Embed Size (px)
Citation preview

A New Splint Design for the Thumb CMC Joint 1
THUMB CMC JOINT & OSTEOARTHRITISThe thumb trapeziometacarpal joint, also called
the thumb carpometacarpal (CMC) or basal joint, is themost common site of upper extremity surgery due todisabling osteoarthritis.1-4 The articulation of the firstmetacarpal bone with one surface of the trapezium isthe locus of this common pathology. The incongruouscontours of these two shallow saddle-shaped joint sur-faces provide no intrinsic osseous stability, requiringthe ligaments and muscles to assume responsibilityfor stability to prevent trans lation during loading.1 Ad-ditionally, the base of the first meta carpal is approxi-mately 34% larger than that of the trapezium whichconcentrates pressure on the trapezial surface.5-9
To allow the normally large range of motion of thethumb CMC joint, a loose but strong joint capsule is re-quired. The inherent joint mobility diminishes the jointstability.10,11 Of the seven ligaments that maintain the
relationship between thebase of the first metacarpaland the trapezium, thedeep anterior oblique liga-ment (also commonly calledthe beak ligament) is con-sidered the most importantstabilizing ligament. It is primarily responsible for pre-venting dorsal translation of the metacarpal on the tra-pezium. With ostearthritis, the beak ligament becomesinsufficient and the meta carpal base moves dorsally inrelationship to the trapezium.Osteoarthritis, also called degenerative joint disease, isa noninflammatory type of arthritis marked by degen-eration of the articular cartilage, overgrowth of bone atthe margins, and changes in the synovial membrane.Usually not as severe as rheumatoid arthritis, os-teoarthritis is considered part of the normal aging
A New Splint Design for the Thumb CMC Joint
Authors:Judy Colditz
Nettie Koekebakker
NOTE TO THE READER: In this paper the terms: 1) splint 2) orthosis and 3) brace are used interchangeably
since common usage varies throughout the world.
Figure 1; Radial view of the hand illustrating the carpometacarpal joint (highlighted).
The insufficient beak ligament allows the
metacarpal base to movedorsally in relationship
to the trapezium.
Nea CMCWhitepaper v2_Opmaak 1 1/12/10 14:46 Pagina 1

A New Splint Design for the Thumb CMC Joint2
process, and is most likelyto involve the joints thatreceive the most use orstress over the years.12
Symptoms of osteoarthritismay include joint pain,tenderness, stiffness or in-
stability. CMC osteoarthritis causes increased laxity ofthe joint capsule, creating the common clinical compli-ant of pain with resisted thumb motion, particularlyforceful pinching. Movement of one bone end againstthe opposing joint surface creates pain.13
Thumb CMC joint osteoarthritis is believed to resultfrom chronic stress to this incongruent joint. Strong as-sociation exists between excessive basal joint laxity andthe development of premature degenerative changes.4
With minimal inherent bony stability, the CMC joint isdependent upon a force couple of muscle tension andpassive ligament tension for stability. Of the eight mus-cles which influence thumb CMC joint motion three of
the extrinsic muscles (ab-ductor pollicis longus, ex-tensor pollicis brevis andextensor pollicis longus)are relatively inefficient ex-tensors and abductors at
the CMC joint. In contrast, three of the four thenarmuscles pull the first metacarpal head toward the palm(into flexion), and thus the balance of motion is loadedtoward flexion. This muscle force inequality explainsthe most common direction of deformity of the firstmetacarpal: flexion and adduction.
DIAGNOSIS / EARLY RECOGNITIONIndividuals with thumb CMC osteoarthritis experiencepain within the joint, tenderness to palpation, and/orexcessive laxity of the joint or joint stiffness, and have
difficulty accomplishing tasks which require forces thatload the joint. Both repetitive and resistive home andwork activities may exacerbate symptoms. Commoncomplaints are pain with tasks such as twisting open ajar lid, turning a key in a lock or turning doorknobs,sustained pinching or writing, picking up a large book,holding a cup of tea/coffee, doing needlework, carryingan object that weighs more than 4.5 kg (10 lbs.), andusing scissors.1, 2, 14,15 Grip strength is diminished inthose with symptomatic hand osteoarthritis.14
The diagnosis of CMC joint osteoarthritis is made basedon pain complaints consistent with CMC osteoarthritis,positive clinical examination, and radiographic find-ings. Clinical examinations commonly used may includeCMC joint palpation which indicates joint inflammation,the grind test which evaluates the quality of the artic-ular surfaces, the crank test which both evaluates thejoint quality and translational laxity, the distractiontest where a pain response indicates joint inflammationand volar compression of the first metacarpal basewhich also indicates joint inflammation.4,6,16 In additionto a positive response tosome or all of these tests,it must be ruled out thatpain is coming from com-pression of the mediannerve or inflammation ofthe tendons in the firstdorsal compartment (DeQuervain’s tenosynovitis) or another cause. Althoughx-ray findings confirm the diagnosis when clinical examis positive, radiographic evidence may be present with-out accompanying symptoms.1,17 Since there is poor cor-relation between radiographic severity and clinicalsymptoms, non-surgical treatment must be based onfunctio nal/pain complaints rather than radiographicfindings.
