Embed Size (px)
Citation preview

Available online at www.sciencedirect.com
www.elsevier.com/locate/yebeh
Epilepsy & Behavior 12 (2008) 340–346
Case Report
A noninvasive, presurgical expressive and receptive languageinvestigation in a 9-year-old epileptic boy using
near-infrared spectroscopy
Anne Gallagher a,b, Danielle Bastien a,b, Isabelle Pelletier a,b, Phetsamone Vannasing a,Alan D. Legatt c, Solomon L. Moshe c, Rana Jehle c, Lionel Carmant a,d,
Franco Lepore a,b, Renee Beland b, Maryse Lassonde a,b,*
a Centre de Recherche du Centre Hospitalier Universitaire Sainte-Justine, Montreal, QC, Canadab Centre de Recherche en Neuropsychologie et Cognition, Universite de Montreal, Montreal, QC, Canada
c Departments of Neurology, Neuroscience, and Pediatrics, Albert Einstein College of Medicine, Yeshiva University, Bronx, NY, USAd Service de Neurologie, Hopital Sainte-Justine, Montreal, QC, Canada
Received 30 August 2007; revised 2 October 2007; accepted 3 October 2007Available online 11 December 2007
Abstract
The intracarotid amobarbital test (IAT) is used for presurgical evaluation of language lateralization. However, this procedure hasmany limitations, especially in children. As an alternative to IAT, in the case described here, near-infrared spectroscopy (NIRS) was usedto investigate expressive and receptive language lateralization as part of the presurgical evaluation of a 9-year-old Yiddish-speaking boywith a probable left temporal epileptic focus. This child could not tolerate IAT or functional MRI. He underwent two NIRS recordingsessions while performing expressive and receptive language tasks. Results indicated predominantly left-sided expressive language in Bro-ca’s area with ipsilateral cortical recruitment of more posterior regions. Receptive language showed a bilateral cerebral pattern, perhapsas an expression of cerebral plasticity or compensation in this young patient. This case report illustrates that NIRS may contribute topresurgical investigation and could become a noninvasive alternative to IAT and functional MRI in determining speech lateralization inchildren.� 2007 Elsevier Inc. All rights reserved.
Keywords: Epilepsy; Surgery; Optical imaging; Intracarotid amobarbital test; Children; Speech lateralization; Cortical functional localization; Brainmapping
1. Introduction
Until recently, the intracarotid amobarbital test (IAT),or Wada test [1,2], has been the most widely used proce-dure for the exploration of language lateralization in epi-leptic patients slated for surgery. This procedure issomewhat invasive, and its validity cannot be verified bymeans of test–retest studies [3]. Moreover, the IAT does
1525-5050/$ - see front matter � 2007 Elsevier Inc. All rights reserved.
doi:10.1016/j.yebeh.2007.10.008
* Corresponding author. Present address: Departement de Psychologie,Universite de Montreal, C.P. 6128, Succusale Centre-Ville, Montreal, QC,H3C 3J7, Canada. Fax: +1 514 343 5787.
E-mail address: [email protected] (M. Lassonde).
not provide precise information about language localiza-tion [4], and it is constrained by the variability of the timingof sodium amytal action [5]. The patients’ altered level ofconsciousness and their behavioral and emotional reactionscan also obscure the results obtained through this tech-nique [6]. Finally, the technique is difficult to apply toyoung children [7] and in patients with mental retardationand language and/or behavior problems [8]. This is animportant limitation because half of epileptic children havecognitive or behavioral problems [9] and also because earlysurgical intervention is crucial in many cases. Clinical evi-dence suggests that the younger the child, the more effectivethe epilepsy surgery [10].

Case Report / Epilepsy & Behavior 12 (2008) 340–346 341
To find noninvasive alternatives to IAT, recent imagingtechniques such as functional magnetic resonance imaging(fMRI) and magnetoencephalography (MEG) have beenused to investigate language dominance [11,12]. However,as with IAT, these techniques are sometimes difficult touse in young children and in patients with serious cognitiveor behavioral problems. Near-infrared spectroscopy(NIRS) is a noninvasive functional imaging technique thatcan easily be applied in pediatric and cognitively limitedpatients [i.e., 13]. NIRS, a relatively new technique, allowsthe measurement of hemodynamic changes associated withneural activity [14]. The different light absorption spectraof oxyhemoglobin (HbO) and deoxyhemoglobin (HbR)within the near-infrared spectrum allow for the measure-ment of concentration changes of these substances in livingtissues [15,16]. Near-infrared light of two wavelengthsbetween 680 and 1000 nm is directed through optic fibersto the head of the patient. The amount of light detectedreflects the amount of absorption of the two wavelengthsin targeted cerebral areas [for review, see 17].
