Embed Size (px)
Citation preview

A
in
AnJana Canb Disc Ded Co
International Journal of Nursing Studies xxx (2014) xxx–xxx
A R
Artic
Rece
Rece
Acce
Keyw
Deli
Edu
Elde
Inpa
Prev
Risk
*
G Model
NS-2320; No. of Pages 9
Plin
002
http
multifaceted educational intervention to prevent delirium older inpatients: A before and after study
ne P.F. Wand a,b,*, William Thoo c, Hayley Sciuriaga a, Vicky Ting c,ett Baker a, Glenn E. Hunt b,d
terbury Hospital, Sydney Local Health District, Campsie, NSW, Australia
cipline of Psychiatry, Sydney Medical School, University of Sydney, Sydney, Australia
partment of Aged Care and Rehabilitation, Canterbury Hospital, Sydney Local Health District, Campsie, NSW, Australia
ncord Centre for Mental Health, Concord, NSW, Australia
T I C L E I N F O
le history:
ived 18 July 2013
ived in revised form 13 September 2013
pted 15 November 2013
ords:
rium
cation
rly
tient
ention
factor
A B S T R A C T
Background: Systematically targeting modifiable risk factors for delirium may reduce its
incidence. However, research interventions have not become part of routine clinical
practice. Particular approaches to the education of clinical staff may improve their practice
and patient outcomes.
Objectives: To evaluate the effectiveness of a multifaceted educational program in
preventing delirium in hospitalised older patients and improving staff practice, knowledge
and confidence.
Design: A before and after study.
Setting: A 22-bed general medical ward of a district hospital in Sydney, Australia.
Participants: Patients were aged 65 years and over and not delirious upon admission. Of
568 eligible patients, 129 were recruited pre-intervention (3 withdrew initial consent) and
129 patients post-intervention.
Methods: Prior to the intervention, in order to establish a baseline, patients were assessed
early after admission and again at discharge. The intervention was a one-hour lecture on
delirium focusing on prevention for medical and nursing staff followed by weekly
interactive tutorials with delirium resource staff and ward modifications. Following the
initial education session, data were gathered in a second group of medical ward patients at
the same time-points to ascertain the effectiveness of the intervention. Pre and post-
intervention data were analysed to determine change in staff objective knowledge and
self-ratings of confidence and clinical practice in relation to delirium. The main outcome
measures were incident delirium and change in staff practice, confidence and knowledge.
Results: The mean age of patients was 81. The pre and post-intervention groups were
comparable, aside from greater co morbidity in the pre-intervention group (F(1,
253) = 9.20, p = 0.003). Post-intervention there was a significant reduction in incident
delirium (19% vs. 10.1%, X2 = 4.14, p = 0.042), and improved function on discharge (mean
improvement 5.3 points, p < 0.001, SD 13.31, 95% CI �7.61 to �2.97). Staff objective
knowledge of delirium improved post-intervention and their confidence assessing and
managing delirious patients. Staff addressed more risk factors for delirium post-
intervention (8.1 vs. 9.8, F(1, 253) = 73.44, p < 0.001).
Conclusions: A low-cost educational intervention reduced the incidence of delirium and
improved function in older medical patients and staff knowledge and practice addressing
Corresponding author. Tel.: +61 291132035; fax: +61 291132098.
E-mail address: [email protected] (Anne P.F. Wand).
Contents lists available at ScienceDirect
International Journal of Nursing Studies
journal homepage: www.elsevier.com/ijns
ease cite this article in press as: Wand, A.P.F., et al., A multifaceted educational intervention to prevent delirium in olderpatients: A before and after study. Int. J. Nurs. Stud. (2014), http://dx.doi.org/10.1016/j.ijnurstu.2013.11.005
0-7489/$ – see front matter . Crown Copyright � 2013 Published by Elsevier Ltd. All rights reserved.
://dx.doi.org/10.1016/j.ijnurstu.2013.11.005
A.P.F. Wand et al. / International Journal of Nursing Studies xxx (2014) xxx–xxx2
G Model
NS-2320; No. of Pages 9
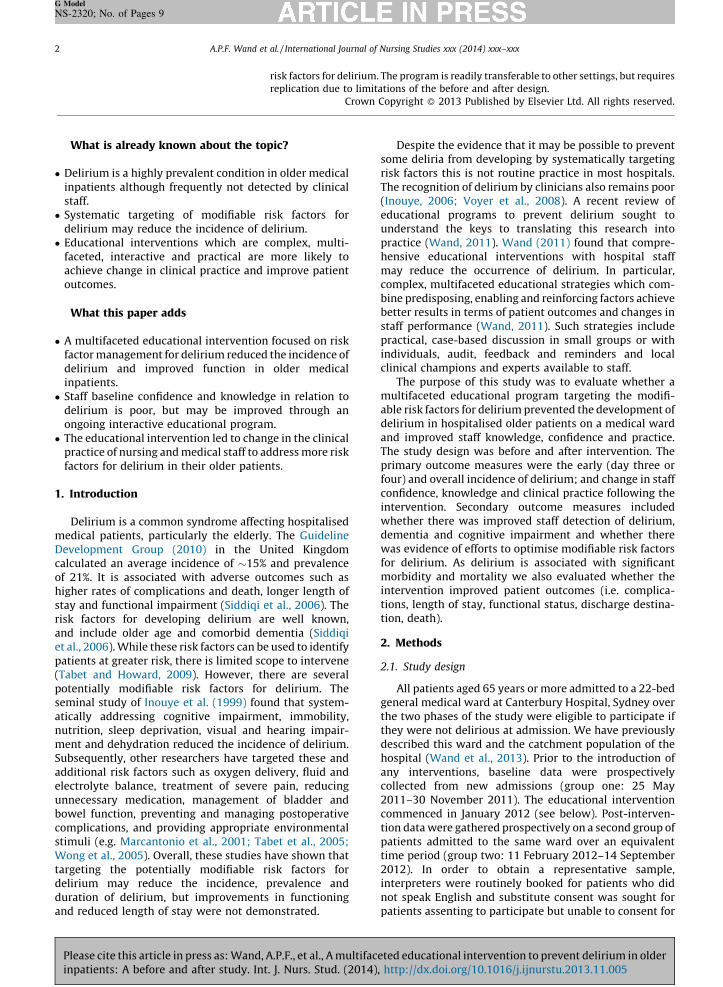
What is already known about the topic?
� Delirium is a highly prevalent condition in older medicalinpatients although frequently not detected by clinicalstaff.� Systematic targeting of modifiable risk factors for
delirium may reduce the incidence of delirium.� Educational interventions which are complex, multi-
faceted, interactive and practical are more likely toachieve change in clinical practice and improve patientoutcomes.
What this paper adds
� A multifaceted educational intervention focused on riskfactor management for delirium reduced the incidence ofdelirium and improved function in older medicalinpatients.� Staff baseline confidence and knowledge in relation to
delirium is poor, but may be improved through anongoing interactive educational program.� The educational intervention led to change in the clinical
practice of nursing and medical staff to address more riskfactors for delirium in their older patients.
1. Introduction
Delirium is a common syndrome affecting hospitalisedmedical patients, particularly the elderly. The GuidelineDevelopment Group (2010) in the United Kingdomcalculated an average incidence of �15% and prevalenceof 21%. It is associated with adverse outcomes such ashigher rates of complications and death, longer length ofstay and functional impairment (Siddiqi et al., 2006). Therisk factors for developing delirium are well known,and include older age and comorbid dementia (Siddiqiet al., 2006). While these risk factors can be used to identifypatients at greater risk, there is limited scope to intervene(Tabet and Howard, 2009). However, there are severalpotentially modifiable risk factors for delirium. Theseminal study of Inouye et al. (1999) found that system-atically addressing cognitive impairment, immobility,nutrition, sleep deprivation, visual and hearing impair-ment and dehydration reduced the incidence of delirium.Subsequently, other researchers have targeted these andadditional risk factors such as oxygen delivery, fluid andelectrolyte balance, treatment of severe pain, reducingunnecessary medication, management of bladder andbowel function, preventing and managing postoperativecomplications, and providing appropriate environmentalstimuli (e.g. Marcantonio et al., 2001; Tabet et al., 2005;Wong et al., 2005). Overall, these studies have shown thattargeting the potentially modifiable risk factors fordelirium may reduce the incidence, prevalence andduration of delirium, but improvements in functioningand reduced length of stay were not demonstrated.
