Embed Size (px)
Citation preview

A New Future In Heart Failure(Should we reshuffle the deck?)
DR. HEMANT SAHA, MD, MRCP(UK)AGA KHAN UNIVERSITY HOSPITAL, NAIROBI

Disclosures
Nothing to disclose.
Objectives1. Historical Perspectives2. Heart Failure to date (GDMT in HFrEF)3. Un‐Met Needs4. HF ‐ Neuroendocrine Disease5. Case Presentations6. PARADIGM‐HF 7. Conclusions
“If I have seen further, it is by standing on the shoulder of giants.”
‐ Isaac Newton, 1676 ‐
1. Historical Perspectives
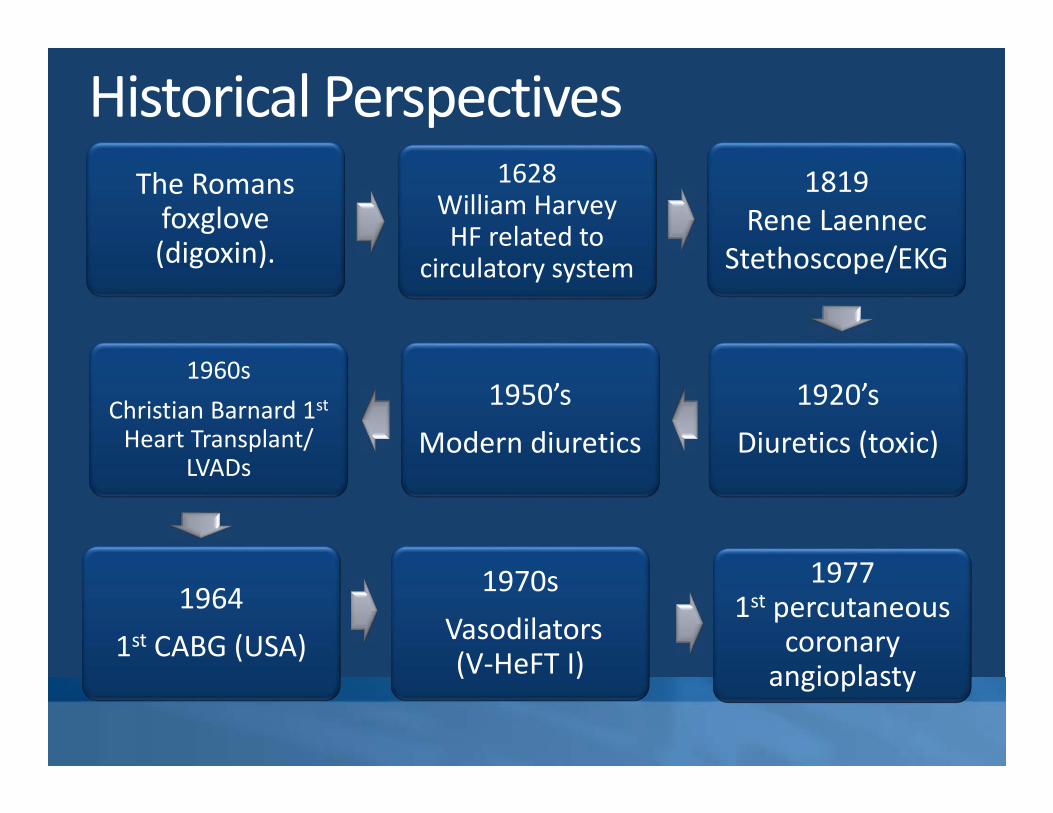
Historical PerspectivesThe Romans foxglove (digoxin).
1628 William Harvey HF related to
circulatory system
1819 Rene Laennec
Stethoscope/EKG
1920’sDiuretics (toxic)
1950’sModern diuretics
1960sChristian Barnard 1stHeart Transplant/
LVADs
1970sVasodilators (V‐HeFT I)
1977 1st percutaneous
coronary angioplasty
19641st CABG (USA)
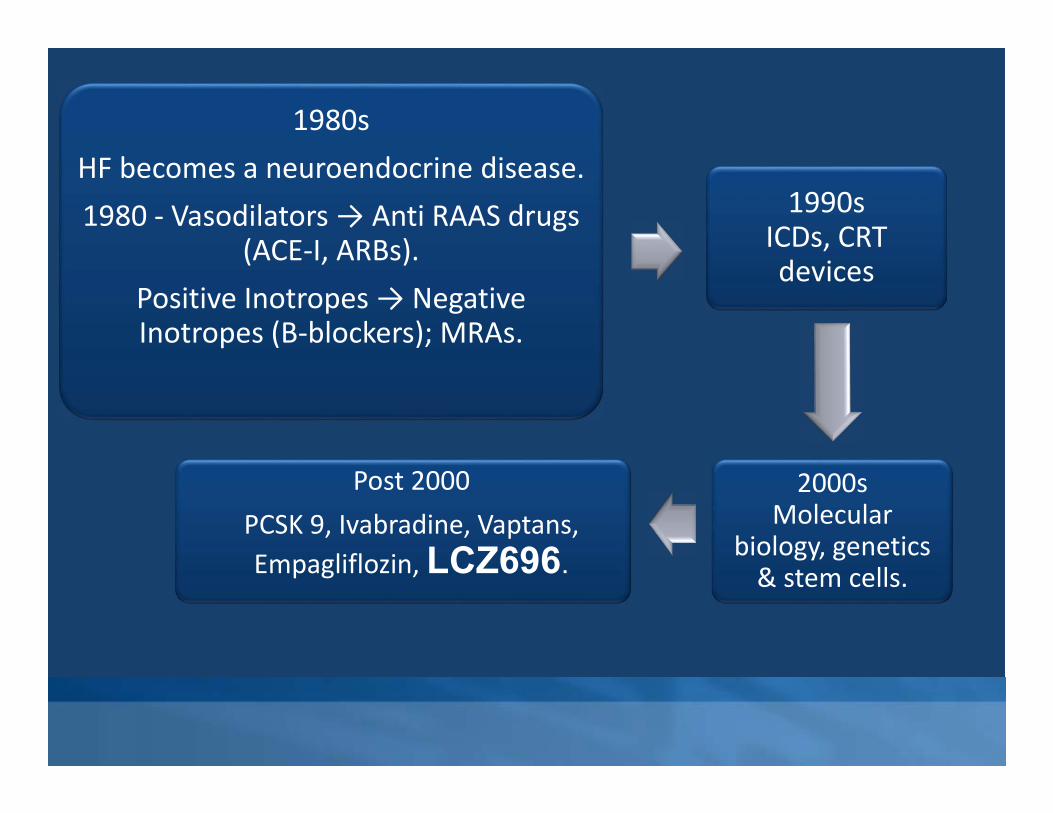
1980sHF becomes a neuroendocrine disease. 1980 ‐ Vasodilators → Anti RAAS drugs
(ACE‐I, ARBs). Positive Inotropes → Negative Inotropes (B‐blockers); MRAs.
1990s ICDs, CRT devices
2000s Molecular
biology, genetics & stem cells.
Post 2000PCSK 9, Ivabradine, Vaptans, Empagliflozin, LCZ696.

