Embed Size (px)
Citation preview

The Official Healthca e ProfessionalJournal of the CDE
A Journal for the healthcare professional with an interest in diabetes
EDITORIAL
ORIGINAL ARTICLES
• Does insulin allergy really exist?
• Diabetes Management in 2017 –
What is new?
• Cardiorespiratory fitne s –
The most potent and ignored solution
to improving health outcomes
• 'Tis the season...
Time to talk Flu Vaccination
• A structured approach to the
diabetes consultation
• Screening for diabetic retinopathy at
the level of primary care
CPD ACCREDITED DIABETES TRAINING
Volume 10 Number 1 • March 2017
Fitness is not about being better
than someone else...It’s about beingbetter than you
used to be

OPTISULIN, the clone of LANTUS
LANTUS and OPTISULIN are identical in all aspects except for the name and price and are therefore interchangeable 6,7,8
For full prescribing information, refer to current package insert.
SCHEDULING STATUS: S3 PROPRIETARY NAME AND DOSAGE FORM: LANTUS® solution for injection. COMPOSITION: Each ml of the solution for injection contains 3.64 mg of the active
ingredient insulin glargine, corresponding to 100 units (u) human insulin, 2.7 mg of the preservative metacresol and 0.0626 mg of zinc chloride as stabiliser. 10 ml vial contains 0.02 mg polysorbate 20
as additional stabiliser. REGISTRATION NUMBER: 34/21.1/0248.
SCHEDULING STATUS: S3 PROPRIETARY NAME AND DOSAGE FORM: OPTISULIN® solution for injection. COMPOSITION: Each ml of the solution for injection contains 3.64 mg of the active
ingredient insulin glargine, corresponding to 100 units (u) human insulin, 2.7 mg of the preservative metacresol and 0.0626 mg of zinc chloride as stabiliser. REGISTRATION NUMBER: 41/21.1/0363.
NAME AND BUSINESS ADDRESS OF THE APPLICANT: Sanofi-Aventis South Africa (Pty) ltd, 2 Bond Street, Midrand, 1685. Tel: 011 256 3700. Reg. No. 1996/10381/07.
SAZA.OPN.15.09.0155
References: 1. DeVries JH, Meneghini L, Barnett AH, et al. A Patient-level Analysis of Efficacy and Hypoglycaemia Outcomes Across Treat-to-target Trials with Insulin Glargine Added to Oral Antidiabetes
Agents in People with Type 2 Diabetes. Eur Endocrinol. 2014;10(1):23-30. 2. Gerstein HC, Bosch J, Dagenais GR, et al., and The ORIGIN Trial Investigators. Basal Insulin and Cardiovascular and Other
Outcomes in Dysglycemia. N Engl J Med. 2012;367:319-328. 3. South African Medicine Price Registry. Available from: http://www.mpr.gov.za/PublishedDocuments.aspx?DocCatId=34. Accessed:
3 September, 2015. 4. Mediscor Pharmaceutical Benefit Management (South Africa). Medicines Review 2014, table 12 of page 17. Mediscor PBM (Pty) Ltd. Accessed September 2015. 5. Discovery
Health, Medicine advisor accessed at www.discovery.co.za on the 28th September 2015. 6. Nissen L. Explainer: how do generic medicines compare with brand leaders? The Conversation [online].
Available from: http://theconversation.com/explainer-how-do-generic-medicines-compare-with-brand-leaders-1386. Accessed: 1 September, 2015. 7. Hollis A. How do Brands’ “Own Generics” Affect
Pharmaceutical Prices? Rev Indus Org. 2005;27:329-350. 8. Integrated Act 101 (2) of the Medicines and Related Substances Control Act 101 of 1965.
Discover another way to say Lantus . . .
IdenticalEffi cacy 1,2
IdenticalSafety 1,2
GreaterAffordability 3,4,5
902323
902323 Optisulin A4Ad rF.indd 1902323 Optisulin A4Ad rF.indd 1 2015/10/27 3:32 PM2015/10/27 3:32 PM

South African Journal of Diabetes - March 2017 | 1
EDITORIAL
The noise around novel therapies and emerging technologies such as continuous glucosemonitoring has never been louder than at present. This Journal is delighted to have ourcontributors write about some of these newer aspects of diabetes care.
What is less known, and thus something attracting little attention, seems to be the slow demise ofone of our country’s most precious resources - the diabetes nurse educator. As funders‘rationalize’ care for the many more patients with diabetes, and for those who will eventually bediagnosed with diabetes, there are moves afoot to diminish this key component of diabetes care.Intuitively prior to, but specifically confirmed after the Diabetes Control and Complications Trial(DCCT) publication in the early 1990’s, was the emerging central role of the diabetes nurseeducator. It is hard to conceive of a comprehensive diabetes service operated by a doctor alone.The notion seems prehistoric.
I am blessed where I work. The DNE team comprises of a staff of eight. We could not operate ourCentre without them. They operate our 24-hour dedicated ‘Hotline’ and undertake all of thesick-day management matters for patients during the office hours, over and above their usualworkloads. We are deeply grateful for their efforts, and have recently recognized that they too arenot immune to the stressors and strains inherent in their work. ‘Counselling the counsellors’ hasjust been rolled out at our Centre, and while only in its infancy, I hope it proves to be a valuableresource we can offer our Team. Much like the harms accrued from failing to screen forpreventable microvascular complications, we should all become more mindful that failing toidentifying team members ‘burning out’ without adequate support and intervention is likeconfining the person with diabetes to ‘conventional care’. Nobody deserves that!
Dr Stan LandauEditor
email: [email protected]
Editor’s comment

9568 SAJD Influvac 2017 Med Ad.indd 1 2017/03/08 1:01 PM

Contents
South African Journal of Diabetes - March 2017 | 3
CONTENTS
Volume 10 Number 1 • March 2017
EDITORDr Stan [email protected]
SUB-EDITORMichael [email protected]
EDITORIAL CONTRIBUTORSDr Larry Distiller:[email protected] Bench:[email protected] Greg Hough:[email protected] Brian Kramer:[email protected] Georgia Torres:[email protected]
ADVERTISING ENQUIRIESAngela BellCell: 082 451 0193 Tel: 011 787 9366 Fax: 088 011 787 9366Email: [email protected]
PUBLISHERSouth African Journal of Diabetesis published by:Homestead Publishing (Pty) Ltd (Reg. No. 2011/128152/07).
Postnet Suite 354Private Bag X11Craighall2024
PRODUCTIONAdéle GouwsOutput Reproductions
PRINTINGBusiness Print Centre
COPYRIGHTMaterial appearing in this Journalbelongs to the South AfricanJournal of Diabetes and/or theindividual contributors. Thecontents of this publication maynot be reproduced in any partwithout the written consent of thepublisher. The views expressed bycontributors do not necessarilyreflect the views of the publisher,editors or advertisers. While everyeffort has been made to ensureaccuracy, the editors, contributorsand publisher do not acceptresponsibility for errors, emissionsor inaccuracies in the publication.
EDITORIAL 1Dr Stan Landau
ORIGINAL ARTICLESDoes insulin allergy really exist? 7Dr Greg Hough
Diabetes Management in 2017 – What is new? 14Dr Larry Distiller
Cardiorespiratory fitness – The most potent and ignored solution to improving health outcomes 21Dr Georgia Torres
'Tis the season... Time to talk Flu Vaccination 24Marjolein Bench
A structured approach to the diabetes consultation 26Dr Stan Landau
Screening for diabetic retinopathy at the level of primary care 30Dr Brian Kramer
PRODUCT NEWSLilly Introduces Basaglar® Insulin Glargine in South Africa 12
CPD Accredited Diabetes Training 34

Specialists in human biosimilar insulins The economic burden of diabetes is increasing worldwide, with the greatest demands and increases in developing countries.1
Globally 415 million people have diabetes, with more than 14 million people in the African Region; The International Diabetes Federation predicts that by 2040 these figures will more than double.2
Three-and-a-half million South Africans (about 6 % of the population) suffer from diabetes and there are many more who are undiagnosed. It is estimated that another five million South Africans have pre-diabetes, a condition where insulin resistance causes blood glucose levels to be higher than normal, but not high enough yet to be type 2 diabetes.3
The need for more cost-effective insulin therapy is critical in reducing the financial burden on patients and health care systems.1
Biosimilars are distinctly different from generic drugs, as they are protein compounds that rely on modification for efficacy and are therefore bioequivalent rather than bioidentical. Biosimilars must follow precise manufacturing, processing and purification procedures, and are regulated to pass stringent laboratory and clinical trials before approval.1
BIOSULIN insulins were approved for use in South Africa more than 10 years ago and are marketed by Ascendis Pharma.
Biosimilar insulins have the potential to dramatically lower healthcare costs by delivering insulin with similar anti-glycaemic effect and adverse reaction profile to standard, more expensive insulin preparations.1
In the BEST study (SAMJ July 2013) BIOSULIN 30/70 insulin was tested to confirm equivalence to other human premixed insulin preparations on the South African market.1 Seventy-seven subjects with type 1 (n = 18) and type 2 diabetes mellitus (n = 59) were switched from their existing human premix insulin to BIOSULIN 30/70. The change in HbA
1c from baseline to 6 months was considered the primary endpoint of the study.1
BIOSULIN 30/70 achieved at least equivalent glycaemic control with no reported new or severe adverse events. In addition there was no significant difference in body weight in the study subjects during the 6-month period on BIOSULIN 30/70.1
Despite the more complex production process and regulatory requirements for biosimilars, they offer a price reduction of between 21 % and 47 % of the parent insulin and analogue insulin.4
For more information regarding Ascendis Pharma and their products, please contact Laurett Correia on [email protected]
References: 1. Segal D, Tupy D, Distiller L. The Biosulin equivalence in standard therapy (BEST) study − a multicentre, open-label, non-randomised, interventional, observational study in subjects using Biosulin 30/70 for the treatment of insulin-dependent type 1 and type 2 diabetes mellitus. SAMJ 2013;103(7):458-460:1-4. 2. South Africa | International Diabetes Federation. Available from https://www.idf.org/membership/afr/south-africa Accessed 15 February 2016. 3. Prevalence of diabetes in South Africa | Health24. Available from http://www.health24.com/Medical/Diabetes/About-diabetes/Diabetes-tsunami-hits-South-Africa- Accessed 15 February 2016. 4. Database of Medicine Prices February 2016. Available from http://www.mpr.gov.za/ Accessed February 2016
S3 Biosulin R (solution for injection). Each Biosulin R solution for injection contains 100 I.U/ml biosynthetic human insulin. Reg. No: 37/21.1/0670 S3 Biosulin N (solution for injection). Each Biosulin N solution for injection contains 100 I.U/ml biosynthetic human insulin. Reg. No: 37/21.1/0671 S3 Biosulin L (solution for injection). Each Biosulin L solution for injection contains 100 I.U/ml biosynthetic human insulin. Reg. No: 37/21.1/0672 S3 Biosulin 30/70 (solution for injection). Each Biosulin 30/70 solution for injection contains 100 I.U/ml biosynthetic human insulin. Reg. No: 37/21.1/0673
Applicant: Dezzo Trading 392 (Pty) Ltd. Co. Reg No: 2002/001923/07 Cnr Birch Road and Bluegum Avenue, Anchorville, Lenasia, 1827. P. O. Box 725 Lawley 1824. Tel: 011 857 2090 Fax: 086 664 6223. Customer Careline: 086 111 4721ZA.BIOS.01 05/2016
Increased use of biosimilar insulins has the potential for significant cost savings with no loss in patients’ glycaemic outcomes.1
Biosimilar insulins, such as BIOSULIN, will play an ever increasing role in the management of diabetes.1
Ascendis Pharma offers a comprehensive range of human insulins in cartridge form, from the short acting BIOSULIN R, to the intermediate acting BIOSULIN N and BIOSULIN L, as well as the biphasic insulin BIOSULIN 30/70.
HbA1c at baseline and after 6 months of therapy with BIOSULIN 30/70
Adapted from Segal D et al 1
Baseline
6 months
Overall Type 1 Type 2
Hb
A1c
(%
)
p=0.14
7.9
7.6
p=0.41
8.4
8.0p=0.19
7.7
7.4
1016-4838 Best Trial update and re-size for SAJD.indd 1 10/31/16 9:43 AM

