Embed Size (px)
Citation preview

Namita Jayaprakash MB BcH BAO, MCEM
A disease of ancient Greeks and modern men

The history of Diabetes
The pathophysiology behind diabetes
Definitions
Management
Diabetic emergencies

Diabetes mellitus is a syndrome of chronic hyperglycemia due to relative insulin deficiency, resistance, or both


Ebers papyrus 1550 B.C
Galen and Arateus further delineated the disease 130 – 201 A.D
Arateus coined the term diabetes 150 A.D
Diabetes = ‘siphon’
‘liquefaction of the flesh and bone into urine’


Lavoisier’s legacy Late 18th century
established the concept of the respiratory quotient
Baron Justus von Liebig Identified protein, carbohydrates and fats

Claude Bernard Questioned role of pancreas in diabetes
Apollinaire Bouchardat and E. Lancereaux
Identified two forms of diabetes


1921 Banting and Best worked on ‘isletin’extraction
1922 ‘insulin’ Leonard Thompson first human recipient
1923 Nobel Prize in Medicine awarded for discovery of insulin

Sulfonylurea Introduced in 1955
Biguanide Phenformin, metformin
α – glucosidase inhibitors 1980’s
Thiazolidinediones 1990’s
Nonsulfonylureas


Key hormone involved in storage and controlled release of chemical energy
Coded for on chromosome 11
Synthesized in β – cells of pancreatic islets
Pre - proinsulin Proinsulin Insulin C-peptide

α – subunit
β – subunit
Insulin

Increases glucose uptake into cells and glycogen formation
Decreases glycogenolysis and gluconeogenesis
Increases fat deposition and decreases lipolysis
Increases protein synthesis
Increases potassium (K+) uptake into cells

Decrease [glucose]
Decrease [amino acid]
Decrease [fatty acid]
Decrease [ketoacid]
Hypokalemia

Carbohydrate metabolism
Normal blood glucose = 63 – 144 mg/dL
Liver is principal organ of glucose homeostasis
Glycogenolysis
Gluconeogenesis

Carbohydrate Glycemia
Insulin
Cell
Glucose

Glucose
Glucose – 6 – phosphate
Fructose 6 – P
Fructose 1,6 – P
Pyruvate
Glycogen
Ribose 5 – P
Uric acid
Fructose
Lactate

Mobilization of substrates for gluconeogenesis and ketogenesis
Accelerated production of glucose and ketones
Overwhelmed excretory mechanisms
Impaired removal by insulin responsive tissues





Insulin deficiency
Glucose cannot enter cells
Alternatives for cellular energy
Lipolysis -> glycerol and free fatty acids
Glycerol -> glucose
Free fatty acids -> ketones

Peripheral resistance to insulin
Increased production of glucose by the liver
Altered pancreatic insulin secretion

Secondary Diabetes Genetic defects in β – cell function
Genetic defects in insulin action
Disease of exocrine pancreas
Drug or chemical induced diabetes
Gestational Diabetes




