Embed Size (px)
Citation preview

A Drug Therapy SmorgasbordA Drug Therapy Smorgasbord Practical Issues for Dietitians Practical Issues for Dietitians
Presented by
David B. Goldwater R.Ph
Clinical Consultant Pharmacist

2
ObjectivesObjectives
1. Review Practical Pharmacokinetic principals to create a deeper understanding of absorption, distribution and excretion of drugs.
2. Review several commonly used drugs often reviewed for consideration by Dietitians which involve considerations of pharmacokinetics and specific drug/ food interactions.

3
Objectives continued….Objectives continued….
3. Discuss important considerations for Warfarin interactions with enteral feedings
4. Review the Pharmacodynamic effects of antipsychotics with specific focus on weight gain and blood sugar control

4
Closer Collaboration between Closer Collaboration between Pharmacists and DietitiansPharmacists and Dietitians
Changes to revised Dietary F Tag: F325. June 2008 AND
Definition of MRR in revised Pharmacy F Tag F425 (Dec 2006)
BOTH REVISIONS have strengthened the need for communications between our two disciplines.
5
Changes to F428 –Med Changes to F428 –Med Regimen Review (Dec 2006)Regimen Review (Dec 2006)
Thorough evaluation of the medication regimen of a resident by a pharmacist with the goal of promoting positive outcomes and minimizing adverse consequences associated with medications;
The review includes: preventing, identifying, reporting, and resolving medication-related problems, medication errors, or other irregularities AND
collaborating with others members of the interdisciplinary team.”

6
Personal impact of working Personal impact of working closer with dietitianscloser with dietitians
1. Appreciation of the positive influence on outcome for residents due to collaborations with Dietitians in LTC.
2. A strong interest in speaking to you as a group today.
3. The topics chosen for review today, have come directly from collaborations and discussions with individual Dietitians in my personal practice.
4. On a lighter note………….

Personal Impact of Personal Impact of Working closer with Working closer with
DietitiansDietitians
British Canadian American
dietiCIAN
dietiTIAN dietiTIAN
Practical Issues For Practical Issues For DietitiansDietitians
Basic Concepts of Pharmacokinetics

9
Study of what the body does to a drug.
How the body → How the body → movesmoves drug in and drug in and out. (out. (AbsorptionAbsorption Distribution Excretion) Distribution Excretion)
Pharmacokinetics
10
Study of the influence (dynamics) of the DRUG
on the BODY
Pharmacodynamics

11
FIRST ORDER KINETICSFIRST ORDER KINETICS
1. The majority of drugs are eliminated in this way.
2. A constant fraction of the drug in the body is eliminated per unit time.
3. The rate of elimination is proportional to the amount of drug in the body.

12
FIRST ORDER ELIMINATIONFIRST ORDER ELIMINATION
ConcentratioConcentration in plasman in plasma
TimeTime

13
Volume of Distribution Volume of Distribution (For(For drugs which follow first order kinetics)
The Volume of Distribution (Vd) is the amount of drug in the body divided by the concentration in the blood.
Highly LIPID SOLUBLE DRUGS, such as digoxin, have a very High Vd.(500liters).
LIPID INSOLUBLE DRUGS, such as neuromuscular blockers, remain in the blood, and have a Low Vd.
14
Clearance (Cl) Clearance (Cl) (For(For drugs which follow first order kinetics)
The Clearance (Cl) of a drug is the VOLUME of plasma from which the drug is COMPLETELY removed per unit time.
The amount of drug eliminated is PROPORTIONAL to the concentration of the drug in the blood.

15
Elimination Elimination (For(For drugs which follow first order kinetics)
RATE of elimination
EQUAL TO
Clearance x Concentration in the blood._______________________________________________________________________________________
Elimination HALF LIFE (t1/2)
EQUAL TO
Time taken for plasma conc. to reduce by 50%.

16
RULE OF THUMBRULE OF THUMB
100% Elimination After 5 HALF-
LIVES (Symbol for Half-life is t ½ )

17
Half-life: ImplicationsHalf-life: Implications
We can determine how long it takes to reach steady state
E.g. DIGOXIN ……t ½ = 40hrs
1. It takes approximately 200 hrs ~8 days for DIGOXIN to reach STEADY STATE LEVELS.
2. It takes approximately ~8 days for DIGOXIN to be COMPLETELY ELIMINATED from the system.

18
Simple, isn't it?
What we discussed above is a SINGLE COMPARTMENT model,
This is what would occur if the bloodstream was the only compartment in the body (or if the Vd = the blood volume).
But the human body is more complex than this! There are many compartments: muscle, fat, brain
tissue etc. In order to describe this, we use MULTI-
COMPARTMENT models.

19
MULTICOMPARTMENT MULTICOMPARTMENT MODELSMODELS
Q. Why does a patient wake up after 5 minutes after an injection of Thiopentone, when we know that it takes several hours to eliminate this drug from the body?
A. Initially the drug is ALL in the blood and this blood goes to "vessel rich" organs; principally the brain.
The drug then redistributes into other tissue compartments. (fat, muscle etc)
In response to the decrease in brain concentration the net effect is that the patient wakes up 5 minutes later!

20
Elimination: MULTI COMPARTMENT MODELElimination: MULTI COMPARTMENT MODEL
TimeTime
Concentration
Rapid distribution phase αα
Elimination phaseβ
Equilibrium phase (Plateau)

21
A SIMPLE A SIMPLE TWO COMPARTMENT MODELTWO COMPARTMENT MODEL
The first part is the rapid redistribution phase: (alpha phase.)
The plateau (equilibrium phase) (where blood concentration = tissue concentration)
The slower phase, the beta phase, is the elimination phase where blood and tissue concentrations fall in tandem

22
BIOAVAILABIILITY BIOAVAILABIILITY
This is the fraction of the administered dose that reaches the systemic circulation.
Bioavailability is 100% for intravenous injection. It varies for other routes depending on
incomplete absorption, first pass hepatic metabolism etc.
When we plots plasma concentration Vs. time, the bioavailability is the area under the curve.