XR 500 mgXR 750 mg
XR 1000 mg
ONCE DAILY
References: 1. Donnelly LA, Morris AD, et al. Adherence in patients transferred from immediate release metformin to a sustained release formulation: a population-based study. Diabetes, Obesity and Metabolism 2009;11:338-342. 2. Blonde L, Dailey GE, et al. Gastrointestinal tolerability of extended-release metformin tablets compared to immediate-release metformin tablets: results of a retrospective cohort study. Curr Med Research Opin 2004;20(4):565-572. 3. SEMDSA Guidelines 2012. Guideline for the Management of Type 2 Diabetes (Revised). Chapter 9.1. Journal of Endocrinology, Metabolism and Diabetes of South Africa. 2012;17(Suppl 1):523-531.
• Better compliance than standard metformin 1
• 77% less diarrhoea than standard metformin 2
• Reduces patient pill burden at optimal daily dose of 2000mg 3
Take your FREE DiabetesOnline Risk Assessment test at
diabetes.merck-africa.com
Glucophage® XR now provides a simple full dose spectrum solution to improve compliance:
S3 GLUCOPHAGE®XR 500 mg Modified Release Tablet. Each tablet contains 500 mg metformin hydrochloride. Reg. No. A39/21.2/0027. S3 GLUCOPHAGE®XR 750 mg Modified Release Tablet. Each tablet contains 750 mg metformin hydrochloride. Reg. No. 43/21.2/0185. S3 GLUCOPHAGE®XR 1000 mg Modified Release Tablet. Each tablet contains 1000 mg metformin hydrochloride. Reg. No. 45/21.2/0066. For full prescribing information, refer to the package insert approved by the Medicines Regulatory Authority. MERCK (PTY) LTD, Reg. no.: 1970/004059/07. 1 Friesland Drive, Longmeadow Business Estate South, Modderfontein. 1645. Tel: 011 372 5000 Fax: 011 372 5252. Report adverse events to [email protected] or +27 11 608 2588 (Fax line). SEA/GLUP/0317/0013
Glucophage XR Advert with DORA A4 V2.indd 1 2017/03/23 11:43

Insulin allergy was a common problem for endocrinologists anddiabetologists in the ‘bad old days’ of the relatively impureheterologous porcine and bovine insulins.
This problem has become much less common with time. The firstbreakthrough was the result of improvements in the purification ofpancreatic extracts. The second was the realisation that non-human insulinfrom each species used was unique and that they should not be mixed -porcine (pig) insulin should only be mixed with porcine insulin and bovine(cow) insulin with bovine insulin. However, the biggest breakthrough inreducing insulin allergies came in the mid 1980’s with the advent of highlypurified ‘mono-component’ human insulin.
The combination of these advances have made insulin allergy a rare andunusual condition with the current incidence estimated to be between 0.1and 3 %, depending on the definition used and the source of the data.
When we suspect insulin allergy in a patient, the initial approach shouldinclude the following considerations:• Rapidity of onset. It is important to establish how long after starting
the insulin the symptoms started. Was it immediate or some timeafterwards? This may help distinguish between immediate and delayedtype hypersensitivity reactions.
• Presence of systemic symptoms. If the reaction is limited to theskin, consider other causes.
• Careful examination of injection site and skin for othercauses. Because this is such a rare and unusual occurrence, considercauses other than an allergic response. Examine the rest of the skincarefully to exclude skin conditions such as dermatitis or urticaria.
• Has there been progression? Has the reaction become worse withsubsequent insulin injections or is it always the same?
• A careful history of insulins used and any recent changes. Thetiming of the reaction to these changes may be crucial in eitherconfirming or excluding an insulin allergy.
Before making a diagnosis of an insulin allergy, consider a simple injectionsite irritation. The following may reduce the likelihood of injection siteirritations and should be encouraged where this is considered.• Stop use of alcohol or other cleaning solutions. Alcohol swabs
can cause a reaction at the injection site, which may be mistaken for anallergy - the alcohol swab or one of its components may be responsiblefor the allergic reaction.
• Rotate injections sites regularly. Repeatedly injecting into thesame site is more likely to cause a reaction as well as lipohypertrophy,which may be mistaken for an allergic reaction.
South African Journal of Diabetes - March 2017 | 7
ORIGINAL
Does insulin allergyreally exist?
Correspondence:Dr Greg HoughE-mail: [email protected]
Dr Gregory HoughMBBCh, FCP (SA), Certificate inEndocrinology and Metabolism (SA)Physician/Endocrinologist/Diabetologist, CDE Branch, Port Elizabeth

• Ensure correct injectiondepth. Is the patient injectingdeeply enough or too deeply?Trying shorter needles maysolve this problem.
• Choose appropriateinjection sites. Avoid siteswhere belt buckles orwaistbands rub as these maycause a contact allergy, whichmay be mistaken for an allergicreaction to insulin.
• Massage injection sites for afew moments after injection.
• Inject in calm environments.
There are two types ofhypersensitivity reactions,immediate and delayed. Theimmunological processes aresignificantly different and a goodunderstanding of these will makeidentifying and treating them easier.
Immediate HypersensitivityReactionsThese occur within 1 hour after aninjection, although usually muchmore rapidly. They can be dividedinto Local immediate Reactionsand Systemic immediate reactions.
• Local immediatehypersensitivity reactions areusually characterized by pruriticerythema at injection sites.
• Systemic ImmediateHypersensitivity reactions willpresent with generalizedurticarial reactions, pruritus,angioedema and other olderinjection sites may react too.Nausea, diarrhoea, confusion,tremor, blurred vision anddiplopia have been reportedless often.
The onset of symptoms is usuallymonths to years after starting aparticular insulin. It may be morerapid if the patient has had previousexposure to a particular antigen,which may have been present inanother insulin preparation thepatient may have used.
Local symptoms may be theinitial response before systemicsymptoms occur.
PathogenesisThese are IgE mediated Type 1immunological reactions to insulinor additives. Sensitization occursbefore the allergic reaction is seen.
Many patients using insulin aresensitized (have IgE antibodies butdo not develop allergic reactions).However, re-exposure in certainsensitized patients results in cross-linking of IgE antibodies on mastcells and basophils with the releaseof histamine and otherinflammatory mediators.
South African Journal of Diabetes - March 2017 | 8
ORIGINAL
Figure 1: A diagnostic algorithm for patients suspected of having aninsulin allergy. Adapted from Heinzerling L, Raile K, Rochlitz H, ZuberbierT, Worm M. Insulin allergies: clinical manifestations and managementstrategies. Allergy 2008; 63: 148–155.
There are two types of hypersensitivityreactions, immediate and delayed. Theimmunological processes are significantlydifferent and a good understanding of these willmake identifying and treating them easier
Figure 2

Table1 : Excipients contained in some insulin preparations available inSouth Africa
Insulin detemir
• Zinc
• Metacresol
• Glycerol
• Phenol
• Disodium phosphate dihydrate
• Sodium chloride
• Water for injection
• Hydrochloric acid and/or sodium hydroxide
Insulin aspart
• Glycerol
• Phenol
• Metacresol
• Zinc chloride
• Disodium phosphate dihydrate
• Sodium chloride
• Hydrochloric acid/Sodium hydroxide
• Water for injections
insulin isophane (human) NPH
• Glycerol
• Phenol
• Metacresol
• Zinc chloride
• Disodium phosphate dihydrate
• Sodium chloride
• Sodium hydroxide or/and hydrochloric acid
• Protamine sulphate
• Water for injections
Insulin glargine
• Meta-cresol
• Glycerol
• Zinc chloride
• Hydrochloric acid
• Sodium hydroxide
• Water for injections
Insulin glulisine
• Tromethamine
• Metacresol
• Sodium chloride
• Polysorbate
• Water for injections
Monocomponent insulin
human (regular)
• Zinc chloride
• Glycerol
• Metacresol
• Sodium hydroxide (for
pH adjustment)
• Hydrochloric acid (for
pH adjustment)
• Water for injections
Both human insulins andinsulin analogues can induceimmediate hypersensitivityallergic reactions by formingantigenic epitopes. These epitopesmay be:• A non-self-epitope,• An altered-self-epitope,• Epitopes created by alternate
protein folding duringproduction or purification,
• Other epitopes exposed bysubcutaneous insulindegradation by proteases.
Insulins contain many othersubstances, which may alsoinduce immediate typehypersensitivity reactions.These substances must beconsidered before concludingthat it is a reaction to the insulinitself (Table 1).
It is important to know a little aboutsome of these substances, which mayindependently cause immediate-typehypersensitivity reactions• Protamine sulphate is a
protein isolated from fishsperm. It is complexed toinsulin to delay absorptionfrom the subcutaneousinjection site into the blood. Itis also used to reverse theanticoagulant effect of heparinand immediate allergicreactions and anaphylaxis havebeen well described. It maycause allergic reactionsthrough both IgE andcomplement-mediatedmechanisms, which means thata negative skin testing may notcompletely exclude it.
• Cresol is present as apreservative in most insulinsand should always beconsidered for immediate-typereactions. It is unfortunatelydifficult to test for, as solutions
are not readily available.• Latex may be found in trace
amounts in many types ofinsulin from the vialstoppers. Many are now latexfree to avoid this. However,consider this if previous latexallergy has been documentedin a patient.
• Zinc alters immunogenicity ofinsulin by changing thestructure of the B chain. Thisresults in a unique epitope,which may elicit animmediate-typehypersensitivity reaction.
South African Journal of Diabetes - March 2017 | 9
ORIGINAL
Insulins contain many other substances,which may also induce immediate typehypersensitivity reactions. These substancesmust be considered before concluding that it isa reaction to the insulin itself (Table 1)
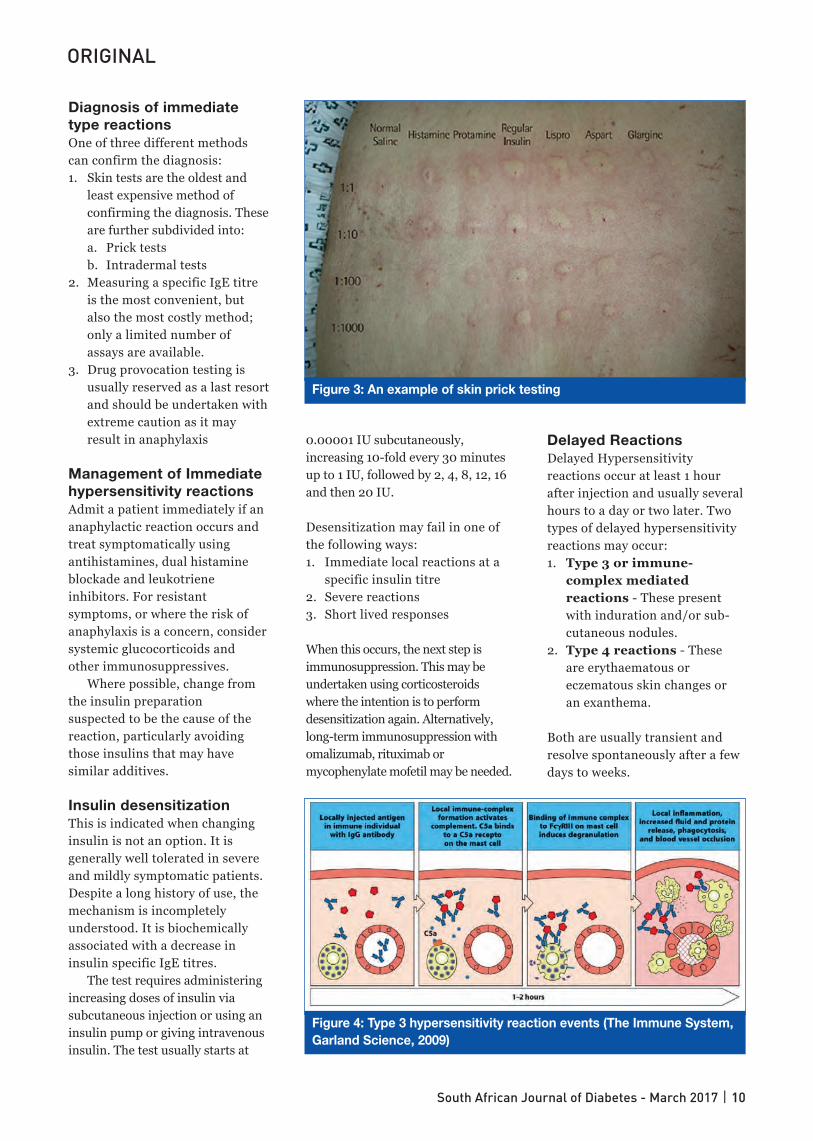
Diagnosis of immediatetype reactionsOne of three different methodscan confirm the diagnosis:1. Skin tests are the oldest and
least expensive method ofconfirming the diagnosis. Theseare further subdivided into:a. Prick testsb. Intradermal tests
2. Measuring a specific IgE titreis the most convenient, butalso the most costly method;only a limited number ofassays are available.
3. Drug provocation testing isusually reserved as a last resortand should be undertaken withextreme caution as it mayresult in anaphylaxis
Management of Immediatehypersensitivity reactionsAdmit a patient immediately if ananaphylactic reaction occurs andtreat symptomatically usingantihistamines, dual histamineblockade and leukotrieneinhibitors. For resistantsymptoms, or where the risk ofanaphylaxis is a concern, considersystemic glucocorticoids andother immunosuppressives.
Where possible, change fromthe insulin preparationsuspected to be the cause of thereaction, particularly avoidingthose insulins that may havesimilar additives.
Insulin desensitizationThis is indicated when changinginsulin is not an option. It isgenerally well tolerated in severeand mildly symptomatic patients.Despite a long history of use, themechanism is incompletelyunderstood. It is biochemicallyassociated with a decrease ininsulin specific IgE titres.
The test requires administeringincreasing doses of insulin viasubcutaneous injection or using aninsulin pump or giving intravenousinsulin. The test usually starts at
0.00001 IU subcutaneously,increasing 10-fold every 30 minutesup to 1 IU, followed by 2, 4, 8, 12, 16and then 20 IU.
Desensitization may fail in one ofthe following ways:1. Immediate local reactions at a
specific insulin titre2. Severe reactions3. Short lived responses
When this occurs, the next step isimmunosuppression. This may beundertaken using corticosteroidswhere the intention is to performdesensitization again. Alternatively,long-term immunosuppression withomalizumab, rituximab ormycophenylate mofetil may be needed.
Delayed ReactionsDelayed Hypersensitivityreactions occur at least 1 hourafter injection and usually severalhours to a day or two later. Twotypes of delayed hypersensitivityreactions may occur:1. Type 3 or immune-
complex mediatedreactions - These presentwith induration and/or sub-cutaneous nodules.
2. Type 4 reactions - Theseare erythaematous oreczematous skin changes oran exanthema.
Both are usually transient andresolve spontaneously after a fewdays to weeks.
South African Journal of Diabetes - March 2017 | 10
ORIGINAL
Figure 4: Type 3 hypersensitivity reaction events (The Immune System,Garland Science, 2009)
Figure 3: An example of skin prick testing

