Embed Size (px)
Citation preview

a division of Managed Resources
Mastering the Audit Process
Presented byLynn Handy CCS-P CPC CPC-I COC LPN
Vice President of Coding amp Audit ServicesCodingAID a division of Managed Resources Inc
Agenda
Why do we perform Audits Types of Audits
o Internal Auditso External AuditsoAuditor Quality Audits (QA)
Defining the Audit Scope Sample Selection Methodology Scoring Methodology Coding Guidelines
Auditor Quality Reviews amp Productivity Standards Audit Reports
oProvider Audit Reportso Executive Summary Reports
Presenting the Audit Results Post Audit EducationHandling Audit Disputes Self Disclosures Refunds and
Corrected Billing
Why do we Perform Audits
To determine outliers before large payers find them in their claims software and request an internal audit be done
To protect against fraudulent claims and billing activity
To reveal whether there is variation from national averages due to inappropriate coding insufficient documentation or lost revenue
To help identify and correct problem areas before insurance or government payers challenge inappropriate coding
To help prevent governmental investigational auditors like recovery audit contractors (RACs) or zone program integrity contractors (ZPICs) from knocking at your door
To remedy undercoding bad unbundling habits and code overuse and to bill appropriately for documented procedures
To identify reimbursement deficiencies and opportunities for appropriate reimbursement
To stop the use of outdated or incorrect codes for procedures
To verify ICD-10-CM and electronic health record (EHR) meaningful use readiness and Risk Adjustment (HCC) reporting
Developing an Internal Audit amp Education Program
Office Inspector General Guidanceo OIG has developed a series of voluntary compliance program guidance documents
directed at various segments of the health care industry such as hospitals nursing homes third-party billers and durable medical equipment suppliers to encourage the development and use of internal controls to monitor adherence to applicable statutes regulations and program requirements
Components of an Effective Compliance Programndash bull Conducting internal monitoring and auditing ndash bull Implementing compliance and practice standards ndash bull Designating a compliance officer or contact ndash bull Conducting appropriate training and education ndash bull Responding appropriately to detected offenses and developing corrective action ndash bull Developing open lines of communication and ndash bull Enforcing disciplinary standards through well-publicized guidelines
Program Development Questions
Who will be auditedHow often will they be auditedWhat is the sample size to be auditedWhat is the sample selection methodologyWhat is the scoring methodologyWhat is the passing scoreWhat is the follow up when the providers fall below the passing
scoreWhat is the process for education and re-audit
What does the OIG recommend
Provider education A baseline audit 3 months after training Audit each provider annually Sample size of at least 5-10 records per provider (industry standard is
at least 10) Include all Federal payers in your sample selection If problems are identified perform follow up focused reviews Educate Educate Educate
OIG Potential Risk Areas
Coding and Billing Reasonable and necessary services Documentation Improper inducements kickbacks and self-referrals
These are not all inclusive but should be a starting point when developing your Compliance Program
Types of Audits
Types of Audits
Internal AuditsoPros
ndash Continuityndash Familiar with internal coding
guidelinesndash Familiar with the providersndash No outside cost
oConsndash Limited resourcesndash Limited expertise in specialty areasndash Employees may not be receptive to a
peer finding their errors
External AuditsoPros
ndash Qualityndash Expertise in specialty areasndash Outside perspectivendash Error findings may be received easier
from an outsider than a peerndash Objective
oConsndash Costndash Quality
Defining the Audit Objective
What is the objective of the auditoCompliance (baseline) audito Financial Audito Investigative Audit (High Risk or Known Issues)oWork Flow Audit
ndash Did the codes get transferred correctly to the claim formndash Staffing analysis (Productivity)
oRevenue Cycle Audit (Billing Audit)o Educational AuditoCoder Quality Audits (QA)
Defining the Audit Scope
Prospective (prebill)o Pros
ndash Errors are fixed before billedndash No refunds to the payersndash Education can be more immediate on
current serviceso Cons
ndash Requires extra effort and focus to completing the audits timely to prevent a negative impact on revenue
ndash May hold up the billing process because claims will be on hold
ndash Limited selection to what the provider is currently billing
ndash Potential to miss timely filing deadlines
Retrospective (postbill)o Pros
ndash Allows more breathing room for completion and workflow
ndash More comprehensive sample selection of all services by each provider
ndash Allows for retrospective review for a focused audit for a specific time period
o Consndash Errors need to be correctndash Corrected claims and possible refunds
will be requiredndash Education is on previous services (but
not always a negative thing)ndash Timely filing contraints when re-billing
for higher reimbursement
Defining the Audit Scope Date Range
o Most audits will look at either current services (prospective) or a recent look back of 3-4 months (retrospective)
Scheduleo Frequency of the audits Annually Quarterlyo Will all providers be audits at onceo Will their be a rolling schedule of audits over a period of timeo How will re-audits be done
Types of Services to includeo E amp M Services onlyo E amp M with office procedureso Will the audit include diagnostic serviceso Surgery onlyo Will ICD-10-CM be included
Sample Sizeo How many encounters per provider
ndash 10-20 is average for a baseline or annual reviewo Types of services provided by each provider can affect sample sizeo Budget can affect sample sizeo Resources can affect sample size
Sample Selection Methodology
Sample Selection Methodologies
Define your sample selection methodologyoRandom Selection
ndash Totally RandomoRandomly Selective Selection
ndash Random within a set of parameterso Focused Selection
ndash Specific to certain services or codesoRATSTATS
ndash Only when a statistically valid sample selection is required
Sample Selection Methodology
Data AnalysisoBell Curve Analysis
ndash Use Medicare Utilization DataoPrior audit results
ndash Make sure your capturing the previous issuesoHigh Risk Areas
ndash Specialtyndash Groupndash Previously Identified issues
oOIG Work PlanoRAC or ZPIC audit findings
Sample Selection Methodology
Sample selection reportsoUtilization reports
ndash Specified Date Range of Servicesndash Providerndash Patient IDndash DOSndash CPT ICD-10 and Modifiers
Sample selection can be done with only CPT but all the codes gives you a better picture ndash Include the payer if you want your sample to be specific to certain payersndash Include the site of service if you want the audit results to identify each site
o You will want this in excel so you can do lots of filtering and sorting
Sample Selection Methodology Turn your filters on Sort by
o Provider (unless you run a separate report for each provider)o CPT code
ndash If you did not do an bell curve analysis prior you can review the volume of each E amp M level here
ndash Determine what types of services (outpatient inpatient EM Surgery etc)ndash How many of each level of service (depends on the providers EM utilization patterns)
o Resort by Patientndash This will allow you to see all services performed for each DOSndash Helps to capture encounters that have both EM amp Procedures Preventive with EM etc
o Pay attention to the Modifiersndash Do you want to include resident documentation Look for GC or GEndash Do you want to include EM with procedure Look for 25
ndash ReportsSample Selectionxlsx
Scoring Methodology
Scoring Methodology
Establish an Accuracy Rateo The OIG recommends that physicians maintain an accuracy rate of 95
ndash Net Error Rate
o Is it realistic to establish a 95 accuracy rate for the providers
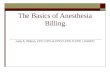
Scoring Examples (automated)
Total Visits Accurately Coded Under CodedBilled Over CodedBilled(+) Wrong Category (WC) Gross Financial Error ()
62 20 3226 4 645 13 2097 29 4677 4203
$123000 $14694 $37000 Provider RVUs User RVUs Points
0 129 5772 6200 (931)
EM Coding Total Sample Size 4 codes EM Detailed Review Total Sample Size 4 codes
Findings Count EM Level appears to be correct 0 0 EM Level appears to be over-coded 3 75 EM Level appears to be under-coded 1 25
CPTreg HCPCS II Coding Total Sample Size 0 codes
Findings Count Code(s) appear to be correct 0 0 Code(s) appear to be incorrect 0 0 Additional code(s) supported 0 0
Findings Count Over coded by 1 level 3 75 Over coded by 2 levels 0 0 Over coded by 3 levels 0 0 Over coded by 4 levels 0 0 Under coded by 1 level 1 25 Under coded by 2 levels 0 0 Under coded by 3 levels 0 0 Under coded by 4 levels 0 0 Number of category changes 0 0
ICD-CM Coding Total Sample Size 5 codes RVU Comparison
Findings Count Code(s) appear to be correct 3 60 Code(s) appear to be incorrect 1 20 Additional code(s) supported 1 20
wRVU Comp Original Audited Change Total wRVU Value 523 429 -18
Dollar Comparison Total Dollar Comp Original Audited Change Total Dollar Value $ 0 $ 0 -

Mastering the Audit Process
Presented byLynn Handy CCS-P CPC CPC-I COC LPN
Vice President of Coding amp Audit ServicesCodingAID a division of Managed Resources Inc
Agenda
Why do we perform Audits Types of Audits
o Internal Auditso External AuditsoAuditor Quality Audits (QA)
Defining the Audit Scope Sample Selection Methodology Scoring Methodology Coding Guidelines
Auditor Quality Reviews amp Productivity Standards Audit Reports
oProvider Audit Reportso Executive Summary Reports
Presenting the Audit Results Post Audit EducationHandling Audit Disputes Self Disclosures Refunds and
Corrected Billing
Why do we Perform Audits
To determine outliers before large payers find them in their claims software and request an internal audit be done
To protect against fraudulent claims and billing activity
To reveal whether there is variation from national averages due to inappropriate coding insufficient documentation or lost revenue
To help identify and correct problem areas before insurance or government payers challenge inappropriate coding
To help prevent governmental investigational auditors like recovery audit contractors (RACs) or zone program integrity contractors (ZPICs) from knocking at your door
To remedy undercoding bad unbundling habits and code overuse and to bill appropriately for documented procedures
To identify reimbursement deficiencies and opportunities for appropriate reimbursement
To stop the use of outdated or incorrect codes for procedures
To verify ICD-10-CM and electronic health record (EHR) meaningful use readiness and Risk Adjustment (HCC) reporting
Developing an Internal Audit amp Education Program
Office Inspector General Guidanceo OIG has developed a series of voluntary compliance program guidance documents
directed at various segments of the health care industry such as hospitals nursing homes third-party billers and durable medical equipment suppliers to encourage the development and use of internal controls to monitor adherence to applicable statutes regulations and program requirements
Components of an Effective Compliance Programndash bull Conducting internal monitoring and auditing ndash bull Implementing compliance and practice standards ndash bull Designating a compliance officer or contact ndash bull Conducting appropriate training and education ndash bull Responding appropriately to detected offenses and developing corrective action ndash bull Developing open lines of communication and ndash bull Enforcing disciplinary standards through well-publicized guidelines
Program Development Questions
Who will be auditedHow often will they be auditedWhat is the sample size to be auditedWhat is the sample selection methodologyWhat is the scoring methodologyWhat is the passing scoreWhat is the follow up when the providers fall below the passing
scoreWhat is the process for education and re-audit
What does the OIG recommend
Provider education A baseline audit 3 months after training Audit each provider annually Sample size of at least 5-10 records per provider (industry standard is
at least 10) Include all Federal payers in your sample selection If problems are identified perform follow up focused reviews Educate Educate Educate
OIG Potential Risk Areas
Coding and Billing Reasonable and necessary services Documentation Improper inducements kickbacks and self-referrals
These are not all inclusive but should be a starting point when developing your Compliance Program
Types of Audits
Types of Audits
Internal AuditsoPros
ndash Continuityndash Familiar with internal coding
guidelinesndash Familiar with the providersndash No outside cost
oConsndash Limited resourcesndash Limited expertise in specialty areasndash Employees may not be receptive to a
peer finding their errors
External AuditsoPros
ndash Qualityndash Expertise in specialty areasndash Outside perspectivendash Error findings may be received easier
from an outsider than a peerndash Objective
oConsndash Costndash Quality
Defining the Audit Objective
What is the objective of the auditoCompliance (baseline) audito Financial Audito Investigative Audit (High Risk or Known Issues)oWork Flow Audit
ndash Did the codes get transferred correctly to the claim formndash Staffing analysis (Productivity)
oRevenue Cycle Audit (Billing Audit)o Educational AuditoCoder Quality Audits (QA)
Defining the Audit Scope
Prospective (prebill)o Pros
ndash Errors are fixed before billedndash No refunds to the payersndash Education can be more immediate on
current serviceso Cons
ndash Requires extra effort and focus to completing the audits timely to prevent a negative impact on revenue
ndash May hold up the billing process because claims will be on hold
ndash Limited selection to what the provider is currently billing
ndash Potential to miss timely filing deadlines
Retrospective (postbill)o Pros
ndash Allows more breathing room for completion and workflow
ndash More comprehensive sample selection of all services by each provider
ndash Allows for retrospective review for a focused audit for a specific time period
o Consndash Errors need to be correctndash Corrected claims and possible refunds
will be requiredndash Education is on previous services (but
not always a negative thing)ndash Timely filing contraints when re-billing
for higher reimbursement
Defining the Audit Scope Date Range
o Most audits will look at either current services (prospective) or a recent look back of 3-4 months (retrospective)
Scheduleo Frequency of the audits Annually Quarterlyo Will all providers be audits at onceo Will their be a rolling schedule of audits over a period of timeo How will re-audits be done
Types of Services to includeo E amp M Services onlyo E amp M with office procedureso Will the audit include diagnostic serviceso Surgery onlyo Will ICD-10-CM be included
Sample Sizeo How many encounters per provider
ndash 10-20 is average for a baseline or annual reviewo Types of services provided by each provider can affect sample sizeo Budget can affect sample sizeo Resources can affect sample size
Sample Selection Methodology
Sample Selection Methodologies
Define your sample selection methodologyoRandom Selection
ndash Totally RandomoRandomly Selective Selection
ndash Random within a set of parameterso Focused Selection
ndash Specific to certain services or codesoRATSTATS
ndash Only when a statistically valid sample selection is required
Sample Selection Methodology
Data AnalysisoBell Curve Analysis
ndash Use Medicare Utilization DataoPrior audit results
ndash Make sure your capturing the previous issuesoHigh Risk Areas
ndash Specialtyndash Groupndash Previously Identified issues
oOIG Work PlanoRAC or ZPIC audit findings
Sample Selection Methodology
Sample selection reportsoUtilization reports
ndash Specified Date Range of Servicesndash Providerndash Patient IDndash DOSndash CPT ICD-10 and Modifiers
Sample selection can be done with only CPT but all the codes gives you a better picture ndash Include the payer if you want your sample to be specific to certain payersndash Include the site of service if you want the audit results to identify each site
o You will want this in excel so you can do lots of filtering and sorting
Sample Selection Methodology Turn your filters on Sort by
o Provider (unless you run a separate report for each provider)o CPT code
ndash If you did not do an bell curve analysis prior you can review the volume of each E amp M level here
ndash Determine what types of services (outpatient inpatient EM Surgery etc)ndash How many of each level of service (depends on the providers EM utilization patterns)
o Resort by Patientndash This will allow you to see all services performed for each DOSndash Helps to capture encounters that have both EM amp Procedures Preventive with EM etc
o Pay attention to the Modifiersndash Do you want to include resident documentation Look for GC or GEndash Do you want to include EM with procedure Look for 25
ndash ReportsSample Selectionxlsx
Scoring Methodology
Scoring Methodology
Establish an Accuracy Rateo The OIG recommends that physicians maintain an accuracy rate of 95
ndash Net Error Rate
o Is it realistic to establish a 95 accuracy rate for the providers
Scoring Examples (automated)
Total Visits Accurately Coded Under CodedBilled Over CodedBilled(+) Wrong Category (WC) Gross Financial Error ()
62 20 3226 4 645 13 2097 29 4677 4203
$123000 $14694 $37000 Provider RVUs User RVUs Points
0 129 5772 6200 (931)
EM Coding Total Sample Size 4 codes EM Detailed Review Total Sample Size 4 codes
Findings Count EM Level appears to be correct 0 0 EM Level appears to be over-coded 3 75 EM Level appears to be under-coded 1 25
CPTreg HCPCS II Coding Total Sample Size 0 codes
Findings Count Code(s) appear to be correct 0 0 Code(s) appear to be incorrect 0 0 Additional code(s) supported 0 0
Findings Count Over coded by 1 level 3 75 Over coded by 2 levels 0 0 Over coded by 3 levels 0 0 Over coded by 4 levels 0 0 Under coded by 1 level 1 25 Under coded by 2 levels 0 0 Under coded by 3 levels 0 0 Under coded by 4 levels 0 0 Number of category changes 0 0
ICD-CM Coding Total Sample Size 5 codes RVU Comparison
Findings Count Code(s) appear to be correct 3 60 Code(s) appear to be incorrect 1 20 Additional code(s) supported 1 20
wRVU Comp Original Audited Change Total wRVU Value 523 429 -18
Dollar Comparison Total Dollar Comp Original Audited Change Total Dollar Value $ 0 $ 0 -

Agenda
Why do we perform Audits Types of Audits
o Internal Auditso External AuditsoAuditor Quality Audits (QA)
Defining the Audit Scope Sample Selection Methodology Scoring Methodology Coding Guidelines
Auditor Quality Reviews amp Productivity Standards Audit Reports
oProvider Audit Reportso Executive Summary Reports
Presenting the Audit Results Post Audit EducationHandling Audit Disputes Self Disclosures Refunds and
Corrected Billing
Why do we Perform Audits
To determine outliers before large payers find them in their claims software and request an internal audit be done
To protect against fraudulent claims and billing activity
To reveal whether there is variation from national averages due to inappropriate coding insufficient documentation or lost revenue
To help identify and correct problem areas before insurance or government payers challenge inappropriate coding
To help prevent governmental investigational auditors like recovery audit contractors (RACs) or zone program integrity contractors (ZPICs) from knocking at your door
To remedy undercoding bad unbundling habits and code overuse and to bill appropriately for documented procedures
To identify reimbursement deficiencies and opportunities for appropriate reimbursement
To stop the use of outdated or incorrect codes for procedures
To verify ICD-10-CM and electronic health record (EHR) meaningful use readiness and Risk Adjustment (HCC) reporting
Developing an Internal Audit amp Education Program
Office Inspector General Guidanceo OIG has developed a series of voluntary compliance program guidance documents
directed at various segments of the health care industry such as hospitals nursing homes third-party billers and durable medical equipment suppliers to encourage the development and use of internal controls to monitor adherence to applicable statutes regulations and program requirements
Components of an Effective Compliance Programndash bull Conducting internal monitoring and auditing ndash bull Implementing compliance and practice standards ndash bull Designating a compliance officer or contact ndash bull Conducting appropriate training and education ndash bull Responding appropriately to detected offenses and developing corrective action ndash bull Developing open lines of communication and ndash bull Enforcing disciplinary standards through well-publicized guidelines
Program Development Questions
Who will be auditedHow often will they be auditedWhat is the sample size to be auditedWhat is the sample selection methodologyWhat is the scoring methodologyWhat is the passing scoreWhat is the follow up when the providers fall below the passing
scoreWhat is the process for education and re-audit
What does the OIG recommend
Provider education A baseline audit 3 months after training Audit each provider annually Sample size of at least 5-10 records per provider (industry standard is
at least 10) Include all Federal payers in your sample selection If problems are identified perform follow up focused reviews Educate Educate Educate
OIG Potential Risk Areas
Coding and Billing Reasonable and necessary services Documentation Improper inducements kickbacks and self-referrals
These are not all inclusive but should be a starting point when developing your Compliance Program
Types of Audits
Types of Audits
Internal AuditsoPros
ndash Continuityndash Familiar with internal coding
guidelinesndash Familiar with the providersndash No outside cost
oConsndash Limited resourcesndash Limited expertise in specialty areasndash Employees may not be receptive to a
peer finding their errors
External AuditsoPros
ndash Qualityndash Expertise in specialty areasndash Outside perspectivendash Error findings may be received easier
from an outsider than a peerndash Objective
oConsndash Costndash Quality
Defining the Audit Objective
What is the objective of the auditoCompliance (baseline) audito Financial Audito Investigative Audit (High Risk or Known Issues)oWork Flow Audit
ndash Did the codes get transferred correctly to the claim formndash Staffing analysis (Productivity)
oRevenue Cycle Audit (Billing Audit)o Educational AuditoCoder Quality Audits (QA)
Defining the Audit Scope
Prospective (prebill)o Pros
ndash Errors are fixed before billedndash No refunds to the payersndash Education can be more immediate on
current serviceso Cons
ndash Requires extra effort and focus to completing the audits timely to prevent a negative impact on revenue
ndash May hold up the billing process because claims will be on hold
ndash Limited selection to what the provider is currently billing
ndash Potential to miss timely filing deadlines
Retrospective (postbill)o Pros
ndash Allows more breathing room for completion and workflow
ndash More comprehensive sample selection of all services by each provider
ndash Allows for retrospective review for a focused audit for a specific time period
o Consndash Errors need to be correctndash Corrected claims and possible refunds
will be requiredndash Education is on previous services (but
not always a negative thing)ndash Timely filing contraints when re-billing
for higher reimbursement
Defining the Audit Scope Date Range
o Most audits will look at either current services (prospective) or a recent look back of 3-4 months (retrospective)
Scheduleo Frequency of the audits Annually Quarterlyo Will all providers be audits at onceo Will their be a rolling schedule of audits over a period of timeo How will re-audits be done
Types of Services to includeo E amp M Services onlyo E amp M with office procedureso Will the audit include diagnostic serviceso Surgery onlyo Will ICD-10-CM be included
Sample Sizeo How many encounters per provider
ndash 10-20 is average for a baseline or annual reviewo Types of services provided by each provider can affect sample sizeo Budget can affect sample sizeo Resources can affect sample size
Sample Selection Methodology
Sample Selection Methodologies
Define your sample selection methodologyoRandom Selection
ndash Totally RandomoRandomly Selective Selection
ndash Random within a set of parameterso Focused Selection
ndash Specific to certain services or codesoRATSTATS
ndash Only when a statistically valid sample selection is required
Sample Selection Methodology
Data AnalysisoBell Curve Analysis
ndash Use Medicare Utilization DataoPrior audit results
ndash Make sure your capturing the previous issuesoHigh Risk Areas
ndash Specialtyndash Groupndash Previously Identified issues
oOIG Work PlanoRAC or ZPIC audit findings
Sample Selection Methodology
Sample selection reportsoUtilization reports
ndash Specified Date Range of Servicesndash Providerndash Patient IDndash DOSndash CPT ICD-10 and Modifiers
Sample selection can be done with only CPT but all the codes gives you a better picture ndash Include the payer if you want your sample to be specific to certain payersndash Include the site of service if you want the audit results to identify each site
o You will want this in excel so you can do lots of filtering and sorting
Sample Selection Methodology Turn your filters on Sort by
o Provider (unless you run a separate report for each provider)o CPT code
ndash If you did not do an bell curve analysis prior you can review the volume of each E amp M level here
ndash Determine what types of services (outpatient inpatient EM Surgery etc)ndash How many of each level of service (depends on the providers EM utilization patterns)
o Resort by Patientndash This will allow you to see all services performed for each DOSndash Helps to capture encounters that have both EM amp Procedures Preventive with EM etc
o Pay attention to the Modifiersndash Do you want to include resident documentation Look for GC or GEndash Do you want to include EM with procedure Look for 25
ndash ReportsSample Selectionxlsx
Scoring Methodology
Scoring Methodology
Establish an Accuracy Rateo The OIG recommends that physicians maintain an accuracy rate of 95
ndash Net Error Rate
o Is it realistic to establish a 95 accuracy rate for the providers
Scoring Examples (automated)
Total Visits Accurately Coded Under CodedBilled Over CodedBilled(+) Wrong Category (WC) Gross Financial Error ()
62 20 3226 4 645 13 2097 29 4677 4203
$123000 $14694 $37000 Provider RVUs User RVUs Points
0 129 5772 6200 (931)
EM Coding Total Sample Size 4 codes EM Detailed Review Total Sample Size 4 codes
Findings Count EM Level appears to be correct 0 0 EM Level appears to be over-coded 3 75 EM Level appears to be under-coded 1 25
CPTreg HCPCS II Coding Total Sample Size 0 codes
Findings Count Code(s) appear to be correct 0 0 Code(s) appear to be incorrect 0 0 Additional code(s) supported 0 0
Findings Count Over coded by 1 level 3 75 Over coded by 2 levels 0 0 Over coded by 3 levels 0 0 Over coded by 4 levels 0 0 Under coded by 1 level 1 25 Under coded by 2 levels 0 0 Under coded by 3 levels 0 0 Under coded by 4 levels 0 0 Number of category changes 0 0
ICD-CM Coding Total Sample Size 5 codes RVU Comparison
Findings Count Code(s) appear to be correct 3 60 Code(s) appear to be incorrect 1 20 Additional code(s) supported 1 20
wRVU Comp Original Audited Change Total wRVU Value 523 429 -18
Dollar Comparison Total Dollar Comp Original Audited Change Total Dollar Value $ 0 $ 0 -

Why do we Perform Audits
To determine outliers before large payers find them in their claims software and request an internal audit be done
To protect against fraudulent claims and billing activity
To reveal whether there is variation from national averages due to inappropriate coding insufficient documentation or lost revenue
To help identify and correct problem areas before insurance or government payers challenge inappropriate coding
To help prevent governmental investigational auditors like recovery audit contractors (RACs) or zone program integrity contractors (ZPICs) from knocking at your door
To remedy undercoding bad unbundling habits and code overuse and to bill appropriately for documented procedures
To identify reimbursement deficiencies and opportunities for appropriate reimbursement
To stop the use of outdated or incorrect codes for procedures
To verify ICD-10-CM and electronic health record (EHR) meaningful use readiness and Risk Adjustment (HCC) reporting
Developing an Internal Audit amp Education Program
Office Inspector General Guidanceo OIG has developed a series of voluntary compliance program guidance documents
directed at various segments of the health care industry such as hospitals nursing homes third-party billers and durable medical equipment suppliers to encourage the development and use of internal controls to monitor adherence to applicable statutes regulations and program requirements
Components of an Effective Compliance Programndash bull Conducting internal monitoring and auditing ndash bull Implementing compliance and practice standards ndash bull Designating a compliance officer or contact ndash bull Conducting appropriate training and education ndash bull Responding appropriately to detected offenses and developing corrective action ndash bull Developing open lines of communication and ndash bull Enforcing disciplinary standards through well-publicized guidelines
Program Development Questions
Who will be auditedHow often will they be auditedWhat is the sample size to be auditedWhat is the sample selection methodologyWhat is the scoring methodologyWhat is the passing scoreWhat is the follow up when the providers fall below the passing
scoreWhat is the process for education and re-audit
What does the OIG recommend
Provider education A baseline audit 3 months after training Audit each provider annually Sample size of at least 5-10 records per provider (industry standard is
at least 10) Include all Federal payers in your sample selection If problems are identified perform follow up focused reviews Educate Educate Educate
OIG Potential Risk Areas
Coding and Billing Reasonable and necessary services Documentation Improper inducements kickbacks and self-referrals
These are not all inclusive but should be a starting point when developing your Compliance Program
Types of Audits
Types of Audits
Internal AuditsoPros
ndash Continuityndash Familiar with internal coding
guidelinesndash Familiar with the providersndash No outside cost
oConsndash Limited resourcesndash Limited expertise in specialty areasndash Employees may not be receptive to a
peer finding their errors
External AuditsoPros
ndash Qualityndash Expertise in specialty areasndash Outside perspectivendash Error findings may be received easier
from an outsider than a peerndash Objective
oConsndash Costndash Quality
Defining the Audit Objective
What is the objective of the auditoCompliance (baseline) audito Financial Audito Investigative Audit (High Risk or Known Issues)oWork Flow Audit
ndash Did the codes get transferred correctly to the claim formndash Staffing analysis (Productivity)
oRevenue Cycle Audit (Billing Audit)o Educational AuditoCoder Quality Audits (QA)
Defining the Audit Scope
Prospective (prebill)o Pros
ndash Errors are fixed before billedndash No refunds to the payersndash Education can be more immediate on
current serviceso Cons
ndash Requires extra effort and focus to completing the audits timely to prevent a negative impact on revenue
ndash May hold up the billing process because claims will be on hold
ndash Limited selection to what the provider is currently billing
ndash Potential to miss timely filing deadlines
Retrospective (postbill)o Pros
ndash Allows more breathing room for completion and workflow
ndash More comprehensive sample selection of all services by each provider
ndash Allows for retrospective review for a focused audit for a specific time period
o Consndash Errors need to be correctndash Corrected claims and possible refunds
will be requiredndash Education is on previous services (but
not always a negative thing)ndash Timely filing contraints when re-billing
for higher reimbursement
Defining the Audit Scope Date Range
o Most audits will look at either current services (prospective) or a recent look back of 3-4 months (retrospective)
Scheduleo Frequency of the audits Annually Quarterlyo Will all providers be audits at onceo Will their be a rolling schedule of audits over a period of timeo How will re-audits be done
Types of Services to includeo E amp M Services onlyo E amp M with office procedureso Will the audit include diagnostic serviceso Surgery onlyo Will ICD-10-CM be included
Sample Sizeo How many encounters per provider
ndash 10-20 is average for a baseline or annual reviewo Types of services provided by each provider can affect sample sizeo Budget can affect sample sizeo Resources can affect sample size
Sample Selection Methodology
Sample Selection Methodologies
Define your sample selection methodologyoRandom Selection
ndash Totally RandomoRandomly Selective Selection
ndash Random within a set of parameterso Focused Selection
ndash Specific to certain services or codesoRATSTATS
ndash Only when a statistically valid sample selection is required
Sample Selection Methodology
Data AnalysisoBell Curve Analysis
ndash Use Medicare Utilization DataoPrior audit results
ndash Make sure your capturing the previous issuesoHigh Risk Areas
ndash Specialtyndash Groupndash Previously Identified issues
oOIG Work PlanoRAC or ZPIC audit findings
Sample Selection Methodology
Sample selection reportsoUtilization reports
ndash Specified Date Range of Servicesndash Providerndash Patient IDndash DOSndash CPT ICD-10 and Modifiers
Sample selection can be done with only CPT but all the codes gives you a better picture ndash Include the payer if you want your sample to be specific to certain payersndash Include the site of service if you want the audit results to identify each site
o You will want this in excel so you can do lots of filtering and sorting
Sample Selection Methodology Turn your filters on Sort by
o Provider (unless you run a separate report for each provider)o CPT code
ndash If you did not do an bell curve analysis prior you can review the volume of each E amp M level here
ndash Determine what types of services (outpatient inpatient EM Surgery etc)ndash How many of each level of service (depends on the providers EM utilization patterns)
o Resort by Patientndash This will allow you to see all services performed for each DOSndash Helps to capture encounters that have both EM amp Procedures Preventive with EM etc
o Pay attention to the Modifiersndash Do you want to include resident documentation Look for GC or GEndash Do you want to include EM with procedure Look for 25
ndash ReportsSample Selectionxlsx
Scoring Methodology
Scoring Methodology
Establish an Accuracy Rateo The OIG recommends that physicians maintain an accuracy rate of 95
ndash Net Error Rate
o Is it realistic to establish a 95 accuracy rate for the providers
Scoring Examples (automated)
Total Visits Accurately Coded Under CodedBilled Over CodedBilled(+) Wrong Category (WC) Gross Financial Error ()
62 20 3226 4 645 13 2097 29 4677 4203
$123000 $14694 $37000 Provider RVUs User RVUs Points
0 129 5772 6200 (931)
EM Coding Total Sample Size 4 codes EM Detailed Review Total Sample Size 4 codes
Findings Count EM Level appears to be correct 0 0 EM Level appears to be over-coded 3 75 EM Level appears to be under-coded 1 25
CPTreg HCPCS II Coding Total Sample Size 0 codes
Findings Count Code(s) appear to be correct 0 0 Code(s) appear to be incorrect 0 0 Additional code(s) supported 0 0
Findings Count Over coded by 1 level 3 75 Over coded by 2 levels 0 0 Over coded by 3 levels 0 0 Over coded by 4 levels 0 0 Under coded by 1 level 1 25 Under coded by 2 levels 0 0 Under coded by 3 levels 0 0 Under coded by 4 levels 0 0 Number of category changes 0 0
ICD-CM Coding Total Sample Size 5 codes RVU Comparison
Findings Count Code(s) appear to be correct 3 60 Code(s) appear to be incorrect 1 20 Additional code(s) supported 1 20
wRVU Comp Original Audited Change Total wRVU Value 523 429 -18
Dollar Comparison Total Dollar Comp Original Audited Change Total Dollar Value $ 0 $ 0 -

Developing an Internal Audit amp Education Program
Office Inspector General Guidanceo OIG has developed a series of voluntary compliance program guidance documents
directed at various segments of the health care industry such as hospitals nursing homes third-party billers and durable medical equipment suppliers to encourage the development and use of internal controls to monitor adherence to applicable statutes regulations and program requirements
Components of an Effective Compliance Programndash bull Conducting internal monitoring and auditing ndash bull Implementing compliance and practice standards ndash bull Designating a compliance officer or contact ndash bull Conducting appropriate training and education ndash bull Responding appropriately to detected offenses and developing corrective action ndash bull Developing open lines of communication and ndash bull Enforcing disciplinary standards through well-publicized guidelines
Program Development Questions
Who will be auditedHow often will they be auditedWhat is the sample size to be auditedWhat is the sample selection methodologyWhat is the scoring methodologyWhat is the passing scoreWhat is the follow up when the providers fall below the passing
scoreWhat is the process for education and re-audit
What does the OIG recommend
Provider education A baseline audit 3 months after training Audit each provider annually Sample size of at least 5-10 records per provider (industry standard is
at least 10) Include all Federal payers in your sample selection If problems are identified perform follow up focused reviews Educate Educate Educate
OIG Potential Risk Areas
Coding and Billing Reasonable and necessary services Documentation Improper inducements kickbacks and self-referrals
These are not all inclusive but should be a starting point when developing your Compliance Program
Types of Audits
Types of Audits
Internal AuditsoPros
ndash Continuityndash Familiar with internal coding
guidelinesndash Familiar with the providersndash No outside cost
oConsndash Limited resourcesndash Limited expertise in specialty areasndash Employees may not be receptive to a
peer finding their errors
External AuditsoPros
ndash Qualityndash Expertise in specialty areasndash Outside perspectivendash Error findings may be received easier
from an outsider than a peerndash Objective
oConsndash Costndash Quality
Defining the Audit Objective
What is the objective of the auditoCompliance (baseline) audito Financial Audito Investigative Audit (High Risk or Known Issues)oWork Flow Audit
ndash Did the codes get transferred correctly to the claim formndash Staffing analysis (Productivity)
oRevenue Cycle Audit (Billing Audit)o Educational AuditoCoder Quality Audits (QA)
Defining the Audit Scope
Prospective (prebill)o Pros
ndash Errors are fixed before billedndash No refunds to the payersndash Education can be more immediate on
current serviceso Cons
ndash Requires extra effort and focus to completing the audits timely to prevent a negative impact on revenue
ndash May hold up the billing process because claims will be on hold
ndash Limited selection to what the provider is currently billing
ndash Potential to miss timely filing deadlines
Retrospective (postbill)o Pros
ndash Allows more breathing room for completion and workflow
ndash More comprehensive sample selection of all services by each provider
ndash Allows for retrospective review for a focused audit for a specific time period
o Consndash Errors need to be correctndash Corrected claims and possible refunds
will be requiredndash Education is on previous services (but
not always a negative thing)ndash Timely filing contraints when re-billing
for higher reimbursement
Defining the Audit Scope Date Range
o Most audits will look at either current services (prospective) or a recent look back of 3-4 months (retrospective)
Scheduleo Frequency of the audits Annually Quarterlyo Will all providers be audits at onceo Will their be a rolling schedule of audits over a period of timeo How will re-audits be done
Types of Services to includeo E amp M Services onlyo E amp M with office procedureso Will the audit include diagnostic serviceso Surgery onlyo Will ICD-10-CM be included
Sample Sizeo How many encounters per provider
ndash 10-20 is average for a baseline or annual reviewo Types of services provided by each provider can affect sample sizeo Budget can affect sample sizeo Resources can affect sample size
Sample Selection Methodology
Sample Selection Methodologies
Define your sample selection methodologyoRandom Selection
ndash Totally RandomoRandomly Selective Selection
ndash Random within a set of parameterso Focused Selection
ndash Specific to certain services or codesoRATSTATS
ndash Only when a statistically valid sample selection is required
Sample Selection Methodology
Data AnalysisoBell Curve Analysis
ndash Use Medicare Utilization DataoPrior audit results
ndash Make sure your capturing the previous issuesoHigh Risk Areas
ndash Specialtyndash Groupndash Previously Identified issues
oOIG Work PlanoRAC or ZPIC audit findings
Sample Selection Methodology
Sample selection reportsoUtilization reports
ndash Specified Date Range of Servicesndash Providerndash Patient IDndash DOSndash CPT ICD-10 and Modifiers
Sample selection can be done with only CPT but all the codes gives you a better picture ndash Include the payer if you want your sample to be specific to certain payersndash Include the site of service if you want the audit results to identify each site
o You will want this in excel so you can do lots of filtering and sorting
Sample Selection Methodology Turn your filters on Sort by
o Provider (unless you run a separate report for each provider)o CPT code
ndash If you did not do an bell curve analysis prior you can review the volume of each E amp M level here
ndash Determine what types of services (outpatient inpatient EM Surgery etc)ndash How many of each level of service (depends on the providers EM utilization patterns)
o Resort by Patientndash This will allow you to see all services performed for each DOSndash Helps to capture encounters that have both EM amp Procedures Preventive with EM etc
o Pay attention to the Modifiersndash Do you want to include resident documentation Look for GC or GEndash Do you want to include EM with procedure Look for 25
ndash ReportsSample Selectionxlsx
Scoring Methodology
Scoring Methodology
Establish an Accuracy Rateo The OIG recommends that physicians maintain an accuracy rate of 95
ndash Net Error Rate
o Is it realistic to establish a 95 accuracy rate for the providers
Scoring Examples (automated)
Total Visits Accurately Coded Under CodedBilled Over CodedBilled(+) Wrong Category (WC) Gross Financial Error ()
62 20 3226 4 645 13 2097 29 4677 4203
$123000 $14694 $37000 Provider RVUs User RVUs Points
0 129 5772 6200 (931)
EM Coding Total Sample Size 4 codes EM Detailed Review Total Sample Size 4 codes
Findings Count EM Level appears to be correct 0 0 EM Level appears to be over-coded 3 75 EM Level appears to be under-coded 1 25
CPTreg HCPCS II Coding Total Sample Size 0 codes
Findings Count Code(s) appear to be correct 0 0 Code(s) appear to be incorrect 0 0 Additional code(s) supported 0 0
Findings Count Over coded by 1 level 3 75 Over coded by 2 levels 0 0 Over coded by 3 levels 0 0 Over coded by 4 levels 0 0 Under coded by 1 level 1 25 Under coded by 2 levels 0 0 Under coded by 3 levels 0 0 Under coded by 4 levels 0 0 Number of category changes 0 0
ICD-CM Coding Total Sample Size 5 codes RVU Comparison
Findings Count Code(s) appear to be correct 3 60 Code(s) appear to be incorrect 1 20 Additional code(s) supported 1 20
wRVU Comp Original Audited Change Total wRVU Value 523 429 -18
Dollar Comparison Total Dollar Comp Original Audited Change Total Dollar Value $ 0 $ 0 -

Program Development Questions
Who will be auditedHow often will they be auditedWhat is the sample size to be auditedWhat is the sample selection methodologyWhat is the scoring methodologyWhat is the passing scoreWhat is the follow up when the providers fall below the passing
scoreWhat is the process for education and re-audit
What does the OIG recommend
Provider education A baseline audit 3 months after training Audit each provider annually Sample size of at least 5-10 records per provider (industry standard is
at least 10) Include all Federal payers in your sample selection If problems are identified perform follow up focused reviews Educate Educate Educate
OIG Potential Risk Areas
Coding and Billing Reasonable and necessary services Documentation Improper inducements kickbacks and self-referrals
These are not all inclusive but should be a starting point when developing your Compliance Program
Types of Audits
Types of Audits
Internal AuditsoPros
ndash Continuityndash Familiar with internal coding
guidelinesndash Familiar with the providersndash No outside cost
oConsndash Limited resourcesndash Limited expertise in specialty areasndash Employees may not be receptive to a
peer finding their errors
External AuditsoPros
ndash Qualityndash Expertise in specialty areasndash Outside perspectivendash Error findings may be received easier
from an outsider than a peerndash Objective
oConsndash Costndash Quality
Defining the Audit Objective
What is the objective of the auditoCompliance (baseline) audito Financial Audito Investigative Audit (High Risk or Known Issues)oWork Flow Audit
ndash Did the codes get transferred correctly to the claim formndash Staffing analysis (Productivity)
oRevenue Cycle Audit (Billing Audit)o Educational AuditoCoder Quality Audits (QA)
Defining the Audit Scope
Prospective (prebill)o Pros
ndash Errors are fixed before billedndash No refunds to the payersndash Education can be more immediate on
current serviceso Cons
ndash Requires extra effort and focus to completing the audits timely to prevent a negative impact on revenue
ndash May hold up the billing process because claims will be on hold
ndash Limited selection to what the provider is currently billing
ndash Potential to miss timely filing deadlines
Retrospective (postbill)o Pros
ndash Allows more breathing room for completion and workflow
ndash More comprehensive sample selection of all services by each provider
ndash Allows for retrospective review for a focused audit for a specific time period
o Consndash Errors need to be correctndash Corrected claims and possible refunds
will be requiredndash Education is on previous services (but
not always a negative thing)ndash Timely filing contraints when re-billing
for higher reimbursement
Defining the Audit Scope Date Range
o Most audits will look at either current services (prospective) or a recent look back of 3-4 months (retrospective)
Scheduleo Frequency of the audits Annually Quarterlyo Will all providers be audits at onceo Will their be a rolling schedule of audits over a period of timeo How will re-audits be done
Types of Services to includeo E amp M Services onlyo E amp M with office procedureso Will the audit include diagnostic serviceso Surgery onlyo Will ICD-10-CM be included
Sample Sizeo How many encounters per provider
ndash 10-20 is average for a baseline or annual reviewo Types of services provided by each provider can affect sample sizeo Budget can affect sample sizeo Resources can affect sample size
Sample Selection Methodology
Sample Selection Methodologies
Define your sample selection methodologyoRandom Selection
ndash Totally RandomoRandomly Selective Selection
ndash Random within a set of parameterso Focused Selection
ndash Specific to certain services or codesoRATSTATS
ndash Only when a statistically valid sample selection is required
Sample Selection Methodology
Data AnalysisoBell Curve Analysis
ndash Use Medicare Utilization DataoPrior audit results
ndash Make sure your capturing the previous issuesoHigh Risk Areas
ndash Specialtyndash Groupndash Previously Identified issues
oOIG Work PlanoRAC or ZPIC audit findings
Sample Selection Methodology
Sample selection reportsoUtilization reports
ndash Specified Date Range of Servicesndash Providerndash Patient IDndash DOSndash CPT ICD-10 and Modifiers
Sample selection can be done with only CPT but all the codes gives you a better picture ndash Include the payer if you want your sample to be specific to certain payersndash Include the site of service if you want the audit results to identify each site
o You will want this in excel so you can do lots of filtering and sorting
Sample Selection Methodology Turn your filters on Sort by
o Provider (unless you run a separate report for each provider)o CPT code
ndash If you did not do an bell curve analysis prior you can review the volume of each E amp M level here
ndash Determine what types of services (outpatient inpatient EM Surgery etc)ndash How many of each level of service (depends on the providers EM utilization patterns)
o Resort by Patientndash This will allow you to see all services performed for each DOSndash Helps to capture encounters that have both EM amp Procedures Preventive with EM etc
o Pay attention to the Modifiersndash Do you want to include resident documentation Look for GC or GEndash Do you want to include EM with procedure Look for 25
ndash ReportsSample Selectionxlsx
Scoring Methodology
Scoring Methodology
Establish an Accuracy Rateo The OIG recommends that physicians maintain an accuracy rate of 95
ndash Net Error Rate
o Is it realistic to establish a 95 accuracy rate for the providers
Scoring Examples (automated)
Total Visits Accurately Coded Under CodedBilled Over CodedBilled(+) Wrong Category (WC) Gross Financial Error ()
62 20 3226 4 645 13 2097 29 4677 4203
$123000 $14694 $37000 Provider RVUs User RVUs Points
0 129 5772 6200 (931)
EM Coding Total Sample Size 4 codes EM Detailed Review Total Sample Size 4 codes
Findings Count EM Level appears to be correct 0 0 EM Level appears to be over-coded 3 75 EM Level appears to be under-coded 1 25
CPTreg HCPCS II Coding Total Sample Size 0 codes
Findings Count Code(s) appear to be correct 0 0 Code(s) appear to be incorrect 0 0 Additional code(s) supported 0 0
Findings Count Over coded by 1 level 3 75 Over coded by 2 levels 0 0 Over coded by 3 levels 0 0 Over coded by 4 levels 0 0 Under coded by 1 level 1 25 Under coded by 2 levels 0 0 Under coded by 3 levels 0 0 Under coded by 4 levels 0 0 Number of category changes 0 0
ICD-CM Coding Total Sample Size 5 codes RVU Comparison
Findings Count Code(s) appear to be correct 3 60 Code(s) appear to be incorrect 1 20 Additional code(s) supported 1 20
wRVU Comp Original Audited Change Total wRVU Value 523 429 -18
Dollar Comparison Total Dollar Comp Original Audited Change Total Dollar Value $ 0 $ 0 -

What does the OIG recommend
Provider education A baseline audit 3 months after training Audit each provider annually Sample size of at least 5-10 records per provider (industry standard is
at least 10) Include all Federal payers in your sample selection If problems are identified perform follow up focused reviews Educate Educate Educate
OIG Potential Risk Areas
Coding and Billing Reasonable and necessary services Documentation Improper inducements kickbacks and self-referrals
These are not all inclusive but should be a starting point when developing your Compliance Program
Types of Audits
Types of Audits
Internal AuditsoPros
ndash Continuityndash Familiar with internal coding
guidelinesndash Familiar with the providersndash No outside cost
oConsndash Limited resourcesndash Limited expertise in specialty areasndash Employees may not be receptive to a
peer finding their errors
External AuditsoPros
ndash Qualityndash Expertise in specialty areasndash Outside perspectivendash Error findings may be received easier
from an outsider than a peerndash Objective
oConsndash Costndash Quality
Defining the Audit Objective
What is the objective of the auditoCompliance (baseline) audito Financial Audito Investigative Audit (High Risk or Known Issues)oWork Flow Audit
ndash Did the codes get transferred correctly to the claim formndash Staffing analysis (Productivity)
oRevenue Cycle Audit (Billing Audit)o Educational AuditoCoder Quality Audits (QA)
Defining the Audit Scope
Prospective (prebill)o Pros
ndash Errors are fixed before billedndash No refunds to the payersndash Education can be more immediate on
current serviceso Cons
ndash Requires extra effort and focus to completing the audits timely to prevent a negative impact on revenue
ndash May hold up the billing process because claims will be on hold
ndash Limited selection to what the provider is currently billing
ndash Potential to miss timely filing deadlines
Retrospective (postbill)o Pros
ndash Allows more breathing room for completion and workflow
ndash More comprehensive sample selection of all services by each provider
ndash Allows for retrospective review for a focused audit for a specific time period
o Consndash Errors need to be correctndash Corrected claims and possible refunds
will be requiredndash Education is on previous services (but
not always a negative thing)ndash Timely filing contraints when re-billing
for higher reimbursement
Defining the Audit Scope Date Range
o Most audits will look at either current services (prospective) or a recent look back of 3-4 months (retrospective)
Scheduleo Frequency of the audits Annually Quarterlyo Will all providers be audits at onceo Will their be a rolling schedule of audits over a period of timeo How will re-audits be done
Types of Services to includeo E amp M Services onlyo E amp M with office procedureso Will the audit include diagnostic serviceso Surgery onlyo Will ICD-10-CM be included
Sample Sizeo How many encounters per provider
ndash 10-20 is average for a baseline or annual reviewo Types of services provided by each provider can affect sample sizeo Budget can affect sample sizeo Resources can affect sample size
Sample Selection Methodology
Sample Selection Methodologies
Define your sample selection methodologyoRandom Selection
ndash Totally RandomoRandomly Selective Selection
ndash Random within a set of parameterso Focused Selection
ndash Specific to certain services or codesoRATSTATS
ndash Only when a statistically valid sample selection is required
Sample Selection Methodology
Data AnalysisoBell Curve Analysis
ndash Use Medicare Utilization DataoPrior audit results
ndash Make sure your capturing the previous issuesoHigh Risk Areas
ndash Specialtyndash Groupndash Previously Identified issues
oOIG Work PlanoRAC or ZPIC audit findings
Sample Selection Methodology
Sample selection reportsoUtilization reports
ndash Specified Date Range of Servicesndash Providerndash Patient IDndash DOSndash CPT ICD-10 and Modifiers
Sample selection can be done with only CPT but all the codes gives you a better picture ndash Include the payer if you want your sample to be specific to certain payersndash Include the site of service if you want the audit results to identify each site
o You will want this in excel so you can do lots of filtering and sorting
Sample Selection Methodology Turn your filters on Sort by
o Provider (unless you run a separate report for each provider)o CPT code
ndash If you did not do an bell curve analysis prior you can review the volume of each E amp M level here
ndash Determine what types of services (outpatient inpatient EM Surgery etc)ndash How many of each level of service (depends on the providers EM utilization patterns)
o Resort by Patientndash This will allow you to see all services performed for each DOSndash Helps to capture encounters that have both EM amp Procedures Preventive with EM etc
o Pay attention to the Modifiersndash Do you want to include resident documentation Look for GC or GEndash Do you want to include EM with procedure Look for 25
ndash ReportsSample Selectionxlsx
Scoring Methodology
Scoring Methodology
Establish an Accuracy Rateo The OIG recommends that physicians maintain an accuracy rate of 95
ndash Net Error Rate
o Is it realistic to establish a 95 accuracy rate for the providers
Scoring Examples (automated)
Total Visits Accurately Coded Under CodedBilled Over CodedBilled(+) Wrong Category (WC) Gross Financial Error ()
62 20 3226 4 645 13 2097 29 4677 4203
$123000 $14694 $37000 Provider RVUs User RVUs Points
0 129 5772 6200 (931)
EM Coding Total Sample Size 4 codes EM Detailed Review Total Sample Size 4 codes
Findings Count EM Level appears to be correct 0 0 EM Level appears to be over-coded 3 75 EM Level appears to be under-coded 1 25
CPTreg HCPCS II Coding Total Sample Size 0 codes
Findings Count Code(s) appear to be correct 0 0 Code(s) appear to be incorrect 0 0 Additional code(s) supported 0 0
Findings Count Over coded by 1 level 3 75 Over coded by 2 levels 0 0 Over coded by 3 levels 0 0 Over coded by 4 levels 0 0 Under coded by 1 level 1 25 Under coded by 2 levels 0 0 Under coded by 3 levels 0 0 Under coded by 4 levels 0 0 Number of category changes 0 0
ICD-CM Coding Total Sample Size 5 codes RVU Comparison
Findings Count Code(s) appear to be correct 3 60 Code(s) appear to be incorrect 1 20 Additional code(s) supported 1 20
wRVU Comp Original Audited Change Total wRVU Value 523 429 -18
Dollar Comparison Total Dollar Comp Original Audited Change Total Dollar Value $ 0 $ 0 -

OIG Potential Risk Areas
Coding and Billing Reasonable and necessary services Documentation Improper inducements kickbacks and self-referrals
These are not all inclusive but should be a starting point when developing your Compliance Program
Types of Audits
Types of Audits
Internal AuditsoPros
ndash Continuityndash Familiar with internal coding
guidelinesndash Familiar with the providersndash No outside cost
oConsndash Limited resourcesndash Limited expertise in specialty areasndash Employees may not be receptive to a
peer finding their errors
External AuditsoPros
ndash Qualityndash Expertise in specialty areasndash Outside perspectivendash Error findings may be received easier
from an outsider than a peerndash Objective
oConsndash Costndash Quality
Defining the Audit Objective
What is the objective of the auditoCompliance (baseline) audito Financial Audito Investigative Audit (High Risk or Known Issues)oWork Flow Audit
ndash Did the codes get transferred correctly to the claim formndash Staffing analysis (Productivity)
oRevenue Cycle Audit (Billing Audit)o Educational AuditoCoder Quality Audits (QA)
Defining the Audit Scope
Prospective (prebill)o Pros
ndash Errors are fixed before billedndash No refunds to the payersndash Education can be more immediate on
current serviceso Cons
ndash Requires extra effort and focus to completing the audits timely to prevent a negative impact on revenue
ndash May hold up the billing process because claims will be on hold
ndash Limited selection to what the provider is currently billing
ndash Potential to miss timely filing deadlines
Retrospective (postbill)o Pros
ndash Allows more breathing room for completion and workflow
ndash More comprehensive sample selection of all services by each provider
ndash Allows for retrospective review for a focused audit for a specific time period
o Consndash Errors need to be correctndash Corrected claims and possible refunds
will be requiredndash Education is on previous services (but
not always a negative thing)ndash Timely filing contraints when re-billing
for higher reimbursement
Defining the Audit Scope Date Range
o Most audits will look at either current services (prospective) or a recent look back of 3-4 months (retrospective)
Scheduleo Frequency of the audits Annually Quarterlyo Will all providers be audits at onceo Will their be a rolling schedule of audits over a period of timeo How will re-audits be done
Types of Services to includeo E amp M Services onlyo E amp M with office procedureso Will the audit include diagnostic serviceso Surgery onlyo Will ICD-10-CM be included
Sample Sizeo How many encounters per provider
ndash 10-20 is average for a baseline or annual reviewo Types of services provided by each provider can affect sample sizeo Budget can affect sample sizeo Resources can affect sample size
Sample Selection Methodology
Sample Selection Methodologies
Define your sample selection methodologyoRandom Selection
ndash Totally RandomoRandomly Selective Selection
ndash Random within a set of parameterso Focused Selection
ndash Specific to certain services or codesoRATSTATS
ndash Only when a statistically valid sample selection is required
Sample Selection Methodology
Data AnalysisoBell Curve Analysis
ndash Use Medicare Utilization DataoPrior audit results
ndash Make sure your capturing the previous issuesoHigh Risk Areas
ndash Specialtyndash Groupndash Previously Identified issues
oOIG Work PlanoRAC or ZPIC audit findings
Sample Selection Methodology
Sample selection reportsoUtilization reports
ndash Specified Date Range of Servicesndash Providerndash Patient IDndash DOSndash CPT ICD-10 and Modifiers
Sample selection can be done with only CPT but all the codes gives you a better picture ndash Include the payer if you want your sample to be specific to certain payersndash Include the site of service if you want the audit results to identify each site
o You will want this in excel so you can do lots of filtering and sorting
Sample Selection Methodology Turn your filters on Sort by
o Provider (unless you run a separate report for each provider)o CPT code
ndash If you did not do an bell curve analysis prior you can review the volume of each E amp M level here
ndash Determine what types of services (outpatient inpatient EM Surgery etc)ndash How many of each level of service (depends on the providers EM utilization patterns)
o Resort by Patientndash This will allow you to see all services performed for each DOSndash Helps to capture encounters that have both EM amp Procedures Preventive with EM etc
o Pay attention to the Modifiersndash Do you want to include resident documentation Look for GC or GEndash Do you want to include EM with procedure Look for 25
ndash ReportsSample Selectionxlsx
Scoring Methodology
Scoring Methodology
Establish an Accuracy Rateo The OIG recommends that physicians maintain an accuracy rate of 95
ndash Net Error Rate
o Is it realistic to establish a 95 accuracy rate for the providers
Scoring Examples (automated)
Total Visits Accurately Coded Under CodedBilled Over CodedBilled(+) Wrong Category (WC) Gross Financial Error ()
62 20 3226 4 645 13 2097 29 4677 4203
$123000 $14694 $37000 Provider RVUs User RVUs Points
0 129 5772 6200 (931)
EM Coding Total Sample Size 4 codes EM Detailed Review Total Sample Size 4 codes
Findings Count EM Level appears to be correct 0 0 EM Level appears to be over-coded 3 75 EM Level appears to be under-coded 1 25
CPTreg HCPCS II Coding Total Sample Size 0 codes
Findings Count Code(s) appear to be correct 0 0 Code(s) appear to be incorrect 0 0 Additional code(s) supported 0 0
Findings Count Over coded by 1 level 3 75 Over coded by 2 levels 0 0 Over coded by 3 levels 0 0 Over coded by 4 levels 0 0 Under coded by 1 level 1 25 Under coded by 2 levels 0 0 Under coded by 3 levels 0 0 Under coded by 4 levels 0 0 Number of category changes 0 0
ICD-CM Coding Total Sample Size 5 codes RVU Comparison
Findings Count Code(s) appear to be correct 3 60 Code(s) appear to be incorrect 1 20 Additional code(s) supported 1 20
wRVU Comp Original Audited Change Total wRVU Value 523 429 -18
Dollar Comparison Total Dollar Comp Original Audited Change Total Dollar Value $ 0 $ 0 -

Types of Audits
Types of Audits
Internal AuditsoPros
ndash Continuityndash Familiar with internal coding
guidelinesndash Familiar with the providersndash No outside cost
oConsndash Limited resourcesndash Limited expertise in specialty areasndash Employees may not be receptive to a
peer finding their errors
External AuditsoPros
ndash Qualityndash Expertise in specialty areasndash Outside perspectivendash Error findings may be received easier
from an outsider than a peerndash Objective
oConsndash Costndash Quality
Defining the Audit Objective
What is the objective of the auditoCompliance (baseline) audito Financial Audito Investigative Audit (High Risk or Known Issues)oWork Flow Audit
ndash Did the codes get transferred correctly to the claim formndash Staffing analysis (Productivity)
oRevenue Cycle Audit (Billing Audit)o Educational AuditoCoder Quality Audits (QA)
Defining the Audit Scope
Prospective (prebill)o Pros
ndash Errors are fixed before billedndash No refunds to the payersndash Education can be more immediate on
current serviceso Cons
ndash Requires extra effort and focus to completing the audits timely to prevent a negative impact on revenue
ndash May hold up the billing process because claims will be on hold
ndash Limited selection to what the provider is currently billing
ndash Potential to miss timely filing deadlines
Retrospective (postbill)o Pros
ndash Allows more breathing room for completion and workflow
ndash More comprehensive sample selection of all services by each provider
ndash Allows for retrospective review for a focused audit for a specific time period
o Consndash Errors need to be correctndash Corrected claims and possible refunds
will be requiredndash Education is on previous services (but
not always a negative thing)ndash Timely filing contraints when re-billing
for higher reimbursement
Defining the Audit Scope Date Range
o Most audits will look at either current services (prospective) or a recent look back of 3-4 months (retrospective)
Scheduleo Frequency of the audits Annually Quarterlyo Will all providers be audits at onceo Will their be a rolling schedule of audits over a period of timeo How will re-audits be done
Types of Services to includeo E amp M Services onlyo E amp M with office procedureso Will the audit include diagnostic serviceso Surgery onlyo Will ICD-10-CM be included
Sample Sizeo How many encounters per provider
ndash 10-20 is average for a baseline or annual reviewo Types of services provided by each provider can affect sample sizeo Budget can affect sample sizeo Resources can affect sample size
Sample Selection Methodology
Sample Selection Methodologies
Define your sample selection methodologyoRandom Selection
ndash Totally RandomoRandomly Selective Selection
ndash Random within a set of parameterso Focused Selection
ndash Specific to certain services or codesoRATSTATS
ndash Only when a statistically valid sample selection is required
Sample Selection Methodology
Data AnalysisoBell Curve Analysis
ndash Use Medicare Utilization DataoPrior audit results
ndash Make sure your capturing the previous issuesoHigh Risk Areas
ndash Specialtyndash Groupndash Previously Identified issues
oOIG Work PlanoRAC or ZPIC audit findings
Sample Selection Methodology
Sample selection reportsoUtilization reports
ndash Specified Date Range of Servicesndash Providerndash Patient IDndash DOSndash CPT ICD-10 and Modifiers
Sample selection can be done with only CPT but all the codes gives you a better picture ndash Include the payer if you want your sample to be specific to certain payersndash Include the site of service if you want the audit results to identify each site
o You will want this in excel so you can do lots of filtering and sorting
Sample Selection Methodology Turn your filters on Sort by
o Provider (unless you run a separate report for each provider)o CPT code
ndash If you did not do an bell curve analysis prior you can review the volume of each E amp M level here
ndash Determine what types of services (outpatient inpatient EM Surgery etc)ndash How many of each level of service (depends on the providers EM utilization patterns)
o Resort by Patientndash This will allow you to see all services performed for each DOSndash Helps to capture encounters that have both EM amp Procedures Preventive with EM etc
o Pay attention to the Modifiersndash Do you want to include resident documentation Look for GC or GEndash Do you want to include EM with procedure Look for 25
ndash ReportsSample Selectionxlsx
Scoring Methodology
Scoring Methodology
Establish an Accuracy Rateo The OIG recommends that physicians maintain an accuracy rate of 95
ndash Net Error Rate
o Is it realistic to establish a 95 accuracy rate for the providers
Scoring Examples (automated)
Total Visits Accurately Coded Under CodedBilled Over CodedBilled(+) Wrong Category (WC) Gross Financial Error ()
62 20 3226 4 645 13 2097 29 4677 4203
$123000 $14694 $37000 Provider RVUs User RVUs Points
0 129 5772 6200 (931)
EM Coding Total Sample Size 4 codes EM Detailed Review Total Sample Size 4 codes
Findings Count EM Level appears to be correct 0 0 EM Level appears to be over-coded 3 75 EM Level appears to be under-coded 1 25
CPTreg HCPCS II Coding Total Sample Size 0 codes
Findings Count Code(s) appear to be correct 0 0 Code(s) appear to be incorrect 0 0 Additional code(s) supported 0 0
Findings Count Over coded by 1 level 3 75 Over coded by 2 levels 0 0 Over coded by 3 levels 0 0 Over coded by 4 levels 0 0 Under coded by 1 level 1 25 Under coded by 2 levels 0 0 Under coded by 3 levels 0 0 Under coded by 4 levels 0 0 Number of category changes 0 0
ICD-CM Coding Total Sample Size 5 codes RVU Comparison
Findings Count Code(s) appear to be correct 3 60 Code(s) appear to be incorrect 1 20 Additional code(s) supported 1 20
wRVU Comp Original Audited Change Total wRVU Value 523 429 -18
Dollar Comparison Total Dollar Comp Original Audited Change Total Dollar Value $ 0 $ 0 -

Types of Audits
Internal AuditsoPros
ndash Continuityndash Familiar with internal coding
guidelinesndash Familiar with the providersndash No outside cost
oConsndash Limited resourcesndash Limited expertise in specialty areasndash Employees may not be receptive to a
peer finding their errors
External AuditsoPros
ndash Qualityndash Expertise in specialty areasndash Outside perspectivendash Error findings may be received easier
from an outsider than a peerndash Objective
oConsndash Costndash Quality
Defining the Audit Objective
What is the objective of the auditoCompliance (baseline) audito Financial Audito Investigative Audit (High Risk or Known Issues)oWork Flow Audit
ndash Did the codes get transferred correctly to the claim formndash Staffing analysis (Productivity)
oRevenue Cycle Audit (Billing Audit)o Educational AuditoCoder Quality Audits (QA)
Defining the Audit Scope
Prospective (prebill)o Pros
ndash Errors are fixed before billedndash No refunds to the payersndash Education can be more immediate on
current serviceso Cons
ndash Requires extra effort and focus to completing the audits timely to prevent a negative impact on revenue
ndash May hold up the billing process because claims will be on hold
ndash Limited selection to what the provider is currently billing
ndash Potential to miss timely filing deadlines
Retrospective (postbill)o Pros
ndash Allows more breathing room for completion and workflow
ndash More comprehensive sample selection of all services by each provider
ndash Allows for retrospective review for a focused audit for a specific time period
o Consndash Errors need to be correctndash Corrected claims and possible refunds
will be requiredndash Education is on previous services (but
not always a negative thing)ndash Timely filing contraints when re-billing
for higher reimbursement
Defining the Audit Scope Date Range
o Most audits will look at either current services (prospective) or a recent look back of 3-4 months (retrospective)
Scheduleo Frequency of the audits Annually Quarterlyo Will all providers be audits at onceo Will their be a rolling schedule of audits over a period of timeo How will re-audits be done
Types of Services to includeo E amp M Services onlyo E amp M with office procedureso Will the audit include diagnostic serviceso Surgery onlyo Will ICD-10-CM be included
Sample Sizeo How many encounters per provider
ndash 10-20 is average for a baseline or annual reviewo Types of services provided by each provider can affect sample sizeo Budget can affect sample sizeo Resources can affect sample size
Sample Selection Methodology
Sample Selection Methodologies
Define your sample selection methodologyoRandom Selection
ndash Totally RandomoRandomly Selective Selection
ndash Random within a set of parameterso Focused Selection
ndash Specific to certain services or codesoRATSTATS
ndash Only when a statistically valid sample selection is required
Sample Selection Methodology
Data AnalysisoBell Curve Analysis
ndash Use Medicare Utilization DataoPrior audit results
ndash Make sure your capturing the previous issuesoHigh Risk Areas
ndash Specialtyndash Groupndash Previously Identified issues
oOIG Work PlanoRAC or ZPIC audit findings
Sample Selection Methodology
Sample selection reportsoUtilization reports
ndash Specified Date Range of Servicesndash Providerndash Patient IDndash DOSndash CPT ICD-10 and Modifiers
Sample selection can be done with only CPT but all the codes gives you a better picture ndash Include the payer if you want your sample to be specific to certain payersndash Include the site of service if you want the audit results to identify each site
o You will want this in excel so you can do lots of filtering and sorting
Sample Selection Methodology Turn your filters on Sort by
o Provider (unless you run a separate report for each provider)o CPT code
ndash If you did not do an bell curve analysis prior you can review the volume of each E amp M level here
ndash Determine what types of services (outpatient inpatient EM Surgery etc)ndash How many of each level of service (depends on the providers EM utilization patterns)
o Resort by Patientndash This will allow you to see all services performed for each DOSndash Helps to capture encounters that have both EM amp Procedures Preventive with EM etc
o Pay attention to the Modifiersndash Do you want to include resident documentation Look for GC or GEndash Do you want to include EM with procedure Look for 25
ndash ReportsSample Selectionxlsx
Scoring Methodology
Scoring Methodology
Establish an Accuracy Rateo The OIG recommends that physicians maintain an accuracy rate of 95
ndash Net Error Rate
o Is it realistic to establish a 95 accuracy rate for the providers
Scoring Examples (automated)
Total Visits Accurately Coded Under CodedBilled Over CodedBilled(+) Wrong Category (WC) Gross Financial Error ()
62 20 3226 4 645 13 2097 29 4677 4203
$123000 $14694 $37000 Provider RVUs User RVUs Points
0 129 5772 6200 (931)
EM Coding Total Sample Size 4 codes EM Detailed Review Total Sample Size 4 codes
Findings Count EM Level appears to be correct 0 0 EM Level appears to be over-coded 3 75 EM Level appears to be under-coded 1 25
CPTreg HCPCS II Coding Total Sample Size 0 codes
Findings Count Code(s) appear to be correct 0 0 Code(s) appear to be incorrect 0 0 Additional code(s) supported 0 0
Findings Count Over coded by 1 level 3 75 Over coded by 2 levels 0 0 Over coded by 3 levels 0 0 Over coded by 4 levels 0 0 Under coded by 1 level 1 25 Under coded by 2 levels 0 0 Under coded by 3 levels 0 0 Under coded by 4 levels 0 0 Number of category changes 0 0
ICD-CM Coding Total Sample Size 5 codes RVU Comparison
Findings Count Code(s) appear to be correct 3 60 Code(s) appear to be incorrect 1 20 Additional code(s) supported 1 20
wRVU Comp Original Audited Change Total wRVU Value 523 429 -18
Dollar Comparison Total Dollar Comp Original Audited Change Total Dollar Value $ 0 $ 0 -

Defining the Audit Objective
What is the objective of the auditoCompliance (baseline) audito Financial Audito Investigative Audit (High Risk or Known Issues)oWork Flow Audit
ndash Did the codes get transferred correctly to the claim formndash Staffing analysis (Productivity)
oRevenue Cycle Audit (Billing Audit)o Educational AuditoCoder Quality Audits (QA)
Defining the Audit Scope
Prospective (prebill)o Pros
ndash Errors are fixed before billedndash No refunds to the payersndash Education can be more immediate on
current serviceso Cons
ndash Requires extra effort and focus to completing the audits timely to prevent a negative impact on revenue
ndash May hold up the billing process because claims will be on hold
ndash Limited selection to what the provider is currently billing
ndash Potential to miss timely filing deadlines
Retrospective (postbill)o Pros
ndash Allows more breathing room for completion and workflow
ndash More comprehensive sample selection of all services by each provider
ndash Allows for retrospective review for a focused audit for a specific time period
o Consndash Errors need to be correctndash Corrected claims and possible refunds
will be requiredndash Education is on previous services (but
not always a negative thing)ndash Timely filing contraints when re-billing
for higher reimbursement
Defining the Audit Scope Date Range
o Most audits will look at either current services (prospective) or a recent look back of 3-4 months (retrospective)
Scheduleo Frequency of the audits Annually Quarterlyo Will all providers be audits at onceo Will their be a rolling schedule of audits over a period of timeo How will re-audits be done
Types of Services to includeo E amp M Services onlyo E amp M with office procedureso Will the audit include diagnostic serviceso Surgery onlyo Will ICD-10-CM be included
Sample Sizeo How many encounters per provider
ndash 10-20 is average for a baseline or annual reviewo Types of services provided by each provider can affect sample sizeo Budget can affect sample sizeo Resources can affect sample size
Sample Selection Methodology
Sample Selection Methodologies
Define your sample selection methodologyoRandom Selection
ndash Totally RandomoRandomly Selective Selection
ndash Random within a set of parameterso Focused Selection
ndash Specific to certain services or codesoRATSTATS
ndash Only when a statistically valid sample selection is required
Sample Selection Methodology
Data AnalysisoBell Curve Analysis
ndash Use Medicare Utilization DataoPrior audit results
ndash Make sure your capturing the previous issuesoHigh Risk Areas
ndash Specialtyndash Groupndash Previously Identified issues
oOIG Work PlanoRAC or ZPIC audit findings
Sample Selection Methodology
Sample selection reportsoUtilization reports
ndash Specified Date Range of Servicesndash Providerndash Patient IDndash DOSndash CPT ICD-10 and Modifiers
Sample selection can be done with only CPT but all the codes gives you a better picture ndash Include the payer if you want your sample to be specific to certain payersndash Include the site of service if you want the audit results to identify each site
o You will want this in excel so you can do lots of filtering and sorting
Sample Selection Methodology Turn your filters on Sort by
o Provider (unless you run a separate report for each provider)o CPT code
ndash If you did not do an bell curve analysis prior you can review the volume of each E amp M level here
ndash Determine what types of services (outpatient inpatient EM Surgery etc)ndash How many of each level of service (depends on the providers EM utilization patterns)
o Resort by Patientndash This will allow you to see all services performed for each DOSndash Helps to capture encounters that have both EM amp Procedures Preventive with EM etc
o Pay attention to the Modifiersndash Do you want to include resident documentation Look for GC or GEndash Do you want to include EM with procedure Look for 25
ndash ReportsSample Selectionxlsx
Scoring Methodology
Scoring Methodology
Establish an Accuracy Rateo The OIG recommends that physicians maintain an accuracy rate of 95
ndash Net Error Rate
o Is it realistic to establish a 95 accuracy rate for the providers
Scoring Examples (automated)
Total Visits Accurately Coded Under CodedBilled Over CodedBilled(+) Wrong Category (WC) Gross Financial Error ()
62 20 3226 4 645 13 2097 29 4677 4203
$123000 $14694 $37000 Provider RVUs User RVUs Points
0 129 5772 6200 (931)
EM Coding Total Sample Size 4 codes EM Detailed Review Total Sample Size 4 codes
Findings Count EM Level appears to be correct 0 0 EM Level appears to be over-coded 3 75 EM Level appears to be under-coded 1 25
CPTreg HCPCS II Coding Total Sample Size 0 codes
Findings Count Code(s) appear to be correct 0 0 Code(s) appear to be incorrect 0 0 Additional code(s) supported 0 0
Findings Count Over coded by 1 level 3 75 Over coded by 2 levels 0 0 Over coded by 3 levels 0 0 Over coded by 4 levels 0 0 Under coded by 1 level 1 25 Under coded by 2 levels 0 0 Under coded by 3 levels 0 0 Under coded by 4 levels 0 0 Number of category changes 0 0
ICD-CM Coding Total Sample Size 5 codes RVU Comparison
Findings Count Code(s) appear to be correct 3 60 Code(s) appear to be incorrect 1 20 Additional code(s) supported 1 20
wRVU Comp Original Audited Change Total wRVU Value 523 429 -18
Dollar Comparison Total Dollar Comp Original Audited Change Total Dollar Value $ 0 $ 0 -

Defining the Audit Scope
Prospective (prebill)o Pros
ndash Errors are fixed before billedndash No refunds to the payersndash Education can be more immediate on
current serviceso Cons
ndash Requires extra effort and focus to completing the audits timely to prevent a negative impact on revenue
ndash May hold up the billing process because claims will be on hold
ndash Limited selection to what the provider is currently billing
ndash Potential to miss timely filing deadlines
Retrospective (postbill)o Pros
ndash Allows more breathing room for completion and workflow
ndash More comprehensive sample selection of all services by each provider
ndash Allows for retrospective review for a focused audit for a specific time period
o Consndash Errors need to be correctndash Corrected claims and possible refunds
will be requiredndash Education is on previous services (but
not always a negative thing)ndash Timely filing contraints when re-billing
for higher reimbursement
Defining the Audit Scope Date Range
o Most audits will look at either current services (prospective) or a recent look back of 3-4 months (retrospective)
Scheduleo Frequency of the audits Annually Quarterlyo Will all providers be audits at onceo Will their be a rolling schedule of audits over a period of timeo How will re-audits be done
Types of Services to includeo E amp M Services onlyo E amp M with office procedureso Will the audit include diagnostic serviceso Surgery onlyo Will ICD-10-CM be included
Sample Sizeo How many encounters per provider
ndash 10-20 is average for a baseline or annual reviewo Types of services provided by each provider can affect sample sizeo Budget can affect sample sizeo Resources can affect sample size
Sample Selection Methodology
Sample Selection Methodologies
Define your sample selection methodologyoRandom Selection
ndash Totally RandomoRandomly Selective Selection
ndash Random within a set of parameterso Focused Selection
ndash Specific to certain services or codesoRATSTATS
ndash Only when a statistically valid sample selection is required
Sample Selection Methodology
Data AnalysisoBell Curve Analysis
ndash Use Medicare Utilization DataoPrior audit results
ndash Make sure your capturing the previous issuesoHigh Risk Areas
ndash Specialtyndash Groupndash Previously Identified issues
oOIG Work PlanoRAC or ZPIC audit findings
Sample Selection Methodology
Sample selection reportsoUtilization reports
ndash Specified Date Range of Servicesndash Providerndash Patient IDndash DOSndash CPT ICD-10 and Modifiers
Sample selection can be done with only CPT but all the codes gives you a better picture ndash Include the payer if you want your sample to be specific to certain payersndash Include the site of service if you want the audit results to identify each site
o You will want this in excel so you can do lots of filtering and sorting
Sample Selection Methodology Turn your filters on Sort by
o Provider (unless you run a separate report for each provider)o CPT code
ndash If you did not do an bell curve analysis prior you can review the volume of each E amp M level here
ndash Determine what types of services (outpatient inpatient EM Surgery etc)ndash How many of each level of service (depends on the providers EM utilization patterns)
o Resort by Patientndash This will allow you to see all services performed for each DOSndash Helps to capture encounters that have both EM amp Procedures Preventive with EM etc
o Pay attention to the Modifiersndash Do you want to include resident documentation Look for GC or GEndash Do you want to include EM with procedure Look for 25
ndash ReportsSample Selectionxlsx
Scoring Methodology
Scoring Methodology
Establish an Accuracy Rateo The OIG recommends that physicians maintain an accuracy rate of 95
ndash Net Error Rate
o Is it realistic to establish a 95 accuracy rate for the providers
Scoring Examples (automated)
Total Visits Accurately Coded Under CodedBilled Over CodedBilled(+) Wrong Category (WC) Gross Financial Error ()
62 20 3226 4 645 13 2097 29 4677 4203
$123000 $14694 $37000 Provider RVUs User RVUs Points
0 129 5772 6200 (931)
EM Coding Total Sample Size 4 codes EM Detailed Review Total Sample Size 4 codes
Findings Count EM Level appears to be correct 0 0 EM Level appears to be over-coded 3 75 EM Level appears to be under-coded 1 25
CPTreg HCPCS II Coding Total Sample Size 0 codes
Findings Count Code(s) appear to be correct 0 0 Code(s) appear to be incorrect 0 0 Additional code(s) supported 0 0
Findings Count Over coded by 1 level 3 75 Over coded by 2 levels 0 0 Over coded by 3 levels 0 0 Over coded by 4 levels 0 0 Under coded by 1 level 1 25 Under coded by 2 levels 0 0 Under coded by 3 levels 0 0 Under coded by 4 levels 0 0 Number of category changes 0 0
ICD-CM Coding Total Sample Size 5 codes RVU Comparison
Findings Count Code(s) appear to be correct 3 60 Code(s) appear to be incorrect 1 20 Additional code(s) supported 1 20
wRVU Comp Original Audited Change Total wRVU Value 523 429 -18
Dollar Comparison Total Dollar Comp Original Audited Change Total Dollar Value $ 0 $ 0 -

Defining the Audit Scope Date Range
o Most audits will look at either current services (prospective) or a recent look back of 3-4 months (retrospective)
Scheduleo Frequency of the audits Annually Quarterlyo Will all providers be audits at onceo Will their be a rolling schedule of audits over a period of timeo How will re-audits be done
Types of Services to includeo E amp M Services onlyo E amp M with office procedureso Will the audit include diagnostic serviceso Surgery onlyo Will ICD-10-CM be included
Sample Sizeo How many encounters per provider
ndash 10-20 is average for a baseline or annual reviewo Types of services provided by each provider can affect sample sizeo Budget can affect sample sizeo Resources can affect sample size
Sample Selection Methodology
Sample Selection Methodologies
Define your sample selection methodologyoRandom Selection
ndash Totally RandomoRandomly Selective Selection
ndash Random within a set of parameterso Focused Selection
ndash Specific to certain services or codesoRATSTATS
ndash Only when a statistically valid sample selection is required
Sample Selection Methodology
Data AnalysisoBell Curve Analysis
ndash Use Medicare Utilization DataoPrior audit results
ndash Make sure your capturing the previous issuesoHigh Risk Areas
ndash Specialtyndash Groupndash Previously Identified issues
oOIG Work PlanoRAC or ZPIC audit findings
Sample Selection Methodology
Sample selection reportsoUtilization reports
ndash Specified Date Range of Servicesndash Providerndash Patient IDndash DOSndash CPT ICD-10 and Modifiers
Sample selection can be done with only CPT but all the codes gives you a better picture ndash Include the payer if you want your sample to be specific to certain payersndash Include the site of service if you want the audit results to identify each site
o You will want this in excel so you can do lots of filtering and sorting
Sample Selection Methodology Turn your filters on Sort by
o Provider (unless you run a separate report for each provider)o CPT code
ndash If you did not do an bell curve analysis prior you can review the volume of each E amp M level here
ndash Determine what types of services (outpatient inpatient EM Surgery etc)ndash How many of each level of service (depends on the providers EM utilization patterns)
o Resort by Patientndash This will allow you to see all services performed for each DOSndash Helps to capture encounters that have both EM amp Procedures Preventive with EM etc
o Pay attention to the Modifiersndash Do you want to include resident documentation Look for GC or GEndash Do you want to include EM with procedure Look for 25
ndash ReportsSample Selectionxlsx
Scoring Methodology
Scoring Methodology
Establish an Accuracy Rateo The OIG recommends that physicians maintain an accuracy rate of 95
ndash Net Error Rate
o Is it realistic to establish a 95 accuracy rate for the providers
Scoring Examples (automated)
Total Visits Accurately Coded Under CodedBilled Over CodedBilled(+) Wrong Category (WC) Gross Financial Error ()
62 20 3226 4 645 13 2097 29 4677 4203
$123000 $14694 $37000 Provider RVUs User RVUs Points
0 129 5772 6200 (931)
EM Coding Total Sample Size 4 codes EM Detailed Review Total Sample Size 4 codes
Findings Count EM Level appears to be correct 0 0 EM Level appears to be over-coded 3 75 EM Level appears to be under-coded 1 25
CPTreg HCPCS II Coding Total Sample Size 0 codes
Findings Count Code(s) appear to be correct 0 0 Code(s) appear to be incorrect 0 0 Additional code(s) supported 0 0
Findings Count Over coded by 1 level 3 75 Over coded by 2 levels 0 0 Over coded by 3 levels 0 0 Over coded by 4 levels 0 0 Under coded by 1 level 1 25 Under coded by 2 levels 0 0 Under coded by 3 levels 0 0 Under coded by 4 levels 0 0 Number of category changes 0 0
ICD-CM Coding Total Sample Size 5 codes RVU Comparison
Findings Count Code(s) appear to be correct 3 60 Code(s) appear to be incorrect 1 20 Additional code(s) supported 1 20
wRVU Comp Original Audited Change Total wRVU Value 523 429 -18
Dollar Comparison Total Dollar Comp Original Audited Change Total Dollar Value $ 0 $ 0 -

Sample Selection Methodology
Sample Selection Methodologies
Define your sample selection methodologyoRandom Selection
ndash Totally RandomoRandomly Selective Selection
ndash Random within a set of parameterso Focused Selection
ndash Specific to certain services or codesoRATSTATS
ndash Only when a statistically valid sample selection is required
Sample Selection Methodology
Data AnalysisoBell Curve Analysis
ndash Use Medicare Utilization DataoPrior audit results
ndash Make sure your capturing the previous issuesoHigh Risk Areas
ndash Specialtyndash Groupndash Previously Identified issues
oOIG Work PlanoRAC or ZPIC audit findings
Sample Selection Methodology
Sample selection reportsoUtilization reports
ndash Specified Date Range of Servicesndash Providerndash Patient IDndash DOSndash CPT ICD-10 and Modifiers
Sample selection can be done with only CPT but all the codes gives you a better picture ndash Include the payer if you want your sample to be specific to certain payersndash Include the site of service if you want the audit results to identify each site
o You will want this in excel so you can do lots of filtering and sorting
Sample Selection Methodology Turn your filters on Sort by
o Provider (unless you run a separate report for each provider)o CPT code
ndash If you did not do an bell curve analysis prior you can review the volume of each E amp M level here
ndash Determine what types of services (outpatient inpatient EM Surgery etc)ndash How many of each level of service (depends on the providers EM utilization patterns)
o Resort by Patientndash This will allow you to see all services performed for each DOSndash Helps to capture encounters that have both EM amp Procedures Preventive with EM etc
o Pay attention to the Modifiersndash Do you want to include resident documentation Look for GC or GEndash Do you want to include EM with procedure Look for 25
ndash ReportsSample Selectionxlsx
Scoring Methodology
Scoring Methodology
Establish an Accuracy Rateo The OIG recommends that physicians maintain an accuracy rate of 95
ndash Net Error Rate
o Is it realistic to establish a 95 accuracy rate for the providers
Scoring Examples (automated)
Total Visits Accurately Coded Under CodedBilled Over CodedBilled(+) Wrong Category (WC) Gross Financial Error ()
62 20 3226 4 645 13 2097 29 4677 4203
$123000 $14694 $37000 Provider RVUs User RVUs Points
0 129 5772 6200 (931)
EM Coding Total Sample Size 4 codes EM Detailed Review Total Sample Size 4 codes
Findings Count EM Level appears to be correct 0 0 EM Level appears to be over-coded 3 75 EM Level appears to be under-coded 1 25
CPTreg HCPCS II Coding Total Sample Size 0 codes
Findings Count Code(s) appear to be correct 0 0 Code(s) appear to be incorrect 0 0 Additional code(s) supported 0 0
Findings Count Over coded by 1 level 3 75 Over coded by 2 levels 0 0 Over coded by 3 levels 0 0 Over coded by 4 levels 0 0 Under coded by 1 level 1 25 Under coded by 2 levels 0 0 Under coded by 3 levels 0 0 Under coded by 4 levels 0 0 Number of category changes 0 0
ICD-CM Coding Total Sample Size 5 codes RVU Comparison
Findings Count Code(s) appear to be correct 3 60 Code(s) appear to be incorrect 1 20 Additional code(s) supported 1 20
wRVU Comp Original Audited Change Total wRVU Value 523 429 -18
Dollar Comparison Total Dollar Comp Original Audited Change Total Dollar Value $ 0 $ 0 -

Sample Selection Methodologies
Define your sample selection methodologyoRandom Selection
ndash Totally RandomoRandomly Selective Selection
ndash Random within a set of parameterso Focused Selection
ndash Specific to certain services or codesoRATSTATS
ndash Only when a statistically valid sample selection is required
Sample Selection Methodology
Data AnalysisoBell Curve Analysis
ndash Use Medicare Utilization DataoPrior audit results
ndash Make sure your capturing the previous issuesoHigh Risk Areas
ndash Specialtyndash Groupndash Previously Identified issues
oOIG Work PlanoRAC or ZPIC audit findings
Sample Selection Methodology
Sample selection reportsoUtilization reports
ndash Specified Date Range of Servicesndash Providerndash Patient IDndash DOSndash CPT ICD-10 and Modifiers
Sample selection can be done with only CPT but all the codes gives you a better picture ndash Include the payer if you want your sample to be specific to certain payersndash Include the site of service if you want the audit results to identify each site
o You will want this in excel so you can do lots of filtering and sorting
Sample Selection Methodology Turn your filters on Sort by
o Provider (unless you run a separate report for each provider)o CPT code
ndash If you did not do an bell curve analysis prior you can review the volume of each E amp M level here
ndash Determine what types of services (outpatient inpatient EM Surgery etc)ndash How many of each level of service (depends on the providers EM utilization patterns)
o Resort by Patientndash This will allow you to see all services performed for each DOSndash Helps to capture encounters that have both EM amp Procedures Preventive with EM etc
o Pay attention to the Modifiersndash Do you want to include resident documentation Look for GC or GEndash Do you want to include EM with procedure Look for 25
ndash ReportsSample Selectionxlsx
Scoring Methodology
Scoring Methodology
Establish an Accuracy Rateo The OIG recommends that physicians maintain an accuracy rate of 95
ndash Net Error Rate
o Is it realistic to establish a 95 accuracy rate for the providers
Scoring Examples (automated)
Total Visits Accurately Coded Under CodedBilled Over CodedBilled(+) Wrong Category (WC) Gross Financial Error ()
62 20 3226 4 645 13 2097 29 4677 4203
$123000 $14694 $37000 Provider RVUs User RVUs Points
0 129 5772 6200 (931)
EM Coding Total Sample Size 4 codes EM Detailed Review Total Sample Size 4 codes
Findings Count EM Level appears to be correct 0 0 EM Level appears to be over-coded 3 75 EM Level appears to be under-coded 1 25
CPTreg HCPCS II Coding Total Sample Size 0 codes
Findings Count Code(s) appear to be correct 0 0 Code(s) appear to be incorrect 0 0 Additional code(s) supported 0 0
Findings Count Over coded by 1 level 3 75 Over coded by 2 levels 0 0 Over coded by 3 levels 0 0 Over coded by 4 levels 0 0 Under coded by 1 level 1 25 Under coded by 2 levels 0 0 Under coded by 3 levels 0 0 Under coded by 4 levels 0 0 Number of category changes 0 0
ICD-CM Coding Total Sample Size 5 codes RVU Comparison
Findings Count Code(s) appear to be correct 3 60 Code(s) appear to be incorrect 1 20 Additional code(s) supported 1 20
wRVU Comp Original Audited Change Total wRVU Value 523 429 -18
Dollar Comparison Total Dollar Comp Original Audited Change Total Dollar Value $ 0 $ 0 -

Sample Selection Methodology
Data AnalysisoBell Curve Analysis
ndash Use Medicare Utilization DataoPrior audit results
ndash Make sure your capturing the previous issuesoHigh Risk Areas
ndash Specialtyndash Groupndash Previously Identified issues
oOIG Work PlanoRAC or ZPIC audit findings
Sample Selection Methodology
Sample selection reportsoUtilization reports
ndash Specified Date Range of Servicesndash Providerndash Patient IDndash DOSndash CPT ICD-10 and Modifiers
Sample selection can be done with only CPT but all the codes gives you a better picture ndash Include the payer if you want your sample to be specific to certain payersndash Include the site of service if you want the audit results to identify each site
o You will want this in excel so you can do lots of filtering and sorting
Sample Selection Methodology Turn your filters on Sort by
o Provider (unless you run a separate report for each provider)o CPT code
ndash If you did not do an bell curve analysis prior you can review the volume of each E amp M level here
ndash Determine what types of services (outpatient inpatient EM Surgery etc)ndash How many of each level of service (depends on the providers EM utilization patterns)
o Resort by Patientndash This will allow you to see all services performed for each DOSndash Helps to capture encounters that have both EM amp Procedures Preventive with EM etc
o Pay attention to the Modifiersndash Do you want to include resident documentation Look for GC or GEndash Do you want to include EM with procedure Look for 25
ndash ReportsSample Selectionxlsx
Scoring Methodology
Scoring Methodology
Establish an Accuracy Rateo The OIG recommends that physicians maintain an accuracy rate of 95
ndash Net Error Rate
o Is it realistic to establish a 95 accuracy rate for the providers
Scoring Examples (automated)
Total Visits Accurately Coded Under CodedBilled Over CodedBilled(+) Wrong Category (WC) Gross Financial Error ()
62 20 3226 4 645 13 2097 29 4677 4203
$123000 $14694 $37000 Provider RVUs User RVUs Points
0 129 5772 6200 (931)
EM Coding Total Sample Size 4 codes EM Detailed Review Total Sample Size 4 codes
Findings Count EM Level appears to be correct 0 0 EM Level appears to be over-coded 3 75 EM Level appears to be under-coded 1 25
CPTreg HCPCS II Coding Total Sample Size 0 codes
Findings Count Code(s) appear to be correct 0 0 Code(s) appear to be incorrect 0 0 Additional code(s) supported 0 0
Findings Count Over coded by 1 level 3 75 Over coded by 2 levels 0 0 Over coded by 3 levels 0 0 Over coded by 4 levels 0 0 Under coded by 1 level 1 25 Under coded by 2 levels 0 0 Under coded by 3 levels 0 0 Under coded by 4 levels 0 0 Number of category changes 0 0
ICD-CM Coding Total Sample Size 5 codes RVU Comparison
Findings Count Code(s) appear to be correct 3 60 Code(s) appear to be incorrect 1 20 Additional code(s) supported 1 20
wRVU Comp Original Audited Change Total wRVU Value 523 429 -18
Dollar Comparison Total Dollar Comp Original Audited Change Total Dollar Value $ 0 $ 0 -

Sample Selection Methodology
Sample selection reportsoUtilization reports
ndash Specified Date Range of Servicesndash Providerndash Patient IDndash DOSndash CPT ICD-10 and Modifiers
Sample selection can be done with only CPT but all the codes gives you a better picture ndash Include the payer if you want your sample to be specific to certain payersndash Include the site of service if you want the audit results to identify each site
o You will want this in excel so you can do lots of filtering and sorting
Sample Selection Methodology Turn your filters on Sort by
o Provider (unless you run a separate report for each provider)o CPT code
ndash If you did not do an bell curve analysis prior you can review the volume of each E amp M level here
ndash Determine what types of services (outpatient inpatient EM Surgery etc)ndash How many of each level of service (depends on the providers EM utilization patterns)
o Resort by Patientndash This will allow you to see all services performed for each DOSndash Helps to capture encounters that have both EM amp Procedures Preventive with EM etc
o Pay attention to the Modifiersndash Do you want to include resident documentation Look for GC or GEndash Do you want to include EM with procedure Look for 25
ndash ReportsSample Selectionxlsx
Scoring Methodology
Scoring Methodology
Establish an Accuracy Rateo The OIG recommends that physicians maintain an accuracy rate of 95
ndash Net Error Rate
o Is it realistic to establish a 95 accuracy rate for the providers
Scoring Examples (automated)
Total Visits Accurately Coded Under CodedBilled Over CodedBilled(+) Wrong Category (WC) Gross Financial Error ()
62 20 3226 4 645 13 2097 29 4677 4203
$123000 $14694 $37000 Provider RVUs User RVUs Points
0 129 5772 6200 (931)
EM Coding Total Sample Size 4 codes EM Detailed Review Total Sample Size 4 codes
Findings Count EM Level appears to be correct 0 0 EM Level appears to be over-coded 3 75 EM Level appears to be under-coded 1 25
CPTreg HCPCS II Coding Total Sample Size 0 codes
Findings Count Code(s) appear to be correct 0 0 Code(s) appear to be incorrect 0 0 Additional code(s) supported 0 0
Findings Count Over coded by 1 level 3 75 Over coded by 2 levels 0 0 Over coded by 3 levels 0 0 Over coded by 4 levels 0 0 Under coded by 1 level 1 25 Under coded by 2 levels 0 0 Under coded by 3 levels 0 0 Under coded by 4 levels 0 0 Number of category changes 0 0
ICD-CM Coding Total Sample Size 5 codes RVU Comparison
Findings Count Code(s) appear to be correct 3 60 Code(s) appear to be incorrect 1 20 Additional code(s) supported 1 20
wRVU Comp Original Audited Change Total wRVU Value 523 429 -18
Dollar Comparison Total Dollar Comp Original Audited Change Total Dollar Value $ 0 $ 0 -

Sample Selection Methodology Turn your filters on Sort by
o Provider (unless you run a separate report for each provider)o CPT code
ndash If you did not do an bell curve analysis prior you can review the volume of each E amp M level here
ndash Determine what types of services (outpatient inpatient EM Surgery etc)ndash How many of each level of service (depends on the providers EM utilization patterns)
o Resort by Patientndash This will allow you to see all services performed for each DOSndash Helps to capture encounters that have both EM amp Procedures Preventive with EM etc
o Pay attention to the Modifiersndash Do you want to include resident documentation Look for GC or GEndash Do you want to include EM with procedure Look for 25
ndash ReportsSample Selectionxlsx
Scoring Methodology
Scoring Methodology
Establish an Accuracy Rateo The OIG recommends that physicians maintain an accuracy rate of 95
ndash Net Error Rate
o Is it realistic to establish a 95 accuracy rate for the providers
Scoring Examples (automated)
Total Visits Accurately Coded Under CodedBilled Over CodedBilled(+) Wrong Category (WC) Gross Financial Error ()
62 20 3226 4 645 13 2097 29 4677 4203
$123000 $14694 $37000 Provider RVUs User RVUs Points
0 129 5772 6200 (931)
EM Coding Total Sample Size 4 codes EM Detailed Review Total Sample Size 4 codes
Findings Count EM Level appears to be correct 0 0 EM Level appears to be over-coded 3 75 EM Level appears to be under-coded 1 25
CPTreg HCPCS II Coding Total Sample Size 0 codes
Findings Count Code(s) appear to be correct 0 0 Code(s) appear to be incorrect 0 0 Additional code(s) supported 0 0
Findings Count Over coded by 1 level 3 75 Over coded by 2 levels 0 0 Over coded by 3 levels 0 0 Over coded by 4 levels 0 0 Under coded by 1 level 1 25 Under coded by 2 levels 0 0 Under coded by 3 levels 0 0 Under coded by 4 levels 0 0 Number of category changes 0 0
ICD-CM Coding Total Sample Size 5 codes RVU Comparison
Findings Count Code(s) appear to be correct 3 60 Code(s) appear to be incorrect 1 20 Additional code(s) supported 1 20
wRVU Comp Original Audited Change Total wRVU Value 523 429 -18
Dollar Comparison Total Dollar Comp Original Audited Change Total Dollar Value $ 0 $ 0 -

Scoring Methodology
Scoring Methodology
Establish an Accuracy Rateo The OIG recommends that physicians maintain an accuracy rate of 95
ndash Net Error Rate
o Is it realistic to establish a 95 accuracy rate for the providers
Scoring Examples (automated)
Total Visits Accurately Coded Under CodedBilled Over CodedBilled(+) Wrong Category (WC) Gross Financial Error ()
62 20 3226 4 645 13 2097 29 4677 4203
$123000 $14694 $37000 Provider RVUs User RVUs Points
0 129 5772 6200 (931)
EM Coding Total Sample Size 4 codes EM Detailed Review Total Sample Size 4 codes
Findings Count EM Level appears to be correct 0 0 EM Level appears to be over-coded 3 75 EM Level appears to be under-coded 1 25
CPTreg HCPCS II Coding Total Sample Size 0 codes
Findings Count Code(s) appear to be correct 0 0 Code(s) appear to be incorrect 0 0 Additional code(s) supported 0 0
Findings Count Over coded by 1 level 3 75 Over coded by 2 levels 0 0 Over coded by 3 levels 0 0 Over coded by 4 levels 0 0 Under coded by 1 level 1 25 Under coded by 2 levels 0 0 Under coded by 3 levels 0 0 Under coded by 4 levels 0 0 Number of category changes 0 0
ICD-CM Coding Total Sample Size 5 codes RVU Comparison
Findings Count Code(s) appear to be correct 3 60 Code(s) appear to be incorrect 1 20 Additional code(s) supported 1 20
wRVU Comp Original Audited Change Total wRVU Value 523 429 -18
Dollar Comparison Total Dollar Comp Original Audited Change Total Dollar Value $ 0 $ 0 -

Scoring Methodology
Establish an Accuracy Rateo The OIG recommends that physicians maintain an accuracy rate of 95
ndash Net Error Rate
o Is it realistic to establish a 95 accuracy rate for the providers
Scoring Examples (automated)
Total Visits Accurately Coded Under CodedBilled Over CodedBilled(+) Wrong Category (WC) Gross Financial Error ()
62 20 3226 4 645 13 2097 29 4677 4203
$123000 $14694 $37000 Provider RVUs User RVUs Points
0 129 5772 6200 (931)
EM Coding Total Sample Size 4 codes EM Detailed Review Total Sample Size 4 codes
Findings Count EM Level appears to be correct 0 0 EM Level appears to be over-coded 3 75 EM Level appears to be under-coded 1 25
CPTreg HCPCS II Coding Total Sample Size 0 codes
Findings Count Code(s) appear to be correct 0 0 Code(s) appear to be incorrect 0 0 Additional code(s) supported 0 0
Findings Count Over coded by 1 level 3 75 Over coded by 2 levels 0 0 Over coded by 3 levels 0 0 Over coded by 4 levels 0 0 Under coded by 1 level 1 25 Under coded by 2 levels 0 0 Under coded by 3 levels 0 0 Under coded by 4 levels 0 0 Number of category changes 0 0
ICD-CM Coding Total Sample Size 5 codes RVU Comparison
Findings Count Code(s) appear to be correct 3 60 Code(s) appear to be incorrect 1 20 Additional code(s) supported 1 20
wRVU Comp Original Audited Change Total wRVU Value 523 429 -18
Dollar Comparison Total Dollar Comp Original Audited Change Total Dollar Value $ 0 $ 0 -

Scoring Examples (automated)
Total Visits Accurately Coded Under CodedBilled Over CodedBilled(+) Wrong Category (WC) Gross Financial Error ()
62 20 3226 4 645 13 2097 29 4677 4203
$123000 $14694 $37000 Provider RVUs User RVUs Points
0 129 5772 6200 (931)
EM Coding Total Sample Size 4 codes EM Detailed Review Total Sample Size 4 codes
Findings Count EM Level appears to be correct 0 0 EM Level appears to be over-coded 3 75 EM Level appears to be under-coded 1 25
CPTreg HCPCS II Coding Total Sample Size 0 codes
Findings Count Code(s) appear to be correct 0 0 Code(s) appear to be incorrect 0 0 Additional code(s) supported 0 0
Findings Count Over coded by 1 level 3 75 Over coded by 2 levels 0 0 Over coded by 3 levels 0 0 Over coded by 4 levels 0 0 Under coded by 1 level 1 25 Under coded by 2 levels 0 0 Under coded by 3 levels 0 0 Under coded by 4 levels 0 0 Number of category changes 0 0
ICD-CM Coding Total Sample Size 5 codes RVU Comparison
Findings Count Code(s) appear to be correct 3 60 Code(s) appear to be incorrect 1 20 Additional code(s) supported 1 20
wRVU Comp Original Audited Change Total wRVU Value 523 429 -18
Dollar Comparison Total Dollar Comp Original Audited Change Total Dollar Value $ 0 $ 0 -

