Embed Size (px)
Citation preview
COSMETIC
A Long-Term Study of Outcomes,Complications, and Patient Satisfactionwith Breast Implants
Neal Handel, M.D.Tracy Cordray, M.D.
Jaime Gutierrez, M.D.J. Arthur Jensen, M.D.
Los Angeles, Calif.
Background: Breast implants have been used worldwide for more than 40 years.Despite extensive clinical experience, there is continued concern about thesafety of these devices. The purpose of this study was to compare the efficacy,complication rates, frequency of reoperation, and degree of patient satisfactionwith different types of implants.Methods: This is a consecutive, population-based study consisting of all patientsreceiving implants at a multidisciplinary breast center between 1979 and 2004(25 years). A prospective implant database was constructed and maintained inExcel, and statistical analysis was performed using SAS 8.2. Various outcomes,including infections, hematomas, undesirable waviness, capsular contracture,deflation, rupture, reoperation, and patient satisfaction, were monitored.Results: Data were collected on 3495 implants in 1529 women. The longerimplants were in place, the greater the cumulative risk of developing contrac-ture; hematoma significantly increased the risk of contracture; smooth andtextured implants had similar contracture rates; polyurethane foam–coveredimplants had a reduced risk of contracture persisting for at least 10 years afterimplantation. There was a relatively high rate of reoperation and a relativelyshort interval between primary surgery and reoperation; the most commonindication for reoperation was capsular contracture. Implant recipients ex-pressed a high overall level of satisfaction.Conclusions: Breast implants are associated with a significant rate of localcomplications and reoperation. There are marked differences in outcomes asa function of implant surface type and surgical indication. Despite relativelyfrequent complications and reoperations, implant recipients are largelysatisfied. (Plast. Reconstr. Surg. 117: 757, 2006.)
Silicone breast implants have been widelyused in the United States and throughoutthe world for more than four decades. Dur-
ing this time, there has been growing concernabout the safety of these devices, with regard toboth local complications and possible systemiceffects. A large body of scientific literature hasbeen published addressing a possible associationbetween silicone implants and cancer.1–6 Thereis overwhelming epidemiologic evidence thatwomen with implants are not at increased riskfor primary or recurrent breast cancer or othertumors.7–11 In fact, some studies suggest a lower
rate of breast cancer in augmented women.12–16
Similarly, there is abundant literature demon-strating lack of an association between siliconebreast implants and immune diseases or any sys-temic illness.17–24
In contrast, recent studies have documented asignificant incidence of local complications andside effects from breast implants.25–45 It has alsobeen determined that a relatively large propor-tion of implant patients require revisionalsurgery.46–51 Long-term follow-up of breast im-plant recipients is difficult for several reasons.Patients who believe they are doing well havelittle incentive to return for routine reexamina-tion. Patients who are dissatisfied often seekopinions (and subsequent treatment) from an-other physician. Also, the population in theUnited States is mobile; thus, over time, patientsfrequently relocate and may be difficult to con-tact. Implant registries and large-scale manda-
From the Division of Plastic Surgery, David Geffen School ofMedicine, University of California.Received for publication February 7, 2005; revised April 6,2005.Copyright ©2006 by the American Society of Plastic Surgeons
DOI: 10.1097/01.prs.0000201457.00772.1d
www.plasreconsurg.org 757

tory trials have only recently been established.Even in national manufacturer-sponsored stud-ies, only a relatively small proportion of patientscomplete the desired follow-up.52–54 For all thesereasons, our knowledge of complication ratesand outcomes following breast implant surgeryremains imprecise. The purpose of the currentstudy was to investigate long-term outcomes,complications, reoperation rates, and patient sat-isfaction among breast implant recipientstreated in a single practice and followed for aslong as 25 years.
PATIENTS AND METHODSThis is a population-based study consisting of
all implant recipients operated on at a multidis-ciplinary breast center (The Breast Center, VanNuys, Calif.) and in a subsequent solo plastic sur-gery practice. The population consists of a con-secutive series of women undergoing breast im-plant surgery during the 25-year period betweenJune of 1979 and June of 2004. All patients re-ceiving implants for cosmetic, reconstructive, orrevisional surgery were included. Reconstructivesurgery was defined as any case where an implantwas used (with or without preceding tissue expan-sion) to restore a breast disfigured by cancer treat-ment. Revisional surgery included all patients(cosmetic or reconstructive) undergoing second-ary implant procedures, regardless of the indica-tion for surgery. Women who were evaluated ortreated at our center for conditions related tobreast implants inserted elsewhere were excludedbecause of the difficulty in obtaining reliable in-formation about implant procedures performedat other facilities.
All surgical procedures were performed byone of two board-certified plastic surgeons work-ing as part of an integrated, multidisciplinary“team.” There was consistency in the care pro-vided, both from surgeon to surgeon and overtime (e.g., the two surgeons used similar operativetechniques, administered antibiotics uniformly,applied similar dressings, used the same postop-erative instructions, and scheduled follow-up visitsin a consistent manner). Implant patients werenever “discharged” or told to “return prn”; allpatients were given appointments for follow-upindefinitely over the course of this study. Patientswere not charged for follow-up visits.
A prospective breast implant database was es-tablished in January of 1990. To incorporate datarelating to implants inserted before inception ofthe database, information was obtained fromchart review of all patients who underwent im-
plantation between June of 1979 and December of1989 (1122 implants in 508 women). The protocolfor chart review called for extraction of data re-lating to patient demographics, details of the sur-gical procedure, type of implant, early and latepostoperative complications, degree of capsularcontracture at intervals, and laboratory and mam-mographic findings. As charts were reviewed, find-ings were entered onto custom-designed datasheets and subsequently transferred into a com-puterized database.
The database was updated in 2003 to 2004 byperforming a comprehensive record review of allimplant recipients for whom charts were available.Data extraction forms were created in collabora-tion with the Department of Biomathematics atthe University of California, Los Angeles School ofMedicine. The data abstraction forms were de-signed to collect demographic information, con-firm details of the surgical procedure, and mon-itor postoperative complications. The databasewas further enhanced with information obtainedfrom a comprehensive patient questionnaire. Thebreast implant questionnaire, also devised in col-laboration with the University of California, LosAngeles Department of Biomathematics, con-sisted of a 21-question instrument designed to so-licit information about patient demographics, im-plant-related complications (including degree ofcapsular contracture), and level of patient satis-faction. Because many patients in this series hadmultiple implants over time, the questionnairecalled only for information relating to the currentimplant(s) or, in the case of explanted patients,the most recent implant(s). The date of implan-tation of the device in question was provided onthe questionnaire to avoid ambiguity. In cases ofbilateral implants, information was collected sep-arately for the right and left sides.
A total of 1555 questionnaires were mailedbetween May of 2003 and May of 2004. The postoffice returned 702 questionnaires (nondeliver-able/incorrect addresses). It is believed that 853questionnaires were delivered to recipients. A per-sistent effort was made to encourage patients tocomplete and return questionnaires. This in-cluded remailing questionnaires in all cases wherethe original questionnaire was not returned by thepost office or completed by the patient, and tele-phone calls to patients who failed to return ques-tionnaires. As a result of these measures, a total of429 patients (50 percent) ultimately completedand returned questionnaires.
