Embed Size (px)
Citation preview
A New Training Curriculum
Subpart B: Readings Only
This is a sub-manual, containing the original Table of Contents from the full manual and the readings associated with the training. Exercises are contained in the full manual, as well as Subpart A: Exercises Only.
Unit 1: Introduction
No Readings
Unit 2: A System in Flux
2.5 Reading: Deegan, P., Spirit Breaking; …page 32.6 Reading: The President’s New Freedom Commission Report, Executive Summary ...page 15
Unit 3: The Birth of the CPS Profession
3.4 Reading: Five Fundamental Rights, Massachusetts …page 243.5 Reading: Chamberlin, J. (1997) A working definition of empowerment. …page 293.6 Reading: Deegan, P. (1996) Recovery and the Conspiracy of Hope. …page 333.7 Reading: Gold, Elizabeth (2007) From Narrative Wreckage to Island of Clarity, …page 47
Unit 4: CPS In-Depth 4.4 Reading Mead, Shery, et al. Peer Support: What Makes it Unique? (Condensed Version) ...page 524.5 Reading Transcom Peer Support Update, 2012 ...page 544.6 Reading, Sample CPS Job Descriptions ...page 674.7 Reading, Power of Peer Support ...page 71 Unit 5: Supervision in the Real World
5.3 Reading: The Job Description ...page 1175.4 Reading: Jacobson, What Do Peer Support Workers Do? ...page 1205.5 References, Unit 5 ...page 144
Unit 6: Avoiding the Potholes
6.3 Reading: Concerns about Recovery ...page 1546.4 Reading: Peer Support...A Review of the Evidence ...page 160
Table of Contents


2.5 Reading, Deegan, P., “Spirit Breaking......”Deegan, Patricia: Spirit Breaking: When the Helping Professions Hurtby Patricia Deegan, Ph.D As published in The Humanistic PsychologistVolume 18(3), pp. 301-313 Autumn 1990
AbstractToo often the human services dehumanize and depersonalize those who come to receive services, as well as those professionals who provide physical disabili-ties and people with psychiatric disabilities are frequently hurt by helping pro-fessionals, the phenomenon of “spirit breaking” is introduced. Suggestions for re-humanizing the human services are made. Including new models for clinical interaction that serve to empower rather than disempower service recipients, and the contributions that people with psychiatric disabilities are making in their own state and national movements for social justice and the right to humane treat-ment and rehabilitation services.
Recently I was asked to speak with a group of graduate students in clinical psy-chology. In preparing my talk I reflected on what the most important message was I could share with these young people who would soon enter professional practice. The message I felt called to share was rather simple: People with dis-abilities are people. When we forget that people with psychiatric disabilities share a common humanity with us then the human is stripped from human services and the stage is set for the emergence of the inhuman and the inhumane. The inhuman and the inhumane emerge from that rupture which occurs when one human being fails to recognize and reverence the humanity and the fundamen-tal sanctity, sovereignty and dignity of another person. Such a rupture in mutual relatedness occurs often in the helping professions and for this reason, helping professionals sometimes hurt rather than help people with disabilities. Too often the human services dehumanize and depersonalize. Many people with disabili-ties refer to this special kind of hurt as “spirit breaking,” or “how the system tries to break your spirit.” I think we can all learn from the paper I shared with those graduate students. It went like this: Being a student is very important work. Beyond merely mastering a finite content area of study and becoming proficient in clinical practice, we also have the obligation to develop and articulate our val-ues and the ideals, which form the foundation of our clinical praxis. We must take the latter aspect of our work very seriously, because when we leave the uni-versity setting and enter the day-to-day business of clinical psychology it is very easy to become compromised in our values and ideals. It is easy to lose sight of our humanity as the common ground we share with those who come to use
for help. When we make the transition from being a student to being a profes-sional clinician, our culture and human service institutions grant us a broad range of power over the lives of people who are in distress. With that power comes enormous responsibility and great risk. Our responsibility is to never lose sight of the fundamental sanctity, dignity and sovereignty of another human being no matter what their diagnosis may be, no matter how “regressed” or “poor” their prognosis may be and no matter what their disability may be. The risk is that the power which is granted and which we also assume as clinicians, can begin to eat away at our values and ideals such that we fail to safeguard and uphold the fun-damental sanctity, dignity and sovereignty of those whom we seek to serve. The danger is that we can over identify with the professional roles we play and forget the people we are. The danger is that our minds can become severed from our hearts such that our human hearts no longer guide, inform or shape our work with people.
In my years of experience working as a clinician in public sector mental health, as well as my experience as a recipient of mental health services, I have found my-self needing to ask some difficult questions about the power granted to clinicians: about the way we assume this power as privilege; about how this use of power can erode our values and ideals; about how our use of this power can systemati-cally disempower those we are supposed to be serving; and about how it can op-press and sometimes hurt the people who come to us for help. These are some of the questions I find myself asking: Is there room for the human heart in the human services? Why does working in human services sometimes feel so dehu-manizing? Why Does receiving human services sometimes feel so dehumanizing? Why do we use the language of war rather than the language of love in the hu-man services? For instance we talk about sending staff out into the field to pro-vide front line services to target populations for whom we develop and implement treatment strategies, whether they want them or not. There are no easy answers to these questions. However I am confident that the only way to overcome the forces of dehumanization is to be bold and daring and brave enough to be fully human in the places where we work and to always recognize that we work with people and not with disabilities or diagnoses. This may seem self-evident, and yet this simple ethic is routinely ignored.
