Embed Size (px)
Citation preview
Innovations in Drug Information Practice and Research 2015
Program Moderator:Patrick M. Malone, PharmD, FASHP
Professor and Associate Dean of Internal AffairsThe University of Findlay
Disclosures
The program chair and presenters for this continuing education activity have reported no relevant financial relationships.
Announcements
A LEAN Approach to Formulary Management
Lauren Karel, PharmD, BCPS
Ellena Anagnostis, PharmD, BCPS
Cindy Wordell, PharmD, BCPS, FASHP
Thomas Jefferson University Hospital
Philadelphia, PA
Objectives
Recognize necessary steps when coordinating the addition or removal of a formulary drug
Identify examples of Lean initiatives that can be applied to processes within health care
Recommend Lean strategies for optimizing the formulary management process
What is Lean?1,2
Performance improvement methodology
Popularized by the Toyota Motor Corporation
Optimized value within each step of a process Increased efficiency
Improved quality
Customer satisfaction
Waste reduction
Decreased turnaround
times
Innovations in Drug Information Practice and Research 2015 2015 Midyear Clinical Meeting & Exhibition
© 2015 American Society of Health-System Pharmacists 1 of 22
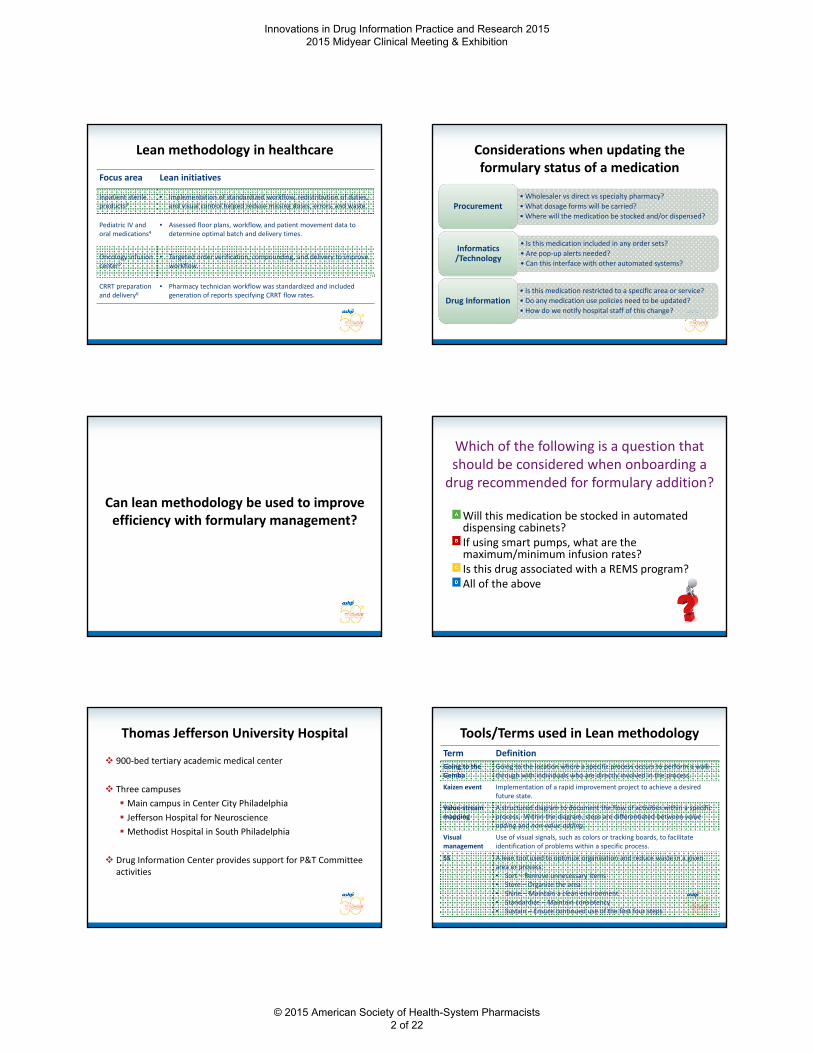
Lean methodology in healthcare
Focus area Lean initiatives
Inpatient sterile products3
• Implementation of standardized workflow, redistribution of duties, and visual control helped reduce missing doses, errors, and waste.
Pediatric IV and oral medications4
• Assessed floor plans, workflow, and patient movement data to determine optimal batch and delivery times.
Oncology infusion center5
• Targeted order verification, compounding, and delivery to improveworkflow.
CRRT preparation and delivery6
• Pharmacy technician workflow was standardized and included generation of reports specifying CRRT flow rates.
Considerations when updating the formulary status of a medication
•Wholesaler vs direct vs specialty pharmacy?
• What dosage forms will be carried?
• Where will the medication be stocked and/or dispensed?Procurement
• Is this medication included in any order sets?
• Are pop‐up alerts needed?
• Can this interface with other automated systems?
Informatics /Technology
• Is this medication restricted to a specific area or service?
• Do any medication use policies need to be updated?
• How do we notify hospital staff of this change?Drug Information
Can lean methodology be used to improve efficiency with formulary management?
Which of the following is a question that should be considered when onboarding a drug recommended for formulary addition?
Will this medication be stocked in automated dispensing cabinets?If using smart pumps, what are the maximum/minimum infusion rates?Is this drug associated with a REMS program?All of the above
Thomas Jefferson University Hospital
900‐bed tertiary academic medical center
Three campuses
Main campus in Center City Philadelphia
Jefferson Hospital for Neuroscience
Methodist Hospital in South Philadelphia
Drug Information Center provides support for P&T Committee activities
Tools/Terms used in Lean methodology
Term Definition
Going to the Gemba
Going to the location where a specific process occurs to perform a walk‐through with individuals who are directly involved in the process.
Kaizen event Implementation of a rapid improvement project to achieve a desired future state.
Value‐stream mapping
A structured diagram to document the flow of activities within a specific process. Within the diagram, steps are differentiated between value adding and non‐value adding.
Visual management
Use of visual signals, such as colors or tracking boards, to facilitate identification of problems within a specific process.
5S A lean tool used to optimize organization and reduce waste in a given area or process:• Sort – Remove unnecessary items• Store – Organize the area• Shine – Maintain a clean environment• Standardize – Maintain consistency• Sustain – Ensure continued use of the first four steps
Innovations in Drug Information Practice and Research 2015 2015 Midyear Clinical Meeting & Exhibition
© 2015 American Society of Health-System Pharmacists 2 of 22
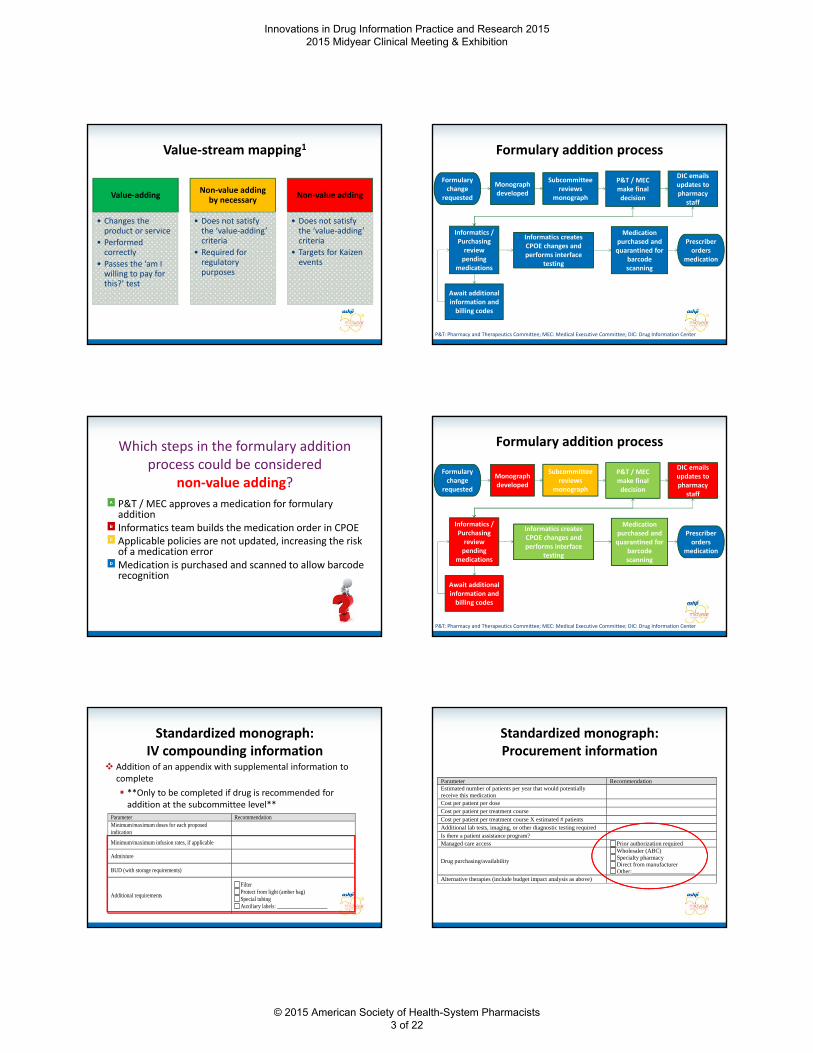
Value‐stream mapping1
Value‐adding
• Changes the product or service
• Performed correctly
• Passes the ‘am I willing to pay for this?’ test
Non‐value adding by necessary
• Does not satisfy the ‘value‐adding’ criteria
• Required for regulatory purposes
Non‐value adding
• Does not satisfy the ‘value‐adding’ criteria
• Targets for Kaizen events
Formulary addition process
Formulary change
requested
Monograph developed
Subcommittee reviews
monograph
P&T / MEC make final decision
DIC emails updates to pharmacy
staff
Informatics / Purchasing review pending
medications
Informatics creates CPOE changes and performs interface
testing
Await additional information and billing codes
Medication purchased and quarantined for
barcode scanning
Prescriber orders
medication
P&T: Pharmacy and Therapeutics Committee; MEC: Medical Executive Committee; DIC: Drug Information Center
Which steps in the formulary addition process could be considered
non‐value adding?
