Embed Size (px)
Citation preview

Acta Oto-Laryngologica, 2011; 131: 779–786
CASE REPORT
A new disease: Pregnancy-induced sudden sensorineural hearing loss?
ZHI-QIANG HOU1,2 & QIU-JU WANG1
1Department of Otolaryngology Head and Neck Surgery, Chinese PLA Institute of Otolaryngology, Chinese PLA GeneralHospital, Beijing and 2Medical College, Nankai University, Tianjin, PR China
AbstractSudden sensorineural hearing loss (SSNHL) may occur during pregnancy, but its prevalence is very low. It is conjectured thatSSNHL is closely related to the changes in the cardiovascular system, hematological system, endocrine system, and/or someother systems due to pregnancy. These changes possibly evoke disorders of cochlear circulation or cochlear fluid homeostasisleading to SSNHL. Two SSNHL cases were observed in our clinic, and their clinical features were analyzed. In one patient theSSNHL was likely to be related to the disturbance of cochlear fluid homestasis and in the other it might be induced by somedisorders in cochlear circulation. Based on their distinct clinic profiles, we defined a new disease, called “pregnancy-induced sudden sensorineural hearing loss,” similar to the definition of “pregnancy-induced hypertension.” This study alsodeepened our understanding of the etiology of SSNHL.
Keywords: Hormone, cochlear circulation, cochlear fluid homeostasis
Introduction
Sudden sensorineural hearing loss (SSNHL) is definedas sensorineural hearing loss of at least 30 dB in threesequential frequencies that occurs with unknown causeover a period less than 72 h [1,2]. To date, the etiologyof SSNHL has not been illustrated clearly. There aremany postulations regarding its etiology, such as vas-cular occlusion, viral infection, immune-mediatedmechanisms, and fractures of the labyrinth [2]. Thevascular etiology has been mentioned most frequently,but direct evidence has not been found and henceno standard therapy guideline has been published sofar [3].SSNHL may occur during pregnancy, although
such incidence is rare, especially in the first trimester[1,4,5]. There are many noticeable physiologicalchanges in the course of pregnancy, imposing greatchallenges on all body systems [6]. These sophisticatedphysiological changes may occur in the cardiovascularsystem, hematological system, endocrine system andothers. The amount of hormones produced during
pregnancy is different, especially for estrogen andprogesterone, which influences the auditory systemat the cochlear or proximal levels. These changesmay impact the circulation of cochlea and/or cochlearfluid homeostasis [7].According to previous studies [8,9], some dysfunc-
tions in the auditory system can happen during preg-nancy, such as a low-frequency hearing loss [8] andtolerance problems [9], and these problems disappearin the post-partumperiod. SSNHLcan occur in healthywomen during uncomplicated pregnancies [5], and itsoutcomes are highly variable [4]. There are few pub-lished reports on SSNHL during pregnancy, so therelationship between SSNHL and pregnancy has notbeen established. Hence, pregnancy-induced SSNHLremains a myth.In this study, we investigated two cases of
SSNHL occurring during pregnancy, in order tounderstand the causes of sudden deafness during preg-nancy and the relationship between sudden deafnessand pregnancy, and their clinical profiles may helpunderstanding of pregnancy-induced SSNHL.
Correspondence: Dr Qiu-Ju Wang, Department of Otolaryngology Head and Neck Surgery, Chinese People’s Liberation Army General Hospital, 28 FuxingRoad, Beijing, 100853, China. E-mail: [email protected] or [email protected]
(Received 8 October 2010; accepted 19 December 2010)
ISSN 0001-6489 print/ISSN 1651-2251 online � 2011 Informa HealthcareDOI: 10.3109/00016489.2011.553630
Act
a O
tola
ryng
ol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y R
MIT
Uni
vers
ity o
n 03
/12/
13Fo
r pe
rson
al u
se o
nly.

Case reports
Case 1
A 30-year-old woman, who was admitted to our hos-pital on January 14, 2009, had suffered sudden tinnitusaccompanied by aural fullness 4 days previously andhearing loss in her right ear 3 days afterwards. Thispatient was in the sixth week of her second pregnancy.During her first pregnancy, she did not have anyauricular symptoms, and she had a uterine-incisiondelivery of full-term birth. She had a history ofcomplete deafness in her left ear.
