Embed Size (px)
Citation preview

A healthy respect for Sexual
Health
Dee Archbold
CNC
Princess Alexandra Sexual Health
2018

Princess Alexandra Sexual Health
(PASH)
• Sexual health service for Metro South (estimated >1million residents
and 23% of QLD population)
• Based at PA Hospital
• Outreach to Logan Hospital (Fridays)
• Our Team
- 2 Consultants (Dr Palmer & Dr Siebert)
- 1 sessional Registrar
- CNC (Dee Archbold)
- Contact tracing support officer (Alan Walker)
- 4.5 Clinical Nurses
- 1 part time Indigenous Clinical nurse & 1 indigenous male
health worker
Princess Alexandra Sexual Health
(PASH)
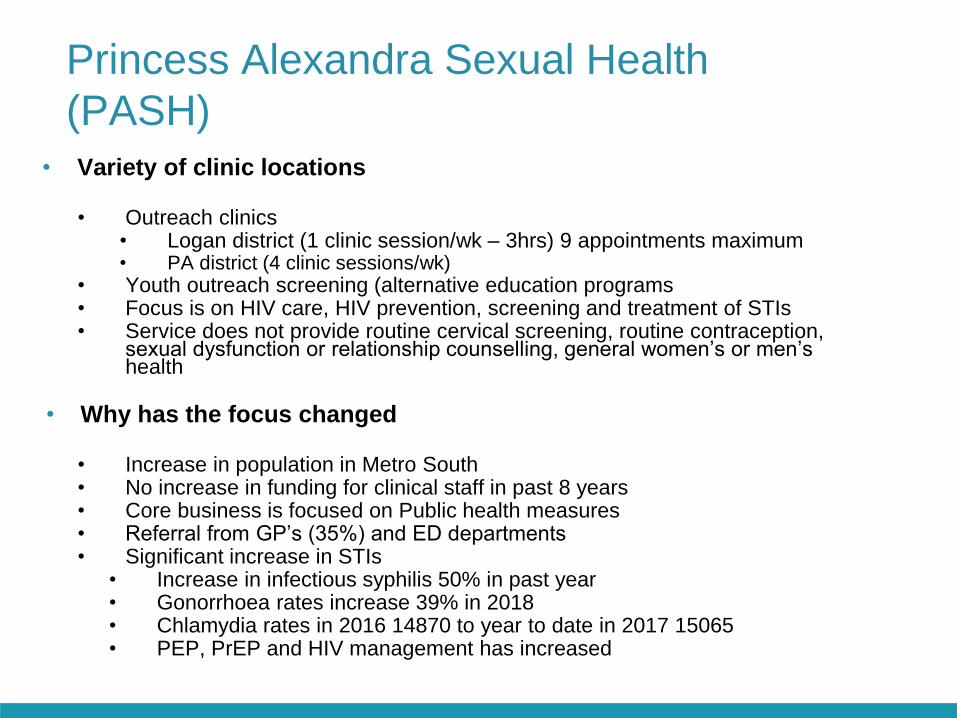
• Variety of clinic locations
• Outreach clinics• Logan district (1 clinic session/wk – 3hrs) 9 appointments maximum• PA district (4 clinic sessions/wk)
• Youth outreach screening (alternative education programs• Focus is on HIV care, HIV prevention, screening and treatment of STIs• Service does not provide routine cervical screening, routine contraception,
sexual dysfunction or relationship counselling, general women’s or men’s health
• Why has the focus changed
• Increase in population in Metro South• No increase in funding for clinical staff in past 8 years• Core business is focused on Public health measures• Referral from GP’s (35%) and ED departments• Significant increase in STIs
• Increase in infectious syphilis 50% in past year• Gonorrhoea rates increase 39% in 2018• Chlamydia rates in 2016 14870 to year to date in 2017 15065• PEP, PrEP and HIV management has increased

