent antibodies.
JNJ-61186372 inhibits receptor phosphorylation of EGFR andcMet
Human lung cancer cell lines, representing different EGFR andcMet genotypes that often occur in NSCLC patients, were selectedto evaluate the cellular activity of JNJ-61186372 (SupplementaryTable S1). These included cell lines with EGFR primary activatingmutations, EGFR T790M mutation (confers resistance to EGFRTKIs), either alone or withMET gene amplification, and cell lineswith wild-type (WT) EGFR and WT levels of cMet. In these celllines, JNJ-61186372 inhibited EGF-induced phosphorylation ofEGFR and HGF-induced phosphorylation of cMet in a dose-dependent manner (Fig. 2A), with activities (IC50) below 100nmol/L (Fig. 2B). The level of phosphorylated EGFR in theuntreated H1975 cells (EGFR mutations L858R; T790M) washigher than that of H292 cells (EGFR WT) due to the activatingmutation in EGFR. Addition of EGF to H1975 cells resulted in asmaller induction of phosphorylated EGFR compared with the
50,000
40,000
30,000
20,000
10,000
0
20,000
10,000
1,000
A
B
H1975
H292
pEGFR pMet
IC50
(nm
ol/L
)
pEGFR (Y1173)
pMet (Y1349)
H292
WT
WT WT WT WT WT WT-AMP WT-AMP
WTEx19del;T790M
ex19del;AMP
L858R;AMP
L858R;T790M
Ex19del;AMPEGFR
MET
HCC827 H1975 H3255 HCC4006 H820 H1993
100
10
1
0.1
0
30,000
10,000
5,000
0
15,000
-2 -2 -1 0 1 2 3-1 0
Unstimulatedcontrol
JNJ-61186372 Concentrationlog (nmol/L)
JNJ-61186372 Concentrationlog (nmol/L)
JNJ-61186372 Concentrationlog (nmol/L)
JNJ-61186372 Concentrationlog (nmol/L)
MSD
Sig
nal (
RC
L un
its)
MSD
Sig
nal (
RC
L un
its)
MSD
Sig
nal (
RC
L un
its)
40,000
20,000
0MSD
Sig
nal (
RC
L un
its)
Ligand-stimulatedcontrol
Unstimulated control
Ligand-stimulatedcontrol
Unstimulatedcontrol
Ligand-stimulatedcontrol
Unstimulatedcontrol
Ligand-stimulatedcontrol
n = 3n = 3
n = 3
n = 3
1 2 3
-2 -1 0 1 2 3 -2 -1 0 1 2 3
Figure 2.
JNJ-61186372 inhibited ligand-induced phosphorylation of both EGFR and cMet in lung cancer cell lines. A, H292 and H1975 cells were serum starved, then stimulatedwith EGF (left) or HGF (right) in the presence of JNJ-61186372. Levels of phospho-EGFR (left) or phospho-cMet (right) were detected (RCL, relativechemiluminescence),with threebiologic replicates at each point.MeanRCLvalues are plotted�SEM.B, summary IC50data for a panel of lung cancer cell lines for JNJ-61186372 inhibition of phospho-EGFR (light bars) and phospho-cMet (dark bars) using MSD assays.
EGFR/cMet–Bispecific Ab in EGFR TKI–Resistant Lung Tumors
www.aacrjournals.org Cancer Res; 76(13) July 1, 2016 3945
on May 11, 2020. © 2016 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Published OnlineFirst May 23, 2016; DOI: 10.1158/0008-5472.CAN-15-2833

magnitude of induction observed with H292 cells. Nevertheless,JNJ-61186372 inhibited phosphorylation of EGFR in the EGF-stimulatedH1975 cells, reducing the phosphorylation of EGFR tolevels below the unstimulated condition.
Enhanced inhibitionofdownstreamsignalingwith JNJ-61186372To determine whether dual inhibition of receptor phosphor-
ylation had downstream signaling consequences, the inhibitionof phospho-ERK and phospho-AKT by JNJ-61186372 wasassessed in the same panel of cell lines (Fig. 3A). JNJ-61186372 demonstrated potent inhibition of both phospho-ERKand phospho-AKT, with IC50 values in the low or subnanomolarrange for most cell lines tested. However, in cell lines with METgene amplification (H820 and H1993), JNJ-61186372 demon-strated either weak or no inhibition of phospho-ERK or phospho-AKT.
Single-pathway inhibition (EGFR or cMet) by monovalentantibodies was also assessed and compared with that of JNJ-61186372 (Fig. 3B–E). In H292 cells, neither treatment with themonovalent EGFR or monovalent cMet antibody caused com-plete inhibition of pERK, whereas the combination of the two
monovalent antibodies caused complete inhibition of pERKwithan IC50 ¼ 35 nmol/L (Fig. 3B). This result demonstrated thatinhibition of both EGFR and cMet was necessary for full inhibi-tion of pERK in this cell line. Interestingly inH292 cells, treatmentwith JNJ-61186372 resulted in complete inhibition of pERK, butwith a lower IC50¼ 0.64 nmol/L, a 55-fold increase in potency (P< 0.0001) for JNJ-61186372 compared with that of the combi-nation of monovalent antibodies. Also in H292 cells, the mono-valent cMet antibody was as effective as the combination ofmonovalent antibodies at inhibiting pAKT, suggesting that pAKTwas more dependent on cMet signaling compared with EGFRsignaling in this cell line (Fig. 3C). Nevertheless, JNJ-61186372was 179-fold more potent for inhibition of pAKT (P < 0.0001)compared with the combination of monovalent antibodies, sug-gesting that the bispecificmolecule had additional biologic effectsnot present in the combination of monovalent antibodies. Sim-ilarly, there was more potent inhibition of pERK and pAKT inH1975 cells using JNJ-61186372 [(65-fold greater inhibition ofpERK (P < 0.0001); 75-fold greater inhibition of pAKT (P <0.0001)] than the combination of monovalent antibodies (Fig.3D and E).