For purposes of this study, each breast implantwas considered separately and its history tracked
Plastic and Reconstructive Surgery • March 2006
758

from the date of insertion until the date of ex-plantation or the last follow-up visit. In patientswho underwent revisional surgery with insertionof a new implant, a new record was created to trackcomplications and outcomes related to the newdevice. In the relatively few cases where surgery(e.g., capsulotomy) was performed and the sameimplant reinserted, the prior record pertaining tothat device was terminated (censored) and a newrecord was created to track the implant from thedate of reinsertion.
Patients with Baker grade 1 or 2 capsules weredefined as free of contracture, and patients withBaker grade 3 or 4 capsules were considered tohave significant contracture. The date of onset ofcontracture was defined as the date a Baker 3 or4 capsule was first documented in the medicalrecord. In the case of patients who self-reportedsignificant contracture (by means of the breastimplant questionnaire), the date of onset was con-sidered to be the date the questionnaire was com-pleted. Contracture rates were expressed in termsof incidence per 1000 patient-months of observa-tion. In addition, the incidence of contractureover time was evaluated using the Kaplan-Meiermethod of survival analysis. In applying theKaplan-Meier method to the study of capsular con-tracture, the assumption was made that when im-plants are placed bilaterally, each is independentof the other with regard to the risk of contracture.This is in accordance with the current prevailingview.55
Complications that tended to occur over a dis-crete time frame in the early postoperative period(e.g., hematoma, infection) were evaluated basedon occurrence as a function of the total numberof cases (raw rate), whereas complications thatoccur over a longer time frame (e.g., implant de-flation, rupture, contracture) were calculated inrelation to the total number of patient-months ofrisk.
Hematoma was diagnosed if there was signif-icantly greater than expected bruising, swelling,and firmness of the breast or if surgical explora-tion revealed the presence of excessive bloodaround the implant. Infection was considered tohave occurred if there were symptoms of abnor-mal swelling, erythema, tenderness, and fever thateither resolved with antibiotics or required ex-plantation. Culture and sensitivity studies were ob-tained when possible to confirm suspected infec-tions. Untoward outcomes such as excessivewaviness or rippling were considered to have oc-curred when the degree of deformity was beyondwhat would normally be expected in a particular
clinical setting, required surgical revision, or wasself-reported by patients as being problematic.
Rupture of silicone gel implants was based onclinical confirmation at the time of explantation.The diagnosis of gel implant rupture was not madeon the basis of mammography, ultrasound, ormagnetic resonance imaging findings. The diag-nosis of saline implant deflation was made fromphysical examination and was confirmed at thetime of implant replacement.
The rates of reoperation, and the indicationsfor revisional surgery, were determined from re-view of progress notes and operative reports. Pa-tient satisfaction was ascertained from medicalrecords and from responses on the breast implantquestionnaire. Patients were given the opportu-nity to rate their overall satisfaction on a five-pointscale, with 1 being least satisfied and 5 being mostsatisfied.
The database was constructed and maintainedin Excel (Microsoft Corp., Redmond, Wash.) andstatistical analysis was performed using SAS 8.2(SAS Institute, Inc., Cary, N.C.). Outcomes werecompared among surgical procedures, differentsurfaces, and different fillers. For comparing theincidence of contracture over time, the Kaplan-Meier method of survival analysis (the log ranktest) was used. This methodology is ideal for study-ing progressive phenomena such as contracturebecause it allows for staggered entry of cases intothe trial and irregular loss to follow-up. With theKaplan-Meier method, only actual observationsare used to determine contracture rates; implantsare eliminated from consideration (censored) asof the date contracture occurs or beyond the dateof the last follow-up visit. Because there are mul-tiple levels of procedures, surfaces, and fillers, theoverall log rank tests do not spotlight where dif-ferences occur; thus, additional log rank tests wereperformed to compare only two of the groups ata time. These are reported after the overall testsamong the multiple groups.
For shorter term outcomes such as infection,overall comparisons were performed using chi-square tests for differences in percentages acrossthe multiple groups. For these outcomes, two ofthe groups were compared by using contrast state-ments in logistic regression. The p values fromthese contrasts are reported after the overall chi-square tests, showing one p value for each two-group comparison. For patient satisfaction, mea-sured on a five-point scale, nonparametricstatistics were used. For the overall model, theKruskal-Wallis test was used. Additional compari-
Volume 117, Number 3 • Breast Implants
759

sons between two groups were made using theWilcoxon rank sum test.
RESULTSThis study yielded information on a total of
1529 patients and 3495 implants. Occasionally, ananalyzed measure has missing data for a few im-plants, which were therefore excluded fromcounts as deemed appropriate. The study in-cluded 825 augmentation patients who received1601 implants, 264 breast reconstruction patientswho received 352 implants, and 695 implant re-vision patients who received a total of 1534 im-plants. Follow-up ranged from 0 to 280 months(23.3 years), with a mean follow-up (per implant)of 37.4 months.
A variety of implants were used over the courseof this study, including 1137 saline-filled devices,778 double-lumen (gel/saline) prostheses, 1537silicone gel-filled implants, and 38 implants withother fillers (e.g., Trilucent, Misti Gold). With re-gard to surface texture, there were 2067 smoothimplants, 848 mechanically textured prostheses,and 568 polyurethane foam-covered devices (Ta-ble 1).
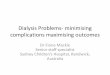
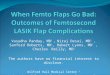
The occurrence of capsular contracture wasstudied as a function of the type of procedureperformed and the surface texture of the implant.Contracture rate (Baker grade 3 or 4 per 1000patient-months) was 1.99 after augmentation, 5.37after breast reconstruction, and 4.36 after implantrevision surgery. The rate of significant contrac-ture was 3.85 with smooth implants, 3.23 with tex-tured implants, and 2.19 with polyurethane foam–covered implants. Survival analysis curves weregenerated using the Kaplan-Meier methodology.These graphs depict the likelihood of remainingcontracture-free over time as a function of type ofsurgical procedure and implant surface charac-teristics (Figs. 1 and 2). Reliable data were avail-able out to 10 years of follow-up.
Hematoma was least frequent following breastaugmentation, occurring in 24 of 1601 (1.50 per-cent) implants; more frequent after implant revi-sion surgery, occurring in 29 of 1534 (1.89 per-cent) implants; and most common in associationwith breast reconstruction, occurring in 10 of 352(2.84 percent) implants. Chi-square analysis andpairwise tests revealed no statistically significantdifference in the incidence of hematoma as a func-tion of the type of surgical procedure performed.Hematoma was also studied as a function of im-plant surface texture. Hematoma occurred in 35of 2067 (1.69 percent) smooth implants, 15 of 848(1.77 percent) textured implants, and 13 of 568(2.29 percent) polyurethane foam–covered im-plants. Chi-square analysis and pairwise testsshowed no significant difference in the incidenceof hematoma as a function of implant surface tex-ture.
The effect of hematoma on the risk of devel-oping contracture was studied by comparing thecontracture rate for implants with and withoutassociated hematomas. Contractures occurred in12 of 63 implants where there was a hematomacompared with 412 of 3432 implants without he-matoma. The contracture rate (number of Bakergrade 3 or 4 contractures per 1000 patient-months) was 7.17 for implants with hematoma and3.27 for implants without hematoma. This was asignificant difference (Kaplan-Meier log rank test,p � 0.0068). The relative risk for contracture inthe event of hematoma was 2.19.
