Embed Size (px)
Citation preview

A New Experimental Model of ARDS and Pulmonary Hypertension in the Dog*
B. Zwisslerl, H.Forst2
, K.lshie , snd K. Messmer1
I Department of Experimental Surgery, Univcrsity of Heidelbcrg, Heidelberg, Federal RepubJic of Gcrmany ~ Dcpartmenl of Aneslhesiology, University of Munich, Medical Center Großhadern, Munich, Federal Republic of Gcrmany 32nd Department of Surgery, Miyazuki Medical College, Kihara KiYOIake-cho, Japan
Summary. The aim of (his study was to establish a stable and reproducible model of pulmonary artery hypertension with concomitant A RDS-Iike changes of lung function and lung morphology. In eight anesthetized and ventilated dogs, 0.01 mVkg oleic acid (OA) was given i. v. fo llowed by repetitive injections of 100 J1m glass beads (OB) ioto the right atrium until a mean pulmonary artery pressure of 35~40 mm Hg was reached. Mean fight ventricular (R VP) and pulmonary artery (PAP) pressures, pulmonary vascular resistance (PVR), lung compliance and resistance, Pa0 2, intrapulmonary shunt and colloidosmotic pressure (COP) were c10sely monitored for 150min. PAP, RVP, and PVR considerably inereased subsequent 10 OAl GB injection, and slabilized at a high level within 70min , showing only a minimal decrease (PAP, RVP) ur no change (PVR) during the following 8O min . A signifieant decrease of Pa02 and pulmonary eomplianee as weil as an inerease of resistance and intrapulmonary shunt were found as early as 30 min after the last embolization and they remained unchanged for 120 min . Reduction of COP suggested transcapiUary leakage of maeromoleeules. Histology revealed an interstitial and intraalveolar edema. We conclude that the eombined injeetion of oleie aeid and glass beads provokes microvascul ar Jung injury and results in stable pulmonary artery hypertension wirh concomitant ARDS-like ehanges of lung funetion. Thus, an aeute mode l is provided in the dog allowing for the study of eardiac funetion in ARDS complicated by pulmonary artery hypertension.
Key words: Adult respiratory distress syndrome - Pulmonary artery hypertension, Model of - Hemodynamics - Lung funetion
.. Supported by Deutsche Forschungsgemeinschaft grant SFB 3201C3. Parts of Ihis work were presented allhe European Sociely fOT Surgical Research XXIII Congress/Joint meeting with the European Shock Socie ly, Bologna, Italy, 2-5 May, 1988
O!fprim reqllests 10: Or. Bernhard Zwissler

lntroduction
The onsel of pulmonary artery hypertension (PAH) in patients suffering from adult respiratory distress syndrome (AROS) has been shown to further increase the mortality rate of this syndrome [33]. Scveral authors have proposed that when ARDS is complicated by elevation of pulmonary vascular resistance (PVR) , ventricular contractility is compromised and the patients' prognosis deteriorates [36] .
To study cardiac function in the presence of both PAH and ARDS, a suitable experimental model is needed in which elevated PVR and the characleristic symptoms of ARDS (microvascular lung injury/pulmonary edema , impairment of lung mechanicslgas exchange) are present simultaneously. Both ARDS and PAH should be stable and easy to induce within a short period of time.
Different models have been developed in the past. Most of them, however, mimic only single aspects of ARDS or PAH. The techniques used indude pulmonary microembolization (e.g., g1ass beads (5, 22, 26, 28], fat emboli [4] , oleie acid [3 , 12, 19, 40] , stareh granules [9J, alpha-naphthyl-thiourea (ANTU) [21], blood dots {39] , air [40], barium sulfate [25]) and the intraveflous (thrombin [1 , 27], bacteria [8 , 38], endotoxin [7 , 15], lycopodium spores [13], heroin , alloxan , pyrroles [21]) , intratracheal (ozone [34] , Hel [16] , papain [30]) or intraperitoneal (ammonium sulfate [21]) administration of agents. Most oCten PAH was induced by constriction or OCclflSioli of the pulmonary artery (10, 32].
However, none of these models meets all criteria of bolh the AROS and PAH mentioned above. Therefore , we have combined two methods commonly used for induction of either PAH (glass beads; GB) or ARDS (oleic acid; DA). After administration of these thc time-course of changes in hemodynamics and lung function and aherations of lung morphology were examined .