Diagnosis of delayedhypersensitivity reactionsWhere the reaction presents withinduration and/or sub-cutaneousnodules (Type 3 hypersensitivity)a biopsy may be helpful:• If vasculitis is present, it may
be expected to respond totopical corticosteroids.
• Granulomas may affect insulinabsorption and may explainodd responses to insulin doses.
• Where the reaction presentswith an erythaematous oreczematous skin change or an
exanthema (Type 4 reactions),patch testing usually showsreaction to insulin additives.This typically occurs to insulinisophane (human) NPH, cresolor zinc.
Management of delayedhypersensitivity reactionsBecause these usually resolvespontaneously, only symptomatictreatment is needed in mostcases. In many instances, thereaction will resolve before thepatient sees the doctor.
Reassurance and carefulexplanation is usually sufficientfor most patients. Wheresymptomatic treatment isneeded, topical corticosteroidsor antihistamines are first lineand will relieve mostsymptoms. Occasionallysystemic antihistamines maybe needed and very rarelysystemic corticosteroids.
South African Journal of Diabetes - March 2017 | 11
ORIGINAL
Figure 5: Type 4 delayed hypersensitivity reaction events (Biyani P (2014)Basics of Hypersensitivity. Available online from www.dentalnotebook.com/basics-hypersensitivity/ (Accessed 09 March 2017))
Because these usually resolve spontaneously,only symptomatic treatment is needed in mostcases. In many instances, the reaction willresolve before the patient sees the doctor
Summary of InsulinAllergy• Yes, insulin allergy does
exist today.• It is very uncommon
occurring in ± 1 % ofpatients using insulin.
• Insulin may be the cause orone of the many additivesand/or contaminants.
• When an insulin allergy issuspected, investigationswill reveal another cause in59 % of cases. For thisreason, we must activelylook for and exclude these asoutlined above.
• Insulin allergies can beclassified into immediateand delayedhypersensitivity reactions.
• Immediate type reactionsmay be progressive andresult in anaphylaxis –handle these carefully and,where indicated, in ahospital setting.
• Delayed type reactionsusually resolvespontaneously and requireonly symptomatic treatment.
References availableon request

Doctors treating people living with diabetes, nowhave access to a new basal insulin glargineoption, to better manage the condition.
Basaglar® (insulin glargine), a biosimilar of insulinglargine, now available in South Africa, is an injectable,prescription medicine designed to be taken at the sametime daily to lower blood glucose. Basaglar® should notbe used to treat diabetic ketoacidosis.
“While basal insulin has been a mainstay of diabetestreatment for many years, challenges still exist forpatients regarding initiating insulin and embracinginsulin therapy as part of their daily lives. Basaglar® is awelcome addition to our insulin portfolio, offering anoption for people with diabetes who need a long-actingsolution, supplemented by easily understandableeducational resources and tools to support patientsthroughout their insulin initiation,” explains Ann-MarieHosang, Managing Director of Lilly South Africa. Lillyhas a long history of developing and manufacturinginsulin, having introduced the world's first commercialinsulin more than 90 years ago.
Education and support are fundamental toadherenceWithout a plan to help patients stay organised and feelsupported throughout the initiation process, many findthe move to insulin therapy challenging to manage.Doctors also experience challenges transitioning apatient to insulin therapy. Patients with concomitantconditions and medications experience greatercomplexity in initiating insulin, therefore requiringsignificant education and support. In response, Lilly hascreated comprehensive healthcare provider and patientsupport materials, supported by diabetes educators, toalleviate this workload, and dispel the myths and stigmasurrounding insulin therapy initiation.
Initiate patients with an optimal solution, at aprice they can affordLilly is at the forefront of reimbursement and access,with Basaglar® having little or no co-payments on mostmedical schemes. This is an important considerationbecause diabetes treatment is a lifelong journey, oftencomplicated by other concomitant conditions thatcompound the ongoing costs of treating diabetes.Managing these costs is important to allow patients toadhere to their insulin regimen while minimising out-of-pocket expenses. Basaglar® represents significantfinancial relief to patients with diabetes. For patients on
South African Journal of Diabetes - March 2017 | 12
PRODUCT NEWS
Lilly Introduces Basaglar®
Insulin Glargine in South Africa medical aid, treatment costs are likely to be fullycovered, while for the uninsured or underinsured,Basaglar® comes at a price of up to 30 % less thancurrent market alternatives, whilst still providing thesame level of efficacy and quality.
Favourable reimbursement across entireinsulin portfolioHumalog®, Lilly’s rapid-acting insulin analogue, indicatedto improve glycaemic control in adults and children,provides an option for doctors to intensify treatment withBasalgar®, if and when required. Lilly offers furtheroptions through Humalog® Mix25™ and Humalog®
Mix50™. Together, these products represent one of themost comprehensive diabetes portfolios for patients, andattracting highly favourable reimbursement from medicalaids. Almost all plans under Discovery Health require noadditional co-payments for either Basaglar® or the entireHumalog® portfolio. Lilly constantly pursues solutions toensure comprehensive patient access.
At the forefront of diabetes careImportantly, doctors and patients need to see insulininitiation and treatment intensification as positivesteps toward the most important goal – which is toachieve as near normal blood glucose levels aspossible, in a manner tailored to patient needs.Through research and collaboration, a broad andgrowing product portfolio and commitment toproviding real solutions (medicines and supportprogrammes), Lilly strives to make life better for thoseaffected by diabetes globally.
Product information: Humalog Solution for injection. Insulinlispro (rDNA origin) 100 IU/ml. Reg. No. 29/21.1/0785.Humalog® Mix25™ Suspension for injection. Insulin lispro(rDNA origin) 25 % Insulin lispro, 75 % Insulin lispro protaminesuspension (NPL) 100 IU/ml. Reg. No. 33/21.1/0073. Humalog®
Mix50™ Suspension for injection. Insulin lispro (rDNA origin)50 % Insulin lispro, 50 % Insulin lispro protamine suspension(NPL) 100 IU/ml. Reg. No. 33/21.1/0074. Basaglar Reg. No.49/21.1/0708. For full prescribing information please refer tothe package insert currently approved by the MedicineRegulatory Authority. Humalog®, Basaglar® and Humalog®
KwikPen™ are trademarks of Eli Lilly and Company.
Eli Lilly (S.A.) (Pty) Ltd. Reg. No. 1957/000371/07. 1st Floor,Golden Oak House, Ballyoaks Office Park, 35 Ballyclare Drive,Bryanston Tel: +27 11 510 9300. ZADBT00573 Jan 2017

Humalog Humalog Humalog Humalog Mix25 Mix50 Humalog Basaglar Mix25 Mix50 Humalog Basaglar Cartridge Cartridge Cartridge Cartridge Kwikpen Kwikpen Kwikpen Kwikpen
NAPPI 861782003 705074001 862355001 722456001 706761001 706762001 706760001 722454001
Executive � �� � � � �� � �� �
Comprehensive � �� � � � � �� � �
Priority � �� � � � CDA CDA � CDA
Saver � �� � � � CDA CDA � CDA
Core � �� � � � CDA CDA � CDA
Smart � �� � � Not on Form Not on Form Not on Form � Not on Form
KeyCare � �� � �� Not on Form Not on Form Not on Form � Not on Form
DISCOVERY HEALTH REIMBURSEMENT SUMMARY
Product information: Humalog Solution for injection. Insulin lispro (rDNA origin) 100 IU/ml. Reg. No. 29/21.1/0785. Humalog®
Mix25™ Suspension for injection. Insulin lispro (rDNA origin) 25% Insulin lispro, 75% Insulin lispro protamine suspension (NPL) 100IU/ml. Reg. No. 33/21.1/0073. Humalog® Mix50™ Suspension for injection. Insulin lispro (rDNA origin) 50% Insulin lispro, 50%Insulin lispro protamine suspension (NPL) 100 IU/ml. Reg. No. 33/21.1/0074. Basaglar Reg. No. 49/21.1/0708.For full prescribing information please refer to the package insert currently approved by the Medicine Regulatory Authority.Humalog®, Basaglar®, Humalog® KwikPen™ and HumaPen SAVVIO™ are trademarks of Eli Lilly and Company.
Eli Lilly (S.A.) (Pty) Ltd. Reg. No. 1957/000371/07. 1st Floor, Golden Oak House, Ballyoaks Office Park, 35 Ballyclare Drive, BryanstonTel: +27 11 510 9300. ZADBT000574 January 2017
S3 S3
S3S3
INTRODUCING THE MOST COMPREHENSIVE INSULIN PORTFOLIO
HumaPen® SAVVIO™ : Designed for confidenceFeatures inspired by the needs of people who use devices every day
Discovery Health Plans
Lilly_reimusement.qxp_Layout 1 2017/03/10 12:27 PM Page 1

In January each year, the American Diabetes Association (ADA)publishes their updated ‘Standards of Medical Care in Diabetes’.Updated guidelines and algorithms from the American Association of
Clinical Endocrinologists (AACE) and American College of Endocrinology(ACE) usually supplement the ADA document. The local Society forEndocrinology, Diabetes and Metabolism of Southern Africa (SEMDSA) lastpublished guidelines for the management of type 2 diabetes in 2012, butnew and updated guidelines are expected by April this year.
When considering guidelines, most of us automatically default in ourminds to drug usage and algorithms. However, guidelines and standards ofcare recommendations should and do go far further than that. Much spacein the ADA and AACE/ACE documents is devoted to treatment and controlof comorbidities and the amelioration of wider cardiovascular risk (lipidsand blood pressure control, weight management and smoking cessation).Recent figures from the USA show that 33 - 49 % of patients still do notmeet targets for glycaemic, blood pressure or cholesterol control - only 14 %meet targets for all three measures, while also avoiding smoking. Althoughwe do not know these figures for South Africa, they are unlikely to be anybetter, and are probably worse.
Patient-centred care and team-facilitated self-managementsupport re-emphasized
The ADA (2017) stresses that a “patient-centred communication style thatuses active listening, elicits patient preferences and beliefs, and assessesliteracy, numeracy, and potential barriers to care should be used tooptimize patient health outcomes and health-related quality of life”.
“A major barrier to optimal care is a health care system that is oftenfragmented, lacks clinical information capabilities, duplicates services andis poorly designed for the coordinated delivery of chronic care” (ADA,2017). The 2017 ADA Standards of Care document notes that in nearly aquarter of patients, uncontrolled diabetes, blood pressure and lipids areassociated with poor medication adherence. Based on this, the documentplaces much emphasis on patient-centred care and recommends that beforeprescribing medication, “Providers should assess social context, includingpotential food insecurity, housing stability, and financial barriers, and applythat information to treatment decisions” (‘A-Grade’ Evidence). Theseconsiderations are especially important and relevant to the socioeconomicsituation in our country.
Patients should also be provided with self-management support fromdiabetes nurse educators, professional or lay health coaches, or communityhealth workers when available.
South African Journal of Diabetes - March 2017 | 14
ORIGINAL
Diabetes Managementin 2017 – What is new?
Correspondence:Dr Larry DistillerE-mail: [email protected]
Dr Larry DistillerSpecialist Physician /Endocrinologist, CDE Houghton