1,000A
B C
ED
100
10
1
0.1
4,000
Vehiclecontrol
Vehiclecontrol
EGFR ¥ gp120gp120 ¥ cMet
(EGFR ¥ gp120)+(gp120 ¥ cMet)JNJ-61186372
Vehiclecontrol
n = 3
Vehiclecontrol
n = 3
n = 3
n = 3
3,000
2,000
MSD
Sig
nal (
RC
L un
its)
MSD
Sig
nal (
RC
L un
its)
MSD
Sig
nal (
RC
L un
its)
MSD
Sig
nal (
RC
L un
its)
1,000
0
4,000
5,000
3,000
2,000
1,000
0
40,000
50,000
30,000
20,000
10,000
0
15,000
20,000
10,000
5,000
0
-2 -1 0 1 2 3 -2 -1 0 1 2 3 4
-4 -2 0 2 4-4 -2 0 2 4
Treatment concentrationlog (nmol/L) Treatment concentration
log (nmol/L)
Treatment concentrationlog (nmol/L)
Treatment concentrationlog (nmol/L)
H292
EGFRMET
pERK pAKT
H292
H1975
HCC827 H1975 H3255 HCC4006
pERK 1/2 (T202/Y204; T185/Y187)pAKT (S473)
IC50
(nm
ol/L
)
H820 H1993
Not
act
ive
Not
act
ive
WT
WT WT WT WT WT WT-AMP WT-AMP
WTEx19del;T790M
ex19del;AMP
L858R;AMP
L858R;T790M
Ex19del;AMP
Figure 3.
JNJ-61186372 inhibited phospho-ERK andphospho-AKT in lung cancer cell lines. A, summary IC50 data for a panel of cell lines for JNJ-61186372 inhibition of phospho-ERK (light bars) and phospho-AKT (dark bars) using MSD assays. B–E, H292 cells (B and C) and H1975 cells (D and E) were treated with antibodies and phospho-ERK (B andD) and phospho-AKT (D and E),measured using theMSD assay (RCL, relative chemiluminescence), with three biologic replicates at each point. Mean RCLvalues are plotted �SEM.
Moores et al.
Cancer Res; 76(13) July 1, 2016 Cancer Research3946
on May 11, 2020. © 2016 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Published OnlineFirst May 23, 2016; DOI: 10.1158/0008-5472.CAN-15-2833

JNJ-61186372 caused tumor cell lysis through enhancedeffector function
We hypothesized that high levels of EGFR and cMet on thesurface of tumor cellsmay allow for selective immune effector celltargeting through ADCC. JNJ-61186372 was engineered to havelow levels of core fucose, which allows for tighter binding tohuman FcgRIIIa on natural killer (NK) cells, thus resulting in amore potent and effective ADCC killing of target cells (14).
The ADCC in vitro activity of JNJ-61186372 was tested usingH292 and H1975 cells with human PBMCs as the source of NKcells (Fig. 4A). For comparison, an analogue of JNJ-61186372, butproduced with normal fucose levels, and cetuximab (anti-EGFRmAb) were assessed in the same assay. The low fucose JNJ-61186372 was more potent and demonstrated increased levelsof tumor cell lysis compared with the EGFR-cMet bispecificantibody with normal fucose levels. Similar results were observedusing additional lung cancer cell lines, including those with eitherWT or mutant EGFR and WT or amplified MET (SupplementaryTable S2). The ADCC capacity of the low fucose JNJ-61186372was similar to the ADCC capacity of cetuximab. However, therewere some cases where JNJ-61186372 demonstrated slightlyimproved ADCC activity in potency (EC50) and/or efficacy (%maximal lysis).
JNJ-61186372 inhibited tumor growth in the H1975-HGFxenograft model
The H1975 cell line carries both an activating mutation(L858R) and a second-site mutation in EGFR (T790M) thatconfers resistance to small-molecule EGFR TKIs, such as erlotinib.
In addition, this line was engineered to express human HGF(H1975-HGF) so the human cMet on the tumor cells would beactivated in the mouse host (mouse HGF does not effectivelyactivate human cMet, ref. 23). H1975-HGF cells were implantedinto immune-compromised mice to assess in vivo efficacy of JNJ-61186372 on xenograft tumors. In addition, the contribution ofeffector function to efficacy in vivo was evaluated.
After subcutaneous tumors were established, the mice weretreated with vehicle control (PBS), JNJ-61186372, or an anti-body with the same EGFR and cMet-binding arms but with anIgG2s framework (JNJ-61186372-IgG2s). Antibodies with anIgG2s framework have less binding to Fc receptors of effectorcells (such as NK cells and macrophages), but maintain similarpharmacokinetics to IgG1 antibodies, so any loss of activityobserved with JNJ-61186372-IgG2s antibody should representthe contribution of the effector-mediated function of JNJ-61186372 (24).
As shown in Fig. 4B, JNJ-61186372 inhibited tumor growth by80% compared with vehicle-treated animals at day 32 (P <0.0001). Interestingly, JNJ-61186372-IgG2s antibody (Fc silentversion) inhibited tumor growth by 47% (P ¼ 0.0232) but wasnot as effective as JNJ-61186372with the FcR-binding framework.These results demonstrate efficacy of JNJ-61186372 in theH1975-HGF model, with EGFR mutations (L858R; T790M) and cMetactivation through autocrine expression of HGF. In addition,without effector function, the inhibition of EGFR and cMet alonereduced tumor growth relative to the vehicle control, but theaddition of the effector function (IgG1 framework) is necessaryfor complete JNJ-61186372 in vivo activity.