2. Heart Failure To Date (GDMT in HFrEF)
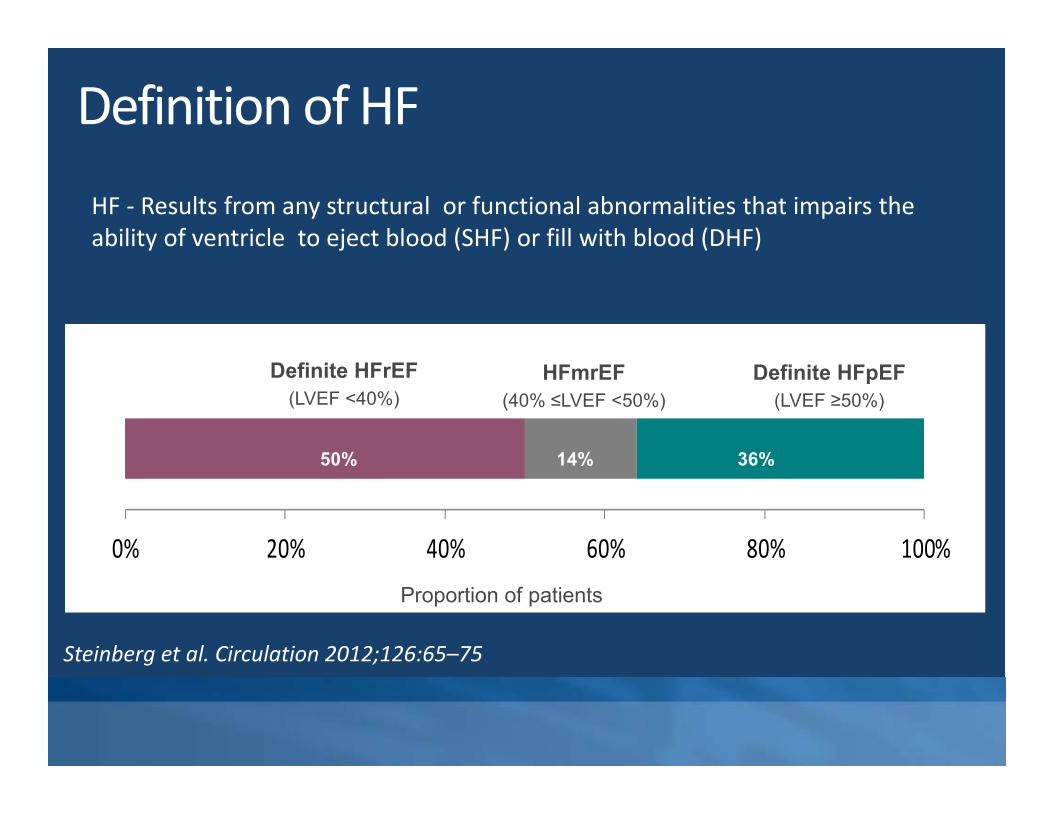
Definition of HF
0% 20% 40% 60% 80% 100%
Definite HFpEF(LVEF ≥50%)
Definite HFrEF(LVEF <40%)
HFmrEF(40% ≤LVEF <50%)
Proportion of patients
14%50% 36%
HF ‐ Results from any structural or functional abnormalities that impairs the ability of ventricle to eject blood (SHF) or fill with blood (DHF)
Steinberg et al. Circulation 2012;126:65–75

GDMT
ESC Guidelines until 2016 (modified)
• Ivabradine, HR>70bpm• ICD +/‐ CRT in Eligible Pts
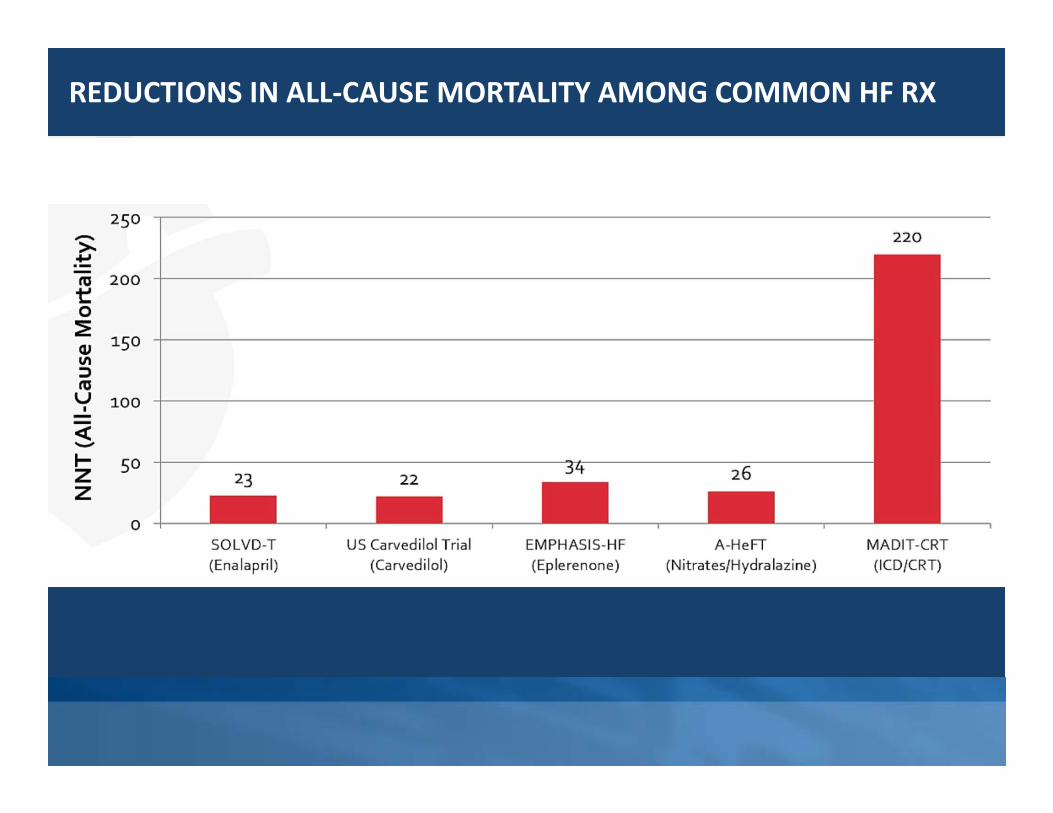
REDUCTIONS IN ALL‐CAUSE MORTALITY AMONG COMMON HF RX

