Embed Size (px)
Citation preview

J A C C : C L I N I C A L E L E C T R O P H Y S I O L O G Y V O L . 4 , N O . 4 , 2 0 1 8
ª 2 0 1 8 B Y T H E AM E R I C A N C O L L E G E O F C A R D I O L O G Y F O UN DA T I O N
P U B L I S H E D B Y E L S E V I E R
PEDIATRIC ARRHYTHMIAS
Life-Threatening Event Risk in ChildrenWith Wolff-Parkinson-White Syndrome
A Multicenter International StudySusan P. Etheridge, MD,a Carolina A. Escudero, MD,b Andrew D. Blaufox, MD,c Ian H. Law, MD,d
Brynn E. Dechert-Crooks, RN, MSN,e Elizabeth A. Stephenson, MD,f Anne M. Dubin, MD,g Scott R. Ceresnak, MD,g
Kara S. Motonaga, MD,g Jonathan R. Skinner, MBCHB, MD,h Luciana D. Marcondes, MD,h James C. Perry, MD,i
Kathryn K. Collins, MD,j Stephen P. Seslar, MD,k Michel Cabrera, MD,l Orhan Uzun, MD,m Bryan C. Cannon, MD,n
Peter F. Aziz, MD,o Peter Kubu�s, MD,p Ronn E. Tanel, MD,q Santiago O. Valdes, MD,r Sara Sami, MD,r
Naomi J. Kertesz, MD,s Jennifer Maldonado, MBA, CCRP,d Christopher Erickson, MD,t Jeremy P. Moore, MD,u
Hiroko Asakai, MD,f LuAnn Mill, RN, BSN,t Mark Abcede, MBA, CCRP,i Zebulon Z. Spector, MD,k Shaji Menon, MD,a
Mark Shwayder, MD,a David J. Bradley, MD,e Mitchell I. Cohen, MD,v Shubhayan Sanatani, MDw
JACC: CLINICAL ELECTROPHYSIOLOGY CME/MOC
Thisarticlehasbeenselectedas themonth’s JACC:ClinicalElectrophysiology
CME/MOCactivity, available onlineatwww.jacc-electrophysiology.org by
selecting the JACC Journals CME/MOC tab.
Accreditation and Designation Statement
The American College of Cardiology Foundation (ACCF) is accredited by
the Accreditation Council for Continuing Medical Education (ACCME) to
provide continuing medical education for physicians.
The ACCF designates this Journal-based CME/MOC activity for a
maximum of 1 AMA PRA Category 1 Credit(s). Physicians should only claim
credit commensurate with the extent of their participation in the activity.
Method of Participation and Receipt of CME/MOC Certificate
To obtain credit for JACC: Clinical Electrophysiology CME/MOC, you must:
1. Be an ACC member or JACC: Clinical Electrophysiology subscriber.
2. Carefully read the CME/MOC-designated article available online and
in this issue of the journal.
3. Answer the post-test questions. At least 2 out of the 3 questions
provided must be answered correctly to obtain CME/MOC credit.
4. Complete a brief evaluation.
ISSN 2405-500X/$36.00
From the aDivision of Cardiology, Department of Pediatrics, Primary ChildrenbDivision of Cardiology, Department of Pediatrics, Stollery Children’s HospitacDivision of Pediatric Cardiology, Department of Pediatrics, Cohen Childre
School of Medicine, New Hyde Park, New York; dDepartment of Pediatric
Hospital, University of Iowa, Iowa City, Iowa; eDivision of Cardiology, Depart
Hospital, University of Michigan, Ann Arbor, Michigan; fLabatt Family Heart
Canada; gDivision of Pediatric Cardiology, Department of Pediatrics, Lucile P
Alto, California; hGreenlane Paediatric and Congenital Cardiac Service, Sta
Auckland, New Zealand; iCardiology Division, Department of Pediatrics, Ra
Diego, San Diego, California; jDivision of Cardiology, Children’s Hospital CkDivision of Pediatric Cardiology, Department of Pediatrics, Seattle Child
Pediatrico William Soler, Havana, Cuba; mDepartment of Paediatric Cardio
United Kingdom; nDepartment of Pediatrics, Division of Pediatric Cardiolog
5. Claim your CME/MOC credit and receive your certificate electronically
by following the instructions given at the conclusion of the activity.
CME/MOC Objective for This Article: Upon completion of this activity, the
learner should be able to: 1) define the clinical features that are associated
with high risk accessory pathways in children; 2) explain the rationale for a
low threshold for performing catheter ablation in children withWPW; and
3) compare the differences between the population of children with a life-
threatening event to children without a previous life-threatening event.
CME/MOC Editor Disclosure: CME/MOC Editor Smit Vasaiwala, MD, has
nothing to declare.
Author Disclosures: Dr. Kubu�s is supported by the Ministry of Health,
Czech Republic (MHCZ-DRO), University Hospital Motol, Prague, Czech
Republic 00064203. All other authors have reported that they have no
relationships relevant to the contents of this paper to disclose.
Medium of Participation: Print (article only); online (article and quiz).
CME/MOC Term of Approval
Issue Date: April 2018
Expiration Date: March 31, 2019
https://doi.org/10.1016/j.jacep.2017.10.009
’s Hospital, University of Utah, Salt Lake City, Utah;
l, University of Alberta, Edmonton, Alberta, Canada;
n’s Medical Center of New York, Hofstra-Northwell
s, Division of Cardiology, Stead Family Children’s
ment of Pediatrics, University of Michigan Children’s
Centre, Hospital for Sick Children, Toronto, Ontario,
ackard Children’s Hospital, Stanford University, Palo
rship Children’s Hospital, University of Auckland,
dy Children’s Hospital, University of California San
olorado, University of Colorado, Aurora, Colorado;
ren’s Hospital, Seattle, Washington; lCardiocentro
logy, University Hospital of Wales, Cardiff, Wales,
y, Mayo Clinic, Rochester, Minnesota; oDivision of

Etheridge et al. J A C C : C L I N I C A L E L E C T R O P H Y S I O L O G Y V O L . 4 , N O . 4 , 2 0 1 8
Life-Threatening Event Risk in Children With WPW Syndrome A P R I L 2 0 1 8 : 4 3 3 – 4 4
434
Life-Threatening Event Risk
in Children WithWolff-Parkinson-White SyndromeA Multicenter International Study
Susan P. Etheridge, MD,a Carolina A. Escudero, MD,b Andrew D. Blaufox, MD,c Ian H. Law, MD,d
Brynn E. Dechert-Crooks, RN, MSN,e Elizabeth A. Stephenson, MD,f Anne M. Dubin, MD,g Scott R. Ceresnak, MD,g
Kara S. Motonaga, MD,g Jonathan R. Skinner, MBCHB, MD,h Luciana D. Marcondes, MD,h James C. Perry, MD,i
Kathryn K. Collins, MD,j Stephen P. Seslar, MD,k Michel Cabrera, MD,l Orhan Uzun, MD,m Bryan C. Cannon, MD,n
Peter F. Aziz, MD,o Peter Kubu�s, MD,p Ronn E. Tanel, MD,q Santiago O. Valdes, MD,r Sara Sami, MD,r
Naomi J. Kertesz, MD,s Jennifer Maldonado, MBA, CCRP,d Christopher Erickson, MD,t Jeremy P. Moore, MD,u
Hiroko Asakai, MD,f LuAnn Mill, RN, BSN,t Mark Abcede, MBA, CCRP,i Zebulon Z. Spector, MD,k Shaji Menon, MD,a
Mark Shwayder, MD,a David J. Bradley, MD,e Mitchell I. Cohen, MD,v Shubhayan Sanatani, MDw
ABSTRACT
Pe
Un
Fra
Ho
atr
UC
Ar
Ch
(M
rel
All
ins
vis
Ma
OBJECTIVES This study sought to characterize risk in children with Wolff-Parkinson-White (WPW) syndrome by
comparing those who had experienced a life-threatening event (LTE) with a control population.