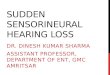
In our hospital, she received detailed audiometrytests including pure tone audiometry (Figure 1),acoustic immittance measurement (Table I), distor-tion product otoacoustic emissions (DPOAEs), andhigh stimulating auditory brainstem response (ABR)(Table II). She also underwent several auxiliary exam-inations including electrocardiogram (ECG), routineblood tests, biochemical blood tests, and blood clot-ting test. Physical examination of the ears, nose, andthroat did not find any abnormal signs. Audiometrytests revealed that her right ear exhibited anascending-type curve and low-frequency hearingloss, her left ear had no hearing. Finally, auxiliary
–10
0
0.25 k 0.5 k 1 k
Frequency (Hz)
2 k 4 k 8 k
10
20
30
40
50
Hea
rin
g le
vel (
dB
HL
)
60
70
80
90
100
110
120
130
–10
0
0.25 k 0.5 k 1 k
Frequency (Hz)
2 k 4 k 8 k
10
20
30
40
50
Hea
rin
g le
vel (
dB
HL
)
60
70
80
90
100
110
120
130
–100
0.25 k 0.5 k 1 kFrequency (Hz)
2 k 4 k 8 k
1020304050
Hea
rin
g le
vel (
dB
HL
)
60708090
100110120130
–100
0.25 k 0.5 k 1 kFrequency (Hz)
2 k 4 k 8 k
1020304050
Hea
rin
g le
vel (
dB
HL
)
60708090
100110120130
5
431
2
2
1
2
1
a b
c d
Figure 1. (a and b) Audiograms for patient 1. (a) Recordings for the right ear: (1) before her hospitalization (January 13, 2009); (2) on themorning of the first day of her hospitalization (January 14, 2009); (3) on the afternoon of the first day of her hospitalization (January 14, 2009);(4) on the second day of her hospitalization (January 15, 2009); (5) 15 months after her hospitalization (April 16, 2010). (b) Left ear. (c and d)Audiograms for patient 2. (c) Recordings for the right ear: (1) when she was in hospital (January 14, 2009); (2) 18 months after herhospitalization (July 29, 2010). (d) Recordings for the left ear: (1) when she was in hospital (January 14, 2009); (2) 18 months after herhospitalization (July 29, 2010).
780 Z.-Q. Hou & Q.-J. Wang
Act
a O
tola
ryng
ol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y R
MIT
Uni
vers
ity o
n 03
/12/
13Fo
r pe
rson
al u
se o
nly.

examinations all showed normal results in this patient(Figure 2 and Table III).On the second day of her hospitalization (January
15), she experienced improvement of hearing in theright ear, and the audiometry tests revealed that herhearing was normal. Hence, she was discharged fromour hospital on the same day. However, after dis-charge, this pregnant woman frequently suffered hear-ing loss in her right ear, accompanied by the persistenttinnitus. Each time her hearing was lost for 3–4 daysand then became normal for 1–2 days. This periodichearing loss occurred repeatedly in her pregnancy.This patient had a uterine-incision delivery on
August 28, 2009. Afterwards, she no longer had
hearing loss in her right ear. Audiometry tests per-formed on April 16, 2010, showed that the hearing inher right ear was normal (Figure 1). She was thenfollowed up until August 11, 2010, showing that herhearing loss did not occur any more, although thetinnitus did not disappear (the symptom attenuatedgradually).
Case 2
A 31-year-old woman, who was admitted to ourhospital on January 14, 2009, had suffered suddenhearing loss in her left ear for 10 days. The sudden
Table I. The results of acoustic immittance measurement.
Stapedial reflexthreshold (dB HL)
Patientno. Left/right
Tympanometriccurves
Tympanometricpressure
Acoustic compliancevalue (ml)
Recordingear
Stimulantear 0.5 kHz 1 kHz 2 kHz 4 kHz
1 Left A Normal 0.8 Left Right 100 100 100 100
Left – NR NR –
Right A Normal 0.6 Right Right – 90 90 –
NRLeft NR NR NR
2 Left A Normal 1.2 Left Right 100 100 100 100
Left – NR NR –
Right A Normal 1.0 Right Right – 90 90 –
Left NR NR NR NR
The normal range of acoustic compliance value is 0.3–1.6 ml. NR, no response; –, the detection was not carried out at this frequency.