Despite the evidence that it may be possible to preventsome deliria from developing by systematically targetingrisk factors this is not routine practice in most hospitals.The recognition of delirium by clinicians also remains poor(Inouye, 2006; Voyer et al., 2008). A recent review ofeducational programs to prevent delirium sought tounderstand the keys to translating this research intopractice (Wand, 2011). Wand (2011) found that compre-hensive educational interventions with hospital staffmay reduce the occurrence of delirium. In particular,complex, multifaceted educational strategies which com-bine predisposing, enabling and reinforcing factors achievebetter results in terms of patient outcomes and changes instaff performance (Wand, 2011). Such strategies includepractical, case-based discussion in small groups or withindividuals, audit, feedback and reminders and localclinical champions and experts available to staff.
The purpose of this study was to evaluate whether amultifaceted educational program targeting the modifi-able risk factors for delirium prevented the development ofdelirium in hospitalised older patients on a medical wardand improved staff knowledge, confidence and practice.The study design was before and after intervention. Theprimary outcome measures were the early (day three orfour) and overall incidence of delirium; and change in staffconfidence, knowledge and clinical practice following theintervention. Secondary outcome measures includedwhether there was improved staff detection of delirium,dementia and cognitive impairment and whether therewas evidence of efforts to optimise modifiable risk factorsfor delirium. As delirium is associated with significantmorbidity and mortality we also evaluated whether theintervention improved patient outcomes (i.e. complica-tions, length of stay, functional status, discharge destina-tion, death).
2. Methods
2.1. Study design
All patients aged 65 years or more admitted to a 22-bedgeneral medical ward at Canterbury Hospital, Sydney overthe two phases of the study were eligible to participate ifthey were not delirious at admission. We have previouslydescribed this ward and the catchment population of thehospital (Wand et al., 2013). Prior to the introduction ofany interventions, baseline data were prospectivelycollected from new admissions (group one: 25 May2011–30 November 2011). The educational interventioncommenced in January 2012 (see below). Post-interven-tion data were gathered prospectively on a second group ofpatients admitted to the same ward over an equivalenttime period (group two: 11 February 2012–14 September2012). In order to obtain a representative sample,interpreters were routinely booked for patients who didnot speak English and substitute consent was sought forpatients assenting to participate but unable to consent for
risk factors for delirium. The program is readily transferable to other settings, but requires
replication due to limitations of the before and after design.
Crown Copyright � 2013 Published by Elsevier Ltd. All rights reserved.
Please cite this article in press as: Wand, A.P.F., et al., A multifaceted educational intervention to prevent delirium in olderinpatients: A before and after study. Int. J. Nurs. Stud. (2014), http://dx.doi.org/10.1016/j.ijnurstu.2013.11.005

theappAlfr
asspereacwetoogerfor
psywhthescrethowaweconand
2.2.
2.2.
thrpubdaythememin197(RUlanand
Tab
Inte
Ri
Bl
Hy
Pa
Nu
Pa
M
Se
Re
Ox
Sle
M
M
Re
A.P.F. Wand et al. / International Journal of Nursing Studies xxx (2014) xxx–xxx 3
G Model
NS-2320; No. of Pages 9
Plin
mselves (Adamis et al., 2005). The research wasroved by the Ethics Review Committee (Royal Princeed Hospital zone).
The procedure for pre and post-intervention patientessments was identical. The assessments wereformed by two specialist registrars in training (one ofh in psychiatry and geriatric medicine). These registrarsre trained to interview and administer the assessmentls to participants and their carer/relative by a senioriatrician (WT). Supervision of assessments was providedthe duration of the study by the geriatrician (WT) andchogeriatrician (AW). As the project sought to determineether the educational intervention prevented delirium,
medical records of participants were reviewed in aening assessment within 24 h of admission to exclude
se with delirium on admission to the ward. Where thiss unclear clinical staff and/or the patient’s carer/relativere consulted to ascertain whether the patient was morefused than usual (Sands et al., 2010) or had symptoms
signs suggestive of delirium.
Participants
1. Patients: Cognitive and functional assessment
A comprehensive clinical interview took place at dayee or four of admission, but allowed some flexibility forlic holidays, weekends or interpreter availability (range
2–6). The interview included a general discussion with participant in addition to administering formal assess-nt tools. Cognitive impairment was assessed using thei-mental status examination (MMSE; Folstein et al.,5) or the Rowland universal dementia assessment scaleDAS; Storey et al., 2004), if English was not their first
guage. The Blessed dementia scale (Blessed et al., 1968) clock-draw test (Watson et al., 1993) were used to
assess for dementia, and the confusion assessment method(CAM; Inouye et al., 1990) to detect delirium. The Barthelactivities of daily living index (Shah et al., 1989; Ranhoff andLaake, 1993) was used to measure overall functioning. Wehave previously described in detail the purpose and scoringcriteria of these assessment tools (Wand et al., 2013). For thepurposes of this analysis, cognitive impairment wasconsidered present when MMSE/RUDAS scores were lessthan 26, and dementia was considered present whenBlessed scale scores were four or more. To achieve a positivescore (i.e. delirium present) on the 4-item CAM, the patientmust have an acute onset or fluctuating course andinattention, and either disorganised thinking or alteredlevel of consciousness (Inouye et al., 1990). To make adiagnosis of delirium, the CAM score was combined withclinical interview and discussion with the carer/relative, todetermine whether the patient appeared more confusedthan usual (Sands et al., 2010).
To improve the reliability of the data, the participant’scarer or relative was interviewed and assisted to completethe Blessed dementia scale and Barthel’s index (Ranhoffand Laake, 1993). Medical records were reviewed atdischarge to objectively determine patient outcomes(incident delirium, functional status (using the Barthel’sindex), length of stay, discharge destination, the numberand type of any complications, death) and staff clinicalpractice (documented evidence of identifying and addres-sing each of the 13 risk factors for delirium emphasised inthe education program- see Table 1) and staff documenta-tion of the diagnoses of delirium, cognitive impairmentand dementia. Incident delirium occurring at any timeduring admission was determined by careful file review,looking for symptoms and signs suggestive of delirium oran explicit reference to this diagnosis (see Wand et al.,2013). This is a strategy adapted from a previously
le 1
rventions to address risk factors for delirium.
sk factor Examples of staff interventions
adder and bowel function Monitor daily for constipation and urinary retention, use stool charts, offer aperients and contact medical
officer if no bowel output, urinalysis if symptoms of urinary tract infection
dration Encourage patient to drink, ensure drinks are accessible (e.g. assist with lids/packaging), monitor fluid status
with clinical examination and fluid chart
in Assess for pain (including non-verbal signs), follow World Health Organisation analgesic ladder and monitor
response, regular rather than pro re nata analgesia
trition Dentures that fit, appropriate consistency of food, food chart to monitor intake, ensure food is accessible (e.g.
