Embed Size (px)
Citation preview

Artificial Organs 8(4):478-480, Raven Press, New York 0 1984 International Society for Artificial Organs
A New Perfusion Circuit for the Newborn with Lung Immaturity: Extracorporeal CO, Removal via an Umbilical
Arteriovenous Shunt During Apneic 0, Diffusion
Stephan Schmidt, Joachim W. Dudenhausen, Klaus Langner, Christian Laiblin, and Erich Z. Saling
Institute of Perinatal Medicine, Free University of Berlin, Berlin, F.R.C.
Abstract: In spite of improved prophylaxis and therapy, the respiratory distress syndrome is still a major cause of morbidity and mortality in premature babies. Owing to the fact that a number of patients are unresponsive to other methods of neonatal care, an increasing number of perinatal centers have started to treat this group of pa- tients with extracorporeal membrane oxygenation suc- cessfully. To make the extracorporeal gas exchange more practicable for the neonate directly after birth, a modifi- cation of this method using an umbilical arteriovenous shunt for CO, removal in apneic premature lambs as an
animal model was evaluated. A miniaturized low-resis- tance extracorporeal circuit that is totally incorporated in a regular intensive care baby incubator was developed. The benefit of using extracorporeal CO, removal in very low birth weight newborns could be a conditioning of the premature lung during a short period of bypass, after which ventilation at nontraumatic pressures and nontoxic 0, concentrations would become possible. Key Words: Respiratory distress syndrome-Premature lamb-Ar- teriovenous shunt - Extracorporeal CO, removal-Ap- neic 0, diffusion.
One main cause of morbidity and mortality in pre- mature babies is the respiratory distress syndrome (1). This is so in spite of the introduction of new methods for the prophylaxis and therapy of this dis- ease in the last years. Recently, long-term respira- tory support with extracorporeal membrane oxy- genation by an extracorporeal circuit in newborn infants with respiratory distress syndrome was per- formed successfully in several pediatric centers as an ultimate mode of therapy (2). A further advance in extracorporeal gas exchange systems was made when Kolobow and co-workers evaluated the method of extracorporeal CO, removal during 0, diffusion in the apneic lung in animal experiments (3-5). The authors have developed such an extra- corporeal circuit that is adapted to the situation of the premature newborn.
MATERIALS AND METHODS The extracorporeal circuit, which was totally in-
corporated into an intensive care baby incubator
Received November 1, 1983; revised April 30, 1984. Address correspondence and reprint requests to Dr. S .
Schmidt at Institute of Perinatal Medicine, Freie Universitat Berlin, Mariendorfer Weg 28, D-1000 Berlin 44, F.R.G.
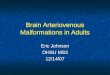
(Dragenverk AG, Lubeck, F.R.G.), included a 0.4- m2 SciMed Kolobow membrane lung (SciMed, Life Systems Inc., Minneapolis, MN, U.S.A.), catheters for the umbilical artery and vein, 3/16-in. Tygon tubing (Norton Industrial Plastics, Chaineux, Bel- gium), and a flow probe Sensor Could-Statham SP 7517 (Medical Products Division, Gould Inc., Ox- nard, CA, U.S.A.) (Fig. 1). It had a priming volume of only 116 ml. After a CO, gas flush, a vacuum was applied to the perfusion circuit, and saline so- lution as well as adult sheep blood were poured into the extracorporeal circuit and brought to a temper- ature of 37°C. The gas mixture of the membrane lungs was pure oxygen at a rate of 2 L/min at max- imum. A controlled vacuum of 200 mm Hg below atmospheric pressure was applied at the gas outlet port during perfusion.
