Embed Size (px)
Citation preview

A IMPORTANCIA ATUAL DA IMUNOFENOTIPAGEM NO DIAGNOSTICO
E CLASSIFICAÇAO DA SMD
HEMO 2016 Congreso Brasileiro de Hematologia, Hemoterapia y Terapia CelularFlorianopolis, 10 de Novembro de 2016
CANCER RESEARCH CENTER IBSAL-UNIVERSITY OF SALAMANCA/CSIC

Conflict of Interest DisclosureI hereby declare the following potential conflicts of interest concerning my presentation:• Membership on an Entity’s Advisory Committee: Janssen, Celgene.
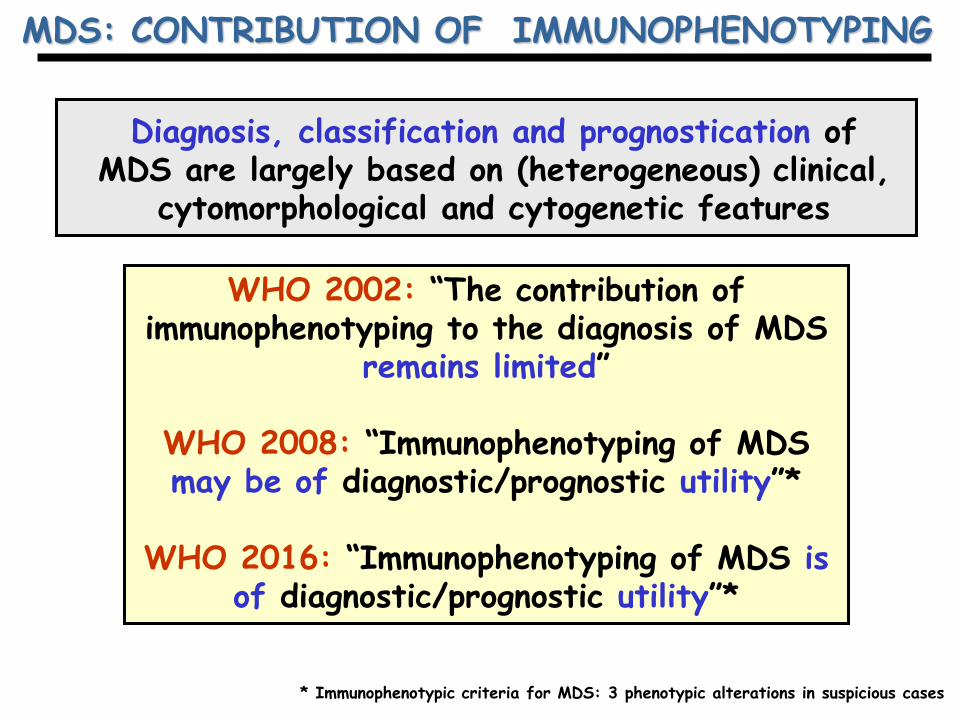
MDS: CONTRIBUTION OF IMMUNOPHENOTYPING
WHO 2002: “The contribution of immunophenotyping to the diagnosis of MDS
remains limited”
WHO 2008: “Immunophenotyping of MDS may be of diagnostic/prognostic utility”*
WHO 2016: “Immunophenotyping of MDS is of diagnostic/prognostic utility”*
Diagnosis, classification and prognostication of MDS are largely based on (heterogeneous) clinical,
cytomorphological and cytogenetic features
* Immunophenotypic criteria for MDS: 3 phenotypic alterations in suspicious cases

Prerequisites:1.- Marked prolonged (≥6months) cytopenia (<110g Hb/L or
< 1500 neutrophils/µl or <100.000 platelets/µl) in >1 cell lineages2.- Other hematological and non-hematological diseases excluded
Additional diagnostic criteria:1.- Morphologic dysplasia in >10% erythroid and/or neutrophil
and/or megakaryocytic lineages or >15% ringed sideroblasts2.- Characteristic cytogenetic abnormalities3.- Blast cell number of between 5% and 19%
Diagnostic co-criteria:1.- Flow cytometry immunophenotypic abnormalities.2.- Molecular signs of clonality (Chromosome X inactivation tests) andmolecular tests (e.g. RAS mutations)3.- Marked and persistently reduced CFU-assays
Valent et al, Leuk Res, 2007
MDS: MINIMAL DIAGNOSTIC CRITERIA

