Embed Size (px)
Citation preview

Vol. 41 No. 1 January 2011 Journal of Pain and Symptom Management 57
Original Article
A Measure of Palliative Carein Nursing HomesSarah Thompson, PhD, RN, FAAN, Marjorie Bott, PhD, RN, Diane Boyle, PhD, RN,Byron Gajewski, PhD, and Virginia P. Tilden, DNSc, RN, FAANUniversity of Nebraska Medical Center College of Nursing (S.T., V.P.T.), Omaha, Nebraska; and
University of Kansas School of Nursing (M.B., D.B., B.G.) and School of Medicine (B.G.), Kansas
City, Kansas, USA
Abstract
Context. Efforts to improve care for nursing home residents stand to beenhanced by measures to assess the degree to which staff provide palliative care.As the incidence of death in nursing homes increases with the aging population,the gap in measurement must be addressed. To that end, we report thedevelopment and psychometric testing of a nursing home palliative care survey.
Objectives. The purpose of this study was to evaluate the psychometricproperties of the Palliative Care Survey (PCS) for use in nursing homes.
Methods. Psychometric evaluation of the instrument was completed in twophases. Phase 1 focused on individual item analyses and subsequent revision ordeletion of items, and Phase 2 evaluated evidence for reliability and validity. Phase1 included 26 nursing homes and staff (n¼ 717), and Phase 2 included 85 nursinghomes and staff (n¼ 2779). Data were analyzed using item-total correlations,Cronbach’s alpha, confirmatory factor analysis, and analysis of variance.
Results. Support was obtained for a 51-item PCS made up of two constructs,Palliative Care Practice and Palliative Care Knowledge.
Conclusion. The PCS measures the extent to which the nursing home staffengage in palliative care practices and have knowledge consistent with goodend-of-life care. Both practice and knowledge are an essential foundation toproviding good end-of-life care to nursing home residents. Efforts to improve carefor the dying in nursing homes have been slowed by an absence of measurementtools that capture care processes, a gap that the PCS reported here helpsfill. J Pain Symptom Manage 2011;41:57e67. � 2011 U.S. Cancer Pain ReliefCommittee. Published by Elsevier Inc. All rights reserved.
Key Words
Palliative care, nursing homesAddress correspondence to: Sarah Thompson, PhD,RN, FAAN, University of Nebraska Medical CenterCollege of Nursing, 985330 Nebraska MedicalCenter, Omaha, NE 68198-5330, USA. E-mail:[email protected]
Accepted for publication: March 31, 2010.
� 2011 U.S. Cancer Pain Relief CommitteePublished by Elsevier Inc. All rights reserved.
IntroductionAs the American population ages, nursing
homes are increasingly a setting for end-of-lifecare. More than 1000 people a day die in long-term care settings nationally, and in some states,
0885-3924/$ - see front matterdoi:10.1016/j.jpainsymman.2010.03.016

58 Vol. 41 No. 1 January 2011Thompson et al.
as many as one in three older adults die in nurs-inghomes.1,2 By the year 2020, 40%of those old-er than 65 years will die in nursing homes.3 Toooften, nursing home residents die in pain withunrelieved physical and psychosocial suffer-ing.4e7 Although death is inevitable for perma-nently placed residents, undue suffering is not.
Long-standing concerns exist about the qual-ity of care in nursing homes. Evidence indicatesthat quality has improved; however, seriousproblems continue in areas that commonlyaffect end of life such as use of feeding tubes,transfer to hospital, and symptommanagementfor dyspnea and pain.5,8e12 These findings indi-cate that incorporating palliative care practices,such as advance care planning, pain manage-ment, andbereavement care for family and staff,is central to improving end-of-life experiencesfor residents.
The World Health Organization13 definespalliative care as an approach to care:
. that improves the quality of life ofpatients and their families facing the prob-lems associated with life-threatening illness,through the prevention and relief of suffer-ing by means of early identification and im-peccable assessment and treatment of painand other problems, physical, psychosocial,and spiritual (http://www.who.int/cancer/palliative/definition/en/).