Scoring Methodology
Evaluation amp Management
7 points if correct5 points if off by one level
0 points if wrong category or if off by 2 or more levels or if not coded
Procedure(s) 7 points if correct4 points if units incorrect0 points if not correct
CPT HCPCS 7 points if correct4 points if units incorrect0 points if not correct
ICD-10-CM 3 points if correct2 points if the primary is correct but not the others1 point if the secondary is correct but not the primary
Modifier(s) -1 if not correct or if missing
Your scoring methodology is an essential component of your audit reports The scoring methodology should
be defined in the Executive Summary Report
In-Patient DRG Scoring Example
Ttl DRG 10 Ttl Assign 12
DRG Accuracy Ttl Chg 3 I-10 Px Accuracy Ttl Chg 1
Accu 70 Ttl Code 13 Accu 92
Ttl Assign 159 Total Cht 10Coding
AccuracyTtl
Chng 16Disposition Acc Ttl Chg 0
Ttl Code 175 Accu 100
Accu 91
Ttl Assign 137 Total Cht 137Dx
Accuracy Ttl Chg 12POA Accuracy Ttl Chg 0
Ttl Code 149 Accu 100
Accu 92
Coding Guidelines
Coding Guidelines
Standardized Coding Guidelines is criticaloCPT Guidelineso ICD-10 GuidelinesoCMS Guidelines
ndash Follow your Medicare Carriers GuidelinesoCCI GuidelinesEditsoMedicaidMedi-Cal Guidelineso Internal Guidelines that define
ndash Gray areas of codingndash Payer specific guidelines
Coding Guidelines
E amp M Guidelineso95 or 97oDefine the 95 detailed examo Is ldquonon contributoryrdquo allowedo2 out of 3 key components (Is MDM required)
Coding Guidelines
Other Risk AreasoMedical Necessityo Teaching Physician Guidelineso Incident To o SplitSharedoCopy amp PasteCloned noteso Scribeso SignatureAuthenticationsoOrders for diagnostic servicesoDate of ServiceoNew versus Established CodesoConsultations
Audit Reports
Goals of the Audit Report
The main goal of an audit report is to communicate where the organization specialty department provider or coder does or does not conform to regulatory standards guidelines and organizational policieso Each identified issue must have a standard it is measured againsto Site the regulation in your audit report or include a link to the regulation
Audit reports should not just contain negative findings Outline the Positives also Identify opportunities for improvement this can be in the form of a
recommendation Prioritize High Risk Findings
Who will be reading the Audit Report
What is the technical knowledge of the readeroCodersHIM ProfessionalsoProvidersoClinical StaffoHIM DirectorsoBillingCoding DirectorsManagersoCEOCFO (Executive Team)
Audit Report Format Tips
Provide perspective for the readero Positive and Negative findings
Be precise avoid redundant phrasing inexact terminology Avoid long sentences when a shorter one will work Avoid stating your opinion State the findings and facts Use bullet points this helps to break up difficult information and makes it
clearer for the reader Use gender neutral terms Avoid audit ldquobuzzwordsrdquo such as ldquogenerally improvedrdquo or ldquosignificant riskrdquo Avoid abbreviations unless they are clearly defined
Benefits of Automating your Audit Reports Results
o Consistent Resultso Better Datao Increases Efficiency
Trackingo Allows audit results to be tracked by provider and by specialty
QAo Allows for an automated approach to your internal quality reviews
Trendingo Allows for data analysis at a detailed level that can be tracked
Productivityo Increases auditor productivityo Decreases re-work
ProviderCoder Audit Reports
Detailed Audit reports should have the ability to be sorted byoProvideroCodero Specialty or GroupoAudit Date
Detailed results for each encounteroMeaningful comments
Key Findingso From all encounters
Recommendations and Resources
Detailed Findings Patient ID Patient Name DOS Payer CPT Reported CPT Audited EM Level Key Component ICD Reported ICD Reported Description ICD Audited ICD Reported Description
1 001 Patient A 02-19-16 Blue Cross
99203 25 1 99202 1 +1 D E L 1 S92302A2 Not Reported
1 Fracture of unspecified metatarsal bone(s) left foot initial encounter for closed fracture
1 S92355D2 W109XXD
1 Nondisplaced fracture of fifth metatarsal bone left foot subsequent encounter for fracture with routine healing2 Fall (on) (from) unspecified stairs and steps subsequent encounter
1 The documentation supports coding for an EM service that is one level below the billed code2 Lacking Exam documentation to support the EM level selected3 1997 MSK exam supports an Expanded Problem Focused exam (99202) 1995 exam supports a Detailed exam (99203)4 1997 Exam template suggestions Neurologic Exam-suggest adding the body part examined (upper extremitylow extremity) Dermatologic Exam-unable to determine if this was performed This should be deleted from the final note if
not examined5 EM time statement is insufficient documentation is lacking a required element total time of visit and counseling time greater than 506 CPT disallowed documentation is not present within the medical record to support the CPT code billed (28485-open treatment of metatarsal fracture includes internal fixation when performed) Fracture care is not supported patient
was seen in the ER 6 weeksrsquo prior ER doctor initiated treatment7 The incorrect pricing modifier was billed Removed modifier 25 (separate and significant EM on the same day as a minor procedure) Fracture care is not billable no modifier needed on EM service8 Diagnosis billed is not the most specific available according to the medical record documentation9 Documentation supports an additional diagnosis code not billed
2 002 Patient B 02-05-16 Blue Cross
99203 25 1 99202 25 1 +1 D E L 1 L03032 1 Cellulitis of left toe 1 L03032 1 Cellulitis of left toe
1 The documentation supports coding for an EM service that is one level below the billed code2 Lacking Exam documentation to support the EM level selected3 1997 MSK exam supports an Expanded Problem Focused exam (99202) 1995 exam supports a Detailed exam (99203)4 EM time statement is insufficient documentation is lacking one or more required elements (total time counseling time greater than 50) If a procedure is performed during a visit the time spent performing the procedure needs to be
carved out of the total visit time5 Allowed modifier 25 due to commercial payer Medicare and NCCI do not require modifier 25 on a new patient EM when a minor procedure is performed the same day 6 Diagnosis supported
Detailed Findings
135 822012 New Consultations - Office
Consultations Detailed Detailed (95) Moderate 99244 99243 1 $3500 N
Provider Code 99244 Reviewer Code 99243 Provider Diagnosis 1 3005 NEURASTHENIA Reviewer Diagnosis 1 3005 NEURASTHENIA Provider Diagnosis 2 7282 MUSC DISUSE ATROPHY NEC Reviewer Diagnosis 2 7282 MUSC DISUSE ATROPHY NEC
bull Assessment (I) The assessment is not clearly stated for this encounter Documentation Guidelines states The documentation for each patient encounter should include assessment clinical impression or diagnosis bull Assessment (R) The assessment should be clearly documented for each encounter Since each note must stand alone it is imperative to accurately document the most specific diagnosis in the assessment impression section of the note
bull Documented Lower Level (I) The documentation substantiates a lower level of service than charged
Chart Level Comments
Group your comments in categoriesoDocumentationo E amp MoProceduresoModifierso ICD-10-CM
oReportsAudit Manager Macros 061218 (version 1)xlsx
Recommendations and ReferencesCategory Short Description Long Description
EM AdmissionDischarge Same Day Review the CMS AdmissionDischarge same day coding guidelines httpswwwcmsgovRegulations-and-GuidanceGuidanceManualsDownloadsclm104c12pdf
EM ConsultationReview the consultation guidelines located in the CPT book
EM Consultation not billable to Medicare CMS no longer recognizes the consultation codeshttpswwwcmsgovOutreach-and-EducationMedicare-Learning-Network-MLNMLNMattersArticlesdownloadsmm6740pdf
EM Critical CareReview the CMS Critical Care guidelines httpswwwcmsgovOutreach-and-EducationMedicare-Learning-Network-MLNMLNMattersArticlesdownloadsmm5993pdf
EM Discharge ServicesReview the CMS Hospital Discharge Services guidelineshttpswwwcmsgovOutreach-and-EducationMedicare-Learning-Network-MLNMLNMattersArticlesdownloadsmm5794pdf
EMEM and Preventive Visit Review AAPC guidance for documenting and billing an EM and Preventive visit same day httpswwwaapccomblog22580-successfully-bill-a-
preventive-service-with-a-sick-visit
EM EM documentation guidelines Review the CMS 1995 amp 1997 EM documentation guidelineshttpswwwcmsgovOutreach-and-EducationMedicare-Learning-Network-MLNMLNEdWebGuideEMDOChtml
EM EM Inpatient vs Outpatient Review the patientrsquos status on the hospital admission order to determine the appropriate EM category to bill (inpatient vs observation)
EM EM New vs EstablishedReview the CMS New vs Established patient guidelines httpswwwcmsgovOutreach-and-EducationMedicare-Learning-Network-MLNMLNProductsDownloadseval-mgmt-serv-guide-ICN006764pdf
EMEM Time billing suggestion
Recommend a time statement is added to the EM medical record when a majority of the visit is spent counseling andor coordination of care Review the CMS 1995 amp 1997 EM documentation guidelines for EM time documentationhttpswwwcmsgovOutreach-and-EducationMedicare-Learning-Network-MLNMLNEdWebGuideEMDOChtml
EM Inpatient hospital servicesReview the CMS Hospital Services (Initial and Subsequent) guidelines httpswwwcmsgovRegulations-and-GuidanceGuidanceManualsDownloadsclm104c12pdf
EM Nursing Facility Services Review the Nursing Facility Services guidelines provided by CMS The guidelines can be downloaded at this linkhttpswwwcmsgovRegulations-and-GuidanceGuidanceManualsDownloadsclm104c12pdf
EM Observation Services Review the CMS Observation Services (Initial and Subsequent) guidelines httpswwwcmsgovRegulations-and-GuidanceGuidanceManualsDownloadsclm104c12pdf
EM Prolonged Services Review the CMS Prolonged Services guidelines httpswwwcmsgovOutreach-and-EducationMedicare-Learning-Network-MLNMLNMattersArticlesdownloadsmm5972pdf
EMReview of Systems Review the CMS 1995 amp 1997 EM documentation guidelines for Review of Systems requirements
httpswwwcmsgovOutreach-and-EducationMedicare-Learning-Network-MLNMLNEdWebGuideEMDOChtml
EMConsultation Documentation Suggestion
Recommend adding verbiage to consultation documentation that indicates the name of the referring provider and the reason for the consultation
Audit Report Examples Automated Solution
Letrsquos look at some report Examples
ReportsStandard Provider Audit SummarypdfReportsProvider Detailed Sample Reportdocx
ReportsProvider Audit Worksheets - Optionalpdf
Audit Report Examples Non Automated Solution
Error Findings by Volume Percentage
CPT Coded Accurately
8 8 Overcoded
8 8 Undercoded
Missed CPTHCPCS Code
Missed or Wrong Modifier
8 8 Incorrect CPT (or Category) Used
Incorrect ICD-9 Codes
8 8 Incorrect Quantity
Inadequate Documentation
Missing Documentation 8 8
Signature Illegible (No Log)
8 8
CLIENT NAME PROJECT TITLE
Review Line Item Detail Prepared Month Year
DRAFT
Client Claim Demographics Client Charge Data Review Result EampM ONLY Findings C C C C C C O OC O O O
Char
t Num
ber
Au
dit D
ate
Audi
tor (
initi
als)
QA
Initi
als
Fa
cilit
y Lo
catio
n Re
porte
d
Pr
ovid
er N
ame
Pa
tient
Nam
e
M
edic
al R
ecor
d Nu
mbe
r
Prim
ary
Carr
ier M
edica
re=
A M
edica
id =
B O
ther
=O
Da
te o
f Ser
vice
CP
T Co
de
Mod
ifier
(s) i
n or
der
Qua
ntity
Diag
nosi
s Co
de(s
) 1
thro
ugh
4
Fe
e ch
arge
d
Pr
imar
y Pa
ymen
t Am
ount
CPT
Code
Mod
ifier
(s) i
n or
der
Qua
ntity
Diag
nosi
s Co
de(s
) 1
thro
ugh
4
CO
RREC
T AL
LOW
ABLE
Prim
ary
PAYM
ENT
Va
rianc
e
Chie
f Com
plai
nt
Hist
ory
Leve
l Sup
port
ed
Exam
Lev
el S
uppo
rted
Med
ical
Dec
Mak
ing
Supp
orte
d (o
r TIM
E)
CPT
Cod
ed A
ccur
atel
y
Ove
rcod
ed
Und
erco
ded
Mis
sed
CPT
HC
PCS
Cod
e
Mis
sed
or W
rong
Mod
ifier
Inco
rrec
t CPT
(or C
ateg
ory)
Use
d
Inco
rrec
t IC
D-9
Cod
es
Inco
rrec
t Qua
ntity
Inad
equa
te D
ocum
enta
tion
Mis
sing
Doc
umen
tatio
n
Sign
atur
e Ill
egib
le (N
o Lo
g)
No
Sign
atur
e by
Pro
vide
r of
Ser
vice
COMMENTS (abbreviations used) PF- PROBLEM FOCUSED EPF- EXPANDED PF DET- DETAILED COMP- COMPREHENSIVE SFWD- STRAIGHT FORWARD MOD- MODERATE MDM- MEDICAL DECISION MAKING
Char
t Num
ber
SAMPLE SAMPLE S MD SAMPLE SAMPLE XXXXX XXX 112001 99212 25 1 1 1234 2 5678 3 4
$30000 $2200 99212 25 1 1 1234 2 5678 3 4
$56400 $54200 YES
DET
CO
MP
MO
D
COMMENTS COMMENTS COMMENTS
0
1 2 3 4
1 2 3 4
$000 0
$30000 $2200 $56400 $54200 10 10 10 10 10 10 10 10 10 10 10 10 TOTALS 917 Error Rate by Volume
Error Findings by Volume 8 CPT Coded Accurately 8 Overcoded 8 Undercoded 8 Missed CPTHCPCS Code 8 Missed or Wrong Modifier 8 Incorrect CPT (or Category) Used 8 Incorrect ICD-9 Codes 8 Incorrect Quantity
Inadequate Documentation 8 8 Missing Documentation 8 Signature Illegible (No Log) 8 No Signature by Provider of Service
1200 Total
Net Payment Error Rate -24636
Primary Payments Total $ Audited Payment Total $ (Total Under Payments)
Total Over Payments
Net OverUnder Payment $
2200 56400
(54200)
Resources Used HCPCS and CPT CodeBook (Current or applilcable year) ICD-10-CM CodeBook (Current or applicable year) CMS 1995 and 1997 EM Guidelines CMS Claims Processing Manual 100-04 Medicare Claims Processing (PUB 100-04) CMS - National Coverage Determinations (NCDs) National Correct Coding Policy Manual Applicable Physician Version
Executive Summary Report
The executive summary provides readers with a short complete document highlighting import information included in the detailed report Executive summaries are created for the senior management readers that donrsquot have time to read the full report and need to walk away with an understanding of the issues and corrective actions
Some would say the executive summary could be written before the detailed report however it is difficult to make sure the most important elements are included until you have spent time reviewing the detail If you want to make sure the most important messages are in the executive
summary this step should be completed after the detail is written As auditors become more seasoned this step could move to the front of the process
Executive Summary Report Structure of the ES Report
o Backgroundndash Specialtyndash Providersndash Sample Selection sizendash Date range of audit
o Audit Scopeo Regulatory Resourceso Type of Medical records reviewedo Overall Accuracy (all providers)o Detailed Audit Findings
ndash Business Impactndash Summary of Findings
o Department Findingso Summary
o ReportsStandard Executive Summary Professional Servicespdf
Department Findings Top Issues
Date ofServiceErrors
MissingDocuments
Missing orInvalid
Signature
TeachingPhysician
Errors
InsufficientConsultation
Documents
OverCoding
EMBundled
IntoGlobal
SurgicalPackage
SplitSharedServiceError
Incorrector
MissingPricing
Modifier
ICD-10Errors
Family Practice
CardiologyInternal Medicine
TOTALS
Top Findings by Provider
E amp M Accuracy Rates
ICD-10-CM Accuracy Rates
Procedure Accuracy Rates
Inpatient DRG Audit Report
TABLE OF CONTENTS
Executive Summaryo Scope of Work
Reimbursement Changes Department Results
o InpatientGeneral Recommendations and Comments
o Secondary DiagnosesoProcedure CodingoPresent on AdmissionoQueries
Scope of WorkCodingAID performed coding audit review of 175 inpatient records The review completed was a random sample that included cases coded by twenty coders for dates of service from May 2016 ndash July 2016
The objective was to determine if the medical record documentation supported the following coding and documentation requirements and any other regulatory requirement for that code set Criteria reviewed
1 ICD-10-CM Official Coding Guidelines for accurate diagnosis code reporting 2 ICD-10-PCS Official Coding Guidelines for accurate procedure code reporting 3 Documentation of procedure compared to the CPT code assigned 4 Identify opportunities for education and training 5 Financial impact of current coding practices
The regulatory agencies and reference materials relied upon include the following in addition to Medicare and Medicaid regulations Additional resources are located in the sub sections below
bull ICD-10-CM and ICD-10-PCS for Hospitals current volume bull Centers for Medicare and Medicaid Services CMS NCCI Edits-Centers for Medicaid and
Medicare Services CMS website wwwcmsgov bull AHA Coding Clinic
The following electronic medical record documents were reviewed and relied upon to compare to the actual codes submitted to the third party payer
bull Discharge summaries HampPs Progress Notes and other provider notes located in the EMR Records
bull Patient History Forms Ancillary Staff Notes bull Procedure Notes bull Orders bull Diagnostic Report
Reimbursement Changes
Coder Acct
Billed Audited
Reimbursement ChangesMS DRG SOI ROM Weight Expected
Payment MS DRG SOI ROM Weight Expected Payment
Coder 1 001 790 52300 $2615000 792 21552 $1077600 -$1537400
Coder 2002
749 26452 $1322600 758 10090 $504500 -$818100
Coder 3 003 669 13111 $655550 694 07294 $364700 -$290850
Coder 4 004 389 08707 $435350 394 09502 $475100 $39750
Coder 5 005 312 07630 $381500 812 08572 $428600 $47100
Coder 6 006 384 08481 $424050 378 09949 $497450 $73400
Coder 7 007 206 08164 $408200 794 12987 $649350 $241150
Coder 8008
344 31029 $1551450 853 51334 $2566700 $1015250
TOTAL $7793700 $6564000 -$1229700
General Recommendations and CommentsFinding Pertinent secondary diagnoses are not coded and diagnoses are code which are not supported in provider documentation Code only those diagnoses which are documented by the provider on the current chart Not all codes are coded to the highest degree of specificity and combination codes were sometimes missed
Recommendation It is important to assign codes for all conditions which meet the definition of a reportable diagnosis Documentation from all providers should be used including but not limited to radiologists pathologists anesthesiologists CRNAs and FNPs
Reference Coding Clinic Official Coding Guidelines
bull Report all secondary diagnoses which meet the definition of a secondary diagnosis which is defined as all conditions that coexist at the time of admission that develop subsequently or that affect the treatment received andor the length of stay Codes which enhance the overall picture of the patientrsquos visit should be added
o Add T45515A to report adverse effect of Coumadin which caused the GI bleed
o Add I2690 for septic pulmonary emboli (MCCSOI4ROM4)
o Add N179 for acute kidney failure (S3M2CC) per the nephrology consult and the 628 progress note
o Add code I429 cardiomyopathy per HampP
o Add B964 to report proteus in a UTI per the 620 hospitalist progress note
o Code for D649 anemia and I701 stenosis of renal artery should be added as secondary diagnoses per the HampP
bull Only report diagnoses which are substantiated by provider documentation in the current chart notes If a suspected condition is not verified at discharge on an inpatient account it cannot be coded
o Remove G4734 (idiopathic sleep related non-obstructive alveolar hypoventilation) as patient was noted to have the sleep study and the hypoventilation was shown to be a possibility but not noted as such on discharge
o Remove G629 (S21) the neuropathy is documented as due to diabetes
o Remove K529 colitis noted on HP as possible but not further noted or confirmed at discharge
Procedure CodingFinding Procedures were sometimes coded incorrectly
Recommendation The entire medical record should be reviewed and all procedures coded as documented Coding procedures incorrectly or assigning incorrect CPT codes may result in lost revenue
bull Incorrect root operation
o Revise principal procedure to 0DQ68ZZ for clipping of the ulcer per OP report clipping is root operation repair
bull Biopsy versus Excision
o Procedure 0DBA0ZX (biopsy of jejunum) should change to 0DBA0ZZ (excision of jejunum) per op note this was not a biopsy procedure
bull Coding Guideline error
o Remove 0RG10K0 for allograft due to being inclusive in principal procedure
o Remove codes for adhesiolysis 0DN80ZZ 0UN10ZZ and 0UN90ZZ due to no significance noted per OP report
bull Incorrect approach
o Revise 0TF63ZZ (fragmentation percutaneous approach) to 0TF68ZZ (fragmentation endoscopic) for procedure performed via scope per the operative report
bull Procedure coded without provider documentation
o Remove secondary procedure of excisional debridement (0JB90ZZ) due to lack of documentation of excisional debridement per operative report The header in the operative report documents IampD and debridement but the body of the operative report only documents an IampD
bull Incorrect CPT code assignment
o Post-op note supports the nerve block injections of four nerves therefore code 64421 (multiple nerve block) should replace 64420 (injection of one intercostal nerve)
Queries Finding Conflicting incomplete and vague documentation is found within provider chart notes
Recommendation Prior to code assignment if the coder finds ambiguous or conflicting documentation the provider should be queried
Reference AHA Coding Clinic 2002 2nd Quarter pages 17-18
bull Query for acute blood loss anemia since hgb has dropped and patient is being transfused PRBC
bull Recommend query to clarify if cardiorenal syndrome is current as it is documented per 627 nephrology consult but unclear if current
bull Documentation does not support SIRS noninfectious without organ failure It is conflicting since patient has respiratory failure Query should be initiated for clarification with or without organ failure or infectious or non-infectious Patient has pneumonia per query as well as last progress note therefore if SIRS is not further specified per query PNA should be sequenced as principal diagnosis and SIRS should be removed
bull Recommend provider query necrotizing lung consolidation noted on DS as principal diagnosis-unclear does the patient have lobar pneumonia Secondary dx states necrotic pneumonia which is coded as principal diagnosis-this diagnosis is clear but consolidation portion is unclear
bull Recommend query for preterm labor delivery at 301 weeks
bull RECOMMEND QUERY no chest pain on admit per ER and HP cardiology provider states no CP with ER stating chest pressure the day prior to admit Appears patient was admitted due to elevated troponins which cardiology says are likely due to hypotension and AKI DS states chest pain but also says bradycardia and hypotension were the reason for admit
bull RECOMMEND QUERY no chest pain on admit per ER and HP cardiology provider states no CP with ER stating chest pressure the day prior to admit Appears patient was admitted due to elevated troponins which cardiology says are likely due to hypotension and AKI DS states chest pain but also says bradycardia and hypotension were the reason for admit
bull Query the provider regarding pathology report notation of endometriosis andor possible re-sequence of stenosis as principal diagnosis as it also meets principal diagnosis guidelines This would result in an MS-DRG change to 742 and APR-DRG change to 513
bull QUERY secondary diagnosis MCC and ROM 4 code T3166 (60 TBSA of which 60 are third degree burns) Chart notes do not specify how much of TBSA was actually third degree If after query TBSA is found to be less than 50 (T3164) then ROM will change from 4 to 3 but no change to overall APR-DRG or weight
Auditor Quality amp Productivity
Audit Productivity Standards
It takes twice as long to audit a chart as it does to code it a statistic that takes into account the time to document an explanation of any coding decision the auditor is not in agreement with o For example in an emergency department audit with a productivity of 12
charts per hour for a coder our auditors would probably be able to review six per hour
o If there are multiple services to audit on each encounter the productivity may only be 4 per hour
o The amount of detail you put into your audit report will also be a factorndash Are you using an automated audit softwarendash Are you using a spreadsheet to auditndash How many Systems are needed to complete the audit
Coder Quality Audits
Quality Audits (QA) should be done on your coders and auditors regularly Frequent reviews with smaller sample size will allow more consistent
review and feedbacko Example 10 charts per month per coder if the coder passes 2-3 months
consecutively with 95 or better score move them to quarterly reviewso Some QA programs review a percentage of the coders work This
methodology requires more time and resources
Auditor QA should also score and comment on the accuracy of the audit comments and recommendations
Presenting the Audit Results
Presenting the Audit Results
Communicating the Audit FindingsoWho requested the AuditoWho are you reporting the finding to
ndash CEOndash CFOndash Physicianndash Revenue Cycle Managerndash HIM Directorndash Billing Managerndash Coding Manager
ReportsAudit Resultspptx
Post Audit Education
Provider Education
Provider Education is best received when it is specific to the provider(s) 11 sessions going over the audit result Look at their notes with them
oHighlight areas for documentation improvementoReinforce Coding Guidelines that are specific to themoAsk them to share how they establish their LOS for E amp M serviceso Integrate their EMR system into the training
Provider Education
Group Training SessionsoUse the audit results to identify common issues within a specialty group
ndash Refer to the Executive Summary reportoVery effective for identifying system issues
ndash Teaching Attestationsndash Templatesndash Copy and Pastendash Cloned notes
o Everyone hears the same messagesoAn Issue may not appear on the individual audit but is still a concern for the
group
Education Delivery
In person or remote sessionso Factors to consider
ndash Providers scheduleavailabilityndash Location(s)ndash Personality of the providerndash Budget
Coder Education
Coders do well in group training so they can learn from each other 11 training allows the coder to get feedback on their coding
Handling Audit Disputes
Handling Audit Disputes
Be open to all points of viewo Let the documentation tell the story
Refer to the guidelines Ask
oCan we defend the reported service with the current documentation
Self Disclosures Refunds and Corrected Billing
Overpayment
In general If a person has received an overpayment the person shallo report and return the overpayment to the Secretary the State an
intermediary a carrier or a contractor as appropriate at the correct address and ndash notify the Secretary State intermediary carrier or contractor to whom the overpayment was returned in writing of the reason for the overpayment
What is an ldquoOverpaymentrdquo ndash The term ldquooverpaymentrdquo means any funds that a person receives or retains under subchapter XVIII or XIX of this chapter to which the person after applicable reconciliation is not entitled under such subchapter
Self Disclosure
The Office of Inspector General (OIG) has several self-disclosure processes that can be used to report potential fraud in Department of Health and Human Services (HHS) programs Choose the one that applies to you from the following descriptions to learn moreo Health Care Provider Self-Disclosures
ndash Health care providers suppliers or other individuals or entities subject to Civil Monetary Penalties can use the Provider Self-Disclosure Protocol which was created in 1998 to voluntarily disclose self-discovered evidence of potential fraud Self-disclosure gives providers the opportunity to avoid the costs and disruptions associated with a Government-directed investigation and civil or administrative litigation Visit the Provider Self-Disclosure Protocol webpage for more information
o HHS Contractor Self-Disclosuresndash Contractors are individuals businesses or other legal entities that are awarded Government contracts or
subcontracts to provide services to the Department of Health and Human Services (HHS) OIGs contractor self-disclosure program enables contractors to self-disclose potential violations of the False Claims Act and various Federal criminal laws involving fraud conflict of interest bribery or gratuity This self-disclosure process is available for those entities with a Federal Acquisition Regulation-based contract Visit the Contractor Self-Disclosure webpage for more information
o HHS Grantee Self-Disclosuresndash HHS grantees or subrecipients may voluntarily disclose evidence of potential violations of Federal criminal law
involving fraud bribery or gratuity violations potentially affecting the Federal award 45 CFR 75113 notes mandatory disclosures of criminal offenses that non-Federal entities must make with respect to HHS grants Recipients submitting disclosures in connection with this requirement should include the subject reference line Mandatory Grant Disclosure Recipients choosing to disclose conduct that may not fit squarely within the scope of offenses described in 45 CFR 75113 should include the following subject reference line in the submission Voluntary Grant Disclosure
Medicare 60 day rule
The 60 Day Rule (Medicare Parts A amp B) o The 60 day time period for reportingreturning begins when either
ndash The reasonable diligence is completed orndash On the day the provider received credible information of a potential overpayment (if the
provider fails to conduct reasonable diligence) o For an investigation to be conducted in a ldquotimelyrdquo manner providers typically
must complete the investigation within 6 months from receipt of credible information indicating there may be an overpayment
ndash ndash 6-month timeframe may potentially be extended under ldquoextraordinary circumstancesrdquo ndash 8 months generally the maximum total time to return overpayments The government recommends that providers maintain records documenting ldquoreasonable diligencerdquo
Medicare 60 Day Rule
Six-year lookback period ndash Sometimes possible to use a shorter period depending on the facts at issue Amount to be repaid ndash May vary depending on the method used to
reportreturn eg Medicare administrative contractor (ldquoMACrdquo) v self-disclosure Overpayment notification ndash After receiving an overpayment
notification from the government you should investigate for related overpayments eg other time periods
Medicare 60 Day Rule
Self-disclosure protocols ndashoA submission to the OIG or CMS protocols suspends the 60 day requirement
for returning overpayments until a settlement agreement is executed ndash ndash OIGrsquos Self-Disclosure Protocol (SDP) ndash ndash CMS Voluntary Self-Referral Disclosure Protocol (SRDP) ndash
o Self-disclosures to other agencies do not suspend the repayment deadlinendash ndash Eg Department of Justice local US Attorneyrsquos Office Medicaid Fraud Control Unit
Medicare 60 Day Rule
Facilitating Compliance With the 60 Day Rule Compliance programs should include o ndash Appropriate policies and procedures o ndash Periodic billing and coding audits to proactively identify overpaymentso ndash Focus on high-risk areas o ndash Utilization of publicly available government resources to guide audit efforts o ndash Investigating any suspected incidents of non-compliance with federal health
care program requirements
Self Disclosure
Choice of AgencyoOIG ndash Self-Disclosure Protocol
ndash ndash Conduct involving false billingndash ndash Conduct involving excluded personsndash ndash Conduct involving the Anti-Kickback Statute (including conduct thatndash violates both the AKS and Stark Law)
oCMS ndash Self-Referral Disclosure Protocolndash ndash Conduct involving only violations of the Stark Law
oDOJndash ndash May be appropriate when provider believes a FCA release is necessary
Summary
The Cost of a Well-Executed Coding Audit ProcessThe costs associated with an auditing program are worth it in the long run Ideally your organization is performing audits on a regular basis across all service types locations and payers Weve all seen claims that have been denied resulting in additional work that may be preventable with a proper audit program The goal is to use the audit feedback to improve coding quality and lower potential risk and cost to the organization Organizations should be investing in an effective coding audit program to make your coders and providers better and enhance documentation improvement from the providers
Questions
Thank you for your attentionLynn Handy
Vice President of Coding amp Audit ServicesLynnhandymanagedresourcesinccom

In-Patient DRG Scoring Example
Ttl DRG 10 Ttl Assign 12
DRG Accuracy Ttl Chg 3 I-10 Px Accuracy Ttl Chg 1
Accu 70 Ttl Code 13 Accu 92
Ttl Assign 159 Total Cht 10Coding
AccuracyTtl
Chng 16Disposition Acc Ttl Chg 0
Ttl Code 175 Accu 100
Accu 91
Ttl Assign 137 Total Cht 137Dx
Accuracy Ttl Chg 12POA Accuracy Ttl Chg 0
Ttl Code 149 Accu 100
Accu 92
Coding Guidelines
Coding Guidelines
Standardized Coding Guidelines is criticaloCPT Guidelineso ICD-10 GuidelinesoCMS Guidelines
ndash Follow your Medicare Carriers GuidelinesoCCI GuidelinesEditsoMedicaidMedi-Cal Guidelineso Internal Guidelines that define
ndash Gray areas of codingndash Payer specific guidelines
Coding Guidelines
E amp M Guidelineso95 or 97oDefine the 95 detailed examo Is ldquonon contributoryrdquo allowedo2 out of 3 key components (Is MDM required)
Coding Guidelines
Other Risk AreasoMedical Necessityo Teaching Physician Guidelineso Incident To o SplitSharedoCopy amp PasteCloned noteso Scribeso SignatureAuthenticationsoOrders for diagnostic servicesoDate of ServiceoNew versus Established CodesoConsultations
Audit Reports
Goals of the Audit Report
The main goal of an audit report is to communicate where the organization specialty department provider or coder does or does not conform to regulatory standards guidelines and organizational policieso Each identified issue must have a standard it is measured againsto Site the regulation in your audit report or include a link to the regulation
Audit reports should not just contain negative findings Outline the Positives also Identify opportunities for improvement this can be in the form of a
recommendation Prioritize High Risk Findings
Who will be reading the Audit Report
What is the technical knowledge of the readeroCodersHIM ProfessionalsoProvidersoClinical StaffoHIM DirectorsoBillingCoding DirectorsManagersoCEOCFO (Executive Team)
Audit Report Format Tips
Provide perspective for the readero Positive and Negative findings
Be precise avoid redundant phrasing inexact terminology Avoid long sentences when a shorter one will work Avoid stating your opinion State the findings and facts Use bullet points this helps to break up difficult information and makes it
clearer for the reader Use gender neutral terms Avoid audit ldquobuzzwordsrdquo such as ldquogenerally improvedrdquo or ldquosignificant riskrdquo Avoid abbreviations unless they are clearly defined
Benefits of Automating your Audit Reports Results
o Consistent Resultso Better Datao Increases Efficiency
Trackingo Allows audit results to be tracked by provider and by specialty
QAo Allows for an automated approach to your internal quality reviews
Trendingo Allows for data analysis at a detailed level that can be tracked
Productivityo Increases auditor productivityo Decreases re-work
ProviderCoder Audit Reports
Detailed Audit reports should have the ability to be sorted byoProvideroCodero Specialty or GroupoAudit Date
Detailed results for each encounteroMeaningful comments
Key Findingso From all encounters
Recommendations and Resources
Detailed Findings Patient ID Patient Name DOS Payer CPT Reported CPT Audited EM Level Key Component ICD Reported ICD Reported Description ICD Audited ICD Reported Description
1 001 Patient A 02-19-16 Blue Cross
99203 25 1 99202 1 +1 D E L 1 S92302A2 Not Reported
1 Fracture of unspecified metatarsal bone(s) left foot initial encounter for closed fracture
1 S92355D2 W109XXD
1 Nondisplaced fracture of fifth metatarsal bone left foot subsequent encounter for fracture with routine healing2 Fall (on) (from) unspecified stairs and steps subsequent encounter
1 The documentation supports coding for an EM service that is one level below the billed code2 Lacking Exam documentation to support the EM level selected3 1997 MSK exam supports an Expanded Problem Focused exam (99202) 1995 exam supports a Detailed exam (99203)4 1997 Exam template suggestions Neurologic Exam-suggest adding the body part examined (upper extremitylow extremity) Dermatologic Exam-unable to determine if this was performed This should be deleted from the final note if
not examined5 EM time statement is insufficient documentation is lacking a required element total time of visit and counseling time greater than 506 CPT disallowed documentation is not present within the medical record to support the CPT code billed (28485-open treatment of metatarsal fracture includes internal fixation when performed) Fracture care is not supported patient
was seen in the ER 6 weeksrsquo prior ER doctor initiated treatment7 The incorrect pricing modifier was billed Removed modifier 25 (separate and significant EM on the same day as a minor procedure) Fracture care is not billable no modifier needed on EM service8 Diagnosis billed is not the most specific available according to the medical record documentation9 Documentation supports an additional diagnosis code not billed
2 002 Patient B 02-05-16 Blue Cross
99203 25 1 99202 25 1 +1 D E L 1 L03032 1 Cellulitis of left toe 1 L03032 1 Cellulitis of left toe
1 The documentation supports coding for an EM service that is one level below the billed code2 Lacking Exam documentation to support the EM level selected3 1997 MSK exam supports an Expanded Problem Focused exam (99202) 1995 exam supports a Detailed exam (99203)4 EM time statement is insufficient documentation is lacking one or more required elements (total time counseling time greater than 50) If a procedure is performed during a visit the time spent performing the procedure needs to be
carved out of the total visit time5 Allowed modifier 25 due to commercial payer Medicare and NCCI do not require modifier 25 on a new patient EM when a minor procedure is performed the same day 6 Diagnosis supported
Detailed Findings
135 822012 New Consultations - Office
Consultations Detailed Detailed (95) Moderate 99244 99243 1 $3500 N
Provider Code 99244 Reviewer Code 99243 Provider Diagnosis 1 3005 NEURASTHENIA Reviewer Diagnosis 1 3005 NEURASTHENIA Provider Diagnosis 2 7282 MUSC DISUSE ATROPHY NEC Reviewer Diagnosis 2 7282 MUSC DISUSE ATROPHY NEC
bull Assessment (I) The assessment is not clearly stated for this encounter Documentation Guidelines states The documentation for each patient encounter should include assessment clinical impression or diagnosis bull Assessment (R) The assessment should be clearly documented for each encounter Since each note must stand alone it is imperative to accurately document the most specific diagnosis in the assessment impression section of the note
bull Documented Lower Level (I) The documentation substantiates a lower level of service than charged
Chart Level Comments
Group your comments in categoriesoDocumentationo E amp MoProceduresoModifierso ICD-10-CM
oReportsAudit Manager Macros 061218 (version 1)xlsx
Recommendations and ReferencesCategory Short Description Long Description
EM AdmissionDischarge Same Day Review the CMS AdmissionDischarge same day coding guidelines httpswwwcmsgovRegulations-and-GuidanceGuidanceManualsDownloadsclm104c12pdf
EM ConsultationReview the consultation guidelines located in the CPT book
EM Consultation not billable to Medicare CMS no longer recognizes the consultation codeshttpswwwcmsgovOutreach-and-EducationMedicare-Learning-Network-MLNMLNMattersArticlesdownloadsmm6740pdf
EM Critical CareReview the CMS Critical Care guidelines httpswwwcmsgovOutreach-and-EducationMedicare-Learning-Network-MLNMLNMattersArticlesdownloadsmm5993pdf
EM Discharge ServicesReview the CMS Hospital Discharge Services guidelineshttpswwwcmsgovOutreach-and-EducationMedicare-Learning-Network-MLNMLNMattersArticlesdownloadsmm5794pdf
EMEM and Preventive Visit Review AAPC guidance for documenting and billing an EM and Preventive visit same day httpswwwaapccomblog22580-successfully-bill-a-
preventive-service-with-a-sick-visit
EM EM documentation guidelines Review the CMS 1995 amp 1997 EM documentation guidelineshttpswwwcmsgovOutreach-and-EducationMedicare-Learning-Network-MLNMLNEdWebGuideEMDOChtml
EM EM Inpatient vs Outpatient Review the patientrsquos status on the hospital admission order to determine the appropriate EM category to bill (inpatient vs observation)
EM EM New vs EstablishedReview the CMS New vs Established patient guidelines httpswwwcmsgovOutreach-and-EducationMedicare-Learning-Network-MLNMLNProductsDownloadseval-mgmt-serv-guide-ICN006764pdf
EMEM Time billing suggestion
Recommend a time statement is added to the EM medical record when a majority of the visit is spent counseling andor coordination of care Review the CMS 1995 amp 1997 EM documentation guidelines for EM time documentationhttpswwwcmsgovOutreach-and-EducationMedicare-Learning-Network-MLNMLNEdWebGuideEMDOChtml
EM Inpatient hospital servicesReview the CMS Hospital Services (Initial and Subsequent) guidelines httpswwwcmsgovRegulations-and-GuidanceGuidanceManualsDownloadsclm104c12pdf
EM Nursing Facility Services Review the Nursing Facility Services guidelines provided by CMS The guidelines can be downloaded at this linkhttpswwwcmsgovRegulations-and-GuidanceGuidanceManualsDownloadsclm104c12pdf
EM Observation Services Review the CMS Observation Services (Initial and Subsequent) guidelines httpswwwcmsgovRegulations-and-GuidanceGuidanceManualsDownloadsclm104c12pdf
EM Prolonged Services Review the CMS Prolonged Services guidelines httpswwwcmsgovOutreach-and-EducationMedicare-Learning-Network-MLNMLNMattersArticlesdownloadsmm5972pdf
EMReview of Systems Review the CMS 1995 amp 1997 EM documentation guidelines for Review of Systems requirements
httpswwwcmsgovOutreach-and-EducationMedicare-Learning-Network-MLNMLNEdWebGuideEMDOChtml
EMConsultation Documentation Suggestion
Recommend adding verbiage to consultation documentation that indicates the name of the referring provider and the reason for the consultation
Audit Report Examples Automated Solution
Letrsquos look at some report Examples
ReportsStandard Provider Audit SummarypdfReportsProvider Detailed Sample Reportdocx
ReportsProvider Audit Worksheets - Optionalpdf
Audit Report Examples Non Automated Solution
Error Findings by Volume Percentage
CPT Coded Accurately
8 8 Overcoded
8 8 Undercoded
Missed CPTHCPCS Code
Missed or Wrong Modifier
8 8 Incorrect CPT (or Category) Used
Incorrect ICD-9 Codes
8 8 Incorrect Quantity
Inadequate Documentation
Missing Documentation 8 8
Signature Illegible (No Log)
8 8
CLIENT NAME PROJECT TITLE
Review Line Item Detail Prepared Month Year
DRAFT
Client Claim Demographics Client Charge Data Review Result EampM ONLY Findings C C C C C C O OC O O O
Char
t Num
ber
Au
dit D
ate
Audi
tor (
initi
als)
QA
Initi
als
Fa
cilit
y Lo
catio
n Re
porte
d
Pr
ovid
er N
ame
Pa
tient
Nam
e
M
edic
al R
ecor
d Nu
mbe
r
Prim
ary
Carr
ier M
edica
re=
A M
edica
id =
B O
ther
=O
Da
te o
f Ser
vice
CP
T Co
de
Mod
ifier
(s) i
n or
der
Qua
ntity
Diag
nosi
s Co
de(s
) 1
thro
ugh
4
Fe
e ch
arge
d
Pr
imar
y Pa
ymen
t Am
ount
CPT
Code
Mod
ifier
(s) i
n or
der
Qua
ntity
Diag
nosi
s Co
de(s
) 1
thro
ugh
4
CO
RREC
T AL
LOW
ABLE
Prim
ary
PAYM
ENT
Va
rianc
e
Chie
f Com
plai
nt
Hist
ory
Leve
l Sup
port
ed
Exam
Lev
el S
uppo
rted
Med
ical
Dec
Mak
ing
Supp
orte
d (o
r TIM
E)
CPT
Cod
ed A
ccur
atel
y
Ove
rcod
ed
Und
erco
ded
Mis
sed
CPT
HC
PCS
Cod
e
Mis
sed
or W
rong
Mod
ifier
Inco
rrec
t CPT
(or C
ateg
ory)
Use
d
Inco
rrec
t IC
D-9
Cod
es
Inco
rrec
t Qua
ntity
Inad
equa
te D
ocum
enta
tion
Mis
sing
Doc
umen
tatio
n
Sign
atur
e Ill
egib
le (N
o Lo
g)
No
Sign
atur
e by
Pro
vide
r of
Ser
vice
COMMENTS (abbreviations used) PF- PROBLEM FOCUSED EPF- EXPANDED PF DET- DETAILED COMP- COMPREHENSIVE SFWD- STRAIGHT FORWARD MOD- MODERATE MDM- MEDICAL DECISION MAKING
Char
t Num
ber
SAMPLE SAMPLE S MD SAMPLE SAMPLE XXXXX XXX 112001 99212 25 1 1 1234 2 5678 3 4
$30000 $2200 99212 25 1 1 1234 2 5678 3 4
$56400 $54200 YES
DET
CO
MP
MO
D
COMMENTS COMMENTS COMMENTS
0
1 2 3 4
1 2 3 4
$000 0
$30000 $2200 $56400 $54200 10 10 10 10 10 10 10 10 10 10 10 10 TOTALS 917 Error Rate by Volume
Error Findings by Volume 8 CPT Coded Accurately 8 Overcoded 8 Undercoded 8 Missed CPTHCPCS Code 8 Missed or Wrong Modifier 8 Incorrect CPT (or Category) Used 8 Incorrect ICD-9 Codes 8 Incorrect Quantity
Inadequate Documentation 8 8 Missing Documentation 8 Signature Illegible (No Log) 8 No Signature by Provider of Service
1200 Total
Net Payment Error Rate -24636
Primary Payments Total $ Audited Payment Total $ (Total Under Payments)
Total Over Payments
Net OverUnder Payment $
2200 56400
(54200)
Resources Used HCPCS and CPT CodeBook (Current or applilcable year) ICD-10-CM CodeBook (Current or applicable year) CMS 1995 and 1997 EM Guidelines CMS Claims Processing Manual 100-04 Medicare Claims Processing (PUB 100-04) CMS - National Coverage Determinations (NCDs) National Correct Coding Policy Manual Applicable Physician Version
Executive Summary Report
The executive summary provides readers with a short complete document highlighting import information included in the detailed report Executive summaries are created for the senior management readers that donrsquot have time to read the full report and need to walk away with an understanding of the issues and corrective actions
Some would say the executive summary could be written before the detailed report however it is difficult to make sure the most important elements are included until you have spent time reviewing the detail If you want to make sure the most important messages are in the executive
summary this step should be completed after the detail is written As auditors become more seasoned this step could move to the front of the process
Executive Summary Report Structure of the ES Report
o Backgroundndash Specialtyndash Providersndash Sample Selection sizendash Date range of audit
o Audit Scopeo Regulatory Resourceso Type of Medical records reviewedo Overall Accuracy (all providers)o Detailed Audit Findings
ndash Business Impactndash Summary of Findings
o Department Findingso Summary
o ReportsStandard Executive Summary Professional Servicespdf
Department Findings Top Issues
Date ofServiceErrors
MissingDocuments
Missing orInvalid
Signature
TeachingPhysician
Errors
InsufficientConsultation
Documents
OverCoding
EMBundled
IntoGlobal
SurgicalPackage
SplitSharedServiceError
Incorrector
MissingPricing
Modifier
ICD-10Errors
Family Practice
CardiologyInternal Medicine
TOTALS
Top Findings by Provider
E amp M Accuracy Rates
ICD-10-CM Accuracy Rates
Procedure Accuracy Rates
Inpatient DRG Audit Report
TABLE OF CONTENTS
Executive Summaryo Scope of Work
Reimbursement Changes Department Results
o InpatientGeneral Recommendations and Comments
o Secondary DiagnosesoProcedure CodingoPresent on AdmissionoQueries
Scope of WorkCodingAID performed coding audit review of 175 inpatient records The review completed was a random sample that included cases coded by twenty coders for dates of service from May 2016 ndash July 2016
The objective was to determine if the medical record documentation supported the following coding and documentation requirements and any other regulatory requirement for that code set Criteria reviewed
1 ICD-10-CM Official Coding Guidelines for accurate diagnosis code reporting 2 ICD-10-PCS Official Coding Guidelines for accurate procedure code reporting 3 Documentation of procedure compared to the CPT code assigned 4 Identify opportunities for education and training 5 Financial impact of current coding practices
The regulatory agencies and reference materials relied upon include the following in addition to Medicare and Medicaid regulations Additional resources are located in the sub sections below
bull ICD-10-CM and ICD-10-PCS for Hospitals current volume bull Centers for Medicare and Medicaid Services CMS NCCI Edits-Centers for Medicaid and
Medicare Services CMS website wwwcmsgov bull AHA Coding Clinic
The following electronic medical record documents were reviewed and relied upon to compare to the actual codes submitted to the third party payer
bull Discharge summaries HampPs Progress Notes and other provider notes located in the EMR Records
bull Patient History Forms Ancillary Staff Notes bull Procedure Notes bull Orders bull Diagnostic Report
Reimbursement Changes
Coder Acct
Billed Audited
Reimbursement ChangesMS DRG SOI ROM Weight Expected
Payment MS DRG SOI ROM Weight Expected Payment
Coder 1 001 790 52300 $2615000 792 21552 $1077600 -$1537400
Coder 2002
749 26452 $1322600 758 10090 $504500 -$818100
Coder 3 003 669 13111 $655550 694 07294 $364700 -$290850
Coder 4 004 389 08707 $435350 394 09502 $475100 $39750
Coder 5 005 312 07630 $381500 812 08572 $428600 $47100
Coder 6 006 384 08481 $424050 378 09949 $497450 $73400
Coder 7 007 206 08164 $408200 794 12987 $649350 $241150
Coder 8008
344 31029 $1551450 853 51334 $2566700 $1015250
TOTAL $7793700 $6564000 -$1229700
General Recommendations and CommentsFinding Pertinent secondary diagnoses are not coded and diagnoses are code which are not supported in provider documentation Code only those diagnoses which are documented by the provider on the current chart Not all codes are coded to the highest degree of specificity and combination codes were sometimes missed
Recommendation It is important to assign codes for all conditions which meet the definition of a reportable diagnosis Documentation from all providers should be used including but not limited to radiologists pathologists anesthesiologists CRNAs and FNPs
Reference Coding Clinic Official Coding Guidelines
bull Report all secondary diagnoses which meet the definition of a secondary diagnosis which is defined as all conditions that coexist at the time of admission that develop subsequently or that affect the treatment received andor the length of stay Codes which enhance the overall picture of the patientrsquos visit should be added
o Add T45515A to report adverse effect of Coumadin which caused the GI bleed
o Add I2690 for septic pulmonary emboli (MCCSOI4ROM4)
o Add N179 for acute kidney failure (S3M2CC) per the nephrology consult and the 628 progress note
o Add code I429 cardiomyopathy per HampP
o Add B964 to report proteus in a UTI per the 620 hospitalist progress note
o Code for D649 anemia and I701 stenosis of renal artery should be added as secondary diagnoses per the HampP
bull Only report diagnoses which are substantiated by provider documentation in the current chart notes If a suspected condition is not verified at discharge on an inpatient account it cannot be coded
o Remove G4734 (idiopathic sleep related non-obstructive alveolar hypoventilation) as patient was noted to have the sleep study and the hypoventilation was shown to be a possibility but not noted as such on discharge
o Remove G629 (S21) the neuropathy is documented as due to diabetes
o Remove K529 colitis noted on HP as possible but not further noted or confirmed at discharge
Procedure CodingFinding Procedures were sometimes coded incorrectly
Recommendation The entire medical record should be reviewed and all procedures coded as documented Coding procedures incorrectly or assigning incorrect CPT codes may result in lost revenue
bull Incorrect root operation
o Revise principal procedure to 0DQ68ZZ for clipping of the ulcer per OP report clipping is root operation repair
bull Biopsy versus Excision
o Procedure 0DBA0ZX (biopsy of jejunum) should change to 0DBA0ZZ (excision of jejunum) per op note this was not a biopsy procedure
bull Coding Guideline error
o Remove 0RG10K0 for allograft due to being inclusive in principal procedure
o Remove codes for adhesiolysis 0DN80ZZ 0UN10ZZ and 0UN90ZZ due to no significance noted per OP report
bull Incorrect approach
o Revise 0TF63ZZ (fragmentation percutaneous approach) to 0TF68ZZ (fragmentation endoscopic) for procedure performed via scope per the operative report
bull Procedure coded without provider documentation
o Remove secondary procedure of excisional debridement (0JB90ZZ) due to lack of documentation of excisional debridement per operative report The header in the operative report documents IampD and debridement but the body of the operative report only documents an IampD
bull Incorrect CPT code assignment
o Post-op note supports the nerve block injections of four nerves therefore code 64421 (multiple nerve block) should replace 64420 (injection of one intercostal nerve)
Queries Finding Conflicting incomplete and vague documentation is found within provider chart notes
Recommendation Prior to code assignment if the coder finds ambiguous or conflicting documentation the provider should be queried
Reference AHA Coding Clinic 2002 2nd Quarter pages 17-18
bull Query for acute blood loss anemia since hgb has dropped and patient is being transfused PRBC
bull Recommend query to clarify if cardiorenal syndrome is current as it is documented per 627 nephrology consult but unclear if current
bull Documentation does not support SIRS noninfectious without organ failure It is conflicting since patient has respiratory failure Query should be initiated for clarification with or without organ failure or infectious or non-infectious Patient has pneumonia per query as well as last progress note therefore if SIRS is not further specified per query PNA should be sequenced as principal diagnosis and SIRS should be removed
bull Recommend provider query necrotizing lung consolidation noted on DS as principal diagnosis-unclear does the patient have lobar pneumonia Secondary dx states necrotic pneumonia which is coded as principal diagnosis-this diagnosis is clear but consolidation portion is unclear
bull Recommend query for preterm labor delivery at 301 weeks
bull RECOMMEND QUERY no chest pain on admit per ER and HP cardiology provider states no CP with ER stating chest pressure the day prior to admit Appears patient was admitted due to elevated troponins which cardiology says are likely due to hypotension and AKI DS states chest pain but also says bradycardia and hypotension were the reason for admit
bull RECOMMEND QUERY no chest pain on admit per ER and HP cardiology provider states no CP with ER stating chest pressure the day prior to admit Appears patient was admitted due to elevated troponins which cardiology says are likely due to hypotension and AKI DS states chest pain but also says bradycardia and hypotension were the reason for admit
bull Query the provider regarding pathology report notation of endometriosis andor possible re-sequence of stenosis as principal diagnosis as it also meets principal diagnosis guidelines This would result in an MS-DRG change to 742 and APR-DRG change to 513
bull QUERY secondary diagnosis MCC and ROM 4 code T3166 (60 TBSA of which 60 are third degree burns) Chart notes do not specify how much of TBSA was actually third degree If after query TBSA is found to be less than 50 (T3164) then ROM will change from 4 to 3 but no change to overall APR-DRG or weight
Auditor Quality amp Productivity
Audit Productivity Standards
It takes twice as long to audit a chart as it does to code it a statistic that takes into account the time to document an explanation of any coding decision the auditor is not in agreement with o For example in an emergency department audit with a productivity of 12
charts per hour for a coder our auditors would probably be able to review six per hour
o If there are multiple services to audit on each encounter the productivity may only be 4 per hour
o The amount of detail you put into your audit report will also be a factorndash Are you using an automated audit softwarendash Are you using a spreadsheet to auditndash How many Systems are needed to complete the audit
Coder Quality Audits
Quality Audits (QA) should be done on your coders and auditors regularly Frequent reviews with smaller sample size will allow more consistent
review and feedbacko Example 10 charts per month per coder if the coder passes 2-3 months
consecutively with 95 or better score move them to quarterly reviewso Some QA programs review a percentage of the coders work This
methodology requires more time and resources
Auditor QA should also score and comment on the accuracy of the audit comments and recommendations
Presenting the Audit Results
Presenting the Audit Results
Communicating the Audit FindingsoWho requested the AuditoWho are you reporting the finding to
ndash CEOndash CFOndash Physicianndash Revenue Cycle Managerndash HIM Directorndash Billing Managerndash Coding Manager
ReportsAudit Resultspptx
Post Audit Education
Provider Education
Provider Education is best received when it is specific to the provider(s) 11 sessions going over the audit result Look at their notes with them
oHighlight areas for documentation improvementoReinforce Coding Guidelines that are specific to themoAsk them to share how they establish their LOS for E amp M serviceso Integrate their EMR system into the training
Provider Education
Group Training SessionsoUse the audit results to identify common issues within a specialty group
ndash Refer to the Executive Summary reportoVery effective for identifying system issues
ndash Teaching Attestationsndash Templatesndash Copy and Pastendash Cloned notes
o Everyone hears the same messagesoAn Issue may not appear on the individual audit but is still a concern for the
group
Education Delivery
In person or remote sessionso Factors to consider
ndash Providers scheduleavailabilityndash Location(s)ndash Personality of the providerndash Budget
Coder Education
Coders do well in group training so they can learn from each other 11 training allows the coder to get feedback on their coding
Handling Audit Disputes
Handling Audit Disputes
Be open to all points of viewo Let the documentation tell the story
Refer to the guidelines Ask
oCan we defend the reported service with the current documentation
Self Disclosures Refunds and Corrected Billing
Overpayment
In general If a person has received an overpayment the person shallo report and return the overpayment to the Secretary the State an
intermediary a carrier or a contractor as appropriate at the correct address and ndash notify the Secretary State intermediary carrier or contractor to whom the overpayment was returned in writing of the reason for the overpayment
What is an ldquoOverpaymentrdquo ndash The term ldquooverpaymentrdquo means any funds that a person receives or retains under subchapter XVIII or XIX of this chapter to which the person after applicable reconciliation is not entitled under such subchapter
Self Disclosure
The Office of Inspector General (OIG) has several self-disclosure processes that can be used to report potential fraud in Department of Health and Human Services (HHS) programs Choose the one that applies to you from the following descriptions to learn moreo Health Care Provider Self-Disclosures
ndash Health care providers suppliers or other individuals or entities subject to Civil Monetary Penalties can use the Provider Self-Disclosure Protocol which was created in 1998 to voluntarily disclose self-discovered evidence of potential fraud Self-disclosure gives providers the opportunity to avoid the costs and disruptions associated with a Government-directed investigation and civil or administrative litigation Visit the Provider Self-Disclosure Protocol webpage for more information
o HHS Contractor Self-Disclosuresndash Contractors are individuals businesses or other legal entities that are awarded Government contracts or
subcontracts to provide services to the Department of Health and Human Services (HHS) OIGs contractor self-disclosure program enables contractors to self-disclose potential violations of the False Claims Act and various Federal criminal laws involving fraud conflict of interest bribery or gratuity This self-disclosure process is available for those entities with a Federal Acquisition Regulation-based contract Visit the Contractor Self-Disclosure webpage for more information
o HHS Grantee Self-Disclosuresndash HHS grantees or subrecipients may voluntarily disclose evidence of potential violations of Federal criminal law
involving fraud bribery or gratuity violations potentially affecting the Federal award 45 CFR 75113 notes mandatory disclosures of criminal offenses that non-Federal entities must make with respect to HHS grants Recipients submitting disclosures in connection with this requirement should include the subject reference line Mandatory Grant Disclosure Recipients choosing to disclose conduct that may not fit squarely within the scope of offenses described in 45 CFR 75113 should include the following subject reference line in the submission Voluntary Grant Disclosure
Medicare 60 day rule
The 60 Day Rule (Medicare Parts A amp B) o The 60 day time period for reportingreturning begins when either
ndash The reasonable diligence is completed orndash On the day the provider received credible information of a potential overpayment (if the
provider fails to conduct reasonable diligence) o For an investigation to be conducted in a ldquotimelyrdquo manner providers typically
must complete the investigation within 6 months from receipt of credible information indicating there may be an overpayment
ndash ndash 6-month timeframe may potentially be extended under ldquoextraordinary circumstancesrdquo ndash 8 months generally the maximum total time to return overpayments The government recommends that providers maintain records documenting ldquoreasonable diligencerdquo
Medicare 60 Day Rule
Six-year lookback period ndash Sometimes possible to use a shorter period depending on the facts at issue Amount to be repaid ndash May vary depending on the method used to
reportreturn eg Medicare administrative contractor (ldquoMACrdquo) v self-disclosure Overpayment notification ndash After receiving an overpayment
notification from the government you should investigate for related overpayments eg other time periods
Medicare 60 Day Rule
Self-disclosure protocols ndashoA submission to the OIG or CMS protocols suspends the 60 day requirement
for returning overpayments until a settlement agreement is executed ndash ndash OIGrsquos Self-Disclosure Protocol (SDP) ndash ndash CMS Voluntary Self-Referral Disclosure Protocol (SRDP) ndash
o Self-disclosures to other agencies do not suspend the repayment deadlinendash ndash Eg Department of Justice local US Attorneyrsquos Office Medicaid Fraud Control Unit
Medicare 60 Day Rule
Facilitating Compliance With the 60 Day Rule Compliance programs should include o ndash Appropriate policies and procedures o ndash Periodic billing and coding audits to proactively identify overpaymentso ndash Focus on high-risk areas o ndash Utilization of publicly available government resources to guide audit efforts o ndash Investigating any suspected incidents of non-compliance with federal health
care program requirements
Self Disclosure
Choice of AgencyoOIG ndash Self-Disclosure Protocol
ndash ndash Conduct involving false billingndash ndash Conduct involving excluded personsndash ndash Conduct involving the Anti-Kickback Statute (including conduct thatndash violates both the AKS and Stark Law)
oCMS ndash Self-Referral Disclosure Protocolndash ndash Conduct involving only violations of the Stark Law
oDOJndash ndash May be appropriate when provider believes a FCA release is necessary
Summary
The Cost of a Well-Executed Coding Audit ProcessThe costs associated with an auditing program are worth it in the long run Ideally your organization is performing audits on a regular basis across all service types locations and payers Weve all seen claims that have been denied resulting in additional work that may be preventable with a proper audit program The goal is to use the audit feedback to improve coding quality and lower potential risk and cost to the organization Organizations should be investing in an effective coding audit program to make your coders and providers better and enhance documentation improvement from the providers
Questions
Thank you for your attentionLynn Handy
Vice President of Coding amp Audit ServicesLynnhandymanagedresourcesinccom

Coding Guidelines
Coding Guidelines
Standardized Coding Guidelines is criticaloCPT Guidelineso ICD-10 GuidelinesoCMS Guidelines
ndash Follow your Medicare Carriers GuidelinesoCCI GuidelinesEditsoMedicaidMedi-Cal Guidelineso Internal Guidelines that define
ndash Gray areas of codingndash Payer specific guidelines
Coding Guidelines
E amp M Guidelineso95 or 97oDefine the 95 detailed examo Is ldquonon contributoryrdquo allowedo2 out of 3 key components (Is MDM required)
Coding Guidelines
Other Risk AreasoMedical Necessityo Teaching Physician Guidelineso Incident To o SplitSharedoCopy amp PasteCloned noteso Scribeso SignatureAuthenticationsoOrders for diagnostic servicesoDate of ServiceoNew versus Established CodesoConsultations
Audit Reports
Goals of the Audit Report
The main goal of an audit report is to communicate where the organization specialty department provider or coder does or does not conform to regulatory standards guidelines and organizational policieso Each identified issue must have a standard it is measured againsto Site the regulation in your audit report or include a link to the regulation
Audit reports should not just contain negative findings Outline the Positives also Identify opportunities for improvement this can be in the form of a
recommendation Prioritize High Risk Findings
Who will be reading the Audit Report
What is the technical knowledge of the readeroCodersHIM ProfessionalsoProvidersoClinical StaffoHIM DirectorsoBillingCoding DirectorsManagersoCEOCFO (Executive Team)
Audit Report Format Tips
Provide perspective for the readero Positive and Negative findings
Be precise avoid redundant phrasing inexact terminology Avoid long sentences when a shorter one will work Avoid stating your opinion State the findings and facts Use bullet points this helps to break up difficult information and makes it
clearer for the reader Use gender neutral terms Avoid audit ldquobuzzwordsrdquo such as ldquogenerally improvedrdquo or ldquosignificant riskrdquo Avoid abbreviations unless they are clearly defined
Benefits of Automating your Audit Reports Results
o Consistent Resultso Better Datao Increases Efficiency
Trackingo Allows audit results to be tracked by provider and by specialty
QAo Allows for an automated approach to your internal quality reviews
Trendingo Allows for data analysis at a detailed level that can be tracked
Productivityo Increases auditor productivityo Decreases re-work
ProviderCoder Audit Reports
Detailed Audit reports should have the ability to be sorted byoProvideroCodero Specialty or GroupoAudit Date
Detailed results for each encounteroMeaningful comments
Key Findingso From all encounters
Recommendations and Resources
Detailed Findings Patient ID Patient Name DOS Payer CPT Reported CPT Audited EM Level Key Component ICD Reported ICD Reported Description ICD Audited ICD Reported Description
1 001 Patient A 02-19-16 Blue Cross
99203 25 1 99202 1 +1 D E L 1 S92302A2 Not Reported
1 Fracture of unspecified metatarsal bone(s) left foot initial encounter for closed fracture
1 S92355D2 W109XXD
1 Nondisplaced fracture of fifth metatarsal bone left foot subsequent encounter for fracture with routine healing2 Fall (on) (from) unspecified stairs and steps subsequent encounter
1 The documentation supports coding for an EM service that is one level below the billed code2 Lacking Exam documentation to support the EM level selected3 1997 MSK exam supports an Expanded Problem Focused exam (99202) 1995 exam supports a Detailed exam (99203)4 1997 Exam template suggestions Neurologic Exam-suggest adding the body part examined (upper extremitylow extremity) Dermatologic Exam-unable to determine if this was performed This should be deleted from the final note if
not examined5 EM time statement is insufficient documentation is lacking a required element total time of visit and counseling time greater than 506 CPT disallowed documentation is not present within the medical record to support the CPT code billed (28485-open treatment of metatarsal fracture includes internal fixation when performed) Fracture care is not supported patient
was seen in the ER 6 weeksrsquo prior ER doctor initiated treatment7 The incorrect pricing modifier was billed Removed modifier 25 (separate and significant EM on the same day as a minor procedure) Fracture care is not billable no modifier needed on EM service8 Diagnosis billed is not the most specific available according to the medical record documentation9 Documentation supports an additional diagnosis code not billed
2 002 Patient B 02-05-16 Blue Cross
99203 25 1 99202 25 1 +1 D E L 1 L03032 1 Cellulitis of left toe 1 L03032 1 Cellulitis of left toe
1 The documentation supports coding for an EM service that is one level below the billed code2 Lacking Exam documentation to support the EM level selected3 1997 MSK exam supports an Expanded Problem Focused exam (99202) 1995 exam supports a Detailed exam (99203)4 EM time statement is insufficient documentation is lacking one or more required elements (total time counseling time greater than 50) If a procedure is performed during a visit the time spent performing the procedure needs to be
carved out of the total visit time5 Allowed modifier 25 due to commercial payer Medicare and NCCI do not require modifier 25 on a new patient EM when a minor procedure is performed the same day 6 Diagnosis supported
Detailed Findings
135 822012 New Consultations - Office
Consultations Detailed Detailed (95) Moderate 99244 99243 1 $3500 N
Provider Code 99244 Reviewer Code 99243 Provider Diagnosis 1 3005 NEURASTHENIA Reviewer Diagnosis 1 3005 NEURASTHENIA Provider Diagnosis 2 7282 MUSC DISUSE ATROPHY NEC Reviewer Diagnosis 2 7282 MUSC DISUSE ATROPHY NEC
bull Assessment (I) The assessment is not clearly stated for this encounter Documentation Guidelines states The documentation for each patient encounter should include assessment clinical impression or diagnosis bull Assessment (R) The assessment should be clearly documented for each encounter Since each note must stand alone it is imperative to accurately document the most specific diagnosis in the assessment impression section of the note
bull Documented Lower Level (I) The documentation substantiates a lower level of service than charged
Chart Level Comments
Group your comments in categoriesoDocumentationo E amp MoProceduresoModifierso ICD-10-CM
oReportsAudit Manager Macros 061218 (version 1)xlsx
Recommendations and ReferencesCategory Short Description Long Description
EM AdmissionDischarge Same Day Review the CMS AdmissionDischarge same day coding guidelines httpswwwcmsgovRegulations-and-GuidanceGuidanceManualsDownloadsclm104c12pdf
EM ConsultationReview the consultation guidelines located in the CPT book
EM Consultation not billable to Medicare CMS no longer recognizes the consultation codeshttpswwwcmsgovOutreach-and-EducationMedicare-Learning-Network-MLNMLNMattersArticlesdownloadsmm6740pdf
EM Critical CareReview the CMS Critical Care guidelines httpswwwcmsgovOutreach-and-EducationMedicare-Learning-Network-MLNMLNMattersArticlesdownloadsmm5993pdf
EM Discharge ServicesReview the CMS Hospital Discharge Services guidelineshttpswwwcmsgovOutreach-and-EducationMedicare-Learning-Network-MLNMLNMattersArticlesdownloadsmm5794pdf
EMEM and Preventive Visit Review AAPC guidance for documenting and billing an EM and Preventive visit same day httpswwwaapccomblog22580-successfully-bill-a-
preventive-service-with-a-sick-visit
EM EM documentation guidelines Review the CMS 1995 amp 1997 EM documentation guidelineshttpswwwcmsgovOutreach-and-EducationMedicare-Learning-Network-MLNMLNEdWebGuideEMDOChtml
EM EM Inpatient vs Outpatient Review the patientrsquos status on the hospital admission order to determine the appropriate EM category to bill (inpatient vs observation)
EM EM New vs EstablishedReview the CMS New vs Established patient guidelines httpswwwcmsgovOutreach-and-EducationMedicare-Learning-Network-MLNMLNProductsDownloadseval-mgmt-serv-guide-ICN006764pdf
EMEM Time billing suggestion
Recommend a time statement is added to the EM medical record when a majority of the visit is spent counseling andor coordination of care Review the CMS 1995 amp 1997 EM documentation guidelines for EM time documentationhttpswwwcmsgovOutreach-and-EducationMedicare-Learning-Network-MLNMLNEdWebGuideEMDOChtml
EM Inpatient hospital servicesReview the CMS Hospital Services (Initial and Subsequent) guidelines httpswwwcmsgovRegulations-and-GuidanceGuidanceManualsDownloadsclm104c12pdf
EM Nursing Facility Services Review the Nursing Facility Services guidelines provided by CMS The guidelines can be downloaded at this linkhttpswwwcmsgovRegulations-and-GuidanceGuidanceManualsDownloadsclm104c12pdf
EM Observation Services Review the CMS Observation Services (Initial and Subsequent) guidelines httpswwwcmsgovRegulations-and-GuidanceGuidanceManualsDownloadsclm104c12pdf
EM Prolonged Services Review the CMS Prolonged Services guidelines httpswwwcmsgovOutreach-and-EducationMedicare-Learning-Network-MLNMLNMattersArticlesdownloadsmm5972pdf
EMReview of Systems Review the CMS 1995 amp 1997 EM documentation guidelines for Review of Systems requirements
httpswwwcmsgovOutreach-and-EducationMedicare-Learning-Network-MLNMLNEdWebGuideEMDOChtml
EMConsultation Documentation Suggestion
Recommend adding verbiage to consultation documentation that indicates the name of the referring provider and the reason for the consultation
Audit Report Examples Automated Solution
Letrsquos look at some report Examples
ReportsStandard Provider Audit SummarypdfReportsProvider Detailed Sample Reportdocx
ReportsProvider Audit Worksheets - Optionalpdf
Audit Report Examples Non Automated Solution
Error Findings by Volume Percentage
CPT Coded Accurately
8 8 Overcoded
8 8 Undercoded
Missed CPTHCPCS Code
Missed or Wrong Modifier
8 8 Incorrect CPT (or Category) Used
Incorrect ICD-9 Codes
8 8 Incorrect Quantity
Inadequate Documentation
Missing Documentation 8 8
Signature Illegible (No Log)
8 8
CLIENT NAME PROJECT TITLE
Review Line Item Detail Prepared Month Year
DRAFT
Client Claim Demographics Client Charge Data Review Result EampM ONLY Findings C C C C C C O OC O O O
Char
t Num
ber
Au
dit D
ate
Audi
tor (
initi
als)
QA
Initi
als
Fa
cilit
y Lo
catio
n Re
porte
d
Pr
ovid
er N
ame
Pa
tient
Nam
e
M
edic
al R
ecor
d Nu
mbe
r
Prim
ary
Carr
ier M
edica
re=
A M
edica
id =
B O
ther
=O
Da
te o
f Ser
vice
CP
T Co
de
Mod
ifier
(s) i
n or
der
Qua
ntity
Diag
nosi
s Co
de(s
) 1
thro
ugh
4
Fe
e ch
arge
d
Pr
imar
y Pa
ymen
t Am
ount
CPT
Code
Mod
ifier
(s) i
n or
der
Qua
ntity
Diag
nosi
s Co
de(s
) 1
thro
ugh
4
CO
RREC
T AL
LOW
ABLE
Prim
ary
PAYM
ENT
Va
rianc
e
Chie
f Com
plai
nt
Hist
ory
Leve
l Sup
port
ed
Exam
Lev
el S
uppo
rted
Med
ical
Dec
Mak
ing
Supp
orte
d (o
r TIM
E)
CPT
Cod
ed A
ccur
atel
y
Ove
rcod
ed
Und
erco
ded
Mis
sed
CPT
HC
PCS
Cod
e
Mis
sed
or W
rong
Mod
ifier
Inco
rrec
t CPT
(or C
ateg
ory)
Use
d
Inco
rrec
t IC
D-9
Cod
es
Inco
rrec
t Qua
ntity
Inad
equa
te D
ocum
enta
tion
Mis
sing
Doc
umen
tatio
n
Sign
atur
e Ill
egib
le (N
o Lo
g)
No
Sign
atur
e by
Pro
vide
r of
Ser
vice
COMMENTS (abbreviations used) PF- PROBLEM FOCUSED EPF- EXPANDED PF DET- DETAILED COMP- COMPREHENSIVE SFWD- STRAIGHT FORWARD MOD- MODERATE MDM- MEDICAL DECISION MAKING
Char
t Num
ber
SAMPLE SAMPLE S MD SAMPLE SAMPLE XXXXX XXX 112001 99212 25 1 1 1234 2 5678 3 4
$30000 $2200 99212 25 1 1 1234 2 5678 3 4
$56400 $54200 YES
DET
CO
MP
MO
D
COMMENTS COMMENTS COMMENTS
0
1 2 3 4
1 2 3 4
$000 0
$30000 $2200 $56400 $54200 10 10 10 10 10 10 10 10 10 10 10 10 TOTALS 917 Error Rate by Volume
Error Findings by Volume 8 CPT Coded Accurately 8 Overcoded 8 Undercoded 8 Missed CPTHCPCS Code 8 Missed or Wrong Modifier 8 Incorrect CPT (or Category) Used 8 Incorrect ICD-9 Codes 8 Incorrect Quantity
Inadequate Documentation 8 8 Missing Documentation 8 Signature Illegible (No Log) 8 No Signature by Provider of Service
1200 Total
Net Payment Error Rate -24636
Primary Payments Total $ Audited Payment Total $ (Total Under Payments)
Total Over Payments
Net OverUnder Payment $
2200 56400
(54200)
Resources Used HCPCS and CPT CodeBook (Current or applilcable year) ICD-10-CM CodeBook (Current or applicable year) CMS 1995 and 1997 EM Guidelines CMS Claims Processing Manual 100-04 Medicare Claims Processing (PUB 100-04) CMS - National Coverage Determinations (NCDs) National Correct Coding Policy Manual Applicable Physician Version
Executive Summary Report
The executive summary provides readers with a short complete document highlighting import information included in the detailed report Executive summaries are created for the senior management readers that donrsquot have time to read the full report and need to walk away with an understanding of the issues and corrective actions
Some would say the executive summary could be written before the detailed report however it is difficult to make sure the most important elements are included until you have spent time reviewing the detail If you want to make sure the most important messages are in the executive
summary this step should be completed after the detail is written As auditors become more seasoned this step could move to the front of the process
Executive Summary Report Structure of the ES Report
o Backgroundndash Specialtyndash Providersndash Sample Selection sizendash Date range of audit
o Audit Scopeo Regulatory Resourceso Type of Medical records reviewedo Overall Accuracy (all providers)o Detailed Audit Findings
ndash Business Impactndash Summary of Findings
o Department Findingso Summary
o ReportsStandard Executive Summary Professional Servicespdf
Department Findings Top Issues
Date ofServiceErrors
MissingDocuments
Missing orInvalid
Signature
TeachingPhysician
Errors
InsufficientConsultation
Documents
OverCoding
EMBundled
IntoGlobal
SurgicalPackage
SplitSharedServiceError
Incorrector
MissingPricing
Modifier
ICD-10Errors
Family Practice
CardiologyInternal Medicine
TOTALS
Top Findings by Provider
E amp M Accuracy Rates
ICD-10-CM Accuracy Rates
Procedure Accuracy Rates
Inpatient DRG Audit Report
TABLE OF CONTENTS
Executive Summaryo Scope of Work
Reimbursement Changes Department Results
o InpatientGeneral Recommendations and Comments
o Secondary DiagnosesoProcedure CodingoPresent on AdmissionoQueries
Scope of WorkCodingAID performed coding audit review of 175 inpatient records The review completed was a random sample that included cases coded by twenty coders for dates of service from May 2016 ndash July 2016
The objective was to determine if the medical record documentation supported the following coding and documentation requirements and any other regulatory requirement for that code set Criteria reviewed
1 ICD-10-CM Official Coding Guidelines for accurate diagnosis code reporting 2 ICD-10-PCS Official Coding Guidelines for accurate procedure code reporting 3 Documentation of procedure compared to the CPT code assigned 4 Identify opportunities for education and training 5 Financial impact of current coding practices
The regulatory agencies and reference materials relied upon include the following in addition to Medicare and Medicaid regulations Additional resources are located in the sub sections below
bull ICD-10-CM and ICD-10-PCS for Hospitals current volume bull Centers for Medicare and Medicaid Services CMS NCCI Edits-Centers for Medicaid and
Medicare Services CMS website wwwcmsgov bull AHA Coding Clinic
The following electronic medical record documents were reviewed and relied upon to compare to the actual codes submitted to the third party payer
bull Discharge summaries HampPs Progress Notes and other provider notes located in the EMR Records
bull Patient History Forms Ancillary Staff Notes bull Procedure Notes bull Orders bull Diagnostic Report
Reimbursement Changes
Coder Acct
Billed Audited
Reimbursement ChangesMS DRG SOI ROM Weight Expected
Payment MS DRG SOI ROM Weight Expected Payment
Coder 1 001 790 52300 $2615000 792 21552 $1077600 -$1537400
Coder 2002
749 26452 $1322600 758 10090 $504500 -$818100
Coder 3 003 669 13111 $655550 694 07294 $364700 -$290850
Coder 4 004 389 08707 $435350 394 09502 $475100 $39750
Coder 5 005 312 07630 $381500 812 08572 $428600 $47100
Coder 6 006 384 08481 $424050 378 09949 $497450 $73400
Coder 7 007 206 08164 $408200 794 12987 $649350 $241150
Coder 8008
344 31029 $1551450 853 51334 $2566700 $1015250
TOTAL $7793700 $6564000 -$1229700
General Recommendations and CommentsFinding Pertinent secondary diagnoses are not coded and diagnoses are code which are not supported in provider documentation Code only those diagnoses which are documented by the provider on the current chart Not all codes are coded to the highest degree of specificity and combination codes were sometimes missed
Recommendation It is important to assign codes for all conditions which meet the definition of a reportable diagnosis Documentation from all providers should be used including but not limited to radiologists pathologists anesthesiologists CRNAs and FNPs
Reference Coding Clinic Official Coding Guidelines
bull Report all secondary diagnoses which meet the definition of a secondary diagnosis which is defined as all conditions that coexist at the time of admission that develop subsequently or that affect the treatment received andor the length of stay Codes which enhance the overall picture of the patientrsquos visit should be added
o Add T45515A to report adverse effect of Coumadin which caused the GI bleed
o Add I2690 for septic pulmonary emboli (MCCSOI4ROM4)
o Add N179 for acute kidney failure (S3M2CC) per the nephrology consult and the 628 progress note
o Add code I429 cardiomyopathy per HampP
o Add B964 to report proteus in a UTI per the 620 hospitalist progress note
o Code for D649 anemia and I701 stenosis of renal artery should be added as secondary diagnoses per the HampP
bull Only report diagnoses which are substantiated by provider documentation in the current chart notes If a suspected condition is not verified at discharge on an inpatient account it cannot be coded
o Remove G4734 (idiopathic sleep related non-obstructive alveolar hypoventilation) as patient was noted to have the sleep study and the hypoventilation was shown to be a possibility but not noted as such on discharge
o Remove G629 (S21) the neuropathy is documented as due to diabetes
o Remove K529 colitis noted on HP as possible but not further noted or confirmed at discharge
Procedure CodingFinding Procedures were sometimes coded incorrectly
Recommendation The entire medical record should be reviewed and all procedures coded as documented Coding procedures incorrectly or assigning incorrect CPT codes may result in lost revenue
bull Incorrect root operation
o Revise principal procedure to 0DQ68ZZ for clipping of the ulcer per OP report clipping is root operation repair
bull Biopsy versus Excision
o Procedure 0DBA0ZX (biopsy of jejunum) should change to 0DBA0ZZ (excision of jejunum) per op note this was not a biopsy procedure
bull Coding Guideline error
o Remove 0RG10K0 for allograft due to being inclusive in principal procedure
o Remove codes for adhesiolysis 0DN80ZZ 0UN10ZZ and 0UN90ZZ due to no significance noted per OP report
bull Incorrect approach
o Revise 0TF63ZZ (fragmentation percutaneous approach) to 0TF68ZZ (fragmentation endoscopic) for procedure performed via scope per the operative report
bull Procedure coded without provider documentation
o Remove secondary procedure of excisional debridement (0JB90ZZ) due to lack of documentation of excisional debridement per operative report The header in the operative report documents IampD and debridement but the body of the operative report only documents an IampD
bull Incorrect CPT code assignment
o Post-op note supports the nerve block injections of four nerves therefore code 64421 (multiple nerve block) should replace 64420 (injection of one intercostal nerve)
Queries Finding Conflicting incomplete and vague documentation is found within provider chart notes
Recommendation Prior to code assignment if the coder finds ambiguous or conflicting documentation the provider should be queried
Reference AHA Coding Clinic 2002 2nd Quarter pages 17-18
bull Query for acute blood loss anemia since hgb has dropped and patient is being transfused PRBC
bull Recommend query to clarify if cardiorenal syndrome is current as it is documented per 627 nephrology consult but unclear if current
bull Documentation does not support SIRS noninfectious without organ failure It is conflicting since patient has respiratory failure Query should be initiated for clarification with or without organ failure or infectious or non-infectious Patient has pneumonia per query as well as last progress note therefore if SIRS is not further specified per query PNA should be sequenced as principal diagnosis and SIRS should be removed
bull Recommend provider query necrotizing lung consolidation noted on DS as principal diagnosis-unclear does the patient have lobar pneumonia Secondary dx states necrotic pneumonia which is coded as principal diagnosis-this diagnosis is clear but consolidation portion is unclear
bull Recommend query for preterm labor delivery at 301 weeks
bull RECOMMEND QUERY no chest pain on admit per ER and HP cardiology provider states no CP with ER stating chest pressure the day prior to admit Appears patient was admitted due to elevated troponins which cardiology says are likely due to hypotension and AKI DS states chest pain but also says bradycardia and hypotension were the reason for admit
bull RECOMMEND QUERY no chest pain on admit per ER and HP cardiology provider states no CP with ER stating chest pressure the day prior to admit Appears patient was admitted due to elevated troponins which cardiology says are likely due to hypotension and AKI DS states chest pain but also says bradycardia and hypotension were the reason for admit
bull Query the provider regarding pathology report notation of endometriosis andor possible re-sequence of stenosis as principal diagnosis as it also meets principal diagnosis guidelines This would result in an MS-DRG change to 742 and APR-DRG change to 513
bull QUERY secondary diagnosis MCC and ROM 4 code T3166 (60 TBSA of which 60 are third degree burns) Chart notes do not specify how much of TBSA was actually third degree If after query TBSA is found to be less than 50 (T3164) then ROM will change from 4 to 3 but no change to overall APR-DRG or weight
Auditor Quality amp Productivity
Audit Productivity Standards
It takes twice as long to audit a chart as it does to code it a statistic that takes into account the time to document an explanation of any coding decision the auditor is not in agreement with o For example in an emergency department audit with a productivity of 12
charts per hour for a coder our auditors would probably be able to review six per hour
o If there are multiple services to audit on each encounter the productivity may only be 4 per hour
o The amount of detail you put into your audit report will also be a factorndash Are you using an automated audit softwarendash Are you using a spreadsheet to auditndash How many Systems are needed to complete the audit
Coder Quality Audits
Quality Audits (QA) should be done on your coders and auditors regularly Frequent reviews with smaller sample size will allow more consistent
review and feedbacko Example 10 charts per month per coder if the coder passes 2-3 months
consecutively with 95 or better score move them to quarterly reviewso Some QA programs review a percentage of the coders work This
methodology requires more time and resources
Auditor QA should also score and comment on the accuracy of the audit comments and recommendations
Presenting the Audit Results
Presenting the Audit Results
Communicating the Audit FindingsoWho requested the AuditoWho are you reporting the finding to
ndash CEOndash CFOndash Physicianndash Revenue Cycle Managerndash HIM Directorndash Billing Managerndash Coding Manager
ReportsAudit Resultspptx
Post Audit Education
Provider Education
Provider Education is best received when it is specific to the provider(s) 11 sessions going over the audit result Look at their notes with them
oHighlight areas for documentation improvementoReinforce Coding Guidelines that are specific to themoAsk them to share how they establish their LOS for E amp M serviceso Integrate their EMR system into the training
Provider Education
Group Training SessionsoUse the audit results to identify common issues within a specialty group
ndash Refer to the Executive Summary reportoVery effective for identifying system issues
ndash Teaching Attestationsndash Templatesndash Copy and Pastendash Cloned notes
o Everyone hears the same messagesoAn Issue may not appear on the individual audit but is still a concern for the
group
Education Delivery
In person or remote sessionso Factors to consider
ndash Providers scheduleavailabilityndash Location(s)ndash Personality of the providerndash Budget
Coder Education
Coders do well in group training so they can learn from each other 11 training allows the coder to get feedback on their coding
Handling Audit Disputes
Handling Audit Disputes
Be open to all points of viewo Let the documentation tell the story
Refer to the guidelines Ask
oCan we defend the reported service with the current documentation
Self Disclosures Refunds and Corrected Billing
Overpayment
In general If a person has received an overpayment the person shallo report and return the overpayment to the Secretary the State an
intermediary a carrier or a contractor as appropriate at the correct address and ndash notify the Secretary State intermediary carrier or contractor to whom the overpayment was returned in writing of the reason for the overpayment
What is an ldquoOverpaymentrdquo ndash The term ldquooverpaymentrdquo means any funds that a person receives or retains under subchapter XVIII or XIX of this chapter to which the person after applicable reconciliation is not entitled under such subchapter
Self Disclosure
The Office of Inspector General (OIG) has several self-disclosure processes that can be used to report potential fraud in Department of Health and Human Services (HHS) programs Choose the one that applies to you from the following descriptions to learn moreo Health Care Provider Self-Disclosures
ndash Health care providers suppliers or other individuals or entities subject to Civil Monetary Penalties can use the Provider Self-Disclosure Protocol which was created in 1998 to voluntarily disclose self-discovered evidence of potential fraud Self-disclosure gives providers the opportunity to avoid the costs and disruptions associated with a Government-directed investigation and civil or administrative litigation Visit the Provider Self-Disclosure Protocol webpage for more information
o HHS Contractor Self-Disclosuresndash Contractors are individuals businesses or other legal entities that are awarded Government contracts or
subcontracts to provide services to the Department of Health and Human Services (HHS) OIGs contractor self-disclosure program enables contractors to self-disclose potential violations of the False Claims Act and various Federal criminal laws involving fraud conflict of interest bribery or gratuity This self-disclosure process is available for those entities with a Federal Acquisition Regulation-based contract Visit the Contractor Self-Disclosure webpage for more information
o HHS Grantee Self-Disclosuresndash HHS grantees or subrecipients may voluntarily disclose evidence of potential violations of Federal criminal law
involving fraud bribery or gratuity violations potentially affecting the Federal award 45 CFR 75113 notes mandatory disclosures of criminal offenses that non-Federal entities must make with respect to HHS grants Recipients submitting disclosures in connection with this requirement should include the subject reference line Mandatory Grant Disclosure Recipients choosing to disclose conduct that may not fit squarely within the scope of offenses described in 45 CFR 75113 should include the following subject reference line in the submission Voluntary Grant Disclosure
Medicare 60 day rule
The 60 Day Rule (Medicare Parts A amp B) o The 60 day time period for reportingreturning begins when either
ndash The reasonable diligence is completed orndash On the day the provider received credible information of a potential overpayment (if the
provider fails to conduct reasonable diligence) o For an investigation to be conducted in a ldquotimelyrdquo manner providers typically
must complete the investigation within 6 months from receipt of credible information indicating there may be an overpayment
ndash ndash 6-month timeframe may potentially be extended under ldquoextraordinary circumstancesrdquo ndash 8 months generally the maximum total time to return overpayments The government recommends that providers maintain records documenting ldquoreasonable diligencerdquo
Medicare 60 Day Rule
Six-year lookback period ndash Sometimes possible to use a shorter period depending on the facts at issue Amount to be repaid ndash May vary depending on the method used to
reportreturn eg Medicare administrative contractor (ldquoMACrdquo) v self-disclosure Overpayment notification ndash After receiving an overpayment
notification from the government you should investigate for related overpayments eg other time periods
Medicare 60 Day Rule
Self-disclosure protocols ndashoA submission to the OIG or CMS protocols suspends the 60 day requirement
for returning overpayments until a settlement agreement is executed ndash ndash OIGrsquos Self-Disclosure Protocol (SDP) ndash ndash CMS Voluntary Self-Referral Disclosure Protocol (SRDP) ndash
o Self-disclosures to other agencies do not suspend the repayment deadlinendash ndash Eg Department of Justice local US Attorneyrsquos Office Medicaid Fraud Control Unit
Medicare 60 Day Rule
Facilitating Compliance With the 60 Day Rule Compliance programs should include o ndash Appropriate policies and procedures o ndash Periodic billing and coding audits to proactively identify overpaymentso ndash Focus on high-risk areas o ndash Utilization of publicly available government resources to guide audit efforts o ndash Investigating any suspected incidents of non-compliance with federal health
care program requirements
Self Disclosure
Choice of AgencyoOIG ndash Self-Disclosure Protocol
ndash ndash Conduct involving false billingndash ndash Conduct involving excluded personsndash ndash Conduct involving the Anti-Kickback Statute (including conduct thatndash violates both the AKS and Stark Law)
oCMS ndash Self-Referral Disclosure Protocolndash ndash Conduct involving only violations of the Stark Law
oDOJndash ndash May be appropriate when provider believes a FCA release is necessary
Summary
The Cost of a Well-Executed Coding Audit ProcessThe costs associated with an auditing program are worth it in the long run Ideally your organization is performing audits on a regular basis across all service types locations and payers Weve all seen claims that have been denied resulting in additional work that may be preventable with a proper audit program The goal is to use the audit feedback to improve coding quality and lower potential risk and cost to the organization Organizations should be investing in an effective coding audit program to make your coders and providers better and enhance documentation improvement from the providers
Questions
Thank you for your attentionLynn Handy
Vice President of Coding amp Audit ServicesLynnhandymanagedresourcesinccom

Coding Guidelines
Standardized Coding Guidelines is criticaloCPT Guidelineso ICD-10 GuidelinesoCMS Guidelines
ndash Follow your Medicare Carriers GuidelinesoCCI GuidelinesEditsoMedicaidMedi-Cal Guidelineso Internal Guidelines that define
ndash Gray areas of codingndash Payer specific guidelines
Coding Guidelines
E amp M Guidelineso95 or 97oDefine the 95 detailed examo Is ldquonon contributoryrdquo allowedo2 out of 3 key components (Is MDM required)
Coding Guidelines
Other Risk AreasoMedical Necessityo Teaching Physician Guidelineso Incident To o SplitSharedoCopy amp PasteCloned noteso Scribeso SignatureAuthenticationsoOrders for diagnostic servicesoDate of ServiceoNew versus Established CodesoConsultations
Audit Reports
Goals of the Audit Report
The main goal of an audit report is to communicate where the organization specialty department provider or coder does or does not conform to regulatory standards guidelines and organizational policieso Each identified issue must have a standard it is measured againsto Site the regulation in your audit report or include a link to the regulation
Audit reports should not just contain negative findings Outline the Positives also Identify opportunities for improvement this can be in the form of a
recommendation Prioritize High Risk Findings
Who will be reading the Audit Report
What is the technical knowledge of the readeroCodersHIM ProfessionalsoProvidersoClinical StaffoHIM DirectorsoBillingCoding DirectorsManagersoCEOCFO (Executive Team)
Audit Report Format Tips
Provide perspective for the readero Positive and Negative findings
Be precise avoid redundant phrasing inexact terminology Avoid long sentences when a shorter one will work Avoid stating your opinion State the findings and facts Use bullet points this helps to break up difficult information and makes it
clearer for the reader Use gender neutral terms Avoid audit ldquobuzzwordsrdquo such as ldquogenerally improvedrdquo or ldquosignificant riskrdquo Avoid abbreviations unless they are clearly defined
Benefits of Automating your Audit Reports Results
o Consistent Resultso Better Datao Increases Efficiency
Trackingo Allows audit results to be tracked by provider and by specialty
QAo Allows for an automated approach to your internal quality reviews
Trendingo Allows for data analysis at a detailed level that can be tracked
Productivityo Increases auditor productivityo Decreases re-work
ProviderCoder Audit Reports
Detailed Audit reports should have the ability to be sorted byoProvideroCodero Specialty or GroupoAudit Date
Detailed results for each encounteroMeaningful comments
Key Findingso From all encounters
Recommendations and Resources
Detailed Findings Patient ID Patient Name DOS Payer CPT Reported CPT Audited EM Level Key Component ICD Reported ICD Reported Description ICD Audited ICD Reported Description
1 001 Patient A 02-19-16 Blue Cross
99203 25 1 99202 1 +1 D E L 1 S92302A2 Not Reported
1 Fracture of unspecified metatarsal bone(s) left foot initial encounter for closed fracture
1 S92355D2 W109XXD
1 Nondisplaced fracture of fifth metatarsal bone left foot subsequent encounter for fracture with routine healing2 Fall (on) (from) unspecified stairs and steps subsequent encounter
1 The documentation supports coding for an EM service that is one level below the billed code2 Lacking Exam documentation to support the EM level selected3 1997 MSK exam supports an Expanded Problem Focused exam (99202) 1995 exam supports a Detailed exam (99203)4 1997 Exam template suggestions Neurologic Exam-suggest adding the body part examined (upper extremitylow extremity) Dermatologic Exam-unable to determine if this was performed This should be deleted from the final note if
not examined5 EM time statement is insufficient documentation is lacking a required element total time of visit and counseling time greater than 506 CPT disallowed documentation is not present within the medical record to support the CPT code billed (28485-open treatment of metatarsal fracture includes internal fixation when performed) Fracture care is not supported patient
was seen in the ER 6 weeksrsquo prior ER doctor initiated treatment7 The incorrect pricing modifier was billed Removed modifier 25 (separate and significant EM on the same day as a minor procedure) Fracture care is not billable no modifier needed on EM service8 Diagnosis billed is not the most specific available according to the medical record documentation9 Documentation supports an additional diagnosis code not billed
2 002 Patient B 02-05-16 Blue Cross
99203 25 1 99202 25 1 +1 D E L 1 L03032 1 Cellulitis of left toe 1 L03032 1 Cellulitis of left toe
1 The documentation supports coding for an EM service that is one level below the billed code2 Lacking Exam documentation to support the EM level selected3 1997 MSK exam supports an Expanded Problem Focused exam (99202) 1995 exam supports a Detailed exam (99203)4 EM time statement is insufficient documentation is lacking one or more required elements (total time counseling time greater than 50) If a procedure is performed during a visit the time spent performing the procedure needs to be
carved out of the total visit time5 Allowed modifier 25 due to commercial payer Medicare and NCCI do not require modifier 25 on a new patient EM when a minor procedure is performed the same day 6 Diagnosis supported
Detailed Findings
135 822012 New Consultations - Office
Consultations Detailed Detailed (95) Moderate 99244 99243 1 $3500 N
Provider Code 99244 Reviewer Code 99243 Provider Diagnosis 1 3005 NEURASTHENIA Reviewer Diagnosis 1 3005 NEURASTHENIA Provider Diagnosis 2 7282 MUSC DISUSE ATROPHY NEC Reviewer Diagnosis 2 7282 MUSC DISUSE ATROPHY NEC
bull Assessment (I) The assessment is not clearly stated for this encounter Documentation Guidelines states The documentation for each patient encounter should include assessment clinical impression or diagnosis bull Assessment (R) The assessment should be clearly documented for each encounter Since each note must stand alone it is imperative to accurately document the most specific diagnosis in the assessment impression section of the note
bull Documented Lower Level (I) The documentation substantiates a lower level of service than charged
Chart Level Comments
Group your comments in categoriesoDocumentationo E amp MoProceduresoModifierso ICD-10-CM
oReportsAudit Manager Macros 061218 (version 1)xlsx
Recommendations and ReferencesCategory Short Description Long Description
EM AdmissionDischarge Same Day Review the CMS AdmissionDischarge same day coding guidelines httpswwwcmsgovRegulations-and-GuidanceGuidanceManualsDownloadsclm104c12pdf
EM ConsultationReview the consultation guidelines located in the CPT book
EM Consultation not billable to Medicare CMS no longer recognizes the consultation codeshttpswwwcmsgovOutreach-and-EducationMedicare-Learning-Network-MLNMLNMattersArticlesdownloadsmm6740pdf
EM Critical CareReview the CMS Critical Care guidelines httpswwwcmsgovOutreach-and-EducationMedicare-Learning-Network-MLNMLNMattersArticlesdownloadsmm5993pdf
EM Discharge ServicesReview the CMS Hospital Discharge Services guidelineshttpswwwcmsgovOutreach-and-EducationMedicare-Learning-Network-MLNMLNMattersArticlesdownloadsmm5794pdf
EMEM and Preventive Visit Review AAPC guidance for documenting and billing an EM and Preventive visit same day httpswwwaapccomblog22580-successfully-bill-a-
preventive-service-with-a-sick-visit
EM EM documentation guidelines Review the CMS 1995 amp 1997 EM documentation guidelineshttpswwwcmsgovOutreach-and-EducationMedicare-Learning-Network-MLNMLNEdWebGuideEMDOChtml
EM EM Inpatient vs Outpatient Review the patientrsquos status on the hospital admission order to determine the appropriate EM category to bill (inpatient vs observation)
EM EM New vs EstablishedReview the CMS New vs Established patient guidelines httpswwwcmsgovOutreach-and-EducationMedicare-Learning-Network-MLNMLNProductsDownloadseval-mgmt-serv-guide-ICN006764pdf
EMEM Time billing suggestion
Recommend a time statement is added to the EM medical record when a majority of the visit is spent counseling andor coordination of care Review the CMS 1995 amp 1997 EM documentation guidelines for EM time documentationhttpswwwcmsgovOutreach-and-EducationMedicare-Learning-Network-MLNMLNEdWebGuideEMDOChtml
EM Inpatient hospital servicesReview the CMS Hospital Services (Initial and Subsequent) guidelines httpswwwcmsgovRegulations-and-GuidanceGuidanceManualsDownloadsclm104c12pdf
EM Nursing Facility Services Review the Nursing Facility Services guidelines provided by CMS The guidelines can be downloaded at this linkhttpswwwcmsgovRegulations-and-GuidanceGuidanceManualsDownloadsclm104c12pdf
EM Observation Services Review the CMS Observation Services (Initial and Subsequent) guidelines httpswwwcmsgovRegulations-and-GuidanceGuidanceManualsDownloadsclm104c12pdf
EM Prolonged Services Review the CMS Prolonged Services guidelines httpswwwcmsgovOutreach-and-EducationMedicare-Learning-Network-MLNMLNMattersArticlesdownloadsmm5972pdf
EMReview of Systems Review the CMS 1995 amp 1997 EM documentation guidelines for Review of Systems requirements
httpswwwcmsgovOutreach-and-EducationMedicare-Learning-Network-MLNMLNEdWebGuideEMDOChtml
EMConsultation Documentation Suggestion
Recommend adding verbiage to consultation documentation that indicates the name of the referring provider and the reason for the consultation
Audit Report Examples Automated Solution
Letrsquos look at some report Examples
ReportsStandard Provider Audit SummarypdfReportsProvider Detailed Sample Reportdocx
ReportsProvider Audit Worksheets - Optionalpdf
Audit Report Examples Non Automated Solution
Error Findings by Volume Percentage
CPT Coded Accurately
8 8 Overcoded
8 8 Undercoded
Missed CPTHCPCS Code
Missed or Wrong Modifier
8 8 Incorrect CPT (or Category) Used
Incorrect ICD-9 Codes
8 8 Incorrect Quantity
Inadequate Documentation
Missing Documentation 8 8
Signature Illegible (No Log)
8 8
CLIENT NAME PROJECT TITLE
Review Line Item Detail Prepared Month Year
DRAFT
Client Claim Demographics Client Charge Data Review Result EampM ONLY Findings C C C C C C O OC O O O
Char
t Num
ber
Au
dit D
ate
Audi
tor (
initi
als)
QA
Initi
als
Fa
cilit
y Lo
catio
n Re
porte
d
Pr
ovid
er N
ame
Pa
tient
Nam
e
M
edic
al R
ecor
d Nu
mbe
r
Prim
ary
Carr
ier M
edica
re=
A M
edica
id =
B O
ther
=O
Da
te o
f Ser
vice
CP
T Co
de
Mod
ifier
(s) i
n or
der
Qua
ntity
Diag
nosi
s Co
de(s
) 1
thro
ugh
4
Fe
e ch
arge
d
Pr
imar
y Pa
ymen
t Am
ount
CPT
Code
Mod
ifier
(s) i
n or
der
Qua
ntity
Diag
nosi
s Co
de(s
) 1
thro
ugh
4
CO
RREC
T AL
LOW
ABLE
Prim
ary
PAYM
ENT
Va
rianc
e
Chie
f Com
plai
nt
Hist
ory
Leve
l Sup
port
ed
Exam
Lev
el S
uppo
rted
Med
ical
Dec
Mak
ing
Supp
orte
d (o
r TIM
E)
CPT
Cod
ed A
ccur
atel
y
Ove
rcod
ed
Und
erco
ded
Mis
sed
CPT
HC
PCS
Cod
e
Mis
sed
or W
rong
Mod
ifier
Inco
rrec
t CPT
(or C
ateg
ory)
Use
d
Inco
rrec
t IC
D-9
Cod
es
Inco
rrec
t Qua
ntity
Inad
equa
te D
ocum
enta
tion
Mis
sing
Doc
umen
tatio
n
Sign
atur
e Ill
egib
le (N
o Lo
g)
No
Sign
atur
e by
Pro
vide
r of
Ser
vice
COMMENTS (abbreviations used) PF- PROBLEM FOCUSED EPF- EXPANDED PF DET- DETAILED COMP- COMPREHENSIVE SFWD- STRAIGHT FORWARD MOD- MODERATE MDM- MEDICAL DECISION MAKING
Char
t Num
ber
SAMPLE SAMPLE S MD SAMPLE SAMPLE XXXXX XXX 112001 99212 25 1 1 1234 2 5678 3 4
$30000 $2200 99212 25 1 1 1234 2 5678 3 4
$56400 $54200 YES
DET
CO
MP
MO
D
COMMENTS COMMENTS COMMENTS
0
1 2 3 4
1 2 3 4
$000 0
$30000 $2200 $56400 $54200 10 10 10 10 10 10 10 10 10 10 10 10 TOTALS 917 Error Rate by Volume
Error Findings by Volume 8 CPT Coded Accurately 8 Overcoded 8 Undercoded 8 Missed CPTHCPCS Code 8 Missed or Wrong Modifier 8 Incorrect CPT (or Category) Used 8 Incorrect ICD-9 Codes 8 Incorrect Quantity
Inadequate Documentation 8 8 Missing Documentation 8 Signature Illegible (No Log) 8 No Signature by Provider of Service
1200 Total
Net Payment Error Rate -24636
Primary Payments Total $ Audited Payment Total $ (Total Under Payments)
Total Over Payments
Net OverUnder Payment $
2200 56400
(54200)
Resources Used HCPCS and CPT CodeBook (Current or applilcable year) ICD-10-CM CodeBook (Current or applicable year) CMS 1995 and 1997 EM Guidelines CMS Claims Processing Manual 100-04 Medicare Claims Processing (PUB 100-04) CMS - National Coverage Determinations (NCDs) National Correct Coding Policy Manual Applicable Physician Version
Executive Summary Report
The executive summary provides readers with a short complete document highlighting import information included in the detailed report Executive summaries are created for the senior management readers that donrsquot have time to read the full report and need to walk away with an understanding of the issues and corrective actions
Some would say the executive summary could be written before the detailed report however it is difficult to make sure the most important elements are included until you have spent time reviewing the detail If you want to make sure the most important messages are in the executive
summary this step should be completed after the detail is written As auditors become more seasoned this step could move to the front of the process
Executive Summary Report Structure of the ES Report
o Backgroundndash Specialtyndash Providersndash Sample Selection sizendash Date range of audit
o Audit Scopeo Regulatory Resourceso Type of Medical records reviewedo Overall Accuracy (all providers)o Detailed Audit Findings
ndash Business Impactndash Summary of Findings
o Department Findingso Summary
o ReportsStandard Executive Summary Professional Servicespdf
Department Findings Top Issues
Date ofServiceErrors
MissingDocuments
Missing orInvalid
Signature
TeachingPhysician
Errors
InsufficientConsultation
Documents
OverCoding
EMBundled
IntoGlobal
SurgicalPackage
SplitSharedServiceError
Incorrector
MissingPricing
Modifier
ICD-10Errors
Family Practice
CardiologyInternal Medicine
TOTALS
Top Findings by Provider
E amp M Accuracy Rates
ICD-10-CM Accuracy Rates
Procedure Accuracy Rates
Inpatient DRG Audit Report
TABLE OF CONTENTS
Executive Summaryo Scope of Work
Reimbursement Changes Department Results
o InpatientGeneral Recommendations and Comments
o Secondary DiagnosesoProcedure CodingoPresent on AdmissionoQueries
Scope of WorkCodingAID performed coding audit review of 175 inpatient records The review completed was a random sample that included cases coded by twenty coders for dates of service from May 2016 ndash July 2016
The objective was to determine if the medical record documentation supported the following coding and documentation requirements and any other regulatory requirement for that code set Criteria reviewed
1 ICD-10-CM Official Coding Guidelines for accurate diagnosis code reporting 2 ICD-10-PCS Official Coding Guidelines for accurate procedure code reporting 3 Documentation of procedure compared to the CPT code assigned 4 Identify opportunities for education and training 5 Financial impact of current coding practices
The regulatory agencies and reference materials relied upon include the following in addition to Medicare and Medicaid regulations Additional resources are located in the sub sections below
bull ICD-10-CM and ICD-10-PCS for Hospitals current volume bull Centers for Medicare and Medicaid Services CMS NCCI Edits-Centers for Medicaid and
Medicare Services CMS website wwwcmsgov bull AHA Coding Clinic
The following electronic medical record documents were reviewed and relied upon to compare to the actual codes submitted to the third party payer
bull Discharge summaries HampPs Progress Notes and other provider notes located in the EMR Records
bull Patient History Forms Ancillary Staff Notes bull Procedure Notes bull Orders bull Diagnostic Report
Reimbursement Changes
Coder Acct
Billed Audited
Reimbursement ChangesMS DRG SOI ROM Weight Expected
Payment MS DRG SOI ROM Weight Expected Payment
Coder 1 001 790 52300 $2615000 792 21552 $1077600 -$1537400
Coder 2002
749 26452 $1322600 758 10090 $504500 -$818100
Coder 3 003 669 13111 $655550 694 07294 $364700 -$290850
Coder 4 004 389 08707 $435350 394 09502 $475100 $39750
Coder 5 005 312 07630 $381500 812 08572 $428600 $47100
Coder 6 006 384 08481 $424050 378 09949 $497450 $73400
Coder 7 007 206 08164 $408200 794 12987 $649350 $241150
Coder 8008
344 31029 $1551450 853 51334 $2566700 $1015250
TOTAL $7793700 $6564000 -$1229700
General Recommendations and CommentsFinding Pertinent secondary diagnoses are not coded and diagnoses are code which are not supported in provider documentation Code only those diagnoses which are documented by the provider on the current chart Not all codes are coded to the highest degree of specificity and combination codes were sometimes missed
Recommendation It is important to assign codes for all conditions which meet the definition of a reportable diagnosis Documentation from all providers should be used including but not limited to radiologists pathologists anesthesiologists CRNAs and FNPs
Reference Coding Clinic Official Coding Guidelines
bull Report all secondary diagnoses which meet the definition of a secondary diagnosis which is defined as all conditions that coexist at the time of admission that develop subsequently or that affect the treatment received andor the length of stay Codes which enhance the overall picture of the patientrsquos visit should be added
o Add T45515A to report adverse effect of Coumadin which caused the GI bleed
o Add I2690 for septic pulmonary emboli (MCCSOI4ROM4)
o Add N179 for acute kidney failure (S3M2CC) per the nephrology consult and the 628 progress note
o Add code I429 cardiomyopathy per HampP
o Add B964 to report proteus in a UTI per the 620 hospitalist progress note
o Code for D649 anemia and I701 stenosis of renal artery should be added as secondary diagnoses per the HampP
bull Only report diagnoses which are substantiated by provider documentation in the current chart notes If a suspected condition is not verified at discharge on an inpatient account it cannot be coded
o Remove G4734 (idiopathic sleep related non-obstructive alveolar hypoventilation) as patient was noted to have the sleep study and the hypoventilation was shown to be a possibility but not noted as such on discharge
o Remove G629 (S21) the neuropathy is documented as due to diabetes
o Remove K529 colitis noted on HP as possible but not further noted or confirmed at discharge
Procedure CodingFinding Procedures were sometimes coded incorrectly
Recommendation The entire medical record should be reviewed and all procedures coded as documented Coding procedures incorrectly or assigning incorrect CPT codes may result in lost revenue
bull Incorrect root operation
o Revise principal procedure to 0DQ68ZZ for clipping of the ulcer per OP report clipping is root operation repair
bull Biopsy versus Excision
o Procedure 0DBA0ZX (biopsy of jejunum) should change to 0DBA0ZZ (excision of jejunum) per op note this was not a biopsy procedure
bull Coding Guideline error
o Remove 0RG10K0 for allograft due to being inclusive in principal procedure
o Remove codes for adhesiolysis 0DN80ZZ 0UN10ZZ and 0UN90ZZ due to no significance noted per OP report
bull Incorrect approach
o Revise 0TF63ZZ (fragmentation percutaneous approach) to 0TF68ZZ (fragmentation endoscopic) for procedure performed via scope per the operative report
bull Procedure coded without provider documentation
o Remove secondary procedure of excisional debridement (0JB90ZZ) due to lack of documentation of excisional debridement per operative report The header in the operative report documents IampD and debridement but the body of the operative report only documents an IampD
bull Incorrect CPT code assignment
o Post-op note supports the nerve block injections of four nerves therefore code 64421 (multiple nerve block) should replace 64420 (injection of one intercostal nerve)
Queries Finding Conflicting incomplete and vague documentation is found within provider chart notes
Recommendation Prior to code assignment if the coder finds ambiguous or conflicting documentation the provider should be queried
Reference AHA Coding Clinic 2002 2nd Quarter pages 17-18
bull Query for acute blood loss anemia since hgb has dropped and patient is being transfused PRBC
bull Recommend query to clarify if cardiorenal syndrome is current as it is documented per 627 nephrology consult but unclear if current
bull Documentation does not support SIRS noninfectious without organ failure It is conflicting since patient has respiratory failure Query should be initiated for clarification with or without organ failure or infectious or non-infectious Patient has pneumonia per query as well as last progress note therefore if SIRS is not further specified per query PNA should be sequenced as principal diagnosis and SIRS should be removed
bull Recommend provider query necrotizing lung consolidation noted on DS as principal diagnosis-unclear does the patient have lobar pneumonia Secondary dx states necrotic pneumonia which is coded as principal diagnosis-this diagnosis is clear but consolidation portion is unclear
bull Recommend query for preterm labor delivery at 301 weeks
bull RECOMMEND QUERY no chest pain on admit per ER and HP cardiology provider states no CP with ER stating chest pressure the day prior to admit Appears patient was admitted due to elevated troponins which cardiology says are likely due to hypotension and AKI DS states chest pain but also says bradycardia and hypotension were the reason for admit
bull RECOMMEND QUERY no chest pain on admit per ER and HP cardiology provider states no CP with ER stating chest pressure the day prior to admit Appears patient was admitted due to elevated troponins which cardiology says are likely due to hypotension and AKI DS states chest pain but also says bradycardia and hypotension were the reason for admit
bull Query the provider regarding pathology report notation of endometriosis andor possible re-sequence of stenosis as principal diagnosis as it also meets principal diagnosis guidelines This would result in an MS-DRG change to 742 and APR-DRG change to 513
bull QUERY secondary diagnosis MCC and ROM 4 code T3166 (60 TBSA of which 60 are third degree burns) Chart notes do not specify how much of TBSA was actually third degree If after query TBSA is found to be less than 50 (T3164) then ROM will change from 4 to 3 but no change to overall APR-DRG or weight
Auditor Quality amp Productivity
Audit Productivity Standards
It takes twice as long to audit a chart as it does to code it a statistic that takes into account the time to document an explanation of any coding decision the auditor is not in agreement with o For example in an emergency department audit with a productivity of 12
charts per hour for a coder our auditors would probably be able to review six per hour
o If there are multiple services to audit on each encounter the productivity may only be 4 per hour
o The amount of detail you put into your audit report will also be a factorndash Are you using an automated audit softwarendash Are you using a spreadsheet to auditndash How many Systems are needed to complete the audit
Coder Quality Audits
Quality Audits (QA) should be done on your coders and auditors regularly Frequent reviews with smaller sample size will allow more consistent
review and feedbacko Example 10 charts per month per coder if the coder passes 2-3 months
consecutively with 95 or better score move them to quarterly reviewso Some QA programs review a percentage of the coders work This
methodology requires more time and resources
Auditor QA should also score and comment on the accuracy of the audit comments and recommendations
Presenting the Audit Results
Presenting the Audit Results
Communicating the Audit FindingsoWho requested the AuditoWho are you reporting the finding to
ndash CEOndash CFOndash Physicianndash Revenue Cycle Managerndash HIM Directorndash Billing Managerndash Coding Manager
ReportsAudit Resultspptx
Post Audit Education
Provider Education
Provider Education is best received when it is specific to the provider(s) 11 sessions going over the audit result Look at their notes with them
oHighlight areas for documentation improvementoReinforce Coding Guidelines that are specific to themoAsk them to share how they establish their LOS for E amp M serviceso Integrate their EMR system into the training
Provider Education
Group Training SessionsoUse the audit results to identify common issues within a specialty group
ndash Refer to the Executive Summary reportoVery effective for identifying system issues
ndash Teaching Attestationsndash Templatesndash Copy and Pastendash Cloned notes
o Everyone hears the same messagesoAn Issue may not appear on the individual audit but is still a concern for the
group
Education Delivery
In person or remote sessionso Factors to consider
ndash Providers scheduleavailabilityndash Location(s)ndash Personality of the providerndash Budget
Coder Education
Coders do well in group training so they can learn from each other 11 training allows the coder to get feedback on their coding
Handling Audit Disputes
Handling Audit Disputes
Be open to all points of viewo Let the documentation tell the story
Refer to the guidelines Ask
oCan we defend the reported service with the current documentation
Self Disclosures Refunds and Corrected Billing
Overpayment
In general If a person has received an overpayment the person shallo report and return the overpayment to the Secretary the State an
intermediary a carrier or a contractor as appropriate at the correct address and ndash notify the Secretary State intermediary carrier or contractor to whom the overpayment was returned in writing of the reason for the overpayment
What is an ldquoOverpaymentrdquo ndash The term ldquooverpaymentrdquo means any funds that a person receives or retains under subchapter XVIII or XIX of this chapter to which the person after applicable reconciliation is not entitled under such subchapter
Self Disclosure
The Office of Inspector General (OIG) has several self-disclosure processes that can be used to report potential fraud in Department of Health and Human Services (HHS) programs Choose the one that applies to you from the following descriptions to learn moreo Health Care Provider Self-Disclosures
ndash Health care providers suppliers or other individuals or entities subject to Civil Monetary Penalties can use the Provider Self-Disclosure Protocol which was created in 1998 to voluntarily disclose self-discovered evidence of potential fraud Self-disclosure gives providers the opportunity to avoid the costs and disruptions associated with a Government-directed investigation and civil or administrative litigation Visit the Provider Self-Disclosure Protocol webpage for more information
o HHS Contractor Self-Disclosuresndash Contractors are individuals businesses or other legal entities that are awarded Government contracts or
subcontracts to provide services to the Department of Health and Human Services (HHS) OIGs contractor self-disclosure program enables contractors to self-disclose potential violations of the False Claims Act and various Federal criminal laws involving fraud conflict of interest bribery or gratuity This self-disclosure process is available for those entities with a Federal Acquisition Regulation-based contract Visit the Contractor Self-Disclosure webpage for more information
o HHS Grantee Self-Disclosuresndash HHS grantees or subrecipients may voluntarily disclose evidence of potential violations of Federal criminal law
involving fraud bribery or gratuity violations potentially affecting the Federal award 45 CFR 75113 notes mandatory disclosures of criminal offenses that non-Federal entities must make with respect to HHS grants Recipients submitting disclosures in connection with this requirement should include the subject reference line Mandatory Grant Disclosure Recipients choosing to disclose conduct that may not fit squarely within the scope of offenses described in 45 CFR 75113 should include the following subject reference line in the submission Voluntary Grant Disclosure
Medicare 60 day rule
The 60 Day Rule (Medicare Parts A amp B) o The 60 day time period for reportingreturning begins when either
ndash The reasonable diligence is completed orndash On the day the provider received credible information of a potential overpayment (if the
provider fails to conduct reasonable diligence) o For an investigation to be conducted in a ldquotimelyrdquo manner providers typically
must complete the investigation within 6 months from receipt of credible information indicating there may be an overpayment
ndash ndash 6-month timeframe may potentially be extended under ldquoextraordinary circumstancesrdquo ndash 8 months generally the maximum total time to return overpayments The government recommends that providers maintain records documenting ldquoreasonable diligencerdquo
Medicare 60 Day Rule
Six-year lookback period ndash Sometimes possible to use a shorter period depending on the facts at issue Amount to be repaid ndash May vary depending on the method used to
reportreturn eg Medicare administrative contractor (ldquoMACrdquo) v self-disclosure Overpayment notification ndash After receiving an overpayment
notification from the government you should investigate for related overpayments eg other time periods
Medicare 60 Day Rule
Self-disclosure protocols ndashoA submission to the OIG or CMS protocols suspends the 60 day requirement
for returning overpayments until a settlement agreement is executed ndash ndash OIGrsquos Self-Disclosure Protocol (SDP) ndash ndash CMS Voluntary Self-Referral Disclosure Protocol (SRDP) ndash
o Self-disclosures to other agencies do not suspend the repayment deadlinendash ndash Eg Department of Justice local US Attorneyrsquos Office Medicaid Fraud Control Unit
Medicare 60 Day Rule
Facilitating Compliance With the 60 Day Rule Compliance programs should include o ndash Appropriate policies and procedures o ndash Periodic billing and coding audits to proactively identify overpaymentso ndash Focus on high-risk areas o ndash Utilization of publicly available government resources to guide audit efforts o ndash Investigating any suspected incidents of non-compliance with federal health
care program requirements
Self Disclosure
Choice of AgencyoOIG ndash Self-Disclosure Protocol
ndash ndash Conduct involving false billingndash ndash Conduct involving excluded personsndash ndash Conduct involving the Anti-Kickback Statute (including conduct thatndash violates both the AKS and Stark Law)
oCMS ndash Self-Referral Disclosure Protocolndash ndash Conduct involving only violations of the Stark Law
oDOJndash ndash May be appropriate when provider believes a FCA release is necessary
Summary
The Cost of a Well-Executed Coding Audit ProcessThe costs associated with an auditing program are worth it in the long run Ideally your organization is performing audits on a regular basis across all service types locations and payers Weve all seen claims that have been denied resulting in additional work that may be preventable with a proper audit program The goal is to use the audit feedback to improve coding quality and lower potential risk and cost to the organization Organizations should be investing in an effective coding audit program to make your coders and providers better and enhance documentation improvement from the providers
Questions
Thank you for your attentionLynn Handy
Vice President of Coding amp Audit ServicesLynnhandymanagedresourcesinccom