This technique has several advantages over other imag-ing methods [17–19]. First, it allows independent measure-ment of concentration changes of HbO and HbR, as well asmeasurement of total hemoglobin (HbT), which is the sumof HbO and HbR. Second, the equipment is portable[20,21] and less costly than that for fMRI or MEG. Finally,and most importantly, there are no major restrictions onmovements or verbalization during recording, which ren-ders the technique suitable for studies in mentally chal-lenged people, as well as in young children, even infants[13].
Previous work suggested that NIRS may be used toexplore expressive language lateralization in adults [22–25] and in epileptic children [26]. However, for a completelanguage lateralization investigation, presurgical assess-ment should provide information not only about expres-sive, but also about receptive language processing. In anintact brain, expressive language and receptive languageare associated with different cerebral areas: Broca’s areaand Wernicke’s area respectively. Thus, each type of lan-guage (expressive and receptive) may be subject to differentfunctional reorganization patterns that could significantlyinfluence postsurgical cognitive and communicative out-come if not taken into account. To our knowledge, nostudy has yet employed NIRS to determine receptive lan-guage lateralization in epileptic children. The present workconstitutes the first attempt to use NIRS to investigate bothexpressive and receptive language processing in a youngepileptic child whose language organization could not beevaluated with other noninvasive techniques.
2. Case report
The patient is a 9-year-old boy with a history of intrac-table seizures. The family history includes two cousins onthe father’s side who have been diagnosed with tuberoussclerosis and one relative on the mother’s side who had a
seizure at the age of 34. However, the patient is the productof a normal pregnancy, labor, and delivery, and had nor-mal developmental milestones. Genetic testing revealedthat he does not have tuberous sclerosis and is not a car-rier. Seizures started at age 5, and were characterized byright facial twitching and staring to the left, followed byclonic movements of the right upper, rather than the lower,extremity, as well as automatisms. Multiple antiepilepticdrugs failed to control seizures. Interictal electroencepha-lography (EEG) revealed left frontal and left temporalspikes. Seizures captured during video/EEG monitoringusing scalp and sphenoidal electrodes had left anterior tem-poral onsets. Brain magnetic resonance imaging (MRI)revealed left-sided cortical atrophy involving predomi-nantly the frontal lobe and abnormal hyperintense signalin the left frontal subcortical white matter. Ictal and inter-ictal single-photon emission computed tomography(SPECT) scans suggested changes within the left temporallobe related to seizures. A positron emission tomography(PET) scan showed hypometabolism in the left hemisphere,most prominent in the left temporal region.
The patient’s first language is Yiddish, and he also haslimited English skills. He does not have any knowledgeof other languages. Neuropsychological assessment per-formed in English was inconclusive because of the languagebarrier. The IAT, which included an object naming taskand a verbal command task, was also inconclusive as thechild was uncooperative, but these tasks suggested thatthere was language representation in the left hemisphere.Finally, only limited functional assessment of languagecould be carried out using fMRI. No response wasachieved during a picture-naming task, possibly due tothe patient’s inability to understand the task’s instructions.However, a word listening task was also administered tothe patient during fMRI, and the results demonstratedright-greater-than-left bilateral activation in primary audi-tory cortex, in parts of the superior temporal plane poster-ior to this cortex, and in the frontal operculum.Consequently, neuropsychological, IAT, and fMRI datawere inconclusive. Because the patient’s epileptic focuswas in the left anterior temporal region, the issue of lan-guage lateralization had to be addressed more preciselybefore surgery. To do so, the patient underwent NIRS toassess his functional expressive and receptive languageorganization, and to evaluate the potential of this noninva-sive technique to assess language lateralization in thisyoung patient with whom conventional techniques hadfailed.