P&T / MEC approves a medication for formulary additionInformatics team builds the medication order in CPOEApplicable policies are not updated, increasing the risk of a medication errorMedication is purchased and scanned to allow barcode recognition
Formulary addition process
Formulary change
requested
Monograph developed
Subcommittee reviews
monograph
P&T / MEC make final decision
DIC emails updates to pharmacy
staff
Informatics / Purchasing review pending
medications
Informatics creates CPOE changes and performs interface
testing
Await additional information and billing codes
Medication purchased and quarantined for
barcode scanning
Prescriber orders
medication
P&T: Pharmacy and Therapeutics Committee; MEC: Medical Executive Committee; DIC: Drug Information Center
Standardized monograph: IV compounding information
Addition of an appendix with supplemental information to complete
**Only to be completed if drug is recommended for addition at the subcommittee level**
Parameter Recommendation Minimum/maximum doses for each proposed indication
Minimum/maximum infusion rates, if applicable
Admixture
BUD (with storage requirements)
Additional requirements
Filter Protect from light (amber bag) Special tubing Auxiliary labels: ___________________
Standardized monograph: Procurement information
Parameter Recommendation Estimated number of patients per year that would potentially receive this medication
Cost per patient per dose
Cost per patient per treatment course
Cost per patient per treatment course X estimated # patients
Additional lab tests, imaging, or other diagnostic testing required
Is there a patient assistance program?
Managed care access Prior authorization required
Drug purchasing/availability
Wholesaler (ABC) Specialty pharmacy Direct from manufacturer Other:_____________________
Alternative therapies (include budget impact analysis as above)
Innovations in Drug Information Practice and Research 2015 2015 Midyear Clinical Meeting & Exhibition
© 2015 American Society of Health-System Pharmacists 3 of 22
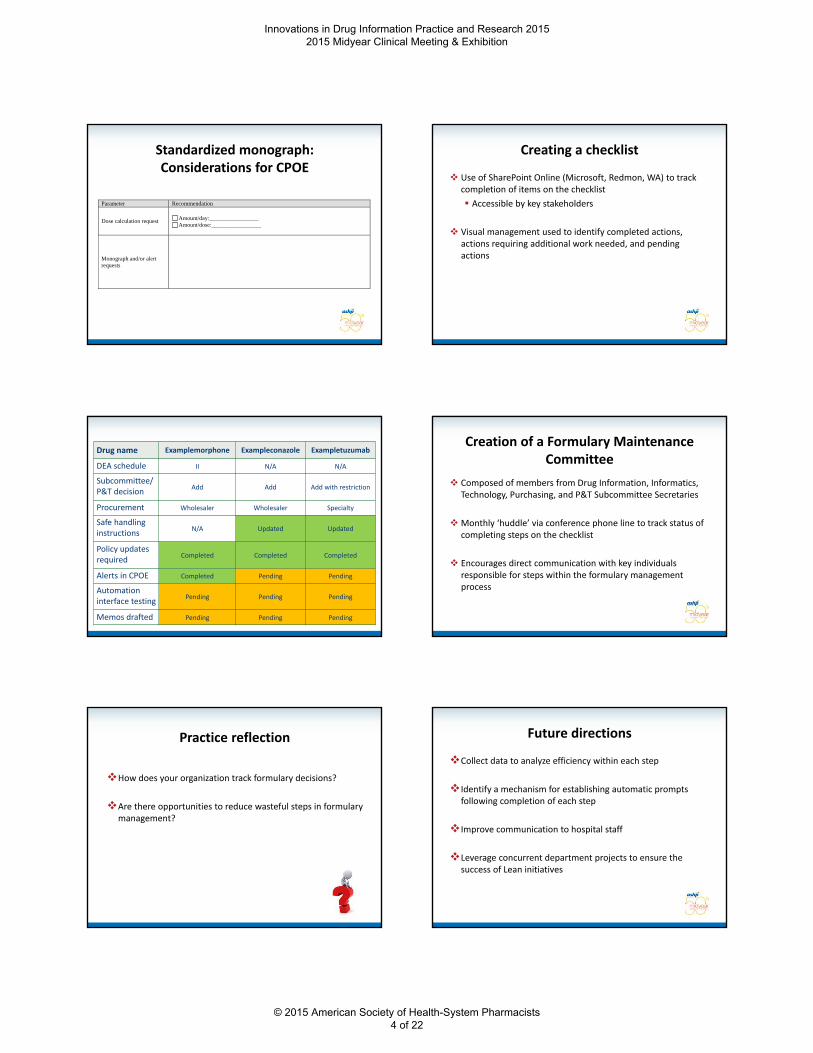
Standardized monograph:Considerations for CPOE
Parameter Recommendation
Dose calculation request
Amount/day:_________________ Amount/dose:_________________
Monograph and/or alert requests
Creating a checklist
Use of SharePoint Online (Microsoft, Redmon, WA) to track completion of items on the checklist
Accessible by key stakeholders
Visual management used to identify completed actions, actions requiring additional work needed, and pending actions
Drug name Examplemorphone Exampleconazole Exampletuzumab
DEA schedule II N/A N/A
Subcommittee/P&T decision
Add Add Add with restriction
Procurement Wholesaler Wholesaler Specialty
Safe handling instructions
N/A Updated Updated
Policy updatesrequired
Completed Completed Completed
Alerts in CPOE Completed Pending Pending
Automation interface testing
Pending Pending Pending
Memos drafted Pending Pending Pending
Creation of a Formulary Maintenance Committee
Composed of members from Drug Information, Informatics, Technology, Purchasing, and P&T Subcommittee Secretaries
Monthly ‘huddle’ via conference phone line to track status of completing steps on the checklist
Encourages direct communication with key individuals responsible for steps within the formulary management process
Practice reflection
How does your organization track formulary decisions?
Are there opportunities to reduce wasteful steps in formulary management?
Future directions
Collect data to analyze efficiency within each step
Identify a mechanism for establishing automatic prompts following completion of each step
Improve communication to hospital staff
Leverage concurrent department projects to ensure the success of Lean initiatives
Innovations in Drug Information Practice and Research 2015 2015 Midyear Clinical Meeting & Exhibition
© 2015 American Society of Health-System Pharmacists 4 of 22
Key takeaways
Lean methodology can be used in various aspects of pharmacy practice to improve efficiency with completing a process
• Not just operational activities!
Staff buy‐in is crucial when enacting changes
Application of Lean process improvement strategies must be an ongoing process
References
1. Graban M. Lean Hospitals: Improving Quality, Patient Safety, and Employee Engagement. 2nd ed. New York, NY: CRC Press; 2011.
2. Lawal AK, et al. Lean management in health care: definition, concepts, methodology and effects reported (systematic review protocol). Syst Rev. 2014;3:103.
3. Hintzen BL, Knoer SJ, Van Dyke CJ, Milavitz BS. Effect of lean process improvement techniques on a university hospital inpatient pharmacy. Am J Health Syst Pharm. 2009;66(22):2042‐2047.
4. Bledsoe S, Little J, Wilkinson RS, Mick A. Using lean methodology to improve operational and clinical efficiency. Am J Health Syst Pharm. 2013;70(17):1476‐1477.