assist with feeding or removing packaging), dietician/speech pathology review as appropriate
tient’s local environment Encourage a key family member to stay, orientation aids (calendars, newspaper, curtains open, familiar
items), minimise noise (from staff or too many visitors), avoid bed moves, optimise patient’s location on the
ward, nurse special if challenging behaviours and/or safety concerns, optimise comfort (temperature, day
activities, lighting)
obilisation Seek physiotherapy assessment if problems with mobility; encourage to mobilise at least 4 times/day; active
range of motion exercises if bed-bound
nsory aids and communication Ensure patient has access to their glasses, hearing aids (or a voice amplifier), dentures, interpreters, language
cards. Treat reversible causes of sensory impairment
move attachments Remove indwelling catheters, intravenous lines and restraints
ygenation Assess for hypoxia and provide supplemental oxygen as required
ep Monitoring for sleeping difficulties and emphasis on non-pharmacological strategies
edication review Wean and cease any deliriogenic medication, stop any non-essential medications to reduce overall number of
medications
anagement of drug dependence Assess for and manage drug dependence (e.g. benzodiazepines, nicotine)
straint use Avoid use of any physical restraint. Use non-pharmacological strategies to manage challenging behaviours
(e.g. walking with a restless patient, utilise a nurse special)
ease cite this article in press as: Wand, A.P.F., et al., A multifaceted educational intervention to prevent delirium in olderpatients: A before and after study. Int. J. Nurs. Stud. (2014), http://dx.doi.org/10.1016/j.ijnurstu.2013.11.005
A.P.F. Wand et al. / International Journal of Nursing Studies xxx (2014) xxx–xxx4
G Model
NS-2320; No. of Pages 9
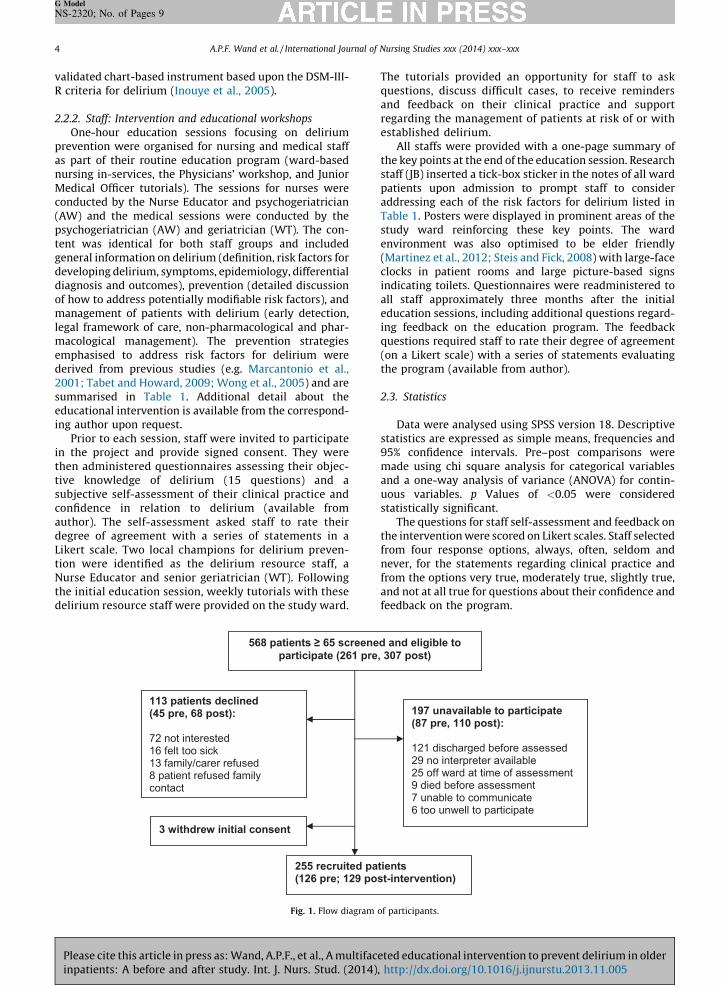
validated chart-based instrument based upon the DSM-III-R criteria for delirium (Inouye et al., 2005).
2.2.2. Staff: Intervention and educational workshops
One-hour education sessions focusing on deliriumprevention were organised for nursing and medical staffas part of their routine education program (ward-basednursing in-services, the Physicians’ workshop, and JuniorMedical Officer tutorials). The sessions for nurses wereconducted by the Nurse Educator and psychogeriatrician(AW) and the medical sessions were conducted by thepsychogeriatrician (AW) and geriatrician (WT). The con-tent was identical for both staff groups and includedgeneral information on delirium (definition, risk factors fordeveloping delirium, symptoms, epidemiology, differentialdiagnosis and outcomes), prevention (detailed discussionof how to address potentially modifiable risk factors), andmanagement of patients with delirium (early detection,legal framework of care, non-pharmacological and phar-macological management). The prevention strategiesemphasised to address risk factors for delirium werederived from previous studies (e.g. Marcantonio et al.,2001; Tabet and Howard, 2009; Wong et al., 2005) and aresummarised in Table 1. Additional detail about theeducational intervention is available from the correspond-ing author upon request.
Prior to each session, staff were invited to participatein the project and provide signed consent. They werethen administered questionnaires assessing their objec-tive knowledge of delirium (15 questions) and asubjective self-assessment of their clinical practice andconfidence in relation to delirium (available fromauthor). The self-assessment asked staff to rate theirdegree of agreement with a series of statements in aLikert scale. Two local champions for delirium preven-tion were identified as the delirium resource staff, aNurse Educator and senior geriatrician (WT). Followingthe initial education session, weekly tutorials with thesedelirium resource staff were provided on the study ward.
The tutorials provided an opportunity for staff to askquestions, discuss difficult cases, to receive remindersand feedback on their clinical practice and supportregarding the management of patients at risk of or withestablished delirium.
All staffs were provided with a one-page summary ofthe key points at the end of the education session. Researchstaff (JB) inserted a tick-box sticker in the notes of all wardpatients upon admission to prompt staff to consideraddressing each of the risk factors for delirium listed inTable 1. Posters were displayed in prominent areas of thestudy ward reinforcing these key points. The wardenvironment was also optimised to be elder friendly(Martinez et al., 2012; Steis and Fick, 2008) with large-faceclocks in patient rooms and large picture-based signsindicating toilets. Questionnaires were readministered toall staff approximately three months after the initialeducation sessions, including additional questions regard-ing feedback on the education program. The feedbackquestions required staff to rate their degree of agreement(on a Likert scale) with a series of statements evaluatingthe program (available from author).
2.3. Statistics
Data were analysed using SPSS version 18. Descriptivestatistics are expressed as simple means, frequencies and95% confidence intervals. Pre–post comparisons weremade using chi square analysis for categorical variablesand a one-way analysis of variance (ANOVA) for contin-uous variables. p Values of <0.05 were consideredstatistically significant.
The questions for staff self-assessment and feedback onthe intervention were scored on Likert scales. Staff selectedfrom four response options, always, often, seldom andnever, for the statements regarding clinical practice andfrom the options very true, moderately true, slightly true,and not at all true for questions about their confidence andfeedback on the program.
568 patients ≥ 65 scree ned and eligibl e to particip ate (261 pre, 307 po st)
113 patie nts de clin ed (45 pre, 68 post):
72 not inte rest ed 16 felt too s ick 13 family/c arer refused 8 patien t re fused family contact
197 un avail able to participate (87 pre, 110 post):
121 disc harged befor e ass ess ed 29 no interp reter available 25 off ward at t ime of assessment 9 died before ass ess ment 7 un able to comm unicat e 6 too unwell to participate
3 withdr ew initi al cons ent
255 recruit ed patien ts (126 pre; 129 po st-int ervention)
Fig. 1. Flow diagram of participants.