Palliative care is both a philosophy and a caredelivery approach. For nursing homes, palliativecare includes a resident/family-centered focus,enhances residents’ quality of life, and comple-ments traditional restorative interventions.14,15
In nursing homes that have a palliative carefocus,4,5,16 staff embrace death as a normal andinevitable outcome for permanently placed res-idents. Furthermore, staff 1) engage in advancecare planning, that is, to talk openly about dyingand elicit residents’ personal preferences re-garding end-of-life care on admission, at careplanmeetings, and whenever a resident’s condi-tion changes; 2) are knowledgeable about andengage in active symptommanagement; 3) inte-grate palliative planning and interventions,demonstrated by fewer unnecessary hospitaliza-tions and feeding tubes andmore hospice refer-rals; 4) provide psychosocial support for dyingresidents and their family members; 5) use be-reavement interventions, such as memorial ser-vices, for staff, other residents, and family
members; and 6) provide staff continuing edu-cation regarding palliative care.4,5,14,17,18
Although palliative care guidelines exist14
and small-scale palliative care models havebeen developed, tested, and found ben-eficial,19e21 the widespread adoption of theseguidelines and/or the diffusion of innovativemodels has not occurred.18 Nursing homesthat regularly refer residents to hospice pro-vide a stronger palliative care focus and dem-onstrate positive outcomes such as fewerhospitalizations, lower feeding tube rates,and better pain management. Hospice mayhave a positive impact on resident care, butonly 6% of nursing home residents nationallyreceive the hospice benefit.22 Additional stud-ies are needed that evaluate and link the pro-cesses of care provided by nursing home staffto resident outcomes at the end of life.From our previous work, largely qualitative,
factors such as staffing levels, staff communica-tion, and teamwork and the provision of palli-ative care interventions significantly impactedcare decisions, such as the use of hospiceand hospitalization, and resident outcomes,such as the degree of physical and psychosocialsuffering.4,5,16,23e25 Nursing homes whose staffdemonstrated stronger communication andteamwork practices had a stronger foundationfor the delivery of palliative care,5,16,25 butcommunication and teamwork are not suffi-cient for the delivery of palliative care. For ex-ample, staff may work well in teams, but if stafflacked sufficient clinical knowledge about painmanagement or did not engage in advancecare planning, the provision of optimal pallia-tive interventions did not occur. Furthermore,if nursing home administrators did not sup-port a positive philosophical orientation to-ward death and dying through activities suchas bereavement support for staff and familyor hospice referrals, the delivery of palliativecare also was impeded.5,17
Efforts to improve care for residents stand tobe enhanced by measures to assess the degreeto which nursing home staff provide palliativecare. Many measures capture variables relatedto good end-of-life outcomes such as satisfac-tion with care, pain management, and honor-ing of preferences.26,27 As the incidence ofdeath in nursing homes increases with theaging population, the gap in measurementregarding care processes must be addressed.

Table 1PCS Example Items
Constructs Example Items
Palliative Care PracticeBereavement When a resident dies, I follow up with his/her roommate to provide emotional support
We have memorials for residents who dieProvider coordination When residents are at the end of life, the primary care provider:
� talks openly with family members� is open to staff suggestions about care
Family communication When a resident approaches death, how often do family members:� disagree with staff about treatments� want more information
Planning/interventions When would a hospice referral be made for Mrs. Davis?a
� On admission� When Mr. Davis requests it� When the provider orders it� Now that she has lost weight� At the next care plan meeting
Palliative Care KnowledgePsychological Anxiety contributes to physical painPhysical Residents can sleep when they have physical painEnd-of-life factors Feeding tubes prevent aspiration
aItem is based on a resident case vignette.
Vol. 41 No. 1 January 2011 59Measuring Palliative Care in Nursing Homes
Illuminating the relationship between careprocesses, that is, what staff do for residentsand resident outcomes (e.g., satisfaction withcare or quality of life), will provide a morecomprehensive evaluation of nursing homecare and offer opportunities to develop tar-geted interventions to enhance care. Giventhe increasing importance of helping nursinghomes achieve the best environment for opti-mal end-of-life care, an assessment methodthat captures the various components of palli-ative care processes is needed. To that end, wereport the development and psychometric test-ing of a nursing home palliative care survey.