Review
www.thelancet.com Published online December 4, 2013 http://dx.doi.org/10.1016/S0140-6736(13)62154-6 5
obtained through these assessments could provide the
level of detail needed to establish the mediator (or
mediators) of the feedback loop that interconnects β cells
with insulin-sensitive tissues, and help to unravel the
heterogeneity of the disease. Furthermore, these
assessments should complement and advance present
understanding of the best approaches to treat the
dysregulated metabolic milieu in type 2 diabetes, which
includes not only glucose but also fatty acids and
aminoacids.
Treatment of type 2 diabetesOral and injectable drugs: present knowledge, lessons learned, and implications for the futureThe increasing prevalence of type 2 diabetes has
stimulated development of many new approaches to
safely treat hyperglycaemia (fi gure 3). The aim of these
therapies is to reduce and maintain glucose
concentrations as close to normal for as long as possible
after diagnosis (panels 1, 2), and thereby prevent
development of complications. Although some therapies
have been unsuccessful because of adverse eff ects or
negligible therapeutic effi cacy, several are very well
accepted and are used worldwide. The mode of action for
most of these drugs has been reported (fi gure 3).
However, individual responses to these drugs can diff er
greatly, probably as a result of the heterogeneous nature
of the pathophysiology of type 2 diabetes. The
appendix provides further discussion on drugs that have
been widely available for more than a decade (eg,
sulfonylurea antidiabetics, biguanide antidiabetics,
α-glucosidase inhibitors, and peroxisome proliferator-
activated receptor γ agonists).
Drugs with actions dependent on the gastro-intestinal tractDrugs that mediate their eff ect through the gastro-
intestinal tract include α-glucosidase inhibitors that slow
glucose absorption by delaying degradation of complex
carbohydrates in the gastrointestinal tract;87 pramlintide,
which slows gastric emptying and thus delays glucose
absorption;88 and the bile-acid-binding resin colesevelam,
which lowers cholesterol and modifi es release of other
gastrointestinal peptides that can reduce plasma
concentrations of glucose. 89
Incretin-related products are designed to mimic or
augment the action of GLP-1 and GIP, which are released
by the intestine. GLP-1 receptor agonists are peptides
with longer half-lives than GLP-1, whereas dipeptidyl
peptidase 4 (DPP4) inhibitors block the action of DPP4,
which is responsible for rapid degradation of GLP-1 and
GIP.90 Improvement of the pharmacokinetics and
pharmaco dynamics of incretin-based drugs is under
investigation to reduce dosing and to improve glucose
control.91 Although not completely understood, infusion
of large doses of GLP-1 intravenously can normalise
glucose concentrations with less nausea or vomiting—
adverse eff ects that can be dose limiting and prevent
normalisation of glucose concentrations—than for
subcutaneous administration.92,93 Whether new drugs
can further improve glucose lowering and reduce nausea
and vomiting remains unknown. In addition to the clear
eff ect of these drugs on improvement of glycaemia,
incretin-related products might also have benefi cial
eff ects on the cardiovascular system,94,95 although
fi ndings from the fi rst two of a series of intervention
studies showed a neutral eff ect.96,97 Incretin-related
medications have been purported to increase the risk of
acute pancreatitis; this suggestion is based on fi ndings
from studies that used the inherently biased
pharmacovigilance and administrative databases.98–101
More recently, GLP-1 receptor agonists and DPP4
inhibitors have been postulated to cause malignant
transformations in the pancreas. However, this
suggestion was based on histological assessments of a
very small number of samples from brain-dead organ
donors that were inadequately matched with controls for
several crucial variables.102,103 Importantly, despite
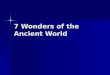
Figure 3: Drugs to treat type 2 diabetes
(A) The rate of introduction of new classes of drugs has accelerated during the past 20 years. Two classes (animal
insulin and inhaled insulin; red) are essentially no longer available as therapeutics. (B) Di ff erent classes of drugs act
on diff erent organ systems. Insulin is a replacement for the natural product of islet β cells. Classic organ systems
that have been targeted for decades comprise the pancreatic islet, liver, muscle, and adipose tissue. Non-classic
targets have been focused on recently, and include the intestine, kidneys, and brain. DPP4=dipeptidyl peptidase 4.
SGLT2=sodium–glucose co- transporter 2. GLP-1=glucagon-like peptide 1.
1940 1950 1960 1970 1980 1990 2000 2010
Sulfonylurea antidiabetics
Metformin
Human insulin
α-glucosidase inhibitors
Insulin analogues
Thiazolidinedione antidiabetics
Glinides
GLP-1 receptor agonists
Pramlintide
Inhaled insulin
DPP4 inhibitors
Colesevelam
Bromocriptine
SGLT2 inhibitors
1920 1930
Animal insulin
00
5
10
15
Cla
sses
of glu
cose
-low
erin
g d
rugs
Year
A
Classic Less classicB
Sulfonylurea antidiabetics
Glinides
GLP-1 receptor agonists
DPP4 inhibitors
Insulin
Lifestyle modification
Metformin
Thiazolidinedione antidiabetics
α-glucosidase inhibitors
Pramlintide
Colesevelam
SGLT2 inhibitors
Bromocriptine
See Online for appendix
2002
2008