MDS:Aberrant granulomonocytic phenotypes
Stetler-Stevenson, Blood, 2001

Diagnostic utility of FCM in MDS
No cases Sensitivity Specificity
Stetler-Stevenson et al, Blood 2001 65 78% N.R.
Wells et al, Blood 2003 115 55% 100%
Cherian et al, Cytometry B 2005 15 73% 90%
Malcovati et al, Leukemia 2005 103 87% 100%
Ogata et al, Blood 2006 27 59% 100%
Loosdrecht et al, Blood 2008 50 82% 100%
Scott et al, Blood 2008 152 60% N.R.
Matarraz et al, Leukemia 2008 50 100% 100%
Ogata et al, Haematologica 2009 81 89% 90%
Differences in: 1) target cell populations, 2) phenotypic criteria for MDS, 3) cohorts of patients & controls

MDS: FCM IMMUNOPHENOTYPIC VARIABLES
Cell populations of interest Phenotypic alterations
Hematopoietic precursors/myeloblastsAltered cell numbers
Maturing neutrophilsAsynchronous maturation
Monocytes and monocytic precursorsAberrant markers
Nucleated red blood cellsMarker overexpression
Other potentially informative cells: Marker underexpression- Platelets- Eosinophils Altered scatter- Basophils - granularity- Mast cells - size- Dendritic cells- Mature red cells

Modified from van der Loordescht, Leukemia 2012 *52 immunophenotypic variables/case

Flow Cytometry Immunophenotyping of CD34+ HPC in MDS vs Normal/ Reactive BM
SUBSET OF CD34+ HPC
IMMATURE
NEUTROPHIL
B-CELL
ERYTHROID
RA RCMD RAEB-1 RAEB-2
Matarraz et al, Leukemia, 2008

RAEB-1
MDS vs normal BM: myelomonocytic maturation
Normal BM
CD34+ HPC:
Neutrophil
Immature
Pre-B
Neutrophil
Immature
CyMPO-PE
CyMPO-PE HLADR-FITC
HLADR-FITC
CD11
7-PE
CD11
7-PE

Diagnostic utility of FCM in MDS: the Ogata “simplified” score

Ogata et al, Haematologica 2012
Diagnostic utility of FCM in MDS: the Ogata “simplified” score

Ogata et al, Haematologica 2012
Diagnostic utility of FCM in MDS: validation of the Ogata “simplified” score

Matarraz et al, Cytometry B 2010; Mathis et al, Leukemia 2013Eidenschink et al, Cytometry B 2015;
Cremers et al, Haematologica 2016; Westerns et al, Haematologica 2016
Diagnostic utility of FCM in MDS:evaluation of the erythroid lineage
Altered erythorid phenotypes:- lower CD71 expression,- greater CD71 CV- greater CD36 CV- greater/lower CD117 expression
Increased sensitivity and specificity
Limited reproducibility
CD71 MFI
Tran
sf-S
SC
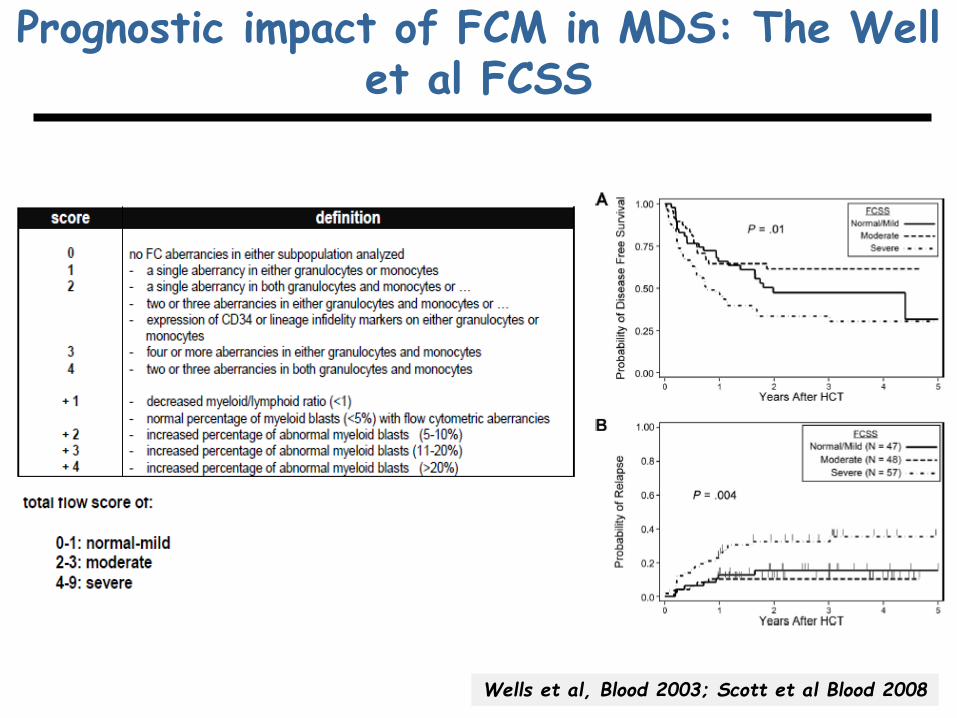
Wells et al, Blood 2003; Scott et al Blood 2008
Prognostic impact of FCM in MDS: The Well et al FCSS