INCIDENCEOsteoarthritis (OA) of the thumb CMC joint is particu-larly prevalent in postmenopausal women, 18, 19 many ofwhom already have normal laxity of this joint.4 From25-40% of individuals over the age of 55 have radi-ographic evidence of CMC osteoarthritis.2, 3, 20 Contactforces are greater in females due to fact that male jointsurfaces are more congruent,21 creating an approximateratio of 1 in 4 women and 1 in 12 men in older agegroups. 1, 15, 17, 18, 22, 23
Figure 2: Photo of the thumb CMC joint surfaces
The common deformity is flexion and adductionof the first metacarpal.
Non-surgical treatmentmust be based on functional/pain complaints, not
radiographic findings.
Osteoarthritis is part of the normal aging
process, involving jointsthat receive the most
stress.
Nea CMCWhitepaper v2_Opmaak 1 1/12/10 14:46 Pagina 2
A New Splint Design for the Thumb CMC Joint 3
As age increases, both thefrequency and severity ofhand OA increases up to80% of those over 70+.24-26
Obesity also appears to bea strong correlation withsymptoms.20, 23 Although
epidemiological studies of hand osteoarthritis are few,one study identified those with symptomatic os-teoarthritis as 17% of women and 9% of men. Of thejoint sites where osteoarthritis is seen in the hand, painand disability is strongly associated with presence ofosteoarthritis at the thumb base joint.22
BIOMECHANICSAs osteoarthritis develops, the already slack capsule ofthe thumb CMC joint becomes excessively lax as thebeak ligament loses its ability to checkrein dorsal trans-lation of the metacarpal on the trapezium.4 When the
thenar muscles contract during pinch, the firstmetacarpal tilts; i.e. the distal end moves toward thepalm and the proximal end shifts dorsally. It is thisshift of motion, even though perhaps slight, which cre-ates pain. A progressive deformity of the thumb CMCjoint ultimately modifies the pull on the thumb MPjoint, creating secondary problems of imbalance at thisjoint.19, 27 If one imagines the thumb as a tent pole tobe stabilized, three evenly spaced guy wires with iden-tical tension are needed. During pinch, the thumb mus-cles must provide this precarious balanced posture totransmit the force of pinchevenly to the base joint. Pellegrini describes thechallenge of treating thumbCMC joint osteoarthritis:“To reconcile and satisfythe competing goals of providing stability and mobilityto the trapeziometacarpal articulation.”28 This goal isthe challenge of any splinting of the thumb CMC jointthat allows continued functional use of the thumb.
SPLINTING/BRACINGSplinting/bracing of the osteoarthritic thumb CMC jointis considered “the mainstay of conservative care,”1 andrelieves pain in patients with osteoarthrtis of the firstCMC joint.1-3, 15, 17, 24, 29-40 When splinting is combinedwith activity modification and non-steriod anti-inflam-matory medication, Berggren, et al showed that 70%of patients at 7 months no longer required surgical in-tervention.2, 31 At 1 year follow-up Boustedt, et al foundthe group given splints/braces (worn day and night),joint protection instruction, heat, and home exercisesignificantly decreased pain and stiffness and improvedin daily activities compared to a control group givenonly joint protection instruction. Hand grip strengthalso increased 27% as compared to 17% increase in con-trol group.30 Both the National Collaborating Centre forChronic Conditions in the United Kingdom and the ev-idence-based European League Against Rheumatism(EULAR) recommends splints/braces as part of thumbCMC osteoarthritis treatment.13, 29
The focus of splinting/bracing the thumb CMC joint maybe to:� Decrease inflammation by providing rest and
immobilization
Figure 3: One in four women and one in 12 men overage 70 have osteoarthritis of the thumb CMC joint.
Pain and disability are strongly associated
with osteoarthritis of the thumb CMC
joint.
Figure 4: X-ray of classic CMC joint deformity: the distalend of the first metacarpal moves toward the palm and
the proximal end shifts dorsally.
Mobility and stability are competing goals.
Nea CMCWhitepaper v2_Opmaak 1 1/12/10 14:46 Pagina 3

A New Splint Design for the Thumb CMC Joint4
� Decrease pain by providing stability during activities that load the joint.
In some cases splints/braces can achieve both purposes.
ImmobilizationImmobilization splinting that is used to decrease in-flammation rarely allows functional use of the thumb.These splints incorporate the wrist and/or the MP jointof the thumb in addition to the CMC joint.1,2, 15, 17, 30, 32,39 Tolerance and compliance are often questioned sinceindividuals cannot accomplish daily tasks with thesesplints.2 Additionally, prolonged use of the splint is not
desirable due to the likelydisuse atrophy of thethenar muscles.36, 39 Becauseof the functional limita-tions such splints impose,these splints/braces are
often worn only at night, although this may follow arelatively short initial period of full time wear.36
Designs which incorporate adjacent joints are deemednecessary by many because the common three-pointpressure design is not possible at the thumb CMC joint.The small size of the trapezium coupled with the in-ability to surround the thumb CMC joint makes it im-possible to apply a stable three point splint. Thusmotion of the thumb CMC joint is commonly limited bycapturing other adjacent joints.