3. Methods
The patient underwent two NIRS recording sessions, during which heperformed language tasks on two consecutive days. One hundred andtwenty-eight NIRS channels (64 channels on the left hemisphere and 64channels on the right hemisphere, 8 detectors, and 16 multiplexed chan-nel–source–detector combinations) placed over cerebral regions that areknown to be related to language functions (Broca’s and Wernicke’s areas,as well as right homologous regions) were recorded using a multichannel

342 Case Report / Epilepsy & Behavior 12 (2008) 340–346
Imagent Tissue Oxymeter (ISS Inc., Champaign, IL, USA). This oxymeteris composed of 32 sources operating at 690 nm, 32 sources operating at830 nm (sources are laser diodes with a power of �1 mW, connected tothe head by 0.4-mm fibers), and 8 detectors (photomultiplier tubes con-nected to the head by 3-mm fiber bundles). Two light wavelengths in thenear-infrared range were used to decompose the signal into HbO andHbR changes using a spectroscopic approach. Hence, 830-nm light is moreabsorbed by HbO, whereas 690-nm light is more absorbed by HbR, allow-ing quantification of both substances. The optical fibers were placed on thesurface of the head, using a light but rigid helmet, which was comfortablyfitted to the child’s head size without restricting head movements. Thesource–detector distance was held constant between 2.5 and 5 cm. A fre-quency-domain time-resolved method was used; light sources varied inintensity over time at 110 MHz, thus providing a precise quantificationof HbO and HbR concentrations. Optical intensity (DC), modulationamplitude (AC), and phase data were sampled at 39.0625 Hz and acquiredin a block design paradigm. DC and AC data were filtered using a low-pass filter of 0.34 Hz, normalized by dividing each value by the mean valueacross time points for each block and channel and pulse corrected [27].Channels were selected based on the standard error of phase variationsacross trials, which eliminates ‘‘noisy’’ channels, whose source–detectordistance is too large to detect higher levels of illumination. Forty usablechannels were recorded in each hemisphere. Data were then averaged byblocks (10 for each task) and transformed to quantify concentrationchanges in HbO and HbR for each channel. A language laterality index(LI) was calculated for each task by using the formula LI = (L � R)/
Fig. 1. (a) Ten-block-averaged time course including baseline (�30 to 0 secondtask (60 to 90 seconds), and resting period (90 to 105 seconds). The graph illuBroca’s and Wernicke’s areas (blue lines), characterized by an increase in HbO (more pronounced in the verbal fluency task than in the control task. A typicalThis hemoglobin pattern is characterized by a first and longer activation peakipeaking at 52 seconds (see pink arrow). A similar hemoglobin pattern is also obHbR data obtained from all channels placed over these regions. It is noteworHbO (peak at 25 seconds) followed by a cerebral activation occurring at 52 secowith the language task in the left hemisphere occurred around 27 secondscalculated at this time (orange vertical line). The pink arrow indicates that theoccurred around 52 seconds after baseline. (b) Three-dimensional reconstructitypically shown on a three-dimensional map because it reflects the addition ofthe same brain reconstruction. Top: The left view reveals an increase in HbT inregion during activation period: between 25 and 45 seconds). Bottom: Increasechannels covering this region during activation period: between 45 and 60 sec
(L + R), where L is the maximal increase in HbO associated with theexpressive or receptive language task, obtained from an averaged curveof all 40 channels covering left Broca’s and Wernicke’s areas. It is calcu-lated with the analysis software by averaging all 20 HbO values togetherand all 20 HbR values together at each time point. Using the same calcu-lation, R is the HbO value obtained from an average curve of all 40 chan-nels covering the right mirror regions of left Broca’s and Wernicke’s areasmeasured at the same time as the maximal left increase in HbO. MaximalHbO values were taken from the left hemisphere data because amplitudeof maximal HbO values was higher in the left hemisphere and occurredprior, compared with the right hemisphere, in both tasks (see Figs. 1and 2). The LI ranges from �1 to 1, where a negative value (�1 to�0.26) indicates right language lateralization, and a positive value (0.26to 1) indicates left language dominance. Finally, a value between �0.25and 0.25 inclusively is considered to reflect bilateral language lateraliza-tion. An anatomically specific setup was created based on MRI of thepatient to ensure that optical fibers were placed over the regions of interest(ROI). This was done using a stereotaxic system (Brainsight Frameless 39,Rogue Research, Canada), which enabled the transfer of ROI, determinedby MRI, onto the helmet. The location of each optical fiber and four fidu-cial points was digitized and recorded by means of the same stereotaxicsystem to allow for precise alignment between the NIRS and anatomicaldata of the patient. The same setup was used in both NIRS sessions.
To investigate language lateralization, the patient performed anexpressive language task (first session) as well as a receptive language task(second session) during NIRS. Because he communicates exclusively in
), language task (0 to 30 seconds), resting period (30 to 60 seconds), controlstrates hemoglobin data from an average of all channels covering the leftthick line) and a small decrease in HbR (thin line) in these cerebral regions,initial dip (short reduction in HbO) is also obtained before the activation.ng at 27 seconds (see blue arrow), followed by a second shorter activationserved in the mirror counterparts (pink lines) from an average of HbO andthy that the latter pattern is characterized by a first very small increase innds. The blue arrow indicates that the maximal increase in HbO associatedafter baseline (5.19 lmol). The expressive language laterality index wasmaximal increase in HbO elicited by the same task in the right hemisphereons of the patient’s MRI on which HbT data are projected. HbT data areHbO and HbR data, which cannot be clearly displayed simultaneously onBroca’s and Wernicke’s areas (average data from all channels covering thisin HbT is also observed in right homologous regions (average data from allonds), but at a lower amplitude.