Table II. Results of high stimulating rate auditory brainstem response (ABR) and DPOAE.
High stimulating rate ABR DPOAE
Patient no. Stimulant rate(/s) Left/right Vt (ms) I–V (ms) Left/rightDI–V(ms) Patient 1 Patient 2
1 11.1 Left NR NR Left NR Frequency(kHz)
Left Right Left Right
Right 5.25 3.88 0.5 No No No No
51.1 Left NR NR Right 0.17 0.75 No No No Yes
Right 5.50 4.05 1 No Yes No Yes
1.5 No Yes No Yes
2 11.1 Left NR NR Left NR 2 No Yes No Yes
Right 5.25 3.70 3 No Yes No YesYes51.1 Left NR NR Right 0.30 4 No Yes No
Right 5.65 4.0 6 No Yes No Yes
8 No Yes No Yes
High stimulating rate ABR is an examination that records responses at the stimulant rate of 11.1 and 51.1/s. NR, no response could be recordedwhen the stimulant sound was given at 100 dB nHL. The DI–V is £ 0.28 ms in normal ears (the normal range used in Chinese People’sLiberation Army General Hospital). When DI–V is > 0.28 ms, posterior circulation ischemia is considered. The high stimulating rate ABR wascarried out on the two patients as soon as they entered our hospital.
A new disease: Pregnancy-induced SSNHL? 781
Act
a O
tola
ryng
ol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y R
MIT
Uni
vers
ity o
n 03
/12/
13Fo
r pe
rson
al u
se o
nly.

hearing loss, accompanied by tinnitus and aural full-ness, occurred after emotional excitation. The patientreceived hyperbaric oxygenation and acupuncturetherapies, but these treatments had no salient effectson her hearing. The patient was in the sixth week ofher first pregnancy.In our hospital, she underwent a series of audio-
metries tests, auxiliary examinations, and physicalexaminations, as for patient 1. Physical examinationof her ears, nose, and throat did not find any abnormalsigns. Audiometry tests showed profound sensorineu-ral hearing loss in her left ear (Figure 1) and normalhearing in her right ear. High stimulating ABR testidentified no response in the right ear and a wider wave(0.30 ms > 0.28 ms) between the inter-peak latencies I
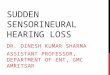
and V in the left ear (Table II). The ECG showed anST segment depression in leads II, aVF and T-waveinversion in lead III (Figure 2). Blood tests revealed anincrease in the platelet count (Table III).She was in our hospital for 7 days, without any
improvement in hearing, although her symptoms suchas tinnitus and aural fullness disappeared. She wasdischarged from our hospital on January 21, 2009.This patient had a cesarean delivery on the day(September 4, 2009) of her full-term pregnancy.She was followed up until July 29, 2010, and therepeated audiometry tests revealed that the hearing inher left ear was markedly improved at low frequencies,although she still suffered profound high-frequencyhearing loss (Figure 1).
Figure 2. Electrocardiogram (ECG) of patient 2. The ECG was conducted on the patients on the first day of their hospitalization. The chartdrive speed was 25.0mm/s, and the standard voltage was 10.0mm/mV. The ECG of patient 1 showed sinusal rhythm and normal manifestationin all leads. Patient 2 showed sinusal arrhythmia, ST segment depression in leadsII, aVF and T-wave inversion in lead III, as indicated in thefigure by arrows.
782 Z.-Q. Hou & Q.-J. Wang
Act
a O
tola
ryng
ol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y R
MIT
Uni
vers
ity o
n 03
/12/
13Fo
r pe
rson
al u
se o
nly.

Table III. Results of hematological laboratory tests.