By developing and characterizing an aeute animal model , we tried tO encompass the clinical features of both ARDS and PAH as closely as possible in order 10 aHow for evaluation of cardiac function under these conditions.
Material and Methods
The study has been pcrformed in cight foxhounds (22 ± 4 kg) of ei lher sex . Afler premedication with 2-3 ml propiomazine (Combelcn, Bayer, Lcverkusen, FRG) , anesthesia was induced by 20 mglkg pcnlobarbilal Lv. (Nembutal, Ceva, Bad Scgeberg, FRG) and maintaincd by infusion of 5 mg kg- 1h-1 pentobarbital , 1 50~g kg-1 h- ' pi rit ramid (Dipidolor, Janssen, Ncuss, FRG) and 75~g kg- 1h- 1 alcuronium (Allofcrin, Roche, Grenzach-Wyhlen, FRG). Ringer's solution 5 mlkg- 1 h- 1 was administe red throughout the experiment. The dogs were intubated and mechanically ventilated with arespiratory rale (RR) of 12 cycleslmin at a tidal volumc (VT) of l8mUkg using 100% O2 (Servo 9OOC, Siemens-Elema, Solna, Sweden).
Surgical Preparation
Fluid-filled calheters (PP27ü, POrlCX, Hylhe, UK) were positioncd in the aOrla and the vena cava superio r. A Swan-Ganz cathe ler (7F, Edwards, Anasco, PuerIo Rioo) was inserIed inlo Ihe pulmonary artery. FOT delermination of ventricular pressures, precalibrated micromanometers (PC350, Miliar Instruments, Houston , Tex., USA) were introduced into the !eft ventriele (LV) via the right carotid arlery and into the right ventric1e (RV) via the right atrium.

Measllrements
Mcasurements were performed with thc dogs in the left la teral position. Mean ancrial (MAP) , ccntral venous (CVP) and pulmonary ancry (PAP) prcssures were recorded u~ing Statham P23D6 transduccrs (Gould-Statham, Oxnard, Ca lif., USA) referred to the right at rium and zeroed to atmosphcrie pressure. Cardiae output (CO) was measured in triplicatc using thermodilution teehnique (SP 1435, Gould-Statham). Artcrial and mixed venous blood was analyzed for PO~, PC02, and pH . CO2 produetion per minute (\rC02) was measured by a CO2-Analyzer 930 (Siemens-Elema, Solna , Sweden). Effeetive pulmonary eomplianee (Celf) and expiratory resistance (R",p) were assessed by a Lung Meehanics Calculator 940 (SiemensElema , Solna, Sweden) conneetcd to the respirator. Colloidosmotie pressure (COP) was detcrmined by an Osmomat 050 (Gonotee, Berlin, FRG).
Experimenwl Protocof
After surgieal prcparation, the animals were isovolcmically hemodiluted with dextran 60 (Makrodex 6% , Sehiwa , Giandorf, FRG) to a hematocrit (Het) of 30% and were a llowed 10 stabilize (or 30min . Hematocrit has been intentionally deereased, beeause most patients with ARDS - consequent on their systemic iIlness or because of multiple blood sampling - are also anemic. The blood removed was used for the replacement of volume losses resulting from laboratory analyscs. Hemodilution per se has been shown to affeet neither extravascular lung wateT nor gas exchange during OA-induced pulmonary edema in dogs [6]. Following a control measurement, 0.01 mllkg OA (Merck , Darmstadt , FRG) was injeeted into the right atrium during expiration. Thcrcafter, non-si lieonized 1001Im glass bcads (LDH, Heidelberg, FRG) were suspended in dextran 60, thoroughly mixed and injected into the right atrium in aliquots ofO.5-1 g evcry 3- 5 min until PAP had reached 35-4Omm Hg. Between 10 and 150min after the last injeetion of GB (TLO- T1SO) , central hemodynami~ and Jung funet ion were assessed cvcry 20and 40min. respective!y. At T 1SO , the animals were killed with KCI; the lungs and tht: heart were removed and sent fo r histological examination.