23
BIOAVAILABILITYBIOAVAILABILITY
TimeTime
ConcentrationConcentration
in plasmain plasma
(for a drug given orally)(for a drug given orally)
BIOAVAILABILITYBIOAVAILABILITY is is the the AREA UNDER THE AREA UNDER THE CURVECURVE

24
DOSAGE REGIMENDOSAGE REGIMEN
The strategy for ADMINISTRATION DOSING is to administer ONLY, sufficient amounts of drug to attain therapeutic effect, but not enough to produces toxicity!
THEREFORE WE APPLY THESE PRINCIPLES…… STEADY STATE CONCENTRATION is achieved
AFTER FIVE half lives, therefore…. At STEADY STATE
Maintenance Dose = Rate of Elimination
WE THEREFORE CONCLUDE THAT…… Rate of Administration = Rate of Elimination
25
DOSAGE REGIMENDOSAGE REGIMEN
Drugs will accumulate within the body if the drug has not been fully eliminated before the next dose.
This is OK only IF, we are willing to wait 5 half lives for the drug to be fully effective ………but what if we cannot wait that long?
Then we need to "load" the volume of distribution WITH the drug to achieve target plasma concentrations RAPIDLY.

26
Hepatic Drug ClearanceHepatic Drug Clearance
Many drugs are extensively metabolized by the liver.
The rate of elimination depends on: The liver's inherent ability to metabolize the drug The amount of drug presented to the liver for
metabolism.

27
Hepatic Drug Clearance(First Pass effect)
This is important because orally administered drugs go from Ingestion →gut → portal vein → liver.
The liver DIVERTS a varying chunk of the administered drug by (pre-systemic elimination) and therefore less is available to the body for therapeutic effect.
EXAMPLE:
This is why we give a higher dose of ORAL morphine, for the equipotent INTRAVENOUS dose
30 MG ORAL Morphine is EQIPOTENT TO
1 MG IV Morphine.
ORAL: PARENTERAL RATIO = 3 : 1

28
Drug distribution
FACTORS THAT EFFECT WHERE THE DRUG ENDS UP:1. BLOOD FLOW
tissues with the highest blood flow receive the drug first.2. PROTEIN BINDING
drugs stuck to plasma proteins are crippled, because they can only go where the proteins go
3. LIPID SOLUBILITY & DEGREE OF IONIZATION this describes the ability of drugs to enter tissues (highly lipid soluble / un-ionized drugs can basically go
anywhere).

29
Protein Binding
Most drugs bind to proteins: Albumin OR Alpha-1 Acid Glycoprotein (AAG),
FREE drug is usually the preferred state, because FREE drug can travel throughout the body, in and out of tissues and exert a biological effect.
Free drug on the other hand is subject to metabolizing enzymes.

30
Protein Binding
HIGHLY BOUND drug has a longer duration of action and a lower volume of distribution.
Why is this important? 1. For HIGHLY protein bound drugs, we need
to give more of it to get a therapeutic effect; as so much is stuck to protein.
2. If another drug comes along and starts to compete with the drug for the binding site on
the protein →
the amount of FREE drug is ↑ ↑ INCREASED

31
Clinical Implications for HIGHLY Clinical Implications for HIGHLY Protein Bound DrugsProtein Bound Drugs
DRUG-A ------ 97% BOUND TO ALBUMIN……3% free drug. Addition of DRUG-B displaces DRUG-A from its binding sites Causing 3% reduction in Protein binding for DRUG-A
RESULTS in a 50% increase in FREE DRUG-A concentration from 3% to 6%
DRUG-X ------ 70% BOUND TO ALBUMIN……30% free drug. Addition of DRUG-Y displaces DRUG-X from its binding sites Causing 3% reduction in Protein binding for DRUG-X
RESULTS in a NEGLIGIBLE increase of FREE DRUG-X concentration from 30% to 33%

32
Clinical Implications for HIGHLY Protein Bound Drugs
The HIGHLY BOUND drugs that we really need to focus on are: warfarin, diazepam, propranolol, phenytoin.
For example, a patient on warfarin is admitted with seizures, you treat the patient with phenytoin, next thing you know - his INR is 10.
The amount of albumin does not appear to be hugely relevant. In disease states such as sepsis, the serum
albumin drops drastically, but the free drug concentration does not appear to increase
HOWEVER: For residents with LOW serum Albumin there is a formula that we apply to DILANTIN levels results to adjust the DILANTIN level

Practical Issues For Practical Issues For DietitiansDietitians
Warfarin Resistance & Enteral Warfarin Resistance & Enteral feeding: New understanding of feeding: New understanding of An Old ProblemAn Old Problem
34
History of History of Enteral feedings & WarfarinEnteral feedings & Warfarin
Warfarin resistance first reported in the early 1980’s was POSITIVELY associated with CONTINUOUSCONTINUOUS enteral tube feedings.
AttributedAttributed to largelarge amounts of vitamin K amounts of vitamin K containedcontained within the feedings.
Patients commonly received several several hundred microgramshundred micrograms per day of vitamin K!

35
CORRECTIVE ACTIONS TAKENCORRECTIVE ACTIONS TAKEN
The pharmaceutical industry subsequently responded to this problem……
Resulting in significantly reduced vitamin K content of liquid enteral nutrition formulations.
Most current liquid enteral formulations Most current liquid enteral formulations NOW CONTAIN LESS NOW CONTAIN LESS THAN 80 MCG/LITER OF VITAMIN K.THAN 80 MCG/LITER OF VITAMIN K.

