Embed Size (px)
Citation preview

Evidence Exchange Network is pleased to present...
A Webinar Series featuring
Health Canada’s Drug Treatment Funding Program (DTFP):
A Look into British Columbia’s Approach
April 19th, 2012 1pm‐2pm EST

About Evidence Exchange NetworkWHAT: Evidence Exchange Network (EENet; formerly OMHAKEN) is a mental
health and addictions network. EENet aims to build a better mental health and addictions system in the province, by creating and sharing evidence about services, supports, and systems.
WHO: EENet connects researchers, service providers, policymakers, system planners, persons with lived experience, and families across Ontario.
HOW: EENet promotes the use of research evidence in decision‐making by providing an infrastructure that links research with mental health and addictions stakeholders
EENet also develops targeted knowledge translation products and tools, and supports interactive exchanges.
For further information about EENet, please visit: http://evidenceexchangenetworkproject.wordpress.com/

• To connect EENet stakeholders with other Canadian jurisdictions to see what they have done to date with the funding provided by Health Canada through its Drug Treatment Funding Program
• Discuss any challenges and similarities that have come up
• To connect stakeholders across provinces and territories as we work towards the shared goal of improving our substance abuse treatment systems.
• For more information about the Ontario DTFP Systems Projects, please visit: www.ontariodtfp.ca
OntarioDTFPDrug Treatment Funding Program Ontario Systems Projects
Why is EENet hosting a Canada‐wide DTFP webinar series?

Health Canada’s Drug Treatment Funding Program: A Look into British Columbia’s
Approach
About the Presenters:
Jane Collins is the Program Manager, Knowledge Exchange with BC Mental Health & Addiction Services, an Agency of the Provincial Health Services Authority. Jane Collins has 17‐years of experience leading and supporting research and knowledge exchange initiatives in addiction and mental health. Jane was the primary author of BC’s DTFP Systems proposal and has been providing program management for B.C.’s DTFP Systems Initiative since July 2010. Jane is the co‐chair of the B.C. Youth Concurrent Disorders Network, and a member of the BC Substance Use Network, and the BC Child and Youth Mental Health Care Advisory Network. Prior to arriving in BC, Jane was the Clinical Project Leader for the Addiction’s Division, Centre for Addiction & Mental Health.
Amanda Seymour is a Manager in the Mental Health and Substance Use Branch of the BC Ministry of Health. Amanda leads multiple projects aimed at strengthening the substance use and mental health system; including the development of a provincial model and standards for the health authority funded residential substance use system, released in October 2011. Prior to joining the BC Provincial Government, Amanda worked for many years in NGOs. She has worked with youth, adults and families dealing with substance use and mental health issues; family violence; child welfare; homelessness; and HIV\AIDS.
Glen Grigg has a Ph.D. in clinical and counseling psychology. He is a practicing psychotherapist and Director of the B.C. Association of Clinical Counsellors since 1998, VP, 1998‐2007 and Chair of Regulation, 2003 to present. He is the former Coordinator of the Master of Arts in Counselling Psychology, City University of Seattle, Instructor in graduate programs in applied psychology since 1996, and the former Program developer/supervisor/family therapist for residential programs for The Children’s Foundation, 1983‐2001. Glen served on the Canadian Counselling and Psychotherapy Association’s Working Group for Labour Mobility, developing and validating national standards for counseling and psychotherapy, 2008‐2011. In 2011 Glen worked with BC’s DTFP team to produce an Appreciate Inquiry entitled “A preliminary scan into clinical supervision in health authorities in BC: An inquiry into possibilities”. Glen is currently working with BC’s DTFP team to develop an Appreciative Inquiry Framework to support the implementation of the residential standards.

House‐keeping
• This webinar will be recorded and posted on the EENet’s website following the presentation.
• Please remember to mute your computer speakers
• Please also remember to mute your telephones until the Q/A session (*1).
• We would appreciate having your feedback on today’s knowledge exchange webinar. An online survey will be sent to you after the webinar. Thanks in advance for the 5 minutes of your time to complete our online feedback survey.

BC’s Drug Treatment Funding Program Systems Initiative Overview
Strengthening Substance Abuse Treatment Systems Evidence-based System Change Using a Change Management Model
April 19, 2012

OutlineBackground about BC’s Drug Treatment Program (DTFP) Systems Initiative
BC context Overall goal
Key concepts Residential Standards
BackgroundKE to support developmentKE to support implementation

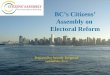
BC Context
8
1. Interior
6. Provincial Health Services (province-wide)
3. Vancouver Coastal4. Vancouver Island
2. Fraser
BC Health Authorities
5. Northern

BC Approach to DTFP Systems Opportunity
Proposal development & initiative managementOpen, transparent, consultative collaborative, adaptive processes Whole systems approach
9

Addiction Knowledge Exchange Team – Collective Stewardship
BC Mental Health & Addiction Services/Provincial Health Services Authority: Co-lead, Shannon Griffin (& project executive lead)Fraser Health Authority: Leader, Marika Sandrelli; Co-lead, Sherry Mumford Vancouver Coastal Health Authority: Leader, Mary Marlow; Co-lead, Yasmin JethaInterior Health Authority: Leader, Kat Hinter/Tara Mochizuki; Co-lead, Cliff Cross, Rae SamsonNorthern Health Authority: Leader, Franca Petrucci; Co-leads, Jim CampbellVancouver Island Health Authority: Leader, Paula Beltgens(Youth)/Chris Goble (Adult); Co-leads, Michelle Dartnall, Janet James, Jan DorlandCentral Team: Program Manager, Jane Collins, Data Analyst, Kristy Hoyak, Admin Asst., Corinne NewellMinistry of Health: Amanda Seymour, Ministry Lead on project

Overall Goal BC’s Drug Treatment Funding Program (DTFP) Strengthening Systems Initiative
Build an addiction knowledge exchange (KE) infrastructure that facilitates the implementation and support of evidence-informed practice and knowledge exchange (KE) activities, and fosters linkages across the system of substance use services and supports in BC.