Calcufations
The following hemodynamic parameters were caleulated: SV = CO ·1000/HR , CI = 10· COI BW(o.1$) (according to [20]). SI"" CI · lOüO/HR, PVR = (PAP-LVEDP)·79.9/CO, SVR = (MAP-RVEDP) . 79.9/CO , RVSW '" PAP·CO·O.t33/HR and LVSW'" MAP· CO·0.1331 HR , where SV = stroke volume, HR = heart rate, CI =- eardiae index , BW = body weight , $1 = stroke index, PVR = pulmonary vascular resistance. LVEDP = LVend-diastolic pressure, SVR = systemic vascular resistance, MAP = mean aonic pressure, RVSW = RV stroke work , RVEDP = RV end-diastolie pressure, and LVSW =- LV stroke work.
Intrapulmonary shunt (0,10,) was ea1culatcd as 0,/0, "" (c"01 - C.0.)/(c,,OCCV01)' where C,Ol = Hb ·1.39 + 0.0031 ' (Pe-47- P.C01). c,,01, C. OI and CV02 are O2 contents in ideal (100% saturated) puJmonary eapillary, systemie arterial and mixed venous blood, respeetively. Pe is barometrie pressure , p.0 2 and P.C02 are arterial POl and PCOI, respcetive1y. Physiological dead spaee/tidal volume ratio (VofVT) was determined by the Enghoff modifieation of the Bohr equation as VOIVT = (p.C02-PECOü·loo/P.C02 [14], where PioCO, (partial pressure of mean expiratory CO2) was ealculated as PEC01 ... V-C01 . (Pe- 47)1 (VT · RR). The alveolar gas equation was used to ca1culate the alveolar-arterial O2 difference (AaD02).
S/atistica/ Analysis
Data are presented as means ± SO. The existenee of an overa ll effeet of OA/GB was tcsted by repeated measures analysis of varianee (rANOVA). On1y in the ease of a signifieant rANOVA (P<0.05) were furt her statistics performcd. To estimate the signifieanec of ehanges after OA/GB , data al T 10, T)O, and T1S1\ were compared with control values by a

Table 1. Scquence of changes in hemodynamics , respiration, blood gases und blood chemistry (not shown in Ihe figures) aft er ONGE injeclion
Control T" T» T~ TM T. TlIo T,» T,~
MAP .. :I06-'::";:~~=S2."---_'" "!.:'0~ _.:::.9i' 100 102 101 102 102m
[mmHgJ ± 18 ± 17 ± 19 ± 19 ± 18 ± 20 ± 20 ± 17 ± 18 LVEDP 0 .2. ;" .8*! _'~ 5.0 5.2 5.4 5.4 5.4 5.2'"
1mmHgJ ± 1.7 ± 1.8 ± 1.9 ± 1.7 ± 1.7 ± 1.8 ± 1.8 ± 1.8 ± 1.9
RVEDP I:~n= _~n!ll 3.8'" 4.0 4.5 4.4 4.3 4.4 4. 5'" [mmHgj ± 2.9 ± 2.7 ± 1.8 ± 2.2 ± 2.0 ± 2.0 ± 1.7 ± 1.3 ±1.4
cvp 1:[9 ... -- --.J,~ 1.8'" 2.1 2.4 2.7 2.6 2.4 2.4'" 1mmHgJ ±U ± 1.4 ± 1.2 ±1.2 ± 0.9 ± 0.8 ± 0.8 ± 0.7 ± 0.7
LVSW [ 540 - .... ,:..." .3$·..::,. _":i~ 433 453 444 424 433 423· [Nm· 10-31 ±309 ± 119 ± 149 ± 163 ± 188 ± 192 ±209 ± 193 ± 199
RYSW ~-- * 1119t" =:'~~-:;:;:;"":lJl. ........... _ J .... 26--. ... H6) 109 110 106-* [Nm' W-3j ± 23 ± 24 ± 30 ± 31 ± 28 ± 26 ± 29 ± 28 ± 29
AaDOz rn6 ..... ...-..- .. _ .. '. -- ::--::,JJ1ill,J 303 324 323u
[mmHgJ ± 45 ± 130 ± 133 ± 148 ± 142
VoIYT 1:j.1_ --= = _~I1!J 58 " 58" 1%1 ± 5 ± 5 ± 6 ± 6 ± 5
pH ~jl·--XL= - 1.2.5l:11 7.26 7.27 7.27* ±0.02 ±0.Q4 tO,03 ±0.02 ±0.D2
p.COz I:5J.' -.. ... ',~~ 43.5 42.5 41.1· [mmHgj ±I.8 ± 4.6 ± 4.1 ± 3.7 ± 3.2
COP ==-'2J.~ --""'.r;t- mJ:l 20.5 20.3 19.8'" [cmH2OJ ± 2.0 ± 3.1 ± 2.3 ± 2.6 ± 2.2
Hb 10.5 10.0 9.8 9.9 10.0 Igldl) ± 1.1 ± 1.2 ± 1.2 ± 1.1 ± 1.0
He< 30 29 28 28 29 1%1 ± 3 ± 4 ± 3 ± 3 ± 4