30
20
10
0
-10
Ab (nmol/L)
JNJ-61186372 (low fucose)
H292A
BCetuximabEGFR-cMet (normal fucose)IgG1 Isotype control mAb
JNJ-61186372 (low fucose)CetuximabEGFR-c Met (normal fucose)IgG1 Isotype control mAb
% L
ysis
H197530
20
10
0
Ab (nmol/L)
Days post tumor cell implant
JNJ-61186372-lgG2s
PBS Vehicle
H1975-HGF(EGFR L858R; T790M)
JNJ-61186372
Mea
n tu
mor
vol
ume
(mm
3 ) ±
SEM
110
200
400
600800
1,0001,200
1,400
1,600
1,800
14 18 21 24 28 32
% L
ysis
-10
0.000
010.0
001
0.001 0.01 0.1 1 10 100
0.000
010.0
001
0.001 0.0
1 0.1 1 10 100
Figure 4.
Fc effector function of JNJ-61186372 was enhanced in vitro and was important for efficacy in vivo. A, ADCC assays were performed using H292 (top) and H1975(bottom) cells. Low fucose JNJ-61186372 was compared with normal fucose EGFR-cMet antibody, cetuximab, and IgG1 control antibody. B, H1975-HGF model wasused to compare JNJ-61186372 with JNJ-61186372-IgG2s for efficacy. Antibodies were dosed at 10 mg/kg two times per week i.p. (10 animals/group).
EGFR/cMet–Bispecific Ab in EGFR TKI–Resistant Lung Tumors
www.aacrjournals.org Cancer Res; 76(13) July 1, 2016 3947
on May 11, 2020. © 2016 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Published OnlineFirst May 23, 2016; DOI: 10.1158/0008-5472.CAN-15-2833

JNJ-61186372 induced receptor downmodulation in vivoTo further understand the function of JNJ-61186372 in vivo,
mice bearing H1975-HGF tumors were treated with either PBSvehicle control or JNJ-61186372 at 1, 5, and 20 mg/kg. Tumorlysates frommice treated with 20mg/kg JNJ-61186372 and thosetreated with vehicle were analyzed for total EGFR and cMet levelsbyWestern blot analysis (Fig. 5A). The average total protein levelsof both EGFR and cMet were significantly decreased followingantibody treatment compared with those of vehicle-treatedtumors by 76% (P < 0.0001) and 61% (P¼ 0.0007), respectively.Not surprisingly, because levels of total receptor were significantlyreduced (Fig. 5A and B), phospho-EGFR and phospho-Met levelswere also significantly reduced at all doses tested compared withthose of vehicle-treated animals (Fig. 5C). Phospho-AKT wassignificantly reduced at 5 and 20 mg/kg antibody treatment, butlevels of phospho-ERK were not significantly decreased in thisexperiment. These results demonstrated downmodulation ofboth receptor targets and downstream signaling in the tumor by
JNJ-61186372 treatment, thus illustrating an additional antitu-mor growth mechanism of action.
JNJ-61186372 is effective in EGFR-mutant xenograft models,with or without cMet activation
JNJ-61186372 was evaluated in a pair of human lung adeno-carcinomaHCC827 xenograft models, both with a primary EGFRmutation (exon 19 deletion), but one with MET amplification(clone of parental HCC827; originally selected to have resistanceto erlotinib; HCC827-ER1). In mice with HCC827 tumors, treat-ment with either erlotinib or JNJ-61186372 fully suppressedtumor growth during the treatment period (28 days) and toapproximately 50 days posttreatment initiation (Fig. 6A). BothJNJ-61186372 and erlotinib inhibited tumor growth by 89%compared with vehicle-treated animals at day 45 (both P <0.05). In mice with HCC827-ER1 tumors, JNJ-61186372 fullysuppressed tumor growth, whereas erlotinib was only partiallyeffective during treatment (days 7–31), and mean tumor volume
PBS-treated JNJ-61186372−treated
ActinEGFR
cMet
GAPDH
pEGFR
A
C
B
pMet4,000 1,000
0.25
Nor
mal
ized
sig
nal t
o ac
tinN
orm
aliz
ed s
igna
l to
GA
PDH
0.20
0.15
0.10
0.05
PBS JNJ-61186372
PBS
0.04
0.03
0.02
0.01
0.00JNJ-61186372
Total Met
Total EGFR
P = 0.0007
P < 0.0001
0.00
40,000100,000pERK pAKT
80,000
60,000
MSD
Sig
nal (
RC
L un
its)
MSD
Sig
nal (
RC
L un
its)
40,000
20,000
0
30,000
20,000
10,000
0
800
600
400P = 0.004 P = 0.001
P = 0.0005P = 0.002
200
PBS 1 5 20
PBS 1 5 20PBS 1 5 20
0
3,000
2,000
MSD
Sig
nal (
RC
L un
its)
MSD
Sig
nal (
RC
L un
its)
1,000
0 PBS
JNJ-61186372 (mg/kg) JNJ-61186372 (mg/kg)
JNJ-61186372 (mg/kg) JNJ-61186372 (mg/kg)
1 5 20
P < 0.0001
P = 0.012
P < 0.0001
Figure 5.
Decreased EGFR and cMet protein, phospho-EGFR, phospho-cMet, and phospho-AKT levels in H1975-HGF tumors frommice treatedwith JNJ-61186372. A,micewithH1975-HGF tumors were treated with a single dose of JNJ-61186372 (20 mg/kg) or vehicle control (PBS). Tumor lysates were examined by Western blotanalysis for total levels of EGFR, cMet, or actin/GAPDH (loading controls). B, average total protein quantitated from Western blots, relative to loading controls.C, mice with H1975-HGF tumors were treated with a single dose of JNJ-61186372 (1, 5, or 20 mg/kg) or vehicle control (PBS). Tumor lysates examined usingMSD assays for phospho-EGFR, phospho-cMet, phospho-ERK, or phospho-AKT.
Moores et al.