Preterm lamb fetuses of 128-130 days of gesta- tion were studied. A cesarean section was per- formed during epidural anesthesia in five pregnant ewes, delivering premature lambs weighing 2.5-3.5 kg. Placed on the abdomen of the ewe, the lamb was then intubated with an endotracheal tube. Up to the moment of connection to the perfusion cir- cuit, manual ventilation with room air was provided
4 78

CO, REMOVAL VIA UMBILICAL A-V SHUNT 4 79
@
by means of a bag. For the cannulation of one um- bilical artery and vein, thin-walled large-bore cath- e te rs embedding a s ta inless-s teel spring were used. These catheters were advanced, respectively, into the aorta and the vena cava. Directly after can- nulation, heparin (0.1 mg/kg) and pancoronium (0.01 mg/kg) were injected into the lamb. The lamb was then placed in the thermostatically heated baby incubator.
After the start of the perfusion, the intratracheal tube was connected to a continuous positive airway pressure (CPAP) system regulated at a pressure of 13 cm H 2 0 to provide a constant intrapulmonary pressure. Oxygen was insufflated through a small catheter, the tip of which was located in the trachea near its bifurcation, at a rate of 200 ml/min. By means of continuous infusion, a prostacyclin ana- log (Schering ZK 36374; Schering AG, Berlin 65, F.R.G.) was applied at a constant rate of 600 ng/ kg/min to inhibit the aggregation of the thrombo- cytes (6).
RESULTS While the flow rate in the extracorporeal circuit
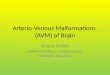
was gradually increased to 70 mlikgimin, sufficient CO, removal and transalveolar oxygenation were provided. In Fig. 2, for example, the synchronously collected data during extracorporeal CO, removal in one lamb are shown polygraphically. Note that there was only a minor drop in blood pressure at the beginning of the perfusion. The range of Pcoz values achieved by a CO, removal of 9-14 ml/kg/ min was between 55 and 65 mm Hg. Whereas Pcoz and Po, values during the perfusion were rather stable, a reversible drop of the pH values during the first 1.5 h was noted.
DISCUSSION The results from several perinatal care centers
that provide extracorporeal gas exchange for new-
13cm H 2 0
FIG. 1. An extracorporeal circuit for COP removal via an umbilical arterio- venous shunt in the premature lamb. 1, infusion; 2, gas flowmeter; 3, blood flowmeter; 4, capnograph; 5, blood pump; 6, vacuum pump; 7, baby incubator; ML, membrane lung; UA, arteria umbilicalis; UV vena umbilicalis. The premature lamb was placed in the intensive care incubator after connection to the extracorporeal circuit and the continuous positive airway pressure (CPAP) system. The perfusion circuit is completely housed within the ther- mostatically heated incubator.
borns who are unresponsive to other modes of therapy indicate that giving the lung time to rest during extracorporeal gas exchange decreases bron- chopulmonary dysplasia, intracranial bleeding, and mortality (2). Such an extracorporeal circuit that was adapted to the situation of the premature new- born using the lamb as an animal model was tested. A cannulating system via the umbilical artery and umbilical vein was used to avoid the sacrifice of other vessels and to make the method more prac- ticable and usable for the human neonate. Although this procedure is manageable at birth while umbil- ical vessels are still pulsating, it might become more difficult to advance large bore catheters via the um- bilical vessels after an interval of time. Using a 0.4-m2 membrane lung, a stable Pco, level was achieved. Absolute values, though, were somewhat elevated compared with the physiological range of arterial Pco, of the newborn. For a 3-kg lamb, the use of a 0.8-m2 membrane might, therefore, be more adequate. With its placement, the necessity of 100% 0, in the extracorporeal gas circuit would be elim- inated. This would considerably increase the safety, as potentially deleterious effects on the natural lungs caused by denitrogenation would be avoided. On the other hand, a 0.4-m2 lung might be sufficient for future application in smaller lambs or premature newborn infants.
With an umbilical artery-to-umbilical vein circuit, a biological circuit was not only imitated, but also the risk of microemboli reaching the brain (com- pared with that of a venoarterial mode of perfusion) was minimized (2). Operation of such an arterio- venous shunt can be tolerated by the myocardium of the newborn infant, so that the necessity of using a mechanical pump may be abandoned if the circuit has a low resistance (7).