Data (means ± SD; n - 8) are levels before (control) and at 10-150 min after embolization (T1o-T lSO)' The lcngth of Ihe rastered area indicates the time nceded for each parameter to stabilize, while the rest of time up to T IM and not marked by araster indicates !he plateau without any significant trend of the data to higher or lower values (for s tatistics sec Methods). The estimale the significance of acme and long- term effeets after OA/GB , data at T u) (hemodynamics). T30 and Tlso havc been compared with control data by means of Student 's Hest (. P < 0.05: *'" P < 0.01) . MAP. mean aortic pressure; LVEDP, lef! ventricular end-diastolie prcssure; RVEDP, right ventdeular end-diastolic pressure; CVP, central venous pressure ; L VSW, left ventricular stroke work: R VSW, right ventricular stroke work: AaDOlt a!veolar-arterial O2 difference; YoIVT , physiological dead space; P.CO~, partia l pressure o f arterial CO2: COP, colloidosmOlic pressure: Hb, hemoglobin; Het, hematocrit

paired t-test (significancc taken as P <O_05). Ta detennine the timepoint at which OA/GB ceased to have directed effects on the parameters, Helmert analysis was performed (SAS. GLMlHclmert). Starting from T IO• this technique compares the mean value of each mcasurement with the mean of all subsequcnt measurements. According to this analysis. a given parameter reaches a stable plateau at tbc time whcn the mean value is tlO langer significantly diffe rent (P>O.05) (rom the subsequenl mcan valucs.
Results
lsovolemic exchange of 9.7 ± 2.3 mllkg of blood by dextran 60 reduced the Het from 34% (0 30% . After hemodilution , Hct and Hb did not change significantly up to T1so (Table 1).
Hemodynamics
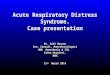
Thc injection of üA and GB (0.46 ± O. 13 g/kg) reslilted in a marked incTease of PAP (11/37 mm Hg) and RVP (8I2Omm Hg) al TIO (Fig. 1a, b). Concomitantly, PVR rose from 115 to 622 dyn· slem5 (Fig. 1e) and RVSW increased from 57 to 149 Nm .10- 3 (Table J). Within the next 40min theTe was a considerable fall in
• • ~
•
l" ...
-. F1g. I A-C. Sequence of ehanges in • A mean pulmonary artery pressure (PAP) . B mean right ventricular - • pressure (RVP) and C ca1culated ["!] pulmonary vascular resistance (PVR) • ... after injection of OAfGB. Dala • (means ± SD; n = S) are levels before 1-. (control) and at JO- lSOmin after embolization Tm-T\So). The length of • the raste red area indicatcs thc time needed for eacb parameter 10 stabi· lize, wbile the rest of time up tO T uo , and not marked by a rasier indicates -thc platcau without any significant '"
§] ... trend (n.s.) of the data to higher or -lower values (for stalistics see Meth- 1-ods). To estimale the signifieance of >-aeute and lang-tenn effects after !-OA/GB, data recorded at TIO. TJO and -T 150 have been compared with contJO] .• data by means of Student's (-test (+ P<O.05: ++ P<O.Ol ; .... P<O.OOI) , .•. - .. • • • .• . _-
'10M .... , ~<><,~ ., .. oS/.~"

• • •
o , 0
~.
0J..-:==_ =:J...j -. '. l ........ uTt]
'.
I~MlDI
•• _ .... " .. .. '" ... ,,, -
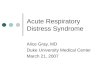
Fig.2A-C. Sequence of changes in A stroke index, B heart ra te, and C cardiac index afler injeclion orONGB. For funhe r explanation sec legend 10 Fig. 1
PAP. RYP, and PVR , as weil as in RVSW. Yet , PVR had completely stabilized at a high plateau al Tso and showed no further change up 10 Tuo- Ahhough HeimeTt analysis revealed a significant trend 10 lower values for RVP/RVSW and PAP up 10 T70 and T9<h respectively, the absolute changes re mained smalt.