Princess Alexandra Sexual Health
(PASH)
• Appointment based outpatient service
– Shared OPD space with other hospital services
• Management of HIV & complex STIs, nPEP and PrEP
• Screening high risk population groups (MSM, CALD, Youth, ATSI)
• Contact tracing
• Referrals: DEM, GPs, RAPID clinic, etc.
• Self referrals Ph: 3176 5881 Mon-Fri 8am- 4pm
– Triaged through the Sexual Health information line by Clinical Nurses
– Priority for MSHHS residents
– Medicare eligibility for some services
– Full names on pathology

Youth Outreach Screening
• Program led by Indigenous Clinical Nurse (Bel Connolly)
• Metro South alternative education facilities
– Yourtown facilities (Capalaba, Woodridge, Kingston, Beenleigh)
– Kingston Y school
– Kingston Centre Ed
– Kingston Adult Learning
– Yeronga SHS
– Babi Wynnum
– Hemmant Flexi
• Urine chlamydia and gonorrhoea PCR
• Education session
• If positive result, referred to PASH or GP for treatment

New Youth Service commencing May 2019
• Shared care for patients accessing LADDERS (Logan
Adolescent Drug Dependencies Early Response
Service) for 12-25 years experiencing problematic
alcohol and other drug use
• Once a week on a Tuesday morning
• Focus on screening and treatment of STIs, contraception
and sexual safety

STIs and young people considerations
• Screening >14 years
• Psychosocial Assessment (HEADSS tool)
Assess ability to consent, risk factors, possible neglect and abuse
• Gillick Competency and informed consent
• Mandatory reporting
• Range of other social issues (home life, schooling, contraception,
mental health, alcohol & drugs)

STI challenges
• Increasing rates of bacterial STIs (MSM,
Indigenous & heterosexual)
– Increasing rates of syphilis
– Increasing rates of gonorrhoea
– Increasing rates of Mycoplasma genitalium
https://kirby.unsw.edu.au/report/annual-surveillance-
report-hiv-viral-hepatitis-and-stis-australia-2017

Biomedical HIV interventions
• HIV testing models
– Rapid testing (community organisations)
– Home testing (purchased online)
• HIV TasP (treatment as prevention)
– U=U (Undetectable = Untransmittable)
• Post-exposure prophylaxis (PEP)
• Pre-exposure prophylaxis (PrEP)

Chlamydia
• The most common bacterial STI >23, 000 cases in QLD in 2017
• > 91, 000 cases nationally in 2017
• Most common in 15-29 years of age (80% of notification are people under 29 yo)
• Particular high notification rates include females, those aged 15–19, ATSI population, and
people residing in regional & remote locations
Chlamydia testing for young people
• General practitioner
• Sexual health service
– Clinic appointment
– Youth outreach program
• Aboriginal Medical Services
• LGBTQIA+ community testing sites (RAPID)
• Web testing
– https://www.qld.gov.au/health/staying-healthy/sexual-health/chlamydia-
test

Chlamydia – right test, right site and right drug
• Consider testing at other anogenital sites if MSM
(throat & rectal) or heterosexual having AIC not
just urine
• PCR testing (correct collection technique)
• First line treatment with Azithromycin has less
clearance rates in throat and rectal sites
• TOC for throat and rectal sites (one month)
• TORI for genital sites (3 months)

Gonorrhoea
Significant increase over last 7 years, > 5000 cases in QLD in 2017
> 28,000 cases nationally in 2017 (10,324 cases 2010)
53% of diagnoses in people aged 15-29 years of age (75% residing in major
cities)
Highest risk for MSM, ATSI population and increase in heterosexual infections
Between 2012 and 2016, there was a 63% increase in notification rates from
61.9 per 100 000 in 2012 to 100.8 per 100 000 in 2016, with increases in both
males (72%) and females (43%) in this period
Almost a third (32%) of gonorrhoea notifications in Aboriginal and Torres Strait
Islander people in 2016 were in people aged 15–19 years, compared with 7%
in the non-Indigenous population

Gonorrhoea
Gonorrhoea challenges
• Increase in young people
• Increase in indigenous people (especially youth and
remote)
• Increase in MSM (asymptomatic, increase in rectal
infections)
• Increase in heterosexual men and women (locally
acquired)
• Increase in young reproductive women (vertical
transmission, asymptomatic, gynaecological
complications) TIP of the Iceberg
• Increasing resistance patterns
• Limited access to treatment in the community

