Embed Size (px)
Citation preview
Comprehensive diagnosis of lower extremity
pathologies requires assessment of the contractile capaci�
ty of muscles. The literature on joint mobility diagnosis
and dynamometry of the femur and crus muscles is enor�
mous [1�3]. There is a correlation between muscle force
and cross�sectional area [4]. This correlation is charac�
terized by age� and gender�dependent factor of
force/cross�sectional area of muscle [5]. This factor
increases twofold from 6 to 20 years of age without gen�
der�related variation and does not depend on sex hor�
mones [6]. In diagnostic practice, it is methodologically
difficult to interpret the results of hand dynamometry.
The physiological basis of this test and test methodology
as well as exact interpretation of test results are the main
problems. Femoral dynamometry is particularly impor�
tant in the case of femur pathology. The methodology of
the test and interpretation of its results require additional
study. In addition to practical purposes, the results of the
test are of considerable theoretical significance [7]. The
literature about functional incompetence of femoral mus�
cles in postural and locomotor behavioral stereotypes is
scarce and scattered.
The femoral dynamometer was constructed at the
Ilizarov Scientific Center for Restorative Traumatology
and Orthopedics, Ministry of Health of the Russian
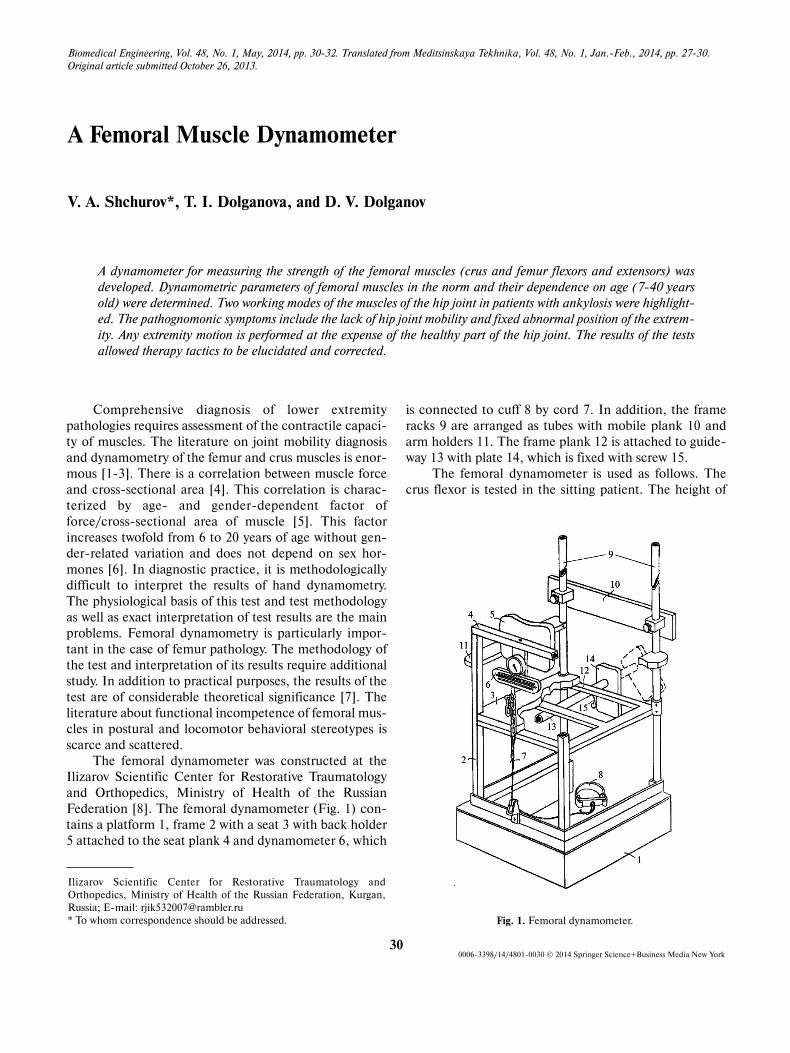
Federation [8]. The femoral dynamometer (Fig. 1) con�
tains a platform 1, frame 2 with a seat 3 with back holder
5 attached to the seat plank 4 and dynamometer 6, which
is connected to cuff 8 by cord 7. In addition, the frame
racks 9 are arranged as tubes with mobile plank 10 and
arm holders 11. The frame plank 12 is attached to guide�
way 13 with plate 14, which is fixed with screw 15.