RVEDP and CVP were slightl y, but persislently, increased afte r injection of OA/GB (Table 1). A significant reduction of SI at T to persisted Ihro ugho ullhe experimen t (Fig. 2A) and was accompan ied by a rise in HR (Fig. 2B) resulti ng in an unchanged Cl (Fig. 2C). Thc injection of OA/GB provoked a sudden fa ll (T,,) 01 LVP (47/43mm Hg; F;g.3A) , MAP ( I06l89mmHg) , LVEDP (5.2/ 3.8mm Hg) , and LVSW (540/358 Nm · 10- \ Table 1). SVR dccreased (Fig.3B) and was the o nly parameter thai did nOI slabilize wilhin 150 min t while LVP, LVED P and MAP relurned 10 conlrol within SO ntin and LVSW remained al low values from Tso- T I50.
LUflg FUrlCl;Orl
Lung mechanics and gas exchange were sign ificanlly allered by injection of OAl GB (Fig. 4): a 17% reduction in Ceff (42/35 mVcm H20) al T 30 was paralleled by a 20% increase o f Rexp (10.4/12 .5 cm H20 . sIl). No change occurred wilhin Ihe next 2 h. P.0 2 decreased by 31 % (547/379 mmHg) at TJlh while O,JOI and

, " "? <
!
• • • I-• " .. .. "
•
A
• • ~ V
• j SVR 1
~(' ..
/'
r
Timt aUt' I .. duell"" <>I ARDS/PAH
A c
~'~I I r ~ .. n .•.
• 1 Roxp l 0
~ .. •• •• I
~ I
•
Fig.3A, B. Sequence of changes in A mean left ventricular pressure and B systemic vascular resistance after injection of ONGB. For further explanat ion see legend to Fig. I
-J Pao-.J
! I r • , •
n .• .
16./0' 1 •
I I r • • ,
n.S .
n .. ......... >0 • , .. _ <OI<T_ >0 70 ". 15'_ Timt ollt. Induello .. 01 ARDS/PAH Timt oUt. I .. duellon <>I ARDS/PAH
Fig.4A-D. Sequence of ehanges in A effective pulmonary compliance, B expiratory pulmonary resistance, C p.O., 3nd D intrapulmonary shunt after injection of ONGB. Data (means ± SO; n '>= 8) are levels before (control) and al 30, 70, 110 and IS0min afterembolizalion (T3O- T LSO). Dal3 recorded al T 30 and T1SO have been compared with control data by means of Sludent's I-test (U P < 0.01). For further explanations see legend 10 Fig. 1

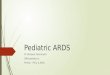
Fig. S. Histological scction of the lung after the administration of olde acid alld glass beads: Note the interstitial and the inuaalveolar edema fonna· tion. GB, glass bcad; JE, interstitial edema; AE, intraalveolar edema (original magnificalion x 60)
AaDOz more than doubled (10.6122.3% and 126/301mmHg, respectively). An increase in VofVT (51/61 %) was accompanied by hypercapnia and mild respiratory acidosis (Table 1). Similarly to lung mechanics, gas exchange had stabilized al T)O and persisted unchanged throughout the study.
COP was significantly reduced at T30 (23.6J19.9cm H 20 ; Table 1) without any further change up to T1SO •
Histo!ogy
Histological examination of the lung revealed a mild, interstitial and intraalveolar edema (Fig. 5). Same of the injected GB were found within alveoles , possibly indicating destruction of the blood-alveolar barrier. GB were not found in coronary vessels or in the myocardial tissue .
Discussion
The acute onsel of PAH has the potential to impair cardiac function [35] and to worsen the prognosis of patients with ARDS [33). To investigate the underlying pathophysiologicaJ mechanisms , an experimental model of AROS and pulmonary artery hypertension has been developed in the present study. Dogs have been chosen as the experimental animal, because Ihis species is commonly used when cardiac function is investigated in the setting of respiratory failure or PAH.