Dynamic StabilityInflammation results from excessive motion that occursat the CMC joint. If motion is minimized, both pain andinflammation are diminished. In contrast to an immo-bilization splint, a dynamic stability splint focuses on
preventing excessive motion during load which alsoserves to check the progressive deformity of dorsaltranslation. The splint is designed to provide stabilityby applying an external substitute for the inadequatebeak ligament.A smaller splint design that includes only the thumbCMC joint can provide dynamic stability. Individualsprefer a short splint.34 Since greater periods of splintwear decrease pain,30, 32, 38, 39 splints/braces that do notimpede daily activities allow longer periods of wear. A thumb CMC splint/orthosis that only includes thefirst CMC joint provides dynamic stability by use of apseudo-hydraulic environment principle.41 This principle(identified by Sarmiento who first applied it to fracturebracing of long bone fractures) provides stability to abone via the pressure created by contained contractingmuscles. As contracting muscles become larger in cir-cumference an external containment device limits mus-cle expansion and the expansion force is directedinward, increasing the pressure which stabilizes thebone within the contained space.
Immobilization splintingrarely allows functional
use of the thumb.
Figure 5: An immobilization splint prevents functionaluse of thumb and/or the wrist.
Copyright Judy C. Colditz, 2010
Figure 6: A small custommolded splint/orthosisthat only includes thethumb CMC joint.
Copyright Judy C. Colditz, 2010
Copyright Judy C. Colditz, 2010
Copyright Judy C. Colditz, 2010
Nea CMCWhitepaper v2_Opmaak 1 1/12/10 14:46 Pagina 4

A New Splint Design for the Thumb CMC Joint 5
In the thumb CMC joint, stability is accomplished byconformed molding around the thenar eminence whenthe muscles are relaxed. During hand use when themuscles contract and attempt to increase in bulk, thepressure is directed inward to stabilize the firstmetacarpal, maximizing the immobilization effect of
the splint during activeuse. Since pain at the CMCjoint is primarily presentduring active loading, thissplint immobilizes the CMCjoint during active pinch/grasp, because it dependson active thenar muscle
contraction. Since symptom severity is influenced byloading of the joint during use,42 a splint which limitstranslation of the metacarpal when the joint is loadedwill be more effective than a splint that immobilizesbut prevents use of the thumb. Since wrist motion doesnot create pain with thumb CMC joint osteoarthritis,2
wrist immobilization is not necessary. Activities requiring pinch are the primary cause ofthumb CMC joint symptoms.4 Since the smaller splintdesign leaves the critical digital sensory area free, itdoes not impede pinching, fingering, handling or grip-ping activities. Since the thenar muscles are activewhile in this splint, concerns about disuse atrophy ofthe thenar muscles is eliminated. Unlike most splints applied to joint/s, this CMC splintcannot be worn too long or too much. The problem at
the thumb CMC joint isone of excessive motion.It would be ideal if thesplint was worn enoughfor the joint to “stiffen”and have greater stabil-ity. Inclusion of the wristhas been common prac-tice in the past and therefore many contend that anysplint for the thumb CMC joint must cross the wrist foradequate stabilization. Others report pain control withthis smaller splint design that excludes all joints butthe thumb CMC. 33, 34, 43, 44
Following the initial period of post-operative immobi-lization, a small dynamic stabilization splint such asdescribed above may also be appropriately used aftersurgical procedures to the CMC joint. The splint main-tains the ideal posture of the first metacarpal while al-lowing increasing strength of the thenar muscles in theideal position during functional use, preparing the in-dividual for effective weaning from external support.Additionally, this small splint design allows continuinguse of the hand while protecting the healing capsulefollowing a sprain/strain injury to the thumb CMC joint.
DEVELOPING A SPLINT/ORTHOSIS TO SOLVE THEPROBLEMHaving identified the widespread need for an effectivesplint/brace to reduce pain at the thumb CMC joint withosteoarthritis, Nea International bv / Push Braces
When the thumb muscles increase in
bulk within the splint, they stabilize the first metacarpal.
Figure 7: The dynamic stabilization splint creates a pseudo-hydraulic environment which was originally used tostabilize long bone fractures: A. A cylinder contains the area to be stabilized. B. The relaxed muscles almost fill the
space C: The contracted (expanded) muscles completely fill the space within the cylinder and D: The expanded muscles create internal pressure which prevents the bone ends from moving.
A. B. C. D.
Copyright Judy C. Colditz, 2010
Disuse atrophy of the thenar muscles does
not occur in the dynamicstability splint: the muscles are active in
the splint.
Nea CMCWhitepaper v2_Opmaak 1 1/12/10 14:46 Pagina 5
A New Splint Design for the Thumb CMC Joint6
[Maastricht, the Netherlands] began development of aunique splint design. Previously intimately fittedbraces were possible only by application of a custommolded device.43, 44 Because of the varying skill of thoseapplying custom molded splints, often frequent adjust-ments of custom molded splints are necessary for maximum comfort.36 Low temperature thermoplasticmate rials used for these splints are relatively rigid whenmolded. A successful splint mandates precise fit, long-term durability, a surface which does not easily abradeor become unsightly, and tolerance to high tempera-tures such as being left in an automobile in hotweather. The challenge in designing a splint/brace is to meet thegoal of allowing maximum mobility while providing pre-cise stability for a variety of hand sizes. To develop theideal splint design for this problem, Push consultedwith recognized experts. Following input from the ex-perts on important requirements of the design, thePush design team developed prototypes which weresent to the experts for critical evaluation and scoring.