5. Sullivan P, Soefje S, Reinhart D, McGeary C, Cabie ED. Using lean methodology to improve productivity in a hospital oncology pharmacy. Am J Health Syst Pharm. 2014;71(17):1491‐1498.
6. Benfield CB, Brummond P, Lucarotti A, et al. Applying lean principles to continuous renal replacement therapy processes. Am J Health Syst Pharm. 2015;72(3):218‐223.
Use of Flipped Classroom Approach for Teaching Drug Literature Evaluation
Robert D. Beckett, PharmD, BCPS
Assistant Professor of Pharmacy Practice
Director of the Drug Information Center
Manchester University College of Pharmacy
Objectives
At the end of the presentation, participants should be able to:
1. Define flipped classroom in the context of other approaches to active learning
2. Recall results from the assessment of student performance and perceptions using this approach, and
3. Identify lessons learned using this approach.
Discussion
With the participants sitting around you, identify and define one active learning approach you could use to teach drug literature evaluation.
Objective 1
Active Learning Approaches
Lecture Incorporating Activities
Team‐Based Learning
Problem‐Based Learning
Flipped Classroom
Innovations in Drug Information Practice and Research 2015 2015 Midyear Clinical Meeting & Exhibition
© 2015 American Society of Health-System Pharmacists 5 of 22
Drug Literature Evaluation at Manchester
Curriculum
• PHRM 322 (Drug Information)
• PHRM 420 (Drug Literature Evaluation)
• PHRM 530 and 531 (Pharmacy Practice Laboratory)
PHRM 420
• Clinical Trial Evaluation
• Biostatistics
• Additional Study Designs
• In‐Class Article Discussions
Bloom’s Taxonomy
Anderson LW, Krathwohl DR, eds. A Taxonomy for Learning, Teaching, and Assessing: A Revision of Bloom’s Taxonomy of Educational Objectives (Complete Edition). New York, NY: Longman Publishing Group; 2000.
Create
Evaluate
Analyze
Apply
Understand
Remember
Flipped Classroom at Manchester
Explanation
Demonstration
Practice
Feedback
Evaluation
In‐Class Activities
Example – Goals
Course Outcome
• Explain and assess the biostatistics used in a piece of primary literature.
Learning Objectives
• Classify an analysis as per protocol, intention to treat, modified intention to treat, or as treated.
• Explain why an investigator might select each of the data analysis strategies above.
Example – Explanation
Intention to treat: This type of analysis includes all patients who are randomized in the study. Using the above example, we would analyze all 250 patients regardless of completion. This is considered to be more conservative and “real world” (as so many patients are not compliant with treatment) and, as such, maximizes external validity. It is also is super cool because it allows investigators to preserve power, even when patients disappear from the study. This approach is USUALLY but not ALWAYS preferred in clinical trials. We will surely talk about this all semester long because it’s a really fun topic (are you excited as I am?!).
Example – Demonstration, Practice, Feedback
Innovations in Drug Information Practice and Research 2015 2015 Midyear Clinical Meeting & Exhibition
© 2015 American Society of Health-System Pharmacists 6 of 22
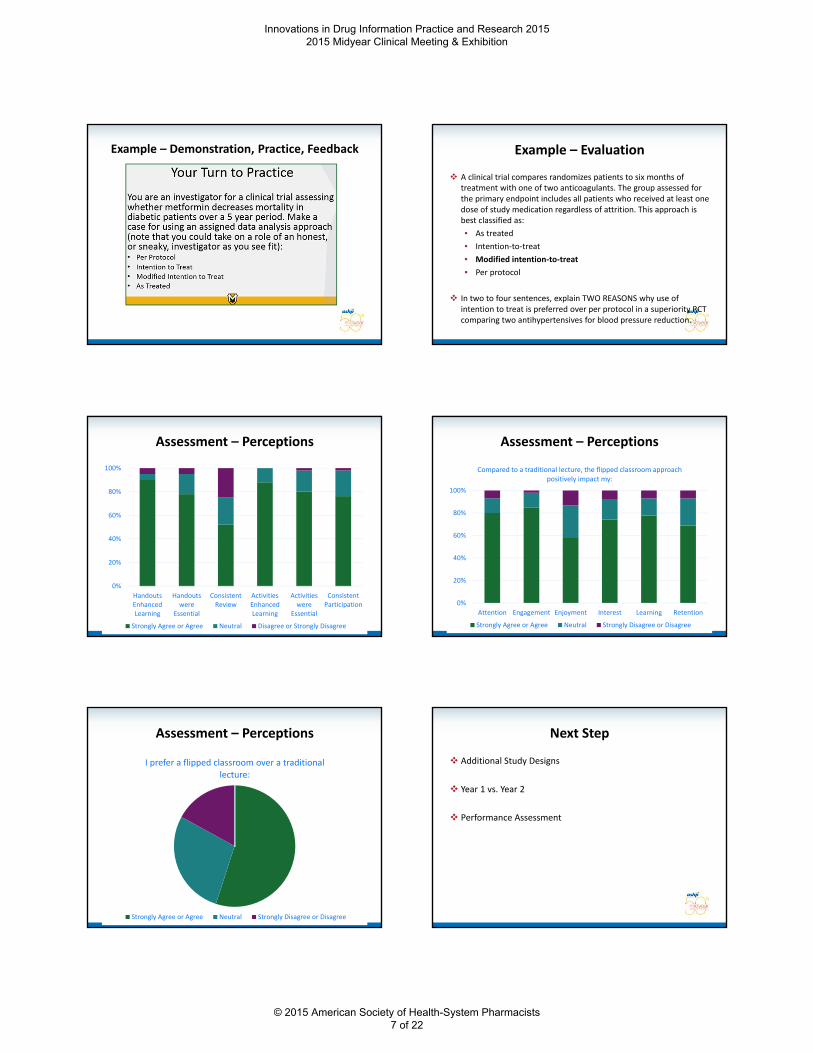
Example – Demonstration, Practice, Feedback Example – Evaluation
A clinical trial compares randomizes patients to six months of treatment with one of two anticoagulants. The group assessed for the primary endpoint includes all patients who received at least one dose of study medication regardless of attrition. This approach is best classified as:
• As treated
• Intention‐to‐treat
• Modified intention‐to‐treat
• Per protocol
In two to four sentences, explain TWO REASONS why use of intention to treat is preferred over per protocol in a superiority RCT comparing two antihypertensives for blood pressure reduction.
Assessment – Perceptions
0%
20%
40%
60%
80%
100%
HandoutsEnhancedLearning
Handoutswere
Essential
ConsistentReview
ActivitiesEnhancedLearning
Activitieswere
Essential
ConsistentParticipation
Strongly Agree or Agree Neutral Disagree or Strongly Disagree
Assessment – Perceptions
0%
20%
40%
60%
80%
100%
Attention Engagement Enjoyment Interest Learning Retention
Compared to a traditional lecture, the flipped classroom approach positively impact my:
Strongly Agree or Agree Neutral Strongly Disagree or Disagree
Assessment – Perceptions
I prefer a flipped classroom over a traditional lecture:
Strongly Agree or Agree Neutral Strongly Disagree or Disagree
Next Step
Additional Study Designs
Year 1 vs. Year 2
Performance Assessment
Innovations in Drug Information Practice and Research 2015 2015 Midyear Clinical Meeting & Exhibition
© 2015 American Society of Health-System Pharmacists 7 of 22
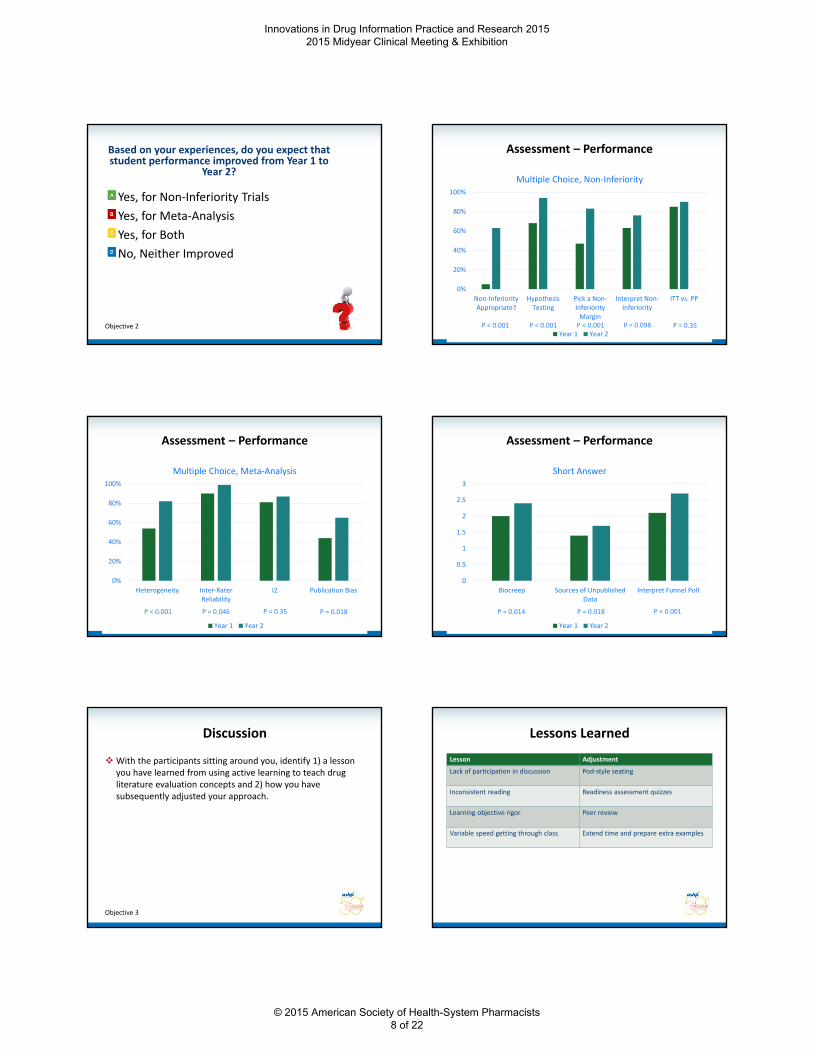
Based on your experiences, do you expect that student performance improved from Year 1 to
Year 2?