BACKGROUND Children with WPW syndrome are at risk of sudden death.
METHODS This retrospective multicenter pediatric study identified 912 subjects #21 years of age with WPW syndrome,
using electrophysiology (EPS) studies. Case subjects had a history of LTE: sudden death, aborted sudden death, or
atrial fibrillation (shortest pre-excited RR interval in atrial fibrillation [SPERRI] of #250 ms or with hemodynamic
compromise); whereas subjects did not. We compared clinical and EPS data between cases and subjects.
RESULTS Case subjects (n ¼ 96) were older and less likely than subjects (n ¼ 816) to have symptoms or documented
tachycardia. Mean age at LTE was 14.1 � 3.9 years of age. The LTE was the sentinel symptom in 65%, consisting of
rapidly conducted pre-excited atrial fibrillation (49%), aborted sudden death (45%), and sudden death (6%). Three risk
components were considered at EPS: SPERRI, accessory pathway effective refractory period (APERP), and shortest paced
cycle length with pre-excitation during atrial pacing (SPPCL), and all were shorter in cases than in control subjects. In
multivariate analysis, risk factors for LTE included male sex, Ebstein malformation, rapid anterograde conduction (APERP,
SPERRI, or SPPCL#250 ms), multiple pathways, and inducible atrial fibrillation. Of case subjects, 60 of 86 (69%) had$2
EPS risk stratification components performed; 22 of 60 (37%) did not have EPS-determined high-risk characteristics, and
15 of 60 (25%) had neither concerning pathway characteristics nor inducible atrioventricular reciprocating tachycardia.
CONCLUSIONS Young patients may experience LTE from WPW syndrome without prior symptoms or markers of high-
risk on EPS. (J Am Coll Cardiol EP 2018;4:433–44) © 2018 by the American College of Cardiology Foundation.
diatric Cardiology, Cleveland Clinic Foundation, Cleveland, Ohio; pChildren’s Heart Centre, Charles University and Motol
iversity Hospital, Prague, Czech Republic; qDepartment of Pediatrics, Benioff Children’s Hospital, University of California San
ncisco, San Francisco, California; rDivision of Pediatric Cardiology, Texas Children’s Hospital, Baylor College of Medicine,
uston Texas; sNationwide Children’s Hospital, Columbus, Ohio; tDivision of Pediatric Cardiology in the Department of Pedi-
ics, Children’s Hospital and Medical Center, Omaha, Nebraska; uDepartment of Pediatrics, Division of Pediatric Cardiology,
LA Health System, University of California Los Angeles, Los Angeles, California; vPhoenix Children’s Hospital, University of
izona College of Medicine, Phoenix, Arizona; and the wDivision of Cardiology, Department of Pediatrics, British Columbia
ildren’s Hospital, Vancouver, British Columbia, Canada. Dr. Kubu�s is supported by the Ministry of Health, Czech Republic
HCZ-DRO), University Hospital Motol, Prague, Czech Republic 00064203. All other authors have reported that they have no
ationships relevant to the contents of this paper to disclose.
authors attest they are in compliance with human studies committees and animal welfare regulations of the authors’
titutions and Food and Drug Administration guidelines, including patient consent where appropriate. For more information,
it the JACC: Clinical Electrophysiology author instructions page.
nuscript received August 16, 2017; revised manuscript received October 3, 2017, accepted October 12, 2017.

AB BR E V I A T I O N S
AND ACRONYM S
APERP = accessory pathway
effective refractory period
ART = antidromic reciprocating
tachycardia
AVRT = atrioventricular
reciprocating tachycardia
CHD = congenital heart disease
EPS = electrophysiology study
LTE = life-threatening event
ORT = orthodromic
reciprocating tachycardia
SPERRI = shortest pre-excited
RR interval in atrial fibrillation
SPPCL = shortest pre-excited
paced cycle length with atrial
pacing
SVT = supraventricular
tachycardia
WPW = Wolff-Parkinson-
White syndrome
J A C C : C L I N I C A L E L E C T R O P H Y S I O L O G Y V O L . 4 , N O . 4 , 2 0 1 8 Etheridge et al.A P R I L 2 0 1 8 : 4 3 3 – 4 4 Life-Threatening Event Risk in Children With WPW Syndrome
435
S udden death in Wolff-Parkinson-White (WPW)syndrome is a rare but potentially preventableproblem affecting young, otherwise healthy
people. Sudden death is usually a consequence ofatrial fibrillation with rapid conduction over an acces-sory pathway resulting in ventricular fibrillation.Because WPW patients develop atrial fibrillationmore frequently than the general population, animportant question is whether there is a risk of ven-tricular fibrillation should atrial fibrillation occur.Assessing accessory pathway conduction propertiesby using electrophysiology study (EPS) is advocatedas a preventive strategy against sudden death, asnoninvasive risk stratification tools are imperfect(1–4). Inducible atrioventricular re-entrant tachy-cardia (AVRT) or EPS data suggesting a pathwaycapable of rapid anterograde conduction are identi-fied as predictors of malignant arrhythmia (5–8).Because catheter ablation can cure WPW syndromeand eliminate risk (9), the small long-term risk of alife-threatening event (LTE) must be balanced withthe immediate albeit low risk of an ablation.
SEE PAGE 445
The low event rate of WPW syndrome, reducedfurther by catheter ablation, makes risk assessment achallenge. Data investigating possible risk factors forLTE in children with WPW syndrome, however,remain critical. In this study, we compared childrenwith WPW syndrome who had experienced an LTEwith a control population (WPW syndrome withoutLTE) to identify characteristics associated with sud-den death risk.
METHODS
This multicenter, international, retrospective case-control study involved 22 centers from 6 countries(United States, Canada, New Zealand, Cuba,Czech Republic, and Wales [United Kingdom]) soli-cited through the Pediatric and Congenital Electro-physiology Society (PACES). Data collectedencompassed the era of catheter ablation in chil-dren, from January 1990 through June 2016. Allcenters obtained local investigational review boardapproval, and institutional databases were searchedto identify children with WPW syndrome. De-identified data were managed using Research Elec-tronic Data Capture (REDCap), hosted at the Uni-versity of Utah. REDCap is a secure, Web-basedapplication designed to support data capture forresearch (10). All data were reviewed by the datacoordinating center and statistician for appropri-ateness for inclusion.
CASE SUBJECTS. Case subjects were chil-dren with WPW syndrome who had experi-enced an LTE at #21 years of age. An LTE wasdefined as sudden death, aborted suddendeath, or a clinical episode of pre-excitedatrial fibrillation with the shortest pre-excited RR interval (SPERRI) in atrial fibril-lation of #250 ms, regardless of symptoms ordocumented pre-excited atrial fibrillationassociated with hemodynamic compromise,syncope, or seizure, regardless of the SPERRI.Subjects who experienced pre-excited atrialfibrillation without associated hemodynamiccompromise, syncope, or seizure and aSPERRI >250 ms were excluded. Cases ofsudden death were included if a pre-mortemelectrocardiogram (ECG) and/or EPS provingWPW syndrome was available.