For instance, in Rosenhan’s now classic study entitled Being Sane in Insane Places he exclaims: Neither anecdotal nor “hard” data can convey the overwhelming sense of powerlessness, which invades the individual as he is continually exposed to the depersonalization of the psychiatric hospital. (p. 256) I, too, have experi-enced the effects of depersonalization and dehumanization. Below is the account of one such experience: It was nighttime. Nighttime in a mental hospital. If I looked out the wire mesh windows I could see the stars assuming their winter formations in the bitter cold December sky. To me the stars were beautiful.
To me they were like beacons of light from another time and place. It was good to see all those stars breaking through all that darkness. And though they gave no warmth, the stars shone through the darkness as a promise, as a hope. But that was on the outside. On the inside of the mental hospital, things were very different.
In some ways nighttime in a mental hospital is the hardest time. It’s hard be-cause you have to stay still long enough to fall asleep. You have to be with your-self, alone and in the dark, with the sound of your own heart beating lonely and scared and in pain and so far away from the people you love. So far away and all alone. And as you lie there at night, sounds amplify and echo down the great empty corridors. Some sounds you get used to real quickly, like the jangle of keys locking and unlocking doors and bathrooms and elevators and nurses sta-tions. You get used to the sound of the keys that separate those who can leave and those who have to stay, those keys that separate those who get to go home and those many who have no home to go to. You get used to the sound of the keys jangling and echoing down the empty nighttime corridors real fast. But there are some sounds you can never get used to. Like the sound of a man strapped down in restraint and crying out “Help. Help me. Someone please help me.”
When I first heard him crying out, I jumped out of bed and hurried down the hall-way. What I found amazed me. There, outside the door of the seclusion room, was a mental health worker sittings with his legs swung casually over the side of a soft lounge chair. He had parked the lounge chair outside of the open door from which the cry was emanating. The mental health worker was flipping through a magazine. He appeared to not hear the cry of the man in the seclusion room. Actually, it was as if he didn’t even recognize that the patient in that room was a person who was in great distress. Quietly, I slipped past the mental health work-er and looked inside the seclusion room. An old man, probably sixty or so, with white hair and very thin, was strapped down on a green rubber mattress. Heavy leather cuffs lashed his wrists and ankles to the cold steel of a metal bed frame. He was stripped naked except for his underwear.
When I saw the mental health worker sitting in casual comfort outside of the room in which a man was restrained, humiliated and crying out for help, I froze in terror and disbelief. For a moment I could not move. I felt numb. Then I felt a tearing pain inside my heart. You see, if you are a patient in a mental hospital and you hear a fellow patient who is in restraint and who is crying out for help, you are not allowed to answer the cry. You are not allowed to be fully human, to be whole and therefore able to respond to another human being compassionately. You are not allowed to go into that room, next to the old man and talk softly to him. You are not allowed to bring him a drink of water or to wipe his brow or to just sit there with him so that he will not feel so
abandoned. In fact, if you respond humanly and with compassion, you get pun-ished. That is, if you are a patient in a mental hospital and you try to go in and comfort a person who is crying out from the seclusion room, you get an initial warning from the staff and, if you repeat the violation, you get your “privileges” revoked for the day.
There is such a great irony in the fact that mental patients get punished for re-sponding to the fullness of their human hearts to the cry of another person who is in distress. That is, there is an anguished feeling of having “fallen to pieces,” or of being “shattered,” or “fragmented” that often is a part of the experience of mental illness. To respond as a whole person, as a wholly human being, to the cry of another patient, is actually a response that could be healing. Indeed, the word “whole” or “wholeness” has the same etymological root as the word “heal-ing.” To respond as a whole person to the cry of another would be healing. But such a response is punished. Thus an opportunity for healing is lost, while bro-kenness, fragmentation and dehumanization are reinforced as prescribed roles for staff as well as patients.
I knew that to stand for too long in front of that seclusion room was dangerous. And so I turned quickly away and returned to my bed. But I could not sleep. Instead, I lay in my bed, my eyes open, staring into the darkness and listening.