Yes, for Non‐Inferiority Trials
Yes, for Meta‐Analysis
Yes, for Both
No, Neither Improved
Objective 2
Assessment – Performance
0%
20%
40%
60%
80%
100%
Non‐InferiorityAppropriate?
HypothesisTesting
Pick a Non‐InferiorityMargin
Interpret Non‐Inferiority
ITT vs. PP
Multiple Choice, Non‐Inferiority
Year 1 Year 2P < 0.001 P < 0.001 P < 0.001 P = 0.098 P = 0.35
Assessment – Performance
0%
20%
40%
60%
80%
100%
Heterogeneity Inter‐RaterReliability
I2 Publication Bias
Multiple Choice, Meta‐Analysis
Year 1 Year 2
P < 0.001 P = 0.046 P = 0.35 P = 0.018
Assessment – Performance
0
0.5
1
1.5
2
2.5
3
Biocreep Sources of UnpublishedData
Interpret Funnel Polt
Short Answer
Year 1 Year 2
P = 0.014 P = 0.018 P < 0.001
Discussion
With the participants sitting around you, identify 1) a lesson you have learned from using active learning to teach drug literature evaluation concepts and 2) how you have subsequently adjusted your approach.
Objective 3
Lessons Learned
Lesson Adjustment
Lack of participation in discussion Pod‐style seating
Inconsistent reading Readiness assessment quizzes
Learning objective rigor Peer review
Variable speed getting through class Extend time and prepare extra examples
Innovations in Drug Information Practice and Research 2015 2015 Midyear Clinical Meeting & Exhibition
© 2015 American Society of Health-System Pharmacists 8 of 22
Key Takeaways
Key Takeaway #1
• Consider increasing the amount of active learning in your drug literature evaluation course (lecture lecture with activities; lecture with activities flipped classroom)
Key Takeaway #2
• Use of flipped classroom resulted in positive student perceptions and a switch from lecture with activities to flipped classroom resulted in improved performance.
Key Takeaway #3
• Be comfortable with spontaneity and incorporate strategies to encourage active participation.
Use of Flipped Classroom Approach for Teaching Drug Literature Evaluation
Robert D. Beckett, PharmD, BCPS
Assistant Professor of Pharmacy Practice
Director of the Drug Information Center
Manchester University College of Pharmacy
Questions, Answers and Discussion Development, Implementation, and Impact of a Mobile Application to Request Drug
Information
Scott Perkins, PharmDCo‐Director, Drug InformationClinical Assistant Professor
Campbell University College of Pharmacy & Health Sciences
Objectives
• Describe aspects important to consider when developing a drug information mobile application (app)
• Discuss strategies for implementing a drug information mobile app
• Describe how a drug information mobile app may impact a drug information center
Campbell Drug Information Center
• Created in 1987 from a grant from GlaxoSmithKline
• Free service for faculty, alumni, students and other healthcare providers
• 2 Co‐Directors, 4 fourth‐year student pharmacists, 1 Program Manager
• Currently receive 180‐250 requests on a monthly basis
40‐50% are literature requests
Innovations in Drug Information Practice and Research 2015 2015 Midyear Clinical Meeting & Exhibition
© 2015 American Society of Health-System Pharmacists 9 of 22
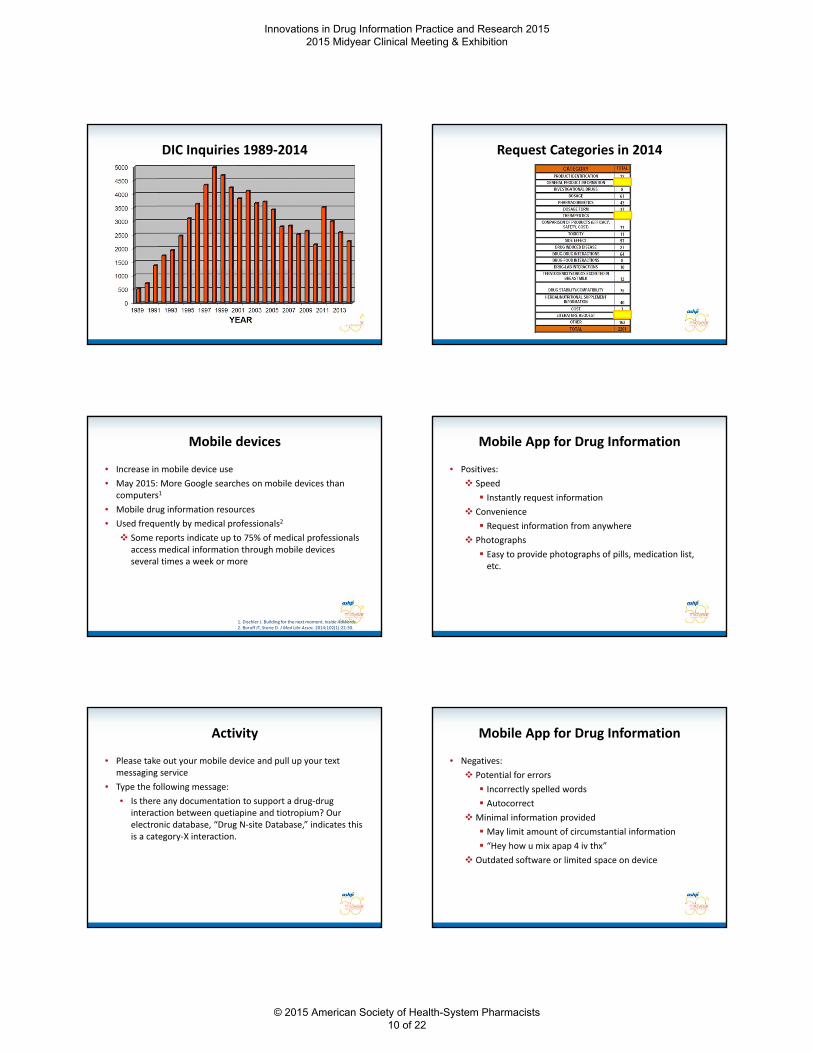
DIC Inquiries 1989‐2014 Request Categories in 2014
Mobile devices
• Increase in mobile device use
• May 2015: More Google searches on mobile devices than computers1
• Mobile drug information resources
• Used frequently by medical professionals2
Some reports indicate up to 75% of medical professionals access medical information through mobile devices several times a week or more
1. Dischler J. Building for the next moment. Inside AdWords.2. Boruff JT, Storie D. J Med Libr Assoc. 2014;102(1):22‐30.
Mobile App for Drug Information
• Positives:
Speed
Instantly request information
Convenience
Request information from anywhere
Photographs
Easy to provide photographs of pills, medication list, etc.
Activity
• Please take out your mobile device and pull up your text messaging service
• Type the following message:
• Is there any documentation to support a drug‐drug interaction between quetiapine and tiotropium? Our electronic database, “Drug N‐site Database,” indicates this is a category‐X interaction.