CaTdiovascular Effecis of OAIGB
The injection of ONGB resulted in a marked increase of pulmonary vascular resistance and RV afterload. This reaction has been already described by Malik et al. . who measured PAP and PVR for a total of 60min after injcction of HX1}lm GB in dogs [28}. Presumably. the rise in PVR is caused by a combination of the effects of mechanical obstruction in small blood vessels (by GB andl or platelets) , of active vasoconstriction subscquen l to stimulation of pulmonary stretch receptors [23], and the release of vasoactive substanccs {26j.
Between T IO and Tso we observed a considerable drop in PVR, PAP, and RVP , followed by a stable plateau at 50-70min post embolization. This is in conlrast 10 Ihc finding of Malik , who did not measure any change in PAP and PVR oncc peak levels had been reached [281. Thc reasons for this discrepancy are not c1ear because the experimental settings have basieally been the same (dogs. lOO).lm GB). The simultaneous use of OA in our experiments - beeause of ils abilily 10 ereate pulmonary edema - could explain a further increasc but not a deereasc in PVR and PAP [19). While tbe latler can be auributed to microemboli being pushed downstream by the blood flow (resulting in less obstruction of larger vessels) or to the elimination of vasoactive substances by melabolism and to active pulmonary vasodilatal ion [24], a stabilization of PVR at the very peak level is more difficuh 10 understand. Possibly, in the study of Malik el al. , PVR was maintained by a higher degrec of hypoxic pulmonary vasoconstriclion consequenl on a low Pa02 afler GB injeclion (60mm Hg) as againsl the high PIOZ of 379 mm Hg obtained in the presenl experiments.
The fall of LVP, LVSW, MAP, and SVR in the initial phase after ONGB is explained by a reduced LVEDP at that time. Excepl for LVSW. the parameters had returned 10 controllevels within 50 min. No depression of eardiac output was observed. Together with normal LV hemodynamics this indicates that the injection of OA and of GB did nol impair LV function in our model. This finding is in agreement with those of Mclntyre and Sasahara , who reported that PAP as high as 38 mm Hg may occur without reduetion of CO after acute pulmon8ry embolism [29]. Furthermore , any possibililY that a progressive depression of myocardial contractility, as described recently after bolus injection of pentobarbital 117). might have influenced our results can be exc1uded. The reduction of CO found in studies using higher doses of OA [19] may be due to the volume deficit originating from thc fluid losses into the lung in prescnce of major endothelial damage [37]. In our model the application of only 0.01 mllkg OA resulted in moderate pulmonary edema, bot obviously did not cause a volurne deficit apt to lower arterial pressure . Thus , the present model anows to study cardiac funclion without disturbanee by time-dependent changes of RV and LV performance inherent in the experimental model.
EffeelS ofOAIGB on Lung Fllnetion
The mechanisms by which OA and GB induce respiratory failure are not yet c1early understood [19, 31J. However, striking pathophysiological and histological similaritics between ARDS and lung injury induced by OA or GB have

been found . S oth substances provoke pulmonary edema. While OA is thought to directly injure the pulmonary endothelium [31], GB results in the release of media tors, wh ich in turn cause lung edema [26). Edema fonnation is potentiated in Ihis situation, because the pulmonary hydrostatic pressure is increased as a resuh of GB injection [26].
In the present study a significant increase of ÖJÖI, AaD02• VoIVT and Rc.:p as weil as a decrease of p.0 2 and 4ff was found. Thus, the typical elinical symptoms of ARDS [2) were prescnt in our model. The relatively high VofVTof 51% at control seems 10 be valid: standard techniques have been used for ils detcnnination and similar values have been demonstratcd by others in anesthctized and ventilated dogs as weil as in baboons [11 , 18J.
11 is difficuh to assess to what extent either OA or GB contribuled to the pathological changes in lung funClion. Using l00}.lm GS alone in nonheparinized dogs at a Fi02 of 1.0. no diSlurbances of gas exchange have been found in our own pilot experiments. This is in accordance with Becketl el al. , who failed to detect a substantial impairment of oxygenation after GB (5]. On the other hand , GS and additional applicalion of more than 0.025-0.05 mVkg OA resulted in severe and progressive hypoxemia with p.0 2 levels 100 low « 50 rum Hg; authors' unpublished data) to bc acceptable for a model designcd to investigate cardiac function. As a consequencc of the low dose of OA used in the present Sludy, O2 saturation did not fall below 90%. Morcover , as demonstrated by Helmert analysis, changes in lung function had stabilized within 30min after the last injection of GB and persisled for2 h. Thus, cardiac function can be Sludied in Ihis model withoul inlerference with time-dependenl alterations in lung function.