CONTROL SUBJECTS. Control subjectswere #21 years of age with WPW syndromewho had not experienced an LTE or clinical
pre-excited atrial fibrillation and had undergone anEPS. For each case subject, 4 age-matched subjects(�24 months of age at EPS or LTE if no EPS was per-formed) and 4 non–age-matched subjects wereselected by each center. Two sets of subjects wereselected to potentially mitigate and investigate in-fluences of age and size on ablation outcomes andrisk. Matched subjects were selected from the sameinstitution when possible or from other participatingcenters. Except for analyses involving age, subjectswere evaluated as a single control group. Congenitalheart disease (CHD) was noted, but cases and subjectswere not matched for this variable.CLINICAL DATA. Demographic data included age atpresentation, EPS information, and last follow-upexamination. Symptoms, documented supraventric-ular tachycardia (SVT), and hemodynamically sig-nificant CHD were noted. Hemodynamicallyinsignificant ventricular and atrial septal defects,ductus arteriosus, mitral valve prolapse, isolated leftsuperior vena cava, and bicuspid aortic valvewithout stenosis or insufficiency were not consid-ered significant CHD. Details of the LTE werecollected, including activity at the time (rest,active but noncompetitive, competitive activity, asdetermined by the contributing center), type ofevent (pre-excited atrial fibrillation, aborted suddendeath or ventricular fibrillation, or sudden death),and outcome (death, full or near full recovery,or recovery with a neurological deficit). All caseswere reviewed by the coordinating center.

TABLE 1 Characteristics of the Study Cohort
Case Subjects(n ¼ 96)
Control Subjects(n ¼ 816) p Value
Age at WPW presentation (yrs) 11.5 � 6.1 9.7 � 5.3* 0.003
Males (%) 78 58 <0.0005
Race (%)
Caucasian 67.7 73.2 NS
African American 9.4 6.5 NS
Native American, Alaskan Native,First Nations
1.0 0.4 NS
Asian (%) 3.1 2.1 NS
Hawaiian/Pacific Islander 1.0 1.7 NS
>1 ethnic group 0 0.9 NS
Symptoms before LTE/EPS (%) 60.0 83.9 <0.0005
Chest pain 3.2 6.5 NS
Syncope 15.1 10.8 NS
Pre-syncope 5.3 5.8 NS
Palpitations 47.4 68.4 <0.0005
Documented SVT (%) 25.5 44.2 0.001
CHD (%) 7.3 3.2 0.042
Follow-up (yrs)
From diagnosis 5.0 � 6.1 4.2 � 4.5 NS
From LTE/EPS 2.3 � 3.6 1.4 � 1.8 <0.0005
Number alive at last follow-up (%) 87 (90.6) 100 (100.0) <0.0005
Death 9 (9) 0 (0)
Values are mean � SD, %, or n (%). *Non–age-matched subjects were used for analysis.
CHD ¼ congenital heart disease; EPS ¼ electrophysiology study; LTE ¼ life-threatening event;NS ¼ not significant; SVT ¼ supraventricular tachycardia; WPW ¼ Wolff-Parkinson-Whitesyndrome.
Etheridge et al. J A C C : C L I N I C A L E L E C T R O P H Y S I O L O G Y V O L . 4 , N O . 4 , 2 0 1 8
Life-Threatening Event Risk in Children With WPW Syndrome A P R I L 2 0 1 8 : 4 3 3 – 4 4
436
ELECTROPHYSIOLOGY STUDIES. By design, an EPSwas performed in all subjects. If case subjects had>1 EPS performed, the earliest study with riskstratification data was included for analysis.EPS data collected included determination of con-duction properties, location of pathway(s), andinduction of tachycardia including orthodromicreciprocating tachycardia (ORT), antidromic recip-rocating tachycardia (ART), atrioventricular nodereentrant tachycardia, atrial flutter, or atrial fibril-lation. We considered risk stratification as per-forming at least one of the following studies:accessory pathway effective refractory period(APERP), shortest paced cycle length with pre-excitation during atrial pacing (SPPCL) or SPERRI.If the atrial effective refractory period (AERP) wasreached before APERP, the AERP was used in placeof APERP. An APERP, SPPCL, or SPERRI valueof #250 ms was considered high-risk. The use ofanesthesia was noted. Data for isoproterenol werereported when available. Ablation success andcomplications were reported.
STATISTICAL ANALYSIS. Frequency tables weregenerated for all categorical variables SPSS version20.0 (IBM Corp., Armonk, New York), with chi-square
or Fisher exact analyses used to detect differencesbetween case and control subjects. Mean � SD werereported for continuous variables. Univariate analysisof variance (ANOVA) was used to compare means forcontinuous variables between cases and subjects.Binomial logistic regression analyses were used topredict risk of LTE (i.e., cases vs. subjects) based onsex and at least one of following variables: APERP,SPERRI, or SPPCL #250 ms; presence of Ebsteinmalformation; inducible atrial fibrillation at EPS; orthe presence of >1 accessory pathway. The EPS-derived data were combined for logistic regressionanalysis because too few subjects had all 3 measure-ments determined. EPS data for univariate andmultivariate analyses were obtained in the baselinestate. Receiver-operating characteristic (ROC) curveswere constructed to determine the sensitivity andspecificity of different cutoff values of APERP,SPERRI, and SPPCL. For some analyses of tachycardiainduction, ORT and ART were combined and desig-nated AVRT. Significance was set at a p valueof #0.05.
RESULTS
DEMOGRAPHIC DATA, ENTIRE COHORT. A total of108 cases and 864 subjects were initially enteredinto the database, but 12 cases were excluded for notmeeting LTE criteria. Thus, a total of 912 subjects (96cases and 816 subjects) were analyzed (the 48 sub-jects age-matched to excluded subjects wereomitted, but the non–age-matched subjects wereretained). The 2 control groups did not differ exceptin age and were combined into a single group for allanalyses except for age. Demographic and clinicaldata are summarized in Table 1. Case subjects weremore likely to be male and were older at presenta-tion than non–age-matched subjects. Case subjectswere less likely to have experienced symptomsbefore the LTE than subjects and were more likely tohave CHD. The most common lesion was Ebsteinmalformation (n ¼ 15), more prevalent in case sub-jects (5.2% vs. 1.2%, respectively; p ¼ 0.004). At lastfollow-up examination, there were 9 deaths, all incase subjects.
CLINICAL DATA, CASE SUBJECTS. Table 2 outlinesthe characteristics of case subjects and LTE details.Mean age at LTE was 14.1 � 3.9 years of age with 3subjects <5 years of age (Table 3). The LTE occurredmost often at rest or with noncompetitive activityand was equally likely to be rapidly conductedpre-excited atrial fibrillation and aborted suddendeath. There were 6 subjects (6%) who presented

TABLE 3 LTE in Children <5 Years of Age
Age Event Details Outcome
0.6 month Aborted suddendeath
Resuscitated cardiac arrestafter weeks of poorfeeding
Seizures, small cerebralhemorrhage. AwaitingEPS on therapy.
0.1 month Aborted suddendeath
Resuscitated cardiac arrest asfirst symptom
EPS at 4.3 yrs with inducibleORT and successfulablation of midseptal AP.
2.4 yrs Ventricularfibrillation
Known WPW patientpresented with ventricularfibrillation whilenoncompliant withamiodarone
EPS at 5.7 yrs inducible ORTand successful ablationof left lateral AP.