Criteria for the Push Brace Design Process The following criteria were required by PushBrace:
Made of materials that:� Are durable and will not break or crack � Are relatively flexible to minimize edge
pressure but also relatively stiff when in acurved contour
� Minimize surface abrasion� Tolerate heat� Are easily cleaned� Are antimicrobial.
Designed so the brace:� Is adjustable to individual thenar eminence
contour and size� Is easily applied and removed with one
hand without applying torque to the thumbCMC joint
� Provides support to the thumb CMC jointbut does not impede any other joint movement
� Minimizes pressure areas regardless ofunderlying contour.
Meets the criteria of:� Effectively controlling thumb CMC joint
pain� Being well tolerated when worn for long pe-
riods� Being preferable to custom molded design/s
or other commercial designs for this prob-lem
� Being cost-effective for individuals withthis problem.
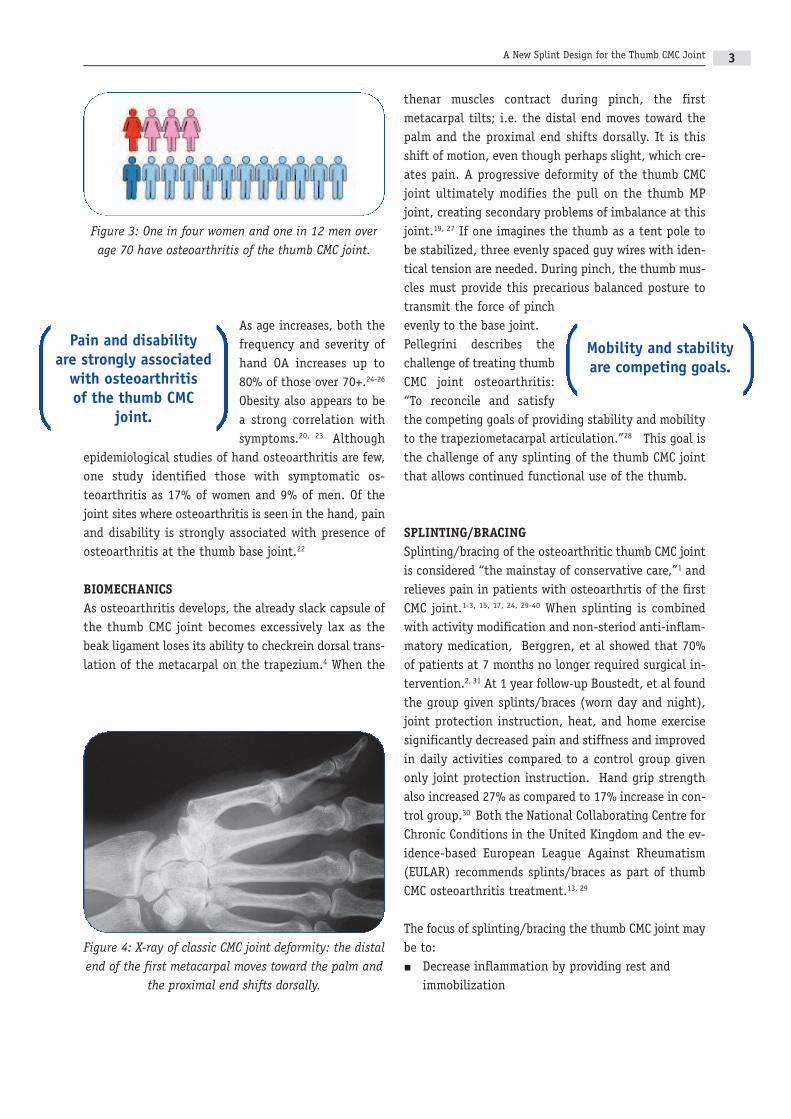
Final DesignThe Push design evolved to a molded base design madeof thermoplastic polyurethane (TPU) into which amulti-curved contoured aluminum insert was specifi-cally positioned around the thenar eminence. After thesplint is applied to the hand with the thumb metacarpalbone positioned with a slight open angle relative to thesecond metacarpal, the aluminum insert is manually
Figure 8: The PushCMC brace showing the adjustable metal insert that stabilizesthe first metacarpalbut leaves all otherjoints free to move.
Nea CMCWhitepaper v2_Opmaak 1 1/12/10 14:46 Pagina 6

A New Splint Design for the Thumb CMC Joint 7
compressed to fit the thenar eminence while the musclesare relaxed. This snug fitting creates the pseudo-hy-
draulic environment whichstabilizes the thumb dur-ing active pinch/grip. Theshape of the molded basecovers a minimal amountof the palmar surface anddoes not impede motion ofthe thumb MP joint or the
wrist joint. The edges of the material are flexible, pre-venting sharp edge pressure seen in many custommolded splints. The double straps run through a slot inthe base material, allowing easy applica tion/removaland application of snug tension upon closure. The cri-teria list was fully met by the final design.