Infection rates were determined in relation toprocedure type and were noted to occur in 19 of1601 implants (1.2 percent) used for augmenta-tion, 16 of 352 of implants (4.6 percent) used forbreast reconstruction, and 32 of 1534 of implants(2.1 percent) used for secondary revisions (Table2). When infections were categorized as a functionof implant surface texture, they were noted tooccur in 30 of 2067 smooth implants (1.5 per-cent), 24 of 848 textured implants (2.8 percent),
Table 1. Implant Characteristics
Augmentation (n � 1601) Reconstruction (n � 352) Revision (n � 1534) Total* (n � 3495)
TextureSmooth 1138 206 717 2067Textured 265 34 548 848Polyurethane foam 194 107 266 568
FillerSaline 743 64 324 1137Double-lumen 398 144 236 778Silicone gel 446 140 949 1537Other 12 3 23 38
*The counts in the column for totals may exceed the row total because of a few implants with missing data. There were eight implants withmissing surgery type, 12 with missing surface, and five with missing filler; some were missing two characteristics.
Plastic and Reconstructive Surgery • March 2006
760

and 11 of 568 polyurethane foam–covered im-plants (1.9 percent) (Table 2).
Excessive waviness and/or rippling occurredleast frequently with implants used for augmen-tation [91 of 1601 (5.7 percent)], more frequentlywith implants used for reconstruction [27 of 352(7.7 percent)], and most frequently when im-plants were used in revision surgery [182 of 1534
(11.9 percent)] (Table 3). The risk of undesirablewaviness was also related to implant surface tex-ture, occurring in 143 of 2067 of smooth implants(6.92 percent), 38 of 568 of polyurethane foamimplants (6.69 percent), and 120 of 848 of tex-tured implants (14.15 percent) (Table 3).
Saline implant deflations occurred in nine of943 smooth surface implants and 13 of 192 tex-
Fig. 1. Kaplan-Meier analysis of the risk of significant (Baker grade 3 or 4) capsular contracture asa function of the type of surgical procedure performed (all implant surfaces). Log rank test, p �
0.0001; augmentation versus reconstruction, p �0.0001; augmentation versus revision, p �0.0001;reconstruction versus revision, p � 0.088.
Fig. 2. Kaplan-Meier analysis of the risk of significant (Baker grade 3 or 4) capsular contracture asa function of implant surface characteristics (all surgical procedures). Log rank test, p � 0.0009;polyurethane foam versus smooth, p � 0.0003; polyurethane foam versus textured, p � 0.0159;smooth versus textured, p � 0.1093.
Volume 117, Number 3 • Breast Implants
761

tured implants. When deflation rates were calcu-lated as a function of the number of patient-months at risk, the rate was 0.34 (per 1000 patient-months) for smooth implants and 2.07 fortextured implants (Table 4). Silicone implant rup-tures occurred in 14 of 1123 smooth implants, sixof 618 textured implants, and eight of 568 poly-urethane foam–covered implants. When calcu-lated in terms of risk of rupture as a function oflength of follow-up, the rate was 0.308 (rupturesper 1000 patient-months) for smooth implants,0.308 for textured implants, and 0.260 for poly-urethane foam implants (no statistically signifi-cant difference) (Table 5).
Reoperation rates (for any reason) were stud-ied as a function of procedure type. For implantsused in breast augmentation, 248 of 1601 (15.5percent) required subsequent revision; when usedfor breast reconstruction, 125 of 352 (35.5 per-cent) underwent reoperation; and when used inrevisional surgery, 336 of 1534 (21.9 percent) re-quired subsequent reoperation (Table 6). Themean duration between operation and revisionsurgery was determined for various procedures. Itwas shortest (16.0 months) in breast reconstruc-tion, longer (38.9 months) following breast revi-sion surgery, and longest (49.1 months) afterbreast augmentation (Table 7). When the meanduration between surgery and subsequent revisionwas analyzed as a function of implant surface tex-ture, it was approximately the same for smooth(36.9 months) and textured (35.5 months) im-plants but significantly longer for polyurethanefoam–covered implants (47.8 months) (Table 7).The most frequent reasons for reoperation werecapsular contracture (56 percent), size change (22percent), and implant malposition (8 percent)(Table 8).
The overall level of patient satisfaction washigh. When gauged as a function of proceduretype, mean satisfaction (scale of 1 to 5) was some-what higher following augmentation (4.40) thanfollowing breast reconstruction (4.00) or implantrevision surgery (4.02) (Table 9). There was nostatistically significant difference in self-assessedpatient satisfaction as a function of implant fillermaterial (saline versus gel). Smooth implants re-ceived higher satisfaction scores than textured(p � 0.0003) and polyurethane foam–covered de-vices (p � 0.0287).
DISCUSSIONThis population-based, long-term follow-up
study of implant recipients reveals significantdifferences in outcome as a result of type ofprocedure performed and type of implant used.Our findings confirm the widely held belief thatcapsular contracture is least frequent afterbreast augmentation, more frequent after revi-sional surgery, and most frequent after breastreconstruction.26,56 –59 Curves from Kaplan-Meiersurvival analyses reveal that contracture is a pro-gressive phenomenon, and the longer any groupof patients is followed, the greater the cumulativerisk of developing contracture. This contradictsthe widely held belief that if patients remain con-tracture-free for a year or two they probably willnot develop significant contracture.60 This findingmay also have some relevance in understandingthe cause of capsular contracture. If the risk ofcontracture persists for many years after implan-tation (as it appears to), it seems less likely that itis related to acute events such as bacterial con-tamination, surgical technique, drains, antibiotics,or other ancillary measures that have a short-term
Table 3. Abnormal Waviness and Rippling
Total
Wavy or Rippling
No. %
Procedure*Augmentation 1601 91 5.7Reconstruction 352 27 7.7Revision 1534 182 11.9
Surface Type†Smooth 2067 143 6.92Polyurethane 568 38 6.69Textured 848 120 14.15
*Overall p � 0.0001; augmentation versus reconstruction, p � 0.1583;augmentation versus revision, p � 0.0001; reconstruction versus re-vision, p � 0.0250.†Overall p � 0.0001; polyurethane versus smooth, p � 0.8492; poly-urethane versus textured, p � 0.0001; smooth versus textured, p �0.0001.
Table 2. Infection
No. ofImplants
No. ofInfections
ImplantsInfected
(%)
Procedure*Augmentation 1601 19 1.2Reconstruction 352 16 4.6Revision 1534 32 2.1
Implant Surface†Smooth 2067 30 1.5Polyurethane 568 11 1.9Textured 848 24 2.8
*Overall p � 0.0001; pairwise: augmentation versus reconstruction,p � 0.0001; augmentation versus revision, p � 0.0496; reconstructionversus revision, p � 0.0100.†Overall p � 0.0437; foam versus smooth, p � 0.4095; foam versustextured, p � 0.2913; smooth versus textured, p � 0.0138.
Plastic and Reconstructive Surgery • March 2006
762

impact and more likely related to some chroniceffect of implants on adjacent tissue.
Our findings further substantiate previous re-ports on the superiority of polyurethane foam–covered implants in reducing the risk of contrac-ture compared with smooth or texturedimplants.61–63 At the end of 10 years of observation,among patients for whom data were available, 75percent of those with polyurethane implants re-mained contracture free compared with 65 per-cent with either smooth or textured implants. Inall categories considered—augmentation, revi-sional surgery, and breast reconstruction—poly-urethane implants proved superior regarding re-duction of contracture. These findings confirmearlier reports on the benefit of the polyurethanefoam in reducing the incidence of contractureand document the long-term duration of this ef-fect. Polyurethane-covered devices were voluntar-ily withdrawn by the manufacturer from the U.S.market in 1992; however, approximately 110,000foam-covered implants were inserted in theUnited States before distribution was discontin-ued, and they continue to be widely used in Eu-rope and South America.