The old man kept crying out all night long. He kept saying, “Help me. Help me “ Sometimes his voice was strong like a lion. At these times I would hear his voice crying out loud and strong and insistent. At other times, I could hear his voice weaken and quaver, like the sound of a lost and broken child. As the night wore on, his voice grew hoarse and dry and weary and drugged. By dawn, his voice became more of a whisper haunting down the empty corridors. It was a terrible thing to hear that man’s struggles. All night I heard that man crying out in an effort to save the last vestiges of his dignity. I heard that man struggling against overwhelming odds to assert his humanity in an environment that was utterly dehumanizing. I heard his voice rising up like a blaze in the darkness, trying to leave a mark or a streak or some trace of dignity before be-ing swallowed up in the darkness and oblivion of chemical restrain. The voice I heard was a human voice. His message was perfectly clear, “Help me.” But the staff did not hear that simply human voice. Perhaps they thought they were hearing a symptom? But it was not just the man in restraint who got hurt that night. I, too, was very deeply wounded. Something inside of me started to break that night. In my heart I felt a deep aching and a profound sense of out-rage. My anger was not a symptom of mental illness. Anger is never a symptom of mental illness. The anger and outrage I felt were human responses to an in-human situation. During the course of that dark night a kind of numbness
settled into my soul. I felt powerless, helpless and trapped in a situation over which I had almost no control. I did not intend for my heart to close up tight and numb. It happened almost like a reflex, like a way of surviving in a place that is not good for the human heart. It is so important we understand that I am not describing an isolated, “merely personal” experience here. In fact, I would argue that a majority of people with disabilities have experienced what I am speaking about. In clinical language we might refer to this as an experience of trauma, with consequent emotional constriction or numbing (van der Kolk, 1987).
Sociologists who study the impact of institutionalization might help us understand the impact of dehumanization and depersonalization on people in total institutions (Goffman, 1961). However, to fully understand this experience, we must look further than clinical explanations.
In many respects, people with disabilities who have lived the experiences of de-humanization, trauma, and depersonalization are the real experts. When those of us with psychiatric disabilities come together and talk among ourselves, we don’t use clinical language. Instead, we talk about the experience of “spirit breaking” or we refer to times when “they almost broke my spirit” or the times when “they broke my spirit.” We use our own language and discover our own words in or-der to reclaim our experiences and validate them. As Paulo Friere (1989) helps us understand, overcoming the effects of dehumanization and oppression means “each man wins back his right to say his own word, to name the world. (p.13)” Indeed, the first step in overcoming oppression is expression. That is why it is so important to listen to people and allow them to find their own words in order to name their own world. The experience of spirit breaking occurs as a result of those cumulative experiences in which we are humiliated and made to feel less than human, in which our will to live is deeply shaken or broken, in which our hopes are shattered and in which “giving up,” apathy and indifference become a way of surviving and protecting the last vestiges of the wounded self.
This experience is not confined to any one disability group. It can and does hap-pen to people with mental retardation, people with physical disabilities, people with head injuries, people who are blind, members of the deaf community and people with psychiatric disabilities. For instance, I work with a man who has a spinal cord injury. He tells of a time his spirit was very nearly broken and a deep, reflexive numbness settled over his heart. His story goes like this:
At fifteen years old he had been recently paralyzed from the neck down. He was lying naked, under a sheet, on his hospital bed. A group of interns came into his room, led by a chief resident who was conducting rounds. Without asking per-mission, the chief resident ripped the sheet off the fifteen-year-old boy and ex-posed his naked body for all to see. The boy began to scream and scream and scream. Just like the old man in restraints, that outraged scream was the
desperate assertion of the boy’s dignity. Dignity safeguards that sacred, inviolate place within the human heart wherein dwells the very integrity of the human spir-it. It was this deepest sense of spirit, of self, of dignity that had been violated. The boy gave witness to that violation in his screams (Des Pres, 1976). But the doctors failed to hear the humanness of the boy’s cry. Instead, they ordered that he be given tranquilizing drugs. And it was at this point when he had been ren-dered powerless and helpless, when no one would listen to him or embrace and acknowledge his humanity, that numbness began to settle into my friend’s heart. That was when he experienced his spirit as being deeply wounded and beginning to break.
It is clear those doctors did not respond humanly and with compassion to the cry of a real person. Just like the mental health worker, who sat in comfortable indif-ference outside the door of the seclusion room, those doctors failed to realize the patient was a real person. I would argue that because both the mental health worker and the doctors failed to see patients as people, they became a little less human themselves. As Paulo Friere puts it, dehumanization “marks not only those whose humanity has been stolen, but also (in a different way) those who have stolen it (p. 28).”
That is how the terrible cycle of dehumanization works. When helpers fail to see and hear the personhood of the people they work with, and when we see diagno-ses and disabilities rather than human beings, then we as helpers become a little less human ourselves. We become a little less able to respond from the fullness of our human hearts to the cry of another person who may be in distress. And it is precisely in situations and relationships which are dehumanizing that people with disabilities suffer the experience of spirit breaking.
The experience of spirit breaking is not confined to specific places. In other words, it does not just happen in mental hospitals or state schools or rehabili-tation hospitals. It can and does happen in community residences, outpatient medication clinics, vocational rehabilitation programs, private practice, home-less shelters, clubhouses and respite centers. For instance, I know a man with a psychiatric disability who approached his community case manager and stated that he “wanted help making friends and getting a girlfriend.” The case manager responded: “What? You can’t expect me to pimp for you!” My friend was deeply hurt and humiliated by this comment. He says the cumulative impact for this and many other humiliating experiences at the hands of helping professionals, nearly broke his spirit.
Spirit breaking can and does happen in any environment in which there are people who have power and people who have been stripped of their power to
direct their own lives and make their own choices. It can happen in any envi-ronment in which there are those in a position of dominance and those who are deemed to be subordinate. It can happen in environments where there are people who are considered by implication to be superior, because they are surrounded by people who are labeled as inferior. Simply put, it occurs when we relate to people as if they are disabilities, as if their personhood is disabled, and as if somehow, they are not real people at all.
