-
REVIEW
A History of Gonioscopy
Wallace L. M. Alward*
ABSTRACTThe first view of the iridocorneal angle in a living
human occurred accidentally in the late 1800s. Lenses were first
usedto see the angle in 1914, but practical gonioscopy would not
come into existence for many years as the slitlamp andlenses that
could be used at the slitlamp were developed. This article reviews
the history of gonioscopy.(Optom Vis Sci 2011;88:2935)
Key Words: gonioscopy, history, direct gonioscopy, indirect
gonioscopy, Salzmann, Trantas, Barkan, Allen
Clinical gonioscopy is just over 100 years old. During those100
years, some remarkable scientists and astute clinicianshave played
roles in the development of this importantexamination technique.
This review will summarize the develop-ment of gonioscopy. The
illustrations, rather than being of thepeople who advanced the
field, will concentrate on the angle im-ages that they
produced.
Gonioscopy is considered to have two fathers, and theprimacy of
the two innovators is dependent on the views of theauthors.
Dellaporta1 wrote a delightful and detailed history ofgonioscopy
that includedmany charming personal anecdotes. Del-laporta focused
on the contributions of Trantas, with whom heshares a Greek
heritage. Other accounts focus on Salzmann, whowas the first to
study the optics behind gonioscopy and the first touse a lens to
view the angle. In their textbook, Gorin and Posner2
say that Salzmann will always be revered by ophthalmologists
asthe father of gonioscopy. This review will consider both
fatherschronologically.
Gonioscopy is required to view the iridocorneal angle,
becauselight from the angle reflects back into the anterior chamber
at thetear-air interface (Fig. 1). This is because of the total
internalreflectionjust as in a fiberoptic cable. The only
circumstances inwhich the angle can be seen without special
manipulation are incases of keratoglobus where the light from the
angle strikes thecornea at an angle perpendicular enough to escape.
This is veryrare.
Direct Gonioscopy
To view the iridocorneal angle, one needs to overcome
totalinternal reflection in some way. We do this today with a
variety of
lenses, but the first gonioscopy was performed with an
ophthalmo-scope and indentation. The first person to examine the
iridocornealangle in a living human was the Greek ophthalmologist
AlexiosTrantas3 in 1898. Trantas was in private practice. He was an
out-standing observerfor example, he first identified the
conjuncti-val infiltrates in vernal conjunctivitis that bear his
name (Trantasdots). Trantas was able to see the angle using a
direct ophthalmo-scope while indenting the sclera with his finger
(Fig. 2).3 He wasactually more interested in viewing the ciliary
body, ora serrata,and anterior retina. His view of the iridocorneal
angle was a fortu-nate accident. In 1900, he described the
appearance of a cyclodi-alysis cleft in a patient with an
iridodialysis (his view was madeeasier by the iridodialysis,
because the iris was not in the way).1 Helater presented remarkably
detailed drawings of the angle (Fig. 3).4
His descriptions of the angle were an afterthought, included in
anappendix of an article describing the retrociliary region.4 It
wasTrantas who coined the term gonioscopy, meaning observationof
the angle, in his native Greek.1
Maximilian Salzmann was a brilliant ophthalmologist who,upon
graduating from college at age 15, went on to contribute inall
aspects of eye research. He was also skilled in languages,
math-ematics, geology, and botany. Salzmann was a gifted painter
whosepaintings were used in many textbooks of his time.5 His
owntextbook, The Anatomy and Histology of the Human Eyeball in
theNormal State, was a classic in German and was translated
intoEnglish. Salzmann was unaware of the work of Trantas,
becausethe descriptions of gonioscopy in the articles of Trantas
did notappear in the titles or abstracts.1 He first recognized the
concept oftotal internal reflection.6 He also determined that total
internalreflection could be overcome with a highly convex lens
(Fig. 4).Salzmannwas the first to view the angle through a contact
lens and,in 1915, published an article with excellent drawings of
the angleobtained by means of a Fick contact lens (a lens designed
to treatkeratoconus).7 He was not satisfied with the view through
the Fick
*MDDepartment of Ophthalmology, University of Iowa Carver
College of Medi-
cine, Iowa City, Iowa.