MethodsInstrument Development
After a review of the literature and the firstauthor’s qualitative data from nursinghomes,4,5,16,23e25,28 palliative care, for the sur-vey, was proposed as an overarching latent con-struct composed of two constructs, eachreflecting different elements of palliative care.The Palliative Care Survey (PCS) encompassesPalliative Care Practice and Palliative CareKnowledge. Palliative Care Practice reflectswhat nursing home staff do, their actions or in-terventions that demonstrate a palliative ap-proach to care, and Palliative Care Knowledge
reflects basic knowledge that underpins careplanning and decision making (Table 1). Pallia-tive Care Practice comprises four subconstructs:bereavement, planning/intervention, familycommunication, and provider coordination. Be-reavement items reflect attention to the grievingprocess such as emotional support for family,staff, and residents and activities such as memo-rial services. Planning/intervention reflects thetiming of care planning decisions includingorders for do-not-resuscitate, hospice referrals,and theuseof feeding tubes. Family communica-tion addresses provider/staff and family under-standing regarding the plan of care. Providercoordination reflects nursing home staff andprovider coordination of palliative interventionssuch as painmanagement and hospice referrals.Palliative Care Knowledge comprises three sub-constructs: psychological, physical, and end-of-life factors. Psychological and physical itemsreflect knowledge regarding palliative practicesto manage pain and symptoms. Items, for exam-ple, focus on when to administer pain medica-tion and factors that influence physicaldiscomfort. The end-of-life factors subconstructreflects knowledge surrounding commonend-of-life issues such as the management ofweight loss.
Initially, care planning/intervention itemswere developed in two formats to comparewhat format elicited greater variability in

Table 2Job Title Characteristics of Study Personnel
Job TitlePhase 1
(n¼ 717), n (%)Phase 2
(n¼ 2779), n (%)
CNA 360 (50) 1424 (51)LPN 76 (11) 472 (17)RN 58 (8) 362 (13)Restorative 23 (3) 126 (5)Activities 12 (2) 156 (6)Social Services 16 (2) 104 (4)Unknown 172 (24) 135 (5)
60 Vol. 41 No. 1 January 2011Thompson et al.
responses. For example, some of the planning/intervention items were embedded within anunfolding resident-centered case vignettewhere respondents were provided a story abouta resident on admission followed by a three-month update where the resident had declined.Questions were based on the admission statusand the resident’s three-month declining sta-tus. The samequestions, without a case vignette,were placed elsewhere in the survey.
The initial draft of the PCS included 94 items.After the initial item development, a debriefingprocess, similar to cognitive interviewing, wasconducted to establish developmental valid-ity.29,30 Participants (n¼ 16) from two nursinghomes known to have palliative care programsincluded anurse practitioner, a director of nurs-ing, a palliative care nurse, social workers, regis-tered nurses (RNs), licensed practical nurses(LPNs), and certified nurse assistants (CNAs).Each staff participant completed the surveyand then participated in a face-to-face discus-sion with an interviewer to give his/her inter-pretation of the items including the casevignette, difficulties completing items, ratio-nale for responses to items, and overall com-ments regarding the relevance of the items topalliative care and the nursing home environ-ment. Clarifying information was elicited aboutthe appropriate wording of items. Items wererevised or deleted based on staff comments,leaving a total of 70 items for further testing.
Psychometric evaluation of the instrumentwas completed in two phases. Phase 1 focusedon individual item analyses and subsequent re-vision or deletion of items. Phase 2 gatheredevidence for reliability and validity. Each phasereceived institutional review board approval.Table 2 displays the job characteristics of studyparticipants in the two phases.
Phase 1Sample and Setting. For the initial testing of the70-item survey, a list of nursing homes withinone hour of a Midwestern metropolitan area(n¼ 99) was generated and randomly sorted.Based on the order of sorting, the first 26 nurs-ing homes were invited to participate, with77% (n¼ 20) of the homes agreeing. In addi-tion, four homes were purposefully selectedandaddedbecauseof their establishedpalliativecare programs. Of the participating homes(n¼ 24), 11 homes (46%) were nonprofit; two
homes were Medicaid only, whereas the remain-ing 22 homes were dually Medicare-Medicaidcertified. The number of nursing home bedsranged from60 to300(mean[M]¼ 126).Directcare staff (n¼ 717), including nursing, socialservice, activities, and restorative personnel,completed the surveys.
Data Analysis. Dimensionality was exploredus-ing principal components exploratory factoranalysis with varimax rotation. Items with<0.30 factor loadings were deleted. Initial fac-tors were examined based on eigenvaluesgreater than one, the scree plot, and conceptualcongruence, which supported the four hypoth-esized subconstructs: bereavement, planning/intervention, family communication, and pro-vider coordination.