36
Why does this issue still occur?Why does this issue still occur?
Still some anecdotal reports of difficulty in achieving therapeutic anticoagulation when warfarin was given concomitantly with CONTINUOUSCONTINUOUS LIQUID ENTERAL FEEDINGS
Still some anecdotal reports of significant increases in the (INR) when the enteral feeding was discontinued.
Schurgers and associates (2004) performed a study to ascertain the CLINICAL IMPACT OF VITAMIN K SUPPLEMENTATION on the anticoagulation effect of the ORAL ANTICOAGULANT ACENOCOUMAROLACENOCOUMAROL.[6]

37
Is Is VIT K CONTENTVIT K CONTENT In Enteral Feeding In Enteral FeedingSTILL THE ISSUE?STILL THE ISSUE?
NOT LIKELY !NOT LIKELY !
They concluded that other factors outside of They concluded that other factors outside of enteral vitamin K intake were playing a enteral vitamin K intake were playing a greater greater rolerole in these ANECDOTAL observations in these ANECDOTAL observations BECAUSE….BECAUSE….
…………..THE TOTAL VIT K INGESTED IN ENTERAL ..THE TOTAL VIT K INGESTED IN ENTERAL FEEDING WAS FEEDING WAS SIGNIFICANTLY LOWERSIGNIFICANTLY LOWER THAN THAN THE SUPPLEMENTAL DOSES USED IN THE THE SUPPLEMENTAL DOSES USED IN THE STUDYSTUDY

38
Guidelines for Daily Vit K IntakeGuidelines for Daily Vit K Intake
Guidelines from the Food and Nutrition Board of the Institute of Medicine for adequate intake of Vit K are as follows:
in healthy adult men : Vit-K 120 mcg/day
In healthy adult women: Vit-K 90 mcg/day

39
Findings by Schurgers and Findings by Schurgers and colleagues [5]colleagues [5]
A statistically significant decrease in INR by 0.4 was found when….
The subjects’ supplemental vitamin K intake was increased to 150 mcg/day. This was in addition to their baseline 55 mcg/day55 mcg/day
______________________________________
The GRAND TOTAL of dietary vitamin K intake was 205 mcg /day

40
Findings by Schurgers and Findings by Schurgers and colleagues [5]colleagues [5]
They confirmed that supplemental intake of up to 100 mcg/day of vitamin K100 mcg/day of vitamin K did NOT significantly interfere with oral anticoagulant therapy in healthy individuals already receiving about 55 mcg of dietary vitamin K.
THEY CONCLUDED: That a total vitamin K intake of about vitamin K intake of about
150 mcg daily150 mcg daily is NOTNOT likely to affect warfarin requirements.[5]

41
Dickerson and Colleagues ReviewDickerson and Colleagues Review
Dickerson and colleagues studied (INR) values in 6 patients requiring continuous enteral feeding during the first 10 days of warfarin therapy.[6]
For 3 consecutive days, feedings were interrupted for 1 hour before and after warfarin administration.
On 3 other consecutive days, feedings were NOT interrupted for warfarin administration.
The INR increased by a mean of 0.74 during the 3-day interval when the enteral feedings were interrupted for warfarin.
In contrast, the INR decreased by a mean of 0.13 during the 3-day interval when enteral feedings were NOT interrupted .
42
Dickerson and Colleagues Dickerson and Colleagues CONCLUSIONCONCLUSION
Holding enteral feeding 1 hour BEFORE and 1 hour AFTER warfarin administration …….lessens warfarin resistance
This strategy is recommended for warfarin This strategy is recommended for warfarin administration administration DURING CONTINUOUSDURING CONTINUOUS ENTERAL FEEDINGSENTERAL FEEDINGS..

43
KEY POINTSKEY POINTS:: Warfarin Management in Enteral Warfarin Management in Enteral
Nutrition Nutrition 1,6,71,6,7
1. Consider an alternative method of anticoagulation.
2. Monitor INR frequently.
3. Administer warfarin BETWEEN feedings
for patients receiving INTERMITTENT tube feedings.
4. Stop feedings ONE hour before and ONE hour after warfarin administration for patients receiving CONTINUOUS tube feedings,.

44
KEY POINTSKEY POINTS::
5. Consider increasing the rate of feedings to avoid loss of calories.***
6. Administer warfarin consistently (ie, hold feedings for all doses)
7. Do not add warfarin directly to the enteral nutrition.
8. Warfarin dose requirements may change if the enteral regimen is altered or if the oral diet is resumed.

45
KEY POINTSKEY POINTS::
9. Warfarin dose requirements may change if the enteral regimen is altered or if the oral diet is resumed.
10. If Enteral feedings are InitiatedEnteral feedings are Initiated in a patient stable on warfarin, the warfarin may require a dose increasemay require a dose increase
11. If WARFARIN is initiatedWARFARIN is initiated in a patient currently receiving enteral nutrition, the warfarin may require a dose decreasedose decrease upon resumption of oral diet.

Selected ReferencesSelected References
1. Lourenco R. Enteral feeding: drug/nutrient interaction. Clin Nutr. 2001;20:187-193.
2. Penrod LE, Allen JB, Cabacungan LR. Warfarin resistance and enteral
feedings: 2 case reports and a supporting in vitro study. Arch Phys Med Rehabil. 2001; 82:1270-1273.
3. Coumadin (package insert). Princeton, NJ: Bristol-Myers Squibb; 2007.
4. Food and Nutrition Board, Institute of Medicine. In: Dietary Reference Intakes for Vitamin A, Vitamin K, Arsenic, Boron, Chromium, Copper, Iodine, Iron, Manganese, Molybdenum, Nickel, Silicon, Vanadium, and Zinc. Washington, DC: National Academy Press; 2001:162-196.
3. Schurgers LJ, Shearer MJ, Hamulyak K, Stocklin E, Vermeer C. Effect of vitamin K intake on the stability of oral anticoagulant treatment: dose-response relationships in health subjects. Blood. 2004;104:2682-2689.
4. Dickerson RN, Garmon WM, Kuhl DA, Minard G, Brown RO. Vitamin K-independent warfarin resistance after concurrent administration of warfarin and continuous enteral nutrition. Pharmacotherapy. 2008; 28:308-313.
5. Engle KK, Hannawa TE. Techniques for administering oral medications to critical care patients receiving continuous enteral nutrition. Am J Health Syst Pharm. 1999; 56:1441-1444.