Patient 1 Patient 2
Parameter Result N/L/H Result N/L/H Normal range
Hb 129 N 118 N 110–179 g/L
RBC 4.18 N 3.78 N 3.5–5.9 � 1012/L
WBC 5.22 N 6.20 N 3.5–10 � 109/L
Neutrophilic granulocytes 0.610 N 0.487 L 0.5–0.7
Lymphocytes 0.293 N 0.365 N 0.2–0.4
MonocytesEosinophils
0.080 N 0.084 H 0.03–0.08
0.015 N 0.058 H 0.01–0.05
BasophilsHct
0.002 N 0.006 N 0–0.01
0.37 N 0.34 L 0.35–0.52 L/L
MCV 89.0 N 91.0 N 80–100 fL
MCH 30.9 N 31.2 N 27–34 pg
MCHC 347 N 343 N 320–360 g/L
RDW 12.4 N 13.1 N 0–14.5%100–300 � 109/LPLT 220 N 311 H
MPVPT
12.2 N 9.5 N 6.8–12.8 fL
13.3 N 13.6 N 12–16 s
Prothrombin activity 84.9 N 82.0 N 60–120%
INR 1.13 N 1.16 N 0.95–1.527–45 sAPTT
Fibrinogen37.6 N 38.3 N
2.712 N 2.677 N 2–4 g/L
TT 17.6 N 18.5 N 16–22 s
ALT 11.4 N 10.2 N 0–40 U/L
AST 12.5 N 15.0 N 0–40 U/L
Albumin 75.4 N 74.3 N 55–80 g/L
Serum albumin 43.4 N 42.9 N 35–50 g/L0–21 mmol/L0–8.6 mmol/L
TBilDbil
26.4 H 8.3 N
7.9 N 2.7 N
TBA 0.8 N 5.2 N 0–10 mmol/L5–20 mmol/L
HCYALP
8.10 N 6.82 N
46.4 N 38.1 N 0–130 U/L
g–GT 16.0 N 12.3 N 0–50 U/L
Glucose 4.65 N 4.47 N 3.4–6.2 mmol/L1.8–7.5 mmol/L
Urea 3.09 N 5.86 N
Cr 45.2 N 48.2 N 30–110 mmol/L104–444 mmol/L
Serum uric acid 189.5 N 177.0 N
Total cholesterol 3.36 N 3.01 L 3.1–5.7 mmol/L
Triglyceride 1.07 N 0.62 N 0.4–1.7 mmol/L
A new disease: Pregnancy-induced SSNHL? 783
Act
a O
tola
ryng
ol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y R
MIT
Uni
vers
ity o
n 03
/12/
13Fo
r pe
rson
al u
se o
nly.

Discussion
Two cases of SSNHL in pregnancy were investigatedin our study and their clinical features were analyzed.One patient had low-frequency fluctuating sensori-neural hearing loss and the other had profoundsensorineural hearing loss. Both of them had hearingloss in the sixth week of pregnancy. The hearing ofpatient 1 returned to normal after delivery, butthe hearing of patient 2 showed little improvement.We supposed that their SSNHL was related topregnancy.It is well known that changes in the cardiovascular
system and hematological system begin from 5 to8 weeks of pregnancy [6], and both these patientshad SSNHL at the sixth week of gestation, which was
just in this period. Furthermore, patient 1 hadhearing loss repeatedly in the pregnancy many timesbut the hearing loss did not occur again after deliveryfor at least 1 year. Therefore, we considered that thehearing loss was closely related to pregnancy, and itmight have been induced by the changes of theprecursor.Pregnancy causes a series of changes in most of the
body systems, such as the cardiovascular system,hematological system, endocrine system, and someother systems. Pregnancy is a hypercoagulable statewith alterations in both the coagulation and fibrino-lysis systems. A rise occurs in coagulation factors VII,VIII, IX, X, XII, fibrinogen, and von Willebrandfactor, and conversely a fall in factor XI [10]. Thelevel of factor V does not change during pregnancy [6].
Table III. Results of hematological laboratory tests (Continued).