In our study, textured implants had a slightlylower risk of developing significant (Baker grade3 or 4) contracture than smooth implants. Thedifference, however, was not statistically signifi-cant, and as patients were followed for a longerperiods of time, the difference became less ap-parent. Although there were initial reports in theliterature that mechanical surface texturing ofbreast implants reduced the incidence ofcontracture,64–66 more recent studies have sug-gested that there is no significant difference be-tween smooth and textured devices.26,67–69 Nega-tive effects of textured breast implants include a
greater propensity to cause visible rippling andwaviness and a higher rate of saline implant de-flation. Both of these observations have previouslybeen reported in the literature26,44,70,71 and areconfirmed by the current study.
It has become increasingly apparent in recentyears that breast implant recipients experience asignificant incidence of complications and a rel-atively high rate of reoperation.46–51,72 In large-scale follow-up studies conducted by manufactur-ers, it was reported that by the end of 5 years,women undergoing augmentation with saline-filled implants had a 10 percent rate of significant(Baker grade 3 or 4) contracture, approximatelya 10 percent incidence of deflation, and evenhigher rates of wrinkling and breast pain. Between20 and 25 percent of saline-augmented patientsunderwent reoperation within the first 5 years.54,72
Complications associated with silicone gel im-plants were even more prevalent.31,73,74 Accordingto manufacturers, at the end of 3 years, womenundergoing gel implant reconstruction had a 20percent risk of contracture (Baker grade 3 or 4),nearly a 30 percent risk of implant removal/re-placement, and an overall reoperation rate of 45to 50 percent.53
The findings in our implant population weresimilar. We noted a high overall rate of reopera-tion. The lowest rate (15.5 percent) and longestmean duration to reoperation (49.1 months) wasamong augmentation patients; the highest rate(35.5 percent) and shortest mean duration to re-operation (16.0 months) was among breast recon-struction patients. The mean duration to reopera-tion also varied as a function of implant surfacetexture. The longest mean duration was with poly-urethane foam–covered implants (47.8 months),and the mean duration was nearly identical withsmooth (36.9 months) and textured (35.5months) implants. It is likely that the longer meanduration until reoperation in cases with polyure-thane foam–covered implants is related to thereduced tendency to develop clinically significantcontracture.
Table 4. Saline Deflation*
Surface No. DeflationsRate per 1000Patient-Months
Smooth 943 9 0.34Textured 192 13 2.07*p � 0.0001.
Table 5. Silicone Rupture*
Implant Surface No.No. of
RupturesRate per 1000Patient-Months
Smooth 1123 14 0.308Textured 618 6 0.308Polyurethane 568 8 0.260*p � 0.1379.
Table 6. Reoperation Rates*
Having Revision
Procedure Total No. %
Augmentation 1601 248 15.5Reconstruction 352 125 35.5Revision 1534 336 21.9*Overall p � 0.0001; augmentation versus reconstruction, p� 0.0001;augmentation versus revision, p� 0.0001; reconstruction versus re-vision, p� 0.0001.
Volume 117, Number 3 • Breast Implants
763

The reasons for reoperation among our pa-tients were similar to the reasons previously re-ported by manufactures. In our series, the mostcommon overall indication for reoperation wascapsular contracture and the second most com-mon was size change. In manufacturers’ studies,the most common reason for reoperation afterbreast augmentation was size/style change andthe most common reason after breast reconstruc-tion was capsular contracture.
Despite a relatively high rate of complicationsand the relatively frequent need for reoperation,breast implant recipients are largely satisfied.Among our patients, the highest level of satisfac-tion was in augmentation patients, but other cat-egories reported favorable satisfaction rates aswell. This high level of patient satisfaction amongimplant recipients has been observed and re-ported by others.40,75,76
Limitations of This StudyBy their very nature, clinical studies have in-
herent limitations. Historically, it has been diffi-cult to obtain long-term follow-up on implant re-cipients. As in all clinical trials, some of our
patients were lost to follow-up. In this particularstudy, however, there were some unique advan-tages. The majority of our patients were treated ata multidisciplinary “breast center” where many ofthem returned annually for screening mammog-raphy. This provided an opportunity to evaluatetheir implants. The majority of cancer patientsundergoing breast reconstruction received theirmedical and surgical oncology follow-up at ourcenter. These patients were seen on a regular basisand the reconstructed breast was routinely evalu-ated. This unique clinical setting provided an op-portunity for long-term follow-up not encoun-tered in the typical clinical practice.
Determining the degree of capsular contrac-ture is always subjective to some extent. The Bakergrading system has been universally adopted forthis purpose and is widely used in the publishedliterature. In our study, Baker grade was ascer-tained by one of two board-certified plastic sur-geons; determination of the degree of contracturewas performed in accordance with the gradingcriteria specified by Baker.77 In an effort to obtaineven longer term follow-up on patients who wouldnot or could not return for personal examination,patients were canvassed with an implant question-naire. Patients were asked to record the degree ofcontracture on each side; the criteria for the Bakergrading system were clearly explained in lay termson the questionnaire. However, there is always thepossibility that the grade assigned by the patientmight differ from that assigned by an independenttrained examiner. It should be emphasized thatthese “self-evaluations” were not a substitute forexamination by the plastic surgeon; they wereused to obtain follow-ups of longer duration andsupplement the data in the medical records. Anumber of the implant questionnaires were actu-ally completed at the time of a follow-up visit, inwhich case the Baker grade was determined by theexamining plastic surgeon and entered onto thequestionnaire by the nurse.
There have been gradual changes in the de-sign of implants over time. As a result, some of thegroupings of implants designated for comparison
Table 8. Reasons for Reoperation in 514 ImplantReplacements
Reason No. of Cases %
Contracture 286 55.6Size change 112 21.8Malposition 42 8.2Waviness 22 4.3Deflation 21 4.1Infection 14 2.7Ruptured gel 8 1.6Palpability 4 0.8Anxiety 2 0.4
Table 9. Patient Satisfaction*
Procedure Type No. Average Level of Satisfaction
Augmentation 494 4.40Reconstruction 48 4.00Revision 562 4.02*Patients ranked satisfaction on a scale of 1 to 5, where 1 � leastsatisfied and 5 � most satisfied. Overall p � 0.0001; augmentationversus reconstruction, p � 0.0029; augmentation versus revision, p �0.0001; reconstruction versus revision, p � 0.6316.
Table 7. Mean Duration between Surgery andReoperation
No. ofReoperations
Mean Duration(months)
Procedure*Augmentation 248 49.1Reconstruction 125 16.0Revision 336 38.9
Surface Type†Smooth 412 36.9Polyurethane 171 35.5Textured 125 47.8
*Overall p � 0.0001; augmentation versus reconstruction, p � 0.0001;augmentation versus revision, p � 0.0001; reconstruction versus re-vision, p � 0.0001.†Overall p � 0.0527; smooth versus textured, p � 0.7349; smoothversus polyurethane, p � 0.0257; polyurethane versus textured, p �0.0280.