The 2017 updates also placemuch emphasis on lifestyleintervention with the openingprinciple of the AACE/ACEConsensus statement beingdevoted to this aspect - “Lifestyleoptimization is essential for allpatients with diabetes. Lifestyleoptimization is multifaceted,ongoing, and should engage theentire diabetes team. However,such efforts should not delayneeded pharmacotherapy, whichcan be initiated simultaneouslyand adjusted based on patientresponse to lifestyle efforts. Theneed for medical therapy shouldnot be interpreted as a failure oflifestyle management, but as anadjunct to it” (AACE/ACE, 2017).While this is not new, both theADA and AACE/ACE documentsonce again stress this vital aspectof care, which is all too often lostwith the excitement around andexpectations of new drugs.
A more insightful approachto obesityAs before, weight loss warrantsspecial mention and should bepromoted in all people with type 2diabetes who are overweight orobese. Obesity should be regardedas a chronic disease, requiring along-term commitment totherapy. Given the knowntherapeutic effects of weight lossto lower glycaemia, improve lipidprofiles, reduce blood pressure,prevent or delay the progressionto type 2 diabetes in those withprediabetes and decreasemechanical strain on the hips andknees, the AACE/ACE documentrecommends consideration ofweight loss in all overweight andobese patients with ‘prediabetes’or type 2 diabetes. Weight losstherapy should consist of anegotiated ‘lifestyle prescription’that includes a healthy,reduced-calorie meal-plan,regular physical activity,sufficient amounts of sleep,
behavioural interventions,smoking cessation and avoidanceof all tobacco products.
The AACE and ACE haveemphasized a complications-centric model as opposed to aBody Mass Index (BMI)-centricapproach for the treatment ofpatients who are obese oroverweight. People who willbenefit most from medical andsurgical intervention have twogeneral categories of obesity-related complications:1. insulin resistance/
cardiometabolic disease and2. biomechanical consequences of
excess body weight.
We should evaluate such patientsfor the risk, presence, and severityof complications, regardless ofBMI, and use our assessment toguide treatment planning andfurther evaluation. Together withour patients, we should setappropriate and achievabletherapeutic goals and selectappropriate types and intensities oftreatment. This may help patientsachieve their weight-loss goalslinked to the prevention oramelioration of weight-relatedcomplications. The primaryclinical goals of weight losstherapy in diabetes andcardiovascular risk managementare to prevent progression to type 2diabetes in patients withprediabetes and to achieve theHbA1c glycaemic target and lipidand blood pressure targets forpatients with established type 2diabetes. Bariatric surgery shouldbe considered for adult patientswith a BMI ≥35 kg/m2 and
comorbidities, especially iftherapeutic goals are not attainablewith other interventions.
Screening for dysglycaemiaand diabetesWith the rising incidence ofundiagnosed type 2 diabetes and‘prediabetes’, the issue ofscreening for these conditions hasbeen under discussion for someyears, with differingrecommendations by differentsocieties. This year, the ADAdevoted an entire section to thisissue. Prediabetes reflects failingpancreatic islet beta-cellcompensation in patients withinsulin resistance, most
commonly caused by excessbodyweight or obesity. Prediabetesincludes the dysglycaemic states ofimpaired glucose tolerance andimpaired fasting glucose. Either ofthese conditions may beassociated with as much as a 5-fold increase in the risk of futuretype 2 diabetes.
The recommendations forscreening now include:• Screening for prediabetes and
risk for future diabetes inasymptomatic adults shouldbegin with an informalassessment of risk factors orthe use of validated riskassessment tools. This requiresan awareness by the healthcare professional that theremay be an increased risk ofdiabetes in those with the‘metabolic syndrome’,hypertension, dyslipidaemia,obesity or a family history oftype 2 diabetes.
South African Journal of Diabetes - March 2017 | 15
ORIGINAL
Together with our patients, we should setappropriate and achievable therapeutic goalsand select appropriate types and intensitiesof treatment

• Testing for prediabetes and riskfor future diabetes inasymptomatic people should beconsidered in adults of any agewho are overweight or obese(BMI >25 kg/m2 and >23 kg/m2
in Asians) and who have oneor more additional risk factorsfor diabetes.
• For all people, testing shouldbegin at age 45 years.
• If tests are normal, repeattesting carried out at aminimum of 3-year intervals isreasonable.
• Testing for type 2 diabetesshould be considered in childrenand adolescents who areoverweight or obese and whohave two or more additional riskfactors for diabetes.
• In patients with diabetes, it isvital to identify and treat otherrisk factors for cardiovasculardisease (CVD).
As for how best to screen for type 2diabetes, the ‘B-Grade’ ADArecommendation is not veryhelpful, regarding fasting plasmaglucose, the 2-hour plasmaglucose after a 75 g oral glucosetolerance test and A1C as“equally appropriate”.
The primary goal of prediabetesmanagement is weight loss.Whether achieved through lifestyletherapy, pharmacotherapy, surgery,or some combination thereof,weight loss reduces insulinresistance and may preventprogression to diabetes as well asimprove plasma lipid profile andblood pressure. When indicated,bariatric surgery can be highlyeffective in preventing progressionfrom prediabetes to type 2 diabetes.
With regard to screening for anddiagnosing type 1 diabetes, the ADArecommends that blood glucoserather than A1C should be used todiagnose the acute onset of type 1diabetes in individuals withsymptoms of hyperglycaemia.Screening for type 1 diabetes by
measuring autoantibodies iscurrently recommended only in thesetting of a research trial or in first-degree family members of someonewith type 1 diabetes. Persistence oftwo or more autoantibodiespredicts future clinical diabetes.
Gestational Diabetes – thewaters are still murky…Gestational diabetes receivessignificant coverage in the ADA2017 Standards of Medical Caredocument. They advise that womenwith risk factors be tested forundiagnosed diabetes at the firstprenatal visit using standarddiagnostic criteria. They thenrecommend that those who testnegative be tested for gestationaldiabetes mellitus at 24–28 weeks ofgestation. If gestational diabetes isfound to be present, these womenshould be tested for persistentdiabetes at 4–12 weeks postpartum,using the oral glucose tolerance testand clinically appropriate non-pregnancy diagnostic criteria.
Women with a history ofgestational diabetes mellitus shouldthen have lifelong screening for thedevelopment of diabetes orprediabetes at least every 3 years.Those found to have prediabetesshould receive intensive lifestyleinterventions or metformin toprevent diabetes.
The diagnostic criteria forscreening for and diagnosinggestational diabetes have been abone of contention for some time.Unfortunately, the 2017 ADAguidelines do not shed any furtherlight in this, but rather giveoptions of:• A traditional ‘One-step strategy’
using a fasting (in the morningafter an overnight fast of at least8 hours) 75-g oral glucosetolerance test (OGTT), at 24-28weeks of gestation in women notpreviously diagnosed with overtdiabetes. Plasma glucose ismeasured fasting and at 1 and 2
hours. The diagnosis of GDM ismade when any of the statedplasma glucose values are metor exceeded (Fasting: 5.1mmol/l, 1 hour: 10.0 mmol/l,2 hour: 8.5 mmol/l).
• A ‘Two-step strategy’ where aninitial 50 g non-fasting ‘glucoseload test’ (GLT) is performed at24–28 weeks of gestation inwomen not previouslydiagnosed with overt diabetes. Ifplasma glucose at 1 hour post-load exceeds a level of 7.2 to7.8 mmol/l (sensitivity andspecificity considerations stillcloud a clear cut-point) a fastingOGTT using a 100 g load isindicated. Plasma glucose levelsare measured fasting and at1, 2, and 3 hours after theOGTT. Unfortunately, noconsensus exists between twosets of cut-pointsrecommended by Carpenter andCoustan or the NationalDiabetes Data Group and thecut-points recommended in the‘one-step strategy’.
So, rather than shedding light onthe diagnosis of GestationalDiabetes, the ADA simplyconfuses the situation further.The AACE/ACE 2017 consensusstatement on type 2 diabetesdoes not deal with gestationaldiabetes at all, choosing to ignorethe condition. We will have towait for the SEMDSA 2017Guidelines, which we hope willclarify the situation.
Glycaemic targetsRegarding glycaemic targets, boththe ADA and AACE/ACE continueto stress the importance ofindividualised targets. Once again,the ADA recommends a targetHbA1c of <7 % for most adults,although AACE/ACE still aims for<6.5 % as their recommendation.The ADA, however, does state thatproviders might reasonablysuggest more stringent A1C goals
South African Journal of Diabetes - March 2017 | 16
ORIGINAL

(such as 6.5 %) for selectedindividual patients, if this can beachieved without significanthypoglycaemia or other adverseeffects of treatment. This mightinclude those with short durationof diabetes, type 2 diabetes treatedwith lifestyle or metformin only,long life expectancy, or nosignificant cardiovascular disease.All societies recommend lessstringent A1C goals (up to 8 %) forpatients with a history of severehypoglycaemia, limited lifeexpectancy, advancedmicrovascular or macrovascularcomplications, extensive comorbidconditions, or long-standingdiabetes in whom a better A1C isdifficult to achieve, despitediabetes self-managementeducation, appropriate glucosemonitoring, and effective doses ofmultiple glucose-lowering agents,including insulin.
Self-Monitoring of BloodGlucose (SMBG)The role of SMBG in patients withtype 2 diabetes has beencontentious for some time, withsome studies showing no benefitfor those on oral agents, whileothers suggesting that regularSMBG may improve patientcompliance and glycaemic controlwhen used as a self-education tool.The ADA concur with the latter,stating that when prescribed aspart of a broad educationalprogramme, SMBG may help toguide treatment decisions and/orself-management for patientstaking less frequent insulininjections or noninsulin therapies.They also recommend that patientsusing intensive insulin regimensshould perform self-monitoring ofblood glucose prior to meals andsnacks, at bedtime, occasionallypostprandially, prior to exercise,when they suspect low bloodglucose, after treating low bloodglucose until they arenormoglycaemic, and prior to
critical tasks such as driving.Importantly, when prescribingSMBG, ensure that patients receiveongoing instruction and regularevaluation of SMBG technique,SMBG results, and their ability touse SMBG data to adjust therapy.
PharmacotherapiesWith the advent of so many newertherapeutic agents on the marketover the past few years, and withmore to come, the appropriatechoice of therapeutic agent isbecoming increasingly difficult.This is compounded by the factthat in the South African context,many of these newer and arguablypossibly better agents are lessaffordable - while they may havefavourable therapeutic profiles,they cannot be widely prescribed inour environment. Thus, reviewingthe therapeutic algorithms for theUS market is probably a pointlessexercise and we will have to awaitthe publication of the updatedSEMDSA Guidelines for SouthAfrica. However, some generalprinciples laid out by theAACE/ACE are worth noting. Onceagain, individualization of choice oftherapies is stressed, based onpatient preferences, and on themedications themselves. Somefactors affecting therapeuticchoices include antihyperglycaemicefficacy, risk of hypoglycaemia, riskof weight gain, other adverseeffects, ease of use, likelyadherence to therapy and cost andsafety with regard to the heart,liver and kidneys. Minimizingthe risk of hypoglycaemia andweight gain is a priority.Furthermore, combinationtherapy is usually required and this
should involve agents withcomplementary mechanisms ofaction. Comprehensivemanagement includes lipid andblood pressure therapies andtreatment of related comorbidities.
Keeping an eye on the ball…Therapy must be evaluatedfrequently (e.g., every 3 months)until stable. Multiple criteria shouldbe used, including A1C, SMBGrecords (fasting and postprandial),documented and suspectedhypoglycaemic events, lipid andblood pressure values, otheradverse events (weight gain, fluidretention, hepatic or renalimpairment, or CVD),comorbidities, other relevantlaboratory data, concomitant drugadministration, complications ofdiabetes, and psychosocial factorsaffecting patient care. Less frequentmonitoring is acceptable oncetargets are achieved. Finally, andimportantly, the therapeuticregimen should be as simple aspossible to optimize adherence.
*All data reported on and discussedhere was obtained from thefollowing two documents, which thereader is encouraged to read in full.• American Diabetes Association.
Standards of Medical Care inDiabetes 2017. Diabetes Care2017: (Supp 1) 40;1-142
• Consensus Statement by theAmerican Association of ClinicalEndocrinologists and AmericanCollege of Endocrinology on theComprehensive Type 2 DiabetesManagement Algorithm – 2017Executive. Summary. EndocrinePractice 2017.Doi:10.4158/EP161682.CS
South African Journal of Diabetes - March 2017 | 17
ORIGINAL
With the advent of so many newer therapeuticagents on the market over the past few years, andwith more to come, the appropriate choice oftherapeutic agent is becoming increasingly difficult