Patient 1 Patient 2
Parameter Result N/L/H Result N/L/H Normal range
Apolipoprotein A1Apolipoprotein B
1.17 N 1.36 N 1–1.6 g/L0.6–1.1 g/L2–200 U/L
0.71 N 0.53 L
CK 41.8 N 44.8 N
LDH 119.7 N 105.4 N 40–250 U/L
CK isoenzyme 7.6 N 7.9 N 2–200 U/L
Ca 2.25 N 2.25 N 2.25–2.75 mmol/L
Pi 1.40 N 1.34 N 0.89–1.60 mmol/L
MgK
0.84 N 0.92 N 0.6–1.4 mmol/L
3.63 N 3.70 N 3.5–5.5 mmol/L130–150 mmol/L
Na 138.0 N 138.5 N
ChloridesCO2
105.3 N 105.2 N 94–110 mmol/L20.2–30 mmol/L
22.2 N 24.6 N
HDL-cholesterol 0.91 L 1.18 N 1–1.6 mmol/L
LDL–cholesterol 2.13 N 1.63 N 0–3.4 mmol/L0–30 mg/L
Serum lipoprotein 6.82 N 4.53 N
Serum glycated protein 159.9 N 174.0 N 125–240 mmol/L
Serum cystatin 0.59 N 0.73 N 0.45–1.25 mg/L
Serum sialic acid 51.5 N 48.6 N 45–75 mg/dl
Free calcium 1.11 N 1.05 N 1.02–1.6 mmol/L
The test was performed on the first day of their hospitalization. N, in the normal range; L, lower than normal range; H, higher than normalrange. Hb, hemoglobin; RBC, red blood cells; WBC, white blood cells; Hct, hematocrit; MCV, mean corpuscular volume; MCH, meancorpuscular hemoglobin; MCHC, mean corpuscular haemoglobin concentration; RDW, red blood cell volume distribution width; PLT,platelet count; MPV, mean platelet volume; PT, prothrombin time; INR, international normalized ratio; APTT, activated partial throm-boplastin time; TT, thrombin time; ALT, alanine aminotransferase; AST, aspartate aminotransferase; TBil, serum total bilirubin; DBil, directbilirubin; TBA, total bile acid; HCY, homocysteine; ALP, alkaline phosphatase; g-GT, g-glutamyltransferase; Cr, creatinine; Al, Apolipo-protein A-1; CK, creatine kinase; LDH, lactate dehydrogenase; Pi, inorganic phosphorus.
784 Z.-Q. Hou & Q.-J. Wang
Act
a O
tola
ryng
ol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y R
MIT
Uni
vers
ity o
n 03
/12/
13Fo
r pe
rson
al u
se o
nly.

These changes induce the risk of venous thrombo-embolism thrombosis, which can rise four- to six-fold[11]. When a thromboembolic episode occurs in thecochlear arteries or veins, ischemia or congestion willresult, and SSNHL may be evoked. It is reported thatperipheral edema can be induced by some physiolog-ical changes in most normal pregnancies. Thesechanges include obstruction of venous return by thegravid uterus, peripheral vasodilation, increasedplasma volume, decreased colloid osmotic pressure,and increased vascular permeability. When peripheraledema occurs in the membranous labyrinth, and itaffects the cochlea just like Meniere’s disease [8], thenSSNHLmay come about. Factors such as pregnancy-related stress and immune-mediated disorders [2]also may play a role in initiation of SSNHL.Some evidence of these mechanisms was found in
our research. When the high stimulating rate ABRwas detected in patient 2, the inter-peak latency ofwave I-V at was 0.30 ms (> 0.28 ms) (Table II). Whenhigh stimulating ABR was detected in patient 2, noresponse was extracted in the right ear and a widerwave (0.30 > 0.28 ms) between the inter-peak laten-cies I and V in left ear was recorded (Table II). TheECG showed ST segment depression in leads II, III,aVF in patient 2 (Figure 2). The ECG showed STsegment depression in leads II, aVF and T-waveinversion in lead III in patient 2 (Figure 2). Someelements of the routine blood tests were also abnor-mal to some degree in patient 2 (Table III). However,these examinations were normal in patient 1.ABR can be used to detect posterior circulation
ischemia (PCI). It is reported that the PCI prolongsthe latency of all the waves of ABR in the experimentscarried out on animals [12]. Some other studies alsosuggested that the mean absolute latency of wave Vwas significantly longer in patients with decreasedanterior circulation. For the purpose of identifyingPCI, the high stimulating rate ABR works muchbetter than conventional ABR. The high stimulatingrate ABR is more sensitive to the response of graymatter in the brain, especially to the response ofsynapse, which is very susceptible to ischemia. Thedifference in the inter-peak latency of wave I-Vbetween high stimulating rate ABR and low stimu-lating rate ABR is the best indication. But some otherreasons can also lead to delay of the latency of ABR,such as demyelination and compression of the audi-tory nerve or internal auditory artery. The ST seg-ment depression in leads II, aVF and T-waveinversion in lead III in ECG is the representationof abnormal function in the heart, especially forischemia in the inferior wall of the heart. This stateis often caused by physiological changes during preg-nancy and usually resolves itself in the post-