Primary focus is insulin replacement
Healthy lifestyle
Prevent long term complications

Category Name
Rapid acting Insulin lispro (Humalog)
Insulin aspart (Novolog)
Insulin glulisine (Apidra)
Short acting Regular insulin (Humulin R, Novolin R)
Intermediate acting NPH (Humulin N, Novolin N)
Insulin detemir (Levemir)
Long acting Insulin glargine (Lantus)
Mixtures 70/30 Humulin/Novolin (70% NPH, 30% regular)
50/50 Humulin/Novolin (50% NPH, 50% regular)
75/25 Humalog (75% NPL, 25% lispro)
50/50 Humalog (50% NPL, 50% lispro)
70/30 NovoLog Neutral (70% protamine aspart, 30% aspart)

Intervention at time of diagnosis Metformin
Lifestyle changes
Aim to achieve and maintain recommended levels of glycemic control
Continuing timely augmentation of therapy


Review
www.thelancet.com Published online December 4, 2013 http://dx.doi.org/10.1016/S0140-6736(13)62154-6 5
obtained through these assessments could provide the
level of detail needed to establish the mediator (or
mediators) of the feedback loop that interconnects β cells
with insulin-sensitive tissues, and help to unravel the
heterogeneity of the disease. Furthermore, these
assessments should complement and advance present
understanding of the best approaches to treat the
dysregulated metabolic milieu in type 2 diabetes, which
includes not only glucose but also fatty acids and
aminoacids.
Treatment of type 2 diabetesOral and injectable drugs: present knowledge, lessons learned, and implications for the futureThe increasing prevalence of type 2 diabetes has
stimulated development of many new approaches to
safely treat hyperglycaemia (fi gure 3). The aim of these
therapies is to reduce and maintain glucose
concentrations as close to normal for as long as possible
after diagnosis (panels 1, 2), and thereby prevent
development of complications. Although some therapies
have been unsuccessful because of adverse eff ects or
negligible therapeutic effi cacy, several are very well
accepted and are used worldwide. The mode of action for
most of these drugs has been reported (fi gure 3).
However, individual responses to these drugs can diff er
greatly, probably as a result of the heterogeneous nature
of the pathophysiology of type 2 diabetes. The
appendix provides further discussion on drugs that have
been widely available for more than a decade (eg,
sulfonylurea antidiabetics, biguanide antidiabetics,
α-glucosidase inhibitors, and peroxisome proliferator-
activated receptor γ agonists).
Drugs with actions dependent on the gastro-intestinal tractDrugs that mediate their eff ect through the gastro-
intestinal tract include α-glucosidase inhibitors that slow
glucose absorption by delaying degradation of complex
carbohydrates in the gastrointestinal tract;87 pramlintide,
which slows gastric emptying and thus delays glucose
absorption;88 and the bile-acid-binding resin colesevelam,
which lowers cholesterol and modifi es release of other
gastrointestinal peptides that can reduce plasma
concentrations of glucose. 89
Incretin-related products are designed to mimic or
augment the action of GLP-1 and GIP, which are released
by the intestine. GLP-1 receptor agonists are peptides
with longer half-lives than GLP-1, whereas dipeptidyl
peptidase 4 (DPP4) inhibitors block the action of DPP4,
which is responsible for rapid degradation of GLP-1 and
GIP.90 Improvement of the pharmacokinetics and
pharmaco dynamics of incretin-based drugs is under
investigation to reduce dosing and to improve glucose
control.91 Although not completely understood, infusion
of large doses of GLP-1 intravenously can normalise
glucose concentrations with less nausea or vomiting—
adverse eff ects that can be dose limiting and prevent
normalisation of glucose concentrations—than for
subcutaneous administration.92,93 Whether new drugs
can further improve glucose lowering and reduce nausea
and vomiting remains unknown. In addition to the clear
eff ect of these drugs on improvement of glycaemia,
incretin-related products might also have benefi cial
eff ects on the cardiovascular system,94,95 although
fi ndings from the fi rst two of a series of intervention
studies showed a neutral eff ect.96,97 Incretin-related
medications have been purported to increase the risk of
acute pancreatitis; this suggestion is based on fi ndings
from studies that used the inherently biased
pharmacovigilance and administrative databases.98–101
More recently, GLP-1 receptor agonists and DPP4
inhibitors have been postulated to cause malignant
transformations in the pancreas. However, this
suggestion was based on histological assessments of a
very small number of samples from brain-dead organ
donors that were inadequately matched with controls for
several crucial variables.102,103 Importantly, despite
Figure 3: Drugs to treat type 2 diabetes
(A) The rate of introduction of new classes of drugs has accelerated during the past 20 years. Two classes (animal
insulin and inhaled insulin; red) are essentially no longer available as therapeutics. (B) Di ff erent classes of drugs act
on diff erent organ systems. Insulin is a replacement for the natural product of islet β cells. Classic organ systems
that have been targeted for decades comprise the pancreatic islet, liver, muscle, and adipose tissue. Non-classic
targets have been focused on recently, and include the intestine, kidneys, and brain. DPP4=dipeptidyl peptidase 4.
SGLT2=sodium–glucose co- transporter 2. GLP-1=glucagon-like peptide 1.
1940 1950 1960 1970 1980 1990 2000 2010
Sulfonylurea antidiabetics
Metformin
Human insulin
α-glucosidase inhibitors
Insulin analogues
Thiazolidinedione antidiabetics
Glinides
GLP-1 receptor agonists
Pramlintide
Inhaled insulin
DPP4 inhibitors
Colesevelam
Bromocriptine
SGLT2 inhibitors
1920 1930
Animal insulin
00
5
10
15
Cla
sses
of glu
cose
-low
erin
g d
rugs
Year
A
Classic Less classicB
Sulfonylurea antidiabetics
Glinides
GLP-1 receptor agonists
DPP4 inhibitors
Insulin
Lifestyle modification
Metformin
Thiazolidinedione antidiabetics
α-glucosidase inhibitors
Pramlintide
Colesevelam
SGLT2 inhibitors
Bromocriptine
See Online for appendix