Please cite this article in press as: Wand, A.P.F., et al., A multifaceted educational intervention to prevent delirium in olderinpatients: A before and after study. Int. J. Nurs. Stud. (2014), http://dx.doi.org/10.1016/j.ijnurstu.2013.11.005
3. R
3.1.
andposparthrpatintegenas areacom(78profrac
priointethe(18patanyass
gronitipreper253cogadmin Bintep <
theass
Tab
Com
inte
M
Ge
Ne
M
M
Co
M
De
M
Ba
Ba
De
Ov
Nu
Le
Di
In
NS =a
A.P.F. Wand et al. / International Journal of Nursing Studies xxx (2014) xxx–xxx 5
G Model
NS-2320; No. of Pages 9
Plin
esults
Patients
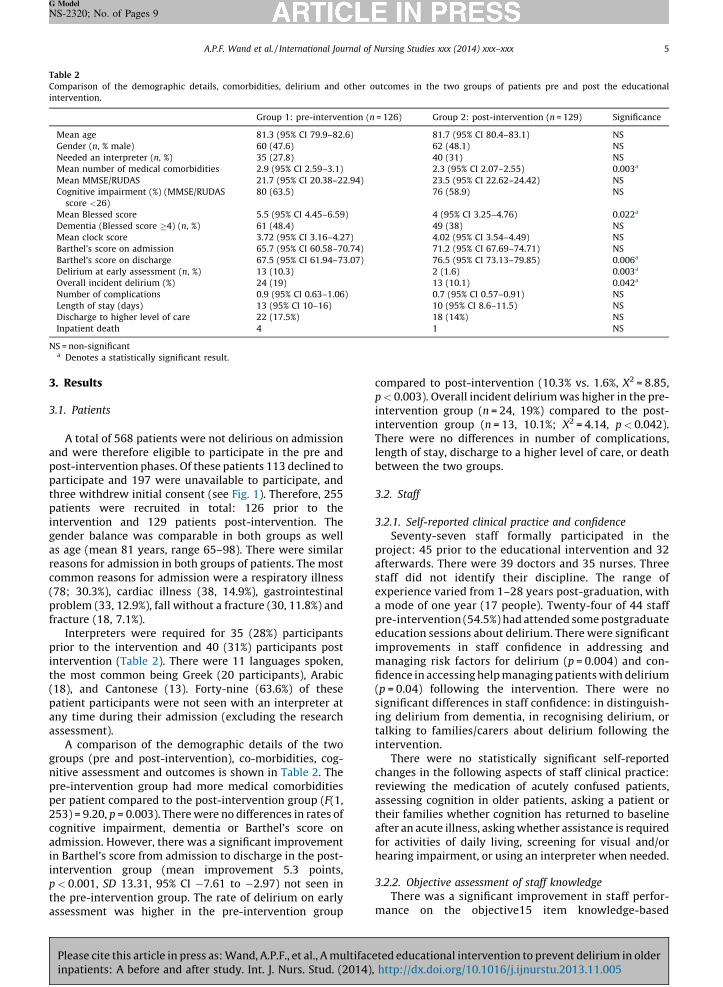
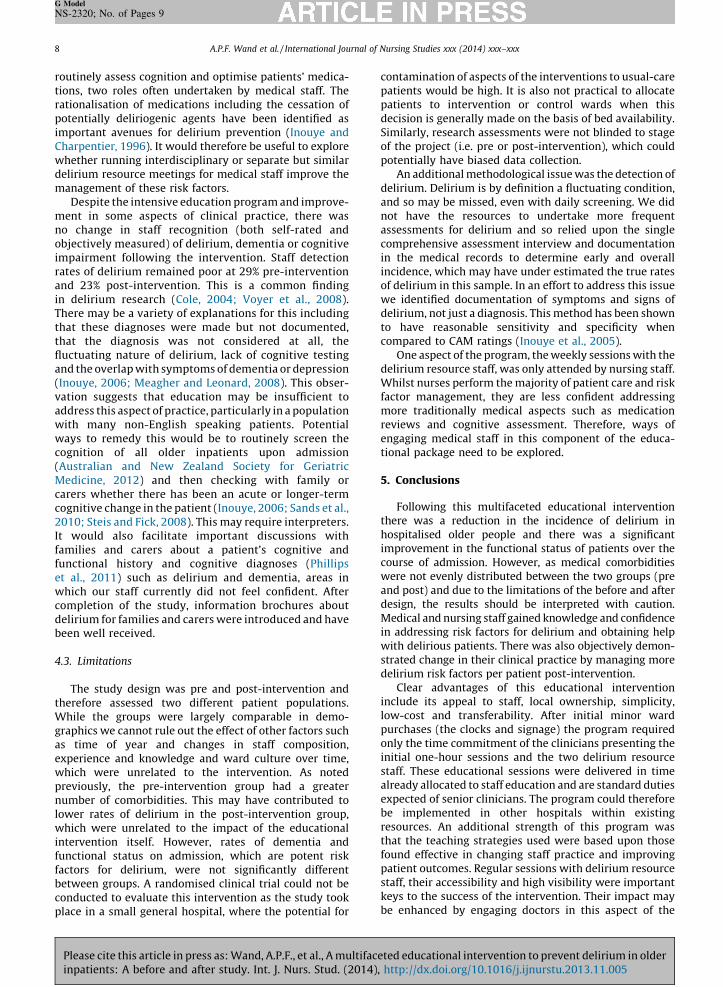
A total of 568 patients were not delirious on admission were therefore eligible to participate in the pre andt-intervention phases. Of these patients 113 declined toticipate and 197 were unavailable to participate, andee withdrew initial consent (see Fig. 1). Therefore, 255ients were recruited in total: 126 prior to thervention and 129 patients post-intervention. Theder balance was comparable in both groups as wellge (mean 81 years, range 65–98). There were similar
sons for admission in both groups of patients. The mostmon reasons for admission were a respiratory illness
; 30.3%), cardiac illness (38, 14.9%), gastrointestinalblem (33, 12.9%), fall without a fracture (30, 11.8%) andture (18, 7.1%).
Interpreters were required for 35 (28%) participantsr to the intervention and 40 (31%) participants postrvention (Table 2). There were 11 languages spoken,
most common being Greek (20 participants), Arabic), and Cantonese (13). Forty-nine (63.6%) of theseient participants were not seen with an interpreter at
time during their admission (excluding the researchessment).A comparison of the demographic details of the twoups (pre and post-intervention), co-morbidities, cog-ve assessment and outcomes is shown in Table 2. The-intervention group had more medical comorbidities patient compared to the post-intervention group (F(1,) = 9.20, p = 0.003). There were no differences in rates ofnitive impairment, dementia or Barthel’s score onission. However, there was a significant improvement
arthel’s score from admission to discharge in the post-rvention group (mean improvement 5.3 points,
0.001, SD 13.31, 95% CI �7.61 to �2.97) not seen in pre-intervention group. The rate of delirium on early
compared to post-intervention (10.3% vs. 1.6%, X2 = 8.85,p < 0.003). Overall incident delirium was higher in the pre-intervention group (n = 24, 19%) compared to the post-intervention group (n = 13, 10.1%; X2 = 4.14, p < 0.042).There were no differences in number of complications,length of stay, discharge to a higher level of care, or deathbetween the two groups.
3.2. Staff
3.2.1. Self-reported clinical practice and confidence
Seventy-seven staff formally participated in theproject: 45 prior to the educational intervention and 32afterwards. There were 39 doctors and 35 nurses. Threestaff did not identify their discipline. The range ofexperience varied from 1–28 years post-graduation, witha mode of one year (17 people). Twenty-four of 44 staffpre-intervention (54.5%) had attended some postgraduateeducation sessions about delirium. There were significantimprovements in staff confidence in addressing andmanaging risk factors for delirium (p = 0.004) and con-fidence in accessing help managing patients with delirium(p = 0.04) following the intervention. There were nosignificant differences in staff confidence: in distinguish-ing delirium from dementia, in recognising delirium, ortalking to families/carers about delirium following theintervention.
There were no statistically significant self-reportedchanges in the following aspects of staff clinical practice:reviewing the medication of acutely confused patients,assessing cognition in older patients, asking a patient ortheir families whether cognition has returned to baselineafter an acute illness, asking whether assistance is requiredfor activities of daily living, screening for visual and/orhearing impairment, or using an interpreter when needed.
