Embed Size (px)
Citation preview

1
A non-interventional, multi-center observational study of Nilotinib in patients with chronic or accelerated phase Philadelphia chromosome
positiVe (Ph+) chronic myElogenous Leukemia with resistance or intolerance to Imatinib mesylate,
(NOVEL) Study in Taiwan - Interim Analysis 2010-07-27~2014-01-07
Data cut-off date: 20-Nov-2012
Ching-Yuan Kuo1, Po-Nan Wang2, Wen-Li Hwang3, Cheng-Hwai Tzeng4, Jih-Luh Tang5,
Li-Yaun Bai6, Ming-Chih Chang7, Yeu-Chin Chen8, Tsai-Yun Chen9, Sheng-Fung Lin10,
Tran-Der Tan11, Cheng-Shyong Chang12 郭景元1, 王博南2, 黃文豊3, 曾成槐4, 唐季祿5, 白禮源6, 張明志7, 陳宇欽8, 陳彩雲9,
林勝豐10, 譚傳德11, 張正雄12
1Kaohsiung Chang Gung Memorial Hospital, 2Linkou Chang Gung Memorial Hospital, 3Taichung Veterans General Hospital, 4Taipei Veteran General Hospital, 5National Taiwan University Hospital, 6 China Medical University Hospital, 7Mackay
Memorial Hospital, 8Tri-Service General Hospital, 9National Cheng Kung University Hospital, 10Kaohsiung Medical University
Chung-Ho Memorial Hospital, 11Koo Foundation Sun Yat-Sen Cancer Center, 12Changhua Christian Hospital
1.高雄長庚醫院 2.林口長庚醫院 3.台中榮民總醫院 4.台北榮民總醫院 5.台灣大學附設醫院 6.中國醫藥大學附設醫院 7.馬偕醫院 8.三軍總醫院 9.成功大學附設醫院 10.高雄醫學大學附設醫院 11.彰化基督教醫院

2
Study design
• Observational
• Non-interventional
• Post marketing surveillance
• Single-arm
• Multi-center:
– 12 centers
• Sample size:
– Enrolled: 85 subjects
– ITT population: 85 subjects

3
Objective
Primary objective
• To collect long-term safety data of nilotinib treatment in chronic phase or accelerated phase Ph+ CML patients during routine clinical practice.
Secondary objective
• To observe efficacy data such as hematological, cytogenetic and molecular response data in nilotinib treated patients.
4
Inclusion Criteria
• Adult male or female patients (18 years of age) with confirmed Ph+ chromosome (or Bcr-Abl) CML in chronic or accelerated phase.
• Resistance or intolerance to at least one prior CML therapy including imatinib (Glivec®). These patients should meet disease/resistance or intolerance criteria already described above.
OR CML patients who have been treated previously with a 2nd
generation tyrosine kinase inhibitor (ex. nilotinib, dasatinib, etc) who otherwise meet the definition of imatinib-resistance or intolerance are eligible.
• ECOG Performance status 0, 1, or 2. • Ability to understand and willingness to give informed consent
to participate in the study.
5
Exclusion Criteria (1/3)
1. Prior or current blast phase CML.
2. Previously documented T315I mutation.
3. Patients who have or who are at significant risk of developing prolongation of QTc, such as those.
– With congenital long QT syndrome or a known family history of long QT syndrome.
– Clinically significant resting bradycardia (< 50 beats per minute).
– myocardial infarction within 12 months prior to study entry.
– Other clinically significant uncontrolled heart disease (e.g. unstable angina, congestive heart failure or uncontrolled hypertension).
– History or presence of clinically significant ventricular or atrial tachyarrhythmias or taking anti-arrhythmic products or substances that can lead to QT prolongation and the treatment cannot be either discontinued or switched to a different medication prior to starting observational drug.