But the point is, people with disabilities are real people. The man in restraint was not a “madman.” First and foremost, he was a human being. The teenage boy in the hospital bed was not a “quadriplegic.” He was a human being. We are not “disabled people.” We are people with disabilities. Our personhood must always come first. It is offensive to refer to us as “the mentally ill” or to refer to people with physical disabilities as “the disabled.” We are people with mental illness, people with psychiatric disabilities, people with physical disabilities. If our person-hood does not come first, that is if we are perceived as disabilities and diagnoses rather than as human beings, then the relational foundations which result in dehu-manization and spirit breaking are laid in place.
Striving to be as fully human as possible is the only way to overcome the forces of dehumanization. Humanizing the human services is a task that begins with you and me. Jean Baker Miller (1976) and Janet Surrey (1987), and other women of the Stone Center at Wellesley College in Massachusetts are pioneering a new and exciting theory and praxis of clinical work, which suggest how we might enter into therapeutic relationships that avoid the pitfalls of dehumanization and depersonal-ization.
The Stone Center scholars note that traditionally and culturally we have come to understand power as signifying domination, control and mastery. In other words, we equate power with “having power over someone or something.” Human ser-vice institutions grant clinicians power in this sense of the word. In fact, the “sick-er” a person is perceived to be, the more power and control we are expected to exercise over nearly every detail of their life.The theorists at the Stone Center argue that these traditional, institutionalized power relationships are dehumanizing, precisely because they lack the possibil-ity of true mutuality. These are hierarchical relationships in which clinicians have most, if not all, of the power and patients have little if any power to control their own lives, destinies and the resources affecting their lives. These hierarchical and paternalistic relationships not only set the stage for dehumanization to occur, but also prescribe a role of passivity, dependence, and learned helplessness for the patient (Seligman, 1975). Esso Leete (1988), a woman who has been diagnosed and treated for schizophrenia and is a nationally recognized spokesperson in the consumer/expatient/psychiatric survivor movement, captures the essence of the
effects of such disempowering and dehumanizing relationships when she says:I can talk, but I may not be heard. I can make suggestions, but they may not be taken seriously. I can voice my thoughts, but they may be seen as delusions. I can recite experiences, but they may be interpreted as fantasies. To be a patient or even an ex-client is to be discounted.
There is an alternative to such hierarchical, dehumanizing and disempowering relationships. Again, following the lead of the Stone Center theorists we find that by definition “power” can also mean the capacity to move or produce change. Surrey (1987) helps us to understand that power need not mean “having power over” but can mean “having power with” or “having power together.” She urges us to enter into relationships that are mutually empowering for both the clinician and the client. Relationships between professionals and clients are empowering when both parties are available to “be moved by” the thoughts, perceptions and feelings of the other.
In such empowering interaction, both people feel able to have an impact on each other (Stiver, 1985) and on the movement of “flow” of the interaction. Each feels “heard” and “responded to” and able to “hear,” “validate,” and “respond to” the other. Each feels empowered through creating and sustaining a context, which leads to increased awareness and understanding. Further, through this process, each participant feels enlarged, able to “see” more clearly and energized to move into action. The capacity to be “moved” and to respond, and to “move” the other, represents the fundamental core of relational empowerment. (Surrey, p.6-7)Because power is often related to the ability to control another person, Surrey (1987) and the other Stone Center theorists recognize that relational empower-ment means learning new ways to relate to clients. It means learning how to have power with rather than power over those who come to us in distress. It means learning how to work with another person such that neither the clinician nor the client is “in control.” Rather, both can learn to experience themselves as being heard and responded to as well as being moved and moving the other. Clearly, this model holds promise for helping us understand how to re-humanize the human services. However, it remains to be seen how (and even if) these insights and values can be incorporated into human services institutions, which seem almost by definition to operate on the hierarchical principles of having pow-er and control over patients/inmates.