3. Un‐Met Needs
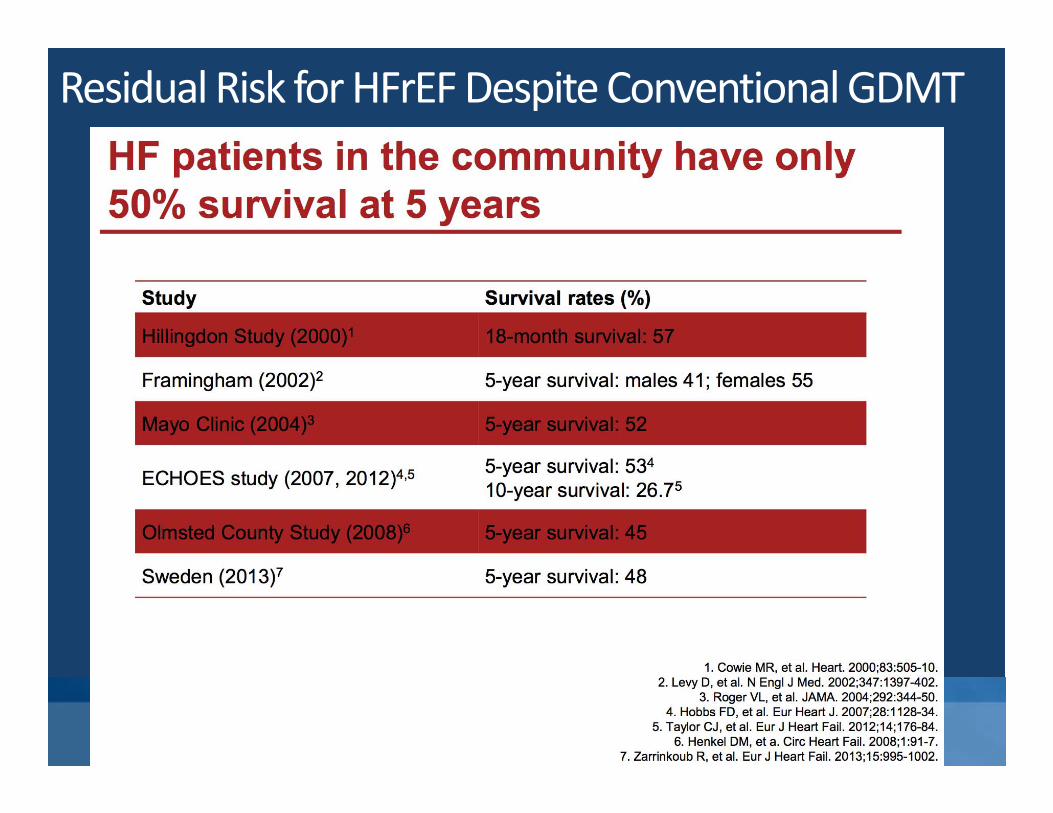
Residual Risk for HFrEFDespite Conventional GDMT
4. HF ‐Neuroendocrine Disease

HFrEF
NEUROENDOCRINE MODEL –Pharmacological Approaches
EpinephrineNorepinephrine α1, β1, β2
receptors
VasoconstrictionRAAS activityVasopressinHeart rate
Contractility
Sympathetic nervous system
Ang II AT1R
VasoconstrictionBlood pressure
Sympathetic toneAldosteroneHypertrophy
Fibrosis
Renin‐angiotensin‐aldosterone‐system
NPRs NPs
VasodilationBlood pressureSympathetic toneVasopressinAldosteroneFibrosisHypertrophy
Natriuretic peptide system1
NEPRILYSIN
SACUBUTRIL
B‐BLOCKER
• The crucial importance of the RAAS is supported by the beneficial effects of ACEIs, ARBs and MRAs1
• Benefits of β‐blockers indicate that the SNS also plays a key role1
LCZ696ARBACE‐IVALSARTAN
1. McMurray et al. Eur Heart J 2012;33:1787–847; Figure References: Levin et al. N Engl J Med 1998;339:321–8; Nathisuwan & Talbert. Pharmacotherapy 2002;22:27–42; Kemp & Conte. Cardiovascular Pathology 2012;365–71; Schrier & Abraham. N Engl J Med 2009;341:577–85

Dual Acting ARNI
Sacubutril(NeprilysinInhibitor)
↑ ANP,BNP,CNP & Other
Vasoactive Peptides
↑ Bradykinin ↑ Ang II
Valsartan (ARB)
AT1Receptor
ARNI CONCEPT
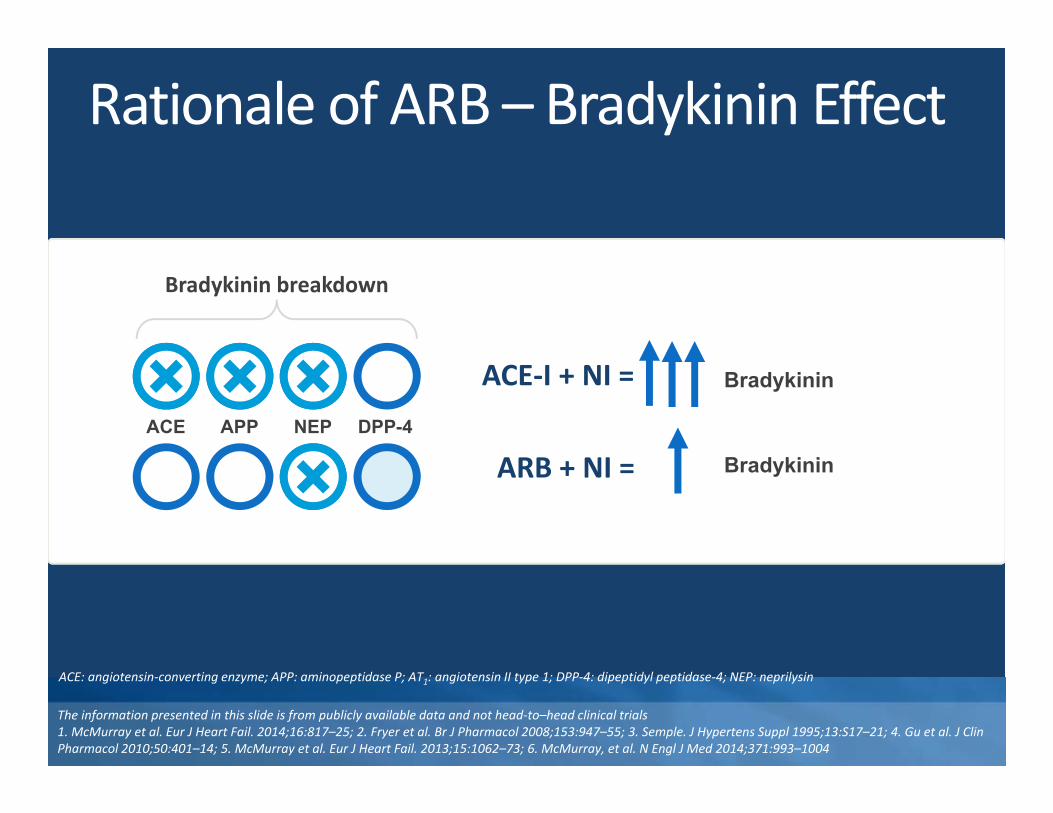
Rationale of ARB – Bradykinin Effect
Bradykinin
ACE APP NEP DPP-4
Bradykinin breakdown
ACE‐I + NI =
ARB + NI = Bradykinin
ACE: angiotensin‐converting enzyme; APP: aminopeptidase P; AT1: angiotensin II type 1; DPP‐4: dipeptidyl peptidase‐4; NEP: neprilysin
The information presented in this slide is from publicly available data and not head‐to–head clinical trials1. McMurray et al. Eur J Heart Fail. 2014;16:817–25; 2. Fryer et al. Br J Pharmacol 2008;153:947–55; 3. Semple. J Hypertens Suppl 1995;13:S17–21; 4. Gu et al. J Clin Pharmacol 2010;50:401–14; 5. McMurray et al. Eur J Heart Fail. 2013;15:1062–73; 6. McMurray, et al. N Engl J Med 2014;371:993–1004
5. Case Presentations