1040-5488/11/8801-0029/0 VOL. 88, NO. 1, PP. 2935OPTOMETRY AND
VISION SCIENCECopyright 2011 American Academy of Optometry
Optometry and Vision Science, Vol. 88, No. 1, January 2011
-
lens and, so, had Zeiss build him a lens with a smaller radius
ofcurvature.2 Although Trantas was the first to see the angle,
Salz-mann was the first to really study the angle. Salzmann
stressed theimportance of gonioscopic examination in the fellow eye
of pa-tients who had suffered an attack of acute glaucoma.2 He
recog-nized that the development of synechiae in the angle did not
alwayslead to increased intraocular pressure.2 Salzmann was also
the first
to describe blood in Schlemms canal.1 Salzmann produced
won-derful drawings of the iridocorneal angle (Figs. 5 and
6).6,7
Through the courtesy of S. Karger AG, Basel, all of
Salzmannsgonioscopy paintings are reproduced at:
http://gonioscopy.org/salzmann/salzmann.html.
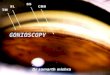
Mizuo examined the inferior angle in patients by everting
thelower lid and filling the cul-de-sac with saline. The saline
meniscusacted like a contact lens.8 He described this technique in
1914.Elschnig had verbally reported to Salzmann the same
techniqueusing the patients own tears.2,7 The technique was
difficult toperform because the saline lens was lost whenever the
patientblinked.8
Many events occurred around 1920 that brought gonioscopyinto
clinical relevance. Zeiss developed the modern slitlamp atabout
this time, which permitted significant advances in gonios-copy. In
1920, Curran9 published his landmark article that recog-nized that
angle-closure glaucoma was caused by forward bulgingof the iris and
that surgical iridectomy (which had been used in-discriminately for
glaucoma) would only work for angle closurecases. He recognized
that the iridectomy worked by reestablishingflow from the posterior
to anterior chambers, not by uncoveringthe trabecular meshwork. In
1919, Koeppe10 used the Zeiss slit-lamp to examine the angle with
his newly developed direct contactlens, which was thicker and more
convex than the lenses used by
FIGURE 1.Total internal reflection occurs when the light from
the iridocorneal anglestrikes the tear-air interface at a shallow
enough angle that all the light isreflected back into the eye.
Reproduced with permission from Color Atlasof Gonioscopy, 2nd ed:
San Francisco, American Academy of Ophthal-mology, 2008.24
FIGURE 2.One can overcome total internal reflection by indenting
the limbus tomake the light from the angle exit the cornea at a
steep enough angle thatit is not reflected back into the eye. This
is the technique that was used byTrantas. Reproduced with
permission from Color Atlas of Gonioscopy,2nd ed: San Francisco,
American Academy of Ophthalmology, 2008.24
FIGURE 3.Trantas made the first drawings of the iridocorneal
angle. This showsremarkable detail given the limitations of his
technique. Published in1918.1,4
FIGURE 4.Direct lens. This lens changes the approach of the
light from the iridocor-neal angle so that it is more
perpendicular, thus overcoming total internalreflection. Reproduced
with permission from Color Atlas of Gonioscopy,2nd ed: San
Francisco, American Academy of Ophthalmology, 2008.24
FIGURE 5.Painting by Salzmann, 1915. Right eye, inferior and
temporal-temporalportion, male, 37 y/o, traumatic cataract, (case
VII) (goniolens). Circum-scribed and incomplete peripheral
synechiae, pigmentation of the trabec-ular meshwork. Reproduced
with permission from Z Augenheilkd, 34,2649, 1915.31
30 A History of GonioscopyAlward
Optometry and Vision Science, Vol. 88, No. 1, January 2011
-
Salzmann. Gonioscopy was performed with the patient seated atthe
slitlamp. A knotted bandage rested on a central depression inthe
lens to secure it to the patient. This technique was effective
onlyfor evaluating the nasal and temporal portions of the angle.
TheKoeppe lens and modifications of the Koeppe lens (Barkan,
Swan-Jacobs, etc.) are still used today for direct gonioscopy.
In 1925, Manuel Uribe Troncoso11 developed a selfilluminat-ing
monocular gonioscope that permitted examination of all partsof the
angle. The handheld device combined the examining ocularswith an
illumination system. He also improved on the Koeppe lensby using
polymethylmethacrylate instead of glass.2 In 1942, hecreated a
handheld stereoscopic gonioscope.