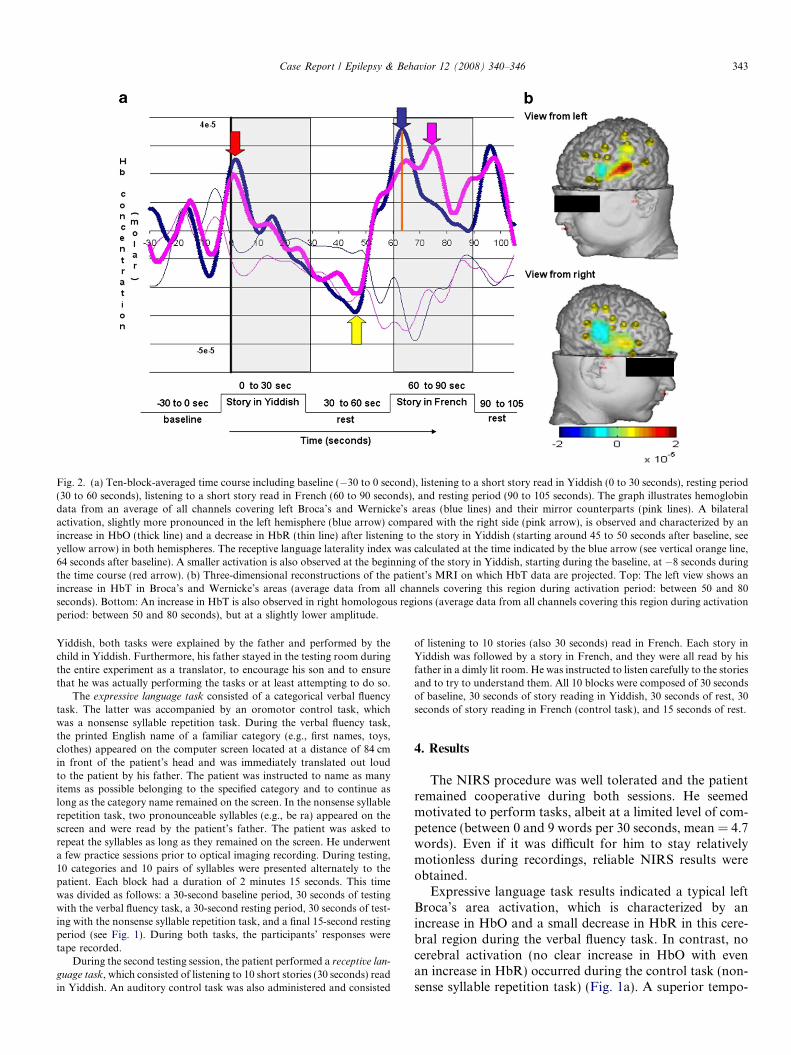
Fig. 2. (a) Ten-block-averaged time course including baseline (�30 to 0 second), listening to a short story read in Yiddish (0 to 30 seconds), resting period(30 to 60 seconds), listening to a short story read in French (60 to 90 seconds), and resting period (90 to 105 seconds). The graph illustrates hemoglobindata from an average of all channels covering left Broca’s and Wernicke’s areas (blue lines) and their mirror counterparts (pink lines). A bilateralactivation, slightly more pronounced in the left hemisphere (blue arrow) compared with the right side (pink arrow), is observed and characterized by anincrease in HbO (thick line) and a decrease in HbR (thin line) after listening to the story in Yiddish (starting around 45 to 50 seconds after baseline, seeyellow arrow) in both hemispheres. The receptive language laterality index was calculated at the time indicated by the blue arrow (see vertical orange line,64 seconds after baseline). A smaller activation is also observed at the beginning of the story in Yiddish, starting during the baseline, at �8 seconds duringthe time course (red arrow). (b) Three-dimensional reconstructions of the patient’s MRI on which HbT data are projected. Top: The left view shows anincrease in HbT in Broca’s and Wernicke’s areas (average data from all channels covering this region during activation period: between 50 and 80seconds). Bottom: An increase in HbT is also observed in right homologous regions (average data from all channels covering this region during activationperiod: between 50 and 80 seconds), but at a slightly lower amplitude.
Case Report / Epilepsy & Behavior 12 (2008) 340–346 343
Yiddish, both tasks were explained by the father and performed by thechild in Yiddish. Furthermore, his father stayed in the testing room duringthe entire experiment as a translator, to encourage his son and to ensurethat he was actually performing the tasks or at least attempting to do so.
The expressive language task consisted of a categorical verbal fluencytask. The latter was accompanied by an oromotor control task, whichwas a nonsense syllable repetition task. During the verbal fluency task,the printed English name of a familiar category (e.g., first names, toys,clothes) appeared on the computer screen located at a distance of 84 cmin front of the patient’s head and was immediately translated out loudto the patient by his father. The patient was instructed to name as manyitems as possible belonging to the specified category and to continue aslong as the category name remained on the screen. In the nonsense syllablerepetition task, two pronounceable syllables (e.g., be ra) appeared on thescreen and were read by the patient’s father. The patient was asked torepeat the syllables as long as they remained on the screen. He underwenta few practice sessions prior to optical imaging recording. During testing,10 categories and 10 pairs of syllables were presented alternately to thepatient. Each block had a duration of 2 minutes 15 seconds. This timewas divided as follows: a 30-second baseline period, 30 seconds of testingwith the verbal fluency task, a 30-second resting period, 30 seconds of test-ing with the nonsense syllable repetition task, and a final 15-second restingperiod (see Fig. 1). During both tasks, the participants’ responses weretape recorded.