Cancer Res; 76(13) July 1, 2016 Cancer Research3948
on May 11, 2020. © 2016 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Published OnlineFirst May 23, 2016; DOI: 10.1158/0008-5472.CAN-15-2833

increased at a similar rate as vehicle-treated tumors followingcessation of treatment (Fig. 6B). However, in animals treated withJNJ-61186372, mean tumor volume slightly increased in 5 weeksfollowing cessation of treatment. At day 37, erlotinib inhibitedtumor growth by 63% (P < 0.05), while JNJ-61186372 inhibitedtumor growth by 92% (P < 0.05), compared with vehicle-treatedanimals. These results suggested that in tumors with both EGFRmutations andMET amplification, dual inhibition of both EGFRand cMet was necessary for complete inhibition of tumor growth.
JNJ-61186372 is effective in PDX models with EGFR mutationsWe tested the bispecific EGFR-cMet antibody efficacy in PDX
models with EGFRmutations. For these studies, we used a versionof JNJ-61186372 prepared with normal fucose levels. LU1235PDX model is derived from a human lung primary adenocarci-noma tumor with a primary activating EGFR mutation (exon 19deletion). In these tumors, treatments with erlotinib and JNJ-61186372 were both effective at regressing tumor volumes, butJNJ-61186372 continued to suppress tumor growth followingcessation of treatment (Fig. 6C). These results demonstrated thatin tumors with a primary activating mutation in EGFR, thebispecific EGFR-cMet antibody led to a more durable responsethan erlotinib treatment. The human lung adenocarcinoma
LU1868 PDXmodel contains both a primary activating mutationin EGFR (L858R) and the second-site mutation in EGFR (T790M,known to cause resistance to erlotinib treatment). As expected inthis model, erlotinib was not effective (Fig. 6D). However, JNJ-61186372 treatment caused regression of the LU1868 tumors in adurable manner for up to 2 months following cessation oftreatment. JNJ-61186372 was effective in PDXmodels with eitherprimary activating mutations in EGFR alone, and with the addi-tion of T790M EGFR TKI resistance mutation.
Combination of JNJ-61186372 and third-generation EGFR TKIresulted in durable tumor regression
Third-generation EGFR TKIs, such as AZD9291 and CO-1686,preferentially inhibit mutant-activated EGFR compared with WTEGFR. To assess whether the combination of a third-generationEGFR TKI and JNJ-61186372 would have benefit, we testedAZD9291 and JNJ-61186372 as single agents and in combinationin the parental H1975 model (Fig. 7A) and the engineeredH1975-HGF model (Fig. 7B). During the treatment period,AZD9291 inhibited tumor growth in both parental H1975 (TGI¼ 100%) and H1975-HGF (TGI ¼ 94%) models, P < 0.05 forboth. However, AZD9291-treated tumors increased in volumeafter treatment cessation in the H1975-HGF model. During the
HCC827-ER1 (EGFR ex19del; MET amp)
PBS Vehicle
Erlotinib
HCC827 (EGFR ex19del)
PBS VehicleDosing phase
1,500
1,000
500
0
1,500
1,000
500
00 20 40 60 800 20 40 60 80
JNJ-61186372Erlotinib
Days Days
A B
LU1235 (EGFR: ex19 del) LU1868 (EGFR: L858R; T790M)
Erlotinib
Erlotinib
0 20 40 60 800
500
1,000
1,500
2,000
2,500
Dosing phase Dosing phase
0 20 40 600
500
1,000
1,500
2,000
2,500
Dosing phase
PBS Vehicle
Days Days
C D
Mea
n tu
mor
vol
ume
(mm
3 ) +
SEM
M
ean
tum
or v
olum
e (m
m3 )
+ S
EM
Mea
n tu
mor
vol
ume
(mm
3 ) +
SEM
M
ean
tum
or v
olum
e (m
m3 )
+ S
EM
JNJ-61186372
JNJ-61186372 JNJ-61186372
PBS Vehicle
Figure 6.
JNJ-61186372 was efficacious in EGFR-mutant models, with or without cMet activation. JNJ-61186372 (10 mg/kg two times/week i.p.) was tested for efficacy inHCC827model (A) andHCC827-ER1model (B; 9 animals/group). JNJ-61186372was efficacious in PDXmodelswith EGFRmutations, exon 19 deletion (C) and L858R,T790M (D). The JNJ-61186372 used in C and D was an earlier preparation with normal fucose levels and residual parental bivalent EGFR antibody remaining (12%).Erlotinib was dosed at 25 or 50 mg/kg daily orally; 9 or 10 animals per group.
EGFR/cMet–Bispecific Ab in EGFR TKI–Resistant Lung Tumors
www.aacrjournals.org Cancer Res; 76(13) July 1, 2016 3949
on May 11, 2020. © 2016 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Published OnlineFirst May 23, 2016; DOI: 10.1158/0008-5472.CAN-15-2833

treatment period, JNJ-61186372 was effective in both models(TGI ¼ 79% and 90%, respectively, P < 0.05 for both). Thecombination treatment with JNJ-61186372 and AZD9291 wasmore effective than either single treatment in the H1975-HGFmodel. After 3 weeks of treatment, tumors were monitored formore than a month and no measurable tumors were observed in
the combination groups in either tumormodel. In a second studyusing theH1975-HGFmodel (Fig. 7C–E), tumorswere grown to alarger size (average of 500 mm3) before treatment initiation.Again, tumors completely regressed with the combination treat-ment, and no tumor growth was observed for up to 85 days oftreatment. Crizotinib, a small-molecule cMet/ALK inhibitor,
A
B
VehicleJNJ-61186372
AZD9291
AZD9291 + JNJ-61186372
H1975(EGFR L858R; T790M) JNJ-61186372
AZD9291
JNJ-61186372 + AZD9291
Days0 20 40 60 80 100
0
500
1,000
1,500
2,000
00 20
2,000
1,500
1,000
500
00 20 40 60 80 100
40 60 80 100Days
Days
500
1,000
1,500
2,000
Tum
or v
olum
e (m
m3 )
Tum
or v
olum
e (m
m3 )
Tum
or v
olum
e (m
m3 )
H1975-HGF(EGFR L858R; T790M; HGF autocrine)
Mea
n tu
mor
vol
ume
(mm
3 ) +
SEM
Mea
n tu
mor
vol
ume
(mm
3 ) +
SEM
Vehicle
JNJ-61186372
AZD9291
AZD9291 + JNJ-61186372
C
D
EDays0
0
1,000
2,000
3,000
00
1,000
2,000
3,000
20 40 60
Dosing phase
Dosing phase
20 40 60
Days
Figure 7.