Practical Issues For Practical Issues For DietitiansDietitians
Other Drug-Enteral feeding Other Drug-Enteral feeding interactionsinteractions

48
Study by Dickerson et. Al.Study by Dickerson et. Al.
Roland N. Dickerson, George O. Maish III, Gayle Minard and Rex O. Brown.
Clinical Relevancy of the Levothyroxine − Continuous Enteral Nutrition Interaction
Nutr Clin Pract 2010 25: 646

49
STUDY CONCLUSION:STUDY CONCLUSION:
1. More than half of our patients receiving concurrent Levothyroxine–continuous EN developed subclinical or overt hypothyroidism within the first 2-3 weeks of therapy.
2. Holding EN for ONE hour PRE- and POST Levothyroxine administration, may be ineffective for some patients.
3. If a Levothyroxine dosage escalation is attempted following development of hypothyroidism, only a 25-mcg dosage increment is suggested.

50
STUDY CONCLUSION:STUDY CONCLUSION:
4. Serial (e.g. weekly) monitoring of TFT’s for allpatients receiving concurrent levothyroxine and EN therapy is recommended.
5. TFT monitoring should be continued until a pharmacokinetic-pharmacodynamic steady state is achieved.
6. If an incremental dosage increase is chosen for therapeutic management of hypothyrotic patients, the dosage should be reduced when the EN is discontinued.
7. Further study to ascertain the best method for managing patients with concurrent levothyroxine-EN is warranted.

Practical Issues For Practical Issues For DietitiansDietitians
Megace-Megace-ESES Vs.Vs.
PLAINPLAIN Megace? Megace?

52
IndicationsIndications
FDA APPROVED:FDA APPROVED: Megace® ES oral suspension is indicated for
the treatment of anorexia, cachexia, or an unexplained significant weight loss in patients with a diagnosis of acquired immunodeficiency syndrome (AIDS)
NON-FDA-APPROVED INDICATION NON-FDA-APPROVED INDICATION †
† For the treatment of anorexia, cachexia, or unexplained weight loss in the elderly.

53
PLAIN Megace vs. Megace ESPLAIN Megace vs. Megace ES
Plasma concentrations of Megestrol Acetate after administration of 625 mg625 mg (125 mg/mL) of Megace® ES oral suspension
IS EQUIVALENT UNDER FED CONDITIONS
TO
800 mg800 mg (40 mg/mL) of Megestrol Acetate oral suspension (see figure below).

54
EQUIVALENT under FED STATEEQUIVALENT under FED STATE

Megace-Megace-ESES 625mg/5ml625mg/5ml . (Empty (Empty Stomach)Stomach)
EFFECTIVE EFFECTIVE SERUM LEVELSERUM LEVELin UNFED Conditionin UNFED Condition
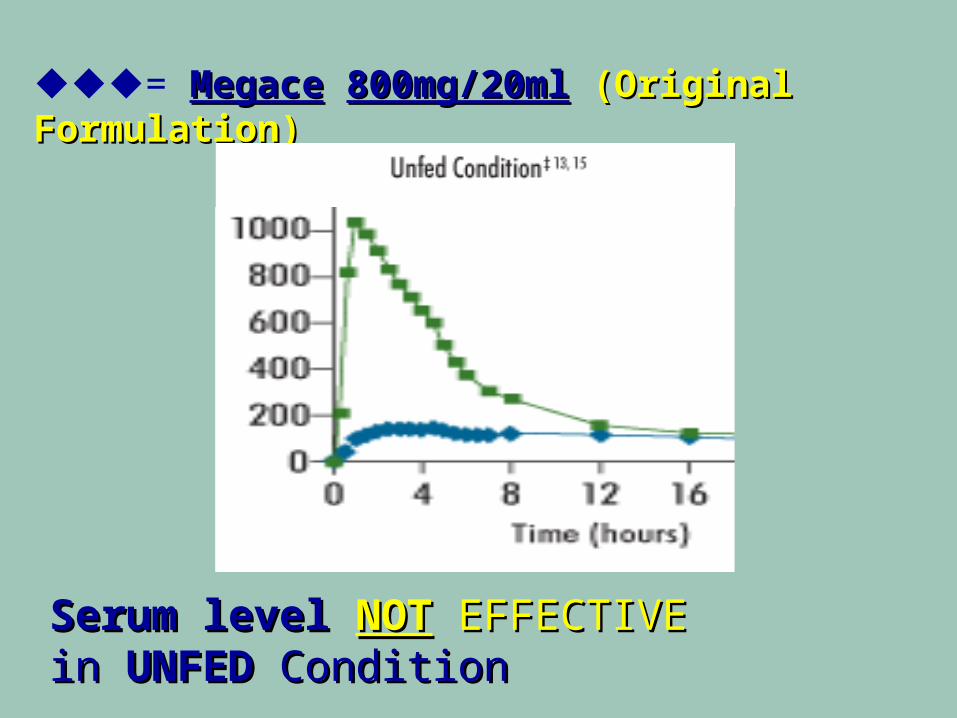
= MegaceMegace 800mg/20ml800mg/20ml (Original Formulation) (Original Formulation)
Serum levelSerum level NOTNOT EFFECTIVEEFFECTIVE inin UNFEDUNFED ConditionCondition

57
- ES- ES = Empty Stomach = Empty Stomach
Megace ES has improvedimproved bioavailability bioavailability in the UNFEDUNFED condition condition vs. original original formulaformula Megace and
ORIGINAL has equivalentORIGINAL has equivalent bioavailabilitybioavailability in the FED conditioncondition
The fed condition is achieved by subjects eating a high-calorie (800-1000 calories)and high-fat (approximately 50% of total calories) meal.