Coding Guidelines
E amp M Guidelineso95 or 97oDefine the 95 detailed examo Is ldquonon contributoryrdquo allowedo2 out of 3 key components (Is MDM required)
Coding Guidelines
Other Risk AreasoMedical Necessityo Teaching Physician Guidelineso Incident To o SplitSharedoCopy amp PasteCloned noteso Scribeso SignatureAuthenticationsoOrders for diagnostic servicesoDate of ServiceoNew versus Established CodesoConsultations
Audit Reports
Goals of the Audit Report
The main goal of an audit report is to communicate where the organization specialty department provider or coder does or does not conform to regulatory standards guidelines and organizational policieso Each identified issue must have a standard it is measured againsto Site the regulation in your audit report or include a link to the regulation
Audit reports should not just contain negative findings Outline the Positives also Identify opportunities for improvement this can be in the form of a
recommendation Prioritize High Risk Findings
Who will be reading the Audit Report
What is the technical knowledge of the readeroCodersHIM ProfessionalsoProvidersoClinical StaffoHIM DirectorsoBillingCoding DirectorsManagersoCEOCFO (Executive Team)
Audit Report Format Tips
Provide perspective for the readero Positive and Negative findings
Be precise avoid redundant phrasing inexact terminology Avoid long sentences when a shorter one will work Avoid stating your opinion State the findings and facts Use bullet points this helps to break up difficult information and makes it
clearer for the reader Use gender neutral terms Avoid audit ldquobuzzwordsrdquo such as ldquogenerally improvedrdquo or ldquosignificant riskrdquo Avoid abbreviations unless they are clearly defined
Benefits of Automating your Audit Reports Results
o Consistent Resultso Better Datao Increases Efficiency
Trackingo Allows audit results to be tracked by provider and by specialty
QAo Allows for an automated approach to your internal quality reviews
Trendingo Allows for data analysis at a detailed level that can be tracked
Productivityo Increases auditor productivityo Decreases re-work
ProviderCoder Audit Reports
Detailed Audit reports should have the ability to be sorted byoProvideroCodero Specialty or GroupoAudit Date
Detailed results for each encounteroMeaningful comments
Key Findingso From all encounters
Recommendations and Resources
Detailed Findings Patient ID Patient Name DOS Payer CPT Reported CPT Audited EM Level Key Component ICD Reported ICD Reported Description ICD Audited ICD Reported Description
1 001 Patient A 02-19-16 Blue Cross
99203 25 1 99202 1 +1 D E L 1 S92302A2 Not Reported
1 Fracture of unspecified metatarsal bone(s) left foot initial encounter for closed fracture
1 S92355D2 W109XXD
1 Nondisplaced fracture of fifth metatarsal bone left foot subsequent encounter for fracture with routine healing2 Fall (on) (from) unspecified stairs and steps subsequent encounter
1 The documentation supports coding for an EM service that is one level below the billed code2 Lacking Exam documentation to support the EM level selected3 1997 MSK exam supports an Expanded Problem Focused exam (99202) 1995 exam supports a Detailed exam (99203)4 1997 Exam template suggestions Neurologic Exam-suggest adding the body part examined (upper extremitylow extremity) Dermatologic Exam-unable to determine if this was performed This should be deleted from the final note if
not examined5 EM time statement is insufficient documentation is lacking a required element total time of visit and counseling time greater than 506 CPT disallowed documentation is not present within the medical record to support the CPT code billed (28485-open treatment of metatarsal fracture includes internal fixation when performed) Fracture care is not supported patient
was seen in the ER 6 weeksrsquo prior ER doctor initiated treatment7 The incorrect pricing modifier was billed Removed modifier 25 (separate and significant EM on the same day as a minor procedure) Fracture care is not billable no modifier needed on EM service8 Diagnosis billed is not the most specific available according to the medical record documentation9 Documentation supports an additional diagnosis code not billed
2 002 Patient B 02-05-16 Blue Cross
99203 25 1 99202 25 1 +1 D E L 1 L03032 1 Cellulitis of left toe 1 L03032 1 Cellulitis of left toe
1 The documentation supports coding for an EM service that is one level below the billed code2 Lacking Exam documentation to support the EM level selected3 1997 MSK exam supports an Expanded Problem Focused exam (99202) 1995 exam supports a Detailed exam (99203)4 EM time statement is insufficient documentation is lacking one or more required elements (total time counseling time greater than 50) If a procedure is performed during a visit the time spent performing the procedure needs to be
carved out of the total visit time5 Allowed modifier 25 due to commercial payer Medicare and NCCI do not require modifier 25 on a new patient EM when a minor procedure is performed the same day 6 Diagnosis supported
Detailed Findings
135 822012 New Consultations - Office
Consultations Detailed Detailed (95) Moderate 99244 99243 1 $3500 N
Provider Code 99244 Reviewer Code 99243 Provider Diagnosis 1 3005 NEURASTHENIA Reviewer Diagnosis 1 3005 NEURASTHENIA Provider Diagnosis 2 7282 MUSC DISUSE ATROPHY NEC Reviewer Diagnosis 2 7282 MUSC DISUSE ATROPHY NEC
bull Assessment (I) The assessment is not clearly stated for this encounter Documentation Guidelines states The documentation for each patient encounter should include assessment clinical impression or diagnosis bull Assessment (R) The assessment should be clearly documented for each encounter Since each note must stand alone it is imperative to accurately document the most specific diagnosis in the assessment impression section of the note
bull Documented Lower Level (I) The documentation substantiates a lower level of service than charged
Chart Level Comments
Group your comments in categoriesoDocumentationo E amp MoProceduresoModifierso ICD-10-CM
oReportsAudit Manager Macros 061218 (version 1)xlsx
Recommendations and ReferencesCategory Short Description Long Description
EM AdmissionDischarge Same Day Review the CMS AdmissionDischarge same day coding guidelines httpswwwcmsgovRegulations-and-GuidanceGuidanceManualsDownloadsclm104c12pdf
EM ConsultationReview the consultation guidelines located in the CPT book
EM Consultation not billable to Medicare CMS no longer recognizes the consultation codeshttpswwwcmsgovOutreach-and-EducationMedicare-Learning-Network-MLNMLNMattersArticlesdownloadsmm6740pdf
EM Critical CareReview the CMS Critical Care guidelines httpswwwcmsgovOutreach-and-EducationMedicare-Learning-Network-MLNMLNMattersArticlesdownloadsmm5993pdf
EM Discharge ServicesReview the CMS Hospital Discharge Services guidelineshttpswwwcmsgovOutreach-and-EducationMedicare-Learning-Network-MLNMLNMattersArticlesdownloadsmm5794pdf
EMEM and Preventive Visit Review AAPC guidance for documenting and billing an EM and Preventive visit same day httpswwwaapccomblog22580-successfully-bill-a-
preventive-service-with-a-sick-visit
EM EM documentation guidelines Review the CMS 1995 amp 1997 EM documentation guidelineshttpswwwcmsgovOutreach-and-EducationMedicare-Learning-Network-MLNMLNEdWebGuideEMDOChtml
EM EM Inpatient vs Outpatient Review the patientrsquos status on the hospital admission order to determine the appropriate EM category to bill (inpatient vs observation)
EM EM New vs EstablishedReview the CMS New vs Established patient guidelines httpswwwcmsgovOutreach-and-EducationMedicare-Learning-Network-MLNMLNProductsDownloadseval-mgmt-serv-guide-ICN006764pdf
EMEM Time billing suggestion
Recommend a time statement is added to the EM medical record when a majority of the visit is spent counseling andor coordination of care Review the CMS 1995 amp 1997 EM documentation guidelines for EM time documentationhttpswwwcmsgovOutreach-and-EducationMedicare-Learning-Network-MLNMLNEdWebGuideEMDOChtml
EM Inpatient hospital servicesReview the CMS Hospital Services (Initial and Subsequent) guidelines httpswwwcmsgovRegulations-and-GuidanceGuidanceManualsDownloadsclm104c12pdf
EM Nursing Facility Services Review the Nursing Facility Services guidelines provided by CMS The guidelines can be downloaded at this linkhttpswwwcmsgovRegulations-and-GuidanceGuidanceManualsDownloadsclm104c12pdf
EM Observation Services Review the CMS Observation Services (Initial and Subsequent) guidelines httpswwwcmsgovRegulations-and-GuidanceGuidanceManualsDownloadsclm104c12pdf
EM Prolonged Services Review the CMS Prolonged Services guidelines httpswwwcmsgovOutreach-and-EducationMedicare-Learning-Network-MLNMLNMattersArticlesdownloadsmm5972pdf
EMReview of Systems Review the CMS 1995 amp 1997 EM documentation guidelines for Review of Systems requirements
httpswwwcmsgovOutreach-and-EducationMedicare-Learning-Network-MLNMLNEdWebGuideEMDOChtml
EMConsultation Documentation Suggestion
Recommend adding verbiage to consultation documentation that indicates the name of the referring provider and the reason for the consultation
Audit Report Examples Automated Solution
Letrsquos look at some report Examples
ReportsStandard Provider Audit SummarypdfReportsProvider Detailed Sample Reportdocx
ReportsProvider Audit Worksheets - Optionalpdf
Audit Report Examples Non Automated Solution
Error Findings by Volume Percentage
CPT Coded Accurately
8 8 Overcoded
8 8 Undercoded
Missed CPTHCPCS Code
Missed or Wrong Modifier
8 8 Incorrect CPT (or Category) Used
Incorrect ICD-9 Codes
8 8 Incorrect Quantity
Inadequate Documentation
Missing Documentation 8 8
Signature Illegible (No Log)
8 8
CLIENT NAME PROJECT TITLE
Review Line Item Detail Prepared Month Year
DRAFT
Client Claim Demographics Client Charge Data Review Result EampM ONLY Findings C C C C C C O OC O O O
Char
t Num
ber
Au
dit D
ate
Audi
tor (
initi
als)
QA
Initi
als
Fa
cilit
y Lo
catio
n Re
porte
d
Pr
ovid
er N
ame
Pa
tient
Nam
e
M
edic
al R
ecor
d Nu
mbe
r
Prim
ary
Carr
ier M
edica
re=
A M
edica
id =
B O
ther
=O
Da
te o
f Ser
vice
CP
T Co
de
Mod
ifier
(s) i
n or
der
Qua
ntity
Diag
nosi
s Co
de(s
) 1
thro
ugh
4
Fe
e ch
arge
d
Pr
imar
y Pa
ymen
t Am
ount
CPT
Code
Mod
ifier
(s) i
n or
der
Qua
ntity
Diag
nosi
s Co
de(s
) 1
thro
ugh
4
CO
RREC
T AL
LOW
ABLE
Prim
ary
PAYM
ENT
Va
rianc
e
Chie
f Com
plai
nt
Hist
ory
Leve
l Sup
port
ed
Exam
Lev
el S
uppo
rted
Med
ical
Dec
Mak
ing
Supp
orte
d (o
r TIM
E)
CPT
Cod
ed A
ccur
atel
y
Ove
rcod
ed
Und
erco
ded
Mis
sed
CPT
HC
PCS
Cod
e
Mis
sed
or W
rong
Mod
ifier
Inco
rrec
t CPT
(or C
ateg
ory)
Use
d
Inco
rrec
t IC
D-9
Cod
es
Inco
rrec
t Qua
ntity
Inad
equa
te D
ocum
enta
tion
Mis
sing
Doc
umen
tatio
n
Sign
atur
e Ill
egib
le (N
o Lo
g)
No
Sign
atur
e by
Pro
vide
r of
Ser
vice
COMMENTS (abbreviations used) PF- PROBLEM FOCUSED EPF- EXPANDED PF DET- DETAILED COMP- COMPREHENSIVE SFWD- STRAIGHT FORWARD MOD- MODERATE MDM- MEDICAL DECISION MAKING
Char
t Num
ber
SAMPLE SAMPLE S MD SAMPLE SAMPLE XXXXX XXX 112001 99212 25 1 1 1234 2 5678 3 4
$30000 $2200 99212 25 1 1 1234 2 5678 3 4
$56400 $54200 YES
DET
CO
MP
MO
D
COMMENTS COMMENTS COMMENTS
0
1 2 3 4
1 2 3 4
$000 0
$30000 $2200 $56400 $54200 10 10 10 10 10 10 10 10 10 10 10 10 TOTALS 917 Error Rate by Volume
Error Findings by Volume 8 CPT Coded Accurately 8 Overcoded 8 Undercoded 8 Missed CPTHCPCS Code 8 Missed or Wrong Modifier 8 Incorrect CPT (or Category) Used 8 Incorrect ICD-9 Codes 8 Incorrect Quantity
Inadequate Documentation 8 8 Missing Documentation 8 Signature Illegible (No Log) 8 No Signature by Provider of Service
1200 Total
Net Payment Error Rate -24636
Primary Payments Total $ Audited Payment Total $ (Total Under Payments)
Total Over Payments
Net OverUnder Payment $
2200 56400
(54200)
Resources Used HCPCS and CPT CodeBook (Current or applilcable year) ICD-10-CM CodeBook (Current or applicable year) CMS 1995 and 1997 EM Guidelines CMS Claims Processing Manual 100-04 Medicare Claims Processing (PUB 100-04) CMS - National Coverage Determinations (NCDs) National Correct Coding Policy Manual Applicable Physician Version
Executive Summary Report
The executive summary provides readers with a short complete document highlighting import information included in the detailed report Executive summaries are created for the senior management readers that donrsquot have time to read the full report and need to walk away with an understanding of the issues and corrective actions
Some would say the executive summary could be written before the detailed report however it is difficult to make sure the most important elements are included until you have spent time reviewing the detail If you want to make sure the most important messages are in the executive
summary this step should be completed after the detail is written As auditors become more seasoned this step could move to the front of the process
Executive Summary Report Structure of the ES Report
o Backgroundndash Specialtyndash Providersndash Sample Selection sizendash Date range of audit
o Audit Scopeo Regulatory Resourceso Type of Medical records reviewedo Overall Accuracy (all providers)o Detailed Audit Findings
ndash Business Impactndash Summary of Findings
o Department Findingso Summary
o ReportsStandard Executive Summary Professional Servicespdf
Department Findings Top Issues
Date ofServiceErrors
MissingDocuments
Missing orInvalid
Signature
TeachingPhysician
Errors
InsufficientConsultation
Documents
OverCoding
EMBundled
IntoGlobal
SurgicalPackage
SplitSharedServiceError
Incorrector
MissingPricing
Modifier
ICD-10Errors
Family Practice
CardiologyInternal Medicine
TOTALS
Top Findings by Provider
E amp M Accuracy Rates
ICD-10-CM Accuracy Rates
Procedure Accuracy Rates
Inpatient DRG Audit Report
TABLE OF CONTENTS
Executive Summaryo Scope of Work
Reimbursement Changes Department Results
o InpatientGeneral Recommendations and Comments
o Secondary DiagnosesoProcedure CodingoPresent on AdmissionoQueries
Scope of WorkCodingAID performed coding audit review of 175 inpatient records The review completed was a random sample that included cases coded by twenty coders for dates of service from May 2016 ndash July 2016
The objective was to determine if the medical record documentation supported the following coding and documentation requirements and any other regulatory requirement for that code set Criteria reviewed
1 ICD-10-CM Official Coding Guidelines for accurate diagnosis code reporting 2 ICD-10-PCS Official Coding Guidelines for accurate procedure code reporting 3 Documentation of procedure compared to the CPT code assigned 4 Identify opportunities for education and training 5 Financial impact of current coding practices
The regulatory agencies and reference materials relied upon include the following in addition to Medicare and Medicaid regulations Additional resources are located in the sub sections below
bull ICD-10-CM and ICD-10-PCS for Hospitals current volume bull Centers for Medicare and Medicaid Services CMS NCCI Edits-Centers for Medicaid and
Medicare Services CMS website wwwcmsgov bull AHA Coding Clinic
The following electronic medical record documents were reviewed and relied upon to compare to the actual codes submitted to the third party payer
bull Discharge summaries HampPs Progress Notes and other provider notes located in the EMR Records
bull Patient History Forms Ancillary Staff Notes bull Procedure Notes bull Orders bull Diagnostic Report
Reimbursement Changes
Coder Acct
Billed Audited
Reimbursement ChangesMS DRG SOI ROM Weight Expected
Payment MS DRG SOI ROM Weight Expected Payment
Coder 1 001 790 52300 $2615000 792 21552 $1077600 -$1537400
Coder 2002
749 26452 $1322600 758 10090 $504500 -$818100
Coder 3 003 669 13111 $655550 694 07294 $364700 -$290850
Coder 4 004 389 08707 $435350 394 09502 $475100 $39750
Coder 5 005 312 07630 $381500 812 08572 $428600 $47100
Coder 6 006 384 08481 $424050 378 09949 $497450 $73400
Coder 7 007 206 08164 $408200 794 12987 $649350 $241150
Coder 8008
344 31029 $1551450 853 51334 $2566700 $1015250
TOTAL $7793700 $6564000 -$1229700
General Recommendations and CommentsFinding Pertinent secondary diagnoses are not coded and diagnoses are code which are not supported in provider documentation Code only those diagnoses which are documented by the provider on the current chart Not all codes are coded to the highest degree of specificity and combination codes were sometimes missed
Recommendation It is important to assign codes for all conditions which meet the definition of a reportable diagnosis Documentation from all providers should be used including but not limited to radiologists pathologists anesthesiologists CRNAs and FNPs
Reference Coding Clinic Official Coding Guidelines
bull Report all secondary diagnoses which meet the definition of a secondary diagnosis which is defined as all conditions that coexist at the time of admission that develop subsequently or that affect the treatment received andor the length of stay Codes which enhance the overall picture of the patientrsquos visit should be added
o Add T45515A to report adverse effect of Coumadin which caused the GI bleed
o Add I2690 for septic pulmonary emboli (MCCSOI4ROM4)
o Add N179 for acute kidney failure (S3M2CC) per the nephrology consult and the 628 progress note
o Add code I429 cardiomyopathy per HampP
o Add B964 to report proteus in a UTI per the 620 hospitalist progress note
o Code for D649 anemia and I701 stenosis of renal artery should be added as secondary diagnoses per the HampP
bull Only report diagnoses which are substantiated by provider documentation in the current chart notes If a suspected condition is not verified at discharge on an inpatient account it cannot be coded
o Remove G4734 (idiopathic sleep related non-obstructive alveolar hypoventilation) as patient was noted to have the sleep study and the hypoventilation was shown to be a possibility but not noted as such on discharge
o Remove G629 (S21) the neuropathy is documented as due to diabetes
o Remove K529 colitis noted on HP as possible but not further noted or confirmed at discharge
Procedure CodingFinding Procedures were sometimes coded incorrectly
Recommendation The entire medical record should be reviewed and all procedures coded as documented Coding procedures incorrectly or assigning incorrect CPT codes may result in lost revenue
bull Incorrect root operation
o Revise principal procedure to 0DQ68ZZ for clipping of the ulcer per OP report clipping is root operation repair
bull Biopsy versus Excision
o Procedure 0DBA0ZX (biopsy of jejunum) should change to 0DBA0ZZ (excision of jejunum) per op note this was not a biopsy procedure
bull Coding Guideline error
o Remove 0RG10K0 for allograft due to being inclusive in principal procedure
o Remove codes for adhesiolysis 0DN80ZZ 0UN10ZZ and 0UN90ZZ due to no significance noted per OP report
bull Incorrect approach
o Revise 0TF63ZZ (fragmentation percutaneous approach) to 0TF68ZZ (fragmentation endoscopic) for procedure performed via scope per the operative report
bull Procedure coded without provider documentation
o Remove secondary procedure of excisional debridement (0JB90ZZ) due to lack of documentation of excisional debridement per operative report The header in the operative report documents IampD and debridement but the body of the operative report only documents an IampD
bull Incorrect CPT code assignment
o Post-op note supports the nerve block injections of four nerves therefore code 64421 (multiple nerve block) should replace 64420 (injection of one intercostal nerve)
Queries Finding Conflicting incomplete and vague documentation is found within provider chart notes
Recommendation Prior to code assignment if the coder finds ambiguous or conflicting documentation the provider should be queried
Reference AHA Coding Clinic 2002 2nd Quarter pages 17-18
bull Query for acute blood loss anemia since hgb has dropped and patient is being transfused PRBC
bull Recommend query to clarify if cardiorenal syndrome is current as it is documented per 627 nephrology consult but unclear if current
bull Documentation does not support SIRS noninfectious without organ failure It is conflicting since patient has respiratory failure Query should be initiated for clarification with or without organ failure or infectious or non-infectious Patient has pneumonia per query as well as last progress note therefore if SIRS is not further specified per query PNA should be sequenced as principal diagnosis and SIRS should be removed
bull Recommend provider query necrotizing lung consolidation noted on DS as principal diagnosis-unclear does the patient have lobar pneumonia Secondary dx states necrotic pneumonia which is coded as principal diagnosis-this diagnosis is clear but consolidation portion is unclear
bull Recommend query for preterm labor delivery at 301 weeks
bull RECOMMEND QUERY no chest pain on admit per ER and HP cardiology provider states no CP with ER stating chest pressure the day prior to admit Appears patient was admitted due to elevated troponins which cardiology says are likely due to hypotension and AKI DS states chest pain but also says bradycardia and hypotension were the reason for admit
bull RECOMMEND QUERY no chest pain on admit per ER and HP cardiology provider states no CP with ER stating chest pressure the day prior to admit Appears patient was admitted due to elevated troponins which cardiology says are likely due to hypotension and AKI DS states chest pain but also says bradycardia and hypotension were the reason for admit
bull Query the provider regarding pathology report notation of endometriosis andor possible re-sequence of stenosis as principal diagnosis as it also meets principal diagnosis guidelines This would result in an MS-DRG change to 742 and APR-DRG change to 513
bull QUERY secondary diagnosis MCC and ROM 4 code T3166 (60 TBSA of which 60 are third degree burns) Chart notes do not specify how much of TBSA was actually third degree If after query TBSA is found to be less than 50 (T3164) then ROM will change from 4 to 3 but no change to overall APR-DRG or weight
Auditor Quality amp Productivity
Audit Productivity Standards
It takes twice as long to audit a chart as it does to code it a statistic that takes into account the time to document an explanation of any coding decision the auditor is not in agreement with o For example in an emergency department audit with a productivity of 12
charts per hour for a coder our auditors would probably be able to review six per hour
o If there are multiple services to audit on each encounter the productivity may only be 4 per hour
o The amount of detail you put into your audit report will also be a factorndash Are you using an automated audit softwarendash Are you using a spreadsheet to auditndash How many Systems are needed to complete the audit
Coder Quality Audits
Quality Audits (QA) should be done on your coders and auditors regularly Frequent reviews with smaller sample size will allow more consistent
review and feedbacko Example 10 charts per month per coder if the coder passes 2-3 months
consecutively with 95 or better score move them to quarterly reviewso Some QA programs review a percentage of the coders work This
methodology requires more time and resources
Auditor QA should also score and comment on the accuracy of the audit comments and recommendations
Presenting the Audit Results
Presenting the Audit Results
Communicating the Audit FindingsoWho requested the AuditoWho are you reporting the finding to
ndash CEOndash CFOndash Physicianndash Revenue Cycle Managerndash HIM Directorndash Billing Managerndash Coding Manager
ReportsAudit Resultspptx
Post Audit Education
Provider Education
Provider Education is best received when it is specific to the provider(s) 11 sessions going over the audit result Look at their notes with them
oHighlight areas for documentation improvementoReinforce Coding Guidelines that are specific to themoAsk them to share how they establish their LOS for E amp M serviceso Integrate their EMR system into the training
Provider Education
Group Training SessionsoUse the audit results to identify common issues within a specialty group
ndash Refer to the Executive Summary reportoVery effective for identifying system issues
ndash Teaching Attestationsndash Templatesndash Copy and Pastendash Cloned notes
o Everyone hears the same messagesoAn Issue may not appear on the individual audit but is still a concern for the
group
Education Delivery
In person or remote sessionso Factors to consider
ndash Providers scheduleavailabilityndash Location(s)ndash Personality of the providerndash Budget
Coder Education
Coders do well in group training so they can learn from each other 11 training allows the coder to get feedback on their coding
Handling Audit Disputes
Handling Audit Disputes
Be open to all points of viewo Let the documentation tell the story
Refer to the guidelines Ask
oCan we defend the reported service with the current documentation
Self Disclosures Refunds and Corrected Billing
Overpayment
In general If a person has received an overpayment the person shallo report and return the overpayment to the Secretary the State an
intermediary a carrier or a contractor as appropriate at the correct address and ndash notify the Secretary State intermediary carrier or contractor to whom the overpayment was returned in writing of the reason for the overpayment
What is an ldquoOverpaymentrdquo ndash The term ldquooverpaymentrdquo means any funds that a person receives or retains under subchapter XVIII or XIX of this chapter to which the person after applicable reconciliation is not entitled under such subchapter
Self Disclosure
The Office of Inspector General (OIG) has several self-disclosure processes that can be used to report potential fraud in Department of Health and Human Services (HHS) programs Choose the one that applies to you from the following descriptions to learn moreo Health Care Provider Self-Disclosures
ndash Health care providers suppliers or other individuals or entities subject to Civil Monetary Penalties can use the Provider Self-Disclosure Protocol which was created in 1998 to voluntarily disclose self-discovered evidence of potential fraud Self-disclosure gives providers the opportunity to avoid the costs and disruptions associated with a Government-directed investigation and civil or administrative litigation Visit the Provider Self-Disclosure Protocol webpage for more information
o HHS Contractor Self-Disclosuresndash Contractors are individuals businesses or other legal entities that are awarded Government contracts or
subcontracts to provide services to the Department of Health and Human Services (HHS) OIGs contractor self-disclosure program enables contractors to self-disclose potential violations of the False Claims Act and various Federal criminal laws involving fraud conflict of interest bribery or gratuity This self-disclosure process is available for those entities with a Federal Acquisition Regulation-based contract Visit the Contractor Self-Disclosure webpage for more information
o HHS Grantee Self-Disclosuresndash HHS grantees or subrecipients may voluntarily disclose evidence of potential violations of Federal criminal law
involving fraud bribery or gratuity violations potentially affecting the Federal award 45 CFR 75113 notes mandatory disclosures of criminal offenses that non-Federal entities must make with respect to HHS grants Recipients submitting disclosures in connection with this requirement should include the subject reference line Mandatory Grant Disclosure Recipients choosing to disclose conduct that may not fit squarely within the scope of offenses described in 45 CFR 75113 should include the following subject reference line in the submission Voluntary Grant Disclosure
Medicare 60 day rule
The 60 Day Rule (Medicare Parts A amp B) o The 60 day time period for reportingreturning begins when either
ndash The reasonable diligence is completed orndash On the day the provider received credible information of a potential overpayment (if the
provider fails to conduct reasonable diligence) o For an investigation to be conducted in a ldquotimelyrdquo manner providers typically
must complete the investigation within 6 months from receipt of credible information indicating there may be an overpayment
ndash ndash 6-month timeframe may potentially be extended under ldquoextraordinary circumstancesrdquo ndash 8 months generally the maximum total time to return overpayments The government recommends that providers maintain records documenting ldquoreasonable diligencerdquo
Medicare 60 Day Rule
Six-year lookback period ndash Sometimes possible to use a shorter period depending on the facts at issue Amount to be repaid ndash May vary depending on the method used to
reportreturn eg Medicare administrative contractor (ldquoMACrdquo) v self-disclosure Overpayment notification ndash After receiving an overpayment
notification from the government you should investigate for related overpayments eg other time periods
Medicare 60 Day Rule
Self-disclosure protocols ndashoA submission to the OIG or CMS protocols suspends the 60 day requirement
for returning overpayments until a settlement agreement is executed ndash ndash OIGrsquos Self-Disclosure Protocol (SDP) ndash ndash CMS Voluntary Self-Referral Disclosure Protocol (SRDP) ndash
o Self-disclosures to other agencies do not suspend the repayment deadlinendash ndash Eg Department of Justice local US Attorneyrsquos Office Medicaid Fraud Control Unit
Medicare 60 Day Rule
Facilitating Compliance With the 60 Day Rule Compliance programs should include o ndash Appropriate policies and procedures o ndash Periodic billing and coding audits to proactively identify overpaymentso ndash Focus on high-risk areas o ndash Utilization of publicly available government resources to guide audit efforts o ndash Investigating any suspected incidents of non-compliance with federal health
care program requirements
Self Disclosure
Choice of AgencyoOIG ndash Self-Disclosure Protocol
ndash ndash Conduct involving false billingndash ndash Conduct involving excluded personsndash ndash Conduct involving the Anti-Kickback Statute (including conduct thatndash violates both the AKS and Stark Law)
oCMS ndash Self-Referral Disclosure Protocolndash ndash Conduct involving only violations of the Stark Law
oDOJndash ndash May be appropriate when provider believes a FCA release is necessary
Summary
The Cost of a Well-Executed Coding Audit ProcessThe costs associated with an auditing program are worth it in the long run Ideally your organization is performing audits on a regular basis across all service types locations and payers Weve all seen claims that have been denied resulting in additional work that may be preventable with a proper audit program The goal is to use the audit feedback to improve coding quality and lower potential risk and cost to the organization Organizations should be investing in an effective coding audit program to make your coders and providers better and enhance documentation improvement from the providers
Questions
Thank you for your attentionLynn Handy
Vice President of Coding amp Audit ServicesLynnhandymanagedresourcesinccom

Coding Guidelines
Other Risk AreasoMedical Necessityo Teaching Physician Guidelineso Incident To o SplitSharedoCopy amp PasteCloned noteso Scribeso SignatureAuthenticationsoOrders for diagnostic servicesoDate of ServiceoNew versus Established CodesoConsultations
Audit Reports
Goals of the Audit Report
The main goal of an audit report is to communicate where the organization specialty department provider or coder does or does not conform to regulatory standards guidelines and organizational policieso Each identified issue must have a standard it is measured againsto Site the regulation in your audit report or include a link to the regulation
Audit reports should not just contain negative findings Outline the Positives also Identify opportunities for improvement this can be in the form of a
recommendation Prioritize High Risk Findings
Who will be reading the Audit Report
What is the technical knowledge of the readeroCodersHIM ProfessionalsoProvidersoClinical StaffoHIM DirectorsoBillingCoding DirectorsManagersoCEOCFO (Executive Team)
Audit Report Format Tips
Provide perspective for the readero Positive and Negative findings
Be precise avoid redundant phrasing inexact terminology Avoid long sentences when a shorter one will work Avoid stating your opinion State the findings and facts Use bullet points this helps to break up difficult information and makes it
clearer for the reader Use gender neutral terms Avoid audit ldquobuzzwordsrdquo such as ldquogenerally improvedrdquo or ldquosignificant riskrdquo Avoid abbreviations unless they are clearly defined
Benefits of Automating your Audit Reports Results
o Consistent Resultso Better Datao Increases Efficiency
Trackingo Allows audit results to be tracked by provider and by specialty
QAo Allows for an automated approach to your internal quality reviews
Trendingo Allows for data analysis at a detailed level that can be tracked
Productivityo Increases auditor productivityo Decreases re-work
ProviderCoder Audit Reports
Detailed Audit reports should have the ability to be sorted byoProvideroCodero Specialty or GroupoAudit Date
Detailed results for each encounteroMeaningful comments
Key Findingso From all encounters
Recommendations and Resources
Detailed Findings Patient ID Patient Name DOS Payer CPT Reported CPT Audited EM Level Key Component ICD Reported ICD Reported Description ICD Audited ICD Reported Description
1 001 Patient A 02-19-16 Blue Cross
99203 25 1 99202 1 +1 D E L 1 S92302A2 Not Reported
1 Fracture of unspecified metatarsal bone(s) left foot initial encounter for closed fracture
1 S92355D2 W109XXD
1 Nondisplaced fracture of fifth metatarsal bone left foot subsequent encounter for fracture with routine healing2 Fall (on) (from) unspecified stairs and steps subsequent encounter
1 The documentation supports coding for an EM service that is one level below the billed code2 Lacking Exam documentation to support the EM level selected3 1997 MSK exam supports an Expanded Problem Focused exam (99202) 1995 exam supports a Detailed exam (99203)4 1997 Exam template suggestions Neurologic Exam-suggest adding the body part examined (upper extremitylow extremity) Dermatologic Exam-unable to determine if this was performed This should be deleted from the final note if
not examined5 EM time statement is insufficient documentation is lacking a required element total time of visit and counseling time greater than 506 CPT disallowed documentation is not present within the medical record to support the CPT code billed (28485-open treatment of metatarsal fracture includes internal fixation when performed) Fracture care is not supported patient
was seen in the ER 6 weeksrsquo prior ER doctor initiated treatment7 The incorrect pricing modifier was billed Removed modifier 25 (separate and significant EM on the same day as a minor procedure) Fracture care is not billable no modifier needed on EM service8 Diagnosis billed is not the most specific available according to the medical record documentation9 Documentation supports an additional diagnosis code not billed
2 002 Patient B 02-05-16 Blue Cross
99203 25 1 99202 25 1 +1 D E L 1 L03032 1 Cellulitis of left toe 1 L03032 1 Cellulitis of left toe
1 The documentation supports coding for an EM service that is one level below the billed code2 Lacking Exam documentation to support the EM level selected3 1997 MSK exam supports an Expanded Problem Focused exam (99202) 1995 exam supports a Detailed exam (99203)4 EM time statement is insufficient documentation is lacking one or more required elements (total time counseling time greater than 50) If a procedure is performed during a visit the time spent performing the procedure needs to be
carved out of the total visit time5 Allowed modifier 25 due to commercial payer Medicare and NCCI do not require modifier 25 on a new patient EM when a minor procedure is performed the same day 6 Diagnosis supported
Detailed Findings
135 822012 New Consultations - Office
Consultations Detailed Detailed (95) Moderate 99244 99243 1 $3500 N
Provider Code 99244 Reviewer Code 99243 Provider Diagnosis 1 3005 NEURASTHENIA Reviewer Diagnosis 1 3005 NEURASTHENIA Provider Diagnosis 2 7282 MUSC DISUSE ATROPHY NEC Reviewer Diagnosis 2 7282 MUSC DISUSE ATROPHY NEC
bull Assessment (I) The assessment is not clearly stated for this encounter Documentation Guidelines states The documentation for each patient encounter should include assessment clinical impression or diagnosis bull Assessment (R) The assessment should be clearly documented for each encounter Since each note must stand alone it is imperative to accurately document the most specific diagnosis in the assessment impression section of the note
bull Documented Lower Level (I) The documentation substantiates a lower level of service than charged
Chart Level Comments
Group your comments in categoriesoDocumentationo E amp MoProceduresoModifierso ICD-10-CM
oReportsAudit Manager Macros 061218 (version 1)xlsx
Recommendations and ReferencesCategory Short Description Long Description
EM AdmissionDischarge Same Day Review the CMS AdmissionDischarge same day coding guidelines httpswwwcmsgovRegulations-and-GuidanceGuidanceManualsDownloadsclm104c12pdf
EM ConsultationReview the consultation guidelines located in the CPT book
EM Consultation not billable to Medicare CMS no longer recognizes the consultation codeshttpswwwcmsgovOutreach-and-EducationMedicare-Learning-Network-MLNMLNMattersArticlesdownloadsmm6740pdf
EM Critical CareReview the CMS Critical Care guidelines httpswwwcmsgovOutreach-and-EducationMedicare-Learning-Network-MLNMLNMattersArticlesdownloadsmm5993pdf
EM Discharge ServicesReview the CMS Hospital Discharge Services guidelineshttpswwwcmsgovOutreach-and-EducationMedicare-Learning-Network-MLNMLNMattersArticlesdownloadsmm5794pdf
EMEM and Preventive Visit Review AAPC guidance for documenting and billing an EM and Preventive visit same day httpswwwaapccomblog22580-successfully-bill-a-
preventive-service-with-a-sick-visit
EM EM documentation guidelines Review the CMS 1995 amp 1997 EM documentation guidelineshttpswwwcmsgovOutreach-and-EducationMedicare-Learning-Network-MLNMLNEdWebGuideEMDOChtml
EM EM Inpatient vs Outpatient Review the patientrsquos status on the hospital admission order to determine the appropriate EM category to bill (inpatient vs observation)
EM EM New vs EstablishedReview the CMS New vs Established patient guidelines httpswwwcmsgovOutreach-and-EducationMedicare-Learning-Network-MLNMLNProductsDownloadseval-mgmt-serv-guide-ICN006764pdf
EMEM Time billing suggestion
Recommend a time statement is added to the EM medical record when a majority of the visit is spent counseling andor coordination of care Review the CMS 1995 amp 1997 EM documentation guidelines for EM time documentationhttpswwwcmsgovOutreach-and-EducationMedicare-Learning-Network-MLNMLNEdWebGuideEMDOChtml
EM Inpatient hospital servicesReview the CMS Hospital Services (Initial and Subsequent) guidelines httpswwwcmsgovRegulations-and-GuidanceGuidanceManualsDownloadsclm104c12pdf
EM Nursing Facility Services Review the Nursing Facility Services guidelines provided by CMS The guidelines can be downloaded at this linkhttpswwwcmsgovRegulations-and-GuidanceGuidanceManualsDownloadsclm104c12pdf
EM Observation Services Review the CMS Observation Services (Initial and Subsequent) guidelines httpswwwcmsgovRegulations-and-GuidanceGuidanceManualsDownloadsclm104c12pdf
EM Prolonged Services Review the CMS Prolonged Services guidelines httpswwwcmsgovOutreach-and-EducationMedicare-Learning-Network-MLNMLNMattersArticlesdownloadsmm5972pdf
EMReview of Systems Review the CMS 1995 amp 1997 EM documentation guidelines for Review of Systems requirements
httpswwwcmsgovOutreach-and-EducationMedicare-Learning-Network-MLNMLNEdWebGuideEMDOChtml
EMConsultation Documentation Suggestion
Recommend adding verbiage to consultation documentation that indicates the name of the referring provider and the reason for the consultation
Audit Report Examples Automated Solution
Letrsquos look at some report Examples
ReportsStandard Provider Audit SummarypdfReportsProvider Detailed Sample Reportdocx
ReportsProvider Audit Worksheets - Optionalpdf
Audit Report Examples Non Automated Solution
Error Findings by Volume Percentage
CPT Coded Accurately
8 8 Overcoded
8 8 Undercoded
Missed CPTHCPCS Code
Missed or Wrong Modifier
8 8 Incorrect CPT (or Category) Used
Incorrect ICD-9 Codes
8 8 Incorrect Quantity
Inadequate Documentation
Missing Documentation 8 8
Signature Illegible (No Log)
8 8
CLIENT NAME PROJECT TITLE
Review Line Item Detail Prepared Month Year
DRAFT
Client Claim Demographics Client Charge Data Review Result EampM ONLY Findings C C C C C C O OC O O O
Char
t Num
ber
Au
dit D
ate
Audi
tor (
initi
als)
QA
Initi
als
Fa
cilit
y Lo
catio
n Re
porte
d
Pr
ovid
er N
ame
Pa
tient
Nam
e
M
edic
al R
ecor
d Nu
mbe
r
Prim
ary
Carr
ier M
edica
re=
A M
edica
id =
B O
ther
=O
Da
te o
f Ser
vice
CP
T Co
de
Mod
ifier
(s) i
n or
der
Qua
ntity
Diag
nosi
s Co
de(s
) 1
thro
ugh
4
Fe
e ch
arge
d
Pr
imar
y Pa
ymen
t Am
ount
CPT
Code
Mod
ifier
(s) i
n or
der
Qua
ntity
Diag
nosi
s Co
de(s
) 1
thro
ugh
4
CO
RREC
T AL
LOW
ABLE
Prim
ary
PAYM
ENT
Va
rianc
e
Chie
f Com
plai
nt
Hist
ory
Leve
l Sup
port
ed
Exam
Lev
el S
uppo
rted
Med
ical
Dec
Mak
ing
Supp
orte
d (o
r TIM
E)
CPT
Cod
ed A
ccur
atel
y
Ove
rcod
ed
Und
erco
ded
Mis
sed
CPT
HC
PCS
Cod
e
Mis
sed
or W
rong
Mod
ifier
Inco
rrec
t CPT
(or C
ateg
ory)
Use
d
Inco
rrec
t IC
D-9
Cod
es
Inco
rrec
t Qua
ntity
Inad
equa
te D
ocum
enta
tion
Mis
sing
Doc
umen
tatio
n
Sign
atur
e Ill
egib
le (N
o Lo
g)
No
Sign
atur
e by
Pro
vide
r of
Ser
vice
COMMENTS (abbreviations used) PF- PROBLEM FOCUSED EPF- EXPANDED PF DET- DETAILED COMP- COMPREHENSIVE SFWD- STRAIGHT FORWARD MOD- MODERATE MDM- MEDICAL DECISION MAKING
Char
t Num
ber
SAMPLE SAMPLE S MD SAMPLE SAMPLE XXXXX XXX 112001 99212 25 1 1 1234 2 5678 3 4
$30000 $2200 99212 25 1 1 1234 2 5678 3 4
$56400 $54200 YES
DET
CO
MP
MO
D
COMMENTS COMMENTS COMMENTS
0
1 2 3 4
1 2 3 4
$000 0
$30000 $2200 $56400 $54200 10 10 10 10 10 10 10 10 10 10 10 10 TOTALS 917 Error Rate by Volume
Error Findings by Volume 8 CPT Coded Accurately 8 Overcoded 8 Undercoded 8 Missed CPTHCPCS Code 8 Missed or Wrong Modifier 8 Incorrect CPT (or Category) Used 8 Incorrect ICD-9 Codes 8 Incorrect Quantity
Inadequate Documentation 8 8 Missing Documentation 8 Signature Illegible (No Log) 8 No Signature by Provider of Service
1200 Total
Net Payment Error Rate -24636
Primary Payments Total $ Audited Payment Total $ (Total Under Payments)
Total Over Payments
Net OverUnder Payment $
2200 56400
(54200)
Resources Used HCPCS and CPT CodeBook (Current or applilcable year) ICD-10-CM CodeBook (Current or applicable year) CMS 1995 and 1997 EM Guidelines CMS Claims Processing Manual 100-04 Medicare Claims Processing (PUB 100-04) CMS - National Coverage Determinations (NCDs) National Correct Coding Policy Manual Applicable Physician Version
Executive Summary Report
The executive summary provides readers with a short complete document highlighting import information included in the detailed report Executive summaries are created for the senior management readers that donrsquot have time to read the full report and need to walk away with an understanding of the issues and corrective actions
Some would say the executive summary could be written before the detailed report however it is difficult to make sure the most important elements are included until you have spent time reviewing the detail If you want to make sure the most important messages are in the executive
summary this step should be completed after the detail is written As auditors become more seasoned this step could move to the front of the process
Executive Summary Report Structure of the ES Report
o Backgroundndash Specialtyndash Providersndash Sample Selection sizendash Date range of audit
o Audit Scopeo Regulatory Resourceso Type of Medical records reviewedo Overall Accuracy (all providers)o Detailed Audit Findings
ndash Business Impactndash Summary of Findings
o Department Findingso Summary
o ReportsStandard Executive Summary Professional Servicespdf
Department Findings Top Issues
Date ofServiceErrors
MissingDocuments
Missing orInvalid
Signature
TeachingPhysician
Errors
InsufficientConsultation
Documents
OverCoding
EMBundled
IntoGlobal
SurgicalPackage
SplitSharedServiceError
Incorrector
MissingPricing
Modifier
ICD-10Errors
Family Practice
CardiologyInternal Medicine
TOTALS
Top Findings by Provider
E amp M Accuracy Rates
ICD-10-CM Accuracy Rates
Procedure Accuracy Rates
Inpatient DRG Audit Report
TABLE OF CONTENTS
Executive Summaryo Scope of Work
Reimbursement Changes Department Results
o InpatientGeneral Recommendations and Comments
o Secondary DiagnosesoProcedure CodingoPresent on AdmissionoQueries
Scope of WorkCodingAID performed coding audit review of 175 inpatient records The review completed was a random sample that included cases coded by twenty coders for dates of service from May 2016 ndash July 2016
The objective was to determine if the medical record documentation supported the following coding and documentation requirements and any other regulatory requirement for that code set Criteria reviewed
1 ICD-10-CM Official Coding Guidelines for accurate diagnosis code reporting 2 ICD-10-PCS Official Coding Guidelines for accurate procedure code reporting 3 Documentation of procedure compared to the CPT code assigned 4 Identify opportunities for education and training 5 Financial impact of current coding practices
The regulatory agencies and reference materials relied upon include the following in addition to Medicare and Medicaid regulations Additional resources are located in the sub sections below
bull ICD-10-CM and ICD-10-PCS for Hospitals current volume bull Centers for Medicare and Medicaid Services CMS NCCI Edits-Centers for Medicaid and
Medicare Services CMS website wwwcmsgov bull AHA Coding Clinic
The following electronic medical record documents were reviewed and relied upon to compare to the actual codes submitted to the third party payer
bull Discharge summaries HampPs Progress Notes and other provider notes located in the EMR Records
bull Patient History Forms Ancillary Staff Notes bull Procedure Notes bull Orders bull Diagnostic Report
Reimbursement Changes
Coder Acct
Billed Audited
Reimbursement ChangesMS DRG SOI ROM Weight Expected
Payment MS DRG SOI ROM Weight Expected Payment
Coder 1 001 790 52300 $2615000 792 21552 $1077600 -$1537400
Coder 2002
749 26452 $1322600 758 10090 $504500 -$818100
Coder 3 003 669 13111 $655550 694 07294 $364700 -$290850
Coder 4 004 389 08707 $435350 394 09502 $475100 $39750
Coder 5 005 312 07630 $381500 812 08572 $428600 $47100
Coder 6 006 384 08481 $424050 378 09949 $497450 $73400
Coder 7 007 206 08164 $408200 794 12987 $649350 $241150
Coder 8008
344 31029 $1551450 853 51334 $2566700 $1015250
TOTAL $7793700 $6564000 -$1229700
General Recommendations and CommentsFinding Pertinent secondary diagnoses are not coded and diagnoses are code which are not supported in provider documentation Code only those diagnoses which are documented by the provider on the current chart Not all codes are coded to the highest degree of specificity and combination codes were sometimes missed
Recommendation It is important to assign codes for all conditions which meet the definition of a reportable diagnosis Documentation from all providers should be used including but not limited to radiologists pathologists anesthesiologists CRNAs and FNPs
Reference Coding Clinic Official Coding Guidelines
bull Report all secondary diagnoses which meet the definition of a secondary diagnosis which is defined as all conditions that coexist at the time of admission that develop subsequently or that affect the treatment received andor the length of stay Codes which enhance the overall picture of the patientrsquos visit should be added
o Add T45515A to report adverse effect of Coumadin which caused the GI bleed
o Add I2690 for septic pulmonary emboli (MCCSOI4ROM4)
o Add N179 for acute kidney failure (S3M2CC) per the nephrology consult and the 628 progress note
o Add code I429 cardiomyopathy per HampP
o Add B964 to report proteus in a UTI per the 620 hospitalist progress note
o Code for D649 anemia and I701 stenosis of renal artery should be added as secondary diagnoses per the HampP
bull Only report diagnoses which are substantiated by provider documentation in the current chart notes If a suspected condition is not verified at discharge on an inpatient account it cannot be coded
o Remove G4734 (idiopathic sleep related non-obstructive alveolar hypoventilation) as patient was noted to have the sleep study and the hypoventilation was shown to be a possibility but not noted as such on discharge
o Remove G629 (S21) the neuropathy is documented as due to diabetes
o Remove K529 colitis noted on HP as possible but not further noted or confirmed at discharge
Procedure CodingFinding Procedures were sometimes coded incorrectly
Recommendation The entire medical record should be reviewed and all procedures coded as documented Coding procedures incorrectly or assigning incorrect CPT codes may result in lost revenue
bull Incorrect root operation
o Revise principal procedure to 0DQ68ZZ for clipping of the ulcer per OP report clipping is root operation repair
bull Biopsy versus Excision
o Procedure 0DBA0ZX (biopsy of jejunum) should change to 0DBA0ZZ (excision of jejunum) per op note this was not a biopsy procedure
bull Coding Guideline error
o Remove 0RG10K0 for allograft due to being inclusive in principal procedure
o Remove codes for adhesiolysis 0DN80ZZ 0UN10ZZ and 0UN90ZZ due to no significance noted per OP report
bull Incorrect approach
o Revise 0TF63ZZ (fragmentation percutaneous approach) to 0TF68ZZ (fragmentation endoscopic) for procedure performed via scope per the operative report
bull Procedure coded without provider documentation
o Remove secondary procedure of excisional debridement (0JB90ZZ) due to lack of documentation of excisional debridement per operative report The header in the operative report documents IampD and debridement but the body of the operative report only documents an IampD
bull Incorrect CPT code assignment
o Post-op note supports the nerve block injections of four nerves therefore code 64421 (multiple nerve block) should replace 64420 (injection of one intercostal nerve)
Queries Finding Conflicting incomplete and vague documentation is found within provider chart notes
Recommendation Prior to code assignment if the coder finds ambiguous or conflicting documentation the provider should be queried
Reference AHA Coding Clinic 2002 2nd Quarter pages 17-18
bull Query for acute blood loss anemia since hgb has dropped and patient is being transfused PRBC
bull Recommend query to clarify if cardiorenal syndrome is current as it is documented per 627 nephrology consult but unclear if current
bull Documentation does not support SIRS noninfectious without organ failure It is conflicting since patient has respiratory failure Query should be initiated for clarification with or without organ failure or infectious or non-infectious Patient has pneumonia per query as well as last progress note therefore if SIRS is not further specified per query PNA should be sequenced as principal diagnosis and SIRS should be removed
bull Recommend provider query necrotizing lung consolidation noted on DS as principal diagnosis-unclear does the patient have lobar pneumonia Secondary dx states necrotic pneumonia which is coded as principal diagnosis-this diagnosis is clear but consolidation portion is unclear
bull Recommend query for preterm labor delivery at 301 weeks
bull RECOMMEND QUERY no chest pain on admit per ER and HP cardiology provider states no CP with ER stating chest pressure the day prior to admit Appears patient was admitted due to elevated troponins which cardiology says are likely due to hypotension and AKI DS states chest pain but also says bradycardia and hypotension were the reason for admit
bull RECOMMEND QUERY no chest pain on admit per ER and HP cardiology provider states no CP with ER stating chest pressure the day prior to admit Appears patient was admitted due to elevated troponins which cardiology says are likely due to hypotension and AKI DS states chest pain but also says bradycardia and hypotension were the reason for admit
bull Query the provider regarding pathology report notation of endometriosis andor possible re-sequence of stenosis as principal diagnosis as it also meets principal diagnosis guidelines This would result in an MS-DRG change to 742 and APR-DRG change to 513
bull QUERY secondary diagnosis MCC and ROM 4 code T3166 (60 TBSA of which 60 are third degree burns) Chart notes do not specify how much of TBSA was actually third degree If after query TBSA is found to be less than 50 (T3164) then ROM will change from 4 to 3 but no change to overall APR-DRG or weight
Auditor Quality amp Productivity
Audit Productivity Standards
It takes twice as long to audit a chart as it does to code it a statistic that takes into account the time to document an explanation of any coding decision the auditor is not in agreement with o For example in an emergency department audit with a productivity of 12
charts per hour for a coder our auditors would probably be able to review six per hour
o If there are multiple services to audit on each encounter the productivity may only be 4 per hour
o The amount of detail you put into your audit report will also be a factorndash Are you using an automated audit softwarendash Are you using a spreadsheet to auditndash How many Systems are needed to complete the audit
Coder Quality Audits
Quality Audits (QA) should be done on your coders and auditors regularly Frequent reviews with smaller sample size will allow more consistent
review and feedbacko Example 10 charts per month per coder if the coder passes 2-3 months
consecutively with 95 or better score move them to quarterly reviewso Some QA programs review a percentage of the coders work This
methodology requires more time and resources
Auditor QA should also score and comment on the accuracy of the audit comments and recommendations
Presenting the Audit Results
Presenting the Audit Results
Communicating the Audit FindingsoWho requested the AuditoWho are you reporting the finding to
ndash CEOndash CFOndash Physicianndash Revenue Cycle Managerndash HIM Directorndash Billing Managerndash Coding Manager
ReportsAudit Resultspptx
Post Audit Education
Provider Education
Provider Education is best received when it is specific to the provider(s) 11 sessions going over the audit result Look at their notes with them
oHighlight areas for documentation improvementoReinforce Coding Guidelines that are specific to themoAsk them to share how they establish their LOS for E amp M serviceso Integrate their EMR system into the training
Provider Education
Group Training SessionsoUse the audit results to identify common issues within a specialty group
ndash Refer to the Executive Summary reportoVery effective for identifying system issues
ndash Teaching Attestationsndash Templatesndash Copy and Pastendash Cloned notes
o Everyone hears the same messagesoAn Issue may not appear on the individual audit but is still a concern for the
group
Education Delivery
In person or remote sessionso Factors to consider
ndash Providers scheduleavailabilityndash Location(s)ndash Personality of the providerndash Budget
Coder Education
Coders do well in group training so they can learn from each other 11 training allows the coder to get feedback on their coding
Handling Audit Disputes
Handling Audit Disputes
Be open to all points of viewo Let the documentation tell the story
Refer to the guidelines Ask
oCan we defend the reported service with the current documentation
Self Disclosures Refunds and Corrected Billing
Overpayment
In general If a person has received an overpayment the person shallo report and return the overpayment to the Secretary the State an
intermediary a carrier or a contractor as appropriate at the correct address and ndash notify the Secretary State intermediary carrier or contractor to whom the overpayment was returned in writing of the reason for the overpayment
What is an ldquoOverpaymentrdquo ndash The term ldquooverpaymentrdquo means any funds that a person receives or retains under subchapter XVIII or XIX of this chapter to which the person after applicable reconciliation is not entitled under such subchapter
Self Disclosure
The Office of Inspector General (OIG) has several self-disclosure processes that can be used to report potential fraud in Department of Health and Human Services (HHS) programs Choose the one that applies to you from the following descriptions to learn moreo Health Care Provider Self-Disclosures
ndash Health care providers suppliers or other individuals or entities subject to Civil Monetary Penalties can use the Provider Self-Disclosure Protocol which was created in 1998 to voluntarily disclose self-discovered evidence of potential fraud Self-disclosure gives providers the opportunity to avoid the costs and disruptions associated with a Government-directed investigation and civil or administrative litigation Visit the Provider Self-Disclosure Protocol webpage for more information
o HHS Contractor Self-Disclosuresndash Contractors are individuals businesses or other legal entities that are awarded Government contracts or
subcontracts to provide services to the Department of Health and Human Services (HHS) OIGs contractor self-disclosure program enables contractors to self-disclose potential violations of the False Claims Act and various Federal criminal laws involving fraud conflict of interest bribery or gratuity This self-disclosure process is available for those entities with a Federal Acquisition Regulation-based contract Visit the Contractor Self-Disclosure webpage for more information
o HHS Grantee Self-Disclosuresndash HHS grantees or subrecipients may voluntarily disclose evidence of potential violations of Federal criminal law
involving fraud bribery or gratuity violations potentially affecting the Federal award 45 CFR 75113 notes mandatory disclosures of criminal offenses that non-Federal entities must make with respect to HHS grants Recipients submitting disclosures in connection with this requirement should include the subject reference line Mandatory Grant Disclosure Recipients choosing to disclose conduct that may not fit squarely within the scope of offenses described in 45 CFR 75113 should include the following subject reference line in the submission Voluntary Grant Disclosure
Medicare 60 day rule
The 60 Day Rule (Medicare Parts A amp B) o The 60 day time period for reportingreturning begins when either
ndash The reasonable diligence is completed orndash On the day the provider received credible information of a potential overpayment (if the
provider fails to conduct reasonable diligence) o For an investigation to be conducted in a ldquotimelyrdquo manner providers typically
must complete the investigation within 6 months from receipt of credible information indicating there may be an overpayment
ndash ndash 6-month timeframe may potentially be extended under ldquoextraordinary circumstancesrdquo ndash 8 months generally the maximum total time to return overpayments The government recommends that providers maintain records documenting ldquoreasonable diligencerdquo
Medicare 60 Day Rule
Six-year lookback period ndash Sometimes possible to use a shorter period depending on the facts at issue Amount to be repaid ndash May vary depending on the method used to
reportreturn eg Medicare administrative contractor (ldquoMACrdquo) v self-disclosure Overpayment notification ndash After receiving an overpayment
notification from the government you should investigate for related overpayments eg other time periods
Medicare 60 Day Rule
Self-disclosure protocols ndashoA submission to the OIG or CMS protocols suspends the 60 day requirement
for returning overpayments until a settlement agreement is executed ndash ndash OIGrsquos Self-Disclosure Protocol (SDP) ndash ndash CMS Voluntary Self-Referral Disclosure Protocol (SRDP) ndash
o Self-disclosures to other agencies do not suspend the repayment deadlinendash ndash Eg Department of Justice local US Attorneyrsquos Office Medicaid Fraud Control Unit
Medicare 60 Day Rule
Facilitating Compliance With the 60 Day Rule Compliance programs should include o ndash Appropriate policies and procedures o ndash Periodic billing and coding audits to proactively identify overpaymentso ndash Focus on high-risk areas o ndash Utilization of publicly available government resources to guide audit efforts o ndash Investigating any suspected incidents of non-compliance with federal health
care program requirements
Self Disclosure
Choice of AgencyoOIG ndash Self-Disclosure Protocol
ndash ndash Conduct involving false billingndash ndash Conduct involving excluded personsndash ndash Conduct involving the Anti-Kickback Statute (including conduct thatndash violates both the AKS and Stark Law)
oCMS ndash Self-Referral Disclosure Protocolndash ndash Conduct involving only violations of the Stark Law
oDOJndash ndash May be appropriate when provider believes a FCA release is necessary
Summary
The Cost of a Well-Executed Coding Audit ProcessThe costs associated with an auditing program are worth it in the long run Ideally your organization is performing audits on a regular basis across all service types locations and payers Weve all seen claims that have been denied resulting in additional work that may be preventable with a proper audit program The goal is to use the audit feedback to improve coding quality and lower potential risk and cost to the organization Organizations should be investing in an effective coding audit program to make your coders and providers better and enhance documentation improvement from the providers
Questions
Thank you for your attentionLynn Handy
Vice President of Coding amp Audit ServicesLynnhandymanagedresourcesinccom

Audit Reports
Goals of the Audit Report
The main goal of an audit report is to communicate where the organization specialty department provider or coder does or does not conform to regulatory standards guidelines and organizational policieso Each identified issue must have a standard it is measured againsto Site the regulation in your audit report or include a link to the regulation
Audit reports should not just contain negative findings Outline the Positives also Identify opportunities for improvement this can be in the form of a
recommendation Prioritize High Risk Findings
Who will be reading the Audit Report
What is the technical knowledge of the readeroCodersHIM ProfessionalsoProvidersoClinical StaffoHIM DirectorsoBillingCoding DirectorsManagersoCEOCFO (Executive Team)
Audit Report Format Tips
Provide perspective for the readero Positive and Negative findings
Be precise avoid redundant phrasing inexact terminology Avoid long sentences when a shorter one will work Avoid stating your opinion State the findings and facts Use bullet points this helps to break up difficult information and makes it
clearer for the reader Use gender neutral terms Avoid audit ldquobuzzwordsrdquo such as ldquogenerally improvedrdquo or ldquosignificant riskrdquo Avoid abbreviations unless they are clearly defined
Benefits of Automating your Audit Reports Results
o Consistent Resultso Better Datao Increases Efficiency
Trackingo Allows audit results to be tracked by provider and by specialty
QAo Allows for an automated approach to your internal quality reviews
Trendingo Allows for data analysis at a detailed level that can be tracked
Productivityo Increases auditor productivityo Decreases re-work
ProviderCoder Audit Reports
Detailed Audit reports should have the ability to be sorted byoProvideroCodero Specialty or GroupoAudit Date
Detailed results for each encounteroMeaningful comments
Key Findingso From all encounters
Recommendations and Resources
Detailed Findings Patient ID Patient Name DOS Payer CPT Reported CPT Audited EM Level Key Component ICD Reported ICD Reported Description ICD Audited ICD Reported Description
1 001 Patient A 02-19-16 Blue Cross
99203 25 1 99202 1 +1 D E L 1 S92302A2 Not Reported
1 Fracture of unspecified metatarsal bone(s) left foot initial encounter for closed fracture
1 S92355D2 W109XXD
1 Nondisplaced fracture of fifth metatarsal bone left foot subsequent encounter for fracture with routine healing2 Fall (on) (from) unspecified stairs and steps subsequent encounter
1 The documentation supports coding for an EM service that is one level below the billed code2 Lacking Exam documentation to support the EM level selected3 1997 MSK exam supports an Expanded Problem Focused exam (99202) 1995 exam supports a Detailed exam (99203)4 1997 Exam template suggestions Neurologic Exam-suggest adding the body part examined (upper extremitylow extremity) Dermatologic Exam-unable to determine if this was performed This should be deleted from the final note if
not examined5 EM time statement is insufficient documentation is lacking a required element total time of visit and counseling time greater than 506 CPT disallowed documentation is not present within the medical record to support the CPT code billed (28485-open treatment of metatarsal fracture includes internal fixation when performed) Fracture care is not supported patient
was seen in the ER 6 weeksrsquo prior ER doctor initiated treatment7 The incorrect pricing modifier was billed Removed modifier 25 (separate and significant EM on the same day as a minor procedure) Fracture care is not billable no modifier needed on EM service8 Diagnosis billed is not the most specific available according to the medical record documentation9 Documentation supports an additional diagnosis code not billed
2 002 Patient B 02-05-16 Blue Cross
99203 25 1 99202 25 1 +1 D E L 1 L03032 1 Cellulitis of left toe 1 L03032 1 Cellulitis of left toe
1 The documentation supports coding for an EM service that is one level below the billed code2 Lacking Exam documentation to support the EM level selected3 1997 MSK exam supports an Expanded Problem Focused exam (99202) 1995 exam supports a Detailed exam (99203)4 EM time statement is insufficient documentation is lacking one or more required elements (total time counseling time greater than 50) If a procedure is performed during a visit the time spent performing the procedure needs to be
carved out of the total visit time5 Allowed modifier 25 due to commercial payer Medicare and NCCI do not require modifier 25 on a new patient EM when a minor procedure is performed the same day 6 Diagnosis supported
Detailed Findings
135 822012 New Consultations - Office
Consultations Detailed Detailed (95) Moderate 99244 99243 1 $3500 N
Provider Code 99244 Reviewer Code 99243 Provider Diagnosis 1 3005 NEURASTHENIA Reviewer Diagnosis 1 3005 NEURASTHENIA Provider Diagnosis 2 7282 MUSC DISUSE ATROPHY NEC Reviewer Diagnosis 2 7282 MUSC DISUSE ATROPHY NEC
bull Assessment (I) The assessment is not clearly stated for this encounter Documentation Guidelines states The documentation for each patient encounter should include assessment clinical impression or diagnosis bull Assessment (R) The assessment should be clearly documented for each encounter Since each note must stand alone it is imperative to accurately document the most specific diagnosis in the assessment impression section of the note
bull Documented Lower Level (I) The documentation substantiates a lower level of service than charged
Chart Level Comments
Group your comments in categoriesoDocumentationo E amp MoProceduresoModifierso ICD-10-CM
oReportsAudit Manager Macros 061218 (version 1)xlsx
Recommendations and ReferencesCategory Short Description Long Description
EM AdmissionDischarge Same Day Review the CMS AdmissionDischarge same day coding guidelines httpswwwcmsgovRegulations-and-GuidanceGuidanceManualsDownloadsclm104c12pdf
EM ConsultationReview the consultation guidelines located in the CPT book
EM Consultation not billable to Medicare CMS no longer recognizes the consultation codeshttpswwwcmsgovOutreach-and-EducationMedicare-Learning-Network-MLNMLNMattersArticlesdownloadsmm6740pdf
EM Critical CareReview the CMS Critical Care guidelines httpswwwcmsgovOutreach-and-EducationMedicare-Learning-Network-MLNMLNMattersArticlesdownloadsmm5993pdf
EM Discharge ServicesReview the CMS Hospital Discharge Services guidelineshttpswwwcmsgovOutreach-and-EducationMedicare-Learning-Network-MLNMLNMattersArticlesdownloadsmm5794pdf
EMEM and Preventive Visit Review AAPC guidance for documenting and billing an EM and Preventive visit same day httpswwwaapccomblog22580-successfully-bill-a-
preventive-service-with-a-sick-visit
EM EM documentation guidelines Review the CMS 1995 amp 1997 EM documentation guidelineshttpswwwcmsgovOutreach-and-EducationMedicare-Learning-Network-MLNMLNEdWebGuideEMDOChtml
EM EM Inpatient vs Outpatient Review the patientrsquos status on the hospital admission order to determine the appropriate EM category to bill (inpatient vs observation)
EM EM New vs EstablishedReview the CMS New vs Established patient guidelines httpswwwcmsgovOutreach-and-EducationMedicare-Learning-Network-MLNMLNProductsDownloadseval-mgmt-serv-guide-ICN006764pdf
EMEM Time billing suggestion
Recommend a time statement is added to the EM medical record when a majority of the visit is spent counseling andor coordination of care Review the CMS 1995 amp 1997 EM documentation guidelines for EM time documentationhttpswwwcmsgovOutreach-and-EducationMedicare-Learning-Network-MLNMLNEdWebGuideEMDOChtml
EM Inpatient hospital servicesReview the CMS Hospital Services (Initial and Subsequent) guidelines httpswwwcmsgovRegulations-and-GuidanceGuidanceManualsDownloadsclm104c12pdf
EM Nursing Facility Services Review the Nursing Facility Services guidelines provided by CMS The guidelines can be downloaded at this linkhttpswwwcmsgovRegulations-and-GuidanceGuidanceManualsDownloadsclm104c12pdf
EM Observation Services Review the CMS Observation Services (Initial and Subsequent) guidelines httpswwwcmsgovRegulations-and-GuidanceGuidanceManualsDownloadsclm104c12pdf
EM Prolonged Services Review the CMS Prolonged Services guidelines httpswwwcmsgovOutreach-and-EducationMedicare-Learning-Network-MLNMLNMattersArticlesdownloadsmm5972pdf
EMReview of Systems Review the CMS 1995 amp 1997 EM documentation guidelines for Review of Systems requirements
httpswwwcmsgovOutreach-and-EducationMedicare-Learning-Network-MLNMLNEdWebGuideEMDOChtml
EMConsultation Documentation Suggestion
Recommend adding verbiage to consultation documentation that indicates the name of the referring provider and the reason for the consultation
Audit Report Examples Automated Solution
Letrsquos look at some report Examples
ReportsStandard Provider Audit SummarypdfReportsProvider Detailed Sample Reportdocx
ReportsProvider Audit Worksheets - Optionalpdf
Audit Report Examples Non Automated Solution
Error Findings by Volume Percentage
CPT Coded Accurately
8 8 Overcoded
8 8 Undercoded
Missed CPTHCPCS Code
Missed or Wrong Modifier
8 8 Incorrect CPT (or Category) Used
Incorrect ICD-9 Codes
8 8 Incorrect Quantity
Inadequate Documentation
Missing Documentation 8 8
Signature Illegible (No Log)
8 8
CLIENT NAME PROJECT TITLE
Review Line Item Detail Prepared Month Year
DRAFT
Client Claim Demographics Client Charge Data Review Result EampM ONLY Findings C C C C C C O OC O O O
Char
t Num
ber
Au
dit D
ate
Audi
tor (
initi
als)
QA
Initi
als
Fa
cilit
y Lo
catio
n Re
porte
d
Pr
ovid
er N
ame
Pa
tient
Nam
e
M
edic
al R
ecor
d Nu
mbe
r
Prim
ary
Carr
ier M
edica
re=
A M
edica
id =
B O
ther
=O
Da
te o
f Ser
vice
CP
T Co
de
Mod
ifier
(s) i
n or
der
Qua
ntity
Diag
nosi
s Co
de(s
) 1
thro
ugh
4
Fe
e ch
arge
d
Pr
imar
y Pa
ymen
t Am
ount
CPT
Code
Mod
ifier
(s) i
n or
der
Qua
ntity
Diag
nosi
s Co
de(s
) 1
thro
ugh
4
CO
RREC
T AL
LOW
ABLE
Prim
ary
PAYM
ENT
Va
rianc
e
Chie
f Com
plai
nt
Hist
ory
Leve
l Sup
port
ed
Exam
Lev
el S
uppo
rted
Med
ical
Dec
Mak
ing
Supp
orte
d (o
r TIM
E)
CPT
Cod
ed A
ccur
atel
y
Ove
rcod
ed
Und
erco
ded
Mis
sed
CPT
HC
PCS
Cod
e
Mis
sed
or W
rong
Mod
ifier
Inco
rrec
t CPT
(or C
ateg
ory)
Use
d
Inco
rrec
t IC
D-9
Cod
es
Inco
rrec
t Qua
ntity
Inad
equa
te D
ocum
enta
tion
Mis
sing
Doc
umen
tatio
n
Sign
atur
e Ill
egib
le (N
o Lo
g)
No
Sign
atur
e by
Pro
vide
r of
Ser
vice
COMMENTS (abbreviations used) PF- PROBLEM FOCUSED EPF- EXPANDED PF DET- DETAILED COMP- COMPREHENSIVE SFWD- STRAIGHT FORWARD MOD- MODERATE MDM- MEDICAL DECISION MAKING
Char
t Num
ber
SAMPLE SAMPLE S MD SAMPLE SAMPLE XXXXX XXX 112001 99212 25 1 1 1234 2 5678 3 4
$30000 $2200 99212 25 1 1 1234 2 5678 3 4
$56400 $54200 YES
DET
CO
MP
MO
D
COMMENTS COMMENTS COMMENTS
0
1 2 3 4
1 2 3 4
$000 0
$30000 $2200 $56400 $54200 10 10 10 10 10 10 10 10 10 10 10 10 TOTALS 917 Error Rate by Volume
Error Findings by Volume 8 CPT Coded Accurately 8 Overcoded 8 Undercoded 8 Missed CPTHCPCS Code 8 Missed or Wrong Modifier 8 Incorrect CPT (or Category) Used 8 Incorrect ICD-9 Codes 8 Incorrect Quantity
Inadequate Documentation 8 8 Missing Documentation 8 Signature Illegible (No Log) 8 No Signature by Provider of Service
1200 Total
Net Payment Error Rate -24636
Primary Payments Total $ Audited Payment Total $ (Total Under Payments)
Total Over Payments
Net OverUnder Payment $
2200 56400
(54200)
Resources Used HCPCS and CPT CodeBook (Current or applilcable year) ICD-10-CM CodeBook (Current or applicable year) CMS 1995 and 1997 EM Guidelines CMS Claims Processing Manual 100-04 Medicare Claims Processing (PUB 100-04) CMS - National Coverage Determinations (NCDs) National Correct Coding Policy Manual Applicable Physician Version
Executive Summary Report
The executive summary provides readers with a short complete document highlighting import information included in the detailed report Executive summaries are created for the senior management readers that donrsquot have time to read the full report and need to walk away with an understanding of the issues and corrective actions
Some would say the executive summary could be written before the detailed report however it is difficult to make sure the most important elements are included until you have spent time reviewing the detail If you want to make sure the most important messages are in the executive
summary this step should be completed after the detail is written As auditors become more seasoned this step could move to the front of the process
Executive Summary Report Structure of the ES Report
o Backgroundndash Specialtyndash Providersndash Sample Selection sizendash Date range of audit
o Audit Scopeo Regulatory Resourceso Type of Medical records reviewedo Overall Accuracy (all providers)o Detailed Audit Findings
ndash Business Impactndash Summary of Findings
o Department Findingso Summary
o ReportsStandard Executive Summary Professional Servicespdf
Department Findings Top Issues
Date ofServiceErrors
MissingDocuments
Missing orInvalid
Signature
TeachingPhysician
Errors
InsufficientConsultation
Documents
OverCoding
EMBundled
IntoGlobal
SurgicalPackage
SplitSharedServiceError
Incorrector
MissingPricing
Modifier
ICD-10Errors
Family Practice
CardiologyInternal Medicine
TOTALS
Top Findings by Provider
E amp M Accuracy Rates
ICD-10-CM Accuracy Rates
Procedure Accuracy Rates
Inpatient DRG Audit Report
TABLE OF CONTENTS
Executive Summaryo Scope of Work
Reimbursement Changes Department Results
o InpatientGeneral Recommendations and Comments
o Secondary DiagnosesoProcedure CodingoPresent on AdmissionoQueries
Scope of WorkCodingAID performed coding audit review of 175 inpatient records The review completed was a random sample that included cases coded by twenty coders for dates of service from May 2016 ndash July 2016
The objective was to determine if the medical record documentation supported the following coding and documentation requirements and any other regulatory requirement for that code set Criteria reviewed
1 ICD-10-CM Official Coding Guidelines for accurate diagnosis code reporting 2 ICD-10-PCS Official Coding Guidelines for accurate procedure code reporting 3 Documentation of procedure compared to the CPT code assigned 4 Identify opportunities for education and training 5 Financial impact of current coding practices
The regulatory agencies and reference materials relied upon include the following in addition to Medicare and Medicaid regulations Additional resources are located in the sub sections below
bull ICD-10-CM and ICD-10-PCS for Hospitals current volume bull Centers for Medicare and Medicaid Services CMS NCCI Edits-Centers for Medicaid and
Medicare Services CMS website wwwcmsgov bull AHA Coding Clinic
The following electronic medical record documents were reviewed and relied upon to compare to the actual codes submitted to the third party payer
bull Discharge summaries HampPs Progress Notes and other provider notes located in the EMR Records
bull Patient History Forms Ancillary Staff Notes bull Procedure Notes bull Orders bull Diagnostic Report
Reimbursement Changes
Coder Acct
Billed Audited
Reimbursement ChangesMS DRG SOI ROM Weight Expected
Payment MS DRG SOI ROM Weight Expected Payment
Coder 1 001 790 52300 $2615000 792 21552 $1077600 -$1537400
Coder 2002
749 26452 $1322600 758 10090 $504500 -$818100
Coder 3 003 669 13111 $655550 694 07294 $364700 -$290850
Coder 4 004 389 08707 $435350 394 09502 $475100 $39750
Coder 5 005 312 07630 $381500 812 08572 $428600 $47100
Coder 6 006 384 08481 $424050 378 09949 $497450 $73400
Coder 7 007 206 08164 $408200 794 12987 $649350 $241150
Coder 8008
344 31029 $1551450 853 51334 $2566700 $1015250
TOTAL $7793700 $6564000 -$1229700
General Recommendations and CommentsFinding Pertinent secondary diagnoses are not coded and diagnoses are code which are not supported in provider documentation Code only those diagnoses which are documented by the provider on the current chart Not all codes are coded to the highest degree of specificity and combination codes were sometimes missed
Recommendation It is important to assign codes for all conditions which meet the definition of a reportable diagnosis Documentation from all providers should be used including but not limited to radiologists pathologists anesthesiologists CRNAs and FNPs
Reference Coding Clinic Official Coding Guidelines
bull Report all secondary diagnoses which meet the definition of a secondary diagnosis which is defined as all conditions that coexist at the time of admission that develop subsequently or that affect the treatment received andor the length of stay Codes which enhance the overall picture of the patientrsquos visit should be added
o Add T45515A to report adverse effect of Coumadin which caused the GI bleed
o Add I2690 for septic pulmonary emboli (MCCSOI4ROM4)
o Add N179 for acute kidney failure (S3M2CC) per the nephrology consult and the 628 progress note
o Add code I429 cardiomyopathy per HampP
o Add B964 to report proteus in a UTI per the 620 hospitalist progress note
o Code for D649 anemia and I701 stenosis of renal artery should be added as secondary diagnoses per the HampP
bull Only report diagnoses which are substantiated by provider documentation in the current chart notes If a suspected condition is not verified at discharge on an inpatient account it cannot be coded
o Remove G4734 (idiopathic sleep related non-obstructive alveolar hypoventilation) as patient was noted to have the sleep study and the hypoventilation was shown to be a possibility but not noted as such on discharge
o Remove G629 (S21) the neuropathy is documented as due to diabetes
o Remove K529 colitis noted on HP as possible but not further noted or confirmed at discharge
Procedure CodingFinding Procedures were sometimes coded incorrectly
Recommendation The entire medical record should be reviewed and all procedures coded as documented Coding procedures incorrectly or assigning incorrect CPT codes may result in lost revenue
bull Incorrect root operation
o Revise principal procedure to 0DQ68ZZ for clipping of the ulcer per OP report clipping is root operation repair
bull Biopsy versus Excision
o Procedure 0DBA0ZX (biopsy of jejunum) should change to 0DBA0ZZ (excision of jejunum) per op note this was not a biopsy procedure
bull Coding Guideline error
o Remove 0RG10K0 for allograft due to being inclusive in principal procedure
o Remove codes for adhesiolysis 0DN80ZZ 0UN10ZZ and 0UN90ZZ due to no significance noted per OP report
bull Incorrect approach
o Revise 0TF63ZZ (fragmentation percutaneous approach) to 0TF68ZZ (fragmentation endoscopic) for procedure performed via scope per the operative report
bull Procedure coded without provider documentation
o Remove secondary procedure of excisional debridement (0JB90ZZ) due to lack of documentation of excisional debridement per operative report The header in the operative report documents IampD and debridement but the body of the operative report only documents an IampD
bull Incorrect CPT code assignment
o Post-op note supports the nerve block injections of four nerves therefore code 64421 (multiple nerve block) should replace 64420 (injection of one intercostal nerve)
Queries Finding Conflicting incomplete and vague documentation is found within provider chart notes
Recommendation Prior to code assignment if the coder finds ambiguous or conflicting documentation the provider should be queried
Reference AHA Coding Clinic 2002 2nd Quarter pages 17-18
bull Query for acute blood loss anemia since hgb has dropped and patient is being transfused PRBC
bull Recommend query to clarify if cardiorenal syndrome is current as it is documented per 627 nephrology consult but unclear if current
bull Documentation does not support SIRS noninfectious without organ failure It is conflicting since patient has respiratory failure Query should be initiated for clarification with or without organ failure or infectious or non-infectious Patient has pneumonia per query as well as last progress note therefore if SIRS is not further specified per query PNA should be sequenced as principal diagnosis and SIRS should be removed
bull Recommend provider query necrotizing lung consolidation noted on DS as principal diagnosis-unclear does the patient have lobar pneumonia Secondary dx states necrotic pneumonia which is coded as principal diagnosis-this diagnosis is clear but consolidation portion is unclear
bull Recommend query for preterm labor delivery at 301 weeks
bull RECOMMEND QUERY no chest pain on admit per ER and HP cardiology provider states no CP with ER stating chest pressure the day prior to admit Appears patient was admitted due to elevated troponins which cardiology says are likely due to hypotension and AKI DS states chest pain but also says bradycardia and hypotension were the reason for admit
bull RECOMMEND QUERY no chest pain on admit per ER and HP cardiology provider states no CP with ER stating chest pressure the day prior to admit Appears patient was admitted due to elevated troponins which cardiology says are likely due to hypotension and AKI DS states chest pain but also says bradycardia and hypotension were the reason for admit
bull Query the provider regarding pathology report notation of endometriosis andor possible re-sequence of stenosis as principal diagnosis as it also meets principal diagnosis guidelines This would result in an MS-DRG change to 742 and APR-DRG change to 513
bull QUERY secondary diagnosis MCC and ROM 4 code T3166 (60 TBSA of which 60 are third degree burns) Chart notes do not specify how much of TBSA was actually third degree If after query TBSA is found to be less than 50 (T3164) then ROM will change from 4 to 3 but no change to overall APR-DRG or weight
Auditor Quality amp Productivity
Audit Productivity Standards
It takes twice as long to audit a chart as it does to code it a statistic that takes into account the time to document an explanation of any coding decision the auditor is not in agreement with o For example in an emergency department audit with a productivity of 12
charts per hour for a coder our auditors would probably be able to review six per hour
o If there are multiple services to audit on each encounter the productivity may only be 4 per hour
o The amount of detail you put into your audit report will also be a factorndash Are you using an automated audit softwarendash Are you using a spreadsheet to auditndash How many Systems are needed to complete the audit
Coder Quality Audits
Quality Audits (QA) should be done on your coders and auditors regularly Frequent reviews with smaller sample size will allow more consistent
review and feedbacko Example 10 charts per month per coder if the coder passes 2-3 months
consecutively with 95 or better score move them to quarterly reviewso Some QA programs review a percentage of the coders work This
methodology requires more time and resources
Auditor QA should also score and comment on the accuracy of the audit comments and recommendations
Presenting the Audit Results
Presenting the Audit Results
Communicating the Audit FindingsoWho requested the AuditoWho are you reporting the finding to
ndash CEOndash CFOndash Physicianndash Revenue Cycle Managerndash HIM Directorndash Billing Managerndash Coding Manager
ReportsAudit Resultspptx
Post Audit Education
Provider Education
Provider Education is best received when it is specific to the provider(s) 11 sessions going over the audit result Look at their notes with them
oHighlight areas for documentation improvementoReinforce Coding Guidelines that are specific to themoAsk them to share how they establish their LOS for E amp M serviceso Integrate their EMR system into the training
Provider Education
Group Training SessionsoUse the audit results to identify common issues within a specialty group
ndash Refer to the Executive Summary reportoVery effective for identifying system issues
ndash Teaching Attestationsndash Templatesndash Copy and Pastendash Cloned notes
o Everyone hears the same messagesoAn Issue may not appear on the individual audit but is still a concern for the
group
Education Delivery
In person or remote sessionso Factors to consider
ndash Providers scheduleavailabilityndash Location(s)ndash Personality of the providerndash Budget
Coder Education
Coders do well in group training so they can learn from each other 11 training allows the coder to get feedback on their coding
Handling Audit Disputes
Handling Audit Disputes
Be open to all points of viewo Let the documentation tell the story
Refer to the guidelines Ask
oCan we defend the reported service with the current documentation
Self Disclosures Refunds and Corrected Billing
Overpayment
In general If a person has received an overpayment the person shallo report and return the overpayment to the Secretary the State an
intermediary a carrier or a contractor as appropriate at the correct address and ndash notify the Secretary State intermediary carrier or contractor to whom the overpayment was returned in writing of the reason for the overpayment
What is an ldquoOverpaymentrdquo ndash The term ldquooverpaymentrdquo means any funds that a person receives or retains under subchapter XVIII or XIX of this chapter to which the person after applicable reconciliation is not entitled under such subchapter
Self Disclosure
The Office of Inspector General (OIG) has several self-disclosure processes that can be used to report potential fraud in Department of Health and Human Services (HHS) programs Choose the one that applies to you from the following descriptions to learn moreo Health Care Provider Self-Disclosures
ndash Health care providers suppliers or other individuals or entities subject to Civil Monetary Penalties can use the Provider Self-Disclosure Protocol which was created in 1998 to voluntarily disclose self-discovered evidence of potential fraud Self-disclosure gives providers the opportunity to avoid the costs and disruptions associated with a Government-directed investigation and civil or administrative litigation Visit the Provider Self-Disclosure Protocol webpage for more information
o HHS Contractor Self-Disclosuresndash Contractors are individuals businesses or other legal entities that are awarded Government contracts or
subcontracts to provide services to the Department of Health and Human Services (HHS) OIGs contractor self-disclosure program enables contractors to self-disclose potential violations of the False Claims Act and various Federal criminal laws involving fraud conflict of interest bribery or gratuity This self-disclosure process is available for those entities with a Federal Acquisition Regulation-based contract Visit the Contractor Self-Disclosure webpage for more information
o HHS Grantee Self-Disclosuresndash HHS grantees or subrecipients may voluntarily disclose evidence of potential violations of Federal criminal law
involving fraud bribery or gratuity violations potentially affecting the Federal award 45 CFR 75113 notes mandatory disclosures of criminal offenses that non-Federal entities must make with respect to HHS grants Recipients submitting disclosures in connection with this requirement should include the subject reference line Mandatory Grant Disclosure Recipients choosing to disclose conduct that may not fit squarely within the scope of offenses described in 45 CFR 75113 should include the following subject reference line in the submission Voluntary Grant Disclosure
Medicare 60 day rule
The 60 Day Rule (Medicare Parts A amp B) o The 60 day time period for reportingreturning begins when either
ndash The reasonable diligence is completed orndash On the day the provider received credible information of a potential overpayment (if the
provider fails to conduct reasonable diligence) o For an investigation to be conducted in a ldquotimelyrdquo manner providers typically
must complete the investigation within 6 months from receipt of credible information indicating there may be an overpayment
ndash ndash 6-month timeframe may potentially be extended under ldquoextraordinary circumstancesrdquo ndash 8 months generally the maximum total time to return overpayments The government recommends that providers maintain records documenting ldquoreasonable diligencerdquo
Medicare 60 Day Rule
Six-year lookback period ndash Sometimes possible to use a shorter period depending on the facts at issue Amount to be repaid ndash May vary depending on the method used to
reportreturn eg Medicare administrative contractor (ldquoMACrdquo) v self-disclosure Overpayment notification ndash After receiving an overpayment
notification from the government you should investigate for related overpayments eg other time periods
Medicare 60 Day Rule
Self-disclosure protocols ndashoA submission to the OIG or CMS protocols suspends the 60 day requirement
for returning overpayments until a settlement agreement is executed ndash ndash OIGrsquos Self-Disclosure Protocol (SDP) ndash ndash CMS Voluntary Self-Referral Disclosure Protocol (SRDP) ndash
o Self-disclosures to other agencies do not suspend the repayment deadlinendash ndash Eg Department of Justice local US Attorneyrsquos Office Medicaid Fraud Control Unit
Medicare 60 Day Rule
Facilitating Compliance With the 60 Day Rule Compliance programs should include o ndash Appropriate policies and procedures o ndash Periodic billing and coding audits to proactively identify overpaymentso ndash Focus on high-risk areas o ndash Utilization of publicly available government resources to guide audit efforts o ndash Investigating any suspected incidents of non-compliance with federal health
care program requirements
Self Disclosure
Choice of AgencyoOIG ndash Self-Disclosure Protocol
ndash ndash Conduct involving false billingndash ndash Conduct involving excluded personsndash ndash Conduct involving the Anti-Kickback Statute (including conduct thatndash violates both the AKS and Stark Law)
oCMS ndash Self-Referral Disclosure Protocolndash ndash Conduct involving only violations of the Stark Law
oDOJndash ndash May be appropriate when provider believes a FCA release is necessary
Summary
The Cost of a Well-Executed Coding Audit ProcessThe costs associated with an auditing program are worth it in the long run Ideally your organization is performing audits on a regular basis across all service types locations and payers Weve all seen claims that have been denied resulting in additional work that may be preventable with a proper audit program The goal is to use the audit feedback to improve coding quality and lower potential risk and cost to the organization Organizations should be investing in an effective coding audit program to make your coders and providers better and enhance documentation improvement from the providers
Questions
Thank you for your attentionLynn Handy
Vice President of Coding amp Audit ServicesLynnhandymanagedresourcesinccom

Goals of the Audit Report
The main goal of an audit report is to communicate where the organization specialty department provider or coder does or does not conform to regulatory standards guidelines and organizational policieso Each identified issue must have a standard it is measured againsto Site the regulation in your audit report or include a link to the regulation
Audit reports should not just contain negative findings Outline the Positives also Identify opportunities for improvement this can be in the form of a
recommendation Prioritize High Risk Findings
Who will be reading the Audit Report
What is the technical knowledge of the readeroCodersHIM ProfessionalsoProvidersoClinical StaffoHIM DirectorsoBillingCoding DirectorsManagersoCEOCFO (Executive Team)
Audit Report Format Tips
Provide perspective for the readero Positive and Negative findings
Be precise avoid redundant phrasing inexact terminology Avoid long sentences when a shorter one will work Avoid stating your opinion State the findings and facts Use bullet points this helps to break up difficult information and makes it
clearer for the reader Use gender neutral terms Avoid audit ldquobuzzwordsrdquo such as ldquogenerally improvedrdquo or ldquosignificant riskrdquo Avoid abbreviations unless they are clearly defined
Benefits of Automating your Audit Reports Results
o Consistent Resultso Better Datao Increases Efficiency
Trackingo Allows audit results to be tracked by provider and by specialty
QAo Allows for an automated approach to your internal quality reviews
Trendingo Allows for data analysis at a detailed level that can be tracked
Productivityo Increases auditor productivityo Decreases re-work
ProviderCoder Audit Reports
Detailed Audit reports should have the ability to be sorted byoProvideroCodero Specialty or GroupoAudit Date
Detailed results for each encounteroMeaningful comments
Key Findingso From all encounters
Recommendations and Resources
Detailed Findings Patient ID Patient Name DOS Payer CPT Reported CPT Audited EM Level Key Component ICD Reported ICD Reported Description ICD Audited ICD Reported Description
1 001 Patient A 02-19-16 Blue Cross
99203 25 1 99202 1 +1 D E L 1 S92302A2 Not Reported
1 Fracture of unspecified metatarsal bone(s) left foot initial encounter for closed fracture
1 S92355D2 W109XXD
1 Nondisplaced fracture of fifth metatarsal bone left foot subsequent encounter for fracture with routine healing2 Fall (on) (from) unspecified stairs and steps subsequent encounter
1 The documentation supports coding for an EM service that is one level below the billed code2 Lacking Exam documentation to support the EM level selected3 1997 MSK exam supports an Expanded Problem Focused exam (99202) 1995 exam supports a Detailed exam (99203)4 1997 Exam template suggestions Neurologic Exam-suggest adding the body part examined (upper extremitylow extremity) Dermatologic Exam-unable to determine if this was performed This should be deleted from the final note if
not examined5 EM time statement is insufficient documentation is lacking a required element total time of visit and counseling time greater than 506 CPT disallowed documentation is not present within the medical record to support the CPT code billed (28485-open treatment of metatarsal fracture includes internal fixation when performed) Fracture care is not supported patient
was seen in the ER 6 weeksrsquo prior ER doctor initiated treatment7 The incorrect pricing modifier was billed Removed modifier 25 (separate and significant EM on the same day as a minor procedure) Fracture care is not billable no modifier needed on EM service8 Diagnosis billed is not the most specific available according to the medical record documentation9 Documentation supports an additional diagnosis code not billed
2 002 Patient B 02-05-16 Blue Cross
99203 25 1 99202 25 1 +1 D E L 1 L03032 1 Cellulitis of left toe 1 L03032 1 Cellulitis of left toe
1 The documentation supports coding for an EM service that is one level below the billed code2 Lacking Exam documentation to support the EM level selected3 1997 MSK exam supports an Expanded Problem Focused exam (99202) 1995 exam supports a Detailed exam (99203)4 EM time statement is insufficient documentation is lacking one or more required elements (total time counseling time greater than 50) If a procedure is performed during a visit the time spent performing the procedure needs to be
carved out of the total visit time5 Allowed modifier 25 due to commercial payer Medicare and NCCI do not require modifier 25 on a new patient EM when a minor procedure is performed the same day 6 Diagnosis supported
Detailed Findings
135 822012 New Consultations - Office
Consultations Detailed Detailed (95) Moderate 99244 99243 1 $3500 N
Provider Code 99244 Reviewer Code 99243 Provider Diagnosis 1 3005 NEURASTHENIA Reviewer Diagnosis 1 3005 NEURASTHENIA Provider Diagnosis 2 7282 MUSC DISUSE ATROPHY NEC Reviewer Diagnosis 2 7282 MUSC DISUSE ATROPHY NEC
bull Assessment (I) The assessment is not clearly stated for this encounter Documentation Guidelines states The documentation for each patient encounter should include assessment clinical impression or diagnosis bull Assessment (R) The assessment should be clearly documented for each encounter Since each note must stand alone it is imperative to accurately document the most specific diagnosis in the assessment impression section of the note
bull Documented Lower Level (I) The documentation substantiates a lower level of service than charged
Chart Level Comments
Group your comments in categoriesoDocumentationo E amp MoProceduresoModifierso ICD-10-CM
oReportsAudit Manager Macros 061218 (version 1)xlsx
Recommendations and ReferencesCategory Short Description Long Description
EM AdmissionDischarge Same Day Review the CMS AdmissionDischarge same day coding guidelines httpswwwcmsgovRegulations-and-GuidanceGuidanceManualsDownloadsclm104c12pdf
EM ConsultationReview the consultation guidelines located in the CPT book
EM Consultation not billable to Medicare CMS no longer recognizes the consultation codeshttpswwwcmsgovOutreach-and-EducationMedicare-Learning-Network-MLNMLNMattersArticlesdownloadsmm6740pdf
EM Critical CareReview the CMS Critical Care guidelines httpswwwcmsgovOutreach-and-EducationMedicare-Learning-Network-MLNMLNMattersArticlesdownloadsmm5993pdf
EM Discharge ServicesReview the CMS Hospital Discharge Services guidelineshttpswwwcmsgovOutreach-and-EducationMedicare-Learning-Network-MLNMLNMattersArticlesdownloadsmm5794pdf
EMEM and Preventive Visit Review AAPC guidance for documenting and billing an EM and Preventive visit same day httpswwwaapccomblog22580-successfully-bill-a-
preventive-service-with-a-sick-visit
EM EM documentation guidelines Review the CMS 1995 amp 1997 EM documentation guidelineshttpswwwcmsgovOutreach-and-EducationMedicare-Learning-Network-MLNMLNEdWebGuideEMDOChtml
EM EM Inpatient vs Outpatient Review the patientrsquos status on the hospital admission order to determine the appropriate EM category to bill (inpatient vs observation)
EM EM New vs EstablishedReview the CMS New vs Established patient guidelines httpswwwcmsgovOutreach-and-EducationMedicare-Learning-Network-MLNMLNProductsDownloadseval-mgmt-serv-guide-ICN006764pdf
EMEM Time billing suggestion
Recommend a time statement is added to the EM medical record when a majority of the visit is spent counseling andor coordination of care Review the CMS 1995 amp 1997 EM documentation guidelines for EM time documentationhttpswwwcmsgovOutreach-and-EducationMedicare-Learning-Network-MLNMLNEdWebGuideEMDOChtml
EM Inpatient hospital servicesReview the CMS Hospital Services (Initial and Subsequent) guidelines httpswwwcmsgovRegulations-and-GuidanceGuidanceManualsDownloadsclm104c12pdf
EM Nursing Facility Services Review the Nursing Facility Services guidelines provided by CMS The guidelines can be downloaded at this linkhttpswwwcmsgovRegulations-and-GuidanceGuidanceManualsDownloadsclm104c12pdf
EM Observation Services Review the CMS Observation Services (Initial and Subsequent) guidelines httpswwwcmsgovRegulations-and-GuidanceGuidanceManualsDownloadsclm104c12pdf
EM Prolonged Services Review the CMS Prolonged Services guidelines httpswwwcmsgovOutreach-and-EducationMedicare-Learning-Network-MLNMLNMattersArticlesdownloadsmm5972pdf
EMReview of Systems Review the CMS 1995 amp 1997 EM documentation guidelines for Review of Systems requirements
httpswwwcmsgovOutreach-and-EducationMedicare-Learning-Network-MLNMLNEdWebGuideEMDOChtml
EMConsultation Documentation Suggestion
Recommend adding verbiage to consultation documentation that indicates the name of the referring provider and the reason for the consultation
Audit Report Examples Automated Solution
Letrsquos look at some report Examples
ReportsStandard Provider Audit SummarypdfReportsProvider Detailed Sample Reportdocx
ReportsProvider Audit Worksheets - Optionalpdf
Audit Report Examples Non Automated Solution
Error Findings by Volume Percentage
CPT Coded Accurately
8 8 Overcoded
8 8 Undercoded
Missed CPTHCPCS Code
Missed or Wrong Modifier
8 8 Incorrect CPT (or Category) Used
Incorrect ICD-9 Codes
8 8 Incorrect Quantity
Inadequate Documentation
Missing Documentation 8 8
Signature Illegible (No Log)
8 8
CLIENT NAME PROJECT TITLE
Review Line Item Detail Prepared Month Year
DRAFT
Client Claim Demographics Client Charge Data Review Result EampM ONLY Findings C C C C C C O OC O O O
Char
t Num
ber
Au
dit D
ate
Audi
tor (
initi
als)
QA
Initi
als
Fa
cilit
y Lo
catio
n Re
porte
d
Pr
ovid
er N
ame
Pa
tient
Nam
e
M
edic
al R
ecor
d Nu
mbe
r
Prim
ary
Carr
ier M
edica
re=
A M
edica
id =
B O
ther
=O
Da
te o
f Ser
vice
CP
T Co
de
Mod
ifier
(s) i
n or
der
Qua
ntity
Diag
nosi
s Co
de(s
) 1
thro
ugh
4
Fe
e ch
arge
d
Pr
imar
y Pa
ymen
t Am
ount
CPT
Code
Mod
ifier
(s) i
n or
der
Qua
ntity
Diag
nosi
s Co
de(s
) 1
thro
ugh
4
CO
RREC
T AL
LOW
ABLE
Prim
ary
PAYM
ENT
Va
rianc
e
Chie
f Com
plai
nt
Hist
ory
Leve
l Sup
port
ed
Exam
Lev
el S
uppo
rted
Med
ical
Dec
Mak
ing
Supp
orte
d (o
r TIM
E)
CPT
Cod
ed A
ccur
atel
y
Ove
rcod
ed
Und
erco
ded
Mis
sed
CPT
HC
PCS
Cod
e
Mis
sed
or W
rong
Mod
ifier
Inco
rrec
t CPT
(or C
ateg
ory)
Use
d
Inco
rrec
t IC
D-9
Cod
es
Inco
rrec
t Qua
ntity
Inad
equa
te D
ocum
enta
tion
Mis
sing
Doc
umen
tatio
n
Sign
atur
e Ill
egib
le (N
o Lo
g)
No
Sign
atur
e by
Pro
vide
r of
Ser
vice
COMMENTS (abbreviations used) PF- PROBLEM FOCUSED EPF- EXPANDED PF DET- DETAILED COMP- COMPREHENSIVE SFWD- STRAIGHT FORWARD MOD- MODERATE MDM- MEDICAL DECISION MAKING
Char
t Num
ber
SAMPLE SAMPLE S MD SAMPLE SAMPLE XXXXX XXX 112001 99212 25 1 1 1234 2 5678 3 4
$30000 $2200 99212 25 1 1 1234 2 5678 3 4
$56400 $54200 YES
DET
CO
MP
MO
D
COMMENTS COMMENTS COMMENTS
0
1 2 3 4
1 2 3 4
$000 0
$30000 $2200 $56400 $54200 10 10 10 10 10 10 10 10 10 10 10 10 TOTALS 917 Error Rate by Volume
Error Findings by Volume 8 CPT Coded Accurately 8 Overcoded 8 Undercoded 8 Missed CPTHCPCS Code 8 Missed or Wrong Modifier 8 Incorrect CPT (or Category) Used 8 Incorrect ICD-9 Codes 8 Incorrect Quantity
Inadequate Documentation 8 8 Missing Documentation 8 Signature Illegible (No Log) 8 No Signature by Provider of Service
1200 Total
Net Payment Error Rate -24636
Primary Payments Total $ Audited Payment Total $ (Total Under Payments)
Total Over Payments
Net OverUnder Payment $
2200 56400
(54200)
Resources Used HCPCS and CPT CodeBook (Current or applilcable year) ICD-10-CM CodeBook (Current or applicable year) CMS 1995 and 1997 EM Guidelines CMS Claims Processing Manual 100-04 Medicare Claims Processing (PUB 100-04) CMS - National Coverage Determinations (NCDs) National Correct Coding Policy Manual Applicable Physician Version
Executive Summary Report
The executive summary provides readers with a short complete document highlighting import information included in the detailed report Executive summaries are created for the senior management readers that donrsquot have time to read the full report and need to walk away with an understanding of the issues and corrective actions
Some would say the executive summary could be written before the detailed report however it is difficult to make sure the most important elements are included until you have spent time reviewing the detail If you want to make sure the most important messages are in the executive
summary this step should be completed after the detail is written As auditors become more seasoned this step could move to the front of the process
Executive Summary Report Structure of the ES Report
o Backgroundndash Specialtyndash Providersndash Sample Selection sizendash Date range of audit
o Audit Scopeo Regulatory Resourceso Type of Medical records reviewedo Overall Accuracy (all providers)o Detailed Audit Findings
ndash Business Impactndash Summary of Findings
o Department Findingso Summary
o ReportsStandard Executive Summary Professional Servicespdf
Department Findings Top Issues
Date ofServiceErrors
MissingDocuments
Missing orInvalid
Signature
TeachingPhysician
Errors
InsufficientConsultation
Documents
OverCoding
EMBundled
IntoGlobal
SurgicalPackage
SplitSharedServiceError
Incorrector
MissingPricing
Modifier
ICD-10Errors
Family Practice
CardiologyInternal Medicine
TOTALS
Top Findings by Provider
E amp M Accuracy Rates
ICD-10-CM Accuracy Rates
Procedure Accuracy Rates
Inpatient DRG Audit Report
TABLE OF CONTENTS
Executive Summaryo Scope of Work
Reimbursement Changes Department Results
o InpatientGeneral Recommendations and Comments
o Secondary DiagnosesoProcedure CodingoPresent on AdmissionoQueries
Scope of WorkCodingAID performed coding audit review of 175 inpatient records The review completed was a random sample that included cases coded by twenty coders for dates of service from May 2016 ndash July 2016
The objective was to determine if the medical record documentation supported the following coding and documentation requirements and any other regulatory requirement for that code set Criteria reviewed
1 ICD-10-CM Official Coding Guidelines for accurate diagnosis code reporting 2 ICD-10-PCS Official Coding Guidelines for accurate procedure code reporting 3 Documentation of procedure compared to the CPT code assigned 4 Identify opportunities for education and training 5 Financial impact of current coding practices
The regulatory agencies and reference materials relied upon include the following in addition to Medicare and Medicaid regulations Additional resources are located in the sub sections below
bull ICD-10-CM and ICD-10-PCS for Hospitals current volume bull Centers for Medicare and Medicaid Services CMS NCCI Edits-Centers for Medicaid and
Medicare Services CMS website wwwcmsgov bull AHA Coding Clinic
The following electronic medical record documents were reviewed and relied upon to compare to the actual codes submitted to the third party payer
bull Discharge summaries HampPs Progress Notes and other provider notes located in the EMR Records
bull Patient History Forms Ancillary Staff Notes bull Procedure Notes bull Orders bull Diagnostic Report
Reimbursement Changes
Coder Acct
Billed Audited
Reimbursement ChangesMS DRG SOI ROM Weight Expected
Payment MS DRG SOI ROM Weight Expected Payment
Coder 1 001 790 52300 $2615000 792 21552 $1077600 -$1537400
Coder 2002
749 26452 $1322600 758 10090 $504500 -$818100
Coder 3 003 669 13111 $655550 694 07294 $364700 -$290850
Coder 4 004 389 08707 $435350 394 09502 $475100 $39750
Coder 5 005 312 07630 $381500 812 08572 $428600 $47100
Coder 6 006 384 08481 $424050 378 09949 $497450 $73400
Coder 7 007 206 08164 $408200 794 12987 $649350 $241150
Coder 8008
344 31029 $1551450 853 51334 $2566700 $1015250
TOTAL $7793700 $6564000 -$1229700
General Recommendations and CommentsFinding Pertinent secondary diagnoses are not coded and diagnoses are code which are not supported in provider documentation Code only those diagnoses which are documented by the provider on the current chart Not all codes are coded to the highest degree of specificity and combination codes were sometimes missed
Recommendation It is important to assign codes for all conditions which meet the definition of a reportable diagnosis Documentation from all providers should be used including but not limited to radiologists pathologists anesthesiologists CRNAs and FNPs
Reference Coding Clinic Official Coding Guidelines
bull Report all secondary diagnoses which meet the definition of a secondary diagnosis which is defined as all conditions that coexist at the time of admission that develop subsequently or that affect the treatment received andor the length of stay Codes which enhance the overall picture of the patientrsquos visit should be added
o Add T45515A to report adverse effect of Coumadin which caused the GI bleed
o Add I2690 for septic pulmonary emboli (MCCSOI4ROM4)
o Add N179 for acute kidney failure (S3M2CC) per the nephrology consult and the 628 progress note
o Add code I429 cardiomyopathy per HampP
o Add B964 to report proteus in a UTI per the 620 hospitalist progress note
o Code for D649 anemia and I701 stenosis of renal artery should be added as secondary diagnoses per the HampP
bull Only report diagnoses which are substantiated by provider documentation in the current chart notes If a suspected condition is not verified at discharge on an inpatient account it cannot be coded
o Remove G4734 (idiopathic sleep related non-obstructive alveolar hypoventilation) as patient was noted to have the sleep study and the hypoventilation was shown to be a possibility but not noted as such on discharge
o Remove G629 (S21) the neuropathy is documented as due to diabetes
o Remove K529 colitis noted on HP as possible but not further noted or confirmed at discharge
Procedure CodingFinding Procedures were sometimes coded incorrectly
Recommendation The entire medical record should be reviewed and all procedures coded as documented Coding procedures incorrectly or assigning incorrect CPT codes may result in lost revenue
bull Incorrect root operation
o Revise principal procedure to 0DQ68ZZ for clipping of the ulcer per OP report clipping is root operation repair
bull Biopsy versus Excision
o Procedure 0DBA0ZX (biopsy of jejunum) should change to 0DBA0ZZ (excision of jejunum) per op note this was not a biopsy procedure
bull Coding Guideline error
o Remove 0RG10K0 for allograft due to being inclusive in principal procedure
o Remove codes for adhesiolysis 0DN80ZZ 0UN10ZZ and 0UN90ZZ due to no significance noted per OP report
bull Incorrect approach
o Revise 0TF63ZZ (fragmentation percutaneous approach) to 0TF68ZZ (fragmentation endoscopic) for procedure performed via scope per the operative report
bull Procedure coded without provider documentation
o Remove secondary procedure of excisional debridement (0JB90ZZ) due to lack of documentation of excisional debridement per operative report The header in the operative report documents IampD and debridement but the body of the operative report only documents an IampD
bull Incorrect CPT code assignment
o Post-op note supports the nerve block injections of four nerves therefore code 64421 (multiple nerve block) should replace 64420 (injection of one intercostal nerve)
Queries Finding Conflicting incomplete and vague documentation is found within provider chart notes
Recommendation Prior to code assignment if the coder finds ambiguous or conflicting documentation the provider should be queried
Reference AHA Coding Clinic 2002 2nd Quarter pages 17-18
bull Query for acute blood loss anemia since hgb has dropped and patient is being transfused PRBC
bull Recommend query to clarify if cardiorenal syndrome is current as it is documented per 627 nephrology consult but unclear if current
bull Documentation does not support SIRS noninfectious without organ failure It is conflicting since patient has respiratory failure Query should be initiated for clarification with or without organ failure or infectious or non-infectious Patient has pneumonia per query as well as last progress note therefore if SIRS is not further specified per query PNA should be sequenced as principal diagnosis and SIRS should be removed
bull Recommend provider query necrotizing lung consolidation noted on DS as principal diagnosis-unclear does the patient have lobar pneumonia Secondary dx states necrotic pneumonia which is coded as principal diagnosis-this diagnosis is clear but consolidation portion is unclear
bull Recommend query for preterm labor delivery at 301 weeks
bull RECOMMEND QUERY no chest pain on admit per ER and HP cardiology provider states no CP with ER stating chest pressure the day prior to admit Appears patient was admitted due to elevated troponins which cardiology says are likely due to hypotension and AKI DS states chest pain but also says bradycardia and hypotension were the reason for admit
bull RECOMMEND QUERY no chest pain on admit per ER and HP cardiology provider states no CP with ER stating chest pressure the day prior to admit Appears patient was admitted due to elevated troponins which cardiology says are likely due to hypotension and AKI DS states chest pain but also says bradycardia and hypotension were the reason for admit
bull Query the provider regarding pathology report notation of endometriosis andor possible re-sequence of stenosis as principal diagnosis as it also meets principal diagnosis guidelines This would result in an MS-DRG change to 742 and APR-DRG change to 513
bull QUERY secondary diagnosis MCC and ROM 4 code T3166 (60 TBSA of which 60 are third degree burns) Chart notes do not specify how much of TBSA was actually third degree If after query TBSA is found to be less than 50 (T3164) then ROM will change from 4 to 3 but no change to overall APR-DRG or weight
Auditor Quality amp Productivity
Audit Productivity Standards
It takes twice as long to audit a chart as it does to code it a statistic that takes into account the time to document an explanation of any coding decision the auditor is not in agreement with o For example in an emergency department audit with a productivity of 12
charts per hour for a coder our auditors would probably be able to review six per hour
o If there are multiple services to audit on each encounter the productivity may only be 4 per hour
o The amount of detail you put into your audit report will also be a factorndash Are you using an automated audit softwarendash Are you using a spreadsheet to auditndash How many Systems are needed to complete the audit
Coder Quality Audits
Quality Audits (QA) should be done on your coders and auditors regularly Frequent reviews with smaller sample size will allow more consistent
review and feedbacko Example 10 charts per month per coder if the coder passes 2-3 months
consecutively with 95 or better score move them to quarterly reviewso Some QA programs review a percentage of the coders work This
methodology requires more time and resources
Auditor QA should also score and comment on the accuracy of the audit comments and recommendations
Presenting the Audit Results
Presenting the Audit Results
Communicating the Audit FindingsoWho requested the AuditoWho are you reporting the finding to
ndash CEOndash CFOndash Physicianndash Revenue Cycle Managerndash HIM Directorndash Billing Managerndash Coding Manager
ReportsAudit Resultspptx
Post Audit Education
Provider Education
Provider Education is best received when it is specific to the provider(s) 11 sessions going over the audit result Look at their notes with them
oHighlight areas for documentation improvementoReinforce Coding Guidelines that are specific to themoAsk them to share how they establish their LOS for E amp M serviceso Integrate their EMR system into the training
Provider Education
Group Training SessionsoUse the audit results to identify common issues within a specialty group
ndash Refer to the Executive Summary reportoVery effective for identifying system issues
ndash Teaching Attestationsndash Templatesndash Copy and Pastendash Cloned notes
o Everyone hears the same messagesoAn Issue may not appear on the individual audit but is still a concern for the
group
Education Delivery
In person or remote sessionso Factors to consider
ndash Providers scheduleavailabilityndash Location(s)ndash Personality of the providerndash Budget
Coder Education
Coders do well in group training so they can learn from each other 11 training allows the coder to get feedback on their coding
Handling Audit Disputes
Handling Audit Disputes
Be open to all points of viewo Let the documentation tell the story
Refer to the guidelines Ask
oCan we defend the reported service with the current documentation
Self Disclosures Refunds and Corrected Billing
Overpayment
In general If a person has received an overpayment the person shallo report and return the overpayment to the Secretary the State an
intermediary a carrier or a contractor as appropriate at the correct address and ndash notify the Secretary State intermediary carrier or contractor to whom the overpayment was returned in writing of the reason for the overpayment
What is an ldquoOverpaymentrdquo ndash The term ldquooverpaymentrdquo means any funds that a person receives or retains under subchapter XVIII or XIX of this chapter to which the person after applicable reconciliation is not entitled under such subchapter
Self Disclosure
The Office of Inspector General (OIG) has several self-disclosure processes that can be used to report potential fraud in Department of Health and Human Services (HHS) programs Choose the one that applies to you from the following descriptions to learn moreo Health Care Provider Self-Disclosures
ndash Health care providers suppliers or other individuals or entities subject to Civil Monetary Penalties can use the Provider Self-Disclosure Protocol which was created in 1998 to voluntarily disclose self-discovered evidence of potential fraud Self-disclosure gives providers the opportunity to avoid the costs and disruptions associated with a Government-directed investigation and civil or administrative litigation Visit the Provider Self-Disclosure Protocol webpage for more information
o HHS Contractor Self-Disclosuresndash Contractors are individuals businesses or other legal entities that are awarded Government contracts or
subcontracts to provide services to the Department of Health and Human Services (HHS) OIGs contractor self-disclosure program enables contractors to self-disclose potential violations of the False Claims Act and various Federal criminal laws involving fraud conflict of interest bribery or gratuity This self-disclosure process is available for those entities with a Federal Acquisition Regulation-based contract Visit the Contractor Self-Disclosure webpage for more information
o HHS Grantee Self-Disclosuresndash HHS grantees or subrecipients may voluntarily disclose evidence of potential violations of Federal criminal law
involving fraud bribery or gratuity violations potentially affecting the Federal award 45 CFR 75113 notes mandatory disclosures of criminal offenses that non-Federal entities must make with respect to HHS grants Recipients submitting disclosures in connection with this requirement should include the subject reference line Mandatory Grant Disclosure Recipients choosing to disclose conduct that may not fit squarely within the scope of offenses described in 45 CFR 75113 should include the following subject reference line in the submission Voluntary Grant Disclosure
Medicare 60 day rule
The 60 Day Rule (Medicare Parts A amp B) o The 60 day time period for reportingreturning begins when either
ndash The reasonable diligence is completed orndash On the day the provider received credible information of a potential overpayment (if the
provider fails to conduct reasonable diligence) o For an investigation to be conducted in a ldquotimelyrdquo manner providers typically
must complete the investigation within 6 months from receipt of credible information indicating there may be an overpayment
ndash ndash 6-month timeframe may potentially be extended under ldquoextraordinary circumstancesrdquo ndash 8 months generally the maximum total time to return overpayments The government recommends that providers maintain records documenting ldquoreasonable diligencerdquo
Medicare 60 Day Rule
Six-year lookback period ndash Sometimes possible to use a shorter period depending on the facts at issue Amount to be repaid ndash May vary depending on the method used to
reportreturn eg Medicare administrative contractor (ldquoMACrdquo) v self-disclosure Overpayment notification ndash After receiving an overpayment
notification from the government you should investigate for related overpayments eg other time periods
Medicare 60 Day Rule
Self-disclosure protocols ndashoA submission to the OIG or CMS protocols suspends the 60 day requirement
for returning overpayments until a settlement agreement is executed ndash ndash OIGrsquos Self-Disclosure Protocol (SDP) ndash ndash CMS Voluntary Self-Referral Disclosure Protocol (SRDP) ndash
o Self-disclosures to other agencies do not suspend the repayment deadlinendash ndash Eg Department of Justice local US Attorneyrsquos Office Medicaid Fraud Control Unit
Medicare 60 Day Rule
Facilitating Compliance With the 60 Day Rule Compliance programs should include o ndash Appropriate policies and procedures o ndash Periodic billing and coding audits to proactively identify overpaymentso ndash Focus on high-risk areas o ndash Utilization of publicly available government resources to guide audit efforts o ndash Investigating any suspected incidents of non-compliance with federal health
care program requirements
Self Disclosure
Choice of AgencyoOIG ndash Self-Disclosure Protocol
ndash ndash Conduct involving false billingndash ndash Conduct involving excluded personsndash ndash Conduct involving the Anti-Kickback Statute (including conduct thatndash violates both the AKS and Stark Law)
oCMS ndash Self-Referral Disclosure Protocolndash ndash Conduct involving only violations of the Stark Law
oDOJndash ndash May be appropriate when provider believes a FCA release is necessary
Summary
The Cost of a Well-Executed Coding Audit ProcessThe costs associated with an auditing program are worth it in the long run Ideally your organization is performing audits on a regular basis across all service types locations and payers Weve all seen claims that have been denied resulting in additional work that may be preventable with a proper audit program The goal is to use the audit feedback to improve coding quality and lower potential risk and cost to the organization Organizations should be investing in an effective coding audit program to make your coders and providers better and enhance documentation improvement from the providers
Questions
Thank you for your attentionLynn Handy
Vice President of Coding amp Audit ServicesLynnhandymanagedresourcesinccom