Knowledge Exchange
12
In search of a KE formula …

Key Concepts
Knowledge exchange (KE) is generally understood as the co-creation of situations, conditions, and ecologies that support a culture of shared learning through knowledge creation, translation, dissemination, uptake, and evaluation.
KE infrastructure is the tangible, tactile, tools, structures, scaffolding, etc. The space to do the work, and the people to move things forward
KE mechanisms are the conceptual approaches guiding the work. The collaborations, frameworks, approaches that are developed to inform decisions and processes.

Knowledge Continuum
14
Achterbergh, Jan & Vriens, Dirk (May-June 2002). “Managing viable knowledge.” Systems Research and Behavioral Science. V19 i3 p223(19).

Conceptual Frame KE to Support
Interconnected KE streamsWorkforce capacity development
Systems-level frameworks, standards, policy, protocol development
15

Key Ingredients – what we’ve learned that makes a difference
LeadershipAdaptabilityRenewal & Regeneration Collaboration
16
Leadership
Renewal & Regeneration
AdaptabilityCollaboration

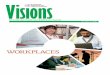
ExampleAddiction KE infrastructure – Fraser Health
Before DTFP Implemented (June 2008-Nov 2009)
After DTFP Implemented (Nov 2009 – March 2011)
Motivational Dialogue ChampionExisting addiction service networkAddiction Services Leadership
Contracted worksite / teamExecutive LeadershipDirect service worksite / teamtext

18
Examples – KE Tools

Whole Systems ApproachKE Infrastructure - Cross sector involvement

Whole Systems ApproachKE Infrastructure - Cross sector involvement

Whole Systems ApproachKE Mechanisms - Cross sector involvement

Residential Standards
Residential Standards
Background
KE to support development
KE to support implementation
22

Residential Standards
Background2008
Provincial review2009
Exploration of practices aligned with National Treatment Strategy principlesExploration of mechanisms to support practice
23

Residential Standards
2009/10 - KE to support development-How
A working group (Ministry of Health & Health Authority representatives)Research + evidence review + debate & discussion } Draft Standards
24

Residential Standards
KE to support development - HowKE forums - inclusive of service provider and clients’ voices, experiences and wisdom
held in each region Stakeholder (service providers, clients and families, cross sector partners) review and feedback
25

Residential Standards20011 – KE to develop standards - What
26
http://www.health.gov.bc.ca/library/publications/year/2011/youth-residential-treatment-standards.pdfhttp://www.health.gov.bc.ca/library/publications/year/2011/adult-residential-treatment-standards.pdf

Residential Standards
KE to support implementationStandards
Some are specific, concrete, pragmatic – relating to physical setting, & covered in other standards (e.g., public health standards, community care licensing, building code)Standards of excellence & aspiration
27

Residential Standards
KE to support implementationAppreciative inquiry
Appreciative of applied competence, that understands programs and their processes are developmental phenomena that are built on a knowledge exchange strategyAppreciative inquiry interview protocolValidation – representative sample of 7 sites
28

Interviewing process
Semi-structured interview about Meaning and missionThe place of standardsApplying the standards
27 interviews of approximately 90 minutes eachAdministrators, supervisors, line staff
29

Emerging ideas and themes…
Proximity counts! As predicted by other research, key influence to practice is the local culture—which is the centre itselfInformants seemed to approach the inquiry as “one more task”, but ended the encounter with apparent enthusiasm—”I got much more from this than I expected!”
30

Residential Standards
Emerging themes to inform development of KE to support implementation
Value of space to talk about practiceIdentity with programCommunityConnection – relationshipsComplexity
31

A major tension …
Being as inclusive as possible about intake…at the same time keeping the milieu safe…and keeping participants focused on the program, not on “what’s going to happen to me after this ends?”
32

Policy sets a context, but
Viable solutions tend to be specific to RelationshipsSystemic contextProgram precedent and philosophy
Professional identity seems to be tied to the residential program, and not to traditional titles like “nurse”, “social worker”
33

“Co-ocurring” disorders ….
Intake assessments have (perhaps necessarily) limited validityMental health issues emergeApproaches are highly variable, but programs with strong consultative support seem to cope better
34

One problem, many approaches
At what point is a resident invited to leave?Wide range of policies, opinions, and proceduresCommon theme: leave room for another approach or for trying againOne of many examples of how KE tools and forums may be of immense value
35

Residential Standards
Exploring for 2012/13Expanding appreciative inquiry Engaging non-funded residential facilitiesEngaging referral agentsCo-creating KE tools (DVD, practice guide)Facilitating a provincial face-to-face meeting with residential service providers to explore on-going learning from each other
36

Thank you
Questions?
37

Thanks to all participants for joining us today!
EENet would also like to give a special thanks to Jane Collins,
Amanda Seymour and Glen Griggfor co‐hosting today’s
presentation!

For upcoming KE webinars, please visit:http://evidenceexchangenetworkproject.wordpress.com/
The recording of today’s webinar also posted on EENet’s website.