Embed Size (px)
Citation preview

2014 Annual Breast Cancer Rehabilitation
Healthcare Provider Event
A Manual Therapy and Exercise Approach to Breast Cancer Rehabilitation Course
November 7th and 8th, 2014
Mercer University, Atlanta, GA
Sponsored By:
TurningPoint’s Edith Van Riper-Haase Breast Cancer
Rehabiltation Advocacy Fund
thevisualab.com
Presentations are
Available on TurningPoint’s Website:
myturningpoint.org
Click on Course Link
www.oncologypt.org itsthejourney.org

A Manual Therapy and Exercise
Approach to Breast Cancer
Rehabilitation Course
Functional Outcome
Measures in Breast
Cancer Rehabilitation
Jill Binkley, PT, MSc, FAAOMPT, CLT
This Presentation is available on TurningPoint’s Website:
myturningpoint.org
From Homepage Click on Course Link

Generic Health Status Condition/Region Specific Patient Specific
• does not refer to a specific
disease or problem
• taps a spectrum of health
concepts
• permits comparison among
groups with different health
problems (e.g. cancer, kidney
disease, OA, stroke)
Example: SF-36
• assesses characteristic or activities
most relevant to the condition or
intervention
Examples:
•Upper Extremity Functional Index
(UEFI), Disabilities of Arm, Shoulder
and Hand (DASH)
• assesses characteristic or
activities that are most
relevant to the individual
Example: PSFS
Functional Assessment of
Cancer Therapy – Breast
Cancer Quality of Life
Instrument
(FACT-B)
EORTC-C30 and BR23 Scales
“Hybrid”
•Measures a spectrum of health
concepts, including physical, social
and emotional
•Characteristics of both generic
health status and condition-specific
Classification of Self-Report Outcome Measures
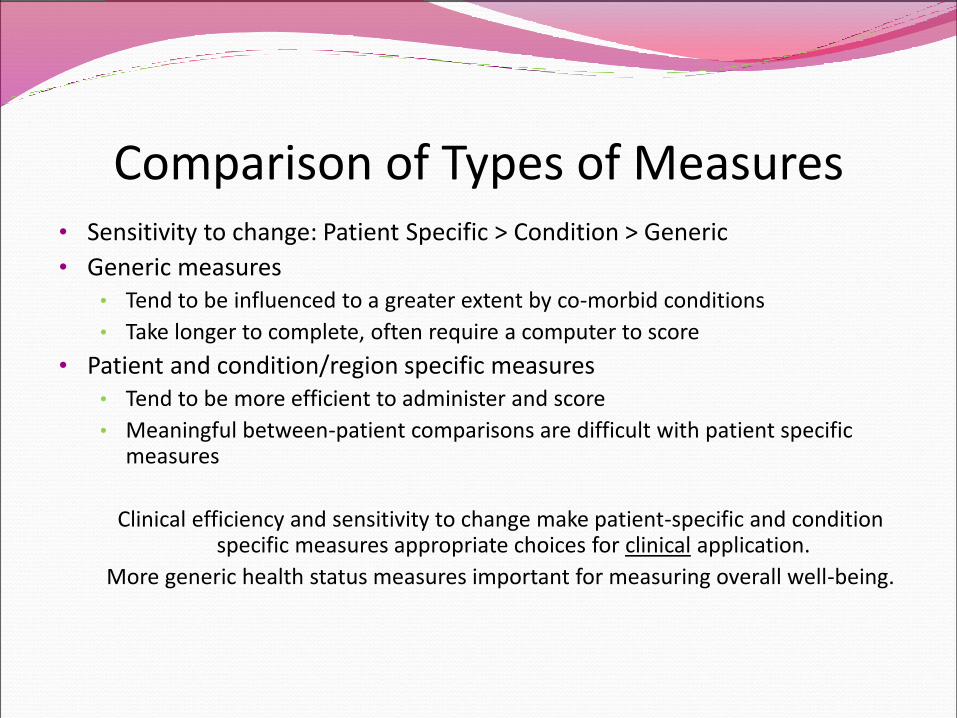
Comparison of Types of Measures• Sensitivity to change: Patient Specific > Condition > Generic
• Generic measures • Tend to be influenced to a greater extent by co-morbid conditions
• Take longer to complete, often require a computer to score
• Patient and condition/region specific measures • Tend to be more efficient to administer and score
• Meaningful between-patient comparisons are difficult with patient specific measures
Clinical efficiency and sensitivity to change make patient-specific and condition specific measures appropriate choices for clinical application.
More generic health status measures important for measuring overall well-being.