Mobile App for Drug Information
• Negatives:
Potential for errors
Incorrectly spelled words
Autocorrect
Minimal information provided
May limit amount of circumstantial information
“Hey how u mix apap 4 iv thx”
Outdated software or limited space on device
Innovations in Drug Information Practice and Research 2015 2015 Midyear Clinical Meeting & Exhibition
© 2015 American Society of Health-System Pharmacists 10 of 22
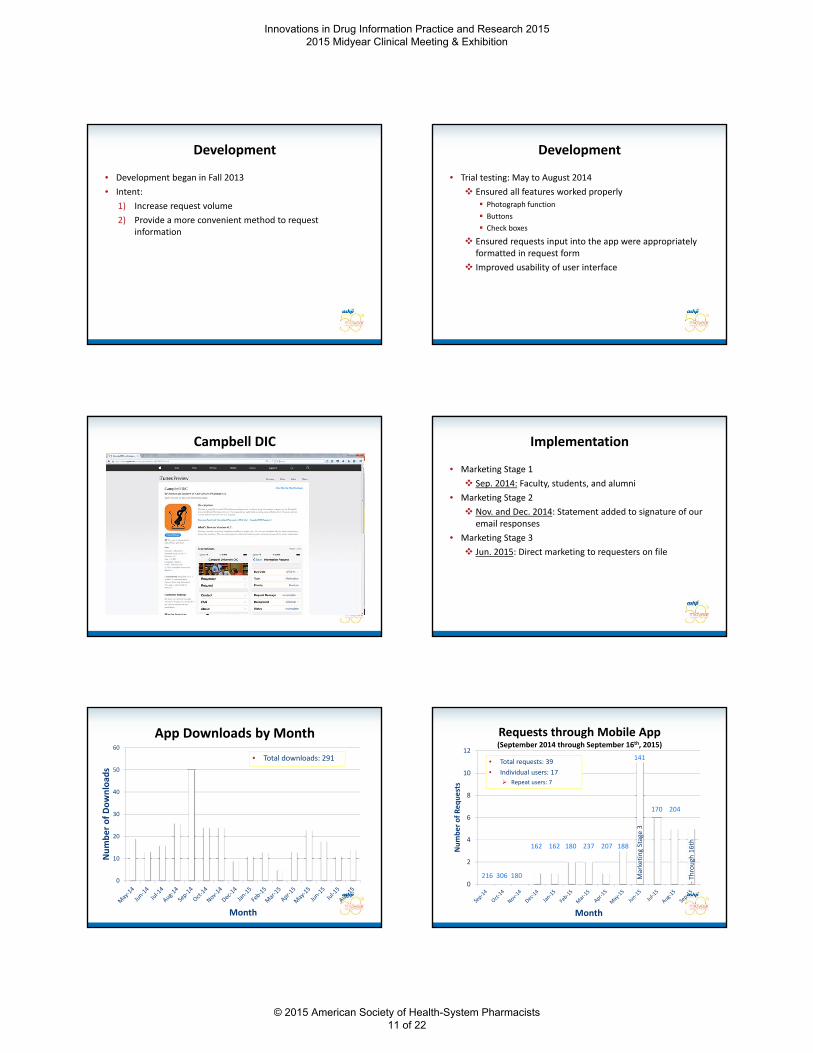
Development
• Development began in Fall 2013
• Intent:
1) Increase request volume
2) Provide a more convenient method to request information
Development
• Trial testing: May to August 2014
Ensured all features worked properly Photograph function
Buttons
Check boxes
Ensured requests input into the app were appropriately formatted in request form
Improved usability of user interface
Campbell DIC Implementation
• Marketing Stage 1
Sep. 2014: Faculty, students, and alumni
• Marketing Stage 2
Nov. and Dec. 2014: Statement added to signature of our email responses
• Marketing Stage 3
Jun. 2015: Direct marketing to requesters on file
App Downloads by Month
0
10
20
30
40
50
60
Number of Download
s
Month
• Total downloads: 291
0
2
4
6
8
10
12
Number of Requests
Month
Requests through Mobile App(September 2014 through September 16th, 2015)
• Total requests: 39
• Individual users: 17
Repeat users: 7
‐Through
16th
Marketing Stage 3
141
162 162 180 237 207 188
216 306 180
170 204
Innovations in Drug Information Practice and Research 2015 2015 Midyear Clinical Meeting & Exhibition
© 2015 American Society of Health-System Pharmacists 11 of 22
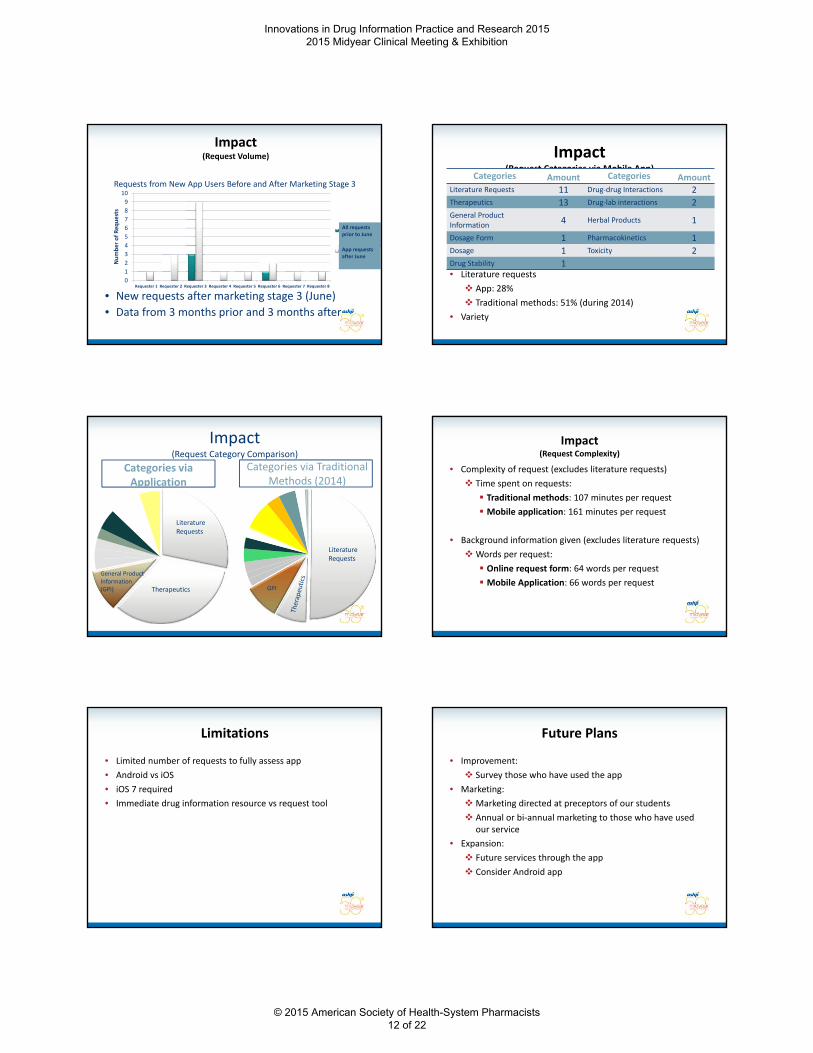
Impact(Request Volume)
Requests from New App Users Before and After Marketing Stage 3
0
1
2
3
4
5
6
7
8
9
10
Requester 1 Requester 2 Requester 3 Requester 4 Requester 5 Requester 6 Requester 7 Requester 8
Number of Req
uests
Requestsprior todownloadRequestswith app
• New requests after marketing stage 3 (June)
• Data from 3 months prior and 3 months after
All requests prior to June
App requests after June
Impact(Request Categories via Mobile App)
Categories Amount Categories AmountLiterature Requests 11 Drug‐drug Interactions 2Therapeutics 13 Drug‐lab interactions 2General Product Information
4 Herbal Products 1
Dosage Form 1 Pharmacokinetics 1Dosage 1 Toxicity 2Drug Stability 1• Literature requests
App: 28%
Traditional methods: 51% (during 2014)
• Variety
Categories via Application
Categories via Traditional Methods (2014)
Literature Requests
Therapeutics
General Product Information(GPI)
Impact(Request Category Comparison)
Literature Requests
GPI
Impact (Request Complexity)
• Complexity of request (excludes literature requests)
Time spent on requests:
Traditional methods: 107 minutes per request
Mobile application: 161 minutes per request
• Background information given (excludes literature requests)
Words per request:
Online request form: 64 words per request
Mobile Application: 66 words per request
Limitations
• Limited number of requests to fully assess app
• Android vs iOS
• iOS 7 required
• Immediate drug information resource vs request tool
Future Plans
• Improvement:
Survey those who have used the app
• Marketing:
Marketing directed at preceptors of our students
Annual or bi‐annual marketing to those who have used our service
• Expansion:
Future services through the app
Consider Android app
Innovations in Drug Information Practice and Research 2015 2015 Midyear Clinical Meeting & Exhibition
© 2015 American Society of Health-System Pharmacists 12 of 22
Conclusion
• Minimal impact on total number of requests
• Appears to have improved convenience for some requesters
• Given time, the trend in initial data indicates this will likely have an impact on the volume of requests we receive in the future without sacrificing quality of requests we receive
Still assessing the degree of this impact
Acknowledgements
• Connie Barnes, PharmD
Vice Chair of Pharmacy Practice
Co‐Director of Drug Information
Professor of Pharmacy Practice
Campbell University College of Pharmacy & Health Sciences
• Ted Hancock, PharmD, CGP, BCACP, CPP, FASCP
Assistant Professor of Pharmacy Practice
Campbell University College of Pharmacy & Health Sciences
References
1. Dischler J. Building for the next moment [internet]. Inside AdWords. Google, Inc. 2015 May 5. [updated 2015 May 5, cited 2017 Sept 7]. Available from: http://adwords.blogspot.com/2015/05/building‐for‐next‐moment.html.