Prognostic impact of FCM in MDS: The Well et al FCSS


POTENTIAL CONTRIBUTION OF IMMUNOPHENOTYPING IN MDS
Diagnosis:Suspected MDS (normal vs MDS),
ICUS,Unexplained monocytosis
Valent at al, Leuk Res, 2007; van de Loosdrecht et al, Haematologica, 2009; Leukemia 2012 & Leuk Lymph 2013; Bene et al, Leukemia 2014
Refine prognostic scoring systems
Yes but, how?
Diagnostic subclassificationUni- vs multi-lineage MDS
MDS with other clonal disorders
Disease monitoring(follow-up of FCM alterations)
Untreated MDS, After therapy
Inconclusive cases


ALTERED NEUTROPHIL MATURATION IN MDS BM
Normal BM RCMD RAEBCompatible with MDS
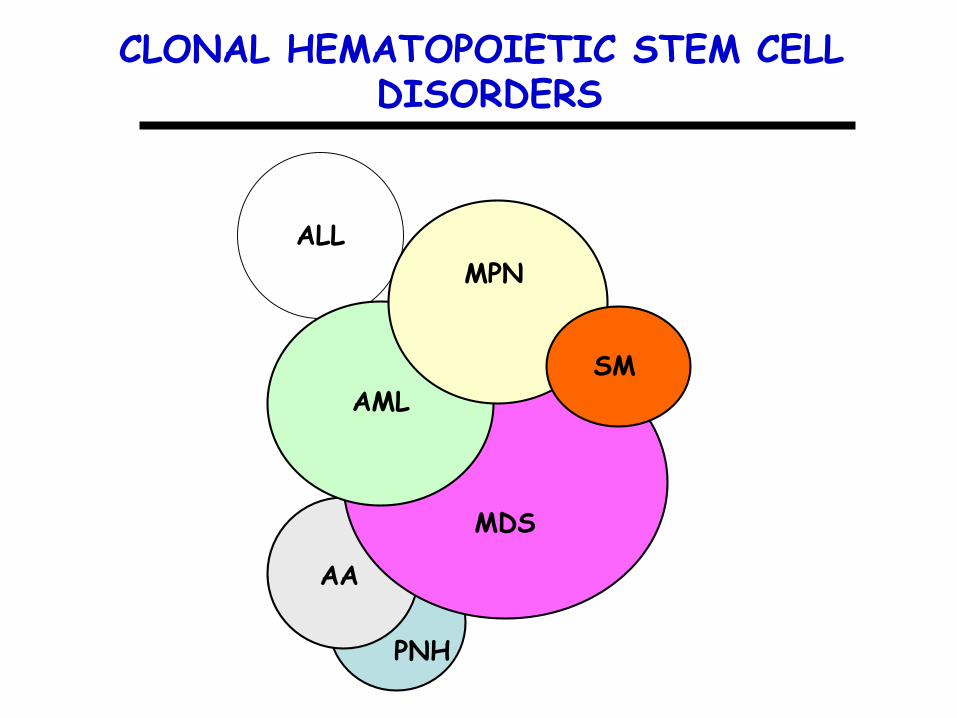
ALL
CLONAL HEMATOPOIETIC STEM CELL DISORDERS
AMLSM
MPN
PNH
AA
MDS

“DE NOVO” AML: ABERRANT PHENOTYPES & CLONAL HEMATOPOIESIS (n=59)
Phenotype Polyclonal AML# Clonal AML*N=10 N=49
Normal phenotype 58% 2%
>2 altered lineages 17% 92%
N. of altered lineages 0.7 2.7
Total 10/59 (17%) 49/59 (83%)
Fernández et al, Leukemia 2013
# One ISM-AML case with KIT mutation restricted to mast cells* Two cases showed coexistence of t(8;21) & D816V KIT mutation in all cellular compartments analyzed