Who will be reading the Audit Report
What is the technical knowledge of the readeroCodersHIM ProfessionalsoProvidersoClinical StaffoHIM DirectorsoBillingCoding DirectorsManagersoCEOCFO (Executive Team)
Audit Report Format Tips
Provide perspective for the readero Positive and Negative findings
Be precise avoid redundant phrasing inexact terminology Avoid long sentences when a shorter one will work Avoid stating your opinion State the findings and facts Use bullet points this helps to break up difficult information and makes it
clearer for the reader Use gender neutral terms Avoid audit ldquobuzzwordsrdquo such as ldquogenerally improvedrdquo or ldquosignificant riskrdquo Avoid abbreviations unless they are clearly defined
Benefits of Automating your Audit Reports Results
o Consistent Resultso Better Datao Increases Efficiency
Trackingo Allows audit results to be tracked by provider and by specialty
QAo Allows for an automated approach to your internal quality reviews
Trendingo Allows for data analysis at a detailed level that can be tracked
Productivityo Increases auditor productivityo Decreases re-work
ProviderCoder Audit Reports
Detailed Audit reports should have the ability to be sorted byoProvideroCodero Specialty or GroupoAudit Date
Detailed results for each encounteroMeaningful comments
Key Findingso From all encounters
Recommendations and Resources
Detailed Findings Patient ID Patient Name DOS Payer CPT Reported CPT Audited EM Level Key Component ICD Reported ICD Reported Description ICD Audited ICD Reported Description
1 001 Patient A 02-19-16 Blue Cross
99203 25 1 99202 1 +1 D E L 1 S92302A2 Not Reported
1 Fracture of unspecified metatarsal bone(s) left foot initial encounter for closed fracture
1 S92355D2 W109XXD
1 Nondisplaced fracture of fifth metatarsal bone left foot subsequent encounter for fracture with routine healing2 Fall (on) (from) unspecified stairs and steps subsequent encounter
1 The documentation supports coding for an EM service that is one level below the billed code2 Lacking Exam documentation to support the EM level selected3 1997 MSK exam supports an Expanded Problem Focused exam (99202) 1995 exam supports a Detailed exam (99203)4 1997 Exam template suggestions Neurologic Exam-suggest adding the body part examined (upper extremitylow extremity) Dermatologic Exam-unable to determine if this was performed This should be deleted from the final note if
not examined5 EM time statement is insufficient documentation is lacking a required element total time of visit and counseling time greater than 506 CPT disallowed documentation is not present within the medical record to support the CPT code billed (28485-open treatment of metatarsal fracture includes internal fixation when performed) Fracture care is not supported patient
was seen in the ER 6 weeksrsquo prior ER doctor initiated treatment7 The incorrect pricing modifier was billed Removed modifier 25 (separate and significant EM on the same day as a minor procedure) Fracture care is not billable no modifier needed on EM service8 Diagnosis billed is not the most specific available according to the medical record documentation9 Documentation supports an additional diagnosis code not billed
2 002 Patient B 02-05-16 Blue Cross
99203 25 1 99202 25 1 +1 D E L 1 L03032 1 Cellulitis of left toe 1 L03032 1 Cellulitis of left toe
1 The documentation supports coding for an EM service that is one level below the billed code2 Lacking Exam documentation to support the EM level selected3 1997 MSK exam supports an Expanded Problem Focused exam (99202) 1995 exam supports a Detailed exam (99203)4 EM time statement is insufficient documentation is lacking one or more required elements (total time counseling time greater than 50) If a procedure is performed during a visit the time spent performing the procedure needs to be
carved out of the total visit time5 Allowed modifier 25 due to commercial payer Medicare and NCCI do not require modifier 25 on a new patient EM when a minor procedure is performed the same day 6 Diagnosis supported
Detailed Findings
135 822012 New Consultations - Office
Consultations Detailed Detailed (95) Moderate 99244 99243 1 $3500 N
Provider Code 99244 Reviewer Code 99243 Provider Diagnosis 1 3005 NEURASTHENIA Reviewer Diagnosis 1 3005 NEURASTHENIA Provider Diagnosis 2 7282 MUSC DISUSE ATROPHY NEC Reviewer Diagnosis 2 7282 MUSC DISUSE ATROPHY NEC
bull Assessment (I) The assessment is not clearly stated for this encounter Documentation Guidelines states The documentation for each patient encounter should include assessment clinical impression or diagnosis bull Assessment (R) The assessment should be clearly documented for each encounter Since each note must stand alone it is imperative to accurately document the most specific diagnosis in the assessment impression section of the note
bull Documented Lower Level (I) The documentation substantiates a lower level of service than charged
Chart Level Comments
Group your comments in categoriesoDocumentationo E amp MoProceduresoModifierso ICD-10-CM
oReportsAudit Manager Macros 061218 (version 1)xlsx
Recommendations and ReferencesCategory Short Description Long Description
EM AdmissionDischarge Same Day Review the CMS AdmissionDischarge same day coding guidelines httpswwwcmsgovRegulations-and-GuidanceGuidanceManualsDownloadsclm104c12pdf
EM ConsultationReview the consultation guidelines located in the CPT book
EM Consultation not billable to Medicare CMS no longer recognizes the consultation codeshttpswwwcmsgovOutreach-and-EducationMedicare-Learning-Network-MLNMLNMattersArticlesdownloadsmm6740pdf
EM Critical CareReview the CMS Critical Care guidelines httpswwwcmsgovOutreach-and-EducationMedicare-Learning-Network-MLNMLNMattersArticlesdownloadsmm5993pdf
EM Discharge ServicesReview the CMS Hospital Discharge Services guidelineshttpswwwcmsgovOutreach-and-EducationMedicare-Learning-Network-MLNMLNMattersArticlesdownloadsmm5794pdf
EMEM and Preventive Visit Review AAPC guidance for documenting and billing an EM and Preventive visit same day httpswwwaapccomblog22580-successfully-bill-a-
preventive-service-with-a-sick-visit
EM EM documentation guidelines Review the CMS 1995 amp 1997 EM documentation guidelineshttpswwwcmsgovOutreach-and-EducationMedicare-Learning-Network-MLNMLNEdWebGuideEMDOChtml
EM EM Inpatient vs Outpatient Review the patientrsquos status on the hospital admission order to determine the appropriate EM category to bill (inpatient vs observation)
EM EM New vs EstablishedReview the CMS New vs Established patient guidelines httpswwwcmsgovOutreach-and-EducationMedicare-Learning-Network-MLNMLNProductsDownloadseval-mgmt-serv-guide-ICN006764pdf
EMEM Time billing suggestion
Recommend a time statement is added to the EM medical record when a majority of the visit is spent counseling andor coordination of care Review the CMS 1995 amp 1997 EM documentation guidelines for EM time documentationhttpswwwcmsgovOutreach-and-EducationMedicare-Learning-Network-MLNMLNEdWebGuideEMDOChtml
EM Inpatient hospital servicesReview the CMS Hospital Services (Initial and Subsequent) guidelines httpswwwcmsgovRegulations-and-GuidanceGuidanceManualsDownloadsclm104c12pdf
EM Nursing Facility Services Review the Nursing Facility Services guidelines provided by CMS The guidelines can be downloaded at this linkhttpswwwcmsgovRegulations-and-GuidanceGuidanceManualsDownloadsclm104c12pdf
EM Observation Services Review the CMS Observation Services (Initial and Subsequent) guidelines httpswwwcmsgovRegulations-and-GuidanceGuidanceManualsDownloadsclm104c12pdf
EM Prolonged Services Review the CMS Prolonged Services guidelines httpswwwcmsgovOutreach-and-EducationMedicare-Learning-Network-MLNMLNMattersArticlesdownloadsmm5972pdf
EMReview of Systems Review the CMS 1995 amp 1997 EM documentation guidelines for Review of Systems requirements
httpswwwcmsgovOutreach-and-EducationMedicare-Learning-Network-MLNMLNEdWebGuideEMDOChtml
EMConsultation Documentation Suggestion
Recommend adding verbiage to consultation documentation that indicates the name of the referring provider and the reason for the consultation
Audit Report Examples Automated Solution
Letrsquos look at some report Examples
ReportsStandard Provider Audit SummarypdfReportsProvider Detailed Sample Reportdocx
ReportsProvider Audit Worksheets - Optionalpdf
Audit Report Examples Non Automated Solution
Error Findings by Volume Percentage
CPT Coded Accurately
8 8 Overcoded
8 8 Undercoded
Missed CPTHCPCS Code
Missed or Wrong Modifier
8 8 Incorrect CPT (or Category) Used
Incorrect ICD-9 Codes
8 8 Incorrect Quantity
Inadequate Documentation
Missing Documentation 8 8
Signature Illegible (No Log)
8 8
CLIENT NAME PROJECT TITLE
Review Line Item Detail Prepared Month Year
DRAFT
Client Claim Demographics Client Charge Data Review Result EampM ONLY Findings C C C C C C O OC O O O
Char
t Num
ber
Au
dit D
ate
Audi
tor (
initi
als)
QA
Initi
als
Fa
cilit
y Lo
catio
n Re
porte
d
Pr
ovid
er N
ame
Pa
tient
Nam
e
M
edic
al R
ecor
d Nu
mbe
r
Prim
ary
Carr
ier M
edica
re=
A M
edica
id =
B O
ther
=O
Da
te o
f Ser
vice
CP
T Co
de
Mod
ifier
(s) i
n or
der
Qua
ntity
Diag
nosi
s Co
de(s
) 1
thro
ugh
4
Fe
e ch
arge
d
Pr
imar
y Pa
ymen
t Am
ount
CPT
Code
Mod
ifier
(s) i
n or
der
Qua
ntity
Diag
nosi
s Co
de(s
) 1
thro
ugh
4
CO
RREC
T AL
LOW
ABLE
Prim
ary
PAYM
ENT
Va
rianc
e
Chie
f Com
plai
nt
Hist
ory
Leve
l Sup
port
ed
Exam
Lev
el S
uppo
rted
Med
ical
Dec
Mak
ing
Supp
orte
d (o
r TIM
E)
CPT
Cod
ed A
ccur
atel
y
Ove
rcod
ed
Und
erco
ded
Mis
sed
CPT
HC
PCS
Cod
e
Mis
sed
or W
rong
Mod
ifier
Inco
rrec
t CPT
(or C
ateg
ory)
Use
d
Inco
rrec
t IC
D-9
Cod
es
Inco
rrec
t Qua
ntity
Inad
equa
te D
ocum
enta
tion
Mis
sing
Doc
umen
tatio
n
Sign
atur
e Ill
egib
le (N
o Lo
g)
No
Sign
atur
e by
Pro
vide
r of
Ser
vice
COMMENTS (abbreviations used) PF- PROBLEM FOCUSED EPF- EXPANDED PF DET- DETAILED COMP- COMPREHENSIVE SFWD- STRAIGHT FORWARD MOD- MODERATE MDM- MEDICAL DECISION MAKING
Char
t Num
ber
SAMPLE SAMPLE S MD SAMPLE SAMPLE XXXXX XXX 112001 99212 25 1 1 1234 2 5678 3 4
$30000 $2200 99212 25 1 1 1234 2 5678 3 4
$56400 $54200 YES
DET
CO
MP
MO
D
COMMENTS COMMENTS COMMENTS
0
1 2 3 4
1 2 3 4
$000 0
$30000 $2200 $56400 $54200 10 10 10 10 10 10 10 10 10 10 10 10 TOTALS 917 Error Rate by Volume
Error Findings by Volume 8 CPT Coded Accurately 8 Overcoded 8 Undercoded 8 Missed CPTHCPCS Code 8 Missed or Wrong Modifier 8 Incorrect CPT (or Category) Used 8 Incorrect ICD-9 Codes 8 Incorrect Quantity
Inadequate Documentation 8 8 Missing Documentation 8 Signature Illegible (No Log) 8 No Signature by Provider of Service
1200 Total
Net Payment Error Rate -24636
Primary Payments Total $ Audited Payment Total $ (Total Under Payments)
Total Over Payments
Net OverUnder Payment $
2200 56400
(54200)
Resources Used HCPCS and CPT CodeBook (Current or applilcable year) ICD-10-CM CodeBook (Current or applicable year) CMS 1995 and 1997 EM Guidelines CMS Claims Processing Manual 100-04 Medicare Claims Processing (PUB 100-04) CMS - National Coverage Determinations (NCDs) National Correct Coding Policy Manual Applicable Physician Version
Executive Summary Report
The executive summary provides readers with a short complete document highlighting import information included in the detailed report Executive summaries are created for the senior management readers that donrsquot have time to read the full report and need to walk away with an understanding of the issues and corrective actions
Some would say the executive summary could be written before the detailed report however it is difficult to make sure the most important elements are included until you have spent time reviewing the detail If you want to make sure the most important messages are in the executive
summary this step should be completed after the detail is written As auditors become more seasoned this step could move to the front of the process
Executive Summary Report Structure of the ES Report
o Backgroundndash Specialtyndash Providersndash Sample Selection sizendash Date range of audit
o Audit Scopeo Regulatory Resourceso Type of Medical records reviewedo Overall Accuracy (all providers)o Detailed Audit Findings
ndash Business Impactndash Summary of Findings
o Department Findingso Summary
o ReportsStandard Executive Summary Professional Servicespdf
Department Findings Top Issues
Date ofServiceErrors
MissingDocuments
Missing orInvalid
Signature
TeachingPhysician
Errors
InsufficientConsultation
Documents
OverCoding
EMBundled
IntoGlobal
SurgicalPackage
SplitSharedServiceError
Incorrector
MissingPricing
Modifier
ICD-10Errors
Family Practice
CardiologyInternal Medicine
TOTALS
Top Findings by Provider
E amp M Accuracy Rates
ICD-10-CM Accuracy Rates
Procedure Accuracy Rates
Inpatient DRG Audit Report
TABLE OF CONTENTS
Executive Summaryo Scope of Work
Reimbursement Changes Department Results
o InpatientGeneral Recommendations and Comments
o Secondary DiagnosesoProcedure CodingoPresent on AdmissionoQueries
Scope of WorkCodingAID performed coding audit review of 175 inpatient records The review completed was a random sample that included cases coded by twenty coders for dates of service from May 2016 ndash July 2016
The objective was to determine if the medical record documentation supported the following coding and documentation requirements and any other regulatory requirement for that code set Criteria reviewed
1 ICD-10-CM Official Coding Guidelines for accurate diagnosis code reporting 2 ICD-10-PCS Official Coding Guidelines for accurate procedure code reporting 3 Documentation of procedure compared to the CPT code assigned 4 Identify opportunities for education and training 5 Financial impact of current coding practices
The regulatory agencies and reference materials relied upon include the following in addition to Medicare and Medicaid regulations Additional resources are located in the sub sections below
bull ICD-10-CM and ICD-10-PCS for Hospitals current volume bull Centers for Medicare and Medicaid Services CMS NCCI Edits-Centers for Medicaid and
Medicare Services CMS website wwwcmsgov bull AHA Coding Clinic
The following electronic medical record documents were reviewed and relied upon to compare to the actual codes submitted to the third party payer
bull Discharge summaries HampPs Progress Notes and other provider notes located in the EMR Records
bull Patient History Forms Ancillary Staff Notes bull Procedure Notes bull Orders bull Diagnostic Report
Reimbursement Changes
Coder Acct
Billed Audited
Reimbursement ChangesMS DRG SOI ROM Weight Expected
Payment MS DRG SOI ROM Weight Expected Payment
Coder 1 001 790 52300 $2615000 792 21552 $1077600 -$1537400
Coder 2002
749 26452 $1322600 758 10090 $504500 -$818100
Coder 3 003 669 13111 $655550 694 07294 $364700 -$290850
Coder 4 004 389 08707 $435350 394 09502 $475100 $39750
Coder 5 005 312 07630 $381500 812 08572 $428600 $47100
Coder 6 006 384 08481 $424050 378 09949 $497450 $73400
Coder 7 007 206 08164 $408200 794 12987 $649350 $241150
Coder 8008
344 31029 $1551450 853 51334 $2566700 $1015250
TOTAL $7793700 $6564000 -$1229700
General Recommendations and CommentsFinding Pertinent secondary diagnoses are not coded and diagnoses are code which are not supported in provider documentation Code only those diagnoses which are documented by the provider on the current chart Not all codes are coded to the highest degree of specificity and combination codes were sometimes missed
Recommendation It is important to assign codes for all conditions which meet the definition of a reportable diagnosis Documentation from all providers should be used including but not limited to radiologists pathologists anesthesiologists CRNAs and FNPs
Reference Coding Clinic Official Coding Guidelines
bull Report all secondary diagnoses which meet the definition of a secondary diagnosis which is defined as all conditions that coexist at the time of admission that develop subsequently or that affect the treatment received andor the length of stay Codes which enhance the overall picture of the patientrsquos visit should be added
o Add T45515A to report adverse effect of Coumadin which caused the GI bleed
o Add I2690 for septic pulmonary emboli (MCCSOI4ROM4)
o Add N179 for acute kidney failure (S3M2CC) per the nephrology consult and the 628 progress note
o Add code I429 cardiomyopathy per HampP
o Add B964 to report proteus in a UTI per the 620 hospitalist progress note
o Code for D649 anemia and I701 stenosis of renal artery should be added as secondary diagnoses per the HampP
bull Only report diagnoses which are substantiated by provider documentation in the current chart notes If a suspected condition is not verified at discharge on an inpatient account it cannot be coded
o Remove G4734 (idiopathic sleep related non-obstructive alveolar hypoventilation) as patient was noted to have the sleep study and the hypoventilation was shown to be a possibility but not noted as such on discharge
o Remove G629 (S21) the neuropathy is documented as due to diabetes
o Remove K529 colitis noted on HP as possible but not further noted or confirmed at discharge
Procedure CodingFinding Procedures were sometimes coded incorrectly
Recommendation The entire medical record should be reviewed and all procedures coded as documented Coding procedures incorrectly or assigning incorrect CPT codes may result in lost revenue
bull Incorrect root operation
o Revise principal procedure to 0DQ68ZZ for clipping of the ulcer per OP report clipping is root operation repair
bull Biopsy versus Excision
o Procedure 0DBA0ZX (biopsy of jejunum) should change to 0DBA0ZZ (excision of jejunum) per op note this was not a biopsy procedure
bull Coding Guideline error
o Remove 0RG10K0 for allograft due to being inclusive in principal procedure
o Remove codes for adhesiolysis 0DN80ZZ 0UN10ZZ and 0UN90ZZ due to no significance noted per OP report
bull Incorrect approach
o Revise 0TF63ZZ (fragmentation percutaneous approach) to 0TF68ZZ (fragmentation endoscopic) for procedure performed via scope per the operative report
bull Procedure coded without provider documentation
o Remove secondary procedure of excisional debridement (0JB90ZZ) due to lack of documentation of excisional debridement per operative report The header in the operative report documents IampD and debridement but the body of the operative report only documents an IampD
bull Incorrect CPT code assignment
o Post-op note supports the nerve block injections of four nerves therefore code 64421 (multiple nerve block) should replace 64420 (injection of one intercostal nerve)
Queries Finding Conflicting incomplete and vague documentation is found within provider chart notes
Recommendation Prior to code assignment if the coder finds ambiguous or conflicting documentation the provider should be queried
Reference AHA Coding Clinic 2002 2nd Quarter pages 17-18
bull Query for acute blood loss anemia since hgb has dropped and patient is being transfused PRBC
bull Recommend query to clarify if cardiorenal syndrome is current as it is documented per 627 nephrology consult but unclear if current
bull Documentation does not support SIRS noninfectious without organ failure It is conflicting since patient has respiratory failure Query should be initiated for clarification with or without organ failure or infectious or non-infectious Patient has pneumonia per query as well as last progress note therefore if SIRS is not further specified per query PNA should be sequenced as principal diagnosis and SIRS should be removed
bull Recommend provider query necrotizing lung consolidation noted on DS as principal diagnosis-unclear does the patient have lobar pneumonia Secondary dx states necrotic pneumonia which is coded as principal diagnosis-this diagnosis is clear but consolidation portion is unclear
bull Recommend query for preterm labor delivery at 301 weeks
bull RECOMMEND QUERY no chest pain on admit per ER and HP cardiology provider states no CP with ER stating chest pressure the day prior to admit Appears patient was admitted due to elevated troponins which cardiology says are likely due to hypotension and AKI DS states chest pain but also says bradycardia and hypotension were the reason for admit
bull RECOMMEND QUERY no chest pain on admit per ER and HP cardiology provider states no CP with ER stating chest pressure the day prior to admit Appears patient was admitted due to elevated troponins which cardiology says are likely due to hypotension and AKI DS states chest pain but also says bradycardia and hypotension were the reason for admit
bull Query the provider regarding pathology report notation of endometriosis andor possible re-sequence of stenosis as principal diagnosis as it also meets principal diagnosis guidelines This would result in an MS-DRG change to 742 and APR-DRG change to 513
bull QUERY secondary diagnosis MCC and ROM 4 code T3166 (60 TBSA of which 60 are third degree burns) Chart notes do not specify how much of TBSA was actually third degree If after query TBSA is found to be less than 50 (T3164) then ROM will change from 4 to 3 but no change to overall APR-DRG or weight
Auditor Quality amp Productivity
Audit Productivity Standards
It takes twice as long to audit a chart as it does to code it a statistic that takes into account the time to document an explanation of any coding decision the auditor is not in agreement with o For example in an emergency department audit with a productivity of 12
charts per hour for a coder our auditors would probably be able to review six per hour
o If there are multiple services to audit on each encounter the productivity may only be 4 per hour
o The amount of detail you put into your audit report will also be a factorndash Are you using an automated audit softwarendash Are you using a spreadsheet to auditndash How many Systems are needed to complete the audit
Coder Quality Audits
Quality Audits (QA) should be done on your coders and auditors regularly Frequent reviews with smaller sample size will allow more consistent
review and feedbacko Example 10 charts per month per coder if the coder passes 2-3 months
consecutively with 95 or better score move them to quarterly reviewso Some QA programs review a percentage of the coders work This
methodology requires more time and resources
Auditor QA should also score and comment on the accuracy of the audit comments and recommendations
Presenting the Audit Results
Presenting the Audit Results
Communicating the Audit FindingsoWho requested the AuditoWho are you reporting the finding to
ndash CEOndash CFOndash Physicianndash Revenue Cycle Managerndash HIM Directorndash Billing Managerndash Coding Manager
ReportsAudit Resultspptx
Post Audit Education
Provider Education
Provider Education is best received when it is specific to the provider(s) 11 sessions going over the audit result Look at their notes with them
oHighlight areas for documentation improvementoReinforce Coding Guidelines that are specific to themoAsk them to share how they establish their LOS for E amp M serviceso Integrate their EMR system into the training
Provider Education
Group Training SessionsoUse the audit results to identify common issues within a specialty group
ndash Refer to the Executive Summary reportoVery effective for identifying system issues
ndash Teaching Attestationsndash Templatesndash Copy and Pastendash Cloned notes
o Everyone hears the same messagesoAn Issue may not appear on the individual audit but is still a concern for the
group
Education Delivery
In person or remote sessionso Factors to consider
ndash Providers scheduleavailabilityndash Location(s)ndash Personality of the providerndash Budget
Coder Education
Coders do well in group training so they can learn from each other 11 training allows the coder to get feedback on their coding
Handling Audit Disputes
Handling Audit Disputes
Be open to all points of viewo Let the documentation tell the story
Refer to the guidelines Ask
oCan we defend the reported service with the current documentation
Self Disclosures Refunds and Corrected Billing
Overpayment
In general If a person has received an overpayment the person shallo report and return the overpayment to the Secretary the State an
intermediary a carrier or a contractor as appropriate at the correct address and ndash notify the Secretary State intermediary carrier or contractor to whom the overpayment was returned in writing of the reason for the overpayment
What is an ldquoOverpaymentrdquo ndash The term ldquooverpaymentrdquo means any funds that a person receives or retains under subchapter XVIII or XIX of this chapter to which the person after applicable reconciliation is not entitled under such subchapter
Self Disclosure
The Office of Inspector General (OIG) has several self-disclosure processes that can be used to report potential fraud in Department of Health and Human Services (HHS) programs Choose the one that applies to you from the following descriptions to learn moreo Health Care Provider Self-Disclosures
ndash Health care providers suppliers or other individuals or entities subject to Civil Monetary Penalties can use the Provider Self-Disclosure Protocol which was created in 1998 to voluntarily disclose self-discovered evidence of potential fraud Self-disclosure gives providers the opportunity to avoid the costs and disruptions associated with a Government-directed investigation and civil or administrative litigation Visit the Provider Self-Disclosure Protocol webpage for more information
o HHS Contractor Self-Disclosuresndash Contractors are individuals businesses or other legal entities that are awarded Government contracts or
subcontracts to provide services to the Department of Health and Human Services (HHS) OIGs contractor self-disclosure program enables contractors to self-disclose potential violations of the False Claims Act and various Federal criminal laws involving fraud conflict of interest bribery or gratuity This self-disclosure process is available for those entities with a Federal Acquisition Regulation-based contract Visit the Contractor Self-Disclosure webpage for more information
o HHS Grantee Self-Disclosuresndash HHS grantees or subrecipients may voluntarily disclose evidence of potential violations of Federal criminal law
involving fraud bribery or gratuity violations potentially affecting the Federal award 45 CFR 75113 notes mandatory disclosures of criminal offenses that non-Federal entities must make with respect to HHS grants Recipients submitting disclosures in connection with this requirement should include the subject reference line Mandatory Grant Disclosure Recipients choosing to disclose conduct that may not fit squarely within the scope of offenses described in 45 CFR 75113 should include the following subject reference line in the submission Voluntary Grant Disclosure
Medicare 60 day rule
The 60 Day Rule (Medicare Parts A amp B) o The 60 day time period for reportingreturning begins when either
ndash The reasonable diligence is completed orndash On the day the provider received credible information of a potential overpayment (if the
provider fails to conduct reasonable diligence) o For an investigation to be conducted in a ldquotimelyrdquo manner providers typically
must complete the investigation within 6 months from receipt of credible information indicating there may be an overpayment
ndash ndash 6-month timeframe may potentially be extended under ldquoextraordinary circumstancesrdquo ndash 8 months generally the maximum total time to return overpayments The government recommends that providers maintain records documenting ldquoreasonable diligencerdquo
Medicare 60 Day Rule
Six-year lookback period ndash Sometimes possible to use a shorter period depending on the facts at issue Amount to be repaid ndash May vary depending on the method used to
reportreturn eg Medicare administrative contractor (ldquoMACrdquo) v self-disclosure Overpayment notification ndash After receiving an overpayment
notification from the government you should investigate for related overpayments eg other time periods
Medicare 60 Day Rule
Self-disclosure protocols ndashoA submission to the OIG or CMS protocols suspends the 60 day requirement
for returning overpayments until a settlement agreement is executed ndash ndash OIGrsquos Self-Disclosure Protocol (SDP) ndash ndash CMS Voluntary Self-Referral Disclosure Protocol (SRDP) ndash
o Self-disclosures to other agencies do not suspend the repayment deadlinendash ndash Eg Department of Justice local US Attorneyrsquos Office Medicaid Fraud Control Unit
Medicare 60 Day Rule
Facilitating Compliance With the 60 Day Rule Compliance programs should include o ndash Appropriate policies and procedures o ndash Periodic billing and coding audits to proactively identify overpaymentso ndash Focus on high-risk areas o ndash Utilization of publicly available government resources to guide audit efforts o ndash Investigating any suspected incidents of non-compliance with federal health
care program requirements
Self Disclosure
Choice of AgencyoOIG ndash Self-Disclosure Protocol
ndash ndash Conduct involving false billingndash ndash Conduct involving excluded personsndash ndash Conduct involving the Anti-Kickback Statute (including conduct thatndash violates both the AKS and Stark Law)
oCMS ndash Self-Referral Disclosure Protocolndash ndash Conduct involving only violations of the Stark Law
oDOJndash ndash May be appropriate when provider believes a FCA release is necessary
Summary
The Cost of a Well-Executed Coding Audit ProcessThe costs associated with an auditing program are worth it in the long run Ideally your organization is performing audits on a regular basis across all service types locations and payers Weve all seen claims that have been denied resulting in additional work that may be preventable with a proper audit program The goal is to use the audit feedback to improve coding quality and lower potential risk and cost to the organization Organizations should be investing in an effective coding audit program to make your coders and providers better and enhance documentation improvement from the providers
Questions
Thank you for your attentionLynn Handy
Vice President of Coding amp Audit ServicesLynnhandymanagedresourcesinccom

Audit Report Format Tips
Provide perspective for the readero Positive and Negative findings
Be precise avoid redundant phrasing inexact terminology Avoid long sentences when a shorter one will work Avoid stating your opinion State the findings and facts Use bullet points this helps to break up difficult information and makes it
clearer for the reader Use gender neutral terms Avoid audit ldquobuzzwordsrdquo such as ldquogenerally improvedrdquo or ldquosignificant riskrdquo Avoid abbreviations unless they are clearly defined
Benefits of Automating your Audit Reports Results
o Consistent Resultso Better Datao Increases Efficiency
Trackingo Allows audit results to be tracked by provider and by specialty
QAo Allows for an automated approach to your internal quality reviews
Trendingo Allows for data analysis at a detailed level that can be tracked
Productivityo Increases auditor productivityo Decreases re-work
ProviderCoder Audit Reports
Detailed Audit reports should have the ability to be sorted byoProvideroCodero Specialty or GroupoAudit Date
Detailed results for each encounteroMeaningful comments
Key Findingso From all encounters
Recommendations and Resources
Detailed Findings Patient ID Patient Name DOS Payer CPT Reported CPT Audited EM Level Key Component ICD Reported ICD Reported Description ICD Audited ICD Reported Description
1 001 Patient A 02-19-16 Blue Cross
99203 25 1 99202 1 +1 D E L 1 S92302A2 Not Reported
1 Fracture of unspecified metatarsal bone(s) left foot initial encounter for closed fracture
1 S92355D2 W109XXD
1 Nondisplaced fracture of fifth metatarsal bone left foot subsequent encounter for fracture with routine healing2 Fall (on) (from) unspecified stairs and steps subsequent encounter
1 The documentation supports coding for an EM service that is one level below the billed code2 Lacking Exam documentation to support the EM level selected3 1997 MSK exam supports an Expanded Problem Focused exam (99202) 1995 exam supports a Detailed exam (99203)4 1997 Exam template suggestions Neurologic Exam-suggest adding the body part examined (upper extremitylow extremity) Dermatologic Exam-unable to determine if this was performed This should be deleted from the final note if
not examined5 EM time statement is insufficient documentation is lacking a required element total time of visit and counseling time greater than 506 CPT disallowed documentation is not present within the medical record to support the CPT code billed (28485-open treatment of metatarsal fracture includes internal fixation when performed) Fracture care is not supported patient
was seen in the ER 6 weeksrsquo prior ER doctor initiated treatment7 The incorrect pricing modifier was billed Removed modifier 25 (separate and significant EM on the same day as a minor procedure) Fracture care is not billable no modifier needed on EM service8 Diagnosis billed is not the most specific available according to the medical record documentation9 Documentation supports an additional diagnosis code not billed
2 002 Patient B 02-05-16 Blue Cross
99203 25 1 99202 25 1 +1 D E L 1 L03032 1 Cellulitis of left toe 1 L03032 1 Cellulitis of left toe
1 The documentation supports coding for an EM service that is one level below the billed code2 Lacking Exam documentation to support the EM level selected3 1997 MSK exam supports an Expanded Problem Focused exam (99202) 1995 exam supports a Detailed exam (99203)4 EM time statement is insufficient documentation is lacking one or more required elements (total time counseling time greater than 50) If a procedure is performed during a visit the time spent performing the procedure needs to be
carved out of the total visit time5 Allowed modifier 25 due to commercial payer Medicare and NCCI do not require modifier 25 on a new patient EM when a minor procedure is performed the same day 6 Diagnosis supported
Detailed Findings
135 822012 New Consultations - Office
Consultations Detailed Detailed (95) Moderate 99244 99243 1 $3500 N
Provider Code 99244 Reviewer Code 99243 Provider Diagnosis 1 3005 NEURASTHENIA Reviewer Diagnosis 1 3005 NEURASTHENIA Provider Diagnosis 2 7282 MUSC DISUSE ATROPHY NEC Reviewer Diagnosis 2 7282 MUSC DISUSE ATROPHY NEC
bull Assessment (I) The assessment is not clearly stated for this encounter Documentation Guidelines states The documentation for each patient encounter should include assessment clinical impression or diagnosis bull Assessment (R) The assessment should be clearly documented for each encounter Since each note must stand alone it is imperative to accurately document the most specific diagnosis in the assessment impression section of the note
bull Documented Lower Level (I) The documentation substantiates a lower level of service than charged
Chart Level Comments
Group your comments in categoriesoDocumentationo E amp MoProceduresoModifierso ICD-10-CM
oReportsAudit Manager Macros 061218 (version 1)xlsx
Recommendations and ReferencesCategory Short Description Long Description
EM AdmissionDischarge Same Day Review the CMS AdmissionDischarge same day coding guidelines httpswwwcmsgovRegulations-and-GuidanceGuidanceManualsDownloadsclm104c12pdf
EM ConsultationReview the consultation guidelines located in the CPT book
EM Consultation not billable to Medicare CMS no longer recognizes the consultation codeshttpswwwcmsgovOutreach-and-EducationMedicare-Learning-Network-MLNMLNMattersArticlesdownloadsmm6740pdf
EM Critical CareReview the CMS Critical Care guidelines httpswwwcmsgovOutreach-and-EducationMedicare-Learning-Network-MLNMLNMattersArticlesdownloadsmm5993pdf
EM Discharge ServicesReview the CMS Hospital Discharge Services guidelineshttpswwwcmsgovOutreach-and-EducationMedicare-Learning-Network-MLNMLNMattersArticlesdownloadsmm5794pdf
EMEM and Preventive Visit Review AAPC guidance for documenting and billing an EM and Preventive visit same day httpswwwaapccomblog22580-successfully-bill-a-
preventive-service-with-a-sick-visit
EM EM documentation guidelines Review the CMS 1995 amp 1997 EM documentation guidelineshttpswwwcmsgovOutreach-and-EducationMedicare-Learning-Network-MLNMLNEdWebGuideEMDOChtml
EM EM Inpatient vs Outpatient Review the patientrsquos status on the hospital admission order to determine the appropriate EM category to bill (inpatient vs observation)
EM EM New vs EstablishedReview the CMS New vs Established patient guidelines httpswwwcmsgovOutreach-and-EducationMedicare-Learning-Network-MLNMLNProductsDownloadseval-mgmt-serv-guide-ICN006764pdf
EMEM Time billing suggestion
Recommend a time statement is added to the EM medical record when a majority of the visit is spent counseling andor coordination of care Review the CMS 1995 amp 1997 EM documentation guidelines for EM time documentationhttpswwwcmsgovOutreach-and-EducationMedicare-Learning-Network-MLNMLNEdWebGuideEMDOChtml
EM Inpatient hospital servicesReview the CMS Hospital Services (Initial and Subsequent) guidelines httpswwwcmsgovRegulations-and-GuidanceGuidanceManualsDownloadsclm104c12pdf
EM Nursing Facility Services Review the Nursing Facility Services guidelines provided by CMS The guidelines can be downloaded at this linkhttpswwwcmsgovRegulations-and-GuidanceGuidanceManualsDownloadsclm104c12pdf
EM Observation Services Review the CMS Observation Services (Initial and Subsequent) guidelines httpswwwcmsgovRegulations-and-GuidanceGuidanceManualsDownloadsclm104c12pdf
EM Prolonged Services Review the CMS Prolonged Services guidelines httpswwwcmsgovOutreach-and-EducationMedicare-Learning-Network-MLNMLNMattersArticlesdownloadsmm5972pdf
EMReview of Systems Review the CMS 1995 amp 1997 EM documentation guidelines for Review of Systems requirements
httpswwwcmsgovOutreach-and-EducationMedicare-Learning-Network-MLNMLNEdWebGuideEMDOChtml
EMConsultation Documentation Suggestion
Recommend adding verbiage to consultation documentation that indicates the name of the referring provider and the reason for the consultation
Audit Report Examples Automated Solution
Letrsquos look at some report Examples
ReportsStandard Provider Audit SummarypdfReportsProvider Detailed Sample Reportdocx
ReportsProvider Audit Worksheets - Optionalpdf
Audit Report Examples Non Automated Solution
Error Findings by Volume Percentage
CPT Coded Accurately
8 8 Overcoded
8 8 Undercoded
Missed CPTHCPCS Code
Missed or Wrong Modifier
8 8 Incorrect CPT (or Category) Used
Incorrect ICD-9 Codes
8 8 Incorrect Quantity
Inadequate Documentation
Missing Documentation 8 8
Signature Illegible (No Log)
8 8
CLIENT NAME PROJECT TITLE
Review Line Item Detail Prepared Month Year
DRAFT
Client Claim Demographics Client Charge Data Review Result EampM ONLY Findings C C C C C C O OC O O O
Char
t Num
ber
Au
dit D
ate
Audi
tor (
initi
als)
QA
Initi
als
Fa
cilit
y Lo
catio
n Re
porte
d
Pr
ovid
er N
ame
Pa
tient
Nam
e
M
edic
al R
ecor
d Nu
mbe
r
Prim
ary
Carr
ier M
edica
re=
A M
edica
id =
B O
ther
=O
Da
te o
f Ser
vice
CP
T Co
de
Mod
ifier
(s) i
n or
der
Qua
ntity
Diag
nosi
s Co
de(s
) 1
thro
ugh
4
Fe
e ch
arge
d
Pr
imar
y Pa
ymen
t Am
ount
CPT
Code
Mod
ifier
(s) i
n or
der
Qua
ntity
Diag
nosi
s Co
de(s
) 1
thro
ugh
4
CO
RREC
T AL
LOW
ABLE
Prim
ary
PAYM
ENT
Va
rianc
e
Chie
f Com
plai
nt
Hist
ory
Leve
l Sup
port
ed
Exam
Lev
el S
uppo
rted
Med
ical
Dec
Mak
ing
Supp
orte
d (o
r TIM
E)
CPT
Cod
ed A
ccur
atel
y
Ove
rcod
ed
Und
erco
ded
Mis
sed
CPT
HC
PCS
Cod
e
Mis
sed
or W
rong
Mod
ifier
Inco
rrec
t CPT
(or C
ateg
ory)
Use
d
Inco
rrec
t IC
D-9
Cod
es
Inco
rrec
t Qua
ntity
Inad
equa
te D
ocum
enta
tion
Mis
sing
Doc
umen
tatio
n
Sign
atur
e Ill
egib
le (N
o Lo
g)
No
Sign
atur
e by
Pro
vide
r of
Ser
vice
COMMENTS (abbreviations used) PF- PROBLEM FOCUSED EPF- EXPANDED PF DET- DETAILED COMP- COMPREHENSIVE SFWD- STRAIGHT FORWARD MOD- MODERATE MDM- MEDICAL DECISION MAKING
Char
t Num
ber
SAMPLE SAMPLE S MD SAMPLE SAMPLE XXXXX XXX 112001 99212 25 1 1 1234 2 5678 3 4
$30000 $2200 99212 25 1 1 1234 2 5678 3 4
$56400 $54200 YES
DET
CO
MP
MO
D
COMMENTS COMMENTS COMMENTS
0
1 2 3 4
1 2 3 4
$000 0
$30000 $2200 $56400 $54200 10 10 10 10 10 10 10 10 10 10 10 10 TOTALS 917 Error Rate by Volume
Error Findings by Volume 8 CPT Coded Accurately 8 Overcoded 8 Undercoded 8 Missed CPTHCPCS Code 8 Missed or Wrong Modifier 8 Incorrect CPT (or Category) Used 8 Incorrect ICD-9 Codes 8 Incorrect Quantity
Inadequate Documentation 8 8 Missing Documentation 8 Signature Illegible (No Log) 8 No Signature by Provider of Service
1200 Total
Net Payment Error Rate -24636
Primary Payments Total $ Audited Payment Total $ (Total Under Payments)
Total Over Payments
Net OverUnder Payment $
2200 56400
(54200)
Resources Used HCPCS and CPT CodeBook (Current or applilcable year) ICD-10-CM CodeBook (Current or applicable year) CMS 1995 and 1997 EM Guidelines CMS Claims Processing Manual 100-04 Medicare Claims Processing (PUB 100-04) CMS - National Coverage Determinations (NCDs) National Correct Coding Policy Manual Applicable Physician Version
Executive Summary Report
The executive summary provides readers with a short complete document highlighting import information included in the detailed report Executive summaries are created for the senior management readers that donrsquot have time to read the full report and need to walk away with an understanding of the issues and corrective actions
Some would say the executive summary could be written before the detailed report however it is difficult to make sure the most important elements are included until you have spent time reviewing the detail If you want to make sure the most important messages are in the executive
summary this step should be completed after the detail is written As auditors become more seasoned this step could move to the front of the process
Executive Summary Report Structure of the ES Report
o Backgroundndash Specialtyndash Providersndash Sample Selection sizendash Date range of audit
o Audit Scopeo Regulatory Resourceso Type of Medical records reviewedo Overall Accuracy (all providers)o Detailed Audit Findings
ndash Business Impactndash Summary of Findings
o Department Findingso Summary
o ReportsStandard Executive Summary Professional Servicespdf
Department Findings Top Issues
Date ofServiceErrors
MissingDocuments
Missing orInvalid
Signature
TeachingPhysician
Errors
InsufficientConsultation
Documents
OverCoding
EMBundled
IntoGlobal
SurgicalPackage
SplitSharedServiceError
Incorrector
MissingPricing
Modifier
ICD-10Errors
Family Practice
CardiologyInternal Medicine
TOTALS
Top Findings by Provider
E amp M Accuracy Rates
ICD-10-CM Accuracy Rates
Procedure Accuracy Rates
Inpatient DRG Audit Report
TABLE OF CONTENTS
Executive Summaryo Scope of Work
Reimbursement Changes Department Results
o InpatientGeneral Recommendations and Comments
o Secondary DiagnosesoProcedure CodingoPresent on AdmissionoQueries
Scope of WorkCodingAID performed coding audit review of 175 inpatient records The review completed was a random sample that included cases coded by twenty coders for dates of service from May 2016 ndash July 2016
The objective was to determine if the medical record documentation supported the following coding and documentation requirements and any other regulatory requirement for that code set Criteria reviewed
1 ICD-10-CM Official Coding Guidelines for accurate diagnosis code reporting 2 ICD-10-PCS Official Coding Guidelines for accurate procedure code reporting 3 Documentation of procedure compared to the CPT code assigned 4 Identify opportunities for education and training 5 Financial impact of current coding practices
The regulatory agencies and reference materials relied upon include the following in addition to Medicare and Medicaid regulations Additional resources are located in the sub sections below
bull ICD-10-CM and ICD-10-PCS for Hospitals current volume bull Centers for Medicare and Medicaid Services CMS NCCI Edits-Centers for Medicaid and
Medicare Services CMS website wwwcmsgov bull AHA Coding Clinic
The following electronic medical record documents were reviewed and relied upon to compare to the actual codes submitted to the third party payer
bull Discharge summaries HampPs Progress Notes and other provider notes located in the EMR Records
bull Patient History Forms Ancillary Staff Notes bull Procedure Notes bull Orders bull Diagnostic Report
Reimbursement Changes
Coder Acct
Billed Audited
Reimbursement ChangesMS DRG SOI ROM Weight Expected
Payment MS DRG SOI ROM Weight Expected Payment
Coder 1 001 790 52300 $2615000 792 21552 $1077600 -$1537400
Coder 2002
749 26452 $1322600 758 10090 $504500 -$818100
Coder 3 003 669 13111 $655550 694 07294 $364700 -$290850
Coder 4 004 389 08707 $435350 394 09502 $475100 $39750
Coder 5 005 312 07630 $381500 812 08572 $428600 $47100
Coder 6 006 384 08481 $424050 378 09949 $497450 $73400
Coder 7 007 206 08164 $408200 794 12987 $649350 $241150
Coder 8008
344 31029 $1551450 853 51334 $2566700 $1015250
TOTAL $7793700 $6564000 -$1229700
General Recommendations and CommentsFinding Pertinent secondary diagnoses are not coded and diagnoses are code which are not supported in provider documentation Code only those diagnoses which are documented by the provider on the current chart Not all codes are coded to the highest degree of specificity and combination codes were sometimes missed
Recommendation It is important to assign codes for all conditions which meet the definition of a reportable diagnosis Documentation from all providers should be used including but not limited to radiologists pathologists anesthesiologists CRNAs and FNPs
Reference Coding Clinic Official Coding Guidelines
bull Report all secondary diagnoses which meet the definition of a secondary diagnosis which is defined as all conditions that coexist at the time of admission that develop subsequently or that affect the treatment received andor the length of stay Codes which enhance the overall picture of the patientrsquos visit should be added
o Add T45515A to report adverse effect of Coumadin which caused the GI bleed
o Add I2690 for septic pulmonary emboli (MCCSOI4ROM4)
o Add N179 for acute kidney failure (S3M2CC) per the nephrology consult and the 628 progress note
o Add code I429 cardiomyopathy per HampP
o Add B964 to report proteus in a UTI per the 620 hospitalist progress note
o Code for D649 anemia and I701 stenosis of renal artery should be added as secondary diagnoses per the HampP
bull Only report diagnoses which are substantiated by provider documentation in the current chart notes If a suspected condition is not verified at discharge on an inpatient account it cannot be coded
o Remove G4734 (idiopathic sleep related non-obstructive alveolar hypoventilation) as patient was noted to have the sleep study and the hypoventilation was shown to be a possibility but not noted as such on discharge
o Remove G629 (S21) the neuropathy is documented as due to diabetes
o Remove K529 colitis noted on HP as possible but not further noted or confirmed at discharge
Procedure CodingFinding Procedures were sometimes coded incorrectly
Recommendation The entire medical record should be reviewed and all procedures coded as documented Coding procedures incorrectly or assigning incorrect CPT codes may result in lost revenue
bull Incorrect root operation
o Revise principal procedure to 0DQ68ZZ for clipping of the ulcer per OP report clipping is root operation repair
bull Biopsy versus Excision
o Procedure 0DBA0ZX (biopsy of jejunum) should change to 0DBA0ZZ (excision of jejunum) per op note this was not a biopsy procedure
bull Coding Guideline error
o Remove 0RG10K0 for allograft due to being inclusive in principal procedure
o Remove codes for adhesiolysis 0DN80ZZ 0UN10ZZ and 0UN90ZZ due to no significance noted per OP report
bull Incorrect approach
o Revise 0TF63ZZ (fragmentation percutaneous approach) to 0TF68ZZ (fragmentation endoscopic) for procedure performed via scope per the operative report
bull Procedure coded without provider documentation
o Remove secondary procedure of excisional debridement (0JB90ZZ) due to lack of documentation of excisional debridement per operative report The header in the operative report documents IampD and debridement but the body of the operative report only documents an IampD
bull Incorrect CPT code assignment
o Post-op note supports the nerve block injections of four nerves therefore code 64421 (multiple nerve block) should replace 64420 (injection of one intercostal nerve)
Queries Finding Conflicting incomplete and vague documentation is found within provider chart notes
Recommendation Prior to code assignment if the coder finds ambiguous or conflicting documentation the provider should be queried
Reference AHA Coding Clinic 2002 2nd Quarter pages 17-18
bull Query for acute blood loss anemia since hgb has dropped and patient is being transfused PRBC
bull Recommend query to clarify if cardiorenal syndrome is current as it is documented per 627 nephrology consult but unclear if current
bull Documentation does not support SIRS noninfectious without organ failure It is conflicting since patient has respiratory failure Query should be initiated for clarification with or without organ failure or infectious or non-infectious Patient has pneumonia per query as well as last progress note therefore if SIRS is not further specified per query PNA should be sequenced as principal diagnosis and SIRS should be removed
bull Recommend provider query necrotizing lung consolidation noted on DS as principal diagnosis-unclear does the patient have lobar pneumonia Secondary dx states necrotic pneumonia which is coded as principal diagnosis-this diagnosis is clear but consolidation portion is unclear
bull Recommend query for preterm labor delivery at 301 weeks
bull RECOMMEND QUERY no chest pain on admit per ER and HP cardiology provider states no CP with ER stating chest pressure the day prior to admit Appears patient was admitted due to elevated troponins which cardiology says are likely due to hypotension and AKI DS states chest pain but also says bradycardia and hypotension were the reason for admit
bull RECOMMEND QUERY no chest pain on admit per ER and HP cardiology provider states no CP with ER stating chest pressure the day prior to admit Appears patient was admitted due to elevated troponins which cardiology says are likely due to hypotension and AKI DS states chest pain but also says bradycardia and hypotension were the reason for admit
bull Query the provider regarding pathology report notation of endometriosis andor possible re-sequence of stenosis as principal diagnosis as it also meets principal diagnosis guidelines This would result in an MS-DRG change to 742 and APR-DRG change to 513
bull QUERY secondary diagnosis MCC and ROM 4 code T3166 (60 TBSA of which 60 are third degree burns) Chart notes do not specify how much of TBSA was actually third degree If after query TBSA is found to be less than 50 (T3164) then ROM will change from 4 to 3 but no change to overall APR-DRG or weight
Auditor Quality amp Productivity
Audit Productivity Standards
It takes twice as long to audit a chart as it does to code it a statistic that takes into account the time to document an explanation of any coding decision the auditor is not in agreement with o For example in an emergency department audit with a productivity of 12
charts per hour for a coder our auditors would probably be able to review six per hour
o If there are multiple services to audit on each encounter the productivity may only be 4 per hour
o The amount of detail you put into your audit report will also be a factorndash Are you using an automated audit softwarendash Are you using a spreadsheet to auditndash How many Systems are needed to complete the audit
Coder Quality Audits
Quality Audits (QA) should be done on your coders and auditors regularly Frequent reviews with smaller sample size will allow more consistent
review and feedbacko Example 10 charts per month per coder if the coder passes 2-3 months
consecutively with 95 or better score move them to quarterly reviewso Some QA programs review a percentage of the coders work This
methodology requires more time and resources
Auditor QA should also score and comment on the accuracy of the audit comments and recommendations
Presenting the Audit Results
Presenting the Audit Results
Communicating the Audit FindingsoWho requested the AuditoWho are you reporting the finding to
ndash CEOndash CFOndash Physicianndash Revenue Cycle Managerndash HIM Directorndash Billing Managerndash Coding Manager
ReportsAudit Resultspptx
Post Audit Education
Provider Education
Provider Education is best received when it is specific to the provider(s) 11 sessions going over the audit result Look at their notes with them
oHighlight areas for documentation improvementoReinforce Coding Guidelines that are specific to themoAsk them to share how they establish their LOS for E amp M serviceso Integrate their EMR system into the training
Provider Education
Group Training SessionsoUse the audit results to identify common issues within a specialty group
ndash Refer to the Executive Summary reportoVery effective for identifying system issues
ndash Teaching Attestationsndash Templatesndash Copy and Pastendash Cloned notes
o Everyone hears the same messagesoAn Issue may not appear on the individual audit but is still a concern for the
group
Education Delivery
In person or remote sessionso Factors to consider
ndash Providers scheduleavailabilityndash Location(s)ndash Personality of the providerndash Budget
Coder Education
Coders do well in group training so they can learn from each other 11 training allows the coder to get feedback on their coding
Handling Audit Disputes
Handling Audit Disputes
Be open to all points of viewo Let the documentation tell the story
Refer to the guidelines Ask
oCan we defend the reported service with the current documentation
Self Disclosures Refunds and Corrected Billing
Overpayment
In general If a person has received an overpayment the person shallo report and return the overpayment to the Secretary the State an
intermediary a carrier or a contractor as appropriate at the correct address and ndash notify the Secretary State intermediary carrier or contractor to whom the overpayment was returned in writing of the reason for the overpayment
What is an ldquoOverpaymentrdquo ndash The term ldquooverpaymentrdquo means any funds that a person receives or retains under subchapter XVIII or XIX of this chapter to which the person after applicable reconciliation is not entitled under such subchapter
Self Disclosure
The Office of Inspector General (OIG) has several self-disclosure processes that can be used to report potential fraud in Department of Health and Human Services (HHS) programs Choose the one that applies to you from the following descriptions to learn moreo Health Care Provider Self-Disclosures
ndash Health care providers suppliers or other individuals or entities subject to Civil Monetary Penalties can use the Provider Self-Disclosure Protocol which was created in 1998 to voluntarily disclose self-discovered evidence of potential fraud Self-disclosure gives providers the opportunity to avoid the costs and disruptions associated with a Government-directed investigation and civil or administrative litigation Visit the Provider Self-Disclosure Protocol webpage for more information
o HHS Contractor Self-Disclosuresndash Contractors are individuals businesses or other legal entities that are awarded Government contracts or
subcontracts to provide services to the Department of Health and Human Services (HHS) OIGs contractor self-disclosure program enables contractors to self-disclose potential violations of the False Claims Act and various Federal criminal laws involving fraud conflict of interest bribery or gratuity This self-disclosure process is available for those entities with a Federal Acquisition Regulation-based contract Visit the Contractor Self-Disclosure webpage for more information
o HHS Grantee Self-Disclosuresndash HHS grantees or subrecipients may voluntarily disclose evidence of potential violations of Federal criminal law
involving fraud bribery or gratuity violations potentially affecting the Federal award 45 CFR 75113 notes mandatory disclosures of criminal offenses that non-Federal entities must make with respect to HHS grants Recipients submitting disclosures in connection with this requirement should include the subject reference line Mandatory Grant Disclosure Recipients choosing to disclose conduct that may not fit squarely within the scope of offenses described in 45 CFR 75113 should include the following subject reference line in the submission Voluntary Grant Disclosure
Medicare 60 day rule
The 60 Day Rule (Medicare Parts A amp B) o The 60 day time period for reportingreturning begins when either
ndash The reasonable diligence is completed orndash On the day the provider received credible information of a potential overpayment (if the
provider fails to conduct reasonable diligence) o For an investigation to be conducted in a ldquotimelyrdquo manner providers typically
must complete the investigation within 6 months from receipt of credible information indicating there may be an overpayment
ndash ndash 6-month timeframe may potentially be extended under ldquoextraordinary circumstancesrdquo ndash 8 months generally the maximum total time to return overpayments The government recommends that providers maintain records documenting ldquoreasonable diligencerdquo
Medicare 60 Day Rule
Six-year lookback period ndash Sometimes possible to use a shorter period depending on the facts at issue Amount to be repaid ndash May vary depending on the method used to
reportreturn eg Medicare administrative contractor (ldquoMACrdquo) v self-disclosure Overpayment notification ndash After receiving an overpayment
notification from the government you should investigate for related overpayments eg other time periods
Medicare 60 Day Rule
Self-disclosure protocols ndashoA submission to the OIG or CMS protocols suspends the 60 day requirement
for returning overpayments until a settlement agreement is executed ndash ndash OIGrsquos Self-Disclosure Protocol (SDP) ndash ndash CMS Voluntary Self-Referral Disclosure Protocol (SRDP) ndash
o Self-disclosures to other agencies do not suspend the repayment deadlinendash ndash Eg Department of Justice local US Attorneyrsquos Office Medicaid Fraud Control Unit
Medicare 60 Day Rule
Facilitating Compliance With the 60 Day Rule Compliance programs should include o ndash Appropriate policies and procedures o ndash Periodic billing and coding audits to proactively identify overpaymentso ndash Focus on high-risk areas o ndash Utilization of publicly available government resources to guide audit efforts o ndash Investigating any suspected incidents of non-compliance with federal health
care program requirements
Self Disclosure
Choice of AgencyoOIG ndash Self-Disclosure Protocol
ndash ndash Conduct involving false billingndash ndash Conduct involving excluded personsndash ndash Conduct involving the Anti-Kickback Statute (including conduct thatndash violates both the AKS and Stark Law)
oCMS ndash Self-Referral Disclosure Protocolndash ndash Conduct involving only violations of the Stark Law
oDOJndash ndash May be appropriate when provider believes a FCA release is necessary
Summary
The Cost of a Well-Executed Coding Audit ProcessThe costs associated with an auditing program are worth it in the long run Ideally your organization is performing audits on a regular basis across all service types locations and payers Weve all seen claims that have been denied resulting in additional work that may be preventable with a proper audit program The goal is to use the audit feedback to improve coding quality and lower potential risk and cost to the organization Organizations should be investing in an effective coding audit program to make your coders and providers better and enhance documentation improvement from the providers
Questions
Thank you for your attentionLynn Handy
Vice President of Coding amp Audit ServicesLynnhandymanagedresourcesinccom

Benefits of Automating your Audit Reports Results
o Consistent Resultso Better Datao Increases Efficiency
Trackingo Allows audit results to be tracked by provider and by specialty
QAo Allows for an automated approach to your internal quality reviews
Trendingo Allows for data analysis at a detailed level that can be tracked
Productivityo Increases auditor productivityo Decreases re-work
ProviderCoder Audit Reports
Detailed Audit reports should have the ability to be sorted byoProvideroCodero Specialty or GroupoAudit Date
Detailed results for each encounteroMeaningful comments
Key Findingso From all encounters
Recommendations and Resources
Detailed Findings Patient ID Patient Name DOS Payer CPT Reported CPT Audited EM Level Key Component ICD Reported ICD Reported Description ICD Audited ICD Reported Description
1 001 Patient A 02-19-16 Blue Cross
99203 25 1 99202 1 +1 D E L 1 S92302A2 Not Reported
1 Fracture of unspecified metatarsal bone(s) left foot initial encounter for closed fracture
1 S92355D2 W109XXD
1 Nondisplaced fracture of fifth metatarsal bone left foot subsequent encounter for fracture with routine healing2 Fall (on) (from) unspecified stairs and steps subsequent encounter
1 The documentation supports coding for an EM service that is one level below the billed code2 Lacking Exam documentation to support the EM level selected3 1997 MSK exam supports an Expanded Problem Focused exam (99202) 1995 exam supports a Detailed exam (99203)4 1997 Exam template suggestions Neurologic Exam-suggest adding the body part examined (upper extremitylow extremity) Dermatologic Exam-unable to determine if this was performed This should be deleted from the final note if
not examined5 EM time statement is insufficient documentation is lacking a required element total time of visit and counseling time greater than 506 CPT disallowed documentation is not present within the medical record to support the CPT code billed (28485-open treatment of metatarsal fracture includes internal fixation when performed) Fracture care is not supported patient
was seen in the ER 6 weeksrsquo prior ER doctor initiated treatment7 The incorrect pricing modifier was billed Removed modifier 25 (separate and significant EM on the same day as a minor procedure) Fracture care is not billable no modifier needed on EM service8 Diagnosis billed is not the most specific available according to the medical record documentation9 Documentation supports an additional diagnosis code not billed
2 002 Patient B 02-05-16 Blue Cross
99203 25 1 99202 25 1 +1 D E L 1 L03032 1 Cellulitis of left toe 1 L03032 1 Cellulitis of left toe
1 The documentation supports coding for an EM service that is one level below the billed code2 Lacking Exam documentation to support the EM level selected3 1997 MSK exam supports an Expanded Problem Focused exam (99202) 1995 exam supports a Detailed exam (99203)4 EM time statement is insufficient documentation is lacking one or more required elements (total time counseling time greater than 50) If a procedure is performed during a visit the time spent performing the procedure needs to be
carved out of the total visit time5 Allowed modifier 25 due to commercial payer Medicare and NCCI do not require modifier 25 on a new patient EM when a minor procedure is performed the same day 6 Diagnosis supported
Detailed Findings
135 822012 New Consultations - Office
Consultations Detailed Detailed (95) Moderate 99244 99243 1 $3500 N
Provider Code 99244 Reviewer Code 99243 Provider Diagnosis 1 3005 NEURASTHENIA Reviewer Diagnosis 1 3005 NEURASTHENIA Provider Diagnosis 2 7282 MUSC DISUSE ATROPHY NEC Reviewer Diagnosis 2 7282 MUSC DISUSE ATROPHY NEC
bull Assessment (I) The assessment is not clearly stated for this encounter Documentation Guidelines states The documentation for each patient encounter should include assessment clinical impression or diagnosis bull Assessment (R) The assessment should be clearly documented for each encounter Since each note must stand alone it is imperative to accurately document the most specific diagnosis in the assessment impression section of the note
bull Documented Lower Level (I) The documentation substantiates a lower level of service than charged
Chart Level Comments
Group your comments in categoriesoDocumentationo E amp MoProceduresoModifierso ICD-10-CM
oReportsAudit Manager Macros 061218 (version 1)xlsx
Recommendations and ReferencesCategory Short Description Long Description
EM AdmissionDischarge Same Day Review the CMS AdmissionDischarge same day coding guidelines httpswwwcmsgovRegulations-and-GuidanceGuidanceManualsDownloadsclm104c12pdf
EM ConsultationReview the consultation guidelines located in the CPT book
EM Consultation not billable to Medicare CMS no longer recognizes the consultation codeshttpswwwcmsgovOutreach-and-EducationMedicare-Learning-Network-MLNMLNMattersArticlesdownloadsmm6740pdf
EM Critical CareReview the CMS Critical Care guidelines httpswwwcmsgovOutreach-and-EducationMedicare-Learning-Network-MLNMLNMattersArticlesdownloadsmm5993pdf
EM Discharge ServicesReview the CMS Hospital Discharge Services guidelineshttpswwwcmsgovOutreach-and-EducationMedicare-Learning-Network-MLNMLNMattersArticlesdownloadsmm5794pdf
EMEM and Preventive Visit Review AAPC guidance for documenting and billing an EM and Preventive visit same day httpswwwaapccomblog22580-successfully-bill-a-
preventive-service-with-a-sick-visit
EM EM documentation guidelines Review the CMS 1995 amp 1997 EM documentation guidelineshttpswwwcmsgovOutreach-and-EducationMedicare-Learning-Network-MLNMLNEdWebGuideEMDOChtml
EM EM Inpatient vs Outpatient Review the patientrsquos status on the hospital admission order to determine the appropriate EM category to bill (inpatient vs observation)
EM EM New vs EstablishedReview the CMS New vs Established patient guidelines httpswwwcmsgovOutreach-and-EducationMedicare-Learning-Network-MLNMLNProductsDownloadseval-mgmt-serv-guide-ICN006764pdf
EMEM Time billing suggestion
Recommend a time statement is added to the EM medical record when a majority of the visit is spent counseling andor coordination of care Review the CMS 1995 amp 1997 EM documentation guidelines for EM time documentationhttpswwwcmsgovOutreach-and-EducationMedicare-Learning-Network-MLNMLNEdWebGuideEMDOChtml
EM Inpatient hospital servicesReview the CMS Hospital Services (Initial and Subsequent) guidelines httpswwwcmsgovRegulations-and-GuidanceGuidanceManualsDownloadsclm104c12pdf
EM Nursing Facility Services Review the Nursing Facility Services guidelines provided by CMS The guidelines can be downloaded at this linkhttpswwwcmsgovRegulations-and-GuidanceGuidanceManualsDownloadsclm104c12pdf
EM Observation Services Review the CMS Observation Services (Initial and Subsequent) guidelines httpswwwcmsgovRegulations-and-GuidanceGuidanceManualsDownloadsclm104c12pdf
EM Prolonged Services Review the CMS Prolonged Services guidelines httpswwwcmsgovOutreach-and-EducationMedicare-Learning-Network-MLNMLNMattersArticlesdownloadsmm5972pdf
EMReview of Systems Review the CMS 1995 amp 1997 EM documentation guidelines for Review of Systems requirements
httpswwwcmsgovOutreach-and-EducationMedicare-Learning-Network-MLNMLNEdWebGuideEMDOChtml
EMConsultation Documentation Suggestion
Recommend adding verbiage to consultation documentation that indicates the name of the referring provider and the reason for the consultation
Audit Report Examples Automated Solution
Letrsquos look at some report Examples
ReportsStandard Provider Audit SummarypdfReportsProvider Detailed Sample Reportdocx
ReportsProvider Audit Worksheets - Optionalpdf
Audit Report Examples Non Automated Solution
Error Findings by Volume Percentage
CPT Coded Accurately
8 8 Overcoded
8 8 Undercoded
Missed CPTHCPCS Code
Missed or Wrong Modifier
8 8 Incorrect CPT (or Category) Used
Incorrect ICD-9 Codes
8 8 Incorrect Quantity
Inadequate Documentation
Missing Documentation 8 8
Signature Illegible (No Log)
8 8
CLIENT NAME PROJECT TITLE
Review Line Item Detail Prepared Month Year
DRAFT
Client Claim Demographics Client Charge Data Review Result EampM ONLY Findings C C C C C C O OC O O O
Char
t Num
ber
Au
dit D
ate
Audi
tor (
initi
als)
QA
Initi
als
Fa
cilit
y Lo
catio
n Re
porte
d
Pr
ovid
er N
ame
Pa
tient
Nam
e
M
edic
al R
ecor
d Nu
mbe
r
Prim
ary
Carr
ier M
edica
re=
A M
edica
id =
B O
ther
=O
Da
te o
f Ser
vice
CP
T Co
de
Mod
ifier
(s) i
n or
der
Qua
ntity
Diag
nosi
s Co
de(s
) 1
thro
ugh
4
Fe
e ch
arge
d
Pr
imar
y Pa
ymen
t Am
ount
CPT
Code
Mod
ifier
(s) i
n or
der
Qua
ntity
Diag
nosi
s Co
de(s
) 1
thro
ugh
4
CO
RREC
T AL
LOW
ABLE
Prim
ary
PAYM
ENT
Va
rianc
e
Chie
f Com
plai
nt
Hist
ory
Leve
l Sup
port
ed
Exam
Lev
el S
uppo
rted
Med
ical
Dec
Mak
ing
Supp
orte
d (o
r TIM
E)
CPT
Cod
ed A
ccur
atel
y
Ove
rcod
ed
Und
erco
ded
Mis
sed
CPT
HC
PCS
Cod
e
Mis
sed
or W
rong
Mod
ifier
Inco
rrec
t CPT
(or C
ateg
ory)
Use
d
Inco
rrec
t IC
D-9
Cod
es
Inco
rrec
t Qua
ntity
Inad
equa
te D
ocum
enta
tion
Mis
sing
Doc
umen
tatio
n
Sign
atur
e Ill
egib
le (N
o Lo
g)
No
Sign
atur
e by
Pro
vide
r of
Ser
vice
COMMENTS (abbreviations used) PF- PROBLEM FOCUSED EPF- EXPANDED PF DET- DETAILED COMP- COMPREHENSIVE SFWD- STRAIGHT FORWARD MOD- MODERATE MDM- MEDICAL DECISION MAKING
Char
t Num
ber
SAMPLE SAMPLE S MD SAMPLE SAMPLE XXXXX XXX 112001 99212 25 1 1 1234 2 5678 3 4
$30000 $2200 99212 25 1 1 1234 2 5678 3 4
$56400 $54200 YES
DET
CO
MP
MO
D
COMMENTS COMMENTS COMMENTS
0
1 2 3 4
1 2 3 4
$000 0
$30000 $2200 $56400 $54200 10 10 10 10 10 10 10 10 10 10 10 10 TOTALS 917 Error Rate by Volume
Error Findings by Volume 8 CPT Coded Accurately 8 Overcoded 8 Undercoded 8 Missed CPTHCPCS Code 8 Missed or Wrong Modifier 8 Incorrect CPT (or Category) Used 8 Incorrect ICD-9 Codes 8 Incorrect Quantity
Inadequate Documentation 8 8 Missing Documentation 8 Signature Illegible (No Log) 8 No Signature by Provider of Service
1200 Total
Net Payment Error Rate -24636
Primary Payments Total $ Audited Payment Total $ (Total Under Payments)
Total Over Payments
Net OverUnder Payment $
2200 56400
(54200)
Resources Used HCPCS and CPT CodeBook (Current or applilcable year) ICD-10-CM CodeBook (Current or applicable year) CMS 1995 and 1997 EM Guidelines CMS Claims Processing Manual 100-04 Medicare Claims Processing (PUB 100-04) CMS - National Coverage Determinations (NCDs) National Correct Coding Policy Manual Applicable Physician Version
Executive Summary Report
The executive summary provides readers with a short complete document highlighting import information included in the detailed report Executive summaries are created for the senior management readers that donrsquot have time to read the full report and need to walk away with an understanding of the issues and corrective actions
Some would say the executive summary could be written before the detailed report however it is difficult to make sure the most important elements are included until you have spent time reviewing the detail If you want to make sure the most important messages are in the executive
summary this step should be completed after the detail is written As auditors become more seasoned this step could move to the front of the process
Executive Summary Report Structure of the ES Report
o Backgroundndash Specialtyndash Providersndash Sample Selection sizendash Date range of audit
o Audit Scopeo Regulatory Resourceso Type of Medical records reviewedo Overall Accuracy (all providers)o Detailed Audit Findings
ndash Business Impactndash Summary of Findings
o Department Findingso Summary
o ReportsStandard Executive Summary Professional Servicespdf
Department Findings Top Issues
Date ofServiceErrors
MissingDocuments
Missing orInvalid
Signature
TeachingPhysician
Errors
InsufficientConsultation
Documents
OverCoding
EMBundled
IntoGlobal
SurgicalPackage
SplitSharedServiceError
Incorrector
MissingPricing
Modifier
ICD-10Errors
Family Practice
CardiologyInternal Medicine
TOTALS
Top Findings by Provider
E amp M Accuracy Rates
ICD-10-CM Accuracy Rates
Procedure Accuracy Rates
Inpatient DRG Audit Report
TABLE OF CONTENTS
Executive Summaryo Scope of Work
Reimbursement Changes Department Results
o InpatientGeneral Recommendations and Comments
o Secondary DiagnosesoProcedure CodingoPresent on AdmissionoQueries
Scope of WorkCodingAID performed coding audit review of 175 inpatient records The review completed was a random sample that included cases coded by twenty coders for dates of service from May 2016 ndash July 2016
The objective was to determine if the medical record documentation supported the following coding and documentation requirements and any other regulatory requirement for that code set Criteria reviewed
1 ICD-10-CM Official Coding Guidelines for accurate diagnosis code reporting 2 ICD-10-PCS Official Coding Guidelines for accurate procedure code reporting 3 Documentation of procedure compared to the CPT code assigned 4 Identify opportunities for education and training 5 Financial impact of current coding practices
The regulatory agencies and reference materials relied upon include the following in addition to Medicare and Medicaid regulations Additional resources are located in the sub sections below
bull ICD-10-CM and ICD-10-PCS for Hospitals current volume bull Centers for Medicare and Medicaid Services CMS NCCI Edits-Centers for Medicaid and
Medicare Services CMS website wwwcmsgov bull AHA Coding Clinic
The following electronic medical record documents were reviewed and relied upon to compare to the actual codes submitted to the third party payer
bull Discharge summaries HampPs Progress Notes and other provider notes located in the EMR Records
bull Patient History Forms Ancillary Staff Notes bull Procedure Notes bull Orders bull Diagnostic Report
Reimbursement Changes
Coder Acct
Billed Audited
Reimbursement ChangesMS DRG SOI ROM Weight Expected
Payment MS DRG SOI ROM Weight Expected Payment
Coder 1 001 790 52300 $2615000 792 21552 $1077600 -$1537400
Coder 2002
749 26452 $1322600 758 10090 $504500 -$818100
Coder 3 003 669 13111 $655550 694 07294 $364700 -$290850
Coder 4 004 389 08707 $435350 394 09502 $475100 $39750
Coder 5 005 312 07630 $381500 812 08572 $428600 $47100
Coder 6 006 384 08481 $424050 378 09949 $497450 $73400
Coder 7 007 206 08164 $408200 794 12987 $649350 $241150
Coder 8008
344 31029 $1551450 853 51334 $2566700 $1015250
TOTAL $7793700 $6564000 -$1229700
General Recommendations and CommentsFinding Pertinent secondary diagnoses are not coded and diagnoses are code which are not supported in provider documentation Code only those diagnoses which are documented by the provider on the current chart Not all codes are coded to the highest degree of specificity and combination codes were sometimes missed
Recommendation It is important to assign codes for all conditions which meet the definition of a reportable diagnosis Documentation from all providers should be used including but not limited to radiologists pathologists anesthesiologists CRNAs and FNPs
Reference Coding Clinic Official Coding Guidelines
bull Report all secondary diagnoses which meet the definition of a secondary diagnosis which is defined as all conditions that coexist at the time of admission that develop subsequently or that affect the treatment received andor the length of stay Codes which enhance the overall picture of the patientrsquos visit should be added
o Add T45515A to report adverse effect of Coumadin which caused the GI bleed
o Add I2690 for septic pulmonary emboli (MCCSOI4ROM4)
o Add N179 for acute kidney failure (S3M2CC) per the nephrology consult and the 628 progress note
o Add code I429 cardiomyopathy per HampP
o Add B964 to report proteus in a UTI per the 620 hospitalist progress note
o Code for D649 anemia and I701 stenosis of renal artery should be added as secondary diagnoses per the HampP
bull Only report diagnoses which are substantiated by provider documentation in the current chart notes If a suspected condition is not verified at discharge on an inpatient account it cannot be coded
o Remove G4734 (idiopathic sleep related non-obstructive alveolar hypoventilation) as patient was noted to have the sleep study and the hypoventilation was shown to be a possibility but not noted as such on discharge
o Remove G629 (S21) the neuropathy is documented as due to diabetes
o Remove K529 colitis noted on HP as possible but not further noted or confirmed at discharge
Procedure CodingFinding Procedures were sometimes coded incorrectly
Recommendation The entire medical record should be reviewed and all procedures coded as documented Coding procedures incorrectly or assigning incorrect CPT codes may result in lost revenue
bull Incorrect root operation
o Revise principal procedure to 0DQ68ZZ for clipping of the ulcer per OP report clipping is root operation repair
bull Biopsy versus Excision
o Procedure 0DBA0ZX (biopsy of jejunum) should change to 0DBA0ZZ (excision of jejunum) per op note this was not a biopsy procedure
bull Coding Guideline error
o Remove 0RG10K0 for allograft due to being inclusive in principal procedure
o Remove codes for adhesiolysis 0DN80ZZ 0UN10ZZ and 0UN90ZZ due to no significance noted per OP report
bull Incorrect approach
o Revise 0TF63ZZ (fragmentation percutaneous approach) to 0TF68ZZ (fragmentation endoscopic) for procedure performed via scope per the operative report
bull Procedure coded without provider documentation
o Remove secondary procedure of excisional debridement (0JB90ZZ) due to lack of documentation of excisional debridement per operative report The header in the operative report documents IampD and debridement but the body of the operative report only documents an IampD
bull Incorrect CPT code assignment
o Post-op note supports the nerve block injections of four nerves therefore code 64421 (multiple nerve block) should replace 64420 (injection of one intercostal nerve)
Queries Finding Conflicting incomplete and vague documentation is found within provider chart notes
Recommendation Prior to code assignment if the coder finds ambiguous or conflicting documentation the provider should be queried
Reference AHA Coding Clinic 2002 2nd Quarter pages 17-18
bull Query for acute blood loss anemia since hgb has dropped and patient is being transfused PRBC
bull Recommend query to clarify if cardiorenal syndrome is current as it is documented per 627 nephrology consult but unclear if current
bull Documentation does not support SIRS noninfectious without organ failure It is conflicting since patient has respiratory failure Query should be initiated for clarification with or without organ failure or infectious or non-infectious Patient has pneumonia per query as well as last progress note therefore if SIRS is not further specified per query PNA should be sequenced as principal diagnosis and SIRS should be removed
bull Recommend provider query necrotizing lung consolidation noted on DS as principal diagnosis-unclear does the patient have lobar pneumonia Secondary dx states necrotic pneumonia which is coded as principal diagnosis-this diagnosis is clear but consolidation portion is unclear
bull Recommend query for preterm labor delivery at 301 weeks
bull RECOMMEND QUERY no chest pain on admit per ER and HP cardiology provider states no CP with ER stating chest pressure the day prior to admit Appears patient was admitted due to elevated troponins which cardiology says are likely due to hypotension and AKI DS states chest pain but also says bradycardia and hypotension were the reason for admit
bull RECOMMEND QUERY no chest pain on admit per ER and HP cardiology provider states no CP with ER stating chest pressure the day prior to admit Appears patient was admitted due to elevated troponins which cardiology says are likely due to hypotension and AKI DS states chest pain but also says bradycardia and hypotension were the reason for admit
bull Query the provider regarding pathology report notation of endometriosis andor possible re-sequence of stenosis as principal diagnosis as it also meets principal diagnosis guidelines This would result in an MS-DRG change to 742 and APR-DRG change to 513
bull QUERY secondary diagnosis MCC and ROM 4 code T3166 (60 TBSA of which 60 are third degree burns) Chart notes do not specify how much of TBSA was actually third degree If after query TBSA is found to be less than 50 (T3164) then ROM will change from 4 to 3 but no change to overall APR-DRG or weight
Auditor Quality amp Productivity
Audit Productivity Standards
It takes twice as long to audit a chart as it does to code it a statistic that takes into account the time to document an explanation of any coding decision the auditor is not in agreement with o For example in an emergency department audit with a productivity of 12
charts per hour for a coder our auditors would probably be able to review six per hour
o If there are multiple services to audit on each encounter the productivity may only be 4 per hour
o The amount of detail you put into your audit report will also be a factorndash Are you using an automated audit softwarendash Are you using a spreadsheet to auditndash How many Systems are needed to complete the audit
Coder Quality Audits
Quality Audits (QA) should be done on your coders and auditors regularly Frequent reviews with smaller sample size will allow more consistent
review and feedbacko Example 10 charts per month per coder if the coder passes 2-3 months
consecutively with 95 or better score move them to quarterly reviewso Some QA programs review a percentage of the coders work This
methodology requires more time and resources
Auditor QA should also score and comment on the accuracy of the audit comments and recommendations
Presenting the Audit Results
Presenting the Audit Results
Communicating the Audit FindingsoWho requested the AuditoWho are you reporting the finding to
ndash CEOndash CFOndash Physicianndash Revenue Cycle Managerndash HIM Directorndash Billing Managerndash Coding Manager
ReportsAudit Resultspptx
Post Audit Education
Provider Education
Provider Education is best received when it is specific to the provider(s) 11 sessions going over the audit result Look at their notes with them
oHighlight areas for documentation improvementoReinforce Coding Guidelines that are specific to themoAsk them to share how they establish their LOS for E amp M serviceso Integrate their EMR system into the training
Provider Education
Group Training SessionsoUse the audit results to identify common issues within a specialty group
ndash Refer to the Executive Summary reportoVery effective for identifying system issues
ndash Teaching Attestationsndash Templatesndash Copy and Pastendash Cloned notes
o Everyone hears the same messagesoAn Issue may not appear on the individual audit but is still a concern for the
group
Education Delivery
In person or remote sessionso Factors to consider
ndash Providers scheduleavailabilityndash Location(s)ndash Personality of the providerndash Budget
Coder Education
Coders do well in group training so they can learn from each other 11 training allows the coder to get feedback on their coding
Handling Audit Disputes
Handling Audit Disputes
Be open to all points of viewo Let the documentation tell the story
Refer to the guidelines Ask
oCan we defend the reported service with the current documentation
Self Disclosures Refunds and Corrected Billing
Overpayment
In general If a person has received an overpayment the person shallo report and return the overpayment to the Secretary the State an
intermediary a carrier or a contractor as appropriate at the correct address and ndash notify the Secretary State intermediary carrier or contractor to whom the overpayment was returned in writing of the reason for the overpayment
What is an ldquoOverpaymentrdquo ndash The term ldquooverpaymentrdquo means any funds that a person receives or retains under subchapter XVIII or XIX of this chapter to which the person after applicable reconciliation is not entitled under such subchapter
Self Disclosure
The Office of Inspector General (OIG) has several self-disclosure processes that can be used to report potential fraud in Department of Health and Human Services (HHS) programs Choose the one that applies to you from the following descriptions to learn moreo Health Care Provider Self-Disclosures
ndash Health care providers suppliers or other individuals or entities subject to Civil Monetary Penalties can use the Provider Self-Disclosure Protocol which was created in 1998 to voluntarily disclose self-discovered evidence of potential fraud Self-disclosure gives providers the opportunity to avoid the costs and disruptions associated with a Government-directed investigation and civil or administrative litigation Visit the Provider Self-Disclosure Protocol webpage for more information
o HHS Contractor Self-Disclosuresndash Contractors are individuals businesses or other legal entities that are awarded Government contracts or
subcontracts to provide services to the Department of Health and Human Services (HHS) OIGs contractor self-disclosure program enables contractors to self-disclose potential violations of the False Claims Act and various Federal criminal laws involving fraud conflict of interest bribery or gratuity This self-disclosure process is available for those entities with a Federal Acquisition Regulation-based contract Visit the Contractor Self-Disclosure webpage for more information
o HHS Grantee Self-Disclosuresndash HHS grantees or subrecipients may voluntarily disclose evidence of potential violations of Federal criminal law
involving fraud bribery or gratuity violations potentially affecting the Federal award 45 CFR 75113 notes mandatory disclosures of criminal offenses that non-Federal entities must make with respect to HHS grants Recipients submitting disclosures in connection with this requirement should include the subject reference line Mandatory Grant Disclosure Recipients choosing to disclose conduct that may not fit squarely within the scope of offenses described in 45 CFR 75113 should include the following subject reference line in the submission Voluntary Grant Disclosure
Medicare 60 day rule
The 60 Day Rule (Medicare Parts A amp B) o The 60 day time period for reportingreturning begins when either
ndash The reasonable diligence is completed orndash On the day the provider received credible information of a potential overpayment (if the
provider fails to conduct reasonable diligence) o For an investigation to be conducted in a ldquotimelyrdquo manner providers typically
must complete the investigation within 6 months from receipt of credible information indicating there may be an overpayment
ndash ndash 6-month timeframe may potentially be extended under ldquoextraordinary circumstancesrdquo ndash 8 months generally the maximum total time to return overpayments The government recommends that providers maintain records documenting ldquoreasonable diligencerdquo
Medicare 60 Day Rule
Six-year lookback period ndash Sometimes possible to use a shorter period depending on the facts at issue Amount to be repaid ndash May vary depending on the method used to
reportreturn eg Medicare administrative contractor (ldquoMACrdquo) v self-disclosure Overpayment notification ndash After receiving an overpayment
notification from the government you should investigate for related overpayments eg other time periods
Medicare 60 Day Rule
Self-disclosure protocols ndashoA submission to the OIG or CMS protocols suspends the 60 day requirement
for returning overpayments until a settlement agreement is executed ndash ndash OIGrsquos Self-Disclosure Protocol (SDP) ndash ndash CMS Voluntary Self-Referral Disclosure Protocol (SRDP) ndash
o Self-disclosures to other agencies do not suspend the repayment deadlinendash ndash Eg Department of Justice local US Attorneyrsquos Office Medicaid Fraud Control Unit
Medicare 60 Day Rule
Facilitating Compliance With the 60 Day Rule Compliance programs should include o ndash Appropriate policies and procedures o ndash Periodic billing and coding audits to proactively identify overpaymentso ndash Focus on high-risk areas o ndash Utilization of publicly available government resources to guide audit efforts o ndash Investigating any suspected incidents of non-compliance with federal health
care program requirements
Self Disclosure
Choice of AgencyoOIG ndash Self-Disclosure Protocol
ndash ndash Conduct involving false billingndash ndash Conduct involving excluded personsndash ndash Conduct involving the Anti-Kickback Statute (including conduct thatndash violates both the AKS and Stark Law)
oCMS ndash Self-Referral Disclosure Protocolndash ndash Conduct involving only violations of the Stark Law
oDOJndash ndash May be appropriate when provider believes a FCA release is necessary
Summary
The Cost of a Well-Executed Coding Audit ProcessThe costs associated with an auditing program are worth it in the long run Ideally your organization is performing audits on a regular basis across all service types locations and payers Weve all seen claims that have been denied resulting in additional work that may be preventable with a proper audit program The goal is to use the audit feedback to improve coding quality and lower potential risk and cost to the organization Organizations should be investing in an effective coding audit program to make your coders and providers better and enhance documentation improvement from the providers
Questions
Thank you for your attentionLynn Handy
Vice President of Coding amp Audit ServicesLynnhandymanagedresourcesinccom