partum period [13]. It is also a manifestation ofabnormality in the circulatory system all over thebody, including cochlear ischemia. The rise of plateletcount (PLT) is a manifestation of hypercoagulation, itincreases the risk of thrombosis in the cochlear vein orthromboembolism in the cochlear artery. All thefactors above increased the possibility of causingSSNHL in patient 2.However, these conditions were not found in
patient 1. The hydrolabyrinth was likely to be thereason, which can provoke hearing loss at low fre-quencies, and often occurs repeatedly just like theearly stage of Meniere’s disease [14].Besides the cardiovascular system and hematolog-
ical system, the endocrine system also plays an impor-tant role in the occurrence of SSNHL duringpregnancy. As we all know, hormones can influencethe physiological functions of many organs and sys-tems in both females and males, including the audi-tory system. Estrogen and progesterone are twoimportant hormones that can affect the auditory sys-tem at different levels. Some research indicates thatthere are estrogen receptors ERa and ERb in thecochlea in both humans and animal models [15].The ER receptors can be found in the spiral ganglion,outer hair cells, inner hair cells, stria vascularis [16],and cochlear vessels. They may modulate auditorytransmission, fluid electrolyte balance, and blood flowin the cochlea. In addition, estrogen may impactauditory function at different levels of the centralnervous system (CNS) by modulating GABA-ergic,serotonergic, and glutamatergic systems [17]. In gen-eral, estrogen has an excitatory and protective effecton the auditory system [18]. However, progesteronehas a mainly inhibitory action on the auditory system,although the specific progesterone receptors have notbeen identified in the auditory system. During preg-nancy, levels of the two hormones are higher thanusual, and some other changes will occur, such as therisk of thrombosis and increase of blood volume.These changes may influence the circulation in thecochlea and cochlear fluid homeostasis by leading tofluid retention and disorder of circulation in thecochlea.SSNHL during pregnancy seems to be closely
related to the changes occurring in the course ofpregnancy. In reviewing the literature, it has beenstated that hearing loss or hearing problems oftenincrease during pregnancy and return to normal afterdelivery [8,9]. Tandon [19] reported that the latencyand threshold of auditory brainstem response wave Vincreases during pregnancy, and the neural conduc-tion process in the brainstem auditory pathway is alsodelayed. If the physiological changes that occur dur-ing pregnancy turn out to be pathological changes,
A new disease: Pregnancy-induced SSNHL? 785
Act
a O
tola
ryng
ol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y R
MIT
Uni
vers
ity o
n 03
/12/
13Fo
r pe
rson
al u
se o
nly.

such as an abnormally high amount of hormones orthe risk of thrombosis is higher than a normal preg-nancy, then the possibility of SSNHL may be higher.Furthermore, SSNHL occurrence during pregnancycould occur again in the same patient who hadSSNHL in a previous pregnancy [20]. This can betreated with Dextran 40, which has been reported tobe safe and effective in improving hearing levels,especially at frequencies of 1, 2, at 4 kHz [1].So,weconcludethatSSNHLduringpregnancythat is
caused by the changes during pregnancy may be a newdisease that isdifferent fromtheusualSSNHL,similar tothe definition of “pregnancy-induced hypertension.”This disease can be called “pregnancy-induced suddensensorineural hearing loss.”However, further studies are necessary to confirm
the hypothesis. We must investigate more patientswith SSNHL in pregnancy and follow them up formore than 1 year after delivery. The detection ofhearing level and hormones must be carried outfrequently before and during this period. In addition,imaging examination (especially magnetic resonanceimaging, MRI) is necessary to check the amount offluid in the cochlea. After that, we can obtain moresubstantial evidence to determine the etiologies andmechanisms of SSNHL during pregnancy.
Acknowledgments
This work was supported by grants from the NationalNatural Science Foundation of China (30830104 and30771203), the Beijing Nature Science and Technol-ogy Major Project (7070002), the National Science &Technology Pillar Program in the 11th Five-year PlanPeriod (2007BAI18B12). We thank the patients andthe patients’ families for their co-operation. We thankthe technicians in the Clinical Auditory MedicineCentre at the Department of Otolaryngology Headand Neck Surgery, Chinese People’s Liberation ArmyGeneral Hospital for their technical support.