ALTERED HEMATOPOIESIS AT DIAGNOSIS IN MULTIPLE MYELOMA & MGUS BONE MAROW
N.of altered cases/ total cases (%)
Matarraz et al, Leukemia 2014
Altered phenotypes* 33/250 (13%)
Cytogenetic changes 15/32 (47%)or clonal HUMARA
- del(5q32), del(7q31), -Y, +8 7/22
- Clonal HUMARA 8/10
*13/25 MM died during the first year after therapy and only 2/25 reached CR
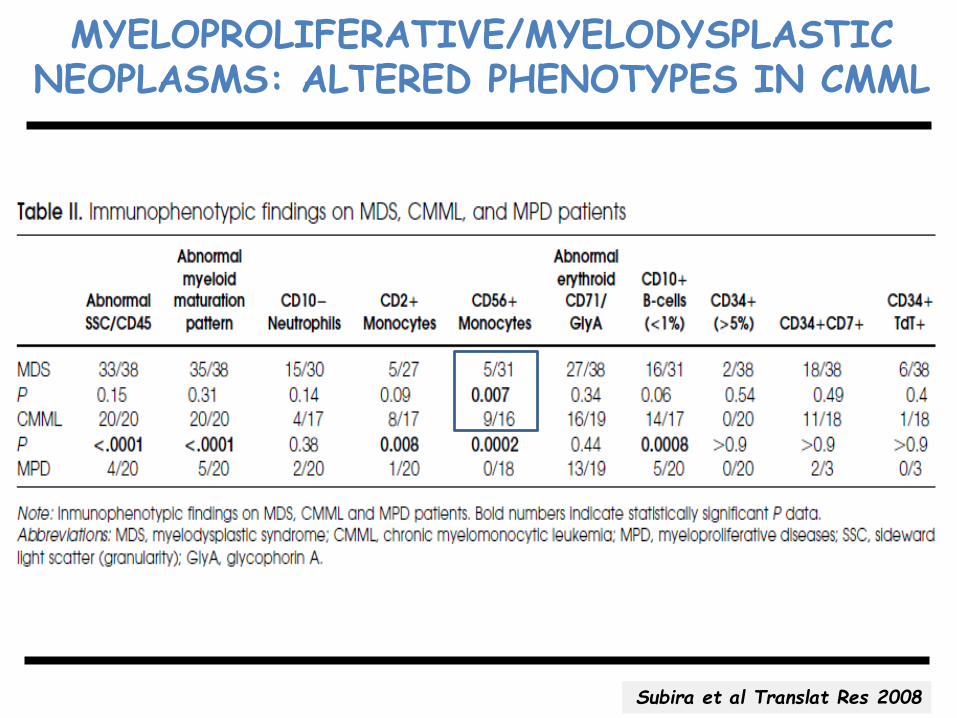
MYELOPROLIFERATIVE/MYELODYSPLASTICNEOPLASMS: ALTERED PHENOTYPES IN CMML
Subira et al Translat Res 2008

Monocyticcells
Maturing neutrophils
CD45 MFI
Tran
sfor
med
SS
C Eosinophils
CD34+ Precursors
Erythroid cells
CD
13 I
MF
CD11b MFI
CD
13 M
FI
CD71 MFI
Tran
sf-S
SC
IMMUNOPHENOTYPIC ALTERATIONS OF BM MYELOID CELLS IN CHRONIC MYELOMONOCYTIC LEUKEMIA
Maturing neutrophils & Monocytic cells
Erythroid precursors
10 10 10 10 100 1 2 3 4
12704.008CD56 PE ->
CD56-PE
T-S
SC
Monocytic cells

EUROFLOW DATABASES: WHAT IS THEIR UTILITY?
- To evaluate the performance of antibody panels.
- To prospectively evaluate new cases against reference groups.
- To identify the most informative markers
- To automatically identify, gate and name multiple cell populations present in a sample.

Neutrophil maturation vs normal BMOverlayed Normal vs cytopenic BM

NEUTROPHIL MATURATION DATA BASE: BM case vs a reference normal BM data base

Neutrophil maturation: reactive vs normal BM
Overlayed Normal vs reactive BM
Overlayed Normal vs MDS BM
+3SD
-3SD
+10SD
-10SD

Concluding remarks
- Multiple studies have shown that FCM can assist in the diagnosis andprognostication in MDS as well as in cases suspected of MDS and in pre-MDS conditions.
- Despite no marker-abnormality or aberrant phenotype is specific forMDS, such alterations might help in the differential diagnosis betweenreactive and MDS bone marrow. However, the final diagnosis of MDShas to be based on other criteria
- Despite all the above, no generally accepted consensus exists as regardsthe optimal SOPs to apply.
- Current efforts and undergoing multi-center projects have the aim tostandardize the approach and to facilitate its reproducible use in routinediagnostics.

THE CIC/USAL-IBSAL TEAM

MUITO OBRIGADO