ProviderCoder Audit Reports
Detailed Audit reports should have the ability to be sorted byoProvideroCodero Specialty or GroupoAudit Date
Detailed results for each encounteroMeaningful comments
Key Findingso From all encounters
Recommendations and Resources
Detailed Findings Patient ID Patient Name DOS Payer CPT Reported CPT Audited EM Level Key Component ICD Reported ICD Reported Description ICD Audited ICD Reported Description
1 001 Patient A 02-19-16 Blue Cross
99203 25 1 99202 1 +1 D E L 1 S92302A2 Not Reported
1 Fracture of unspecified metatarsal bone(s) left foot initial encounter for closed fracture
1 S92355D2 W109XXD
1 Nondisplaced fracture of fifth metatarsal bone left foot subsequent encounter for fracture with routine healing2 Fall (on) (from) unspecified stairs and steps subsequent encounter
1 The documentation supports coding for an EM service that is one level below the billed code2 Lacking Exam documentation to support the EM level selected3 1997 MSK exam supports an Expanded Problem Focused exam (99202) 1995 exam supports a Detailed exam (99203)4 1997 Exam template suggestions Neurologic Exam-suggest adding the body part examined (upper extremitylow extremity) Dermatologic Exam-unable to determine if this was performed This should be deleted from the final note if
not examined5 EM time statement is insufficient documentation is lacking a required element total time of visit and counseling time greater than 506 CPT disallowed documentation is not present within the medical record to support the CPT code billed (28485-open treatment of metatarsal fracture includes internal fixation when performed) Fracture care is not supported patient
was seen in the ER 6 weeksrsquo prior ER doctor initiated treatment7 The incorrect pricing modifier was billed Removed modifier 25 (separate and significant EM on the same day as a minor procedure) Fracture care is not billable no modifier needed on EM service8 Diagnosis billed is not the most specific available according to the medical record documentation9 Documentation supports an additional diagnosis code not billed
2 002 Patient B 02-05-16 Blue Cross
99203 25 1 99202 25 1 +1 D E L 1 L03032 1 Cellulitis of left toe 1 L03032 1 Cellulitis of left toe
1 The documentation supports coding for an EM service that is one level below the billed code2 Lacking Exam documentation to support the EM level selected3 1997 MSK exam supports an Expanded Problem Focused exam (99202) 1995 exam supports a Detailed exam (99203)4 EM time statement is insufficient documentation is lacking one or more required elements (total time counseling time greater than 50) If a procedure is performed during a visit the time spent performing the procedure needs to be
carved out of the total visit time5 Allowed modifier 25 due to commercial payer Medicare and NCCI do not require modifier 25 on a new patient EM when a minor procedure is performed the same day 6 Diagnosis supported
Detailed Findings
135 822012 New Consultations - Office
Consultations Detailed Detailed (95) Moderate 99244 99243 1 $3500 N
Provider Code 99244 Reviewer Code 99243 Provider Diagnosis 1 3005 NEURASTHENIA Reviewer Diagnosis 1 3005 NEURASTHENIA Provider Diagnosis 2 7282 MUSC DISUSE ATROPHY NEC Reviewer Diagnosis 2 7282 MUSC DISUSE ATROPHY NEC
bull Assessment (I) The assessment is not clearly stated for this encounter Documentation Guidelines states The documentation for each patient encounter should include assessment clinical impression or diagnosis bull Assessment (R) The assessment should be clearly documented for each encounter Since each note must stand alone it is imperative to accurately document the most specific diagnosis in the assessment impression section of the note
bull Documented Lower Level (I) The documentation substantiates a lower level of service than charged
Chart Level Comments
Group your comments in categoriesoDocumentationo E amp MoProceduresoModifierso ICD-10-CM
oReportsAudit Manager Macros 061218 (version 1)xlsx
Recommendations and ReferencesCategory Short Description Long Description
EM AdmissionDischarge Same Day Review the CMS AdmissionDischarge same day coding guidelines httpswwwcmsgovRegulations-and-GuidanceGuidanceManualsDownloadsclm104c12pdf
EM ConsultationReview the consultation guidelines located in the CPT book
EM Consultation not billable to Medicare CMS no longer recognizes the consultation codeshttpswwwcmsgovOutreach-and-EducationMedicare-Learning-Network-MLNMLNMattersArticlesdownloadsmm6740pdf
EM Critical CareReview the CMS Critical Care guidelines httpswwwcmsgovOutreach-and-EducationMedicare-Learning-Network-MLNMLNMattersArticlesdownloadsmm5993pdf
EM Discharge ServicesReview the CMS Hospital Discharge Services guidelineshttpswwwcmsgovOutreach-and-EducationMedicare-Learning-Network-MLNMLNMattersArticlesdownloadsmm5794pdf
EMEM and Preventive Visit Review AAPC guidance for documenting and billing an EM and Preventive visit same day httpswwwaapccomblog22580-successfully-bill-a-
preventive-service-with-a-sick-visit
EM EM documentation guidelines Review the CMS 1995 amp 1997 EM documentation guidelineshttpswwwcmsgovOutreach-and-EducationMedicare-Learning-Network-MLNMLNEdWebGuideEMDOChtml
EM EM Inpatient vs Outpatient Review the patientrsquos status on the hospital admission order to determine the appropriate EM category to bill (inpatient vs observation)
EM EM New vs EstablishedReview the CMS New vs Established patient guidelines httpswwwcmsgovOutreach-and-EducationMedicare-Learning-Network-MLNMLNProductsDownloadseval-mgmt-serv-guide-ICN006764pdf
EMEM Time billing suggestion
Recommend a time statement is added to the EM medical record when a majority of the visit is spent counseling andor coordination of care Review the CMS 1995 amp 1997 EM documentation guidelines for EM time documentationhttpswwwcmsgovOutreach-and-EducationMedicare-Learning-Network-MLNMLNEdWebGuideEMDOChtml
EM Inpatient hospital servicesReview the CMS Hospital Services (Initial and Subsequent) guidelines httpswwwcmsgovRegulations-and-GuidanceGuidanceManualsDownloadsclm104c12pdf
EM Nursing Facility Services Review the Nursing Facility Services guidelines provided by CMS The guidelines can be downloaded at this linkhttpswwwcmsgovRegulations-and-GuidanceGuidanceManualsDownloadsclm104c12pdf
EM Observation Services Review the CMS Observation Services (Initial and Subsequent) guidelines httpswwwcmsgovRegulations-and-GuidanceGuidanceManualsDownloadsclm104c12pdf
EM Prolonged Services Review the CMS Prolonged Services guidelines httpswwwcmsgovOutreach-and-EducationMedicare-Learning-Network-MLNMLNMattersArticlesdownloadsmm5972pdf
EMReview of Systems Review the CMS 1995 amp 1997 EM documentation guidelines for Review of Systems requirements
httpswwwcmsgovOutreach-and-EducationMedicare-Learning-Network-MLNMLNEdWebGuideEMDOChtml
EMConsultation Documentation Suggestion
Recommend adding verbiage to consultation documentation that indicates the name of the referring provider and the reason for the consultation
Audit Report Examples Automated Solution
Letrsquos look at some report Examples
ReportsStandard Provider Audit SummarypdfReportsProvider Detailed Sample Reportdocx
ReportsProvider Audit Worksheets - Optionalpdf
Audit Report Examples Non Automated Solution
Error Findings by Volume Percentage
CPT Coded Accurately
8 8 Overcoded
8 8 Undercoded
Missed CPTHCPCS Code
Missed or Wrong Modifier
8 8 Incorrect CPT (or Category) Used
Incorrect ICD-9 Codes
8 8 Incorrect Quantity
Inadequate Documentation
Missing Documentation 8 8
Signature Illegible (No Log)
8 8
CLIENT NAME PROJECT TITLE
Review Line Item Detail Prepared Month Year
DRAFT
Client Claim Demographics Client Charge Data Review Result EampM ONLY Findings C C C C C C O OC O O O
Char
t Num
ber
Au
dit D
ate
Audi
tor (
initi
als)
QA
Initi
als
Fa
cilit
y Lo
catio
n Re
porte
d
Pr
ovid
er N
ame
Pa
tient
Nam
e
M
edic
al R
ecor
d Nu
mbe
r
Prim
ary
Carr
ier M
edica
re=
A M
edica
id =
B O
ther
=O
Da
te o
f Ser
vice
CP
T Co
de
Mod
ifier
(s) i
n or
der
Qua
ntity
Diag
nosi
s Co
de(s
) 1
thro
ugh
4
Fe
e ch
arge
d
Pr
imar
y Pa
ymen
t Am
ount
CPT
Code
Mod
ifier
(s) i
n or
der
Qua
ntity
Diag
nosi
s Co
de(s
) 1
thro
ugh
4
CO
RREC
T AL
LOW
ABLE
Prim
ary
PAYM
ENT
Va
rianc
e
Chie
f Com
plai
nt
Hist
ory
Leve
l Sup
port
ed
Exam
Lev
el S
uppo
rted
Med
ical
Dec
Mak
ing
Supp
orte
d (o
r TIM
E)
CPT
Cod
ed A
ccur
atel
y
Ove
rcod
ed
Und
erco
ded
Mis
sed
CPT
HC
PCS
Cod
e
Mis
sed
or W
rong
Mod
ifier
Inco
rrec
t CPT
(or C
ateg
ory)
Use
d
Inco
rrec
t IC
D-9
Cod
es
Inco
rrec
t Qua
ntity
Inad
equa
te D
ocum
enta
tion
Mis
sing
Doc
umen
tatio
n
Sign
atur
e Ill
egib
le (N
o Lo
g)
No
Sign
atur
e by
Pro
vide
r of
Ser
vice
COMMENTS (abbreviations used) PF- PROBLEM FOCUSED EPF- EXPANDED PF DET- DETAILED COMP- COMPREHENSIVE SFWD- STRAIGHT FORWARD MOD- MODERATE MDM- MEDICAL DECISION MAKING
Char
t Num
ber
SAMPLE SAMPLE S MD SAMPLE SAMPLE XXXXX XXX 112001 99212 25 1 1 1234 2 5678 3 4
$30000 $2200 99212 25 1 1 1234 2 5678 3 4
$56400 $54200 YES
DET
CO
MP
MO
D
COMMENTS COMMENTS COMMENTS
0
1 2 3 4
1 2 3 4
$000 0
$30000 $2200 $56400 $54200 10 10 10 10 10 10 10 10 10 10 10 10 TOTALS 917 Error Rate by Volume
Error Findings by Volume 8 CPT Coded Accurately 8 Overcoded 8 Undercoded 8 Missed CPTHCPCS Code 8 Missed or Wrong Modifier 8 Incorrect CPT (or Category) Used 8 Incorrect ICD-9 Codes 8 Incorrect Quantity
Inadequate Documentation 8 8 Missing Documentation 8 Signature Illegible (No Log) 8 No Signature by Provider of Service
1200 Total
Net Payment Error Rate -24636
Primary Payments Total $ Audited Payment Total $ (Total Under Payments)
Total Over Payments
Net OverUnder Payment $
2200 56400
(54200)
Resources Used HCPCS and CPT CodeBook (Current or applilcable year) ICD-10-CM CodeBook (Current or applicable year) CMS 1995 and 1997 EM Guidelines CMS Claims Processing Manual 100-04 Medicare Claims Processing (PUB 100-04) CMS - National Coverage Determinations (NCDs) National Correct Coding Policy Manual Applicable Physician Version
Executive Summary Report
The executive summary provides readers with a short complete document highlighting import information included in the detailed report Executive summaries are created for the senior management readers that donrsquot have time to read the full report and need to walk away with an understanding of the issues and corrective actions
Some would say the executive summary could be written before the detailed report however it is difficult to make sure the most important elements are included until you have spent time reviewing the detail If you want to make sure the most important messages are in the executive
summary this step should be completed after the detail is written As auditors become more seasoned this step could move to the front of the process
Executive Summary Report Structure of the ES Report
o Backgroundndash Specialtyndash Providersndash Sample Selection sizendash Date range of audit
o Audit Scopeo Regulatory Resourceso Type of Medical records reviewedo Overall Accuracy (all providers)o Detailed Audit Findings
ndash Business Impactndash Summary of Findings
o Department Findingso Summary
o ReportsStandard Executive Summary Professional Servicespdf
Department Findings Top Issues
Date ofServiceErrors
MissingDocuments
Missing orInvalid
Signature
TeachingPhysician
Errors
InsufficientConsultation
Documents
OverCoding
EMBundled
IntoGlobal
SurgicalPackage
SplitSharedServiceError
Incorrector
MissingPricing
Modifier
ICD-10Errors
Family Practice
CardiologyInternal Medicine
TOTALS
Top Findings by Provider
E amp M Accuracy Rates
ICD-10-CM Accuracy Rates
Procedure Accuracy Rates
Inpatient DRG Audit Report
TABLE OF CONTENTS
Executive Summaryo Scope of Work
Reimbursement Changes Department Results
o InpatientGeneral Recommendations and Comments
o Secondary DiagnosesoProcedure CodingoPresent on AdmissionoQueries
Scope of WorkCodingAID performed coding audit review of 175 inpatient records The review completed was a random sample that included cases coded by twenty coders for dates of service from May 2016 ndash July 2016
The objective was to determine if the medical record documentation supported the following coding and documentation requirements and any other regulatory requirement for that code set Criteria reviewed
1 ICD-10-CM Official Coding Guidelines for accurate diagnosis code reporting 2 ICD-10-PCS Official Coding Guidelines for accurate procedure code reporting 3 Documentation of procedure compared to the CPT code assigned 4 Identify opportunities for education and training 5 Financial impact of current coding practices
The regulatory agencies and reference materials relied upon include the following in addition to Medicare and Medicaid regulations Additional resources are located in the sub sections below
bull ICD-10-CM and ICD-10-PCS for Hospitals current volume bull Centers for Medicare and Medicaid Services CMS NCCI Edits-Centers for Medicaid and
Medicare Services CMS website wwwcmsgov bull AHA Coding Clinic
The following electronic medical record documents were reviewed and relied upon to compare to the actual codes submitted to the third party payer
bull Discharge summaries HampPs Progress Notes and other provider notes located in the EMR Records
bull Patient History Forms Ancillary Staff Notes bull Procedure Notes bull Orders bull Diagnostic Report
Reimbursement Changes
Coder Acct
Billed Audited
Reimbursement ChangesMS DRG SOI ROM Weight Expected
Payment MS DRG SOI ROM Weight Expected Payment
Coder 1 001 790 52300 $2615000 792 21552 $1077600 -$1537400
Coder 2002
749 26452 $1322600 758 10090 $504500 -$818100
Coder 3 003 669 13111 $655550 694 07294 $364700 -$290850
Coder 4 004 389 08707 $435350 394 09502 $475100 $39750
Coder 5 005 312 07630 $381500 812 08572 $428600 $47100
Coder 6 006 384 08481 $424050 378 09949 $497450 $73400
Coder 7 007 206 08164 $408200 794 12987 $649350 $241150
Coder 8008
344 31029 $1551450 853 51334 $2566700 $1015250
TOTAL $7793700 $6564000 -$1229700
General Recommendations and CommentsFinding Pertinent secondary diagnoses are not coded and diagnoses are code which are not supported in provider documentation Code only those diagnoses which are documented by the provider on the current chart Not all codes are coded to the highest degree of specificity and combination codes were sometimes missed
Recommendation It is important to assign codes for all conditions which meet the definition of a reportable diagnosis Documentation from all providers should be used including but not limited to radiologists pathologists anesthesiologists CRNAs and FNPs
Reference Coding Clinic Official Coding Guidelines
bull Report all secondary diagnoses which meet the definition of a secondary diagnosis which is defined as all conditions that coexist at the time of admission that develop subsequently or that affect the treatment received andor the length of stay Codes which enhance the overall picture of the patientrsquos visit should be added
o Add T45515A to report adverse effect of Coumadin which caused the GI bleed
o Add I2690 for septic pulmonary emboli (MCCSOI4ROM4)
o Add N179 for acute kidney failure (S3M2CC) per the nephrology consult and the 628 progress note
o Add code I429 cardiomyopathy per HampP
o Add B964 to report proteus in a UTI per the 620 hospitalist progress note
o Code for D649 anemia and I701 stenosis of renal artery should be added as secondary diagnoses per the HampP
bull Only report diagnoses which are substantiated by provider documentation in the current chart notes If a suspected condition is not verified at discharge on an inpatient account it cannot be coded
o Remove G4734 (idiopathic sleep related non-obstructive alveolar hypoventilation) as patient was noted to have the sleep study and the hypoventilation was shown to be a possibility but not noted as such on discharge
o Remove G629 (S21) the neuropathy is documented as due to diabetes
o Remove K529 colitis noted on HP as possible but not further noted or confirmed at discharge
Procedure CodingFinding Procedures were sometimes coded incorrectly
Recommendation The entire medical record should be reviewed and all procedures coded as documented Coding procedures incorrectly or assigning incorrect CPT codes may result in lost revenue
bull Incorrect root operation
o Revise principal procedure to 0DQ68ZZ for clipping of the ulcer per OP report clipping is root operation repair
bull Biopsy versus Excision
o Procedure 0DBA0ZX (biopsy of jejunum) should change to 0DBA0ZZ (excision of jejunum) per op note this was not a biopsy procedure
bull Coding Guideline error
o Remove 0RG10K0 for allograft due to being inclusive in principal procedure
o Remove codes for adhesiolysis 0DN80ZZ 0UN10ZZ and 0UN90ZZ due to no significance noted per OP report
bull Incorrect approach
o Revise 0TF63ZZ (fragmentation percutaneous approach) to 0TF68ZZ (fragmentation endoscopic) for procedure performed via scope per the operative report
bull Procedure coded without provider documentation
o Remove secondary procedure of excisional debridement (0JB90ZZ) due to lack of documentation of excisional debridement per operative report The header in the operative report documents IampD and debridement but the body of the operative report only documents an IampD
bull Incorrect CPT code assignment
o Post-op note supports the nerve block injections of four nerves therefore code 64421 (multiple nerve block) should replace 64420 (injection of one intercostal nerve)
Queries Finding Conflicting incomplete and vague documentation is found within provider chart notes
Recommendation Prior to code assignment if the coder finds ambiguous or conflicting documentation the provider should be queried
Reference AHA Coding Clinic 2002 2nd Quarter pages 17-18
bull Query for acute blood loss anemia since hgb has dropped and patient is being transfused PRBC
bull Recommend query to clarify if cardiorenal syndrome is current as it is documented per 627 nephrology consult but unclear if current
bull Documentation does not support SIRS noninfectious without organ failure It is conflicting since patient has respiratory failure Query should be initiated for clarification with or without organ failure or infectious or non-infectious Patient has pneumonia per query as well as last progress note therefore if SIRS is not further specified per query PNA should be sequenced as principal diagnosis and SIRS should be removed
bull Recommend provider query necrotizing lung consolidation noted on DS as principal diagnosis-unclear does the patient have lobar pneumonia Secondary dx states necrotic pneumonia which is coded as principal diagnosis-this diagnosis is clear but consolidation portion is unclear
bull Recommend query for preterm labor delivery at 301 weeks
bull RECOMMEND QUERY no chest pain on admit per ER and HP cardiology provider states no CP with ER stating chest pressure the day prior to admit Appears patient was admitted due to elevated troponins which cardiology says are likely due to hypotension and AKI DS states chest pain but also says bradycardia and hypotension were the reason for admit
bull RECOMMEND QUERY no chest pain on admit per ER and HP cardiology provider states no CP with ER stating chest pressure the day prior to admit Appears patient was admitted due to elevated troponins which cardiology says are likely due to hypotension and AKI DS states chest pain but also says bradycardia and hypotension were the reason for admit
bull Query the provider regarding pathology report notation of endometriosis andor possible re-sequence of stenosis as principal diagnosis as it also meets principal diagnosis guidelines This would result in an MS-DRG change to 742 and APR-DRG change to 513
bull QUERY secondary diagnosis MCC and ROM 4 code T3166 (60 TBSA of which 60 are third degree burns) Chart notes do not specify how much of TBSA was actually third degree If after query TBSA is found to be less than 50 (T3164) then ROM will change from 4 to 3 but no change to overall APR-DRG or weight
Auditor Quality amp Productivity
Audit Productivity Standards
It takes twice as long to audit a chart as it does to code it a statistic that takes into account the time to document an explanation of any coding decision the auditor is not in agreement with o For example in an emergency department audit with a productivity of 12
charts per hour for a coder our auditors would probably be able to review six per hour
o If there are multiple services to audit on each encounter the productivity may only be 4 per hour
o The amount of detail you put into your audit report will also be a factorndash Are you using an automated audit softwarendash Are you using a spreadsheet to auditndash How many Systems are needed to complete the audit
Coder Quality Audits
Quality Audits (QA) should be done on your coders and auditors regularly Frequent reviews with smaller sample size will allow more consistent
review and feedbacko Example 10 charts per month per coder if the coder passes 2-3 months
consecutively with 95 or better score move them to quarterly reviewso Some QA programs review a percentage of the coders work This
methodology requires more time and resources
Auditor QA should also score and comment on the accuracy of the audit comments and recommendations
Presenting the Audit Results
Presenting the Audit Results
Communicating the Audit FindingsoWho requested the AuditoWho are you reporting the finding to
ndash CEOndash CFOndash Physicianndash Revenue Cycle Managerndash HIM Directorndash Billing Managerndash Coding Manager
ReportsAudit Resultspptx
Post Audit Education
Provider Education
Provider Education is best received when it is specific to the provider(s) 11 sessions going over the audit result Look at their notes with them
oHighlight areas for documentation improvementoReinforce Coding Guidelines that are specific to themoAsk them to share how they establish their LOS for E amp M serviceso Integrate their EMR system into the training
Provider Education
Group Training SessionsoUse the audit results to identify common issues within a specialty group
ndash Refer to the Executive Summary reportoVery effective for identifying system issues
ndash Teaching Attestationsndash Templatesndash Copy and Pastendash Cloned notes
o Everyone hears the same messagesoAn Issue may not appear on the individual audit but is still a concern for the
group
Education Delivery
In person or remote sessionso Factors to consider
ndash Providers scheduleavailabilityndash Location(s)ndash Personality of the providerndash Budget
Coder Education
Coders do well in group training so they can learn from each other 11 training allows the coder to get feedback on their coding
Handling Audit Disputes
Handling Audit Disputes
Be open to all points of viewo Let the documentation tell the story
Refer to the guidelines Ask
oCan we defend the reported service with the current documentation
Self Disclosures Refunds and Corrected Billing
Overpayment
In general If a person has received an overpayment the person shallo report and return the overpayment to the Secretary the State an
intermediary a carrier or a contractor as appropriate at the correct address and ndash notify the Secretary State intermediary carrier or contractor to whom the overpayment was returned in writing of the reason for the overpayment
What is an ldquoOverpaymentrdquo ndash The term ldquooverpaymentrdquo means any funds that a person receives or retains under subchapter XVIII or XIX of this chapter to which the person after applicable reconciliation is not entitled under such subchapter
Self Disclosure
The Office of Inspector General (OIG) has several self-disclosure processes that can be used to report potential fraud in Department of Health and Human Services (HHS) programs Choose the one that applies to you from the following descriptions to learn moreo Health Care Provider Self-Disclosures
ndash Health care providers suppliers or other individuals or entities subject to Civil Monetary Penalties can use the Provider Self-Disclosure Protocol which was created in 1998 to voluntarily disclose self-discovered evidence of potential fraud Self-disclosure gives providers the opportunity to avoid the costs and disruptions associated with a Government-directed investigation and civil or administrative litigation Visit the Provider Self-Disclosure Protocol webpage for more information
o HHS Contractor Self-Disclosuresndash Contractors are individuals businesses or other legal entities that are awarded Government contracts or
subcontracts to provide services to the Department of Health and Human Services (HHS) OIGs contractor self-disclosure program enables contractors to self-disclose potential violations of the False Claims Act and various Federal criminal laws involving fraud conflict of interest bribery or gratuity This self-disclosure process is available for those entities with a Federal Acquisition Regulation-based contract Visit the Contractor Self-Disclosure webpage for more information
o HHS Grantee Self-Disclosuresndash HHS grantees or subrecipients may voluntarily disclose evidence of potential violations of Federal criminal law
involving fraud bribery or gratuity violations potentially affecting the Federal award 45 CFR 75113 notes mandatory disclosures of criminal offenses that non-Federal entities must make with respect to HHS grants Recipients submitting disclosures in connection with this requirement should include the subject reference line Mandatory Grant Disclosure Recipients choosing to disclose conduct that may not fit squarely within the scope of offenses described in 45 CFR 75113 should include the following subject reference line in the submission Voluntary Grant Disclosure
Medicare 60 day rule
The 60 Day Rule (Medicare Parts A amp B) o The 60 day time period for reportingreturning begins when either
ndash The reasonable diligence is completed orndash On the day the provider received credible information of a potential overpayment (if the
provider fails to conduct reasonable diligence) o For an investigation to be conducted in a ldquotimelyrdquo manner providers typically
must complete the investigation within 6 months from receipt of credible information indicating there may be an overpayment
ndash ndash 6-month timeframe may potentially be extended under ldquoextraordinary circumstancesrdquo ndash 8 months generally the maximum total time to return overpayments The government recommends that providers maintain records documenting ldquoreasonable diligencerdquo
Medicare 60 Day Rule
Six-year lookback period ndash Sometimes possible to use a shorter period depending on the facts at issue Amount to be repaid ndash May vary depending on the method used to
reportreturn eg Medicare administrative contractor (ldquoMACrdquo) v self-disclosure Overpayment notification ndash After receiving an overpayment
notification from the government you should investigate for related overpayments eg other time periods
Medicare 60 Day Rule
Self-disclosure protocols ndashoA submission to the OIG or CMS protocols suspends the 60 day requirement
for returning overpayments until a settlement agreement is executed ndash ndash OIGrsquos Self-Disclosure Protocol (SDP) ndash ndash CMS Voluntary Self-Referral Disclosure Protocol (SRDP) ndash
o Self-disclosures to other agencies do not suspend the repayment deadlinendash ndash Eg Department of Justice local US Attorneyrsquos Office Medicaid Fraud Control Unit
Medicare 60 Day Rule
Facilitating Compliance With the 60 Day Rule Compliance programs should include o ndash Appropriate policies and procedures o ndash Periodic billing and coding audits to proactively identify overpaymentso ndash Focus on high-risk areas o ndash Utilization of publicly available government resources to guide audit efforts o ndash Investigating any suspected incidents of non-compliance with federal health
care program requirements
Self Disclosure
Choice of AgencyoOIG ndash Self-Disclosure Protocol
ndash ndash Conduct involving false billingndash ndash Conduct involving excluded personsndash ndash Conduct involving the Anti-Kickback Statute (including conduct thatndash violates both the AKS and Stark Law)
oCMS ndash Self-Referral Disclosure Protocolndash ndash Conduct involving only violations of the Stark Law
oDOJndash ndash May be appropriate when provider believes a FCA release is necessary
Summary
The Cost of a Well-Executed Coding Audit ProcessThe costs associated with an auditing program are worth it in the long run Ideally your organization is performing audits on a regular basis across all service types locations and payers Weve all seen claims that have been denied resulting in additional work that may be preventable with a proper audit program The goal is to use the audit feedback to improve coding quality and lower potential risk and cost to the organization Organizations should be investing in an effective coding audit program to make your coders and providers better and enhance documentation improvement from the providers
Questions
Thank you for your attentionLynn Handy
Vice President of Coding amp Audit ServicesLynnhandymanagedresourcesinccom

Detailed Findings Patient ID Patient Name DOS Payer CPT Reported CPT Audited EM Level Key Component ICD Reported ICD Reported Description ICD Audited ICD Reported Description
1 001 Patient A 02-19-16 Blue Cross
99203 25 1 99202 1 +1 D E L 1 S92302A2 Not Reported
1 Fracture of unspecified metatarsal bone(s) left foot initial encounter for closed fracture
1 S92355D2 W109XXD
1 Nondisplaced fracture of fifth metatarsal bone left foot subsequent encounter for fracture with routine healing2 Fall (on) (from) unspecified stairs and steps subsequent encounter
1 The documentation supports coding for an EM service that is one level below the billed code2 Lacking Exam documentation to support the EM level selected3 1997 MSK exam supports an Expanded Problem Focused exam (99202) 1995 exam supports a Detailed exam (99203)4 1997 Exam template suggestions Neurologic Exam-suggest adding the body part examined (upper extremitylow extremity) Dermatologic Exam-unable to determine if this was performed This should be deleted from the final note if
not examined5 EM time statement is insufficient documentation is lacking a required element total time of visit and counseling time greater than 506 CPT disallowed documentation is not present within the medical record to support the CPT code billed (28485-open treatment of metatarsal fracture includes internal fixation when performed) Fracture care is not supported patient
was seen in the ER 6 weeksrsquo prior ER doctor initiated treatment7 The incorrect pricing modifier was billed Removed modifier 25 (separate and significant EM on the same day as a minor procedure) Fracture care is not billable no modifier needed on EM service8 Diagnosis billed is not the most specific available according to the medical record documentation9 Documentation supports an additional diagnosis code not billed
2 002 Patient B 02-05-16 Blue Cross
99203 25 1 99202 25 1 +1 D E L 1 L03032 1 Cellulitis of left toe 1 L03032 1 Cellulitis of left toe
1 The documentation supports coding for an EM service that is one level below the billed code2 Lacking Exam documentation to support the EM level selected3 1997 MSK exam supports an Expanded Problem Focused exam (99202) 1995 exam supports a Detailed exam (99203)4 EM time statement is insufficient documentation is lacking one or more required elements (total time counseling time greater than 50) If a procedure is performed during a visit the time spent performing the procedure needs to be
carved out of the total visit time5 Allowed modifier 25 due to commercial payer Medicare and NCCI do not require modifier 25 on a new patient EM when a minor procedure is performed the same day 6 Diagnosis supported
Detailed Findings
135 822012 New Consultations - Office
Consultations Detailed Detailed (95) Moderate 99244 99243 1 $3500 N
Provider Code 99244 Reviewer Code 99243 Provider Diagnosis 1 3005 NEURASTHENIA Reviewer Diagnosis 1 3005 NEURASTHENIA Provider Diagnosis 2 7282 MUSC DISUSE ATROPHY NEC Reviewer Diagnosis 2 7282 MUSC DISUSE ATROPHY NEC
bull Assessment (I) The assessment is not clearly stated for this encounter Documentation Guidelines states The documentation for each patient encounter should include assessment clinical impression or diagnosis bull Assessment (R) The assessment should be clearly documented for each encounter Since each note must stand alone it is imperative to accurately document the most specific diagnosis in the assessment impression section of the note
bull Documented Lower Level (I) The documentation substantiates a lower level of service than charged
Chart Level Comments
Group your comments in categoriesoDocumentationo E amp MoProceduresoModifierso ICD-10-CM
oReportsAudit Manager Macros 061218 (version 1)xlsx
Recommendations and ReferencesCategory Short Description Long Description
EM AdmissionDischarge Same Day Review the CMS AdmissionDischarge same day coding guidelines httpswwwcmsgovRegulations-and-GuidanceGuidanceManualsDownloadsclm104c12pdf
EM ConsultationReview the consultation guidelines located in the CPT book
EM Consultation not billable to Medicare CMS no longer recognizes the consultation codeshttpswwwcmsgovOutreach-and-EducationMedicare-Learning-Network-MLNMLNMattersArticlesdownloadsmm6740pdf
EM Critical CareReview the CMS Critical Care guidelines httpswwwcmsgovOutreach-and-EducationMedicare-Learning-Network-MLNMLNMattersArticlesdownloadsmm5993pdf
EM Discharge ServicesReview the CMS Hospital Discharge Services guidelineshttpswwwcmsgovOutreach-and-EducationMedicare-Learning-Network-MLNMLNMattersArticlesdownloadsmm5794pdf
EMEM and Preventive Visit Review AAPC guidance for documenting and billing an EM and Preventive visit same day httpswwwaapccomblog22580-successfully-bill-a-
preventive-service-with-a-sick-visit
EM EM documentation guidelines Review the CMS 1995 amp 1997 EM documentation guidelineshttpswwwcmsgovOutreach-and-EducationMedicare-Learning-Network-MLNMLNEdWebGuideEMDOChtml
EM EM Inpatient vs Outpatient Review the patientrsquos status on the hospital admission order to determine the appropriate EM category to bill (inpatient vs observation)
EM EM New vs EstablishedReview the CMS New vs Established patient guidelines httpswwwcmsgovOutreach-and-EducationMedicare-Learning-Network-MLNMLNProductsDownloadseval-mgmt-serv-guide-ICN006764pdf
EMEM Time billing suggestion
Recommend a time statement is added to the EM medical record when a majority of the visit is spent counseling andor coordination of care Review the CMS 1995 amp 1997 EM documentation guidelines for EM time documentationhttpswwwcmsgovOutreach-and-EducationMedicare-Learning-Network-MLNMLNEdWebGuideEMDOChtml
EM Inpatient hospital servicesReview the CMS Hospital Services (Initial and Subsequent) guidelines httpswwwcmsgovRegulations-and-GuidanceGuidanceManualsDownloadsclm104c12pdf
EM Nursing Facility Services Review the Nursing Facility Services guidelines provided by CMS The guidelines can be downloaded at this linkhttpswwwcmsgovRegulations-and-GuidanceGuidanceManualsDownloadsclm104c12pdf
EM Observation Services Review the CMS Observation Services (Initial and Subsequent) guidelines httpswwwcmsgovRegulations-and-GuidanceGuidanceManualsDownloadsclm104c12pdf
EM Prolonged Services Review the CMS Prolonged Services guidelines httpswwwcmsgovOutreach-and-EducationMedicare-Learning-Network-MLNMLNMattersArticlesdownloadsmm5972pdf
EMReview of Systems Review the CMS 1995 amp 1997 EM documentation guidelines for Review of Systems requirements
httpswwwcmsgovOutreach-and-EducationMedicare-Learning-Network-MLNMLNEdWebGuideEMDOChtml
EMConsultation Documentation Suggestion
Recommend adding verbiage to consultation documentation that indicates the name of the referring provider and the reason for the consultation
Audit Report Examples Automated Solution
Letrsquos look at some report Examples
ReportsStandard Provider Audit SummarypdfReportsProvider Detailed Sample Reportdocx
ReportsProvider Audit Worksheets - Optionalpdf
Audit Report Examples Non Automated Solution
Error Findings by Volume Percentage
CPT Coded Accurately
8 8 Overcoded
8 8 Undercoded
Missed CPTHCPCS Code
Missed or Wrong Modifier
8 8 Incorrect CPT (or Category) Used
Incorrect ICD-9 Codes
8 8 Incorrect Quantity
Inadequate Documentation
Missing Documentation 8 8
Signature Illegible (No Log)
8 8
CLIENT NAME PROJECT TITLE
Review Line Item Detail Prepared Month Year
DRAFT
Client Claim Demographics Client Charge Data Review Result EampM ONLY Findings C C C C C C O OC O O O
Char
t Num
ber
Au
dit D
ate
Audi
tor (
initi
als)
QA
Initi
als
Fa
cilit
y Lo
catio
n Re
porte
d
Pr
ovid
er N
ame
Pa
tient
Nam
e
M
edic
al R
ecor
d Nu
mbe
r
Prim
ary
Carr
ier M
edica
re=
A M
edica
id =
B O
ther
=O
Da
te o
f Ser
vice
CP
T Co
de
Mod
ifier
(s) i
n or
der
Qua
ntity
Diag
nosi
s Co
de(s
) 1
thro
ugh
4
Fe
e ch
arge
d
Pr
imar
y Pa
ymen
t Am
ount
CPT
Code
Mod
ifier
(s) i
n or
der
Qua
ntity
Diag
nosi
s Co
de(s
) 1
thro
ugh
4
CO
RREC
T AL
LOW
ABLE
Prim
ary
PAYM
ENT
Va
rianc
e
Chie
f Com
plai
nt
Hist
ory
Leve
l Sup
port
ed
Exam
Lev
el S
uppo
rted
Med
ical
Dec
Mak
ing
Supp
orte
d (o
r TIM
E)
CPT
Cod
ed A
ccur
atel
y
Ove
rcod
ed
Und
erco
ded
Mis
sed
CPT
HC
PCS
Cod
e
Mis
sed
or W
rong
Mod
ifier
Inco
rrec
t CPT
(or C
ateg
ory)
Use
d
Inco
rrec
t IC
D-9
Cod
es
Inco
rrec
t Qua
ntity
Inad
equa
te D
ocum
enta
tion
Mis
sing
Doc
umen
tatio
n
Sign
atur
e Ill
egib
le (N
o Lo
g)
No
Sign
atur
e by
Pro
vide
r of
Ser
vice
COMMENTS (abbreviations used) PF- PROBLEM FOCUSED EPF- EXPANDED PF DET- DETAILED COMP- COMPREHENSIVE SFWD- STRAIGHT FORWARD MOD- MODERATE MDM- MEDICAL DECISION MAKING
Char
t Num
ber
SAMPLE SAMPLE S MD SAMPLE SAMPLE XXXXX XXX 112001 99212 25 1 1 1234 2 5678 3 4
$30000 $2200 99212 25 1 1 1234 2 5678 3 4
$56400 $54200 YES
DET
CO
MP
MO
D
COMMENTS COMMENTS COMMENTS
0
1 2 3 4
1 2 3 4
$000 0
$30000 $2200 $56400 $54200 10 10 10 10 10 10 10 10 10 10 10 10 TOTALS 917 Error Rate by Volume
Error Findings by Volume 8 CPT Coded Accurately 8 Overcoded 8 Undercoded 8 Missed CPTHCPCS Code 8 Missed or Wrong Modifier 8 Incorrect CPT (or Category) Used 8 Incorrect ICD-9 Codes 8 Incorrect Quantity
Inadequate Documentation 8 8 Missing Documentation 8 Signature Illegible (No Log) 8 No Signature by Provider of Service
1200 Total
Net Payment Error Rate -24636
Primary Payments Total $ Audited Payment Total $ (Total Under Payments)
Total Over Payments
Net OverUnder Payment $
2200 56400
(54200)
Resources Used HCPCS and CPT CodeBook (Current or applilcable year) ICD-10-CM CodeBook (Current or applicable year) CMS 1995 and 1997 EM Guidelines CMS Claims Processing Manual 100-04 Medicare Claims Processing (PUB 100-04) CMS - National Coverage Determinations (NCDs) National Correct Coding Policy Manual Applicable Physician Version
Executive Summary Report
The executive summary provides readers with a short complete document highlighting import information included in the detailed report Executive summaries are created for the senior management readers that donrsquot have time to read the full report and need to walk away with an understanding of the issues and corrective actions
Some would say the executive summary could be written before the detailed report however it is difficult to make sure the most important elements are included until you have spent time reviewing the detail If you want to make sure the most important messages are in the executive
summary this step should be completed after the detail is written As auditors become more seasoned this step could move to the front of the process
Executive Summary Report Structure of the ES Report
o Backgroundndash Specialtyndash Providersndash Sample Selection sizendash Date range of audit
o Audit Scopeo Regulatory Resourceso Type of Medical records reviewedo Overall Accuracy (all providers)o Detailed Audit Findings
ndash Business Impactndash Summary of Findings
o Department Findingso Summary
o ReportsStandard Executive Summary Professional Servicespdf
Department Findings Top Issues
Date ofServiceErrors
MissingDocuments
Missing orInvalid
Signature
TeachingPhysician
Errors
InsufficientConsultation
Documents
OverCoding
EMBundled
IntoGlobal
SurgicalPackage
SplitSharedServiceError
Incorrector
MissingPricing
Modifier
ICD-10Errors
Family Practice
CardiologyInternal Medicine
TOTALS
Top Findings by Provider
E amp M Accuracy Rates
ICD-10-CM Accuracy Rates
Procedure Accuracy Rates
Inpatient DRG Audit Report
TABLE OF CONTENTS
Executive Summaryo Scope of Work
Reimbursement Changes Department Results
o InpatientGeneral Recommendations and Comments
o Secondary DiagnosesoProcedure CodingoPresent on AdmissionoQueries
Scope of WorkCodingAID performed coding audit review of 175 inpatient records The review completed was a random sample that included cases coded by twenty coders for dates of service from May 2016 ndash July 2016
The objective was to determine if the medical record documentation supported the following coding and documentation requirements and any other regulatory requirement for that code set Criteria reviewed
1 ICD-10-CM Official Coding Guidelines for accurate diagnosis code reporting 2 ICD-10-PCS Official Coding Guidelines for accurate procedure code reporting 3 Documentation of procedure compared to the CPT code assigned 4 Identify opportunities for education and training 5 Financial impact of current coding practices
The regulatory agencies and reference materials relied upon include the following in addition to Medicare and Medicaid regulations Additional resources are located in the sub sections below
bull ICD-10-CM and ICD-10-PCS for Hospitals current volume bull Centers for Medicare and Medicaid Services CMS NCCI Edits-Centers for Medicaid and
Medicare Services CMS website wwwcmsgov bull AHA Coding Clinic
The following electronic medical record documents were reviewed and relied upon to compare to the actual codes submitted to the third party payer
bull Discharge summaries HampPs Progress Notes and other provider notes located in the EMR Records
bull Patient History Forms Ancillary Staff Notes bull Procedure Notes bull Orders bull Diagnostic Report
Reimbursement Changes
Coder Acct
Billed Audited
Reimbursement ChangesMS DRG SOI ROM Weight Expected
Payment MS DRG SOI ROM Weight Expected Payment
Coder 1 001 790 52300 $2615000 792 21552 $1077600 -$1537400
Coder 2002
749 26452 $1322600 758 10090 $504500 -$818100
Coder 3 003 669 13111 $655550 694 07294 $364700 -$290850
Coder 4 004 389 08707 $435350 394 09502 $475100 $39750
Coder 5 005 312 07630 $381500 812 08572 $428600 $47100
Coder 6 006 384 08481 $424050 378 09949 $497450 $73400
Coder 7 007 206 08164 $408200 794 12987 $649350 $241150
Coder 8008
344 31029 $1551450 853 51334 $2566700 $1015250
TOTAL $7793700 $6564000 -$1229700
General Recommendations and CommentsFinding Pertinent secondary diagnoses are not coded and diagnoses are code which are not supported in provider documentation Code only those diagnoses which are documented by the provider on the current chart Not all codes are coded to the highest degree of specificity and combination codes were sometimes missed
Recommendation It is important to assign codes for all conditions which meet the definition of a reportable diagnosis Documentation from all providers should be used including but not limited to radiologists pathologists anesthesiologists CRNAs and FNPs
Reference Coding Clinic Official Coding Guidelines
bull Report all secondary diagnoses which meet the definition of a secondary diagnosis which is defined as all conditions that coexist at the time of admission that develop subsequently or that affect the treatment received andor the length of stay Codes which enhance the overall picture of the patientrsquos visit should be added
o Add T45515A to report adverse effect of Coumadin which caused the GI bleed
o Add I2690 for septic pulmonary emboli (MCCSOI4ROM4)
o Add N179 for acute kidney failure (S3M2CC) per the nephrology consult and the 628 progress note
o Add code I429 cardiomyopathy per HampP
o Add B964 to report proteus in a UTI per the 620 hospitalist progress note
o Code for D649 anemia and I701 stenosis of renal artery should be added as secondary diagnoses per the HampP
bull Only report diagnoses which are substantiated by provider documentation in the current chart notes If a suspected condition is not verified at discharge on an inpatient account it cannot be coded
o Remove G4734 (idiopathic sleep related non-obstructive alveolar hypoventilation) as patient was noted to have the sleep study and the hypoventilation was shown to be a possibility but not noted as such on discharge
o Remove G629 (S21) the neuropathy is documented as due to diabetes
o Remove K529 colitis noted on HP as possible but not further noted or confirmed at discharge
Procedure CodingFinding Procedures were sometimes coded incorrectly
Recommendation The entire medical record should be reviewed and all procedures coded as documented Coding procedures incorrectly or assigning incorrect CPT codes may result in lost revenue
bull Incorrect root operation
o Revise principal procedure to 0DQ68ZZ for clipping of the ulcer per OP report clipping is root operation repair
bull Biopsy versus Excision
o Procedure 0DBA0ZX (biopsy of jejunum) should change to 0DBA0ZZ (excision of jejunum) per op note this was not a biopsy procedure
bull Coding Guideline error
o Remove 0RG10K0 for allograft due to being inclusive in principal procedure
o Remove codes for adhesiolysis 0DN80ZZ 0UN10ZZ and 0UN90ZZ due to no significance noted per OP report
bull Incorrect approach
o Revise 0TF63ZZ (fragmentation percutaneous approach) to 0TF68ZZ (fragmentation endoscopic) for procedure performed via scope per the operative report
bull Procedure coded without provider documentation
o Remove secondary procedure of excisional debridement (0JB90ZZ) due to lack of documentation of excisional debridement per operative report The header in the operative report documents IampD and debridement but the body of the operative report only documents an IampD
bull Incorrect CPT code assignment
o Post-op note supports the nerve block injections of four nerves therefore code 64421 (multiple nerve block) should replace 64420 (injection of one intercostal nerve)
Queries Finding Conflicting incomplete and vague documentation is found within provider chart notes
Recommendation Prior to code assignment if the coder finds ambiguous or conflicting documentation the provider should be queried
Reference AHA Coding Clinic 2002 2nd Quarter pages 17-18
bull Query for acute blood loss anemia since hgb has dropped and patient is being transfused PRBC
bull Recommend query to clarify if cardiorenal syndrome is current as it is documented per 627 nephrology consult but unclear if current
bull Documentation does not support SIRS noninfectious without organ failure It is conflicting since patient has respiratory failure Query should be initiated for clarification with or without organ failure or infectious or non-infectious Patient has pneumonia per query as well as last progress note therefore if SIRS is not further specified per query PNA should be sequenced as principal diagnosis and SIRS should be removed
bull Recommend provider query necrotizing lung consolidation noted on DS as principal diagnosis-unclear does the patient have lobar pneumonia Secondary dx states necrotic pneumonia which is coded as principal diagnosis-this diagnosis is clear but consolidation portion is unclear
bull Recommend query for preterm labor delivery at 301 weeks
bull RECOMMEND QUERY no chest pain on admit per ER and HP cardiology provider states no CP with ER stating chest pressure the day prior to admit Appears patient was admitted due to elevated troponins which cardiology says are likely due to hypotension and AKI DS states chest pain but also says bradycardia and hypotension were the reason for admit
bull RECOMMEND QUERY no chest pain on admit per ER and HP cardiology provider states no CP with ER stating chest pressure the day prior to admit Appears patient was admitted due to elevated troponins which cardiology says are likely due to hypotension and AKI DS states chest pain but also says bradycardia and hypotension were the reason for admit
bull Query the provider regarding pathology report notation of endometriosis andor possible re-sequence of stenosis as principal diagnosis as it also meets principal diagnosis guidelines This would result in an MS-DRG change to 742 and APR-DRG change to 513
bull QUERY secondary diagnosis MCC and ROM 4 code T3166 (60 TBSA of which 60 are third degree burns) Chart notes do not specify how much of TBSA was actually third degree If after query TBSA is found to be less than 50 (T3164) then ROM will change from 4 to 3 but no change to overall APR-DRG or weight
Auditor Quality amp Productivity
Audit Productivity Standards
It takes twice as long to audit a chart as it does to code it a statistic that takes into account the time to document an explanation of any coding decision the auditor is not in agreement with o For example in an emergency department audit with a productivity of 12
charts per hour for a coder our auditors would probably be able to review six per hour
o If there are multiple services to audit on each encounter the productivity may only be 4 per hour
o The amount of detail you put into your audit report will also be a factorndash Are you using an automated audit softwarendash Are you using a spreadsheet to auditndash How many Systems are needed to complete the audit
Coder Quality Audits
Quality Audits (QA) should be done on your coders and auditors regularly Frequent reviews with smaller sample size will allow more consistent
review and feedbacko Example 10 charts per month per coder if the coder passes 2-3 months
consecutively with 95 or better score move them to quarterly reviewso Some QA programs review a percentage of the coders work This
methodology requires more time and resources
Auditor QA should also score and comment on the accuracy of the audit comments and recommendations
Presenting the Audit Results
Presenting the Audit Results
Communicating the Audit FindingsoWho requested the AuditoWho are you reporting the finding to
ndash CEOndash CFOndash Physicianndash Revenue Cycle Managerndash HIM Directorndash Billing Managerndash Coding Manager
ReportsAudit Resultspptx
Post Audit Education
Provider Education
Provider Education is best received when it is specific to the provider(s) 11 sessions going over the audit result Look at their notes with them
oHighlight areas for documentation improvementoReinforce Coding Guidelines that are specific to themoAsk them to share how they establish their LOS for E amp M serviceso Integrate their EMR system into the training
Provider Education
Group Training SessionsoUse the audit results to identify common issues within a specialty group
ndash Refer to the Executive Summary reportoVery effective for identifying system issues
ndash Teaching Attestationsndash Templatesndash Copy and Pastendash Cloned notes
o Everyone hears the same messagesoAn Issue may not appear on the individual audit but is still a concern for the
group
Education Delivery
In person or remote sessionso Factors to consider
ndash Providers scheduleavailabilityndash Location(s)ndash Personality of the providerndash Budget
Coder Education
Coders do well in group training so they can learn from each other 11 training allows the coder to get feedback on their coding
Handling Audit Disputes
Handling Audit Disputes
Be open to all points of viewo Let the documentation tell the story
Refer to the guidelines Ask
oCan we defend the reported service with the current documentation
Self Disclosures Refunds and Corrected Billing
Overpayment
In general If a person has received an overpayment the person shallo report and return the overpayment to the Secretary the State an
intermediary a carrier or a contractor as appropriate at the correct address and ndash notify the Secretary State intermediary carrier or contractor to whom the overpayment was returned in writing of the reason for the overpayment
What is an ldquoOverpaymentrdquo ndash The term ldquooverpaymentrdquo means any funds that a person receives or retains under subchapter XVIII or XIX of this chapter to which the person after applicable reconciliation is not entitled under such subchapter
Self Disclosure
The Office of Inspector General (OIG) has several self-disclosure processes that can be used to report potential fraud in Department of Health and Human Services (HHS) programs Choose the one that applies to you from the following descriptions to learn moreo Health Care Provider Self-Disclosures
ndash Health care providers suppliers or other individuals or entities subject to Civil Monetary Penalties can use the Provider Self-Disclosure Protocol which was created in 1998 to voluntarily disclose self-discovered evidence of potential fraud Self-disclosure gives providers the opportunity to avoid the costs and disruptions associated with a Government-directed investigation and civil or administrative litigation Visit the Provider Self-Disclosure Protocol webpage for more information
o HHS Contractor Self-Disclosuresndash Contractors are individuals businesses or other legal entities that are awarded Government contracts or
subcontracts to provide services to the Department of Health and Human Services (HHS) OIGs contractor self-disclosure program enables contractors to self-disclose potential violations of the False Claims Act and various Federal criminal laws involving fraud conflict of interest bribery or gratuity This self-disclosure process is available for those entities with a Federal Acquisition Regulation-based contract Visit the Contractor Self-Disclosure webpage for more information
o HHS Grantee Self-Disclosuresndash HHS grantees or subrecipients may voluntarily disclose evidence of potential violations of Federal criminal law
involving fraud bribery or gratuity violations potentially affecting the Federal award 45 CFR 75113 notes mandatory disclosures of criminal offenses that non-Federal entities must make with respect to HHS grants Recipients submitting disclosures in connection with this requirement should include the subject reference line Mandatory Grant Disclosure Recipients choosing to disclose conduct that may not fit squarely within the scope of offenses described in 45 CFR 75113 should include the following subject reference line in the submission Voluntary Grant Disclosure
Medicare 60 day rule
The 60 Day Rule (Medicare Parts A amp B) o The 60 day time period for reportingreturning begins when either
ndash The reasonable diligence is completed orndash On the day the provider received credible information of a potential overpayment (if the
provider fails to conduct reasonable diligence) o For an investigation to be conducted in a ldquotimelyrdquo manner providers typically
must complete the investigation within 6 months from receipt of credible information indicating there may be an overpayment
ndash ndash 6-month timeframe may potentially be extended under ldquoextraordinary circumstancesrdquo ndash 8 months generally the maximum total time to return overpayments The government recommends that providers maintain records documenting ldquoreasonable diligencerdquo
Medicare 60 Day Rule
Six-year lookback period ndash Sometimes possible to use a shorter period depending on the facts at issue Amount to be repaid ndash May vary depending on the method used to
reportreturn eg Medicare administrative contractor (ldquoMACrdquo) v self-disclosure Overpayment notification ndash After receiving an overpayment
notification from the government you should investigate for related overpayments eg other time periods
Medicare 60 Day Rule
Self-disclosure protocols ndashoA submission to the OIG or CMS protocols suspends the 60 day requirement
for returning overpayments until a settlement agreement is executed ndash ndash OIGrsquos Self-Disclosure Protocol (SDP) ndash ndash CMS Voluntary Self-Referral Disclosure Protocol (SRDP) ndash
o Self-disclosures to other agencies do not suspend the repayment deadlinendash ndash Eg Department of Justice local US Attorneyrsquos Office Medicaid Fraud Control Unit
Medicare 60 Day Rule
Facilitating Compliance With the 60 Day Rule Compliance programs should include o ndash Appropriate policies and procedures o ndash Periodic billing and coding audits to proactively identify overpaymentso ndash Focus on high-risk areas o ndash Utilization of publicly available government resources to guide audit efforts o ndash Investigating any suspected incidents of non-compliance with federal health
care program requirements
Self Disclosure
Choice of AgencyoOIG ndash Self-Disclosure Protocol
ndash ndash Conduct involving false billingndash ndash Conduct involving excluded personsndash ndash Conduct involving the Anti-Kickback Statute (including conduct thatndash violates both the AKS and Stark Law)
oCMS ndash Self-Referral Disclosure Protocolndash ndash Conduct involving only violations of the Stark Law
oDOJndash ndash May be appropriate when provider believes a FCA release is necessary
Summary
The Cost of a Well-Executed Coding Audit ProcessThe costs associated with an auditing program are worth it in the long run Ideally your organization is performing audits on a regular basis across all service types locations and payers Weve all seen claims that have been denied resulting in additional work that may be preventable with a proper audit program The goal is to use the audit feedback to improve coding quality and lower potential risk and cost to the organization Organizations should be investing in an effective coding audit program to make your coders and providers better and enhance documentation improvement from the providers
Questions
Thank you for your attentionLynn Handy
Vice President of Coding amp Audit ServicesLynnhandymanagedresourcesinccom

Detailed Findings
135 822012 New Consultations - Office
Consultations Detailed Detailed (95) Moderate 99244 99243 1 $3500 N
Provider Code 99244 Reviewer Code 99243 Provider Diagnosis 1 3005 NEURASTHENIA Reviewer Diagnosis 1 3005 NEURASTHENIA Provider Diagnosis 2 7282 MUSC DISUSE ATROPHY NEC Reviewer Diagnosis 2 7282 MUSC DISUSE ATROPHY NEC
bull Assessment (I) The assessment is not clearly stated for this encounter Documentation Guidelines states The documentation for each patient encounter should include assessment clinical impression or diagnosis bull Assessment (R) The assessment should be clearly documented for each encounter Since each note must stand alone it is imperative to accurately document the most specific diagnosis in the assessment impression section of the note
bull Documented Lower Level (I) The documentation substantiates a lower level of service than charged
Chart Level Comments
Group your comments in categoriesoDocumentationo E amp MoProceduresoModifierso ICD-10-CM
oReportsAudit Manager Macros 061218 (version 1)xlsx
Recommendations and ReferencesCategory Short Description Long Description
EM AdmissionDischarge Same Day Review the CMS AdmissionDischarge same day coding guidelines httpswwwcmsgovRegulations-and-GuidanceGuidanceManualsDownloadsclm104c12pdf
EM ConsultationReview the consultation guidelines located in the CPT book
EM Consultation not billable to Medicare CMS no longer recognizes the consultation codeshttpswwwcmsgovOutreach-and-EducationMedicare-Learning-Network-MLNMLNMattersArticlesdownloadsmm6740pdf
EM Critical CareReview the CMS Critical Care guidelines httpswwwcmsgovOutreach-and-EducationMedicare-Learning-Network-MLNMLNMattersArticlesdownloadsmm5993pdf
EM Discharge ServicesReview the CMS Hospital Discharge Services guidelineshttpswwwcmsgovOutreach-and-EducationMedicare-Learning-Network-MLNMLNMattersArticlesdownloadsmm5794pdf
EMEM and Preventive Visit Review AAPC guidance for documenting and billing an EM and Preventive visit same day httpswwwaapccomblog22580-successfully-bill-a-
preventive-service-with-a-sick-visit
EM EM documentation guidelines Review the CMS 1995 amp 1997 EM documentation guidelineshttpswwwcmsgovOutreach-and-EducationMedicare-Learning-Network-MLNMLNEdWebGuideEMDOChtml
EM EM Inpatient vs Outpatient Review the patientrsquos status on the hospital admission order to determine the appropriate EM category to bill (inpatient vs observation)
EM EM New vs EstablishedReview the CMS New vs Established patient guidelines httpswwwcmsgovOutreach-and-EducationMedicare-Learning-Network-MLNMLNProductsDownloadseval-mgmt-serv-guide-ICN006764pdf
EMEM Time billing suggestion
Recommend a time statement is added to the EM medical record when a majority of the visit is spent counseling andor coordination of care Review the CMS 1995 amp 1997 EM documentation guidelines for EM time documentationhttpswwwcmsgovOutreach-and-EducationMedicare-Learning-Network-MLNMLNEdWebGuideEMDOChtml
EM Inpatient hospital servicesReview the CMS Hospital Services (Initial and Subsequent) guidelines httpswwwcmsgovRegulations-and-GuidanceGuidanceManualsDownloadsclm104c12pdf
EM Nursing Facility Services Review the Nursing Facility Services guidelines provided by CMS The guidelines can be downloaded at this linkhttpswwwcmsgovRegulations-and-GuidanceGuidanceManualsDownloadsclm104c12pdf
EM Observation Services Review the CMS Observation Services (Initial and Subsequent) guidelines httpswwwcmsgovRegulations-and-GuidanceGuidanceManualsDownloadsclm104c12pdf
EM Prolonged Services Review the CMS Prolonged Services guidelines httpswwwcmsgovOutreach-and-EducationMedicare-Learning-Network-MLNMLNMattersArticlesdownloadsmm5972pdf
EMReview of Systems Review the CMS 1995 amp 1997 EM documentation guidelines for Review of Systems requirements
httpswwwcmsgovOutreach-and-EducationMedicare-Learning-Network-MLNMLNEdWebGuideEMDOChtml
EMConsultation Documentation Suggestion
Recommend adding verbiage to consultation documentation that indicates the name of the referring provider and the reason for the consultation
Audit Report Examples Automated Solution
Letrsquos look at some report Examples
ReportsStandard Provider Audit SummarypdfReportsProvider Detailed Sample Reportdocx
ReportsProvider Audit Worksheets - Optionalpdf
Audit Report Examples Non Automated Solution
Error Findings by Volume Percentage
CPT Coded Accurately
8 8 Overcoded
8 8 Undercoded
Missed CPTHCPCS Code
Missed or Wrong Modifier
8 8 Incorrect CPT (or Category) Used
Incorrect ICD-9 Codes
8 8 Incorrect Quantity
Inadequate Documentation
Missing Documentation 8 8
Signature Illegible (No Log)
8 8
CLIENT NAME PROJECT TITLE
Review Line Item Detail Prepared Month Year
DRAFT
Client Claim Demographics Client Charge Data Review Result EampM ONLY Findings C C C C C C O OC O O O
Char
t Num
ber
Au
dit D
ate
Audi
tor (
initi
als)
QA
Initi
als
Fa
cilit
y Lo
catio
n Re
porte
d
Pr
ovid
er N
ame
Pa
tient
Nam
e
M
edic
al R
ecor
d Nu
mbe
r
Prim
ary
Carr
ier M
edica
re=
A M
edica
id =
B O
ther
=O
Da
te o
f Ser
vice
CP
T Co
de
Mod
ifier
(s) i
n or
der
Qua
ntity
Diag
nosi
s Co
de(s
) 1
thro
ugh
4
Fe
e ch
arge
d
Pr
imar
y Pa
ymen
t Am
ount
CPT
Code
Mod
ifier
(s) i
n or
der
Qua
ntity
Diag
nosi
s Co
de(s
) 1
thro
ugh
4
CO
RREC
T AL
LOW
ABLE
Prim
ary
PAYM
ENT
Va
rianc
e
Chie
f Com
plai
nt
Hist
ory
Leve
l Sup
port
ed
Exam
Lev
el S
uppo
rted
Med
ical
Dec
Mak
ing
Supp
orte
d (o
r TIM
E)
CPT
Cod
ed A
ccur
atel
y
Ove
rcod
ed
Und
erco
ded
Mis
sed
CPT
HC
PCS
Cod
e
Mis
sed
or W
rong
Mod
ifier
Inco
rrec
t CPT
(or C
ateg
ory)
Use
d
Inco
rrec
t IC
D-9
Cod
es
Inco
rrec
t Qua
ntity
Inad
equa
te D
ocum
enta
tion
Mis
sing
Doc
umen
tatio
n
Sign
atur
e Ill
egib
le (N
o Lo
g)
No
Sign
atur
e by
Pro
vide
r of
Ser
vice
COMMENTS (abbreviations used) PF- PROBLEM FOCUSED EPF- EXPANDED PF DET- DETAILED COMP- COMPREHENSIVE SFWD- STRAIGHT FORWARD MOD- MODERATE MDM- MEDICAL DECISION MAKING
Char
t Num
ber
SAMPLE SAMPLE S MD SAMPLE SAMPLE XXXXX XXX 112001 99212 25 1 1 1234 2 5678 3 4
$30000 $2200 99212 25 1 1 1234 2 5678 3 4
$56400 $54200 YES
DET
CO
MP
MO
D
COMMENTS COMMENTS COMMENTS
0
1 2 3 4
1 2 3 4
$000 0
$30000 $2200 $56400 $54200 10 10 10 10 10 10 10 10 10 10 10 10 TOTALS 917 Error Rate by Volume
Error Findings by Volume 8 CPT Coded Accurately 8 Overcoded 8 Undercoded 8 Missed CPTHCPCS Code 8 Missed or Wrong Modifier 8 Incorrect CPT (or Category) Used 8 Incorrect ICD-9 Codes 8 Incorrect Quantity
Inadequate Documentation 8 8 Missing Documentation 8 Signature Illegible (No Log) 8 No Signature by Provider of Service
1200 Total
Net Payment Error Rate -24636
Primary Payments Total $ Audited Payment Total $ (Total Under Payments)
Total Over Payments
Net OverUnder Payment $
2200 56400
(54200)
Resources Used HCPCS and CPT CodeBook (Current or applilcable year) ICD-10-CM CodeBook (Current or applicable year) CMS 1995 and 1997 EM Guidelines CMS Claims Processing Manual 100-04 Medicare Claims Processing (PUB 100-04) CMS - National Coverage Determinations (NCDs) National Correct Coding Policy Manual Applicable Physician Version
Executive Summary Report
The executive summary provides readers with a short complete document highlighting import information included in the detailed report Executive summaries are created for the senior management readers that donrsquot have time to read the full report and need to walk away with an understanding of the issues and corrective actions
Some would say the executive summary could be written before the detailed report however it is difficult to make sure the most important elements are included until you have spent time reviewing the detail If you want to make sure the most important messages are in the executive
summary this step should be completed after the detail is written As auditors become more seasoned this step could move to the front of the process
Executive Summary Report Structure of the ES Report
o Backgroundndash Specialtyndash Providersndash Sample Selection sizendash Date range of audit
o Audit Scopeo Regulatory Resourceso Type of Medical records reviewedo Overall Accuracy (all providers)o Detailed Audit Findings
ndash Business Impactndash Summary of Findings
o Department Findingso Summary
o ReportsStandard Executive Summary Professional Servicespdf
Department Findings Top Issues
Date ofServiceErrors
MissingDocuments
Missing orInvalid
Signature
TeachingPhysician
Errors
InsufficientConsultation
Documents
OverCoding
EMBundled
IntoGlobal
SurgicalPackage
SplitSharedServiceError
Incorrector
MissingPricing
Modifier
ICD-10Errors
Family Practice
CardiologyInternal Medicine
TOTALS
Top Findings by Provider
E amp M Accuracy Rates
ICD-10-CM Accuracy Rates
Procedure Accuracy Rates
Inpatient DRG Audit Report
TABLE OF CONTENTS
Executive Summaryo Scope of Work
Reimbursement Changes Department Results
o InpatientGeneral Recommendations and Comments
o Secondary DiagnosesoProcedure CodingoPresent on AdmissionoQueries
Scope of WorkCodingAID performed coding audit review of 175 inpatient records The review completed was a random sample that included cases coded by twenty coders for dates of service from May 2016 ndash July 2016
The objective was to determine if the medical record documentation supported the following coding and documentation requirements and any other regulatory requirement for that code set Criteria reviewed
1 ICD-10-CM Official Coding Guidelines for accurate diagnosis code reporting 2 ICD-10-PCS Official Coding Guidelines for accurate procedure code reporting 3 Documentation of procedure compared to the CPT code assigned 4 Identify opportunities for education and training 5 Financial impact of current coding practices
The regulatory agencies and reference materials relied upon include the following in addition to Medicare and Medicaid regulations Additional resources are located in the sub sections below
bull ICD-10-CM and ICD-10-PCS for Hospitals current volume bull Centers for Medicare and Medicaid Services CMS NCCI Edits-Centers for Medicaid and
Medicare Services CMS website wwwcmsgov bull AHA Coding Clinic
The following electronic medical record documents were reviewed and relied upon to compare to the actual codes submitted to the third party payer
bull Discharge summaries HampPs Progress Notes and other provider notes located in the EMR Records
bull Patient History Forms Ancillary Staff Notes bull Procedure Notes bull Orders bull Diagnostic Report
Reimbursement Changes
Coder Acct
Billed Audited
Reimbursement ChangesMS DRG SOI ROM Weight Expected
Payment MS DRG SOI ROM Weight Expected Payment
Coder 1 001 790 52300 $2615000 792 21552 $1077600 -$1537400
Coder 2002
749 26452 $1322600 758 10090 $504500 -$818100
Coder 3 003 669 13111 $655550 694 07294 $364700 -$290850
Coder 4 004 389 08707 $435350 394 09502 $475100 $39750
Coder 5 005 312 07630 $381500 812 08572 $428600 $47100
Coder 6 006 384 08481 $424050 378 09949 $497450 $73400
Coder 7 007 206 08164 $408200 794 12987 $649350 $241150
Coder 8008
344 31029 $1551450 853 51334 $2566700 $1015250
TOTAL $7793700 $6564000 -$1229700
General Recommendations and CommentsFinding Pertinent secondary diagnoses are not coded and diagnoses are code which are not supported in provider documentation Code only those diagnoses which are documented by the provider on the current chart Not all codes are coded to the highest degree of specificity and combination codes were sometimes missed
Recommendation It is important to assign codes for all conditions which meet the definition of a reportable diagnosis Documentation from all providers should be used including but not limited to radiologists pathologists anesthesiologists CRNAs and FNPs
Reference Coding Clinic Official Coding Guidelines
bull Report all secondary diagnoses which meet the definition of a secondary diagnosis which is defined as all conditions that coexist at the time of admission that develop subsequently or that affect the treatment received andor the length of stay Codes which enhance the overall picture of the patientrsquos visit should be added
o Add T45515A to report adverse effect of Coumadin which caused the GI bleed
o Add I2690 for septic pulmonary emboli (MCCSOI4ROM4)
o Add N179 for acute kidney failure (S3M2CC) per the nephrology consult and the 628 progress note
o Add code I429 cardiomyopathy per HampP
o Add B964 to report proteus in a UTI per the 620 hospitalist progress note
o Code for D649 anemia and I701 stenosis of renal artery should be added as secondary diagnoses per the HampP
bull Only report diagnoses which are substantiated by provider documentation in the current chart notes If a suspected condition is not verified at discharge on an inpatient account it cannot be coded
o Remove G4734 (idiopathic sleep related non-obstructive alveolar hypoventilation) as patient was noted to have the sleep study and the hypoventilation was shown to be a possibility but not noted as such on discharge
o Remove G629 (S21) the neuropathy is documented as due to diabetes
o Remove K529 colitis noted on HP as possible but not further noted or confirmed at discharge
Procedure CodingFinding Procedures were sometimes coded incorrectly
Recommendation The entire medical record should be reviewed and all procedures coded as documented Coding procedures incorrectly or assigning incorrect CPT codes may result in lost revenue
bull Incorrect root operation
o Revise principal procedure to 0DQ68ZZ for clipping of the ulcer per OP report clipping is root operation repair
bull Biopsy versus Excision
o Procedure 0DBA0ZX (biopsy of jejunum) should change to 0DBA0ZZ (excision of jejunum) per op note this was not a biopsy procedure
bull Coding Guideline error
o Remove 0RG10K0 for allograft due to being inclusive in principal procedure
o Remove codes for adhesiolysis 0DN80ZZ 0UN10ZZ and 0UN90ZZ due to no significance noted per OP report
bull Incorrect approach
o Revise 0TF63ZZ (fragmentation percutaneous approach) to 0TF68ZZ (fragmentation endoscopic) for procedure performed via scope per the operative report
bull Procedure coded without provider documentation
o Remove secondary procedure of excisional debridement (0JB90ZZ) due to lack of documentation of excisional debridement per operative report The header in the operative report documents IampD and debridement but the body of the operative report only documents an IampD
bull Incorrect CPT code assignment
o Post-op note supports the nerve block injections of four nerves therefore code 64421 (multiple nerve block) should replace 64420 (injection of one intercostal nerve)
Queries Finding Conflicting incomplete and vague documentation is found within provider chart notes
Recommendation Prior to code assignment if the coder finds ambiguous or conflicting documentation the provider should be queried
Reference AHA Coding Clinic 2002 2nd Quarter pages 17-18
bull Query for acute blood loss anemia since hgb has dropped and patient is being transfused PRBC
bull Recommend query to clarify if cardiorenal syndrome is current as it is documented per 627 nephrology consult but unclear if current
bull Documentation does not support SIRS noninfectious without organ failure It is conflicting since patient has respiratory failure Query should be initiated for clarification with or without organ failure or infectious or non-infectious Patient has pneumonia per query as well as last progress note therefore if SIRS is not further specified per query PNA should be sequenced as principal diagnosis and SIRS should be removed
bull Recommend provider query necrotizing lung consolidation noted on DS as principal diagnosis-unclear does the patient have lobar pneumonia Secondary dx states necrotic pneumonia which is coded as principal diagnosis-this diagnosis is clear but consolidation portion is unclear
bull Recommend query for preterm labor delivery at 301 weeks
bull RECOMMEND QUERY no chest pain on admit per ER and HP cardiology provider states no CP with ER stating chest pressure the day prior to admit Appears patient was admitted due to elevated troponins which cardiology says are likely due to hypotension and AKI DS states chest pain but also says bradycardia and hypotension were the reason for admit
bull RECOMMEND QUERY no chest pain on admit per ER and HP cardiology provider states no CP with ER stating chest pressure the day prior to admit Appears patient was admitted due to elevated troponins which cardiology says are likely due to hypotension and AKI DS states chest pain but also says bradycardia and hypotension were the reason for admit
bull Query the provider regarding pathology report notation of endometriosis andor possible re-sequence of stenosis as principal diagnosis as it also meets principal diagnosis guidelines This would result in an MS-DRG change to 742 and APR-DRG change to 513
bull QUERY secondary diagnosis MCC and ROM 4 code T3166 (60 TBSA of which 60 are third degree burns) Chart notes do not specify how much of TBSA was actually third degree If after query TBSA is found to be less than 50 (T3164) then ROM will change from 4 to 3 but no change to overall APR-DRG or weight
Auditor Quality amp Productivity
Audit Productivity Standards
It takes twice as long to audit a chart as it does to code it a statistic that takes into account the time to document an explanation of any coding decision the auditor is not in agreement with o For example in an emergency department audit with a productivity of 12
charts per hour for a coder our auditors would probably be able to review six per hour
o If there are multiple services to audit on each encounter the productivity may only be 4 per hour
o The amount of detail you put into your audit report will also be a factorndash Are you using an automated audit softwarendash Are you using a spreadsheet to auditndash How many Systems are needed to complete the audit
Coder Quality Audits
Quality Audits (QA) should be done on your coders and auditors regularly Frequent reviews with smaller sample size will allow more consistent
review and feedbacko Example 10 charts per month per coder if the coder passes 2-3 months
consecutively with 95 or better score move them to quarterly reviewso Some QA programs review a percentage of the coders work This
methodology requires more time and resources
Auditor QA should also score and comment on the accuracy of the audit comments and recommendations
Presenting the Audit Results
Presenting the Audit Results
Communicating the Audit FindingsoWho requested the AuditoWho are you reporting the finding to
ndash CEOndash CFOndash Physicianndash Revenue Cycle Managerndash HIM Directorndash Billing Managerndash Coding Manager
ReportsAudit Resultspptx
Post Audit Education
Provider Education
Provider Education is best received when it is specific to the provider(s) 11 sessions going over the audit result Look at their notes with them
oHighlight areas for documentation improvementoReinforce Coding Guidelines that are specific to themoAsk them to share how they establish their LOS for E amp M serviceso Integrate their EMR system into the training
Provider Education
Group Training SessionsoUse the audit results to identify common issues within a specialty group
ndash Refer to the Executive Summary reportoVery effective for identifying system issues
ndash Teaching Attestationsndash Templatesndash Copy and Pastendash Cloned notes
o Everyone hears the same messagesoAn Issue may not appear on the individual audit but is still a concern for the
group
Education Delivery
In person or remote sessionso Factors to consider
ndash Providers scheduleavailabilityndash Location(s)ndash Personality of the providerndash Budget
Coder Education
Coders do well in group training so they can learn from each other 11 training allows the coder to get feedback on their coding
Handling Audit Disputes
Handling Audit Disputes
Be open to all points of viewo Let the documentation tell the story
Refer to the guidelines Ask
oCan we defend the reported service with the current documentation
Self Disclosures Refunds and Corrected Billing
Overpayment
In general If a person has received an overpayment the person shallo report and return the overpayment to the Secretary the State an
intermediary a carrier or a contractor as appropriate at the correct address and ndash notify the Secretary State intermediary carrier or contractor to whom the overpayment was returned in writing of the reason for the overpayment
What is an ldquoOverpaymentrdquo ndash The term ldquooverpaymentrdquo means any funds that a person receives or retains under subchapter XVIII or XIX of this chapter to which the person after applicable reconciliation is not entitled under such subchapter
Self Disclosure
The Office of Inspector General (OIG) has several self-disclosure processes that can be used to report potential fraud in Department of Health and Human Services (HHS) programs Choose the one that applies to you from the following descriptions to learn moreo Health Care Provider Self-Disclosures
ndash Health care providers suppliers or other individuals or entities subject to Civil Monetary Penalties can use the Provider Self-Disclosure Protocol which was created in 1998 to voluntarily disclose self-discovered evidence of potential fraud Self-disclosure gives providers the opportunity to avoid the costs and disruptions associated with a Government-directed investigation and civil or administrative litigation Visit the Provider Self-Disclosure Protocol webpage for more information
o HHS Contractor Self-Disclosuresndash Contractors are individuals businesses or other legal entities that are awarded Government contracts or
subcontracts to provide services to the Department of Health and Human Services (HHS) OIGs contractor self-disclosure program enables contractors to self-disclose potential violations of the False Claims Act and various Federal criminal laws involving fraud conflict of interest bribery or gratuity This self-disclosure process is available for those entities with a Federal Acquisition Regulation-based contract Visit the Contractor Self-Disclosure webpage for more information
o HHS Grantee Self-Disclosuresndash HHS grantees or subrecipients may voluntarily disclose evidence of potential violations of Federal criminal law
involving fraud bribery or gratuity violations potentially affecting the Federal award 45 CFR 75113 notes mandatory disclosures of criminal offenses that non-Federal entities must make with respect to HHS grants Recipients submitting disclosures in connection with this requirement should include the subject reference line Mandatory Grant Disclosure Recipients choosing to disclose conduct that may not fit squarely within the scope of offenses described in 45 CFR 75113 should include the following subject reference line in the submission Voluntary Grant Disclosure
Medicare 60 day rule
The 60 Day Rule (Medicare Parts A amp B) o The 60 day time period for reportingreturning begins when either
ndash The reasonable diligence is completed orndash On the day the provider received credible information of a potential overpayment (if the
provider fails to conduct reasonable diligence) o For an investigation to be conducted in a ldquotimelyrdquo manner providers typically
must complete the investigation within 6 months from receipt of credible information indicating there may be an overpayment
ndash ndash 6-month timeframe may potentially be extended under ldquoextraordinary circumstancesrdquo ndash 8 months generally the maximum total time to return overpayments The government recommends that providers maintain records documenting ldquoreasonable diligencerdquo
Medicare 60 Day Rule
Six-year lookback period ndash Sometimes possible to use a shorter period depending on the facts at issue Amount to be repaid ndash May vary depending on the method used to
reportreturn eg Medicare administrative contractor (ldquoMACrdquo) v self-disclosure Overpayment notification ndash After receiving an overpayment
notification from the government you should investigate for related overpayments eg other time periods
Medicare 60 Day Rule
Self-disclosure protocols ndashoA submission to the OIG or CMS protocols suspends the 60 day requirement
for returning overpayments until a settlement agreement is executed ndash ndash OIGrsquos Self-Disclosure Protocol (SDP) ndash ndash CMS Voluntary Self-Referral Disclosure Protocol (SRDP) ndash
o Self-disclosures to other agencies do not suspend the repayment deadlinendash ndash Eg Department of Justice local US Attorneyrsquos Office Medicaid Fraud Control Unit
Medicare 60 Day Rule
Facilitating Compliance With the 60 Day Rule Compliance programs should include o ndash Appropriate policies and procedures o ndash Periodic billing and coding audits to proactively identify overpaymentso ndash Focus on high-risk areas o ndash Utilization of publicly available government resources to guide audit efforts o ndash Investigating any suspected incidents of non-compliance with federal health
care program requirements
Self Disclosure
Choice of AgencyoOIG ndash Self-Disclosure Protocol
ndash ndash Conduct involving false billingndash ndash Conduct involving excluded personsndash ndash Conduct involving the Anti-Kickback Statute (including conduct thatndash violates both the AKS and Stark Law)
oCMS ndash Self-Referral Disclosure Protocolndash ndash Conduct involving only violations of the Stark Law
oDOJndash ndash May be appropriate when provider believes a FCA release is necessary
Summary
The Cost of a Well-Executed Coding Audit ProcessThe costs associated with an auditing program are worth it in the long run Ideally your organization is performing audits on a regular basis across all service types locations and payers Weve all seen claims that have been denied resulting in additional work that may be preventable with a proper audit program The goal is to use the audit feedback to improve coding quality and lower potential risk and cost to the organization Organizations should be investing in an effective coding audit program to make your coders and providers better and enhance documentation improvement from the providers
Questions
Thank you for your attentionLynn Handy
Vice President of Coding amp Audit ServicesLynnhandymanagedresourcesinccom

Chart Level Comments
Group your comments in categoriesoDocumentationo E amp MoProceduresoModifierso ICD-10-CM
oReportsAudit Manager Macros 061218 (version 1)xlsx
Recommendations and ReferencesCategory Short Description Long Description
EM AdmissionDischarge Same Day Review the CMS AdmissionDischarge same day coding guidelines httpswwwcmsgovRegulations-and-GuidanceGuidanceManualsDownloadsclm104c12pdf
EM ConsultationReview the consultation guidelines located in the CPT book
EM Consultation not billable to Medicare CMS no longer recognizes the consultation codeshttpswwwcmsgovOutreach-and-EducationMedicare-Learning-Network-MLNMLNMattersArticlesdownloadsmm6740pdf
EM Critical CareReview the CMS Critical Care guidelines httpswwwcmsgovOutreach-and-EducationMedicare-Learning-Network-MLNMLNMattersArticlesdownloadsmm5993pdf
EM Discharge ServicesReview the CMS Hospital Discharge Services guidelineshttpswwwcmsgovOutreach-and-EducationMedicare-Learning-Network-MLNMLNMattersArticlesdownloadsmm5794pdf
EMEM and Preventive Visit Review AAPC guidance for documenting and billing an EM and Preventive visit same day httpswwwaapccomblog22580-successfully-bill-a-
preventive-service-with-a-sick-visit
EM EM documentation guidelines Review the CMS 1995 amp 1997 EM documentation guidelineshttpswwwcmsgovOutreach-and-EducationMedicare-Learning-Network-MLNMLNEdWebGuideEMDOChtml
EM EM Inpatient vs Outpatient Review the patientrsquos status on the hospital admission order to determine the appropriate EM category to bill (inpatient vs observation)
EM EM New vs EstablishedReview the CMS New vs Established patient guidelines httpswwwcmsgovOutreach-and-EducationMedicare-Learning-Network-MLNMLNProductsDownloadseval-mgmt-serv-guide-ICN006764pdf
EMEM Time billing suggestion
Recommend a time statement is added to the EM medical record when a majority of the visit is spent counseling andor coordination of care Review the CMS 1995 amp 1997 EM documentation guidelines for EM time documentationhttpswwwcmsgovOutreach-and-EducationMedicare-Learning-Network-MLNMLNEdWebGuideEMDOChtml
EM Inpatient hospital servicesReview the CMS Hospital Services (Initial and Subsequent) guidelines httpswwwcmsgovRegulations-and-GuidanceGuidanceManualsDownloadsclm104c12pdf
EM Nursing Facility Services Review the Nursing Facility Services guidelines provided by CMS The guidelines can be downloaded at this linkhttpswwwcmsgovRegulations-and-GuidanceGuidanceManualsDownloadsclm104c12pdf
EM Observation Services Review the CMS Observation Services (Initial and Subsequent) guidelines httpswwwcmsgovRegulations-and-GuidanceGuidanceManualsDownloadsclm104c12pdf
EM Prolonged Services Review the CMS Prolonged Services guidelines httpswwwcmsgovOutreach-and-EducationMedicare-Learning-Network-MLNMLNMattersArticlesdownloadsmm5972pdf
EMReview of Systems Review the CMS 1995 amp 1997 EM documentation guidelines for Review of Systems requirements
httpswwwcmsgovOutreach-and-EducationMedicare-Learning-Network-MLNMLNEdWebGuideEMDOChtml
EMConsultation Documentation Suggestion
Recommend adding verbiage to consultation documentation that indicates the name of the referring provider and the reason for the consultation
Audit Report Examples Automated Solution
Letrsquos look at some report Examples
ReportsStandard Provider Audit SummarypdfReportsProvider Detailed Sample Reportdocx
ReportsProvider Audit Worksheets - Optionalpdf
Audit Report Examples Non Automated Solution
Error Findings by Volume Percentage
CPT Coded Accurately
8 8 Overcoded
8 8 Undercoded
Missed CPTHCPCS Code
Missed or Wrong Modifier
8 8 Incorrect CPT (or Category) Used
Incorrect ICD-9 Codes
8 8 Incorrect Quantity
Inadequate Documentation
Missing Documentation 8 8
Signature Illegible (No Log)
8 8
CLIENT NAME PROJECT TITLE
Review Line Item Detail Prepared Month Year
DRAFT
Client Claim Demographics Client Charge Data Review Result EampM ONLY Findings C C C C C C O OC O O O
Char
t Num
ber
Au
dit D
ate
Audi
tor (
initi
als)
QA
Initi
als
Fa
cilit
y Lo
catio
n Re
porte
d
Pr
ovid
er N
ame
Pa
tient
Nam
e
M
edic
al R
ecor
d Nu
mbe
r
Prim
ary
Carr
ier M
edica
re=
A M
edica
id =
B O
ther
=O
Da
te o
f Ser
vice
CP
T Co
de
Mod
ifier
(s) i
n or
der
Qua
ntity
Diag
nosi
s Co
de(s
) 1
thro
ugh
4
Fe
e ch
arge
d
Pr
imar
y Pa
ymen
t Am
ount
CPT
Code
Mod
ifier
(s) i
n or
der
Qua
ntity
Diag
nosi
s Co
de(s
) 1
thro
ugh
4
CO
RREC
T AL
LOW
ABLE
Prim
ary
PAYM
ENT
Va
rianc
e
Chie
f Com
plai
nt
Hist
ory
Leve
l Sup
port
ed
Exam
Lev
el S
uppo
rted
Med
ical
Dec
Mak
ing
Supp
orte
d (o
r TIM
E)
CPT
Cod
ed A
ccur
atel
y
Ove
rcod
ed
Und
erco
ded
Mis
sed
CPT
HC
PCS
Cod
e
Mis
sed
or W
rong
Mod
ifier
Inco
rrec
t CPT
(or C
ateg
ory)
Use
d
Inco
rrec
t IC
D-9
Cod
es
Inco
rrec
t Qua
ntity
Inad
equa
te D
ocum
enta
tion
Mis
sing
Doc
umen
tatio
n
Sign
atur
e Ill
egib
le (N
o Lo
g)
No
Sign
atur
e by
Pro
vide
r of
Ser
vice
COMMENTS (abbreviations used) PF- PROBLEM FOCUSED EPF- EXPANDED PF DET- DETAILED COMP- COMPREHENSIVE SFWD- STRAIGHT FORWARD MOD- MODERATE MDM- MEDICAL DECISION MAKING
Char
t Num
ber
SAMPLE SAMPLE S MD SAMPLE SAMPLE XXXXX XXX 112001 99212 25 1 1 1234 2 5678 3 4
$30000 $2200 99212 25 1 1 1234 2 5678 3 4
$56400 $54200 YES
DET
CO
MP
MO
D
COMMENTS COMMENTS COMMENTS
0
1 2 3 4
1 2 3 4
$000 0
$30000 $2200 $56400 $54200 10 10 10 10 10 10 10 10 10 10 10 10 TOTALS 917 Error Rate by Volume
Error Findings by Volume 8 CPT Coded Accurately 8 Overcoded 8 Undercoded 8 Missed CPTHCPCS Code 8 Missed or Wrong Modifier 8 Incorrect CPT (or Category) Used 8 Incorrect ICD-9 Codes 8 Incorrect Quantity
Inadequate Documentation 8 8 Missing Documentation 8 Signature Illegible (No Log) 8 No Signature by Provider of Service
1200 Total
Net Payment Error Rate -24636
Primary Payments Total $ Audited Payment Total $ (Total Under Payments)
Total Over Payments
Net OverUnder Payment $
2200 56400
(54200)
Resources Used HCPCS and CPT CodeBook (Current or applilcable year) ICD-10-CM CodeBook (Current or applicable year) CMS 1995 and 1997 EM Guidelines CMS Claims Processing Manual 100-04 Medicare Claims Processing (PUB 100-04) CMS - National Coverage Determinations (NCDs) National Correct Coding Policy Manual Applicable Physician Version
Executive Summary Report
The executive summary provides readers with a short complete document highlighting import information included in the detailed report Executive summaries are created for the senior management readers that donrsquot have time to read the full report and need to walk away with an understanding of the issues and corrective actions
Some would say the executive summary could be written before the detailed report however it is difficult to make sure the most important elements are included until you have spent time reviewing the detail If you want to make sure the most important messages are in the executive
summary this step should be completed after the detail is written As auditors become more seasoned this step could move to the front of the process
Executive Summary Report Structure of the ES Report
o Backgroundndash Specialtyndash Providersndash Sample Selection sizendash Date range of audit
o Audit Scopeo Regulatory Resourceso Type of Medical records reviewedo Overall Accuracy (all providers)o Detailed Audit Findings
ndash Business Impactndash Summary of Findings
o Department Findingso Summary
o ReportsStandard Executive Summary Professional Servicespdf
Department Findings Top Issues
Date ofServiceErrors
MissingDocuments
Missing orInvalid
Signature
TeachingPhysician
Errors
InsufficientConsultation
Documents
OverCoding
EMBundled
IntoGlobal
SurgicalPackage
SplitSharedServiceError
Incorrector
MissingPricing
Modifier
ICD-10Errors
Family Practice
CardiologyInternal Medicine
TOTALS
Top Findings by Provider
E amp M Accuracy Rates
ICD-10-CM Accuracy Rates
Procedure Accuracy Rates
Inpatient DRG Audit Report
TABLE OF CONTENTS
Executive Summaryo Scope of Work
Reimbursement Changes Department Results
o InpatientGeneral Recommendations and Comments
o Secondary DiagnosesoProcedure CodingoPresent on AdmissionoQueries
Scope of WorkCodingAID performed coding audit review of 175 inpatient records The review completed was a random sample that included cases coded by twenty coders for dates of service from May 2016 ndash July 2016
The objective was to determine if the medical record documentation supported the following coding and documentation requirements and any other regulatory requirement for that code set Criteria reviewed
1 ICD-10-CM Official Coding Guidelines for accurate diagnosis code reporting 2 ICD-10-PCS Official Coding Guidelines for accurate procedure code reporting 3 Documentation of procedure compared to the CPT code assigned 4 Identify opportunities for education and training 5 Financial impact of current coding practices
The regulatory agencies and reference materials relied upon include the following in addition to Medicare and Medicaid regulations Additional resources are located in the sub sections below
bull ICD-10-CM and ICD-10-PCS for Hospitals current volume bull Centers for Medicare and Medicaid Services CMS NCCI Edits-Centers for Medicaid and
Medicare Services CMS website wwwcmsgov bull AHA Coding Clinic
The following electronic medical record documents were reviewed and relied upon to compare to the actual codes submitted to the third party payer
bull Discharge summaries HampPs Progress Notes and other provider notes located in the EMR Records
bull Patient History Forms Ancillary Staff Notes bull Procedure Notes bull Orders bull Diagnostic Report
Reimbursement Changes
Coder Acct
Billed Audited
Reimbursement ChangesMS DRG SOI ROM Weight Expected
Payment MS DRG SOI ROM Weight Expected Payment
Coder 1 001 790 52300 $2615000 792 21552 $1077600 -$1537400
Coder 2002
749 26452 $1322600 758 10090 $504500 -$818100
Coder 3 003 669 13111 $655550 694 07294 $364700 -$290850
Coder 4 004 389 08707 $435350 394 09502 $475100 $39750
Coder 5 005 312 07630 $381500 812 08572 $428600 $47100
Coder 6 006 384 08481 $424050 378 09949 $497450 $73400
Coder 7 007 206 08164 $408200 794 12987 $649350 $241150
Coder 8008
344 31029 $1551450 853 51334 $2566700 $1015250
TOTAL $7793700 $6564000 -$1229700
General Recommendations and CommentsFinding Pertinent secondary diagnoses are not coded and diagnoses are code which are not supported in provider documentation Code only those diagnoses which are documented by the provider on the current chart Not all codes are coded to the highest degree of specificity and combination codes were sometimes missed
Recommendation It is important to assign codes for all conditions which meet the definition of a reportable diagnosis Documentation from all providers should be used including but not limited to radiologists pathologists anesthesiologists CRNAs and FNPs
Reference Coding Clinic Official Coding Guidelines
bull Report all secondary diagnoses which meet the definition of a secondary diagnosis which is defined as all conditions that coexist at the time of admission that develop subsequently or that affect the treatment received andor the length of stay Codes which enhance the overall picture of the patientrsquos visit should be added
o Add T45515A to report adverse effect of Coumadin which caused the GI bleed
o Add I2690 for septic pulmonary emboli (MCCSOI4ROM4)
o Add N179 for acute kidney failure (S3M2CC) per the nephrology consult and the 628 progress note
o Add code I429 cardiomyopathy per HampP
o Add B964 to report proteus in a UTI per the 620 hospitalist progress note
o Code for D649 anemia and I701 stenosis of renal artery should be added as secondary diagnoses per the HampP
bull Only report diagnoses which are substantiated by provider documentation in the current chart notes If a suspected condition is not verified at discharge on an inpatient account it cannot be coded
o Remove G4734 (idiopathic sleep related non-obstructive alveolar hypoventilation) as patient was noted to have the sleep study and the hypoventilation was shown to be a possibility but not noted as such on discharge
o Remove G629 (S21) the neuropathy is documented as due to diabetes
o Remove K529 colitis noted on HP as possible but not further noted or confirmed at discharge
Procedure CodingFinding Procedures were sometimes coded incorrectly
Recommendation The entire medical record should be reviewed and all procedures coded as documented Coding procedures incorrectly or assigning incorrect CPT codes may result in lost revenue
bull Incorrect root operation
o Revise principal procedure to 0DQ68ZZ for clipping of the ulcer per OP report clipping is root operation repair
bull Biopsy versus Excision
o Procedure 0DBA0ZX (biopsy of jejunum) should change to 0DBA0ZZ (excision of jejunum) per op note this was not a biopsy procedure
bull Coding Guideline error
o Remove 0RG10K0 for allograft due to being inclusive in principal procedure
o Remove codes for adhesiolysis 0DN80ZZ 0UN10ZZ and 0UN90ZZ due to no significance noted per OP report
bull Incorrect approach
o Revise 0TF63ZZ (fragmentation percutaneous approach) to 0TF68ZZ (fragmentation endoscopic) for procedure performed via scope per the operative report
bull Procedure coded without provider documentation
o Remove secondary procedure of excisional debridement (0JB90ZZ) due to lack of documentation of excisional debridement per operative report The header in the operative report documents IampD and debridement but the body of the operative report only documents an IampD
bull Incorrect CPT code assignment
o Post-op note supports the nerve block injections of four nerves therefore code 64421 (multiple nerve block) should replace 64420 (injection of one intercostal nerve)
Queries Finding Conflicting incomplete and vague documentation is found within provider chart notes
Recommendation Prior to code assignment if the coder finds ambiguous or conflicting documentation the provider should be queried
Reference AHA Coding Clinic 2002 2nd Quarter pages 17-18
bull Query for acute blood loss anemia since hgb has dropped and patient is being transfused PRBC
bull Recommend query to clarify if cardiorenal syndrome is current as it is documented per 627 nephrology consult but unclear if current
bull Documentation does not support SIRS noninfectious without organ failure It is conflicting since patient has respiratory failure Query should be initiated for clarification with or without organ failure or infectious or non-infectious Patient has pneumonia per query as well as last progress note therefore if SIRS is not further specified per query PNA should be sequenced as principal diagnosis and SIRS should be removed
bull Recommend provider query necrotizing lung consolidation noted on DS as principal diagnosis-unclear does the patient have lobar pneumonia Secondary dx states necrotic pneumonia which is coded as principal diagnosis-this diagnosis is clear but consolidation portion is unclear
bull Recommend query for preterm labor delivery at 301 weeks
bull RECOMMEND QUERY no chest pain on admit per ER and HP cardiology provider states no CP with ER stating chest pressure the day prior to admit Appears patient was admitted due to elevated troponins which cardiology says are likely due to hypotension and AKI DS states chest pain but also says bradycardia and hypotension were the reason for admit
bull RECOMMEND QUERY no chest pain on admit per ER and HP cardiology provider states no CP with ER stating chest pressure the day prior to admit Appears patient was admitted due to elevated troponins which cardiology says are likely due to hypotension and AKI DS states chest pain but also says bradycardia and hypotension were the reason for admit
bull Query the provider regarding pathology report notation of endometriosis andor possible re-sequence of stenosis as principal diagnosis as it also meets principal diagnosis guidelines This would result in an MS-DRG change to 742 and APR-DRG change to 513
bull QUERY secondary diagnosis MCC and ROM 4 code T3166 (60 TBSA of which 60 are third degree burns) Chart notes do not specify how much of TBSA was actually third degree If after query TBSA is found to be less than 50 (T3164) then ROM will change from 4 to 3 but no change to overall APR-DRG or weight
Auditor Quality amp Productivity
Audit Productivity Standards
It takes twice as long to audit a chart as it does to code it a statistic that takes into account the time to document an explanation of any coding decision the auditor is not in agreement with o For example in an emergency department audit with a productivity of 12
charts per hour for a coder our auditors would probably be able to review six per hour
o If there are multiple services to audit on each encounter the productivity may only be 4 per hour
o The amount of detail you put into your audit report will also be a factorndash Are you using an automated audit softwarendash Are you using a spreadsheet to auditndash How many Systems are needed to complete the audit
Coder Quality Audits
Quality Audits (QA) should be done on your coders and auditors regularly Frequent reviews with smaller sample size will allow more consistent
review and feedbacko Example 10 charts per month per coder if the coder passes 2-3 months
consecutively with 95 or better score move them to quarterly reviewso Some QA programs review a percentage of the coders work This
methodology requires more time and resources
Auditor QA should also score and comment on the accuracy of the audit comments and recommendations
Presenting the Audit Results
Presenting the Audit Results
Communicating the Audit FindingsoWho requested the AuditoWho are you reporting the finding to
ndash CEOndash CFOndash Physicianndash Revenue Cycle Managerndash HIM Directorndash Billing Managerndash Coding Manager
ReportsAudit Resultspptx
Post Audit Education
Provider Education
Provider Education is best received when it is specific to the provider(s) 11 sessions going over the audit result Look at their notes with them
oHighlight areas for documentation improvementoReinforce Coding Guidelines that are specific to themoAsk them to share how they establish their LOS for E amp M serviceso Integrate their EMR system into the training
Provider Education
Group Training SessionsoUse the audit results to identify common issues within a specialty group
ndash Refer to the Executive Summary reportoVery effective for identifying system issues
ndash Teaching Attestationsndash Templatesndash Copy and Pastendash Cloned notes
o Everyone hears the same messagesoAn Issue may not appear on the individual audit but is still a concern for the
group
Education Delivery
In person or remote sessionso Factors to consider
ndash Providers scheduleavailabilityndash Location(s)ndash Personality of the providerndash Budget
Coder Education
Coders do well in group training so they can learn from each other 11 training allows the coder to get feedback on their coding
Handling Audit Disputes
Handling Audit Disputes
Be open to all points of viewo Let the documentation tell the story
Refer to the guidelines Ask
oCan we defend the reported service with the current documentation
Self Disclosures Refunds and Corrected Billing
Overpayment
In general If a person has received an overpayment the person shallo report and return the overpayment to the Secretary the State an
intermediary a carrier or a contractor as appropriate at the correct address and ndash notify the Secretary State intermediary carrier or contractor to whom the overpayment was returned in writing of the reason for the overpayment
What is an ldquoOverpaymentrdquo ndash The term ldquooverpaymentrdquo means any funds that a person receives or retains under subchapter XVIII or XIX of this chapter to which the person after applicable reconciliation is not entitled under such subchapter
Self Disclosure
The Office of Inspector General (OIG) has several self-disclosure processes that can be used to report potential fraud in Department of Health and Human Services (HHS) programs Choose the one that applies to you from the following descriptions to learn moreo Health Care Provider Self-Disclosures
ndash Health care providers suppliers or other individuals or entities subject to Civil Monetary Penalties can use the Provider Self-Disclosure Protocol which was created in 1998 to voluntarily disclose self-discovered evidence of potential fraud Self-disclosure gives providers the opportunity to avoid the costs and disruptions associated with a Government-directed investigation and civil or administrative litigation Visit the Provider Self-Disclosure Protocol webpage for more information
o HHS Contractor Self-Disclosuresndash Contractors are individuals businesses or other legal entities that are awarded Government contracts or
subcontracts to provide services to the Department of Health and Human Services (HHS) OIGs contractor self-disclosure program enables contractors to self-disclose potential violations of the False Claims Act and various Federal criminal laws involving fraud conflict of interest bribery or gratuity This self-disclosure process is available for those entities with a Federal Acquisition Regulation-based contract Visit the Contractor Self-Disclosure webpage for more information
o HHS Grantee Self-Disclosuresndash HHS grantees or subrecipients may voluntarily disclose evidence of potential violations of Federal criminal law
involving fraud bribery or gratuity violations potentially affecting the Federal award 45 CFR 75113 notes mandatory disclosures of criminal offenses that non-Federal entities must make with respect to HHS grants Recipients submitting disclosures in connection with this requirement should include the subject reference line Mandatory Grant Disclosure Recipients choosing to disclose conduct that may not fit squarely within the scope of offenses described in 45 CFR 75113 should include the following subject reference line in the submission Voluntary Grant Disclosure
Medicare 60 day rule
The 60 Day Rule (Medicare Parts A amp B) o The 60 day time period for reportingreturning begins when either
ndash The reasonable diligence is completed orndash On the day the provider received credible information of a potential overpayment (if the
provider fails to conduct reasonable diligence) o For an investigation to be conducted in a ldquotimelyrdquo manner providers typically
must complete the investigation within 6 months from receipt of credible information indicating there may be an overpayment
ndash ndash 6-month timeframe may potentially be extended under ldquoextraordinary circumstancesrdquo ndash 8 months generally the maximum total time to return overpayments The government recommends that providers maintain records documenting ldquoreasonable diligencerdquo
Medicare 60 Day Rule
Six-year lookback period ndash Sometimes possible to use a shorter period depending on the facts at issue Amount to be repaid ndash May vary depending on the method used to
reportreturn eg Medicare administrative contractor (ldquoMACrdquo) v self-disclosure Overpayment notification ndash After receiving an overpayment
notification from the government you should investigate for related overpayments eg other time periods
Medicare 60 Day Rule
Self-disclosure protocols ndashoA submission to the OIG or CMS protocols suspends the 60 day requirement
for returning overpayments until a settlement agreement is executed ndash ndash OIGrsquos Self-Disclosure Protocol (SDP) ndash ndash CMS Voluntary Self-Referral Disclosure Protocol (SRDP) ndash
o Self-disclosures to other agencies do not suspend the repayment deadlinendash ndash Eg Department of Justice local US Attorneyrsquos Office Medicaid Fraud Control Unit
Medicare 60 Day Rule
Facilitating Compliance With the 60 Day Rule Compliance programs should include o ndash Appropriate policies and procedures o ndash Periodic billing and coding audits to proactively identify overpaymentso ndash Focus on high-risk areas o ndash Utilization of publicly available government resources to guide audit efforts o ndash Investigating any suspected incidents of non-compliance with federal health
care program requirements
Self Disclosure
Choice of AgencyoOIG ndash Self-Disclosure Protocol
ndash ndash Conduct involving false billingndash ndash Conduct involving excluded personsndash ndash Conduct involving the Anti-Kickback Statute (including conduct thatndash violates both the AKS and Stark Law)
oCMS ndash Self-Referral Disclosure Protocolndash ndash Conduct involving only violations of the Stark Law
oDOJndash ndash May be appropriate when provider believes a FCA release is necessary
Summary
The Cost of a Well-Executed Coding Audit ProcessThe costs associated with an auditing program are worth it in the long run Ideally your organization is performing audits on a regular basis across all service types locations and payers Weve all seen claims that have been denied resulting in additional work that may be preventable with a proper audit program The goal is to use the audit feedback to improve coding quality and lower potential risk and cost to the organization Organizations should be investing in an effective coding audit program to make your coders and providers better and enhance documentation improvement from the providers
Questions
Thank you for your attentionLynn Handy
Vice President of Coding amp Audit ServicesLynnhandymanagedresourcesinccom

Recommendations and ReferencesCategory Short Description Long Description
EM AdmissionDischarge Same Day Review the CMS AdmissionDischarge same day coding guidelines httpswwwcmsgovRegulations-and-GuidanceGuidanceManualsDownloadsclm104c12pdf
EM ConsultationReview the consultation guidelines located in the CPT book
EM Consultation not billable to Medicare CMS no longer recognizes the consultation codeshttpswwwcmsgovOutreach-and-EducationMedicare-Learning-Network-MLNMLNMattersArticlesdownloadsmm6740pdf
EM Critical CareReview the CMS Critical Care guidelines httpswwwcmsgovOutreach-and-EducationMedicare-Learning-Network-MLNMLNMattersArticlesdownloadsmm5993pdf
EM Discharge ServicesReview the CMS Hospital Discharge Services guidelineshttpswwwcmsgovOutreach-and-EducationMedicare-Learning-Network-MLNMLNMattersArticlesdownloadsmm5794pdf
EMEM and Preventive Visit Review AAPC guidance for documenting and billing an EM and Preventive visit same day httpswwwaapccomblog22580-successfully-bill-a-
preventive-service-with-a-sick-visit
EM EM documentation guidelines Review the CMS 1995 amp 1997 EM documentation guidelineshttpswwwcmsgovOutreach-and-EducationMedicare-Learning-Network-MLNMLNEdWebGuideEMDOChtml
EM EM Inpatient vs Outpatient Review the patientrsquos status on the hospital admission order to determine the appropriate EM category to bill (inpatient vs observation)
EM EM New vs EstablishedReview the CMS New vs Established patient guidelines httpswwwcmsgovOutreach-and-EducationMedicare-Learning-Network-MLNMLNProductsDownloadseval-mgmt-serv-guide-ICN006764pdf
EMEM Time billing suggestion
Recommend a time statement is added to the EM medical record when a majority of the visit is spent counseling andor coordination of care Review the CMS 1995 amp 1997 EM documentation guidelines for EM time documentationhttpswwwcmsgovOutreach-and-EducationMedicare-Learning-Network-MLNMLNEdWebGuideEMDOChtml
EM Inpatient hospital servicesReview the CMS Hospital Services (Initial and Subsequent) guidelines httpswwwcmsgovRegulations-and-GuidanceGuidanceManualsDownloadsclm104c12pdf
EM Nursing Facility Services Review the Nursing Facility Services guidelines provided by CMS The guidelines can be downloaded at this linkhttpswwwcmsgovRegulations-and-GuidanceGuidanceManualsDownloadsclm104c12pdf
EM Observation Services Review the CMS Observation Services (Initial and Subsequent) guidelines httpswwwcmsgovRegulations-and-GuidanceGuidanceManualsDownloadsclm104c12pdf
EM Prolonged Services Review the CMS Prolonged Services guidelines httpswwwcmsgovOutreach-and-EducationMedicare-Learning-Network-MLNMLNMattersArticlesdownloadsmm5972pdf
EMReview of Systems Review the CMS 1995 amp 1997 EM documentation guidelines for Review of Systems requirements
httpswwwcmsgovOutreach-and-EducationMedicare-Learning-Network-MLNMLNEdWebGuideEMDOChtml
EMConsultation Documentation Suggestion
Recommend adding verbiage to consultation documentation that indicates the name of the referring provider and the reason for the consultation
Audit Report Examples Automated Solution
Letrsquos look at some report Examples
ReportsStandard Provider Audit SummarypdfReportsProvider Detailed Sample Reportdocx
ReportsProvider Audit Worksheets - Optionalpdf
Audit Report Examples Non Automated Solution
Error Findings by Volume Percentage
CPT Coded Accurately
8 8 Overcoded
8 8 Undercoded
Missed CPTHCPCS Code
Missed or Wrong Modifier
8 8 Incorrect CPT (or Category) Used
Incorrect ICD-9 Codes
8 8 Incorrect Quantity
Inadequate Documentation
Missing Documentation 8 8
Signature Illegible (No Log)
8 8
CLIENT NAME PROJECT TITLE
Review Line Item Detail Prepared Month Year
DRAFT
Client Claim Demographics Client Charge Data Review Result EampM ONLY Findings C C C C C C O OC O O O
Char
t Num
ber
Au
dit D
ate
Audi
tor (
initi
als)
QA
Initi
als
Fa
cilit
y Lo
catio
n Re
porte
d
Pr
ovid
er N
ame
Pa
tient
Nam
e
M
edic
al R
ecor
d Nu
mbe
r
Prim
ary
Carr
ier M
edica
re=
A M
edica
id =
B O
ther
=O
Da
te o
f Ser
vice
CP
T Co
de
Mod
ifier
(s) i
n or
der
Qua
ntity
Diag
nosi
s Co
de(s
) 1
thro
ugh
4
Fe
e ch
arge
d
Pr
imar
y Pa
ymen
t Am
ount
CPT
Code
Mod
ifier
(s) i
n or
der
Qua
ntity
Diag
nosi
s Co
de(s
) 1
thro
ugh
4
CO
RREC
T AL
LOW
ABLE
Prim
ary
PAYM
ENT
Va
rianc
e
Chie
f Com
plai
nt
Hist
ory
Leve
l Sup
port
ed
Exam
Lev
el S
uppo
rted
Med
ical
Dec
Mak
ing
Supp
orte
d (o
r TIM
E)
CPT
Cod
ed A
ccur
atel
y
Ove
rcod
ed
Und
erco
ded
Mis
sed
CPT
HC
PCS
Cod
e
Mis
sed
or W
rong
Mod
ifier
Inco
rrec
t CPT
(or C
ateg
ory)
Use
d
Inco
rrec
t IC
D-9
Cod
es
Inco
rrec
t Qua
ntity
Inad
equa
te D
ocum
enta
tion
Mis
sing
Doc
umen
tatio
n
Sign
atur
e Ill
egib
le (N
o Lo
g)
No
Sign
atur
e by
Pro
vide
r of
Ser
vice
COMMENTS (abbreviations used) PF- PROBLEM FOCUSED EPF- EXPANDED PF DET- DETAILED COMP- COMPREHENSIVE SFWD- STRAIGHT FORWARD MOD- MODERATE MDM- MEDICAL DECISION MAKING
Char
t Num
ber
SAMPLE SAMPLE S MD SAMPLE SAMPLE XXXXX XXX 112001 99212 25 1 1 1234 2 5678 3 4
$30000 $2200 99212 25 1 1 1234 2 5678 3 4
$56400 $54200 YES
DET
CO
MP
MO
D
COMMENTS COMMENTS COMMENTS
0
1 2 3 4
1 2 3 4
$000 0
$30000 $2200 $56400 $54200 10 10 10 10 10 10 10 10 10 10 10 10 TOTALS 917 Error Rate by Volume
Error Findings by Volume 8 CPT Coded Accurately 8 Overcoded 8 Undercoded 8 Missed CPTHCPCS Code 8 Missed or Wrong Modifier 8 Incorrect CPT (or Category) Used 8 Incorrect ICD-9 Codes 8 Incorrect Quantity
Inadequate Documentation 8 8 Missing Documentation 8 Signature Illegible (No Log) 8 No Signature by Provider of Service
1200 Total
Net Payment Error Rate -24636
Primary Payments Total $ Audited Payment Total $ (Total Under Payments)
Total Over Payments
Net OverUnder Payment $
2200 56400
(54200)
Resources Used HCPCS and CPT CodeBook (Current or applilcable year) ICD-10-CM CodeBook (Current or applicable year) CMS 1995 and 1997 EM Guidelines CMS Claims Processing Manual 100-04 Medicare Claims Processing (PUB 100-04) CMS - National Coverage Determinations (NCDs) National Correct Coding Policy Manual Applicable Physician Version
Executive Summary Report
The executive summary provides readers with a short complete document highlighting import information included in the detailed report Executive summaries are created for the senior management readers that donrsquot have time to read the full report and need to walk away with an understanding of the issues and corrective actions
Some would say the executive summary could be written before the detailed report however it is difficult to make sure the most important elements are included until you have spent time reviewing the detail If you want to make sure the most important messages are in the executive
summary this step should be completed after the detail is written As auditors become more seasoned this step could move to the front of the process
Executive Summary Report Structure of the ES Report
o Backgroundndash Specialtyndash Providersndash Sample Selection sizendash Date range of audit
o Audit Scopeo Regulatory Resourceso Type of Medical records reviewedo Overall Accuracy (all providers)o Detailed Audit Findings
ndash Business Impactndash Summary of Findings
o Department Findingso Summary
o ReportsStandard Executive Summary Professional Servicespdf
Department Findings Top Issues
Date ofServiceErrors
MissingDocuments
Missing orInvalid
Signature
TeachingPhysician
Errors
InsufficientConsultation
Documents
OverCoding
EMBundled
IntoGlobal
SurgicalPackage
SplitSharedServiceError
Incorrector
MissingPricing
Modifier
ICD-10Errors
Family Practice
CardiologyInternal Medicine
TOTALS
Top Findings by Provider
E amp M Accuracy Rates
ICD-10-CM Accuracy Rates
Procedure Accuracy Rates
Inpatient DRG Audit Report
TABLE OF CONTENTS
Executive Summaryo Scope of Work
Reimbursement Changes Department Results
o InpatientGeneral Recommendations and Comments
o Secondary DiagnosesoProcedure CodingoPresent on AdmissionoQueries
Scope of WorkCodingAID performed coding audit review of 175 inpatient records The review completed was a random sample that included cases coded by twenty coders for dates of service from May 2016 ndash July 2016
The objective was to determine if the medical record documentation supported the following coding and documentation requirements and any other regulatory requirement for that code set Criteria reviewed
1 ICD-10-CM Official Coding Guidelines for accurate diagnosis code reporting 2 ICD-10-PCS Official Coding Guidelines for accurate procedure code reporting 3 Documentation of procedure compared to the CPT code assigned 4 Identify opportunities for education and training 5 Financial impact of current coding practices
The regulatory agencies and reference materials relied upon include the following in addition to Medicare and Medicaid regulations Additional resources are located in the sub sections below
bull ICD-10-CM and ICD-10-PCS for Hospitals current volume bull Centers for Medicare and Medicaid Services CMS NCCI Edits-Centers for Medicaid and
Medicare Services CMS website wwwcmsgov bull AHA Coding Clinic
The following electronic medical record documents were reviewed and relied upon to compare to the actual codes submitted to the third party payer
bull Discharge summaries HampPs Progress Notes and other provider notes located in the EMR Records
bull Patient History Forms Ancillary Staff Notes bull Procedure Notes bull Orders bull Diagnostic Report
Reimbursement Changes
Coder Acct
Billed Audited
Reimbursement ChangesMS DRG SOI ROM Weight Expected
Payment MS DRG SOI ROM Weight Expected Payment
Coder 1 001 790 52300 $2615000 792 21552 $1077600 -$1537400
Coder 2002
749 26452 $1322600 758 10090 $504500 -$818100
Coder 3 003 669 13111 $655550 694 07294 $364700 -$290850
Coder 4 004 389 08707 $435350 394 09502 $475100 $39750
Coder 5 005 312 07630 $381500 812 08572 $428600 $47100
Coder 6 006 384 08481 $424050 378 09949 $497450 $73400
Coder 7 007 206 08164 $408200 794 12987 $649350 $241150
Coder 8008
344 31029 $1551450 853 51334 $2566700 $1015250
TOTAL $7793700 $6564000 -$1229700
General Recommendations and CommentsFinding Pertinent secondary diagnoses are not coded and diagnoses are code which are not supported in provider documentation Code only those diagnoses which are documented by the provider on the current chart Not all codes are coded to the highest degree of specificity and combination codes were sometimes missed
Recommendation It is important to assign codes for all conditions which meet the definition of a reportable diagnosis Documentation from all providers should be used including but not limited to radiologists pathologists anesthesiologists CRNAs and FNPs
Reference Coding Clinic Official Coding Guidelines
bull Report all secondary diagnoses which meet the definition of a secondary diagnosis which is defined as all conditions that coexist at the time of admission that develop subsequently or that affect the treatment received andor the length of stay Codes which enhance the overall picture of the patientrsquos visit should be added
o Add T45515A to report adverse effect of Coumadin which caused the GI bleed
o Add I2690 for septic pulmonary emboli (MCCSOI4ROM4)
o Add N179 for acute kidney failure (S3M2CC) per the nephrology consult and the 628 progress note
o Add code I429 cardiomyopathy per HampP
o Add B964 to report proteus in a UTI per the 620 hospitalist progress note
o Code for D649 anemia and I701 stenosis of renal artery should be added as secondary diagnoses per the HampP
bull Only report diagnoses which are substantiated by provider documentation in the current chart notes If a suspected condition is not verified at discharge on an inpatient account it cannot be coded
o Remove G4734 (idiopathic sleep related non-obstructive alveolar hypoventilation) as patient was noted to have the sleep study and the hypoventilation was shown to be a possibility but not noted as such on discharge
o Remove G629 (S21) the neuropathy is documented as due to diabetes
o Remove K529 colitis noted on HP as possible but not further noted or confirmed at discharge
Procedure CodingFinding Procedures were sometimes coded incorrectly
Recommendation The entire medical record should be reviewed and all procedures coded as documented Coding procedures incorrectly or assigning incorrect CPT codes may result in lost revenue
bull Incorrect root operation
o Revise principal procedure to 0DQ68ZZ for clipping of the ulcer per OP report clipping is root operation repair
bull Biopsy versus Excision
o Procedure 0DBA0ZX (biopsy of jejunum) should change to 0DBA0ZZ (excision of jejunum) per op note this was not a biopsy procedure
bull Coding Guideline error
o Remove 0RG10K0 for allograft due to being inclusive in principal procedure
o Remove codes for adhesiolysis 0DN80ZZ 0UN10ZZ and 0UN90ZZ due to no significance noted per OP report
bull Incorrect approach
o Revise 0TF63ZZ (fragmentation percutaneous approach) to 0TF68ZZ (fragmentation endoscopic) for procedure performed via scope per the operative report
bull Procedure coded without provider documentation
o Remove secondary procedure of excisional debridement (0JB90ZZ) due to lack of documentation of excisional debridement per operative report The header in the operative report documents IampD and debridement but the body of the operative report only documents an IampD
bull Incorrect CPT code assignment
o Post-op note supports the nerve block injections of four nerves therefore code 64421 (multiple nerve block) should replace 64420 (injection of one intercostal nerve)
Queries Finding Conflicting incomplete and vague documentation is found within provider chart notes
Recommendation Prior to code assignment if the coder finds ambiguous or conflicting documentation the provider should be queried
Reference AHA Coding Clinic 2002 2nd Quarter pages 17-18
bull Query for acute blood loss anemia since hgb has dropped and patient is being transfused PRBC
bull Recommend query to clarify if cardiorenal syndrome is current as it is documented per 627 nephrology consult but unclear if current
bull Documentation does not support SIRS noninfectious without organ failure It is conflicting since patient has respiratory failure Query should be initiated for clarification with or without organ failure or infectious or non-infectious Patient has pneumonia per query as well as last progress note therefore if SIRS is not further specified per query PNA should be sequenced as principal diagnosis and SIRS should be removed
bull Recommend provider query necrotizing lung consolidation noted on DS as principal diagnosis-unclear does the patient have lobar pneumonia Secondary dx states necrotic pneumonia which is coded as principal diagnosis-this diagnosis is clear but consolidation portion is unclear
bull Recommend query for preterm labor delivery at 301 weeks
bull RECOMMEND QUERY no chest pain on admit per ER and HP cardiology provider states no CP with ER stating chest pressure the day prior to admit Appears patient was admitted due to elevated troponins which cardiology says are likely due to hypotension and AKI DS states chest pain but also says bradycardia and hypotension were the reason for admit
bull RECOMMEND QUERY no chest pain on admit per ER and HP cardiology provider states no CP with ER stating chest pressure the day prior to admit Appears patient was admitted due to elevated troponins which cardiology says are likely due to hypotension and AKI DS states chest pain but also says bradycardia and hypotension were the reason for admit
bull Query the provider regarding pathology report notation of endometriosis andor possible re-sequence of stenosis as principal diagnosis as it also meets principal diagnosis guidelines This would result in an MS-DRG change to 742 and APR-DRG change to 513
bull QUERY secondary diagnosis MCC and ROM 4 code T3166 (60 TBSA of which 60 are third degree burns) Chart notes do not specify how much of TBSA was actually third degree If after query TBSA is found to be less than 50 (T3164) then ROM will change from 4 to 3 but no change to overall APR-DRG or weight
Auditor Quality amp Productivity
Audit Productivity Standards
It takes twice as long to audit a chart as it does to code it a statistic that takes into account the time to document an explanation of any coding decision the auditor is not in agreement with o For example in an emergency department audit with a productivity of 12
charts per hour for a coder our auditors would probably be able to review six per hour
o If there are multiple services to audit on each encounter the productivity may only be 4 per hour
o The amount of detail you put into your audit report will also be a factorndash Are you using an automated audit softwarendash Are you using a spreadsheet to auditndash How many Systems are needed to complete the audit
Coder Quality Audits
Quality Audits (QA) should be done on your coders and auditors regularly Frequent reviews with smaller sample size will allow more consistent
review and feedbacko Example 10 charts per month per coder if the coder passes 2-3 months
consecutively with 95 or better score move them to quarterly reviewso Some QA programs review a percentage of the coders work This
methodology requires more time and resources
Auditor QA should also score and comment on the accuracy of the audit comments and recommendations
Presenting the Audit Results
Presenting the Audit Results
Communicating the Audit FindingsoWho requested the AuditoWho are you reporting the finding to
ndash CEOndash CFOndash Physicianndash Revenue Cycle Managerndash HIM Directorndash Billing Managerndash Coding Manager
ReportsAudit Resultspptx
Post Audit Education
Provider Education
Provider Education is best received when it is specific to the provider(s) 11 sessions going over the audit result Look at their notes with them
oHighlight areas for documentation improvementoReinforce Coding Guidelines that are specific to themoAsk them to share how they establish their LOS for E amp M serviceso Integrate their EMR system into the training
Provider Education
Group Training SessionsoUse the audit results to identify common issues within a specialty group
ndash Refer to the Executive Summary reportoVery effective for identifying system issues
ndash Teaching Attestationsndash Templatesndash Copy and Pastendash Cloned notes
o Everyone hears the same messagesoAn Issue may not appear on the individual audit but is still a concern for the
group
Education Delivery
In person or remote sessionso Factors to consider
ndash Providers scheduleavailabilityndash Location(s)ndash Personality of the providerndash Budget
Coder Education
Coders do well in group training so they can learn from each other 11 training allows the coder to get feedback on their coding
Handling Audit Disputes
Handling Audit Disputes
Be open to all points of viewo Let the documentation tell the story
Refer to the guidelines Ask
oCan we defend the reported service with the current documentation
Self Disclosures Refunds and Corrected Billing
Overpayment
In general If a person has received an overpayment the person shallo report and return the overpayment to the Secretary the State an
intermediary a carrier or a contractor as appropriate at the correct address and ndash notify the Secretary State intermediary carrier or contractor to whom the overpayment was returned in writing of the reason for the overpayment
What is an ldquoOverpaymentrdquo ndash The term ldquooverpaymentrdquo means any funds that a person receives or retains under subchapter XVIII or XIX of this chapter to which the person after applicable reconciliation is not entitled under such subchapter
Self Disclosure
The Office of Inspector General (OIG) has several self-disclosure processes that can be used to report potential fraud in Department of Health and Human Services (HHS) programs Choose the one that applies to you from the following descriptions to learn moreo Health Care Provider Self-Disclosures
ndash Health care providers suppliers or other individuals or entities subject to Civil Monetary Penalties can use the Provider Self-Disclosure Protocol which was created in 1998 to voluntarily disclose self-discovered evidence of potential fraud Self-disclosure gives providers the opportunity to avoid the costs and disruptions associated with a Government-directed investigation and civil or administrative litigation Visit the Provider Self-Disclosure Protocol webpage for more information
o HHS Contractor Self-Disclosuresndash Contractors are individuals businesses or other legal entities that are awarded Government contracts or
subcontracts to provide services to the Department of Health and Human Services (HHS) OIGs contractor self-disclosure program enables contractors to self-disclose potential violations of the False Claims Act and various Federal criminal laws involving fraud conflict of interest bribery or gratuity This self-disclosure process is available for those entities with a Federal Acquisition Regulation-based contract Visit the Contractor Self-Disclosure webpage for more information
o HHS Grantee Self-Disclosuresndash HHS grantees or subrecipients may voluntarily disclose evidence of potential violations of Federal criminal law
involving fraud bribery or gratuity violations potentially affecting the Federal award 45 CFR 75113 notes mandatory disclosures of criminal offenses that non-Federal entities must make with respect to HHS grants Recipients submitting disclosures in connection with this requirement should include the subject reference line Mandatory Grant Disclosure Recipients choosing to disclose conduct that may not fit squarely within the scope of offenses described in 45 CFR 75113 should include the following subject reference line in the submission Voluntary Grant Disclosure
Medicare 60 day rule
The 60 Day Rule (Medicare Parts A amp B) o The 60 day time period for reportingreturning begins when either
ndash The reasonable diligence is completed orndash On the day the provider received credible information of a potential overpayment (if the
provider fails to conduct reasonable diligence) o For an investigation to be conducted in a ldquotimelyrdquo manner providers typically
must complete the investigation within 6 months from receipt of credible information indicating there may be an overpayment
ndash ndash 6-month timeframe may potentially be extended under ldquoextraordinary circumstancesrdquo ndash 8 months generally the maximum total time to return overpayments The government recommends that providers maintain records documenting ldquoreasonable diligencerdquo
Medicare 60 Day Rule
Six-year lookback period ndash Sometimes possible to use a shorter period depending on the facts at issue Amount to be repaid ndash May vary depending on the method used to
reportreturn eg Medicare administrative contractor (ldquoMACrdquo) v self-disclosure Overpayment notification ndash After receiving an overpayment
notification from the government you should investigate for related overpayments eg other time periods
Medicare 60 Day Rule
Self-disclosure protocols ndashoA submission to the OIG or CMS protocols suspends the 60 day requirement
for returning overpayments until a settlement agreement is executed ndash ndash OIGrsquos Self-Disclosure Protocol (SDP) ndash ndash CMS Voluntary Self-Referral Disclosure Protocol (SRDP) ndash
o Self-disclosures to other agencies do not suspend the repayment deadlinendash ndash Eg Department of Justice local US Attorneyrsquos Office Medicaid Fraud Control Unit
Medicare 60 Day Rule
Facilitating Compliance With the 60 Day Rule Compliance programs should include o ndash Appropriate policies and procedures o ndash Periodic billing and coding audits to proactively identify overpaymentso ndash Focus on high-risk areas o ndash Utilization of publicly available government resources to guide audit efforts o ndash Investigating any suspected incidents of non-compliance with federal health
care program requirements
Self Disclosure
Choice of AgencyoOIG ndash Self-Disclosure Protocol
ndash ndash Conduct involving false billingndash ndash Conduct involving excluded personsndash ndash Conduct involving the Anti-Kickback Statute (including conduct thatndash violates both the AKS and Stark Law)
oCMS ndash Self-Referral Disclosure Protocolndash ndash Conduct involving only violations of the Stark Law
oDOJndash ndash May be appropriate when provider believes a FCA release is necessary
Summary
The Cost of a Well-Executed Coding Audit ProcessThe costs associated with an auditing program are worth it in the long run Ideally your organization is performing audits on a regular basis across all service types locations and payers Weve all seen claims that have been denied resulting in additional work that may be preventable with a proper audit program The goal is to use the audit feedback to improve coding quality and lower potential risk and cost to the organization Organizations should be investing in an effective coding audit program to make your coders and providers better and enhance documentation improvement from the providers
Questions
Thank you for your attentionLynn Handy
Vice President of Coding amp Audit ServicesLynnhandymanagedresourcesinccom