Histology
Histology of the lung revealed palhological alterations similar to ARDS. The presence of inlerstil'iaJ and intraalveolar edcma together with a decrease in COP indicates microvascular lung injury with endothelial defects and parlial destruction of the blood-alveolar barrier .
A complete first-pass trapping in the lungs has already beeil described for particles much smaller than 100 11m. Since no GB have been encounlered in sections of the myocardium, we can exclude that GB passing through the lungs caused microinfarctions.
We conelude that the present model satisfics the criteria for both ARDS and PAH in the dog and allows for the study of cardiac function in the presence of respiratory insufficicncy and a high PVR. It may therefore contribu te to a better understanding of mechanisms limiting cardiac performance in patien ts with ARDS and PAH.
Acknowledgeme/l/. The authors thank PD Dr. G. Mall for the histological analysis. The expert Icchnical assiSlancc of Mn;. R. Schwan, J. SchullC, and K. Sonnenberg is gratefull y acknowledged.

References
I. Arfors KE, Busch C, Jacobson S, Lindquist 0, Malmberg P, Rammer L, Saldeen T (1972) Pulmonary insufficiency following inlravenous infusion of thrombin and AMCA (tranexamic aeid) in the dog. Acta Chir Scand 138: 445- 452
2. Artigas A (1988) Adult respiratory distress syndrome: Changing concepts of c1inical evolution and recovery. In : Vincent JL (ed) Update in intensive care and emergency medieine, vol5. Springer, Beflin Heidelberg New York, p 97
3. Ashbaugh DG, Uzawa T (1968) Rcspiratory and hcmodynamie ehanges after injeetion of free fauy acids. J Surg Res 8 :417-423
4. Barie PS, Minnear FL, Malik AB (1981) lncreased lung vascular penneability after bone marrow injection in shccp. Am Rev Respir Dis 123: 648-653
5. Beckelt RC, Gray BA ( 1982) Effect of atelectasis and embolization on eXlravascular ther· mal volume of the lungs. J Appl Physiol53: 1614-1619
6. Bisbop MJ , Cheney FW (1983) The eneels of hcmodilution during pulrnonary edema in dogs. Ann Surg 198: 96- 101
7. Brigham KL, Myrick B (1986) Endotoxin and lung injury. Am Rev Respir Dis 133 :913-927
8. Brigham KL, Woolverton WC, Blake LH , Staub NC (1974) Increased sheep lung vascular permeability caused by pseudomonas bacteremia. J ain Invest 54: 792-804
9. Busch C, Rammer L (1973) Quantitation of fibrin deposition and elimination in organs of rats injeeted with labelIed fibrinogen by isolation of the labe lIed fibrin from water soluble tracer. Thromb Diath Haemorrh 29 : 108-114
10. Calvin JE, Baer RW, Glantz SA (1985) Pulmonary artery constrietion produces a greater right ventricular dynamic afterload than lung microvascular injury in the open chest dog. Cire Res 56 : 40-56
11. Coney RL, Albert R, Robertson HT (1983) Meehanisms of physiological dead space response to PEEP after acute oleic acid lung injury. J Appl Physiol 55: 1550- 1557
12. Derks CM, JacobovilZ-Derks D (1977) Embolie pneumopathy induced by olcic aeid. Am J Pathol87 : 143-158
13. Dexter L, Smitb GT (1964) Quantitative studies of pulmonary embolism. Am J Med Sei 35 :641- 648
14. Enghoff H (1938) Volumen inefficax. Bemerkungen zur Frage des schädlichen Raumes. Upsala Laekarefoeren Foerh 44: 191-218
15. Esbenshade AM , Newman JH , Lams PM , lolles H , Brigham KL (1982) Respiratory failure after endotoxin infusion in sheep: lung mechanies and lung fluid balance. J Appl Physiol 53: 967-m6
16. Gottlieb 55 , Wood LOH, Hansen OE, Long GR (1987) The effeet of nit roprusside on pulmonary edema , oxygen exchange , and blond flow in hydrochloric acid aspiration. Anesthesiology 67: 203- 210