Case 1
55 year old diplomat.
Known to have anthracycline induced long
standing DCM (EF‐25%)
Admitted with ADHF secondary to pneumonia
This was a second admission within 3 months .
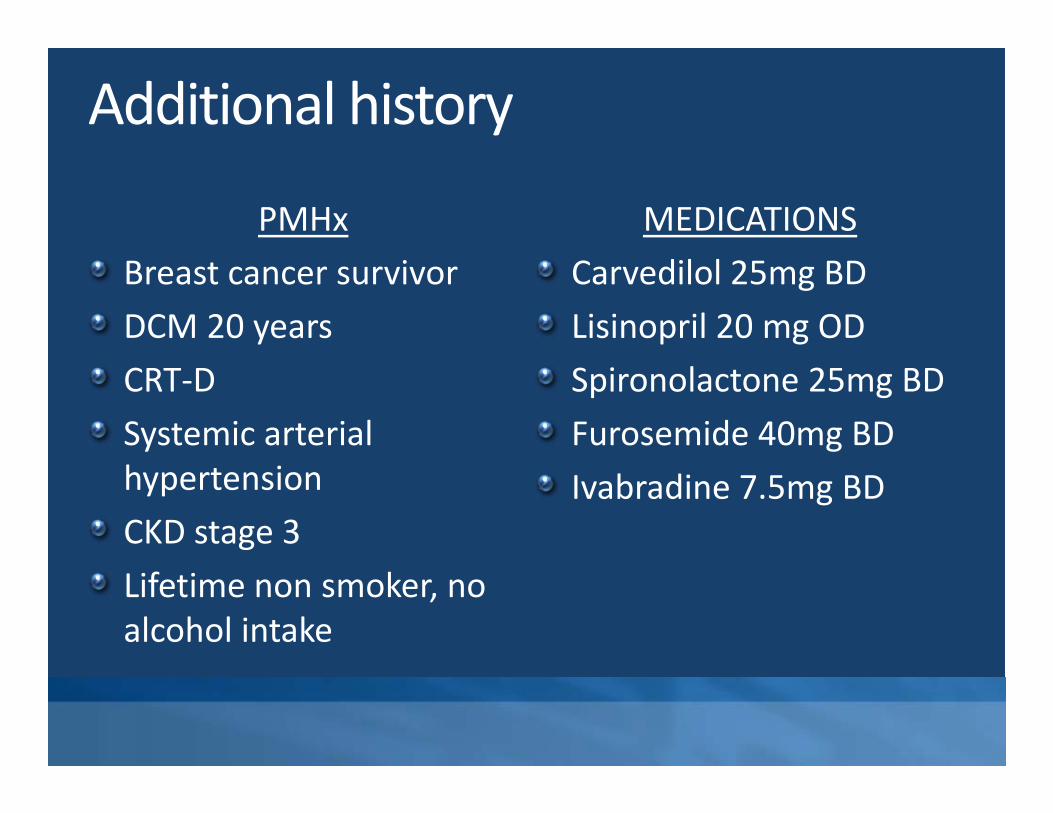
Additional history
PMHxBreast cancer survivorDCM 20 yearsCRT‐D Systemic arterial hypertensionCKD stage 3Lifetime non smoker, no alcohol intake
MEDICATIONSCarvedilol 25mg BDLisinopril 20 mg ODSpironolactone 25mg BDFurosemide 40mg BDIvabradine 7.5mg BD

Cardiac work‐up
12 lead ECGSinus rhythm, LBBB, QRS 130msec
2D ECHOLVEF 25%Global hypokinesiaMild MRPASP 45mmHg
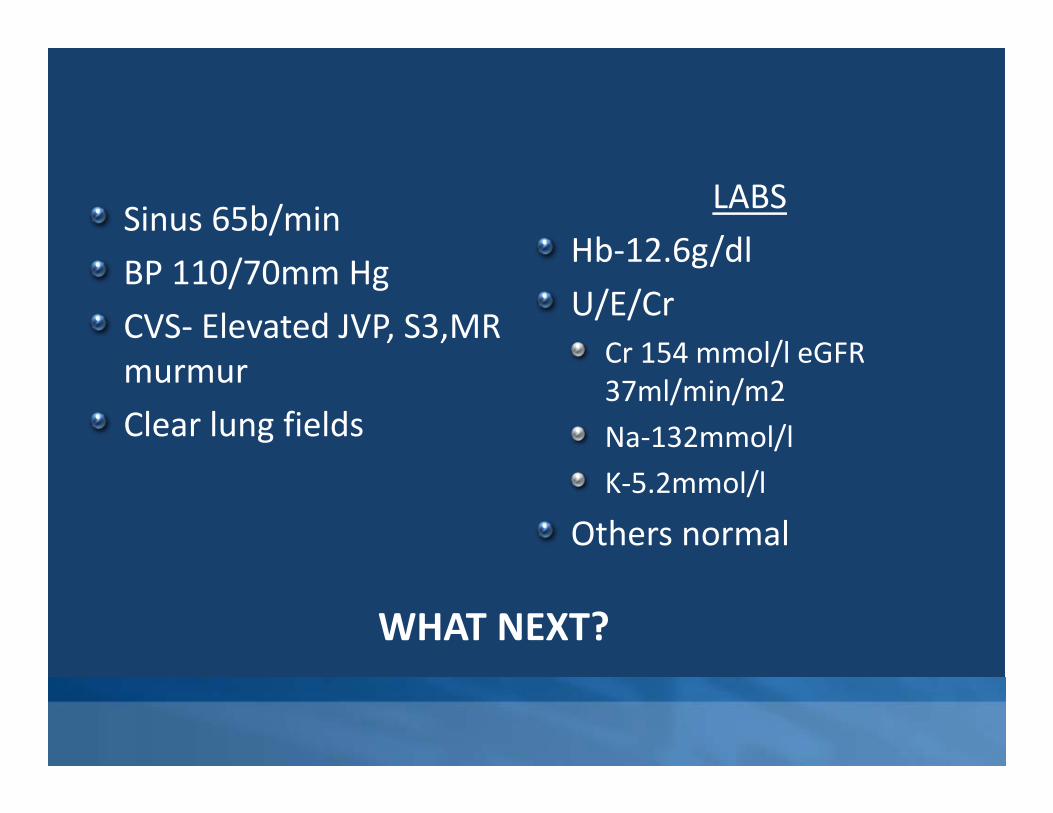
Sinus 65b/minBP 110/70mm HgCVS‐ Elevated JVP, S3,MR murmur Clear lung fields
LABS Hb‐12.6g/dlU/E/Cr
Cr 154 mmol/l eGFR37ml/min/m2Na‐132mmol/lK‐5.2mmol/l
Others normal
WHAT NEXT?