Certainly clinicians can help re-humanize the human services, but my real hope for achieving this goal rests with the community of people with disabilities. There are over 43 million people with disabilities in this country. We are the largest mi-nority group in America. Slowly but surely we are becoming organized and em-powered to act. The recent passage of the Americans with Disabilities Act (ADA) is a landmark piece of civil rights legislation for us. The ADA confirms what we have known for a long time. That is, whereas clinicians usually insist the
disability resides “within us,” we understand that what is truly disabling to us are the barriers in our environment preventing us from living out the full range of our human interests and gifts and preventing us from living, loving, worshipping and working in the community of our choice. What is truly disabling to us is stigma, which, though rampant in the general population, is also widespread in the help-ing professions. In human service institutions, policies and clinical/rehabilitation praxis, stigma often disguises itself as a kind of benevolent paternalism or the sympathy of “false charity” which Friere (1989) characterizes as follows:False charity constrains the fearful and subdued, the “rejects of life,” to ex-tend their trembling hands. True generosity lies in striving so that these hands whether of individuals or entire peoples need to be extended less and less in supplication, so that more and more they become human hands which work and, working, transform the world. (p.29)
These stigmatizing and infantilizing attitudes are disabling to us. In addition to the stigma we find discrimination in employment, housing and education are dis-abling. Poverty, oppression, segregation and unemployment are conditions we find disabling. Staff attitudes characterized by low expectations, prophecies, and prognoses of doom, as well as policies, procedures and practices which teach us to be passive, helpless, dependent and irresponsible are also disabling to us. Finally, those aspects of the human services, which dehumanize and break (or try to break) our spirit are disabling to us. These wounds “numb” or at times “break” our will to live, rob us of hope, and instill a deep sense of apathy, despair, person-al worthlessness, and self-hatred. Many of us experience these wounds as more disabling than the mental illness or physical injury/syndrome we may have been diagnosed with. It is these wounds that take a long, long time to heal.My real hope for re-humanizing the human services rests with people with dis-abilities as we begin learning that we can organize, that we have power in our numbers, and that we can overcome oppression through expression. The days of silence are over. As professionals and as fellow human beings, we have a great deal to learn from the people we seek to serve. It is important to listen to people with disabilities. For instance, Bill LaLime is a member of a Massachusetts grass-roots organization made up entirely of people with psychiatric disabilities. This organization is called M*POWER (Massachusetts People/Patients Organized for Wellness, Empowerment and Rights). Mr. LaLime has written about his struggle to remain human while receiving what, at times, can only be characterized as “in-human services.” He also suggests what we can do to help bring about change:I want to have my story written down so I can remember where I’ve been and so I don’t forget what I’ve been through. If I have it on paper, I know it’s not a lie; it’s something I’ve been through.
If people read our stories, they know what we have been through. People who haven’t been through what we’ve been through need to hear our stories so they’ll know what we experience. The system sucks. I’ve been though the whole nine yards. The system has to change. One way we can help it to change is to tell our stories.
I couldn’t fight the system myself; it was really hard. They tried to break me to a point where I lost my values. There were things happening that could have bro-ken my spirit. But I still had enough of myself to keep going, even though I got sick and tired of being locked up. When I went in the hospital, I lost my values, my intellectual thoughts, my thinking, my self-esteem. I know it’s my values that I lost. Values means my morals. They force you to do things against your will, against your values.
When I was at [a well-known private hospital], they drugged me with medica-tion and when I got up in the middle of the night, I didn’t know where I was and I fell against a metal hinge with my back and had a big black and blue mark, and it was bleeding. I told the nurse and asked her to look at it and she did, but she wouldn’t do anything about it. She said, “What happened to you?” and I told her. She and the other staff said, “Just lay down in bed and rest and it will go away.” But it didn’t go away.
I kept complaining to the staff. I asked for aspirin but they wouldn’t give me anything for the pain because there were no doctors on call. They kept telling me to wait till the next shift and they wouldn’t do anything about it. And then the next shift would tell me to wait for the next shift, and on and on. Finally, on Sunday morn-ing, I told a mental health aide I’d been trying to get help for my hurt back for three days and the aide told me to wait until it goes away. I said I couldn’t wait anymore and threw the aide against the window, and they finally took me to the hospital to get some treatment for my back.
At [an in-patient community mental health center], they took my cheese away from me. I was eating too much food that day, and at night they took my cheese away from me and I got violent. I threw a chair at them and they locked me up, and I swallowed money to aggravate them while I was in seclusion. They were watching me through the window. I’d say, “here’s a coin. I’m eating it,” and I’d swallow it. They’d laugh at me, and they’d say, “Swallow another one.” And so I’d do it again. I’d swallowed thirteen coins in all. I stopped because they lost interest, they weren’t amused anymore and they went away.
When I was in the hospital, the loneliness in there and no one to talk to, the only ones to talk to were the other patients. It was a horrible thing. Other patients meant a lot to me. It was beautiful. They helped me a lot. The patients kept me going. The way they felt, too. We talked about our problems outside the hospi-tal. I got very discouraged, because when I left the hospital, I couldn’t visit my friends because I was a former patient and there was a rule against my visiting. I felt lonely after I got out of the hospital.
At [ ] and other hospitals, they took my rights away. I wrote letters, but I nev-er got any back because the staff wouldn’t give them to me, or if they did, they opened them first and read them. I didn’t have that much privacy. I couldn’t bring my girlfriend in my room. Or every five minutes they came in to check on
me. Without privacy, you feel you can’t trust anyone. I lost my freedom. The locked doors, I couldn’t leave. I was very scared by that. I didn’t have many visitors because they didn’t like where I was. They were scared to come visit be-cause of where I was. I was very lonely.
Talking on the phone to my teacher and minister kept me going, because they knew what I was going through. I’d tell my minister and my teacher and they could see how I was. For example, Thorazine made me slur my words. They were concerned about me, but the staff weren’t concerned. They didn’t care.
I was in a state hospital. I was in the shower and four men patients came in and raped me, and the guard, who was watching, laughed about it. I remember and I don’t forget about it. You’re in a daze in there. Visitors stare at you. Once they gave me Haldol and I was screwed up for seven hours. My neck muscles were all tightened up and my legs were all locked up. I was on the floor for seven hours because of this reaction to Haldol. They gave me two shots of Benadryl, but it took two or three hours to work. I didn’t know what happened to me. My mouth tightened up and I tried to tell them I was having a bad reaction, but I couldn’t talk well and they told me I was just fine, there was nothing wrong with me. But I wasn’t fine.