AP ¼ accessory pathway; ECG ¼ electrocardiogram; ORT ¼ orthodromic reciprocating tachycardia; otherabbreviations as in Table 1.
TABLE 2 Clinical Characteristics of Case Subjects (N ¼ 96)
Age at LTE (yrs) 14.1 � 3.9 (range 0.4months-21 yrs)
Known WPW 40 (42)
LTE as presenting symptom 62 (65)
LTE diagnosis
Pre-excited atrial fibrillation 47 (49)
Aborted sudden death 43 (45)
Sudden death 6 (6)
Activity at time of LTE
Rest 37 (39)
Active, noncompetitive 33 (34)
Active, competitive 10 (10)
Unknown 16 (17)
Outcome of the LTE
Full/near full recovery 82 (85)
Recovery with neurological injury 5 (5)
Death 9 (9)
Values are mean � SD or n (%).
Abbreviations as in Table 1.
J A C C : C L I N I C A L E L E C T R O P H Y S I O L O G Y V O L . 4 , N O . 4 , 2 0 1 8 Etheridge et al.A P R I L 2 0 1 8 : 4 3 3 – 4 4 Life-Threatening Event Risk in Children With WPW Syndrome
437
with sudden death who had a pre-mortem ECG and/orEPS demonstrate WPW syndrome, and post-mortemevaluation did not reveal an identifiable alternativecause of death. Three case subjects experienced2 LTEs, and 1 had stable pre-excited atrial fibrillationbefore experiencing an LTE. Among case subjects,age <12 years (n ¼ 16) was associated with abortedsudden death as the LTE (88% vs 36%,; p <0.0005)and age $12 years (n ¼ 80) was associated withpre-excited atrial fibrillation as the LTE (56% vs 13%;p ¼ 0.002).
Clinical SPERRI was reported in 46 cases with pre-excited atrial fibrillation as their LTE (1 was classifiedas aborted sudden death due to degeneration toventricular fibrillation). The mean SPERRI was 202 �33 ms (range 150 to 320 ms). Two case subjects hadpre-excited atrial fibrillation and an unknownSPERRI, 1 with recurrent seizures requiring intuba-tion and a second subject with poor perfusion andhypotension. An additional case subject had syncopewhile running and a clinical SPERRI upon presenta-tion of 320 ms.
Sudden death or aborted sudden death was thepresenting symptom in 31 case subjects, and pre-excited atrial fibrillation was the presenting symptomin 31 subjects. There were 38 (40%) of case subjectswho had not complained of previous symptomsbefore the LTE. There were 56 case subjects (58%)who were not known to have WPW syndrome beforethe LTE. Of these, 32 (33%) were symptom free. Theremaining 24 reported prior symptoms includingdocumented SVT (n ¼ 1), palpitations alone (n ¼ 11),palpitations and syncope (n ¼ 5), palpitations andnear syncope (n ¼ 4), and syncope alone (n ¼ 3).
Full or near full recovery was likely in case subjectsafter LTE. Five subjects recovered with a neurologicaldeficit; of these, 1 subject had acute kidney failure,and 1 had right leg compartment syndrome afterextracorporeal membrane oxygenation support. TheLTE was sudden death in 6 cases. Three additionalcases were removed from life support due to devas-tating neurological injury. One death occurred in achild who became a heart transplant donor, and WPWsyndrome was diagnosed in the recipient subsequentto transplantation.
ELECTROPHYSIOLOGY STUDY DATA, ENTIRE
COHORT. Table 4 outlines EPS data and ablationoutcomes. EPS data were available in all subjects and91% of cases. EPS data were not available in 8 casesubjects, 7 of whom died without a previous EPS, andan infant who had yet to undergo EPS (Table 3). In 4case subjects, EPS data were from a procedure
performed before LTE. One case subject had EPSperformed at a nonparticipating institution, and datawere not available. One case subject was lost tofollow-up after an acutely successful ablation. Hepresented in ventricular fibrillation with unsuccessfulresuscitation. He had mild Ebstein malformation withtrivial tricuspid regurgitation; autopsy findings wereotherwise unremarkable. In the remaining 83 casesubjects, EPS data were from a procedure after theLTE, including EPS and ablation data from a proced-ure performed in a recipient of a heart transplantedfrom a donor with WPW syndrome.
Tachycard ia induct ion . Table 4 outlines tachycar-dias induced. Case subjects were less likely to haveORT but more likely to have ART, atrial flutter, andatrial fibrillation.

TABLE 4 Baseline EPS Data and Ablation Outcomes
Case Subjects(n ¼ 96)
Control Subjects(n ¼ 816) p Value
Age at EPS (yrs) 14.3 � 3.6 13.4 � 3.9* 0.042
EPS performed 87 (91) 816 (100) NS
General anesthesia used (%) 86 87 NS
SVT induced (%) 82 74 NS
AVRT 56 64 NS
ORT 52 63 0.035
ART 6 1 0.001
Atrial fibrillation 52 27 <0.0005
Atrial flutter 5 1 0.038
AVNRT 2.3 0.7 NS
Risk stratification undertaken 77 (89) 766 (94) 0.056
APERP (ms) 271 � 50 309 � 55 <0.0005
SPERRI (ms) 247 � 61 315 � 77 <0.0005
SPPCL (ms) 279 � 89 315 � 74 0.001
APERP #250 ms (%) 41 12 <0.0005
SPERRI #250 ms (%) 64 18 <0.0005
SPPCL #250 ms (%) 46 21 <0.0005
$1 functional measurement #250 ms 48 (62) 186 (24.5) <0.0005
>1 accessory pathway (%) 18.4 5.2 <0.0005
Ablation performed 85 (98) 789 (97) NS
Ablation successful 71 (82) 353 (93) 0.001
Procedure complications 8 (9) 23 (3) 0.002
Values are mean � SD, n (%), or %. *Non–age-matched controls were included for analysis.
APERP ¼ accessory pathway effective refractory period; ART ¼ antidromic reciprocating tachycardia; AVNRT ¼atrioventricular node reentry tachycardia; AVRT ¼ atrioventricular reciprocating tachycardia; SPERRI ¼ shortestpre-excited RR interval in atrial fibrillation; SPPCL ¼ shortest paced cycle length with pre-excitation during atrialpacing; other abbreviations as in Table 1.
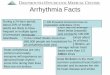
FIGURE 1 EPS-Der
Percentage of case a
(value #250 ms) is s
APERP ¼ accessory p
SPERRI ¼ shortest p
cycle length with pr
Etheridge et al. J A C C : C L I N I C A L E L E C T R O P H Y S I O L O G Y V O L . 4 , N O . 4 , 2 0 1 8
Life-Threatening Event Risk in Children With WPW Syndrome A P R I L 2 0 1 8 : 4 3 3 – 4 4
438
Accessory pathway anterograde funct ionalpropert ies . Risk stratification, defined as the deter-mination of accessory pathway anterograde func-tional property (APERP, SPERRI, or SPPCL) during
ived Accessory Pathway Characteristics
nd control subjects with pathway characteristics suggesting high-risk
hown. *p #0.05. AP ¼ accessory pathway; ms ¼ milliseconds;
athway effective refractory period; EPS ¼ electrophysiology study;
re-excited RR interval in atrial fibrillation; SPPCL ¼ shortest paced
e-excitation during atrial pacing.