Results. Descriptive statistics and central ten-dency were examined for each item, deletingthose that were skewed and lacked variability(14 items deleted). Generally, planning/inter-vention items, which were not embedded withina vignette, lacked variability. For example, whenstaff were asked to indicate when discussions re-garding preferences for resuscitation occurred,they overwhelmingly selected on admission,thus eliciting little variability. When this ques-tion was posed as part of an unfolding, residentcase vignette, the same question elicited greatervariability and staff selected other options suchas “at the next care plan meeting” or “whenthe provider orders it.” Therefore, the items as-sociated with the case vignette were retainedfor further testing.Item-to-total correlations ranged from0.40 to
0.90 for all but three items, which were revisedfor additional testing. Because the PalliativeCare Knowledge construct contains dichoto-mous items, it was analyzed separately and the

Vol. 41 No. 1 January 2011 61Measuring Palliative Care in Nursing Homes
three subconstructs remained: psychological,physical, and end-of-life factors.
The initial testingof thePCSprovided encour-aging results. Fifty-six items were retained foradditional testing: 36 items for Palliative CarePractice (bereavement, eight items; planning/intervention, 20 items; family communication,three items; and provider coordination, fiveitems) and 20 items for Palliative Care Knowl-edge (psychological, four items; physical, fiveitems; and end-of-life factors, 11 items).
Phase 2Setting and Sample. Phase 2 was completed aspart of a larger ongoing study that is assessingthe relationship of staff communication, team-work, and palliative care practices to end-of-lifeoutcomes for nursing home residents andtheir family members.31 One hundred ran-domly selected nursing homes in two midwest-ern states were recruited to participate. Theparent study had a 39% refusal rate. Fromthe initial sample of 100 nursing homes, 15homes were removed from the parent studybecause of missing data. Thus, data from 85nursing homes comprised the sample forPhase 2 and were used to psychometricallyevaluate the PCS. To assess factorial validity,the resulting model from Phase 1 was evalu-ated using confirmatory factor analyses to fitthe hypothesized model to the data in Phase 2.
Based on the authors’ preliminary stud-ies,4,5,16,25 the following hypotheses were gener-ated to evaluate construct validity: 1) nursinghome staff communication and teamwork willbe positively related to the survey subconstructsof Palliative Care Practice (bereavement, plan-ning/intervention, family communication,and provider coordination); and 2) licensedstaff (RNs and LPNs) will have higher scoreson the Palliative Care Knowledge constructthan unlicensed staff (certified nurse aides).
Procedures. Nursing home administrators wereinvited to participate and gave informed con-sent before approaching direct care staff fordata collection. Staff were provided writtenand verbal information about the study andprovided their agreement for participation. Re-searchpersonnel gave an inservicepresentation,unrelated to palliative care, as an incentive fornursing home and staff participation. After theinservice presentation, staff completed both
the PCS and Shortell’s Organization and Man-agement Survey in 20e30 minutes.
Measures
Palliative Care Practice. Four subconstructscomprised the Palliative Care Practice model:bereavement (eight items), planning/interven-tion (20 items), family communication (threeitems), and provider coordination (five items).Responses are rated on a 4-point Likert-typescale ranging from never to always. The plan-ning/intervention items are summed to createfour weighted scores for analysis procedures.Summation criteria were determined based onexpert opinion and evidence-based practice inpalliative care.
Palliative Care Knowledge. Three subconstructscomprised the Palliative Care Knowledgemodel. They included factors that influencepain: psychological (four items) and physical(five items), and end-of-life factors (11 items).Items are dichotomous.
Communication and Teamwork. Staff communi-cation and teamwork were measured usingShortell’s Organization and Management Sur-vey. This survey has established reliability andvalidity in the hospital setting32,33 and has beenadapted to reflect the language of the nursinghome setting.34,35 Communication has five di-mensions with a total of 18 items: openness(four items), accuracy (four items), timeliness(four items), effectiveness (two items), and un-derstanding (four items). Teamwork has threedimensions with a total of 12 items: cohesion(six items), meeting effectiveness (two items),and unit relations (four items). Responses arerated on a five-point Likert-type scale rangingfrom strongly disagree to strongly agree. Onboth measures, teamwork and communication,all items are summed and the mean score wasused for analysis. In nursing homes, Cronbach’salphas have ranged from 0.83 to 0.90. Constructvalidity hasbeen supportedbyhypothesis testingwith divergent groups.34,35
Data Analysis. Item statistics were generated toevaluate variability, central tendency, missingdata, and distribution characteristics. Internalconsistency reliability was examined usingCronbach’s alpha, evaluating the interitem

Table 3Phase 2 Staff Demographics
Demographics Frequency (%)a
Number of years employed at this nursing home<1 582 (21)1e5 942 (34)6e10 377 (14)11e15 224 (8)16e20 146 (5)>20 226 (8)Missing 282 (10)
Education levelLess than high school 92 (3)High school 1378 (50)Associate’s degree 839 (30)Bachelor’s degree 308 (11)Master’s degree 69 (2)Missing 93 (3)
EthnicityAfrican American 75 (3)Asian American 40 (1)Multiracial 33 (1)Caucasian 2175 (78)Hispanic American 81 (3)Native American 142 (5)Other 149 (5)Missing 84 (3)
GenderMale 151 (5)Female 2430 (87)Missing 198 (7)
Age, in years#24 424 (15)25e34 583 (21)35e44 518 (18)45e54 675 (24)55e64 408 (15)$65 121 (4.3)Missing 50 (2)
Percentages (%) are based on all data including missing.aMissing data varied per demographic item.