Metformin
Reduces hepatic glucose production
Improves peripheral glucose utilzation
Reduces plasma glucose and insulin levels
Improves lipid profile
Promotes moderate weight loss

Pioglitazone, rosiglitazone
Binds to PPAR – γ
Reduces insulin resistance
Promote redistribution of fat from central to peripheral

Stimulate insulin secretion
Act on ATP – sensitive potassium channel on the β – cell
Most effective in Type II diabetics onset < 5 years

Sulfonylureas
Reduce fasting and post prandial glucose
Increase insulin acutely
Hypoglycemia can be related to delayed meals, increased physical activity, alcohol intake, renal insufficiency

Incretins
Amplify glucose – stimulated insulin secretion
Mimic or augment the action of GLP – 1 and GIP
GLP – 1 analogue or GLP – 1 receptor agonist Exanatide
Gila monster saliva
Liraglutide

DPP – IV inhibitors
Inhibit degradation of native GLP – 1
Promote insulin secretion
Absence of weight gain and hypoglycemia
Have preferential effect on post prandial glucose

α – glucosidase inhibitors Slow glucose absorption
Delay degradation of complex carbohydrates
Pramlintide
Slows gastric emptying
Colesevelam Lowers cholesterols
Modifies release of GI peptides that reduce plasma [glucose]