Common Self-Report Measures of Upper Extremity Function
DASH = Disabilities of the Arm, Shoulder and Hand (Hudak, 1996)
UEFI = Upper Extremity Functional Index(Binkley, 2001)
ULDQ = Upper Limb Disability Questionnaire(Springer, 2010)
KAPS = Kwan Arm Problem Scale(Kwan, 2002)
* Developed for Breast Cancer Population

Breast Cancer EDGE Tool to Evaluate Physical Therapy Outcome Measures for Breast Cancer:
• 5= highly recommended; the outcome measure has excellent psychometric properties and clinical utility.
• 4 = recommended; lacking psychometric properties, but the measure was specifically designed for use in Breast Cancer population.
• 3= recommended; the outcome measure has good psychometric properties and good clinical utility.
• 2= unable to recommend at this time; there is insufficient information to support a recommendation of this outcome measure.
• 1= not recommended; the outcome measure has poor psychometric properties and/or poor clinical utility.
Evaluation Database to Guide Effectiveness (EDGE) Task Force on Outcome Measures
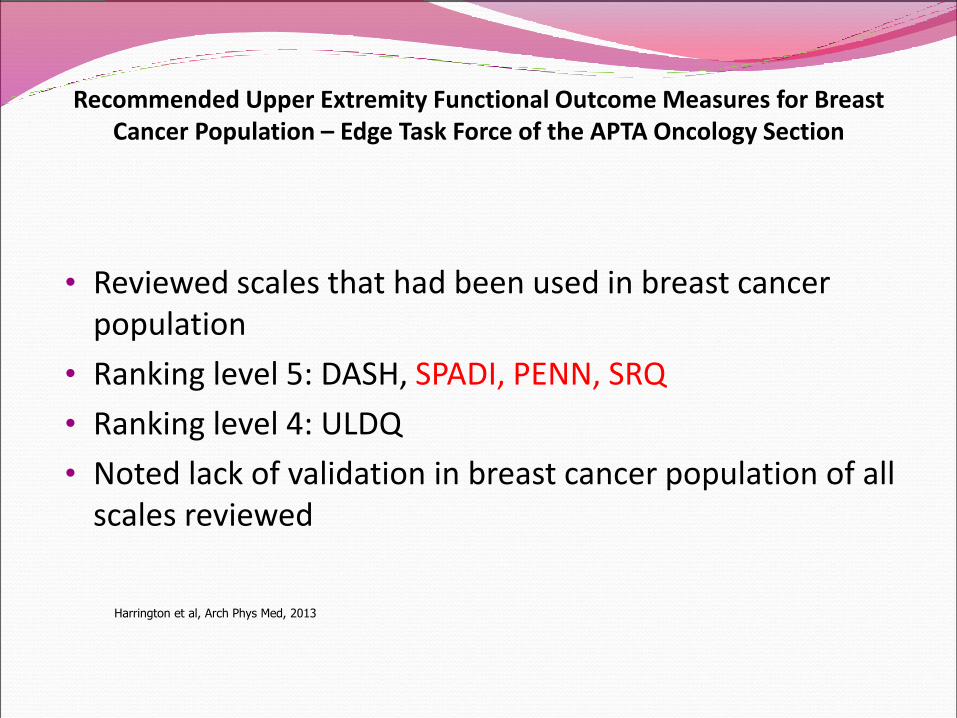
Recommended Upper Extremity Functional Outcome Measures for Breast Cancer Population – Edge Task Force of the APTA Oncology Section
• Reviewed scales that had been used in breast cancer population
• Ranking level 5: DASH, SPADI, PENN, SRQ
• Ranking level 4: ULDQ
• Noted lack of validation in breast cancer population of all scales reviewed
Harrington et al, Arch Phys Med, 2013