The femoral dynamometer is used as follows. The
crus flexor is tested in the sitting patient. The height of
Biomedical Engineering, Vol. 48, No. 1, May, 2014, pp. 30�32. Translated from Meditsinskaya Tekhnika, Vol. 48, No. 1, Jan.�Feb., 2014, pp. 27�30.
Original article submitted October 26, 2013.
300006�3398/14/4801�0030 © 2014 Springer Science+Business Media New York
Ilizarov Scientific Center for Restorative Traumatology and
Orthopedics, Ministry of Health of the Russian Federation, Kurgan,
Russia; E�mail: [email protected]
* To whom correspondence should be addressed.
A Femoral Muscle Dynamometer
V. A. Shchurov*, T. I. Dolganova, and D. V. Dolganov
A dynamometer for measuring the strength of the femoral muscles (crus and femur flexors and extensors) was
developed. Dynamometric parameters of femoral muscles in the norm and their dependence on age (7�40 years
old) were determined. Two working modes of the muscles of the hip joint in patients with ankylosis were highlight�
ed. The pathognomonic symptoms include the lack of hip joint mobility and fixed abnormal position of the extrem�
ity. Any extremity motion is performed at the expense of the healthy part of the hip joint. The results of the tests
allowed therapy tactics to be elucidated and corrected.
Fig. 1. Femoral dynamometer.
Femoral Muscle Dynamometer 31
platform 1 is 20 cm. Cuff 8 is attached to the ankle joint
above the crus. If knee contracture is absent, the crus is
bent at an angle of 90о. If knee contracture is present, the
angle is increased as much as possible. Unit 7 is used to
regulate the length of the cord. The muscle force is meas�
ured by the Tokar dynamometer with cord connected to
the dynamometer (certificate No. 86/1027�68) attached
to plank 4. The maximal force is tested for the standing
patient. The patient faces frame 9, while his/her knee
contacts plate 14. The total force of the crus flexor is
measured. Plate 14 is extracted from cylinder 13 and fixed
using screw 15.
The crus–extensor force moment is calculated by the
formula:
М = F·L·cos(α – 90°).
The crus–flexor force moment is calculated as:
М = F·L·cos(180° – α).
The parameters of the femur extensor and flexor as
well as femur adductors and abductors were determined.
Plate 14 is inserted into cylinder 13. The patient’s hip is
attached to plank 10. The standing patient contacts plank
10 and the dynamometer. The distance from the patient’s
hip to cuff 8 determines the lever length L. The hip cen�
ter is 1 cm above femoral artery, close to the trochanter.