Case Presentation ‐ 2D.W. - 75YRS, MaleCo-morbids: HTN, IHD – PCI → LAD (2011), Ca. ProstatePresentation – Dyspnea, NYHA IV, fluid overload statePrevious Drug Regime
Lasix 40mg ODAldactone 25mg ODRamipril 5mg ODAtorvastatin 20mg ODAspirin 75mg ODCarvedilol 6.25mg BD

LabsNTProBNP>3000Hb 11.8Creatinine 86Urea 9.4Na 130/ K 4.2HsTrop x 2 ‐ <3.0Others ‐ normalX‐Ray
Increased CTR, Right small pleural effusion, mild pulmonary edema
ExaminationHR 90bpm; RR 25/min; BP 108/60mmHgJVP raised, S3 gallop, no murmurs Right pleural effusion – mildTender hepatomegaly, ascites, gross scrotal edema.Neurological exam ‐ Normal
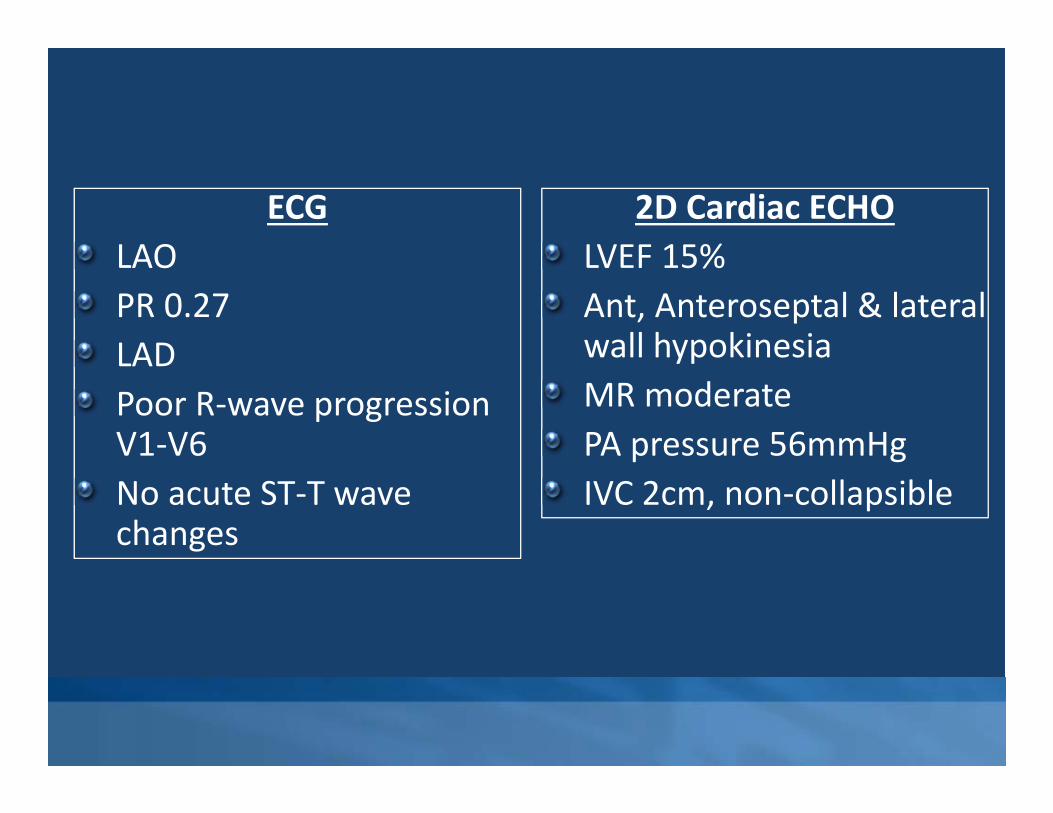
ECGLAOPR 0.27LADPoor R‐wave progression V1‐V6No acute ST‐T wave changes
2D Cardiac ECHOLVEF 15%Ant, Anteroseptal & lateral wall hypokinesiaMR moderatePA pressure 56mmHgIVC 2cm, non‐collapsible
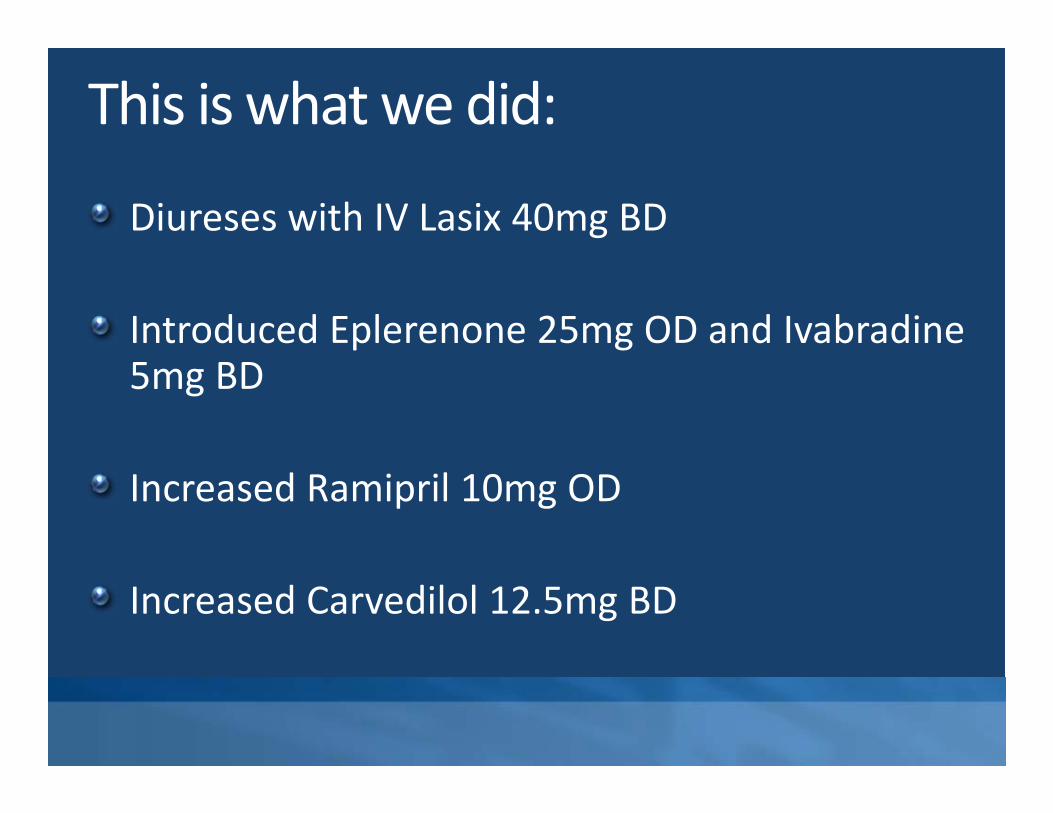
This is what we did:
Diureses with IV Lasix 40mg BD
Introduced Eplerenone 25mg OD and Ivabradine5mg BD
Increased Ramipril 10mg OD
Increased Carvedilol 12.5mg BD
OutcomeHR stabilized 60bpm, occasional PVCsBP 108/65mmHg. Minimal pedal edemaS3 positive, mild mitral systolic murmurNo lung rales.Lab parameters remained normal with slight worsening UEC’s.Urea 14; Creatinine 100; Na 137; K 4.0LVEF – 20%

Despite optimization of therapy both patients remained symptomatic with intermittent dyspnea and had repeated readmissions due to decompensated heart failure

Prospective comparison of ARNI with ACE‐I to Determine Impact on Global Mortality and morbidity in Heart Failure trial (PARADIGM‐HF)