Audit Report Examples Automated Solution
Letrsquos look at some report Examples
ReportsStandard Provider Audit SummarypdfReportsProvider Detailed Sample Reportdocx
ReportsProvider Audit Worksheets - Optionalpdf
Audit Report Examples Non Automated Solution
Error Findings by Volume Percentage
CPT Coded Accurately
8 8 Overcoded
8 8 Undercoded
Missed CPTHCPCS Code
Missed or Wrong Modifier
8 8 Incorrect CPT (or Category) Used
Incorrect ICD-9 Codes
8 8 Incorrect Quantity
Inadequate Documentation
Missing Documentation 8 8
Signature Illegible (No Log)
8 8
CLIENT NAME PROJECT TITLE
Review Line Item Detail Prepared Month Year
DRAFT
Client Claim Demographics Client Charge Data Review Result EampM ONLY Findings C C C C C C O OC O O O
Char
t Num
ber
Au
dit D
ate
Audi
tor (
initi
als)
QA
Initi
als
Fa
cilit
y Lo
catio
n Re
porte
d
Pr
ovid
er N
ame
Pa
tient
Nam
e
M
edic
al R
ecor
d Nu
mbe
r
Prim
ary
Carr
ier M
edica
re=
A M
edica
id =
B O
ther
=O
Da
te o
f Ser
vice
CP
T Co
de
Mod
ifier
(s) i
n or
der
Qua
ntity
Diag
nosi
s Co
de(s
) 1
thro
ugh
4
Fe
e ch
arge
d
Pr
imar
y Pa
ymen
t Am
ount
CPT
Code
Mod
ifier
(s) i
n or
der
Qua
ntity
Diag
nosi
s Co
de(s
) 1
thro
ugh
4
CO
RREC
T AL
LOW
ABLE
Prim
ary
PAYM
ENT
Va
rianc
e
Chie
f Com
plai
nt
Hist
ory
Leve
l Sup
port
ed
Exam
Lev
el S
uppo
rted
Med
ical
Dec
Mak
ing
Supp
orte
d (o
r TIM
E)
CPT
Cod
ed A
ccur
atel
y
Ove
rcod
ed
Und
erco
ded
Mis
sed
CPT
HC
PCS
Cod
e
Mis
sed
or W
rong
Mod
ifier
Inco
rrec
t CPT
(or C
ateg
ory)
Use
d
Inco
rrec
t IC
D-9
Cod
es
Inco
rrec
t Qua
ntity
Inad
equa
te D
ocum
enta
tion
Mis
sing
Doc
umen
tatio
n
Sign
atur
e Ill
egib
le (N
o Lo
g)
No
Sign
atur
e by
Pro
vide
r of
Ser
vice
COMMENTS (abbreviations used) PF- PROBLEM FOCUSED EPF- EXPANDED PF DET- DETAILED COMP- COMPREHENSIVE SFWD- STRAIGHT FORWARD MOD- MODERATE MDM- MEDICAL DECISION MAKING
Char
t Num
ber
SAMPLE SAMPLE S MD SAMPLE SAMPLE XXXXX XXX 112001 99212 25 1 1 1234 2 5678 3 4
$30000 $2200 99212 25 1 1 1234 2 5678 3 4
$56400 $54200 YES
DET
CO
MP
MO
D
COMMENTS COMMENTS COMMENTS
0
1 2 3 4
1 2 3 4
$000 0
$30000 $2200 $56400 $54200 10 10 10 10 10 10 10 10 10 10 10 10 TOTALS 917 Error Rate by Volume
Error Findings by Volume 8 CPT Coded Accurately 8 Overcoded 8 Undercoded 8 Missed CPTHCPCS Code 8 Missed or Wrong Modifier 8 Incorrect CPT (or Category) Used 8 Incorrect ICD-9 Codes 8 Incorrect Quantity
Inadequate Documentation 8 8 Missing Documentation 8 Signature Illegible (No Log) 8 No Signature by Provider of Service
1200 Total
Net Payment Error Rate -24636
Primary Payments Total $ Audited Payment Total $ (Total Under Payments)
Total Over Payments
Net OverUnder Payment $
2200 56400
(54200)
Resources Used HCPCS and CPT CodeBook (Current or applilcable year) ICD-10-CM CodeBook (Current or applicable year) CMS 1995 and 1997 EM Guidelines CMS Claims Processing Manual 100-04 Medicare Claims Processing (PUB 100-04) CMS - National Coverage Determinations (NCDs) National Correct Coding Policy Manual Applicable Physician Version
Executive Summary Report
The executive summary provides readers with a short complete document highlighting import information included in the detailed report Executive summaries are created for the senior management readers that donrsquot have time to read the full report and need to walk away with an understanding of the issues and corrective actions
Some would say the executive summary could be written before the detailed report however it is difficult to make sure the most important elements are included until you have spent time reviewing the detail If you want to make sure the most important messages are in the executive
summary this step should be completed after the detail is written As auditors become more seasoned this step could move to the front of the process
Executive Summary Report Structure of the ES Report
o Backgroundndash Specialtyndash Providersndash Sample Selection sizendash Date range of audit
o Audit Scopeo Regulatory Resourceso Type of Medical records reviewedo Overall Accuracy (all providers)o Detailed Audit Findings
ndash Business Impactndash Summary of Findings
o Department Findingso Summary
o ReportsStandard Executive Summary Professional Servicespdf
Department Findings Top Issues
Date ofServiceErrors
MissingDocuments
Missing orInvalid
Signature
TeachingPhysician
Errors
InsufficientConsultation
Documents
OverCoding
EMBundled
IntoGlobal
SurgicalPackage
SplitSharedServiceError
Incorrector
MissingPricing
Modifier
ICD-10Errors
Family Practice
CardiologyInternal Medicine
TOTALS
Top Findings by Provider
E amp M Accuracy Rates
ICD-10-CM Accuracy Rates
Procedure Accuracy Rates
Inpatient DRG Audit Report
TABLE OF CONTENTS
Executive Summaryo Scope of Work
Reimbursement Changes Department Results
o InpatientGeneral Recommendations and Comments
o Secondary DiagnosesoProcedure CodingoPresent on AdmissionoQueries
Scope of WorkCodingAID performed coding audit review of 175 inpatient records The review completed was a random sample that included cases coded by twenty coders for dates of service from May 2016 ndash July 2016
The objective was to determine if the medical record documentation supported the following coding and documentation requirements and any other regulatory requirement for that code set Criteria reviewed
1 ICD-10-CM Official Coding Guidelines for accurate diagnosis code reporting 2 ICD-10-PCS Official Coding Guidelines for accurate procedure code reporting 3 Documentation of procedure compared to the CPT code assigned 4 Identify opportunities for education and training 5 Financial impact of current coding practices
The regulatory agencies and reference materials relied upon include the following in addition to Medicare and Medicaid regulations Additional resources are located in the sub sections below
bull ICD-10-CM and ICD-10-PCS for Hospitals current volume bull Centers for Medicare and Medicaid Services CMS NCCI Edits-Centers for Medicaid and
Medicare Services CMS website wwwcmsgov bull AHA Coding Clinic
The following electronic medical record documents were reviewed and relied upon to compare to the actual codes submitted to the third party payer
bull Discharge summaries HampPs Progress Notes and other provider notes located in the EMR Records
bull Patient History Forms Ancillary Staff Notes bull Procedure Notes bull Orders bull Diagnostic Report
Reimbursement Changes
Coder Acct
Billed Audited
Reimbursement ChangesMS DRG SOI ROM Weight Expected
Payment MS DRG SOI ROM Weight Expected Payment
Coder 1 001 790 52300 $2615000 792 21552 $1077600 -$1537400
Coder 2002
749 26452 $1322600 758 10090 $504500 -$818100
Coder 3 003 669 13111 $655550 694 07294 $364700 -$290850
Coder 4 004 389 08707 $435350 394 09502 $475100 $39750
Coder 5 005 312 07630 $381500 812 08572 $428600 $47100
Coder 6 006 384 08481 $424050 378 09949 $497450 $73400
Coder 7 007 206 08164 $408200 794 12987 $649350 $241150
Coder 8008
344 31029 $1551450 853 51334 $2566700 $1015250
TOTAL $7793700 $6564000 -$1229700
General Recommendations and CommentsFinding Pertinent secondary diagnoses are not coded and diagnoses are code which are not supported in provider documentation Code only those diagnoses which are documented by the provider on the current chart Not all codes are coded to the highest degree of specificity and combination codes were sometimes missed
Recommendation It is important to assign codes for all conditions which meet the definition of a reportable diagnosis Documentation from all providers should be used including but not limited to radiologists pathologists anesthesiologists CRNAs and FNPs
Reference Coding Clinic Official Coding Guidelines
bull Report all secondary diagnoses which meet the definition of a secondary diagnosis which is defined as all conditions that coexist at the time of admission that develop subsequently or that affect the treatment received andor the length of stay Codes which enhance the overall picture of the patientrsquos visit should be added
o Add T45515A to report adverse effect of Coumadin which caused the GI bleed
o Add I2690 for septic pulmonary emboli (MCCSOI4ROM4)
o Add N179 for acute kidney failure (S3M2CC) per the nephrology consult and the 628 progress note
o Add code I429 cardiomyopathy per HampP
o Add B964 to report proteus in a UTI per the 620 hospitalist progress note
o Code for D649 anemia and I701 stenosis of renal artery should be added as secondary diagnoses per the HampP
bull Only report diagnoses which are substantiated by provider documentation in the current chart notes If a suspected condition is not verified at discharge on an inpatient account it cannot be coded
o Remove G4734 (idiopathic sleep related non-obstructive alveolar hypoventilation) as patient was noted to have the sleep study and the hypoventilation was shown to be a possibility but not noted as such on discharge
o Remove G629 (S21) the neuropathy is documented as due to diabetes
o Remove K529 colitis noted on HP as possible but not further noted or confirmed at discharge
Procedure CodingFinding Procedures were sometimes coded incorrectly
Recommendation The entire medical record should be reviewed and all procedures coded as documented Coding procedures incorrectly or assigning incorrect CPT codes may result in lost revenue
bull Incorrect root operation
o Revise principal procedure to 0DQ68ZZ for clipping of the ulcer per OP report clipping is root operation repair
bull Biopsy versus Excision
o Procedure 0DBA0ZX (biopsy of jejunum) should change to 0DBA0ZZ (excision of jejunum) per op note this was not a biopsy procedure
bull Coding Guideline error
o Remove 0RG10K0 for allograft due to being inclusive in principal procedure
o Remove codes for adhesiolysis 0DN80ZZ 0UN10ZZ and 0UN90ZZ due to no significance noted per OP report
bull Incorrect approach
o Revise 0TF63ZZ (fragmentation percutaneous approach) to 0TF68ZZ (fragmentation endoscopic) for procedure performed via scope per the operative report
bull Procedure coded without provider documentation
o Remove secondary procedure of excisional debridement (0JB90ZZ) due to lack of documentation of excisional debridement per operative report The header in the operative report documents IampD and debridement but the body of the operative report only documents an IampD
bull Incorrect CPT code assignment
o Post-op note supports the nerve block injections of four nerves therefore code 64421 (multiple nerve block) should replace 64420 (injection of one intercostal nerve)
Queries Finding Conflicting incomplete and vague documentation is found within provider chart notes
Recommendation Prior to code assignment if the coder finds ambiguous or conflicting documentation the provider should be queried
Reference AHA Coding Clinic 2002 2nd Quarter pages 17-18
bull Query for acute blood loss anemia since hgb has dropped and patient is being transfused PRBC
bull Recommend query to clarify if cardiorenal syndrome is current as it is documented per 627 nephrology consult but unclear if current
bull Documentation does not support SIRS noninfectious without organ failure It is conflicting since patient has respiratory failure Query should be initiated for clarification with or without organ failure or infectious or non-infectious Patient has pneumonia per query as well as last progress note therefore if SIRS is not further specified per query PNA should be sequenced as principal diagnosis and SIRS should be removed
bull Recommend provider query necrotizing lung consolidation noted on DS as principal diagnosis-unclear does the patient have lobar pneumonia Secondary dx states necrotic pneumonia which is coded as principal diagnosis-this diagnosis is clear but consolidation portion is unclear
bull Recommend query for preterm labor delivery at 301 weeks
bull RECOMMEND QUERY no chest pain on admit per ER and HP cardiology provider states no CP with ER stating chest pressure the day prior to admit Appears patient was admitted due to elevated troponins which cardiology says are likely due to hypotension and AKI DS states chest pain but also says bradycardia and hypotension were the reason for admit
bull RECOMMEND QUERY no chest pain on admit per ER and HP cardiology provider states no CP with ER stating chest pressure the day prior to admit Appears patient was admitted due to elevated troponins which cardiology says are likely due to hypotension and AKI DS states chest pain but also says bradycardia and hypotension were the reason for admit
bull Query the provider regarding pathology report notation of endometriosis andor possible re-sequence of stenosis as principal diagnosis as it also meets principal diagnosis guidelines This would result in an MS-DRG change to 742 and APR-DRG change to 513
bull QUERY secondary diagnosis MCC and ROM 4 code T3166 (60 TBSA of which 60 are third degree burns) Chart notes do not specify how much of TBSA was actually third degree If after query TBSA is found to be less than 50 (T3164) then ROM will change from 4 to 3 but no change to overall APR-DRG or weight
Auditor Quality amp Productivity
Audit Productivity Standards
It takes twice as long to audit a chart as it does to code it a statistic that takes into account the time to document an explanation of any coding decision the auditor is not in agreement with o For example in an emergency department audit with a productivity of 12
charts per hour for a coder our auditors would probably be able to review six per hour
o If there are multiple services to audit on each encounter the productivity may only be 4 per hour
o The amount of detail you put into your audit report will also be a factorndash Are you using an automated audit softwarendash Are you using a spreadsheet to auditndash How many Systems are needed to complete the audit
Coder Quality Audits
Quality Audits (QA) should be done on your coders and auditors regularly Frequent reviews with smaller sample size will allow more consistent
review and feedbacko Example 10 charts per month per coder if the coder passes 2-3 months
consecutively with 95 or better score move them to quarterly reviewso Some QA programs review a percentage of the coders work This
methodology requires more time and resources
Auditor QA should also score and comment on the accuracy of the audit comments and recommendations
Presenting the Audit Results
Presenting the Audit Results
Communicating the Audit FindingsoWho requested the AuditoWho are you reporting the finding to
ndash CEOndash CFOndash Physicianndash Revenue Cycle Managerndash HIM Directorndash Billing Managerndash Coding Manager
ReportsAudit Resultspptx
Post Audit Education
Provider Education
Provider Education is best received when it is specific to the provider(s) 11 sessions going over the audit result Look at their notes with them
oHighlight areas for documentation improvementoReinforce Coding Guidelines that are specific to themoAsk them to share how they establish their LOS for E amp M serviceso Integrate their EMR system into the training
Provider Education
Group Training SessionsoUse the audit results to identify common issues within a specialty group
ndash Refer to the Executive Summary reportoVery effective for identifying system issues
ndash Teaching Attestationsndash Templatesndash Copy and Pastendash Cloned notes
o Everyone hears the same messagesoAn Issue may not appear on the individual audit but is still a concern for the
group
Education Delivery
In person or remote sessionso Factors to consider
ndash Providers scheduleavailabilityndash Location(s)ndash Personality of the providerndash Budget
Coder Education
Coders do well in group training so they can learn from each other 11 training allows the coder to get feedback on their coding
Handling Audit Disputes
Handling Audit Disputes
Be open to all points of viewo Let the documentation tell the story
Refer to the guidelines Ask
oCan we defend the reported service with the current documentation
Self Disclosures Refunds and Corrected Billing
Overpayment
In general If a person has received an overpayment the person shallo report and return the overpayment to the Secretary the State an
intermediary a carrier or a contractor as appropriate at the correct address and ndash notify the Secretary State intermediary carrier or contractor to whom the overpayment was returned in writing of the reason for the overpayment
What is an ldquoOverpaymentrdquo ndash The term ldquooverpaymentrdquo means any funds that a person receives or retains under subchapter XVIII or XIX of this chapter to which the person after applicable reconciliation is not entitled under such subchapter
Self Disclosure
The Office of Inspector General (OIG) has several self-disclosure processes that can be used to report potential fraud in Department of Health and Human Services (HHS) programs Choose the one that applies to you from the following descriptions to learn moreo Health Care Provider Self-Disclosures
ndash Health care providers suppliers or other individuals or entities subject to Civil Monetary Penalties can use the Provider Self-Disclosure Protocol which was created in 1998 to voluntarily disclose self-discovered evidence of potential fraud Self-disclosure gives providers the opportunity to avoid the costs and disruptions associated with a Government-directed investigation and civil or administrative litigation Visit the Provider Self-Disclosure Protocol webpage for more information
o HHS Contractor Self-Disclosuresndash Contractors are individuals businesses or other legal entities that are awarded Government contracts or
subcontracts to provide services to the Department of Health and Human Services (HHS) OIGs contractor self-disclosure program enables contractors to self-disclose potential violations of the False Claims Act and various Federal criminal laws involving fraud conflict of interest bribery or gratuity This self-disclosure process is available for those entities with a Federal Acquisition Regulation-based contract Visit the Contractor Self-Disclosure webpage for more information
o HHS Grantee Self-Disclosuresndash HHS grantees or subrecipients may voluntarily disclose evidence of potential violations of Federal criminal law
involving fraud bribery or gratuity violations potentially affecting the Federal award 45 CFR 75113 notes mandatory disclosures of criminal offenses that non-Federal entities must make with respect to HHS grants Recipients submitting disclosures in connection with this requirement should include the subject reference line Mandatory Grant Disclosure Recipients choosing to disclose conduct that may not fit squarely within the scope of offenses described in 45 CFR 75113 should include the following subject reference line in the submission Voluntary Grant Disclosure
Medicare 60 day rule
The 60 Day Rule (Medicare Parts A amp B) o The 60 day time period for reportingreturning begins when either
ndash The reasonable diligence is completed orndash On the day the provider received credible information of a potential overpayment (if the
provider fails to conduct reasonable diligence) o For an investigation to be conducted in a ldquotimelyrdquo manner providers typically
must complete the investigation within 6 months from receipt of credible information indicating there may be an overpayment
ndash ndash 6-month timeframe may potentially be extended under ldquoextraordinary circumstancesrdquo ndash 8 months generally the maximum total time to return overpayments The government recommends that providers maintain records documenting ldquoreasonable diligencerdquo
Medicare 60 Day Rule
Six-year lookback period ndash Sometimes possible to use a shorter period depending on the facts at issue Amount to be repaid ndash May vary depending on the method used to
reportreturn eg Medicare administrative contractor (ldquoMACrdquo) v self-disclosure Overpayment notification ndash After receiving an overpayment
notification from the government you should investigate for related overpayments eg other time periods
Medicare 60 Day Rule
Self-disclosure protocols ndashoA submission to the OIG or CMS protocols suspends the 60 day requirement
for returning overpayments until a settlement agreement is executed ndash ndash OIGrsquos Self-Disclosure Protocol (SDP) ndash ndash CMS Voluntary Self-Referral Disclosure Protocol (SRDP) ndash
o Self-disclosures to other agencies do not suspend the repayment deadlinendash ndash Eg Department of Justice local US Attorneyrsquos Office Medicaid Fraud Control Unit
Medicare 60 Day Rule
Facilitating Compliance With the 60 Day Rule Compliance programs should include o ndash Appropriate policies and procedures o ndash Periodic billing and coding audits to proactively identify overpaymentso ndash Focus on high-risk areas o ndash Utilization of publicly available government resources to guide audit efforts o ndash Investigating any suspected incidents of non-compliance with federal health
care program requirements
Self Disclosure
Choice of AgencyoOIG ndash Self-Disclosure Protocol
ndash ndash Conduct involving false billingndash ndash Conduct involving excluded personsndash ndash Conduct involving the Anti-Kickback Statute (including conduct thatndash violates both the AKS and Stark Law)
oCMS ndash Self-Referral Disclosure Protocolndash ndash Conduct involving only violations of the Stark Law
oDOJndash ndash May be appropriate when provider believes a FCA release is necessary
Summary
The Cost of a Well-Executed Coding Audit ProcessThe costs associated with an auditing program are worth it in the long run Ideally your organization is performing audits on a regular basis across all service types locations and payers Weve all seen claims that have been denied resulting in additional work that may be preventable with a proper audit program The goal is to use the audit feedback to improve coding quality and lower potential risk and cost to the organization Organizations should be investing in an effective coding audit program to make your coders and providers better and enhance documentation improvement from the providers
Questions
Thank you for your attentionLynn Handy
Vice President of Coding amp Audit ServicesLynnhandymanagedresourcesinccom

Audit Report Examples Non Automated Solution
Error Findings by Volume Percentage
CPT Coded Accurately
8 8 Overcoded
8 8 Undercoded
Missed CPTHCPCS Code
Missed or Wrong Modifier
8 8 Incorrect CPT (or Category) Used
Incorrect ICD-9 Codes
8 8 Incorrect Quantity
Inadequate Documentation
Missing Documentation 8 8
Signature Illegible (No Log)
8 8
CLIENT NAME PROJECT TITLE
Review Line Item Detail Prepared Month Year
DRAFT
Client Claim Demographics Client Charge Data Review Result EampM ONLY Findings C C C C C C O OC O O O
Char
t Num
ber
Au
dit D
ate
Audi
tor (
initi
als)
QA
Initi
als
Fa
cilit
y Lo
catio
n Re
porte
d
Pr
ovid
er N
ame
Pa
tient
Nam
e
M
edic
al R
ecor
d Nu
mbe
r
Prim
ary
Carr
ier M
edica
re=
A M
edica
id =
B O
ther
=O
Da
te o
f Ser
vice
CP
T Co
de
Mod
ifier
(s) i
n or
der
Qua
ntity
Diag
nosi
s Co
de(s
) 1
thro
ugh
4
Fe
e ch
arge
d
Pr
imar
y Pa
ymen
t Am
ount
CPT
Code
Mod
ifier
(s) i
n or
der
Qua
ntity
Diag
nosi
s Co
de(s
) 1
thro
ugh
4
CO
RREC
T AL
LOW
ABLE
Prim
ary
PAYM
ENT
Va
rianc
e
Chie
f Com
plai
nt
Hist
ory
Leve
l Sup
port
ed
Exam
Lev
el S
uppo
rted
Med
ical
Dec
Mak
ing
Supp
orte
d (o
r TIM
E)
CPT
Cod
ed A
ccur
atel
y
Ove
rcod
ed
Und
erco
ded
Mis
sed
CPT
HC
PCS
Cod
e
Mis
sed
or W
rong
Mod
ifier
Inco
rrec
t CPT
(or C
ateg
ory)
Use
d
Inco
rrec
t IC
D-9
Cod
es
Inco
rrec
t Qua
ntity
Inad
equa
te D
ocum
enta
tion
Mis
sing
Doc
umen
tatio
n
Sign
atur
e Ill
egib
le (N
o Lo
g)
No
Sign
atur
e by
Pro
vide
r of
Ser
vice
COMMENTS (abbreviations used) PF- PROBLEM FOCUSED EPF- EXPANDED PF DET- DETAILED COMP- COMPREHENSIVE SFWD- STRAIGHT FORWARD MOD- MODERATE MDM- MEDICAL DECISION MAKING
Char
t Num
ber
SAMPLE SAMPLE S MD SAMPLE SAMPLE XXXXX XXX 112001 99212 25 1 1 1234 2 5678 3 4
$30000 $2200 99212 25 1 1 1234 2 5678 3 4
$56400 $54200 YES
DET
CO
MP
MO
D
COMMENTS COMMENTS COMMENTS
0
1 2 3 4
1 2 3 4
$000 0
$30000 $2200 $56400 $54200 10 10 10 10 10 10 10 10 10 10 10 10 TOTALS 917 Error Rate by Volume
Error Findings by Volume 8 CPT Coded Accurately 8 Overcoded 8 Undercoded 8 Missed CPTHCPCS Code 8 Missed or Wrong Modifier 8 Incorrect CPT (or Category) Used 8 Incorrect ICD-9 Codes 8 Incorrect Quantity
Inadequate Documentation 8 8 Missing Documentation 8 Signature Illegible (No Log) 8 No Signature by Provider of Service
1200 Total
Net Payment Error Rate -24636
Primary Payments Total $ Audited Payment Total $ (Total Under Payments)
Total Over Payments
Net OverUnder Payment $
2200 56400
(54200)
Resources Used HCPCS and CPT CodeBook (Current or applilcable year) ICD-10-CM CodeBook (Current or applicable year) CMS 1995 and 1997 EM Guidelines CMS Claims Processing Manual 100-04 Medicare Claims Processing (PUB 100-04) CMS - National Coverage Determinations (NCDs) National Correct Coding Policy Manual Applicable Physician Version
Executive Summary Report
The executive summary provides readers with a short complete document highlighting import information included in the detailed report Executive summaries are created for the senior management readers that donrsquot have time to read the full report and need to walk away with an understanding of the issues and corrective actions
Some would say the executive summary could be written before the detailed report however it is difficult to make sure the most important elements are included until you have spent time reviewing the detail If you want to make sure the most important messages are in the executive
summary this step should be completed after the detail is written As auditors become more seasoned this step could move to the front of the process
Executive Summary Report Structure of the ES Report
o Backgroundndash Specialtyndash Providersndash Sample Selection sizendash Date range of audit
o Audit Scopeo Regulatory Resourceso Type of Medical records reviewedo Overall Accuracy (all providers)o Detailed Audit Findings
ndash Business Impactndash Summary of Findings
o Department Findingso Summary
o ReportsStandard Executive Summary Professional Servicespdf
Department Findings Top Issues
Date ofServiceErrors
MissingDocuments
Missing orInvalid
Signature
TeachingPhysician
Errors
InsufficientConsultation
Documents
OverCoding
EMBundled
IntoGlobal
SurgicalPackage
SplitSharedServiceError
Incorrector
MissingPricing
Modifier
ICD-10Errors
Family Practice
CardiologyInternal Medicine
TOTALS
Top Findings by Provider
E amp M Accuracy Rates
ICD-10-CM Accuracy Rates
Procedure Accuracy Rates
Inpatient DRG Audit Report
TABLE OF CONTENTS
Executive Summaryo Scope of Work
Reimbursement Changes Department Results
o InpatientGeneral Recommendations and Comments
o Secondary DiagnosesoProcedure CodingoPresent on AdmissionoQueries
Scope of WorkCodingAID performed coding audit review of 175 inpatient records The review completed was a random sample that included cases coded by twenty coders for dates of service from May 2016 ndash July 2016
The objective was to determine if the medical record documentation supported the following coding and documentation requirements and any other regulatory requirement for that code set Criteria reviewed
1 ICD-10-CM Official Coding Guidelines for accurate diagnosis code reporting 2 ICD-10-PCS Official Coding Guidelines for accurate procedure code reporting 3 Documentation of procedure compared to the CPT code assigned 4 Identify opportunities for education and training 5 Financial impact of current coding practices
The regulatory agencies and reference materials relied upon include the following in addition to Medicare and Medicaid regulations Additional resources are located in the sub sections below
bull ICD-10-CM and ICD-10-PCS for Hospitals current volume bull Centers for Medicare and Medicaid Services CMS NCCI Edits-Centers for Medicaid and
Medicare Services CMS website wwwcmsgov bull AHA Coding Clinic
The following electronic medical record documents were reviewed and relied upon to compare to the actual codes submitted to the third party payer
bull Discharge summaries HampPs Progress Notes and other provider notes located in the EMR Records
bull Patient History Forms Ancillary Staff Notes bull Procedure Notes bull Orders bull Diagnostic Report
Reimbursement Changes
Coder Acct
Billed Audited
Reimbursement ChangesMS DRG SOI ROM Weight Expected
Payment MS DRG SOI ROM Weight Expected Payment
Coder 1 001 790 52300 $2615000 792 21552 $1077600 -$1537400
Coder 2002
749 26452 $1322600 758 10090 $504500 -$818100
Coder 3 003 669 13111 $655550 694 07294 $364700 -$290850
Coder 4 004 389 08707 $435350 394 09502 $475100 $39750
Coder 5 005 312 07630 $381500 812 08572 $428600 $47100
Coder 6 006 384 08481 $424050 378 09949 $497450 $73400
Coder 7 007 206 08164 $408200 794 12987 $649350 $241150
Coder 8008
344 31029 $1551450 853 51334 $2566700 $1015250
TOTAL $7793700 $6564000 -$1229700
General Recommendations and CommentsFinding Pertinent secondary diagnoses are not coded and diagnoses are code which are not supported in provider documentation Code only those diagnoses which are documented by the provider on the current chart Not all codes are coded to the highest degree of specificity and combination codes were sometimes missed
Recommendation It is important to assign codes for all conditions which meet the definition of a reportable diagnosis Documentation from all providers should be used including but not limited to radiologists pathologists anesthesiologists CRNAs and FNPs
Reference Coding Clinic Official Coding Guidelines
bull Report all secondary diagnoses which meet the definition of a secondary diagnosis which is defined as all conditions that coexist at the time of admission that develop subsequently or that affect the treatment received andor the length of stay Codes which enhance the overall picture of the patientrsquos visit should be added
o Add T45515A to report adverse effect of Coumadin which caused the GI bleed
o Add I2690 for septic pulmonary emboli (MCCSOI4ROM4)
o Add N179 for acute kidney failure (S3M2CC) per the nephrology consult and the 628 progress note
o Add code I429 cardiomyopathy per HampP
o Add B964 to report proteus in a UTI per the 620 hospitalist progress note
o Code for D649 anemia and I701 stenosis of renal artery should be added as secondary diagnoses per the HampP
bull Only report diagnoses which are substantiated by provider documentation in the current chart notes If a suspected condition is not verified at discharge on an inpatient account it cannot be coded
o Remove G4734 (idiopathic sleep related non-obstructive alveolar hypoventilation) as patient was noted to have the sleep study and the hypoventilation was shown to be a possibility but not noted as such on discharge
o Remove G629 (S21) the neuropathy is documented as due to diabetes
o Remove K529 colitis noted on HP as possible but not further noted or confirmed at discharge
Procedure CodingFinding Procedures were sometimes coded incorrectly
Recommendation The entire medical record should be reviewed and all procedures coded as documented Coding procedures incorrectly or assigning incorrect CPT codes may result in lost revenue
bull Incorrect root operation
o Revise principal procedure to 0DQ68ZZ for clipping of the ulcer per OP report clipping is root operation repair
bull Biopsy versus Excision
o Procedure 0DBA0ZX (biopsy of jejunum) should change to 0DBA0ZZ (excision of jejunum) per op note this was not a biopsy procedure
bull Coding Guideline error
o Remove 0RG10K0 for allograft due to being inclusive in principal procedure
o Remove codes for adhesiolysis 0DN80ZZ 0UN10ZZ and 0UN90ZZ due to no significance noted per OP report
bull Incorrect approach
o Revise 0TF63ZZ (fragmentation percutaneous approach) to 0TF68ZZ (fragmentation endoscopic) for procedure performed via scope per the operative report
bull Procedure coded without provider documentation
o Remove secondary procedure of excisional debridement (0JB90ZZ) due to lack of documentation of excisional debridement per operative report The header in the operative report documents IampD and debridement but the body of the operative report only documents an IampD
bull Incorrect CPT code assignment
o Post-op note supports the nerve block injections of four nerves therefore code 64421 (multiple nerve block) should replace 64420 (injection of one intercostal nerve)
Queries Finding Conflicting incomplete and vague documentation is found within provider chart notes
Recommendation Prior to code assignment if the coder finds ambiguous or conflicting documentation the provider should be queried
Reference AHA Coding Clinic 2002 2nd Quarter pages 17-18
bull Query for acute blood loss anemia since hgb has dropped and patient is being transfused PRBC
bull Recommend query to clarify if cardiorenal syndrome is current as it is documented per 627 nephrology consult but unclear if current
bull Documentation does not support SIRS noninfectious without organ failure It is conflicting since patient has respiratory failure Query should be initiated for clarification with or without organ failure or infectious or non-infectious Patient has pneumonia per query as well as last progress note therefore if SIRS is not further specified per query PNA should be sequenced as principal diagnosis and SIRS should be removed
bull Recommend provider query necrotizing lung consolidation noted on DS as principal diagnosis-unclear does the patient have lobar pneumonia Secondary dx states necrotic pneumonia which is coded as principal diagnosis-this diagnosis is clear but consolidation portion is unclear
bull Recommend query for preterm labor delivery at 301 weeks
bull RECOMMEND QUERY no chest pain on admit per ER and HP cardiology provider states no CP with ER stating chest pressure the day prior to admit Appears patient was admitted due to elevated troponins which cardiology says are likely due to hypotension and AKI DS states chest pain but also says bradycardia and hypotension were the reason for admit
bull RECOMMEND QUERY no chest pain on admit per ER and HP cardiology provider states no CP with ER stating chest pressure the day prior to admit Appears patient was admitted due to elevated troponins which cardiology says are likely due to hypotension and AKI DS states chest pain but also says bradycardia and hypotension were the reason for admit
bull Query the provider regarding pathology report notation of endometriosis andor possible re-sequence of stenosis as principal diagnosis as it also meets principal diagnosis guidelines This would result in an MS-DRG change to 742 and APR-DRG change to 513
bull QUERY secondary diagnosis MCC and ROM 4 code T3166 (60 TBSA of which 60 are third degree burns) Chart notes do not specify how much of TBSA was actually third degree If after query TBSA is found to be less than 50 (T3164) then ROM will change from 4 to 3 but no change to overall APR-DRG or weight
Auditor Quality amp Productivity
Audit Productivity Standards
It takes twice as long to audit a chart as it does to code it a statistic that takes into account the time to document an explanation of any coding decision the auditor is not in agreement with o For example in an emergency department audit with a productivity of 12
charts per hour for a coder our auditors would probably be able to review six per hour
o If there are multiple services to audit on each encounter the productivity may only be 4 per hour
o The amount of detail you put into your audit report will also be a factorndash Are you using an automated audit softwarendash Are you using a spreadsheet to auditndash How many Systems are needed to complete the audit
Coder Quality Audits
Quality Audits (QA) should be done on your coders and auditors regularly Frequent reviews with smaller sample size will allow more consistent
review and feedbacko Example 10 charts per month per coder if the coder passes 2-3 months
consecutively with 95 or better score move them to quarterly reviewso Some QA programs review a percentage of the coders work This
methodology requires more time and resources
Auditor QA should also score and comment on the accuracy of the audit comments and recommendations
Presenting the Audit Results
Presenting the Audit Results
Communicating the Audit FindingsoWho requested the AuditoWho are you reporting the finding to
ndash CEOndash CFOndash Physicianndash Revenue Cycle Managerndash HIM Directorndash Billing Managerndash Coding Manager
ReportsAudit Resultspptx
Post Audit Education
Provider Education
Provider Education is best received when it is specific to the provider(s) 11 sessions going over the audit result Look at their notes with them
oHighlight areas for documentation improvementoReinforce Coding Guidelines that are specific to themoAsk them to share how they establish their LOS for E amp M serviceso Integrate their EMR system into the training
Provider Education
Group Training SessionsoUse the audit results to identify common issues within a specialty group
ndash Refer to the Executive Summary reportoVery effective for identifying system issues
ndash Teaching Attestationsndash Templatesndash Copy and Pastendash Cloned notes
o Everyone hears the same messagesoAn Issue may not appear on the individual audit but is still a concern for the
group
Education Delivery
In person or remote sessionso Factors to consider
ndash Providers scheduleavailabilityndash Location(s)ndash Personality of the providerndash Budget
Coder Education
Coders do well in group training so they can learn from each other 11 training allows the coder to get feedback on their coding
Handling Audit Disputes
Handling Audit Disputes
Be open to all points of viewo Let the documentation tell the story
Refer to the guidelines Ask
oCan we defend the reported service with the current documentation
Self Disclosures Refunds and Corrected Billing
Overpayment
In general If a person has received an overpayment the person shallo report and return the overpayment to the Secretary the State an
intermediary a carrier or a contractor as appropriate at the correct address and ndash notify the Secretary State intermediary carrier or contractor to whom the overpayment was returned in writing of the reason for the overpayment
What is an ldquoOverpaymentrdquo ndash The term ldquooverpaymentrdquo means any funds that a person receives or retains under subchapter XVIII or XIX of this chapter to which the person after applicable reconciliation is not entitled under such subchapter
Self Disclosure
The Office of Inspector General (OIG) has several self-disclosure processes that can be used to report potential fraud in Department of Health and Human Services (HHS) programs Choose the one that applies to you from the following descriptions to learn moreo Health Care Provider Self-Disclosures
ndash Health care providers suppliers or other individuals or entities subject to Civil Monetary Penalties can use the Provider Self-Disclosure Protocol which was created in 1998 to voluntarily disclose self-discovered evidence of potential fraud Self-disclosure gives providers the opportunity to avoid the costs and disruptions associated with a Government-directed investigation and civil or administrative litigation Visit the Provider Self-Disclosure Protocol webpage for more information
o HHS Contractor Self-Disclosuresndash Contractors are individuals businesses or other legal entities that are awarded Government contracts or
subcontracts to provide services to the Department of Health and Human Services (HHS) OIGs contractor self-disclosure program enables contractors to self-disclose potential violations of the False Claims Act and various Federal criminal laws involving fraud conflict of interest bribery or gratuity This self-disclosure process is available for those entities with a Federal Acquisition Regulation-based contract Visit the Contractor Self-Disclosure webpage for more information
o HHS Grantee Self-Disclosuresndash HHS grantees or subrecipients may voluntarily disclose evidence of potential violations of Federal criminal law
involving fraud bribery or gratuity violations potentially affecting the Federal award 45 CFR 75113 notes mandatory disclosures of criminal offenses that non-Federal entities must make with respect to HHS grants Recipients submitting disclosures in connection with this requirement should include the subject reference line Mandatory Grant Disclosure Recipients choosing to disclose conduct that may not fit squarely within the scope of offenses described in 45 CFR 75113 should include the following subject reference line in the submission Voluntary Grant Disclosure
Medicare 60 day rule
The 60 Day Rule (Medicare Parts A amp B) o The 60 day time period for reportingreturning begins when either
ndash The reasonable diligence is completed orndash On the day the provider received credible information of a potential overpayment (if the
provider fails to conduct reasonable diligence) o For an investigation to be conducted in a ldquotimelyrdquo manner providers typically
must complete the investigation within 6 months from receipt of credible information indicating there may be an overpayment
ndash ndash 6-month timeframe may potentially be extended under ldquoextraordinary circumstancesrdquo ndash 8 months generally the maximum total time to return overpayments The government recommends that providers maintain records documenting ldquoreasonable diligencerdquo
Medicare 60 Day Rule
Six-year lookback period ndash Sometimes possible to use a shorter period depending on the facts at issue Amount to be repaid ndash May vary depending on the method used to
reportreturn eg Medicare administrative contractor (ldquoMACrdquo) v self-disclosure Overpayment notification ndash After receiving an overpayment
notification from the government you should investigate for related overpayments eg other time periods
Medicare 60 Day Rule
Self-disclosure protocols ndashoA submission to the OIG or CMS protocols suspends the 60 day requirement
for returning overpayments until a settlement agreement is executed ndash ndash OIGrsquos Self-Disclosure Protocol (SDP) ndash ndash CMS Voluntary Self-Referral Disclosure Protocol (SRDP) ndash
o Self-disclosures to other agencies do not suspend the repayment deadlinendash ndash Eg Department of Justice local US Attorneyrsquos Office Medicaid Fraud Control Unit
Medicare 60 Day Rule
Facilitating Compliance With the 60 Day Rule Compliance programs should include o ndash Appropriate policies and procedures o ndash Periodic billing and coding audits to proactively identify overpaymentso ndash Focus on high-risk areas o ndash Utilization of publicly available government resources to guide audit efforts o ndash Investigating any suspected incidents of non-compliance with federal health
care program requirements
Self Disclosure
Choice of AgencyoOIG ndash Self-Disclosure Protocol
ndash ndash Conduct involving false billingndash ndash Conduct involving excluded personsndash ndash Conduct involving the Anti-Kickback Statute (including conduct thatndash violates both the AKS and Stark Law)
oCMS ndash Self-Referral Disclosure Protocolndash ndash Conduct involving only violations of the Stark Law
oDOJndash ndash May be appropriate when provider believes a FCA release is necessary
Summary
The Cost of a Well-Executed Coding Audit ProcessThe costs associated with an auditing program are worth it in the long run Ideally your organization is performing audits on a regular basis across all service types locations and payers Weve all seen claims that have been denied resulting in additional work that may be preventable with a proper audit program The goal is to use the audit feedback to improve coding quality and lower potential risk and cost to the organization Organizations should be investing in an effective coding audit program to make your coders and providers better and enhance documentation improvement from the providers
Questions
Thank you for your attentionLynn Handy
Vice President of Coding amp Audit ServicesLynnhandymanagedresourcesinccom

Executive Summary Report
The executive summary provides readers with a short complete document highlighting import information included in the detailed report Executive summaries are created for the senior management readers that donrsquot have time to read the full report and need to walk away with an understanding of the issues and corrective actions
Some would say the executive summary could be written before the detailed report however it is difficult to make sure the most important elements are included until you have spent time reviewing the detail If you want to make sure the most important messages are in the executive
summary this step should be completed after the detail is written As auditors become more seasoned this step could move to the front of the process
Executive Summary Report Structure of the ES Report
o Backgroundndash Specialtyndash Providersndash Sample Selection sizendash Date range of audit
o Audit Scopeo Regulatory Resourceso Type of Medical records reviewedo Overall Accuracy (all providers)o Detailed Audit Findings
ndash Business Impactndash Summary of Findings
o Department Findingso Summary
o ReportsStandard Executive Summary Professional Servicespdf
Department Findings Top Issues
Date ofServiceErrors
MissingDocuments
Missing orInvalid
Signature
TeachingPhysician
Errors
InsufficientConsultation
Documents
OverCoding
EMBundled
IntoGlobal
SurgicalPackage
SplitSharedServiceError
Incorrector
MissingPricing
Modifier
ICD-10Errors
Family Practice
CardiologyInternal Medicine
TOTALS
Top Findings by Provider
E amp M Accuracy Rates
ICD-10-CM Accuracy Rates
Procedure Accuracy Rates
Inpatient DRG Audit Report
TABLE OF CONTENTS
Executive Summaryo Scope of Work
Reimbursement Changes Department Results
o InpatientGeneral Recommendations and Comments
o Secondary DiagnosesoProcedure CodingoPresent on AdmissionoQueries
Scope of WorkCodingAID performed coding audit review of 175 inpatient records The review completed was a random sample that included cases coded by twenty coders for dates of service from May 2016 ndash July 2016
The objective was to determine if the medical record documentation supported the following coding and documentation requirements and any other regulatory requirement for that code set Criteria reviewed
1 ICD-10-CM Official Coding Guidelines for accurate diagnosis code reporting 2 ICD-10-PCS Official Coding Guidelines for accurate procedure code reporting 3 Documentation of procedure compared to the CPT code assigned 4 Identify opportunities for education and training 5 Financial impact of current coding practices
The regulatory agencies and reference materials relied upon include the following in addition to Medicare and Medicaid regulations Additional resources are located in the sub sections below
bull ICD-10-CM and ICD-10-PCS for Hospitals current volume bull Centers for Medicare and Medicaid Services CMS NCCI Edits-Centers for Medicaid and
Medicare Services CMS website wwwcmsgov bull AHA Coding Clinic
The following electronic medical record documents were reviewed and relied upon to compare to the actual codes submitted to the third party payer
bull Discharge summaries HampPs Progress Notes and other provider notes located in the EMR Records
bull Patient History Forms Ancillary Staff Notes bull Procedure Notes bull Orders bull Diagnostic Report
Reimbursement Changes
Coder Acct
Billed Audited
Reimbursement ChangesMS DRG SOI ROM Weight Expected
Payment MS DRG SOI ROM Weight Expected Payment
Coder 1 001 790 52300 $2615000 792 21552 $1077600 -$1537400
Coder 2002
749 26452 $1322600 758 10090 $504500 -$818100
Coder 3 003 669 13111 $655550 694 07294 $364700 -$290850
Coder 4 004 389 08707 $435350 394 09502 $475100 $39750
Coder 5 005 312 07630 $381500 812 08572 $428600 $47100
Coder 6 006 384 08481 $424050 378 09949 $497450 $73400
Coder 7 007 206 08164 $408200 794 12987 $649350 $241150
Coder 8008
344 31029 $1551450 853 51334 $2566700 $1015250
TOTAL $7793700 $6564000 -$1229700
General Recommendations and CommentsFinding Pertinent secondary diagnoses are not coded and diagnoses are code which are not supported in provider documentation Code only those diagnoses which are documented by the provider on the current chart Not all codes are coded to the highest degree of specificity and combination codes were sometimes missed
Recommendation It is important to assign codes for all conditions which meet the definition of a reportable diagnosis Documentation from all providers should be used including but not limited to radiologists pathologists anesthesiologists CRNAs and FNPs
Reference Coding Clinic Official Coding Guidelines
bull Report all secondary diagnoses which meet the definition of a secondary diagnosis which is defined as all conditions that coexist at the time of admission that develop subsequently or that affect the treatment received andor the length of stay Codes which enhance the overall picture of the patientrsquos visit should be added
o Add T45515A to report adverse effect of Coumadin which caused the GI bleed
o Add I2690 for septic pulmonary emboli (MCCSOI4ROM4)
o Add N179 for acute kidney failure (S3M2CC) per the nephrology consult and the 628 progress note
o Add code I429 cardiomyopathy per HampP
o Add B964 to report proteus in a UTI per the 620 hospitalist progress note
o Code for D649 anemia and I701 stenosis of renal artery should be added as secondary diagnoses per the HampP
bull Only report diagnoses which are substantiated by provider documentation in the current chart notes If a suspected condition is not verified at discharge on an inpatient account it cannot be coded
o Remove G4734 (idiopathic sleep related non-obstructive alveolar hypoventilation) as patient was noted to have the sleep study and the hypoventilation was shown to be a possibility but not noted as such on discharge
o Remove G629 (S21) the neuropathy is documented as due to diabetes
o Remove K529 colitis noted on HP as possible but not further noted or confirmed at discharge
Procedure CodingFinding Procedures were sometimes coded incorrectly
Recommendation The entire medical record should be reviewed and all procedures coded as documented Coding procedures incorrectly or assigning incorrect CPT codes may result in lost revenue
bull Incorrect root operation
o Revise principal procedure to 0DQ68ZZ for clipping of the ulcer per OP report clipping is root operation repair
bull Biopsy versus Excision
o Procedure 0DBA0ZX (biopsy of jejunum) should change to 0DBA0ZZ (excision of jejunum) per op note this was not a biopsy procedure
bull Coding Guideline error
o Remove 0RG10K0 for allograft due to being inclusive in principal procedure
o Remove codes for adhesiolysis 0DN80ZZ 0UN10ZZ and 0UN90ZZ due to no significance noted per OP report
bull Incorrect approach
o Revise 0TF63ZZ (fragmentation percutaneous approach) to 0TF68ZZ (fragmentation endoscopic) for procedure performed via scope per the operative report
bull Procedure coded without provider documentation
o Remove secondary procedure of excisional debridement (0JB90ZZ) due to lack of documentation of excisional debridement per operative report The header in the operative report documents IampD and debridement but the body of the operative report only documents an IampD
bull Incorrect CPT code assignment
o Post-op note supports the nerve block injections of four nerves therefore code 64421 (multiple nerve block) should replace 64420 (injection of one intercostal nerve)
Queries Finding Conflicting incomplete and vague documentation is found within provider chart notes
Recommendation Prior to code assignment if the coder finds ambiguous or conflicting documentation the provider should be queried
Reference AHA Coding Clinic 2002 2nd Quarter pages 17-18
bull Query for acute blood loss anemia since hgb has dropped and patient is being transfused PRBC
bull Recommend query to clarify if cardiorenal syndrome is current as it is documented per 627 nephrology consult but unclear if current
bull Documentation does not support SIRS noninfectious without organ failure It is conflicting since patient has respiratory failure Query should be initiated for clarification with or without organ failure or infectious or non-infectious Patient has pneumonia per query as well as last progress note therefore if SIRS is not further specified per query PNA should be sequenced as principal diagnosis and SIRS should be removed
bull Recommend provider query necrotizing lung consolidation noted on DS as principal diagnosis-unclear does the patient have lobar pneumonia Secondary dx states necrotic pneumonia which is coded as principal diagnosis-this diagnosis is clear but consolidation portion is unclear
bull Recommend query for preterm labor delivery at 301 weeks
bull RECOMMEND QUERY no chest pain on admit per ER and HP cardiology provider states no CP with ER stating chest pressure the day prior to admit Appears patient was admitted due to elevated troponins which cardiology says are likely due to hypotension and AKI DS states chest pain but also says bradycardia and hypotension were the reason for admit
bull RECOMMEND QUERY no chest pain on admit per ER and HP cardiology provider states no CP with ER stating chest pressure the day prior to admit Appears patient was admitted due to elevated troponins which cardiology says are likely due to hypotension and AKI DS states chest pain but also says bradycardia and hypotension were the reason for admit
bull Query the provider regarding pathology report notation of endometriosis andor possible re-sequence of stenosis as principal diagnosis as it also meets principal diagnosis guidelines This would result in an MS-DRG change to 742 and APR-DRG change to 513
bull QUERY secondary diagnosis MCC and ROM 4 code T3166 (60 TBSA of which 60 are third degree burns) Chart notes do not specify how much of TBSA was actually third degree If after query TBSA is found to be less than 50 (T3164) then ROM will change from 4 to 3 but no change to overall APR-DRG or weight
Auditor Quality amp Productivity
Audit Productivity Standards
It takes twice as long to audit a chart as it does to code it a statistic that takes into account the time to document an explanation of any coding decision the auditor is not in agreement with o For example in an emergency department audit with a productivity of 12
charts per hour for a coder our auditors would probably be able to review six per hour
o If there are multiple services to audit on each encounter the productivity may only be 4 per hour
o The amount of detail you put into your audit report will also be a factorndash Are you using an automated audit softwarendash Are you using a spreadsheet to auditndash How many Systems are needed to complete the audit
Coder Quality Audits
Quality Audits (QA) should be done on your coders and auditors regularly Frequent reviews with smaller sample size will allow more consistent
review and feedbacko Example 10 charts per month per coder if the coder passes 2-3 months
consecutively with 95 or better score move them to quarterly reviewso Some QA programs review a percentage of the coders work This
methodology requires more time and resources
Auditor QA should also score and comment on the accuracy of the audit comments and recommendations
Presenting the Audit Results
Presenting the Audit Results
Communicating the Audit FindingsoWho requested the AuditoWho are you reporting the finding to
ndash CEOndash CFOndash Physicianndash Revenue Cycle Managerndash HIM Directorndash Billing Managerndash Coding Manager
ReportsAudit Resultspptx
Post Audit Education
Provider Education
Provider Education is best received when it is specific to the provider(s) 11 sessions going over the audit result Look at their notes with them
oHighlight areas for documentation improvementoReinforce Coding Guidelines that are specific to themoAsk them to share how they establish their LOS for E amp M serviceso Integrate their EMR system into the training
Provider Education
Group Training SessionsoUse the audit results to identify common issues within a specialty group
ndash Refer to the Executive Summary reportoVery effective for identifying system issues
ndash Teaching Attestationsndash Templatesndash Copy and Pastendash Cloned notes
o Everyone hears the same messagesoAn Issue may not appear on the individual audit but is still a concern for the
group
Education Delivery
In person or remote sessionso Factors to consider
ndash Providers scheduleavailabilityndash Location(s)ndash Personality of the providerndash Budget
Coder Education
Coders do well in group training so they can learn from each other 11 training allows the coder to get feedback on their coding
Handling Audit Disputes
Handling Audit Disputes
Be open to all points of viewo Let the documentation tell the story
Refer to the guidelines Ask
oCan we defend the reported service with the current documentation
Self Disclosures Refunds and Corrected Billing
Overpayment
In general If a person has received an overpayment the person shallo report and return the overpayment to the Secretary the State an
intermediary a carrier or a contractor as appropriate at the correct address and ndash notify the Secretary State intermediary carrier or contractor to whom the overpayment was returned in writing of the reason for the overpayment
What is an ldquoOverpaymentrdquo ndash The term ldquooverpaymentrdquo means any funds that a person receives or retains under subchapter XVIII or XIX of this chapter to which the person after applicable reconciliation is not entitled under such subchapter
Self Disclosure
The Office of Inspector General (OIG) has several self-disclosure processes that can be used to report potential fraud in Department of Health and Human Services (HHS) programs Choose the one that applies to you from the following descriptions to learn moreo Health Care Provider Self-Disclosures
ndash Health care providers suppliers or other individuals or entities subject to Civil Monetary Penalties can use the Provider Self-Disclosure Protocol which was created in 1998 to voluntarily disclose self-discovered evidence of potential fraud Self-disclosure gives providers the opportunity to avoid the costs and disruptions associated with a Government-directed investigation and civil or administrative litigation Visit the Provider Self-Disclosure Protocol webpage for more information
o HHS Contractor Self-Disclosuresndash Contractors are individuals businesses or other legal entities that are awarded Government contracts or
subcontracts to provide services to the Department of Health and Human Services (HHS) OIGs contractor self-disclosure program enables contractors to self-disclose potential violations of the False Claims Act and various Federal criminal laws involving fraud conflict of interest bribery or gratuity This self-disclosure process is available for those entities with a Federal Acquisition Regulation-based contract Visit the Contractor Self-Disclosure webpage for more information
o HHS Grantee Self-Disclosuresndash HHS grantees or subrecipients may voluntarily disclose evidence of potential violations of Federal criminal law
involving fraud bribery or gratuity violations potentially affecting the Federal award 45 CFR 75113 notes mandatory disclosures of criminal offenses that non-Federal entities must make with respect to HHS grants Recipients submitting disclosures in connection with this requirement should include the subject reference line Mandatory Grant Disclosure Recipients choosing to disclose conduct that may not fit squarely within the scope of offenses described in 45 CFR 75113 should include the following subject reference line in the submission Voluntary Grant Disclosure
Medicare 60 day rule
The 60 Day Rule (Medicare Parts A amp B) o The 60 day time period for reportingreturning begins when either
ndash The reasonable diligence is completed orndash On the day the provider received credible information of a potential overpayment (if the
provider fails to conduct reasonable diligence) o For an investigation to be conducted in a ldquotimelyrdquo manner providers typically
must complete the investigation within 6 months from receipt of credible information indicating there may be an overpayment
ndash ndash 6-month timeframe may potentially be extended under ldquoextraordinary circumstancesrdquo ndash 8 months generally the maximum total time to return overpayments The government recommends that providers maintain records documenting ldquoreasonable diligencerdquo
Medicare 60 Day Rule
Six-year lookback period ndash Sometimes possible to use a shorter period depending on the facts at issue Amount to be repaid ndash May vary depending on the method used to
reportreturn eg Medicare administrative contractor (ldquoMACrdquo) v self-disclosure Overpayment notification ndash After receiving an overpayment
notification from the government you should investigate for related overpayments eg other time periods
Medicare 60 Day Rule
Self-disclosure protocols ndashoA submission to the OIG or CMS protocols suspends the 60 day requirement
for returning overpayments until a settlement agreement is executed ndash ndash OIGrsquos Self-Disclosure Protocol (SDP) ndash ndash CMS Voluntary Self-Referral Disclosure Protocol (SRDP) ndash
o Self-disclosures to other agencies do not suspend the repayment deadlinendash ndash Eg Department of Justice local US Attorneyrsquos Office Medicaid Fraud Control Unit
Medicare 60 Day Rule
Facilitating Compliance With the 60 Day Rule Compliance programs should include o ndash Appropriate policies and procedures o ndash Periodic billing and coding audits to proactively identify overpaymentso ndash Focus on high-risk areas o ndash Utilization of publicly available government resources to guide audit efforts o ndash Investigating any suspected incidents of non-compliance with federal health
care program requirements
Self Disclosure
Choice of AgencyoOIG ndash Self-Disclosure Protocol
ndash ndash Conduct involving false billingndash ndash Conduct involving excluded personsndash ndash Conduct involving the Anti-Kickback Statute (including conduct thatndash violates both the AKS and Stark Law)
oCMS ndash Self-Referral Disclosure Protocolndash ndash Conduct involving only violations of the Stark Law
oDOJndash ndash May be appropriate when provider believes a FCA release is necessary
Summary
The Cost of a Well-Executed Coding Audit ProcessThe costs associated with an auditing program are worth it in the long run Ideally your organization is performing audits on a regular basis across all service types locations and payers Weve all seen claims that have been denied resulting in additional work that may be preventable with a proper audit program The goal is to use the audit feedback to improve coding quality and lower potential risk and cost to the organization Organizations should be investing in an effective coding audit program to make your coders and providers better and enhance documentation improvement from the providers
Questions
Thank you for your attentionLynn Handy
Vice President of Coding amp Audit ServicesLynnhandymanagedresourcesinccom

Executive Summary Report Structure of the ES Report
o Backgroundndash Specialtyndash Providersndash Sample Selection sizendash Date range of audit
o Audit Scopeo Regulatory Resourceso Type of Medical records reviewedo Overall Accuracy (all providers)o Detailed Audit Findings
ndash Business Impactndash Summary of Findings
o Department Findingso Summary
o ReportsStandard Executive Summary Professional Servicespdf
Department Findings Top Issues
Date ofServiceErrors
MissingDocuments
Missing orInvalid
Signature
TeachingPhysician
Errors
InsufficientConsultation
Documents
OverCoding
EMBundled
IntoGlobal
SurgicalPackage
SplitSharedServiceError
Incorrector
MissingPricing
Modifier
ICD-10Errors
Family Practice
CardiologyInternal Medicine
TOTALS
Top Findings by Provider
E amp M Accuracy Rates
ICD-10-CM Accuracy Rates
Procedure Accuracy Rates
Inpatient DRG Audit Report
TABLE OF CONTENTS
Executive Summaryo Scope of Work
Reimbursement Changes Department Results
o InpatientGeneral Recommendations and Comments
o Secondary DiagnosesoProcedure CodingoPresent on AdmissionoQueries
Scope of WorkCodingAID performed coding audit review of 175 inpatient records The review completed was a random sample that included cases coded by twenty coders for dates of service from May 2016 ndash July 2016
The objective was to determine if the medical record documentation supported the following coding and documentation requirements and any other regulatory requirement for that code set Criteria reviewed
1 ICD-10-CM Official Coding Guidelines for accurate diagnosis code reporting 2 ICD-10-PCS Official Coding Guidelines for accurate procedure code reporting 3 Documentation of procedure compared to the CPT code assigned 4 Identify opportunities for education and training 5 Financial impact of current coding practices
The regulatory agencies and reference materials relied upon include the following in addition to Medicare and Medicaid regulations Additional resources are located in the sub sections below
bull ICD-10-CM and ICD-10-PCS for Hospitals current volume bull Centers for Medicare and Medicaid Services CMS NCCI Edits-Centers for Medicaid and
Medicare Services CMS website wwwcmsgov bull AHA Coding Clinic
The following electronic medical record documents were reviewed and relied upon to compare to the actual codes submitted to the third party payer
bull Discharge summaries HampPs Progress Notes and other provider notes located in the EMR Records
bull Patient History Forms Ancillary Staff Notes bull Procedure Notes bull Orders bull Diagnostic Report
Reimbursement Changes
Coder Acct
Billed Audited
Reimbursement ChangesMS DRG SOI ROM Weight Expected
Payment MS DRG SOI ROM Weight Expected Payment
Coder 1 001 790 52300 $2615000 792 21552 $1077600 -$1537400
Coder 2002
749 26452 $1322600 758 10090 $504500 -$818100
Coder 3 003 669 13111 $655550 694 07294 $364700 -$290850
Coder 4 004 389 08707 $435350 394 09502 $475100 $39750
Coder 5 005 312 07630 $381500 812 08572 $428600 $47100
Coder 6 006 384 08481 $424050 378 09949 $497450 $73400
Coder 7 007 206 08164 $408200 794 12987 $649350 $241150
Coder 8008
344 31029 $1551450 853 51334 $2566700 $1015250
TOTAL $7793700 $6564000 -$1229700
General Recommendations and CommentsFinding Pertinent secondary diagnoses are not coded and diagnoses are code which are not supported in provider documentation Code only those diagnoses which are documented by the provider on the current chart Not all codes are coded to the highest degree of specificity and combination codes were sometimes missed
Recommendation It is important to assign codes for all conditions which meet the definition of a reportable diagnosis Documentation from all providers should be used including but not limited to radiologists pathologists anesthesiologists CRNAs and FNPs
Reference Coding Clinic Official Coding Guidelines
bull Report all secondary diagnoses which meet the definition of a secondary diagnosis which is defined as all conditions that coexist at the time of admission that develop subsequently or that affect the treatment received andor the length of stay Codes which enhance the overall picture of the patientrsquos visit should be added
o Add T45515A to report adverse effect of Coumadin which caused the GI bleed
o Add I2690 for septic pulmonary emboli (MCCSOI4ROM4)
o Add N179 for acute kidney failure (S3M2CC) per the nephrology consult and the 628 progress note
o Add code I429 cardiomyopathy per HampP
o Add B964 to report proteus in a UTI per the 620 hospitalist progress note
o Code for D649 anemia and I701 stenosis of renal artery should be added as secondary diagnoses per the HampP
bull Only report diagnoses which are substantiated by provider documentation in the current chart notes If a suspected condition is not verified at discharge on an inpatient account it cannot be coded
o Remove G4734 (idiopathic sleep related non-obstructive alveolar hypoventilation) as patient was noted to have the sleep study and the hypoventilation was shown to be a possibility but not noted as such on discharge
o Remove G629 (S21) the neuropathy is documented as due to diabetes
o Remove K529 colitis noted on HP as possible but not further noted or confirmed at discharge
Procedure CodingFinding Procedures were sometimes coded incorrectly
Recommendation The entire medical record should be reviewed and all procedures coded as documented Coding procedures incorrectly or assigning incorrect CPT codes may result in lost revenue
bull Incorrect root operation
o Revise principal procedure to 0DQ68ZZ for clipping of the ulcer per OP report clipping is root operation repair
bull Biopsy versus Excision
o Procedure 0DBA0ZX (biopsy of jejunum) should change to 0DBA0ZZ (excision of jejunum) per op note this was not a biopsy procedure
bull Coding Guideline error
o Remove 0RG10K0 for allograft due to being inclusive in principal procedure
o Remove codes for adhesiolysis 0DN80ZZ 0UN10ZZ and 0UN90ZZ due to no significance noted per OP report
bull Incorrect approach
o Revise 0TF63ZZ (fragmentation percutaneous approach) to 0TF68ZZ (fragmentation endoscopic) for procedure performed via scope per the operative report
bull Procedure coded without provider documentation
o Remove secondary procedure of excisional debridement (0JB90ZZ) due to lack of documentation of excisional debridement per operative report The header in the operative report documents IampD and debridement but the body of the operative report only documents an IampD
bull Incorrect CPT code assignment
o Post-op note supports the nerve block injections of four nerves therefore code 64421 (multiple nerve block) should replace 64420 (injection of one intercostal nerve)
Queries Finding Conflicting incomplete and vague documentation is found within provider chart notes
Recommendation Prior to code assignment if the coder finds ambiguous or conflicting documentation the provider should be queried
Reference AHA Coding Clinic 2002 2nd Quarter pages 17-18
bull Query for acute blood loss anemia since hgb has dropped and patient is being transfused PRBC
bull Recommend query to clarify if cardiorenal syndrome is current as it is documented per 627 nephrology consult but unclear if current
bull Documentation does not support SIRS noninfectious without organ failure It is conflicting since patient has respiratory failure Query should be initiated for clarification with or without organ failure or infectious or non-infectious Patient has pneumonia per query as well as last progress note therefore if SIRS is not further specified per query PNA should be sequenced as principal diagnosis and SIRS should be removed
bull Recommend provider query necrotizing lung consolidation noted on DS as principal diagnosis-unclear does the patient have lobar pneumonia Secondary dx states necrotic pneumonia which is coded as principal diagnosis-this diagnosis is clear but consolidation portion is unclear
bull Recommend query for preterm labor delivery at 301 weeks
bull RECOMMEND QUERY no chest pain on admit per ER and HP cardiology provider states no CP with ER stating chest pressure the day prior to admit Appears patient was admitted due to elevated troponins which cardiology says are likely due to hypotension and AKI DS states chest pain but also says bradycardia and hypotension were the reason for admit
bull RECOMMEND QUERY no chest pain on admit per ER and HP cardiology provider states no CP with ER stating chest pressure the day prior to admit Appears patient was admitted due to elevated troponins which cardiology says are likely due to hypotension and AKI DS states chest pain but also says bradycardia and hypotension were the reason for admit
bull Query the provider regarding pathology report notation of endometriosis andor possible re-sequence of stenosis as principal diagnosis as it also meets principal diagnosis guidelines This would result in an MS-DRG change to 742 and APR-DRG change to 513
bull QUERY secondary diagnosis MCC and ROM 4 code T3166 (60 TBSA of which 60 are third degree burns) Chart notes do not specify how much of TBSA was actually third degree If after query TBSA is found to be less than 50 (T3164) then ROM will change from 4 to 3 but no change to overall APR-DRG or weight
Auditor Quality amp Productivity
Audit Productivity Standards
It takes twice as long to audit a chart as it does to code it a statistic that takes into account the time to document an explanation of any coding decision the auditor is not in agreement with o For example in an emergency department audit with a productivity of 12
charts per hour for a coder our auditors would probably be able to review six per hour
o If there are multiple services to audit on each encounter the productivity may only be 4 per hour
o The amount of detail you put into your audit report will also be a factorndash Are you using an automated audit softwarendash Are you using a spreadsheet to auditndash How many Systems are needed to complete the audit
Coder Quality Audits
Quality Audits (QA) should be done on your coders and auditors regularly Frequent reviews with smaller sample size will allow more consistent
review and feedbacko Example 10 charts per month per coder if the coder passes 2-3 months
consecutively with 95 or better score move them to quarterly reviewso Some QA programs review a percentage of the coders work This
methodology requires more time and resources
Auditor QA should also score and comment on the accuracy of the audit comments and recommendations
Presenting the Audit Results
Presenting the Audit Results
Communicating the Audit FindingsoWho requested the AuditoWho are you reporting the finding to
ndash CEOndash CFOndash Physicianndash Revenue Cycle Managerndash HIM Directorndash Billing Managerndash Coding Manager
ReportsAudit Resultspptx
Post Audit Education
Provider Education
Provider Education is best received when it is specific to the provider(s) 11 sessions going over the audit result Look at their notes with them
oHighlight areas for documentation improvementoReinforce Coding Guidelines that are specific to themoAsk them to share how they establish their LOS for E amp M serviceso Integrate their EMR system into the training
Provider Education
Group Training SessionsoUse the audit results to identify common issues within a specialty group
ndash Refer to the Executive Summary reportoVery effective for identifying system issues
ndash Teaching Attestationsndash Templatesndash Copy and Pastendash Cloned notes
o Everyone hears the same messagesoAn Issue may not appear on the individual audit but is still a concern for the
group
Education Delivery
In person or remote sessionso Factors to consider
ndash Providers scheduleavailabilityndash Location(s)ndash Personality of the providerndash Budget
Coder Education
Coders do well in group training so they can learn from each other 11 training allows the coder to get feedback on their coding
Handling Audit Disputes
Handling Audit Disputes
Be open to all points of viewo Let the documentation tell the story
Refer to the guidelines Ask
oCan we defend the reported service with the current documentation
Self Disclosures Refunds and Corrected Billing
Overpayment
In general If a person has received an overpayment the person shallo report and return the overpayment to the Secretary the State an
intermediary a carrier or a contractor as appropriate at the correct address and ndash notify the Secretary State intermediary carrier or contractor to whom the overpayment was returned in writing of the reason for the overpayment
What is an ldquoOverpaymentrdquo ndash The term ldquooverpaymentrdquo means any funds that a person receives or retains under subchapter XVIII or XIX of this chapter to which the person after applicable reconciliation is not entitled under such subchapter
Self Disclosure
The Office of Inspector General (OIG) has several self-disclosure processes that can be used to report potential fraud in Department of Health and Human Services (HHS) programs Choose the one that applies to you from the following descriptions to learn moreo Health Care Provider Self-Disclosures
ndash Health care providers suppliers or other individuals or entities subject to Civil Monetary Penalties can use the Provider Self-Disclosure Protocol which was created in 1998 to voluntarily disclose self-discovered evidence of potential fraud Self-disclosure gives providers the opportunity to avoid the costs and disruptions associated with a Government-directed investigation and civil or administrative litigation Visit the Provider Self-Disclosure Protocol webpage for more information
o HHS Contractor Self-Disclosuresndash Contractors are individuals businesses or other legal entities that are awarded Government contracts or
subcontracts to provide services to the Department of Health and Human Services (HHS) OIGs contractor self-disclosure program enables contractors to self-disclose potential violations of the False Claims Act and various Federal criminal laws involving fraud conflict of interest bribery or gratuity This self-disclosure process is available for those entities with a Federal Acquisition Regulation-based contract Visit the Contractor Self-Disclosure webpage for more information
o HHS Grantee Self-Disclosuresndash HHS grantees or subrecipients may voluntarily disclose evidence of potential violations of Federal criminal law
involving fraud bribery or gratuity violations potentially affecting the Federal award 45 CFR 75113 notes mandatory disclosures of criminal offenses that non-Federal entities must make with respect to HHS grants Recipients submitting disclosures in connection with this requirement should include the subject reference line Mandatory Grant Disclosure Recipients choosing to disclose conduct that may not fit squarely within the scope of offenses described in 45 CFR 75113 should include the following subject reference line in the submission Voluntary Grant Disclosure
Medicare 60 day rule
The 60 Day Rule (Medicare Parts A amp B) o The 60 day time period for reportingreturning begins when either
ndash The reasonable diligence is completed orndash On the day the provider received credible information of a potential overpayment (if the
provider fails to conduct reasonable diligence) o For an investigation to be conducted in a ldquotimelyrdquo manner providers typically
must complete the investigation within 6 months from receipt of credible information indicating there may be an overpayment
ndash ndash 6-month timeframe may potentially be extended under ldquoextraordinary circumstancesrdquo ndash 8 months generally the maximum total time to return overpayments The government recommends that providers maintain records documenting ldquoreasonable diligencerdquo
Medicare 60 Day Rule
Six-year lookback period ndash Sometimes possible to use a shorter period depending on the facts at issue Amount to be repaid ndash May vary depending on the method used to
reportreturn eg Medicare administrative contractor (ldquoMACrdquo) v self-disclosure Overpayment notification ndash After receiving an overpayment
notification from the government you should investigate for related overpayments eg other time periods
Medicare 60 Day Rule
Self-disclosure protocols ndashoA submission to the OIG or CMS protocols suspends the 60 day requirement
for returning overpayments until a settlement agreement is executed ndash ndash OIGrsquos Self-Disclosure Protocol (SDP) ndash ndash CMS Voluntary Self-Referral Disclosure Protocol (SRDP) ndash
o Self-disclosures to other agencies do not suspend the repayment deadlinendash ndash Eg Department of Justice local US Attorneyrsquos Office Medicaid Fraud Control Unit
Medicare 60 Day Rule
Facilitating Compliance With the 60 Day Rule Compliance programs should include o ndash Appropriate policies and procedures o ndash Periodic billing and coding audits to proactively identify overpaymentso ndash Focus on high-risk areas o ndash Utilization of publicly available government resources to guide audit efforts o ndash Investigating any suspected incidents of non-compliance with federal health
care program requirements
Self Disclosure
Choice of AgencyoOIG ndash Self-Disclosure Protocol
ndash ndash Conduct involving false billingndash ndash Conduct involving excluded personsndash ndash Conduct involving the Anti-Kickback Statute (including conduct thatndash violates both the AKS and Stark Law)
oCMS ndash Self-Referral Disclosure Protocolndash ndash Conduct involving only violations of the Stark Law
oDOJndash ndash May be appropriate when provider believes a FCA release is necessary
Summary
The Cost of a Well-Executed Coding Audit ProcessThe costs associated with an auditing program are worth it in the long run Ideally your organization is performing audits on a regular basis across all service types locations and payers Weve all seen claims that have been denied resulting in additional work that may be preventable with a proper audit program The goal is to use the audit feedback to improve coding quality and lower potential risk and cost to the organization Organizations should be investing in an effective coding audit program to make your coders and providers better and enhance documentation improvement from the providers
Questions
Thank you for your attentionLynn Handy
Vice President of Coding amp Audit ServicesLynnhandymanagedresourcesinccom

Department Findings Top Issues
Date ofServiceErrors
MissingDocuments
Missing orInvalid
Signature
TeachingPhysician
Errors
InsufficientConsultation
Documents
OverCoding
EMBundled
IntoGlobal
SurgicalPackage
SplitSharedServiceError
Incorrector
MissingPricing
Modifier
ICD-10Errors
Family Practice
CardiologyInternal Medicine
TOTALS
Top Findings by Provider
E amp M Accuracy Rates
ICD-10-CM Accuracy Rates
Procedure Accuracy Rates
Inpatient DRG Audit Report
TABLE OF CONTENTS
Executive Summaryo Scope of Work
Reimbursement Changes Department Results
o InpatientGeneral Recommendations and Comments
o Secondary DiagnosesoProcedure CodingoPresent on AdmissionoQueries
Scope of WorkCodingAID performed coding audit review of 175 inpatient records The review completed was a random sample that included cases coded by twenty coders for dates of service from May 2016 ndash July 2016
The objective was to determine if the medical record documentation supported the following coding and documentation requirements and any other regulatory requirement for that code set Criteria reviewed
1 ICD-10-CM Official Coding Guidelines for accurate diagnosis code reporting 2 ICD-10-PCS Official Coding Guidelines for accurate procedure code reporting 3 Documentation of procedure compared to the CPT code assigned 4 Identify opportunities for education and training 5 Financial impact of current coding practices
The regulatory agencies and reference materials relied upon include the following in addition to Medicare and Medicaid regulations Additional resources are located in the sub sections below
bull ICD-10-CM and ICD-10-PCS for Hospitals current volume bull Centers for Medicare and Medicaid Services CMS NCCI Edits-Centers for Medicaid and
Medicare Services CMS website wwwcmsgov bull AHA Coding Clinic
The following electronic medical record documents were reviewed and relied upon to compare to the actual codes submitted to the third party payer
bull Discharge summaries HampPs Progress Notes and other provider notes located in the EMR Records
bull Patient History Forms Ancillary Staff Notes bull Procedure Notes bull Orders bull Diagnostic Report
Reimbursement Changes
Coder Acct
Billed Audited
Reimbursement ChangesMS DRG SOI ROM Weight Expected
Payment MS DRG SOI ROM Weight Expected Payment
Coder 1 001 790 52300 $2615000 792 21552 $1077600 -$1537400
Coder 2002
749 26452 $1322600 758 10090 $504500 -$818100
Coder 3 003 669 13111 $655550 694 07294 $364700 -$290850
Coder 4 004 389 08707 $435350 394 09502 $475100 $39750
Coder 5 005 312 07630 $381500 812 08572 $428600 $47100
Coder 6 006 384 08481 $424050 378 09949 $497450 $73400
Coder 7 007 206 08164 $408200 794 12987 $649350 $241150
Coder 8008
344 31029 $1551450 853 51334 $2566700 $1015250
TOTAL $7793700 $6564000 -$1229700
General Recommendations and CommentsFinding Pertinent secondary diagnoses are not coded and diagnoses are code which are not supported in provider documentation Code only those diagnoses which are documented by the provider on the current chart Not all codes are coded to the highest degree of specificity and combination codes were sometimes missed
Recommendation It is important to assign codes for all conditions which meet the definition of a reportable diagnosis Documentation from all providers should be used including but not limited to radiologists pathologists anesthesiologists CRNAs and FNPs
Reference Coding Clinic Official Coding Guidelines
bull Report all secondary diagnoses which meet the definition of a secondary diagnosis which is defined as all conditions that coexist at the time of admission that develop subsequently or that affect the treatment received andor the length of stay Codes which enhance the overall picture of the patientrsquos visit should be added
o Add T45515A to report adverse effect of Coumadin which caused the GI bleed
o Add I2690 for septic pulmonary emboli (MCCSOI4ROM4)
o Add N179 for acute kidney failure (S3M2CC) per the nephrology consult and the 628 progress note
o Add code I429 cardiomyopathy per HampP
o Add B964 to report proteus in a UTI per the 620 hospitalist progress note
o Code for D649 anemia and I701 stenosis of renal artery should be added as secondary diagnoses per the HampP
bull Only report diagnoses which are substantiated by provider documentation in the current chart notes If a suspected condition is not verified at discharge on an inpatient account it cannot be coded
o Remove G4734 (idiopathic sleep related non-obstructive alveolar hypoventilation) as patient was noted to have the sleep study and the hypoventilation was shown to be a possibility but not noted as such on discharge
o Remove G629 (S21) the neuropathy is documented as due to diabetes
o Remove K529 colitis noted on HP as possible but not further noted or confirmed at discharge
Procedure CodingFinding Procedures were sometimes coded incorrectly
Recommendation The entire medical record should be reviewed and all procedures coded as documented Coding procedures incorrectly or assigning incorrect CPT codes may result in lost revenue
bull Incorrect root operation
o Revise principal procedure to 0DQ68ZZ for clipping of the ulcer per OP report clipping is root operation repair
bull Biopsy versus Excision
o Procedure 0DBA0ZX (biopsy of jejunum) should change to 0DBA0ZZ (excision of jejunum) per op note this was not a biopsy procedure
bull Coding Guideline error
o Remove 0RG10K0 for allograft due to being inclusive in principal procedure
o Remove codes for adhesiolysis 0DN80ZZ 0UN10ZZ and 0UN90ZZ due to no significance noted per OP report
bull Incorrect approach
o Revise 0TF63ZZ (fragmentation percutaneous approach) to 0TF68ZZ (fragmentation endoscopic) for procedure performed via scope per the operative report
bull Procedure coded without provider documentation
o Remove secondary procedure of excisional debridement (0JB90ZZ) due to lack of documentation of excisional debridement per operative report The header in the operative report documents IampD and debridement but the body of the operative report only documents an IampD
bull Incorrect CPT code assignment
o Post-op note supports the nerve block injections of four nerves therefore code 64421 (multiple nerve block) should replace 64420 (injection of one intercostal nerve)
Queries Finding Conflicting incomplete and vague documentation is found within provider chart notes
Recommendation Prior to code assignment if the coder finds ambiguous or conflicting documentation the provider should be queried
Reference AHA Coding Clinic 2002 2nd Quarter pages 17-18
bull Query for acute blood loss anemia since hgb has dropped and patient is being transfused PRBC
bull Recommend query to clarify if cardiorenal syndrome is current as it is documented per 627 nephrology consult but unclear if current
bull Documentation does not support SIRS noninfectious without organ failure It is conflicting since patient has respiratory failure Query should be initiated for clarification with or without organ failure or infectious or non-infectious Patient has pneumonia per query as well as last progress note therefore if SIRS is not further specified per query PNA should be sequenced as principal diagnosis and SIRS should be removed
bull Recommend provider query necrotizing lung consolidation noted on DS as principal diagnosis-unclear does the patient have lobar pneumonia Secondary dx states necrotic pneumonia which is coded as principal diagnosis-this diagnosis is clear but consolidation portion is unclear
bull Recommend query for preterm labor delivery at 301 weeks
bull RECOMMEND QUERY no chest pain on admit per ER and HP cardiology provider states no CP with ER stating chest pressure the day prior to admit Appears patient was admitted due to elevated troponins which cardiology says are likely due to hypotension and AKI DS states chest pain but also says bradycardia and hypotension were the reason for admit
bull RECOMMEND QUERY no chest pain on admit per ER and HP cardiology provider states no CP with ER stating chest pressure the day prior to admit Appears patient was admitted due to elevated troponins which cardiology says are likely due to hypotension and AKI DS states chest pain but also says bradycardia and hypotension were the reason for admit
bull Query the provider regarding pathology report notation of endometriosis andor possible re-sequence of stenosis as principal diagnosis as it also meets principal diagnosis guidelines This would result in an MS-DRG change to 742 and APR-DRG change to 513
bull QUERY secondary diagnosis MCC and ROM 4 code T3166 (60 TBSA of which 60 are third degree burns) Chart notes do not specify how much of TBSA was actually third degree If after query TBSA is found to be less than 50 (T3164) then ROM will change from 4 to 3 but no change to overall APR-DRG or weight
Auditor Quality amp Productivity
Audit Productivity Standards
It takes twice as long to audit a chart as it does to code it a statistic that takes into account the time to document an explanation of any coding decision the auditor is not in agreement with o For example in an emergency department audit with a productivity of 12
charts per hour for a coder our auditors would probably be able to review six per hour
o If there are multiple services to audit on each encounter the productivity may only be 4 per hour
o The amount of detail you put into your audit report will also be a factorndash Are you using an automated audit softwarendash Are you using a spreadsheet to auditndash How many Systems are needed to complete the audit
Coder Quality Audits
Quality Audits (QA) should be done on your coders and auditors regularly Frequent reviews with smaller sample size will allow more consistent
review and feedbacko Example 10 charts per month per coder if the coder passes 2-3 months
consecutively with 95 or better score move them to quarterly reviewso Some QA programs review a percentage of the coders work This
methodology requires more time and resources
Auditor QA should also score and comment on the accuracy of the audit comments and recommendations
Presenting the Audit Results
Presenting the Audit Results
Communicating the Audit FindingsoWho requested the AuditoWho are you reporting the finding to
ndash CEOndash CFOndash Physicianndash Revenue Cycle Managerndash HIM Directorndash Billing Managerndash Coding Manager
ReportsAudit Resultspptx
Post Audit Education
Provider Education
Provider Education is best received when it is specific to the provider(s) 11 sessions going over the audit result Look at their notes with them
oHighlight areas for documentation improvementoReinforce Coding Guidelines that are specific to themoAsk them to share how they establish their LOS for E amp M serviceso Integrate their EMR system into the training
Provider Education
Group Training SessionsoUse the audit results to identify common issues within a specialty group
ndash Refer to the Executive Summary reportoVery effective for identifying system issues
ndash Teaching Attestationsndash Templatesndash Copy and Pastendash Cloned notes
o Everyone hears the same messagesoAn Issue may not appear on the individual audit but is still a concern for the
group
Education Delivery
In person or remote sessionso Factors to consider
ndash Providers scheduleavailabilityndash Location(s)ndash Personality of the providerndash Budget
Coder Education
Coders do well in group training so they can learn from each other 11 training allows the coder to get feedback on their coding
Handling Audit Disputes
Handling Audit Disputes
Be open to all points of viewo Let the documentation tell the story
Refer to the guidelines Ask
oCan we defend the reported service with the current documentation
Self Disclosures Refunds and Corrected Billing
Overpayment
In general If a person has received an overpayment the person shallo report and return the overpayment to the Secretary the State an
intermediary a carrier or a contractor as appropriate at the correct address and ndash notify the Secretary State intermediary carrier or contractor to whom the overpayment was returned in writing of the reason for the overpayment
What is an ldquoOverpaymentrdquo ndash The term ldquooverpaymentrdquo means any funds that a person receives or retains under subchapter XVIII or XIX of this chapter to which the person after applicable reconciliation is not entitled under such subchapter
Self Disclosure
The Office of Inspector General (OIG) has several self-disclosure processes that can be used to report potential fraud in Department of Health and Human Services (HHS) programs Choose the one that applies to you from the following descriptions to learn moreo Health Care Provider Self-Disclosures
ndash Health care providers suppliers or other individuals or entities subject to Civil Monetary Penalties can use the Provider Self-Disclosure Protocol which was created in 1998 to voluntarily disclose self-discovered evidence of potential fraud Self-disclosure gives providers the opportunity to avoid the costs and disruptions associated with a Government-directed investigation and civil or administrative litigation Visit the Provider Self-Disclosure Protocol webpage for more information
o HHS Contractor Self-Disclosuresndash Contractors are individuals businesses or other legal entities that are awarded Government contracts or
subcontracts to provide services to the Department of Health and Human Services (HHS) OIGs contractor self-disclosure program enables contractors to self-disclose potential violations of the False Claims Act and various Federal criminal laws involving fraud conflict of interest bribery or gratuity This self-disclosure process is available for those entities with a Federal Acquisition Regulation-based contract Visit the Contractor Self-Disclosure webpage for more information
o HHS Grantee Self-Disclosuresndash HHS grantees or subrecipients may voluntarily disclose evidence of potential violations of Federal criminal law
involving fraud bribery or gratuity violations potentially affecting the Federal award 45 CFR 75113 notes mandatory disclosures of criminal offenses that non-Federal entities must make with respect to HHS grants Recipients submitting disclosures in connection with this requirement should include the subject reference line Mandatory Grant Disclosure Recipients choosing to disclose conduct that may not fit squarely within the scope of offenses described in 45 CFR 75113 should include the following subject reference line in the submission Voluntary Grant Disclosure
Medicare 60 day rule
The 60 Day Rule (Medicare Parts A amp B) o The 60 day time period for reportingreturning begins when either
ndash The reasonable diligence is completed orndash On the day the provider received credible information of a potential overpayment (if the
provider fails to conduct reasonable diligence) o For an investigation to be conducted in a ldquotimelyrdquo manner providers typically
must complete the investigation within 6 months from receipt of credible information indicating there may be an overpayment
ndash ndash 6-month timeframe may potentially be extended under ldquoextraordinary circumstancesrdquo ndash 8 months generally the maximum total time to return overpayments The government recommends that providers maintain records documenting ldquoreasonable diligencerdquo
Medicare 60 Day Rule
Six-year lookback period ndash Sometimes possible to use a shorter period depending on the facts at issue Amount to be repaid ndash May vary depending on the method used to
reportreturn eg Medicare administrative contractor (ldquoMACrdquo) v self-disclosure Overpayment notification ndash After receiving an overpayment
notification from the government you should investigate for related overpayments eg other time periods
Medicare 60 Day Rule
Self-disclosure protocols ndashoA submission to the OIG or CMS protocols suspends the 60 day requirement
for returning overpayments until a settlement agreement is executed ndash ndash OIGrsquos Self-Disclosure Protocol (SDP) ndash ndash CMS Voluntary Self-Referral Disclosure Protocol (SRDP) ndash
o Self-disclosures to other agencies do not suspend the repayment deadlinendash ndash Eg Department of Justice local US Attorneyrsquos Office Medicaid Fraud Control Unit
Medicare 60 Day Rule
Facilitating Compliance With the 60 Day Rule Compliance programs should include o ndash Appropriate policies and procedures o ndash Periodic billing and coding audits to proactively identify overpaymentso ndash Focus on high-risk areas o ndash Utilization of publicly available government resources to guide audit efforts o ndash Investigating any suspected incidents of non-compliance with federal health
care program requirements
Self Disclosure
Choice of AgencyoOIG ndash Self-Disclosure Protocol
ndash ndash Conduct involving false billingndash ndash Conduct involving excluded personsndash ndash Conduct involving the Anti-Kickback Statute (including conduct thatndash violates both the AKS and Stark Law)
oCMS ndash Self-Referral Disclosure Protocolndash ndash Conduct involving only violations of the Stark Law
oDOJndash ndash May be appropriate when provider believes a FCA release is necessary
Summary
The Cost of a Well-Executed Coding Audit ProcessThe costs associated with an auditing program are worth it in the long run Ideally your organization is performing audits on a regular basis across all service types locations and payers Weve all seen claims that have been denied resulting in additional work that may be preventable with a proper audit program The goal is to use the audit feedback to improve coding quality and lower potential risk and cost to the organization Organizations should be investing in an effective coding audit program to make your coders and providers better and enhance documentation improvement from the providers
Questions
Thank you for your attentionLynn Handy
Vice President of Coding amp Audit ServicesLynnhandymanagedresourcesinccom

Top Findings by Provider
E amp M Accuracy Rates
ICD-10-CM Accuracy Rates
Procedure Accuracy Rates
Inpatient DRG Audit Report
TABLE OF CONTENTS
Executive Summaryo Scope of Work
Reimbursement Changes Department Results
o InpatientGeneral Recommendations and Comments
o Secondary DiagnosesoProcedure CodingoPresent on AdmissionoQueries
Scope of WorkCodingAID performed coding audit review of 175 inpatient records The review completed was a random sample that included cases coded by twenty coders for dates of service from May 2016 ndash July 2016
The objective was to determine if the medical record documentation supported the following coding and documentation requirements and any other regulatory requirement for that code set Criteria reviewed
1 ICD-10-CM Official Coding Guidelines for accurate diagnosis code reporting 2 ICD-10-PCS Official Coding Guidelines for accurate procedure code reporting 3 Documentation of procedure compared to the CPT code assigned 4 Identify opportunities for education and training 5 Financial impact of current coding practices
The regulatory agencies and reference materials relied upon include the following in addition to Medicare and Medicaid regulations Additional resources are located in the sub sections below
bull ICD-10-CM and ICD-10-PCS for Hospitals current volume bull Centers for Medicare and Medicaid Services CMS NCCI Edits-Centers for Medicaid and
Medicare Services CMS website wwwcmsgov bull AHA Coding Clinic
The following electronic medical record documents were reviewed and relied upon to compare to the actual codes submitted to the third party payer
bull Discharge summaries HampPs Progress Notes and other provider notes located in the EMR Records
bull Patient History Forms Ancillary Staff Notes bull Procedure Notes bull Orders bull Diagnostic Report
Reimbursement Changes
Coder Acct
Billed Audited
Reimbursement ChangesMS DRG SOI ROM Weight Expected
Payment MS DRG SOI ROM Weight Expected Payment
Coder 1 001 790 52300 $2615000 792 21552 $1077600 -$1537400
Coder 2002
749 26452 $1322600 758 10090 $504500 -$818100
Coder 3 003 669 13111 $655550 694 07294 $364700 -$290850
Coder 4 004 389 08707 $435350 394 09502 $475100 $39750
Coder 5 005 312 07630 $381500 812 08572 $428600 $47100
Coder 6 006 384 08481 $424050 378 09949 $497450 $73400
Coder 7 007 206 08164 $408200 794 12987 $649350 $241150
Coder 8008
344 31029 $1551450 853 51334 $2566700 $1015250
TOTAL $7793700 $6564000 -$1229700
General Recommendations and CommentsFinding Pertinent secondary diagnoses are not coded and diagnoses are code which are not supported in provider documentation Code only those diagnoses which are documented by the provider on the current chart Not all codes are coded to the highest degree of specificity and combination codes were sometimes missed
Recommendation It is important to assign codes for all conditions which meet the definition of a reportable diagnosis Documentation from all providers should be used including but not limited to radiologists pathologists anesthesiologists CRNAs and FNPs
Reference Coding Clinic Official Coding Guidelines
bull Report all secondary diagnoses which meet the definition of a secondary diagnosis which is defined as all conditions that coexist at the time of admission that develop subsequently or that affect the treatment received andor the length of stay Codes which enhance the overall picture of the patientrsquos visit should be added
o Add T45515A to report adverse effect of Coumadin which caused the GI bleed
o Add I2690 for septic pulmonary emboli (MCCSOI4ROM4)
o Add N179 for acute kidney failure (S3M2CC) per the nephrology consult and the 628 progress note
o Add code I429 cardiomyopathy per HampP
o Add B964 to report proteus in a UTI per the 620 hospitalist progress note
o Code for D649 anemia and I701 stenosis of renal artery should be added as secondary diagnoses per the HampP
bull Only report diagnoses which are substantiated by provider documentation in the current chart notes If a suspected condition is not verified at discharge on an inpatient account it cannot be coded
o Remove G4734 (idiopathic sleep related non-obstructive alveolar hypoventilation) as patient was noted to have the sleep study and the hypoventilation was shown to be a possibility but not noted as such on discharge
o Remove G629 (S21) the neuropathy is documented as due to diabetes
o Remove K529 colitis noted on HP as possible but not further noted or confirmed at discharge
Procedure CodingFinding Procedures were sometimes coded incorrectly
Recommendation The entire medical record should be reviewed and all procedures coded as documented Coding procedures incorrectly or assigning incorrect CPT codes may result in lost revenue
bull Incorrect root operation
o Revise principal procedure to 0DQ68ZZ for clipping of the ulcer per OP report clipping is root operation repair
bull Biopsy versus Excision
o Procedure 0DBA0ZX (biopsy of jejunum) should change to 0DBA0ZZ (excision of jejunum) per op note this was not a biopsy procedure
bull Coding Guideline error
o Remove 0RG10K0 for allograft due to being inclusive in principal procedure
o Remove codes for adhesiolysis 0DN80ZZ 0UN10ZZ and 0UN90ZZ due to no significance noted per OP report
bull Incorrect approach
o Revise 0TF63ZZ (fragmentation percutaneous approach) to 0TF68ZZ (fragmentation endoscopic) for procedure performed via scope per the operative report
bull Procedure coded without provider documentation
o Remove secondary procedure of excisional debridement (0JB90ZZ) due to lack of documentation of excisional debridement per operative report The header in the operative report documents IampD and debridement but the body of the operative report only documents an IampD
bull Incorrect CPT code assignment
o Post-op note supports the nerve block injections of four nerves therefore code 64421 (multiple nerve block) should replace 64420 (injection of one intercostal nerve)
Queries Finding Conflicting incomplete and vague documentation is found within provider chart notes
Recommendation Prior to code assignment if the coder finds ambiguous or conflicting documentation the provider should be queried
Reference AHA Coding Clinic 2002 2nd Quarter pages 17-18
bull Query for acute blood loss anemia since hgb has dropped and patient is being transfused PRBC
bull Recommend query to clarify if cardiorenal syndrome is current as it is documented per 627 nephrology consult but unclear if current
bull Documentation does not support SIRS noninfectious without organ failure It is conflicting since patient has respiratory failure Query should be initiated for clarification with or without organ failure or infectious or non-infectious Patient has pneumonia per query as well as last progress note therefore if SIRS is not further specified per query PNA should be sequenced as principal diagnosis and SIRS should be removed
bull Recommend provider query necrotizing lung consolidation noted on DS as principal diagnosis-unclear does the patient have lobar pneumonia Secondary dx states necrotic pneumonia which is coded as principal diagnosis-this diagnosis is clear but consolidation portion is unclear
bull Recommend query for preterm labor delivery at 301 weeks
bull RECOMMEND QUERY no chest pain on admit per ER and HP cardiology provider states no CP with ER stating chest pressure the day prior to admit Appears patient was admitted due to elevated troponins which cardiology says are likely due to hypotension and AKI DS states chest pain but also says bradycardia and hypotension were the reason for admit
bull RECOMMEND QUERY no chest pain on admit per ER and HP cardiology provider states no CP with ER stating chest pressure the day prior to admit Appears patient was admitted due to elevated troponins which cardiology says are likely due to hypotension and AKI DS states chest pain but also says bradycardia and hypotension were the reason for admit
bull Query the provider regarding pathology report notation of endometriosis andor possible re-sequence of stenosis as principal diagnosis as it also meets principal diagnosis guidelines This would result in an MS-DRG change to 742 and APR-DRG change to 513
bull QUERY secondary diagnosis MCC and ROM 4 code T3166 (60 TBSA of which 60 are third degree burns) Chart notes do not specify how much of TBSA was actually third degree If after query TBSA is found to be less than 50 (T3164) then ROM will change from 4 to 3 but no change to overall APR-DRG or weight
Auditor Quality amp Productivity
Audit Productivity Standards
It takes twice as long to audit a chart as it does to code it a statistic that takes into account the time to document an explanation of any coding decision the auditor is not in agreement with o For example in an emergency department audit with a productivity of 12
charts per hour for a coder our auditors would probably be able to review six per hour
o If there are multiple services to audit on each encounter the productivity may only be 4 per hour
o The amount of detail you put into your audit report will also be a factorndash Are you using an automated audit softwarendash Are you using a spreadsheet to auditndash How many Systems are needed to complete the audit
Coder Quality Audits
Quality Audits (QA) should be done on your coders and auditors regularly Frequent reviews with smaller sample size will allow more consistent
review and feedbacko Example 10 charts per month per coder if the coder passes 2-3 months
consecutively with 95 or better score move them to quarterly reviewso Some QA programs review a percentage of the coders work This
methodology requires more time and resources
Auditor QA should also score and comment on the accuracy of the audit comments and recommendations
Presenting the Audit Results
Presenting the Audit Results
Communicating the Audit FindingsoWho requested the AuditoWho are you reporting the finding to
ndash CEOndash CFOndash Physicianndash Revenue Cycle Managerndash HIM Directorndash Billing Managerndash Coding Manager
ReportsAudit Resultspptx
Post Audit Education
Provider Education
Provider Education is best received when it is specific to the provider(s) 11 sessions going over the audit result Look at their notes with them
oHighlight areas for documentation improvementoReinforce Coding Guidelines that are specific to themoAsk them to share how they establish their LOS for E amp M serviceso Integrate their EMR system into the training
Provider Education
Group Training SessionsoUse the audit results to identify common issues within a specialty group
ndash Refer to the Executive Summary reportoVery effective for identifying system issues
ndash Teaching Attestationsndash Templatesndash Copy and Pastendash Cloned notes
o Everyone hears the same messagesoAn Issue may not appear on the individual audit but is still a concern for the
group
Education Delivery
In person or remote sessionso Factors to consider
ndash Providers scheduleavailabilityndash Location(s)ndash Personality of the providerndash Budget
Coder Education
Coders do well in group training so they can learn from each other 11 training allows the coder to get feedback on their coding
Handling Audit Disputes
Handling Audit Disputes
Be open to all points of viewo Let the documentation tell the story
Refer to the guidelines Ask
oCan we defend the reported service with the current documentation
Self Disclosures Refunds and Corrected Billing
Overpayment
In general If a person has received an overpayment the person shallo report and return the overpayment to the Secretary the State an
intermediary a carrier or a contractor as appropriate at the correct address and ndash notify the Secretary State intermediary carrier or contractor to whom the overpayment was returned in writing of the reason for the overpayment
What is an ldquoOverpaymentrdquo ndash The term ldquooverpaymentrdquo means any funds that a person receives or retains under subchapter XVIII or XIX of this chapter to which the person after applicable reconciliation is not entitled under such subchapter
Self Disclosure
The Office of Inspector General (OIG) has several self-disclosure processes that can be used to report potential fraud in Department of Health and Human Services (HHS) programs Choose the one that applies to you from the following descriptions to learn moreo Health Care Provider Self-Disclosures
ndash Health care providers suppliers or other individuals or entities subject to Civil Monetary Penalties can use the Provider Self-Disclosure Protocol which was created in 1998 to voluntarily disclose self-discovered evidence of potential fraud Self-disclosure gives providers the opportunity to avoid the costs and disruptions associated with a Government-directed investigation and civil or administrative litigation Visit the Provider Self-Disclosure Protocol webpage for more information
o HHS Contractor Self-Disclosuresndash Contractors are individuals businesses or other legal entities that are awarded Government contracts or
subcontracts to provide services to the Department of Health and Human Services (HHS) OIGs contractor self-disclosure program enables contractors to self-disclose potential violations of the False Claims Act and various Federal criminal laws involving fraud conflict of interest bribery or gratuity This self-disclosure process is available for those entities with a Federal Acquisition Regulation-based contract Visit the Contractor Self-Disclosure webpage for more information
o HHS Grantee Self-Disclosuresndash HHS grantees or subrecipients may voluntarily disclose evidence of potential violations of Federal criminal law
involving fraud bribery or gratuity violations potentially affecting the Federal award 45 CFR 75113 notes mandatory disclosures of criminal offenses that non-Federal entities must make with respect to HHS grants Recipients submitting disclosures in connection with this requirement should include the subject reference line Mandatory Grant Disclosure Recipients choosing to disclose conduct that may not fit squarely within the scope of offenses described in 45 CFR 75113 should include the following subject reference line in the submission Voluntary Grant Disclosure
Medicare 60 day rule
The 60 Day Rule (Medicare Parts A amp B) o The 60 day time period for reportingreturning begins when either
ndash The reasonable diligence is completed orndash On the day the provider received credible information of a potential overpayment (if the
provider fails to conduct reasonable diligence) o For an investigation to be conducted in a ldquotimelyrdquo manner providers typically
must complete the investigation within 6 months from receipt of credible information indicating there may be an overpayment
ndash ndash 6-month timeframe may potentially be extended under ldquoextraordinary circumstancesrdquo ndash 8 months generally the maximum total time to return overpayments The government recommends that providers maintain records documenting ldquoreasonable diligencerdquo
Medicare 60 Day Rule
Six-year lookback period ndash Sometimes possible to use a shorter period depending on the facts at issue Amount to be repaid ndash May vary depending on the method used to
reportreturn eg Medicare administrative contractor (ldquoMACrdquo) v self-disclosure Overpayment notification ndash After receiving an overpayment
notification from the government you should investigate for related overpayments eg other time periods
Medicare 60 Day Rule
Self-disclosure protocols ndashoA submission to the OIG or CMS protocols suspends the 60 day requirement
for returning overpayments until a settlement agreement is executed ndash ndash OIGrsquos Self-Disclosure Protocol (SDP) ndash ndash CMS Voluntary Self-Referral Disclosure Protocol (SRDP) ndash
o Self-disclosures to other agencies do not suspend the repayment deadlinendash ndash Eg Department of Justice local US Attorneyrsquos Office Medicaid Fraud Control Unit
Medicare 60 Day Rule
Facilitating Compliance With the 60 Day Rule Compliance programs should include o ndash Appropriate policies and procedures o ndash Periodic billing and coding audits to proactively identify overpaymentso ndash Focus on high-risk areas o ndash Utilization of publicly available government resources to guide audit efforts o ndash Investigating any suspected incidents of non-compliance with federal health
care program requirements
Self Disclosure
Choice of AgencyoOIG ndash Self-Disclosure Protocol
ndash ndash Conduct involving false billingndash ndash Conduct involving excluded personsndash ndash Conduct involving the Anti-Kickback Statute (including conduct thatndash violates both the AKS and Stark Law)
oCMS ndash Self-Referral Disclosure Protocolndash ndash Conduct involving only violations of the Stark Law
oDOJndash ndash May be appropriate when provider believes a FCA release is necessary
Summary
The Cost of a Well-Executed Coding Audit ProcessThe costs associated with an auditing program are worth it in the long run Ideally your organization is performing audits on a regular basis across all service types locations and payers Weve all seen claims that have been denied resulting in additional work that may be preventable with a proper audit program The goal is to use the audit feedback to improve coding quality and lower potential risk and cost to the organization Organizations should be investing in an effective coding audit program to make your coders and providers better and enhance documentation improvement from the providers
Questions
Thank you for your attentionLynn Handy
Vice President of Coding amp Audit ServicesLynnhandymanagedresourcesinccom