The stuff I’ve been through was like a nightmare. Sometimes I go back into the nightmare. I cry every night about it. Remembering it is like being in the night-mare again. But I’m going to remember it till the day I die. It will be with me for the rest of my life. Sometimes I scream at night because I’ve dreamed about the hospital I was raped in or some other hospital I was in.
When I came home from the hospital I was raped in, I went to a lake where I could listen to the birds chirping in the sky and I could watch the waves on the water, and it gave me peace of mind, and if I wanted to scream, I could and no one would hear me. I was all alone and it was really beautiful. If I’m up in my room by myself, I can think about my own problems. It isn’t easy, but I can deal with it. Today, I don’t have to think about it so often.
We need better doctors, people who care and help people. We need to say what we want, what the problems are. If they can’t listen the first time, we go back again and again until they’ll listen to us. Things might not change overnight. But if we can come together as a group to work towards change, it gives us some-thing to look forward to.
Bill LaLime is right. We need better doctors. We need people who care and who can help people. We need people who will listen to us and if they don’t listen we need to keep going back until they do listen.
ReferencesDes Pres, T. (1976). The survivor: An anatomy of life in the death camps. New York: Pocket Books.Friere, P. (1989). Pedagogy of the oppressed (M.B. Ramos, trans.). New York: Con-tinuum.Goffman, E. (1961). Asylums: Essays on the social situations of mental patients and other inmates. New York: Anchor Books.LaLime, W. (1990). Untitled speech used as part of Lowell M*POWER’s Anti-Stigma workshop, Lowell, Massachusetts.Leete, E. (1989). The role of the consumer movement and persons with mental illness. Presentation at the twelfth Mary Switzer Memorial Seminar in Rehabilitation, Washington DC, June 15-16.Miller, J.B. (1976). Toward a new psychology of women. Boston: Beacon Press.Rosenhan, D.L. (1973). On being sane in insane places. Science, 178, 250-258.Seligman, M.E.P. (1975). Helplessness: On depression, development and death. San Francisco: Freeman.Stiver, I. (1985). The meaning of care: Reframing treatment models. Work in Progess, #20. Wellesley, MA: Stone Center Working Papers Series.Surrey, J. (1987). Relationship and empowerment. Work in Progress #30. Wellesley, MA: Stone Center Working Papers Series.Van der Kolk, B.A. (1987). Psychological trauma. Washington DC: American Psychiatric Press.
2.6 Reading, Presidential New Freedom Report


3.4 Reading, Five Fundamental Rights (Massachusetts)
KNOW YOUR RIGHTS!
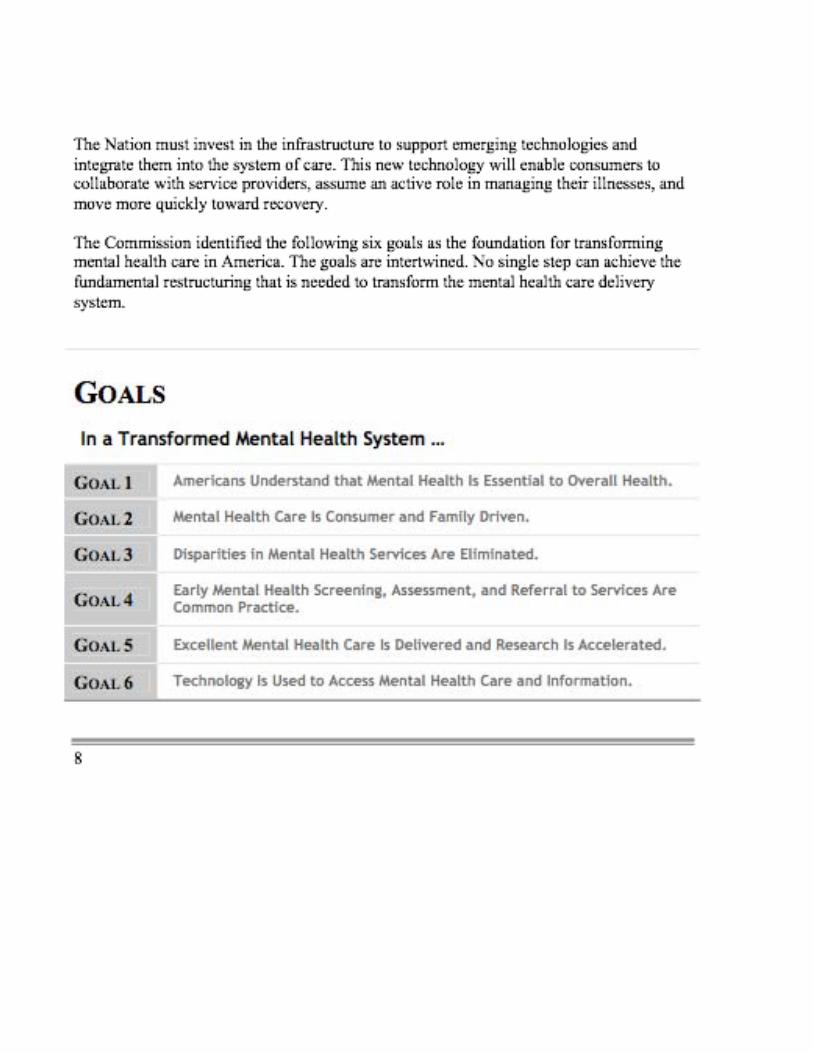
The Five Fundamental Rights
(Massachusetts General Laws, Chapter 123, Section 23) These are YOUR RIGHTS under LAW. Here are ways the law can be violated. (Legal language is paraphrased).