3.2.2. Objective assessment of staff knowledge
There was a significant improvement in staff perfor-
le 2
parison of the demographic details, comorbidities, delirium and other outcomes in the two groups of patients pre and post the educational
rvention.
Group 1: pre-intervention (n = 126) Group 2: post-intervention (n = 129) Significance
ean age 81.3 (95% CI 79.9–82.6) 81.7 (95% CI 80.4–83.1) NS
nder (n, % male) 60 (47.6) 62 (48.1) NS
eded an interpreter (n, %) 35 (27.8) 40 (31) NS
ean number of medical comorbidities 2.9 (95% CI 2.59–3.1) 2.3 (95% CI 2.07–2.55) 0.003a
ean MMSE/RUDAS 21.7 (95% CI 20.38–22.94) 23.5 (95% CI 22.62–24.42) NS
gnitive impairment (%) (MMSE/RUDAS
score <26)
80 (63.5) 76 (58.9) NS
ean Blessed score 5.5 (95% CI 4.45–6.59) 4 (95% CI 3.25–4.76) 0.022a
mentia (Blessed score �4) (n, %) 61 (48.4) 49 (38) NS
ean clock score 3.72 (95% CI 3.16–4.27) 4.02 (95% CI 3.54–4.49) NS
rthel’s score on admission 65.7 (95% CI 60.58–70.74) 71.2 (95% CI 67.69–74.71) NS
rthel’s score on discharge 67.5 (95% CI 61.94–73.07) 76.5 (95% CI 73.13–79.85) 0.006a
lirium at early assessment (n, %) 13 (10.3) 2 (1.6) 0.003a
erall incident delirium (%) 24 (19) 13 (10.1) 0.042a
mber of complications 0.9 (95% CI 0.63–1.06) 0.7 (95% CI 0.57–0.91) NS
ngth of stay (days) 13 (95% CI 10–16) 10 (95% CI 8.6–11.5) NS
scharge to higher level of care 22 (17.5%) 18 (14%) NS
patient death 4 1 NS
non-significant
Denotes a statistically significant result.
nce on the objective15 item knowledge-based
essment was higher in the pre-intervention group maease cite this article in press as: Wand, A.P.F., et al., A multifaceted educational intervention to prevent delirium in olderpatients: A before and after study. Int. J. Nurs. Stud. (2014), http://dx.doi.org/10.1016/j.ijnurstu.2013.11.005
A.P.F. Wand et al. / International Journal of Nursing Studies xxx (2014) xxx–xxx6
G Model
NS-2320; No. of Pages 9
questionnaire about delirium after the intervention (F(1,73) = 4.34, p = 0.041).
3.2.3. Objective assessment of clinical practice (chart review)
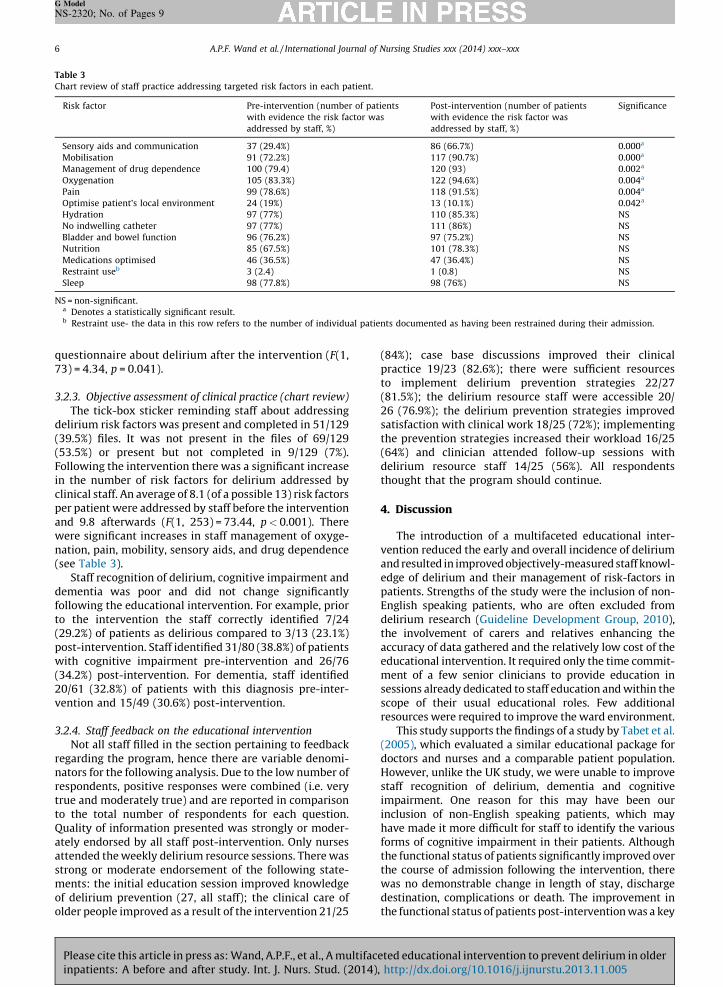
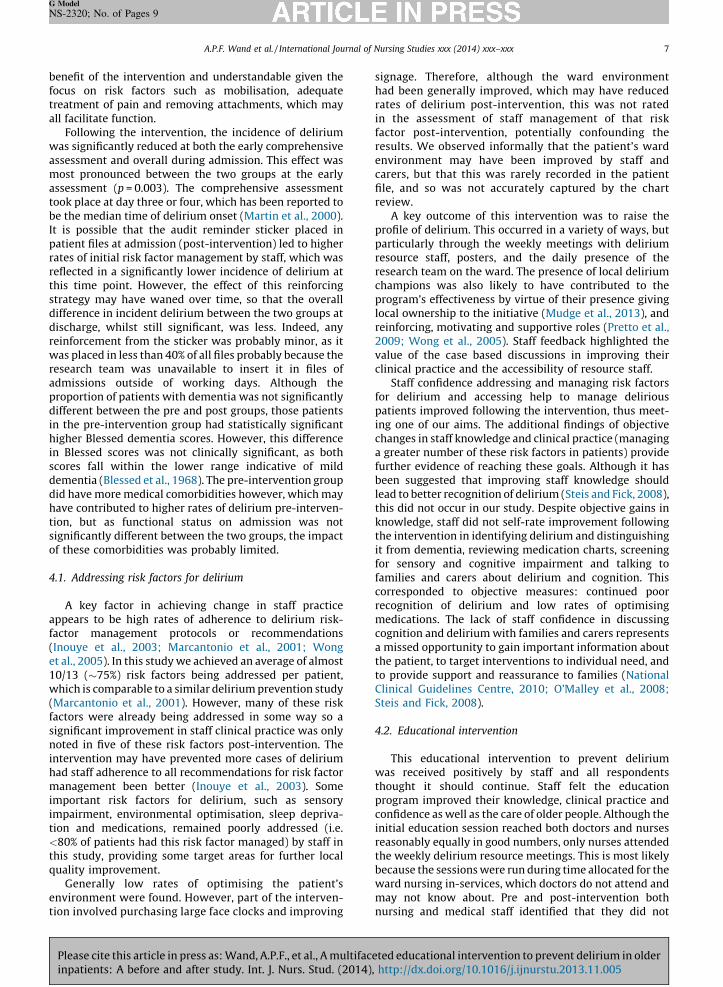
The tick-box sticker reminding staff about addressingdelirium risk factors was present and completed in 51/129(39.5%) files. It was not present in the files of 69/129(53.5%) or present but not completed in 9/129 (7%).Following the intervention there was a significant increasein the number of risk factors for delirium addressed byclinical staff. An average of 8.1 (of a possible 13) risk factorsper patient were addressed by staff before the interventionand 9.8 afterwards (F(1, 253) = 73.44, p < 0.001). Therewere significant increases in staff management of oxyge-nation, pain, mobility, sensory aids, and drug dependence(see Table 3).