Inhibitors of Sodium – glucose co transporter 2
Increases urinary glucose excretion
Inhibits SGLT 2 reabsorption of glucose
Dapagliflozin and canagliflozin available
Reduce plasma glucose, body weight and BP

Parameter Normal Target
Pre – prandial plasma glucose (mg/dL) < 100 90 – 130
2 –hr post – prandial plasma glucose (mg/dL)
< 140 < 160 – 180
Bedtime plasma glucose (mg/dL) < 120 110 – 150
Hemoglobin A1c (%) < 6 < 7
LDL cholesterol (mg/dL) < 130 < 100
HDL cholesterol (mg/dL) > 40 (m), > 50 (w) > 45 (m), > 55 (w)
Fasting triglycerides (mg/dL) < 150 < 150
Blood pressure (mmHg) < 140/90 < 130/80

Sugar = 28.8g
Sugar = 14.8g
Sugar = 21.7g


Diabetic Ketoacidosis (DKA)
Hyperosmolar Hyperglycemic state (HHS)

Insulin deficiency
Increased counter – regulatory mechanisms Glucagon
Catecholamines
Cortisol
Growth hormone

Triad of hyperglycemia, ketosis and acidemia
Mortality is < 5% but remains most common cause of death in young people

Blood glucose > 250 mg/dL (13.8 mmol/L)
pH < 7.30
Serum bicarbonate < 18 mmol/L
Anion gap > 10
Ketonemia

DKA forms rapidly Symptoms may be present for several days before
ketoacidosis forms
Presenting symptoms
Polyuria, polydipsia, weight loss
Vomiting and abdominal pain

Physical signs
Increased respiratory rate
Kussmaul breathing
Fruity breath
Evidence of dehydration with hypotension Fluid depletion of 5 – 8 L

Diagnostic criteria [Glucose], pH, [bicarbonate], ketones, osmolality
Electrolyte abnormalities Sodium
Pseudohyponatremia Glucose and triglyceride elevation
Potassium Loss and cellular shifts
Magnesium
Phosphate High levels at presentation with decreases with DKA treatment

Correct fluid depletion
Decrease blood glucose levels
Correct electrolyte imbalance
Treat precipitating causes

Isotonic saline (0.9% normal saline)
First hour aim to restore renal perfusion
Rate of fluid infusion depends on clinical status
Corrects blood glucose and plasma osmolality

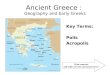
Severe hypovolemia Mild dehydration Cardiogenic shock
Administer 0.9% normal saline at
1L/hour
Hemodynamic monitoring/pressorsEvaluate corrected
Sodium (Na+)
Serum Na+ high Sodium Na+ normal Sodium Na+ low
0.45% NaCl (250 – 500 ml/hr) depending on
hydration status
0.9% NaCl (250 – 500 ml/hr) depending on
hydration status
When glucose reaches 200 mg/dL, change to 5% dextrose with 0.45% NaCl at 150 – 250 ml/hr

Lowers blood glucose Increases peripheral glucose utilization
Decreases hepatic glucose production
Lowers ketones
Inhibits release of free fatty acidsCorrects acidosis

Dose of insulin
Intravenous Bolus 0.1 U/kg
Infusion at 0.1 U/kg/hr
Subcutaneous Rapid acting insulin
0.3 U/kg, then 0.2 U/kg one hour later
0.2 U/kg subcutaneous every two hours
If serum glucose does not fall by 50 – 70 mg/dL in first hour, double dose of insulin

Alternatives
Low dose infusions as effective as standard
Randomized controlled trial Compared load with infusion, no load, and no load with twice
the infusion dose
0.14 U/kg/hr
Longer time to reach peak free insulin levels
No differences in times to reach glucose < 250 mg/dL, pH = 7.3, and HCO3 > 15 mmol/L

Aim to correct glucose to 200 mg/dL
Reduce insulin infusion to 0.02 – 0.05 U/kg/hr
Give rapid acting insulin at 0.1 U/kg sc every 2 hours
Keep serum glucose at 150 – 200 mg/dL until DKA resolves