EPS, was undertaken in 89% of case and 94% ofcontrol subjects. There were 60 of 87 case subjects(69%) who underwent an EPS with $2 accessorypathway functional properties determined. Casesubjects had significantly shorter APERP, SPERRI, andSPPCL values and were more likely to have multipleaccessory pathways (Table 4, Figure 1). Case subjectswere more likely to have at least 1 functional propertyconsidered high-risk. There were values for EPS-derived SPERRI reported in 39 (45%) of case subjects(mean 247 � 61 ms). However, in 14 of 39 (36%), theSPERRI was >250 ms. In 13 of these subjects, theprocedure was performed using general anesthesia;in 1 subject, conscious sedation was used. This is notdifferent from the group where the SPERRIwas #250 ms, 18 had general anesthesia and 7 hadconscious sedation (p ¼ 0.20). Among 60 case sub-jects who had risk stratification that included $2accessory pathway characteristics, 22 of 60 (37%) didnot have concerning pathway characteristics, and 15of 60 (25%) had neither concerning pathway charac-teristics nor inducible AVRT. Figure 1 shows the pro-portion with pathway functional characteristicsconsidered high-risk (APERP, SPERRI, or SPPCLof #250 ms) and with multiple accessory pathways.Figure 2 shows the distribution of EPS data in casesand subjects, and although there is overlap betweencase and subjects, a low-risk cutoff can be noted. Nocase subject had a SPERRI >370 ms or an APERP >400ms. One case subject had a SPPCL >440 ms. Figure 3demonstrates ROC curves for the risk stratificationmaneuvers and demonstrates no significant differ-ences between the areas under the curve for each riskstratification maneuver.
When EPS data from case subjects with pre-excitedatrial fibrillation were compared to those of subjectswith aborted sudden death, there were no significantdifferences in mean APERP, SPERRI, or SPPCL valuesand no differences in the proportion with any of thesevalues #250 ms or the presence of multiple accessorypathways.
I soproterenol . EPS data during isoproterenol infu-sion were not available for the entire cohort (Table 5).Isoproterenol therapy resulted in a shortening ofpathway functional properties in both groups,although case subjects continued to have signifi-cantly shorter SPERRI and SPPCL. Only 3 case subjectshad all 3 functional characteristic studies performedwhile they were receiving isoproterenol therapy, toofew to make meaningful conclusions.
PREDICTORS OF LIFE-THREATENING EVENTS. Factorsassociated with LTE were identified by univariateanalysis (Table 6), including APERP, SPERRI, and

FIGURE 2 Distribution of EPS-Derived Data
Box-and-whisker plots of APERP, SPERRI, and SPPCL in case and control subjects. Shown are mean values (solid line), and the SDs (thicker
solid lines), and all values for data obtained, case subjects (red), and subjects (blue). The dotted line marks 250 ms. There were 2 outliers in
which SPERRI was >600 ms (2 subjects) and 4 outliers (1 case and 3 subjects) with SPPCL >600 ms, these are not represented in the graphs.
Abbreviations as in Figure 1.
J A C C : C L I N I C A L E L E C T R O P H Y S I O L O G Y V O L . 4 , N O . 4 , 2 0 1 8 Etheridge et al.A P R I L 2 0 1 8 : 4 3 3 – 4 4 Life-Threatening Event Risk in Children With WPW Syndrome
439
SPPCL #250 ms; presence of Ebstein malformation;inducible atrial fibrillation at EPS; and presence ofmultiple pathways. Logistic regression was statisti-cally significant (chi-square: 5 ¼ 82.94; df ¼ 5; p <
0.0005). Table 7 outlines the features that wereindependently associated with increased odds ofhaving an LTE.
Of those who underwent EPS, ablation wasattempted in 98% of cases and 97% of subjects. Suc-cess was lower in case subjects (82% vs. 93%,respectively; p ¼ 0.001). Table 8 outlines the pathwaylocations. More complications were noted in casesubjects (Table 4), including atrioventricular block(2.3% vs. 0.2%, respectively; p ¼ 0.048). There wereno deaths resulting from EPS or ablation.
DISCUSSION
This multicenter, international study is the largest tohave addressed pediatric WPW syndrome and hasincreased our understanding of risk. Although thechildren were treated in the contemporary era ofcatheter ablation, sudden death still occurred. An LTEwas the sentinel event in 65%, with sudden death oraborted sudden death sentinel in nearly 1 of 3 sub-jects. Importantly, case subjects were less likely thansubjects to have experienced previous symptoms.
In this study, we sought to better characterize LTEsin children. Events occurred most often in adoles-cent males who were not engaged in competition.Although competitive athletics are considered to

FIGURE 3 ROC Curves
(A) APERP, AUC ¼ 0.702 (95% CI: 0.633 to 0.770; p < 0.0005), and#250 ms has a sensitivity of 41% and specificity of 88% in differentiating
between cases and subjects. (B)SPERRI, AUC¼0.768 (95%CI: 0.679 to0.858; p<0.0005), and#250mshas a sensitivity of 64%and specificity
of 82% in differentiating between cases and subjects. (C) SPPCL, AUC ¼ 0.703 (95% CI: 0.629 to 0.778; p<0.0005), and #250 ms has a
sensitivity of 46%and specificity of 79% indifferentiating between cases and subjects. Therewereno significant differences inAUCamongAPERP,
SPERRI, and SPPCL. AUC ¼ area under the curve; ROC ¼ receiver operating characteristic; other abbreviations as in Figure 1.
Etheridge et al. J A C C : C L I N I C A L E L E C T R O P H Y S I O L O G Y V O L . 4 , N O . 4 , 2 0 1 8
Life-Threatening Event Risk in Children With WPW Syndrome A P R I L 2 0 1 8 : 4 3 3 – 4 4
440
increase risk (11–14), sports restriction would not haveprevented LTEs in the 73% of our case subjects whoseevents did not occur with competition. Our data areconsistent with previous series exploring suddendeath in the young, where most events occurredduring rest or sleep (15–17). The 10% of eventsoccurring with sports, however, remains dispropor-tionately high when one considers the percentage oftime engaged in sports compared with time spent atrest and in noncompetitive activities. Thus, our data
do not support unrestricted sports participation inpatients with WPW syndrome but demonstrate thatsports restriction does not keep children safe.
Many studies have assessed pacing maneuvers forrisk stratification. A prospective study found shorterAPERP and degeneration into atrial fibrillation afterAVRT were associated with development of malig-nant arrhythmias (9). Other studies have proposedthat SPERRI best predicts risk, as patients with ven-tricular fibrillation had a SPERRI #250 ms (7). Our

TABLE 5 EPS Data for Isoproterenol
Cases Subjects p Value
Risk stratification on isoproterenolperformed
18/96 (19%) 201/816 (25%) NS
APERP, ms 249 � 54 265 � 40 NS
SPERRI, ms 237 � 47 284 � 44 0.009
SPPCL, ms 205 � 74 259 � 51 0.001
APERP #250 ms (%) 71 (10/14) 43 (63/148) 0.05
SPERRI #250 ms (%) 56 (5/9) 26 (9/35) NS
SPPCL #250 ms (%) 91 (10/11) 58 (86/149) 0.05
$1 functional measurement #250 ms (%) 78 (14/18) 59 (119/201) NS
Values are n/N (%), mean � SD, or % (n/N).
Abbreviations as in Tables 1 and 4.