During the second testing session, the patient performed a receptive lan-
guage task, which consisted of listening to 10 short stories (30 seconds) readin Yiddish. An auditory control task was also administered and consisted
of listening to 10 stories (also 30 seconds) read in French. Each story inYiddish was followed by a story in French, and they were all read by hisfather in a dimly lit room. He was instructed to listen carefully to the storiesand to try to understand them. All 10 blocks were composed of 30 secondsof baseline, 30 seconds of story reading in Yiddish, 30 seconds of rest, 30seconds of story reading in French (control task), and 15 seconds of rest.
4. Results
The NIRS procedure was well tolerated and the patientremained cooperative during both sessions. He seemedmotivated to perform tasks, albeit at a limited level of com-petence (between 0 and 9 words per 30 seconds, mean = 4.7words). Even if it was difficult for him to stay relativelymotionless during recordings, reliable NIRS results wereobtained.
Expressive language task results indicated a typical leftBroca’s area activation, which is characterized by anincrease in HbO and a small decrease in HbR in this cere-bral region during the verbal fluency task. In contrast, nocerebral activation (no clear increase in HbO with evenan increase in HbR) occurred during the control task (non-sense syllable repetition task) (Fig. 1a). A superior tempo-

344 Case Report / Epilepsy & Behavior 12 (2008) 340–346
ral gyrus (Wernicke’s area) activation, extending posteri-orly, was also measured during the fluency task, but at alower intensity than the Broca’s area activation (Fig. 1b).However, the temporal evolution of activations in Broca’sand Wernicke’s areas was similar (see legend to Fig. 1). TheHbO pattern in their mirror image counterparts in the righthemisphere (Fig. 1a, pink curve) followed that observed inthe left hemisphere (Fig. 1a, blue curve): a first activationduring the language task (Fig. 1a, blue arrow) followed25 seconds later by a second peak (Fig. 1a, pink arrow,in the first rest period). However, the first activation wasmuch more pronounced in the left hemisphere than in theright, whereas the second peak was similar in both hemi-spheres. The maximal increase in HbO obtained from anaverage of all 40 channels covering left Broca’s and Wer-nicke’s areas was recorded 27 seconds after baseline andhad a value of 5.19 lmol, whereas the value measured atthe same time from an average of all 40 channels coveringright mirror regions of left Broca’s and Wernicke’s areaswas 1.17 lmol. The expressive language laterality index,(5.19–1.17)/(5.19 + 1.17) = 0.63, suggested left hemisphericlanguage representation.
Results from the receptive language task revealed simul-taneous activation of Wernicke’s and Broca’s areas andtheir corresponding areas on the right side. As indicatedin Fig. 2, enhanced HbO and reduced HbR concentrationswere seen in the left and right superior temporal gyri, aswell as in Broca’s area and its right homologous region.A first small cerebral activation was measured at the begin-ning of the story in Yiddish, starting during the baseline ataround �8 seconds. A second more pronounced activationwas also observed following the story in Yiddish. It is note-worthy that temporally, this cerebral activation startedbetween both stories (Yiddish and French) at around 45seconds and ended during the reading in French. One-tenth-hertz activity was also noted in HbO and HbR dataduring the whole time course. Pilot studies conducted inour laboratory on healthy adults using the same receptivetask but administered in French (language condition) andscrambled French (control condition) indicated an analo-gous temporal pattern of activation, but spatially, the acti-vation remained limited to the left side, in Wernicke’s area.As in these pilot studies, the receptive language lateraliza-tion index was calculated from the most prominent activa-tion 4 seconds after the beginning of the French story (seeFig. 2a, blue arrow), but here it showed bilateral receptivelanguage representation, (3.58 – 2.47)/(3.58 + 2.47) = 0.18.
After the NIRS sessions had been completed, arrays ofsubdural grid and strip electrodes were implanted over theleft frontal, temporal, and parietal lobes. Implanted elec-trodes were stimulated while the patient was performing lan-guage tasks (naming pictures and counting). Resultsindicated language localization in Broca’s area, as speecharrest or marked slowing of speech was produced by electri-cal stimulation of this area. The patient was able to speakduring electrical stimulation of electrodes in the anteriortemporal lobe. The presence of eloquent cortex in the poster-
ior part of the superior temporal gyrus (Wernicke’s area)could not be demonstrated because stimulation there pro-duced an intense sensation of nausea. There were noimplanted electrodes on the right side. Nine seizures werecaptured during video/EEG monitoring using the implantedelectrodes. Eight of them had left temporal lobe EEG onsets;one had a possible orbitofrontal EEG onset. A left temporallobectomy including hippocampo-amygdalectomy was per-formed. Pathological examination of the resected left tempo-ral lobe tissue revealed gliosis and focal cortical dysplasiatype IA [28]. Postoperatively there was no change in lan-guage function. Seizures were decreased in frequency, butthe patient did not become completely seizure free.