Start after 1st liter of fluid
Aim to maintain concentration at 4 – 5 mmol/L
K+ < 3.3 mmol/L Hold insulin
Give 20 – 30 mEq/hr until K+ > 3.3 mmol/L
K+ > 5.3 mmol/L
Do not give K+, check serum K+ every 2 hours

Rarely need > 20 mEq K+/500 mls of fluid
If serum K+ > 3.3 and < 5.3 Give 20 – 30 mEq K+ in each liter of IV fluid

Replacement remains controversial
RCT’s have not shown clear benefit
Experts advise use if pH < 7
Worsens hypokalemia
NaHCO3 (100 mmol) in 400 ml H2O with 20 mEq KCL over 2 hours

No clear benefit from iv replacement
Can be harmful
If needed replace with oral forms

Caused by an inadequacy of insulin
High mortality As high as 15%
Higher in elderly

Blood glucose > 600 mg/dL (> 33.3 mmol/L)
pH > 7.30
Bicarbonate > 15 mmol/L
Serum osmolality > 320 mOsm/kg
Small amount of ketones may be present

Correct fluid depletion
Decrease blood glucose levels
Correct electrolyte imbalance
Treat precipitating causes

Severe hypovolemia Mild dehydration Cardiogenic shock
Administer 0.9% normal saline at
1L/hour
Hemodynamic monitoring/pressorsEvaluate corrected
Sodium (Na+)
Serum Na+ high Sodium Na+ normal Sodium Na+ low
0.45% NaCl (250 – 500 ml/hr) depending on
hydration status
0.9% NaCl (250 – 500 ml/hr) depending on
hydration status
When glucose reaches 300 mg/dL, change to 5% dextrose with 0.45% NaCl at150 – 250 ml/hr

Regular insulin
Bolus dose of 0.1 U/kg
Intravenous infusion of 0.1 U/kg/hr
If serum glucose does not fall by 50 – 75 mg/dL in the first hour, double the infusion dose
When serum glucose reaches 300 mg/dL, reduce insulin infusion to 0.02 – 0.05 U/kg/hr.
Aim to keep serum glucose 250 – 300 mg/dL until patient is mentally alert

Glucose every hour until stable
Serum electrolytes, BUN, serum creatinine, pH (venous), osmolality every 2 – 4 hours depending on severity of illness

Hypoglycemia
Hypokalemia
Cerebral edema
Non cardiogenic pulmonary edema

Lower limit of normal plasma glucose 70 mg/dL (3.9 mmol/L)
Hypoglycemia occurs at < 50 – 55 mg/dL
Diabetic Hypoglycemia occurs at < 63 mg/dL

Neurogenic Tremor
Palpitations
Anxiety/arousal
Sweating
Hunger
Paresthesias
Neuroglycopenic
Cognitive impairment
Behavioral changes
Psychomotor abnormalities
Seizure
Coma

Pallor
Diaphoresis
Rise in heart rate and systolic blood pressure
Transient neurological deficits

Glucose Oral carbohydrate
Fruit juice, dextrose drink
Simple sugars Buccal absorption from honey, chewable toffees or candy
Complex carbohydrates Meal substitutes, biscuits, bread
Parenteral glucose IV dextrose 50%, 25%, 10%, 5%

Glucagon 1 – 2 mg IM or sc
IV Hydrocortisone
SC adrenaline
SC terbutaline

Primarily disease of children treated for DKA
Associated mortality rate of 20 – 40%
Clinical features
Headache, lethargy, decreased arousal
Rapid neurological deterioration Seizures, incontinence, bradycardia, respiratory arrest

Avoiding cerebral edema Gradual replacement of sodium and water deficits
Addition of glucose to the solution once serum levels reach 200 mg/dL in DKA or 250 – 300 mg/dL in HHS
Maintain serum glucose in HHS at 250 – 300 mg/dL until hyperosmolality and mental status improve
Treatment with mannitol (0.2 – 1.0 g/kg) or 3% hypertonic saline (5 – 10 ml/kg over 30 mins.)