FIELD TESTING OF FINAL PUSH CMC BRACE DESIGN
Field TestA field test was conducted with the final Push CMC pro-totype by Nettie Koekebakker at 4hands, a private out-patient hand therapy clinic in Amsterdam, theNetherlands. The study included 13 patients with amean age of 52.8 years who were diagnosed with thumbCMC osteoarthritis and already being treated in theclinic. Nine patients had a diagnosis of thumb CMC os-teoarthritis, three had recently undergone thumb CMCarthroplasty surgery and one had thumb CMC instabil-ity/laxity. These patients were already wearing a pre-viously fitted custom molded thermoplastic splint,which supported the thumb CMC joint and also includedthe thumb MP joint. The patients had been advised towear the splint during daily repetitive and resistedhome or work activities that would increase pain with-out wearing a splint but not wear the splint at night.All patients received joint protection instruction, adviceon how to use their hand optimally during daily activ-ities, and instruction for home exercises. Home exer-cises were performed 2-3 times a day and includedstrengthening of the intrinsic thumb muscles and activeisometric pinch grip exercises with a balanced arch.At the beginning of the field test the Push CMC proto-type was fitted and all patients were asked to wear theprototype for 6 weeks using the same wearing protocolas the splint they had been using previously. At the
time the splint was fitted, the following informationwas recorded:� Visual Analogue Scale (VAS) Score for pain (score
range 0 -10) 45
� Thumb opposition (according to the 0-10 Kapandjiopposition score) 46
� Maximal voluntary isometric grip strength withoutbrace (Jamar hand held dynamometer) 47-48
� Maximal voluntary isometric two-point, tripod andkey pinch strength without brace (pinch gauge) 48
� Self-report questionnaire that records physicalfunction and symptoms.
In addition, during the field test the patients wereasked to maintain a written diary in whichthey noted their daily experiences with the brace.
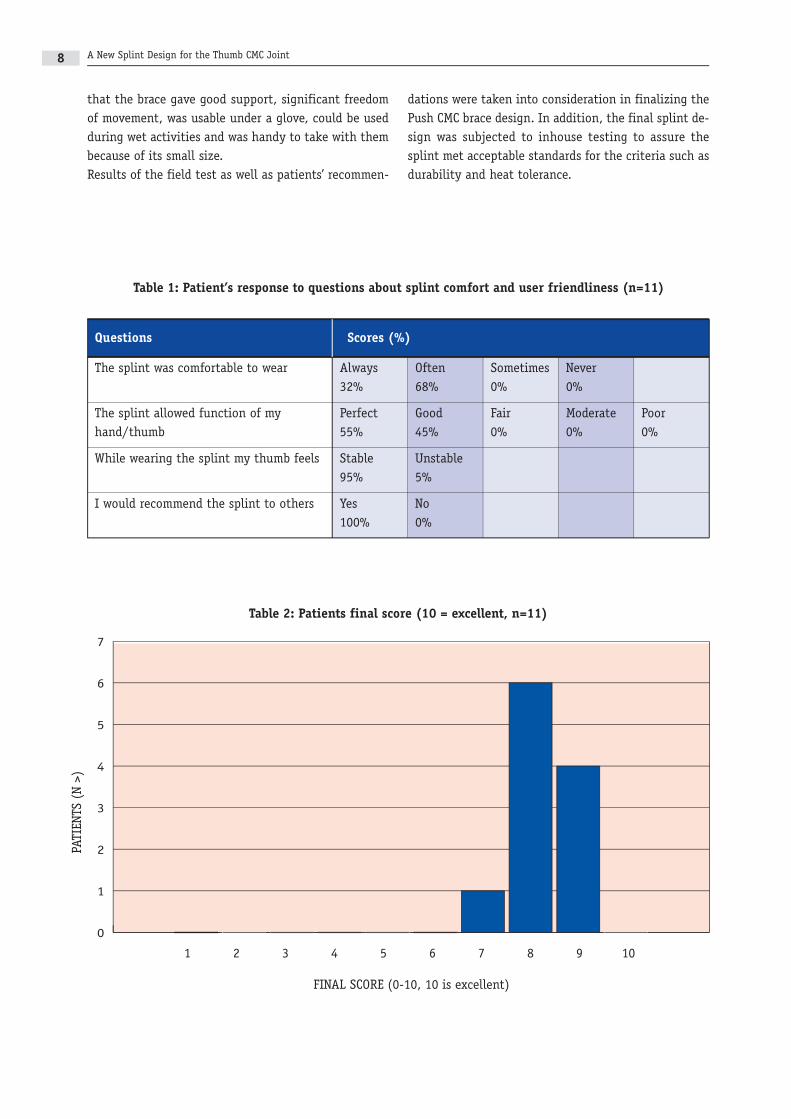
Results of Field Test After wearing the Push CMC prototype for 6 weeks allassessments were repeated. Grip and pinch strengthwere measured while wearing the brace. Comfort leveland user friendliness of the thumb splint were evalu-ated with a questionnaire specifically designed for thisstudy (Table 1) and the participants were asked to as-sign a final score of the brace on a visual analogue scale(0-10). (Table 2) For all participants the wearing sched-ule was different. A dentist and a photographer worethe splint mostly all day at work. Other patients usedthe splint from thirty minutes to two hours dependingon daily activities, such as computer work.According to the post wear assessments no significantchanges of thumb opposition, VAS for pain, or grip andpinch strength were noted. The self-report question-naire that records physical function and symptomsshowed significant improvement, indicating the pa-tients were able to function at a higher level with thissplint. Eleven participants answered the questionnaireon comfort level and userfriendliness of the thumbsplint, stating they foundthe brace always or oftenpleasant to wear. The func-tional use of the splintscored from very good to excellent. All patients wouldrecommend this brace to patients with a similar problem(Table 1). The brace was scored on the visual analoguescale (range 0-10, 10 is excellent) with a mean score of8.16 (SD 0.59). In the diary notes, patients mentioned
The aluminum insert is fitted to the thenararea while the muscles
are relaxed.