PARADIGM‐HF: the most geographically diverse trial in patients with HFrEF
• 8,442 patients were randomized at 985 sites in 47 countries
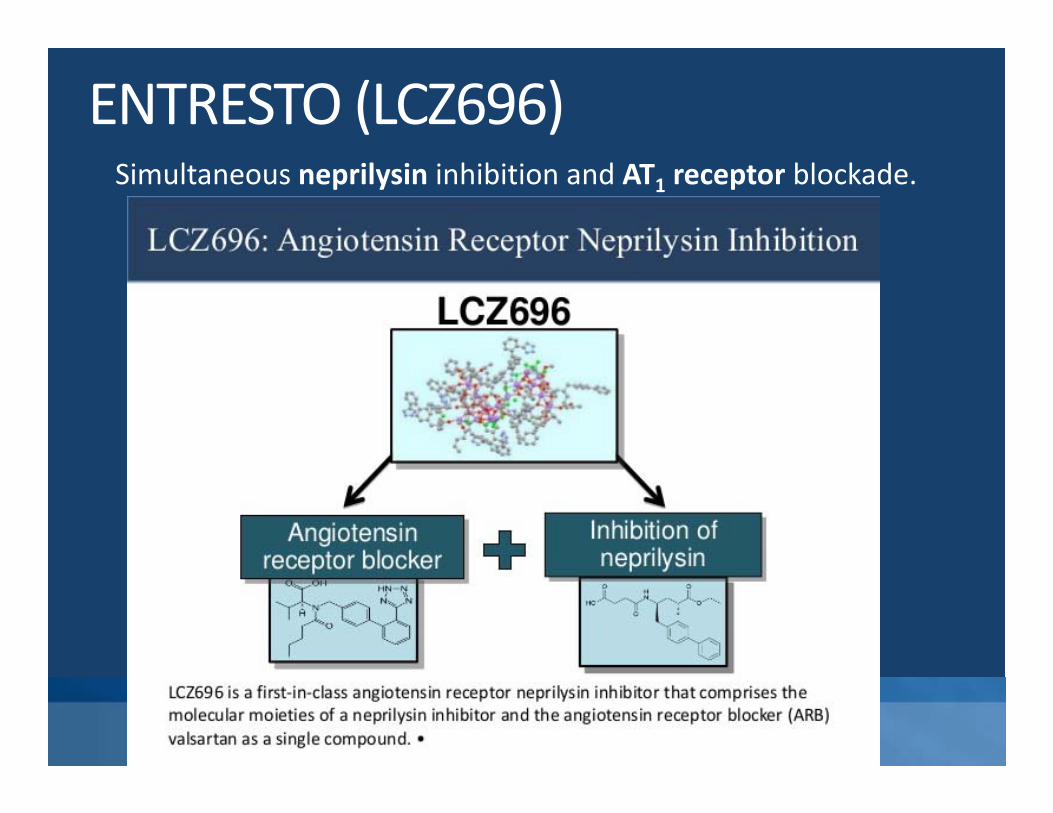
ENTRESTO (LCZ696)Simultaneous neprilysin inhibition and AT1 receptor blockade.

PARADIGM‐HF STUDY DESIGN
Entresto®200 mg BID§
Randomizationn=8,442
2 Weeks 1–2 Weeks 2–4 Weeks
Single‐blind activerun‐in period
Double‐blind Treatment period
On top of standard HFrEF therapy (excluding ACEIs and ARBs)
Median of 27 months’ follow‐up
Entresto®100 mg BID‡
Enalapril 10 mg BID*
Enalapril 10 mg BID#
Entresto® 200 mg BID§
Objectives
• Primary endpoint – CV mortality/HF
hospitalization.
• Secondary endpoint – all cause mortality, AF,
renal decline, KCCQ(symptom score)
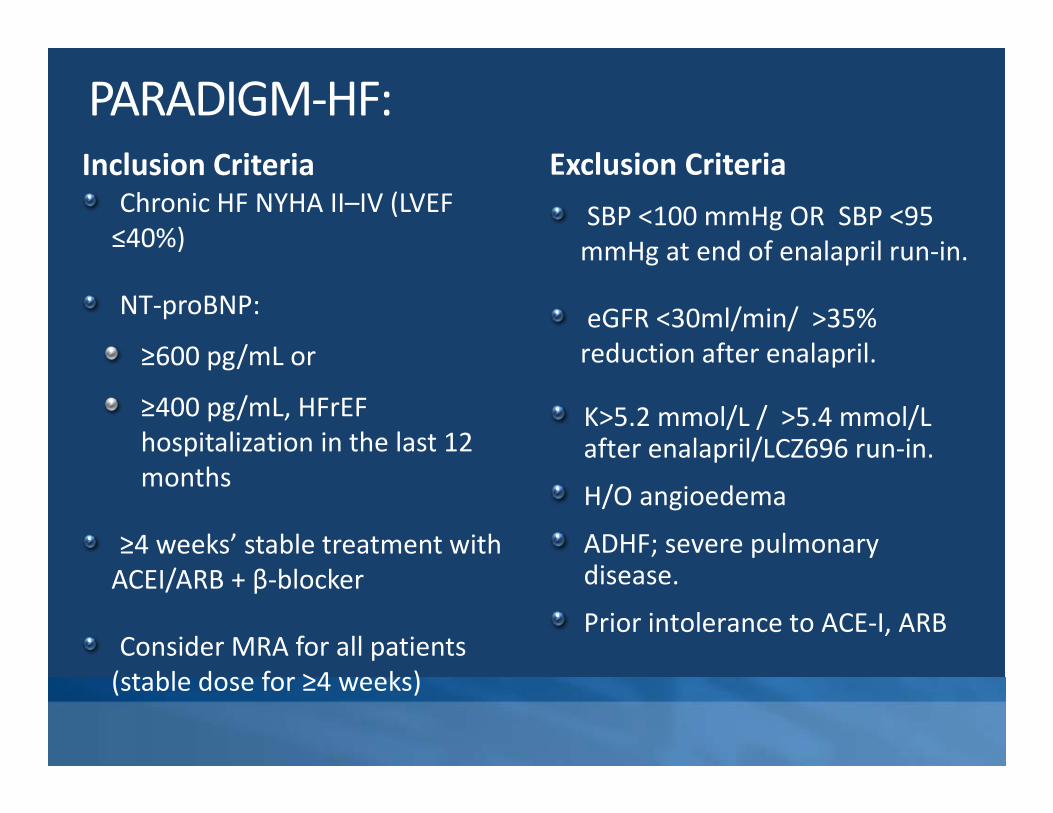
PARADIGM‐HF: Inclusion Criteria
Chronic HF NYHA II–IV (LVEF ≤40%)
NT‐proBNP:
≥600 pg/mL or
≥400 pg/mL, HFrEFhospitalization in the last 12 months
≥4 weeks’ stable treatment with ACEI/ARB + β‐blocker
Consider MRA for all patients (stable dose for ≥4 weeks)
Exclusion CriteriaSBP <100 mmHg OR SBP <95 mmHg at end of enalapril run‐in.
eGFR <30ml/min/ >35% reduction after enalapril.
K>5.2 mmol/L / >5.4 mmol/L after enalapril/LCZ696 run‐in.
H/O angioedema
ADHF; severe pulmonary disease.
Prior intolerance to ACE‐I, ARB