6
Exclusion Criteria (2/3)
4. Patients with hypokalemia or hypomagnesaemia must have
electrolytes corrected prior to nilotinib therapy. Other concurrent
severe and/or uncontrolled medical conditions that in the
opinion of the investigator could cause unacceptable safety risks (e.g., uncontrolled diabetes, active or uncontrolled infection, renal disease, acute or chronic pancreatitis, or impairment of gastrointestinal (GI) function or GI disease that may significantly alter the absorption of nilotinib).
5. Patients with rare hereditary problems of galactose intolerance, the Lapp lactase deficiency or glucose-galactose malabsorption.

7
Exclusion Criteria (3/3)
6. Concurrent other malignancy that is clinically significant or require active systemic intervention (except non-melanoma skin cancer, carcinoma in situ of cervix or other primary malignancy which is neither clinically significant nor requires active systemic intervention).
7. Patients who are: (a) pregnant, (b) breast feeding, (c) male or female of childbearing potential unwilling to use a reliable or effective contraceptive method(s).
8. Patients who have received prior TKIs (ex. dasatinib, etc) who had not yet recovered from side effects of such therapy prior to starting observational drug.

8
Summary recruitment by site
Site Investigator Number of Recruitment
(N=85)
1: NTUH Jih-Luh Tang 5
2. SYSCC Tran-Der Tan 2
3. VGH-TP Cheng-Hwai Tzeng 10
4. TSGH Yeu-Chin Chen 3
5. MMH Ming-Chih Chang 4
6. CGMH-LK Po-Nan Wang 15
7. VGH-TC Wen-Li Hwang 13
8. CCH Cheng-Shyong Chang 6
9. CGMH-KS Ching-Yuan Kuo 15
10. CMUH Li-Yaun Bai 5
12. NCKUH Tsai-Yun Chen 3
13. KMUH Sheng-Fung Lin 4

9
Month 15, N=55
Month 18, N=47 Month 1,
N=83
Screening/Baseline, N=85
Withdrawal (N=2) Withdrawal of consent: 1 Development of intolerable toxicities or adverse event(s): 1
Month 2, N=81
Month 3, N=79
Month 6, N=74
Month 9, N=67
Month 12, N=63
Withdrawal (N=2) Withdrawal of consent: 1 Death: 1
Withdrawal (N=5) Unsatisfactory therapeutic effect: 3 Development of intolerable toxicities or adverse event(s): 2
Ongoing, N=7
Patient Disposition (N=85) Interim analysis cutoff time point: Data cut-off date: 20 Nov 2012
Ongoing, N=5
Month 24, N=33
Month 21, N=39
Withdrawal (N=2) Withdrawal of consent: 1 Unsatisfactory therapeutic effect: 1
Withdrawal (N=5) Withdrawal of consent: 1 Unsatisfactory therapeutic effect: 3 Other: 1
Withdrawal (N=4) Death: 2 Unsatisfactory therapeutic effect: 2
Withdrawal (N=4) Unsatisfactory therapeutic effect: 3 Discontinue observational drug or switch to another drug : 1
Ongoing, N=6
Withdrawal (N=3) Death: 1 Unsatisfactory therapeutic effect: 1 Discontinue observational drug or switch to another drug : 1
Withdrawal (N=1) Pregnancy: 1
Withdrawal (N=1) Administrative problems: 1
Ongoing, N=2
Ongoing, N=4
Ongoing, N=5
• 29 patients withdrew from the study • 33 patients finished 24 months F/U
• 23 patients ongoing
(M6: 2; M12: 4; M15: 5; M18: 7; M21: 5)


11
Variables Status Overall (N=85)
Development of mutation No 26
ND 52
Type: E450G 1
Type: E543A 1
Type: F317L 1
Type: F486S 1
Type: G250E 1
Type: M244V 1
Type: M351T 1
Previous medication: Imatinib (N=85, 100%)
- Intolerance: 24 (28.2%)
- Lack of response: 59 (69.4%)
- Intolerance, Lack of response: 1 (1.2%)
- Other: 1 (1.2%)
Last treatment dose (mg/day)
Mean (SD) (Min, Median, Max)
473 (153) (200, 400, 800)
Previous medication: Dasatinib (N=19, 22.4%)
- Intolerance: 9 (47.4%)
- Lack of response: 8 (42.1%)
- Other: 2 (10.5%)
Last treatment dose (mg/day)
Mean (SD) (Min, Median, Max)
98.9 (21.9) (50, 100, 140)