2. Boruff JT, Storie D. Mobile devices in medicine: a survey of how medical students, residents, and faculty use smartphones and other mobile devices to find information. J Med Libr Assoc. 2014;102(1):22‐30.
Everyone is a Winner: Leveraging your EMR to Optimize Formulary Restriction Compliance
Genevieve (Jeni) Hayes, PharmD, MSPharm, BCPS
Clinical Specialist, Outcomes Management
MUSC Health
Charleston, South Carolina
Objectives
Understand strategies for restricting medications on an institution formulary
Compare approaches for presenting medication restriction information in the electronic medical record (EMR)
Assess adherence to formulary restrictions in one’s organization
Our Charge
Ensure appropriate use of medications throughout the organization
Innovations in Drug Information Practice and Research 2015 2015 Midyear Clinical Meeting & Exhibition
© 2015 American Society of Health-System Pharmacists 13 of 22
Restriction Overview
Many health systems place restrictions on certain formulary medications to improve the appropriateness of their use
• Antimicrobial resistance
• High‐cost medications
• Serious safety concerns
J Managed Care Spec Pharm. 2014;20(7):677‐84.
Am J Hosp Pharm. 1982;39(11):1898‐901.
How many audience members have at least 1 formulary medication restricted in some manner?
Yes
No
Standardize restriction language
Ensure restriction criteria are objective
Build EMR functionality
Assess adherence to formulary restrictions
Phase 1: Standardize Language
Phase 1: Standardize Language
Consistency among types
• Service
• Location
• Provider type (eg, Attending, Fellow)
• Indication
• Miscellaneous
Word document Online database
Phase 1: Standardize Language
Innovations in Drug Information Practice and Research 2015 2015 Midyear Clinical Meeting & Exhibition
© 2015 American Society of Health-System Pharmacists 14 of 22
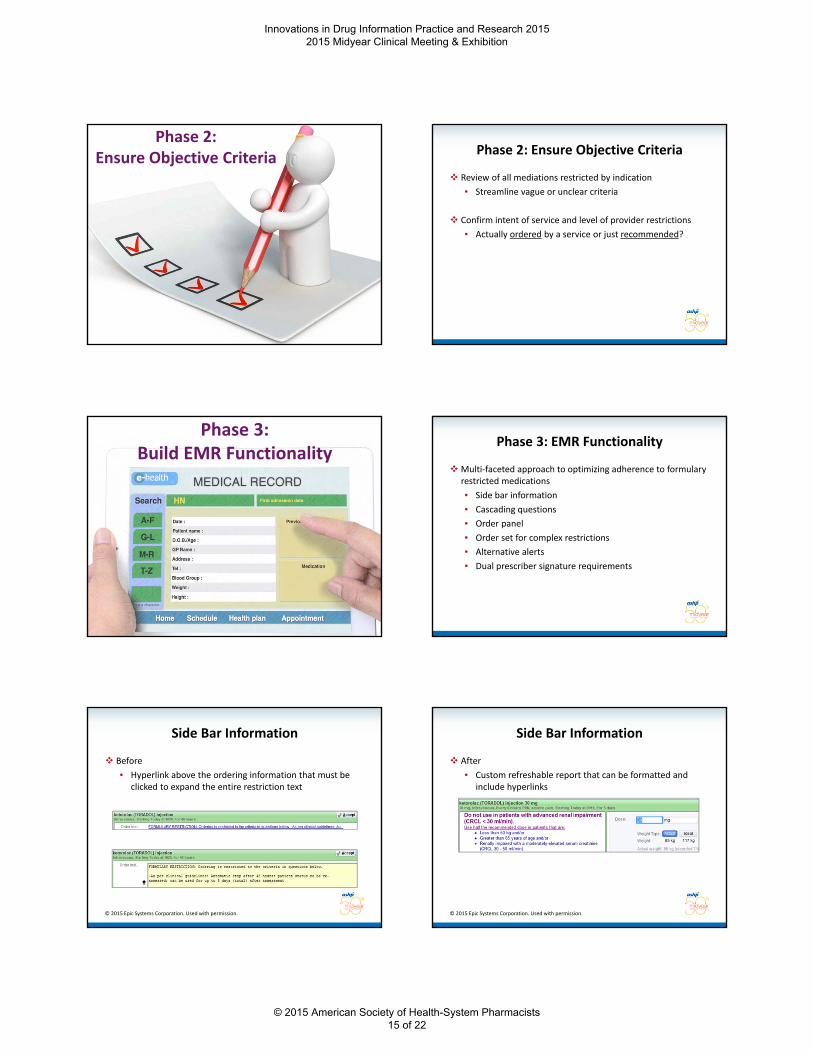
Phase 2: Ensure Objective Criteria Phase 2: Ensure Objective Criteria
Review of all mediations restricted by indication
• Streamline vague or unclear criteria
Confirm intent of service and level of provider restrictions
• Actually ordered by a service or just recommended?
Phase 3:Build EMR Functionality
Phase 3: EMR Functionality
Multi‐faceted approach to optimizing adherence to formulary restricted medications
• Side bar information
• Cascading questions
• Order panel
• Order set for complex restrictions
• Alternative alerts
• Dual prescriber signature requirements
Side Bar Information
Before
• Hyperlink above the ordering information that must be clicked to expand the entire restriction text
© 2015 Epic Systems Corporation. Used with permission.
Side Bar Information
After
• Custom refreshable report that can be formatted and include hyperlinks
© 2015 Epic Systems Corporation. Used with permission.
Innovations in Drug Information Practice and Research 2015 2015 Midyear Clinical Meeting & Exhibition
© 2015 American Society of Health-System Pharmacists 15 of 22
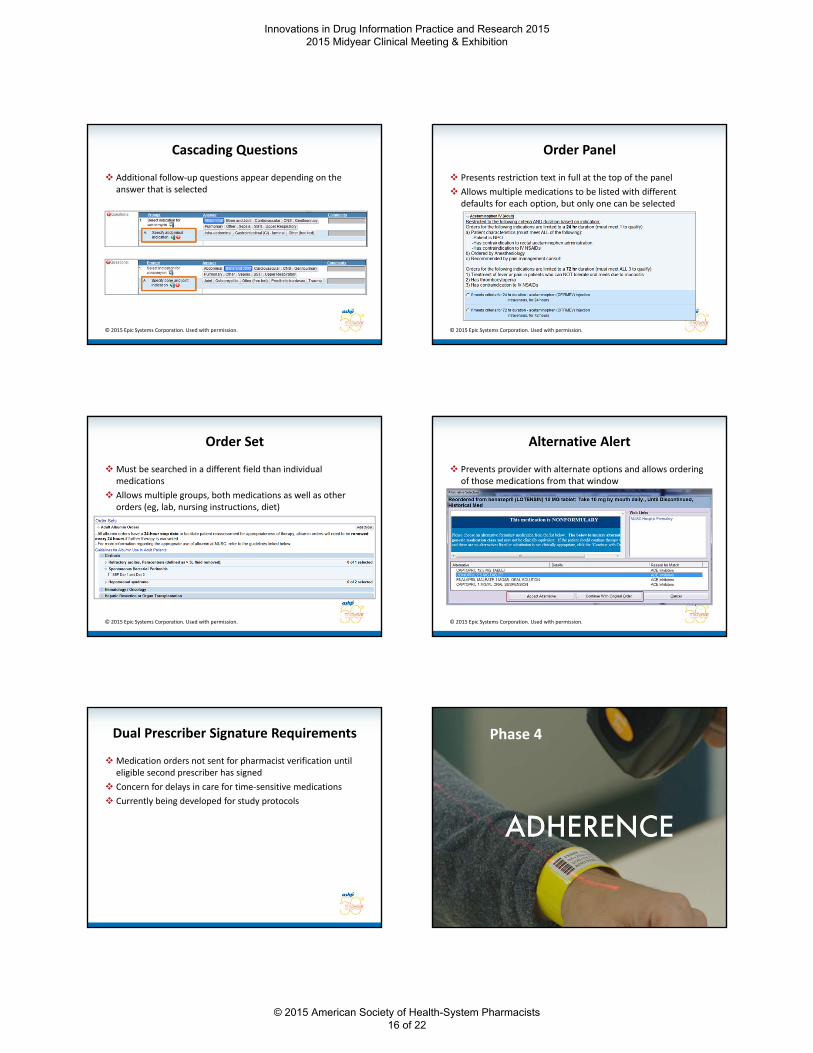
Cascading Questions
Additional follow‐up questions appear depending on the answer that is selected
© 2015 Epic Systems Corporation. Used with permission.