5. Discussion
The aim of the present work was to investigate expres-sive and receptive language lateralization in a young Yid-dish-speaking epileptic child with whom otherinvestigating techniques had failed. Contrary to IAT andfMRI, NIRS was well tolerated by this 9-year-old boy,who stayed cooperative during the entire procedure. Hekept moving around for the major part of the NIRSrecordings; however clear and reliable data were collected.
Results from the expressive language task demonstratedactivation of left Broca’s and Wernicke’s areas. A right acti-vation in the homologous areas was also obtained but at amuch lower intensity. A second activation occurring 25 sec-onds after the first left activation was also measured in bothhemispheres. In neurologically intact individuals, verbal flu-ency tasks typically recruit the left Broca’s area, which hasbeen associated with expressive language [29]. Our patientalso showed such a frontal activation pattern during wordproduction, a result that was confirmed by electrical stimu-lation of implanted electrodes. However, the word fluencytask also elicited activation of the left Wernicke’s area.Cerebral reorganization can occur following brain damage,especially in younger and impaired patients. In the presentcase, the left frontal atrophy seen on the MRI scan mayhave induced a reorganization of speech production net-works. Thus, recruitment of the left superior temporal gyrusseems to have occurred through compensation or plasticityprocesses. The right hemisphere activation (second peak) inhomologous regions of Broca’s and Wernicke’s areas couldindicate the emergence of an independent language areathat would be another sign of cerebral reorganization in thisyoung epileptic patient. In fact, cerebral reorganization forexpressive language in epileptic adults and children has alsobeen reported in the few previous studies using NIRS[25,26]. We ourselves [26] have previously reported a bilat-eral speech lateralization profile in a 9-year child also pre-senting with left temporal lobe epilepsy.
Story listening paradigms have been used in fMRI toassess receptive language lateralization in adults [30–32]and children [33,34]. Such paradigms are easy to use withpediatric and mentally impaired patients. In neurologicallyintact individuals, this task is typically associated with acti-

Case Report / Epilepsy & Behavior 12 (2008) 340–346 345
vation of a left Wernicke’s area [35]. Our patient’s resultsindicate a bilateral pattern of activation involving bothanterior and posterior regions. The left anterior temporalfocus in this participant may have forced reorganizationby extending the receptive language region from the leftWernicke’s area to more anterior ipsilateral regions (Bro-ca’s areas) as well as to their right homologous regions(superior temporal gyrus and inferofrontal regions). Thispattern of activation may again suggest that compensationoccurred through plasticity. Alternately, it is possible thatthe very nature of the task, which proved to be difficultfor this child, may have elicited a more extended recruit-ment of cerebral regions. Such a cerebral reorganizationpattern of recruitment has previously been reported in Alz-heimer’s patients who were performing memory tasks dur-ing PET recording [36].
In the receptive paradigm, we found a first activationpeak of relatively weak amplitude starting just prior tothe beginning of the Yiddish story. The latter activationcannot be associated with the story read in Yiddish becauseit started during baseline, 8 seconds before the beginning ofthe Yiddish story. This first peak may reflect expectationfrom the patient for the beginning of the story. In fact,the main cerebral activations did not occur during the storyread in Yiddish, but started between the Yiddish andFrench stories and ended while the story was being readin French (second and third activation peaks on the graph,Fig. 2). During the reading in Yiddish the patient remainedcalm, enjoying the story. When the reader stopped, he wasprobably trying to rehearse the story and expecting thenext part of it, which was coming in the next block. Thus,the main activation (second activation peak) occurringafter the story in Yiddish should reflect the semantic inte-gration processes usually associated with Wernicke’s area,whereas the third activation peak should indicate cognitivepreparation and/or the expectation of more semantic infor-mation to come. The delay between the story in Yiddishand the cerebral activation is expected because the partici-pant needs semantic information to proceed to a linguistictreatment. This pattern of cerebral activation has previ-ously been obtained in our laboratory from pilot healthyparticipants, except that it was limited to unilateral activa-tion of the left Wernicke’s area, thus suggesting that itreflects linguistic processing.