29 patients withdrew from the study Type Pt No. Events or comments
Treatment failure, no progression to AP/BC
13 One developed 2 mutations: F359C & E459K; One loss of CCyR
Death 4 Cardiopulmonary failure; accident; natural death; thrombocytopenia related SAH
Disease progression 3 AP -> AML x 1; loss of CHR x 2
Toxicities 3 • AST/ALT elevation; • Increase of Bilirubin; • Hypocellular marrow with anemia & thrombocytopenia;
Withdrawal of consent 2
Suboptimal response 1
Intolerance 1
Administrative problems 1
Pregnancy 1
12

• A total of 907 AEs from 65 subjects were reported in this study
• There were 356 (39.3 %) drug-related AEs, and most of our AEs were in mild or moderate severity grades (Grade 1 + 2, 91.2%)
* mild (Grade 1, 63.2%) * moderate (Grade 2, 28%) * severe (Grade 3): 67(7.39%) * life-threatening (Grade 4): 11 (1.21%) * two deaths (Grade 5, 0.221%)
• The most common drug-related AE were “thrombocytopenia (16.5%)”, “elevated ALT (16.5%)”, ”pruritis (16.5%)”, follow by “hyperbilirubinemia (12.9%)”, “rash (11.8%)”, “anemia (10.6%)”, and “elevated AST (5.88%)”.
• The most common Grade 3/4 AEs were “Thrombocytopenia” (7.1%) and
“elevated ALT” (2.4%).
13
Adverse Events & Serious Adverse Events(1)

14
Adverse Events & Serious Adverse Events(2)
PNO. Adverse Event Severity Enrolled
Date
On-set
Date
Study
Drug
Dosage
Adjusted
Tasigna
Dosage
(mg)
Initial
Tasigna
dose
(mg)
003-001 jaundice Mild 2010-08-11 2011-03-11 1, 4, 6 800 800
012-001 palpitation Severe 2010-11-30 2010-08-08 4 800 800
Study drug dosage adjusted 0 = No action taken; 1 = Study drug dosage adjusted/ temporarily interrupted 2= Study drug permanently discontinued due to this adverse event; 3= Non drug-therapy given 4= Concomitant medication taken; 5= Non-drug therapy given; 6=Hospitalization/ Prolonged hospitalization
• Cardiovascular AEs: 26.19% with dizziness (13.1%) and palpitation (7.14%), there was only 3 documented QT interval prolongation events from one subject were noted at EKG study in our study. • Twenty-sevene serious adverse events (SAE) were reported, 2 SAEs were related to Nilotinib

15
Variable Status CHR MCyR CCyR MMR CMR
All patients (N=85)
Event No. /Total No.
(%)
83/85
(97.6%)
68/85
(80.0%)
58/85
(68.2%)
44/85
(51.8%)
8/85
(9.4%)
Median Time
(95% CI) (Months)
7.3
(5.7, 10.0)
11.0
(7.5, 15.0)
14.8
(9.5, 17.8)
18.0
(14.5, 34.9)
NA
(38.3, -)
Lack of response in
previous Imatinib
treatment (N=50)
Event No. / Total No.
(%)
50/50
(100.0%)
41/50
(82.0%)
34/50
(68.0%)
25/50
(50.0%)
5/50
(10.0%)
Median Time
(95% CI) (Months)
7.9
(6.0, 11.0)
9.5
(7.5, 15.1)
15.1
(9.0, 17.8)
18.0
(13.8, 38.3)
NA
(38.3, -)
No lack of response
in previous Imatinib
treatment
(N=25)
Event No. / Total No.
(%)
24/25
(96.0%)
20/25
(80.0%)
18/25
(72.0%)
14/25
(56.0%)
3/25
(12.0%)
Median Time
(95% CI) (Months)
5.0
(3.0, 14.5)
6.0
(3.3, 15.0)
11.0
(4.0, 18.6)
15.0
(5.4, .) NA
Log-Rank test
(Lack of response vs.
No lack of response)
P-value 0.4869 0.3125 0.3223 0.2387 0.6142
Cumulative incidences of response at data cut-off date