In 1927, Thorburn first photographed the angle in a case ofangle
closure brought on by mydriatics and subsequently reversedby
physostigmine. He also observed that the majority of his pa-tients
with glaucoma had open angles.12
Barkan et al.13 used a binocular slitlamp suspended from
theceiling and a handheld illuminator to view the angle through
aKoeppe lens. His technique had the advantage of bright
illumina-tion and sufficient magnification. The flexibility of the
ceiling-mounted handheld slitlamp enabled the entirety of the angle
to beevaluated with the Koeppe lens in a supine patient. Barkans
appa-ratus brought gonioscopy into practical clinical
application.
Barkan14,15 was also the first to describe goniotomy under
directvisualization for primary congenital glaucoma. Before Barkan,
go-
niotomy had been performed without visualizing the angle.
Hedeveloped a special variation of the Koeppe lens in which one
sidewas flattened to permit passage of the knife through the
temporalcornea. Barkan felt that the eyes of children with
congenital glau-coma had a membrane covering the iridocorneal angle
(Barkansmembrane) because of the glistening appearance of the
angles ofbabies with glaucoma.16 It is now recognized that there is
no Bar-kans membrane, simply compressed trabecular beams.17
Clinical use of direct gonioscopy is now limited to the
operatingroom for examining babies under general anesthesia and for
per-forming angle surgery. Direct gonioscopy is required for
somesurgical techniques such as for goniotomy for infantile
glaucomaangle and for the Trabectome for open-angle glaucoma.
Directgonioscopy is rarely used in the clinic because it is
inconvenient.The patient needs to be supine in a special room with
a ceiling-mounted counterbalanced slitlamp. Any examination
techniquethat is inconvenient is less likely to be performed. The
Van Herickestimation of angle depth was developed because it was
not prac-tical to perform direct gonioscopy on every patient, and
it washelpful to have a means of identifying worrisomely narrow
anglesat the slitlamp. To quote Van Herick et al.,18 In the
routineexamination of nonglaucomatous patients, it is impractical
to per-form gonioscopy; it is only done of the angles are thought
to benarrow. In 2010, indirect gonioscopy is easy and
convenientenough that the Van Herick technique should simply be an
ad-junct to gonioscopy.
Indirect Gonioscopy
Modern indirect gonioscopy was introduced in 1938 with
theGoldmann mirrored contact lens.19 The Goldmann lens uses a
FIGURE 7.Indirect gonioscopy lens. Light from the iridocorneal
angle is reflected bya mirror so that it is visible to an observer
at a slitlamp. Reproduced withpermission from Color Atlas of
Gonioscopy, 2nd ed: San Francisco,American Academy of
Ophthalmology, 2008.24
FIGURE 6.Painting by Salzmann 1915. Left eye, temporal quadrant,
male, 37 y/o,small rupture of the corneoscleral border (case XIV).
Displacement of theiris because of the vitreous coming forward and
radial tear. Visible coronaciliaris (pars plicata). Reproduced with
permission from Z Augenheilkd,34, 2649, 1915.
A History of GonioscopyAlward 31
Optometry and Vision Science, Vol. 88, No. 1, January 2011
-
mirror to redirect the light from the iridocorneal angle, so
that it isvisible to the examiner viewing through a slitlamp (Fig.
7). Gold-mann was another polymath whose name is familiar because
of thegonioscopy lens, tonometer, and perimeter that bear his name.
Hiscontributions to the understanding of the eye in health and
diseasewere too numerous to list here.20 With the Goldmann lens at
aslitlamp, one could readily examine the entire angle using
thereadily available slitlamp, rather than a separate apparatus.
Gonios-copy was no longer reserved for those with suspiciously
narrowangles on slitlamp examination. The Allen lens, developed a
fewyears later, used totally refractive prisms rather than a
mirror.21
This was later modified into the Allen-Thorpe gonioprism,
whichhad four prisms and permitted most of the angle to be
viewedwithout rotation of the lens (Fig. 8).22 The Allen-Thorpe
lens hadflanges that held it in place allowing the examiner time
and free
hands to make detailed drawings of the findings.