62 Vol. 41 No. 1 January 2011Thompson et al.
correlations (acceptable range¼ 0.30e0.70),corrected item-to-total correlation ($0.30),and alpha if item deleted (increase of #0.01).Cronbach’s alphas were calculated usingTetrachoric correlations36 among the items forall constructs (a$ 0.70).37 Evidence for con-struct validity was evaluated usingMplus Version5.21 software systems to conduct the confirma-tory factor analysis (structural equation model-ing) and for the hypothesis testing. For theconfirmatory factor analysis, goodness-of-fit indi-ces were generated including the comparativefitindex (CFI) and the root mean square error ofapproximation (RMSEA).38,39 Desirable indicesinclude a CFI greater than 0.90 or an RMSEAless than 0.08.38 For construct validity, the firsthypothesis was evaluated using Pearson’s corre-lation between Palliative Care Practice subcon-structs with communication and teamwork,and the second hypothesis was using analysisof variance of Palliative Care Knowledge acrossstaff type.
Results. Of the 85 homes that comprised thesample, 52 were in rural locations and 33 were ur-ban; where 45 were for profit and 40 were not forprofit. Thenumber of nursinghomebeds rangedfrom 60 to 193 (M¼ 89). Description of nursinghome staff positions is presented in Table 2. Staffdemographics are presented in Table 3.
Item Analysis. All items on the Palliative CarePractice subconstructs exhibited variabilityacross all response options with item meansranging from 1.84 to 3.63 (range: 1e4). ForPalliative Care Knowledge, all items exhibitedvariability with the mean proportion correctranging from 0.27 to 0.99 (range: 0.00e1.00).
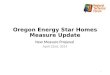
Confirmatory Factor Analysis. Separate second-order factor analytic modeling procedureswere conducted for the hypothesized structuresfor the Palliative Care Practice (Fig. 1) andPalliative Care Knowledge (Fig. 2) constructs.The hypothesized (H) model for PalliativeCare Practice had adequate fit of the model tothe data (Table 4). On review, however, five ofthe measured items did not load on theircorresponding subconstruct; three items on be-reavement, one itemon family communication,and one item on provider coordination. Withthese five items removed, the final model ex-hibited a better fit to the data (CFI¼ 0.94;
RMSEA¼ 0.04). Thus, a parsimonious Pallia-tive Care Practice model contained 31 items.The correlations of the second-order factor, Pal-liativeCarePractice, with the four subconstructswere bereavement (r¼ 0.68, P< 0.001); plan-ning/interventions (r¼ 0.44, P< 0.001); familycommunication (r¼ 0.24, P< 0.001); and pro-vider coordination (r¼ 0.70 P< 0.001).The hypothesized model for Palliative Care
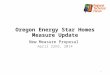
Knowledge had excellent fit to the data (Table4). One variable measured (feeding tubes pro-long life) did not have a significant loading onthe subconstruct, end-of-life factors. Becauseof the importance of this information in provid-ing end-of-life care, a decision was made to re-tain this item in the model. The correlationsof the three subconstructs with the second-order Palliative Care Knowledge factor were

Fig. 1. Palliative care practice second-order confirmatory factor analysis (CFI¼ 0.94, RMSEA¼ 0.04). *Twentyitems that are summed to make four weighted scores for the planning/intervention subconstruct.
Vol. 41 No. 1 January 2011 63Measuring Palliative Care in Nursing Homes
psychological (r¼ 0.84, P< 0.001), physical(r¼ 0.52, P< 0.001), and end-of-life factors(r¼ 0.60, P< 0.001).