JNJ-61186372 in combinationwithAZD9291was effective anddurable inH1975 andH1975-HGFxenograftmodelswith andwithout cMet pathway activation. A, H1975model. B, H1975-HGF model. C–E, results of a different study in H1975-HGF, starting with larger tumors (�500 mm3) and plotting individual tumor volumes overtime. A and B, JNJ-61186372 dosed at 10 mg/kg two times per week i.p.; AZD9291 dosed at 30 mg/kg daily orally. Note that in A, the curves for AZD9291 and forJNJ-61186372 þ AZD9291 are superimposed. C and E, JNJ-61186372 was dosed at 10 mg/kg two times per week i.p. D and E, AZD9291 was dosed at 5 mg/kg dailyorally. C–E, dosing was continuous throughout the study.
Moores et al.
Cancer Res; 76(13) July 1, 2016 Cancer Research3950
on May 11, 2020. © 2016 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Published OnlineFirst May 23, 2016; DOI: 10.1158/0008-5472.CAN-15-2833

showed no efficacy in either model (Supplementary Fig. S3).Altogether, these results demonstrated that combination of athird-generation EGFR TKI and JNJ-61186372 caused regressionof tumors in a sustained and durable manner.
Absence of EGFR-mediated skin rash after repeatadministration of JNJ-61186372
Both Good Laboratory Practice (GLP) and non-GLP safetystudies were performed in cynomolgus monkeys. Animals weregiven JNJ-61186372 intravenously at doses up to 120mg/kg onceper week for up to 5 weeks. No toxicities were observed in eitherstudy, including none of the skin or gut adverse events that arecommonly observed with other anti-EGFR agents (25). Notably,JNJ-61186372 recovered in serum from cynomolgus monkeystreated with JNJ-61186372 was fully functional in inhibition ofphospho-EGFR and phospho-Met in vitro using H292 humancancer cell line (Supplementary Fig. S4). Our preliminary datasuggested that this lack of skin toxicity may be attributable to alower single-arm binding affinity for purified EGFR protein com-pared with cetuximab [JNJ-61186372 KD ¼ 1.4 nmol/L (19);cetuximab KD ¼ 0.4 nmol/L in same assay format]. This loweraffinity then translates into less potent binding to cells expressinglow levels of EGFR and cMet, such as primary human dermalfibroblasts. We found that JNJ-61186372 bound to primaryhuman dermal fibroblasts with an EC50 ¼ 2.0 nmol/L, whereascetuximab bound 20-fold tighter, with an EC50 ¼ 0.1 nmol/L.Binding to normal tissues is also likely enhanced by the bivalentnature of cetuximab, compared with the monovalent EGFR bind-ing of JNJ-61186372.
DiscussionExtensive evidence has demonstrated that the EGFR and cMet
signaling pathways are partially compensatory and mediate crossresistance to inhibitors of either pathway (4, 8, 9). Standard-of-care treatment for lung cancer patients with activating mutationsin EGFR involves small-molecule EGFR TKIs, such as erlotinib orgefitinib. These therapies, although often initially very effective,ultimately fail due to resistance mediated by second-site EGFRmutations, such as T790M, or activation of bypass pathways, suchas the cMet pathway (4, 9, 10, 26). Second- and third-generationEGFR TKIs, such as afatinib, AZD9291, and CO-1686, haveproduced exciting clinical results, but resistance to therapyremains a prominent challenge. Resistance mechanisms tothird-generation EGFR TKIs are still being defined in patientsamples, but an emerging frequent mechanism is mutation ofEGFR (C797S; ref. 27). Evidence of MET amplification in lungtumor cells from a patient treated with AZD9291 has also beenreported, suggesting that activation of the cMet pathway is clin-ically relevant for the third-generation EGFR TKIs (28).
To address these resistance issues, we have created a bispecificantibody, JNJ-61186372, that recognizes both EGFR and cMet.We have demonstrated that JNJ-61186372 inhibits tumor growthand progression by three distinct mechanisms. Two of thesemechanisms involve inhibition of EGFR and cMet signaling, firstby inhibition of ligand-induced activation via blocking ligandbinding to each receptor and second by receptor inactivation viadegradation. The third mechanism utilizes Fc effector-mediatedkilling of EGFR- and cMet-expressing tumor cells by ADCC.Through these mechanisms of action, JNJ-61186372 showedactivity in multiple xenograft models containing diverse EGFR
mutations (exon 19 deletion, L858R, T790M). Given that JNJ-61186372 recognizes the extracellular region of EGFR, this bis-pecific antibody has the potential to be active in tumors withC797Smutation (located intracellularly) as well. In addition, JNJ-61186372 was active in models with cMet pathway activation,either by autocrine ligand production or through MET geneamplification. JNJ-61186372 was also active in a model with WTEGFR and autocrine HGF production (Supplementary Fig. S5).Collectively, the unique mechanisms of action of JNJ-61186372cover the spectrum of EGFR mutations and also inhibit the keypathways driving EGFR TKI–acquired resistances.