One-tenth-hertz activity was also measured in HbO andHbR data during the entire duration of the receptive task.This activity was not observed in expressive task data. Thiscomponent can most probably be attributed to Mayerphysiological activity. Mayer waves are described as oscil-lations of arterial pressure occurring spontaneously inhumans at �0.1 Hz [for reviews, see 37,38]. This physiolog-ical noise still constitutes a challenge in NIRS data analysisbecause it cannot be properly filtered considering its similarfrequency to the optical signal. The physiological mecha-nism inducing Mayer waves is not completely understoodyet, but it has been reported that these waves’ amplitudeand frequency are not constant in time, are dependent on
the individual, and can vary between tasks [37,38]. All thesefactors contribute to the difficulty in eliminating Mayerwaves. Task differences may explain why we did notobserve Mayer waves during the expressive task when thepatient was more active compared with the receptive task,which is a passive protocol. However, in the present study,this component does not significantly interfere with theinterpretation of the data because the amplitude of themeasured cerebral activations is superior to that of theMayer waves.
Finally, even though there were significant languagebarriers with this patient and he was moving during record-ings, reliable data were obtained using NIRS, allowing theassessment of expressive and receptive language organiza-tion patterns in this young boy. Data suggest that NIRSis a useful technique for pediatric and mentally challengedpatients. Replication in larger populations could lead toNIRS becoming a noninvasive alternative to IAT, andcould also serve as guidance for further investigations oflanguage using implanted electrodes.
Acknowledgments
We are grateful to Martin Theriault for programmingstimulus presentation and to Julie Tremblay for helpingin NIRS data analyses. We are also indebted to the engi-neering and orthotic prosthesis team of the Sainte-JustineUniversity Hospital Center for their help in developingthe optical imaging helmet.
This work was supported by funds from the Canada Re-search Chair in Developmental Neuropsychology held byDr. Maryse Lassonde; the Canada Research Chair in Cog-nitive Neurosciences held by Dr. Franco Lepore; researchgrants by the Fonds de la Recherche en Sante du Quebec(FRSQ), the Natural Sciences and Engineering ResearchCouncil of Canada (NSERC), awarded to Maryse Las-sonde and Franco Lepore, the Social Sciences and Human-ities Research Council of Canada (SSHRC), and the FondQuebecois de la Recherche sur la Nature et les Technolo-gies (RQRNT) awarded to Renee Beland; as well as schol-arships from the Canadian Institutes of Health Research(CIHR), the Canadian Federation of University Women(CFUW), and the Fonds de la Recherche en Sante du Que-bec (FRSQ) awarded to Anne Gallagher, M.Ps.
References
[1] Wada J, Rasmussen T. Intracarotid injection of sodium amytal forthe lateralization of cerebral speech dominance: Experimental andclinical observations. J Neurosurg 1960;17:266–82.
[2] Rutten GJM, Ramsey NF, Van Rijen PC, Alpherts WC, Van VeelenWM. fMRI-determined language lateralization in patients withunilateral or mixed language dominance according to the Wada test.NeuroImage 2002;17:447–60.
[3] Boas WVE, Juhn A. Wada and the sodium amytal test; the first (andlast?) 50 years. J Hist Neurosci 1999;8:286–92.
[4] Gaillard WD, Bookheimer SY, Hertz-Pannier L, Blaxton TA. Thenon-invasive identification of language function. Neurosurg ClinNorth Am 1997;8:321–35.

346 Case Report / Epilepsy & Behavior 12 (2008) 340–346
[5] Bouwer MS, Jones-Gotman M, Gotman J. Duration of sodiumamytal effect: Behavioral and EEG measures. Epilepsia 1993;34:61–8.
[6] Trenerry MR, Loring DW. Intracarotid amobarbital procedure. TheWada test. Neuroimaging Clin North Am 1995;5:721–8.
[7] Williams J, Rausch R. Factors in children that predict performanceon the intracarotid amobarbital procedure. Epilepsia1992;33:1036–41.
[8] Pelletier I, Sauerwein HC, Lepore F, Saint-Amour D, Lassonde M.Non-invasive alternatives to the Wada test in the presurgicalevaluation of language and memory functions in epilepsy patients.Epileptic Disord 2007;9:111–26.
[9] Jambaque I, Lassonde M, Dulac O, editors. Neuropsychology ofchildhood epilepsy. New York: KluwerAcademic/Plenum; 2001.
[10] Engel J, editor. Surgical treatment of the epilepsies. New York: Ra-ven Press; 1987.
[11] Gaillard WD, Balsamo L, Xu B, et al. fMRI language task panelimproves determination of language dominance. Neurology2004;63:1403–8.
[12] Papanicolaou AC, Simos PG, Castillo EM, et al. Magnetocephalog-raphy: A non-invasive alternative to the Wada procedure. J Neuro-surg 2004;100:867–76.
[13] Wilcox T, Bortfeld H, Woods R, Wruck E, Boas DA. Using near-infrared spectroscopy to assess neural activation during objectprocessing in infants. J Biomed Opt 2005;10:11010.
[14] Villringer A, Plank J, Hock C, Schleinkofer L, Dirnagl U. Nearinfrared spectroscopy (NIRS): a new tool to study hemodynamicchanges during activation of brain function in adults. Neurosci Lett1993;154:101–4.