Plastic and Reconstructive Surgery • March 2006
764

in this study may be nonhomogenous. For exam-ple, there were changes in the design of the fillervalve of saline implants that might have altered therate of deflation; likewise, there have beenchanges in the characteristics of the elastomershell of silicone gel implants that might affect therupture rate. This study reports on actual clinicalexperience with breast implants over an extendedperiod of time and reflects experience with prod-ucts that have gradually evolved. The conclusionsderived from our data are valid for the populationof implants observed over this time frame. It ispossible that our findings may not exactly predictthe behavior of breast implants currently in use orimplants that may be used in the future.
An implant questionnaire was mailed to allpatients, and we achieved a 50 percent responserate, which is higher than the rate reported inmost survey studies. We believe this high responserate was attributable to persistent efforts to contactpatients and encourage them to complete andreturn the questionnaire. However, there is thepossibility of some inherent difference betweenresponders and nonresponders; for example, thelevel of satisfaction might affect the likelihood ofa patient to respond. Although we believe the highoverall response rate contributes to the credibilityof our conclusions, we acknowledge the possibilityof selection bias that might impact our findings.
CONCLUSIONSBased on long-term follow-up of a large num-
ber of breast implant patients, we believe certainconclusions are warranted. Implant recipientshave a significant incidence of local complicationsand a relatively high rate of reoperation. The mostcommon overall indication for reoperation is cap-sular contracture. The incidence of symptomaticcapsular contracture does not diminish after 1 or2 years. The longer implants are in place, thegreater the cumulative risk for developing con-tracture. The occurrence of hematomas signifi-cantly increases the risk of developing contrac-ture.
Polyurethane foam–covered implants are as-sociated with a dramatically reduced rate of con-tracture for at least 10 years following implanta-tion. Polyurethane implants do not appear toincrease the risk of other complications such asinfection or rupture. Textured implants do notafford significant protection against contractureand are associated with an increased risk of wrin-kling and waviness and a higher rate of salineimplant deflation.
Among all groups of implant recipients, theoverall level of satisfaction is great despite a rela-tively high incidence of complications and rela-tively frequent need for revisions. We were unableto ascertain any difference in patient satisfactionas a function of filler material; smooth implantsreceived a higher satisfaction score than texturedimplants but were not statistically different frompolyurethane foam.
Neal Handel, M.D.427 W. Pueblo Street, Suite C
Santa Barbara, Calif. [email protected]
ACKNOWLEDGMENTS
The authors acknowledge the contributions of JeffreyGornbein, Dr.P.H., Department of Biomathematics,University of California, Los Angeles, who assisted indesign of the patient questionnaires and data extractionforms; and Rita Engelhardt, Dr.P.H., Department ofBiomathematics, University of California, Los Angeles,who assisted in analysis of data. Jamie Carter and JoyLindlief, O.R.T., were instrumental in collection andtabulation of data.
Jaime Gutierrez, M.D., was a fellow at the Divisionof Plastic Surgery at the University of California, LosAngeles Medical Center from July of 2002 to July of2003. Dr. Gutierrez spent approximately 20 percent ofhis time working with Dr. Handel in the capacity ofresearch assistant, and the Division of Plastic Surgeryreceived a grant from Polytech Silimed, a breast implantmanufacturer located in Dieberg, Germany, in anamount equal to 20 percent of Dr. Gutierrez’s salary.Tracy Cordray, M.D., was a fellow at the Division ofPlastic Surgery at University of California, Los AngelesMedical Center from July of 2003 to July of 2004. Dr.Cordray spent approximately 20 percent of her time work-ing with Dr. Handel in the capacity of research assistant,and the Division of Plastic Surgery received a grant fromPolytech Silimed in an amount equal to 20 percent of Dr.Cordray’s salary. The implant questionnaire and dataextraction forms used in this study were developed inconjunction with the Department of Biomathematics atUniversity of California, Los Angeles Medical Center(David Geffen School of Medicine). In addition, thestatistical analysis of data was performed by the Uni-versity of California, Los Angeles Department of Bi-omathematics. Polytech Silimed paid the costs for theseservices. The expenses incurred by Dr. Handel in pro-ducing and mailing patient questionnaires (photocopy-ing, postage, secretarial) were reimbursed by PolytechSilimed.
Volume 117, Number 3 • Breast Implants
765

REFERENCES1. Harris, H. I. Study of breast implants from the point of view
of carcinogenesis. Plast. Reconstr. Surg. 28: 81, 1961.2. Hoopes, J. E., Edgerton, M. T., and Shelley, W. Organic
synthetics for augmentation mammaplasty: Their relation tobreast cancer. Plast. Reconstr. Surg. 39: 263, 1967.
3. Brand, K. G. Risk assessment of carcinogenesis at implanta-tion sites. Plast. Reconstr. Surg. 66: 591, 1980.
4. Brand, K. G. Do implanted medical devices cause cancer?J. Biomater. Appl. 8: 325, 1994.
5. Kern, K. A., Flannery, J. T., and Kuehn, P. G. Carcinogenicpotential of silicone breast implants: A Connecticut statewidestudy. Plast. Reconstr. Surg. 100: 737, 1997.
6. Gerszten, K., and Gerszten, P. C. Silicone breast implants: Anoncologic perspective. Oncology 12: 1427, 1998.
7. Berkel, H., Birdsell, D. C., and Jenkins, H. Breast augmen-tation: A risk factor for breast cancer? N. Engl. J. Med. 326:1649, 1992.
8. Spear, S. L., Slack, C., and Howard, M. A. Postmastectomyreconstruction of the previously augmented breast: Diagno-sis, staging, methodology and outcome. Plast. Reconstr. Surg.107: 1167, 2001.
9. McLaughlin, J. K., Nyren, O., Blot, W. J., et al. Cancer riskamong women with cosmetic breast implants: A population-based cohort study in Sweden. J. Natl. Cancer Inst. 90: 156,1998.
10. Deapen, D. M., Pike, M. C., Casagrande, J. T., et al. Therelationship between breast cancer an augmentation mam-maplasty: An epidemiologic study. Plast. Reconstr. Surg. 77:361, 1986.
11. Deapen, D. M., Hamilton, A., Bernstein, L., et al. Breastcancer stage at diagnosis and survival among patients withprior breast implants. Plast. Reconstr. Surg. 105: 535, 2000.
12. Su, C. W., Dreyfuss, D. A., Krizek, T. J., et al. Silicone implantsand the inhibition of cancer. Plast. Reconstr. Surg. 96: 513,1995.
13. Bryan, H., and Brasher, P. Breast implants and breast cancer:Reanalysis of a linkage study. N. Engl. J. Med. 332: 1535, 1995.
14. Deapen, D. M., Bernstein, L., and Brody, G. S. Are breastimplants anticarcinogenic? A 14-year follow-up of the LosAngeles study. Plast. Reconstr. Surg. 99: 1346, 1997.
15. Malone, K. E., Stanford, J. L., Daling, J., et al. Implants andbreast cancer. Lancet 339: 1365, 1992.
16. Brinton, L. A., Malone, K. E., Coates, R. J., et al. Breastenlargement and reduction: Results from a breast cancercase-control study. Plast. Reconstr. Surg. 97: 269, 1996.
17. Tugwell, P., Wells, G., Peterson, J., et al. Do silicone breastimplants cause rheumatologic disorders? A systematic reviewfor a court-appointed national science panel. Arthritis Rheum.44: 2477, 2001.
18. Janowksy, E. C., Kupper, L. L., and Hulka, B. S. Meta-analysisof the relation between silicone breast implants and the riskof connective-tissue diseases. N. Engl. J. Med. 342: 781, 2000.