Combination therapies may be necessary to fully suppress theEGFR pathway and prevent resistance from occurring throughmultiple mechanisms. The combination of afatinib and cetux-imabwas shown to cause near complete tumor regression inmicewith L858R/T790M erlotinib-resistant tumors (29) by depletingphosphorylated and total EGFR more completely than eithersingle agent alone. Combining JNJ-61186372 with third-gener-ation EGFR TKIs might have the advantage, in addition to simul-taneous inhibition of the cMet pathway, of more completeinhibition of the EGFR pathway through the ligand inhibitionand receptor degradation mechanisms. Addition of the immuneeffector–based mechanisms of JNJ-61186372 may also attacktumor cells resistant due to EGFR- and cMet-independentmechanisms. We have shown here that the combination ofJNJ-61186372 and AZD9291 was very effective at inhibitingtumor growth in xenograft models with EGFR mutations andcMet activation. Furthermore, in contrast to monotherapy, treat-ment with the combination prevented tumor regrowth in allanimals tested. In patients, tumor heterogeneity likely contributesto resistance; recent observations suggest that T790M-positive andT790M-WT coexist in some lung cancers with acquired resistanceto initial EGFR TKI treatment (28, 30). Combination therapywithJNJ-61186372 may delay or prevent the emergence of resistance,with activity on clonal populations with varying EGFRmutationswithin the same tumor, more complete suppression of the EGFRpathway, and inhibition of cMet, a key bypass pathway.
Recently, advances in protein engineering have made the pro-duction of intact bispecific human antibodies, such as JNJ-61186372, more practical. One potential advantage of the bis-pecific configuration is the significantly improved inhibition ofdownstream signaling when both targets are present on the sametumor cell. This property may be explained by an avidity effect, inwhich cells expressing both targets engage both arms of thebispecific (cross-arm binding) with increased apparent affinityas compared with those expressing only one target or otherwiseengaging a single Fab arm. We have described correlationsbetween binding affinity, receptor density, and receptor phos-phorylation with JNJ-61186372 (19). Furthermore, we haveshown that JNJ-61186372 was more effective than the combina-tion therapy of anti-EGFR and anti-cMet monovalent antibodiesin decreasing tumor growth in the H1975-HGF model (31).
This bispecific structure may also confer unexpected propertieson JNJ-61186372. In contrast with other EGFR-targeted agents(25), we did not observe EGFR-mediated skin toxicity with JNJ-61186372 in cynomolgus monkeys, typically a critical limitationof this class of agents, even at doses up to 120 mg/kg. Wehypothesize that the lack of skin rash in cynomolgus monkeystreated with JNJ-61186372 is linked to weaker, monovalentbinding of JNJ-61186372 to EGFR compared with strongerbinding of antibodies interacting bivalently with EGFR
www.aacrjournals.org Cancer Res; 76(13) July 1, 2016 3951
EGFR/cMet–Bispecific Ab in EGFR TKI–Resistant Lung Tumors
on May 11, 2020. © 2016 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Published OnlineFirst May 23, 2016; DOI: 10.1158/0008-5472.CAN-15-2833

(e.g., cetuximab, panitumumab) to normal skin and gut cells.Indeed, we found a 20-fold difference in affinity between JNJ-61186372 and cetuximab in binding to normal human dermalfibroblasts. Because normal tissues express low levels of cMet, thecMet-binding arm of JNJ-61186372 is not engaged, thus resultingin overall weaker binding to skin and gut cells, along with lowerinhibition of EGFR in these normal tissues. In contrast in tumorcells, where high levels of EGFR and cMet are coexpressed, botharms of JNJ-61186372 are engaged, and stronger binding andfunctional inhibition is achieved. Alternatively, species differ-ences in binding and activity could contribute to the observedlack of skin toxicity. The potential lower toxicity profile of JNJ-61186372 may also be an advantage in combination therapies,where efficacy may be limited by toxicity issues, such as with thecombination of afatinib and cetuximab (32).
We have demonstrated three distinct mechanisms of action forJNJ-61186372 that modulate both EGFR and cMet signaling axes.The unique structure of JNJ-61186372 enables attack of tumorcells with multiple mechanisms in a single agent, resulting indurable antitumor effects in preclinical models resistant to othertherapeutic approaches. These results support testing in humanclinical trials, as monotherapy in selected patients and in com-bination with other agents addressing the same pathways, in lungcancer and other malignancies.
Disclosure of Potential Conflicts of InterestS.L. Moores is an Associate Director at Janssen R&D. P. Haytko is a Senior
Associate Scientist at Janssen Pharmaceuticals. J. Neijssen has ownership interest(including patents) in Genmab. P.W.H.I. Parren is a Professor at LeidenUniversity Medical Center and has ownership interest (including patents) inGenmab. J. Schuurman has ownership interest (including patents) in Genmaband is a consultant/advisory boardmember for Joint Research Committee. R.M.
Attar is a Senior Director at Janssen Pharmaceuticals. G.M. Anderson is aScientific Director at Janssen R&D. No potential conflicts of interest weredisclosed by the other authors.
Authors' ContributionsConception and design: S.L. Moores, M.L. Chiu, P.L. Martin, J. Neijssen,P.W.H.I. Parren, R.M. Attar, S. Laquerre, M.V. Lorenzi, G.M. AndersonDevelopment of methodology: S.L. Moores, M.L. Chiu, B.S. Bushey,K. Chevalier, R.J. Brezski, P. Haytko, S.-J. Wu, J. NeijssenAcquisition of data (provided animals, acquired and managed patients,provided facilities, etc.): B.S. Bushey, K. Chevalier, L. Luistro, K. Dorn,R.J. Brezski, P. Haytko, T. Kelly, S.-J. Wu, P.L. MartinAnalysis and interpretation of data (e.g., statistical analysis, biostatistics,computational analysis): S.L. Moores, M.L. Chiu, B.S. Bushey, L. Luistro,K. Dorn, S.-J. Wu, P.L. Martin, P.W.H.I. Parren, S. Laquerre, G.M. AndersonWriting, review, and/or revision of the manuscript: S.L. Moores, M.L. Chiu,L. Luistro, R.J. Brezski, P. Haytko, P.L. Martin, J. Neijssen, P.W.H.I. Parren,J. Schuurman, S. Laquerre, M.V. Lorenzi, G.M. AndersonAdministrative, technical, or material support (i.e., reporting or organizingdata, constructing databases): M.L. Chiu, B.S. Bushey, K. Chevalier,L. Luistro, P.L. Martin, J. NeijssenStudy supervision: S.L. Moores, M.L. Chiu, P.L. Martin, P.W.H.I. Parren,J. Schuurman, R.M. Attar, S. Laquerre, G.M. Anderson
AcknowledgmentsThe authors acknowledge the contributions of Amy Wong, Yi Tang, Diana
Chin, Hillary Quinn, Frank McCabe, Jeff Nemeth, Kerry Brosnan, and EvaEmmell to the in vivo studies in this report. The authors thank Jeroen Lammertsvan Bueren and Aran Labrijn for expert advice and helpful discussions.