Baseline characteristicsCharacteristic*
Entresto®(n=4,187)
Enalapril (n=4,212)
Age, years 63.8 ± 11.5 63.8 ± 11.3Women, n (%) 879 (21.0) 953 (22.6)Ischemic cardiomyopathy, n (%) 2,506 (59.9) 2,530 (60.1)LV ejection fraction, % 29.6 ± 6.1 29.4 ± 6.3NYHA functional class, n (%)
II III
2,998 (71.6)969 (23.1)
2,921 (69.3)1,049 (24.9)
SBP, mmHg 122 ± 15 121 ± 15Heart rate, beats/min 72 ± 12 73 ± 12NT‐proBNP, pg/mL (IQR) 1,631 (885–3,154) 1,594 (886–3,305)BNP, pg/mL (IQR) 255 (155–474) 251 (153–465)History of diabetes, n (%) 1,451 (34.7) 1,456 (34.6)Treatments at randomization, n (%)
Diuretics 3,363 (80.3) 3,375 (80.1)Digitalis 1,223 (29.2) 1,316 (31.2)β‐blockers 3,899 (93.1) 3,912 (92.9)Mineralocorticoid antagonists 2,271 (54.2) 2,400 (57.0)ICD 623 (14.9) 620 (14.7)CRT 292 (7.0) 282 (6.7)
McMurray et al. N Engl Med 2014;371:993–1004

Primary Composite Endpoint
CI: confidence interval; CV: cardiovascular; HF: heart failureMcMurray et al. N Engl Med 2014;371:993–1004.
Cum
ulat
ive
prob
abili
ty
0.4
0
1.0
0.6
0.2
0 180 360 540 720 900 1,080 1,260
4,187 3,922 3,663 3,018 2,257 1,544 896 249
4,212 3,883 3,579 2,922 2,123 1,488 853 236
Entresto®
Enalapril
No. at risk
Hazard ratio = 0.80(95% CI: 0.73–0.87)
p<0.001
EnalaprilEntresto®
Days since randomization
Entresto®
Enalapril
No. at risk
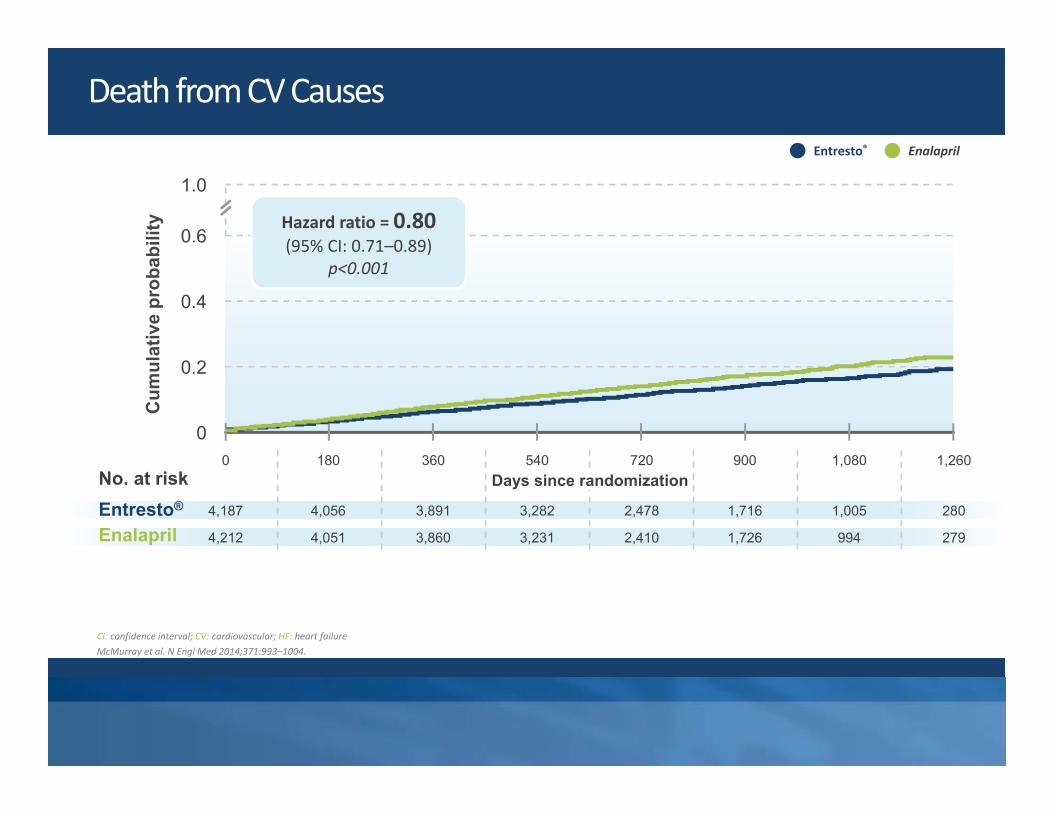
Death from CV CausesC
umul
ativ
e pr
obab
ility
0.4
0
1.0
0.6
0.2
0 180 360 540 720 900 1,080 1,260
4,187 4,056 3,891 3,282 2,478 1,716 1,005 280
4,212 4,051 3,860 3,231 2,410 1,726 994 279
Hazard ratio = 0.80(95% CI: 0.71–0.89)
p<0.001
EnalaprilEntresto®
Days since randomization
CI: confidence interval; CV: cardiovascular; HF: heart failureMcMurray et al. N Engl Med 2014;371:993–1004.

Entresto®
Enalapril
No. at risk
Death From Any CauseC
umul
ativ
e pr
obab
ility
0.4
0
1.0
0.6
0.2
0 180 360 540 720 900 1,080 1,260
4,187 4,056 3,891 3,282 2,478 1,716 1,005 280
4,212 4,051 3,860 3,231 2,410 1,726 994 279
Hazard ratio = 0.84(95% CI: 0.76–0.93)
p<0.001
EnalaprilEntresto®
Days since randomization
CI: confidence intervalMcMurray et al. N Engl Med 2014;371:993–1004.