TABLE 6 Factors Associated With LTE: Univariate Analysis
Odds Ratio(95% CI) p Value
APERP, #250 ms 5.32 (3.14–9.01) <0.0001
SPERRI, #250 ms 8.28 (3.89–17.62) <0.0001
SPPCL, #250 ms 3.27 (1.83–5.83) <0.0001
>1 AP 4.11 (2.19–7.69) <0.0001
At least 1 functionalcharacteristic #250 ms
5.10 (3.12–8.31) <0.0001
Males 2.58 (1.56–4.26) 0.0002
CHD 2.39 (1.01–5.67) 0.0478
Ebstein malformationof the tricuspid valve
4.43 (1.48–13.24) 0.0077
Symptomatic status 0.29 (0.18–0.45) <0.0001
Inducible ORT 0.63 (0.40–0.97) 0.0366
Inducible ART 5.47 (1.79–16.70) 0.0029
Inducible atrial flutter 3.88 (1.19–12.66) 0.0244
Inducible atrial fibrillation 2.96 (1.89–4.63) <0.0001
Isoproterenol APERP #250 ms 3.37 (1.01–11.25) 0.0479
Isoproterenol SPERRI #250 ms 3.61 (0.79–16.47) 0.0973
Isoproterenol SPPCL #250 ms 7.33 (0.91–58.71) 0.0607
Isoproterenol at least 1 functionalcharacteristic #250 ms
2.38 (0.76–7.50) 0.1378
CI ¼ confidence interval; other abbreviations as in Tables 1, 3, and 4.
J A C C : C L I N I C A L E L E C T R O P H Y S I O L O G Y V O L . 4 , N O . 4 , 2 0 1 8 Etheridge et al.A P R I L 2 0 1 8 : 4 3 3 – 4 4 Life-Threatening Event Risk in Children With WPW Syndrome
441
data suggest that substantial risk is present evenwithout evidence of rapid anterograde pathway con-duction at EPS, as commonly defined. Instead, thecutoff value at EPS identified in this cohort washigher: no case subject had an APERP >400 ms or aSPERRI >370 ms.
Assessing each EPS-determined risk factor is notalways possible. If AERP is reached before APERP, thetrue APERP cannot be determined. Assessment ofSPERRI requires induction of atrial fibrillation, whichis not always possible, although SPCCL may be usedas a surrogate. Atrial fibrillation was induced, and aSPERRI of >250 ms was reported in 36% of case sub-jects and in 82% of subjects. This is in contrast to astudy where symptomatic children with WPW syn-drome, syncope and atrial fibrillation had aSPERRI <220 ms (18). Although an EPS that includedall 3 functional characteristics was not always per-formed, 60 case subjects had at least 2 characteristicsmeasured. Of these, 37% would have been classifiedas low-risk if functional characteristics alone wereused. SVT induction at EPS is also associated withincreased risk (19,20). In 25% of case subjects who hada more complete EPS performed, there were neitherconcerning pathway characteristics nor inducibleAVRT. Thus, had EPS been undertaken solely for riskstratification, these children would not have had aconventional indication for ablation. These datasuggest that EPS-derived risk factors developed inadult patients may not be applicable to children.
Historically, decisions about patient managementwere based on the distinction between asymptomaticand symptomatic patients. This approach has beencalled into question. In >2,000 patients with WPWsyndrome, symptomatic patients were more likely tohave had an ablation than asymptomatic patients (9).However, except for symptoms, there were no dif-ferences in clinical or EPS characteristics. Presentdata confirm the fact that asymptomatic WPW syn-drome is not without risk, and although malignantarrhythmias correlate better with EPS-derived riskstratification data than with symptoms, EPS is animperfect predictor, and a low threshold for ablationshould be considered.
In the seminal 1979 series (7), the only asymp-tomatic WPW patients who presented with ventricu-lar fibrillation were children. The lack of symptoms inchildren may be a lack of recognition of symptoms,failure to report them, or an insufficient period overwhich to develop them; an asymptomatic child maybe a pre-symptomatic child. We often strive to treatchildren in the pre-symptomatic phase of a disease,most crucially when the first symptom may be suddendeath.
Serious complications from catheter ablation arerare but are not uniform across childhood (21–23).Ablation success rates in very young children may besimilar to those in older, larger patients, but rates ofadverse events may be higher, and ablation shouldnot be the routine approach to the smallest patients(24). In addition to procedural complications, theremay be potential for lesions that are larger thanintended or lesion growth over time in these patients(23–25). The small but potentially life-long risk inWPW syndrome must be balanced with the slight butimmediate risk of ablation.
In the present report, most EPS were performedwith subjects under general anesthesia, common inpediatric EPS (26). Initial high-risk criteria werederived from procedures without general anesthesia,

TABLE 7 Predictors of Life-Threatening Events on
Multivariate Analysis
Odds Ratio(95% CI) p Value
Male 2.35 (1.28–4.33) 0.006
APERP, SPERRI, and SPPCL #250 ms 3.85 (2.29–6.45) <0.0005
Presence of Ebstein malformation 4.10 (1.10–15.27) 0.035
Inducible atrial fibrillation at EPS 2.85 (1.70–4.76) <0.0005
>1 AP 3.83 (1.86–7.90) <0.0005
Abbreviations as in Tables 1 and 4.
Etheridge et al. J A C C : C L I N I C A L E L E C T R O P H Y S I O L O G Y V O L . 4 , N O . 4 , 2 0 1 8
Life-Threatening Event Risk in Children With WPW Syndrome A P R I L 2 0 1 8 : 4 3 3 – 4 4
442
which is known to affect pathway conduction anddecrease SVT induction (7,14,27). General anesthesiamay limit comparison with historical data and limitoptimal EPS risk stratification. The role of isoproter-enol therapy during risk stratification is not clearlydefined. Isoproterenol has been shown to increase thenumber of subjects meeting risk criteria for ablation(28) and may decrease the specificity of the EPS (29).Data for isoproterenol therapy were available in asmall proportion of our subjects. Similar to previousreports (30), pathway functional properties shortenedin case and control groups, increasing the numberwith pathway characteristics suggesting high-risk. Inorder to prevent LTE, we may need to consider usingisoproterenol and/or performing studies withoutgeneral anesthesia to improve risk assessment, evenat the risk of decreasing specificity.
When case and control patients were comparedusing multivariate analysis, Ebstein malformationwas independently associated with risk. Many pa-tients with Ebstein malformation have WPW
TABLE 8 Accessory Pathway Locations
Case Subjects(n ¼ 87)
Control Subjects(n ¼ 816) p Value
Ablation attempted 85 (98) 789 (97) NS
Left lateral (%) 33.3 25.9 NS
Left posterolateral (%) 10.3 8.9 NS
Left anterolateral (%) 11.5 4.9 0.012
Left posterior (%) 8.0 6.7 NS
Right posterior (%) 4.6 6.2 NS
Left posteroseptal (%) 8.0 5.8 NS
Right posteroseptal (%) 24.1 19.9 NS
Midseptal (%) 4.6 5.1 NS
Anteroseptal (%) 4.6 6.3 NS
Right anterior (%) 0 4.1 NS
Right anterolateral (%) 5.7 3.7 NS
Right posterolateral (%) 3.4 2.7 NS
Right lateral (%) 1.1 5.7 NS
>1 AP (%) 18.4 5.2 <0.0005
Values are n (%) or %.
Abbreviations as in Table 3.
syndrome and, not uncommonly, multiple pathways(31). The annual hazard rate for death, highest in thefirst year of life, persists throughout life withcontinuing attrition in part due to sudden death (32).Although procedures may be difficult, patients withEbstein malformation improve after ablation (33,34).