58
FDA DefinitionFDA Definition
The fed conditionThe fed condition is achieved by subjects eating a high-calorie & high-fat meal.
HIGH-CALORIE (800-1000 calories)
*** Plus ***
HIGH-FAT (aprox 50% of total calories)

59
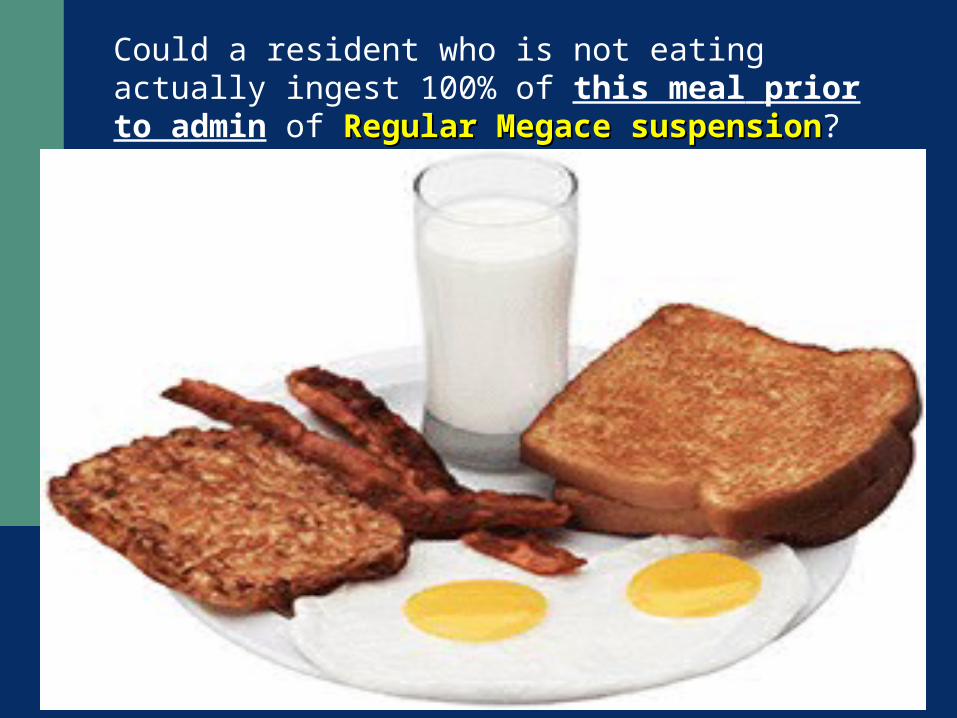
An FDA example mealAn FDA example meal
2 eggs fried in butter 2 eggs fried in butter
2 strips of bacon, 2 strips of bacon,
2 slices of toast with butter, 2 slices of toast with butter,
4 ounces of hash brown potatoes, 4 ounces of hash brown potatoes,
8 ounces of whole milk.8 ounces of whole milk.
60
Could a resident who is not eating actually ingest 100% of this meal prior to admin of Regular Regular MegaceMegace suspensionsuspension?

61
Assess EffectivenessAssess Effectiveness
The trial studies for the treatment weight loss in patients with a diagnosis of acquired immunodeficiency syndrome (AIDS) only looked at effectiveness at 12 weeks duration.
Use Megace-ES for 12 weeks. If NO or LITTLE response after 12 weeks,
then taper and then D/C

62
Serious and Otherwise Important Serious and Otherwise Important Adverse ReactionsAdverse Reactions
Hypersensitivity Pregnancy Fetal Effects Thromboembolic Disease Adrenal Insufficiency

63
WARNINGS AND PRECAUTIONS
Use with caution in patients with a history of thromboembolic disease
Clinical cases of overt Cushing’s Syndrome have been reported in association with the chronic use of Megestrol acetate.
In addition, clinical cases of adrenal insufficiency have been observed in patients receiving or being withdrawn from chronic Megestrol acetate in the stressed and non-stressed state.
New onset and exacerbation of pre-existing diabetes have been reported.

64
Megace: Adverse Consequences Megace: Adverse Consequences of DVT or PEof DVT or PE
Thromboembolism is of most significant concern
Residents of long term care who are less mobile in general and more prone to mild dehydration, may be at greater risk for the these complications.
For the clinician in the long term care setting, a careful evaluation of risk benefit ratio must be considered and based on the evidence to date.

65
Advantages of MEGACE-ESAdvantages of MEGACE-ES
LESS VOLUME and reduced viscosityand reduced viscosity Megace ES has 75% less total volume per dose Megace ES has 75% less total volume per dose
compared with Megace 800 mg/20 mL.compared with Megace 800 mg/20 mL. Megace ES is also 94% less viscous than original
formula Megace. This may be important for patients struggling with
their ability and desire to eat. Megace ES is substantially less viscoussubstantially less viscous than some
common OTC products, including Mylanta®‡1 Lower viscosity may make Megace ES easier to
take and may be important for patients who have trouble swallowing

66
Mirtazepine (Remeron)Mirtazepine (Remeron)**
Although commonly used for the purposes of promoting weight gain…….
No studies exist to date that have specifically explored the use of Mirtazepine as an appetite stimulant in the long term care setting.
* D. Rudolph : Appetite Stimulants in Long Term Care: A Literature Review. The Internet Journal of Advanced Nursing Practice. 2010 Volume 11 Number 1

Practical Issues For Practical Issues For DietitiansDietitians
Newest ORAL Anticoagulant Since The Approval of
Warfarin (Over 50 Years Ago)
68
Newest ORAL Anticoagulant Since The Approval of Warfarin (Over 50 Years Ago)
PRADAXA® (Dabigatran)
Pronounced…..
D a – bee – g´́a t t – t r a n
Approved October 2010