Any person hospitalized in a psychiatric unit licensed by the Department of Mental Health (this includes all private psychiatric hospitals), State hospitals, or living in DMH or DMH-licensed residential facilities, shall have the following rights:
Fundamental Right #1: (a) The right to have reasonable access to a telephone to make and receive confidential phone calls, in private.
Violations include:
• No phones are available on psychiatric units.
• Patients aren’t allowed to make calls, no matter how important.
• Only pay phones are available, and a reasonable source of money or assistance to make calls is not provided.
• Telephones are located in hallways or common rooms.
• Telephones are located adjacent to/next to nursing stations, so staff members can hear your conversations.
• Staff listens to phone calls.
• Telephones are shut off for unreasonably long periods of time.

“Empowerment” has become a popular term in mentalhealth programs, yet it has lacked a clear definition. In a research projectdesigned to measure empowerment in programs run by and for mentalhealth service users, we first undertook to come up with a working defini-tion. Key elements of empowerment were identified, including access to information, ability to make choices, assertiveness, and self-esteem.Empowerment has both an individual and a group dimension. Details of thedefinition are provided, along with a discussion of the implications of em-powerment for psychiatric rehabilitation programs.
A WORKING DEFINITIONOF EMPOWERMENT
▼
JUDI CHAMBERLIN
Judi Chamberlin is a psychiatricsurvivor and a long-time activist
for patients’ rights. She is theauthor of On Our Own: Patient
Controlled Alternatives to the MentalHealth System, as well as numerousarticles on the topics of self-helpand alternatives. She is affiliatedwith the Center for Psychiatric
Rehabilitation, Boston University,and with the NationalEmpowerment Center,
Lawrence, Massachusetts.
For information contact theauthor at the Center for
Psychiatric Rehabilitation, 930Commonwealth Avenue,
Boston, MA 02215, U.S.A.
INTRODUCTION
“Empowerment” is a term that hasbecome very popular in mental healthservices (at least in the United States).Nearly every kind of mental health pro-gram claims to “empower” its clients,yet in practice there have been few op-erational definitions of the term, and itis far from clear that programs that usethe term are in any measurable way dif-ferent from those that do not.