Patient status CHR MCyR CCyR MMR CMR
Overall response 83/85 (97.6%) 68/85 (80.0%) 58/85 (68.2%) 44/85 (51.8%) 8/85 (9.4%)
No lack of response in previous Imatinib Tx
24/25 (96.0%) 20/25 (80.0%) 18/25 (72.0%) 14/25 (56.0%) 3/25 (12.0%)
Lack of response in previous Imatinib Tx
50/50 (100.0%) 41/50 (82.0%) 34/50 (68.0%) 25/50 (50.0%) 5/50 (10.0%)
Not achieved CHR before starting of Nilotinib Tx
20/22 (90.9%) 15/22 (68.2%) 13/22 (59.1%) 12/22 (54.5%) 3/22 (13.6%)
No mutation at baseline 76/78 (97.4%) 64/78 (82.1%) 55/78 (70.5%) 41/78 (52.6%) 8/78 (10.3%)
Had mutation at baseline 7/7 (100.0%) 4/7 (57.1%) 3/7 (42.9%) 3/7 (42.9%) 0/7 (0.0%)
Lack of response in previous Imatinib and
Dasatinib Tx 3/4 (75.0%) 3/4 (75.0%) 3/4 (75.0%) 2/4 (50.0%) 0/4 (0.0%)
16

17
Overall Survival (OS) Overall patients
Overall Survival Total
Event No. / Total No. (%) 7/85 (8.2%)
Median Time (95% CI) (Months) NA (44.0, -)

18
Overall Survival (OS) By CP (N=76) and AP (N=9) phase
Overall Survival CP AP
Event No. / Total No. (%) 3/76 (3.9%) 4/9 (44.4%)
Median Time (95% CI) (Months) NA(44.0, -) 42.3(4.4, 42.3)

19
Overall Survival (OS) By response
Overall Survival CHR MCyR CCyR MMR CMR
Event No. / Total No. (%) 7/83 (8.4%) 1/68 (1.5%) 1/58 (1.7%) 1/44 (2.3%) 1/8 (12.5%)
Median Time (95% CI)
(Months) NA(44.0, -) - - - NA (21.8, -)
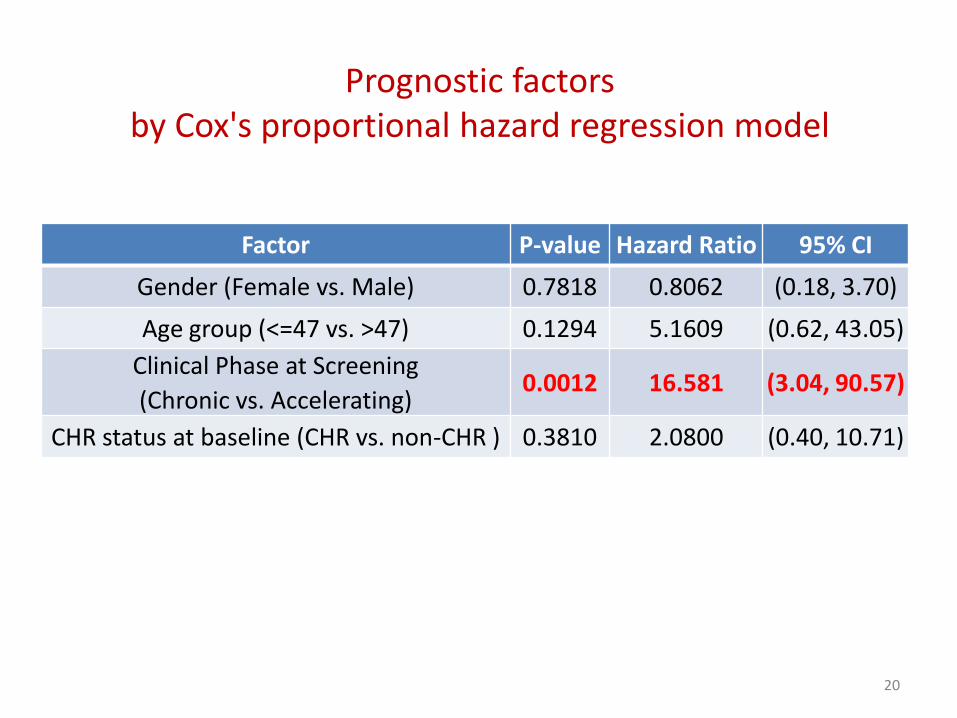
Prognostic factors by Cox's proportional hazard regression model
Factor P-value Hazard Ratio 95% CI
Gender (Female vs. Male) 0.7818 0.8062 (0.18, 3.70)
Age group (<=47 vs. >47) 0.1294 5.1609 (0.62, 43.05)
Clinical Phase at Screening
(Chronic vs. Accelerating) 0.0012 16.581 (3.04, 90.57)
CHR status at baseline (CHR vs. non-CHR ) 0.3810 2.0800 (0.40, 10.71)
20