0328 ACCU_Instant_A4Ad_FA1.indd 1 3/7/17 4:24 PM

C
M
Y
CM
MY
CY
CMY
K
0411 ACCU_FastClix A4 Ad_FA.pdf 1 3/30/17 8:38 AM


Asignificant amount of scientific evidence has established that lowcardiorespiratory fitness (CRF) levels are associated with a highrisk of cardiovascular disease (CVD) and all-cause mortality,
including mortality attributed to cancers of the breast and digestive tract(Blair et al., 1989; Sui et al., 2007; Khan et al., 2012; Sawada et al., 2014).Furthermore, improvements in CRF have been associated with a reductionin mortality risk (Lee et al., 2010; Lee et al., 2011). Thus, CRF isrecognized as an important marker of cardiovascular health. Yet, it is theonly major risk factor not routinely and regularly assessed in a clinicalsetting (Mark et al., 2003; Kaminsky et al., 2013).
This article will review the evidence for the importance of measuringand improving CRF in healthy individuals and in individuals with disease.
CRF as a predictor of health outcomesCRF has been shown to be a strong and independent risk factor forcardiovascular disease (CVD) and all-cause mortality, for the healthyand individuals with disease (Church et al., 2005; Sui et al., 2007;Kodama et al., 2009; Kokkinos et al., 2010; Swift et al., 2013).
Data from Blair et al. (1989) showed that increasing CRF from a lowto a moderate level among healthy men and women reduces death rateby 59 %.
The meta-analysis of Kodama et al. (2009) found that subjects with lowCRF, when compared with subjects in the most-fit tertile, had a 70 % and56 % higher risk for all cause and cardiovascular mortality, respectively.
Cardio-respiratory fitness is the risk factor that contributes the highestpercentage to all-cause deaths when compared with other traditional riskfactors (Blair 2009). Gupta et al. (2011) and Vigen et al. (2012) also foundthat cardiorespiratory fitness is a stronger predictor of CVD mortalitywhen compared to other traditional risk factors.
Dietary patterns and regular physical activity were 2 of 9 factorsidentified by the INTERHEART Study (Yusuf et al., 2004) accounting formost of the risk of myocardial infarction globally in both sexes and at all
South African Journal of Diabetes - March 2017 | 21
ORIGINAL
Correspondence:Dr Georgia TorresE-mail: [email protected]
Dr Georgia TorresMedical Wellness Director,Activate Executive & Medical Wellness Centre,Bryanston, Sandton
Cardiorespiratoryfitness – The mostpotent and ignoredsolution to improvinghealth outcomes

ages in all regions. However,other studies have furtherdemonstrated CRF to be a morepowerful predictor of mortalityrisk than traditional risk factors(smoking, hyperlipidaemia,hypertension, obesity, type 2diabetes) and traditional testvariables (ST-segmentdepression, haemodynamicresponses) (Myers et al., 2002;Mora et al., 2003; Gulati et al.,2003; Myers, 2014). Recently,CRF (and not just exercise) hasbeen identified as anindependent predictor,improving the risk of predictionover and above the traditionalCV risk factors.
Moreover, the associationbetween CRF, CVD and all-cause mortality is independentof existing cardiovasculardisease (Franklin, 2002) or thepresence of chronic diseaseand/or other CVD risk factors(Blair, 2009, Myers et al., 2002,Myers et al., 2014). Forexample, the data of Myers et al.(2002), showed a 44 % decreasein all-cause mortality amongpeople with diabetes whenincreasing CRF by 22 %. Inaddition, Myers et al. (2002)found that individuals withCVD had the same relativerisk of death as those withoutCVD (and at a CRF levelachieved at the end of the finalstage of a graded exercise test of>13 MET*) when their CRF levelwas >10.7 MET.
In addition, these individualshad a reduced mortality ratewhen compared with thosewithout CVD disease who had aCRF level of <12.9 MET. Myers etal. (2002) further demonstrated
that the least fit individuals (withor without CVD), had a morethan 4-fold increase in all-causemortality risk compared with themost fit individuals.
Myers et al. (2014) also citedthe independent and interwovenimportance of CRF to health status.
The association of CRF andmortality reduction is alsoindependent of age. Blair et al.(2000) found that an 80-year-oldat a moderate level of CRF hasthe same crude death rate as a60 year old at a low CRF level. Inaddition, Nylen et al. (2010)highlighted that increasing CRFlowers the mortality risk inpeople with diabetes irrespectiveof age.
In addition, an individual’sdecline in CRF level has beenshown to predict thedevelopment of hypertension,hypercholesterolemia, metabolicsyndrome and midlife metabolicoutcomes (Lee et al., 2012; Chowet al., 2014).
A decrement in CRF of 2 - 3MET was associated with a 2 - to5-fold higher CVD risk or all-causedeath rate in the Lipid ResearchClinics Mortality Follow-up study(Ekelund et al., 1988).
CRF also favourablyinfluences the biologicalmechanisms for disease. Forexample, women with a CRF level of< 35 ml O2.kg-1.min-1 and men
with a level of < 44.2 ml O2.kg-1.min-1
were 5 and 8 times respectively, morelikely to have a cluster ofcardiovascular risk factors than thosein the highest quartile of CRF levels(≥40.8 and ≥50.5 ml O2.kg-1.min-1
in women and men, respectively -Aspenes et al., 2011). Similarly,a higher CRF has beenassociated with lower visceraladiposity, improved insulinsensitivity, lower levels ofinflammation and morefavourable lipoprotein profiles(Arsenault et al., 2007; Kawanoet al., 2009; Lavie et al., 2011).
Lee et al. (2011) found thatincreases in CRF level decreasedall-cause and CVD mortality. Incontrast, changes in percentagebody fat or body weight, did notaffect all-cause and CVDmortality. The authors thushighlighted the importance ofpreventing fitness loss with age,regardless of whether BMIchanges. Maintaining orimproving fitness may alsoattenuate some potentiallynegative effects of weight gain onmortality. This data confirms thatthe long-term effect of CRFchange is likely to be at least asimportant as weight loss forreducing premature mortality.Therefore, increased attentionneeds to be placed on strategiesto maintain or improve fitness.
Church et al. (2004) alsoinvestigated body compositionand exercise capacity (CRF) aspredictors of mortality amongmen with diabetes. They found asteep, inverse gradient betweenCRF and mortality among thiscohort. This association was
South African Journal of Diabetes - March 2017 | 22
ORIGINAL
Recently, CRF (and not just exercise) has beenidentified as an independent predictor,improving the risk of prediction over and abovethe traditional CV risk factors
*The Metabolic Equivalent of Task [MET] is a physiological measureexpressing the energy cost of various physical activities by the amount of oxygen uptake, circulation and utilization needed at the muscle level toperform work at a certain level of physical activity, compared to the energyexpended by an individual while seated at rest (1 MET ~ 3.5 ml O2.kg-1.min-1).

independent of BMI. Even inthose individuals with diabetesand an obese BMI classification,a 63.6 % reduction in mortalityrisk was seen when CRFimproved from < 8.8 MET to8.8–10.08 MET. Should the focusthen be on improving CRF orreducing obesity in individualswith diabetes?
Furthermore, a single baselinemeasure of low fitness has beenassociated with both CVD andnon-CVD mortality across threedecades of follow-up in men andwomen (Vigen et al., 2012).
CRF has recently beenexpressed in the context ofsurvival benefit per metabolicequivalent (MET) multiples of theresting metabolic rate (3.5 mlO2.kg-1.min-1). The St JamesWomen Take Heart Project(Gulati et al., 2003) showed thata 1 MET increase in CRF (a smallincrement achievable by mostindividuals) is associated with a17 % improvement in survivalrate. Other studies noted a 10 -25 % improvement in survival per1 MET increase in CRF (Mark etal., 2003; Mora et al., 2003;Myers et al., 2004; Kokkinos etal., 2008; Nes et al., 2014).
It should be noted that highlevels of CRF are not necessaryto provide all the healthbenefits outlined above.Individuals with CRF levels of< 5 MET have a high risk ofmortality, whereas those withlevels at >8 to 10 MET areassociated with significantlylow mortality rates (Myers etal., 2002; Church et al., 2004;Kodama et al., 2009).
CRF and preoperativeprediction of surgical risk This article will not review thisarea except to highlight that CRFhas been found to be a strongpredictor of preoperative surgicalrisk, even to the extent thatrecently, CRF testing has beenused as a primary assessment inpatients with heart failure to assessthe timing of heart transplantation(Arena et al., 2014).
CRF, Mental illness andStressStudies have linked higher levelsof CRF to a reduced risk ofdeveloping both dementia andAlzheimer’s disease (Defina etal., 2013; Burns et al., 2008;Liu et al., 2012).
Higher levels of CRF are alsoassociated with lower measuresof anxiety and symptoms ofdepression (Dunn et al., 2005).
CRF, ‘Metabolic Syndrome’and Type 2 Diabetes There is an inverse associationbetween CRF and the risk ofdeveloping metabolic syndrome,‘prediabetes’ and type 2 diabetes(Lee et al., 2009; Earnest et al.,2013; Sieverdes et al., 2010).
CRF and CancerHigher levels of CRF areassociated with a lower risk ofdeveloping certain cancers (Peel
South African Journal of Diabetes - March 2017 | 23
ORIGINAL
Studies have linked higher levels of CRF to areduced risk of developing both dementia andAlzheimer’s disease (Defina et al., 2013; Burnset al., 2008; Liu et al., 2012)
The consistent research findings cited in thisarticle should convince us to alter our focus inthe health industry
et al., 2009; Sui et al., 2010).A meta-analysis (Schmid et
al., 2015) reported a 20 - 45 %lower risk of all-cause cancermortality in individuals with amoderate and high CRF level,respectively, when compared tothe low CRF group, irrespectiveof adiposity.
CRF and DisabilityImprovements in CRF have beenassociated with a reduced risk ofdeveloping disability amongobese adults with type 2 diabetes(Rejeski et al., 2012).
ConclusionThe consistent researchfindings cited in this articleshould convince us to alter ourfocus in the health industry.Our focus should shift fromweight loss, aesthetics andspecific disease parameters toimproving CRF as a majorhealth outcome. Thus, CRFshould be added as a vital signand efforts to improve CRFshould become a standard partof health care provider andfitness professional protocol.
In addition, CRF isresponsive to therapy (exerciseintervention), and thus serialmeasures of this variable arevaluable in risk classification.Individuals in whom CRFincreases betweenexaminations have a decreasedrisk of adverse health outcomes(Ross et al., 2016). This is animportant message that allhealth care providers shouldcommunicate to their patients.
References available on request

Seasonal influenza is an acute viral infection caused by an influenza virus.There are three types of seasonal influenza - A, B and C. Type Ainfluenza viruses are further typed into subtypes according to different
kinds and combinations of virus surface proteins. Among the many subtypesof influenza A viruses, influenza A(H1N1) and A(H3N2) subtypes are currentlycirculating among humans in every part of the world. Type C influenzainfections occur much less frequently than A and B. That is why only influenzaA and B strains are included in seasonal influenza vaccines.
All people with diabetes, including those who are pregnant, should bevaccinated against influenza (flu) regardless of the type of diabetes management.This is because people with diabetes have a higher risk of potentially seriouscomplications of flu infections such as pneumonia. Elevated blood glucose levels,and increased insulin requirements, as responses to infection, can increase therisk of diabetic ketoacidosis (DKA) or Hyperglycaemic Hyperosmolar State(HHS), both of which can be potentially fatal if left untreated.
A large, 7-year epidemiologic study from the United Kingdom suggests thatpeople who have type 2 diabetes can significantly lower their risk of majorcardiovascular events such as stroke and heart failure during the influenzaseason by receiving the flu vaccine.
Researchers from Imperial College, London found that people with type 2diabetes who were vaccinated had a 30 % lower risk of hospitalization for stroke,a 22 % lower risk for heart failure, and a 15 % lower risk for pneumonia or flu,compared with their unvaccinated counterparts. In addition, the vaccinatedpatients had a 24 % lower risk of death from any cause during the flu season.
An annual flu vaccination is thus one of the 15 Healthcare Essentials, the vital checksand services that Diabetes UK recommends as the minimum level of healthcare everyperson with diabetes deserves and should expect (Diabetes UK, 2016).
What are the 15 Healthcare Essentials?1. Get your blood glucose levels measured (HbA1c blood test)2. Have your blood pressure measured3. Have your blood fats measured4. Have your eyes screened for signs of retinopathy5. Have your feet and legs checked6. Have your kidney function monitored7. Get ongoing, individual dietary advice8. Get emotional and psychological support9. Be offered a local education course10. See specialist healthcare professionals11. Get a free flu vaccination12. Receive high-quality care if admitted to hospital13. Have the chance to talk about any sexual problems14. If you smoke, get support to quit15. Get information and specialist care if you are planning to have a baby
South African Journal of Diabetes - March 2017 | 24
ORIGINAL
Correspondence:Marjolein BenchE-mail: [email protected]
Marjolein BenchBPharm IMM
'Tis the season...Time to talk Flu Vaccination