Declaration of interest: The authors report noconflicts of interest. The authors alone are responsiblefor the content and writing of the paper.
References
[1] Wang YP, Young YH. Experience in the treatment of suddendeafness during pregnancy. Acta Otolaryngol 2006;126:271–6.
[2] Schreiber BE, Agrup C, Haskard DO, Luxon LM. Suddensensorineural hearing loss. Lancet 2010;375:1203–11.
[3] Rauch SD. Clinical practice. Idiopathic sudden sensorineuralhearing loss. N Engl J Med 2008;359:833–40.
[4] Lavy JA. Sudden onset deafness: two cases associated withpregnancy. Int J Clin Pract 1998;52:129–30.
[5] Kanadys WM, Oleszczuk J. [Sudden sensorineural hearingloss during pregnancy.] Ginekol Pol 2005;76:225–7 (inPolish).
[6] Carlin A, Alfirevic Z. Physiological changes of pregnancy andmonitoring. Best Pract Res Clin Obstet Gynaecol 2008;22:801–23.
[7] Al-Mana D, Ceranic B, Djahanbakhch O, Luxon LM. Hor-mones and the auditory system: a review of physiology andpathophysiology. Neuroscience 2008;153:881–900.
[8] Sennaroglu G, Belgin E. Audiological findings in pregnancy.J Laryngol Otol 2001;115:617–21.
[9] Tsunoda K, Takahashi S, Takanosawa M, Shimoji Y. Theinfluence of pregnancy on sensation of ear problems – earproblems associated with healthy pregnancy. J Laryngol Otol1999;113:318–20.
[10] Hellgren M. Hemostasis during normal pregnancy and puer-perium. Semin Thromb Hemost 2003;29:125–30.
[11] Heit JA, Kobbervig CE, James AH, Petterson TM,Bailey KR, Melton LJ 3rd. Trends in the incidence of venousthromboembolism during pregnancy or postpartum:a 30-year population-based study. Ann Intern Med 2005;143:697–706.
[12] Tang A, Ura M, Yamauchi M, Noda Y. [The changes incochlear blood flow and auditory brainstem response in thepressure-induced animal model of acoustic neuroma.]Nippon Jibiinkoka Gakkai Kaiho 1996;99:370–8 (inJapanese).
[13] Hameed AB, Sklansky MS. Pregnancy: maternal andfetal heart disease. Curr Probl Cardiol 2007;32:419–94.
[14] Sajjadi H, Paparella MM. Meniere’s disease. Lancet 2008;372:406–14.
[15] Stenberg AE, Wang H, Fish J 3rd, Schrott-Fischer A,Sahlin L, Hultcrantz M. Estrogen receptors in the normaladult and developing human inner ear and in Turner’ssyndrome. Hear Res 2001;157:87–92.
[16] Lee JH, Marcus DC. Estrogen acutely inhibits ion trans-port by isolated stria vascularis. Hear Res 2001;158:123–30.
[17] Woolley CS, Weiland NG, McEwen BS, Schwartzkroin PA.Estradiol increases the sensitivity of hippocampalCA1 pyramidal cells to NMDA receptor-mediated synapticinput: correlation with dendritic spine density. J Neurosci1997;17:1848–59.
[18] Guimaraes P, Zhu X, Cannon T, Kim S, Frisina RD.Sex differences in distortion product otoacoustic emissionsas a function of age in CBA mice. Hear Res 2004;192:83–9.
[19] Tandon OP, Misra R, Tandon I. Brainstem auditory evokedpotentials (BAEPs) in pregnant women. Indian J PhysiolPharmacol 1990;34:42–4.
[20] Pawlak-Osinska K, Burduk PK, Kopczynski A. Episodes ofrepeated sudden deafness following pregnancies. Am JObstet Gynecol 2009;200:e7–9.
786 Z.-Q. Hou & Q.-J. Wang
Act
a O
tola
ryng
ol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y R
MIT
Uni
vers
ity o
n 03
/12/
13Fo
r pe
rson
al u
se o
nly.