69
PRADAXAPRADAXA®® (Dabigatran) (Dabigatran)
THE THE FIRSTFIRST DIRECT DIRECT ORALTHROMBIN THROMBIN INHIBITORINHIBITOR

70
PRADAXAPRADAXA®® (Dabigatran) (Dabigatran) Pronounced…..Pronounced…..D a – bee – gD a – bee – g´a´a t t – t r t t – t r a na n
USA INDICATIONS AT THIS TIME ! Indicated toIndicated to reduce the reduce the risk of strokerisk of stroke and and
systemic embolismsystemic embolism in patients with in patients with NON NON VALVULAR ATRIAL FIBRILLATION.VALVULAR ATRIAL FIBRILLATION.
ADDITIONAL INDICATION (Approved in Canada and Europe (Only!)
For thromboprophylaxis in patients S/P thromboprophylaxis in patients S/P hip and knee replacement surgeries hip and knee replacement surgeries

71
Warfarin… DISADVANTAGESWarfarin… DISADVANTAGES
Warfarin has a long history of SUCCESSFUL clinical use but also has many limitations to its use.
Warfarin has an unpredictable and variable effect, It has a narrow therapeutic window requiring
frequent INRfrequent INR monitoring monitoring
It possesses numerous food and drug interactions, which all contribute to poor compliance in the ambulatory setting.

72
Particularly Dangerous DrugParticularly Dangerous Drug Interactions In Long Interactions In Long
Term CareTerm CareCompiled by AMDA American Medical Directors Association & ASCP American Compiled by AMDA American Medical Directors Association & ASCP American
Society of Consultant PharmacistsSociety of Consultant Pharmacists
WARFARIN NSAIDS
WARFARIN SULFA DRUGS
Bactrim
WARFARIN MACROLIDS
E- mycin Azithromycin
WARFARIN QUINALONES
Levaquin Cipro
WARFARIN PHENYTOIN

73
Major Advantage of WarfarinMajor Advantage of Warfarin
Warfarin has an antidote available for patients with major bleeding,

74
Dabigatran…. Pros and ConsDabigatran…. Pros and Cons
MAJOR ADVANTAGEMAJOR ADVANTAGE Dabigatran DOES Dabigatran DOES NOTNOT REQUIRE REQUIRE
ROUTINE MONITORINGROUTINE MONITORING Few drug interactions are seen with
Dabigatran.
DISADVANTAGE There is no specific antidote for Dabigatran
in patients with major bleeding.

75
MECHANISM OF ACTIONMECHANISM OF ACTION
Dabigatran and its metabolites, Acyl-Gluc-u-ron-ides (Acyl-Gluc) are competitive, DIRECT THROMBIN INHIBITORS.
THROMBIN (aka Serine Protease) enables the conversion of FIBRINOGEN into FIBRIN during the coagulation cascade…..
Inhibition of THROMBIN prevents the development of a thrombus.
Dabigatran and Acyl-Gluc INHIBIT:Dabigatran and Acyl-Gluc INHIBIT: Clot-bound and Un-bound THROMBIN …..in addition to INHIBITING thrombin-induced platelet aggregation

76
PharmacokineticsPharmacokinetics
Dabigatran is metabolized to 4 different acyl glucuronides and both the glucuronides and dabigatran have similar pharmacological activity.
Dabigatran displays dose-proportional pharmacokinetics in healthy subjects and patients in the range of doses from 10 to 400 mg.

77
ABSORPTIONABSORPTION
The absolute bioavailability of dabigatran following oral administration is approximately 3 to 7%. (Area under the curve)
After oral administration of dabigatran etexilate, CmaxCmax occurs at 1 hour post-administration in the fasted state.

78
ABSORPTIONABSORPTION
Co-administration of PRADAXACo-administration of PRADAXA with awith a HIGH-FAT HIGH-FAT meal …..meal …..ONLY DELAYS ONLY DELAYS thethe TIMETIME to to Cmax Cmax byby approximately 2 hoursapproximately 2 hours
HOWEVERHOWEVER Has NO EFFECT ON THEHas NO EFFECT ON THE ACTUALACTUAL
BIOAVAILABILITY BIOAVAILABILITY OF DABIGATRAN OF DABIGATRAN itself.itself.
KeyCmax = Maximum Concentration

79
DISTRIBUTIONDISTRIBUTION
Dabigatran is approximately 35% bound to human plasma proteins.
The volume of distribution of dabigatran is 50 to 70 L.
Dabigatran pharmacokinetics are dose proportional after single doses of 10 to 400 mg. Given twice daily.
80
ELIMINATIONELIMINATION
Dabigatran is eliminated primarily in the urine After oral administration of radio labeled
dabigatran, 7% of radioactivity is recovered in urine and 86% in feces.
The half-life of dabigatran in healthy The half-life of dabigatran in healthy subjects is 12 to 17 hours.subjects is 12 to 17 hours.

81
METABOLISMMETABOLISM
After oral administration, dabigatran etexilate is converted to dabigatran by esterase catalyzed hydrolysis to the active principal dabigatran.
DABIGATRAN IS DABIGATRAN IS NOTNOT A A SUBSTRATE SUBSTRATE INHIBITOR OR INDUCERINHIBITOR OR INDUCER OF CYP450 OF CYP450 ENZYMESENZYMES.

82
ADMINISTRATION CAUTIONADMINISTRATION CAUTION
1. The oral bioavailability of PRADAXA increases increases by 75%by 75% when the when the pelletspellets are taken are taken without without the the capsule shellcapsule shell ……………… ……………… compared to the compared to the intact capsuleintact capsule formulation. formulation.
2.2. PRADAXA capsules should therefore NOT BE PRADAXA capsules should therefore NOT BE BROKEN, CHEWED, OR OPENED BROKEN, CHEWED, OR OPENED beforebefore administration.administration.
3. PRADAXA may be administered WITH or WITHOUT FOOD
83
CRITICAL IMPLICATIONSCRITICAL IMPLICATIONS
DABIGATRAN is NOT APPROPRIATE DABIGATRAN is NOT APPROPRIATE in the following situations:in the following situations:
Administration via G-TubeAdministration via G-Tube In residents who have In residents who have difficultly difficultly
swallowing whole capsulesswallowing whole capsules