People with diabetes can usethis list to talk to their diabetesteam about their individualneeds as part of their annualcare planning review. In thisreview, patient and practitionershould agree on care priorities,discuss personal targets andagree on a written plan of actionto help the person with diabetesto reach them.
The flu virus changes ormutates, which is why every yeara vaccine is produced based onthe strains of the virus expectedto be circulating. The flu vaccineis not 'live' and cannot give aperson the flu, but because fullimmunity can take about twoweeks to develop, some peoplemay develop the illness afterbeing vaccinated if they arealready incubating the virus intheir system.
Vaccination should bepostponed for people with afeverish illness or infection,and avoided for those whohave experienced seriousallergic reaction to a fluvaccination in the past.
People who have an eggallergy may be at increased riskof reaction to flu vaccinationbecause some flu vaccines arecultured using eggs.
Timing of the influenzaseason and vaccinationThe South African influenzaseason falls in the wintermonths. The average onset ofthe influenza season over thepast 28 years has been firstweek of June. However, theseason has started as early aslast week of April and as late as
first week of July, so it’simportant that the vaccine beadministered in time for the fluseason. A protective antibodyresponse to influenzavaccination generally takesabout 2 weeks to developfollowing vaccination and the fluseason typically starts aroundMay. Thus, for the South Africaninfluenza season, the optimaltime for vaccination is aroundMarch/April each year. Thelength of the protection varies,but usually lasts 6 to 12 months.Patients vaccinated a short timebefore the start of the expectedinfluenza activity (March /April in the southernhemisphere) may therefore beexpected to be protected forinfluenza infections or itscomplications during the wholeinfluenza season.
Contraindications to theInfluenza vaccine• Persons with a history of
anaphylaxis (severeallergic/hypersensitivereactions) following receipt ofany vaccine componentincluding eggs, neomycin orpolymixin antibiotics
• Persons with a history of
severe reaction to previousinfluenza vaccination
• Persons who developedGuillain-Barrè syndromewithin 6 weeks of receiving aninfluenza vaccine
• Children <6 months of age• The presence of febrile illness
or active infection. (Thevaccine should be postponeduntil after recovery).
Recommended everydaypreventive actions to stopthe spread of flu• Cover the nose and mouth with
a tissue when coughing orsneezing and throw the tissueaway after using it;
• Wash hands often with soapand water, especially aftercoughing or sneezing;
• Avoid touching eyes, nose, andmouth (flu viruses are spreadthat way); and
• Patients with flu-likesymptoms should stay at homefor 24 hours after the fever isgone (without the use ofanalgesics / antipyretics).
People with type 2 diabetes mayderive substantial benefits fromcurrent vaccines, includingprotection against hospitaladmission for some majorcardiovascular events. Thisunderlines the importance ofinfluenza vaccination as part ofcomprehensive preventative carein this high-risk population.
References on request
South African Journal of Diabetes - March 2017 | 25
ORIGINAL
Vaccination should be postponed for peoplewith a feverish illness or infection, and avoidedfor those who have experienced serious allergicreaction to a flu vaccination in the past
Patients vaccinated a short time before thestart of the expected influenza activity (March /April in the southern hemisphere) maytherefore be expected to be protected forinfluenza infections or its complications duringthe whole influenza season

Any interaction with a patient typically follows a structured approach ofcareful history taking, detailed and focused clinical examination and theperformance, if needed, of laboratory tests. Complacency is the enemy
here, turning an interaction with a patient into a tedious melodrama instead of anexciting mix of diplomacy, psychology and challenging medical detective work.
Both type 1 and type 2 diabetes are chronic medical conditions. More oftenthan not, interaction with these patients will be for matters unrelated to thediabetes state e.g. bronchitis or a skin rash. In this review, I shall focus on anapproach for conducting the bi-annual examination. Often, these patients arewell and asymptomatic.
All interactions with a patient should be looked upon as a means to furthertheir wellbeing. Sufficient time should therefore be set aside to evaluate theglycaemic control, look for complications, review medications and reassess thechronic care plan. It is seldom possible to complete this assessment in less than30 minutes.
Prior to the visitIt is recommended that all patients be contacted prior to their impending visitand reminded to bring along their blood glucose meter and home blood glucosediary and a complete list of current medications – this must include any overthe counter preparations, no matter how trivial the patient may regard these.Furthermore, because their feet will be examined, patients should avoiddonning elastic stockings and female patients should be forewarned that hosierywould need to be removed at the visit. Should the performance of an effort ECGbe required, reminding patients to wear comfortable athletic gear and to bring atowel will go a long way in optimizing their comfort.
Because several therapeutic decisions are made at a single visit, havingthe ‘typical’ blood tests performed prior to the visit will allow amplediscussion at the time of the examination. Patients are also more likely to bereceptive to amendments made in terms of their treatments if these are doneat the consultation.
Biochemical tests should always include the HbA1c, (at least twice yearly) andannual fasting lipogram and renal function. Additional testing such as formicroalbuminuria may only be required annually if negative, but if positive,repeat testing should follow current guidelines. These tests would constitute thevery minimum of care required to evaluate the person with diabetes.
At our facility, we encourage people with diabetes to prepare a list ofconcerns or questions they wish to pursue. It is vital to set aside enough time todeal with these matters and to inform patients that it may be necessary toprioritize issues. If needed, a second visit can follow.
South African Journal of Diabetes - March 2017 | 26
ORIGINAL
Correspondence:Dr Stan Landauemail: [email protected]
Dr Stan LandauSpecialist Physician, Centre forDiabetes and Endocrinology,Houghton
A structured approachto the diabetesconsultation

The visitDownloading the blood glucosemeter can be undertaken while thepatient is waiting. Almost all of themanufacturers will install, at no cost,proprietary software that will bringthe glucose readings to life. Recordscan thus be created and filed for laterreview and comparison.
Be aware of who is attending thevisit:• Is the wayward teenager
presenting with an unreliablesource such as a distant relative?
• Are the parents busy at work?Could this suggest reducedparental involvement or merelyan economic reality?
• Is the older person with reducedhearing present with a partner?
• Are you able to speak thepatient’s home language?
All of these seemingly minordetails set the stage for the next30 minutes.
When seated, what is theinteraction like?• Is the teen miserable,
forehead deeply browed andthe arms folded?
• Is the old age home caregiverseated in the reception whilea family member attendsthe session?
• Can you sense impendingconflict?
What is the employment situationat present?• Is the patient able to take time
out from his or her own businessto attend the session with you?
• Has the patient moved workpositions and what are the travelarrangements? (It is commonfor people to leave home in thepre-dawn period, administertheir short acting insulin and eatonly 90 minutes later at work).
• Do they use public transport, dothey walk and if so, how far?(This is most relevant to theschool-going child).
When assessing the glucosetrends over the past few weeksand months it is relevant to elicita history of any intercurrentnon-diabetes illness. A dose ofcortisone, a relapse in gout orhigh ambient stress is more thansufficient to upset a previouslystable glucose pattern. Do not behasty simply to elevate anti-diabetes treatment doseswithout investigating andaddressing the provocatoryinsult. The negative effect of along acting cortisone depot maylinger for up to a month.
In terms of glucose control,one aspect that is oftenoverlooked or even ignored ishypoglycaemia. It must beremembered, that this entity isperhaps THE commonest causeof why a number of people withdiabetes on insulin treatment failto attain good glycaemic control.In addition to the frequency andseverity of hypos, it is vital toassess the patient’s awareness ofthese episodes. Factorsincreasing the risk ofhypoglycaemic unawarenessinclude longer duration ofdiabetes, previous severehypoglycaemic episodes andadvanced age.
Weight fluctuations, the mealplan and eating habits will needto be addressed. It is important tofind out whether or not thepatient has seen a registereddietician in the last year. If theyhave not, ask if they are followingany other dietary programme orusing any over-the-counter dietproducts. Few healthcarepractitioners can match the skillsof dieticians in being able tounearth possible eating disorders.Such disorders may commonlypresent with persistently poorglycaemic control and weightfluctuations. Simply enquiringabout food intake alone isunlikely to be sufficient inattaining the desired information.
It is therefore useful to enquireabout eating habits and to askgeneral questions such as• Does the family eat together?• Where are meals enjoyed?• Do you eat at regular times?• Is consumption of food
occurring outside the meal timesor late at night?
In this vein, knowing when thediabetes medication is given relativeto a meal is vital.
The hallmarks of diabetes as adisease are the classically describedmicrovascular complications. It isthus incumbent on the healthcarepractitioner to evaluate for these atevery visit. This is done by means ofboth focused history taking andclinical examination.
Be sure to enquire about achange in visual acuity and if thereis any ocular discomfort. Apersistently dry eye could raisesuspicion of the often-overlookedSjögren's Syndrome. Additionalautoimmune disease may keepcompany with type 1 diabetes. It isthus appropriate to enquire abouttypical symptoms suggestive ofhypothyroidism and coeliac disease.
To elicit a suspicion of diabeticfoot disease, typical complaints mayinclude burning or discomfort,typically worse at night and when inbed. Tingling or pins-and-needlelike sensations may also beexpressed. Enquire about any recentfoot injuries or falls. Ask patients ifthey examine their feet daily andhow often and who cuts theirtoenails. Be especially curious in theelderly, those with limited mobilityand in those patients with reducedvisual acuity.
Often claudication symptoms inpeople with diabetes might beminimised and misdiagnosed asneuropathy. Enquire regarding thewalking distance tolerated beforefatigue sets in and whether or notrest relieves any leg discomfort.
Symptoms suggesting early renaldisease are at best vague. It is
South African Journal of Diabetes - March 2017 | 27
ORIGINAL

essential to test for thiscomplication by biochemical means.
As with all examinations, thegeneral broad systemic inquirynow follows. Because diabetes canaffect all organ systems, eachsystem’s inquiry should focus onpossible associations withdiabetes. If the inquiry is problemfocussed, it is unlikely thatsymptoms will be overlooked.
True silent myocardialischaemia is well described inpopulations with diabetes. Thisshould not imply avoidingenquiry regarding any typicalangina-like chest pain. Areduction in effort tolerance,unexplained upper gut symptomsexpressed perhaps as ‘wind’ andbreathlessness can be suggestiveof underlying cardiac disease.
Persistent cough could suggestunderlying gastro-oesophagealreflux disorder (GORD). This iscommon in the overweightpopulation. ACE inhibitorintolerance may also present withpersistent cough. The latter may bepresent for years and is typically dryand irritating.
Healthcare practitioners oftenneglect to reinforce the need toquit smoking. Patients will morereadily quit if this issue is raisedrepeatedly. Have you offered anyquitting techniques such ascounselling, group sessions orprescribed medications?
In recent times, there isemerging interest in theassociation between metabolicderangements and sleepdisorders. Restless leg syndromeand obstructive sleep apnoea(OSA) are the 2 commonest suchdisorders occurring in people withdiabetes. OSA is the morecommon. Symptoms suggestive ofOSA include heavy snoring,daytime sleepiness, drowsinesswhile driving and a host of non-specific complaints such asheadache, moodiness andirritability. OSA is often associated
with other features of themetabolic syndrome, butspecifically with obesity. It is oftenhelpful to elicit a history from thebed-partner in terms of snoringand discrete apnoea episodes. Ifyou are suspicious of underlyingOSA, then referral to a sleeplaboratory is mandated.
Male patients must be askedabout any symptoms that couldsuggest erectile dysfunction (ED). Ifpresent, this should further raisesuspicion for underlyingcardiovascular disease. Ideally,every interaction should also becentred on identifyingcardiovascular risk factors andpursuing ways to reduce these risks.
In the discussion of ED, probingof the libido is also of value.Contemporary thinking is centringon the role of late agehypogonadism in males. In certainindividuals, parenteral testosteronereplacement may be appropriate.Enquire further though to excludeother sources of low libido such asdepression, drugs orhyperprolactinaemia. Only withthorough biochemical assessmentcan hypogonadism be confirmed.
Additional uro-genitalcomplaints are common in peoplewith diabetes. By their very nature,they are typically not expressed bythe patient, so it is vital to explorethem proactively. Enquireregarding the continence of urine.An overactive bladder in an olderwoman may limit social interaction.Persistent urination, incontinenceand prostate problems may resultin perceived polyuria, which in turnmay be presumed by the patient toreflect poor glycaemic control. Ingeneral, females are less likely tohave their uro-genital symptomsdiscussed. In this vein, libidoproblems as well as vaginal drynesswith resultant sexual dysfunctionmay be ignored, to the detriment ofthe patient and her partner.Timeous referral to a gynaecologistcan have a positive effect in
restoring sexual health.Menstrual irregularities are
common in women with diabetes.Glycaemic flux can be seen in thepre-menstrual period. Bloodglucose meter downloads oftenreveal these patterns quitespectacularly. Simply raising thisissue with the patient and advisingadditional measures over that time,such as amending the insulin dose,can mitigate a persistentlyoccurring issue. Secondaryamenorrhea may occur when thediabetes control deteriorates,sometimes seen in the context ofanorexia nervosa in young females.The less common prematureovarian failure is an autoimmunecondition, which can be found inthe presence of type 1 diabetes.Persistent vaginal thrush is morecommonly reported in women withpoor glycaemic control.
Bowel habits are often derangedin people with diabetes. The simpleuse of metformin may inducepersistent nausea and a change instool quality and gut motility. It isnot uncommon for diarrhoea to beoverlooked even years after thecommencement of this widelyprescribed drug. A simple drugholiday may be needed to separatemetformin-induced problems fromother causes.
Persistent diarrhoea, possiblywhen worse at night, may reflectautonomic dysfunction. Typically,this will occur in individuals withlong standing poorly controlledtype 1 diabetes. Now would be theideal time to assess for furthercommonly overlooked symptomssuggestive of a more generalizeddysautonomia. These may includepost-gustatory sweating andorthostatic hypotension. The latteris commonly encountered ingeneral practice e.g. the elderly onantihypertensive treatment.Additional symptoms with respectto dysautonomia includeunexplained palpations and ED.As will be discussed later, the
South African Journal of Diabetes - March 2017 | 28
ORIGINAL