[15] Gratton G, Fabiani M. Optical imaging of brain function. In:Parasuraman R, Rizzo M, editors. Neuroergonomics: the brain atwork. Cambridge, MA: Oxford Univ. Press; 2007. p. 65–81.
[16] Boas DA, Gaudette T, Strangman G, Cheng X, Marota JJA,Mandeville JB. The accuracy of near infrared spectroscopy andimaging during focal changes in cerebral hemodynamics. NeuroIm-age 2001;10:76–90.
[17] Villringer A, Chance B. Non-invasive optical spectroscopy andimaging of human brain function. Trends Neurosci 1997;20:435–42.
[18] Gratton G, Fabiani M. Shedding light on brain function: the event-related optical signal. Trends Cogn Sci 2001;5:357–63.
[19] Gratton G, Fabiani M. The event-related optical signal: A new toolfor studying brain function. Int J Psychophysiol 2001;42:109–21.
[20] Hintz SR, Benaron DA, Siegel AM, Zourabian A, Stevenson DK,Boas DA. Bedside functional imaging of the premature infant brainduring passive motor activation. J Prenat Med 2001;29:335–43.
[21] Liebert A, Wabnitz H, Steinbrink J, et al. Bed-side assessment ofcerebral perfusion in stroke patients based on optical monitoring of adye bolus by time-resolved diffuse reflectance. NeuroImage2006;24:426–35.
[22] Watanabe E, Maki A, Kawaguchi F, et al. Non-invasive assessmentof language dominance with near-infrared spectroscopy mapping.Neurosci Lett 1998;256:49–52.
[23] Kennan RP, Kim D, Maki A, Koizumi H, Constable RT. Non-invasive assessment of language lateralization by transcranial near-infrared optical topography and functional MRI. Hum Brain Mapp2002;16:183–9.
[24] Noguchi Y, Takeuchi T, Sakai KL. Lateralized activation in theinferior frontal cortex during syntactic processing: event-relatedoptical topography study. Hum Brain Mapp 2002;17:89–99.
[25] Watson NF, Dodrill C, Farrell D, Holmes MD, Miller JW.Determination of language dominance with near-infrared spectros-copy: comparison with the intracarotid amobarbital procedure.Seizure 2004;13:399–402.
[26] Gallagher A, Theriault M, Maclin E, et al. Near-infrared spectros-copy as an alternative to the Wada test for language mapping inchildren, adults and special populations. Epileptic Disord2007;9(3):141–55.
[27] Gratton G, Corballis PM. Removing the heart from the brain:Compensation for the pulse artefact in the photon migration signal.Psychophysiology 1995;32:292–9.
[28] Palmini A, Najm I, Avanzini G, et al. Terminology and classificationof the cortical dysplasias. Neurology 2004;62(Suppl. 3):S2–8.
[29] Lurito JT, Dzemidzic M. Determination of cerebral hemispherelanguage dominance with functional magnetic resonance imaging.Neuroimaging Clin North Am 2001;11:355–63.
[30] Lehericy S, Cohen L, Bazin B, et al. Functional MR evaluation oftemporal and frontal language dominance compared with the Wadatest. Neurology 2000;54:1625–33.
[31] Lurito JT, Lowe MJ, Sartorius C, Mathews VP. Comparison offMRI and intraoperative direct cortical stimulation in localization ofreceptive language areas. J Comput Assist Tomogr 2000;24:99–105.
[32] Schlosser MJ, Luby M, Spencer DD, Awad IA, McCarthy G.Comparative localization of auditory comprehension by usingfunctional magnetic resonance imaging and cortical stimulation. JNeurosurg 1999;91:626–35.
[33] Ahmad Z, Balsamo LM, Sachs BC, Xu B, Gaillard WD. Auditorycomprehension of language in young children: neural networksidentified with fMRI. Neurology 2003;60:1598–605.
[34] Hertz-Pannier L, Chiron C, van de Moortele PF, et al. Multi-taskfMRI presurgical language mapping in children with cognitiveimpairment. Paper presented at the Fifth International Conferenceon Functional Mapping of the Human Brain, Germany, 1999.
[35] Schlosser MJ, Aoyagi N, Fulbright RK, Gore JC, McCarthy G.Functional MRI studies of auditory comprehension. Hum BrainMapp 1998;6:1–13.
[36] Desgranges B, Baron JC, de la Sayette V, et al. The neural substratesof memory systems impairment in Alzheimer’s disease. Brain1998;121:611–31.
[37] Julien C. The enigma of Mayer waves: Facts and models. CardiovascRes 2006;70:12–21.
[38] Obrig H, Neufang M, Wenzel R, et al. Spontaneous low frequencyoscillations of cerebral hemodynamics and metabolism in humanadults. NeuroImage 2000;12:623–39.