19. Strom, B. L., Reidenberg, M. M., Freundlich, D., et al. Breastsilicone implant and risk of systemic lupus erythematosus.J. Clin. Epidemiol. 47: 1211, 1994.
20. Englert, H. J., and Brooks, P. Scleroderma and augmentationmammaplasty: A causal relationship? Aust. N. Z. J. Med. 24:74, 1994.
21. Gabriel, S. E., O’Fallon, M., Kurland, L. T., et al. Risk ofconnective-tissue disease and other disorders after breastimplantation. N. Engl. J. Med. 330: 1697, 1994.
22. Sanchez-Guerrero, J., Colditz, G. A., Karlson, E. W., et al.Silicone breast implants and the risk of connective-tissuedisease and symptoms. N. Engl. J. Med. 332: 1666, 1994.
23. Angell, M. Shattuck lecture: Evaluating the health risks ofbreast implants. The interplay of medical science, the law,and public opinion. N. Engl. J. Med. 334: 1513, 1996.
24. Blackburn, W. D., and Everson, M. P. Silicone-associatedrheumatic disease: An unsupported myth. Plast. Reconstr.Surg. 99: 1362, 1997.
25. Rohrich, R. J., Adams, W. P., Jr., Beran, S. J., et al. An analysisof silicone gel-filled breast implants: Diagnosis and failurerates. Plast. Reconstr. Surg. 102: 2304, 1998.
26. Handel, N., Jensen, J. A., Black, Q., Waisman, J. R., andSilverstein, M. J. The fate of breast implants: A critical analysisof complications and outcomes. Plast. Reconstr. Surg. 96: 1521,1995.
27. Peters, W., Smith, D., and Lugowski, S. Failure properties of352 explanted silicone-gel breast implants. Can. J. Plast. Surg.4: 1, 1996.
28. de Camara, D. L., Sheridan, J. M., and Kammer, B. A. Rup-ture and aging of silicone gel breast implants. Plast. Reconstr.Surg. 91: 828, 1993.
29. Collis, N., and Sharpe, D. T. Silicone gel-filled breast implantintegrity: A retrospective review of 478 consecutively ex-planted implants. Plast. Reconstr. Surg. 105: 1979, 2000.
30. Duffy, M. J., and Woods, J. E. Health risks of failed siliconegel breast implants: A 30-year clinical experience. Plast. Re-constr. Surg. 94: 295, 1994.
31. Gabriel, S. E., Woods, J. E., O’Fallon, W. M., Beard, C. M.,Kurland, L. T., and Melton, L. J., III. Complications leadingto surgery after breast implantation. N. Engl. J. Med. 336: 677,1997.
32. Goldberg, E. P., Widenhouse, C., Marotta, J., and Martin, P.Failure of silicone gel breast implants: Analysis of literaturedata for 1652 explanted prostheses. Plast. Reconstr. Surg. 100:281, 1997.
33. Brown, S. L., Heflin, B., Woo, E. K., and Parmentier, C. M.Infections related to breast implants reported to the Foodand Drug Administration, 1977–1997. J. Long Term Eff. Med.Implants 11: 1, 2001.
34. Courtiss, E. H., Goldwyn, R. M., and Anastasi, G. W. The fateof implants with infections around them. Plast. Reconstr. Surg.63: 812, 1979.
35. Armstrong, R. W., Berkowitz, R. L., and Bolding, F. Infectionfollowing breast reconstruction. Ann. Plast. Surg. 23: 284,1989.
36. Nahabedian, M. Y., Tsangaris, T., Momen, B., et al. Infectiouscomplications following breast reconstruction with expand-ers and implants. Plast. Reconstr. Surg. 112: 467, 2003.
37. Leibman, A. J. Imaging of complications of augmentationmammaplasty. Plast. Reconstr. Surg. 93: 1134, 1994.
38. Slavin, S. A., and Goldwyn, R. M. Silicone gel implant ex-plantation: Reasons, results, and admonitions. Plast. Reconstr.Surg. 95: 63, 1995.
39. Cohen, B. E., Biggs, T. M., Cronin, E. D., et al. Assessmentand longevity of the silicone gel breast implant. Plast. Recon-str. Surg. 99: 1597, 1997.
40. Gutowski, K. A., Mesna, G. T., and Cunningham, B. L. Saline-filled breast implants: A Plastic Surgery Educational Foun-dation multicenter outcomes study. Plast. Reconstr. Surg. 100:1019, 1997.
41. Lavine, D. M. Saline inflatable prostheses: 14 years’ experi-ence. Aesthetic Plast. Surg. 17: 325, 1993.
42. McKinney, P., and Tresley, G. Long-term comparison of pa-tients with gel and saline mammary implants. Plast. Reconstr.Surg. 72: 27, 1983.
43. McGrath, M. H., and Burkhardt, B. R. The safety and efficacyof breast implants for augmentation mammaplasty. Plast.Reconstr. Surg. 74: 550, 1984.
Plastic and Reconstructive Surgery • March 2006
766

44. Cunningham, B. L., Lokeh, A., and Gutowski, K. A. Saline-filled breast implant safety and efficacy: A multicenter ret-rospective review. Plast. Reconstr. Surg. 105: 2143, 2000.
45. Holmich, L. R., Vejborg, I. M., Conrad C., et al. Untreatedsilicone breast implant rupture. Plast. Reconstr. Surg. 114: 204,2004.
46. Handel, N. Managing local implant-related problems. In S. L.Spear (Ed.), Surgery of the Breast: Principles and Art. Philadel-phia: Lippincott-Raven, 1998.
47. Netscher, D. T., Sharma, S., Thornby, J., et al. Aestheticoutcome of breast implant removal in 85 consecutive pa-tients. Plast. Reconstr. Surg. 100: 206, 1997.
48. Melmed, E. P. A review of explantation in 240 symptomaticwomen: A description of explanation and capsulectomy withreconstruction using a periareolar technique. Plast. Reconstr.Surg. 101: 1364, 1998.
49. Rohrich, R. J., Beran, S. J., Restifo, R. J., et al. Aestheticmanagement of the breast following explantation: Evalua-tion and mastopexy options. Plast. Reconstr. Surg. 101: 827,1998.
50. Handel, N. Managing complications of breast augmentation.In S. Shenaq (Ed.), Perspectives in Plastic Surgery. New York:Thieme Medical, 2001.
51. Hammond, D. C., Hidalgo, D., Slavin, S., et al. Revising theunsatisfactory breast augmentation. Plast. Reconstr. Surg. 104:277, 1999.
52. McLaughlin, J. K. Long-term follow-up of women with cos-metic breast implants: How long is long enough? Plast. Re-constr. Surg. 114: 801, 2004.
53. Summary of safety and effectiveness data: McGhan siliconefilled breast implants. PMA P020056, Inamed Corporation,Santa Barbara, Calif., 2003.
54. Saline filled breast implant surgery: Making an informeddecision, 102864-001 Rev A, January 2204. Mentor Corpo-ration, Santa Barbara, Calif., 2004.
55. Burkhardt, B. R. Comparing contracture rates: Probabilitytheory and the unilateral contracture. Plast. Reconstr. Surg. 74:527, 1984.
56. Mahler, D., and Hauben, D. J. Retromammary vs. retropec-toral augmentation: A comparative study. Ann. Plast. Surg. 8:370, 1982.
57. Hipps, C., Raju, D., and Straith, R. Influence of some oper-ative and postoperative factors on capsular contracturearound breast prostheses. Plast. Reconstr. Surg. 61: 384, 1978.