Reliability. After the final delineation of boththe Palliative Care Practice and Palliative CareKnowledge constructs, Cronbach’s alpha was
$0.70 for Palliative Care Practice (a¼ 0.75)and for Palliative Care Knowledge (a¼ 0.81).Two of the four subconstructs for PalliativeCare Practice met the minimum requirement,with family communication, provider coordina-tion, bereavement, and planning/interventionsubconstructs having a¼ 0.77, 0.79, 0.62, and

Fig. 2. Palliative care beliefs second-order confirmatory factor analysis (CFI¼ 0.99, RMSEA¼ 0.033).
64 Vol. 41 No. 1 January 2011Thompson et al.
0.69, respectively. For the Palliative Care Knowl-edge construct, the Cronbach’s alphas for thethree subconstructs were 0.97 (psychological),0.90 (physical), and 0.60 (end-of-life factors).Removalof anyof the itemson the subconstructs
did not improve alpha; thus, all items wereretained.
Hypotheses Testing. For the first hypothesis,there were strong correlations between

Table 4Fit Indices for the Measurement Models of Palliative Care Practice and Knowledge
Fit Indices Measurement Model c2 df c(0)2 df(0) CFI RMSEA (90% CI)
PCS (H) 689.75 162 0.92 0.05 (0.04, 0.05)PCS (F) 338.31 86 4011.59 105 0.94 0.04 (0.04, 0.05)Knowledge (H/F) 240.63 88 10,674.09 79 0.99 0.03
H¼ hypothesized model; F¼ final model; c2¼ chi2 model fit; df¼ degrees of freedom model fit; c(0)2¼ chi2 baseline model fit; df(0)¼ degreesof freedom baseline model fit; CI¼ confidence interval.
Vol. 41 No. 1 January 2011 65Measuring Palliative Care in Nursing Homes
Palliative Care Practice and communication(r¼ 0.72, P< 0.001) and teamwork (r¼ 0.74,P< 0.001). There were weak-to-moderate corre-lations between communication and teamworkwith bereavement (r¼ 0.51, P< 0.001 andr¼ 0.58, P< 0.001, respectively); with plan-ning/intervention (r¼ 0.23, P< 0.001 andr¼ 0.26, P< 0.001, respectively); with familycommunication (r¼ 0.32, P< 0.001 andr¼ 0.35, P< 0.001, respectively); and with pro-vider coordination (r¼ 0.48, P< 0.001 andr¼ 0.43, P< 0.001, respectively). Thus, the firsthypothesis was supported, lending evidence ofconstruct validity.
For the second hypothesis, there was a signifi-cant difference between licensed staff (RNsand LPNs) and unlicensed staff on the Palliat-ive Care Knowledge (F(3)¼ 131.78, P< 0.001)and the three subconstructs: psychological(F(3)¼ 50.26, P< 0.001), physical (F(3)¼ 17.47,P< 0.001), and end-of-life factors (F(3)¼ 97.82,P< 0.001). On Palliative Care Knowledge, RNs(M¼ 0.812) scored significantly (P< 0.001)higher than LPNs (M¼ 0.76) or CNA/CertifiedMedical Assistants (M¼ 0.64). Although the dif-ferences were not as large, the same pattern ex-isted among the three levels of staff forPalliative Care Knowledge. This support forthe secondhypothesis provided evidenceof con-struct validity for the knowledge items.
DiscussionThe 51-item PCS made up of Palliative Care
Practice and Palliative Care Knowledge mea-sures the extent to which nursing home staffengage in palliative care practices and haveknowledge consistent with good end-of-lifecare. Both practice and knowledge are an es-sential foundation to providing good end-of-life care to nursing home residents.
There is strong empirical and psychometricsupport for the PCS and evidence of adequate
validity and reliability. It is psychometricallychallenging to design items that capture whatstaff actually do as opposed to what they thinkthey do or think they are supposed to do. Forexample, staff typically are aware of federalregulations requiring discussion of advance di-rectives on admission, and they answered suchdirect questions accordingly. On the otherhand, planning/intervention items based onvignettes that ask staff what typically is donein their nursing home elicit greater variabilityand less missing data than questions posed di-rectly. In addition, response patterns from thevignette-based questions were more consistentwith data from our qualitative studies. For ex-ample, both qualitative data and data fromthe PCS indicate that most discussions aboutdying are triggered by an event such as weightloss or hospitalization as opposed to ongoingplanning initiated at admission or shortlythereafter. The PCS was developed to covera range of practices and levels of knowledgeof licensed and unlicensed nursing personnel.This study shows the PCS-captured variation inthe staff behavior and knowledge.