Patients scored functional use of the
splint good to excellent.
Nea CMCWhitepaper v2_Opmaak 1 1/12/10 14:46 Pagina 7
A New Splint Design for the Thumb CMC Joint8
that the brace gave good support, significant freedomof movement, was usable under a glove, could be usedduring wet activities and was handy to take with thembecause of its small size.Results of the field test as well as patients’ recommen-
dations were taken into consideration in finalizing thePush CMC brace design. In addition, the final splint de-sign was subjected to inhouse testing to assure thesplint met acceptable standards for the criteria such asdurability and heat tolerance.
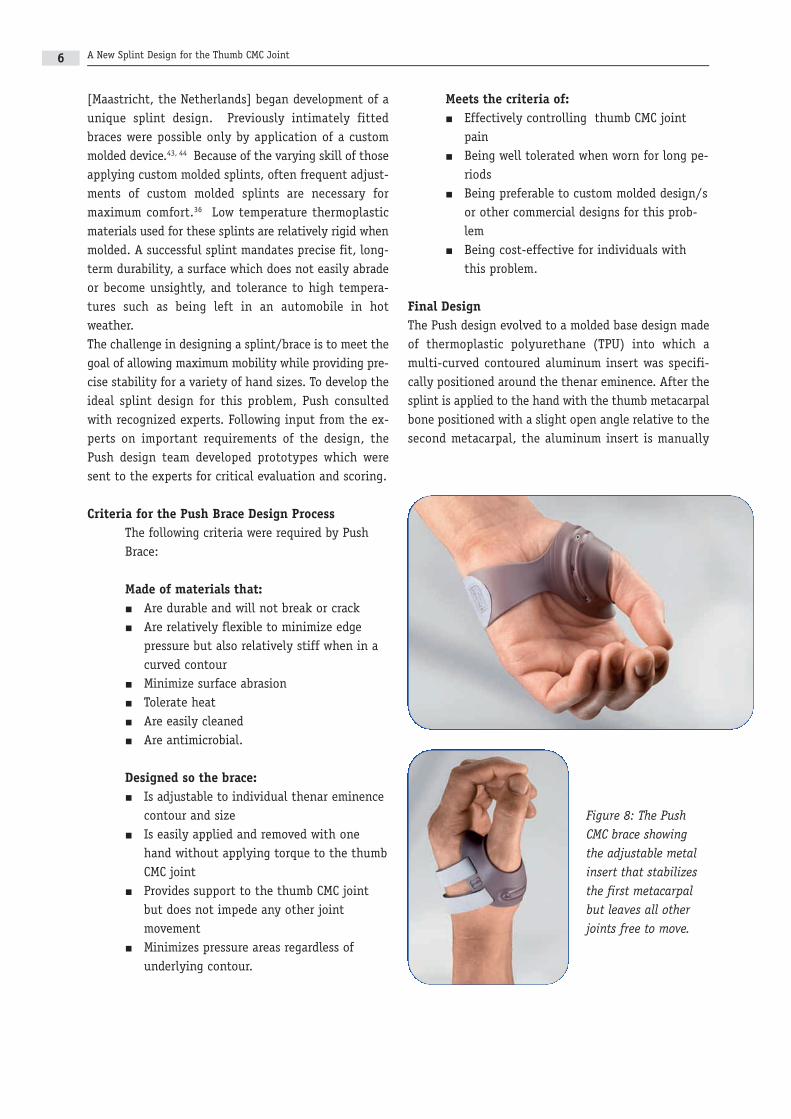
Table 1: Patient’s response to questions about splint comfort and user friendliness (n=11)
Questions Scores (%)
The splint was comfortable to wear Always Often Sometimes Never32% 68% 0% 0%
The splint allowed function of my Perfect Good Fair Moderate Poorhand/thumb 55% 45% 0% 0% 0%
While wearing the splint my thumb feels Stable Unstable95% 5%
I would recommend the splint to others Yes No100% 0%
Table 2: Patients final score (10 = excellent, n=11)
0
1
2
3
4
5
6
7
7654321 8 9 10
PATIEN
TS (N >)
FINAL SCORE (0-10, 10 is excellent)
Nea CMCWhitepaper v2_Opmaak 1 1/12/10 14:46 Pagina 8
A New Splint Design for the Thumb CMC Joint 9
CONCLUSIONS AND RECOMMENDATIONS
The authors find the final Push brace design highly de-sirable. Ms. Koekebakker feels the Push CMC brace is a
break-through in the treat -ment of thumb CMC jointpathology, optimally sup-porting the thumb CMCjoint while leaving otherjoints completely free. Shewas impressed by the abil-ity of the splint to be com-fortably worn by her
patients while maintaining thumb function. One par-ticipant, a dentist, was able to fully execute all activi-ties in his dental practice while wearing the splint andusing gloves.Ms. Colditz, having designed the small custom-fitteddesign discussed above, finds the Push splint to be anexceptional design. It is the only manufactured splintthat can be custom fitted around the thenar muscles toprecisely stabilize the thumb CMC joint while also al-lowing full mobility of the surrounding joints. She feelsthis design will change the current splinting approachto thumb CMC osteoarthritis.