Order Panel
Presents restriction text in full at the top of the panel
Allows multiple medications to be listed with different defaults for each option, but only one can be selected
© 2015 Epic Systems Corporation. Used with permission.
Order Set
Must be searched in a different field than individual medications
Allows multiple groups, both medications as well as other orders (eg, lab, nursing instructions, diet)
© 2015 Epic Systems Corporation. Used with permission.
Alternative Alert
Prevents provider with alternate options and allows ordering of those medications from that window
© 2015 Epic Systems Corporation. Used with permission.
Dual Prescriber Signature Requirements
Medication orders not sent for pharmacist verification until eligible second prescriber has signed
Concern for delays in care for time‐sensitive medications
Currently being developed for study protocols
Phase 4
Innovations in Drug Information Practice and Research 2015 2015 Midyear Clinical Meeting & Exhibition
© 2015 American Society of Health-System Pharmacists 16 of 22

Assessing Restriction Adherence
Medication use evaluations (MUEs)
• Individual agents (eg, albumin, IV acetaminophen)
• Classes of medications (eg, antiretrovirals)
Mechanisms
• Manual chart abstraction
• EMR documentation (interventions?)
Restricted medications should be built in the electronic medical record to
make it easy to do the right thing and difficult to do the wrong thing.
True
False
Key Takeaways
Key Takeaway #1
• Having objective criteria facilitates evaluation of adherence to formulary restrictions.
Key Takeaway #2
• Multiple strategies in the electronic medical record can be used to inform clinicians and enforce formulary restrictions.
Key Takeaway #3
• Continuous assessment of your formulary can help ensure medication stewardship throughout one’s organization.
Questions, Answers and Discussion
Formulary Management Through SharePoint and InfoPath Tracking and Communication
Jamie M. Gomes, PharmD, BCPS
Clinical Specialist, Drug Information
The Children’s Hospital of Philadelphia
Objectives
Evaluate tools available in Microsoft SharePoint and Microsoft InfoPath forms to aid in formulary management.
Identify opportunities for use of SharePoint and InfoPath for formulary management and documentation.
Innovations in Drug Information Practice and Research 2015 2015 Midyear Clinical Meeting & Exhibition
© 2015 American Society of Health-System Pharmacists 17 of 22
The Children’s Hospital of Philadelphia (CHOP)
CHOP Care Network
• Main Campus
535 inpatient beds
Outpatient services
Rehabilitation services
• Primary Care, Specialty Care, Ambulatory Surgery, CHOP Care Network Newborn and Pediatric Inpatient Care, Home Care
Therapeutic Standards Committee (TSC)
• Number of Drugs on Formulary: 693
Hospital Wide Drug Information
Electronic Formulary
CPOE medication orders/order sets
Clinical Pathways
Smart Pumps
Intranet
Policies/Procedures/Job Aids
• Hazardous Medications List
• High Alert Medications List
• Look‐alike sound‐alike List
Ketogenic Diet Database
Department of Pharmacy Services
5 production/dispensing pharmacies
• 24 hour pharmacy
• Oral Preparation
• Anesthesia/TPN
• Emergency Department
• Oncology Clinic
Pyxis MedStations
Sterile Products
• Robotic IV Automation (RIVA)
• DoseEdge Pharmacy Workflow Manager
Non‐Sterile Products
• Swisslog Automated Tablet Packaging System
• Pentapack Unit Dosing Machine
• Extemporaneous Compounding
Formulary Change Involvement
Therapeutic Standards Committee
Drug Information Pharmacists
LexicompFormulary
Epic Willow/
Core Clinical
(5) Pharmacy Supervisors
(5) Distribution Pharmacies and Technology
Pyxis
GO LIVE
Question: How do you currently track formulary changes?
Paper Files
Shared Drive
Excel Spreadsheet
E‐mail
Microsoft SharePoint
Web platform for Microsoft Office Suite
@CHOP – Intranet Sites
Capabilities:
• Store, organize, share, and access information
• Calendars
• Social Feeds – Newsfeed/Blogs
• Document Folders
• Libraries/Lists
Innovations in Drug Information Practice and Research 2015 2015 Midyear Clinical Meeting & Exhibition
© 2015 American Society of Health-System Pharmacists 18 of 22
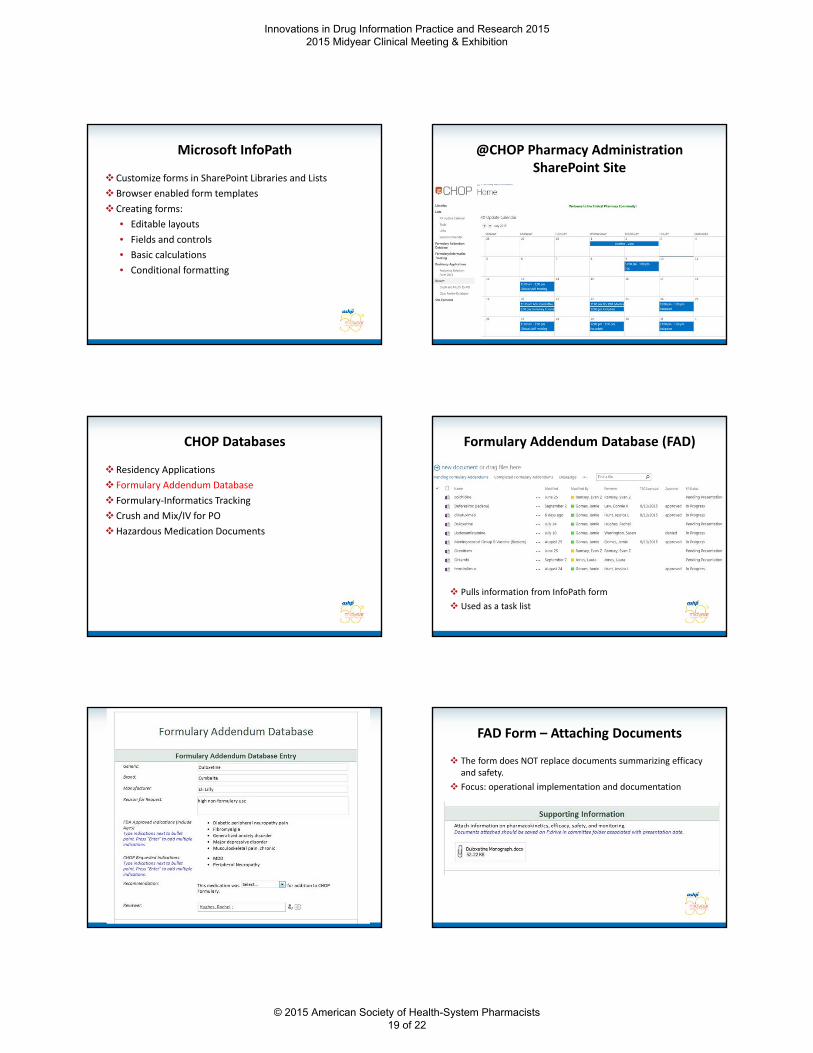
Microsoft InfoPath
Customize forms in SharePoint Libraries and Lists
Browser enabled form templates
Creating forms:
• Editable layouts
• Fields and controls
• Basic calculations
• Conditional formatting
@CHOP Pharmacy Administration SharePoint Site
CHOP Databases
Residency Applications
Formulary Addendum Database
Formulary‐Informatics Tracking
Crush and Mix/IV for PO
Hazardous Medication Documents
Formulary Addendum Database (FAD)
Pulls information from InfoPath form
Used as a task list
FAD Form – Attaching Documents
The form does NOT replace documents summarizing efficacy and safety.