Still lacking a definition, the word hasbecome common political rhetoric,with a flexibility of meaning so broadthat it seems to be in danger of losing
any inherent meaning at all. Some conservative U.S. politicians have pro-moted welfare “reform,” for example,by claiming that cutting off benefits will“empower” recipients (who wouldthus, presumably, become self-suffi-cient)! Such usages make it difficult toclaim that “empowerment” is a mean-ingful concept.
The problem of using the term meaning-fully becomes even more problematic inother countries and other languages.When I have spoken abroad, I find thatthe word is usually not translated; thetranslator merely repeats “empower-ment,” in English, perhaps hoping thatthe listeners will be able to draw some
spring 1997—Volume 20 Number 4
43
SPECIAL SECTION
3.5 Reading, A Working Definition of Empowerment



3.6 Reading, Conspiracy of Hope


3.7 Reading, From Narrative Wreckage to Islands of Clarity




4.4 Reading, What Makes Peer Support Unique? (Condensed)
Full version available at http://www.mentalhealthpeers.com/pdfs/PeerSupportUnique.pdf
4.5 Reading, Transcom Update on Peer Support
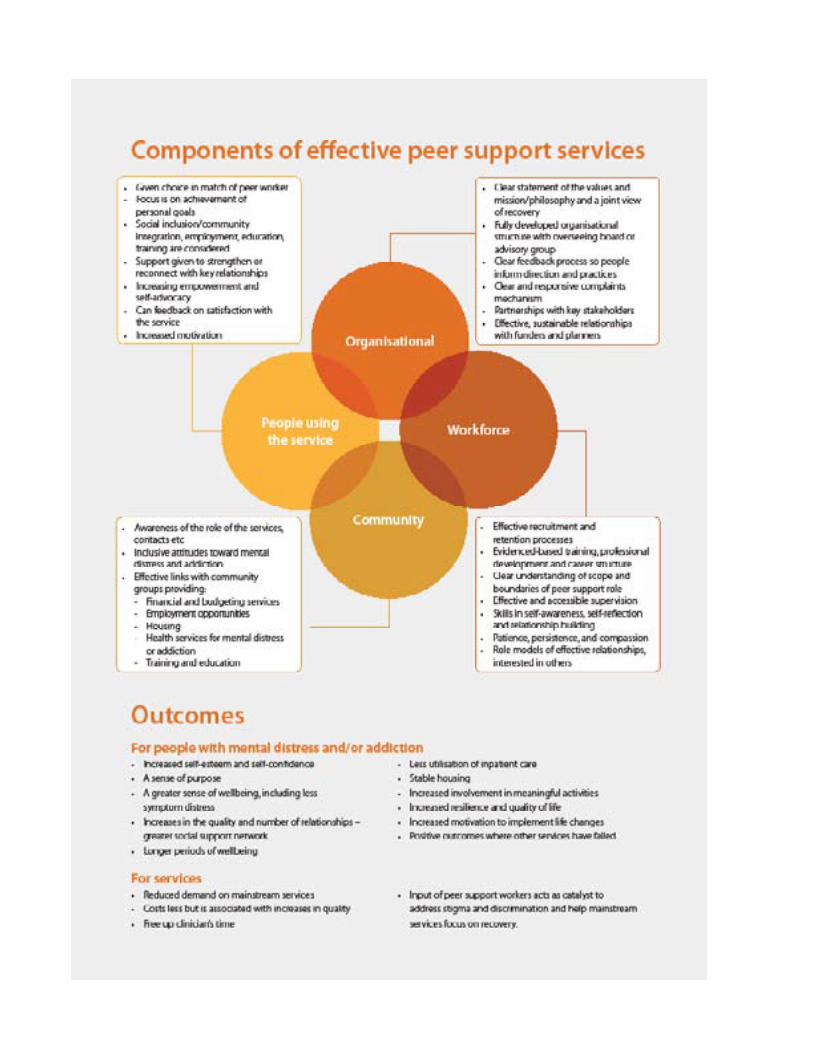
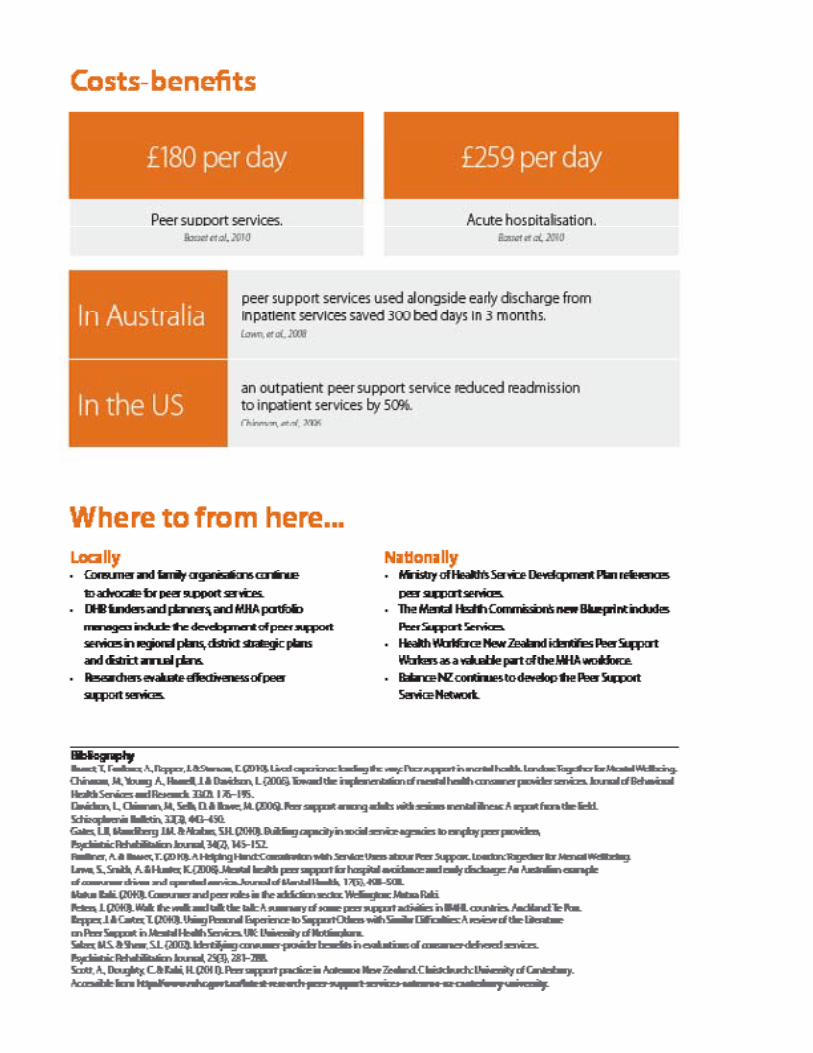
Power of Peer Support Servicesin mental health and addiction
Personal choice For each person the journey of mental distress or addiction and how they achieve recovery, is unique; this means services need to be responsive to a range of needs; peer support has the flexibility to achieve this.
Wanted by consumers Has been driven by consumers of services and is based on the accumulated knowledge of people with lived experience. There is wide support from service users, consumer leaders and advocates to develop peer services.
Recovery focussed Peer support workers are powerful role models who inspire hope in those with whom they work.
Occurs within the community Recovery happens within the ‘everyday’. Peer support workers walk beside a person to navigate through their communities to support the personal and social goals that give recovery its meaning and lead to greater long term wellbeing.
For further information go to www.mhc.govt.nz
4.7 Reading, Power of Peer Support

5.4 Reading, CPS Job Description
6.3 Reading, Concerns about Recovery




6.4 Reading, Peer Support