Staff recognition of delirium, cognitive impairment anddementia was poor and did not change significantlyfollowing the educational intervention. For example, priorto the intervention the staff correctly identified 7/24(29.2%) of patients as delirious compared to 3/13 (23.1%)post-intervention. Staff identified 31/80 (38.8%) of patientswith cognitive impairment pre-intervention and 26/76(34.2%) post-intervention. For dementia, staff identified20/61 (32.8%) of patients with this diagnosis pre-inter-vention and 15/49 (30.6%) post-intervention.
3.2.4. Staff feedback on the educational intervention
Not all staff filled in the section pertaining to feedbackregarding the program, hence there are variable denomi-nators for the following analysis. Due to the low number ofrespondents, positive responses were combined (i.e. verytrue and moderately true) and are reported in comparisonto the total number of respondents for each question.Quality of information presented was strongly or moder-ately endorsed by all staff post-intervention. Only nursesattended the weekly delirium resource sessions. There wasstrong or moderate endorsement of the following state-ments: the initial education session improved knowledgeof delirium prevention (27, all staff); the clinical care ofolder people improved as a result of the intervention 21/25
(84%); case base discussions improved their clinicalpractice 19/23 (82.6%); there were sufficient resourcesto implement delirium prevention strategies 22/27(81.5%); the delirium resource staff were accessible 20/26 (76.9%); the delirium prevention strategies improvedsatisfaction with clinical work 18/25 (72%); implementingthe prevention strategies increased their workload 16/25(64%) and clinician attended follow-up sessions withdelirium resource staff 14/25 (56%). All respondentsthought that the program should continue.
4. Discussion
The introduction of a multifaceted educational inter-vention reduced the early and overall incidence of deliriumand resulted in improved objectively-measured staff knowl-edge of delirium and their management of risk-factors inpatients. Strengths of the study were the inclusion of non-English speaking patients, who are often excluded fromdelirium research (Guideline Development Group, 2010),the involvement of carers and relatives enhancing theaccuracy of data gathered and the relatively low cost of theeducational intervention. It required only the time commit-ment of a few senior clinicians to provide education insessions already dedicated to staff education and within thescope of their usual educational roles. Few additionalresources were required to improve the ward environment.
This study supports the findings of a study by Tabet et al.(2005), which evaluated a similar educational package fordoctors and nurses and a comparable patient population.However, unlike the UK study, we were unable to improvestaff recognition of delirium, dementia and cognitiveimpairment. One reason for this may have been ourinclusion of non-English speaking patients, which mayhave made it more difficult for staff to identify the variousforms of cognitive impairment in their patients. Althoughthe functional status of patients significantly improved overthe course of admission following the intervention, therewas no demonstrable change in length of stay, dischargedestination, complications or death. The improvement inthe functional status of patients post-intervention was a key
Table 3
Chart review of staff practice addressing targeted risk factors in each patient.
Risk factor Pre-intervention (number of patients
with evidence the risk factor was
addressed by staff, %)
Post-intervention (number of patients
with evidence the risk factor was
addressed by staff, %)
Significance
Sensory aids and communication 37 (29.4%) 86 (66.7%) 0.000a
Mobilisation 91 (72.2%) 117 (90.7%) 0.000a
Management of drug dependence 100 (79.4) 120 (93) 0.002a
Oxygenation 105 (83.3%) 122 (94.6%) 0.004a
Pain 99 (78.6%) 118 (91.5%) 0.004a
Optimise patient’s local environment 24 (19%) 13 (10.1%) 0.042a
Hydration 97 (77%) 110 (85.3%) NS
No indwelling catheter 97 (77%) 111 (86%) NS
Bladder and bowel function 96 (76.2%) 97 (75.2%) NS
Nutrition 85 (67.5%) 101 (78.3%) NS
Medications optimised 46 (36.5%) 47 (36.4%) NS
Restraint useb 3 (2.4) 1 (0.8) NS
Sleep 98 (77.8%) 98 (76%) NS
NS = non-significant.a Denotes a statistically significant result.b Restraint use- the data in this row refers to the number of individual patients documented as having been restrained during their admission.
Please cite this article in press as: Wand, A.P.F., et al., A multifaceted educational intervention to prevent delirium in olderinpatients: A before and after study. Int. J. Nurs. Stud. (2014), http://dx.doi.org/10.1016/j.ijnurstu.2013.11.005
benfoctreaall
waassmoasstoobe
It ipatratereflthisstradiffdiscreinwaresadmprodiffin thigin
scodemdidhavtionsignof t
4.1.
appfact(Inoet a10/wh(Mafactsignnotintehadmaimpimption<8thisqua
envtion
A.P.F. Wand et al. / International Journal of Nursing Studies xxx (2014) xxx–xxx 7
G Model
NS-2320; No. of Pages 9
Plin
efit of the intervention and understandable given theus on risk factors such as mobilisation, adequatetment of pain and removing attachments, which may
facilitate function.Following the intervention, the incidence of deliriums significantly reduced at both the early comprehensiveessment and overall during admission. This effect wasst pronounced between the two groups at the earlyessment (p = 0.003). The comprehensive assessmentk place at day three or four, which has been reported tothe median time of delirium onset (Martin et al., 2000).s possible that the audit reminder sticker placed inient files at admission (post-intervention) led to highers of initial risk factor management by staff, which was
ected in a significantly lower incidence of delirium at time point. However, the effect of this reinforcingtegy may have waned over time, so that the overallerence in incident delirium between the two groups atharge, whilst still significant, was less. Indeed, anyforcement from the sticker was probably minor, as it
s placed in less than 40% of all files probably because theearch team was unavailable to insert it in files of
issions outside of working days. Although theportion of patients with dementia was not significantlyerent between the pre and post groups, those patientshe pre-intervention group had statistically significanther Blessed dementia scores. However, this differenceBlessed scores was not clinically significant, as bothres fall within the lower range indicative of mild
entia (Blessed et al., 1968). The pre-intervention group have more medical comorbidities however, which maye contributed to higher rates of delirium pre-interven-, but as functional status on admission was notificantly different between the two groups, the impact
hese comorbidities was probably limited.
Addressing risk factors for delirium
A key factor in achieving change in staff practiceears to be high rates of adherence to delirium risk-or management protocols or recommendationsuye et al., 2003; Marcantonio et al., 2001; Wongl., 2005). In this study we achieved an average of almost13 (�75%) risk factors being addressed per patient,ich is comparable to a similar delirium prevention studyrcantonio et al., 2001). However, many of these riskors were already being addressed in some way so aificant improvement in staff clinical practice was only
ed in five of these risk factors post-intervention. Thervention may have prevented more cases of delirium
staff adherence to all recommendations for risk factornagement been better (Inouye et al., 2003). Someortant risk factors for delirium, such as sensoryairment, environmental optimisation, sleep depriva- and medications, remained poorly addressed (i.e.
0% of patients had this risk factor managed) by staff in study, providing some target areas for further locallity improvement.
Generally low rates of optimising the patient’sironment were found. However, part of the interven-
involved purchasing large face clocks and improving
signage. Therefore, although the ward environmenthad been generally improved, which may have reducedrates of delirium post-intervention, this was not ratedin the assessment of staff management of that riskfactor post-intervention, potentially confounding theresults. We observed informally that the patient’s wardenvironment may have been improved by staff andcarers, but that this was rarely recorded in the patientfile, and so was not accurately captured by the chartreview.
A key outcome of this intervention was to raise theprofile of delirium. This occurred in a variety of ways, butparticularly through the weekly meetings with deliriumresource staff, posters, and the daily presence of theresearch team on the ward. The presence of local deliriumchampions was also likely to have contributed to theprogram’s effectiveness by virtue of their presence givinglocal ownership to the initiative (Mudge et al., 2013), andreinforcing, motivating and supportive roles (Pretto et al.,2009; Wong et al., 2005). Staff feedback highlighted thevalue of the case based discussions in improving theirclinical practice and the accessibility of resource staff.