Four-mirroredlenses, such as the Zeiss, Posner, Sussman, andVolkG-4
lenses, arecommonly used today.Unlike theGoldmann lens, these
lenses do notrequire a methylcellulose coupling solution. The
remarkable anglepaintings of Lee Allen were created with the
Allen-Thorpe lens (Figs.9 and 10).Many of the Lee Allens paintings
are included in theColorAtlas of Gonioscopy,23,24 and all of his
gonioscopy paintings are avail-able at:
http://gonioscopy.org/leeAllenPaintings.html.
There have been no major developments in lens design over
thelast several decades. There have been modifications to the
Gold-mann and Allen-Thorpe/Zeiss lenses. Variations of the
Goldmannlens include lenses with one to four mirrors. In the
three-mirrorlens, two of the mirrors are for viewing the peripheral
retina. Other
FIGURE 8.Allen-Thorpe lens. This was the original four-mirror
lens. It actually usedprisms instead of mirrors and had a flange to
hold it into place. The prismswere replaced by mirrors in
subsequent lenses (Zeiss, Posner, etc.).
FIGURE 9.A Lee Allen painting and sketch of a normal
iridocorneal angle with deep trabecular pigmentation. Reproduced
with permission from the Universityof Iowa.
FIGURE 10.A Lee Allen painting showing blood in Schlemms canal.
Reproduced withpermission from the University of Iowa.
32 A History of GonioscopyAlward
Optometry and Vision Science, Vol. 88, No. 1, January 2011
-
Goldmann-style lenses (such as the Ritch lens) are specially
de-signed and coated with antireflective material for the delivery
oflaser energy. Others have mirrors that magnify slightly. The
Zeissstyle lenses are now available in plastic or glass withmirrors
that areless fragile than the original Zeiss lens. These are
available withhandles (e.g., Posner and Volk G-4 with optional
handle) or with-out handles (e.g., Sussman and Volk G-4), and there
is even asix-mirror version (Volk G-6). However, the recent changes
ingonioscopy lenses have been evolutionary, not revolutionary.
A major advance in gonioscopy technique was the introductionof
the technique of indentation gonioscopy. First taught by Drs.Becker
andMoses atWashingtonUniversity with a handheld Zeissgoniolens, it
was refined by using the Zeiss lens on anUnger handlebyMax Forbes
in 1966.25 Indentation gonioscopy requires the useof a gonioscopy
lens with an area of contact smaller than the cornea(e.g., Zeiss,
Posner, Sussman, Volk G-4, etc.). By using one of
these lenses, the examiner pushes against the cornea, which
drivesthe lens-iris diaphragm posteriorly. This permits the
examiner todetermine whether areas of angle closure are because of
appositionor synechiae. Indentation gonioscopy can also reveal a
peripheraliris hump in plateau iris syndrome. Lenses with large
areas ofcontact (such as the Goldmann lens) are not ideal for
this.
Grading Systems
The first system to grade the angle was that of Gradle
andSugar26 in 1940. They used an Ulbrich drum mounted on
theslitlamp to measure the chamber depth in millimetersnot
some-thing that could be practically used in the clinic. Scheie27
devel-oped a grading system based on the visible structures. The
Scheiesystem was opposite of our current systems. In the Scheie
system,there was a category called Wide followed by grade I, which
was
FIGURE 11.An illustration by Emil Bethke from Troncosos
textbook. Reproduced with permission from Gonioscopy: Philadelphia,
FA Davis, 1947.32
TABLE 1.Important textbooks and atlases of gonioscopy
Year Authors Title Publisher
1947 Troncoso Gonioscopy FA Davis1955 Van Beuningen Atlas der
Spaltlampengonioskopie Thieme1957 Gorin and Posner Slit Lamp
Gonioscopy Williams & Wilkins1962 Shaffer Stereoscopic Manual
of Gonioscopy CV Mosby1973 Kimura Color Atlas of Gonioscopy Igaku
Shoin1994 Alward Color Atlas of Gonioscopy CV Mosby2008 Alward and
Longmuir Color Atlas of Gonioscopy, 2nd ed. American Academy of
Ophthalmology
A History of GonioscopyAlward 33
Optometry and Vision Science, Vol. 88, No. 1, January 2011
-
slightly narrowed through grade IV, which was completely
closed.Today, some still use a system in which they describe the
visiblestructure such as open to the ciliary body face etc.