As empirical evidence emerges and standardsfor practice change, additional subscales maybe added to the PCS. For example, althoughthe PCS captures key aspects of end-of-lifecare, such as bereavement care, it does not as-sess staff members’ attention to the spiritualneeds of residents or family. As practices de-velop to address additional aspects of palliativecare, users of the PCS may wish to augment itwith other appropriate measures of those con-cepts. Also, the PCS covers a range of practicesand levels of knowledge of licensed and unli-censed staff. It is possible that separate versionstailored to the roles and desired knowledgelevels of different levels of staff may be war-ranted in some investigations. Furthermore,the PCS has been developed and evaluated inthe Midwest. Additional testing across a widergeographic area is warranted.

66 Vol. 41 No. 1 January 2011Thompson et al.
Nursing homes are complex organizationswith multiple interacting structures and pro-cesses that influence resident outcomes.Investigators have examined structural charac-teristics such as staffing levels or skill mix and re-lated these to resident outcomes.5 However,efforts to improve care and quality of life for res-idents would be incomplete without consideringpalliative care as an essential clinical process forall permanently placed residents. Many nursinghomes in the United States struggle to provideeven basic attention to palliative care at theend of life.40 Given the rapid increase of dyingin nursing homes in light of the aging popula-tion, there is urgent need for empirical researchand soundpsychometricmeasuresof salient vari-ables in the provision of palliative care. Efforts toimprove care for the dying in nursing homeshavebeen slowedby an absenceofmeasurementtools for research,1 a gap that the PCS reportedhere helps fill.
Disclosures and AcknowledgmentsThis study was partially funded by Na-
tional Institute of Nursing Research grant5RO1NR009547. The authors declare noconflicts of interest.
References1. Munn JC, Zimmerman S, Hanson LC, et al.Measuring the quality of dying in long-term care.J Am Geriatr Soc 2007;55:1371e1379.
2. Teno JM. Brown Atlas of dying. Available fromhttp://www.chcr.brown.edu/dying/brownatlas.htm.Accessed October 11, 2008.
3. Brock DB, Foley DJ. Demography and epidemi-ology of dying in the U.S. with emphasis on deathsof older persons. Hosp J 1998;13:49e60.
4. Forbes S. This is Heaven’s waiting room: end oflife in one nursing home. J Gerontol Nurs 2001;27:37e45.
5. Forbes-Thompson S, Gessert CE. End of life innursing homes: connections between structure, pro-cess, and outcomes. J Palliat Med 2005;8:545e555.
6. Kayser-Jones J. The experience of dying: an eth-nographic nursing home study. Gerontologist 2002;42(Spec No 3):11e19.
7. Kayser-Jones J, Schell E, Lyons W, et al. Factorsthat influence end-of-life care in nursing homes:the physical environment, inadequate staffing, andlack of supervision. Gerontologist 2003;43(SpecNo 2):76e84.
8. Hanson LC, Eckert JK, Dobbs D, et al. Symptomexperience of dying long-term care residents. J AmGeriatr Soc 2008;56:91e98.
9. Hodgson NA, Lehning AJ. Palliative care innursing homes: a comparison of high- and low-level providers. Int J Palliat Nurs 2008;14:38e44.
10. Johnson VM, Teno JM, Bourbonniere M, Mor V.Palliative care needs of cancer patients in U.S. nurs-ing homes. J Palliat Med 2005;8:273e279.
11. Oliver DP, Porock D, Zweig S. End-of-life care inU.S. nursing homes: a review of the evidence. J AmMed Dir Assoc 2004;5:147e155.
12. Wunderlich GS, Kohler PO, eds. Improving thequality of long-term care. Washington, DC: NationalAcademies Press, 2001.
13. World Health Organization. WHO definition ofpalliative care. Available from http://www.who.int/cancer/palliative/definition/en/. Accessed January16, 2009.
14. National Consensus Project for Quality Pallia-tive Care (2009). Clinical practice guidelines forquality palliative care, 2nd ed. http://www.nationalconsensusproject.org.
15. Thompson S, Church L. The structure and pro-cess of advanced chronic illness and palliative carein nursing homes. In: Bern-Klug M, ed. Transform-ing palliative care in nursing homes: The socialwork role. New York: Columbia University Press,2010:31e58.
16. Forbes-Thompson S, Gessert CE. Nursinghomes and suffering: part of the problem or partof the solution? J Appl Gerontol 2006;25:234e251.