performance of specialised tests toevaluate the autonomic systemwould be considered appropriate.
Joint and musculoskeletalcomplaints are highly prevalent inpeople with diabetes. Causes caninclude gout and age appropriateosteo-arthritis. However, oneshould consider a widerdifferential to include statin-induced myopathy / arthropathy,autoimmune mediatedrheumatoid arthritis andhaemochromatosis. The latter isalso associated withhypogonadism and liverdysfunction. Frozen shoulder andtrigger finger also occur morecommonly in people with diabetes.
Modest alcohol consumptionmay still be regarded asappropriate in people withdiabetes. This if they are aware ofthe carbohydrate content and areoffered a dietary exchange. Thoseat high risk for the development ofhypoglycaemia must be madeaware of the dangers of excessiveor inappropriate alcoholconsumption, particularly whenfollowing a full dose of insulin anda reduced meal size. Advise youngdrinkers accordingly and assistthem in fostering safer practicesshould they chose to indulge. Nowis ideal time to ensure that allpeople with diabetes, butespecially those on insulin, have amedic-alert tag / bracelet.
Do not be afraid to talk aboutcovert drinking or drug abuse withunderage teens. It is well knownthat additional risk takingbehaviours such as substanceabuse tend to occur more so inyoung people with type 1 diabetes.If the parent is present for theinterview, you may want to raisethis topic alone with the patient,perhaps in private during thephysical examination.
Clearly, the examination of thepatient begins as the patiententers your consulting room. Earlyimpressions will be formed while
watching the patient move fromthe reception area to your office.Remain alert! Many diagnoses canalready be made at this stage. Byconstantly refining your methods,the start of each examination canbe dealt with expeditiously and
will help to solidify the long-termrelationship you are likely to havewith these patients.
PART 2 will cover some of themore common clinical features ofthe examination.
South African Journal of Diabetes - March 2017 | 29
ORIGINAL
Preparing for your diabetes consultation – A patient handout
Diabetes Consultations are a valuable resource. Plan well to get the most out ofeach visit. Please attend all scheduled appointments or, if this is not possible,please cancel at least 24 workday hours prior to the scheduled time. This willallow someone who is on a waiting list for appointments to be booked instead.
Please arrive 30 minutes prior to your scheduled appointment to fill in formsand do blood tests as necessary. Take the distance, route and likely trafficconditions at the time into account when planning your journey.
Please bring the following to your consultation:• SA National ID book or passport;• Medical Aid Card (if applicable);• Blood glucose meter and diary;• Current Insulin delivery device (pen & needle, syringe, pump – as /
if applicable);• Results of any recent laboratory tests;• A list of the names and dosages of all current medications (include any
over-the-counter preparations);• Any letter of referral or report/s from other doctors / healthcare providers;• A list of concerns or questions you may wish to discuss.
Because your feet will be examined, please do not wear elastic stockings toyour consultation. If you choose to wear fashion stockings, these will need tobe removed.
Allow a further hour in your schedule after your appointment with a doctorfor the completion of any supplementary (usually annual) tests. You may wantto bring the following for these:
For Treadmill ECG:• Comfortable clothing suitable for exercise;• Running shoes / takkies;• Blood glucose meter and strips;• Glucose sweets and a snack in case of low blood glucose levels;• Soap and a towel, if you would like to shower after the procedure.
For Eye Test & Examination:• Normal spectacles used for distance vision;• If wearing contact lenses – solution and container so you can remove them.
To facilitate your regular diabetes care and to avoid future lengthy waitingperiods, you are advised to book your next appointment/s as you leave
We look forward to being of assistance to you!

Screening for disease or the complications thereof is an importantaspect of primary care, relating to the need to detecttreatable/communicable disease at the earliest time. Ideally,
screening should employ highly sensitive diagnostic modalities to ensuredetection of all possible cases. It is therefore implicit that with thisapproach, some subjects without the condition in question will bewrongly classified.
This often requires additional expensive tests, and more expertise,to delineate those with the condition in question accurately. Thisapproach is acceptable provided screening is inexpensive, widelyavailable and requires modest skills and equipment. Above all, thetechnique used for screening should be sensitive enough to ensure thatfew or no cases are missed.
The prevalence of diabetes mellitus ranges from 4 – 15 % and more,depending on the population studied. Using a conservative prevalence of5 %, approximately 2.75 million people with diagnosed diabetes in SouthAfrica are at risk to develop Diabetic Retinopathy (DR) and thus willneed regular screening. Moreover, the prevalence of DR in a populationwith diabetes is by no means negligible (Kalk et al reported a prevalenceof 30 % at the then Johannesburg Hospital Diabetes Clinic, of which onethird required referral) and is considered one of the most common,preventable causes of blindness in developed and developing countries.
Although better diabetes control may reduce the incidence ofretinopathy, this objective remains chimerical and out of reach for most,with the available treatment modalities. Given that timeousophthalmological intervention will make a huge impact on the progressionto the more serious sight-threatening stages of DR, the case for screeningfor early changes is clearly unassailable.
Screening for diabetic retinopathyAn appropriate and desirable, although expensive way to screen, would be tohave a regular examination by an ophthalmologist (who would also be in aposition to accurately identify, stage and treat the more serious cases, as well asdetect other diseases such as glaucoma and age related macular degeneration).This is clearly not achievable in South Africa at present due to cost implicationsand the relative paucity of ophthalmologists. Several other countries havetherefore devised cost-effective screening programmes achieving an equal orsuperior rate of DR detection as compared with screening by ophthalmologists(e.g. England and Wales - retinal photography through dilated pupils; Scotland
South African Journal of Diabetes - March 2017 | 30
ORIGINAL
Screening for diabeticretinopathy at the levelof primary care
Correspondence:Dr Brian Krameremail: [email protected]
Dr Brian D. KramerMBBCh (Rand) DMRD (London)FCP (SA) DTM&H (WITS) Specialist Physician /Endocrinologist

- non-mydriatic retinalphotography; Holland -technicians/nurses trained inophthalmoscopy). In South Africa,screening has been achieved on avery limited scale and an effectivefar-reaching programme remains afanciful dream.
With this in mind, is there anyplace, in a resource-poorenvironment, for the humbleophthalmoscope in the hands ofthe non-ophthalmologist? Thereare several pitfalls:1) Ophthalmoscopy has a poor
sensitivity, especially in thehands of a non-specialist, fordetecting sight-threateninglesions - perhaps only 20 - 50 %of such lesions are detected.However, the purpose ofscreening should be to detect anydiabetic retinal changes and torefer these for expert assessment.In this respect, ophthalmoscopyperforms better.
2) Inexperience - obtaining goodfundal views requires constantand regular practice.
3) Poor viewing conditions,including an undarkenedroom, uncomfortable positionvis-à-vis the patient, lack oftime/patience and of course asmall pupil.
The most obvious way toimprove retinal views is to dilatethe pupil. However, this israrely performed outside of theophthalmologist’s rooms –adequate mydriasis takes time(particularly in some peoplewith diabetes) and patientsdon’t particularly like itbecause of the resulting blurredvision which persists for sometime afterwards.
However, although theexceptional patient may allow ofadequate viewing of the funduswithout dilatation, this is veryrare. It must be clear that failureto dilate the pupils adequatelydoes not constitute adequatescreening - whatever one’sexperience. It is important to behonest with oneself in relationto all of this – does one havesufficient experience to detectrelevant abnormalities andwere adequately clear andsufficient views of the fundi
obtained? If not, the patientdeserves referral.
Even in a resource-poorenvironment, it should bepossible to ameliorate, to anextent, some of thesedifficulties. Try to see all thepatients on a particular day;warn them to expect dilatationon arrival; if this is planned,they may wish to bring along achaperone to assist withtransportation later on, set up amakeshift darkened room andensure that you and the patientare both comfortably seated.
Invariably, opportunisticscreening still has to beperformed on known patientswith diabetes who simply ‘pitchup’ to a clinic or consultingroom, having, to all intents andpurposes, been lost to follow-up.Often, these individuals are athigher risk and the opportunityto examine their fundi carefullyshould not be missed.
South African Journal of Diabetes - March 2017 | 31
ORIGINAL
Retinal photograph of the left eye. A: hard exudates, B: deep haemorrhage, C: soft exudates, D: new vessels, E: flame-shaped haemorrhage.
Retinal photograph of the right eye. A: optic disk (appears normal),B: the macula and C: microaneurysms. Given the location of thesemicroaneurysms, referral of this patient is mandated.
The most obvious way to improve retinal viewsis to dilate the pupil. However, this is rarelyperformed outside of the ophthalmologist’srooms – adequate mydriasis takes time

How often to screen• Type 2 diabetes - at diagnosis
and annually thereafter• Type 1 diabetes - within 5
years after diagnosis andannually thereafter
This is more frequent than strictlynecessary but it will reduce theoverall number of patientsinappropriately not referred (The‘second bite’ principle…).
Whom to screen• Women, before a projected
pregnancy and during eachtrimester, since rapidprogression of retinopathymay occur during pregnancy.
• Poorly controlled patients,prior to instituting intensiveglycaemic control, since rapidreduction of ambient glucosemay be associated with rapiddeterioration of retinopathy.
• Patients with nephropathyand patients with a history ofpoor follow-up should bescreened at each visit.
Assuming the screeningexamination provides adequateviews, what should the criteriabe for referral for expertevaluation by anophthalmologist? Bear in mindthat the screening is notintended to be a diagnosticmanoeuvre, but simply to selectthose who are at risk for, or thatmight have significant disease,but usually do not. Indeed thecriteria for referral are calibratedto ensure over-referral of non-significant changes in anattempt to maximize the
sensitivity of this process withregard to not missing, andtherefore not referring, unseensignificant lesions.
What goes wrong?The pathology of DR begins inthe retinal microcirculationleading to vascular leakage,haemorrhage, ischaemia andinfarction. Physiologicalcompensatory adaptions follow,including the development offibro-vascular proliferation. Thepurpose of screening is to detectsigns that indicatemicrovascular pathology at anearly stage in the developmentof this train of events.
Signs to look for; whatto refer1. Microaneurysms – small
round red dots. Bythemselves, these are not anindication for referral unlessthey are close to the macula(within 3 disc diameters of themacula) or numerous (morethan 5 in number).
2. Haemorrhage – larger reddots, blots or smudges. Itwould be wise to refer anyhaemorrhage within thetemporal vascular arcades.
3. Soft Exudates – fluffy white,often cloud-like patches
representing infarction of thenerve fibre layer. These aremost often observed withinthe temporal arcades wherethe nerve fibre layer isthickest – these are anindication for referral.
4. Hard Exudates - yellowish,often bright and clearlydefined patches - these can bequite small and representlipoproteins laid down becauseof local vascular leakage. Theymay assume a circinate patternand be a clue to local retinaloedema. When close to themacula, hard exudates may beassociated with macularoedema or even cystic change(Diabetic macular oedema).These require urgent referral!
By convention, any exudate within2.5 disc diameters of the macula isreferred to as ClinicallySignificant Macular Oedema(CSMO) and must be referred.However, it is also wise to refer allsuch exudates seen within thetemporal arcades.
From this, it is clear, given thepoor sensitivity of theophthalmoscope in detectingsight-threatening lesions, thatapart from a few microaneurysmsdistant from the macula, virtuallyall lesions within the temporalarcades are reasonable groundsfor referral.
Do not underestimate thesignificance of lesions outside thetemporal arcades - these may bethe site for future vitreoushaemorrhage. Additionally, whenperipheral retinal ischaemia ispresent, these sites may also
South African Journal of Diabetes - March 2017 | 32
ORIGINAL
Bear in mind that the screening is not intendedto be a diagnostic manoeuvre, but simply toselect those who are at risk for, or that mighthave significant disease, but usually do not
The purpose of screening is to detect signsthat indicate microvascular pathology at anearly stage in the development of this trainof events