DASH and QuickDASH(Hudak, 1996; Gummerson, 2006; Mintken, 2009; SooHoo, 2002)
DASH is 30 items, 2 pages + optional work and sports modules
QuickDASH is 11 items, 1 page + work/sports modules
Low score – no disability, high score (100) – high disability
Requires a calculator to score
DASH and Quick DASH have been show to be reliable, valid and
sensitive to change in an orthopaedic population (Roy, 2009;
Poison, 2010; Lebman 2010)
Multi-dimensional – includes impairments such as pain and
numbness and tingling in addition to function
Not validated in BC population, but are the scales most widely in
assessing function in this population in research studies

Upper Extremity Functional Index (UEFI)(Stratford, Binkley, Stratford, 2001, Chesworth, 2009; Razmjou, 2006)
20 item self-report functional status measure
Items scored on a 5 point scale (0 to 4)
Total score value 0 (low function) to 80 (high)
< 15 seconds to score without computational aids
Reliable and valid in orthopaedic population (Stratford, 2001;
Chesworth, 2009; Razmjou, 2006)
Unidimensional – only contains items related to function
Not validated in BC population
Companion Scale to the Lower Extremity Functional Scale
(LEFS) which is widely used – both were designed to be efficient
clinically for patients to complete and clinicians to score


Reliability Validity including Sensitivity to Change Clinical Utility
and Application to BC
UEFI (/80) Internal consistency a=.96Test-retest: ICC .86 to .95(Stratford, Binkley, 2001; Chesworth, 2009)
MDC = 10 scale points (Stratford, Binkley, 2001)
Discriminates between subjects by work status (Stratford, Binkley, 2001) Convergent cross-sectional validity with UEFS (Stratford, Binkley, 2001; Chesworth, 2009)
Sensitivity to Change•Correlation of UEFI and Pooled Rating of Change (UEFS change, prognostic rating, pain severity change): r=.7 (.50-.83) (Stratford, Binkley, 2001)•SRM UEFI 1.54 (superior RC-QOL, WORC Index, ASES) (Razmjou, 2006) •UEFI superior compared to UEFS, RC-QOL, WORC Index and ASES standard shoulder form using global rating of change and SRM calculation (Chesworth, 2009; Razmjou, 2006
1 page, easy to complete
and score
DASH
And QuickDASH (/100)
Poor Function=100
No disability = 0
Test-retest : ICC = .77-.88
(Roy, 2009)
MDC = 11 (Roy, 2009; Polson,
2010)
(DASH and QuickDASH)
MID = 19 (QuickDASH)
•Convergent Validity and Sensitivity to Change well
established (Roy, 2009; Beaton, 2006, Slobogean,
2010)
•SRM DASH 0.5-2.0 (Roy, 2009)
•No significant difference in sensitivity to change
between DASH and UEFI using GRC and area under
ROC curve (Lehman, 2010)
UEFI shorter to complete
than DASH (3-5 minutes
versus 5-7 minutes)
(Lehman, 2010)
UEFI faster to score (20 s
versus 5 minutes) (Lehman,
2010)
DASH
And QuickDASH
(subjects with breast
cancer)
Not available DASH correlates with UE strength, ROM, grip
strength (Hayes, 2005)
DASH appears to have adequate construct validity
and responsiveness in breast cancer patients
(Harrington, 2013)
Comparison of Measurement Properties of Upper Extremity Functional Index (UEFI) with Disabilities of the Arm, Shoulder, Hand (DASH) Self-Report Measures for Women with Breast Cancer
UEFS = Upper Extremity Functional Scale; RC-QOL = Rotator Cuff-Quality of Life; WORC = Western Ontario Rotator Cuff Index; ASES = American Shoulder and Elbow Surgeons Standardized Shoulder Assessment Form

Patient Specific Functional Scale(Stratford & Binkley, 1995; Chatman, Binkley et al, 1997; Westaway, Stratford, Binkley 1998)
Initial Assessment Script
I’m going to ask you to identify up to 3 important activities that you are
unable to do or have difficulty with as a result of your breast cancer.
0 1 2 3 4 5 6 7 8 9 10
Unable to Able to
perform activity at perform activity
fully
Patient specific measures assess functional status activities that are most relevant to the individual patient

Patient Specific Functional Scale
• Measurement properties of the PSFS have been reported for patients with low back pain, knee, neck and upper limb dysfunction (Stratford, Binkley 95; Chatham, Binkley 97; Westaway, 98; Stewart, 07, Hefford, 2012)
• The Patient Specific Functional Scale (PSFS) has been shown to be highly reliable and valid and sensitivity to change is superior than relevant condition-specific or generic health status measures
• Minimal Detectable Change (MDC) = 1 scale point (average); 2 scale points (individual items)
• MCID = 2 (upper extremity problems)
• Takes approximately 4 minutes to complete with patient