E amp M Accuracy Rates
ICD-10-CM Accuracy Rates
Procedure Accuracy Rates
Inpatient DRG Audit Report
TABLE OF CONTENTS
Executive Summaryo Scope of Work
Reimbursement Changes Department Results
o InpatientGeneral Recommendations and Comments
o Secondary DiagnosesoProcedure CodingoPresent on AdmissionoQueries
Scope of WorkCodingAID performed coding audit review of 175 inpatient records The review completed was a random sample that included cases coded by twenty coders for dates of service from May 2016 ndash July 2016
The objective was to determine if the medical record documentation supported the following coding and documentation requirements and any other regulatory requirement for that code set Criteria reviewed
1 ICD-10-CM Official Coding Guidelines for accurate diagnosis code reporting 2 ICD-10-PCS Official Coding Guidelines for accurate procedure code reporting 3 Documentation of procedure compared to the CPT code assigned 4 Identify opportunities for education and training 5 Financial impact of current coding practices
The regulatory agencies and reference materials relied upon include the following in addition to Medicare and Medicaid regulations Additional resources are located in the sub sections below
bull ICD-10-CM and ICD-10-PCS for Hospitals current volume bull Centers for Medicare and Medicaid Services CMS NCCI Edits-Centers for Medicaid and
Medicare Services CMS website wwwcmsgov bull AHA Coding Clinic
The following electronic medical record documents were reviewed and relied upon to compare to the actual codes submitted to the third party payer
bull Discharge summaries HampPs Progress Notes and other provider notes located in the EMR Records
bull Patient History Forms Ancillary Staff Notes bull Procedure Notes bull Orders bull Diagnostic Report
Reimbursement Changes
Coder Acct
Billed Audited
Reimbursement ChangesMS DRG SOI ROM Weight Expected
Payment MS DRG SOI ROM Weight Expected Payment
Coder 1 001 790 52300 $2615000 792 21552 $1077600 -$1537400
Coder 2002
749 26452 $1322600 758 10090 $504500 -$818100
Coder 3 003 669 13111 $655550 694 07294 $364700 -$290850
Coder 4 004 389 08707 $435350 394 09502 $475100 $39750
Coder 5 005 312 07630 $381500 812 08572 $428600 $47100
Coder 6 006 384 08481 $424050 378 09949 $497450 $73400
Coder 7 007 206 08164 $408200 794 12987 $649350 $241150
Coder 8008
344 31029 $1551450 853 51334 $2566700 $1015250
TOTAL $7793700 $6564000 -$1229700
General Recommendations and CommentsFinding Pertinent secondary diagnoses are not coded and diagnoses are code which are not supported in provider documentation Code only those diagnoses which are documented by the provider on the current chart Not all codes are coded to the highest degree of specificity and combination codes were sometimes missed
Recommendation It is important to assign codes for all conditions which meet the definition of a reportable diagnosis Documentation from all providers should be used including but not limited to radiologists pathologists anesthesiologists CRNAs and FNPs
Reference Coding Clinic Official Coding Guidelines
bull Report all secondary diagnoses which meet the definition of a secondary diagnosis which is defined as all conditions that coexist at the time of admission that develop subsequently or that affect the treatment received andor the length of stay Codes which enhance the overall picture of the patientrsquos visit should be added
o Add T45515A to report adverse effect of Coumadin which caused the GI bleed
o Add I2690 for septic pulmonary emboli (MCCSOI4ROM4)
o Add N179 for acute kidney failure (S3M2CC) per the nephrology consult and the 628 progress note
o Add code I429 cardiomyopathy per HampP
o Add B964 to report proteus in a UTI per the 620 hospitalist progress note
o Code for D649 anemia and I701 stenosis of renal artery should be added as secondary diagnoses per the HampP
bull Only report diagnoses which are substantiated by provider documentation in the current chart notes If a suspected condition is not verified at discharge on an inpatient account it cannot be coded
o Remove G4734 (idiopathic sleep related non-obstructive alveolar hypoventilation) as patient was noted to have the sleep study and the hypoventilation was shown to be a possibility but not noted as such on discharge
o Remove G629 (S21) the neuropathy is documented as due to diabetes
o Remove K529 colitis noted on HP as possible but not further noted or confirmed at discharge
Procedure CodingFinding Procedures were sometimes coded incorrectly
Recommendation The entire medical record should be reviewed and all procedures coded as documented Coding procedures incorrectly or assigning incorrect CPT codes may result in lost revenue
bull Incorrect root operation
o Revise principal procedure to 0DQ68ZZ for clipping of the ulcer per OP report clipping is root operation repair
bull Biopsy versus Excision
o Procedure 0DBA0ZX (biopsy of jejunum) should change to 0DBA0ZZ (excision of jejunum) per op note this was not a biopsy procedure
bull Coding Guideline error
o Remove 0RG10K0 for allograft due to being inclusive in principal procedure
o Remove codes for adhesiolysis 0DN80ZZ 0UN10ZZ and 0UN90ZZ due to no significance noted per OP report
bull Incorrect approach
o Revise 0TF63ZZ (fragmentation percutaneous approach) to 0TF68ZZ (fragmentation endoscopic) for procedure performed via scope per the operative report
bull Procedure coded without provider documentation
o Remove secondary procedure of excisional debridement (0JB90ZZ) due to lack of documentation of excisional debridement per operative report The header in the operative report documents IampD and debridement but the body of the operative report only documents an IampD
bull Incorrect CPT code assignment
o Post-op note supports the nerve block injections of four nerves therefore code 64421 (multiple nerve block) should replace 64420 (injection of one intercostal nerve)
Queries Finding Conflicting incomplete and vague documentation is found within provider chart notes
Recommendation Prior to code assignment if the coder finds ambiguous or conflicting documentation the provider should be queried
Reference AHA Coding Clinic 2002 2nd Quarter pages 17-18
bull Query for acute blood loss anemia since hgb has dropped and patient is being transfused PRBC
bull Recommend query to clarify if cardiorenal syndrome is current as it is documented per 627 nephrology consult but unclear if current
bull Documentation does not support SIRS noninfectious without organ failure It is conflicting since patient has respiratory failure Query should be initiated for clarification with or without organ failure or infectious or non-infectious Patient has pneumonia per query as well as last progress note therefore if SIRS is not further specified per query PNA should be sequenced as principal diagnosis and SIRS should be removed
bull Recommend provider query necrotizing lung consolidation noted on DS as principal diagnosis-unclear does the patient have lobar pneumonia Secondary dx states necrotic pneumonia which is coded as principal diagnosis-this diagnosis is clear but consolidation portion is unclear
bull Recommend query for preterm labor delivery at 301 weeks
bull RECOMMEND QUERY no chest pain on admit per ER and HP cardiology provider states no CP with ER stating chest pressure the day prior to admit Appears patient was admitted due to elevated troponins which cardiology says are likely due to hypotension and AKI DS states chest pain but also says bradycardia and hypotension were the reason for admit
bull RECOMMEND QUERY no chest pain on admit per ER and HP cardiology provider states no CP with ER stating chest pressure the day prior to admit Appears patient was admitted due to elevated troponins which cardiology says are likely due to hypotension and AKI DS states chest pain but also says bradycardia and hypotension were the reason for admit
bull Query the provider regarding pathology report notation of endometriosis andor possible re-sequence of stenosis as principal diagnosis as it also meets principal diagnosis guidelines This would result in an MS-DRG change to 742 and APR-DRG change to 513
bull QUERY secondary diagnosis MCC and ROM 4 code T3166 (60 TBSA of which 60 are third degree burns) Chart notes do not specify how much of TBSA was actually third degree If after query TBSA is found to be less than 50 (T3164) then ROM will change from 4 to 3 but no change to overall APR-DRG or weight
Auditor Quality amp Productivity
Audit Productivity Standards
It takes twice as long to audit a chart as it does to code it a statistic that takes into account the time to document an explanation of any coding decision the auditor is not in agreement with o For example in an emergency department audit with a productivity of 12
charts per hour for a coder our auditors would probably be able to review six per hour
o If there are multiple services to audit on each encounter the productivity may only be 4 per hour
o The amount of detail you put into your audit report will also be a factorndash Are you using an automated audit softwarendash Are you using a spreadsheet to auditndash How many Systems are needed to complete the audit
Coder Quality Audits
Quality Audits (QA) should be done on your coders and auditors regularly Frequent reviews with smaller sample size will allow more consistent
review and feedbacko Example 10 charts per month per coder if the coder passes 2-3 months
consecutively with 95 or better score move them to quarterly reviewso Some QA programs review a percentage of the coders work This
methodology requires more time and resources
Auditor QA should also score and comment on the accuracy of the audit comments and recommendations
Presenting the Audit Results
Presenting the Audit Results
Communicating the Audit FindingsoWho requested the AuditoWho are you reporting the finding to
ndash CEOndash CFOndash Physicianndash Revenue Cycle Managerndash HIM Directorndash Billing Managerndash Coding Manager
ReportsAudit Resultspptx
Post Audit Education
Provider Education
Provider Education is best received when it is specific to the provider(s) 11 sessions going over the audit result Look at their notes with them
oHighlight areas for documentation improvementoReinforce Coding Guidelines that are specific to themoAsk them to share how they establish their LOS for E amp M serviceso Integrate their EMR system into the training
Provider Education
Group Training SessionsoUse the audit results to identify common issues within a specialty group
ndash Refer to the Executive Summary reportoVery effective for identifying system issues
ndash Teaching Attestationsndash Templatesndash Copy and Pastendash Cloned notes
o Everyone hears the same messagesoAn Issue may not appear on the individual audit but is still a concern for the
group
Education Delivery
In person or remote sessionso Factors to consider
ndash Providers scheduleavailabilityndash Location(s)ndash Personality of the providerndash Budget
Coder Education
Coders do well in group training so they can learn from each other 11 training allows the coder to get feedback on their coding
Handling Audit Disputes
Handling Audit Disputes
Be open to all points of viewo Let the documentation tell the story
Refer to the guidelines Ask
oCan we defend the reported service with the current documentation
Self Disclosures Refunds and Corrected Billing
Overpayment
In general If a person has received an overpayment the person shallo report and return the overpayment to the Secretary the State an
intermediary a carrier or a contractor as appropriate at the correct address and ndash notify the Secretary State intermediary carrier or contractor to whom the overpayment was returned in writing of the reason for the overpayment
What is an ldquoOverpaymentrdquo ndash The term ldquooverpaymentrdquo means any funds that a person receives or retains under subchapter XVIII or XIX of this chapter to which the person after applicable reconciliation is not entitled under such subchapter
Self Disclosure
The Office of Inspector General (OIG) has several self-disclosure processes that can be used to report potential fraud in Department of Health and Human Services (HHS) programs Choose the one that applies to you from the following descriptions to learn moreo Health Care Provider Self-Disclosures
ndash Health care providers suppliers or other individuals or entities subject to Civil Monetary Penalties can use the Provider Self-Disclosure Protocol which was created in 1998 to voluntarily disclose self-discovered evidence of potential fraud Self-disclosure gives providers the opportunity to avoid the costs and disruptions associated with a Government-directed investigation and civil or administrative litigation Visit the Provider Self-Disclosure Protocol webpage for more information
o HHS Contractor Self-Disclosuresndash Contractors are individuals businesses or other legal entities that are awarded Government contracts or
subcontracts to provide services to the Department of Health and Human Services (HHS) OIGs contractor self-disclosure program enables contractors to self-disclose potential violations of the False Claims Act and various Federal criminal laws involving fraud conflict of interest bribery or gratuity This self-disclosure process is available for those entities with a Federal Acquisition Regulation-based contract Visit the Contractor Self-Disclosure webpage for more information
o HHS Grantee Self-Disclosuresndash HHS grantees or subrecipients may voluntarily disclose evidence of potential violations of Federal criminal law
involving fraud bribery or gratuity violations potentially affecting the Federal award 45 CFR 75113 notes mandatory disclosures of criminal offenses that non-Federal entities must make with respect to HHS grants Recipients submitting disclosures in connection with this requirement should include the subject reference line Mandatory Grant Disclosure Recipients choosing to disclose conduct that may not fit squarely within the scope of offenses described in 45 CFR 75113 should include the following subject reference line in the submission Voluntary Grant Disclosure
Medicare 60 day rule
The 60 Day Rule (Medicare Parts A amp B) o The 60 day time period for reportingreturning begins when either
ndash The reasonable diligence is completed orndash On the day the provider received credible information of a potential overpayment (if the
provider fails to conduct reasonable diligence) o For an investigation to be conducted in a ldquotimelyrdquo manner providers typically
must complete the investigation within 6 months from receipt of credible information indicating there may be an overpayment
ndash ndash 6-month timeframe may potentially be extended under ldquoextraordinary circumstancesrdquo ndash 8 months generally the maximum total time to return overpayments The government recommends that providers maintain records documenting ldquoreasonable diligencerdquo
Medicare 60 Day Rule
Six-year lookback period ndash Sometimes possible to use a shorter period depending on the facts at issue Amount to be repaid ndash May vary depending on the method used to
reportreturn eg Medicare administrative contractor (ldquoMACrdquo) v self-disclosure Overpayment notification ndash After receiving an overpayment
notification from the government you should investigate for related overpayments eg other time periods
Medicare 60 Day Rule
Self-disclosure protocols ndashoA submission to the OIG or CMS protocols suspends the 60 day requirement
for returning overpayments until a settlement agreement is executed ndash ndash OIGrsquos Self-Disclosure Protocol (SDP) ndash ndash CMS Voluntary Self-Referral Disclosure Protocol (SRDP) ndash
o Self-disclosures to other agencies do not suspend the repayment deadlinendash ndash Eg Department of Justice local US Attorneyrsquos Office Medicaid Fraud Control Unit
Medicare 60 Day Rule
Facilitating Compliance With the 60 Day Rule Compliance programs should include o ndash Appropriate policies and procedures o ndash Periodic billing and coding audits to proactively identify overpaymentso ndash Focus on high-risk areas o ndash Utilization of publicly available government resources to guide audit efforts o ndash Investigating any suspected incidents of non-compliance with federal health
care program requirements
Self Disclosure
Choice of AgencyoOIG ndash Self-Disclosure Protocol
ndash ndash Conduct involving false billingndash ndash Conduct involving excluded personsndash ndash Conduct involving the Anti-Kickback Statute (including conduct thatndash violates both the AKS and Stark Law)
oCMS ndash Self-Referral Disclosure Protocolndash ndash Conduct involving only violations of the Stark Law
oDOJndash ndash May be appropriate when provider believes a FCA release is necessary
Summary
The Cost of a Well-Executed Coding Audit ProcessThe costs associated with an auditing program are worth it in the long run Ideally your organization is performing audits on a regular basis across all service types locations and payers Weve all seen claims that have been denied resulting in additional work that may be preventable with a proper audit program The goal is to use the audit feedback to improve coding quality and lower potential risk and cost to the organization Organizations should be investing in an effective coding audit program to make your coders and providers better and enhance documentation improvement from the providers
Questions
Thank you for your attentionLynn Handy
Vice President of Coding amp Audit ServicesLynnhandymanagedresourcesinccom

ICD-10-CM Accuracy Rates
Procedure Accuracy Rates
Inpatient DRG Audit Report
TABLE OF CONTENTS
Executive Summaryo Scope of Work
Reimbursement Changes Department Results
o InpatientGeneral Recommendations and Comments
o Secondary DiagnosesoProcedure CodingoPresent on AdmissionoQueries
Scope of WorkCodingAID performed coding audit review of 175 inpatient records The review completed was a random sample that included cases coded by twenty coders for dates of service from May 2016 ndash July 2016
The objective was to determine if the medical record documentation supported the following coding and documentation requirements and any other regulatory requirement for that code set Criteria reviewed
1 ICD-10-CM Official Coding Guidelines for accurate diagnosis code reporting 2 ICD-10-PCS Official Coding Guidelines for accurate procedure code reporting 3 Documentation of procedure compared to the CPT code assigned 4 Identify opportunities for education and training 5 Financial impact of current coding practices
The regulatory agencies and reference materials relied upon include the following in addition to Medicare and Medicaid regulations Additional resources are located in the sub sections below
bull ICD-10-CM and ICD-10-PCS for Hospitals current volume bull Centers for Medicare and Medicaid Services CMS NCCI Edits-Centers for Medicaid and
Medicare Services CMS website wwwcmsgov bull AHA Coding Clinic
The following electronic medical record documents were reviewed and relied upon to compare to the actual codes submitted to the third party payer
bull Discharge summaries HampPs Progress Notes and other provider notes located in the EMR Records
bull Patient History Forms Ancillary Staff Notes bull Procedure Notes bull Orders bull Diagnostic Report
Reimbursement Changes
Coder Acct
Billed Audited
Reimbursement ChangesMS DRG SOI ROM Weight Expected
Payment MS DRG SOI ROM Weight Expected Payment
Coder 1 001 790 52300 $2615000 792 21552 $1077600 -$1537400
Coder 2002
749 26452 $1322600 758 10090 $504500 -$818100
Coder 3 003 669 13111 $655550 694 07294 $364700 -$290850
Coder 4 004 389 08707 $435350 394 09502 $475100 $39750
Coder 5 005 312 07630 $381500 812 08572 $428600 $47100
Coder 6 006 384 08481 $424050 378 09949 $497450 $73400
Coder 7 007 206 08164 $408200 794 12987 $649350 $241150
Coder 8008
344 31029 $1551450 853 51334 $2566700 $1015250
TOTAL $7793700 $6564000 -$1229700
General Recommendations and CommentsFinding Pertinent secondary diagnoses are not coded and diagnoses are code which are not supported in provider documentation Code only those diagnoses which are documented by the provider on the current chart Not all codes are coded to the highest degree of specificity and combination codes were sometimes missed
Recommendation It is important to assign codes for all conditions which meet the definition of a reportable diagnosis Documentation from all providers should be used including but not limited to radiologists pathologists anesthesiologists CRNAs and FNPs
Reference Coding Clinic Official Coding Guidelines
bull Report all secondary diagnoses which meet the definition of a secondary diagnosis which is defined as all conditions that coexist at the time of admission that develop subsequently or that affect the treatment received andor the length of stay Codes which enhance the overall picture of the patientrsquos visit should be added
o Add T45515A to report adverse effect of Coumadin which caused the GI bleed
o Add I2690 for septic pulmonary emboli (MCCSOI4ROM4)
o Add N179 for acute kidney failure (S3M2CC) per the nephrology consult and the 628 progress note
o Add code I429 cardiomyopathy per HampP
o Add B964 to report proteus in a UTI per the 620 hospitalist progress note
o Code for D649 anemia and I701 stenosis of renal artery should be added as secondary diagnoses per the HampP
bull Only report diagnoses which are substantiated by provider documentation in the current chart notes If a suspected condition is not verified at discharge on an inpatient account it cannot be coded
o Remove G4734 (idiopathic sleep related non-obstructive alveolar hypoventilation) as patient was noted to have the sleep study and the hypoventilation was shown to be a possibility but not noted as such on discharge
o Remove G629 (S21) the neuropathy is documented as due to diabetes
o Remove K529 colitis noted on HP as possible but not further noted or confirmed at discharge
Procedure CodingFinding Procedures were sometimes coded incorrectly
Recommendation The entire medical record should be reviewed and all procedures coded as documented Coding procedures incorrectly or assigning incorrect CPT codes may result in lost revenue
bull Incorrect root operation
o Revise principal procedure to 0DQ68ZZ for clipping of the ulcer per OP report clipping is root operation repair
bull Biopsy versus Excision
o Procedure 0DBA0ZX (biopsy of jejunum) should change to 0DBA0ZZ (excision of jejunum) per op note this was not a biopsy procedure
bull Coding Guideline error
o Remove 0RG10K0 for allograft due to being inclusive in principal procedure
o Remove codes for adhesiolysis 0DN80ZZ 0UN10ZZ and 0UN90ZZ due to no significance noted per OP report
bull Incorrect approach
o Revise 0TF63ZZ (fragmentation percutaneous approach) to 0TF68ZZ (fragmentation endoscopic) for procedure performed via scope per the operative report
bull Procedure coded without provider documentation
o Remove secondary procedure of excisional debridement (0JB90ZZ) due to lack of documentation of excisional debridement per operative report The header in the operative report documents IampD and debridement but the body of the operative report only documents an IampD
bull Incorrect CPT code assignment
o Post-op note supports the nerve block injections of four nerves therefore code 64421 (multiple nerve block) should replace 64420 (injection of one intercostal nerve)
Queries Finding Conflicting incomplete and vague documentation is found within provider chart notes
Recommendation Prior to code assignment if the coder finds ambiguous or conflicting documentation the provider should be queried
Reference AHA Coding Clinic 2002 2nd Quarter pages 17-18
bull Query for acute blood loss anemia since hgb has dropped and patient is being transfused PRBC
bull Recommend query to clarify if cardiorenal syndrome is current as it is documented per 627 nephrology consult but unclear if current
bull Documentation does not support SIRS noninfectious without organ failure It is conflicting since patient has respiratory failure Query should be initiated for clarification with or without organ failure or infectious or non-infectious Patient has pneumonia per query as well as last progress note therefore if SIRS is not further specified per query PNA should be sequenced as principal diagnosis and SIRS should be removed
bull Recommend provider query necrotizing lung consolidation noted on DS as principal diagnosis-unclear does the patient have lobar pneumonia Secondary dx states necrotic pneumonia which is coded as principal diagnosis-this diagnosis is clear but consolidation portion is unclear
bull Recommend query for preterm labor delivery at 301 weeks
bull RECOMMEND QUERY no chest pain on admit per ER and HP cardiology provider states no CP with ER stating chest pressure the day prior to admit Appears patient was admitted due to elevated troponins which cardiology says are likely due to hypotension and AKI DS states chest pain but also says bradycardia and hypotension were the reason for admit
bull RECOMMEND QUERY no chest pain on admit per ER and HP cardiology provider states no CP with ER stating chest pressure the day prior to admit Appears patient was admitted due to elevated troponins which cardiology says are likely due to hypotension and AKI DS states chest pain but also says bradycardia and hypotension were the reason for admit
bull Query the provider regarding pathology report notation of endometriosis andor possible re-sequence of stenosis as principal diagnosis as it also meets principal diagnosis guidelines This would result in an MS-DRG change to 742 and APR-DRG change to 513
bull QUERY secondary diagnosis MCC and ROM 4 code T3166 (60 TBSA of which 60 are third degree burns) Chart notes do not specify how much of TBSA was actually third degree If after query TBSA is found to be less than 50 (T3164) then ROM will change from 4 to 3 but no change to overall APR-DRG or weight
Auditor Quality amp Productivity
Audit Productivity Standards
It takes twice as long to audit a chart as it does to code it a statistic that takes into account the time to document an explanation of any coding decision the auditor is not in agreement with o For example in an emergency department audit with a productivity of 12
charts per hour for a coder our auditors would probably be able to review six per hour
o If there are multiple services to audit on each encounter the productivity may only be 4 per hour
o The amount of detail you put into your audit report will also be a factorndash Are you using an automated audit softwarendash Are you using a spreadsheet to auditndash How many Systems are needed to complete the audit
Coder Quality Audits
Quality Audits (QA) should be done on your coders and auditors regularly Frequent reviews with smaller sample size will allow more consistent
review and feedbacko Example 10 charts per month per coder if the coder passes 2-3 months
consecutively with 95 or better score move them to quarterly reviewso Some QA programs review a percentage of the coders work This
methodology requires more time and resources
Auditor QA should also score and comment on the accuracy of the audit comments and recommendations
Presenting the Audit Results
Presenting the Audit Results
Communicating the Audit FindingsoWho requested the AuditoWho are you reporting the finding to
ndash CEOndash CFOndash Physicianndash Revenue Cycle Managerndash HIM Directorndash Billing Managerndash Coding Manager
ReportsAudit Resultspptx
Post Audit Education
Provider Education
Provider Education is best received when it is specific to the provider(s) 11 sessions going over the audit result Look at their notes with them
oHighlight areas for documentation improvementoReinforce Coding Guidelines that are specific to themoAsk them to share how they establish their LOS for E amp M serviceso Integrate their EMR system into the training
Provider Education
Group Training SessionsoUse the audit results to identify common issues within a specialty group
ndash Refer to the Executive Summary reportoVery effective for identifying system issues
ndash Teaching Attestationsndash Templatesndash Copy and Pastendash Cloned notes
o Everyone hears the same messagesoAn Issue may not appear on the individual audit but is still a concern for the
group
Education Delivery
In person or remote sessionso Factors to consider
ndash Providers scheduleavailabilityndash Location(s)ndash Personality of the providerndash Budget
Coder Education
Coders do well in group training so they can learn from each other 11 training allows the coder to get feedback on their coding
Handling Audit Disputes
Handling Audit Disputes
Be open to all points of viewo Let the documentation tell the story
Refer to the guidelines Ask
oCan we defend the reported service with the current documentation
Self Disclosures Refunds and Corrected Billing
Overpayment
In general If a person has received an overpayment the person shallo report and return the overpayment to the Secretary the State an
intermediary a carrier or a contractor as appropriate at the correct address and ndash notify the Secretary State intermediary carrier or contractor to whom the overpayment was returned in writing of the reason for the overpayment
What is an ldquoOverpaymentrdquo ndash The term ldquooverpaymentrdquo means any funds that a person receives or retains under subchapter XVIII or XIX of this chapter to which the person after applicable reconciliation is not entitled under such subchapter
Self Disclosure
The Office of Inspector General (OIG) has several self-disclosure processes that can be used to report potential fraud in Department of Health and Human Services (HHS) programs Choose the one that applies to you from the following descriptions to learn moreo Health Care Provider Self-Disclosures
ndash Health care providers suppliers or other individuals or entities subject to Civil Monetary Penalties can use the Provider Self-Disclosure Protocol which was created in 1998 to voluntarily disclose self-discovered evidence of potential fraud Self-disclosure gives providers the opportunity to avoid the costs and disruptions associated with a Government-directed investigation and civil or administrative litigation Visit the Provider Self-Disclosure Protocol webpage for more information
o HHS Contractor Self-Disclosuresndash Contractors are individuals businesses or other legal entities that are awarded Government contracts or
subcontracts to provide services to the Department of Health and Human Services (HHS) OIGs contractor self-disclosure program enables contractors to self-disclose potential violations of the False Claims Act and various Federal criminal laws involving fraud conflict of interest bribery or gratuity This self-disclosure process is available for those entities with a Federal Acquisition Regulation-based contract Visit the Contractor Self-Disclosure webpage for more information
o HHS Grantee Self-Disclosuresndash HHS grantees or subrecipients may voluntarily disclose evidence of potential violations of Federal criminal law
involving fraud bribery or gratuity violations potentially affecting the Federal award 45 CFR 75113 notes mandatory disclosures of criminal offenses that non-Federal entities must make with respect to HHS grants Recipients submitting disclosures in connection with this requirement should include the subject reference line Mandatory Grant Disclosure Recipients choosing to disclose conduct that may not fit squarely within the scope of offenses described in 45 CFR 75113 should include the following subject reference line in the submission Voluntary Grant Disclosure
Medicare 60 day rule
The 60 Day Rule (Medicare Parts A amp B) o The 60 day time period for reportingreturning begins when either
ndash The reasonable diligence is completed orndash On the day the provider received credible information of a potential overpayment (if the
provider fails to conduct reasonable diligence) o For an investigation to be conducted in a ldquotimelyrdquo manner providers typically
must complete the investigation within 6 months from receipt of credible information indicating there may be an overpayment
ndash ndash 6-month timeframe may potentially be extended under ldquoextraordinary circumstancesrdquo ndash 8 months generally the maximum total time to return overpayments The government recommends that providers maintain records documenting ldquoreasonable diligencerdquo
Medicare 60 Day Rule
Six-year lookback period ndash Sometimes possible to use a shorter period depending on the facts at issue Amount to be repaid ndash May vary depending on the method used to
reportreturn eg Medicare administrative contractor (ldquoMACrdquo) v self-disclosure Overpayment notification ndash After receiving an overpayment
notification from the government you should investigate for related overpayments eg other time periods
Medicare 60 Day Rule
Self-disclosure protocols ndashoA submission to the OIG or CMS protocols suspends the 60 day requirement
for returning overpayments until a settlement agreement is executed ndash ndash OIGrsquos Self-Disclosure Protocol (SDP) ndash ndash CMS Voluntary Self-Referral Disclosure Protocol (SRDP) ndash
o Self-disclosures to other agencies do not suspend the repayment deadlinendash ndash Eg Department of Justice local US Attorneyrsquos Office Medicaid Fraud Control Unit
Medicare 60 Day Rule
Facilitating Compliance With the 60 Day Rule Compliance programs should include o ndash Appropriate policies and procedures o ndash Periodic billing and coding audits to proactively identify overpaymentso ndash Focus on high-risk areas o ndash Utilization of publicly available government resources to guide audit efforts o ndash Investigating any suspected incidents of non-compliance with federal health
care program requirements
Self Disclosure
Choice of AgencyoOIG ndash Self-Disclosure Protocol
ndash ndash Conduct involving false billingndash ndash Conduct involving excluded personsndash ndash Conduct involving the Anti-Kickback Statute (including conduct thatndash violates both the AKS and Stark Law)
oCMS ndash Self-Referral Disclosure Protocolndash ndash Conduct involving only violations of the Stark Law
oDOJndash ndash May be appropriate when provider believes a FCA release is necessary
Summary
The Cost of a Well-Executed Coding Audit ProcessThe costs associated with an auditing program are worth it in the long run Ideally your organization is performing audits on a regular basis across all service types locations and payers Weve all seen claims that have been denied resulting in additional work that may be preventable with a proper audit program The goal is to use the audit feedback to improve coding quality and lower potential risk and cost to the organization Organizations should be investing in an effective coding audit program to make your coders and providers better and enhance documentation improvement from the providers
Questions
Thank you for your attentionLynn Handy
Vice President of Coding amp Audit ServicesLynnhandymanagedresourcesinccom

Procedure Accuracy Rates
Inpatient DRG Audit Report
TABLE OF CONTENTS
Executive Summaryo Scope of Work
Reimbursement Changes Department Results
o InpatientGeneral Recommendations and Comments
o Secondary DiagnosesoProcedure CodingoPresent on AdmissionoQueries
Scope of WorkCodingAID performed coding audit review of 175 inpatient records The review completed was a random sample that included cases coded by twenty coders for dates of service from May 2016 ndash July 2016
The objective was to determine if the medical record documentation supported the following coding and documentation requirements and any other regulatory requirement for that code set Criteria reviewed
1 ICD-10-CM Official Coding Guidelines for accurate diagnosis code reporting 2 ICD-10-PCS Official Coding Guidelines for accurate procedure code reporting 3 Documentation of procedure compared to the CPT code assigned 4 Identify opportunities for education and training 5 Financial impact of current coding practices
The regulatory agencies and reference materials relied upon include the following in addition to Medicare and Medicaid regulations Additional resources are located in the sub sections below
bull ICD-10-CM and ICD-10-PCS for Hospitals current volume bull Centers for Medicare and Medicaid Services CMS NCCI Edits-Centers for Medicaid and
Medicare Services CMS website wwwcmsgov bull AHA Coding Clinic
The following electronic medical record documents were reviewed and relied upon to compare to the actual codes submitted to the third party payer
bull Discharge summaries HampPs Progress Notes and other provider notes located in the EMR Records
bull Patient History Forms Ancillary Staff Notes bull Procedure Notes bull Orders bull Diagnostic Report
Reimbursement Changes
Coder Acct
Billed Audited
Reimbursement ChangesMS DRG SOI ROM Weight Expected
Payment MS DRG SOI ROM Weight Expected Payment
Coder 1 001 790 52300 $2615000 792 21552 $1077600 -$1537400
Coder 2002
749 26452 $1322600 758 10090 $504500 -$818100
Coder 3 003 669 13111 $655550 694 07294 $364700 -$290850
Coder 4 004 389 08707 $435350 394 09502 $475100 $39750
Coder 5 005 312 07630 $381500 812 08572 $428600 $47100
Coder 6 006 384 08481 $424050 378 09949 $497450 $73400
Coder 7 007 206 08164 $408200 794 12987 $649350 $241150
Coder 8008
344 31029 $1551450 853 51334 $2566700 $1015250
TOTAL $7793700 $6564000 -$1229700
General Recommendations and CommentsFinding Pertinent secondary diagnoses are not coded and diagnoses are code which are not supported in provider documentation Code only those diagnoses which are documented by the provider on the current chart Not all codes are coded to the highest degree of specificity and combination codes were sometimes missed
Recommendation It is important to assign codes for all conditions which meet the definition of a reportable diagnosis Documentation from all providers should be used including but not limited to radiologists pathologists anesthesiologists CRNAs and FNPs
Reference Coding Clinic Official Coding Guidelines
bull Report all secondary diagnoses which meet the definition of a secondary diagnosis which is defined as all conditions that coexist at the time of admission that develop subsequently or that affect the treatment received andor the length of stay Codes which enhance the overall picture of the patientrsquos visit should be added
o Add T45515A to report adverse effect of Coumadin which caused the GI bleed
o Add I2690 for septic pulmonary emboli (MCCSOI4ROM4)
o Add N179 for acute kidney failure (S3M2CC) per the nephrology consult and the 628 progress note
o Add code I429 cardiomyopathy per HampP
o Add B964 to report proteus in a UTI per the 620 hospitalist progress note
o Code for D649 anemia and I701 stenosis of renal artery should be added as secondary diagnoses per the HampP
bull Only report diagnoses which are substantiated by provider documentation in the current chart notes If a suspected condition is not verified at discharge on an inpatient account it cannot be coded
o Remove G4734 (idiopathic sleep related non-obstructive alveolar hypoventilation) as patient was noted to have the sleep study and the hypoventilation was shown to be a possibility but not noted as such on discharge
o Remove G629 (S21) the neuropathy is documented as due to diabetes
o Remove K529 colitis noted on HP as possible but not further noted or confirmed at discharge
Procedure CodingFinding Procedures were sometimes coded incorrectly
Recommendation The entire medical record should be reviewed and all procedures coded as documented Coding procedures incorrectly or assigning incorrect CPT codes may result in lost revenue
bull Incorrect root operation
o Revise principal procedure to 0DQ68ZZ for clipping of the ulcer per OP report clipping is root operation repair
bull Biopsy versus Excision
o Procedure 0DBA0ZX (biopsy of jejunum) should change to 0DBA0ZZ (excision of jejunum) per op note this was not a biopsy procedure
bull Coding Guideline error
o Remove 0RG10K0 for allograft due to being inclusive in principal procedure
o Remove codes for adhesiolysis 0DN80ZZ 0UN10ZZ and 0UN90ZZ due to no significance noted per OP report
bull Incorrect approach
o Revise 0TF63ZZ (fragmentation percutaneous approach) to 0TF68ZZ (fragmentation endoscopic) for procedure performed via scope per the operative report
bull Procedure coded without provider documentation
o Remove secondary procedure of excisional debridement (0JB90ZZ) due to lack of documentation of excisional debridement per operative report The header in the operative report documents IampD and debridement but the body of the operative report only documents an IampD
bull Incorrect CPT code assignment
o Post-op note supports the nerve block injections of four nerves therefore code 64421 (multiple nerve block) should replace 64420 (injection of one intercostal nerve)
Queries Finding Conflicting incomplete and vague documentation is found within provider chart notes
Recommendation Prior to code assignment if the coder finds ambiguous or conflicting documentation the provider should be queried
Reference AHA Coding Clinic 2002 2nd Quarter pages 17-18
bull Query for acute blood loss anemia since hgb has dropped and patient is being transfused PRBC
bull Recommend query to clarify if cardiorenal syndrome is current as it is documented per 627 nephrology consult but unclear if current
bull Documentation does not support SIRS noninfectious without organ failure It is conflicting since patient has respiratory failure Query should be initiated for clarification with or without organ failure or infectious or non-infectious Patient has pneumonia per query as well as last progress note therefore if SIRS is not further specified per query PNA should be sequenced as principal diagnosis and SIRS should be removed
bull Recommend provider query necrotizing lung consolidation noted on DS as principal diagnosis-unclear does the patient have lobar pneumonia Secondary dx states necrotic pneumonia which is coded as principal diagnosis-this diagnosis is clear but consolidation portion is unclear
bull Recommend query for preterm labor delivery at 301 weeks
bull RECOMMEND QUERY no chest pain on admit per ER and HP cardiology provider states no CP with ER stating chest pressure the day prior to admit Appears patient was admitted due to elevated troponins which cardiology says are likely due to hypotension and AKI DS states chest pain but also says bradycardia and hypotension were the reason for admit
bull RECOMMEND QUERY no chest pain on admit per ER and HP cardiology provider states no CP with ER stating chest pressure the day prior to admit Appears patient was admitted due to elevated troponins which cardiology says are likely due to hypotension and AKI DS states chest pain but also says bradycardia and hypotension were the reason for admit
bull Query the provider regarding pathology report notation of endometriosis andor possible re-sequence of stenosis as principal diagnosis as it also meets principal diagnosis guidelines This would result in an MS-DRG change to 742 and APR-DRG change to 513
bull QUERY secondary diagnosis MCC and ROM 4 code T3166 (60 TBSA of which 60 are third degree burns) Chart notes do not specify how much of TBSA was actually third degree If after query TBSA is found to be less than 50 (T3164) then ROM will change from 4 to 3 but no change to overall APR-DRG or weight
Auditor Quality amp Productivity
Audit Productivity Standards
It takes twice as long to audit a chart as it does to code it a statistic that takes into account the time to document an explanation of any coding decision the auditor is not in agreement with o For example in an emergency department audit with a productivity of 12
charts per hour for a coder our auditors would probably be able to review six per hour
o If there are multiple services to audit on each encounter the productivity may only be 4 per hour
o The amount of detail you put into your audit report will also be a factorndash Are you using an automated audit softwarendash Are you using a spreadsheet to auditndash How many Systems are needed to complete the audit
Coder Quality Audits
Quality Audits (QA) should be done on your coders and auditors regularly Frequent reviews with smaller sample size will allow more consistent
review and feedbacko Example 10 charts per month per coder if the coder passes 2-3 months
consecutively with 95 or better score move them to quarterly reviewso Some QA programs review a percentage of the coders work This
methodology requires more time and resources
Auditor QA should also score and comment on the accuracy of the audit comments and recommendations
Presenting the Audit Results
Presenting the Audit Results
Communicating the Audit FindingsoWho requested the AuditoWho are you reporting the finding to
ndash CEOndash CFOndash Physicianndash Revenue Cycle Managerndash HIM Directorndash Billing Managerndash Coding Manager
ReportsAudit Resultspptx
Post Audit Education
Provider Education
Provider Education is best received when it is specific to the provider(s) 11 sessions going over the audit result Look at their notes with them
oHighlight areas for documentation improvementoReinforce Coding Guidelines that are specific to themoAsk them to share how they establish their LOS for E amp M serviceso Integrate their EMR system into the training
Provider Education
Group Training SessionsoUse the audit results to identify common issues within a specialty group
ndash Refer to the Executive Summary reportoVery effective for identifying system issues
ndash Teaching Attestationsndash Templatesndash Copy and Pastendash Cloned notes
o Everyone hears the same messagesoAn Issue may not appear on the individual audit but is still a concern for the
group
Education Delivery
In person or remote sessionso Factors to consider
ndash Providers scheduleavailabilityndash Location(s)ndash Personality of the providerndash Budget
Coder Education
Coders do well in group training so they can learn from each other 11 training allows the coder to get feedback on their coding
Handling Audit Disputes
Handling Audit Disputes
Be open to all points of viewo Let the documentation tell the story
Refer to the guidelines Ask
oCan we defend the reported service with the current documentation
Self Disclosures Refunds and Corrected Billing
Overpayment
In general If a person has received an overpayment the person shallo report and return the overpayment to the Secretary the State an
intermediary a carrier or a contractor as appropriate at the correct address and ndash notify the Secretary State intermediary carrier or contractor to whom the overpayment was returned in writing of the reason for the overpayment
What is an ldquoOverpaymentrdquo ndash The term ldquooverpaymentrdquo means any funds that a person receives or retains under subchapter XVIII or XIX of this chapter to which the person after applicable reconciliation is not entitled under such subchapter
Self Disclosure
The Office of Inspector General (OIG) has several self-disclosure processes that can be used to report potential fraud in Department of Health and Human Services (HHS) programs Choose the one that applies to you from the following descriptions to learn moreo Health Care Provider Self-Disclosures
ndash Health care providers suppliers or other individuals or entities subject to Civil Monetary Penalties can use the Provider Self-Disclosure Protocol which was created in 1998 to voluntarily disclose self-discovered evidence of potential fraud Self-disclosure gives providers the opportunity to avoid the costs and disruptions associated with a Government-directed investigation and civil or administrative litigation Visit the Provider Self-Disclosure Protocol webpage for more information
o HHS Contractor Self-Disclosuresndash Contractors are individuals businesses or other legal entities that are awarded Government contracts or
subcontracts to provide services to the Department of Health and Human Services (HHS) OIGs contractor self-disclosure program enables contractors to self-disclose potential violations of the False Claims Act and various Federal criminal laws involving fraud conflict of interest bribery or gratuity This self-disclosure process is available for those entities with a Federal Acquisition Regulation-based contract Visit the Contractor Self-Disclosure webpage for more information
o HHS Grantee Self-Disclosuresndash HHS grantees or subrecipients may voluntarily disclose evidence of potential violations of Federal criminal law
involving fraud bribery or gratuity violations potentially affecting the Federal award 45 CFR 75113 notes mandatory disclosures of criminal offenses that non-Federal entities must make with respect to HHS grants Recipients submitting disclosures in connection with this requirement should include the subject reference line Mandatory Grant Disclosure Recipients choosing to disclose conduct that may not fit squarely within the scope of offenses described in 45 CFR 75113 should include the following subject reference line in the submission Voluntary Grant Disclosure
Medicare 60 day rule
The 60 Day Rule (Medicare Parts A amp B) o The 60 day time period for reportingreturning begins when either
ndash The reasonable diligence is completed orndash On the day the provider received credible information of a potential overpayment (if the
provider fails to conduct reasonable diligence) o For an investigation to be conducted in a ldquotimelyrdquo manner providers typically
must complete the investigation within 6 months from receipt of credible information indicating there may be an overpayment
ndash ndash 6-month timeframe may potentially be extended under ldquoextraordinary circumstancesrdquo ndash 8 months generally the maximum total time to return overpayments The government recommends that providers maintain records documenting ldquoreasonable diligencerdquo
Medicare 60 Day Rule
Six-year lookback period ndash Sometimes possible to use a shorter period depending on the facts at issue Amount to be repaid ndash May vary depending on the method used to
reportreturn eg Medicare administrative contractor (ldquoMACrdquo) v self-disclosure Overpayment notification ndash After receiving an overpayment
notification from the government you should investigate for related overpayments eg other time periods
Medicare 60 Day Rule
Self-disclosure protocols ndashoA submission to the OIG or CMS protocols suspends the 60 day requirement
for returning overpayments until a settlement agreement is executed ndash ndash OIGrsquos Self-Disclosure Protocol (SDP) ndash ndash CMS Voluntary Self-Referral Disclosure Protocol (SRDP) ndash
o Self-disclosures to other agencies do not suspend the repayment deadlinendash ndash Eg Department of Justice local US Attorneyrsquos Office Medicaid Fraud Control Unit
Medicare 60 Day Rule
Facilitating Compliance With the 60 Day Rule Compliance programs should include o ndash Appropriate policies and procedures o ndash Periodic billing and coding audits to proactively identify overpaymentso ndash Focus on high-risk areas o ndash Utilization of publicly available government resources to guide audit efforts o ndash Investigating any suspected incidents of non-compliance with federal health
care program requirements
Self Disclosure
Choice of AgencyoOIG ndash Self-Disclosure Protocol
ndash ndash Conduct involving false billingndash ndash Conduct involving excluded personsndash ndash Conduct involving the Anti-Kickback Statute (including conduct thatndash violates both the AKS and Stark Law)
oCMS ndash Self-Referral Disclosure Protocolndash ndash Conduct involving only violations of the Stark Law
oDOJndash ndash May be appropriate when provider believes a FCA release is necessary
Summary
The Cost of a Well-Executed Coding Audit ProcessThe costs associated with an auditing program are worth it in the long run Ideally your organization is performing audits on a regular basis across all service types locations and payers Weve all seen claims that have been denied resulting in additional work that may be preventable with a proper audit program The goal is to use the audit feedback to improve coding quality and lower potential risk and cost to the organization Organizations should be investing in an effective coding audit program to make your coders and providers better and enhance documentation improvement from the providers
Questions
Thank you for your attentionLynn Handy
Vice President of Coding amp Audit ServicesLynnhandymanagedresourcesinccom

Inpatient DRG Audit Report
TABLE OF CONTENTS
Executive Summaryo Scope of Work
Reimbursement Changes Department Results
o InpatientGeneral Recommendations and Comments
o Secondary DiagnosesoProcedure CodingoPresent on AdmissionoQueries
Scope of WorkCodingAID performed coding audit review of 175 inpatient records The review completed was a random sample that included cases coded by twenty coders for dates of service from May 2016 ndash July 2016
The objective was to determine if the medical record documentation supported the following coding and documentation requirements and any other regulatory requirement for that code set Criteria reviewed
1 ICD-10-CM Official Coding Guidelines for accurate diagnosis code reporting 2 ICD-10-PCS Official Coding Guidelines for accurate procedure code reporting 3 Documentation of procedure compared to the CPT code assigned 4 Identify opportunities for education and training 5 Financial impact of current coding practices
The regulatory agencies and reference materials relied upon include the following in addition to Medicare and Medicaid regulations Additional resources are located in the sub sections below
bull ICD-10-CM and ICD-10-PCS for Hospitals current volume bull Centers for Medicare and Medicaid Services CMS NCCI Edits-Centers for Medicaid and
Medicare Services CMS website wwwcmsgov bull AHA Coding Clinic
The following electronic medical record documents were reviewed and relied upon to compare to the actual codes submitted to the third party payer
bull Discharge summaries HampPs Progress Notes and other provider notes located in the EMR Records
bull Patient History Forms Ancillary Staff Notes bull Procedure Notes bull Orders bull Diagnostic Report
Reimbursement Changes
Coder Acct
Billed Audited
Reimbursement ChangesMS DRG SOI ROM Weight Expected
Payment MS DRG SOI ROM Weight Expected Payment
Coder 1 001 790 52300 $2615000 792 21552 $1077600 -$1537400
Coder 2002
749 26452 $1322600 758 10090 $504500 -$818100
Coder 3 003 669 13111 $655550 694 07294 $364700 -$290850
Coder 4 004 389 08707 $435350 394 09502 $475100 $39750
Coder 5 005 312 07630 $381500 812 08572 $428600 $47100
Coder 6 006 384 08481 $424050 378 09949 $497450 $73400
Coder 7 007 206 08164 $408200 794 12987 $649350 $241150
Coder 8008
344 31029 $1551450 853 51334 $2566700 $1015250
TOTAL $7793700 $6564000 -$1229700
General Recommendations and CommentsFinding Pertinent secondary diagnoses are not coded and diagnoses are code which are not supported in provider documentation Code only those diagnoses which are documented by the provider on the current chart Not all codes are coded to the highest degree of specificity and combination codes were sometimes missed
Recommendation It is important to assign codes for all conditions which meet the definition of a reportable diagnosis Documentation from all providers should be used including but not limited to radiologists pathologists anesthesiologists CRNAs and FNPs
Reference Coding Clinic Official Coding Guidelines
bull Report all secondary diagnoses which meet the definition of a secondary diagnosis which is defined as all conditions that coexist at the time of admission that develop subsequently or that affect the treatment received andor the length of stay Codes which enhance the overall picture of the patientrsquos visit should be added
o Add T45515A to report adverse effect of Coumadin which caused the GI bleed
o Add I2690 for septic pulmonary emboli (MCCSOI4ROM4)
o Add N179 for acute kidney failure (S3M2CC) per the nephrology consult and the 628 progress note
o Add code I429 cardiomyopathy per HampP
o Add B964 to report proteus in a UTI per the 620 hospitalist progress note
o Code for D649 anemia and I701 stenosis of renal artery should be added as secondary diagnoses per the HampP
bull Only report diagnoses which are substantiated by provider documentation in the current chart notes If a suspected condition is not verified at discharge on an inpatient account it cannot be coded
o Remove G4734 (idiopathic sleep related non-obstructive alveolar hypoventilation) as patient was noted to have the sleep study and the hypoventilation was shown to be a possibility but not noted as such on discharge
o Remove G629 (S21) the neuropathy is documented as due to diabetes
o Remove K529 colitis noted on HP as possible but not further noted or confirmed at discharge
Procedure CodingFinding Procedures were sometimes coded incorrectly
Recommendation The entire medical record should be reviewed and all procedures coded as documented Coding procedures incorrectly or assigning incorrect CPT codes may result in lost revenue
bull Incorrect root operation
o Revise principal procedure to 0DQ68ZZ for clipping of the ulcer per OP report clipping is root operation repair
bull Biopsy versus Excision
o Procedure 0DBA0ZX (biopsy of jejunum) should change to 0DBA0ZZ (excision of jejunum) per op note this was not a biopsy procedure
bull Coding Guideline error
o Remove 0RG10K0 for allograft due to being inclusive in principal procedure
o Remove codes for adhesiolysis 0DN80ZZ 0UN10ZZ and 0UN90ZZ due to no significance noted per OP report
bull Incorrect approach
o Revise 0TF63ZZ (fragmentation percutaneous approach) to 0TF68ZZ (fragmentation endoscopic) for procedure performed via scope per the operative report
bull Procedure coded without provider documentation
o Remove secondary procedure of excisional debridement (0JB90ZZ) due to lack of documentation of excisional debridement per operative report The header in the operative report documents IampD and debridement but the body of the operative report only documents an IampD
bull Incorrect CPT code assignment
o Post-op note supports the nerve block injections of four nerves therefore code 64421 (multiple nerve block) should replace 64420 (injection of one intercostal nerve)
Queries Finding Conflicting incomplete and vague documentation is found within provider chart notes
Recommendation Prior to code assignment if the coder finds ambiguous or conflicting documentation the provider should be queried
Reference AHA Coding Clinic 2002 2nd Quarter pages 17-18
bull Query for acute blood loss anemia since hgb has dropped and patient is being transfused PRBC
bull Recommend query to clarify if cardiorenal syndrome is current as it is documented per 627 nephrology consult but unclear if current
bull Documentation does not support SIRS noninfectious without organ failure It is conflicting since patient has respiratory failure Query should be initiated for clarification with or without organ failure or infectious or non-infectious Patient has pneumonia per query as well as last progress note therefore if SIRS is not further specified per query PNA should be sequenced as principal diagnosis and SIRS should be removed
bull Recommend provider query necrotizing lung consolidation noted on DS as principal diagnosis-unclear does the patient have lobar pneumonia Secondary dx states necrotic pneumonia which is coded as principal diagnosis-this diagnosis is clear but consolidation portion is unclear
bull Recommend query for preterm labor delivery at 301 weeks
bull RECOMMEND QUERY no chest pain on admit per ER and HP cardiology provider states no CP with ER stating chest pressure the day prior to admit Appears patient was admitted due to elevated troponins which cardiology says are likely due to hypotension and AKI DS states chest pain but also says bradycardia and hypotension were the reason for admit
bull RECOMMEND QUERY no chest pain on admit per ER and HP cardiology provider states no CP with ER stating chest pressure the day prior to admit Appears patient was admitted due to elevated troponins which cardiology says are likely due to hypotension and AKI DS states chest pain but also says bradycardia and hypotension were the reason for admit
bull Query the provider regarding pathology report notation of endometriosis andor possible re-sequence of stenosis as principal diagnosis as it also meets principal diagnosis guidelines This would result in an MS-DRG change to 742 and APR-DRG change to 513
bull QUERY secondary diagnosis MCC and ROM 4 code T3166 (60 TBSA of which 60 are third degree burns) Chart notes do not specify how much of TBSA was actually third degree If after query TBSA is found to be less than 50 (T3164) then ROM will change from 4 to 3 but no change to overall APR-DRG or weight
Auditor Quality amp Productivity
Audit Productivity Standards
It takes twice as long to audit a chart as it does to code it a statistic that takes into account the time to document an explanation of any coding decision the auditor is not in agreement with o For example in an emergency department audit with a productivity of 12
charts per hour for a coder our auditors would probably be able to review six per hour
o If there are multiple services to audit on each encounter the productivity may only be 4 per hour
o The amount of detail you put into your audit report will also be a factorndash Are you using an automated audit softwarendash Are you using a spreadsheet to auditndash How many Systems are needed to complete the audit
Coder Quality Audits
Quality Audits (QA) should be done on your coders and auditors regularly Frequent reviews with smaller sample size will allow more consistent
review and feedbacko Example 10 charts per month per coder if the coder passes 2-3 months
consecutively with 95 or better score move them to quarterly reviewso Some QA programs review a percentage of the coders work This
methodology requires more time and resources
Auditor QA should also score and comment on the accuracy of the audit comments and recommendations
Presenting the Audit Results
Presenting the Audit Results
Communicating the Audit FindingsoWho requested the AuditoWho are you reporting the finding to
ndash CEOndash CFOndash Physicianndash Revenue Cycle Managerndash HIM Directorndash Billing Managerndash Coding Manager
ReportsAudit Resultspptx
Post Audit Education
Provider Education
Provider Education is best received when it is specific to the provider(s) 11 sessions going over the audit result Look at their notes with them
oHighlight areas for documentation improvementoReinforce Coding Guidelines that are specific to themoAsk them to share how they establish their LOS for E amp M serviceso Integrate their EMR system into the training
Provider Education
Group Training SessionsoUse the audit results to identify common issues within a specialty group
ndash Refer to the Executive Summary reportoVery effective for identifying system issues
ndash Teaching Attestationsndash Templatesndash Copy and Pastendash Cloned notes
o Everyone hears the same messagesoAn Issue may not appear on the individual audit but is still a concern for the
group
Education Delivery
In person or remote sessionso Factors to consider
ndash Providers scheduleavailabilityndash Location(s)ndash Personality of the providerndash Budget
Coder Education
Coders do well in group training so they can learn from each other 11 training allows the coder to get feedback on their coding
Handling Audit Disputes
Handling Audit Disputes
Be open to all points of viewo Let the documentation tell the story
Refer to the guidelines Ask
oCan we defend the reported service with the current documentation
Self Disclosures Refunds and Corrected Billing
Overpayment
In general If a person has received an overpayment the person shallo report and return the overpayment to the Secretary the State an
intermediary a carrier or a contractor as appropriate at the correct address and ndash notify the Secretary State intermediary carrier or contractor to whom the overpayment was returned in writing of the reason for the overpayment
What is an ldquoOverpaymentrdquo ndash The term ldquooverpaymentrdquo means any funds that a person receives or retains under subchapter XVIII or XIX of this chapter to which the person after applicable reconciliation is not entitled under such subchapter
Self Disclosure
The Office of Inspector General (OIG) has several self-disclosure processes that can be used to report potential fraud in Department of Health and Human Services (HHS) programs Choose the one that applies to you from the following descriptions to learn moreo Health Care Provider Self-Disclosures
ndash Health care providers suppliers or other individuals or entities subject to Civil Monetary Penalties can use the Provider Self-Disclosure Protocol which was created in 1998 to voluntarily disclose self-discovered evidence of potential fraud Self-disclosure gives providers the opportunity to avoid the costs and disruptions associated with a Government-directed investigation and civil or administrative litigation Visit the Provider Self-Disclosure Protocol webpage for more information
o HHS Contractor Self-Disclosuresndash Contractors are individuals businesses or other legal entities that are awarded Government contracts or
subcontracts to provide services to the Department of Health and Human Services (HHS) OIGs contractor self-disclosure program enables contractors to self-disclose potential violations of the False Claims Act and various Federal criminal laws involving fraud conflict of interest bribery or gratuity This self-disclosure process is available for those entities with a Federal Acquisition Regulation-based contract Visit the Contractor Self-Disclosure webpage for more information
o HHS Grantee Self-Disclosuresndash HHS grantees or subrecipients may voluntarily disclose evidence of potential violations of Federal criminal law
involving fraud bribery or gratuity violations potentially affecting the Federal award 45 CFR 75113 notes mandatory disclosures of criminal offenses that non-Federal entities must make with respect to HHS grants Recipients submitting disclosures in connection with this requirement should include the subject reference line Mandatory Grant Disclosure Recipients choosing to disclose conduct that may not fit squarely within the scope of offenses described in 45 CFR 75113 should include the following subject reference line in the submission Voluntary Grant Disclosure
Medicare 60 day rule
The 60 Day Rule (Medicare Parts A amp B) o The 60 day time period for reportingreturning begins when either
ndash The reasonable diligence is completed orndash On the day the provider received credible information of a potential overpayment (if the
provider fails to conduct reasonable diligence) o For an investigation to be conducted in a ldquotimelyrdquo manner providers typically
must complete the investigation within 6 months from receipt of credible information indicating there may be an overpayment
ndash ndash 6-month timeframe may potentially be extended under ldquoextraordinary circumstancesrdquo ndash 8 months generally the maximum total time to return overpayments The government recommends that providers maintain records documenting ldquoreasonable diligencerdquo
Medicare 60 Day Rule
Six-year lookback period ndash Sometimes possible to use a shorter period depending on the facts at issue Amount to be repaid ndash May vary depending on the method used to
reportreturn eg Medicare administrative contractor (ldquoMACrdquo) v self-disclosure Overpayment notification ndash After receiving an overpayment
notification from the government you should investigate for related overpayments eg other time periods
Medicare 60 Day Rule
Self-disclosure protocols ndashoA submission to the OIG or CMS protocols suspends the 60 day requirement
for returning overpayments until a settlement agreement is executed ndash ndash OIGrsquos Self-Disclosure Protocol (SDP) ndash ndash CMS Voluntary Self-Referral Disclosure Protocol (SRDP) ndash
o Self-disclosures to other agencies do not suspend the repayment deadlinendash ndash Eg Department of Justice local US Attorneyrsquos Office Medicaid Fraud Control Unit
Medicare 60 Day Rule
Facilitating Compliance With the 60 Day Rule Compliance programs should include o ndash Appropriate policies and procedures o ndash Periodic billing and coding audits to proactively identify overpaymentso ndash Focus on high-risk areas o ndash Utilization of publicly available government resources to guide audit efforts o ndash Investigating any suspected incidents of non-compliance with federal health
care program requirements
Self Disclosure
Choice of AgencyoOIG ndash Self-Disclosure Protocol
ndash ndash Conduct involving false billingndash ndash Conduct involving excluded personsndash ndash Conduct involving the Anti-Kickback Statute (including conduct thatndash violates both the AKS and Stark Law)
oCMS ndash Self-Referral Disclosure Protocolndash ndash Conduct involving only violations of the Stark Law
oDOJndash ndash May be appropriate when provider believes a FCA release is necessary
Summary
The Cost of a Well-Executed Coding Audit ProcessThe costs associated with an auditing program are worth it in the long run Ideally your organization is performing audits on a regular basis across all service types locations and payers Weve all seen claims that have been denied resulting in additional work that may be preventable with a proper audit program The goal is to use the audit feedback to improve coding quality and lower potential risk and cost to the organization Organizations should be investing in an effective coding audit program to make your coders and providers better and enhance documentation improvement from the providers
Questions
Thank you for your attentionLynn Handy
Vice President of Coding amp Audit ServicesLynnhandymanagedresourcesinccom

Scope of WorkCodingAID performed coding audit review of 175 inpatient records The review completed was a random sample that included cases coded by twenty coders for dates of service from May 2016 ndash July 2016
The objective was to determine if the medical record documentation supported the following coding and documentation requirements and any other regulatory requirement for that code set Criteria reviewed
1 ICD-10-CM Official Coding Guidelines for accurate diagnosis code reporting 2 ICD-10-PCS Official Coding Guidelines for accurate procedure code reporting 3 Documentation of procedure compared to the CPT code assigned 4 Identify opportunities for education and training 5 Financial impact of current coding practices
The regulatory agencies and reference materials relied upon include the following in addition to Medicare and Medicaid regulations Additional resources are located in the sub sections below
bull ICD-10-CM and ICD-10-PCS for Hospitals current volume bull Centers for Medicare and Medicaid Services CMS NCCI Edits-Centers for Medicaid and
Medicare Services CMS website wwwcmsgov bull AHA Coding Clinic
The following electronic medical record documents were reviewed and relied upon to compare to the actual codes submitted to the third party payer
bull Discharge summaries HampPs Progress Notes and other provider notes located in the EMR Records
bull Patient History Forms Ancillary Staff Notes bull Procedure Notes bull Orders bull Diagnostic Report
Reimbursement Changes
Coder Acct
Billed Audited
Reimbursement ChangesMS DRG SOI ROM Weight Expected
Payment MS DRG SOI ROM Weight Expected Payment
Coder 1 001 790 52300 $2615000 792 21552 $1077600 -$1537400
Coder 2002
749 26452 $1322600 758 10090 $504500 -$818100
Coder 3 003 669 13111 $655550 694 07294 $364700 -$290850
Coder 4 004 389 08707 $435350 394 09502 $475100 $39750
Coder 5 005 312 07630 $381500 812 08572 $428600 $47100
Coder 6 006 384 08481 $424050 378 09949 $497450 $73400
Coder 7 007 206 08164 $408200 794 12987 $649350 $241150
Coder 8008
344 31029 $1551450 853 51334 $2566700 $1015250
TOTAL $7793700 $6564000 -$1229700
General Recommendations and CommentsFinding Pertinent secondary diagnoses are not coded and diagnoses are code which are not supported in provider documentation Code only those diagnoses which are documented by the provider on the current chart Not all codes are coded to the highest degree of specificity and combination codes were sometimes missed
Recommendation It is important to assign codes for all conditions which meet the definition of a reportable diagnosis Documentation from all providers should be used including but not limited to radiologists pathologists anesthesiologists CRNAs and FNPs
Reference Coding Clinic Official Coding Guidelines
bull Report all secondary diagnoses which meet the definition of a secondary diagnosis which is defined as all conditions that coexist at the time of admission that develop subsequently or that affect the treatment received andor the length of stay Codes which enhance the overall picture of the patientrsquos visit should be added
o Add T45515A to report adverse effect of Coumadin which caused the GI bleed
o Add I2690 for septic pulmonary emboli (MCCSOI4ROM4)
o Add N179 for acute kidney failure (S3M2CC) per the nephrology consult and the 628 progress note
o Add code I429 cardiomyopathy per HampP
o Add B964 to report proteus in a UTI per the 620 hospitalist progress note
o Code for D649 anemia and I701 stenosis of renal artery should be added as secondary diagnoses per the HampP
bull Only report diagnoses which are substantiated by provider documentation in the current chart notes If a suspected condition is not verified at discharge on an inpatient account it cannot be coded
o Remove G4734 (idiopathic sleep related non-obstructive alveolar hypoventilation) as patient was noted to have the sleep study and the hypoventilation was shown to be a possibility but not noted as such on discharge
o Remove G629 (S21) the neuropathy is documented as due to diabetes
o Remove K529 colitis noted on HP as possible but not further noted or confirmed at discharge
Procedure CodingFinding Procedures were sometimes coded incorrectly
Recommendation The entire medical record should be reviewed and all procedures coded as documented Coding procedures incorrectly or assigning incorrect CPT codes may result in lost revenue
bull Incorrect root operation
o Revise principal procedure to 0DQ68ZZ for clipping of the ulcer per OP report clipping is root operation repair
bull Biopsy versus Excision
o Procedure 0DBA0ZX (biopsy of jejunum) should change to 0DBA0ZZ (excision of jejunum) per op note this was not a biopsy procedure
bull Coding Guideline error
o Remove 0RG10K0 for allograft due to being inclusive in principal procedure
o Remove codes for adhesiolysis 0DN80ZZ 0UN10ZZ and 0UN90ZZ due to no significance noted per OP report
bull Incorrect approach
o Revise 0TF63ZZ (fragmentation percutaneous approach) to 0TF68ZZ (fragmentation endoscopic) for procedure performed via scope per the operative report
bull Procedure coded without provider documentation
o Remove secondary procedure of excisional debridement (0JB90ZZ) due to lack of documentation of excisional debridement per operative report The header in the operative report documents IampD and debridement but the body of the operative report only documents an IampD
bull Incorrect CPT code assignment
o Post-op note supports the nerve block injections of four nerves therefore code 64421 (multiple nerve block) should replace 64420 (injection of one intercostal nerve)
Queries Finding Conflicting incomplete and vague documentation is found within provider chart notes
Recommendation Prior to code assignment if the coder finds ambiguous or conflicting documentation the provider should be queried
Reference AHA Coding Clinic 2002 2nd Quarter pages 17-18
bull Query for acute blood loss anemia since hgb has dropped and patient is being transfused PRBC
bull Recommend query to clarify if cardiorenal syndrome is current as it is documented per 627 nephrology consult but unclear if current
bull Documentation does not support SIRS noninfectious without organ failure It is conflicting since patient has respiratory failure Query should be initiated for clarification with or without organ failure or infectious or non-infectious Patient has pneumonia per query as well as last progress note therefore if SIRS is not further specified per query PNA should be sequenced as principal diagnosis and SIRS should be removed
bull Recommend provider query necrotizing lung consolidation noted on DS as principal diagnosis-unclear does the patient have lobar pneumonia Secondary dx states necrotic pneumonia which is coded as principal diagnosis-this diagnosis is clear but consolidation portion is unclear
bull Recommend query for preterm labor delivery at 301 weeks
bull RECOMMEND QUERY no chest pain on admit per ER and HP cardiology provider states no CP with ER stating chest pressure the day prior to admit Appears patient was admitted due to elevated troponins which cardiology says are likely due to hypotension and AKI DS states chest pain but also says bradycardia and hypotension were the reason for admit
bull RECOMMEND QUERY no chest pain on admit per ER and HP cardiology provider states no CP with ER stating chest pressure the day prior to admit Appears patient was admitted due to elevated troponins which cardiology says are likely due to hypotension and AKI DS states chest pain but also says bradycardia and hypotension were the reason for admit
bull Query the provider regarding pathology report notation of endometriosis andor possible re-sequence of stenosis as principal diagnosis as it also meets principal diagnosis guidelines This would result in an MS-DRG change to 742 and APR-DRG change to 513
bull QUERY secondary diagnosis MCC and ROM 4 code T3166 (60 TBSA of which 60 are third degree burns) Chart notes do not specify how much of TBSA was actually third degree If after query TBSA is found to be less than 50 (T3164) then ROM will change from 4 to 3 but no change to overall APR-DRG or weight
Auditor Quality amp Productivity
Audit Productivity Standards
It takes twice as long to audit a chart as it does to code it a statistic that takes into account the time to document an explanation of any coding decision the auditor is not in agreement with o For example in an emergency department audit with a productivity of 12
charts per hour for a coder our auditors would probably be able to review six per hour
o If there are multiple services to audit on each encounter the productivity may only be 4 per hour
o The amount of detail you put into your audit report will also be a factorndash Are you using an automated audit softwarendash Are you using a spreadsheet to auditndash How many Systems are needed to complete the audit
Coder Quality Audits
Quality Audits (QA) should be done on your coders and auditors regularly Frequent reviews with smaller sample size will allow more consistent
review and feedbacko Example 10 charts per month per coder if the coder passes 2-3 months
consecutively with 95 or better score move them to quarterly reviewso Some QA programs review a percentage of the coders work This
methodology requires more time and resources
Auditor QA should also score and comment on the accuracy of the audit comments and recommendations
Presenting the Audit Results
Presenting the Audit Results
Communicating the Audit FindingsoWho requested the AuditoWho are you reporting the finding to
ndash CEOndash CFOndash Physicianndash Revenue Cycle Managerndash HIM Directorndash Billing Managerndash Coding Manager
ReportsAudit Resultspptx
Post Audit Education
Provider Education
Provider Education is best received when it is specific to the provider(s) 11 sessions going over the audit result Look at their notes with them
oHighlight areas for documentation improvementoReinforce Coding Guidelines that are specific to themoAsk them to share how they establish their LOS for E amp M serviceso Integrate their EMR system into the training
Provider Education
Group Training SessionsoUse the audit results to identify common issues within a specialty group
ndash Refer to the Executive Summary reportoVery effective for identifying system issues
ndash Teaching Attestationsndash Templatesndash Copy and Pastendash Cloned notes
o Everyone hears the same messagesoAn Issue may not appear on the individual audit but is still a concern for the
group
Education Delivery
In person or remote sessionso Factors to consider
ndash Providers scheduleavailabilityndash Location(s)ndash Personality of the providerndash Budget
Coder Education
Coders do well in group training so they can learn from each other 11 training allows the coder to get feedback on their coding
Handling Audit Disputes
Handling Audit Disputes
Be open to all points of viewo Let the documentation tell the story
Refer to the guidelines Ask
oCan we defend the reported service with the current documentation
Self Disclosures Refunds and Corrected Billing
Overpayment
In general If a person has received an overpayment the person shallo report and return the overpayment to the Secretary the State an
intermediary a carrier or a contractor as appropriate at the correct address and ndash notify the Secretary State intermediary carrier or contractor to whom the overpayment was returned in writing of the reason for the overpayment
What is an ldquoOverpaymentrdquo ndash The term ldquooverpaymentrdquo means any funds that a person receives or retains under subchapter XVIII or XIX of this chapter to which the person after applicable reconciliation is not entitled under such subchapter
Self Disclosure
The Office of Inspector General (OIG) has several self-disclosure processes that can be used to report potential fraud in Department of Health and Human Services (HHS) programs Choose the one that applies to you from the following descriptions to learn moreo Health Care Provider Self-Disclosures
ndash Health care providers suppliers or other individuals or entities subject to Civil Monetary Penalties can use the Provider Self-Disclosure Protocol which was created in 1998 to voluntarily disclose self-discovered evidence of potential fraud Self-disclosure gives providers the opportunity to avoid the costs and disruptions associated with a Government-directed investigation and civil or administrative litigation Visit the Provider Self-Disclosure Protocol webpage for more information
o HHS Contractor Self-Disclosuresndash Contractors are individuals businesses or other legal entities that are awarded Government contracts or
subcontracts to provide services to the Department of Health and Human Services (HHS) OIGs contractor self-disclosure program enables contractors to self-disclose potential violations of the False Claims Act and various Federal criminal laws involving fraud conflict of interest bribery or gratuity This self-disclosure process is available for those entities with a Federal Acquisition Regulation-based contract Visit the Contractor Self-Disclosure webpage for more information
o HHS Grantee Self-Disclosuresndash HHS grantees or subrecipients may voluntarily disclose evidence of potential violations of Federal criminal law
involving fraud bribery or gratuity violations potentially affecting the Federal award 45 CFR 75113 notes mandatory disclosures of criminal offenses that non-Federal entities must make with respect to HHS grants Recipients submitting disclosures in connection with this requirement should include the subject reference line Mandatory Grant Disclosure Recipients choosing to disclose conduct that may not fit squarely within the scope of offenses described in 45 CFR 75113 should include the following subject reference line in the submission Voluntary Grant Disclosure
Medicare 60 day rule
The 60 Day Rule (Medicare Parts A amp B) o The 60 day time period for reportingreturning begins when either
ndash The reasonable diligence is completed orndash On the day the provider received credible information of a potential overpayment (if the
provider fails to conduct reasonable diligence) o For an investigation to be conducted in a ldquotimelyrdquo manner providers typically
must complete the investigation within 6 months from receipt of credible information indicating there may be an overpayment
ndash ndash 6-month timeframe may potentially be extended under ldquoextraordinary circumstancesrdquo ndash 8 months generally the maximum total time to return overpayments The government recommends that providers maintain records documenting ldquoreasonable diligencerdquo
Medicare 60 Day Rule
Six-year lookback period ndash Sometimes possible to use a shorter period depending on the facts at issue Amount to be repaid ndash May vary depending on the method used to
reportreturn eg Medicare administrative contractor (ldquoMACrdquo) v self-disclosure Overpayment notification ndash After receiving an overpayment
notification from the government you should investigate for related overpayments eg other time periods
Medicare 60 Day Rule
Self-disclosure protocols ndashoA submission to the OIG or CMS protocols suspends the 60 day requirement
for returning overpayments until a settlement agreement is executed ndash ndash OIGrsquos Self-Disclosure Protocol (SDP) ndash ndash CMS Voluntary Self-Referral Disclosure Protocol (SRDP) ndash
o Self-disclosures to other agencies do not suspend the repayment deadlinendash ndash Eg Department of Justice local US Attorneyrsquos Office Medicaid Fraud Control Unit
Medicare 60 Day Rule
Facilitating Compliance With the 60 Day Rule Compliance programs should include o ndash Appropriate policies and procedures o ndash Periodic billing and coding audits to proactively identify overpaymentso ndash Focus on high-risk areas o ndash Utilization of publicly available government resources to guide audit efforts o ndash Investigating any suspected incidents of non-compliance with federal health
care program requirements
Self Disclosure
Choice of AgencyoOIG ndash Self-Disclosure Protocol
ndash ndash Conduct involving false billingndash ndash Conduct involving excluded personsndash ndash Conduct involving the Anti-Kickback Statute (including conduct thatndash violates both the AKS and Stark Law)
oCMS ndash Self-Referral Disclosure Protocolndash ndash Conduct involving only violations of the Stark Law
oDOJndash ndash May be appropriate when provider believes a FCA release is necessary
Summary
The Cost of a Well-Executed Coding Audit ProcessThe costs associated with an auditing program are worth it in the long run Ideally your organization is performing audits on a regular basis across all service types locations and payers Weve all seen claims that have been denied resulting in additional work that may be preventable with a proper audit program The goal is to use the audit feedback to improve coding quality and lower potential risk and cost to the organization Organizations should be investing in an effective coding audit program to make your coders and providers better and enhance documentation improvement from the providers
Questions
Thank you for your attentionLynn Handy
Vice President of Coding amp Audit ServicesLynnhandymanagedresourcesinccom

Reimbursement Changes
Coder Acct
Billed Audited
Reimbursement ChangesMS DRG SOI ROM Weight Expected
Payment MS DRG SOI ROM Weight Expected Payment
Coder 1 001 790 52300 $2615000 792 21552 $1077600 -$1537400
Coder 2002
749 26452 $1322600 758 10090 $504500 -$818100
Coder 3 003 669 13111 $655550 694 07294 $364700 -$290850
Coder 4 004 389 08707 $435350 394 09502 $475100 $39750
Coder 5 005 312 07630 $381500 812 08572 $428600 $47100
Coder 6 006 384 08481 $424050 378 09949 $497450 $73400
Coder 7 007 206 08164 $408200 794 12987 $649350 $241150
Coder 8008
344 31029 $1551450 853 51334 $2566700 $1015250
TOTAL $7793700 $6564000 -$1229700
General Recommendations and CommentsFinding Pertinent secondary diagnoses are not coded and diagnoses are code which are not supported in provider documentation Code only those diagnoses which are documented by the provider on the current chart Not all codes are coded to the highest degree of specificity and combination codes were sometimes missed
Recommendation It is important to assign codes for all conditions which meet the definition of a reportable diagnosis Documentation from all providers should be used including but not limited to radiologists pathologists anesthesiologists CRNAs and FNPs
Reference Coding Clinic Official Coding Guidelines
bull Report all secondary diagnoses which meet the definition of a secondary diagnosis which is defined as all conditions that coexist at the time of admission that develop subsequently or that affect the treatment received andor the length of stay Codes which enhance the overall picture of the patientrsquos visit should be added
o Add T45515A to report adverse effect of Coumadin which caused the GI bleed
o Add I2690 for septic pulmonary emboli (MCCSOI4ROM4)
o Add N179 for acute kidney failure (S3M2CC) per the nephrology consult and the 628 progress note
o Add code I429 cardiomyopathy per HampP
o Add B964 to report proteus in a UTI per the 620 hospitalist progress note
o Code for D649 anemia and I701 stenosis of renal artery should be added as secondary diagnoses per the HampP
bull Only report diagnoses which are substantiated by provider documentation in the current chart notes If a suspected condition is not verified at discharge on an inpatient account it cannot be coded
o Remove G4734 (idiopathic sleep related non-obstructive alveolar hypoventilation) as patient was noted to have the sleep study and the hypoventilation was shown to be a possibility but not noted as such on discharge
o Remove G629 (S21) the neuropathy is documented as due to diabetes
o Remove K529 colitis noted on HP as possible but not further noted or confirmed at discharge
Procedure CodingFinding Procedures were sometimes coded incorrectly
Recommendation The entire medical record should be reviewed and all procedures coded as documented Coding procedures incorrectly or assigning incorrect CPT codes may result in lost revenue
bull Incorrect root operation
o Revise principal procedure to 0DQ68ZZ for clipping of the ulcer per OP report clipping is root operation repair
bull Biopsy versus Excision
o Procedure 0DBA0ZX (biopsy of jejunum) should change to 0DBA0ZZ (excision of jejunum) per op note this was not a biopsy procedure
bull Coding Guideline error
o Remove 0RG10K0 for allograft due to being inclusive in principal procedure
o Remove codes for adhesiolysis 0DN80ZZ 0UN10ZZ and 0UN90ZZ due to no significance noted per OP report
bull Incorrect approach
o Revise 0TF63ZZ (fragmentation percutaneous approach) to 0TF68ZZ (fragmentation endoscopic) for procedure performed via scope per the operative report
bull Procedure coded without provider documentation
o Remove secondary procedure of excisional debridement (0JB90ZZ) due to lack of documentation of excisional debridement per operative report The header in the operative report documents IampD and debridement but the body of the operative report only documents an IampD
bull Incorrect CPT code assignment
o Post-op note supports the nerve block injections of four nerves therefore code 64421 (multiple nerve block) should replace 64420 (injection of one intercostal nerve)
Queries Finding Conflicting incomplete and vague documentation is found within provider chart notes
Recommendation Prior to code assignment if the coder finds ambiguous or conflicting documentation the provider should be queried
Reference AHA Coding Clinic 2002 2nd Quarter pages 17-18
bull Query for acute blood loss anemia since hgb has dropped and patient is being transfused PRBC
bull Recommend query to clarify if cardiorenal syndrome is current as it is documented per 627 nephrology consult but unclear if current
bull Documentation does not support SIRS noninfectious without organ failure It is conflicting since patient has respiratory failure Query should be initiated for clarification with or without organ failure or infectious or non-infectious Patient has pneumonia per query as well as last progress note therefore if SIRS is not further specified per query PNA should be sequenced as principal diagnosis and SIRS should be removed
bull Recommend provider query necrotizing lung consolidation noted on DS as principal diagnosis-unclear does the patient have lobar pneumonia Secondary dx states necrotic pneumonia which is coded as principal diagnosis-this diagnosis is clear but consolidation portion is unclear
bull Recommend query for preterm labor delivery at 301 weeks
bull RECOMMEND QUERY no chest pain on admit per ER and HP cardiology provider states no CP with ER stating chest pressure the day prior to admit Appears patient was admitted due to elevated troponins which cardiology says are likely due to hypotension and AKI DS states chest pain but also says bradycardia and hypotension were the reason for admit
bull RECOMMEND QUERY no chest pain on admit per ER and HP cardiology provider states no CP with ER stating chest pressure the day prior to admit Appears patient was admitted due to elevated troponins which cardiology says are likely due to hypotension and AKI DS states chest pain but also says bradycardia and hypotension were the reason for admit
bull Query the provider regarding pathology report notation of endometriosis andor possible re-sequence of stenosis as principal diagnosis as it also meets principal diagnosis guidelines This would result in an MS-DRG change to 742 and APR-DRG change to 513
bull QUERY secondary diagnosis MCC and ROM 4 code T3166 (60 TBSA of which 60 are third degree burns) Chart notes do not specify how much of TBSA was actually third degree If after query TBSA is found to be less than 50 (T3164) then ROM will change from 4 to 3 but no change to overall APR-DRG or weight
Auditor Quality amp Productivity
Audit Productivity Standards
It takes twice as long to audit a chart as it does to code it a statistic that takes into account the time to document an explanation of any coding decision the auditor is not in agreement with o For example in an emergency department audit with a productivity of 12
charts per hour for a coder our auditors would probably be able to review six per hour
o If there are multiple services to audit on each encounter the productivity may only be 4 per hour
o The amount of detail you put into your audit report will also be a factorndash Are you using an automated audit softwarendash Are you using a spreadsheet to auditndash How many Systems are needed to complete the audit
Coder Quality Audits
Quality Audits (QA) should be done on your coders and auditors regularly Frequent reviews with smaller sample size will allow more consistent
review and feedbacko Example 10 charts per month per coder if the coder passes 2-3 months
consecutively with 95 or better score move them to quarterly reviewso Some QA programs review a percentage of the coders work This
methodology requires more time and resources
Auditor QA should also score and comment on the accuracy of the audit comments and recommendations
Presenting the Audit Results
Presenting the Audit Results
Communicating the Audit FindingsoWho requested the AuditoWho are you reporting the finding to
ndash CEOndash CFOndash Physicianndash Revenue Cycle Managerndash HIM Directorndash Billing Managerndash Coding Manager
ReportsAudit Resultspptx
Post Audit Education
Provider Education
Provider Education is best received when it is specific to the provider(s) 11 sessions going over the audit result Look at their notes with them
oHighlight areas for documentation improvementoReinforce Coding Guidelines that are specific to themoAsk them to share how they establish their LOS for E amp M serviceso Integrate their EMR system into the training
Provider Education
Group Training SessionsoUse the audit results to identify common issues within a specialty group
ndash Refer to the Executive Summary reportoVery effective for identifying system issues
ndash Teaching Attestationsndash Templatesndash Copy and Pastendash Cloned notes
o Everyone hears the same messagesoAn Issue may not appear on the individual audit but is still a concern for the
group
Education Delivery
In person or remote sessionso Factors to consider
ndash Providers scheduleavailabilityndash Location(s)ndash Personality of the providerndash Budget
Coder Education
Coders do well in group training so they can learn from each other 11 training allows the coder to get feedback on their coding
Handling Audit Disputes
Handling Audit Disputes
Be open to all points of viewo Let the documentation tell the story
Refer to the guidelines Ask
oCan we defend the reported service with the current documentation
Self Disclosures Refunds and Corrected Billing
Overpayment
In general If a person has received an overpayment the person shallo report and return the overpayment to the Secretary the State an
intermediary a carrier or a contractor as appropriate at the correct address and ndash notify the Secretary State intermediary carrier or contractor to whom the overpayment was returned in writing of the reason for the overpayment
What is an ldquoOverpaymentrdquo ndash The term ldquooverpaymentrdquo means any funds that a person receives or retains under subchapter XVIII or XIX of this chapter to which the person after applicable reconciliation is not entitled under such subchapter
Self Disclosure
The Office of Inspector General (OIG) has several self-disclosure processes that can be used to report potential fraud in Department of Health and Human Services (HHS) programs Choose the one that applies to you from the following descriptions to learn moreo Health Care Provider Self-Disclosures
ndash Health care providers suppliers or other individuals or entities subject to Civil Monetary Penalties can use the Provider Self-Disclosure Protocol which was created in 1998 to voluntarily disclose self-discovered evidence of potential fraud Self-disclosure gives providers the opportunity to avoid the costs and disruptions associated with a Government-directed investigation and civil or administrative litigation Visit the Provider Self-Disclosure Protocol webpage for more information
o HHS Contractor Self-Disclosuresndash Contractors are individuals businesses or other legal entities that are awarded Government contracts or
subcontracts to provide services to the Department of Health and Human Services (HHS) OIGs contractor self-disclosure program enables contractors to self-disclose potential violations of the False Claims Act and various Federal criminal laws involving fraud conflict of interest bribery or gratuity This self-disclosure process is available for those entities with a Federal Acquisition Regulation-based contract Visit the Contractor Self-Disclosure webpage for more information
o HHS Grantee Self-Disclosuresndash HHS grantees or subrecipients may voluntarily disclose evidence of potential violations of Federal criminal law
involving fraud bribery or gratuity violations potentially affecting the Federal award 45 CFR 75113 notes mandatory disclosures of criminal offenses that non-Federal entities must make with respect to HHS grants Recipients submitting disclosures in connection with this requirement should include the subject reference line Mandatory Grant Disclosure Recipients choosing to disclose conduct that may not fit squarely within the scope of offenses described in 45 CFR 75113 should include the following subject reference line in the submission Voluntary Grant Disclosure
Medicare 60 day rule
The 60 Day Rule (Medicare Parts A amp B) o The 60 day time period for reportingreturning begins when either
ndash The reasonable diligence is completed orndash On the day the provider received credible information of a potential overpayment (if the
provider fails to conduct reasonable diligence) o For an investigation to be conducted in a ldquotimelyrdquo manner providers typically
must complete the investigation within 6 months from receipt of credible information indicating there may be an overpayment
ndash ndash 6-month timeframe may potentially be extended under ldquoextraordinary circumstancesrdquo ndash 8 months generally the maximum total time to return overpayments The government recommends that providers maintain records documenting ldquoreasonable diligencerdquo
Medicare 60 Day Rule
Six-year lookback period ndash Sometimes possible to use a shorter period depending on the facts at issue Amount to be repaid ndash May vary depending on the method used to
reportreturn eg Medicare administrative contractor (ldquoMACrdquo) v self-disclosure Overpayment notification ndash After receiving an overpayment
notification from the government you should investigate for related overpayments eg other time periods
Medicare 60 Day Rule
Self-disclosure protocols ndashoA submission to the OIG or CMS protocols suspends the 60 day requirement
for returning overpayments until a settlement agreement is executed ndash ndash OIGrsquos Self-Disclosure Protocol (SDP) ndash ndash CMS Voluntary Self-Referral Disclosure Protocol (SRDP) ndash
o Self-disclosures to other agencies do not suspend the repayment deadlinendash ndash Eg Department of Justice local US Attorneyrsquos Office Medicaid Fraud Control Unit
Medicare 60 Day Rule
Facilitating Compliance With the 60 Day Rule Compliance programs should include o ndash Appropriate policies and procedures o ndash Periodic billing and coding audits to proactively identify overpaymentso ndash Focus on high-risk areas o ndash Utilization of publicly available government resources to guide audit efforts o ndash Investigating any suspected incidents of non-compliance with federal health
care program requirements
Self Disclosure
Choice of AgencyoOIG ndash Self-Disclosure Protocol
ndash ndash Conduct involving false billingndash ndash Conduct involving excluded personsndash ndash Conduct involving the Anti-Kickback Statute (including conduct thatndash violates both the AKS and Stark Law)
oCMS ndash Self-Referral Disclosure Protocolndash ndash Conduct involving only violations of the Stark Law
oDOJndash ndash May be appropriate when provider believes a FCA release is necessary
Summary
The Cost of a Well-Executed Coding Audit ProcessThe costs associated with an auditing program are worth it in the long run Ideally your organization is performing audits on a regular basis across all service types locations and payers Weve all seen claims that have been denied resulting in additional work that may be preventable with a proper audit program The goal is to use the audit feedback to improve coding quality and lower potential risk and cost to the organization Organizations should be investing in an effective coding audit program to make your coders and providers better and enhance documentation improvement from the providers
Questions
Thank you for your attentionLynn Handy
Vice President of Coding amp Audit ServicesLynnhandymanagedresourcesinccom

General Recommendations and CommentsFinding Pertinent secondary diagnoses are not coded and diagnoses are code which are not supported in provider documentation Code only those diagnoses which are documented by the provider on the current chart Not all codes are coded to the highest degree of specificity and combination codes were sometimes missed
Recommendation It is important to assign codes for all conditions which meet the definition of a reportable diagnosis Documentation from all providers should be used including but not limited to radiologists pathologists anesthesiologists CRNAs and FNPs
Reference Coding Clinic Official Coding Guidelines
bull Report all secondary diagnoses which meet the definition of a secondary diagnosis which is defined as all conditions that coexist at the time of admission that develop subsequently or that affect the treatment received andor the length of stay Codes which enhance the overall picture of the patientrsquos visit should be added
o Add T45515A to report adverse effect of Coumadin which caused the GI bleed
o Add I2690 for septic pulmonary emboli (MCCSOI4ROM4)
o Add N179 for acute kidney failure (S3M2CC) per the nephrology consult and the 628 progress note
o Add code I429 cardiomyopathy per HampP
o Add B964 to report proteus in a UTI per the 620 hospitalist progress note
o Code for D649 anemia and I701 stenosis of renal artery should be added as secondary diagnoses per the HampP
bull Only report diagnoses which are substantiated by provider documentation in the current chart notes If a suspected condition is not verified at discharge on an inpatient account it cannot be coded
o Remove G4734 (idiopathic sleep related non-obstructive alveolar hypoventilation) as patient was noted to have the sleep study and the hypoventilation was shown to be a possibility but not noted as such on discharge
o Remove G629 (S21) the neuropathy is documented as due to diabetes
o Remove K529 colitis noted on HP as possible but not further noted or confirmed at discharge
Procedure CodingFinding Procedures were sometimes coded incorrectly
Recommendation The entire medical record should be reviewed and all procedures coded as documented Coding procedures incorrectly or assigning incorrect CPT codes may result in lost revenue
bull Incorrect root operation
o Revise principal procedure to 0DQ68ZZ for clipping of the ulcer per OP report clipping is root operation repair
bull Biopsy versus Excision
o Procedure 0DBA0ZX (biopsy of jejunum) should change to 0DBA0ZZ (excision of jejunum) per op note this was not a biopsy procedure
bull Coding Guideline error
o Remove 0RG10K0 for allograft due to being inclusive in principal procedure
o Remove codes for adhesiolysis 0DN80ZZ 0UN10ZZ and 0UN90ZZ due to no significance noted per OP report
bull Incorrect approach
o Revise 0TF63ZZ (fragmentation percutaneous approach) to 0TF68ZZ (fragmentation endoscopic) for procedure performed via scope per the operative report
bull Procedure coded without provider documentation
o Remove secondary procedure of excisional debridement (0JB90ZZ) due to lack of documentation of excisional debridement per operative report The header in the operative report documents IampD and debridement but the body of the operative report only documents an IampD
bull Incorrect CPT code assignment
o Post-op note supports the nerve block injections of four nerves therefore code 64421 (multiple nerve block) should replace 64420 (injection of one intercostal nerve)
Queries Finding Conflicting incomplete and vague documentation is found within provider chart notes
Recommendation Prior to code assignment if the coder finds ambiguous or conflicting documentation the provider should be queried
Reference AHA Coding Clinic 2002 2nd Quarter pages 17-18
bull Query for acute blood loss anemia since hgb has dropped and patient is being transfused PRBC
bull Recommend query to clarify if cardiorenal syndrome is current as it is documented per 627 nephrology consult but unclear if current
bull Documentation does not support SIRS noninfectious without organ failure It is conflicting since patient has respiratory failure Query should be initiated for clarification with or without organ failure or infectious or non-infectious Patient has pneumonia per query as well as last progress note therefore if SIRS is not further specified per query PNA should be sequenced as principal diagnosis and SIRS should be removed
bull Recommend provider query necrotizing lung consolidation noted on DS as principal diagnosis-unclear does the patient have lobar pneumonia Secondary dx states necrotic pneumonia which is coded as principal diagnosis-this diagnosis is clear but consolidation portion is unclear
bull Recommend query for preterm labor delivery at 301 weeks
bull RECOMMEND QUERY no chest pain on admit per ER and HP cardiology provider states no CP with ER stating chest pressure the day prior to admit Appears patient was admitted due to elevated troponins which cardiology says are likely due to hypotension and AKI DS states chest pain but also says bradycardia and hypotension were the reason for admit
bull RECOMMEND QUERY no chest pain on admit per ER and HP cardiology provider states no CP with ER stating chest pressure the day prior to admit Appears patient was admitted due to elevated troponins which cardiology says are likely due to hypotension and AKI DS states chest pain but also says bradycardia and hypotension were the reason for admit
bull Query the provider regarding pathology report notation of endometriosis andor possible re-sequence of stenosis as principal diagnosis as it also meets principal diagnosis guidelines This would result in an MS-DRG change to 742 and APR-DRG change to 513
bull QUERY secondary diagnosis MCC and ROM 4 code T3166 (60 TBSA of which 60 are third degree burns) Chart notes do not specify how much of TBSA was actually third degree If after query TBSA is found to be less than 50 (T3164) then ROM will change from 4 to 3 but no change to overall APR-DRG or weight
Auditor Quality amp Productivity
Audit Productivity Standards
It takes twice as long to audit a chart as it does to code it a statistic that takes into account the time to document an explanation of any coding decision the auditor is not in agreement with o For example in an emergency department audit with a productivity of 12
charts per hour for a coder our auditors would probably be able to review six per hour
o If there are multiple services to audit on each encounter the productivity may only be 4 per hour
o The amount of detail you put into your audit report will also be a factorndash Are you using an automated audit softwarendash Are you using a spreadsheet to auditndash How many Systems are needed to complete the audit
Coder Quality Audits
Quality Audits (QA) should be done on your coders and auditors regularly Frequent reviews with smaller sample size will allow more consistent
review and feedbacko Example 10 charts per month per coder if the coder passes 2-3 months
consecutively with 95 or better score move them to quarterly reviewso Some QA programs review a percentage of the coders work This
methodology requires more time and resources
Auditor QA should also score and comment on the accuracy of the audit comments and recommendations
Presenting the Audit Results
Presenting the Audit Results
Communicating the Audit FindingsoWho requested the AuditoWho are you reporting the finding to
ndash CEOndash CFOndash Physicianndash Revenue Cycle Managerndash HIM Directorndash Billing Managerndash Coding Manager
ReportsAudit Resultspptx
Post Audit Education
Provider Education
Provider Education is best received when it is specific to the provider(s) 11 sessions going over the audit result Look at their notes with them
oHighlight areas for documentation improvementoReinforce Coding Guidelines that are specific to themoAsk them to share how they establish their LOS for E amp M serviceso Integrate their EMR system into the training
Provider Education
Group Training SessionsoUse the audit results to identify common issues within a specialty group
ndash Refer to the Executive Summary reportoVery effective for identifying system issues
ndash Teaching Attestationsndash Templatesndash Copy and Pastendash Cloned notes
o Everyone hears the same messagesoAn Issue may not appear on the individual audit but is still a concern for the
group
Education Delivery
In person or remote sessionso Factors to consider
ndash Providers scheduleavailabilityndash Location(s)ndash Personality of the providerndash Budget
Coder Education
Coders do well in group training so they can learn from each other 11 training allows the coder to get feedback on their coding
Handling Audit Disputes
Handling Audit Disputes
Be open to all points of viewo Let the documentation tell the story
Refer to the guidelines Ask
oCan we defend the reported service with the current documentation
Self Disclosures Refunds and Corrected Billing
Overpayment
In general If a person has received an overpayment the person shallo report and return the overpayment to the Secretary the State an
intermediary a carrier or a contractor as appropriate at the correct address and ndash notify the Secretary State intermediary carrier or contractor to whom the overpayment was returned in writing of the reason for the overpayment
What is an ldquoOverpaymentrdquo ndash The term ldquooverpaymentrdquo means any funds that a person receives or retains under subchapter XVIII or XIX of this chapter to which the person after applicable reconciliation is not entitled under such subchapter
Self Disclosure
The Office of Inspector General (OIG) has several self-disclosure processes that can be used to report potential fraud in Department of Health and Human Services (HHS) programs Choose the one that applies to you from the following descriptions to learn moreo Health Care Provider Self-Disclosures
ndash Health care providers suppliers or other individuals or entities subject to Civil Monetary Penalties can use the Provider Self-Disclosure Protocol which was created in 1998 to voluntarily disclose self-discovered evidence of potential fraud Self-disclosure gives providers the opportunity to avoid the costs and disruptions associated with a Government-directed investigation and civil or administrative litigation Visit the Provider Self-Disclosure Protocol webpage for more information
o HHS Contractor Self-Disclosuresndash Contractors are individuals businesses or other legal entities that are awarded Government contracts or
subcontracts to provide services to the Department of Health and Human Services (HHS) OIGs contractor self-disclosure program enables contractors to self-disclose potential violations of the False Claims Act and various Federal criminal laws involving fraud conflict of interest bribery or gratuity This self-disclosure process is available for those entities with a Federal Acquisition Regulation-based contract Visit the Contractor Self-Disclosure webpage for more information
o HHS Grantee Self-Disclosuresndash HHS grantees or subrecipients may voluntarily disclose evidence of potential violations of Federal criminal law
involving fraud bribery or gratuity violations potentially affecting the Federal award 45 CFR 75113 notes mandatory disclosures of criminal offenses that non-Federal entities must make with respect to HHS grants Recipients submitting disclosures in connection with this requirement should include the subject reference line Mandatory Grant Disclosure Recipients choosing to disclose conduct that may not fit squarely within the scope of offenses described in 45 CFR 75113 should include the following subject reference line in the submission Voluntary Grant Disclosure
Medicare 60 day rule
The 60 Day Rule (Medicare Parts A amp B) o The 60 day time period for reportingreturning begins when either
ndash The reasonable diligence is completed orndash On the day the provider received credible information of a potential overpayment (if the
provider fails to conduct reasonable diligence) o For an investigation to be conducted in a ldquotimelyrdquo manner providers typically
must complete the investigation within 6 months from receipt of credible information indicating there may be an overpayment
ndash ndash 6-month timeframe may potentially be extended under ldquoextraordinary circumstancesrdquo ndash 8 months generally the maximum total time to return overpayments The government recommends that providers maintain records documenting ldquoreasonable diligencerdquo
Medicare 60 Day Rule
Six-year lookback period ndash Sometimes possible to use a shorter period depending on the facts at issue Amount to be repaid ndash May vary depending on the method used to
reportreturn eg Medicare administrative contractor (ldquoMACrdquo) v self-disclosure Overpayment notification ndash After receiving an overpayment
notification from the government you should investigate for related overpayments eg other time periods
Medicare 60 Day Rule
Self-disclosure protocols ndashoA submission to the OIG or CMS protocols suspends the 60 day requirement
for returning overpayments until a settlement agreement is executed ndash ndash OIGrsquos Self-Disclosure Protocol (SDP) ndash ndash CMS Voluntary Self-Referral Disclosure Protocol (SRDP) ndash
o Self-disclosures to other agencies do not suspend the repayment deadlinendash ndash Eg Department of Justice local US Attorneyrsquos Office Medicaid Fraud Control Unit
Medicare 60 Day Rule
Facilitating Compliance With the 60 Day Rule Compliance programs should include o ndash Appropriate policies and procedures o ndash Periodic billing and coding audits to proactively identify overpaymentso ndash Focus on high-risk areas o ndash Utilization of publicly available government resources to guide audit efforts o ndash Investigating any suspected incidents of non-compliance with federal health
care program requirements
Self Disclosure
Choice of AgencyoOIG ndash Self-Disclosure Protocol
ndash ndash Conduct involving false billingndash ndash Conduct involving excluded personsndash ndash Conduct involving the Anti-Kickback Statute (including conduct thatndash violates both the AKS and Stark Law)
oCMS ndash Self-Referral Disclosure Protocolndash ndash Conduct involving only violations of the Stark Law
oDOJndash ndash May be appropriate when provider believes a FCA release is necessary
Summary
The Cost of a Well-Executed Coding Audit ProcessThe costs associated with an auditing program are worth it in the long run Ideally your organization is performing audits on a regular basis across all service types locations and payers Weve all seen claims that have been denied resulting in additional work that may be preventable with a proper audit program The goal is to use the audit feedback to improve coding quality and lower potential risk and cost to the organization Organizations should be investing in an effective coding audit program to make your coders and providers better and enhance documentation improvement from the providers
Questions
Thank you for your attentionLynn Handy
Vice President of Coding amp Audit ServicesLynnhandymanagedresourcesinccom

Procedure CodingFinding Procedures were sometimes coded incorrectly
Recommendation The entire medical record should be reviewed and all procedures coded as documented Coding procedures incorrectly or assigning incorrect CPT codes may result in lost revenue
bull Incorrect root operation
o Revise principal procedure to 0DQ68ZZ for clipping of the ulcer per OP report clipping is root operation repair
bull Biopsy versus Excision
o Procedure 0DBA0ZX (biopsy of jejunum) should change to 0DBA0ZZ (excision of jejunum) per op note this was not a biopsy procedure
bull Coding Guideline error
o Remove 0RG10K0 for allograft due to being inclusive in principal procedure
o Remove codes for adhesiolysis 0DN80ZZ 0UN10ZZ and 0UN90ZZ due to no significance noted per OP report
bull Incorrect approach
o Revise 0TF63ZZ (fragmentation percutaneous approach) to 0TF68ZZ (fragmentation endoscopic) for procedure performed via scope per the operative report
bull Procedure coded without provider documentation
o Remove secondary procedure of excisional debridement (0JB90ZZ) due to lack of documentation of excisional debridement per operative report The header in the operative report documents IampD and debridement but the body of the operative report only documents an IampD
bull Incorrect CPT code assignment
o Post-op note supports the nerve block injections of four nerves therefore code 64421 (multiple nerve block) should replace 64420 (injection of one intercostal nerve)
Queries Finding Conflicting incomplete and vague documentation is found within provider chart notes
Recommendation Prior to code assignment if the coder finds ambiguous or conflicting documentation the provider should be queried
Reference AHA Coding Clinic 2002 2nd Quarter pages 17-18
bull Query for acute blood loss anemia since hgb has dropped and patient is being transfused PRBC
bull Recommend query to clarify if cardiorenal syndrome is current as it is documented per 627 nephrology consult but unclear if current
bull Documentation does not support SIRS noninfectious without organ failure It is conflicting since patient has respiratory failure Query should be initiated for clarification with or without organ failure or infectious or non-infectious Patient has pneumonia per query as well as last progress note therefore if SIRS is not further specified per query PNA should be sequenced as principal diagnosis and SIRS should be removed
bull Recommend provider query necrotizing lung consolidation noted on DS as principal diagnosis-unclear does the patient have lobar pneumonia Secondary dx states necrotic pneumonia which is coded as principal diagnosis-this diagnosis is clear but consolidation portion is unclear
bull Recommend query for preterm labor delivery at 301 weeks
bull RECOMMEND QUERY no chest pain on admit per ER and HP cardiology provider states no CP with ER stating chest pressure the day prior to admit Appears patient was admitted due to elevated troponins which cardiology says are likely due to hypotension and AKI DS states chest pain but also says bradycardia and hypotension were the reason for admit
bull RECOMMEND QUERY no chest pain on admit per ER and HP cardiology provider states no CP with ER stating chest pressure the day prior to admit Appears patient was admitted due to elevated troponins which cardiology says are likely due to hypotension and AKI DS states chest pain but also says bradycardia and hypotension were the reason for admit
bull Query the provider regarding pathology report notation of endometriosis andor possible re-sequence of stenosis as principal diagnosis as it also meets principal diagnosis guidelines This would result in an MS-DRG change to 742 and APR-DRG change to 513
bull QUERY secondary diagnosis MCC and ROM 4 code T3166 (60 TBSA of which 60 are third degree burns) Chart notes do not specify how much of TBSA was actually third degree If after query TBSA is found to be less than 50 (T3164) then ROM will change from 4 to 3 but no change to overall APR-DRG or weight
Auditor Quality amp Productivity
Audit Productivity Standards
It takes twice as long to audit a chart as it does to code it a statistic that takes into account the time to document an explanation of any coding decision the auditor is not in agreement with o For example in an emergency department audit with a productivity of 12
charts per hour for a coder our auditors would probably be able to review six per hour
o If there are multiple services to audit on each encounter the productivity may only be 4 per hour
o The amount of detail you put into your audit report will also be a factorndash Are you using an automated audit softwarendash Are you using a spreadsheet to auditndash How many Systems are needed to complete the audit
Coder Quality Audits
Quality Audits (QA) should be done on your coders and auditors regularly Frequent reviews with smaller sample size will allow more consistent
review and feedbacko Example 10 charts per month per coder if the coder passes 2-3 months
consecutively with 95 or better score move them to quarterly reviewso Some QA programs review a percentage of the coders work This
methodology requires more time and resources
Auditor QA should also score and comment on the accuracy of the audit comments and recommendations
Presenting the Audit Results
Presenting the Audit Results
Communicating the Audit FindingsoWho requested the AuditoWho are you reporting the finding to
ndash CEOndash CFOndash Physicianndash Revenue Cycle Managerndash HIM Directorndash Billing Managerndash Coding Manager
ReportsAudit Resultspptx
Post Audit Education
Provider Education
Provider Education is best received when it is specific to the provider(s) 11 sessions going over the audit result Look at their notes with them
oHighlight areas for documentation improvementoReinforce Coding Guidelines that are specific to themoAsk them to share how they establish their LOS for E amp M serviceso Integrate their EMR system into the training
Provider Education
Group Training SessionsoUse the audit results to identify common issues within a specialty group
ndash Refer to the Executive Summary reportoVery effective for identifying system issues
ndash Teaching Attestationsndash Templatesndash Copy and Pastendash Cloned notes
o Everyone hears the same messagesoAn Issue may not appear on the individual audit but is still a concern for the
group
Education Delivery
In person or remote sessionso Factors to consider
ndash Providers scheduleavailabilityndash Location(s)ndash Personality of the providerndash Budget
Coder Education
Coders do well in group training so they can learn from each other 11 training allows the coder to get feedback on their coding
Handling Audit Disputes
Handling Audit Disputes
Be open to all points of viewo Let the documentation tell the story
Refer to the guidelines Ask
oCan we defend the reported service with the current documentation
Self Disclosures Refunds and Corrected Billing
Overpayment
In general If a person has received an overpayment the person shallo report and return the overpayment to the Secretary the State an
intermediary a carrier or a contractor as appropriate at the correct address and ndash notify the Secretary State intermediary carrier or contractor to whom the overpayment was returned in writing of the reason for the overpayment
What is an ldquoOverpaymentrdquo ndash The term ldquooverpaymentrdquo means any funds that a person receives or retains under subchapter XVIII or XIX of this chapter to which the person after applicable reconciliation is not entitled under such subchapter
Self Disclosure
The Office of Inspector General (OIG) has several self-disclosure processes that can be used to report potential fraud in Department of Health and Human Services (HHS) programs Choose the one that applies to you from the following descriptions to learn moreo Health Care Provider Self-Disclosures
ndash Health care providers suppliers or other individuals or entities subject to Civil Monetary Penalties can use the Provider Self-Disclosure Protocol which was created in 1998 to voluntarily disclose self-discovered evidence of potential fraud Self-disclosure gives providers the opportunity to avoid the costs and disruptions associated with a Government-directed investigation and civil or administrative litigation Visit the Provider Self-Disclosure Protocol webpage for more information
o HHS Contractor Self-Disclosuresndash Contractors are individuals businesses or other legal entities that are awarded Government contracts or
subcontracts to provide services to the Department of Health and Human Services (HHS) OIGs contractor self-disclosure program enables contractors to self-disclose potential violations of the False Claims Act and various Federal criminal laws involving fraud conflict of interest bribery or gratuity This self-disclosure process is available for those entities with a Federal Acquisition Regulation-based contract Visit the Contractor Self-Disclosure webpage for more information
o HHS Grantee Self-Disclosuresndash HHS grantees or subrecipients may voluntarily disclose evidence of potential violations of Federal criminal law
involving fraud bribery or gratuity violations potentially affecting the Federal award 45 CFR 75113 notes mandatory disclosures of criminal offenses that non-Federal entities must make with respect to HHS grants Recipients submitting disclosures in connection with this requirement should include the subject reference line Mandatory Grant Disclosure Recipients choosing to disclose conduct that may not fit squarely within the scope of offenses described in 45 CFR 75113 should include the following subject reference line in the submission Voluntary Grant Disclosure
Medicare 60 day rule
The 60 Day Rule (Medicare Parts A amp B) o The 60 day time period for reportingreturning begins when either
ndash The reasonable diligence is completed orndash On the day the provider received credible information of a potential overpayment (if the
provider fails to conduct reasonable diligence) o For an investigation to be conducted in a ldquotimelyrdquo manner providers typically
must complete the investigation within 6 months from receipt of credible information indicating there may be an overpayment
ndash ndash 6-month timeframe may potentially be extended under ldquoextraordinary circumstancesrdquo ndash 8 months generally the maximum total time to return overpayments The government recommends that providers maintain records documenting ldquoreasonable diligencerdquo
Medicare 60 Day Rule
Six-year lookback period ndash Sometimes possible to use a shorter period depending on the facts at issue Amount to be repaid ndash May vary depending on the method used to
reportreturn eg Medicare administrative contractor (ldquoMACrdquo) v self-disclosure Overpayment notification ndash After receiving an overpayment
notification from the government you should investigate for related overpayments eg other time periods
Medicare 60 Day Rule
Self-disclosure protocols ndashoA submission to the OIG or CMS protocols suspends the 60 day requirement
for returning overpayments until a settlement agreement is executed ndash ndash OIGrsquos Self-Disclosure Protocol (SDP) ndash ndash CMS Voluntary Self-Referral Disclosure Protocol (SRDP) ndash
o Self-disclosures to other agencies do not suspend the repayment deadlinendash ndash Eg Department of Justice local US Attorneyrsquos Office Medicaid Fraud Control Unit
Medicare 60 Day Rule
Facilitating Compliance With the 60 Day Rule Compliance programs should include o ndash Appropriate policies and procedures o ndash Periodic billing and coding audits to proactively identify overpaymentso ndash Focus on high-risk areas o ndash Utilization of publicly available government resources to guide audit efforts o ndash Investigating any suspected incidents of non-compliance with federal health
care program requirements
Self Disclosure
Choice of AgencyoOIG ndash Self-Disclosure Protocol
ndash ndash Conduct involving false billingndash ndash Conduct involving excluded personsndash ndash Conduct involving the Anti-Kickback Statute (including conduct thatndash violates both the AKS and Stark Law)
oCMS ndash Self-Referral Disclosure Protocolndash ndash Conduct involving only violations of the Stark Law
oDOJndash ndash May be appropriate when provider believes a FCA release is necessary
Summary
The Cost of a Well-Executed Coding Audit ProcessThe costs associated with an auditing program are worth it in the long run Ideally your organization is performing audits on a regular basis across all service types locations and payers Weve all seen claims that have been denied resulting in additional work that may be preventable with a proper audit program The goal is to use the audit feedback to improve coding quality and lower potential risk and cost to the organization Organizations should be investing in an effective coding audit program to make your coders and providers better and enhance documentation improvement from the providers
Questions
Thank you for your attentionLynn Handy
Vice President of Coding amp Audit ServicesLynnhandymanagedresourcesinccom