Gonorrhoea resistance• WHO has listed highly drug-resistant Neisseria gonorrhoea as one of the
twelve priority pathogens posing a threat to human health globally due to
drug resistance
– 3 cases of extensively drug resistant gonorrhoea (XDR)
• Penicillin and ciprofloxacin resistant is widespread in Australia with
increasing resistance to azithromycin
• High level resistance to both Azithromycin and Ceftriaxone is currently rare,
but there has been two Australian cases of high resistance to both these
drugs
Issues– Change to PCR testing (less culture sensitivities to identify changing
resistance patterns for individual and surveillance)
– Increase in asymptomatic presentations (identified by screening and
contact tracing)
– Decrease in condom usage in all groups
– Increased need for contact tracing and TOC follow up
– Change in sexual networks (websites, phone apps)
– Increased and fast pace partner change
Public health strategies
• Increase testing awareness (health providers & community)
• Dual PCR testing for both chlamydia & gonorrhoea
• All positive PCR samples and symptomatic presentations to include
culture and sensitivities
• Surveillance of resistance patterns (public health units & state
notifications)
• Improve access to ceftriaxone in community settings
• Intensive contact tracing and TOC
• Rapid testing in community (GeneXpert)
– Automated and rapid detection
– Urine, endocervical swabs, throat and rectal
– Sometimes individual pooled samples rather than site specific
– Results 30-90 minutes (dependant on how many cycles)
– Inhibitory substances (blood, mucus, semen, anogenital
medication or products)
– Sensitivity 86 -91% and specificity 99.2 -100%

Syphilis
Significant increase over last 7 years, > 1000 cases in QLD in 2017 (338 Cases in
2011) 310% increase
> 4,000 cases nationally in 2017 (887 cases nationally in 2006)
16% notification in ATSI, 87% of infectious syphilis were in men, 36% aged 15-29
years and 70% residing in major cities
Highest risk for MSM, ATSI population and increasing cases in heterosexuals
(antenatal)
High rates of missing data for indigenous status and likely to underestimate rates
within the indigenous community

Syphilis in Indigenous communities • There is an ongoing outbreak of infectious syphilis affecting young Aboriginal and
Torres Strait Islander people, predominately aged between 15 and 29 years, living in
northern Australia.
• The outbreak began in northern Queensland in January 2011, extended to the
Northern Territory in July 2013, and then onto the Kimberley region of Western
Australia in June 2014. In March 2017, South Australia declared an outbreak in the
Western, Eyre and Far North regions from November 2016.
• The Australian Health Protection Principal Committee (AHPPC) Governance Group
has developed a National strategic approach for an enhanced response to the
disproportionately high rates of STI and BBV in Aboriginal and Torres Strait Islander
people (Strategic Approach).
• This will address the disproportionately high rates of syphilis and other Blood-Borne
Viruses (BBV) and Sexually Transmissible Infections (STI) in regional and remote
Indigenous communities.

Syphilis Action Plan
• Testing and treatment
– PoCT and STI testing guidelines
– Rapid access to treatment
– Workforce development and community engagement
– Increasing primary health screening (ED, other health
checks)
• Surveillance and reporting
– Improved data collection (including indigenous status)
• Education and awareness
– Workforce training and resources
– Culturally appropriate education/health promotion resources
• Sporting venues, use of positive role models (enablers/influences),
indigenous radio, incentives, peer education models
– Targeting young women, long term ramifications and
engagement in antenatal care
• Antenatal care
– Improve antenatal guidelines for testing and retesting
– Surveillance and investigation of congenital syphilis cases

Mycoplasma genitalium

• Smallest free-living micro-organisms
• In the urogenital tract
– M.genitalium
– Ureaplasma urealyticum
– U.parvum
– M.hominis
• Mg first isolated in 1980
Mycoplasma genitalium
Mycoplasma genitalium
• Associated with male non-chlamydial non-gonococcal urethritis (NCNGU), with consequences of urethritis, balanoposthitis, prostatitis, proctitis and possible male infertility (70% symptomatic)
• Most common clinical manifestation is acute and chronic urethritis
• Ranges from 10% to 35% cause for NCNGU
• In women, association with urethritis, cervicitis, endometritis and pelvic inflammatory disease, abnormal vaginal bleeding (40-75% are asymptomatic)
• Associated with increased risk of tubal factor infertility
• No suggestion of pharyngitis
Limited health promotion programs