The costs of publication of this articlewere defrayed inpart by the payment ofpage charges. This article must therefore be hereby marked advertisement inaccordance with 18 U.S.C. Section 1734 solely to indicate this fact.
ReceivedOctober 12, 2015; revised February 25, 2016; accepted April 6, 2016;published OnlineFirst May 23, 2016.
References1. Kobayashi S, BoggonTJ,DayaramT, J€anne PA, KocherO,MeyersonM, et al.
EGFRmutation and resistance of non-small-cell lung cancer to gefitinib. NEngl J Med 2005;352:786–92.
2. Perez-Soler R, Chachoua A, Hammond LA, Rowinsky EK, Huberman M,Karp D, et al. Determinants of tumor response and survival with erlotinibin patients with non–small-cell lung cancer. J Clin Oncol 2004;22:3238–47.
3. Chen HJ, Mok TS, Chen ZH, Guo AL, Zhang XC, Su J, et al. Clinicopath-ologic and molecular features of epidermal growth factor receptor T790Mmutation and c-MET amplification in tyrosine kinase inhibitor-resistantChinese non-small cell lung cancer. Pathol Oncol Res 2009;15:651–8.
4. Engelman JA, Zejnullahu K, Mitsudomi T, Song Y, Hyland C, Park JO, et al.MET amplification leads to gefitinib resistance in lung cancer by activatingERBB3 signaling. Science 2007;316:1039–43.
5. Sequist LV,Waltman BA, Dias-SantagataD, Digumarthy S, Turke AB, FidiasP, et al. Genotypic and histological evolution of lung cancers acquiringresistance to EGFR inhibitors. Sci Transl Med 2011;3:75ra26.
6. Pao W, Miller VA, Politi KA, Riely GJ, Somwar R, Zakowski MF, et al.Acquired resistance of lung adenocarcinomas to gefitinib or erlotinib isassociated with a second mutation in the EGFR kinase domain. PLoS Med2005;2:e73.
7. Yun CH, Mengwasser KE, Toms AV, Woo MS, Greulich H, Wong KK, et al.The T790M mutation in EGFR kinase causes drug resistance by increasingthe affinity for ATP. Proc Natl Acad Sci U S A 2008;105:2070–5.
8. Yano S, Yamada T, Takeuchi S, Tachibana K, Minami Y, Yatabe Y, et al.Hepatocyte growth factor expression in EGFR mutant lung cancer withintrinsic and acquired resistance to tyrosine kinase inhibitors in a Japanesecohort. J Thorac Oncol 2011;6:2011–7.
9. Turke AB, Zejnullahu K, Wu YL, Song Y, Dias-Santagata D, Lifshits E, et al.Preexistence and clonal selection of MET amplification in EGFR mutantNSCLC. Cancer Cell 2010;17:77–88.
10. Bean J, Brennan C, Shih JY, Riely G, Viale A, Wang L, et al. MET ampli-fication occurs with or without T790M mutations in EGFR mutant lungtumors with acquired resistance to gefitinib or erlotinib. Proc Natl Acad SciU S A 2007;104:20932–7.
11. Jiang SX, YamashitaK, YamamotoM, PiaoCJ,UmezawaA, SaegusaM, et al.EGFR genetic heterogeneity of nonsmall cell lung cancers contributing toacquired gefitinib resistance. Int J Cancer 2008;123:2480–6.
12. Labrijn AF, Meesters JI, de Goeij BE, van den Bremer ET, Neijssen J, vanKampen MD, et al. Efficient generation of stable bispecific IgG1 bycontrolled Fab-arm exchange. ProcNatl Acad Sci U S A 2013;110:5145–50.
13. Labrijn AF, Meesters JI, Priem P, de Jong RN, van den Bremer ET, vanKampen MD, et al. Controlled Fab-arm exchange for the generation ofstable bispecific IgG1. Nat Protoc 2014;9:2450–63.
14. Satoh M, Iida S, Shitara K. Non-fucosylated therapeutic antibodies asnext-generation therapeutic antibodies. Expert Opin Biol Ther 2006;6:1161–73.
15. Lammerts van Bueren JJ, Bleeker WK, Br€annstr€om A, von Euler A, JanssonM, Peipp M, et al. The antibody zalutumumab inhibits epidermal growthfactor receptor signaling by limiting intra- and intermolecular flexibility.Proc Natl Acad Sci U S A 2008;105:6109–14.
16. Li S, Schmitz KR, Jeffrey PD, Wiltzius JJ, Kussie P, Ferguson KM. Structuralbasis for inhibition of the epidermal growth factor receptor by cetuximab.Cancer Cell 2005;7:301–11.
17. Voigt M, Braig F, G€othel M, Schulte A, Lamszus K, Bokemeyer C, et al.Functional dissection of the epidermal growth factor receptorepitopes targeted by panitumumab and cetuximab. Neoplasia 2012;14:1023–31.