17. Forbes-Thompson S, Gajewski B, Scott-Cawiezell J, Dunton N. An exploration of nursinghome organizational processes. West J Nurs Res2006;28:935e954.
18. Hanson LC, Ersek M. Meeting palliative careneeds in post-acute care settings: “to help themlive until they die”. JAMA 2006;295:681e686.
19. Levy C, Morris M, Kramer A. Improving end-of-life outcomes in nursing homes by targeting resi-dents at high-risk of mortality for palliative care:program description and evaluation. J Palliat Med2008;11:217e225.
20. Strumpf NE, Tuch H, Stillman D, Parrish P,Morrison N. Implementing palliative care in thenursing home. Ann Longterm Care 2004;12:35e41.
21. Stillman D, Strumpf N, Capezuti E, Tuch H.Staff perceptions concerning barriers and facilita-tors to end-of-life care in the nursing home. GeriatrNurs 2005;26:259e264.
22. Stevenson DG, Bramson JS. Hospice care in thenursing home setting: a review of the literature.J Pain Symptom Manage 2009;38:440e451.
23. Forbes S, Bern-Klug M, Gessert C. End-of-lifedecision making for nursing home residents withdementia. J Nurs Scholarsh 2000;32:251e258.

Vol. 41 No. 1 January 2011 67Measuring Palliative Care in Nursing Homes
24. Bern-Klug M, Gessert C, Forbes S. The need torevise assumptions about the end of life: implica-tions for social work practice. Health Soc Work2001;26:38e48.
25. Forbes-Thompson S, Leiker T, Bleich MR. High-performing and low-performing nursing homes:a view from complexity science. Health Care Man-age Rev 2007;32:341e351.
26. Teno JM, Clarridge B, Casey V, et al. Validationof Toolkit After-Death Bereaved Family Member In-terview. J Pain Symptom Manage 2001;22:752e758.http://www.chcr.brown.edu/pcoc/toolkit.htm.
27. Kiely DK, Volicer L, Teno J, et al. The validityand reliability of scales for the evaluation ofend-of-life care in advanced dementia. AlzheimerDis Assoc Disord 2006;20:176e181.
28. Thompson S, Parker-Oliver D. A new model forlong-term care: balancing palliative and restorativecare delivery. J Hous Elderly 2008;22:1e26.
29. Irwin DE, Varni JW, Yeatts K, DeWalt DA. Cogni-tive interviewing methodology in the developmentof a pediatric item bank: a patient reported out-comes measurement information system (PROMIS)study. Health Qual Life Outcomes 2009;7:3.
30. Woolley ME, Bowen GL, Bowen NK. Cognitivepretesting and the developmental validity of childself-report instruments: theory and applications.Res Soc Work Pract 2004;14:191e200.
31. Forbes-Thompson SA. The impact of quality end-of-life care in nursing homes. 2006; 5RO1NR009547-04National Institute ofNursing Research 2006e2010.
32. Shortell SM, RousseauDM, Gillies RR, Devers KJ,Simons TL. Organizational assessment in intensivecare units (ICUs): construct development, reliability,and validity of the ICU nurse-physician question-naire. Med Care 1991;29:709e726.
33. Shortell SM, Zimmerman JE, RousseauDM, et al.The performance of intensive care units: does goodmanagement make a difference? Med Care 1994;32:508e525.
34. Scott J, Vojir C, Jones K, Moore L. Assessingnursing homes’ capacity to create and sustain im-provement. J Nurs Care Qual 2005;20:36e42.
35. Scott-Cawiezell J, Schenkman M, Moore L, et al.Exploring nursing home staff’s perceptions ofcommunication and leadership to facilitate qualityimprovement. J Nurs Care Qual 2004;19:242e252.
36. Gajewski BJ, Boyle DK, Thompson S. Howa Bayesian might estimate the distribution ofCronbach’s alpha form ordinal-dynamic scaled data:a case study measuring nursing home residentsquality of life. Methodology (Gott) 2010;6:71e82.
37. Nunnally JC. Psychometric theory. New York:McGraw-Hill, 1978.
38. Brown TA. Confirmatory factor analysis for ap-plied research. New York: The Guilford Press, 2006.
39. Kline RB. Principles and practice of structuralequation modeling. New York: The Guilford Press,1998.
40. Miller SC, Han B. End-of-life care in U.S. nurs-ing homes: nursing homes with special programsand trained staff for hospice or palliative/end-of-life care. J Palliat Med 2008;11:866e877.