Prospective Surveillance Model
Feasibility Study
Prospective observational study conducted at the Avon Breast
Cancer Center at Grady Memorial Hospital, Atlanta, GA
Subjects: Patients undergoing surgical interventions for breast
cancer.
•Stage 0-III breast cancer
•Breast conserving surgery (BCS) or mastectomy, with or without
reconstruction
•Willing to complete surveys and consent
Demographics 120 patients enrolled
Age: 58, sd 11 years of age (range 26-95)
Race:
87% African-American
7% Black/Caribbean
4% Caucasian/white (non-Latino)
2 % other
Employment:
42% Homemaker
20% Employed Full Time
16% Unemployed
10% Employed Part Time
8% Retired/Students
Insurance:
• 44% Medicaid and/or Medicare/Medicaid
• 30% Medicare
• 8% Public Insurance (VA, etc)
• 11% Private Insurance
• 7% No Insurance

Convergent Construct Validity:
Reasonable correlation of scales with Fact B Physical subscales:
UEFI r= .74
DASH r= - .75
Reasonable correlation of both scales with Shoulder Range of
Motion at Single Point in Time:
UEFI r=.55
DASH r= - .48
Validity of Quick DASH and UEFI in Breast Cancer Population

T=2.55, df=32, p=.02
T=0.40, df=32, p=.70
Validity Construct:
Subjects with
mastectomy
versus breast
conserving
surgery will
have lower
functional
measures.

Sensitivity to Change of Quick DASH and UEFI in Breast Cancer Population
Correlation of Change in Quick DASH and UEFI with Change in Patient-Rated Quality of Life
and Change in Flexion between Early Post-op and 6 week Post-op Period
Change in QOL
(95% CI)
Change in Flexion
(95% CI)
UEFI 0.55 (0.17, 0.79) 0.41 (0, 0.71)
Quick DASH 0.49 (0.09, 0.46) 0 (-0.42, 0.42)
FACT-B Physical 0.39 (-0.04, 0.70) 0.28 (-0.16, 0.63)

Model of Evaluation of Pain, Function and Health-Related Quality of Life in Women with Breast Cancer
Discharge from PT
Pain Scale, PSFS, UEFI FACT-B
Intermittent (e.g. weekly) Re-evaluation of Functional Status and Goals
Pain Scale, PSFS, UEFI/DASH
Admission (Pre-Operative or Early Post-Op)Pain, Patient Specific Functional Scale, Condition Specific Scale and Multi-Dimensional Health Status Measure
Pain Scale, PSFS, UEFI/DASH FACT-B

Goal Setting Using Self-Report Functional Scales
• Select relevant measure
• Select measures that are expected to change related to your intervention
• Make goals measureable – goals of change should be greater than MDC for given scale and ideally greater than MCID if known
• Final anticipated functional level based on factors that impact expectations of change, including treatment factors (e.g. radiation), age, severity, chronicity
• Setting goals requires clinical experience with measures
• Individual PSFS items can be used to set goals or as PSFS average
• Examples:
• Initial UEFI = 45: 2 week goal to UEFI > ? 4 week goal > ?
• Initial Average PSFS = 3: 2 week goal PSFS > ? 4 week goal PSFS > ?

FUNCTIONAL GOAL AND OUTCOME WORKSHEET
PATIENT SPECIFIC FUNCTIONAL SCALE ACTIVITIES
(10 = full function)
Initial
1. Driving 5
2. Lifting Baby 3
3. Playing tennis 0
Average PSFS: 2.7
PAIN SCORE: (0 = no pain)
3
Upper Extremity Functional Index (N=80)
53
FACT-B
Physical Well-Being ( /28) 12
Social/Family Well-Being ( /28) 10
Emotional Well-Being ( /24) 6
Functional Well-Being ( /28) 15
Additional Concerns ( /40) 18
KEY IMPAIRMENT MEASURES:
1. Shoulder Flexion R/L (deg) 145/123
2.
GOALS:
1. Increase UEFI >75/80
2. Increase PSFS > 8/10
3. Increase Tennis > 7/10
4. Decrease Pain < 1/10