The force moment is calculated from the absolute
force F measured using the dynamometer and distance L
from hip to cuff 8, as well as knee joint angle α other than
90°.
The force moment is calculated as:
М = F·L.
The femoral dynamometer provides comfortable
testing conditions. The goal of this work was to test
dynamometric parameters of femur and crus flexor and
extensor as well as femoral adductors and abductors.
Results
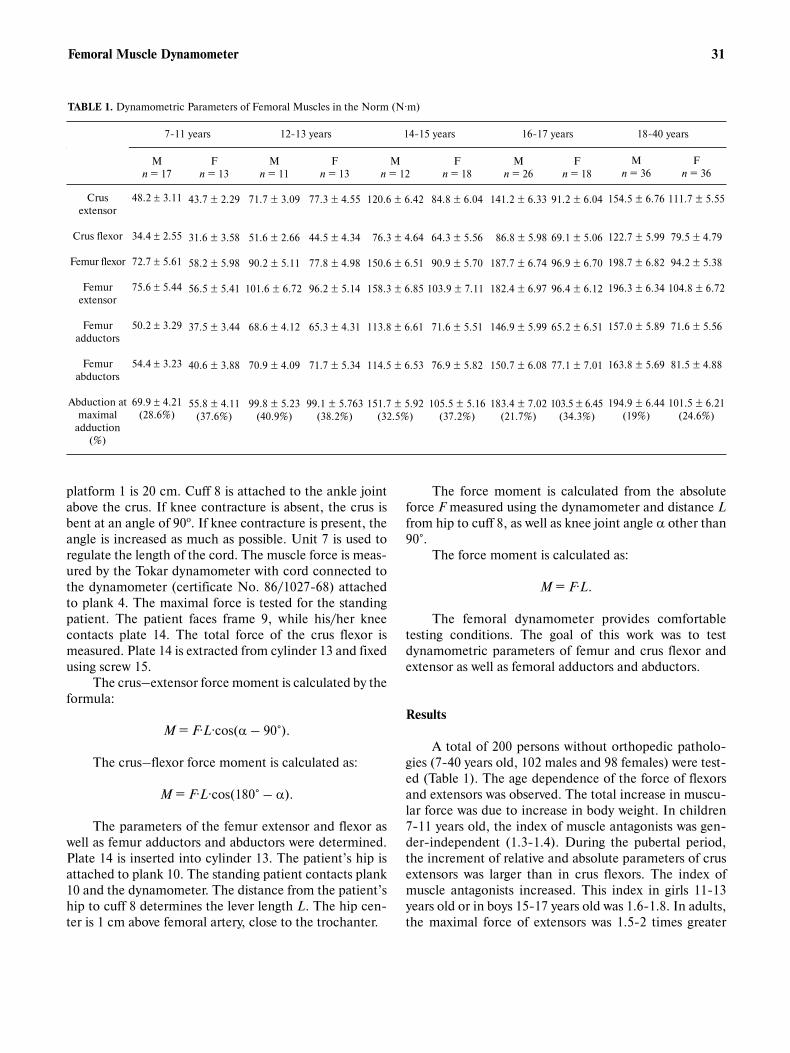
A total of 200 persons without orthopedic patholo�
gies (7�40 years old, 102 males and 98 females) were test�
ed (Table 1). The age dependence of the force of flexors
and extensors was observed. The total increase in muscu�
lar force was due to increase in body weight. In children
7�11 years old, the index of muscle antagonists was gen�
der�independent (1.3�1.4). During the pubertal period,
the increment of relative and absolute parameters of crus
extensors was larger than in crus flexors. The index of
muscle antagonists increased. This index in girls 11�13
years old or in boys 15�17 years old was 1.6�1.8. In adults,
the maximal force of extensors was 1.5�2 times greater
TABLE 1. Dynamometric Parameters of Femoral Muscles in the Norm (N·m)
M
n = 17
48.2 ± 3.11
34.4 ± 2.55
72.7 ± 5.61
75.6 ± 5.44
50.2 ± 3.29
54.4 ± 3.23
69.9 ± 4.21
(28.6%)
F
n = 13
43.7 ± 2.29
31.6 ± 3.58
58.2 ± 5.98
56.5 ± 5.41
37.5 ± 3.44
40.6 ± 3.88
55.8 ± 4.11
(37.6%)
M
n = 11
71.7 ± 3.09
51.6 ± 2.66
90.2 ± 5.11
101.6 ± 6.72
68.6 ± 4.12
70.9 ± 4.09
99.8 ± 5.23
(40.9%)
F
n = 13
77.3 ± 4.55
44.5 ± 4.34
77.8 ± 4.98
96.2 ± 5.14
65.3 ± 4.31
71.7 ± 5.34
99.1 ± 5.763
(38.2%)
M
n = 12
120.6 ± 6.42
76.3 ± 4.64
150.6 ± 6.51
158.3 ± 6.85
113.8 ± 6.61
114.5 ± 6.53
151.7 ± 5.92
(32.5%)
F
n = 18
84.8 ± 6.04
64.3 ± 5.56
90.9 ± 5.70
103.9 ± 7.11
71.6 ± 5.51
76.9 ± 5.82
105.5 ± 5.16
(37.2%)
M
n = 26
141.2 ± 6.33
86.8 ± 5.98
187.7 ± 6.74
182.4 ± 6.97
146.9 ± 5.99
150.7 ± 6.08
183.4 ± 7.02
(21.7%)
F
n = 18
91.2 ± 6.04
69.1 ± 5.06
96.9 ± 6.70
96.4 ± 6.12
65.2 ± 6.51
77.1 ± 7.01
103.5 ± 6.45
(34.3%)
7�11 years 12�13 years 14�15 years 16�17 years 18�40 years
Crus
extensor
Crus flexor
Femur flexor
Femur
extensor
Femur
adductors
Femur
abductors
Abduction at
maximal
adduction
(%)
M
n = 36
154.5 ± 6.76
122.7 ± 5.99
198.7 ± 6.82
196.3 ± 6.34
157.0 ± 5.89
163.8 ± 5.69
194.9 ± 6.44
(19%)
F
n = 36
111.7 ± 5.55
79.5 ± 4.79
94.2 ± 5.38
104.8 ± 6.72
71.6 ± 5.56
81.5 ± 4.88
101.5 ± 6.21
(24.6%)

32 Shchurov et al.
than the maximal force of flexors, which was training�
dependent [9].