18. Merchant M, Ma X, Maun HR, Zheng Z, Peng J, Romero M, et al. Mono-valent antibody design and mechanism of action of onartuzumab, a METantagonist with anti-tumor activity as a therapeutic agent. Proc Natl AcadSci U S A 2013;110:E2987–96.
Cancer Res; 76(13) July 1, 2016 Cancer Research3952
Moores et al.
on May 11, 2020. © 2016 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Published OnlineFirst May 23, 2016; DOI: 10.1158/0008-5472.CAN-15-2833

19. Jarantow SW, Bushey BS, Pardinas JR, Boakye K, Lacy E, Sanders R, et al.Impact of cell-surface antigen expression on target engagement and func-tion of an EGFR x c-Met bispecific antibody. J Biol Chem 2015;290:24689–704.
20. CartronG, Dacheu L, Salles G, Solal-Celigny P, Bardos P, Colombat P, et al.Therapeutic activity of humanized anti-CD20 monoclonal antibody andpolymorphism in IgG Fc receptor FcgammaRIIIa gene. Blood 2002;99:754–8.
21. Scallon BJ, Tam SH, McCarthy SG, Cai AN, Raju TS. Higher levels ofsialylated Fc glycans in immunoglobulinGmolecules can adversely impactfunctionality. Mol Immunol 2007;44:1524–34.
22. Brezski RJ, Luongo JL, Petrone D, Ryan MH, Zhong D, Tam SH, et al.Human anti-IgG1 hinge autoantibodies reconstitute the effector functionsof proteolytically inactivated IgGs. J Immunol 2008;181:3183–92.
23. Jeffers M, Rong S, Woude GF. Hepatocyte growth factor/scatter factor-Metsignaling in tumorigenicity and invasion/metastasis. J Mol Med 1996;74:505–13.
24. Vafa O, Gilliland GL, Brezski RJ, Strake B, Wilkinson T, Lacy ER, et al. Anengineered Fc variant of an IgG eliminates all immune effector functionsvia structural perturbations. Methods 2014;65:114–26.
25. U.S. Food and Drug Administration. FDA approval information. Availablefrom: http://www.accessdata.fda.gov/drugsatfda_docs/bla/2004/125084_ERBITUX_PHARMR_P3.PDF; http://www.accessdata.fda.gov/drugsatfda_docs/nda/2006/125147s0000_PharmR.pdf.
26. Yu HA, Arcila ME, Rekhtman N, Sima CS, Zakowski MF, Pao W, et al.Analysis of tumor specimens at the time of acquired resistance to EGFR-TKItherapy in 155 patients with EGFR-mutant lung cancers. Clin Cancer Res2013;19:2240–7.
27. Thress KS, Paweletz CP, Felip E, Cho BC, Stetson D, Dougherty B, et al.Acquired EGFR C797S mutation mediates resistance to AXD9291 in non-small cell lung cancer harboring EGFR T790M. Nat Med 2015;21:560–4.
28. Planchard D, Loriot Y, Andr�e F, Gobert A, Auger N, Lacroix L, et al. EGFRindependent mechanisms of acquired resistance to AZD9291 in EGFRT790M-positive NSCLC patients. Ann Oncol 2015;26:2073–8.
29. Regales L, Gong Y, Shen R, de Stanchina E, Vivanco I, Goel A, et al. Dualtargetingof EGFR canovercome amajor drug resistancemutation inmousemodels of EGFR mutant lung cancer. J Clin Invest 2009;119:3000–10.
30. Piotrowska Z, Niederst MJ, Karlovich CA, Wakelee HA, Neal JW, Mino-Kenudson M, et al. Heterogeneity underlies the emergence of EGFR T790wild-type clones following treatment of T790M-positive cancers with athird-generation EGFR inhibitor. Cancer Discov 2015;7:713–22.
31. Zheng S,Moores S, Jarantow S, Pardinas J, ChiuM,ZhouH, et al. Cross-armbinding efficiency of an EGFR x c-Met bispecific antibody. MAbs 2016;8:551–61.
32. Janjigian YY, Smit EF, Groen HJ, Horn L, Gettinger S, Camidge DR, et al.Dual inhibition of EGFR with afatinib and cetuximab in kinase inhibitor-resistant EGFR-mutant lung cancer with and without T790M mutations.Cancer Discov 2014;4:1036–45.
www.aacrjournals.org Cancer Res; 76(13) July 1, 2016 3953
EGFR/cMet–Bispecific Ab in EGFR TKI–Resistant Lung Tumors
on May 11, 2020. © 2016 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Published OnlineFirst May 23, 2016; DOI: 10.1158/0008-5472.CAN-15-2833

2016;76:3942-3953. Published OnlineFirst May 23, 2016.Cancer Res Sheri L. Moores, Mark L. Chiu, Barbara S. Bushey, et al.
Resistant Lung Tumors−against EGFR Inhibitor A Novel Bispecific Antibody Targeting EGFR and cMet Is Effective
Updated version
10.1158/0008-5472.CAN-15-2833doi:
Access the most recent version of this article at:
Material
Supplementary
http://cancerres.aacrjournals.org/content/suppl/2016/05/21/0008-5472.CAN-15-2833.DC1
Access the most recent supplemental material at:
Cited articles
http://cancerres.aacrjournals.org/content/76/13/3942.full#ref-list-1
This article cites 31 articles, 13 of which you can access for free at:
Citing articles
http://cancerres.aacrjournals.org/content/76/13/3942.full#related-urls
This article has been cited by 5 HighWire-hosted articles. Access the articles at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications Department at
Permissions
Rightslink site. Click on "Request Permissions" which will take you to the Copyright Clearance Center's (CCC)
.http://cancerres.aacrjournals.org/content/76/13/3942To request permission to re-use all or part of this article, use this link
on May 11, 2020. © 2016 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Published OnlineFirst May 23, 2016; DOI: 10.1158/0008-5472.CAN-15-2833