REFERENCES
1. Barron OA, Glickel SZ, Eaton RG. Basal jointarthritis of the thumb. J Am Acad Orthop Surg2000;8(5):314-323.
2. Pai S, Talwalkar S, Hayton M. Presentation andmanagement of arthritis affecting the trapezio-metacarpal joint. Acta Ortho Belg 2006;72:3-10.
3. Van Heest A, Kallemeier P. Thumb carpalmetacarpal arthritis. J Am Acad Orthop Surg2008;16:140-151.
4. Pellegrini VDJ. Osteoarthritis at the base of thethumb. Orthop Clin North Am 1992;23(1):83-102.
5. Kuczynski K. Carpometacarpal joint of the humanthumb. J Anat 1974;118(1):119-126.
6. Pellegrini VDJ. Pathomechanics of the thumbtrapeziometacarpal joint. Hand Clin2001;17(2):175-184.
7. Leversedge FJ. Anatomy and pathomechanics ofthe thumb. Hand Clin 2008;24:219-229.
8. King JA, Tomaino MM. Surgical treatment of therheumatoid thumb. Hand Clin 2001;17(2):275-289.
9. Bettinger P, Berger RA. Functional ligamentousanatomy of the trapezium andtrapeziometacarpal joint (gross and arthro-scopic). Hand Clin 2001;17(2):151-168.
10. Bojsen-Møller F. Osteoligamentous guidance ofthe movements of the human thumb. Am J Anat1976;147(1):71-80.
11. Kuczynski K. Configuration of the articular sur-faces of the carpometacarpal joint of the thumb.Handchir Mikrochir Plast Chir 1983;15(3):191-193.
12. Dorland’s Medical Dictionary [online] 2010. 13. National Collaborating Centre for Chronic Condi-
tions. Osteoarthritis: national clinical guidelinefor care and management in adults. London:Royal College of Physicians, 2008.
14. Zhang Y, Niu J, Kelly-Hayes M, et al. Prevalanceof symptomatic hand osteoarthritis and its im-pact on functional status among the elderly: TheFramingham Study. Am J Epidemiol2002;156(11):1021-1027.
15. Dias R, Chandrasenan V, Burke F. Basal thumbarthritis. Postgrad Med J 2007;83:40-43.
The Push brace meetsthe criteria of providingprecise stability while
allowing maximum mobility of the
surrounding joints.
Nea CMCWhitepaper v2_Opmaak 1 1/12/10 14:46 Pagina 9
A New Splint Design for the Thumb CMC Joint10
16. Poole JU, Pellegrini VDJ. Arthritis of the thumbbasal joint complex. J Hand Ther 2000;13(2):91-107.
17. Swigart CR. Arthritis of the base of the thumb.Curr Rev Musculoskelet 2008;1:142-146.
18. Armstrong A, Hunter JDT. The prelevance of de-generative arthritis of the base of the thumb inpostmenopausal women. J Hand Surg Am.1994;24A(1):340-341.
19. Eaton RG, Glickel SZ. Trapeziometacarpal os-teoarthritis: staging as a rationale for treatment.Hand Clin 1987;3(4):455-471.
20. Sonne-Holm S, Jacobsen S. Osteoarthritis of thefirst carpometacarpal joint: a study of radiologyand clinical epidemiology. Results from theCopenhagen osteoarthritis study. Osteoarth Cart2006;14:496-500.
21. Fontana L, Neel S, Claise J-M, Ughetto S, CatilinaP. Osteoarthritis of the thumb carpometacarpaljoint in women and occupational risk factors: acase-control study. J Hand Sur Am.2007;32A(4):459-456.
22. Dahaghin S, Bierma-Zeinstra S, Ginai A, et al.Prevalence and pattern of radiographic hand os-teoarthritis and association with pain and dis-ability (the Rotterdam study). Ann Rheum Dis2005;64(5):682-687.
23. Haara M, Heliövaara M, Kröger H, et al. Osteoarthritis in the carpometacarpal joint of thethumb. Prevalance and associations with disabil-ity and mortality. J Bone Joint Surg 2004;86-A(7):1452-1457.
24. Murphy N, Dasari B, Adams J. A review of os-teoarthritis of the trapeziometacarpal joint(TMJ). Jour Rheum Occup Ther 2009;24(1):8-11.
25. Wilder F, Barrett J, Farina E. Joint-specificprevalance of osteoarthritis of the hand. Os-teoarth Cartilage 2006;14(9):953-957.
26. Dziedzic K, Thomas E, Hill S, Wilkie R, Peat G,Croft P. The impact of musuloskeletal hand problems in older adults: findings from the NorthStaffordshire Osteoarthritis Project (NorstOP).Rheumatology 2007;46:963-967.
27. Terrono AL, Nalebuff EA, Philips CA. The rheuma-toid thumb. In: Hunter JM, Mackin EJ, CallahanAD, editors. Rehabilitation of the Hand. 4 ed. St.Louis: Mosby-Year Book, Inc.; 1995:1329-1343.