17. Hansen OE, Borow KM, Neumann A, Lang RM, Fujii AM , Sehumacker PT, Wood LOH (1986) Effects of aeute lung injury and anesthesia on left ventricular mechanies. Am J Physiol 251: 1195-1204
18. Hammon JW, Wolfe WG , Moran JF, lones RH, Sabiston DC (1976) Tbe effeet ofpositive end-expiratory pressure on regional ventilation and perfusion in the normal and injured primate lung. J Thorac Cardiovasc Surg 72: 680-689
19. Hofman WF, Ebrhart [C, Granger WM, Miller DA (1985) Sequcntial cardiopulmonaf)' changes after o leic-aeid injury in dogs. Cri t Care Med 13 : 22-27
20. Holt IP, Rhode EA , Kines H (1968) Ventricular volumes and body weight in mammals . Am J Physiol215: 704- 715
21. Hurley N (Im7) Current views on the mechanisms ofpulmonary oedema. J Pathol125: 59-79
22 . Johnson A, Malik AB (198 1) Effects of different·size microemboli on lung fluid and protein exchange. Am J Physiol51 :461-464
23. Juratsch CE, Lengo JA, Laks MM (1977) Role ofthe autonomic nervous system and pulmonary artery receptors in production of experimental pulmonaf)' hypertension . Chest 71 [Suppl):265-268

24. Kealey GP, Brody MJ (1977) Studies on the meehanism of pulmonary vascular responses to miliary pulmonary cmbolism. Cire Res 41 : 807~8t4
25. Machida K, Rapapon E (1971) Left ventricular function in cxperimental pulmonary embolism. Jpn Heart J 12 :221~232
26. Malik AB (1983) Pulmonary microembolism. Physiol Rev 63: 1114-1207 27. Malik AB , Van der Zee H (19n) Thrombin-induced pulmonary insufficiency. Thromb
Res 11 :497-506 28. Malik AB , Van der Zee H (1977) Timecourse of pulmonary vascular response to micro
embolization. J Appl PhysioI 43:51 - 58 29. Mclntyre KM , Sasahara AA (1971) The hemodynamic response to pulmonary embolism
in paticnls without prior cardiopulmonary discasc. Am J Cardiol 28 :288- 294 30. Mink SN , Gomez A , Whit ley L, Coalson JJ (1986) Hemodynamics in dogs with pulmo
nary h)'pertension due 10 emphysema. Lung 164:41- 54 31. Motohiro A , Furukawa T , Yasumoto K, Inokuchi K (1986) Mechanisms involvcd in acute
lung edema induced in dogs by oleic acid . Eur Surg Res 18: 50- 57 32. Ohkuda K, Na kahara K, Weidner WJ , Binder A, Staub NC (1978) Lung Duid exchange
after uneven pulmonary artery obstruction in sheep. Cire Res 43: 152- 161 33. O liphant LD , Sibbald WJ (1987) Right ventricular performance in the adult respiralory
distrcS$ syndrome. In : Vincenl JL, Suter PM (eds) Update in intensive cafe and emergency mcdicine, vol4. Springer, Berlin Heidelberg New York, p 25
34. PloppeT CG, Ounwonh OL, Tyler WS (1973) Pulmonary lesions in rats cxposed to ozone. Am J Pathol 71 :375-394
35. Qvist J , Mygind T , Crotlogini A, Jordening H, Mogenscn T, Dorph S, Laver MB (1988) Cardiovaseular adjustments to pulmonary vascular injury in dogs. Anesthesiology 68: 341 - 349
36. Raper R, Sibbald WJ (1987) Right ventricular fun ction in thc surgical patient. World J Surg 11: 154-160
37. Schuster OP, Trulock EP (1984) Corrclation of changcs in oxygenation, lung water and hemodynamics afler oleie acid-induced aeute lung injury in dogs. Crit Care Med 12: 1044-\048
38. SielaffTO, Sugerman HJ , Tatum JL, Blocher CR (1987) Successful treatment of adult respiralory distress syndrome by histamin and prostaghm din blockade in a porcine pseudomonas model. Surgery 102 :350-357
39. Woolverton WC, Hyman AL (1972) The pulmonary hemodynamie effeels of lung Ihromboemboli in dogs. Surgery 73 : 572- 578
40. Zelter M, Douguet D (1986) Experimental pulmonary oedcmas. Bull EUT Physiopathol Respir 22: 281-314