21
Progression-Free Survival (PFS) Overall patients
Progression-Free Survival Overall Event No. / Total No. (%) 7/85 (8.2%) Median Time (95% CI) (Months) NA (42.3, -)

22
Progression-Free Survival (PFS) By CP and AP phase
Progression-Free Survival CP AP Event No. / Total No. (%) 3/76 (3.9%) 4/9 (44.4%) Median Time (95% CI) (Months) - 42.3 (4.4, 42.3)
23
• A total of 85 CML patients were included in the ITT population for analysis. There were 48 (56.5%) male patients and 37 (43.5%) female patients; The median age (min, max) was 47(21, 85) years; 76 (89.4%) subjects with chronic phase and 9 (10.6%) with accelerating phase.
• There were 29 patients withdrew from the study, 39.3 % drug-related adverse events (AEs). Most AEs were in mild or moderate severity grades (Grade 1 + 2, 91.2%). Only 11 (1.21%) had life-threatening (Grade 4) AEs. Two deaths (Grade 5, 0.221%) related to AEs were noted.
• The most common Grade 3/4 AEs were “Thrombocytopenia” (7.1%) and “elevated ALT” (2.4%).
• Only 3 documented QT interval prolongation events from one subject were noted.
Results (1)

• Cumulative incidences of response at data cut-off date were:
CHR: 97.6%, MCyR: 80%, CCyR: 68.2%, MMR: 51.8% and CMR: 9.4%.
• There were 5 patients expired during the study, two were related to study drug, the median survival time was not available. Regarding the prognostic factors by Cox's proportional hazard regression model, only the clinical phase at screening (Chronic vs. Accelerating) was statistically significant (P-value: 0.0046).
• Progression free survival (PFS): There were 7 (8.2%) of 85 patients experienced disease progression or death. For accelerated phase, there were 4 (44.4%) of 9 patients experienced disease progression or death, and the median time of progression-free survival was 42.3 months (95% CI: 4.4-42.3 months).
24
Results (2)

Conclusion
• Nilotinib is a safe, well tolerant and effective therapy for chronic or accelerated phase Ph+ CML with imatinib resistance or intolerance.
• Adverse events should be monitored closely with adequate management
Key words
Imatinib, Nilitinib, Chronic myeloid leukemia.






![Chronic Pain Update.pptx [Read-Only] · • Pain Assessment • Multi-disciplinary Approach • Updates in Management • Pharmacotherapeutic • Technological Updates • Interventional](https://img.pdfslide.us/doc/110x75/60333e3c7f60c251fc6b299e/chronic-pain-read-only-a-pain-assessment-a-multi-disciplinary-approach-a.jpg)






