PARADIGM‐HF: Effect of LCZ696 vs Enalapril on Primary Endpoint and Its Components
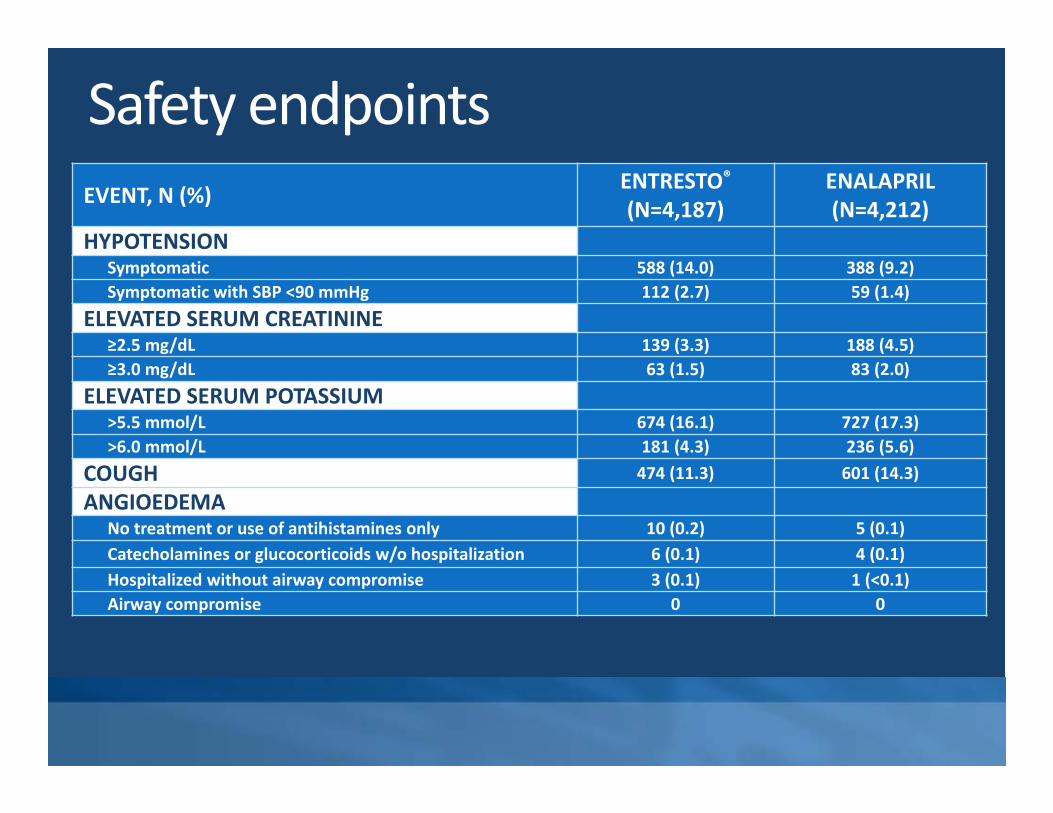
Safety endpointsEVENT, N (%) ENTRESTO®
(N=4,187)ENALAPRIL(N=4,212)
HYPOTENSIONSymptomatic 588 (14.0) 388 (9.2)Symptomatic with SBP <90 mmHg 112 (2.7) 59 (1.4)
ELEVATED SERUM CREATININE≥2.5 mg/dL 139 (3.3) 188 (4.5)≥3.0 mg/dL 63 (1.5) 83 (2.0)
ELEVATED SERUM POTASSIUM>5.5 mmol/L 674 (16.1) 727 (17.3)>6.0 mmol/L 181 (4.3) 236 (5.6)
COUGH 474 (11.3) 601 (14.3)
ANGIOEDEMA No treatment or use of antihistamines only 10 (0.2) 5 (0.1)Catecholamines or glucocorticoids w/o hospitalization 6 (0.1) 4 (0.1)Hospitalized without airway compromise 3 (0.1) 1 (<0.1)Airway compromise 0 0

LCZ696 dosingPopulation Initial Dose
Enalapril>10mg/dayValsartan>160mg/day 49/51mg twice daily
Naïve to ACE‐I/ARB, or onSuboptimal ACE‐I/ARB 24/26 mg twice daily
GFR<30ml/min/1.73m2 24/26 mg twice daily
Hepatic impairment (Child‐Pugh B) 24/26 twice daily
Titration Schedule: Double the dose of sacubutril/valsartan every 2‐4 weeks as tolerated to a target dose of 97/103mg twice daily
CritiqueSuboptimal background therapy.Efficacy and safety in specific subpopulations.
Black patientsNYHA Class I,IV, AHF
Patients not previously on ACE inhibitors or ARBsImpact on Blood Pressure ProBNP and NT ProBNP monitoring Off target effects of neprilysin inhibition
Alzheimer DiseaseMalignancy

Back to our Patients
Introduced Entresto as per guidelines.
Titrated dose upwards from 50mg BD to target
200mg BD.
To date:
No hospitalizations for ADHF.
Marked symptomatic & clinical improvement.
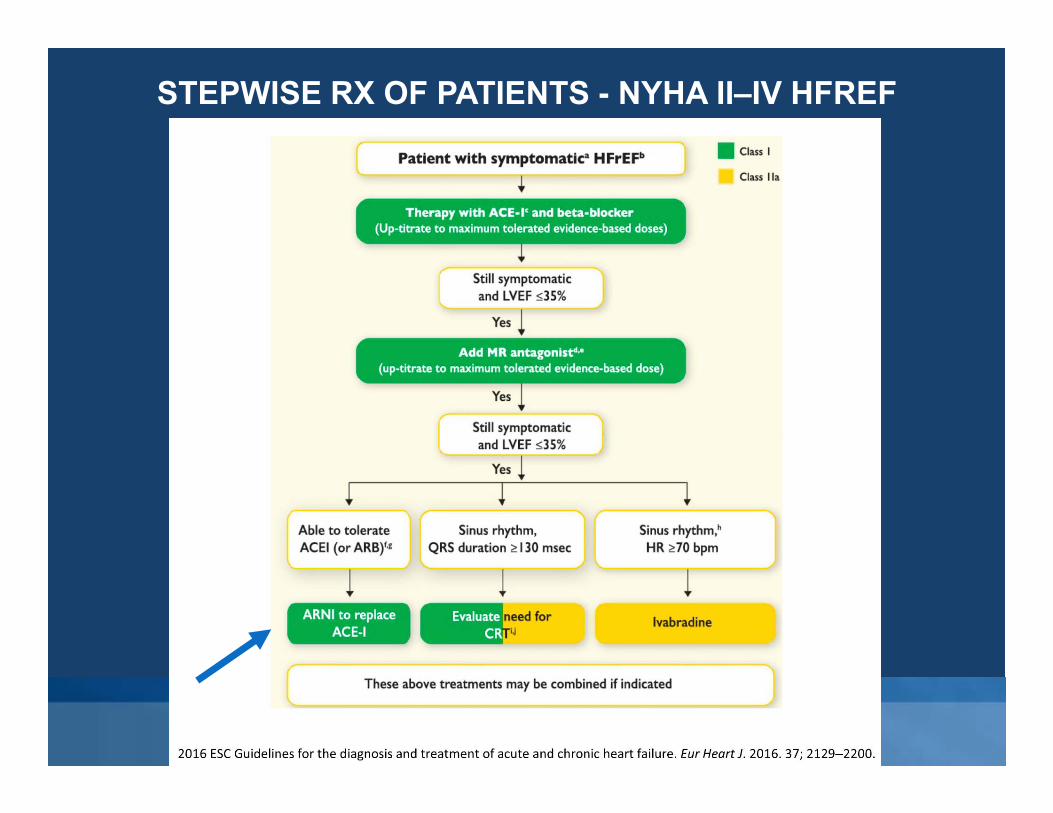
STEPWISE RX OF PATIENTS - NYHA II–IV HFREF

Conclusions1. Inhibition of RAAS + SNS + MRA (if possible)is central.2. Adding Neprilysin inhibition in PARADIGM‐HF to
increase vasoactive peptides has unquestioned superiority.
3. ARNI reduces CVS death/hospitalization 20%, all cause mortality 16%.
4. Strong case for ARNI to replace ACE‐I/ARB in NYHA II‐IV HF.
5. Studies ongoing for ARNI in HFpEF, ADHF & CRS (PARAGON Trial)

Thank You.





