Queries Finding Conflicting incomplete and vague documentation is found within provider chart notes
Recommendation Prior to code assignment if the coder finds ambiguous or conflicting documentation the provider should be queried
Reference AHA Coding Clinic 2002 2nd Quarter pages 17-18
bull Query for acute blood loss anemia since hgb has dropped and patient is being transfused PRBC
bull Recommend query to clarify if cardiorenal syndrome is current as it is documented per 627 nephrology consult but unclear if current
bull Documentation does not support SIRS noninfectious without organ failure It is conflicting since patient has respiratory failure Query should be initiated for clarification with or without organ failure or infectious or non-infectious Patient has pneumonia per query as well as last progress note therefore if SIRS is not further specified per query PNA should be sequenced as principal diagnosis and SIRS should be removed
bull Recommend provider query necrotizing lung consolidation noted on DS as principal diagnosis-unclear does the patient have lobar pneumonia Secondary dx states necrotic pneumonia which is coded as principal diagnosis-this diagnosis is clear but consolidation portion is unclear
bull Recommend query for preterm labor delivery at 301 weeks
bull RECOMMEND QUERY no chest pain on admit per ER and HP cardiology provider states no CP with ER stating chest pressure the day prior to admit Appears patient was admitted due to elevated troponins which cardiology says are likely due to hypotension and AKI DS states chest pain but also says bradycardia and hypotension were the reason for admit
bull RECOMMEND QUERY no chest pain on admit per ER and HP cardiology provider states no CP with ER stating chest pressure the day prior to admit Appears patient was admitted due to elevated troponins which cardiology says are likely due to hypotension and AKI DS states chest pain but also says bradycardia and hypotension were the reason for admit
bull Query the provider regarding pathology report notation of endometriosis andor possible re-sequence of stenosis as principal diagnosis as it also meets principal diagnosis guidelines This would result in an MS-DRG change to 742 and APR-DRG change to 513
bull QUERY secondary diagnosis MCC and ROM 4 code T3166 (60 TBSA of which 60 are third degree burns) Chart notes do not specify how much of TBSA was actually third degree If after query TBSA is found to be less than 50 (T3164) then ROM will change from 4 to 3 but no change to overall APR-DRG or weight
Auditor Quality amp Productivity
Audit Productivity Standards
It takes twice as long to audit a chart as it does to code it a statistic that takes into account the time to document an explanation of any coding decision the auditor is not in agreement with o For example in an emergency department audit with a productivity of 12
charts per hour for a coder our auditors would probably be able to review six per hour
o If there are multiple services to audit on each encounter the productivity may only be 4 per hour
o The amount of detail you put into your audit report will also be a factorndash Are you using an automated audit softwarendash Are you using a spreadsheet to auditndash How many Systems are needed to complete the audit
Coder Quality Audits
Quality Audits (QA) should be done on your coders and auditors regularly Frequent reviews with smaller sample size will allow more consistent
review and feedbacko Example 10 charts per month per coder if the coder passes 2-3 months
consecutively with 95 or better score move them to quarterly reviewso Some QA programs review a percentage of the coders work This
methodology requires more time and resources
Auditor QA should also score and comment on the accuracy of the audit comments and recommendations
Presenting the Audit Results
Presenting the Audit Results
Communicating the Audit FindingsoWho requested the AuditoWho are you reporting the finding to
ndash CEOndash CFOndash Physicianndash Revenue Cycle Managerndash HIM Directorndash Billing Managerndash Coding Manager
ReportsAudit Resultspptx
Post Audit Education
Provider Education
Provider Education is best received when it is specific to the provider(s) 11 sessions going over the audit result Look at their notes with them
oHighlight areas for documentation improvementoReinforce Coding Guidelines that are specific to themoAsk them to share how they establish their LOS for E amp M serviceso Integrate their EMR system into the training
Provider Education
Group Training SessionsoUse the audit results to identify common issues within a specialty group
ndash Refer to the Executive Summary reportoVery effective for identifying system issues
ndash Teaching Attestationsndash Templatesndash Copy and Pastendash Cloned notes
o Everyone hears the same messagesoAn Issue may not appear on the individual audit but is still a concern for the
group
Education Delivery
In person or remote sessionso Factors to consider
ndash Providers scheduleavailabilityndash Location(s)ndash Personality of the providerndash Budget
Coder Education
Coders do well in group training so they can learn from each other 11 training allows the coder to get feedback on their coding
Handling Audit Disputes
Handling Audit Disputes
Be open to all points of viewo Let the documentation tell the story
Refer to the guidelines Ask
oCan we defend the reported service with the current documentation
Self Disclosures Refunds and Corrected Billing
Overpayment
In general If a person has received an overpayment the person shallo report and return the overpayment to the Secretary the State an
intermediary a carrier or a contractor as appropriate at the correct address and ndash notify the Secretary State intermediary carrier or contractor to whom the overpayment was returned in writing of the reason for the overpayment
What is an ldquoOverpaymentrdquo ndash The term ldquooverpaymentrdquo means any funds that a person receives or retains under subchapter XVIII or XIX of this chapter to which the person after applicable reconciliation is not entitled under such subchapter
Self Disclosure
The Office of Inspector General (OIG) has several self-disclosure processes that can be used to report potential fraud in Department of Health and Human Services (HHS) programs Choose the one that applies to you from the following descriptions to learn moreo Health Care Provider Self-Disclosures
ndash Health care providers suppliers or other individuals or entities subject to Civil Monetary Penalties can use the Provider Self-Disclosure Protocol which was created in 1998 to voluntarily disclose self-discovered evidence of potential fraud Self-disclosure gives providers the opportunity to avoid the costs and disruptions associated with a Government-directed investigation and civil or administrative litigation Visit the Provider Self-Disclosure Protocol webpage for more information
o HHS Contractor Self-Disclosuresndash Contractors are individuals businesses or other legal entities that are awarded Government contracts or
subcontracts to provide services to the Department of Health and Human Services (HHS) OIGs contractor self-disclosure program enables contractors to self-disclose potential violations of the False Claims Act and various Federal criminal laws involving fraud conflict of interest bribery or gratuity This self-disclosure process is available for those entities with a Federal Acquisition Regulation-based contract Visit the Contractor Self-Disclosure webpage for more information
o HHS Grantee Self-Disclosuresndash HHS grantees or subrecipients may voluntarily disclose evidence of potential violations of Federal criminal law
involving fraud bribery or gratuity violations potentially affecting the Federal award 45 CFR 75113 notes mandatory disclosures of criminal offenses that non-Federal entities must make with respect to HHS grants Recipients submitting disclosures in connection with this requirement should include the subject reference line Mandatory Grant Disclosure Recipients choosing to disclose conduct that may not fit squarely within the scope of offenses described in 45 CFR 75113 should include the following subject reference line in the submission Voluntary Grant Disclosure
Medicare 60 day rule
The 60 Day Rule (Medicare Parts A amp B) o The 60 day time period for reportingreturning begins when either
ndash The reasonable diligence is completed orndash On the day the provider received credible information of a potential overpayment (if the
provider fails to conduct reasonable diligence) o For an investigation to be conducted in a ldquotimelyrdquo manner providers typically
must complete the investigation within 6 months from receipt of credible information indicating there may be an overpayment
ndash ndash 6-month timeframe may potentially be extended under ldquoextraordinary circumstancesrdquo ndash 8 months generally the maximum total time to return overpayments The government recommends that providers maintain records documenting ldquoreasonable diligencerdquo
Medicare 60 Day Rule
Six-year lookback period ndash Sometimes possible to use a shorter period depending on the facts at issue Amount to be repaid ndash May vary depending on the method used to
reportreturn eg Medicare administrative contractor (ldquoMACrdquo) v self-disclosure Overpayment notification ndash After receiving an overpayment
notification from the government you should investigate for related overpayments eg other time periods
Medicare 60 Day Rule
Self-disclosure protocols ndashoA submission to the OIG or CMS protocols suspends the 60 day requirement
for returning overpayments until a settlement agreement is executed ndash ndash OIGrsquos Self-Disclosure Protocol (SDP) ndash ndash CMS Voluntary Self-Referral Disclosure Protocol (SRDP) ndash
o Self-disclosures to other agencies do not suspend the repayment deadlinendash ndash Eg Department of Justice local US Attorneyrsquos Office Medicaid Fraud Control Unit
Medicare 60 Day Rule
Facilitating Compliance With the 60 Day Rule Compliance programs should include o ndash Appropriate policies and procedures o ndash Periodic billing and coding audits to proactively identify overpaymentso ndash Focus on high-risk areas o ndash Utilization of publicly available government resources to guide audit efforts o ndash Investigating any suspected incidents of non-compliance with federal health
care program requirements
Self Disclosure
Choice of AgencyoOIG ndash Self-Disclosure Protocol
ndash ndash Conduct involving false billingndash ndash Conduct involving excluded personsndash ndash Conduct involving the Anti-Kickback Statute (including conduct thatndash violates both the AKS and Stark Law)
oCMS ndash Self-Referral Disclosure Protocolndash ndash Conduct involving only violations of the Stark Law
oDOJndash ndash May be appropriate when provider believes a FCA release is necessary
Summary
The Cost of a Well-Executed Coding Audit ProcessThe costs associated with an auditing program are worth it in the long run Ideally your organization is performing audits on a regular basis across all service types locations and payers Weve all seen claims that have been denied resulting in additional work that may be preventable with a proper audit program The goal is to use the audit feedback to improve coding quality and lower potential risk and cost to the organization Organizations should be investing in an effective coding audit program to make your coders and providers better and enhance documentation improvement from the providers
Questions
Thank you for your attentionLynn Handy
Vice President of Coding amp Audit ServicesLynnhandymanagedresourcesinccom

Auditor Quality amp Productivity
Audit Productivity Standards
It takes twice as long to audit a chart as it does to code it a statistic that takes into account the time to document an explanation of any coding decision the auditor is not in agreement with o For example in an emergency department audit with a productivity of 12
charts per hour for a coder our auditors would probably be able to review six per hour
o If there are multiple services to audit on each encounter the productivity may only be 4 per hour
o The amount of detail you put into your audit report will also be a factorndash Are you using an automated audit softwarendash Are you using a spreadsheet to auditndash How many Systems are needed to complete the audit
Coder Quality Audits
Quality Audits (QA) should be done on your coders and auditors regularly Frequent reviews with smaller sample size will allow more consistent
review and feedbacko Example 10 charts per month per coder if the coder passes 2-3 months
consecutively with 95 or better score move them to quarterly reviewso Some QA programs review a percentage of the coders work This
methodology requires more time and resources
Auditor QA should also score and comment on the accuracy of the audit comments and recommendations
Presenting the Audit Results
Presenting the Audit Results
Communicating the Audit FindingsoWho requested the AuditoWho are you reporting the finding to
ndash CEOndash CFOndash Physicianndash Revenue Cycle Managerndash HIM Directorndash Billing Managerndash Coding Manager
ReportsAudit Resultspptx
Post Audit Education
Provider Education
Provider Education is best received when it is specific to the provider(s) 11 sessions going over the audit result Look at their notes with them
oHighlight areas for documentation improvementoReinforce Coding Guidelines that are specific to themoAsk them to share how they establish their LOS for E amp M serviceso Integrate their EMR system into the training
Provider Education
Group Training SessionsoUse the audit results to identify common issues within a specialty group
ndash Refer to the Executive Summary reportoVery effective for identifying system issues
ndash Teaching Attestationsndash Templatesndash Copy and Pastendash Cloned notes
o Everyone hears the same messagesoAn Issue may not appear on the individual audit but is still a concern for the
group
Education Delivery
In person or remote sessionso Factors to consider
ndash Providers scheduleavailabilityndash Location(s)ndash Personality of the providerndash Budget
Coder Education
Coders do well in group training so they can learn from each other 11 training allows the coder to get feedback on their coding
Handling Audit Disputes
Handling Audit Disputes
Be open to all points of viewo Let the documentation tell the story
Refer to the guidelines Ask
oCan we defend the reported service with the current documentation
Self Disclosures Refunds and Corrected Billing
Overpayment
In general If a person has received an overpayment the person shallo report and return the overpayment to the Secretary the State an
intermediary a carrier or a contractor as appropriate at the correct address and ndash notify the Secretary State intermediary carrier or contractor to whom the overpayment was returned in writing of the reason for the overpayment
What is an ldquoOverpaymentrdquo ndash The term ldquooverpaymentrdquo means any funds that a person receives or retains under subchapter XVIII or XIX of this chapter to which the person after applicable reconciliation is not entitled under such subchapter
Self Disclosure
The Office of Inspector General (OIG) has several self-disclosure processes that can be used to report potential fraud in Department of Health and Human Services (HHS) programs Choose the one that applies to you from the following descriptions to learn moreo Health Care Provider Self-Disclosures
ndash Health care providers suppliers or other individuals or entities subject to Civil Monetary Penalties can use the Provider Self-Disclosure Protocol which was created in 1998 to voluntarily disclose self-discovered evidence of potential fraud Self-disclosure gives providers the opportunity to avoid the costs and disruptions associated with a Government-directed investigation and civil or administrative litigation Visit the Provider Self-Disclosure Protocol webpage for more information
o HHS Contractor Self-Disclosuresndash Contractors are individuals businesses or other legal entities that are awarded Government contracts or
subcontracts to provide services to the Department of Health and Human Services (HHS) OIGs contractor self-disclosure program enables contractors to self-disclose potential violations of the False Claims Act and various Federal criminal laws involving fraud conflict of interest bribery or gratuity This self-disclosure process is available for those entities with a Federal Acquisition Regulation-based contract Visit the Contractor Self-Disclosure webpage for more information
o HHS Grantee Self-Disclosuresndash HHS grantees or subrecipients may voluntarily disclose evidence of potential violations of Federal criminal law
involving fraud bribery or gratuity violations potentially affecting the Federal award 45 CFR 75113 notes mandatory disclosures of criminal offenses that non-Federal entities must make with respect to HHS grants Recipients submitting disclosures in connection with this requirement should include the subject reference line Mandatory Grant Disclosure Recipients choosing to disclose conduct that may not fit squarely within the scope of offenses described in 45 CFR 75113 should include the following subject reference line in the submission Voluntary Grant Disclosure
Medicare 60 day rule
The 60 Day Rule (Medicare Parts A amp B) o The 60 day time period for reportingreturning begins when either
ndash The reasonable diligence is completed orndash On the day the provider received credible information of a potential overpayment (if the
provider fails to conduct reasonable diligence) o For an investigation to be conducted in a ldquotimelyrdquo manner providers typically
must complete the investigation within 6 months from receipt of credible information indicating there may be an overpayment
ndash ndash 6-month timeframe may potentially be extended under ldquoextraordinary circumstancesrdquo ndash 8 months generally the maximum total time to return overpayments The government recommends that providers maintain records documenting ldquoreasonable diligencerdquo
Medicare 60 Day Rule
Six-year lookback period ndash Sometimes possible to use a shorter period depending on the facts at issue Amount to be repaid ndash May vary depending on the method used to
reportreturn eg Medicare administrative contractor (ldquoMACrdquo) v self-disclosure Overpayment notification ndash After receiving an overpayment
notification from the government you should investigate for related overpayments eg other time periods
Medicare 60 Day Rule
Self-disclosure protocols ndashoA submission to the OIG or CMS protocols suspends the 60 day requirement
for returning overpayments until a settlement agreement is executed ndash ndash OIGrsquos Self-Disclosure Protocol (SDP) ndash ndash CMS Voluntary Self-Referral Disclosure Protocol (SRDP) ndash
o Self-disclosures to other agencies do not suspend the repayment deadlinendash ndash Eg Department of Justice local US Attorneyrsquos Office Medicaid Fraud Control Unit
Medicare 60 Day Rule
Facilitating Compliance With the 60 Day Rule Compliance programs should include o ndash Appropriate policies and procedures o ndash Periodic billing and coding audits to proactively identify overpaymentso ndash Focus on high-risk areas o ndash Utilization of publicly available government resources to guide audit efforts o ndash Investigating any suspected incidents of non-compliance with federal health
care program requirements
Self Disclosure
Choice of AgencyoOIG ndash Self-Disclosure Protocol
ndash ndash Conduct involving false billingndash ndash Conduct involving excluded personsndash ndash Conduct involving the Anti-Kickback Statute (including conduct thatndash violates both the AKS and Stark Law)
oCMS ndash Self-Referral Disclosure Protocolndash ndash Conduct involving only violations of the Stark Law
oDOJndash ndash May be appropriate when provider believes a FCA release is necessary
Summary
The Cost of a Well-Executed Coding Audit ProcessThe costs associated with an auditing program are worth it in the long run Ideally your organization is performing audits on a regular basis across all service types locations and payers Weve all seen claims that have been denied resulting in additional work that may be preventable with a proper audit program The goal is to use the audit feedback to improve coding quality and lower potential risk and cost to the organization Organizations should be investing in an effective coding audit program to make your coders and providers better and enhance documentation improvement from the providers
Questions
Thank you for your attentionLynn Handy
Vice President of Coding amp Audit ServicesLynnhandymanagedresourcesinccom

Audit Productivity Standards
It takes twice as long to audit a chart as it does to code it a statistic that takes into account the time to document an explanation of any coding decision the auditor is not in agreement with o For example in an emergency department audit with a productivity of 12
charts per hour for a coder our auditors would probably be able to review six per hour
o If there are multiple services to audit on each encounter the productivity may only be 4 per hour
o The amount of detail you put into your audit report will also be a factorndash Are you using an automated audit softwarendash Are you using a spreadsheet to auditndash How many Systems are needed to complete the audit
Coder Quality Audits
Quality Audits (QA) should be done on your coders and auditors regularly Frequent reviews with smaller sample size will allow more consistent
review and feedbacko Example 10 charts per month per coder if the coder passes 2-3 months
consecutively with 95 or better score move them to quarterly reviewso Some QA programs review a percentage of the coders work This
methodology requires more time and resources
Auditor QA should also score and comment on the accuracy of the audit comments and recommendations
Presenting the Audit Results
Presenting the Audit Results
Communicating the Audit FindingsoWho requested the AuditoWho are you reporting the finding to
ndash CEOndash CFOndash Physicianndash Revenue Cycle Managerndash HIM Directorndash Billing Managerndash Coding Manager
ReportsAudit Resultspptx
Post Audit Education
Provider Education
Provider Education is best received when it is specific to the provider(s) 11 sessions going over the audit result Look at their notes with them
oHighlight areas for documentation improvementoReinforce Coding Guidelines that are specific to themoAsk them to share how they establish their LOS for E amp M serviceso Integrate their EMR system into the training
Provider Education
Group Training SessionsoUse the audit results to identify common issues within a specialty group
ndash Refer to the Executive Summary reportoVery effective for identifying system issues
ndash Teaching Attestationsndash Templatesndash Copy and Pastendash Cloned notes
o Everyone hears the same messagesoAn Issue may not appear on the individual audit but is still a concern for the
group
Education Delivery
In person or remote sessionso Factors to consider
ndash Providers scheduleavailabilityndash Location(s)ndash Personality of the providerndash Budget
Coder Education
Coders do well in group training so they can learn from each other 11 training allows the coder to get feedback on their coding
Handling Audit Disputes
Handling Audit Disputes
Be open to all points of viewo Let the documentation tell the story
Refer to the guidelines Ask
oCan we defend the reported service with the current documentation
Self Disclosures Refunds and Corrected Billing
Overpayment
In general If a person has received an overpayment the person shallo report and return the overpayment to the Secretary the State an
intermediary a carrier or a contractor as appropriate at the correct address and ndash notify the Secretary State intermediary carrier or contractor to whom the overpayment was returned in writing of the reason for the overpayment
What is an ldquoOverpaymentrdquo ndash The term ldquooverpaymentrdquo means any funds that a person receives or retains under subchapter XVIII or XIX of this chapter to which the person after applicable reconciliation is not entitled under such subchapter
Self Disclosure
The Office of Inspector General (OIG) has several self-disclosure processes that can be used to report potential fraud in Department of Health and Human Services (HHS) programs Choose the one that applies to you from the following descriptions to learn moreo Health Care Provider Self-Disclosures
ndash Health care providers suppliers or other individuals or entities subject to Civil Monetary Penalties can use the Provider Self-Disclosure Protocol which was created in 1998 to voluntarily disclose self-discovered evidence of potential fraud Self-disclosure gives providers the opportunity to avoid the costs and disruptions associated with a Government-directed investigation and civil or administrative litigation Visit the Provider Self-Disclosure Protocol webpage for more information
o HHS Contractor Self-Disclosuresndash Contractors are individuals businesses or other legal entities that are awarded Government contracts or
subcontracts to provide services to the Department of Health and Human Services (HHS) OIGs contractor self-disclosure program enables contractors to self-disclose potential violations of the False Claims Act and various Federal criminal laws involving fraud conflict of interest bribery or gratuity This self-disclosure process is available for those entities with a Federal Acquisition Regulation-based contract Visit the Contractor Self-Disclosure webpage for more information
o HHS Grantee Self-Disclosuresndash HHS grantees or subrecipients may voluntarily disclose evidence of potential violations of Federal criminal law
involving fraud bribery or gratuity violations potentially affecting the Federal award 45 CFR 75113 notes mandatory disclosures of criminal offenses that non-Federal entities must make with respect to HHS grants Recipients submitting disclosures in connection with this requirement should include the subject reference line Mandatory Grant Disclosure Recipients choosing to disclose conduct that may not fit squarely within the scope of offenses described in 45 CFR 75113 should include the following subject reference line in the submission Voluntary Grant Disclosure
Medicare 60 day rule
The 60 Day Rule (Medicare Parts A amp B) o The 60 day time period for reportingreturning begins when either
ndash The reasonable diligence is completed orndash On the day the provider received credible information of a potential overpayment (if the
provider fails to conduct reasonable diligence) o For an investigation to be conducted in a ldquotimelyrdquo manner providers typically
must complete the investigation within 6 months from receipt of credible information indicating there may be an overpayment
ndash ndash 6-month timeframe may potentially be extended under ldquoextraordinary circumstancesrdquo ndash 8 months generally the maximum total time to return overpayments The government recommends that providers maintain records documenting ldquoreasonable diligencerdquo
Medicare 60 Day Rule
Six-year lookback period ndash Sometimes possible to use a shorter period depending on the facts at issue Amount to be repaid ndash May vary depending on the method used to
reportreturn eg Medicare administrative contractor (ldquoMACrdquo) v self-disclosure Overpayment notification ndash After receiving an overpayment
notification from the government you should investigate for related overpayments eg other time periods
Medicare 60 Day Rule
Self-disclosure protocols ndashoA submission to the OIG or CMS protocols suspends the 60 day requirement
for returning overpayments until a settlement agreement is executed ndash ndash OIGrsquos Self-Disclosure Protocol (SDP) ndash ndash CMS Voluntary Self-Referral Disclosure Protocol (SRDP) ndash
o Self-disclosures to other agencies do not suspend the repayment deadlinendash ndash Eg Department of Justice local US Attorneyrsquos Office Medicaid Fraud Control Unit
Medicare 60 Day Rule
Facilitating Compliance With the 60 Day Rule Compliance programs should include o ndash Appropriate policies and procedures o ndash Periodic billing and coding audits to proactively identify overpaymentso ndash Focus on high-risk areas o ndash Utilization of publicly available government resources to guide audit efforts o ndash Investigating any suspected incidents of non-compliance with federal health
care program requirements
Self Disclosure
Choice of AgencyoOIG ndash Self-Disclosure Protocol
ndash ndash Conduct involving false billingndash ndash Conduct involving excluded personsndash ndash Conduct involving the Anti-Kickback Statute (including conduct thatndash violates both the AKS and Stark Law)
oCMS ndash Self-Referral Disclosure Protocolndash ndash Conduct involving only violations of the Stark Law
oDOJndash ndash May be appropriate when provider believes a FCA release is necessary
Summary
The Cost of a Well-Executed Coding Audit ProcessThe costs associated with an auditing program are worth it in the long run Ideally your organization is performing audits on a regular basis across all service types locations and payers Weve all seen claims that have been denied resulting in additional work that may be preventable with a proper audit program The goal is to use the audit feedback to improve coding quality and lower potential risk and cost to the organization Organizations should be investing in an effective coding audit program to make your coders and providers better and enhance documentation improvement from the providers
Questions
Thank you for your attentionLynn Handy
Vice President of Coding amp Audit ServicesLynnhandymanagedresourcesinccom

Coder Quality Audits
Quality Audits (QA) should be done on your coders and auditors regularly Frequent reviews with smaller sample size will allow more consistent
review and feedbacko Example 10 charts per month per coder if the coder passes 2-3 months
consecutively with 95 or better score move them to quarterly reviewso Some QA programs review a percentage of the coders work This
methodology requires more time and resources
Auditor QA should also score and comment on the accuracy of the audit comments and recommendations
Presenting the Audit Results
Presenting the Audit Results
Communicating the Audit FindingsoWho requested the AuditoWho are you reporting the finding to
ndash CEOndash CFOndash Physicianndash Revenue Cycle Managerndash HIM Directorndash Billing Managerndash Coding Manager
ReportsAudit Resultspptx
Post Audit Education
Provider Education
Provider Education is best received when it is specific to the provider(s) 11 sessions going over the audit result Look at their notes with them
oHighlight areas for documentation improvementoReinforce Coding Guidelines that are specific to themoAsk them to share how they establish their LOS for E amp M serviceso Integrate their EMR system into the training
Provider Education
Group Training SessionsoUse the audit results to identify common issues within a specialty group
ndash Refer to the Executive Summary reportoVery effective for identifying system issues
ndash Teaching Attestationsndash Templatesndash Copy and Pastendash Cloned notes
o Everyone hears the same messagesoAn Issue may not appear on the individual audit but is still a concern for the
group
Education Delivery
In person or remote sessionso Factors to consider
ndash Providers scheduleavailabilityndash Location(s)ndash Personality of the providerndash Budget
Coder Education
Coders do well in group training so they can learn from each other 11 training allows the coder to get feedback on their coding
Handling Audit Disputes
Handling Audit Disputes
Be open to all points of viewo Let the documentation tell the story
Refer to the guidelines Ask
oCan we defend the reported service with the current documentation
Self Disclosures Refunds and Corrected Billing
Overpayment
In general If a person has received an overpayment the person shallo report and return the overpayment to the Secretary the State an
intermediary a carrier or a contractor as appropriate at the correct address and ndash notify the Secretary State intermediary carrier or contractor to whom the overpayment was returned in writing of the reason for the overpayment
What is an ldquoOverpaymentrdquo ndash The term ldquooverpaymentrdquo means any funds that a person receives or retains under subchapter XVIII or XIX of this chapter to which the person after applicable reconciliation is not entitled under such subchapter
Self Disclosure
The Office of Inspector General (OIG) has several self-disclosure processes that can be used to report potential fraud in Department of Health and Human Services (HHS) programs Choose the one that applies to you from the following descriptions to learn moreo Health Care Provider Self-Disclosures
ndash Health care providers suppliers or other individuals or entities subject to Civil Monetary Penalties can use the Provider Self-Disclosure Protocol which was created in 1998 to voluntarily disclose self-discovered evidence of potential fraud Self-disclosure gives providers the opportunity to avoid the costs and disruptions associated with a Government-directed investigation and civil or administrative litigation Visit the Provider Self-Disclosure Protocol webpage for more information
o HHS Contractor Self-Disclosuresndash Contractors are individuals businesses or other legal entities that are awarded Government contracts or
subcontracts to provide services to the Department of Health and Human Services (HHS) OIGs contractor self-disclosure program enables contractors to self-disclose potential violations of the False Claims Act and various Federal criminal laws involving fraud conflict of interest bribery or gratuity This self-disclosure process is available for those entities with a Federal Acquisition Regulation-based contract Visit the Contractor Self-Disclosure webpage for more information
o HHS Grantee Self-Disclosuresndash HHS grantees or subrecipients may voluntarily disclose evidence of potential violations of Federal criminal law
involving fraud bribery or gratuity violations potentially affecting the Federal award 45 CFR 75113 notes mandatory disclosures of criminal offenses that non-Federal entities must make with respect to HHS grants Recipients submitting disclosures in connection with this requirement should include the subject reference line Mandatory Grant Disclosure Recipients choosing to disclose conduct that may not fit squarely within the scope of offenses described in 45 CFR 75113 should include the following subject reference line in the submission Voluntary Grant Disclosure
Medicare 60 day rule
The 60 Day Rule (Medicare Parts A amp B) o The 60 day time period for reportingreturning begins when either
ndash The reasonable diligence is completed orndash On the day the provider received credible information of a potential overpayment (if the
provider fails to conduct reasonable diligence) o For an investigation to be conducted in a ldquotimelyrdquo manner providers typically
must complete the investigation within 6 months from receipt of credible information indicating there may be an overpayment
ndash ndash 6-month timeframe may potentially be extended under ldquoextraordinary circumstancesrdquo ndash 8 months generally the maximum total time to return overpayments The government recommends that providers maintain records documenting ldquoreasonable diligencerdquo
Medicare 60 Day Rule
Six-year lookback period ndash Sometimes possible to use a shorter period depending on the facts at issue Amount to be repaid ndash May vary depending on the method used to
reportreturn eg Medicare administrative contractor (ldquoMACrdquo) v self-disclosure Overpayment notification ndash After receiving an overpayment
notification from the government you should investigate for related overpayments eg other time periods
Medicare 60 Day Rule
Self-disclosure protocols ndashoA submission to the OIG or CMS protocols suspends the 60 day requirement
for returning overpayments until a settlement agreement is executed ndash ndash OIGrsquos Self-Disclosure Protocol (SDP) ndash ndash CMS Voluntary Self-Referral Disclosure Protocol (SRDP) ndash
o Self-disclosures to other agencies do not suspend the repayment deadlinendash ndash Eg Department of Justice local US Attorneyrsquos Office Medicaid Fraud Control Unit
Medicare 60 Day Rule
Facilitating Compliance With the 60 Day Rule Compliance programs should include o ndash Appropriate policies and procedures o ndash Periodic billing and coding audits to proactively identify overpaymentso ndash Focus on high-risk areas o ndash Utilization of publicly available government resources to guide audit efforts o ndash Investigating any suspected incidents of non-compliance with federal health
care program requirements
Self Disclosure
Choice of AgencyoOIG ndash Self-Disclosure Protocol
ndash ndash Conduct involving false billingndash ndash Conduct involving excluded personsndash ndash Conduct involving the Anti-Kickback Statute (including conduct thatndash violates both the AKS and Stark Law)
oCMS ndash Self-Referral Disclosure Protocolndash ndash Conduct involving only violations of the Stark Law
oDOJndash ndash May be appropriate when provider believes a FCA release is necessary
Summary
The Cost of a Well-Executed Coding Audit ProcessThe costs associated with an auditing program are worth it in the long run Ideally your organization is performing audits on a regular basis across all service types locations and payers Weve all seen claims that have been denied resulting in additional work that may be preventable with a proper audit program The goal is to use the audit feedback to improve coding quality and lower potential risk and cost to the organization Organizations should be investing in an effective coding audit program to make your coders and providers better and enhance documentation improvement from the providers
Questions
Thank you for your attentionLynn Handy
Vice President of Coding amp Audit ServicesLynnhandymanagedresourcesinccom

Presenting the Audit Results
Presenting the Audit Results
Communicating the Audit FindingsoWho requested the AuditoWho are you reporting the finding to
ndash CEOndash CFOndash Physicianndash Revenue Cycle Managerndash HIM Directorndash Billing Managerndash Coding Manager
ReportsAudit Resultspptx
Post Audit Education
Provider Education
Provider Education is best received when it is specific to the provider(s) 11 sessions going over the audit result Look at their notes with them
oHighlight areas for documentation improvementoReinforce Coding Guidelines that are specific to themoAsk them to share how they establish their LOS for E amp M serviceso Integrate their EMR system into the training
Provider Education
Group Training SessionsoUse the audit results to identify common issues within a specialty group
ndash Refer to the Executive Summary reportoVery effective for identifying system issues
ndash Teaching Attestationsndash Templatesndash Copy and Pastendash Cloned notes
o Everyone hears the same messagesoAn Issue may not appear on the individual audit but is still a concern for the
group
Education Delivery
In person or remote sessionso Factors to consider
ndash Providers scheduleavailabilityndash Location(s)ndash Personality of the providerndash Budget
Coder Education
Coders do well in group training so they can learn from each other 11 training allows the coder to get feedback on their coding
Handling Audit Disputes
Handling Audit Disputes
Be open to all points of viewo Let the documentation tell the story
Refer to the guidelines Ask
oCan we defend the reported service with the current documentation
Self Disclosures Refunds and Corrected Billing
Overpayment
In general If a person has received an overpayment the person shallo report and return the overpayment to the Secretary the State an
intermediary a carrier or a contractor as appropriate at the correct address and ndash notify the Secretary State intermediary carrier or contractor to whom the overpayment was returned in writing of the reason for the overpayment
What is an ldquoOverpaymentrdquo ndash The term ldquooverpaymentrdquo means any funds that a person receives or retains under subchapter XVIII or XIX of this chapter to which the person after applicable reconciliation is not entitled under such subchapter
Self Disclosure
The Office of Inspector General (OIG) has several self-disclosure processes that can be used to report potential fraud in Department of Health and Human Services (HHS) programs Choose the one that applies to you from the following descriptions to learn moreo Health Care Provider Self-Disclosures
ndash Health care providers suppliers or other individuals or entities subject to Civil Monetary Penalties can use the Provider Self-Disclosure Protocol which was created in 1998 to voluntarily disclose self-discovered evidence of potential fraud Self-disclosure gives providers the opportunity to avoid the costs and disruptions associated with a Government-directed investigation and civil or administrative litigation Visit the Provider Self-Disclosure Protocol webpage for more information
o HHS Contractor Self-Disclosuresndash Contractors are individuals businesses or other legal entities that are awarded Government contracts or
subcontracts to provide services to the Department of Health and Human Services (HHS) OIGs contractor self-disclosure program enables contractors to self-disclose potential violations of the False Claims Act and various Federal criminal laws involving fraud conflict of interest bribery or gratuity This self-disclosure process is available for those entities with a Federal Acquisition Regulation-based contract Visit the Contractor Self-Disclosure webpage for more information
o HHS Grantee Self-Disclosuresndash HHS grantees or subrecipients may voluntarily disclose evidence of potential violations of Federal criminal law
involving fraud bribery or gratuity violations potentially affecting the Federal award 45 CFR 75113 notes mandatory disclosures of criminal offenses that non-Federal entities must make with respect to HHS grants Recipients submitting disclosures in connection with this requirement should include the subject reference line Mandatory Grant Disclosure Recipients choosing to disclose conduct that may not fit squarely within the scope of offenses described in 45 CFR 75113 should include the following subject reference line in the submission Voluntary Grant Disclosure
Medicare 60 day rule
The 60 Day Rule (Medicare Parts A amp B) o The 60 day time period for reportingreturning begins when either
ndash The reasonable diligence is completed orndash On the day the provider received credible information of a potential overpayment (if the
provider fails to conduct reasonable diligence) o For an investigation to be conducted in a ldquotimelyrdquo manner providers typically
must complete the investigation within 6 months from receipt of credible information indicating there may be an overpayment
ndash ndash 6-month timeframe may potentially be extended under ldquoextraordinary circumstancesrdquo ndash 8 months generally the maximum total time to return overpayments The government recommends that providers maintain records documenting ldquoreasonable diligencerdquo
Medicare 60 Day Rule
Six-year lookback period ndash Sometimes possible to use a shorter period depending on the facts at issue Amount to be repaid ndash May vary depending on the method used to
reportreturn eg Medicare administrative contractor (ldquoMACrdquo) v self-disclosure Overpayment notification ndash After receiving an overpayment
notification from the government you should investigate for related overpayments eg other time periods
Medicare 60 Day Rule
Self-disclosure protocols ndashoA submission to the OIG or CMS protocols suspends the 60 day requirement
for returning overpayments until a settlement agreement is executed ndash ndash OIGrsquos Self-Disclosure Protocol (SDP) ndash ndash CMS Voluntary Self-Referral Disclosure Protocol (SRDP) ndash
o Self-disclosures to other agencies do not suspend the repayment deadlinendash ndash Eg Department of Justice local US Attorneyrsquos Office Medicaid Fraud Control Unit
Medicare 60 Day Rule
Facilitating Compliance With the 60 Day Rule Compliance programs should include o ndash Appropriate policies and procedures o ndash Periodic billing and coding audits to proactively identify overpaymentso ndash Focus on high-risk areas o ndash Utilization of publicly available government resources to guide audit efforts o ndash Investigating any suspected incidents of non-compliance with federal health
care program requirements
Self Disclosure
Choice of AgencyoOIG ndash Self-Disclosure Protocol
ndash ndash Conduct involving false billingndash ndash Conduct involving excluded personsndash ndash Conduct involving the Anti-Kickback Statute (including conduct thatndash violates both the AKS and Stark Law)
oCMS ndash Self-Referral Disclosure Protocolndash ndash Conduct involving only violations of the Stark Law
oDOJndash ndash May be appropriate when provider believes a FCA release is necessary
Summary
The Cost of a Well-Executed Coding Audit ProcessThe costs associated with an auditing program are worth it in the long run Ideally your organization is performing audits on a regular basis across all service types locations and payers Weve all seen claims that have been denied resulting in additional work that may be preventable with a proper audit program The goal is to use the audit feedback to improve coding quality and lower potential risk and cost to the organization Organizations should be investing in an effective coding audit program to make your coders and providers better and enhance documentation improvement from the providers
Questions
Thank you for your attentionLynn Handy
Vice President of Coding amp Audit ServicesLynnhandymanagedresourcesinccom

Presenting the Audit Results
Communicating the Audit FindingsoWho requested the AuditoWho are you reporting the finding to
ndash CEOndash CFOndash Physicianndash Revenue Cycle Managerndash HIM Directorndash Billing Managerndash Coding Manager
ReportsAudit Resultspptx
Post Audit Education
Provider Education
Provider Education is best received when it is specific to the provider(s) 11 sessions going over the audit result Look at their notes with them
oHighlight areas for documentation improvementoReinforce Coding Guidelines that are specific to themoAsk them to share how they establish their LOS for E amp M serviceso Integrate their EMR system into the training
Provider Education
Group Training SessionsoUse the audit results to identify common issues within a specialty group
ndash Refer to the Executive Summary reportoVery effective for identifying system issues
ndash Teaching Attestationsndash Templatesndash Copy and Pastendash Cloned notes
o Everyone hears the same messagesoAn Issue may not appear on the individual audit but is still a concern for the
group
Education Delivery
In person or remote sessionso Factors to consider
ndash Providers scheduleavailabilityndash Location(s)ndash Personality of the providerndash Budget
Coder Education
Coders do well in group training so they can learn from each other 11 training allows the coder to get feedback on their coding
Handling Audit Disputes
Handling Audit Disputes
Be open to all points of viewo Let the documentation tell the story
Refer to the guidelines Ask
oCan we defend the reported service with the current documentation
Self Disclosures Refunds and Corrected Billing
Overpayment
In general If a person has received an overpayment the person shallo report and return the overpayment to the Secretary the State an
intermediary a carrier or a contractor as appropriate at the correct address and ndash notify the Secretary State intermediary carrier or contractor to whom the overpayment was returned in writing of the reason for the overpayment
What is an ldquoOverpaymentrdquo ndash The term ldquooverpaymentrdquo means any funds that a person receives or retains under subchapter XVIII or XIX of this chapter to which the person after applicable reconciliation is not entitled under such subchapter
Self Disclosure
The Office of Inspector General (OIG) has several self-disclosure processes that can be used to report potential fraud in Department of Health and Human Services (HHS) programs Choose the one that applies to you from the following descriptions to learn moreo Health Care Provider Self-Disclosures
ndash Health care providers suppliers or other individuals or entities subject to Civil Monetary Penalties can use the Provider Self-Disclosure Protocol which was created in 1998 to voluntarily disclose self-discovered evidence of potential fraud Self-disclosure gives providers the opportunity to avoid the costs and disruptions associated with a Government-directed investigation and civil or administrative litigation Visit the Provider Self-Disclosure Protocol webpage for more information
o HHS Contractor Self-Disclosuresndash Contractors are individuals businesses or other legal entities that are awarded Government contracts or
subcontracts to provide services to the Department of Health and Human Services (HHS) OIGs contractor self-disclosure program enables contractors to self-disclose potential violations of the False Claims Act and various Federal criminal laws involving fraud conflict of interest bribery or gratuity This self-disclosure process is available for those entities with a Federal Acquisition Regulation-based contract Visit the Contractor Self-Disclosure webpage for more information
o HHS Grantee Self-Disclosuresndash HHS grantees or subrecipients may voluntarily disclose evidence of potential violations of Federal criminal law
involving fraud bribery or gratuity violations potentially affecting the Federal award 45 CFR 75113 notes mandatory disclosures of criminal offenses that non-Federal entities must make with respect to HHS grants Recipients submitting disclosures in connection with this requirement should include the subject reference line Mandatory Grant Disclosure Recipients choosing to disclose conduct that may not fit squarely within the scope of offenses described in 45 CFR 75113 should include the following subject reference line in the submission Voluntary Grant Disclosure
Medicare 60 day rule
The 60 Day Rule (Medicare Parts A amp B) o The 60 day time period for reportingreturning begins when either
ndash The reasonable diligence is completed orndash On the day the provider received credible information of a potential overpayment (if the
provider fails to conduct reasonable diligence) o For an investigation to be conducted in a ldquotimelyrdquo manner providers typically
must complete the investigation within 6 months from receipt of credible information indicating there may be an overpayment
ndash ndash 6-month timeframe may potentially be extended under ldquoextraordinary circumstancesrdquo ndash 8 months generally the maximum total time to return overpayments The government recommends that providers maintain records documenting ldquoreasonable diligencerdquo
Medicare 60 Day Rule
Six-year lookback period ndash Sometimes possible to use a shorter period depending on the facts at issue Amount to be repaid ndash May vary depending on the method used to
reportreturn eg Medicare administrative contractor (ldquoMACrdquo) v self-disclosure Overpayment notification ndash After receiving an overpayment
notification from the government you should investigate for related overpayments eg other time periods
Medicare 60 Day Rule
Self-disclosure protocols ndashoA submission to the OIG or CMS protocols suspends the 60 day requirement
for returning overpayments until a settlement agreement is executed ndash ndash OIGrsquos Self-Disclosure Protocol (SDP) ndash ndash CMS Voluntary Self-Referral Disclosure Protocol (SRDP) ndash
o Self-disclosures to other agencies do not suspend the repayment deadlinendash ndash Eg Department of Justice local US Attorneyrsquos Office Medicaid Fraud Control Unit
Medicare 60 Day Rule
Facilitating Compliance With the 60 Day Rule Compliance programs should include o ndash Appropriate policies and procedures o ndash Periodic billing and coding audits to proactively identify overpaymentso ndash Focus on high-risk areas o ndash Utilization of publicly available government resources to guide audit efforts o ndash Investigating any suspected incidents of non-compliance with federal health
care program requirements
Self Disclosure
Choice of AgencyoOIG ndash Self-Disclosure Protocol
ndash ndash Conduct involving false billingndash ndash Conduct involving excluded personsndash ndash Conduct involving the Anti-Kickback Statute (including conduct thatndash violates both the AKS and Stark Law)
oCMS ndash Self-Referral Disclosure Protocolndash ndash Conduct involving only violations of the Stark Law
oDOJndash ndash May be appropriate when provider believes a FCA release is necessary
Summary
The Cost of a Well-Executed Coding Audit ProcessThe costs associated with an auditing program are worth it in the long run Ideally your organization is performing audits on a regular basis across all service types locations and payers Weve all seen claims that have been denied resulting in additional work that may be preventable with a proper audit program The goal is to use the audit feedback to improve coding quality and lower potential risk and cost to the organization Organizations should be investing in an effective coding audit program to make your coders and providers better and enhance documentation improvement from the providers
Questions
Thank you for your attentionLynn Handy
Vice President of Coding amp Audit ServicesLynnhandymanagedresourcesinccom

Post Audit Education
Provider Education
Provider Education is best received when it is specific to the provider(s) 11 sessions going over the audit result Look at their notes with them
oHighlight areas for documentation improvementoReinforce Coding Guidelines that are specific to themoAsk them to share how they establish their LOS for E amp M serviceso Integrate their EMR system into the training
Provider Education
Group Training SessionsoUse the audit results to identify common issues within a specialty group
ndash Refer to the Executive Summary reportoVery effective for identifying system issues
ndash Teaching Attestationsndash Templatesndash Copy and Pastendash Cloned notes
o Everyone hears the same messagesoAn Issue may not appear on the individual audit but is still a concern for the
group
Education Delivery
In person or remote sessionso Factors to consider
ndash Providers scheduleavailabilityndash Location(s)ndash Personality of the providerndash Budget
Coder Education
Coders do well in group training so they can learn from each other 11 training allows the coder to get feedback on their coding
Handling Audit Disputes
Handling Audit Disputes
Be open to all points of viewo Let the documentation tell the story
Refer to the guidelines Ask
oCan we defend the reported service with the current documentation
Self Disclosures Refunds and Corrected Billing
Overpayment
In general If a person has received an overpayment the person shallo report and return the overpayment to the Secretary the State an
intermediary a carrier or a contractor as appropriate at the correct address and ndash notify the Secretary State intermediary carrier or contractor to whom the overpayment was returned in writing of the reason for the overpayment
What is an ldquoOverpaymentrdquo ndash The term ldquooverpaymentrdquo means any funds that a person receives or retains under subchapter XVIII or XIX of this chapter to which the person after applicable reconciliation is not entitled under such subchapter
Self Disclosure
The Office of Inspector General (OIG) has several self-disclosure processes that can be used to report potential fraud in Department of Health and Human Services (HHS) programs Choose the one that applies to you from the following descriptions to learn moreo Health Care Provider Self-Disclosures
ndash Health care providers suppliers or other individuals or entities subject to Civil Monetary Penalties can use the Provider Self-Disclosure Protocol which was created in 1998 to voluntarily disclose self-discovered evidence of potential fraud Self-disclosure gives providers the opportunity to avoid the costs and disruptions associated with a Government-directed investigation and civil or administrative litigation Visit the Provider Self-Disclosure Protocol webpage for more information
o HHS Contractor Self-Disclosuresndash Contractors are individuals businesses or other legal entities that are awarded Government contracts or
subcontracts to provide services to the Department of Health and Human Services (HHS) OIGs contractor self-disclosure program enables contractors to self-disclose potential violations of the False Claims Act and various Federal criminal laws involving fraud conflict of interest bribery or gratuity This self-disclosure process is available for those entities with a Federal Acquisition Regulation-based contract Visit the Contractor Self-Disclosure webpage for more information
o HHS Grantee Self-Disclosuresndash HHS grantees or subrecipients may voluntarily disclose evidence of potential violations of Federal criminal law
involving fraud bribery or gratuity violations potentially affecting the Federal award 45 CFR 75113 notes mandatory disclosures of criminal offenses that non-Federal entities must make with respect to HHS grants Recipients submitting disclosures in connection with this requirement should include the subject reference line Mandatory Grant Disclosure Recipients choosing to disclose conduct that may not fit squarely within the scope of offenses described in 45 CFR 75113 should include the following subject reference line in the submission Voluntary Grant Disclosure
Medicare 60 day rule
The 60 Day Rule (Medicare Parts A amp B) o The 60 day time period for reportingreturning begins when either
ndash The reasonable diligence is completed orndash On the day the provider received credible information of a potential overpayment (if the
provider fails to conduct reasonable diligence) o For an investigation to be conducted in a ldquotimelyrdquo manner providers typically
must complete the investigation within 6 months from receipt of credible information indicating there may be an overpayment
ndash ndash 6-month timeframe may potentially be extended under ldquoextraordinary circumstancesrdquo ndash 8 months generally the maximum total time to return overpayments The government recommends that providers maintain records documenting ldquoreasonable diligencerdquo
Medicare 60 Day Rule
Six-year lookback period ndash Sometimes possible to use a shorter period depending on the facts at issue Amount to be repaid ndash May vary depending on the method used to
reportreturn eg Medicare administrative contractor (ldquoMACrdquo) v self-disclosure Overpayment notification ndash After receiving an overpayment
notification from the government you should investigate for related overpayments eg other time periods
Medicare 60 Day Rule
Self-disclosure protocols ndashoA submission to the OIG or CMS protocols suspends the 60 day requirement
for returning overpayments until a settlement agreement is executed ndash ndash OIGrsquos Self-Disclosure Protocol (SDP) ndash ndash CMS Voluntary Self-Referral Disclosure Protocol (SRDP) ndash
o Self-disclosures to other agencies do not suspend the repayment deadlinendash ndash Eg Department of Justice local US Attorneyrsquos Office Medicaid Fraud Control Unit
Medicare 60 Day Rule
Facilitating Compliance With the 60 Day Rule Compliance programs should include o ndash Appropriate policies and procedures o ndash Periodic billing and coding audits to proactively identify overpaymentso ndash Focus on high-risk areas o ndash Utilization of publicly available government resources to guide audit efforts o ndash Investigating any suspected incidents of non-compliance with federal health
care program requirements
Self Disclosure
Choice of AgencyoOIG ndash Self-Disclosure Protocol
ndash ndash Conduct involving false billingndash ndash Conduct involving excluded personsndash ndash Conduct involving the Anti-Kickback Statute (including conduct thatndash violates both the AKS and Stark Law)
oCMS ndash Self-Referral Disclosure Protocolndash ndash Conduct involving only violations of the Stark Law
oDOJndash ndash May be appropriate when provider believes a FCA release is necessary
Summary
The Cost of a Well-Executed Coding Audit ProcessThe costs associated with an auditing program are worth it in the long run Ideally your organization is performing audits on a regular basis across all service types locations and payers Weve all seen claims that have been denied resulting in additional work that may be preventable with a proper audit program The goal is to use the audit feedback to improve coding quality and lower potential risk and cost to the organization Organizations should be investing in an effective coding audit program to make your coders and providers better and enhance documentation improvement from the providers
Questions
Thank you for your attentionLynn Handy
Vice President of Coding amp Audit ServicesLynnhandymanagedresourcesinccom

Provider Education
Provider Education is best received when it is specific to the provider(s) 11 sessions going over the audit result Look at their notes with them
oHighlight areas for documentation improvementoReinforce Coding Guidelines that are specific to themoAsk them to share how they establish their LOS for E amp M serviceso Integrate their EMR system into the training
Provider Education
Group Training SessionsoUse the audit results to identify common issues within a specialty group
ndash Refer to the Executive Summary reportoVery effective for identifying system issues
ndash Teaching Attestationsndash Templatesndash Copy and Pastendash Cloned notes
o Everyone hears the same messagesoAn Issue may not appear on the individual audit but is still a concern for the
group
Education Delivery
In person or remote sessionso Factors to consider
ndash Providers scheduleavailabilityndash Location(s)ndash Personality of the providerndash Budget
Coder Education
Coders do well in group training so they can learn from each other 11 training allows the coder to get feedback on their coding
Handling Audit Disputes
Handling Audit Disputes
Be open to all points of viewo Let the documentation tell the story
Refer to the guidelines Ask
oCan we defend the reported service with the current documentation
Self Disclosures Refunds and Corrected Billing
Overpayment
In general If a person has received an overpayment the person shallo report and return the overpayment to the Secretary the State an
intermediary a carrier or a contractor as appropriate at the correct address and ndash notify the Secretary State intermediary carrier or contractor to whom the overpayment was returned in writing of the reason for the overpayment
What is an ldquoOverpaymentrdquo ndash The term ldquooverpaymentrdquo means any funds that a person receives or retains under subchapter XVIII or XIX of this chapter to which the person after applicable reconciliation is not entitled under such subchapter
Self Disclosure
The Office of Inspector General (OIG) has several self-disclosure processes that can be used to report potential fraud in Department of Health and Human Services (HHS) programs Choose the one that applies to you from the following descriptions to learn moreo Health Care Provider Self-Disclosures
ndash Health care providers suppliers or other individuals or entities subject to Civil Monetary Penalties can use the Provider Self-Disclosure Protocol which was created in 1998 to voluntarily disclose self-discovered evidence of potential fraud Self-disclosure gives providers the opportunity to avoid the costs and disruptions associated with a Government-directed investigation and civil or administrative litigation Visit the Provider Self-Disclosure Protocol webpage for more information
o HHS Contractor Self-Disclosuresndash Contractors are individuals businesses or other legal entities that are awarded Government contracts or
subcontracts to provide services to the Department of Health and Human Services (HHS) OIGs contractor self-disclosure program enables contractors to self-disclose potential violations of the False Claims Act and various Federal criminal laws involving fraud conflict of interest bribery or gratuity This self-disclosure process is available for those entities with a Federal Acquisition Regulation-based contract Visit the Contractor Self-Disclosure webpage for more information
o HHS Grantee Self-Disclosuresndash HHS grantees or subrecipients may voluntarily disclose evidence of potential violations of Federal criminal law
involving fraud bribery or gratuity violations potentially affecting the Federal award 45 CFR 75113 notes mandatory disclosures of criminal offenses that non-Federal entities must make with respect to HHS grants Recipients submitting disclosures in connection with this requirement should include the subject reference line Mandatory Grant Disclosure Recipients choosing to disclose conduct that may not fit squarely within the scope of offenses described in 45 CFR 75113 should include the following subject reference line in the submission Voluntary Grant Disclosure
Medicare 60 day rule
The 60 Day Rule (Medicare Parts A amp B) o The 60 day time period for reportingreturning begins when either
ndash The reasonable diligence is completed orndash On the day the provider received credible information of a potential overpayment (if the
provider fails to conduct reasonable diligence) o For an investigation to be conducted in a ldquotimelyrdquo manner providers typically
must complete the investigation within 6 months from receipt of credible information indicating there may be an overpayment
ndash ndash 6-month timeframe may potentially be extended under ldquoextraordinary circumstancesrdquo ndash 8 months generally the maximum total time to return overpayments The government recommends that providers maintain records documenting ldquoreasonable diligencerdquo
Medicare 60 Day Rule
Six-year lookback period ndash Sometimes possible to use a shorter period depending on the facts at issue Amount to be repaid ndash May vary depending on the method used to
reportreturn eg Medicare administrative contractor (ldquoMACrdquo) v self-disclosure Overpayment notification ndash After receiving an overpayment
notification from the government you should investigate for related overpayments eg other time periods
Medicare 60 Day Rule
Self-disclosure protocols ndashoA submission to the OIG or CMS protocols suspends the 60 day requirement
for returning overpayments until a settlement agreement is executed ndash ndash OIGrsquos Self-Disclosure Protocol (SDP) ndash ndash CMS Voluntary Self-Referral Disclosure Protocol (SRDP) ndash
o Self-disclosures to other agencies do not suspend the repayment deadlinendash ndash Eg Department of Justice local US Attorneyrsquos Office Medicaid Fraud Control Unit
Medicare 60 Day Rule
Facilitating Compliance With the 60 Day Rule Compliance programs should include o ndash Appropriate policies and procedures o ndash Periodic billing and coding audits to proactively identify overpaymentso ndash Focus on high-risk areas o ndash Utilization of publicly available government resources to guide audit efforts o ndash Investigating any suspected incidents of non-compliance with federal health
care program requirements
Self Disclosure
Choice of AgencyoOIG ndash Self-Disclosure Protocol
ndash ndash Conduct involving false billingndash ndash Conduct involving excluded personsndash ndash Conduct involving the Anti-Kickback Statute (including conduct thatndash violates both the AKS and Stark Law)
oCMS ndash Self-Referral Disclosure Protocolndash ndash Conduct involving only violations of the Stark Law
oDOJndash ndash May be appropriate when provider believes a FCA release is necessary
Summary
The Cost of a Well-Executed Coding Audit ProcessThe costs associated with an auditing program are worth it in the long run Ideally your organization is performing audits on a regular basis across all service types locations and payers Weve all seen claims that have been denied resulting in additional work that may be preventable with a proper audit program The goal is to use the audit feedback to improve coding quality and lower potential risk and cost to the organization Organizations should be investing in an effective coding audit program to make your coders and providers better and enhance documentation improvement from the providers
Questions
Thank you for your attentionLynn Handy
Vice President of Coding amp Audit ServicesLynnhandymanagedresourcesinccom

Provider Education
Group Training SessionsoUse the audit results to identify common issues within a specialty group
ndash Refer to the Executive Summary reportoVery effective for identifying system issues
ndash Teaching Attestationsndash Templatesndash Copy and Pastendash Cloned notes
o Everyone hears the same messagesoAn Issue may not appear on the individual audit but is still a concern for the
group
Education Delivery
In person or remote sessionso Factors to consider
ndash Providers scheduleavailabilityndash Location(s)ndash Personality of the providerndash Budget
Coder Education
Coders do well in group training so they can learn from each other 11 training allows the coder to get feedback on their coding
Handling Audit Disputes
Handling Audit Disputes
Be open to all points of viewo Let the documentation tell the story
Refer to the guidelines Ask
oCan we defend the reported service with the current documentation
Self Disclosures Refunds and Corrected Billing
Overpayment
In general If a person has received an overpayment the person shallo report and return the overpayment to the Secretary the State an
intermediary a carrier or a contractor as appropriate at the correct address and ndash notify the Secretary State intermediary carrier or contractor to whom the overpayment was returned in writing of the reason for the overpayment
What is an ldquoOverpaymentrdquo ndash The term ldquooverpaymentrdquo means any funds that a person receives or retains under subchapter XVIII or XIX of this chapter to which the person after applicable reconciliation is not entitled under such subchapter
Self Disclosure
The Office of Inspector General (OIG) has several self-disclosure processes that can be used to report potential fraud in Department of Health and Human Services (HHS) programs Choose the one that applies to you from the following descriptions to learn moreo Health Care Provider Self-Disclosures
ndash Health care providers suppliers or other individuals or entities subject to Civil Monetary Penalties can use the Provider Self-Disclosure Protocol which was created in 1998 to voluntarily disclose self-discovered evidence of potential fraud Self-disclosure gives providers the opportunity to avoid the costs and disruptions associated with a Government-directed investigation and civil or administrative litigation Visit the Provider Self-Disclosure Protocol webpage for more information
o HHS Contractor Self-Disclosuresndash Contractors are individuals businesses or other legal entities that are awarded Government contracts or
subcontracts to provide services to the Department of Health and Human Services (HHS) OIGs contractor self-disclosure program enables contractors to self-disclose potential violations of the False Claims Act and various Federal criminal laws involving fraud conflict of interest bribery or gratuity This self-disclosure process is available for those entities with a Federal Acquisition Regulation-based contract Visit the Contractor Self-Disclosure webpage for more information
o HHS Grantee Self-Disclosuresndash HHS grantees or subrecipients may voluntarily disclose evidence of potential violations of Federal criminal law
involving fraud bribery or gratuity violations potentially affecting the Federal award 45 CFR 75113 notes mandatory disclosures of criminal offenses that non-Federal entities must make with respect to HHS grants Recipients submitting disclosures in connection with this requirement should include the subject reference line Mandatory Grant Disclosure Recipients choosing to disclose conduct that may not fit squarely within the scope of offenses described in 45 CFR 75113 should include the following subject reference line in the submission Voluntary Grant Disclosure
Medicare 60 day rule
The 60 Day Rule (Medicare Parts A amp B) o The 60 day time period for reportingreturning begins when either
ndash The reasonable diligence is completed orndash On the day the provider received credible information of a potential overpayment (if the
provider fails to conduct reasonable diligence) o For an investigation to be conducted in a ldquotimelyrdquo manner providers typically
must complete the investigation within 6 months from receipt of credible information indicating there may be an overpayment
ndash ndash 6-month timeframe may potentially be extended under ldquoextraordinary circumstancesrdquo ndash 8 months generally the maximum total time to return overpayments The government recommends that providers maintain records documenting ldquoreasonable diligencerdquo
Medicare 60 Day Rule
Six-year lookback period ndash Sometimes possible to use a shorter period depending on the facts at issue Amount to be repaid ndash May vary depending on the method used to
reportreturn eg Medicare administrative contractor (ldquoMACrdquo) v self-disclosure Overpayment notification ndash After receiving an overpayment
notification from the government you should investigate for related overpayments eg other time periods
Medicare 60 Day Rule
Self-disclosure protocols ndashoA submission to the OIG or CMS protocols suspends the 60 day requirement
for returning overpayments until a settlement agreement is executed ndash ndash OIGrsquos Self-Disclosure Protocol (SDP) ndash ndash CMS Voluntary Self-Referral Disclosure Protocol (SRDP) ndash
o Self-disclosures to other agencies do not suspend the repayment deadlinendash ndash Eg Department of Justice local US Attorneyrsquos Office Medicaid Fraud Control Unit
Medicare 60 Day Rule
Facilitating Compliance With the 60 Day Rule Compliance programs should include o ndash Appropriate policies and procedures o ndash Periodic billing and coding audits to proactively identify overpaymentso ndash Focus on high-risk areas o ndash Utilization of publicly available government resources to guide audit efforts o ndash Investigating any suspected incidents of non-compliance with federal health
care program requirements
Self Disclosure
Choice of AgencyoOIG ndash Self-Disclosure Protocol
ndash ndash Conduct involving false billingndash ndash Conduct involving excluded personsndash ndash Conduct involving the Anti-Kickback Statute (including conduct thatndash violates both the AKS and Stark Law)
oCMS ndash Self-Referral Disclosure Protocolndash ndash Conduct involving only violations of the Stark Law
oDOJndash ndash May be appropriate when provider believes a FCA release is necessary
Summary
The Cost of a Well-Executed Coding Audit ProcessThe costs associated with an auditing program are worth it in the long run Ideally your organization is performing audits on a regular basis across all service types locations and payers Weve all seen claims that have been denied resulting in additional work that may be preventable with a proper audit program The goal is to use the audit feedback to improve coding quality and lower potential risk and cost to the organization Organizations should be investing in an effective coding audit program to make your coders and providers better and enhance documentation improvement from the providers
Questions
Thank you for your attentionLynn Handy
Vice President of Coding amp Audit ServicesLynnhandymanagedresourcesinccom

Education Delivery
In person or remote sessionso Factors to consider
ndash Providers scheduleavailabilityndash Location(s)ndash Personality of the providerndash Budget
Coder Education
Coders do well in group training so they can learn from each other 11 training allows the coder to get feedback on their coding
Handling Audit Disputes
Handling Audit Disputes
Be open to all points of viewo Let the documentation tell the story
Refer to the guidelines Ask
oCan we defend the reported service with the current documentation
Self Disclosures Refunds and Corrected Billing
Overpayment
In general If a person has received an overpayment the person shallo report and return the overpayment to the Secretary the State an
intermediary a carrier or a contractor as appropriate at the correct address and ndash notify the Secretary State intermediary carrier or contractor to whom the overpayment was returned in writing of the reason for the overpayment
What is an ldquoOverpaymentrdquo ndash The term ldquooverpaymentrdquo means any funds that a person receives or retains under subchapter XVIII or XIX of this chapter to which the person after applicable reconciliation is not entitled under such subchapter
Self Disclosure
The Office of Inspector General (OIG) has several self-disclosure processes that can be used to report potential fraud in Department of Health and Human Services (HHS) programs Choose the one that applies to you from the following descriptions to learn moreo Health Care Provider Self-Disclosures
ndash Health care providers suppliers or other individuals or entities subject to Civil Monetary Penalties can use the Provider Self-Disclosure Protocol which was created in 1998 to voluntarily disclose self-discovered evidence of potential fraud Self-disclosure gives providers the opportunity to avoid the costs and disruptions associated with a Government-directed investigation and civil or administrative litigation Visit the Provider Self-Disclosure Protocol webpage for more information
o HHS Contractor Self-Disclosuresndash Contractors are individuals businesses or other legal entities that are awarded Government contracts or
subcontracts to provide services to the Department of Health and Human Services (HHS) OIGs contractor self-disclosure program enables contractors to self-disclose potential violations of the False Claims Act and various Federal criminal laws involving fraud conflict of interest bribery or gratuity This self-disclosure process is available for those entities with a Federal Acquisition Regulation-based contract Visit the Contractor Self-Disclosure webpage for more information
o HHS Grantee Self-Disclosuresndash HHS grantees or subrecipients may voluntarily disclose evidence of potential violations of Federal criminal law
involving fraud bribery or gratuity violations potentially affecting the Federal award 45 CFR 75113 notes mandatory disclosures of criminal offenses that non-Federal entities must make with respect to HHS grants Recipients submitting disclosures in connection with this requirement should include the subject reference line Mandatory Grant Disclosure Recipients choosing to disclose conduct that may not fit squarely within the scope of offenses described in 45 CFR 75113 should include the following subject reference line in the submission Voluntary Grant Disclosure
Medicare 60 day rule
The 60 Day Rule (Medicare Parts A amp B) o The 60 day time period for reportingreturning begins when either
ndash The reasonable diligence is completed orndash On the day the provider received credible information of a potential overpayment (if the
provider fails to conduct reasonable diligence) o For an investigation to be conducted in a ldquotimelyrdquo manner providers typically
must complete the investigation within 6 months from receipt of credible information indicating there may be an overpayment
ndash ndash 6-month timeframe may potentially be extended under ldquoextraordinary circumstancesrdquo ndash 8 months generally the maximum total time to return overpayments The government recommends that providers maintain records documenting ldquoreasonable diligencerdquo
Medicare 60 Day Rule
Six-year lookback period ndash Sometimes possible to use a shorter period depending on the facts at issue Amount to be repaid ndash May vary depending on the method used to
reportreturn eg Medicare administrative contractor (ldquoMACrdquo) v self-disclosure Overpayment notification ndash After receiving an overpayment
notification from the government you should investigate for related overpayments eg other time periods
Medicare 60 Day Rule
Self-disclosure protocols ndashoA submission to the OIG or CMS protocols suspends the 60 day requirement
for returning overpayments until a settlement agreement is executed ndash ndash OIGrsquos Self-Disclosure Protocol (SDP) ndash ndash CMS Voluntary Self-Referral Disclosure Protocol (SRDP) ndash
o Self-disclosures to other agencies do not suspend the repayment deadlinendash ndash Eg Department of Justice local US Attorneyrsquos Office Medicaid Fraud Control Unit
Medicare 60 Day Rule
Facilitating Compliance With the 60 Day Rule Compliance programs should include o ndash Appropriate policies and procedures o ndash Periodic billing and coding audits to proactively identify overpaymentso ndash Focus on high-risk areas o ndash Utilization of publicly available government resources to guide audit efforts o ndash Investigating any suspected incidents of non-compliance with federal health
care program requirements
Self Disclosure
Choice of AgencyoOIG ndash Self-Disclosure Protocol
ndash ndash Conduct involving false billingndash ndash Conduct involving excluded personsndash ndash Conduct involving the Anti-Kickback Statute (including conduct thatndash violates both the AKS and Stark Law)
oCMS ndash Self-Referral Disclosure Protocolndash ndash Conduct involving only violations of the Stark Law
oDOJndash ndash May be appropriate when provider believes a FCA release is necessary
Summary
The Cost of a Well-Executed Coding Audit ProcessThe costs associated with an auditing program are worth it in the long run Ideally your organization is performing audits on a regular basis across all service types locations and payers Weve all seen claims that have been denied resulting in additional work that may be preventable with a proper audit program The goal is to use the audit feedback to improve coding quality and lower potential risk and cost to the organization Organizations should be investing in an effective coding audit program to make your coders and providers better and enhance documentation improvement from the providers
Questions
Thank you for your attentionLynn Handy
Vice President of Coding amp Audit ServicesLynnhandymanagedresourcesinccom

Coder Education
Coders do well in group training so they can learn from each other 11 training allows the coder to get feedback on their coding
Handling Audit Disputes
Handling Audit Disputes
Be open to all points of viewo Let the documentation tell the story
Refer to the guidelines Ask
oCan we defend the reported service with the current documentation
Self Disclosures Refunds and Corrected Billing
Overpayment
In general If a person has received an overpayment the person shallo report and return the overpayment to the Secretary the State an
intermediary a carrier or a contractor as appropriate at the correct address and ndash notify the Secretary State intermediary carrier or contractor to whom the overpayment was returned in writing of the reason for the overpayment
What is an ldquoOverpaymentrdquo ndash The term ldquooverpaymentrdquo means any funds that a person receives or retains under subchapter XVIII or XIX of this chapter to which the person after applicable reconciliation is not entitled under such subchapter
Self Disclosure
The Office of Inspector General (OIG) has several self-disclosure processes that can be used to report potential fraud in Department of Health and Human Services (HHS) programs Choose the one that applies to you from the following descriptions to learn moreo Health Care Provider Self-Disclosures
ndash Health care providers suppliers or other individuals or entities subject to Civil Monetary Penalties can use the Provider Self-Disclosure Protocol which was created in 1998 to voluntarily disclose self-discovered evidence of potential fraud Self-disclosure gives providers the opportunity to avoid the costs and disruptions associated with a Government-directed investigation and civil or administrative litigation Visit the Provider Self-Disclosure Protocol webpage for more information
o HHS Contractor Self-Disclosuresndash Contractors are individuals businesses or other legal entities that are awarded Government contracts or
subcontracts to provide services to the Department of Health and Human Services (HHS) OIGs contractor self-disclosure program enables contractors to self-disclose potential violations of the False Claims Act and various Federal criminal laws involving fraud conflict of interest bribery or gratuity This self-disclosure process is available for those entities with a Federal Acquisition Regulation-based contract Visit the Contractor Self-Disclosure webpage for more information
o HHS Grantee Self-Disclosuresndash HHS grantees or subrecipients may voluntarily disclose evidence of potential violations of Federal criminal law
involving fraud bribery or gratuity violations potentially affecting the Federal award 45 CFR 75113 notes mandatory disclosures of criminal offenses that non-Federal entities must make with respect to HHS grants Recipients submitting disclosures in connection with this requirement should include the subject reference line Mandatory Grant Disclosure Recipients choosing to disclose conduct that may not fit squarely within the scope of offenses described in 45 CFR 75113 should include the following subject reference line in the submission Voluntary Grant Disclosure
Medicare 60 day rule
The 60 Day Rule (Medicare Parts A amp B) o The 60 day time period for reportingreturning begins when either
ndash The reasonable diligence is completed orndash On the day the provider received credible information of a potential overpayment (if the
provider fails to conduct reasonable diligence) o For an investigation to be conducted in a ldquotimelyrdquo manner providers typically
must complete the investigation within 6 months from receipt of credible information indicating there may be an overpayment
ndash ndash 6-month timeframe may potentially be extended under ldquoextraordinary circumstancesrdquo ndash 8 months generally the maximum total time to return overpayments The government recommends that providers maintain records documenting ldquoreasonable diligencerdquo
Medicare 60 Day Rule
Six-year lookback period ndash Sometimes possible to use a shorter period depending on the facts at issue Amount to be repaid ndash May vary depending on the method used to
reportreturn eg Medicare administrative contractor (ldquoMACrdquo) v self-disclosure Overpayment notification ndash After receiving an overpayment
notification from the government you should investigate for related overpayments eg other time periods
Medicare 60 Day Rule
Self-disclosure protocols ndashoA submission to the OIG or CMS protocols suspends the 60 day requirement
for returning overpayments until a settlement agreement is executed ndash ndash OIGrsquos Self-Disclosure Protocol (SDP) ndash ndash CMS Voluntary Self-Referral Disclosure Protocol (SRDP) ndash
o Self-disclosures to other agencies do not suspend the repayment deadlinendash ndash Eg Department of Justice local US Attorneyrsquos Office Medicaid Fraud Control Unit
Medicare 60 Day Rule
Facilitating Compliance With the 60 Day Rule Compliance programs should include o ndash Appropriate policies and procedures o ndash Periodic billing and coding audits to proactively identify overpaymentso ndash Focus on high-risk areas o ndash Utilization of publicly available government resources to guide audit efforts o ndash Investigating any suspected incidents of non-compliance with federal health
care program requirements
Self Disclosure
Choice of AgencyoOIG ndash Self-Disclosure Protocol
ndash ndash Conduct involving false billingndash ndash Conduct involving excluded personsndash ndash Conduct involving the Anti-Kickback Statute (including conduct thatndash violates both the AKS and Stark Law)
oCMS ndash Self-Referral Disclosure Protocolndash ndash Conduct involving only violations of the Stark Law
oDOJndash ndash May be appropriate when provider believes a FCA release is necessary
Summary
The Cost of a Well-Executed Coding Audit ProcessThe costs associated with an auditing program are worth it in the long run Ideally your organization is performing audits on a regular basis across all service types locations and payers Weve all seen claims that have been denied resulting in additional work that may be preventable with a proper audit program The goal is to use the audit feedback to improve coding quality and lower potential risk and cost to the organization Organizations should be investing in an effective coding audit program to make your coders and providers better and enhance documentation improvement from the providers
Questions
Thank you for your attentionLynn Handy
Vice President of Coding amp Audit ServicesLynnhandymanagedresourcesinccom

Handling Audit Disputes
Handling Audit Disputes
Be open to all points of viewo Let the documentation tell the story
Refer to the guidelines Ask
oCan we defend the reported service with the current documentation
Self Disclosures Refunds and Corrected Billing
Overpayment
In general If a person has received an overpayment the person shallo report and return the overpayment to the Secretary the State an
intermediary a carrier or a contractor as appropriate at the correct address and ndash notify the Secretary State intermediary carrier or contractor to whom the overpayment was returned in writing of the reason for the overpayment
What is an ldquoOverpaymentrdquo ndash The term ldquooverpaymentrdquo means any funds that a person receives or retains under subchapter XVIII or XIX of this chapter to which the person after applicable reconciliation is not entitled under such subchapter
Self Disclosure
The Office of Inspector General (OIG) has several self-disclosure processes that can be used to report potential fraud in Department of Health and Human Services (HHS) programs Choose the one that applies to you from the following descriptions to learn moreo Health Care Provider Self-Disclosures
ndash Health care providers suppliers or other individuals or entities subject to Civil Monetary Penalties can use the Provider Self-Disclosure Protocol which was created in 1998 to voluntarily disclose self-discovered evidence of potential fraud Self-disclosure gives providers the opportunity to avoid the costs and disruptions associated with a Government-directed investigation and civil or administrative litigation Visit the Provider Self-Disclosure Protocol webpage for more information
o HHS Contractor Self-Disclosuresndash Contractors are individuals businesses or other legal entities that are awarded Government contracts or
subcontracts to provide services to the Department of Health and Human Services (HHS) OIGs contractor self-disclosure program enables contractors to self-disclose potential violations of the False Claims Act and various Federal criminal laws involving fraud conflict of interest bribery or gratuity This self-disclosure process is available for those entities with a Federal Acquisition Regulation-based contract Visit the Contractor Self-Disclosure webpage for more information
o HHS Grantee Self-Disclosuresndash HHS grantees or subrecipients may voluntarily disclose evidence of potential violations of Federal criminal law
involving fraud bribery or gratuity violations potentially affecting the Federal award 45 CFR 75113 notes mandatory disclosures of criminal offenses that non-Federal entities must make with respect to HHS grants Recipients submitting disclosures in connection with this requirement should include the subject reference line Mandatory Grant Disclosure Recipients choosing to disclose conduct that may not fit squarely within the scope of offenses described in 45 CFR 75113 should include the following subject reference line in the submission Voluntary Grant Disclosure
Medicare 60 day rule
The 60 Day Rule (Medicare Parts A amp B) o The 60 day time period for reportingreturning begins when either
ndash The reasonable diligence is completed orndash On the day the provider received credible information of a potential overpayment (if the
provider fails to conduct reasonable diligence) o For an investigation to be conducted in a ldquotimelyrdquo manner providers typically
must complete the investigation within 6 months from receipt of credible information indicating there may be an overpayment
ndash ndash 6-month timeframe may potentially be extended under ldquoextraordinary circumstancesrdquo ndash 8 months generally the maximum total time to return overpayments The government recommends that providers maintain records documenting ldquoreasonable diligencerdquo
Medicare 60 Day Rule
Six-year lookback period ndash Sometimes possible to use a shorter period depending on the facts at issue Amount to be repaid ndash May vary depending on the method used to
reportreturn eg Medicare administrative contractor (ldquoMACrdquo) v self-disclosure Overpayment notification ndash After receiving an overpayment
notification from the government you should investigate for related overpayments eg other time periods
Medicare 60 Day Rule
Self-disclosure protocols ndashoA submission to the OIG or CMS protocols suspends the 60 day requirement
for returning overpayments until a settlement agreement is executed ndash ndash OIGrsquos Self-Disclosure Protocol (SDP) ndash ndash CMS Voluntary Self-Referral Disclosure Protocol (SRDP) ndash
o Self-disclosures to other agencies do not suspend the repayment deadlinendash ndash Eg Department of Justice local US Attorneyrsquos Office Medicaid Fraud Control Unit
Medicare 60 Day Rule
Facilitating Compliance With the 60 Day Rule Compliance programs should include o ndash Appropriate policies and procedures o ndash Periodic billing and coding audits to proactively identify overpaymentso ndash Focus on high-risk areas o ndash Utilization of publicly available government resources to guide audit efforts o ndash Investigating any suspected incidents of non-compliance with federal health
care program requirements
Self Disclosure
Choice of AgencyoOIG ndash Self-Disclosure Protocol
ndash ndash Conduct involving false billingndash ndash Conduct involving excluded personsndash ndash Conduct involving the Anti-Kickback Statute (including conduct thatndash violates both the AKS and Stark Law)
oCMS ndash Self-Referral Disclosure Protocolndash ndash Conduct involving only violations of the Stark Law
oDOJndash ndash May be appropriate when provider believes a FCA release is necessary
Summary
The Cost of a Well-Executed Coding Audit ProcessThe costs associated with an auditing program are worth it in the long run Ideally your organization is performing audits on a regular basis across all service types locations and payers Weve all seen claims that have been denied resulting in additional work that may be preventable with a proper audit program The goal is to use the audit feedback to improve coding quality and lower potential risk and cost to the organization Organizations should be investing in an effective coding audit program to make your coders and providers better and enhance documentation improvement from the providers
Questions
Thank you for your attentionLynn Handy
Vice President of Coding amp Audit ServicesLynnhandymanagedresourcesinccom

Handling Audit Disputes
Be open to all points of viewo Let the documentation tell the story
Refer to the guidelines Ask
oCan we defend the reported service with the current documentation
Self Disclosures Refunds and Corrected Billing
Overpayment
In general If a person has received an overpayment the person shallo report and return the overpayment to the Secretary the State an
intermediary a carrier or a contractor as appropriate at the correct address and ndash notify the Secretary State intermediary carrier or contractor to whom the overpayment was returned in writing of the reason for the overpayment
What is an ldquoOverpaymentrdquo ndash The term ldquooverpaymentrdquo means any funds that a person receives or retains under subchapter XVIII or XIX of this chapter to which the person after applicable reconciliation is not entitled under such subchapter
Self Disclosure
The Office of Inspector General (OIG) has several self-disclosure processes that can be used to report potential fraud in Department of Health and Human Services (HHS) programs Choose the one that applies to you from the following descriptions to learn moreo Health Care Provider Self-Disclosures
ndash Health care providers suppliers or other individuals or entities subject to Civil Monetary Penalties can use the Provider Self-Disclosure Protocol which was created in 1998 to voluntarily disclose self-discovered evidence of potential fraud Self-disclosure gives providers the opportunity to avoid the costs and disruptions associated with a Government-directed investigation and civil or administrative litigation Visit the Provider Self-Disclosure Protocol webpage for more information
o HHS Contractor Self-Disclosuresndash Contractors are individuals businesses or other legal entities that are awarded Government contracts or
subcontracts to provide services to the Department of Health and Human Services (HHS) OIGs contractor self-disclosure program enables contractors to self-disclose potential violations of the False Claims Act and various Federal criminal laws involving fraud conflict of interest bribery or gratuity This self-disclosure process is available for those entities with a Federal Acquisition Regulation-based contract Visit the Contractor Self-Disclosure webpage for more information
o HHS Grantee Self-Disclosuresndash HHS grantees or subrecipients may voluntarily disclose evidence of potential violations of Federal criminal law
involving fraud bribery or gratuity violations potentially affecting the Federal award 45 CFR 75113 notes mandatory disclosures of criminal offenses that non-Federal entities must make with respect to HHS grants Recipients submitting disclosures in connection with this requirement should include the subject reference line Mandatory Grant Disclosure Recipients choosing to disclose conduct that may not fit squarely within the scope of offenses described in 45 CFR 75113 should include the following subject reference line in the submission Voluntary Grant Disclosure
Medicare 60 day rule
The 60 Day Rule (Medicare Parts A amp B) o The 60 day time period for reportingreturning begins when either
ndash The reasonable diligence is completed orndash On the day the provider received credible information of a potential overpayment (if the
provider fails to conduct reasonable diligence) o For an investigation to be conducted in a ldquotimelyrdquo manner providers typically
must complete the investigation within 6 months from receipt of credible information indicating there may be an overpayment
ndash ndash 6-month timeframe may potentially be extended under ldquoextraordinary circumstancesrdquo ndash 8 months generally the maximum total time to return overpayments The government recommends that providers maintain records documenting ldquoreasonable diligencerdquo
Medicare 60 Day Rule
Six-year lookback period ndash Sometimes possible to use a shorter period depending on the facts at issue Amount to be repaid ndash May vary depending on the method used to
reportreturn eg Medicare administrative contractor (ldquoMACrdquo) v self-disclosure Overpayment notification ndash After receiving an overpayment
notification from the government you should investigate for related overpayments eg other time periods
Medicare 60 Day Rule
Self-disclosure protocols ndashoA submission to the OIG or CMS protocols suspends the 60 day requirement
for returning overpayments until a settlement agreement is executed ndash ndash OIGrsquos Self-Disclosure Protocol (SDP) ndash ndash CMS Voluntary Self-Referral Disclosure Protocol (SRDP) ndash
o Self-disclosures to other agencies do not suspend the repayment deadlinendash ndash Eg Department of Justice local US Attorneyrsquos Office Medicaid Fraud Control Unit
Medicare 60 Day Rule
Facilitating Compliance With the 60 Day Rule Compliance programs should include o ndash Appropriate policies and procedures o ndash Periodic billing and coding audits to proactively identify overpaymentso ndash Focus on high-risk areas o ndash Utilization of publicly available government resources to guide audit efforts o ndash Investigating any suspected incidents of non-compliance with federal health
care program requirements
Self Disclosure
Choice of AgencyoOIG ndash Self-Disclosure Protocol
ndash ndash Conduct involving false billingndash ndash Conduct involving excluded personsndash ndash Conduct involving the Anti-Kickback Statute (including conduct thatndash violates both the AKS and Stark Law)
oCMS ndash Self-Referral Disclosure Protocolndash ndash Conduct involving only violations of the Stark Law
oDOJndash ndash May be appropriate when provider believes a FCA release is necessary
Summary
The Cost of a Well-Executed Coding Audit ProcessThe costs associated with an auditing program are worth it in the long run Ideally your organization is performing audits on a regular basis across all service types locations and payers Weve all seen claims that have been denied resulting in additional work that may be preventable with a proper audit program The goal is to use the audit feedback to improve coding quality and lower potential risk and cost to the organization Organizations should be investing in an effective coding audit program to make your coders and providers better and enhance documentation improvement from the providers
Questions
Thank you for your attentionLynn Handy
Vice President of Coding amp Audit ServicesLynnhandymanagedresourcesinccom

Self Disclosures Refunds and Corrected Billing
Overpayment
In general If a person has received an overpayment the person shallo report and return the overpayment to the Secretary the State an
intermediary a carrier or a contractor as appropriate at the correct address and ndash notify the Secretary State intermediary carrier or contractor to whom the overpayment was returned in writing of the reason for the overpayment
What is an ldquoOverpaymentrdquo ndash The term ldquooverpaymentrdquo means any funds that a person receives or retains under subchapter XVIII or XIX of this chapter to which the person after applicable reconciliation is not entitled under such subchapter
Self Disclosure
The Office of Inspector General (OIG) has several self-disclosure processes that can be used to report potential fraud in Department of Health and Human Services (HHS) programs Choose the one that applies to you from the following descriptions to learn moreo Health Care Provider Self-Disclosures
ndash Health care providers suppliers or other individuals or entities subject to Civil Monetary Penalties can use the Provider Self-Disclosure Protocol which was created in 1998 to voluntarily disclose self-discovered evidence of potential fraud Self-disclosure gives providers the opportunity to avoid the costs and disruptions associated with a Government-directed investigation and civil or administrative litigation Visit the Provider Self-Disclosure Protocol webpage for more information
o HHS Contractor Self-Disclosuresndash Contractors are individuals businesses or other legal entities that are awarded Government contracts or
subcontracts to provide services to the Department of Health and Human Services (HHS) OIGs contractor self-disclosure program enables contractors to self-disclose potential violations of the False Claims Act and various Federal criminal laws involving fraud conflict of interest bribery or gratuity This self-disclosure process is available for those entities with a Federal Acquisition Regulation-based contract Visit the Contractor Self-Disclosure webpage for more information
o HHS Grantee Self-Disclosuresndash HHS grantees or subrecipients may voluntarily disclose evidence of potential violations of Federal criminal law
involving fraud bribery or gratuity violations potentially affecting the Federal award 45 CFR 75113 notes mandatory disclosures of criminal offenses that non-Federal entities must make with respect to HHS grants Recipients submitting disclosures in connection with this requirement should include the subject reference line Mandatory Grant Disclosure Recipients choosing to disclose conduct that may not fit squarely within the scope of offenses described in 45 CFR 75113 should include the following subject reference line in the submission Voluntary Grant Disclosure
Medicare 60 day rule
The 60 Day Rule (Medicare Parts A amp B) o The 60 day time period for reportingreturning begins when either
ndash The reasonable diligence is completed orndash On the day the provider received credible information of a potential overpayment (if the
provider fails to conduct reasonable diligence) o For an investigation to be conducted in a ldquotimelyrdquo manner providers typically
must complete the investigation within 6 months from receipt of credible information indicating there may be an overpayment
ndash ndash 6-month timeframe may potentially be extended under ldquoextraordinary circumstancesrdquo ndash 8 months generally the maximum total time to return overpayments The government recommends that providers maintain records documenting ldquoreasonable diligencerdquo
Medicare 60 Day Rule
Six-year lookback period ndash Sometimes possible to use a shorter period depending on the facts at issue Amount to be repaid ndash May vary depending on the method used to
reportreturn eg Medicare administrative contractor (ldquoMACrdquo) v self-disclosure Overpayment notification ndash After receiving an overpayment
notification from the government you should investigate for related overpayments eg other time periods
Medicare 60 Day Rule
Self-disclosure protocols ndashoA submission to the OIG or CMS protocols suspends the 60 day requirement
for returning overpayments until a settlement agreement is executed ndash ndash OIGrsquos Self-Disclosure Protocol (SDP) ndash ndash CMS Voluntary Self-Referral Disclosure Protocol (SRDP) ndash
o Self-disclosures to other agencies do not suspend the repayment deadlinendash ndash Eg Department of Justice local US Attorneyrsquos Office Medicaid Fraud Control Unit
Medicare 60 Day Rule
Facilitating Compliance With the 60 Day Rule Compliance programs should include o ndash Appropriate policies and procedures o ndash Periodic billing and coding audits to proactively identify overpaymentso ndash Focus on high-risk areas o ndash Utilization of publicly available government resources to guide audit efforts o ndash Investigating any suspected incidents of non-compliance with federal health
care program requirements
Self Disclosure
Choice of AgencyoOIG ndash Self-Disclosure Protocol
ndash ndash Conduct involving false billingndash ndash Conduct involving excluded personsndash ndash Conduct involving the Anti-Kickback Statute (including conduct thatndash violates both the AKS and Stark Law)
oCMS ndash Self-Referral Disclosure Protocolndash ndash Conduct involving only violations of the Stark Law
oDOJndash ndash May be appropriate when provider believes a FCA release is necessary
Summary
The Cost of a Well-Executed Coding Audit ProcessThe costs associated with an auditing program are worth it in the long run Ideally your organization is performing audits on a regular basis across all service types locations and payers Weve all seen claims that have been denied resulting in additional work that may be preventable with a proper audit program The goal is to use the audit feedback to improve coding quality and lower potential risk and cost to the organization Organizations should be investing in an effective coding audit program to make your coders and providers better and enhance documentation improvement from the providers
Questions
Thank you for your attentionLynn Handy
Vice President of Coding amp Audit ServicesLynnhandymanagedresourcesinccom

Overpayment
In general If a person has received an overpayment the person shallo report and return the overpayment to the Secretary the State an
intermediary a carrier or a contractor as appropriate at the correct address and ndash notify the Secretary State intermediary carrier or contractor to whom the overpayment was returned in writing of the reason for the overpayment
What is an ldquoOverpaymentrdquo ndash The term ldquooverpaymentrdquo means any funds that a person receives or retains under subchapter XVIII or XIX of this chapter to which the person after applicable reconciliation is not entitled under such subchapter
Self Disclosure
The Office of Inspector General (OIG) has several self-disclosure processes that can be used to report potential fraud in Department of Health and Human Services (HHS) programs Choose the one that applies to you from the following descriptions to learn moreo Health Care Provider Self-Disclosures
ndash Health care providers suppliers or other individuals or entities subject to Civil Monetary Penalties can use the Provider Self-Disclosure Protocol which was created in 1998 to voluntarily disclose self-discovered evidence of potential fraud Self-disclosure gives providers the opportunity to avoid the costs and disruptions associated with a Government-directed investigation and civil or administrative litigation Visit the Provider Self-Disclosure Protocol webpage for more information
o HHS Contractor Self-Disclosuresndash Contractors are individuals businesses or other legal entities that are awarded Government contracts or
subcontracts to provide services to the Department of Health and Human Services (HHS) OIGs contractor self-disclosure program enables contractors to self-disclose potential violations of the False Claims Act and various Federal criminal laws involving fraud conflict of interest bribery or gratuity This self-disclosure process is available for those entities with a Federal Acquisition Regulation-based contract Visit the Contractor Self-Disclosure webpage for more information
o HHS Grantee Self-Disclosuresndash HHS grantees or subrecipients may voluntarily disclose evidence of potential violations of Federal criminal law
involving fraud bribery or gratuity violations potentially affecting the Federal award 45 CFR 75113 notes mandatory disclosures of criminal offenses that non-Federal entities must make with respect to HHS grants Recipients submitting disclosures in connection with this requirement should include the subject reference line Mandatory Grant Disclosure Recipients choosing to disclose conduct that may not fit squarely within the scope of offenses described in 45 CFR 75113 should include the following subject reference line in the submission Voluntary Grant Disclosure
Medicare 60 day rule
The 60 Day Rule (Medicare Parts A amp B) o The 60 day time period for reportingreturning begins when either
ndash The reasonable diligence is completed orndash On the day the provider received credible information of a potential overpayment (if the
provider fails to conduct reasonable diligence) o For an investigation to be conducted in a ldquotimelyrdquo manner providers typically
must complete the investigation within 6 months from receipt of credible information indicating there may be an overpayment
ndash ndash 6-month timeframe may potentially be extended under ldquoextraordinary circumstancesrdquo ndash 8 months generally the maximum total time to return overpayments The government recommends that providers maintain records documenting ldquoreasonable diligencerdquo
Medicare 60 Day Rule
Six-year lookback period ndash Sometimes possible to use a shorter period depending on the facts at issue Amount to be repaid ndash May vary depending on the method used to
reportreturn eg Medicare administrative contractor (ldquoMACrdquo) v self-disclosure Overpayment notification ndash After receiving an overpayment
notification from the government you should investigate for related overpayments eg other time periods
Medicare 60 Day Rule
Self-disclosure protocols ndashoA submission to the OIG or CMS protocols suspends the 60 day requirement
for returning overpayments until a settlement agreement is executed ndash ndash OIGrsquos Self-Disclosure Protocol (SDP) ndash ndash CMS Voluntary Self-Referral Disclosure Protocol (SRDP) ndash
o Self-disclosures to other agencies do not suspend the repayment deadlinendash ndash Eg Department of Justice local US Attorneyrsquos Office Medicaid Fraud Control Unit
Medicare 60 Day Rule
Facilitating Compliance With the 60 Day Rule Compliance programs should include o ndash Appropriate policies and procedures o ndash Periodic billing and coding audits to proactively identify overpaymentso ndash Focus on high-risk areas o ndash Utilization of publicly available government resources to guide audit efforts o ndash Investigating any suspected incidents of non-compliance with federal health
care program requirements
Self Disclosure
Choice of AgencyoOIG ndash Self-Disclosure Protocol
ndash ndash Conduct involving false billingndash ndash Conduct involving excluded personsndash ndash Conduct involving the Anti-Kickback Statute (including conduct thatndash violates both the AKS and Stark Law)
oCMS ndash Self-Referral Disclosure Protocolndash ndash Conduct involving only violations of the Stark Law
oDOJndash ndash May be appropriate when provider believes a FCA release is necessary
Summary
The Cost of a Well-Executed Coding Audit ProcessThe costs associated with an auditing program are worth it in the long run Ideally your organization is performing audits on a regular basis across all service types locations and payers Weve all seen claims that have been denied resulting in additional work that may be preventable with a proper audit program The goal is to use the audit feedback to improve coding quality and lower potential risk and cost to the organization Organizations should be investing in an effective coding audit program to make your coders and providers better and enhance documentation improvement from the providers
Questions
Thank you for your attentionLynn Handy
Vice President of Coding amp Audit ServicesLynnhandymanagedresourcesinccom

Self Disclosure
The Office of Inspector General (OIG) has several self-disclosure processes that can be used to report potential fraud in Department of Health and Human Services (HHS) programs Choose the one that applies to you from the following descriptions to learn moreo Health Care Provider Self-Disclosures
ndash Health care providers suppliers or other individuals or entities subject to Civil Monetary Penalties can use the Provider Self-Disclosure Protocol which was created in 1998 to voluntarily disclose self-discovered evidence of potential fraud Self-disclosure gives providers the opportunity to avoid the costs and disruptions associated with a Government-directed investigation and civil or administrative litigation Visit the Provider Self-Disclosure Protocol webpage for more information
o HHS Contractor Self-Disclosuresndash Contractors are individuals businesses or other legal entities that are awarded Government contracts or
subcontracts to provide services to the Department of Health and Human Services (HHS) OIGs contractor self-disclosure program enables contractors to self-disclose potential violations of the False Claims Act and various Federal criminal laws involving fraud conflict of interest bribery or gratuity This self-disclosure process is available for those entities with a Federal Acquisition Regulation-based contract Visit the Contractor Self-Disclosure webpage for more information
o HHS Grantee Self-Disclosuresndash HHS grantees or subrecipients may voluntarily disclose evidence of potential violations of Federal criminal law
involving fraud bribery or gratuity violations potentially affecting the Federal award 45 CFR 75113 notes mandatory disclosures of criminal offenses that non-Federal entities must make with respect to HHS grants Recipients submitting disclosures in connection with this requirement should include the subject reference line Mandatory Grant Disclosure Recipients choosing to disclose conduct that may not fit squarely within the scope of offenses described in 45 CFR 75113 should include the following subject reference line in the submission Voluntary Grant Disclosure
Medicare 60 day rule
The 60 Day Rule (Medicare Parts A amp B) o The 60 day time period for reportingreturning begins when either
ndash The reasonable diligence is completed orndash On the day the provider received credible information of a potential overpayment (if the
provider fails to conduct reasonable diligence) o For an investigation to be conducted in a ldquotimelyrdquo manner providers typically
must complete the investigation within 6 months from receipt of credible information indicating there may be an overpayment
ndash ndash 6-month timeframe may potentially be extended under ldquoextraordinary circumstancesrdquo ndash 8 months generally the maximum total time to return overpayments The government recommends that providers maintain records documenting ldquoreasonable diligencerdquo
Medicare 60 Day Rule
Six-year lookback period ndash Sometimes possible to use a shorter period depending on the facts at issue Amount to be repaid ndash May vary depending on the method used to
reportreturn eg Medicare administrative contractor (ldquoMACrdquo) v self-disclosure Overpayment notification ndash After receiving an overpayment
notification from the government you should investigate for related overpayments eg other time periods
Medicare 60 Day Rule
Self-disclosure protocols ndashoA submission to the OIG or CMS protocols suspends the 60 day requirement
for returning overpayments until a settlement agreement is executed ndash ndash OIGrsquos Self-Disclosure Protocol (SDP) ndash ndash CMS Voluntary Self-Referral Disclosure Protocol (SRDP) ndash
o Self-disclosures to other agencies do not suspend the repayment deadlinendash ndash Eg Department of Justice local US Attorneyrsquos Office Medicaid Fraud Control Unit
Medicare 60 Day Rule
Facilitating Compliance With the 60 Day Rule Compliance programs should include o ndash Appropriate policies and procedures o ndash Periodic billing and coding audits to proactively identify overpaymentso ndash Focus on high-risk areas o ndash Utilization of publicly available government resources to guide audit efforts o ndash Investigating any suspected incidents of non-compliance with federal health
care program requirements
Self Disclosure
Choice of AgencyoOIG ndash Self-Disclosure Protocol
ndash ndash Conduct involving false billingndash ndash Conduct involving excluded personsndash ndash Conduct involving the Anti-Kickback Statute (including conduct thatndash violates both the AKS and Stark Law)
oCMS ndash Self-Referral Disclosure Protocolndash ndash Conduct involving only violations of the Stark Law
oDOJndash ndash May be appropriate when provider believes a FCA release is necessary
Summary
The Cost of a Well-Executed Coding Audit ProcessThe costs associated with an auditing program are worth it in the long run Ideally your organization is performing audits on a regular basis across all service types locations and payers Weve all seen claims that have been denied resulting in additional work that may be preventable with a proper audit program The goal is to use the audit feedback to improve coding quality and lower potential risk and cost to the organization Organizations should be investing in an effective coding audit program to make your coders and providers better and enhance documentation improvement from the providers
Questions
Thank you for your attentionLynn Handy
Vice President of Coding amp Audit ServicesLynnhandymanagedresourcesinccom

Medicare 60 day rule
The 60 Day Rule (Medicare Parts A amp B) o The 60 day time period for reportingreturning begins when either
ndash The reasonable diligence is completed orndash On the day the provider received credible information of a potential overpayment (if the
provider fails to conduct reasonable diligence) o For an investigation to be conducted in a ldquotimelyrdquo manner providers typically
must complete the investigation within 6 months from receipt of credible information indicating there may be an overpayment
ndash ndash 6-month timeframe may potentially be extended under ldquoextraordinary circumstancesrdquo ndash 8 months generally the maximum total time to return overpayments The government recommends that providers maintain records documenting ldquoreasonable diligencerdquo
Medicare 60 Day Rule
Six-year lookback period ndash Sometimes possible to use a shorter period depending on the facts at issue Amount to be repaid ndash May vary depending on the method used to
reportreturn eg Medicare administrative contractor (ldquoMACrdquo) v self-disclosure Overpayment notification ndash After receiving an overpayment
notification from the government you should investigate for related overpayments eg other time periods
Medicare 60 Day Rule
Self-disclosure protocols ndashoA submission to the OIG or CMS protocols suspends the 60 day requirement
for returning overpayments until a settlement agreement is executed ndash ndash OIGrsquos Self-Disclosure Protocol (SDP) ndash ndash CMS Voluntary Self-Referral Disclosure Protocol (SRDP) ndash
o Self-disclosures to other agencies do not suspend the repayment deadlinendash ndash Eg Department of Justice local US Attorneyrsquos Office Medicaid Fraud Control Unit
Medicare 60 Day Rule
Facilitating Compliance With the 60 Day Rule Compliance programs should include o ndash Appropriate policies and procedures o ndash Periodic billing and coding audits to proactively identify overpaymentso ndash Focus on high-risk areas o ndash Utilization of publicly available government resources to guide audit efforts o ndash Investigating any suspected incidents of non-compliance with federal health
care program requirements
Self Disclosure
Choice of AgencyoOIG ndash Self-Disclosure Protocol
ndash ndash Conduct involving false billingndash ndash Conduct involving excluded personsndash ndash Conduct involving the Anti-Kickback Statute (including conduct thatndash violates both the AKS and Stark Law)
oCMS ndash Self-Referral Disclosure Protocolndash ndash Conduct involving only violations of the Stark Law
oDOJndash ndash May be appropriate when provider believes a FCA release is necessary
Summary
The Cost of a Well-Executed Coding Audit ProcessThe costs associated with an auditing program are worth it in the long run Ideally your organization is performing audits on a regular basis across all service types locations and payers Weve all seen claims that have been denied resulting in additional work that may be preventable with a proper audit program The goal is to use the audit feedback to improve coding quality and lower potential risk and cost to the organization Organizations should be investing in an effective coding audit program to make your coders and providers better and enhance documentation improvement from the providers
Questions
Thank you for your attentionLynn Handy
Vice President of Coding amp Audit ServicesLynnhandymanagedresourcesinccom

Medicare 60 Day Rule
Six-year lookback period ndash Sometimes possible to use a shorter period depending on the facts at issue Amount to be repaid ndash May vary depending on the method used to
reportreturn eg Medicare administrative contractor (ldquoMACrdquo) v self-disclosure Overpayment notification ndash After receiving an overpayment
notification from the government you should investigate for related overpayments eg other time periods
Medicare 60 Day Rule
Self-disclosure protocols ndashoA submission to the OIG or CMS protocols suspends the 60 day requirement
for returning overpayments until a settlement agreement is executed ndash ndash OIGrsquos Self-Disclosure Protocol (SDP) ndash ndash CMS Voluntary Self-Referral Disclosure Protocol (SRDP) ndash
o Self-disclosures to other agencies do not suspend the repayment deadlinendash ndash Eg Department of Justice local US Attorneyrsquos Office Medicaid Fraud Control Unit
Medicare 60 Day Rule
Facilitating Compliance With the 60 Day Rule Compliance programs should include o ndash Appropriate policies and procedures o ndash Periodic billing and coding audits to proactively identify overpaymentso ndash Focus on high-risk areas o ndash Utilization of publicly available government resources to guide audit efforts o ndash Investigating any suspected incidents of non-compliance with federal health
care program requirements
Self Disclosure
Choice of AgencyoOIG ndash Self-Disclosure Protocol
ndash ndash Conduct involving false billingndash ndash Conduct involving excluded personsndash ndash Conduct involving the Anti-Kickback Statute (including conduct thatndash violates both the AKS and Stark Law)
oCMS ndash Self-Referral Disclosure Protocolndash ndash Conduct involving only violations of the Stark Law
oDOJndash ndash May be appropriate when provider believes a FCA release is necessary
Summary
The Cost of a Well-Executed Coding Audit ProcessThe costs associated with an auditing program are worth it in the long run Ideally your organization is performing audits on a regular basis across all service types locations and payers Weve all seen claims that have been denied resulting in additional work that may be preventable with a proper audit program The goal is to use the audit feedback to improve coding quality and lower potential risk and cost to the organization Organizations should be investing in an effective coding audit program to make your coders and providers better and enhance documentation improvement from the providers
Questions
Thank you for your attentionLynn Handy
Vice President of Coding amp Audit ServicesLynnhandymanagedresourcesinccom

Medicare 60 Day Rule
Self-disclosure protocols ndashoA submission to the OIG or CMS protocols suspends the 60 day requirement
for returning overpayments until a settlement agreement is executed ndash ndash OIGrsquos Self-Disclosure Protocol (SDP) ndash ndash CMS Voluntary Self-Referral Disclosure Protocol (SRDP) ndash
o Self-disclosures to other agencies do not suspend the repayment deadlinendash ndash Eg Department of Justice local US Attorneyrsquos Office Medicaid Fraud Control Unit
Medicare 60 Day Rule
Facilitating Compliance With the 60 Day Rule Compliance programs should include o ndash Appropriate policies and procedures o ndash Periodic billing and coding audits to proactively identify overpaymentso ndash Focus on high-risk areas o ndash Utilization of publicly available government resources to guide audit efforts o ndash Investigating any suspected incidents of non-compliance with federal health
care program requirements
Self Disclosure
Choice of AgencyoOIG ndash Self-Disclosure Protocol
ndash ndash Conduct involving false billingndash ndash Conduct involving excluded personsndash ndash Conduct involving the Anti-Kickback Statute (including conduct thatndash violates both the AKS and Stark Law)
oCMS ndash Self-Referral Disclosure Protocolndash ndash Conduct involving only violations of the Stark Law
oDOJndash ndash May be appropriate when provider believes a FCA release is necessary
Summary
The Cost of a Well-Executed Coding Audit ProcessThe costs associated with an auditing program are worth it in the long run Ideally your organization is performing audits on a regular basis across all service types locations and payers Weve all seen claims that have been denied resulting in additional work that may be preventable with a proper audit program The goal is to use the audit feedback to improve coding quality and lower potential risk and cost to the organization Organizations should be investing in an effective coding audit program to make your coders and providers better and enhance documentation improvement from the providers
Questions
Thank you for your attentionLynn Handy
Vice President of Coding amp Audit ServicesLynnhandymanagedresourcesinccom

Medicare 60 Day Rule
Facilitating Compliance With the 60 Day Rule Compliance programs should include o ndash Appropriate policies and procedures o ndash Periodic billing and coding audits to proactively identify overpaymentso ndash Focus on high-risk areas o ndash Utilization of publicly available government resources to guide audit efforts o ndash Investigating any suspected incidents of non-compliance with federal health
care program requirements
Self Disclosure
Choice of AgencyoOIG ndash Self-Disclosure Protocol
ndash ndash Conduct involving false billingndash ndash Conduct involving excluded personsndash ndash Conduct involving the Anti-Kickback Statute (including conduct thatndash violates both the AKS and Stark Law)
oCMS ndash Self-Referral Disclosure Protocolndash ndash Conduct involving only violations of the Stark Law
oDOJndash ndash May be appropriate when provider believes a FCA release is necessary
Summary
The Cost of a Well-Executed Coding Audit ProcessThe costs associated with an auditing program are worth it in the long run Ideally your organization is performing audits on a regular basis across all service types locations and payers Weve all seen claims that have been denied resulting in additional work that may be preventable with a proper audit program The goal is to use the audit feedback to improve coding quality and lower potential risk and cost to the organization Organizations should be investing in an effective coding audit program to make your coders and providers better and enhance documentation improvement from the providers
Questions
Thank you for your attentionLynn Handy
Vice President of Coding amp Audit ServicesLynnhandymanagedresourcesinccom

Self Disclosure
Choice of AgencyoOIG ndash Self-Disclosure Protocol
ndash ndash Conduct involving false billingndash ndash Conduct involving excluded personsndash ndash Conduct involving the Anti-Kickback Statute (including conduct thatndash violates both the AKS and Stark Law)
oCMS ndash Self-Referral Disclosure Protocolndash ndash Conduct involving only violations of the Stark Law
oDOJndash ndash May be appropriate when provider believes a FCA release is necessary
Summary
The Cost of a Well-Executed Coding Audit ProcessThe costs associated with an auditing program are worth it in the long run Ideally your organization is performing audits on a regular basis across all service types locations and payers Weve all seen claims that have been denied resulting in additional work that may be preventable with a proper audit program The goal is to use the audit feedback to improve coding quality and lower potential risk and cost to the organization Organizations should be investing in an effective coding audit program to make your coders and providers better and enhance documentation improvement from the providers
Questions
Thank you for your attentionLynn Handy
Vice President of Coding amp Audit ServicesLynnhandymanagedresourcesinccom

Summary
The Cost of a Well-Executed Coding Audit ProcessThe costs associated with an auditing program are worth it in the long run Ideally your organization is performing audits on a regular basis across all service types locations and payers Weve all seen claims that have been denied resulting in additional work that may be preventable with a proper audit program The goal is to use the audit feedback to improve coding quality and lower potential risk and cost to the organization Organizations should be investing in an effective coding audit program to make your coders and providers better and enhance documentation improvement from the providers
Questions
Thank you for your attentionLynn Handy
Vice President of Coding amp Audit ServicesLynnhandymanagedresourcesinccom

Questions
Thank you for your attentionLynn Handy
Vice President of Coding amp Audit ServicesLynnhandymanagedresourcesinccom