Staff confidence addressing and managing risk factorsfor delirium and accessing help to manage deliriouspatients improved following the intervention, thus meet-ing one of our aims. The additional findings of objectivechanges in staff knowledge and clinical practice (managinga greater number of these risk factors in patients) providefurther evidence of reaching these goals. Although it hasbeen suggested that improving staff knowledge shouldlead to better recognition of delirium (Steis and Fick, 2008),this did not occur in our study. Despite objective gains inknowledge, staff did not self-rate improvement followingthe intervention in identifying delirium and distinguishingit from dementia, reviewing medication charts, screeningfor sensory and cognitive impairment and talking tofamilies and carers about delirium and cognition. Thiscorresponded to objective measures: continued poorrecognition of delirium and low rates of optimisingmedications. The lack of staff confidence in discussingcognition and delirium with families and carers representsa missed opportunity to gain important information aboutthe patient, to target interventions to individual need, andto provide support and reassurance to families (NationalClinical Guidelines Centre, 2010; O’Malley et al., 2008;Steis and Fick, 2008).
4.2. Educational intervention
This educational intervention to prevent deliriumwas received positively by staff and all respondentsthought it should continue. Staff felt the educationprogram improved their knowledge, clinical practice andconfidence as well as the care of older people. Although theinitial education session reached both doctors and nursesreasonably equally in good numbers, only nurses attendedthe weekly delirium resource meetings. This is most likelybecause the sessions were run during time allocated for theward nursing in-services, which doctors do not attend andmay not know about. Pre and post-intervention bothnursing and medical staff identified that they did not
ease cite this article in press as: Wand, A.P.F., et al., A multifaceted educational intervention to prevent delirium in olderpatients: A before and after study. Int. J. Nurs. Stud. (2014), http://dx.doi.org/10.1016/j.ijnurstu.2013.11.005
A.P.F. Wand et al. / International Journal of Nursing Studies xxx (2014) xxx–xxx8
G Model
NS-2320; No. of Pages 9
routinely assess cognition and optimise patients’ medica-tions, two roles often undertaken by medical staff. Therationalisation of medications including the cessation ofpotentially deliriogenic agents have been identified asimportant avenues for delirium prevention (Inouye andCharpentier, 1996). It would therefore be useful to explorewhether running interdisciplinary or separate but similardelirium resource meetings for medical staff improve themanagement of these risk factors.
Despite the intensive education program and improve-ment in some aspects of clinical practice, there wasno change in staff recognition (both self-rated andobjectively measured) of delirium, dementia or cognitiveimpairment following the intervention. Staff detectionrates of delirium remained poor at 29% pre-interventionand 23% post-intervention. This is a common findingin delirium research (Cole, 2004; Voyer et al., 2008).There may be a variety of explanations for this includingthat these diagnoses were made but not documented,that the diagnosis was not considered at all, thefluctuating nature of delirium, lack of cognitive testingand the overlap with symptoms of dementia or depression(Inouye, 2006; Meagher and Leonard, 2008). This obser-vation suggests that education may be insufficient toaddress this aspect of practice, particularly in a populationwith many non-English speaking patients. Potentialways to remedy this would be to routinely screen thecognition of all older inpatients upon admission(Australian and New Zealand Society for GeriatricMedicine, 2012) and then checking with family orcarers whether there has been an acute or longer-termcognitive change in the patient (Inouye, 2006; Sands et al.,2010; Steis and Fick, 2008). This may require interpreters.It would also facilitate important discussions withfamilies and carers about a patient’s cognitive andfunctional history and cognitive diagnoses (Phillipset al., 2011) such as delirium and dementia, areas inwhich our staff currently did not feel confident. Aftercompletion of the study, information brochures aboutdelirium for families and carers were introduced and havebeen well received.
4.3. Limitations
The study design was pre and post-intervention andtherefore assessed two different patient populations.While the groups were largely comparable in demo-graphics we cannot rule out the effect of other factors suchas time of year and changes in staff composition,experience and knowledge and ward culture over time,which were unrelated to the intervention. As notedpreviously, the pre-intervention group had a greaternumber of comorbidities. This may have contributed tolower rates of delirium in the post-intervention group,which were unrelated to the impact of the educationalintervention itself. However, rates of dementia andfunctional status on admission, which are potent riskfactors for delirium, were not significantly differentbetween groups. A randomised clinical trial could not beconducted to evaluate this intervention as the study took
contamination of aspects of the interventions to usual-carepatients would be high. It is also not practical to allocatepatients to intervention or control wards when thisdecision is generally made on the basis of bed availability.Similarly, research assessments were not blinded to stageof the project (i.e. pre or post-intervention), which couldpotentially have biased data collection.
An additional methodological issue was the detection ofdelirium. Delirium is by definition a fluctuating condition,and so may be missed, even with daily screening. We didnot have the resources to undertake more frequentassessments for delirium and so relied upon the singlecomprehensive assessment interview and documentationin the medical records to determine early and overallincidence, which may have under estimated the true ratesof delirium in this sample. In an effort to address this issuewe identified documentation of symptoms and signs ofdelirium, not just a diagnosis. This method has been shownto have reasonable sensitivity and specificity whencompared to CAM ratings (Inouye et al., 2005).
One aspect of the program, the weekly sessions with thedelirium resource staff, was only attended by nursing staff.Whilst nurses perform the majority of patient care and riskfactor management, they are less confident addressingmore traditionally medical aspects such as medicationreviews and cognitive assessment. Therefore, ways ofengaging medical staff in this component of the educa-tional package need to be explored.
5. Conclusions
Following this multifaceted educational interventionthere was a reduction in the incidence of delirium inhospitalised older people and there was a significantimprovement in the functional status of patients over thecourse of admission. However, as medical comorbiditieswere not evenly distributed between the two groups (preand post) and due to the limitations of the before and afterdesign, the results should be interpreted with caution.Medical and nursing staff gained knowledge and confidencein addressing risk factors for delirium and obtaining helpwith delirious patients. There was also objectively demon-strated change in their clinical practice by managing moredelirium risk factors per patient post-intervention.
Clear advantages of this educational interventioninclude its appeal to staff, local ownership, simplicity,low-cost and transferability. After initial minor wardpurchases (the clocks and signage) the program requiredonly the time commitment of the clinicians presenting theinitial one-hour sessions and the two delirium resourcestaff. These educational sessions were delivered in timealready allocated to staff education and are standard dutiesexpected of senior clinicians. The program could thereforebe implemented in other hospitals within existingresources. An additional strength of this program wasthat the teaching strategies used were based upon thosefound effective in changing staff practice and improvingpatient outcomes. Regular sessions with delirium resourcestaff, their accessibility and high visibility were importantkeys to the success of the intervention. Their impact may
be enhanced by engaging doctors in this aspect of the place in a small general hospital, where the potential forPlease cite this article in press as: Wand, A.P.F., et al., A multifaceted educational intervention to prevent delirium in olderinpatients: A before and after study. Int. J. Nurs. Stud. (2014), http://dx.doi.org/10.1016/j.ijnurstu.2013.11.005

prohoseduin
innsyn
Dec
Fun
Eth
Com
Ack
deldelstu
Ref
Ada
Aus
Bles
Cole
Fols
Guid
Inou
Inou
Inou
Inou
A.P.F. Wand et al. / International Journal of Nursing Studies xxx (2014) xxx–xxx 9
G Model
NS-2320; No. of Pages 9
Plin
gram. Given the scale of the problem of delirium in thepitalised elderly, deficits in postgraduate deliriumcation and the significant associated adverse outcomespatients, further study of sustainable, affordableovations to reduce the incidence of this preventabledrome in real-world settings is imperative.
laration of conflict of interest
None declared.
ding
None declared.
ical approval
The research was approved by the Ethics Reviewmittee (Royal Prince Alfred Hospital zone).