28. Pellegrini VDJ. The basal articulations of thethumb: pain, instability, and osteoarthritis. In:Peimer CA, editor. Surgery of the hand and upperextremity. New York: McGraw-Hill; 1996:1019-1042.
29. Zhang W, Doherty M, Leeb B et al. EULAR evi-dence based recommendations for the diagnosisof hand osteoarthritis-report of task force of theEULAR Standing Committee for InternationalClinical Studies Including Therapeutics (ESCISIT).Ann Rheum Dis 2007;66:377-388.
30. Boustedt C, Nordenskiöld U, Lundgren Nilsson A.Effects of a hand-joint protection programmewith an addition of splinting and exercise. ClinRheumatol 2009;28:793-799.
31. Berggren M, Joost-Davidsson A, Lindstrand J, Ny-lander G, Povlsen B. Reduction in the need foroperation after conservative treatment of os-teoarthritis of the first carpometacarpal joint: aseven year prospective study. Scand J Plast Re-constr Hand Surg 2001;35:415-417.
32. Swigart C, Eaton R, Glickel S, Johnson C. Splint-ing in the treatment of arthritis of the first car-pometacarpal joint. J Hand Surg Am.1999;24A(10):86-91.
33. Weiss S, LaStayo P, Mills A, Bramlet D. Prospec-tive analysis of splinting the first car-pometacarpal joint: an objective, subjective andradiographic assessment. J Hand Ther2000;13(3):218-227.
34. Weiss S, LaStayo P, Mills A, Bramlet D. Splintingthe degenerative basal joint: Custom-made orprefabricated neoprene? J Hand Ther2004;17(4):401-406.
35. Egan M, Brousseau L. Splinting for osteoarthritisof the carpometacarpal joint: review of the evi-dence. Am J Occup Ther 2007;61(1):70-78.
36. Rannou F, Dimet J, Boutron I, et al. Splint forbase-of-thumb osteoarthritis. Annals Int Med2009;150(10):661-669.
37. Wajon A. Clinical splinting successes: the thumb“strap splint” for dynamic stability of thetrapeziometacarpal joint. J Hand Ther2000;13(3):236-237.
Nea CMCWhitepaper v2_Opmaak 1 1/12/10 14:46 Pagina 10
A New Splint Design for the Thumb CMC Joint 11
38. Wajon A, Ada L. No difference between two splintand exercise regimens for people with osteo -arthritis of the thumb: A randomised controlledtrial. Aust J Physio 2005;51:245-249.
39. Carreira A, Jones A, Natour J. Assessment of theeffectiveness of a functional splint for os-teoarthritis of the trapeziometacarpal joint of thedominant hand: a randomized controlled study. JRehabil Med 2010;42:469-474.
40. Valdes KA, Marik T. A systematic review of conservative interventions for osteoarthritis ofthe hand. J Hand Ther 2010;23(4):334-351.
41. Sarmiento A. Functional fracture bracing: an up-date. Instr Course Lect 1987;36:371-376.
42. Segal R, Avrahami E, Lebdinski E, et al. The im-pact of hemiparalysis on the expression of os-teoarthritis. Arthritis Rheum 1998;41:2249-2256.
43. Colditz JC. Anatomic considerations for splintingthe thumb. In: Hunter JM, Mackin EJ, CallahanAD, editors. Rehabilitation of the hand. 4th ed.St. Louis: Mosby; 1995:1161-1172.
44. Colditz JC. The biomechanics of a thumb CMC im-mobilization splint: design and fitting. JourHand Ther 2000;13:228-235.
45. Carlsson AM. Assessment of chronic pain. I. As-pects of the reliability and validity of the visualscale. Pain 1983;16(1):87-101.
46. Kapandji A. Clinical evaluation of the thumb’sopposition. J Hand Ther 1992;5:102-106.
47. American Society of Hand Therapists. Clinical as-sessment recommendations. Garner, NC: AmericanSociety of Hand Therapists; 1981.
48. Mathiowetz V, Weber K, Volland G, Kashman N.Reliability and validity of grip and pinchstrength evaluations. J Hand Surg 1984;9A:222-226.
About the Authors
Judy Colditz is an internationally recognized expert onhand therapy who has written numerous articles,chapters and given papers and workshops in morethan 24 countries. Currently Ms. Colditz developseducational DVD/CD modules for hand therapists.In her 38 years of experience she has focused onthe problems of the CMC thumb joint. Ms. Colditzis past president of both the American Society ofHand Therapists and the International Federationof Societies for Hand Therapy.
Nettie Koekebakker is a Certified Hand Therapist inthe Netherlands who has worked in the AcademicMedical Centre in Amsterdam for 30 years and forthe last 20 years has specialized as a hand thera-pist. Since 2007 she has worked at 4hands, a pri-vate hand therapy clinic in Amsterdam. Ms.Koekebakker is an active member of the Dutch As-sociation of Hand Therapists.
Colditz JC, Koekebakker N. (2010) A New Splint Designfor the Thumb CMC Joint [White Paper] published byNea International bv / Push Braces, Maastricht-Airport,the Netherlands, www.push.eu
Nea CMCWhitepaper v2_Opmaak 1 1/12/10 14:46 Pagina 11

Nea CMCWhitepaper v2_Opmaak 1 1/12/10 14:46 Pagina 12