Seventy patients with pathologies of the proximal
segment of the femoral bone were observed. In patients
with dysplasia of the hip joint, there was a significant
decrease in the parameters of femoral flexor dynamome�
try (m. psoas and m. iliac), as well as femoral adductor
(gluteus minimus and gluteus medius muscles). Femoral
extensors prevent kyphosis of the hip. One�year�long
therapy completely restored parameters of muscle
dynamometry. This provided for the recovery of the
femoral muscular apparatus. Nevertheless, 6 months after
the Ilizarov apparatus was removed, the femoral dynamo�
metric parameters remained constant. One year after the
Ilizarov apparatus was removed, the parameters were at
the level of 79% of the initial value. Crus flexors and
femoral abductors recovered more slowly [3].
In 20 patients with hip ankylosis (18�34 years old)
the movement of the pathological extremity was imple�
mented at the expense of the healthy hip part [10].
The intact extremity muscles operate in two modes:
1) femur movement at the expense of hip movement; 2)
intact extremity movement. In mode 1, the ankylosed leg
was tested using the dynamometer plank 10 set at various
heights. In mode 2, the intact leg was tested using
dynamometer plank 10.
In patients with hip ankylosis, there was a 20�40%
decrease in the muscular force of the intact extremity in
mode 1 before therapy relative to mode 2. The index of
antagonists was constant in the intact extremity in the two
modes. This index for femoral adductors/abductors was
96�105%, while for extensors it was 75�85%.
Conclusion
1. The femoral muscle dynamometer suggested in
this work allows the functional state of femoral muscles to
be tested quantitatively in adequate units and their
dynamics to be measured objectively.
2. The tests of the dynamometer in healthy subjects
and patients with locomotor pathologies demonstrated
that there are age and gender variations in the force
parameters of the tested muscles. Their recovery dynam�
ics were also studied.
3. Compensatory mechanism was observed in
patients with hip ankylosis. Any pathological extremity
motion was performed at the expense of the healthy part
of the hip joint.
4. The mathematical expectation of the force
moment of the muscles given in Table 1 with regard to the
age and gender can be used as a measure of pathology
severity.
5. The dynamometric parameters of the tested mus�
cles are additional diagnostic symptoms and allow reha�
bilitation tactics to be corrected.
REFERENCES
1. A. Rasch, N. Dalén, and H. E. Berg, Acta Orthop., 81, 183�188 (2010).
2. M. Kargarfard, M. Dehghadani, and R. Ghias, Int. J. Prev. Med.,
4, 50�56 (2013).
3. E. V. Oleinikov, T. I. Dolganova, M. P. Teplen’kii, D. V. Dolganov,
and T. V. Sizova, Vrach�Aspir., 54, 472�479 (2012).
4. J. M. Scanlan, K. L. Ballmann, J. L. Mayhew, and C. D. Lantz, J.
Sports Med. Phys. Fitness, 39, 54�60 (1999).
5. K. Funato, H. Kanehisa, and T. Fukunada, J. Sports Med. Phys.
Fitness, 40, 312�318 (2000).
6. C. M. Neu, F. Rauch, J. Rittweger et al., Amer. J. Physiol., No. 1,
E103�107 (2002).
7. T. I. Dolganova, Functional Processes in Human Body
Accompanying Treatment with Ilizarov Apparatus, LAP LAM�
BERT Academic Publishing, Saarbrücktn (2011).
8. V. A. Shchurov, D. V. Dolganov, T. I. Dolganova, and I. A.
Atmanskii, “A Device for Determining Hip Muscle Force”, RF
Patent No. 118782/20 (2003).
9. A. S. Vitenzon, Features of Normal and Pathological Trait [in
Russian], Zerkalo�M, Moscow (1998).
10. V. I. Shevtsov, I. A. Atmanskii, and S. G. Tyutrin, Gen. Ortoped.,
No. 2, 75�81 (1997).





