Importantly,Scheie introduced a scale of grading the pigmentation
of the pos-terior trabecular meshwork (from none to grade IV) that
is usedtoday.
The most widely used systems nowadays are the Shaffer andSpaeth
systems. The Shaffer28 grading technique was described inhis 1962
textbook. Shaffer determined an angle width in degrees(e.g., grade
110 and grade 4 3545). It has the advantage ofbeing widely
recognized and easy to understand. A disadvantage isthat it
provides only angular width information and tells nothingabout the
iris shape or the level at which the iris inserts.
Spaeth29 modified the Shaffer system to provide
informationregarding the level of iris insertion (on a scale of A
to E, with Abeing anterior to Schwalbes line and E being extremely
deep intothe ciliary body), the angle of iris approach (in
degrees), and theconfiguration of the iris (b for bowed forward, f
for flat, c forconcave, and p for plateau). To this, one adds the
angle pigmen-tation. For example, the Spaeth system would grade the
angle inthe Lee Allen painting in Fig. 9 to beD45f, with 2
pigmentation.The Spaeth system also permits information on
indentation go-nioscopy findings. This system is somewhat harder to
learn butprovides much more information than any other
alphanumericgrading system.
Textbooks of Gonioscopy
In 1947, Troncoso published a comprehensive 306-page text-book
entitled Gonioscopy. The text contains comparative anatomyand
gonioscopy as well as beautifully illustrated descriptions of
theangle in health and disease. Many of the illustrations were
paintedby Emil G. Bethke (Fig. 11). Interestingly, Bethke had been
amedical illustrator at the University of Iowa where he roomed
witha fellow artist, E. Lee Allen. When Bethke left the University,
LeeAllen became the artist for the Department of Ophthalmology
anddeveloped a life-long interest in gonioscopy (see Figs. 8 to
10).Since Troncosos book, there have been a handful of
gonioscopytexts and atlases; the most important of which are
included inTable 1.
Shaffers Stereoscopic Manual of Gonioscopy is a wonderful
re-source, now out of print.28 His book includes beautiful
drawingsby Joan Esperson and three-dimensional photographs
viewedthrough a View-Master. Kimuras Color Atlas of Gonioscopy
hasbeautiful photographs of the angle.30 Kimuras atlas was out
ofprint when my book of the same name was published in 1994.23
Because gonioscopy is a dynamic examination, it may be
besttaught with video, instead of still images. I created a webpage
toteach gonioscopy (www.gonioscopy.org). The site is free and is
notindustry supported. It includes detailed descriptions of basic
andadvanced examination techniques as well as hundreds of
videoexamples of pathology.
There are new ways to evaluate the iridocorneal angle, such
asultrasound biomicroscopy and optical coherence tomography.
Thesetechniques can describe the width of the angle and perhaps the
riskof developing angle closure. They are excellent tools, but
theycannot replace gonioscopy, which tells us so much more
thanwhether the angle is open or closed. We are
fortunatethrough
the efforts of Trantas, Salzmann, Zeiss, Barkan, Goldmann,
Allen,and othersto be able to actually look at the dysfunctional
mesh-work rather than having to rely on imaging.
Received April 26, 2010; accepted August 11, 2010.
REFERENCES
1. Dellaporta A. Historical notes on gonioscopy. Surv
Ophthalmol1975;20:13749.
2. Gorin G, Posner A. Slit Lamp Gonioscopy, 3rd ed. Baltimore,
MD:Williams & Wilkins; 1967.
3. Trantas A. Ophtalmoscopie de la region ciliaire et
retrociliaire. ArchOphtalmol (Paris) 1907;27:581606.
4. Trantas A. Lophtalmoscopie de langle irido-corneen. Arch
Ophtal-mol (Paris) 1918;36:25776.
5. Sugar HS, Foster CC. Maximilian Salzmann. Ophthalmic
pioneerand artist. Surv Ophthalmol 1981;26:2830.
6. Salzmann M. Die Ophthalmoskopie der Kammberbucht. Z
Augen-heilk 1914;31:119.
7. Salzmann M. Nachtrag zu ophthalmoskopie der kammerbucht.
ZAugenheilk 1915;34:1602.