Longer-term studies will determine if a blood flow of 70 ml/kg/min from an artery to a vein in the
A r r f Organs, Vol. 8, N o . 4 , 1984

480 S . SCHMIDT ET A L .
rnllrnin. kg 20
1 5 1 VCO,
rnrnHg A P C O ~
mrnHg
loo 1
5 o J
rnrnHg
180 P o 2
120
80 100 ' 7.2
blrnin 200
HF
100
rnrnHg 70 -. BPM
6 0 j j 50
rnllrnin Q
I I I I I I I I
0 120 240 360 480Imin) t
FIG. 2. Synchronously collected data during extracorporeal CO, removal in a premature lamb. Vco,, volume of extracor- poreal CO, removal; A Pco,, Pco, difference between blood inlet and blood outlet port of membrane lung; Pco,, PCO, of the umbilical artery; Po,, Po, of the umbilical artery; pH, pH of the umbilical artery; HF, heart frequency; BPM, blood pressure (aorta); Q, blood flow in the perfusion circuit.
presence of a closed ductus arteriosus is too high a load on a chronic basis. In a pumpless arteriove- nous shunt, the blood flow rate will depend on the arterial pressure. The vasomotor effect of CO, may in this way be an element of feedback, as a rise of CO, would lead to a higher flow through the shunt and thereby to a higher CO, removal. In this way, the pumpless operation of an arteriovenous shunt might be extremely stable and simplify the manage- ment of an extracorporeal circuit (7).
Although extracorporeal gas exchange has been proposed as an additional mode of therapy for the premature newborn with lung immaturity, it has not yet become widespread. Thus, further evaluation of such systems should aim at simplifying the perfu- sion technology and improving the biocompatibility of the systems to make technological or biological complications less likely. The evaluation of the per- fusion circuit described in this article might be a step in this direction.
Acknowledgment: This work was supported by a grant from the Deutsche Forschungsgemeinschaft (DU
REFERENCES 1 . Taghizadeh A, Reynolds EOR. Pathogenesis of broncho-
pulmonary dysplasia following hyaline membrane disease. A m J Pathol 1976;82:241-7.
2. Bartlett RH, Andrews AF, Toomasian JM, Haiduc NJ, Gaz- zaniga AB. Extracorporeal membrane oxygenation for new- born respiratory failure: forty-five cases. Surgery 1982;92: 425 -33.
3. Kolobow T, Gattinoni L, Tomlinson T, Pierce JE. An alter- native to breathing. J Thorac Cardiovnsc Surg 1979;75: 261-6.
4. Gattinoni L, Agostoni A, Pesenti A, Pelizzola A, Rossi GP, Langer M, Vesconi S , Uziel L, Fox U, Longoni L, Kolobow T, Damia G . Treatment of acute respiratory failure with low frequency positive pressure ventilation and extracorporeal removal of CO,. Lancet 1980;2:292-4.
5 . Pesenti A, Kolobow T, Buckhold DK, Pierce JE, Huang H, Catchen V. Prevention of hyaline membrane disease in pre- mature lambs by apneic oxygenation and extracorporeal carbon dioxide removal. Intens Cure Med 1982;8:11-5.
6 . Schror K, Darius H, Matzky R , Ohlendorf R. The anti- platelet and cardiovascular actions of a new carbacyclin de- rivative (ZK 36 374) equipotent to PGJ, in vitro. Naunyn Schmiedebergs Arch Pharmacol 1982;29(suppl R):3 16-20.
7. Barthelemy R, Galletti PM, Trudell LA, MacAndrew J , Richardson PD, Puel P, Enjalbert A. Total extracorporeal C0,-removal in a pumpless artery-to-vein shunt. Trans Am SOC Artif Intern Organs 1982;28:354-7.
126/1-1).
Artif Organs, Vol. 8, No . 4 , 1984