elaborate angiogenic factors andpromote neovascularisationelsewhere in the retina. Althoughthe criteria for referringperipheral lesions is far lessstrict, fairly florid lesions otherthan microaneurysms (morethan 5) or a localizedconcentration of any type oflesion should also mandateprompt referral.
Note that the other moreadvanced retinal lesions such asIRMA (IntraretinalMicrovascular Abnormality),venous beading andneovascularisation are importantfor staging and determiningtreatment and have not beendiscussed. Any of these changesanywhere on the retina shouldalso prompt referral.
The lesions described aboveare typically present when otherreferral criteria are absent.
We can do better with verylittle effort…Macular oedema, or any retinaloedema, which requires anappreciation of retinalthickening, without theaccompanying sentinel sign ofhard exudation, is not readilydiagnosed with anophthalmoscope (or with retinalphotography for that matter) andis therefore likely to be missedby the non-specialist. Althoughthis is a serious deficiency, thenumber of cases in this categoryis considered very small anddeemed acceptable whenweighed against the benefit to begained from widespread
screening using simpletechniques. Testing visual acuityusing Snellen charts with pinholescreens, as well as visual fieldsusing an Amsler grid, both ofwhich cost virtually nothing, areeasy to use and may increase theyield in this respect.
Many patients withhypertension or proteinuria mayalso have retinal changes. Theperception that the patient mayhave ‘hypertensive retinopathy’should not deter referral basedon the above criteria.
Bear in mind that poor vision(uncorrected by pinhole viewing)should always be referred andthat many elderly patients whohave resigned themselves tobecoming or being blind, mayhave a cataract. Unfortunately,many may also have non-diabetes-related diseasesaccounting for this.
It is clear that considerablescope exists in South Africa fordesigning and implementing an
effective population-basedscreening programme using, forexample, mobile digitalphotography units with tiers ofexperts reviewing the imagescentrally. This unfortunately isnot the present reality.Ophthalmologists propagate theattitude that ophthalmoscopy is avery poor screening tool fordetecting sight threatening DR(they are correct). However, thishas provided the justification fornot performing this examinationand possibly leading in resource-poor areas, to the situation whereno screening of any sort isperformed. This is unacceptablegiven that ophthalmoscopyreadily detects lesionsconstituting the criteria forreferral. Primary care Physiciansshould be encouraged to havespare batteries for theirophthalmoscopes and a mydriaticon the shelf.
ConclusionThe limitations associated withophthalmoscopy should not leadto its demise in the primary caresetting – adopting a low thresholdfor referral can offset theseconsiderably. In a resource-poorsetting, regular fundal inspectionthrough dilated pupils remains avaluable tool for those preparedto take the trouble to do so.
South African Journal of Diabetes - March 2017 | 33
ORIGINAL
Referral Criteria
• Lesions within the temporal arcades other than microaneurysms distant fromthe macula
• Florid or focal lesions elsewhere• Recent deterioration in visual acuity• Poor vision (uncorrected by pinhole)
Bear in mind that poor vision (uncorrected bypinhole viewing) should always be referred andthat many elderly patients who have resignedthemselves to becoming or being blind, mayhave a cataract
The limitations associated with ophthalmoscopyshould not lead to its demise in the primary caresetting – adopting a low threshold for referralcan offset these considerably

South African Journal of Diabetes - March 2017 | 34
Presents a Five-Day Advanced Course in Diabetes Care for Health Professionals
2017
WHO SHOULD ATTEND THE COURSE? This is an Advanced Course, and is aimed at Health Care Professionals who have a basic knowledge and understanding ofdiabetes mellitus. It is designed to give an extensive overview of the core principles of modern team diabetes management,so enabling the participants to understand the condition in sufficient depth, to make a real difference in the lives of peoplewith diabetes. Pre and Post Course multiple-choice knowledge evaluation tests are administered, to allow for evaluation ofthe learning experience.
Attendance is also part of the contractual requirements for Practitioners wanting to open CDE affiliated “Centre forDiabetes Excellence” Branches.
DIABETES ~ THE BURDEN, THE RELIEF Latest estimates place the age-adjusted (20-79) comparative prevalence of Diabetes Mellitus in South Africa at 7.6 %(International Diabetes Federation, 2015) and this is increasing. Up to 62 % of persons with the condition are undiagnosedand at risk from disabling and life threatening complications. Diabetes, together with its associated cardiovascular risk factorsis one of the leading causes of death, either directly or indirectly, in our population.
Over the past three decades, it has become evident that good control of diabetes, as well as the common co-morbiditiesof hypertension and the dyslipidaemias, is vital to prevent or delay the devastating long-term complications of diabetes.To achieve this, people with diabetes need to understand their largely silent condition and the correct principles of self-care.
Health professionals often do not have access to updated approaches to a chronic, mostly self-managed condition such asdiabetes ~ vital opportunities for therapeutic interaction and patient education are lost. Additionally, insight is needed intothe ever-widening range of available medications and treatment strategies as well as the relationships betweencardiovascular and other risk factors and diabetes.
As health services evolve, there is a move towards Team Management of Chronic Conditions. This has resulted in the restof the Health Care Team (Nurses, Pharmacists, Dieticians, Podiatrists, Biokineticists and others) playing an ever-increasingrole in diabetes care.
COMMENTS FROM DELEGATES TO PREVIOUS 5-DAY COURSES: I realise that I had been blundering around in the dark in treating my patients with diabetes and now someone has turned onthe light! This a life changing Course. You have reformed my medical practice forever - General Practitioner
It was a superb Course & should result in a marked improvement in the care of people with diabetes - Registered Nurse
I enjoyed the Course thoroughly. I will manage patients with diabetes with more self-confidence. The talks were excellent, wellorganized and well presented - Registered Dietician
The message that you convey is that you care. The variety of topics was great. The balance between active participation andlistening was great. The great teaching skills in all lectures promote learning - Registered Nurse
All speakers were excellent and displayed an impressive knowledge of their subjects. Your commitment as professionals is highlycommendable. I learned a lot from this superb Course. Consequently, I will be able to treat my patients better - Medical Specialist

2328_HOM_GlucoCheck A2 Poster Design_PRESS.ai 1 2015/07/03 03:50:03 PM
C
M
Y
CM
MY
CY
CMY
K
HOM_GlucoCheck A4 Ad Design_PRESS.ai 1 2017/03/13 03:42:34 PMHOM_GlucoCheck A4 Ad Design_PRESS.ai 1 2017/03/13 03:42:34 PM

South African Journal of Diabetes - March 2017 | 36
CPD ACCREDITED DIABETES TRAINING
CPD ACCREDITEDThe Course offers 34 contact hours. The Course is accredited to provide 30 CPD points for Medical Practitioners and otherHealthcare Practitioners registered with the Health Professions Council of South Africa.
Pre-Course readings will be supplied by e-mail to all delegates and an electronic manual of all speaker notes will beprovided on the first day of each Course.
Official completion certificates will be provided to delegates who achieve a mark of at least 60 % in the final Post-CourseKnowledge Evaluation.
ANSWERS TO FREQUENTLY ASKED QUESTIONS Presented at: Glenhove Conference Centre, 52 Glenhove Road, Melrose Estate, Johannesburg. Dates & Fees: Available at www.cdediabetes.co.za (Click on Diabetes Courses). Early bookings are advised. Course Hours: Five days of lectures, workshops and discussion (08h00 – 17h00). Dress: Comfortable, smart-casual Language Medium: English Course Information: The Course Coordinator Tel: +27 11 053-4400 / Fax: +27 (0)86 247-0674E-mail: [email protected]
PROGRAMME SUMMARYThe Course is aligned with the latest evidence based treatment guidelines. Case studies and problem solving approachesare a vital part of the learning process.
TOPICS INCLUDE: • Holistic Team Care Philosophy & Educational Approaches • Diagnosis, Classification, Pathophysiology & Prevention of Type 1 & Type 2 Diabetes Mellitus • Other types of diabetes including Gestational Diabetes • Treatment of Type 1 & Type 2 Diabetes • Psychological Adjustment to Diabetes • Meal Planning & Nutrition in Diabetes • The Importance of Exercise in Diabetes • The Medical Management of Diabetic Ketoacidosis • The Foot of the Person with Diabetes • Acute Complications of Diabetes • Diabetes as a Micro- & Macro-vascular Disease & Risk Factor Control • Managed care in diabetes • Interactive Team-facilitated Case Study Sessions • Practical Workshop on Self Care Devices & Equipment
OUR INTERDISCIPLINARY TEAM OF COURSE LECTURERS AND FACILITATORSLarry A. Distiller BSc MBBCh (Rand) FCP (SA) FRCP (London) FACE Specialist Physician, Endocrinologist Brian D. Kramer MBBCh (Rand) DMRD (London) FCP (SA) DTM&H (Wits) Specialist Physician, Endocrinologist Barry I. Joffe MB FRCP FCP (SA) DSc Specialist Physician, Endocrinologist David Segal MBBCh (Wits) FAAP (USA) Paediatric Endocrinologist Laura Blacking MBBCh (Wits) FCP (SA) Specialist Physician, Endocrinologist Stan Landau MBChB (Stell) FCP (SA) Specialist Physician Andrew Heilbrunn B PHYS ED (Wits) BA (Hons) Biokinetics Biokineticist Michelle Daniels BSc Dietetics (Natal) Dip. Hosp. Dietetics (Pretoria) Registered Dietician Gerda Janse van Rensburg ND Pod SA IIWCC (Toronto, US) PgDipDM (Glamorgan) Podiatrist Michael Brown B. Nursing (Wits) ACDM (Wits) Diabetes Specialist Nurse Rosemary Flynn MSc (Clinical Psychology) Clinical Psychologist

Improved Glycaemic Control, With Or Without Insulin3
*The concurrent use of BYETTA® with thiazolidinediones, D-phenylalanine derivatives, meglitinides, or alpha-glucosidase inhibitors has not been studied.3**BYETTA® is not indicated for the management of obesity and weight change was a secondary endpoint in clinical trials.
References: 1. Nauck MA, Duran S, Kim D, et al. A comparison of twice-daily exenatide and biphasic insulin aspart in patients with type 2 diabetes who were suboptimally controlled with sulfonylurea and metformin: a non-inferiority study. Diabetologia 2007;50:259-267. 2. Diamant M, Nauck MA, Shaginian R, et al. Glucagon-like peptide 1 receptor agonist or bolus insulin with optimised basal insulin in type 2 diabetes. Diabetes Care 2014;37:2763-2773. 3. BYETTA® package insert. August 2016.
Before or after basal insulin1,2,3,There is BYETTA®
Before basal insulin BYETTA® can be started in patients not achieving adequate glycaemic control with oral therapies*3
After basal insulin BYETTA® can be added to basal insulin ± oral therapies in patients not achieving adequate glycaemic control3
Instead of mealtime insulin BYETTA® reduces HbA1c similarly to mealtime insulin and offers the added benefits of weight loss** and fewer episodes of hypoglycaemia vs. insulin1,2
S3 BYETTA® 5 μg, solution for injection. Reg. No. 41/34/0068. Each dose contains 5 microgram (μg) exenatide in 20 microlitres (μl), (0,25 mg synthetic exenatide per ml). One pre-filled pen contains 60 doses of sterile, preserved solution (approximately 1,2 ml). S3 BYETTA® 10 μg, solution for injection. Reg. No. 41/34/0069. Each dose contains 10 microgram (μg) exenatide in 40 microlitres (μl), (0,25 mg synthetic exenatide per ml). One pre-filled pen contains 60 doses of sterile, preserved solution (approximately 2,4 ml). PHARMACOLOGICAL CLASSIFICATION: 32.16 Others. INDICATIONS: BYETTA® is indicated as add-on therapy for patients with type 2 diabetes mellitus inadequately controlled by lifestyle modification, other oral antidiabetic therapy and basal insulin. For full prescribing information refer to the package insert approved by the Medicines Regulatory Authority. AstraZeneca Pharmaceuticals (Pty) Ltd. Reg. No. 1992/005854/07. Building 2, Northdowns Office Park, 17 Georgian Crescent West, Bryanston, 2191. Private Bag X23, Bryanston, 2021. Tel: 011 797-6000. Fax: 011 797-6001. www.astrazeneca.co.za. Expiry Date: November 2018. Activity ID: 810137.
4721 Byetta Dup Advert for SAJD.indd 1 2017/01/26 9:54 AM






