8. Mizuo. Ein Verfahren zur Besichtigung der Kammberbucht.
KlinMonatsbl Augenheilkd 1914;52:561.
9. Curran EJ. A new operation for glaucoma involving a new
principlein the etiology and treatment of chronic primary glaucoma.
ArchOphthalmol 1920;49:13155.
10. Koeppe L. Diemikroskopie des lebenden Kammerwinkels im
fokalenLichte der Gullstrandschen Nernstspaltlampe. Albrecht von
GraefesArch Klin Ophthalmol 1919;101:4866.
11. TroncosoMU. Gonioscopy with the Electric Ophthalmoscope.
NewYork, NY: New York Academy of Medicine; 1921.
12. Thorburn T. A gonioscopical study of anterior peripheral
synechiaein primary glaucoma. Svenska Lakaresallskapets Handligar
1927;53:25291.
13. Barkan O, Boyle SF, Maisler S. On the genesis of glaucoma.
Animproved method based on slit lamp microscopy of the angle of
theanterior chamber. Am J Ophthalmol 1936;19:20915.
14. Barkan O. Glaucoma: classification, causes, and surgical
control. Re-sults of microgonioscopic research. Am J Ophthalmol
1938;21:1099117.
15. Barkan O. Recent advances in the surgery of chronic
glaucoma. Am JOphthalmol 1937;20:123745.
16. Barkan O. Pathogenesis of congenital glaucoma: gonioscopic
andanatomic observation of the angle of the anterior chamber in
thenormal eye and in congenital glaucoma. Am J Ophthalmol
1955;40:111.
17. Anderson DR. The development of the trabecular meshwork and
itsabnormality in primary infantile glaucoma. Trans Am
OphthalmolSoc 1981;79:45885.
18. VanHerickW, Shaffer RN, Schwartz A. Estimation of width of
angleof anterior chamber. Incidence and significance of the narrow
angle.Am J Ophthalmol 1969;68:6269.
19. Goldmann H. Zur Technik der Spaltlampenmikroskopie.
Ophthal-mologica 1938;96:907.
20. Fankhauser F. Hans Goldmann. Ophthalmic Surg 1994;25:812.21.
Allen L, OBrien CS. Gonioscopy simplified by a contact prism.
Arch
Ophthalmol 1945;34:4134.22. Allen L, Braley AE, Thorpe HE. An
improved gonioscopic contact
prism. AMA Arch Ophthalmol 1954;51:4515.23. Alward WL. Color
Atlas of Gonioscopy. London: Wolfe; 1994.24. Alward WL, Longmuir
RA. Color Atlas of Gonioscopy, 2nd ed. San
Francisco, CA: American Academy of Ophthalmology; 2008.
34 A History of GonioscopyAlward
Optometry and Vision Science, Vol. 88, No. 1, January 2011
-
25. Forbes M. Gonioscopy with corneal indentation. A method for
dis-tinguishing between appositional closure and synechial closure.
ArchOphthalmol 1966;76:48892.
26. Gradle HS, Sugar HS. Concerning the anterior chamber angle.
III. Aclinical method of goniometry. Am J Ophthalmol
1940;23:11359.
27. Scheie HG. Width and pigmentation of the angle of the
anteriorchamber; a system of grading by gonioscopy.
AMAArchOphthalmol1957;58:5102.
28. Shaffer RN. Stereoscopic Manual of Gonioscopy. St. Louis,
MO:Mosby; 1962.
29. Spaeth GL. The normal development of the human anterior
chamberangle: a new system of grading. Trans Ophthalmol Soc UK
1971;91:70939.
30. Kimura R. Color Atlas of Gonioscopy. Tokyo: Igaku Shorin
Ltd.;1974.
31. Salzmann M. Die Ophthalmoskopie der Kammerbucht. Z
Augen-heilkd 1915;34:2649.
32. Troncoso MU. Gonioscopy. Philadelphia, PA: FA Davis;
1947.
Wallace L. M. AlwardDepartment of Ophthalmology
University of Iowa Carver College of Medicine200 Hawkins
Drive
Iowa City, Iowa 52242e-mail: [email protected]
A History of GonioscopyAlward 35
Optometry and Vision Science, Vol. 88, No. 1, January 2011