58. Luke, J. L., Kalasinsky, V. F., Turnicky, R. P., et al. Patho-logical and biophysical findings associated with siliconebreast implants: A study of capsular tissues from 86 cases.Plast. Reconstr. Surg. 100: 1558, 1997.
59. Brown, S. L., Parmentier, C. M., Woo, E. K., et al. Silicone gelbreast implant adverse event reports to the Food and DrugAdministration, 1984-1995. Public Health Rep. 113: 535, 1998.
60. Camirand, A., Doucet, J., and Harris, J. Breast augmentation:Compression. A very important factor in preventing capsularcontracture. Plast. Reconstr. Surg. 104: 529, 1999.
61. Melmed, E. P. Polyurethane implants: A 6-year review of 416patients. Plast. Reconstr. Surg. 82: 285, 1988.
62. Hester, T. R., Jr., Nahai, F., Bostwick, J., et al. A 5-year ex-perience with polyurethane-covered mammary prostheses
for the treatment of capsular contracture, primary augmen-tation mammoplasty, and breast reconstruction. Clin. Plast.Surg. 15: 569, 1988.
63. Handel, N., Silverstein, M. J., Jensen, J. A., et al. Comparativeexperience with smooth and polyurethane breast implantsusing the Kaplan-Meier method of survival analysis. Plast.Reconstr. Surg. 88: 475, 1991.
64. Hakelius, L., and Ohlsen, L. Tendency to capsular contrac-ture around smooth and textured gel-filled silicone mam-mary implants: A 5-year follow-up. Plast. Reconstr. Surg. 100:1566, 1997.
65. Burkhardt, B. R., and Demas, C. P. The effect of Siltextexturing and povidone-iodine irrigation on capsular con-tracture around saline inflatable breast implants. Plast. Re-constr. Surg. 93: 123, 1994.
66. Coleman, D. J., Foo, I. T. H., and Sharpe, D. T. Textured orsmooth implants for breast augmentation? A prospective,controlled trial. Br. J. Plast. Surg. 44: 444, 1991.
67. Asplund, O., Gylbert, L., Jurell, G., et al. Textured or smoothimplants for submuscular breast augmentation: A controlledstudy. Plast. Reconstr. Surg. 97: 1200, 1996.
68. Fagrell, D., Berggren, A., and Tarpila, E. Capsular contrac-ture around saline-filled fine textured and smooth mammaryimplants: A prospective 7.5-year follow-up. Plast. Reconstr.Surg. 108: 2108, 2001.
69. Tarpila, E., Ghassemifar, R., Fagrell, D., et al. Capsular con-tracture with textured versus smooth saline-filled implantsfor breast augmentation: A prospective clinical study. Plast.Reconstr. Surg. 99: 1934, 1997.
70. Worseg, A., Kuzbari, R., Tairych, G., et al. Long term resultsof inflatable mammary implants. Br. J. Plast. Surg. 48: 183,1995.
71. Schuster, D. I., and Lavine, D. M. Nine-year experience withsubpectoral breast reconstruction after subcutaneous mas-tectomy in 98 patients utilizing saline-inflatable prostheses.Ann. Plast. Surg. 21: 444, 1988.
72. Making an informed decision: Saline filled breast implantsurgery, 2002 Update, Inamed Aesthetics, Santa Barbara,Calif., 2002.
73. Mammary Implants for Augmentation and Reconstructionof the Breast (AR90 Clinical Study). Preliminary Report:Silicone-Filled Implants at Five Years. McGhan Medical Cor-poration, Santa Barbara, Calif., 1998.
74. Fryzek, J. P., Signorello, L. B., Hakelius, L., et al. Localcomplications and subsequent symptom reporting amongwomen with cosmetic breast implants. Plast. Reconstr. Surg.107: 214, 2001.
75. Handel, N., Wellisch, D., Silverstein, M. J., et al. Knowledge,concern and satisfaction among augmentation mamma-plasty patients. Ann. Plast. Surg. 30: 13, 1993.
76. Young, V. L., Watson, M. E., Boswell, C. B., et al. Initial resultsfrom an online breast augmentation survey. Aesthetic Surg. J.24: 117, 2004.
77. Little, G., and Baker, J. L., Jr. Results of closed compressioncapsulotomy for treatment of contracted breast implant cap-sules. Plast. Reconstr. Surg. 65: 30, 1980.
Volume 117, Number 3 • Breast Implants
767

DISCUSSION
A Long-Term Study of Outcomes, Complications, andPatient Satisfaction with Breast Implants
Scott L. Spear, M.D.Washington, D.C.
Iread with considerable interest the article byDr. Handel and his fellow authors regarding
long-term study of outcomes, complications, andpatient satisfaction with breast implants. Thistopic is of particular interest to me and manyother plastic surgeons because of the shortage oflong-term data regarding how these devices per-form in the local setting. The authors share withus a 25-year experience covering the years be-tween June of 1979 and June of 2004. Patientsreviewed included those undergoing cosmeticsurgery, reconstructive surgery, and revisionalsurgery. The study included the practices of twoplastic surgeons, both working within a well-integrated multidisciplinary team and thus pro-viding a fair amount of consistency in terms ofthe type and quality of surgery performed. Aprospective breast implant database was begunin January of 1990 and a retrospective databasewas obtained by chart review going back for theyears between June of 1979 and December of1989. Five hundred eight of the women with1122 implants were collected in the retrospectivedatabase. The study, like many similar studies, iscomplicated by the fact that many of the patientshad multiple implants over time, thus makingthe evaluation more complex. The authorstherefore specifically looked at the experience ofthe patients with their most recent implant. It isof note that, in cases of bilateral implants, infor-mation was collected separately for the right andleft sides, thus making double entries for all ofthe augmentation patients and single entries formost of the reconstruction patients.
The authors report that 1555 questionnaireswere mailed and that the post office returnednearly half (n � 702) because they were nonde-liverable. Of the 853 questionnaires believed tobe deliverable, 429 were returned, for an ap-proximate 50 percent response rate to the deliv-erable questionnaires. Response rate overall,however, was closer to 25 percent rather than 50percent. In their study, each breast implant wasconsidered separately and its history tracked sep-
arately from the date of insertion until the dateof explantation or last follow-up. This is in con-tradistinction to the breast implant manufactur-er’s Food and Drug Administration PremarketApproval data, which tracked patients ratherthan devices.
The data are reported in several ways, includ-ing complications that tended to occur over adiscrete time frame that were reported as rawdata, such as hematoma and infection, whichalmost always occur promptly after surgery. Incontrast, events that occur over time were re-ported as incidents per 1000 patient-months.These included events such as implant deflation,rupture, and capsular contracture. Rupture re-quired confirmation at the time of surgery andwas not included if only suggested by magneticresonance imaging, mammography, or physicalexamination.
One remarkable aspect of this study is thenumber of different statistical methods that wereused, including the Kaplan-Maier method, thechi-square test, the Kruskal-Wallis test, and theWilcoxon rank sum test. The authors report thatthe study yielded information on a total of 1529patients and 3495 implants. This included 825augmentation patients (1601 implants), 264 re-construction patients (352 implants), and 695revision patients (1534 implants). Follow-up av-eraged 37.4 months per implant. In terms oftypes of implants, there were 1137 saline-filledimplants, 778 double-lumen implants, 1537 sili-cone gel-filled implants, and 38 implants withother fillers such as the Trilucent implant; 2067implants were smooth, 848 were mechanicallytextured, and 568 had polyurethane covering.