Focus: operational implementation and documentation
Innovations in Drug Information Practice and Research 2015 2015 Midyear Clinical Meeting & Exhibition
© 2015 American Society of Health-System Pharmacists 19 of 22
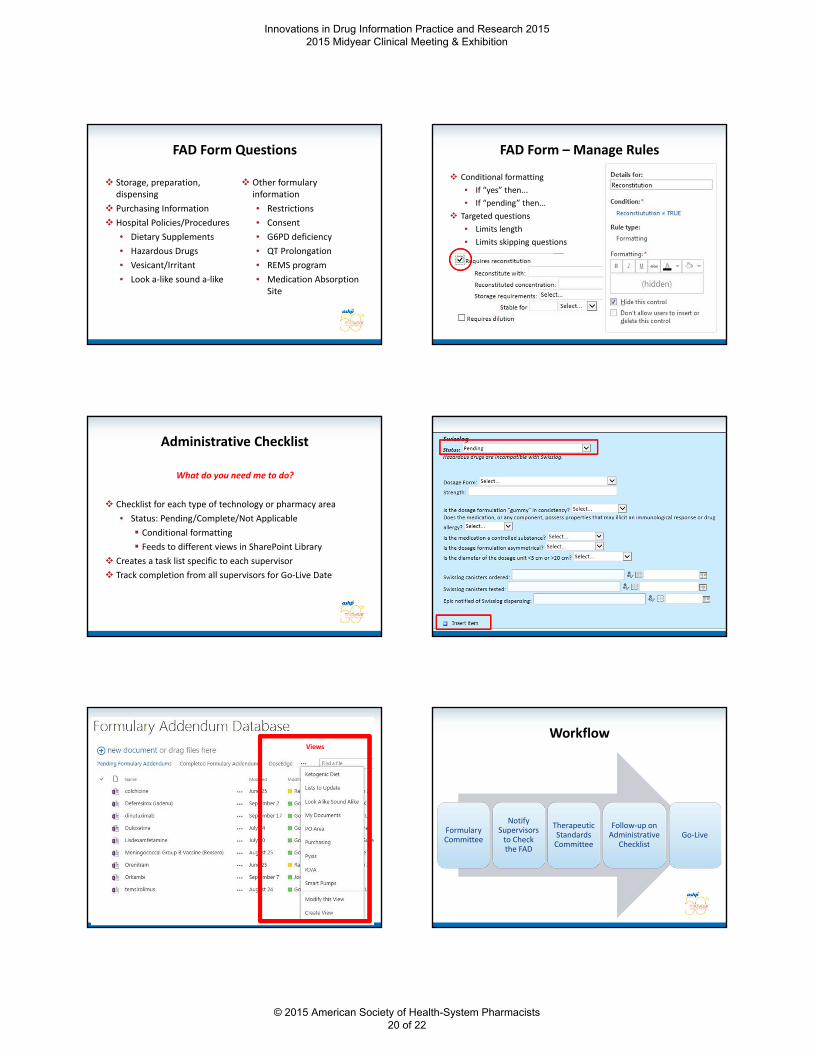
FAD Form Questions
Storage, preparation, dispensing
Purchasing Information
Hospital Policies/Procedures
• Dietary Supplements
• Hazardous Drugs
• Vesicant/Irritant
• Look a‐like sound a‐like
Other formulary information
• Restrictions
• Consent
• G6PD deficiency
• QT Prolongation
• REMS program
• Medication Absorption Site
FAD Form – Manage Rules
Conditional formatting
• If “yes” then...
• If “pending” then…
Targeted questions
• Limits length
• Limits skipping questions
Administrative Checklist
Checklist for each type of technology or pharmacy area
• Status: Pending/Complete/Not Applicable
Conditional formatting
Feeds to different views in SharePoint Library
Creates a task list specific to each supervisor
Track completion from all supervisors for Go‐Live Date
What do you need me to do?
Views
Workflow
Formulary Committee
Notify Supervisors to Check the FAD
Therapeutic Standards Committee
Follow‐up on Administrative
ChecklistGo‐Live
Innovations in Drug Information Practice and Research 2015 2015 Midyear Clinical Meeting & Exhibition
© 2015 American Society of Health-System Pharmacists 20 of 22
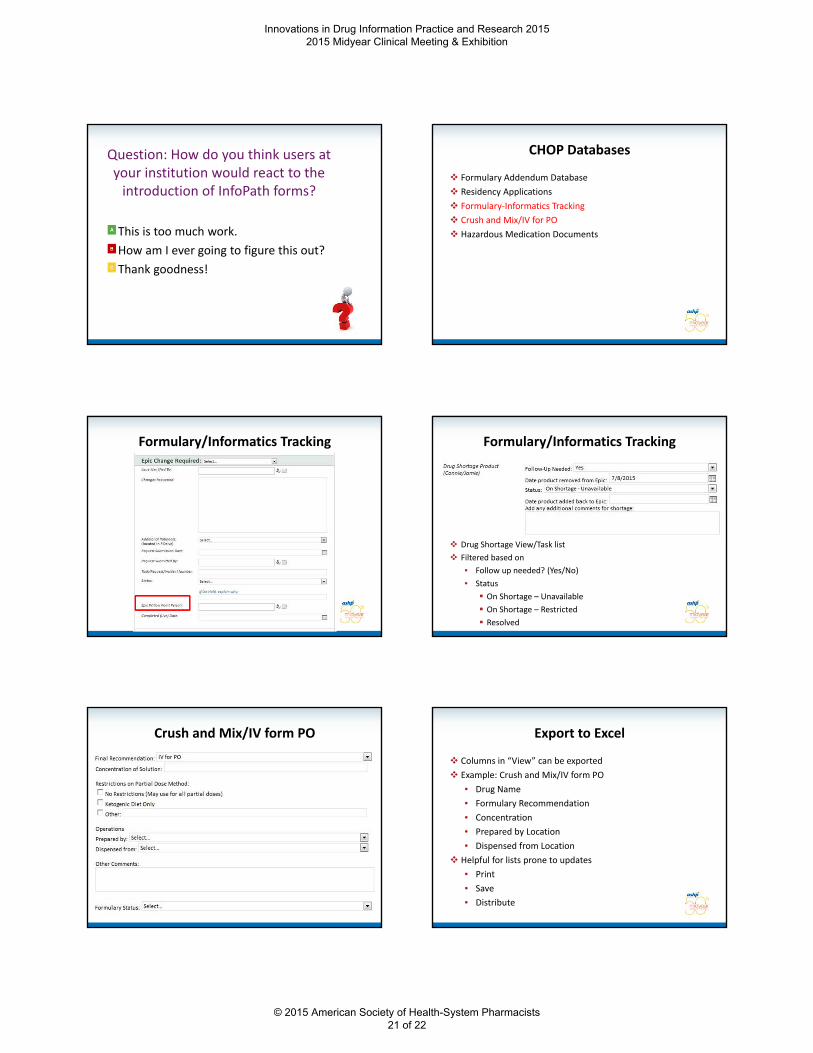
Question: How do you think users at your institution would react to the introduction of InfoPath forms?
This is too much work.
How am I ever going to figure this out?
Thank goodness!
CHOP Databases
Formulary Addendum Database
Residency Applications
Formulary‐Informatics Tracking
Crush and Mix/IV for PO
Hazardous Medication Documents
Formulary/Informatics Tracking Formulary/Informatics Tracking
Drug Shortage View/Task list
Filtered based on
• Follow up needed? (Yes/No)
• Status
On Shortage – Unavailable
On Shortage – Restricted
Resolved
Crush and Mix/IV form PO Export to Excel
Columns in “View” can be exported
Example: Crush and Mix/IV form PO
• Drug Name
• Formulary Recommendation
• Concentration
• Prepared by Location
• Dispensed from Location
Helpful for lists prone to updates
• Save
• Distribute
Innovations in Drug Information Practice and Research 2015 2015 Midyear Clinical Meeting & Exhibition
© 2015 American Society of Health-System Pharmacists 21 of 22
True or False: SharePoint is only useful if you design forms in
InfoPath.
True
False
Discussion
Ideas for Use of SharePoint/InfoPath
Class Reviews
Drug information question documentation
Formulary addition requests
Removal from Formulary
Key Takeaways
Microsoft InfoPath is a program used to create browser enabled forms in Microsoft SharePoint.
Utilize fields and controls in Microsoft InfoPath to optimize questions and length of forms as well as to control “views” in Microsoft SharePoint.
Microsoft SharePoint can be a useful program to create checklists for items requiring follow up and to aid in communication and documentation of formulary changes.
Formulary Management Through SharePoint and InfoPath Tracking and Communication
Jamie M. Gomes, PharmD, BCPS
Clinical Specialist, Drug Information
The Children’s Hospital of Philadelphia
Questions, Answers and Discussion
Innovations in Drug Information Practice and Research 2015 2015 Midyear Clinical Meeting & Exhibition
© 2015 American Society of Health-System Pharmacists 22 of 22





