Drug InteractionsDrug InteractionsInteracting Drug
Dabigatran Effect
Comments
Rifampin Ketoconazole However, the manufacturer of dabigatran does not
recommend a dosage adjustment
Clopidogrel However capillary bleeding times were not further prolonged compared to clopidogrel monotherapy
Amiodarone However, the manufacturer of dabigatran does not recommend a dosage adjustment
Quinidine At present, the use of dabigatran is contraindicated with quinidine, a potent P-glycoprotein inducer
Verapamil Increased If VERAPAMIL given 1
hr BEFORE Dabigatran
However, the manufacturer of dabigatran does not recommend a dosage adjustment
Verapamil NO change If VERAPAMIL given 2 hr AFTER Dabigatran
Always give Dabigatran 2 hr BEFORE VERAPAMIL

85
DOSAGE AND ADMINISTRATIONDOSAGE AND ADMINISTRATION
PRADAXA 150 mg by mouth TWICE daily, with or without food. (For creatinine clearance (CrCl) >30 mL/min)
PRADAXA 75 mg by mouth TWICE daily, with or without food. (For creatinine clearance (CrCl) 15-30 mL/min)

Practical Issues For Practical Issues For DietitiansDietitians
Metabolic Effects of Metabolic Effects of Atypical Atypical
AntipsychoticsAntipsychotics
87
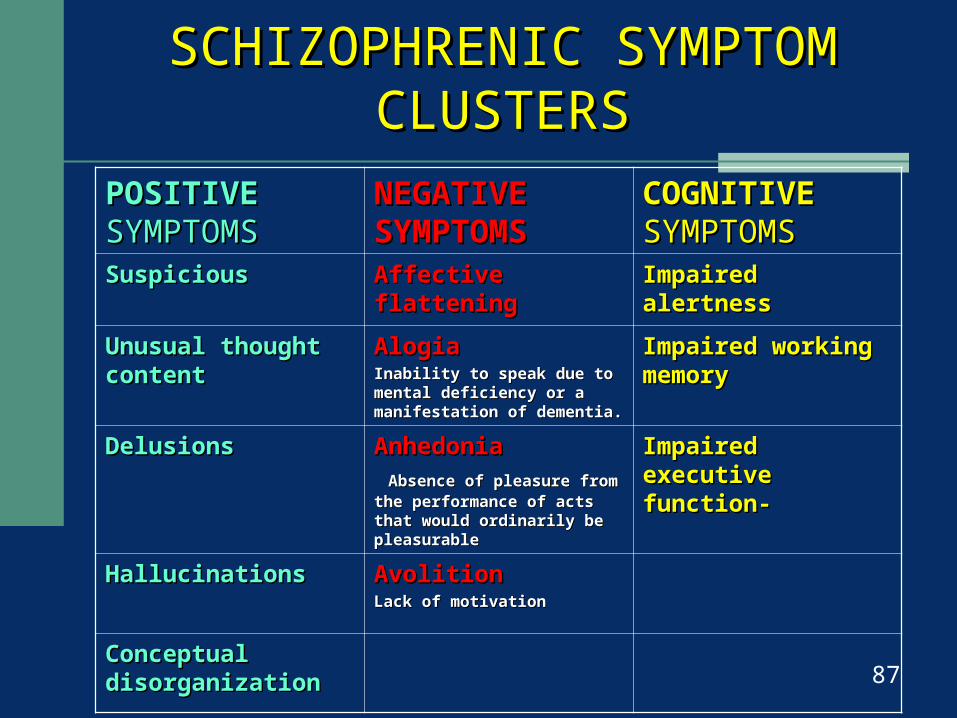
SCHIZOPHRENIC SYMPTOM SCHIZOPHRENIC SYMPTOM CLUSTERSCLUSTERS
POSITIVEPOSITIVE SYMPTOMSSYMPTOMS
NEGATIVE NEGATIVE SYMPTOMSSYMPTOMS
COGNITIVECOGNITIVE SYMPTOMSSYMPTOMS
SuspiciousSuspicious Affective flatteningAffective flattening Impaired alertnessImpaired alertness
Unusual thought Unusual thought contentcontent
AlogiaAlogiaInability to speak due to mental Inability to speak due to mental deficiency or a manifestation of deficiency or a manifestation of dementia.dementia.
Impaired working Impaired working memorymemory
DelusionsDelusions AnhedoniaAnhedonia Absence of pleasure from the Absence of pleasure from the performance of acts that would performance of acts that would ordinarily be pleasurableordinarily be pleasurable
Impaired executive Impaired executive function-function-
HallucinationsHallucinations Avolition Avolition Lack of motivationLack of motivation
Conceptual Conceptual disorganizationdisorganization

88
ATYPICAL AntipsychoticsCOMMON SIDE EFFECTS
Movement disorders HypERprolactinemia Sleep disorders Weight gain/ obesity Diabetes Cardiovascular Dyslipidemia Extrapyramidal side effects Cognitive effects

89
Adapted from Diepiero J 6th Edition 2005. page 1221 RELATIVERELATIVE SIDE EFFECTS OF ATYPICAL SIDE EFFECTS OF ATYPICAL
ANTIPSYCHOTICSANTIPSYCHOTICS
Brand Generic ANTI-CHOLINERGIC
ORTHO-
STASIS
EPS
Abilify® Aripiprazole + + +Risperdal® Risperidone + ++ ++Geodon® Ziprasidone + + ++Zyprexa® Olanzapine ++ ++ ++Seroquel® Quetiapine + ++ +Clozaril® Clozapine ++++ ++++ ++ NEGLIGIBLE ++ MODERATE
+ LOW +++ MODERATE-HIGH ++++ HIGH