Ablation was undertaken in 96% of subjects andwas less successful in case subjects who also experi-enced increased complications. Multiple pathwaysand a higher proportion with Ebstein malformationmay have contributed to this lower success. Theincreased complications may be related to moreaggressive ablation attempts in this high-risk popu-lation, coupled with a possible selection bias in thecontrol group. This study provides data for proce-dural success and risk in the control population.Comparable to previous pediatric ablation data, suc-cess rates were high, complications rare, and therewere no deaths (35,36).
STUDY LIMITATIONS. This is a retrospective studywith inherent limitations. There was no uniformclinical or EPS evaluation, and very few subjects hadan EPS that included all 3 functional characteristics.There are limited data for noninvasive testing, andthis study is not powered to outline a noninvasivestrategy for risk stratification. There are strategiesusing pharmacologic testing for risk stratification(37–39), that were not evaluated here. For controlsubjects, we used children with available EPS data.One cannot conclude that this population is neces-sarily low risk but is only representative of thepopulation who undergo an EPS, and we cannotknow if these children would have gone on toexperience an LTE without ablation. We cannot becertain that the 2 infants presenting with abortedsudden death experienced ventricular fibrillationversus a prolonged episode of unrecognized SVT.Operator variability in arrhythmia induction mayhave contributed to the lack of SVT induction andSPERRI data. One could speculate that, after an LTE,as an ablation was indicated, and a less rigorous EPSrisk assessment was performed. Limited EPS data forisoproterenol therapy allow for only limited conclu-sions. The significant differences in ablation out-comes and complications between control and casesubjects may reflect selection bias, although out-comes are similar to data reported in large pediatricablation series (23,35,40).
CONCLUSIONS
This large contemporary study of children with WPWsyndrome identified 96 children with an LTE, many

PERSPECTIVES
COMPETENCY IN MEDICAL KNOWLEDGE: In children with
WPW syndrome, an LTE can be the first symptom, and risk
stratification using clinical and EPS-derived data are imperfect
and fail to identify all those at risk.
TRANSLATIONAL OUTLOOK: A prospective study of children
with WPW syndrome and the WPW syndrome pattern on ECG is
needed to better assess the burden of sudden death and the risk
in children with WPW syndrome where a catheter ablation is
required.
J A C C : C L I N I C A L E L E C T R O P H Y S I O L O G Y V O L . 4 , N O . 4 , 2 0 1 8 Etheridge et al.A P R I L 2 0 1 8 : 4 3 3 – 4 4 Life-Threatening Event Risk in Children With WPW Syndrome
443
without previous symptoms. Although most wouldhave been identified as high-risk, a third would havebeen missed. Male sex, Ebstein malformation,inducible atrial fibrillation, and conventional EPSmeasurements of risk were independently associatedwith LTE. Although the lifetime risk of sudden deathin WPW syndrome is low, it is “front loaded” in theyoung (41). Indications to perform a catheter ablationare varied and not entirely based on risk. Occupationchoices, insurability, and the psychological impact ofhaving WPW syndrome may influence this decision.Because EPS is an imperfect predictor and the risk ofan ablation is low, once an invasive EPS is performed,moving forward to a catheter ablation seems appro-priate. We advocate a low threshold for catheterablation to cure WPW syndrome in children aftercareful consideration of age and size-based risks.
ACKNOWLEDGMENTS The authors thank theFischerkeller Rock-for-the-Heart Foundation fortheir support and interest in this project and theirongoing support of research in children with WPWsyndrome. They also thank the Pediatric andCongenital Electrophysiology Society, without which
the research team would not have met, organized, orcollaborated.
ADDRESS FOR CORRESPONDENCE: Dr. Susan P.Etheridge, University of Utah and Primary Children’sHospital, Pediatrics, 81 North Mario Capecchi Drive,Salt Lake City, Utah 84113. E-mail: [email protected].
RE F E RENCE S
1. Kiger ME, McCanta AC, Tong S, Schaffer M,Runciman M, Collins KK. Intermittent versus persis-tent Wolff-Parkinson-White syndrome in children:electrophysiologic properties and clinical outcomes.Pacing Clin Electrophysiol 2016;39:14–20.
2. Pediatric, Congenital Electrophysiology S, HeartRhythm S, et al. PACES/HRS expert consensusstatement on the management of the asymp-tomatic young patient with a Wolff-Parkinson-White (WPW, ventricular preexcitation)electrocardiographic pattern: developed in part-nership between the Pediatric and CongenitalElectrophysiology Society (PACES) and the HeartRhythm Society (HRS). Endorsed by the governingbodies of PACES, HRS, the American College ofCardiology Foundation (ACCF), the AmericanHeart Association (AHA), the American Academyof Pediatrics (AAP), and the Canadian HeartRhythm Society (CHRS). Heart Rhythm 2012;9:1006–24.
3. Sharma AD, Yee R, Guiraudon G, Klein GJ.Sensitivity and specificity of invasive and nonin-vasive testing for risk of sudden death in Wolff-Parkinson-White syndrome. J Am Coll Cardiol1987;10:373–81.
4. Dalili M, Vahidshahi K, Aarabi-Moghaddam MY, Rao JY, Brugada P. Exercisetesting in children with Wolff-Parkinson-Whitesyndrome: what is its value? Pediatr Cardiol2014;35:1142–6.
5. Bromberg BI, Lindsay BD, Cain ME, Cox JL.Impact of clinical history and electrophysiologiccharacterization of accessory pathways on man-agement strategies to reduce sudden death
among children with Wolff-Parkinson-White syn-drome. J Am Coll Cardiol 1996;27:690–5.
6. Milstein S, Sharma AD, Klein GJ. Electrophysi-ologic profile of asymptomatic Wolff-Parkinson-White pattern. Am J Cardiol 1986;57:1097–100.
7. Klein GJ, Bashore TM, Sellers TD, Pritchett EL,Smith WM, Gallagher JJ. Ventricular fibrillation inthe Wolff-Parkinson-White syndrome. N Engl JMed 1979;301:1080–5.
8. Klein GJ, Prystowsky EN, Yee R, Sharma AD,Laupacis A. Asymptomatic Wolff-Parkinson-White.Should we intervene? Circulation 1989;80:1902–5.
9. Pappone C, Vicedomini G, Manguso F, et al.Wolff-Parkinson-White syndrome in the era ofcatheter ablation: insights from a registry study of2169 patients. Circulation 2014;130:811–9.
10. Harris PA, Taylor R, Thielke R, Payne J,Gonzalez N, Conde JG. Research electronic datacapture (REDCap)—a metadata-driven methodol-ogy and workflow process for providing trans-lational research informatics support. J BiomedInform 2009;42:377–81.
11. Heidbuchel H, Corrado D, Biffi A, et al. Rec-ommendations for participation in leisure-timephysical activity and competitive sports of pa-tients with arrhythmias and potentially arrhyth-mogenic conditions. Part II: ventriculararrhythmias, channelopathies and implantabledefibrillators. Eur J Cardiovasc Prev Rehabil 2006;13:676–86.
12. Maron BJ, Doerer JJ, Haas TS, Tierney DM,Mueller FO. Sudden deaths in young competitive
athletes: analysis of 1866 deaths in the UnitedStates, 1980-2006. Circulation 2009;119:1085–92.