nowledgements
The authors thank Ms Anthea Temple for providing theirium prevention posters and allowing the use of heririum questionnaire, which was adapted for use in thisdy.
erences
mis, D., Martin, F.C., Treloar, A., Macdonald, A.J.D., 2005. Capacity,consent, and selection bias in a study of delirium. Journal of MedicalEthics 31, 137–143.tralian and New Zealand Society for Geriatric Medicine, 2012. PositionStatement 13. Delirium in Older People. Australian and New ZealandSociety for Geriatric Medicine, Sydney. Retrieved from http://www.anzsgm.org/documents/PS13DeliriumstatementRevi-sion2012.pdf, Accessed 1/7/2013.sed, G., Tomlinson, B.E., Roth, M., 1968. The association betweenquantitative measures of dementia and of senile change in thecerebral grey matter of elderly subjects. British Journal of Psychiatry114, 797–811., M.G., 2004. Delirium in elderly patients. American Journal of Ger-iatric Psychiatry 12, 7–21.tein, M.F., Folstein, S.E., McHugh, P.R., 1975. Mini-mental state: apractical method for grading the cognitive state of patients for theclinician. Journal of Psychiatric Research 12, 189–198.eline Development Group, 2010. Delirium: Diagnosis, Prevention,
and Management—Clinical Guideline 103. National Clinical GuidelineCentre, Royal College of Physicians, London. Retrieved from http://www.nice.org.uk/nicemedia/live/13060/49908/49908.pdf, Accessed1/7/2013.ye, S.K., Charpentier, P.A., 1996. Precipitating factors for delirium in
hospitalised elderly persons: predictive model and interrelationshipwith baseline vulnerability. Journal of the American Medical Associa-tion 275, 852–857.ye, S.K., Bogardus, S.T., Charpentier, P.A., Leo-Summers, L., Acampora,
D., Holford, T.R., Cooney Jr., L.M., 1999. A multicomponent interven-tion to prevent delirium in hospitalised older patients. New EnglandJournal of Medicine 340, 669–676.ye, S.K., Van Dyck, C.H., Alessi, C.A., Balkin, S., Siegal, A.P., Horwitz, R.I.,
1990. Clarifying confusion: the confusion assessment method: a newmethod for detection of delirium. Annals of Internal Medicine 113,941–948.ye, S.K., Bogardus, T., Williams, C.S., Leo-Summers, L., Agostini, J.V.,
2003. The role of adherence on the effectiveness of nonpharmacologicinterventions: evidence from the delirium prevention trial. Archivesof Internal Medicine 163, 958–964.
Inouye, S.K., Leo-Summers, L., Zhang, Y., Bogardus Jr., S.T., Leslie, D.L.,Agostini, J.V., 2005. A chart-based method for identification ofdelirium: validation compared with interviewer ratings using theconfusion assessment method. Journal of the American GeriatricsSociety 53, 312–318.
Inouye, S.K., 2006. Delirium in older persons. New England Journal ofMedicine 354, 1157–1165.
Martin, N.J., Stones, M.J., Young, J.E., Bedard, M., 2000. Development ofdelirium: a prospective cohort study in a community hospital. Inter-national Psychogeriatrics 12, 117–127.
Martinez, F.T., Tobar, C., Beddings, C.I., Vallejo, G., Fuentes, P., 2012.Preventing delirium in an acute hospital using a non-pharmacologicalintervention. Age and Ageing 41, 629–634.
Marcantonio, E.R., Flacker, J.M., Wright, J., Resnick, N.M., 2001. Reducingdelirium after hip fracture: a randomised trial. Journal of the Amer-ican Geriatric Society 49, 516–522.
Meagher, D., Leonard, M., 2008. The active management of delirium:improving detection and treatment. Advances in Psychiatric Treat-ment 14, 292–293.
Mudge, A.M., Maussen, C., Duncan, J., Denaro, C.P., 2013. Improving thequality of delirium care in a general medical service with establishedinterdisciplinary care: a controlled trial. Internal Medicine Journal 43,270–277.
National Clinical Guidelines Centre, 2010. Delirium: Diagnosis, Preventionand Management. National Clinical Guidelines Centre at the RoyalCollege of Physicians, London. Retrieved from http://www.nice.or-g.uk/nicemedia/live/13060/49908/49908.pdf, Accessed 1/7/2013.
O’Malley, G., Leonard, M., Meagher, D., O’Keeffe, S.T., 2008. The deliriumexperience: a review. Journal of Psychosomatic Research 65, 223–228.
Phillips, J., Pond, D., Goode, S., 2011. Timely Diagnosis of Dementia: CanWe Do Better? A Report for Alzheimer’s Australia. Paper 24Scullin,Australian Capital Territory. Retrieved from http://www.fightdemen-tia.org.au/common/files/NAT/Timely_Diagnosis_Can_we_do_bet-ter.pdf, Accessed 1/7/2013.
Pretto, M., Spirig, R., Milisen, K., Degeest, S., Regazzoni, P., Hasemann, W.,2009. Effects of an interdisciplinary nurse-led delirium preventionand management program (DPMP) on nursing workload: a pilotstudy. International Journal of Nursing Studies 46, 804–812.
Ranhoff, A., Laake, K., 1993. The Barthel activities of daily living index:scoring by the physician from patient interview is not reliable. Ageand Ageing 22, 171–174.
Sands, M.B., Dantoc, B.P., Hartshorn, A., Ryan, C.J., Lujic, S., 2010. Singlequestion in delirium (SQiD): testing its efficacy against psychiatristinterview, the confusion assessment method and memorial deliriumassessment scale. Palliative Medicine 24, 561–565.
Shah, S., Vanclay, F., Cooper, B., 1989. Improving the sensitivity of theBarthel index for stroke rehabilitation. Journal of Clinical Epidemiol-ogy 42, 703–709.
Siddiqi, N., House, A., Holmes, J., 2006. Occurrence and outcome ofdelirium in medical in-patients: a systematic literature review. Ageand Ageing 35, 350–364.
Steis, M.R., Fick, D.M., 2008. Are nurses recognising delirium? Journal ofGerontological Nursing 34, 40–48.
Storey, J.E., Rowland, J.T., Conforti, D.A., Dickson, H.G., 2004. The Rowlanduniversal dementia assessment scale (RUDAS): a multicultural cog-nitive assessment scale. International Psychogeriatrics 16, 13–31.
Tabet, N., Hudson, S., Sweeney, V., Sauer, J., Bryant, C., Macdonald, A.,Howard, R., 2005. An educational intervention can prevent deliriumon acute medical wards. Age and Ageing 34, 152–156.
Tabet, N., Howard, R., 2009. Non-pharmacological interventions in theprevention of delirium. Age and Ageing 38, 374–379.
Voyer, P., Cole, M.C., McCusker, J., St-Jacques, S., Laplante, J., 2008.Accuracy of nurse documentation of delirium symptoms in medicalcharts. International Journal of Nursing Practice 14, 165–177.
Wand, A.P.F., 2011. Evaluating the effectiveness of educational inter-ventions to prevent delirium. Australasian Journal on Ageing 30,175–185.
Wand, A.P.F., Thoo, B., Ting, V., Baker, J., Sciuriaga, H., Hunt, G.E., 2013.Identification and rates of delirium in elderly medical inpatients fromdiverse language groups. Geriatric Nursing 34, 355–360.
Watson, Y.I., Arfken, C.L., Birge, S.J., 1993. Clock completion: an objectivescreening test for dementia. Journal of the American GeriatricsSociety 41, 1235–1240.
Wong, D.M., Bruce, J.J., Bruce, D.G., 2005. Quality project to preventdelirium after hip fracture. Australasian Journal on Ageing 24,174–177.
ease cite this article in press as: Wand, A.P.F., et al., A multifaceted educational intervention to prevent delirium in olderpatients: A before and after study. Int. J. Nurs. Stud. (2014), http://dx.doi.org/10.1016/j.ijnurstu.2013.11.005