The occurrence of capsular contracture wasstudied and revealed the figure of 1.99 capsularcontractures per 1000 patient-months for theaugmentation implants, 5.37 per 1000 patient-months after breast reconstruction, and 4.36 per1000 patient-months after breast implant revi-sion. When looking at types of implants, thenumbers were 3.85 for smooth implants, 3.23 fortextured implants, and 2.19 for polyurethane-covered implants. Hematomas were rare and didnot vary particularly with either type of surgeryor type of implant. One noteworthy aspect of the
Received for publication October 17, 2005.Copyright ©2006 by the American Society of Plastic Surgeons
DOI: 10.1097/01.prs.0000200058.24671.01
www.plasreconsurg.org768

study was the association of hematoma and therisk of developing capsular contracture. Therewas statistically significant evidence that hemato-mas increased the likelihood of capsular contrac-ture. The contracture rate was 7.17 contracturesper 1000 patient-months for patients with hema-tomas and 3.27 per 1000 patient-months for im-plants without hematoma. The relative risk ofcontracture in the event of hematoma was 2.19.Infections were relatively rare and were morecommon in breast reconstruction, but infectionsacross the range of use of implants did not varysignificantly with implant types. Excessive wavi-ness or rippling, in contrast, was more frequentwith textured implants and more common inrevision than in reconstruction or augmenta-tion.
Another notable aspect of the study was adeflation rate that occurred in nine of 943smooth surface implants versus 13 of 192 tex-tured implants. The rate of deflation per patient-month risk was 0.34 for smooth implants and2.07 for textured implants. This difference wasstatistically significant. Among silicone implants,there was no difference with diagnosed rupturesbetween smooth, textured, and polyurethane im-plants.
The authors reviewed the reoperation ratesper implant and found that the per-1000 patient-month augmentation risk number was 15.5 per-cent; the rate was 35.5 percent for breast recon-struction and 21.9 percent for revision surgery.Of interest was the mean duration between op-eration and revision surgery, with it being short-est after breast reconstruction (16 months),longer after revision surgery (38.9 months), andlongest after breast augmentation (49.9months). The duration for revision surgery waslongest in patients with polyurethane-coveredimplants. The most common reason for the op-eration was capsular contracture (56 percent),followed by size change (22 percent) and im-plant malposition (8 percent).
Despite the tremendous amount of work in-volved in putting this study together and thelarge amount of data presented, there are rela-tively few major new significant findings. Thefirst is that capsular contracture in this authors’study was a progressive phenomenon, with pa-tients being at risk for capsular contracturethroughout the length of the study. As the au-thors state, this contradicts the widely held beliefthat capsular contracture tends to be a short-term event. The authors argue, credibly, that forcontracture to progress over years stands in op-
position to the belief that acute events such asbacterial contamination or surgical techniqueare key players in the incidence of capsular con-tracture. Another key finding of this study was ahigher rate of deflation with textured saline im-plants as compared with smooth saline implants.
The study included other findings that areconsistent with previously published work in-cluding the fact that capsular contracture is lessfrequent in breast augmentation as comparedwith revision surgery and breast reconstruction.The authors also report that the patients withpolyurethane-covered implants had a lower inci-dence of capsular contracture in the first severalyears as compared with smooth or textured sili-cone gel implants. Also in agreement with otherstudies, the authors report that rippling and wav-iness was more common with textured implantsas compared with smooth ones.
This article comes at an interesting moment inour knowledge of breast implants. We have re-cently seen submitted by several implant manu-facturers device-specific data to the Food andDrug Administration both on saline and siliconeimplants and in both textured and smooth vari-eties. The data in those Food and Drug Admin-istration–sponsored Premarket Approvals aremultiyear prospective population studies onthousands of women broken down into groupsof those who have saline implants and those whohave silicone implants used for augmentation,revision, and reconstruction. The studies aremanufacturer-specific and device-specific andhave follow-up at a minimum of 3 years and aslong as 9 years in the cases of saline studies. Thepatients were enrolled prospectively at the begin-ning and have compliance in the 70 to 80 per-cent range in terms of follow-up. The data fromthose studies are per patient rather than perimplant, which gives a higher rate or incidenceof events because the denominator is smallerthan it would be if it were per implant, whichwould be roughly double the number of im-plants as compared with per patient, particularlyfor augmentation.
What is interesting is the extent to which thedata from those prospective Premarket Approvalstudies of thousands of patients from each man-ufacturer with both silicone and saline implantsare in agreement with this 25-year retrospectivestudy. Thus, in terms of the frequency of reop-eration and the incidence of capsular contrac-ture, there is general agreement between thestudies. What is new in this study is the correla-tion between surface texture and saline device
Volume 117, Number 3 • Discussion
769

rupture and the correlation between early hema-toma and the eventual development of capsular con-tracture. The number and complexity of the statisti-cal tests used in this article and the way the data arereported gives evidence of how complex and sophis-ticated this subject is and how difficult it may be totrack large numbers of patients with disparate clinicalstories for a long period. This is aggravated by the factthat the authors report some of their data in a rela-tively novel way, at least as compared with other im-plant studies. The use of occurrences as measuredagainst 1000 patient implant months is a relativelyuncommon method of describing the data. Thismakes it difficult to compare the authors’ results withthose of other studies that report their data differ-ently. Other issues with this study include the fact thatit does not discriminate between different types oftexturing and the different manufacturers of devices.This requires, to some extent, a leap of faith to be-lieve that the various texturing processes would yieldthe same results or that the devices from differentmanufacturers would be homogeneous enough thatthey could be lumped together. The low rate of fol-low-up is another concern, with only approximately25 percent of patients being available for follow-up.
This study raises the broader question re-garding whether a long-term, large-patient-population study with relatively poor follow-upwill provide more accurate or more useful dataas compared with a smaller prospective studywith better compliance such as those con-ducted by the manufacturers to obtain Foodand Drug Administration approval. It alsoraises the question regarding the value of stud-ies that go out 20 or more years in light of thefact that, by that time, the devices will haveevolved and the data will be pretty much ofhistorical interest only. Thus, for example, in
the authors’ current study, the informationregarding saline implants will probably be-come less relevant as saline implants are re-placed by silicone implants with the impend-ing U.S. Food and Drug Administrationapproval. Likewise, polyurethane implants, al-though performing well in the short run, arenot on U.S. markets and are unlikely to returnto the United States for some time, if ever.Finally, even many of the silicone implantsdiscussed in this article are no longer used,such as double-lumen silicone implants, whichare not available in the open market or core oradjunct studies in the United States at thepresent time. The information that plastic sur-geons will be most interested in would be thatregarding single-lumen textured and smoothsilicone gel implants. The very best data re-garding those devices are available from thecore clinical studies that were submitted to theFood and Drug Administration over the lastyear as part of the Premarket Approval processby both Inamed and Mentor. As the breastimplant industry, the Food and Drug Admin-istration, and plastic surgeons consider howpostmarket surveillance should be under-taken, the issue of what data should be col-lected on how many patients, and for howlong, will become increasingly important. Ar-ticles such as this help remind us of the signif-icance of ongoing study of these devices asthey become used in a large number of pa-tients.
Scott L. Spear, M.D.Georgetown University Hospital
3800 Reservoir RoadWashington, D.C. 20007-2113
Plastic and Reconstructive Surgery • March 2006
770