13. Wiedermann CJ, Becker AE, Hopferwieser T,Muhlberger V, Knapp E. Sudden death in a youngcompetitive athlete with Wolff-Parkinson-Whitesyndrome. Eur Heart J 1987;8:651–5.
14. Timmermans C, Smeets JL, Rodriguez LM,Vrouchos G, van den Dool A, Wellens HJ. Abortedsudden death in the Wolff-Parkinson-White syn-drome. Am J Cardiol 1995;76:492–4.
15. Bagnall RD, Weintraub RG, Ingles J, et al.A prospective study of sudden cardiac deathamong children and young adults. N Engl J Med2016;374:2441–52.
16. Mellor G, Raju H, de Noronha SV, et al. Clinicalcharacteristics and circumstances of death in thesudden arrhythmic death syndrome. Circ ArrhythmElectrophysiol 2014;7:1078–83.
17. Finocchiaro G, Papadakis M, Behr ER,Sharma S, Sheppard M. Sudden cardiac death inpre-excitation and Wolff-Parkinson-White: de-mographic and clinical features. J Am Coll Cardiol2017;69:1644–5.
18. Paul T, Guccione P, Garson A Jr. Relation ofsyncope in young patients with Wolff-Parkinson-White syndrome to rapid ventricular responseduring atrial fibrillation. Am J Cardiol 1990;65:318–21.
19. Pappone C, Santinelli V, Rosanio S, et al.Usefulness of invasive electrophysiologic testingto stratify the risk of arrhythmic events inasymptomatic patients with Wolff-Parkinson-White pattern: results from a large prospective

Etheridge et al. J A C C : C L I N I C A L E L E C T R O P H Y S I O L O G Y V O L . 4 , N O . 4 , 2 0 1 8
Life-Threatening Event Risk in Children With WPW Syndrome A P R I L 2 0 1 8 : 4 3 3 – 4 4
444
long-term follow-up study. J Am Coll Cardiol2003;41:239–44.
20. Wellens HJ. Should catheter ablation beperformed in asymptomatic patients withWolff-Parkinson-White syndrome? When toperform catheter ablation in asymptomaticpatients with a Wolff-Parkinson-White electro-cardiogram. Circulation 2005;112:2201–7; dis-cussion, 2216.
21. Schaeffer B, Hoffmann BA, Meyer C, et al.Characterization, mapping, and ablation of com-plex atrial tachycardia: initial experience with anovel method of ultra high-density 3D mapping.J Cardiovasc Electrophysiol 2016;27:1139–50.
22. Van Hare GF, Javitz H, Carmelli D, et al.Prospective assessment after pediatric cardiacablation: recurrence at 1 year after initiallysuccessful ablation of supraventricular tachy-cardia. Heart Rhythm 2004;1:188–96.
23. Kugler JD, Danford DA, Deal BJ, et al. Radio-frequency catheter ablation for tachyarrhythmiasin children and adolescents. The Pediatric Elec-trophysiology Society. N Engl J Med 1994;330:1481–7.
24. Blaufox AD, Felix GL, Saul JP, Pediatric Cath-eter Ablation Registry. Radiofrequency catheterablation in infants </ ¼ 18 months old: when is itdone and how do they fare?: short-term data fromthe pediatric ablation registry. Circulation 2001;104:2803–8.
25. Saul JP, Hulse JE, Papagiannis J, Van Praagh R,Walsh EP. Late enlargement of radiofrequencylesions in infant lambs. Implications for ablationprocedures in small children. Circulation 1994;90:492–9.
26. Pecht B, Maginot KR, Boramanand NK,Perry JC. Techniques to avoid atrioventricularblock during radiofrequency catheterablation of septal tachycardia substrates inyoung patients. J Invert Card Electrophysiol2002;7:83–8.
27. Montoya PT, Brugada P, Smeets J, et al. Ven-tricular fibrillation in the Wolff-Parkinson-Whitesyndrome. Eur Heart J 1991;12:144–50.
28. Moore JP, Kannankeril PJ, Fish FA. Isoproterenoladministration during general anesthesia for theevaluationof childrenwith ventricular preexcitation.Circ Arrhythm Electrophysiol 2011;4:73–8.
29. Szabo TS, Klein GJ, Sharma AD, Yee R,Milstein S. Usefulness of isoproterenol duringatrial fibrillation in evaluation of asymptomaticWolff-Parkinson-White pattern. Am J Cardiol1989;63:187–92.
30. Kubus P, Vit P, Gebauer RA, Materna O,Janousek J. Electrophysiologic profile and resultsof invasive risk stratification in asymptomaticchildren and adolescents with the Wolff-Parkinson-White electrocardiographic pattern.Circ Arrhythm Electrophysiol 2014;7:218–23.
31. Zachariah JP, Walsh EP, Triedman JK, et al.Multiple accessory pathways in the young: theimpact of structural heart disease. Am Heart J2013;165:87–92.
32. Celermajer DS, Bull C, Till JA, et al. Ebstein’sanomaly: presentation and outcome from fetus toadult. J Am Coll Cardiol 1994;23:170–6.
33. Pressley JC, Wharton JM, Tang AS,Lowe JE, Gallagher JJ, Prystowsky EN. Effectof Ebstein’s anomaly on short- and long-termoutcome of surgically treated patients withWolff-Parkinson-White syndrome. Circulation1992;86:1147–55.
34. Walsh EP. Interventional electrophysiology inpatients with congenital heart disease. Circulation2007;115:3224–34.
35. Kugler JD, Danford DA, Houston KA, Felix G.Pediatric Radiofrequency Ablation Registry of thePediatric Radiofrequency Ablation Registry ofthe Pediatric Electrophysiology S. Pediatric radio-frequency catheter ablation registry success,fluoroscopy time, and complication rate for sup-raventricular tachycardia: comparison of early and
recent eras. J Cardiovasc Electrophysiol 2002;13:336–41.
36. Van Hare GF, Javitz H, Carmelli D, et al. Pro-spective assessment after pediatric cardiac abla-tion: demographics, medical profiles, and initialoutcomes. J Cardiovasc Electrophysiol 2004;15:759–70.
37. Gaita F, Giustetto C, Riccardi R, Mangiardi L,Brusca A. Stress and pharmacologic tests asmethods to identify patients with Wolff-Parkinson-White syndrome at risk of suddendeath. Am J Cardiol 1989;64:487–90.
38. Chimienti M, Moizi M, Klersy C, Guasti L,Salerno JA. A modified ajmaline test for predictionof the effective refractory period of the accessorypathway in the Wolff-Parkinson-White syndrome.Am J Cardiol 1987;59:164–5.
39. Wellens HJ, Bar FW, Gorgels AP, Vanagt EJ.Use of ajmaline in patients with the Wolff-Parkinson-White syndrome to disclose short re-fractory period of the accessory pathway. Am JCardiol 1980;45:130–3.
40. Van Hare GF, Lesh MD, Stanger P. Radio-frequency catheter ablation of supraventriculararrhythmias in patients with congenital heart dis-ease: results and technical considerations. J AmColl Cardiol 1993;22:883–90.
41. Klein GJ, Gula LJ, Krahn AD, Skanes AC, Yee R.WPW pattern in the asymptomatic individual: hasanything changed? Circ Arrhythm Electrophysiol2009;2:97–9.
KEY WORDS pediatrics, sudden death,Wolff-Parkinson-White syndrome
Go to http://www.acc.org/jacc-journals-cme to takethe CME/MOC quiz forthis article.