ADA CONSENSUS ON ANTIPSYCHOTIC ADA CONSENSUS ON ANTIPSYCHOTIC DRUGS, OBESITY AND DIABETES DRUGS, OBESITY AND DIABETES
Brand Generic WEIGHT GAIN
DIABETES RISK
DYSLIPIDEMIA
Clozaril® Clozapine +++ + +
Zyprexa® Olanzapine
+++ + +
Risperdal®
Risperidone
++ D D
Seroquel®
Quetiapine ++ D D
Abilify® **
Aripiprazole
+/- -- --
Geodon® **
Ziprasidone
+/- -- --[+] increased effect [D] discrepant results [─] no effect [ ** ] Newer Drugs w/ limited long term data
American Diabetes Assoc; American Psychiatric Assoc; American Assoc of Clinical Endocrinologists; North American Assoc for the
Study of Obesity. Diabetes Care. 2004; 27:596
91
Diabetes Secondary to Atypical Diabetes Secondary to Atypical AntipsychoticsAntipsychotics
Schizophrenia has been identified as a risk factor for diabetes Mellitus independent of medication.28
An increased prevalence of diabetes has been associated with bipolar disorder.29
End organ damage may begin 7 yrs before a diabetes Dx. 30

92
Diabetes Secondary to Atypical Diabetes Secondary to Atypical AntipsychoticsAntipsychotics
Use of antipsychotics may be associated with a higher risk of diabetes & glucose dysregulation 6.17
Symptoms include fatigue, wt loss, polyuria & polydipsia.
Risk factors may be difficult to interpret in patients.
Diabetes is a risk factor for cardiovascular disease, kidney disease, retinopathy and neuropathy.17,28

93
Weight Gain &ObesityWeight Gain &Obesity Individuals with Schizophrenia or bipolar D/O
are more at risk than the general population for weight gain & obesity. 23, 24
Antipsychotics have been associated with various degrees of weight gain. 17,25
Weight gain can decrease medication compliance. 17

Weight Gain &ObesityWeight Gain &ObesityAbdominal obesity waist circumference17
MEN > 102 cm (40 in)Women >88 cm (35 in)
Body Mass Index17,26
= BMI (kg/m2)
Overweight BMI =25-29
Obesity BMI> 30
Management StrategiesManagement Strategies
• Monitor weight, BMI wait circumference at baseline & at regular intervals
• Intervention recommended if BMI> 25&/or abdominal 1 BMI unit obesity, or if INCRESE of 1 BMI unit (except if underweight)

6. Lahaman AF et al: Working Group on Schizophrenia. American Psychiatric Association. Practice Guidelines for the treatment of patients with schizophrenia, 2nd edition. Am J Psychiatry 2004;161 (suppl-2):1-56
17. Marder SR, et al. Physical health monitoring of patients with schizophrenia. Am J Psychol. 2004;161(8):1334-49
28. Canadian Database Association .Screening & prevention.2003 Clinical Practice Guideline. Avail on the web: www.databasecalcpg2003/downloads/screenprevent.pdf
29. Alison DB et al. The distribution of body mass index among individuals with and without schizophrenia. J Clin Psychiatry 1999; 60 (4):215-220
30. Keck PE et al. Bipolar disorder, obesity & pharmacotherapy-associated weight gain. J Clin Psychiatry 2003:64(121) 1426-1435
31. Schwartz TL et al. Psychiatric medical induced obesity: treatment options. Obs. Rev. 2004:5(4);233-238
28. Canadian Database Association: Screening and Prevention. 2003 Clinical Practice Guidelines.
29. Reginold WT et.al. Increased prevalence of type 2 DM among psychiatric inpatients with Bipolar-1 affective and schizoaffective D/O independent of psychotropic drug use. J Affect Disord. 2002 70(1): 19-26
30. Lelter LA et.al. Diabetes Screening in Canada. DAIASCAN Study:Prevelence of undiagnosed diabetes and glucose intolerance in family physician offices. DIABETES CARE 2001 24(6) 1038-43
Selected References

96
Weight gain with AntipsychoticsWeight gain with AntipsychoticsGreatest gainOlanzapine (Zyprexa)
Clozapine (Clozaril)
Significant gainMost ( Older original TYPICAL Antipsychotics)
Moderate gainRisperidone (Risperdal)
Quetiapine (SeroQUEL)
Little or No gain
Aripiprazole (Abilify)
Ziprasidone (Geodon)
American Diabetes Association: American Psychiatric Association: American society of Clinical Endocrinologists: North American Association for the Study of Obesity. Diabetes Care 2004: 27: 596. Gangul R. J Clin Psychiatry: 1999; 60 (Suppl 21): 20-24.

Metabolic Complications of Atypical Antipsychotics: Metabolic Complications of Atypical Antipsychotics:
Results from the CATIE Study Results from the CATIE Study ** Reference value compared to baseline
OLANZAPINE
ZyprexaZyprexaQUETIAPINE
SeroquelSeroquel RESPERIDONE
RisperdalRisperdalZIPRASIDONE
Geodon Geodon CLOZAPINE
ClozarilClozaril **
ARIPIPRAZOLE
Abilify Abilify **
Weight Weight Change Change lbs/ Month
2 lbs 0.5 lbs
0.4 lbs
-0.3 -0.3 lbslbs
0.5 lbs ---
HbA1c (%) HbA1c (%) 0.4 0.04 0.07 0.1 0.1 ---
Blood Blood Glucose Glucose (mg/dl)(mg/dl)
13.7 7.57.5 6.66.6 2.9 13.2 0.9
Total Total CholesterolCholesterol (mg/dl)(mg/dl)
9.4 6.6 -1.3-1.3 -8.2-8.2 7.3 -0.7-0.7
Triglyceride Triglyceride
(mg/dl)(mg/dl) 40.5 21.2 -2.4 -16.5 52.6 0.6
The CATIE TRIAL (Clinical Antipsychotic Trials of Intervention Effectiveness) N Eng J Med 2005;353:1209-1223 ** Data for Clozapine & Aripiprazole are from Data for Clozapine & Aripiprazole are from separateseparate sources sources

Questions / Comments?Questions / Comments?