Prevalence
• Few studies to determine the prevalence of Mg
• Variation of prevalence in different populations is
multi-factorial
– Different types of samples
– Self collected vs clinician collected
– Storage conditions
– Restrictions for enrolment (often symptomatic
only)
• Overall prevalence is 1% in low risk to 8% in
higher risk groups

Transmission & risk factors
• High concordance rates within couples (up to 43%)
• HIV positive MSM have higher rates of Mg
• Adherence of mycoplasma to HIV infected cells can
increase HIV virus release, and may play a role in the
replication and pathogenicity of HIV
• Direct genital to genital mucosal contact
• Minimal incubation period is two weeks

Specimen collection
• PCR testing (access to macrolide resistance
testing in some settings)
• No consensus which specimens are preferable
• Sensitivities
– Vaginal/cervical swabs (85.7%)
– First catch urine (97.4%)
– Rectal swabs (24.3%)

Who to test
• All men who present with urethritis
– Urine sample of first catch and use yellow urine
jar not PCR kits for CH/GC
• All contacts of positive Mg (men and women)
• Women with cervicitis
• Urine and Rectal swabs for MSM
• Pharyngeal swabs not recommended

Treatment
• Only few antimicrobial classes have activity against mycoplasmas
including tetracyclines (doxycycline, macrolides (azithromycin) and
fluoroquinolones (moxifloxacin), streptogramins (Pristinamycin)
• Doxycycline has poor efficacy (cure rates 30-40%)
• Azithromycin 1 g single dose (cure rates 85% in macrolide
susceptible infections)
• Macrolide resistance of up to 50% and combined
macrolide/fluoroquinolones resistance of 8.6%
• Moxifloxacin has a cure rate approaching 75% in infections with
susceptible strains but resistance is up to 15% in macrolide
resistance strains
• Pristinamycin if failure to both Azithromycin, Moxifloxacin
• Possible use of extended doxycycline for 14 days

Treatment – International debate
First line
• doxycycline 100mg twice a day for 7 days to reduce
bacterial load prior to other treatment options
• Followed by azithromycin 1g first dose then 500mg daily for
further 3 days
Persistent infection (symptomatic or positive TOC)
• Moxifloxacin 400mg daily for 7 days
Persistent infection post Moxifloxacin course
(symptomatic or positive TOC)
• Pristinamycin 1g four times a day for 10 days

Management
• Abstain from UP sexual contact (approx. 5 weeks) until
partners have completed treatment, symptoms resolved
and test of cure negative Patients with anal infection
should be informed about the risk of transmission and
maybe more difficult to eradicate and therefore TOC is
important
• Patient’s with Mg should be screened for other STI’s
• Mg during pregnancy may be associated with a increase
of spontaneous abortion and preterm birth

Test of cure
• Repeat PCR (including all positive sites)
• TOC at 4 weeks (after completion of treatment)
• If tested sooner, possible false positive result rather than
reinfection or persistence
• Due to limited treatment options, important to ensure
TOC done at optimal interval
Contact tracing
• Unknown time period
• Focus on direct partners of symptomatic or persistent
infection

Media promotion

Sexual Health Check for young people
campaign
• https://stoptherise.initiatives.qld.gov.au/
• https://www.qld.gov.au/health/staying-healthy/sexual-health
• 13HEALTH (13432584)
• What are some of the challenges arising from health promotion campaigns
• How do we meet the needs of young people requesting sexual health screening

Sexual health resources
• https://www.health.qld.gov.au/clinical-
practice/guidelines-procedures/sex-
health/resources
• Animations about sexual health

Health promotion resources
• https://youngdeadlyfree.org.au
/resources/ (indigenous young
people includes factsheets,
posters, videos