Rare complication of DKA treatment
Hypoxemia Reduced colloid oncotic pressure
Increased lung water content and decreased lung compliance
Pulmonary edema Higher risk if widened alveolar – arterial gradient noted on initial
ABG

DKA resolution Serum glucose < 200 mg/dL
Serum anion gap < 12
Serum bicarbonate > 18 mmol/L
Venous pH > 7.30
HHS
Serum glucose 250 – 300 mg/dL
Mentally alert
Plasma osmolality < 315 mOsm/kg

If known diabetic, give previous insulin dose
Insulin naïve patients
Multi – dose insulin regimen
0.5 – 0.8 U/kg/day
Timing of switch Rapid acting sc insulins 15 – 30 mins
Regular insulin 1 – 2 hours
Intermediate and long acting longer with a gradual taper of infusion

Before breakfast 2/3 of total daily dose
1/3 as rapid acting insulin
2/3 as intermediate acting insulin
Before dinner 1/3 of total daily dose
1/3 as rapid acting insulin
2/3 as intermediate acting insulin

Diabetes Mellitus treatment goal to reduce hyperglycemia and prevent long term complications
Diabetic emergencies: DKA and HHS
Treatment goals in DKA and HHS correct fluid depletion and electrolyte losses, reduce hyperglycemia, treat underlying precipitants
During treatment watch for complications including hypoglycemia


Kumar P, Clark M. Clinical Medicine. Edinburgh: Elsevier Saunders; 2005
Kahn RC, Weir GC, King GL et al. Joslin’s Diabetes Mellitus. Philadelphia: Lippincott Williams & Wilkins; 2005
Kolwicz Jr. SC, Tian R. Glucose metabolism and cardiac hypertrophy. Cardiovasc Res. 2011; 90 (2): 194 – 201
Goldman L, Schafer AI. Goldman’s Cecil Medicine, 24th Ed. Elsevier; 2012
Jellinger PS. Metabolic consequences of hyperglycemia and insulin resistance. Clin Cornerstone. 2007; 8 (7): S30 – 42
Mealey BL. Diabetes Pathophysiology. American Health Network [Diabetes Health Center]. 2000 – 2006. Available at http://www.health.am/db/diabetes-pathophysiology/
Kahn SE, Cooper ME, Del Prato S. Pathophysiology and treatment of type 2 diabetes: perspectives on the past, present and future. Lancet. 2013. doi: 10.1016/S0140-6736(13)62154-6

Longo DL, Fauci AS, Kasper DL, Hause SL, Jameson JL, Loscalzo J. Harrison’s Principles of Internal medicine, 18th edition: www.accessmedicine.com
Kearney T, Dang C. Diabetic and endocrine emergencies. Postgrad Med J. 2007; 83 (976): 79 – 86
Kitabchi AE, Nathan DM. Treatment of diabetic ketoacidosis and hyperosmolar hyperglycemic states in adults. In UpToDate, Post TW (Ed), UpToDate, Waltham, MA. (Accessed March 15, 2014)
Kitabachi AE, Murphy MB, Spencer J, Matteri R, Karas J. Is a priming dose of insulin necessary in a low-dose insulin protocol for the treatment of diabetic ketoacidosis? Diabetes Care. 2008; 31(11): 2081 – 5
Sivanandan S, Sinha A, Jain V, Lodha R. Management of diabetic ketoacidosis. Indian J Pediatr. 2011; 8(5): 576 – 84
American Diabetes Association. Standard of Medical Care in Diabetes – 2010. Diabetes Care. 2010; 33(1): s11 – s61
Service FJ, Cryer PE. Hypoglycemia in adults: Clinical manifestations, definitions, and causes. In: UpToDate, Hirsch IB (Ed), UpToDate, Waltham, MA (Accessed November 27, 2013)